Monday, August 1, 2016
CMMI Project Demonstrating the Value of Palliative Care
Janet Bull MD, MBA, FAAHPM
CMO Four Seasons
Objectives
- Discuss components of palliative care
- Demonstrate the benefits to dementia patients
- Discuss payment reform in hospice and palliative care
Four Seasons
- Located in Hendersonville, NC
- Retirement community
- 25% population over 65 years old (compared to 13%)
- High dementia population -- number 1 referring diagnosis for both hospice and palliative care
Why Palliative Care?
- Need to improve care for seriously ill patients
- Aligned with Mission of providing exceptional end of life care
- Provide care across the continuum of care settings
- Unsustainable financial model under current reimbursement structure
Palliative Care Services Focus on...
- Symptom management
- Prognostication
- Advance care planning
- Establish goals of care
- Educate patients on their disease process
- Spiritual and psychosocial support
- Assist with community resources
- Coordination of Care
- Help patients navigate the healthcare system
Mary's Story
74 year old black female with advanced dementia, living with her daughter at home
- major behavioral issues -- combativeness, agitation
- polypharmacy
- hospitalized 2 times in past 12 months (fall, pneumonia)
- daughter quit work to provide care - exhausted & stressed
- no advanced care planning
Impact of Palliative Care
- Improving Helath of Individuals & Populations
- Improving Patient Experience
- Reducing the Cost of Care
CMS Innovations Grant
- Scale model into 14 counties, delivered longitudinal across all care settings
- Track Quality
- Define Costs
- Test innovation -- Tele-palliative care
- Developing/Testing a New Payment System
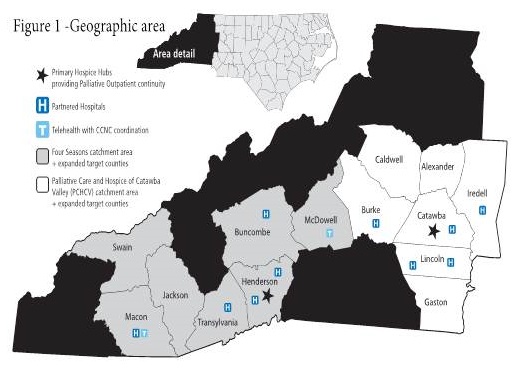
Four Seasons Expanding Palliative Care Across Western NC and Upstate SC
| Western North Carolina |
Update South Carolina |
 |
 |
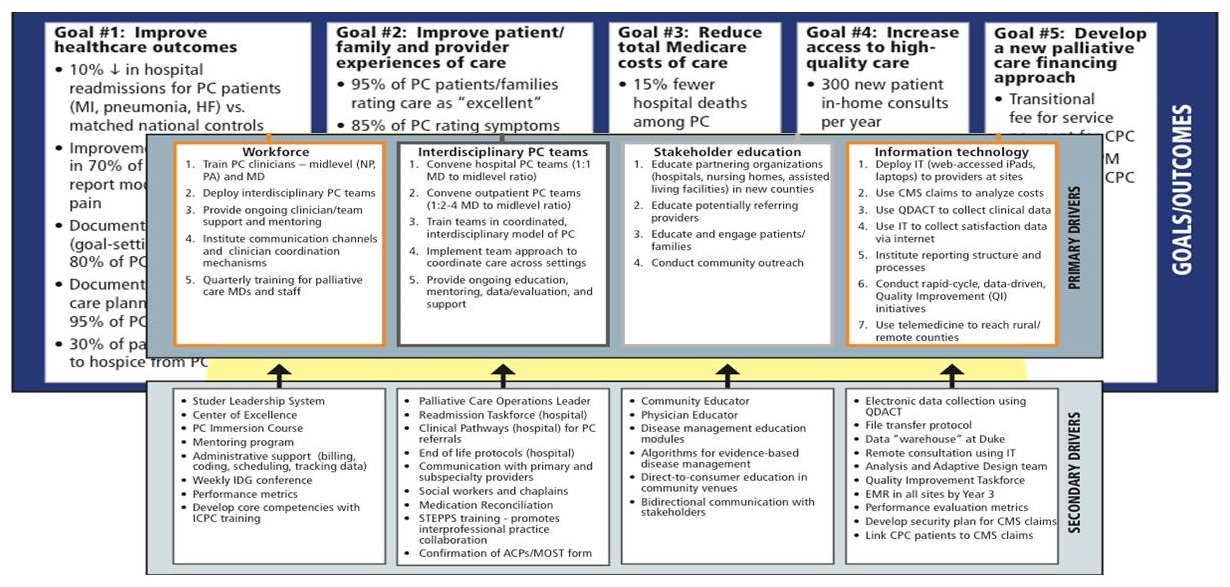
Goals and Driver Diagram
Eligibility
- Medicare Age Eligible
- Patients with life limiting illness in last 3 years of life
- Uncertainty of appropriateness of therapy (curative, palliative, hospice)
- Excludes 54% of palliative care patients (younger, Medicare Advantage, etc)
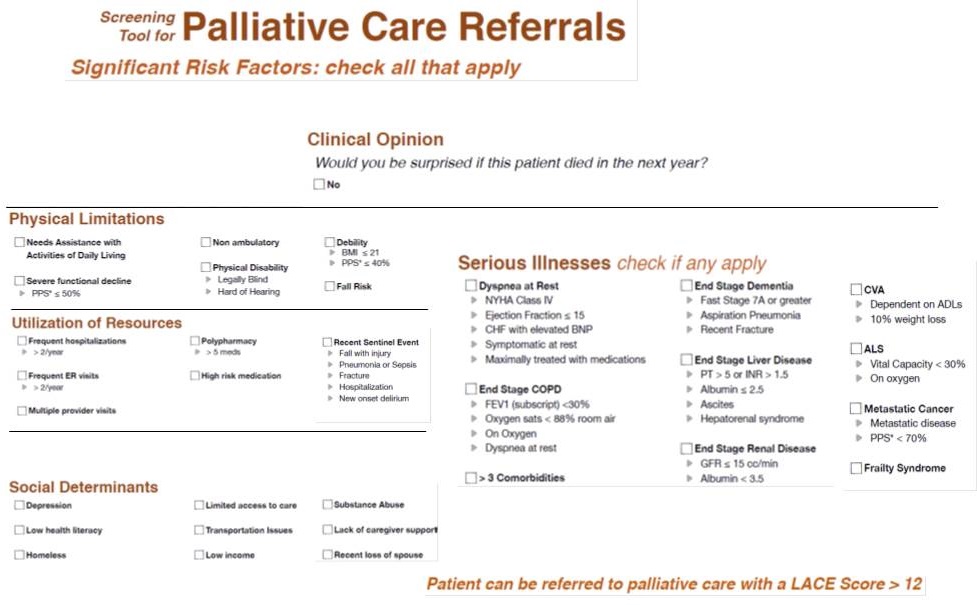
Screening Tool for Palliative Care Referrals
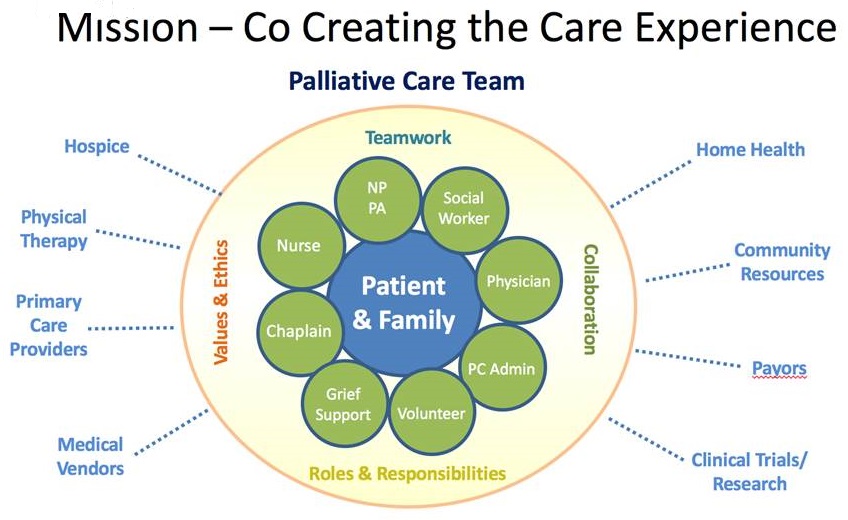
Four Seasons Palliative Care Model
Standardizing Care
- Developing good processes/procedures
- Data collection
- Data analysis/tracking
- Quality improvements
- Measuring satisfaction
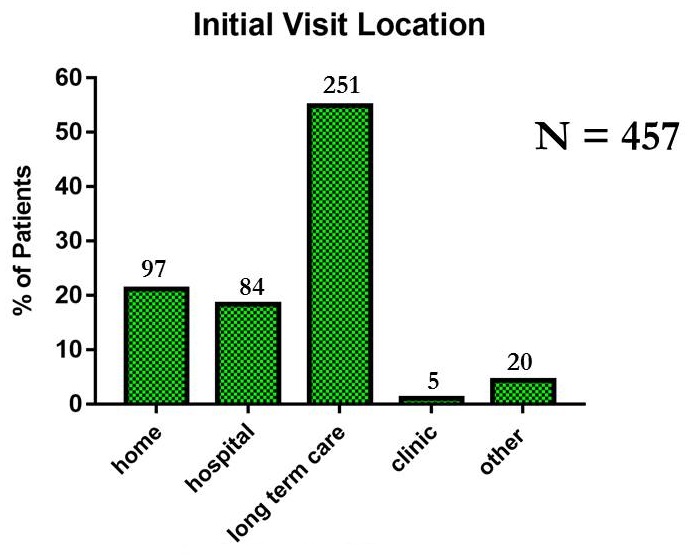
The Initial Palliative Care Visit by MD, DO, NP, PA, and RN
- PRE-VISIT
- Determine reason for consult
- Review H&P, meds, labs, xray, etc.
- Identify other agency involvement
- Clinic -- New Patient Packet at Sign-In
- New Patient Packet:
- Confident Care booklet
- Consent
- Letter
- VISIT
- RN
- Explain program and review New Patient Packet
- Review symptoms
- Reconcile meds and list allergies
- Obtain social history
- Do spiritual assessment
- Discuss ACP
- Identify goals
- Assess functional status and safety
- Assess VS, O2 sat, ht/wt, consitution, eyes, ENT, lymph, resp, cardio, GI, GU, MS, skin, neuro, psych
- Formulate care plan with patient/family
- MD, DO, NP, PA
- Explain program and review New Patient Packet
- Review symptoms
- Reconcile meds and list allergies
- Obtain social history
- Do spiritual assessment
- Discuss ACP
- Identify goals
- Assess functional status and safety
- Assess VS, O2 sat, ht/wt, constitution, eyes, ENT, lymph, resp, cardio, GI, GU, MS, skin, neuro, psych
- Determine prognosis
- Formulate care plan with patient/family
- POST-VISIT
- Determine Risk Level
- Complete visit documentation- to include QDACT
- Forward copy of notes to facility and/or referrer
- Collaborate with other members of IDG
Rist Assessment
| PRIORITY OF VISIT |
High |
Medium |
Low |
| Transition |
Transition from hospital within last 2 weeks |
Transition from hospital within last 15-30 days |
No hospitalization or ER visits within last 3 months |
| Symptom |
Mod-Severe Symptoms: pain, dyspnea, constipation, N&V |
|
|
| Function |
20% drop in PPS |
10% drop in PPS |
PPS stable by <50% |
| Meds |
- 3 or more medication changes within last week
- Initiation of opioids
|
1-2 medication changes within last 15-30 days (opioids, anti-psychotics, cardiac meds) |
<1 medication change within last 3 months |
| Nutrition |
- Sudden nutritional decline (5% weight loss in 1 month) with BMI <21
- Albumin <2.5
|
- >5% weight loss over last 2-3 months with BMI <21
- Albumin 2.5-3
|
<5% weight loss in last 3 months |
| Infection |
- Infection with systemic symptoms within last 2 weeks
- > Stage 2 pressure ulcer
- Aspiration
|
- 2 infections within last 2 months
- Stage 2 pressure ulcer within last 2 months
|
No infections within last 3 months |
PSYCHOSOCIAL RISK ASSESSMENT
| RISK |
High |
Medium |
Low |
| Psychosocial |
- Sudden cognitive changes
- Mental health diagnosis accompanied by disruptive verbalizations/behaviors. Concern for patient or caregiver safety.
- Suicidal ideation, especially with plan. Despair.
- Signs/Symptoms of abuse/neglect. Unsafe situation for patient.
- Caregiver decompensation. Immediate safety concerns.
|
- Anhedonia- flat affect and not participating in > 3 activities
- Significant losses in last 2 years. Unresolved grief issues.
- Depression.
- Expresses fear/anxiety about money, worried about caring for family, concerned about paying for services
- Caregiver stressed, showing some signs of burnout, but no immediate danger to patient or caregiver. Placement issues.
- Transition to hospice- pt/family require psychosocial support in making decision for hospice care. Complex family dynamics.
|
- Caregiver available and adequate to manage patient care. May need some self-care strategies or information on community resources.
- Advance care planning needs.
|
Quality Data Assessment Tool
PC Tracking
| Enrollment |
N = 2450 Total |
N = 522 Dementia |
| Hospice Transitions |
700 (33%) |
181 (35%) |
| Palliative Care Deaths |
237 (11%) |
59 (11%) |
| Palliative Care Discharges |
665 (31 %) |
141 (27%) |
| Active PC Caseload |
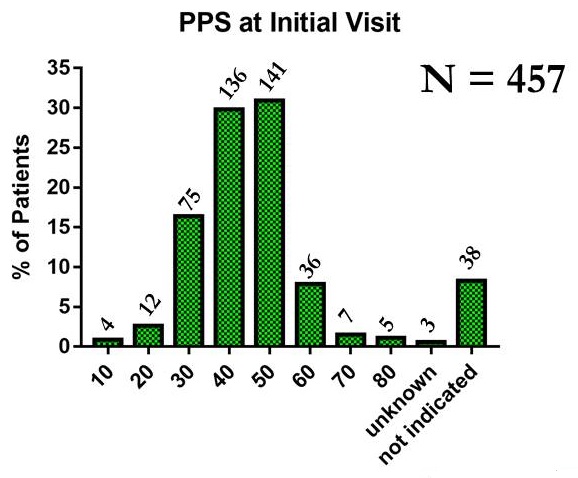
457 (24.3%) |
141 (27%) |
Story tells....
- 50-60% die within 1 year (80% from data 2 years ago)... PC moving upstream
- 33% discharged after acute episode; of these ~ 10% readmitted
Dementia
- Challenges
- Difficult to prognosticate
- Slow disease trajectory
- High caregiver distress/burnout
- Often stabilize/improve with supportive services
Palliative Care -- Dementia CMMI patients
Add
Functional Status of PC Dementia Patients
 |
| Palliative Performance Scale (PPS) |
| % |
Ambulation |
Activity and Evidence of Disease |
Self-Care |
Intake |
Level of Conscious |
| 100 |
Full |
Normal activity, no evidence of disease |
Full |
Normal |
Full |
| 90 |
Full |
Normal activity, some evidence of disease |
Full |
Normal |
Full |
| 80 |
Full |
Normal activity with effort, some evidence of disease |
Full |
Normal or reduced |
Full |
| 70 |
Reduced |
Unable to do normal work, some evidence of disease |
Full |
Normal or reduced |
Full |
| 60 |
Reduced |
Unable to do hobby or some housework, significant disease |
Occasional assist necessary |
Normal or reduced |
Full or confusion |
| 50 |
Mainly sit/lie |
Unable to do any work, extensive disease |
Considerable assistance required |
Normal or reduced |
Full or confusion |
| 40 |
Mainly in bed |
Unable to do any work, extensive disease |
Mainly assistance |
Normal or reduced |
Full, drowsy, or confusion |
| 30 |
Totally bed bound |
Unable to do any work, extensive disease |
Total care |
Reduced |
Full, drowsy, or confusion |
| 20 |
Totally bed bound |
Unable to do any work, extensive disease |
Total care |
Minimal sips |
Full, drowsy, or confusion |
| 10 |
Totally bed bound |
Unable to do any work, extensive disease |
Total care |
Mouth care only |
Drowsy or coma |
| 0 |
Death |
--- |
--- |
--- |
--- |
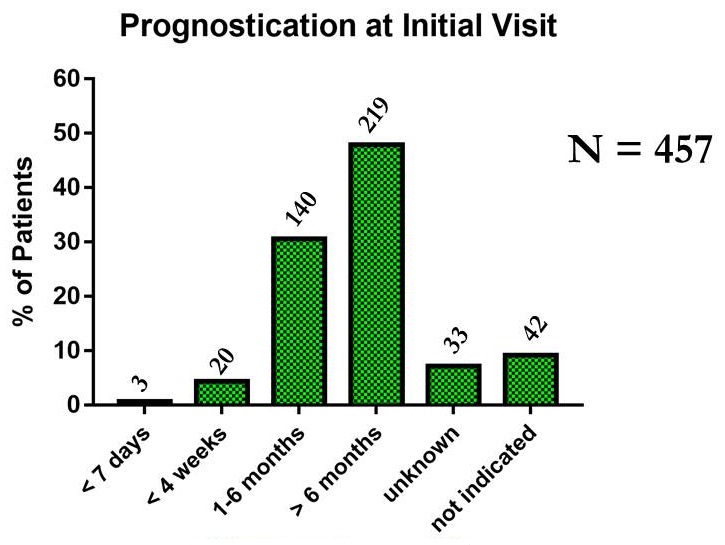
Prognostication by Clinicians
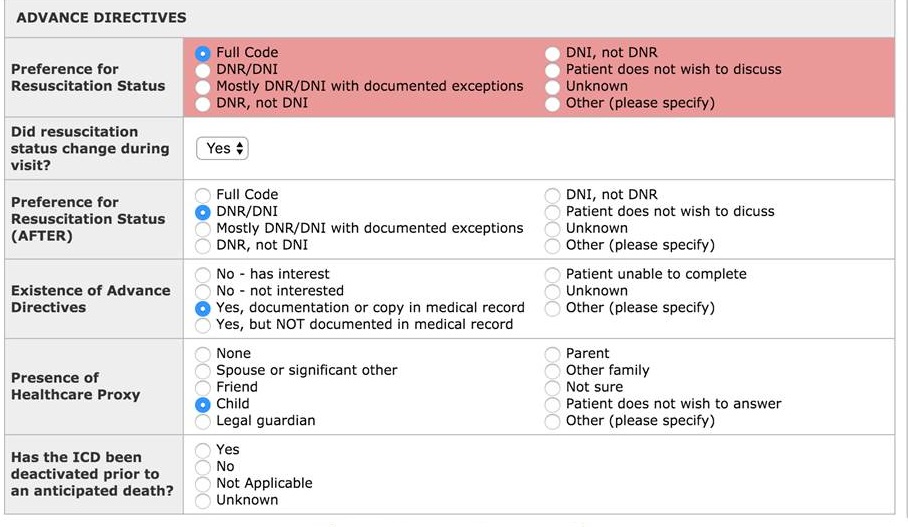
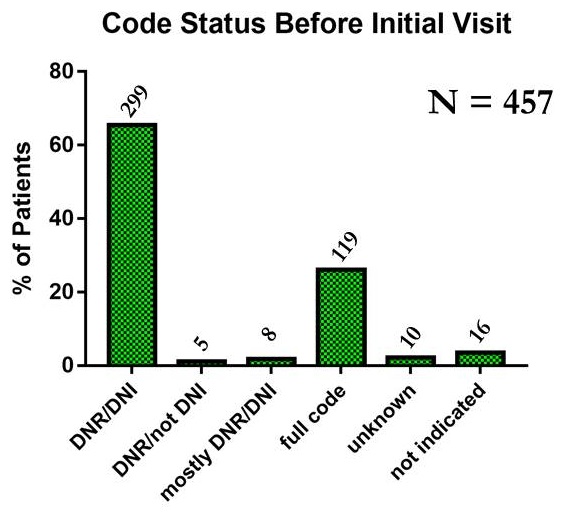
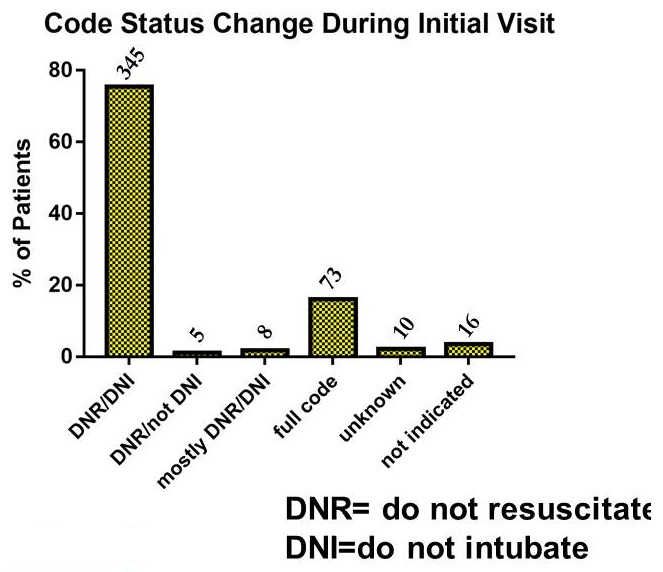
Code Status -- Dementia Patients - PC
Policy Issues
- Lack of long term care benefit
- Little reimbursement for other disciplines
- New Care Management codes
- Advance care planning
- Transitional care codes
- Chronic care codes
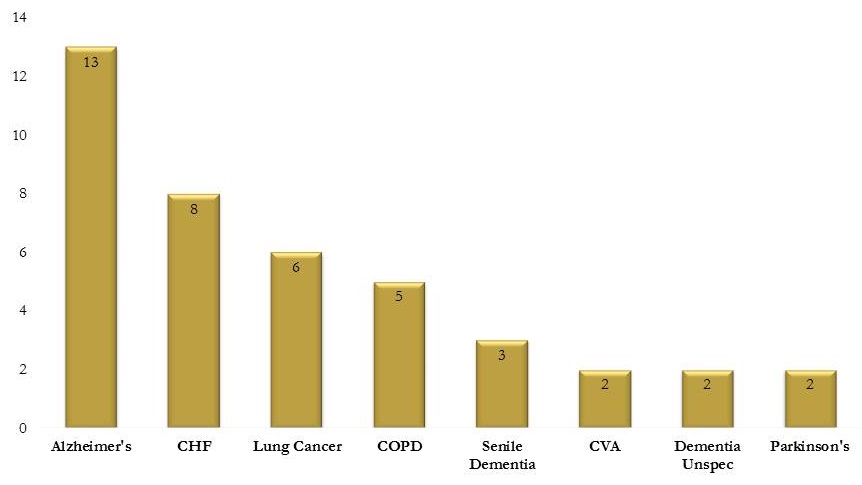
Diagnosis Hospice Claims 2015
Differences - Hospice vs Palliative
| |
Hospice |
Palliative Care |
| Life Expectancy |
< 6 months |
Any stage of illness |
| Treatment |
Comfort |
Curative or comfort |
| Care settings |
All |
All |
| Resources |
Significant |
Limited |
| Delivery model |
Interdisciplinary Team |
Interdisciplinary Team |
| Payment Model |
Medicare Hospice Benefit |
Medicare Part B E/M codes |
How to Pay for Services?
Developing Alternative Payment Approaches
- Covered Services
- Advance care planning
- Goals of care (3 meetings)
- Social work, chaplain, patient family volunteers
- RN case management and care coordination
- Not covered (hospitalization, primary care, specialty care)
As the World Turns (Grant submission to today)
2013
- Transitional Fee for Service payment for CPC
- 1-3yr analysis
- Bundled PBPM Payment for CPC
- Promote PC clinical care model Expansion
- Promote best practice ACO integration of transitional care models
- Financial Ecosystem changes through Legislation and Policy
- Changing Accountable Care Act implementation
- Accountable Care Organization alignment -- Incentives
- Hospice -- Hospital -- Transitional Facility FFS/PBPM changing
- Payment Approach Replication Throughout Medicare
- Dependent on Financial alignment
- Value Proposition in patient outcomes
- Value Proposition in reducing Total Cost of Care
2016
- Jan 1, 2016 *2 CPT codes for Advanced Care Planning (MD only, Outpatient Primarily, State interpretation)
- 2015 *CCM Chronic Care Management $42 monthly PBPM
Questions Around Payment Approaches
Challenges for Evaluation
- Medicare Part A vs Part B -- increase Part B while reducing Part A costs
- PBPM payment 30/60/120
- Bundled payment (60/120 days) Who holds?
- Care management codes (increase Part B bucket)
- Changes in hospice payment (two tiered payment, Service Add on)
Susan's Story
82 year old white female with end stage dementia admitted to the hospital with second episode of aspiration pneumonia
- wandering, behavioral issues
- feeding issues -- considering PEG tube
- lives with son and his wifej who are overwhelmed
Questions?
jbull@fourseasonscfl.org