Recommendations
The Summit received almost 700 research recommendations from various sources before the cut-off date, October 17, 2017 (see chart below). A careful review of the recommendations indicated that they fall into 12 broad themes as described in the Summit Final Report and the presentation that was made to the NAPA Advisory Council on April 27 2017.
Currently Available:
CROSS-CUTTING THEME PAPERS
FINAL REPORT
NAPA ADVISORY COUNCIL PRESENTATIONS
PUBLIC COMMENTS
SESSION PAPERS
STAKEHOLDER PAPERS
Comments and questions, or alerts to broken links, should be sent to napa@hhs.gov.
VIDEO PRESENTATION: Final Report to the NAPA Advisory Council
Rohini Khillan and Laura Gitlin discuss the Care Summit Final Report. [Video]
National Research Summit on Care, Services, and Supports for Persons with Dementia and Their Caregivers: Report to the National Advisory Council on Alzheimer's Research, Care, and Services
This report to the Advisory Council on Alzheimer's Research, Care and Services presents the results of the first National Research Summit on Care, Services, and Supports for Persons with Dementia and their Caregivers (the Summit), held on the National Institutes of Health (NIH) campus on October 16-17, 2017. The Summit complements the National Institute on Aging's (NIA) Alzheimer's Disease Research Summits and the National Institute for Neurological Disease and Stroke (NINDS) Alzheimer's Disease Related Dementias Summits, and follows the same general structure. These conferences are coordinated planning efforts that respond to the National Plan to Address Alzheimer's Disease, first released in 2012 and now updated annually. Following the example of the earlier NIA and NINDS Summits, this Summit was intended to set national research recommendations that reflect critical scientific priorities for research on care and services for persons with dementia and their families. The Steering Committee and organizers of this Summit solicited input from nationally and internationally recognized experts and researchers, and other public and private sector stakeholders, to develop prioritized recommendations. The recommendations included in this report will help guide investments by a number of public and private stakeholders in the field of care, services, and supports, and will provide the structure for future summits. [HTML Version] [PDF Version] Originally dated April 27, 2018; small changes were made on May 16, 2018.
Main Summit Recommendations
This paper is the recommendations section of the report National Research Summit on Care, Services, and Supports for Persons with Dementia and Their Caregivers: Report to the National Advisory Council on Alzheimer's Research, Care, and Services. [HTML Version] [PDF Version] Originally dated April 27, 2018; small changes were made on May 16, 2018.
Additional presentations about the Care Summit were made at NAPA Advisory Council meetings leading up October 2017. All presentation materials are available at the NAPA Advisory Council on Alzheimer's Research, Care, and Services Meetings Page. Listed below are presentations that specifically discuss the recommendations received during the Summit.
NAPA ADVISORY COUNCIL PRESENTATION: Final Report to the NAPA Advisory Council
This presentation was made to the NAPA Advisory Council on April 27, 2018 describing the final recommendations. [HTML Version] [PDF Version] [Video]
NAPA ADVISORY COUNCIL PRESENTATION: Overview and Recommendations Presentation to the Advisory Council on Alzheimer's Research, Care, and Services
A careful review of the recommendations indicated that they fall into 11 categories, or 'buckets' as described in this presentation that was made to the NAPA Advisory Council on October 27, 2017. [HTML Version] [PDF Version] [Video]
CROSS-CUTTING THEME PAPER: Diversity Recommendations
This paper is a summary of the research recommendations that were developed by the Diversity Cross-cutting Chair. [PDF Version]
CROSS-CUTTING THEME PAPER: Etiology Recommendations
This paper is a summary of the research recommendations that were developed by the Etiology Cross-cutting Chair. [PDF Version]
CROSS-CUTTING THEME PAPER: Technology Recommendations
This paper is a summary of the research recommendations that were developed by the Technology Cross-cutting Chair. [PDF Version]
CROSS-CUTTING THEME PAPER: Women's Issues Recommendations
This paper is a summary of the research recommendations that were developed by the Women's Issues Cross-cutting Chair. [PDF Version]
STAKEHOLDER GROUP PAPER: Family Caregiver Stakeholder Workgroup Research Recommendations
This report is a summary of the research recommendations that were developed as a result of six meetings with the members of the Family Caregiver Stakeholder workgroup. [PDF Version]
STAKEHOLDER GROUP PAPER: Research Recommendations: Top 6 Outcomes that Matter
The Stakeholder Group of Persons Living with Dementia includes 12 retired professionals from diverse backgrounds who are each committed to advocacy about dementia care, services and research. All members experience mild or moderate symptoms of a cognitive disorder. The group is co-chaired by two persons living with dementia and the leadership also includes a geriatric psychiatrist and a project coordinator experienced in leading groups of people in the early stages of a cognitive disorder. To prepare these research recommendations, monthly 90-minute meetings were conduced by videoconference, and each meeting included one or more guest senior research leaders. Between monthly meetings, a subgroup met to address logistical concerns regarding the preparation of research recommendations, responses to requests for input about specific research questions, plans for travel to participate in the Summit, and preparations to support persons living with dementia who attend the Summit. Time limitations and the personal experiences of the Group members resulted in an emphasis on research recommendations addressing early stages of illness. The Group produced recommendations categorized into the general areas of research on: new care practices to improve dementia treatment; access to care and services; strategies to promote participation in clinical trials; the experience of living with a cognitive disorder; best practices for working with family members, caregivers and proxy decision-makers; and, use of new terminology and language for public education. After a voting process, the Group decided on the following "Top 6 Outcomes that Matter." [PDF Version]
STAKEHOLDER GROUP PAPER: Final Recommendations on Outcomes that Matter
This report gives a summary of two conference calls the Stakeholder Group held, and a list of the recommendations put forth to the Summit. [PDF Version]
STAKEHOLDER GROUP PAPER: Provider Stakeholder Workgroup Recommendations
This paper outlines the Provider Stakeholder Group recommendations. [PDF Version]
STAKEHOLDER GROUP PAPER: Provider Stakeholder Workgroup Recommendations II
This paper provides accompanying comments for the Provider Stakeholder Group recommendations. [PDF Version]
STAKEHOLDER GROUP PAPER: Workforce Gaps in Dementia Education and Training
Workforce was identified by the Summit Steering Committee as one of the key stakeholder groups that should recommend research focus areas for educating and training the workforce. Informal and formal caregivers are an integral part of the dementia care workforce. More broadly, informal caregivers are defined as family members, neighbors, friends, and fictive kin who provide unpaid care, while formal caregivers, covering the spectrum from home health aides to health care professionals, have some training in the care of persons living with dementia and are paid for their services. This paper, written by the Workforce Development Workgroup (WDW), focuses on gaps in educating and training the workforce to address the goals of the Summit. The WDW is an interprofessional team of health professionals from academia, professional organizations, and the federal government with expertise in dementia workforce development. [PDF Version]
SESSION RECOMMENDATIONS: Summit Recommendations from the Plenary Session: Nomenclature, Words Matter
This paper is a summary of the research recommendations that were developed by the Chair of the Plenary Session: Nomenclature, Words Matter. [PDF Version]
SESSION RECOMMENDATIONS: Summit Recommendations from the Summit and Session Chairs: Day 3 Review Session
This paper is a summary of the Recommendations Review Session. This Session was held on October 18 (Day 3), and was attended by the Summit Co-Chairs and each of the Session Chairs. [PDF Version]
NOTE: The Public Comments included on this page are not an endorsement of the views or information by National Alzheimer's Project Act, its Advisory Council members, the Administration, or the federal agencies and organizations involved in this Summit.
|
Viewers and attendees were asked to share with their twitter followers that they were participating in the Summit using the hashtag "Dementiacaresummit". [link to #Dementiacaresummit feed]
|
|
|
Congratulations on convening the first-ever National Research Summit on Care, Services, and Supports for Persons with Dementia and Their Caregivers! We thought it was an excellent program and we were happy to be in attendance.
The Alliance for Aging Research (http://www.agingresearch.org/) is the leading national nonprofit organization dedicated to accelerating the pace of scientific discoveries and their application to vastly improve the universal human experience of aging and health. We appreciate the opportunity to offer the following ideas for the steering committee's consideration in the summit summary and recommendations:
- We recommend that the National Advisory Council on Aging expand its ex officio membership to include a representative from CMS and a representative from the FDA. These agency perspectives would be exceptionally valuable for consistent identification of research gaps in dementia care research, and to offer overall comment and guidance on the advisory council.
- We recommend that CMS work with the NIA, AHRQ, and relevant stakeholders to conduct a review of the established research on REACH, Savvy Caregiver, and other family caregiver evidence-based training programs to determine what additional research/evidence would be needed to either approach CMMI for a pilot or demonstration program; or, what additional evidence would be needed to incorporate one or more programs as a covered benefit.
- When Medicare expanded in 1972 to include individuals with significant disabilities, Congress stipulated that people with disabilities must first receive Social Security Disability Insurance (SSDI) for 24 months before gaining Medicare eligibility. This legislation was created to keep costs down and to avoid replacing coverage for a disabled worker still receiving benefits under a private group health plan. Since SSDI recipients are unable to work, they cannot access the principal source of coverage for people under 65--employer-sponsored insurance. Instead, people in the Medicare waiting period generally obtain coverage if they qualify for Medicaid, or if they can pay the premium, they continue under their former employer's plan under COBRA. There are significant research gaps on the impact of this 24-month waiting period in general, and specifically for SSDI early-onset beneficiaries, incluing: on the health status of these SSDI early-onset beneficiaries during the 24-month period; their access to coverage; as well as on the economic impacts to beneficiaries, the Medicaid program, and employer-based plans. We request that the summit steering committee specifically recommend that the Division of Behavioral and Social Research (DBSR) at the National Institute on Aging (NIA) develop an RFP to explore this issue.
- In May 2011, the Office of Inspector General (OIG) released a widely publicized report, "Medicare Atypical Antipsychotic Drug Claims for Elderly Nursing Home Residents," revealing that 83% of atypical antipsychotic drug claims were prescribed for nursing home residents without a US Food and Drug Administration (FDA) indication, and that 88% of claims were related to use in residents with dementia, for whom antipsychotics are associated with an increased risk of mortality as specified in the FDA black box warning. At a hearing of the U.S. Senate Special Committee on Aging on November 30, 2011, Inspector General for the Department of Health and Human Services Daniel Levinson testified that nursing home residents often received antipsychotic drugs in ways that violated federal standards and that CMS should "hold nursing homes accountable." The OIG report gained widespread attention from the media, nursing home advocacy organizations, and legislators from both parties. In response, CMS launched the National Partnership to Improve Dementia Care in Nursing Homes in March 2012, with a focus on "protecting residents from being prescribed antipsychotic medications unless there is a valid, clinical indication and a systematic process to evaluate each individual's need." By the end of 2016, the percentage of long-term residents receiving antipsychotic therapy had decreased to 16%, a 33% relative reduction. However, at least two issues remain that the summit research recommendations could seek to resolve.
- What are the corresponding percentages of residents with dementia in nursing homes during this same period? These percentages would help inform whether the number/percentage of people with dementia using antipsychotics went down due to changes in prescribing practices, or if some facilities may have reduced the number/percentage of residents with dementia who were taking those medications. The numbers CMS currently presents otherwise assumes that the percentage of dementia residents stays consistent during the time periods covered. Information on prescriptions for other psychotropic medication by medication class among this population during this time period should also be explored.
- Nursing homes are notoriously understaffed. Studies have shown that more staff leads to better care, but employees are often overworked and turnover can be high. Federal law requires Medicare and Medicaid certified nursing homes to have a registered nurse (RN) on duty at least 8 hours a day, 7 days a week; and a licensed nurse (RN or LPN) on duty 24 hours a day. However, there are no minimum staffing levels for nurse's aides, who provide most of the day-to-day care. Instead, nursing homes are required "to provide sufficient staff and services to attain or maintain the highest possible level of physical, mental, and psychosocial well-being of each resident." In addition, nursing homes must provide a minimum of 75 hours of training for the aides. The important factor in improving quality of care is the amount of nurse time each patient receives. If a nursing home met only the federal nurse staffing requirements described above, a resident would receive 20 minutes of nurse time per day. According to a study, the key to improving nursing home staffing levels is increasing state standards. The study by Charlene Harrington, a UCSF School of Nursing professor, found that states with the highest standards for nursing staff levels are the only states where nursing homes have enough staff to prevent serious safety violations. According to the study, the act of raising the state minimum staffing ratio has a direct impact on the quality of care nursing home residents receive. The Division of Geriatrics and Gerontology at the NIA should explore these issues with CMS to inform policies on dementia training, staff ratios, and psychotropic medication use in nursing homes.
- There are also significant research gaps regarding utilization, health outcomes, and comparative effectiveness of community-based care: including respite care, adult day care, home care, and caregiver training programs. AHRQ could conduct an evidence review of existing research, and then work with PCORI and CMS/CMMI to explore opportunities for pilot programs.
- Last, the summit steering committee should consider including a recommendation to study the potential impact of proposed cuts to the Medicaid program on people with Alzheimer's disease and related dementias. According to a Kaiser Commission on Medicaid and the Uninsured (KCMU) analysis of pooled 2010-2012 Medical Expenditures Panel Survey data, about one in four (24%) adults living with AD/ADRD in the community rely on Medicaid coverage over the course of a year. Medicaid covers services that Medicare does not, such as long-term care in nursing homes, assisted living, and at-home care. Home- and community-based long-term care provides assistance with routine self-care tasks, such as eating, bathing, and dressing, and household activities, such as preparing meals, managing medication, and doing laundry. Many of our nation's seniors are living in poverty (10%) or near poverty (22%) and are unlikely to be able to afford paid help. Medicaid coverage helps many of the most vulnerable adults with AD/ADRD in our communities, and its necessity is only going to increase with the 85 and older age group--the group most likely to need long-term care--increasing by almost 70 percent over the next two decades. What would proposals to change Medicaid financing by limiting federal funding to states through per capita caps mean for this population? Such changes would likely force states to cut eligibility, reduce benefits, and lower provider reimbursement, particularly for AD/ADRD high-cost enrollees who need substantial services under the program, but we don't know for sure. Additionally, what would be the impact on states with higher aging populations?
Thank you for considering our ideas, and we look forward to seeing the summit summary and recommendations.
|
|
|
With apologies if this is reflected already in other folks' recommendations, but I'd be grateful if we could consider including in the writing group work consideration of encouraging research into this two-parter:
- Does the Timely, Accurate, Compassionate and Actionable ("TACA") communication of detection and diagnosis information from clinician to patient/caregiver make a difference in outcomes? (I see this as related to, but much deeper than the IDEAS study -- i.e. not just diagnosis making a difference but specifically differentiating my push for "TACA" against the routinely late, sometimes inaccurate, often insensitive, and usually lacking in action steps diagnois.)
- If so, how can we train more clinicians both in how to do "TACA" detection and diagnosis and then persuade them to actually do detection and diagnosis in this way?
I understand that there isn't a formal standard -- much less curriculum or model -- for what I call "TACA." But I hope/gatther you get my point about wanting research on whether we can/should replicate the way some docs do detection and diagnosis to a wider level of adoption/implementation among more docs.
|
|
|
Several different comments within the stakeholder summaries as well as during the summit have highlighted economic strain especially for families and friends providing unpaid care. Likewise the importance of a livable wage for the frontline care provider.
There is evidence from the NIA supported HRS that caregiving increases the risk of poverty and that 70% of the workforce in the bottom 25% have no paid time off--(regardless of purpose)
PLease be sure to highlight the issue of financial strain in research outcomes as well as consider experiments in how we can involve other key stakeholders like employers, etc. What can we do to help advance economic improvements in these key groups.
I don't know if we know about what happens with these individuals--but iif we believe in the social determinants of health I am concerned that we are creating future generations with significant health problems etc. and even dementia.
|
|
|
Reach out to Long-term Care Insurance industry with research-based, patient-centered data on the benefits of at-home care for persons with dementia. In their coverage, they still do favor nursing home care over at-home care which only gets 75% of maximum daily amount as compared to nursing home.
|
|
|
We would like to submit into the conference materials for the committee and attendees a description of a community based comprehensive dementia care program that integrates medical care for persons living with dementia with education, training and support for their caregivers. MemoryCare has 17 years of experience incorporating most of the best practices in dementia care identified during the National Research Summit on Care, Services and Supports for Persons with Dementia and their Caregivers.
We serve suburban and rural areas throughout the western North Carolina. We do not have formal academic ties that would make an RCT possible internally but welcome others to study this program and the descriptive and financial/value outcomes that we detail in the attached paper. Our internal tracking data over the past 5 years shows consistent savings to the health care system and high levels of caregiver satisfaction. We welcome sharing more about this work.
Quality Dementia Care: Integrating Caregivers Into a Chronic Disease Management Model, http://journals.sagepub.com/doi/10.1177/0733464815589986
|
|
|
Just want to bring up the issue that poor people with dementia face when they don't have a caregiver. If they had financial resources, they could hire private fiduciaries. My understanding is that without a trusted friend or family member to act as agent, poor people with dementia do not have resources to engage in ACP to the extent that people with money have. I wonder if there is a way to collaborate with colleagues in legal sector to offer more options?
|
|
|
I am wondering if there are mechanisms (regulations or incentives) to make EMRs more useful and integrated across health systems and community based organizations. The goal would be to enable integrated collaborative care plans that are easy to access and update by all stakeholders including patients and families. Are there other countries have better EMR technology that's integrated and accessible? It is very costly and inefficient for care programs to pay to develop individual software care management programs.
|
|
|
Just wanted to share this website that might offer a mechanism for replicating the VA foster care program in the community. https://room2care.com/
|
|
- There are clearly different dementia "phenotypes" including Alzheimer's disease, FTD, and Lewy body dementia. While there are overlapping symptoms, at least early on, the clinical syndromes are more distinct. As such, from a research standpoint, the different dementias need to be studied separately. This is as true for caregiver research for caregiver research as it is for treatment/prevention research.
- Support groups are a powerful counseling/psychotherapy tool to reach groups of persons with dementia, their caregivers, or both. I am hoping that any RFAs generated from this summit will include research on support groups.
- I direct a counseling program in which providers see persons with dementia and their family caregivers. We use a variety of psychotherapeutic approaches including mindfulness, Acceptance and Commitment Therapy (ACT), cognitive behavioral therapy, Eye Movement Desensitization & Reprocessing (EMDR), sand tray, and solution-focused or behavioral strategies. Hopefully, the RFAs will allow one to address the efficacy of a given intervention, or compare several entitites (randomizing pts to one intervention versus another for depression, for example).
- One group of caregivers not discussed during the summit are paid certified nursing assistants. CNAs do the majority of the work for individuals living at home with dementia. By and large, CNAs are minority women with a high school education or GED earning anywhere from minimum wage to $10-12. They usually participate in a brief educational program (may be a few days to a few months) before being placed with someone who often has middle to late stage dementia. Education interventions would be great to test in this population.
|
|
|
After attending the first day or the two day summit, and speaking with Michael Splaine, an available opportunity is being missed
It would seem that it might be very possible to have pause moments in the day after sets of recommendations are made and the live and on-line audiences could be asked to identify their top 1-3 and any recommendations that the person believes/feels would NOT be pursued. Adding in a option to provide space for rationale and degree of involvement or investment or other highlights --
Collecting this information, and then making this available to attendees, speakers, and sponsors for review and further refinement
Given the brain trust that is present both physically and on-line, much more could be done to engage the attendees/participants and provide feedback than the global message to Tweet or E-mail
|
|
|
Based on many statements made during the Care and Support Research Summit, please consider adding to the national research agenda, the impact of communities that work to enhance supports and access within all sectors of community in order to support and extend the independence of a person who is living with dementia and his/her caregiver e.g., dementia friendly communities. We currently have communities in 37 states working to became dementia friendly using best and emerging practice tools and resources provided by a collaboration called Dementia Friendly America, http://www.dfamerica.org.
We need to learn whether communities adopting dementia friendly practices extends independence and quality of life for people living with dementia, slows disease progression, avoids expensive unnecessary care, reduces more formal and expensive long term care and helps the caregiver sustain his/her role. Understanding the impact of supports in the broader community will be critical as we face shortages in LTC workers and lack of funding for LTSS. Many countries in the world are implementing dementia friendly communities, but no country has gauged its impact through a research study. Dementia friendly communities can also be a vehicle for clinical research recruitment and participation, especially in communities that are highly impacted by dementia, but not prone to participate in clinical research.
Dementia Friendly America and its partcipating communities across the U.S. stand ready to engage in shared research and has developed mulitple study aims to pursue this course of study.
|
|
|
Great summit and thank you for organizing and opportunity.
Fantastic recommendations on all fronts.
A thought if I may. In addition to the slides would there be compilation of recommendations and possibly an attempt to prioritize them with few focus/ action items across a specific period.
|
|
|
I watched Day 1 of the NIH Summit on October 16, 2018.
My question is: what is happening in the areas of qualitative rather than quantitative research?
Many of the research presentations focused on things that were scientifically verifiable with control groups, consistent group characteristics, etc.
The challenge as I see it is that there is very little uniformity in symptoms for people living with certain dementias such as FTD.
In fact, FTD is only a "probable" diagnosis, only confirmed at autopsy, so collecting a group of study participants "with" FTD is challenging in itself. Some families learn after autopsy that their loved one had a different type of dementia than the one suspected.
I encourage the NIH to explore other kinds of research which is more qualitative, such as focus groups etc who may be willing to experiment with interventions and report on their personal results.
|
|
|
I live with Alzheimer's disease.
Simply... the word Mild is hurtful to me. Whether with MCI or with Alzheimer's it waters down the level of my disability as if it is a mild disability.
When it comes to Salsa at a restaurant, there is mild, medium, and hot. Mild is the one with 'barely any, if any, heat.'
I understand that the word mild came into use on the clinical side, but the clinical side meets the 'patient' side at many points. Some of those points they bleed over out of the clinical world into my world.
I don't hear people saying 'I have mild cancer'. I do hear them describing it by stages. They say, "I have stage 3 cancer'.
Stages, of course, describe a continuum. Alzheimer's is a progressive disease, so it is also on a continuum. I tell people I have 'early onset' or 'early stage' Alzheimer's.
This allows for them to understand that I have a real, serious, disability. And that my disability is progressive, and that I am at a particular stage of that progression.
Using terms like mild, tell a non-clinically trained person that I have a disease but it isn't really a big deal... it is barely there. It is stagnant, not progressive. It is just mild. No real impact on my life. Just like my mild cancer...
I lost more than just some of my cognitive abilities to Alzheimer's I have lost my family, dogs, house, cars, career, and now live alone. I don't consider any of that mild.
Thank you for listening, the last time someone told me I had mild Alzheimer's I got pretty hot. So hot, I had to apologize once I cooled down.
|
|
|
This summit is awesome, I hope there are many more in the future!
Regarding technology that might enable persons with dementia remain independent longer and participate in research without a caregiver. This group at UC Berkeley has a startup that is doing great work to prevent falls in memory care facilities. It was not easily adopted by family caregivers who had concerns about privacy. But I think it could be used to evaluate function and sleep and perhaps for evaluating ways to modify the environment to make it more supportive! George Netscher, the lead scientist is a super genuine guy who sincerely wants to help people with dementia. I think he can!http://skydeck.berkeley.edu/portfolio_page/safelyyou/
The other technology I am excited about is being used by Kristine Williams a nurse scientist at U of Iowa. It is Bahavior Capture technology by Behavior Imaging. It records behavior and up to 30 min preceding behavior to help caregivers evaluate triggers. It can also be used for evaluating behavior and function for people without proxy historians. https://behaviorimaging.com/behavior-capture-mobile-kb-home/
|
|
R. Qiu | 10-16-2017
|
The programs in this summit (#DementiaCareSummit) are great. I am sure that everyone enjoyed the first day's meeting very much. I am looking forward to learning more tomorrow. Thanks for putting together this wonderful summit.
One interesting and important concept that was quite discussed today is the care partnership. Instead of emphasizing caregivers and care recipients in their respective perspectives, care partners might be better used with a focus on their engagements and active participation. This could be very encouraging and promising as demented patients would become more positive over the lifecourse, psychologically and behaviorally. This is particularly true for persons with dementia at their early stages. In Service Science, we are mainly concerned with the quality of service encounters, paying great attention to sequence effects, duration effects, rationalization effects, and perceived control. The same principle should be also applied here.
With the help of the fast advances of mobile computing, IoT, and machine learning, we should be able to make a difference in helping personalized the needed care for persons with dementia and their caregivers or care partners in an individual case in an efficient and cost-effective manner.
|
|
|
The National Study on Caregivers (NSOC) should change its sampling design to include family caregivers of older adults residing in nursing homes. This is important because most nursing home residents have dementia. Additionally, NSOC's prevalence estimate of family caregivers of older adults under-represents the estimated number of family caregivers of older adults--what these family caregivers do, and the impact of family care regardless of care setting.
|
|
|
The Research Summit on Dementia Care has raised many great questions. The level of sophistication is evidenced by the speakers' awareness of key issues for both valid science and meaningful implementation. I have noticed that the potential value of technology to assist caregiving has been touched on by several speakers and focused on by one. Several speakers spoke to the need to properly integrate any intervention into all the processes that support the individual needs or care recipients and caregivers.
What concerns me is the characterization of technology. The discussion seems to center around either the overgeneralized concept of technology or the far too specific concept of product/device. The Summit Issue Brief: "The Use of Assistive Technology to Reduce Caregiver Burden" seems to suffer from looking at the problem through these two polar constructs. Although all of the issues raised are relevant, perhaps the primary problem in the field is how to pose the question. The question should be, what combination of technologies can achieve meaningful benefits for one or more well-define subgroups of persons with dementia and their caregivers? If we can be more bold, I would ask, How do we develop a suite of technologies that will match the abilities of a human caregiver? Indeed, this is the best goal to strive for if we expect some success.
I have been part of a research group with this aim. We are a diverse group and the last point in the Issue Brief is a great description of what this area of research absolutely requires:
- interdisciplinary research: researchers in engineering, computer science, mathematics, and robotics would benefit from collaboration with professionals in gerontology, psychiatry,social work, nursing, and occupational therapy, with direct experience providing services to people with dementia living in the community.
|
|
|
Please consider the attached recommendations for the summit.
|
ATTACHMENT:
|
Develop and evaluate ways to support and maintain cognitive and functional abilities in persons with dementia.
- Convene an expert advisory group: the advisory group should identify approaches and interventions for this purpose that should be developed and evaluated; the advisory group should include persons with dementia, researchers, clinicians, service providers, and family caregivers.
- Focus first on approaches and interventions for persons in the early stages of dementia: initial efforts should focus on approaches and interventions to support and maintain cognitive and functional abilities in persons in the early stages of dementia because there has been relatively less research on such approaches and interventions for persons in the early stages of dementia than for persons in later stages of dementia.*
- Use outcome measures that evaluate the effect of the approaches and interventions on particular cognitive and functional abilities: such outcome measures should be used instead of global measures of cognition or functioning; positive outcomes for particular cognitive and functional abilities would be valuable for individuals with dementia even if outcomes for other cognitive and functional abilities or global outcomes are not affected.
- Conduct research interviews with persons with dementia: persons with dementia should be interviewed about the effects of the tested approaches and interventions, whether or not research interviews are conducted with family caregivers, clinicians, or service providers.
- Use sufficiently large and well-specified research samples: Samples for this research should be large enough and the characteristics of sample members should be specified in enough detail so that findings differentiate the effects of the evaluated approaches and interventions for persons who differ in age, gender, and etiology and stage of dementia.
- Design research that lasts long enough to provide useful findings: studies of approaches and interventions to support and maintain cognitive and function abilities should evaluate the approaches and interventions over long enough time periods that persons with dementia, family caregivers, service providers and funders of care, services, supports can use the findings to determine the value of the interventions.
- Consider a multi-funder or consortium-based initiative to support this research.
*Examples of approaches and interventions that could be evaluated include:
Goal setting interventions
Interventions to maintain safety in driving, alcohol and drug use, and the use of guns
Physical activity of various kinds
Volunteering as a buddy, mentor, or research participant
Art activities
Music activities
Nutrition counseling
Psychological counseling & support groups
Groups related to individuals' interests e.g., sports, gardening, museum visits
Meditation/mindfulness, yoga, and tai chi
Medical care for co-existing health conditions
|
|
|
Why is lack of recovery or maintenance of functional ability expected in a condition that is destroying the brain Why are we not considering a spectrum of support matching demonstrated abilities and retained points of interest
|
|
|
In DICE where do you add in the variable of task and task expectations in your triad if care provider, PLwD and environment??? Big missing piece and a key factor in symptom appearance
|
|
|
This is a comment on a central reason behind forced institutionalization of dementia patients, and the resulting family financial stress that results from nursing home costs. When a dementia patient is forced into long term care because they are too difficult to care for in the home, the costs range from $65K annually in Arkansas to $125K in New York.
These costs quickly consume the savings of the patient and their families. The caregiver's burden is often increased substantially as this financial stress increases and they approach bankruptcy. Medicaid leaves families with less the $20K savings in most states before it begins paying for long term care.
One of the central reasons dementia patients are forced into nursing homes is that they become bedfast and lose mobility. When a patient is confused and cannot consistently follow the caregiver's directions, they cannot be transferred to the wheelchair, commode, or shower without assistive technology (a transfer chair or patient lift).
The issues associated with bed confinement are difficulties with incontinence (changing briefs or diapers, clothes, and sheets) along with UTIs, decubitus ulcers, contractures, poor circulation, blood clots, and hypostatic pneumonia. Bed confinement and its resultant problems is often the central thing that forces dementia patients into costly nursing homes. So the central questions become:
How do dementia homecare dementia patients become bedfast, and what can be done to avoid this"?
The answers are:
Current assistive technologies are inadequate for home use, and improved assistive technologies need to be developed.
Existing transfer or repositioning chairs are too expensive costing $5,000-$15,000. They are therefore rarely used in the home. Patient (or "Hoyer") Lifts require two skilled caregivers, considerable space to use, smooth floors, and a large storage space. Patients can also be dropped if the device tips over during use or the sling chosen is the wrong size or type, or wrongly positioned under the patient. Though Medicaid will pay for rental of these devices, they are also rarely used in homecare.
A central concern of the Dementia Summit should therefore be how to support improved assistive technologies to reduce bed confinement and facilitate ADLs in the home. This will allow dementia patients to stay in homecare longer and help their families avoid financial stress. Better assistive devices that make transfer, showering, and toileting faster, safer and easier are needed for both home and institutional use.
At a recent RERC TeckSage conference (http://ipat.gatech.edu/events/techsage-state-science-conference) to "Identify the Needs of People Aging with Disability" at the Georgia Institute of Technology, the author asked the attendees "who in the field was working to design and develop better transfer and mobility devices? " The collective answer of these medical device experts was: "Someone in Japan might be working in this area but we were not sure who".
If dementia care is a $250B problem currently, it is unacceptable in the author's opinion that there is virtually no NIH support for R&D in this area (based on an extensive search of the NIH's Reporter database).
We therefore request that NIA Program Officers step up and change their priorities to address this critical need through new FOAs, RFAs, and targeted funding.
|
|
|
Three comments of note:
- Missing one LARGE stakeholder group -- EDUCATORS of health care professional groups, legal personnel, public service personnel, paraprofessionals, volunteer sectors, post-degree practitioners -- moving from what is known to what is done by those attempting to deliver support and care
- Missing a large group of People Living with Dementia as Stakeholders -- Those past the early stages who demonstrate difficulty participating in relationships and communicating in the current format and frame, although they are certainly involved and still trying frequently desperately to communicate their preferences, challenges, and discontent -- they have been left out of this program
- When will the leaders start staying true to the concept of DEMENTIA versus Alzheimers in their language and research
|
|
|
I am completing my last year at George Mason University in the Doctor of Nursing Practice program. Upon graduation, I will also be credentialed as an Adult Geriatric Nurse Practitioner. I have a strong interest in dementia care, as well as caregiver burden. My final project that I will defend in April looks at how individualized music for those with dementia can decrease caregiver burden. I'm also assisting a professor at GMU to hopefully write individualized music into the Virginia Dementia Care Plan. If there are any projects where I may be of assistance I would love to help in any way. I am able to conduct literature searches, complete literature and systematic reviews, and take notes among many other tasks. Thank you for your time and I look forward to being in touch.
|
|
|
I'd like to submit a story of my husband and my journey with FTD.
|
ATTACHMENT:
|
My husband, Jack and I met and fell in love in 1987. He had served in the Marines and worked construction before we met but spent most of his life working in the field of caregiving. The final years he was able to work he was a CNA and activities assistant at a care facility and took wonderful care of elderly and dementia patients.
Jack was a loving, funny and kind man but eventually excessive drinking made him very depressed. He went to alcohol rehab three times in his late 40's and in 2009, the year he turned 50, a counselor convinced us to live a part until he fully recovered. He lived in a clean and sober house and went back to college earning straight A's and an AAS degree. He set up a routine including going to an early meeting, walking for miles each day and calling me each morning and evening.
When he moved back home, he was different but I assumed it was because he was sober and we'd been living apart. I decided to just be happy he was sober, content and healthy. I now see the beginnings of bvFTD in his behaviors and changes, even many years earlier.
January of 2015, at 56, he wasn't working, had quit going to school and was watching TV and sleeping a lot. Some of his behaviors reminded me of when he was drinking but I was sure he wasn't. One day he bought $500 of frozen meat from a door-to-door salesman (which now I know is common behavior for someone bvFTD but at the time I was mad and so confused). By summer I told him he had to get a job or move out. He got a job but was let go after first day. That weekend I drove him 200 miles to stay with friends until he could get his life back on track.
The next three weeks it became clear to his good friends there was something very wrong. He wasn't his old friendly, funny self. The final straw was his car being towed because he ran out of gas and walked away leaving it in the middle of a busy road. I asked his friend to get him on a shuttle to come home.
I insisted on going with him to see his doctor. Jack had been going to the same GP for 12 years but hadn't been in a few years. Jack said he was fine but I told his doctor some of what was going on including the car being towed. He ordered blood tests and CT scan. When we walked out his doctor called me back to say this isn't him, I don't know what's wrong but I'm going to find out, hang in there with him. Then said he was afraid it was a tumor on his frontal lobe.
A week after the CT was an MRI. His doctor pulled up the results as we sat there and said this isn't good. That's when we first heard of FTD. He printed out pages explaining it and after Jack walked out said he'd call me over the weekend. He later said the loss on MRI was striking. On the way home my husband said, that's rather disturbing what he said about my frontal lobe disappearing but I don't have dementia, my memory is really good. I agreed.
That night after Jack went to bed at his new normal time of 7pm, I stayed up late reading online about FTD. I was scared by what I read and also relieved in a way to find an explanation for the odd behaviors and frustrating personality changes. From that day forward the anger and frustration I'd felt towards him in the past year disappeared. The next day he started taking low dose of Paxil and we had the nicest day in a long time. I think in a way he was also relieved to have an idea why things were getting difficult for him. I'm thankful he had no interest in reading about the illness.
Jack's GP said he'd only seen FTD once before in his 20 some years of being a doctor. He explained it would need to be confirmed through a neuropsych eval and a neurologist exam. He also gave me great advice like that I should let his family know right away, see an elder care attorney and apply for SSDI. He said some people with FTD get angry and agitated but Jack might just stay easy going, he was living in the moment. He also told me that he may only have two years to live and suggested trying to show him the best time possible and live life to fullest possible.
I'm not sure the neurologist we saw had met anyone with FTD before. The first 15 minutes of the first visit he seemed like he didn't really see anything wrong with my husband. Then my husband went to the bathroom so I was able to tell him some of the most concerning behaviors. When Jack returned he paced the little room and answered a few more questions with answers that didn't make as much sense. I think the neurologist started seeing behavior I had been seeing. Later we changed to a neurologist at Virginia Mason who specializes in FTD.
We managed to get in for a neuropsych eval within a month due to a cancelation. My husband only lasted one of the two hours before telling him he was done. The neuropsychologist told me afterwards that in a short, casual conversation with Jack he wouldn't have guessed many issues but the test confirmed the major deficiencies and FTD.
I took his doctor's advice to live life to the fullest. Soon after diagnosis we made a trip to the coast and a couple months later flew across country to see his family. We also went to concerts and festivals in the spring and summer. I had worry and stress during trips and outings with my husband but I'm thankful we did those things while we could and it was worth it for the good moments. I know how fortunate I am that my husband stayed sweet and easy going, that we had an excellent doctor and supportive family and friends.
Thankfully in addition to helpful information on the AFTD website I also found the FTD spouse facebook group. There I learned how to deal with the new normal of my husband not wanting to brush his teeth, shave, shower, change clothes, the heartbreak when it was time for depends and the other sad stages that followed. It was from the amazing people in that group I learned his muscle twitches sounded like beginning signs of ALS so we went back to Virginia Mason for testing. In September 2016, my husband was diagnosed with ALS. I believe both illnesses were caused by his time in the Marines stationed at Camp Lejeune when the water was toxic. I also know Jack was so proud of his service and didn't regret the time he spent in the USMC.
On the evening of December 29, 2016, fifteen months after bvFTD diagnosis, I called 911 because he was having trouble breathing. I gave the EMTs his advance directive paperwork but asked that they take him to the hospital. When I arrived at ER I asked them to remove the intubation. I was able to lay down next to him and he slept peacefully for a couple hours. He even woke one last time and pulled me in for a kiss. He passed away about 15 minutes later. I always used to think ALS was the worst disease but now I agree with others who have said ALS actually saved their loved one from the devastating and heartbreaking end stages of FTD. I miss him so much. I'm forever grateful for all the years we had including the last 15 months after diagnosis.
|
|
|
The care of later stage dementia patients is frustrating, labor-intensive, and prone to adverse events primarily because of inadequate assistive technology. Activities of daily living (ADLs) require the use of "patient lifts" for fully or maximally dependent patients in the highly repetitive activities of bed transfer, toileting, and showering.
For instance the cost of 56 transfers per patient per week for toileting (to and from commode x 4 daily visits x 7 days) uses up enormous nursing resources and results in numerous nursing back injuries (and added Workers Comp costs). 39% of the cost of long term care is nursing labor costs and ADLs for the most dependent patients (i.e., dementia patients) consume a significant portion of this money.
The NIA Dementia Summit does not appear to be addressing this critical issue. Patient care and ADLs needs to become much easier, safer, and less labor-intensive than they are today if Medicaid is to remain solvent (http://www.alz.org predicts dementia will cost a staggering $1200B annually by 2050).
As an assistive technology engineer and a former nursing aide who has interviewed dozens of nurses, caretakers, and healthcare administrators on this subject, I can say that this issue is critical to confronting the challenge of dementia care.
Research to improve medical devices for Safe Patient Handling (lifts are a antiquated 60-year old technology) is desperately needed. Such research seems to have received essentially zero funding from the NIH in the past decades. Given the current crisis in dementia care, it needs to be given a higher priority at the NIA/NIH.
|
|
|
The Physicians Committee for Responsible Medicine, a Washington DC-based nonprofit organization working to advance medical research, would like to applaud the steering committee for bringing together such a comprehensive agenda for the upcoming National Research Summit on Dementia Care. We look forward to the important discussion and recommendations that emerge from this meeting and urge the steering committee to prioritize the need to advance non-pharmacological interventions for ADRD as a synergistic part of NAPA's strategy to support ADRD care and services.
While pharmacological drug candidates for ADRD continues to fail in clinical trials, non-pharmacological treatment strategies for ADRD are showing great promise in delaying or halting the course of the disease . Hence, it is very exciting to see the following two research recommendations in the 2017 National Plan "aimed to improve uptake, spread and delivery of evidence-based and evidence-informed care and services" [National Plan to Address Alzheimer's Disease: Update 2017 - Appendix 2: 2017 Recommendations and Federal Response - Recommendation 3 (https://aspe.hhs.gov/report/national-plan-address-alzheimers-disease-2017-update)]:
- Identify and evaluate (non-drug) care strategies that reduce disease burden and delay disease progression and evaluate their costs and downstream effects.
- Convene a conference of key stakeholders to identify a meaningful pathway or pipeline for developing and testing non-pharmacological treatments, and scaling up and implementing effective approaches
Although these are two essential steps towards addressing the needs for people living with dementia and their caregivers, the NIH must do more to specifically respond to these recommendations. The NIH has an excellent opportunity during this Summit to address the research gaps to advance care and services in the form of developing additional funding opportunities for non-drug treatment strategies. The importance of non-drug treatment and care strategies has been recognized by the working groups of the Research Summit on Dementia Care, as evidenced in the background paper for Session I: Research on Care Needs and Supportive Approaches for Persons with Dementia (https://aspe.hhs.gov/pdf-report/research-care-needs-and-supportive-approaches-persons-dementia):
- Relatively few nonpharmacologic therapies have been tested in multiple large randomized controlled studies or have shown consistent results... Maslow (2012) identifies several other topics requiring additional research, including nonpharmacological treatments for those with non-Alzheimer's type dementia or young onset dementia, and for people with dementia from various racial and ethnic groups.
More randomized-controlled clinical trials are needed to test promising non-pharmacologic therapies, which can be more rapidly and safely implemented than their drug therapy counterparts. In addition, although exercise and cognitive training currently show the strongest evidence for treating ADRD among non-pharmacological interventions thus far, dietary patterns are an under-researched yet promising area for intervention. Moreover, dietary counseling is often a component of multimodal interventions. However, more clinical trial studies are needed to determine effective dietary patterns and their independent efficacy in order to combine the intervention with other non-pharmacological dementia therapies. This can only be achieved with adequately supported research programs and funding opportunities.
In order to take these nonpharmacological treatments from clinical study to implementation, we would also like to draw attention to the Summit's session on "Thinking Outside the Box". We look forward to the recommendations that tackle issues including the translation, dissemination, implementation, and scaling up of effective care and services - of which nonpharmacological interventions will require research to understand not only the external but also internal factors necessary for successful adoption of these interventions. The background paper of this session notes that, "rigorous research has shown, however, that some nonpharmacological interventions can have positive effects for people with dementia and their family caregivers," however, these types of interventions share similar challenges in implementation as other evidence-based interventions in that, "The lack of stable, ongoing, and sufficient funding to sustain evidence-based programs that have achieved positive outcomes in translation projects is a major barrier to sustaining these programs over time." (https://aspe.hhs.gov/pdf-report/translation-dissemination-implementation-and-scaling-effective-care-services-and-supportive-approaches-persons-dementia-and-their-caregivers). Thus, recommendations that not only emphasize sustained and sufficient research support to understand the external environments relevant for translation, but also increase understanding of internal factors that drive behavioral change in people with dementia will be essential to translating nonpharmacological interventions. Specially, what types of programs are most effective for creating life-long changes in dietary patterns or exercise? Do dietary patterns with quantitative or qualitative restrictions have higher adherence rates? These and other similar questions relating to behavioral change are also important to address for translation of non-pharmacologic interventions.
We thank the steering committee, working groups, and stakeholder participants for putting together this much needed Summit on Care and Services Research. Many essential topics will be covered in the coming days, and we strongly believe that developing priorities in nonpharmacological therapy and care will greatly improve the current landscape of ADRD.
|
|
|
As an early onset Alzheimer's caregiver who was recently "released from duty" with my wife's passing, I want to offer a suggestion and support for a simple, HIPAA-compliant buddy system to aid new caregivers in getting the right information when they need it.
"Reading the Internet" for ideas and strategies is very inefficient for new caregivers and a trained buddy would save time and help new caregivers work through immediate issues and thus regain a sense of control and confidence.
I missed this help four years ago, yet I know there are many 'buddies' available. We need to build on the knowledge already present within the caregiver community to make caregiving more efficient and effective for so many families.
|
|
|
Thank you for this opportunity to submit a comment. I would like to express my view that more research on supportive services and non-pharmacological approaches is needed. Because these approaches lack the financial incentives that drug development has, they tend to be studied much less, despite promising results. In particular, I would advocate for more research on arts-based programs, that have promise in reducing social isolation, improving quality of life for both individuals living with dementia and their care partners, and possibly in slowing cognitive decline.
I coordinate the Percolator Memory Café Network of Massachusetts, a mutual assistance group that has helped to spread the café model throughout our state. We now have 75 independently-run memory cafés in Massachusetts, including 2 Spanish-speaking cafés, and 11 that are specifically designed to include individuals living with both an intellectual/developmental disability and dementia. Our network of café coordinators observes tremendous benefits to people living with dementia and care partners from their participation in this low-cost, social and creative engagement model. We would love to see a rigorous study of the memory café model to help us learn about its most beneficial elements and to help us further its spread so that more people can benefit.
For information about Massachusetts Memory Cafés, please visit http://www.jfcsboston.org/MemoryCafeDirectory.
|
|
|
You have all these speakers with degrees etc. Is there a caregiver that will be speaking about living with the disease, hands on. I have lost my father through dementia and have learnt that no one really knows what happens between the four walls that the caregivers live with there loved one. Also they are the experts, the caregivers living with the disease, they are the ones that most helpful. The true stories between the caregiver, loved one and the walls what really happens.
Also drugs. My father was put on marijuana oil, whig helped tremendously, but because of our health care system and the lack of knowledge, to no fault of anyones, had to discontinue it. Is there research happening in this element of the disease?
|
|
|
This is my husband Warren Burke with 2 of his grandchildren one month before he died. Warren was diagnosed with depression and bipolar disorder before he was diagnosed with FTD in July of 2015. Warren's brother and father died of ALS. I cared for Warren at home until the day he died June 10th 2017. Warren was a construction superintendent and was the most "alive" person I had ever met. He was a gentle and kind person who always saw the best in everyone. FTD took everything from him in a span of just a year. He started with horrible anxiety and impulse control and ended with OCD and the inability to communicate or swallow. There are way too many behaviors to state here but life was a literal hell for us in the last year. I can't even explain to you what it feels like to go from wife to caregiver unless you have experienced it yourself. We were unable to get help putting him in a facility. I would have to choose between getting help with him or losing my home and other things we had worked for our entire lives. I also suffer from Psoriatic Arthritis and there were some days I truly thought we were going to go to the grave together. His children and grandchildren loved him very much and also suffered watching their grandfather waste away and become someone they didn't even recognize. My faith in God is absolutely the only thing that saved me and I know God released us from our suffering. Now that he is gone all the wonderful things we shared have come back. I was divinely favored to have this man in my life! I pray every day now that a cure will be found so Warren's family and other people in this world will not have to be afraid that this horrible disease will come into their lives leaving devastation!
|
 |
|
|
I saw your website about the summit and wanted to introduce myself as a future presenter and collaborator.
I'm the founder of HCEI.org which teaches resiliency skills to persons at risk for stress and burnout. Our seminar "Celebrating Ourselves: Beating Burnout" has been presented for a variety of audiences across the US and UK and I'd like to present for wider audiences.
Can you please visit HCEI.org and view the 3-minute video on our homepage? Then, who there can I talk with about collaboration? Thanks! R. Scott Boots, MPA Chicago 773-509-6402 www.HCEI.org
|
ATTACHMENT:
|
Celebrating Ourselves: Beating Burnout
The Health Cares Exchange Initiative, Inc.
HCEICares@HCEI.org
Celebrating Ourselves
Who cares for the care provider? Both paid and non-paid persons who offer their compassion, skills and resources to those in need are often at risk for stress, compassion fatigue or vicarious traumatization, creating costly health and emotional challenges and also gaps in expertise and caring. Care providers must be reminded how to assert themselves, set healthy boundaries and respond to stress in healthy ways. Focus groups held by HCEI across the US confirm the need to celebrate the spirit and journey of caring persons while teaching self-preservation skills for the future. When caring persons care for themselves they provide better care for others.
Presentation Outline
Beginning 1996 in the United States, HCEI held the first-ever nationwide focus groups with both paid and non-paid care providers to document their experiences and needs. From Boston to Kansas, caregivers expressed their needs. In response, this dynamic, interactive and empowering seminar was developed and has been presented to thousands of caregivers. Participants self-identify based on their own experiences and learn through a series of writing, visual and other experiential exercises. The session includes appreciation of dedication and encourages caring persons to set healthy future goals.
Objectives
Seminar participants will be able to:
- Understand dynamics of providing care
- Articulate how each person experiences stress uniquely
- Identify symptoms of compassion fatigue
- Utilize practical, proven solutions and exercises for stress reduction
- Set healthy goals and create a future response plan for personal/professional stress
Presentation
Founder and Director R. Scott Boots received his MPA degree at the University of Illinois at Chicago and is also a graduate of the University of Iowa and Interlochen Center for the Arts. A caregiver himself, he has worked as a training and administration consultant with the Massachusetts Departments of Environmental Protection, Social Services and Public Health and served as Co-Chair of Pastoral Care and Chair of the AIDS Support Committee at Trinity Church in the City of Boston. After founding HCEI in 1992, Scott studied wellness at the Touch Therapy Institute in Cambridge, MA and the Mind-Body Clinic at Boston¡¦s Beth-Israel Deaconess Hospital. His seminars have been presented to thousands of caring persons internationally. Recent audiences include Mt. Sinai Health System, Chicago, Scripps Mercy Hospital San Diego, Oregon Alzheimer¡¦s Association, Greater Iowa Alzheimer¡¦s Association, Chicago Medical School, Wake Forest University School of Medicine, and the MN Academy of Audiologists.
For more information please visit HCEI.org
|
|
|
This week is FTD awareness week. FTD stands for frontotemporal dementia and my family and I know this disease all too well. My mother was finally diagnosed two years ago after being misdiagnosed several times with things such as depression. We started to notice signs but we never considered it to be dementia because she was so young. At 59, she has been through multiple nursing homes and we've watched her lose almost every part of herself. Most of her day is spent in a wheelchair because she can no longer walk. The nurses have to help clean, feed and do everyday things. She can no longer talk or express herself in a way that makes sense. Being almost 6 feet tall, she weighs less than 100 pounds. The only thing I can do now is to keep the memory of her alive and fight to find a cure for this awful disease.
|
|
|
I cared for my husband, Alan after his diagnosis with FTD in 2007 at age 52. He had no physical infirmities at all and was fit and healthy pretty much all the way through his FTD. Alan was able to be at home alone for quite a while once he had to stop working in 2008. I worked full time to support us.
His symptoms began like those of PPA and as the disease progressed, his behavioral symptoms got worse. He started going to adult day care in 2011 but, following dental surgery in November of that year, he declined significantly and I could no longer care for him at home. His behaviors -agitation and aggression, mainly arose from frustration due to his aphasia. He chased me out of the house several times and threw things at me violently. However, there was still enough of him left at that point to feel remorse afterwards, even if he did not quite know what it was he had done. As with most FTD-diagnosed people, he suffered from apathy and lack of insight into his illness.
There were many admissions for psychiatric evaluation and three different facilities. He spent the last three months of his life in a wonderful place with caring staff, and died on September 17, 2012. You can read our story in my memoir, "The Dance". We married at age 20 and 21. He was 57 when he died. Our whole adult lives together were shattered by his death. Our sons lost a friend and father, I lost more than I could ever describe in this or any other writing. My biggest take aways from the challenges that FTD brought to our 40-year life together were:
- The U.S healthcare system is not even close to being able to support the deluge of dementia that is here and coming.
- The general public are also not even close to understanding how this massive issue will affect our world.
- Much more support and resource allocation is and will be needed if caregivers are expected to come from family members who often have to give up employment in order to stay at home with those diagnosed with FTD and other degenerative brain diseases.
None of this is news, I know. Our voices will need to be MUCH louder to be heard above the cacophony of voices striving for support from government and the public. The Care Summit is a wonderful step towards greater awareness and understanding of our FTD world.
|
|
|
I would like to draw attention to a form of dementia less common than Alzheimer's Disease. My father was diagnosed with Frontotemporal Dementia at the age of 47. He succumbed to the disease shortly after his 50th birthday. Onset of FTD often occurs in a person's 50s and 60s; the average age of diagnosis is about 57, which is a full 13 years before the average Alzheimer patient is diagnosed. Since patients with FTD are typically affected much earlier in life than those with Alzheimer's, FTD can affect work and family in a way dementia in older patients does not. My father lost his job 5 months prior to his diagnosis due to behavioral issues. Because of the nature of these symptoms (and the fact that a patient is often "too young" for dementia to be considered), FTD is often initially misdiagnosed as a variety of other ailments. Existing care facilities and programs may not be appropriate for--indeed, many do not accept--younger individuals as patients without additional education and support about FTD. During your summit, please acknowledge that there is more than one form of dementia, each having their own unique challenges for the affected person and their loved ones/caretakers.
|
|
|
Our FTD Story! I would love to help be a VOICE for all the young families dealing with bvFTD, and how we are lost through the cracks of our healthcare. I have so many incidents that NO family should have to go through.
My loved one is now living 3 hours from ANY family or Friends due to the funding and Nursing homes rights to not accept a patient younger then 62. We live in IOWA and we need to make a change, this is not QUALITY of LIFE for the loved one nor the FAMILY!
FTD attacks the younger generation and the caretaker is still having to work full- time.This is leaving a HUGE gap in the way we can care for our loved one, we can not keep them at home due to wandering, and needing to be watched, but at times the patient is not bad enough to be admitted into a NH- but our hands are tied because we need to continue to work, WE need more options for in home care. FTD patients go through different stages in the disease requiring different management of care-
IN our situation our loved one is 3 hours away due to his age - MANY of the Nursing homes in IOWA can choose WHAT age they will accept- MOST do not accept anyone under the age of 62- The closest one that would accept him due to age and behaviors is 3 hours away. This is so unfair.
ALSO in IOWA the cuts in Medicare and Medicaid have now limited the State Ombudsmen to do their work properly. Our family is lucky enough that we are very active in his care, but I feel for the patients that have no one helping them get the quality of care they need. We need watch dogs for the patients and making sure they are being managed properly and not just put behind closed doors. They need a life also.
I have attached a little piece that I wrote explaining our story- SO much more can be added, but just a glimpse of how FTD affected our lives! This was in the area newspaper- Our family will NOT give up for a CURE!
|
ATTACHMENT:
|
Tom is not going to help us find a cure for FTD because he doesn't understand that he has this terrible disease. Tommy doesn't even understand at times that he is ill. One of the many symptoms of this life ending disease is the person afflicted is in complete denial.
Tommy graduated from Rockford Senior High School and received his Associate of applied science in automotive technology at NIACC in Iowa. After years of working in the automotive field, and with Benttines Repair for 10 years, he bought the Repair Business from his former boss and renamed it Nash's Repair, He was a successful business owner with 3 full-time employees form 2003-2008 in Osage, Iowa at the end of the 5th year he began to have memory and personality changes that he decided he should pursue a different career path, thinking maybe it was the stress from owning the business causing the changes in him.
FTD can strike people of all ages but unlike Alzheimer's or dementia it strikes at an early age. It takes away memory, changes the personality, and steals the ability to communicate, function normally and causes one to say and do things completely out of character, and that are socially unacceptable. Ultimately, this disease takes away the ability to swallow and breathe.
Tommy has had this disease for about 5 years. I write 5 years because the doctors do not know exactly how long he has had it. That is why research is so important. This disease is misdiagnosed by competent doctors on a routine basis. Tommy had test after test taken at Mayo hospital and clinics. He was seen by, an endless list of pristine doctors and was misdiagnosed by them for 2 years. Finally in 2015, at the age of 44 we got the answers we were looking for; NOT what we ever wanted but, at least an answer and reason for the behavior. Tommy has been living in a memory care unit going on 3 years now. This is such a hard thing for young families to go through. Tom was blessed with 2 beautiful children, they are now 21 and 25 years old and they try and visit him as much as possible. His son Dylan has followed in his footsteps and is an Automotive Master Ford Technician down at Ames Ford, Dylan's wife Taylor is in her last 2 years of Vet school. Tommy's daughter Alyssa is a junior at UNI majoring in Art. They are very active with raising awareness for FTD and putting a golf tournament on for their father.
Through awareness we will find the cause and then and only then a cure will be found. This is why we are trying to raise funds for research. Your help and donations will be greatly appreciated especially by the individuals that will contract FTD in the future.
|
|
|
Not all dementia is Alzheimer's. FTD carries with it very specific and unique challenges on many different levels than Alzheimer's and it is devastating.
My mother passed away at the age of 65 in 2011 after a 4 year battle with FTD. At the time I was 39 years old, working full time and had two small children.
|
|
E. Masi | 09-20-2017
|
Today was the first day I saw a commercial about FTD. I am so happy that I saw this as we think my mother suffered from this disease. We saw her personality change, and so we took her first to the family Dr. then to a Neurologist with no diagnosis or guidance. Several months later we took her to the same Neurologist who still did not diagnose her, so I turned to another Neurologist who said she simply had dimensia and her paperwork said Alzheimers. The problem I had was that she did not fit most of the typical symptoms. Her memory was great, she was just overly agitated, had difficulties driving, was impatient, and more or less turning in to a person we did not know. She then spent a week at a Psych Hospital in Dayton OH with no new diagnosis given, other than she was "dimented". When it was no longer safe for her to stay at home, we opted for assisted living. The assisted living facillites could not handle her though. She was turned away twice and when the behavioral wing at another facility could not care for her, she ended up at a Psych Hospital in Sandusky OH. It was not until she was here that a doctor mentioned FTD. At that point she lived only a couple more weeks.
It was so frustrating to us that we could not find a diagnosis for my mother. I spent countless hours on the phone and internet trying to figure it out myself as well at draggin her to multiple doctors.
I am so happy that I saw the commerical so that hopefully more people will be aware of the disease. Even though there is no cure, it helps to at least have a diagnosis.
Then next step after diagnosis is to develop places that can care for people with this disease. My mom was 68 and with my sister and I being married with jobs and kids, we could not offer her full time care.
|
|
|
I attended a NAPA meeting several years back and there was a presentation offered regarding a study on the value of palliative and hospice care services for persons living with dementia.
I have been emersed both personally and professionally for 10 years with families living with dementia, and am amazed how these helpful services are so often offered and then taken away when they are working and serving to help a family.
I would like to know if the topic and value of pallative care services can be discussed at the summit and what it might take for this to be addressed as a most helpful form benefit for quality of life and well being of person's living with dementia and their caregivers.
I believe I remember the NAPA study showing reduced health care costs for families as they were able to manage co morbidities and other secondary medical challenges due to dementia in the home both keeping the person from traumatic and difficult trips to the doctor and ER while also reducing health care costs, and providing support for family care partners.
I am amazed the criteria for persons with dementia continue to require a very "end of life" stage of dementia.
I have searched for the study that was presented at the NAPA meeting, I believe in Jan or February of 2015 and have been unable to find it.
Also, do you have a list serve of sorts that I could be included on regarding NAPA updates?
Thank you for the opportunity to inquire about the value of pallative care services for families living with dementia.
|
ANSWER
|
|
My concern is the issue of persons with dementia who live alone and how to find them and provide assistance and services.
|
|
|
I'd like to take this opportunity to share with you my article which was published last week:
Caspi, E. (2017). "Trust at stake: Is the "dual mission" of the U.S. Alzheimer's Association out of balance?" Dementia: The International Journal of Social Research and Practice. Available at http://journals.sagepub.com/doi/full/10.1177/1471301217719789.
Hope you'll find it useful during your Summit.
|
|
|
My husband was diagnosed in 11/2014 with LBD after a trip/fall and subsequent surgery.
From 11/2014 until his death in 04/2017, I photographed and documented the DISCRIMINATION, ABUSE and NEGLECT incurred by LTC FACILITIES including the Healthcare Providers employed by the Facility, Administration of the Facility, Medical Staff of the facility including Nursing Administration, Nursing Staff both Licensed and Unlicensed, Physical Therapy, Social Services, Maintenance. BEHAVIORAL FACILITIES both IN-HOSPITAL and FREESTANDING are also included but documentation only d/t facility policy. LTC Facilities number SEVEN. (2 classified as DEMENTIA specific.) BEHAVIORAl Facility number TWO. As an LVN in the great state of TEXAS since 1973, I worked LTC, Skilled, Acute Care, Clinic, Geri-Psych and at present Correctional Care.
Please put me on your list as a presenter.
There is a desperate need for a serious overhaul of LTC specifically the treatment of individuals with LBD.
My husband was my ongoing "case study." He could communicate all aspects of the hallucinations, verbalize his needs, complaints, concerns, observations and interactions. That was the nature of Jack's LBD beast.
|
|


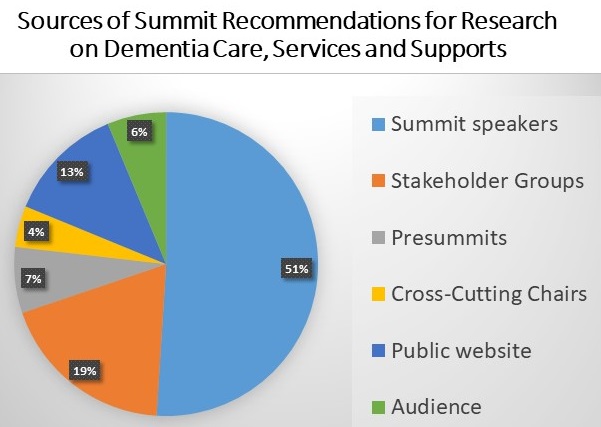

 Summit Home Page
Summit Home Page