
Friday, April 27, 2018
Printer Friendly Version in PDF Format (13 PDF pages)
Care Planning and Health Information Technology: How to Aid Dementia Quality Care
Liz Palena Hall, RN, MIS, MBA
LTPAC Coordinator
Office of the National Coordinator for Health Information Technology
Agenda
- Need for Longitudinal Person-Centered Care Planning
- Policy Levers Supporting Person-Centered Care and Health IT Enabled Care Plan Exchange
- Electronic Care Plan Information Gathering Sessions
- Exemplar Care Plan Standards Based Initiatives
What is a Care Plan?
- Long-Term Services & Supports Care Plan
- Plan of Care
- Comprehensive Care Plan
- Person-Centered Care Plan
- Shared Care Plan
- Longitudinal Care Plan
- Emergency Care Plan
- Plan of Treatment
Many terms used to define output of care planning process
Meet Mrs. M
- 11 Issues
- Congestive Heart Failure
- Atrial Fibrillation
- Old stroke
- Unstable gait
- Occasional Fall
- Osteoarthritis
- Hypertension
- Dementia
- 12 medications
- Fear of falling
- Isolated
- 8 Team Members
- Cardiologist
- Neurologist
- Orthopedist
- Primary Care Team
- Visiting Nurses
- Homemaker/ Home Health Aide
- Meals on Wheels Provider
- Transportation Provider
5 Basic Components of a Care Plan
- Care Team Member Information
- Health Concerns / Needs
- Goals/ Objectives
- Interventions/ Activity
- Progress/ Outcomes
Longitudinal Person-Centered Care Plan
 |
POLICY LEVERS SUPPORTING PERSON-CENTERED CARE AND HEALTH IT ENABLED CARE PLAN EXCHANGE
ONC 2015 Edition Care Plan Criterion
- Requires a Health IT Module to enable a user to record, change, access, create and receive care plan information in accordance with the HL7 Consolidated Clinical Document Architecture (C-CDA) Release 2.1 Implementation Guide, including the Health Status Evaluations and Outcomes Section
- Supports broader information about the patient, including education, physical therapy/range of motion, and social interventions
- Distinct from "Plan of Care Section" in previous C-CDA versions
- System must be able to receive care plan in accordance to standard but is NOT required to enable a user to reconcile care plan data
- "Optional" criterion not required as part of the CEHRT definition referenced in QPP or EHR Incentive Programs
Source: https://www.healthit.gov/sites/default/files/2015Ed_CCG_b9-Care-plan.pdf
CMS Quality Payment Program (QPP): MIPS
- MIPS Quality Measures: Measure #47 Care Plan
- % of patients aged 65+ who have advance care plan documented in medical record
- MIPS Improvement Activities:
- (IA_PM_13) Chronic care and preventative care management for empaneled patients
- (IA_BMH_7) Implementation of integrated patient centered behavioral health model
- (IA_CC_9) Implementation of practices/processes to develop regularly updated individual care plans for at-risk patients that are shared with beneficiary or caregivers
- (IA_BE_23) Provide coaching between visits with follow-up on care plan and goals
Source: https://qpp.cms.gov/
CMS QPP: Alternative Payment Models (APM)
- Two models have specific care plan requirements
- Comprehensive Primary Care Plus (CPC+) Model (Track 2)
- Practices must adopt certified health IT for two ONC 2015 Edition Criteria: Care Plan and Social, Behavioral and Psychological Data
- Oncology Care Plan Model
- Requires documentation of care plan using IOM guideline
- Comprehensive Primary Care Plus (CPC+) Model (Track 2)
Source: https://qpp.cms.gov/
CPC+ Care Plan Health IT Requirements
CPC+ practices should utilize an IT-enabled, patient-centered care planning tool in order to support holistic care and a focus on beneficiary goals and preferences.
- Enable providers to electronically capture the following care plan elements:
- Advance directives and preferences for care
- Patient health concerns, goals and self-management plans
- Action plans for specific conditions
- Interventions and health status evaluations and outcomes
- Identified care gaps
- The practice should have the ability to customize which of these elements are included within the care plan and how these elements are displayed.
- Providers should be able to incorporate relevant triggers (e.g. a risk score or event) that indicate different care management actions.
- The care plan tool should facilitate version control across care team members by capturing the date of the last review or change in plan and generating a scheduled date for reviewing and updating the plan.
- Practices should be able to populate the care plan using data entered in the patient's record (e.g. without duplicative data entry).
- The care plan should be available to the patient on paper and electronically, and available in electronic format to care team members outside of the practice that are involved in the patient's care. Care plan information should also be remotely accessible to practice team members delivering care outside of normal business hours.
- To support this objective, practices must adopt certified health IT that meets the 2015 Edition "Care Plan" criterion found at 45 CFR 170.315 (b)(9).
Medicare Chronic Care Management (CCM) Codes
- Included Services are:
- Use of Certified Electronic Health Record
- Continuity of Care with Designated Care Team Member
- Comprehensive Care Management and Care Planning
- Transitional Care Management
- Coordination with HCBS Clinical Service Providers
- Advance Consent
Source: CMS Medicare Learning Network https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/Downloads/ChronicCareManagementServicesChanges2017.pdf
State Medicaid Director's Letter 16-003
- Updated guidance allows Medicaid HITECH funds to support all Medicaid providers that Eligible Providers want to coordinate care with.
- Medicaid HITECH funds can now support HIE onboarding and systems for behavioral health providers, long term care providers, substance abuse treatment providers, home health providers, correctional health providers, social workers, and so on.
- States may claim the 90 percent HITECH match for costs related to the design, development, and implementation of interoperable systems and HIEs that facilitate the exchange of electronic care plans between Eligible Providers and other Medicaid providers.
Source: https://www.medicaid.gov/federal-policy-guidance/downloads/smd16003.pdf
Reform of Requirements for Long-Term Care Facilities Final Rule -- Interpretive Guidance
- Includes requirements for Comprehensive Care Plan
- Nursing homes develop baseline care plan within first 48 hrs. of admission
- Care Plan must be person-centered--includes what is important to the resident and supports each resident in making his or her own choices
- Care Plan includes services that maintain the resident's highest practicable physical, mental, and psychosocial well being
- Format and location of care plan are at facility discretion, but the clinical record must contain evidence that care planning process was conducted alongside the resident and include resident identified goals and outcomes of care
Electronic Care Plan Information Gathering Sessions
Electronic Care Plan Information Gathering Sessions
- In May 2017, ONC facilitated four virtual convening sessions with 12 health IT vendors
- Each vendor presented on their electronic care planning capabilities and participated in an open discussion with other participants and ONC staff
- Sessions provided valuable insight into state of electronic care plan capture, exchange and sharing and use of health IT standards
Key Takeaways
- Care plan ownership and management varies depending on the type of care team engaged and the care setting
- Care plan is not physician driven; physicians are interested in parts of the care plan and are dependent on broader care team to manage care plan
- Majority of vendors are 'learning' alongside their clients on how best to implement electronic care planning
- New CMS Medicare and Medicaid Innovation programs such as CPC+ and longitudinal care management payment codes such as Medicare Chronic Care Management are driving care plan technology development and adoption
- Standards are helpful for capturing clinical data but limit ability to capture non-clinical and non-codifiable patient identified data
- All vendors have implemented HL7 C-CDA based document templates with majority using Release 1.1 instead of ONC 2015 required Release 2.1 which includes standardized Care Plan document template
- HL7 C-CDA Care Plan document considered a starting point for effective care planning but remains limited in robustness of data elements for longitudinal and holistic care and ability to support emerging extended care team models
- HL7 C-CDA and FHIR Care Plan standards need to be further harmonized to enable systems that use one type to communicate with other systems using another type
- Vendors see tremendous value in capturing social and behavioral determinants of health in care plans but are not yet doing so in a structured or standardized way
EXEMPLAR CARE PLAN STANDARDS BASED INITIATIVES
electronic Long-Term Services & Supports (eLTSS) Initiative
- Launched in November 2014 as a joint project between CMS and ONC
- Focused on the identification and harmonization of a service plan standard to enable electronic exchange of information relevant to the care of persons receiving community based LTSS
- Driven by the requirements of the CMS Testing Experience and Functional Tools (TEFT) in Medicaid community-based long term services & supports (LTSS) Planning and Demonstration Grant Program
- eLTSS is one of the four TEFT Program Components
- 6 of 9 TEFT grantees participated in the eLTSS component of TEFT: CO, CT, GA, KY, MD, MN
- Supports CMS Requirements for Person-Centered Service Plans (PCSPs) as defined within the HCBS 1915 (c) Waiver Final Rule https://www.medicaid.gov/medicaid/hcbs/authorities/1915-c/index.html
- PCSPs support the person, make him or her central to the process, and recognize the person as the expert on goals and needs
https://www.medicaid.gov/medicaid/ltss/teft-program/index.html
eLTSS Final Dataset
Total Number of Elements: 56
| Beneficiary Demographics: 10 Elements | Person Centered Planning: 11 Elements | Plan Information: 1 Element | Risks: 2 Elements | Service Provider Information: 5 Elements |
|---|---|---|---|---|
| Person Name | Assessed Need | Plan Effective Date | Identified Risk | Support Planner Name |
| Person Identifier | Preference | Plan Signatures: 12 Elements | Risk Management Plan | Support Planner Phone Number |
| Person Identifier Type | Person Setting Choice Indicator | Plan Signatures: 12 Elements | Service Information: 12 Elements | Service Provider Name |
| Person Date of Birth | Person Setting Choice Options | Person Signature | Service Name | Service Provider Phone Number |
| Person Phone Number | Service Options Given Indicator | Person Printed Name | Self-Directed Service Indicator | Non-Paid Provider Relationship |
| Person Address | Service Selection Indicator | Person Signature Date | Service Start Date | |
| Emergency Contact Name | Service Provider Options Given Indicator | Guardian/Legal Representative Signature | Service End Date | |
| Emergency Contact Relationship | Service Provider Selection Agreement Indicator | Guardian/Legal Representative Printed Name | Service Delivery Address | |
| Emergency Contact Phone Number | Service Plan Agreement Indicator | Guardian/Legal Representative Signature Date | Service Comment | |
| Emergency Backup Plan | Plan Monitor Name | Support Planner Signature | Service Funding Source | |
| Goals & Strengths: 3 Elements | Plan Monitor Phone Number | Support Planner Printed Name | Service Unit Quantity | |
| Goal | Support Planner Signature Date | Unit of Service Type | ||
| Step or Action | Service Provider Signature | Service Unit Quantity Interval | ||
| Strength | Service Provider Printed Name | Service Rate per Unit | ||
| Service Provider Signature Date | Total Cost of Service | |||
| Final dataset and information on HL7 (standards) engagement available at: https://oncprojectracking.healthit.gov/wiki/display/TechLabSC/eLTSS+Home | ||||
Vision for eLTSS Dataset Integration
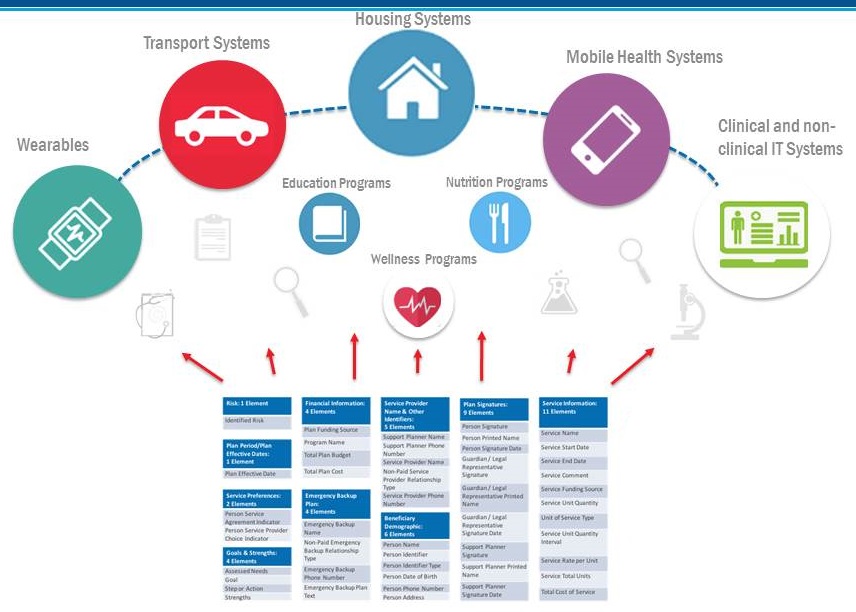 |
| eLTSS Dataset can be incorporated into various programs and health/wellness IT systems For interoperability, eLTSS dataset needs to be represented using nationally recognized vocabularies and content standards |
| Initiative | Standard(s) |
|---|---|
| HL7/BCBSA: Care Plan Proof of Concept (2015) http://wiki.hl7.org/images/f/ff/01_CM-DM_Care_Plan_Review_and_Recommendations_May_2015.pdf |
|
| Greater New York Hospital Association and HealhIX Care Plan Implementation https://www.health.ny.gov/health_care/medicaid/redesign/dsrip/pps_workshops/learning_symposiums/docs/sept2016_presentations/day2_breakout_d1.pdf |
|
| VA Care Coordination for Improved Outcomes Challenge http://www.health2con.com/devchallenge/va-care-coordination-for-improved-outcomes-challenge/ |
|
| NIH NIDDK Chronic Kidney Disease (CKD) Care Plan Project https://www.niddk.nih.gov/health-information/health-communication-programs/nkdep/working-groups/health-information-technology-working-group/Pages/default.aspx#careplan |
|
| My Care Guide for Veterans http://clinicalcloud.solutions/my-care-guide-veterans/ |
|
| Early Hearing Detection and Intervention (EHDI) Hearing Care Plan Pilot: Oregon Health Authority (June 2015) http://www.infanthearing.org/meeting/archive/ehdi2015/ehdimeeting.org/archive/2015/System/Uploads/pdfs/Poster_DinaDickerson_1673.pdf |
|
| Utah Health Department Newborn hearing screening care coordinaiton (ONC HIE Grantee): Utah Department of Health, Utah Health Information Network (UHIN) and Intermountain Healthcare (Sept 2015 to Sept 2016) https://www.healthit.gov/techlab/ipg/node/4/submission/1211 |
|
| ONC/CMS eLTSS Initiative https://oncprojectracking.healthit.gov/wiki/display/TechLabSC/eLTSS+Home |
|
NCPDP/HL7 Pharmacist eCare Plan Pilots
|
|
| Comprehensive Primary Care Initiative (CPC+) Track 2 CMMI Grantee (target Q12019) https://innovation.cms.gov/initiatives/comprehensive-primary-care-plus |
|
| Veterans Administration (VA) Salt Lake City Health Care System: Shared Care Planning http://www.saltlakecity.va.gov/rupper_shared_care_planning.asp |
|
| Argonaut Project http://argonautwiki.hl7.org/index.php?title=Main_Page/Background |
|
 |
April 27, 2018 -- Advisory Council Meeting #28
The meeting was held on Friday, April 27, 2018, in Washington, DC. During the meeting, the Clinical Care Subcommittee took charge of the theme, focusing on advancing consensus on dementia care elements to guide new outcomes measurement. The Council heard speakers in two sessions, one focused on developing consensus about dementia care elements, and the second on models that are informing outcomes measurement. The meeting also included updates on work from the previous meetings, a presentation on the final report from the October 2017 Care Summit, and federal workgroup updates. Material available from this meeting is listed below or at https://aspe.hhs.gov/advisory-council-alzheimers-research-care-and-services-meetings#Apr2018.
Comments and questions, or alerts to broken links, should be sent to napa@hhs.gov.
General Information
-
Agenda -- [HTML Version] [PDF Version]
-
Meeting Announcement -- [HTML Version] [PDF Version]
-
Meeting Summary -- [HTML Version] [PDF Version]
-
Public Comments -- [HTML Version]
Handouts
-
Main Summit Recommendations -- [HTML Version] [PDF Version]
-
National Research Summit on Care, Services, and Supports for Persons with Dementia and Their Caregivers: Report to the National Advisory Council on Alzheimer's Research, Care, and Services -- [HTML Version] [PDF Version]
Presentation Slides
-
Age-Friendly Health Systems -- [HTML Version] [PDF Version]
-
Alzheimer's Disease and Related Dementias Research Update -- [HTML Version] [PDF Version]
-
Care Planning and Health Information Technology: How to Aid Dementia Quality Care -- [HTML Version] [PDF Version]
-
Clinical Care Subcommittee Agenda: Advancing Consensus on Dementia Care Elements to Guide New Outcomes Measurement -- [HTML Version] [PDF Version]
-
Clinical Subcommittee Update -- [HTML Version] [PDF Version]
-
Defining Quality Dementia Care -- [HTML Version] [PDF Version]
-
Final Report to the NAPA Advisory Council -- [HTML Version] [PDF Version]
-
Long-Term Services and Supports Committee Update -- [HTML Version] [PDF Version]
-
Quality Care from the Perspectives of People Living with Dementia -- [HTML Version] [PDF Version]
-
Research Summit on Dementia Care: Building Evidence for Services and Supports Process Report -- [HTML Version] [PDF Version]
-
Testing the Promise of Primary Care: Comprehensive Primary Care Plus (CPC+) -- [HTML Version] [PDF Version]
-
Updates and Follow-Up from January Meeting -- [HTML Version] [PDF Version]