
Friday, April 27, 2018
Printer Friendly Version in PDF Format (13 PDF pages)
Testing the Promise of Primary Care: Comprehensive Primary Care Plus (CPC+)
Laura Sessums, JD, MD, FACP
Director, Division of Advanced Primary Care
Center for Medicare & Medicaid Innovation
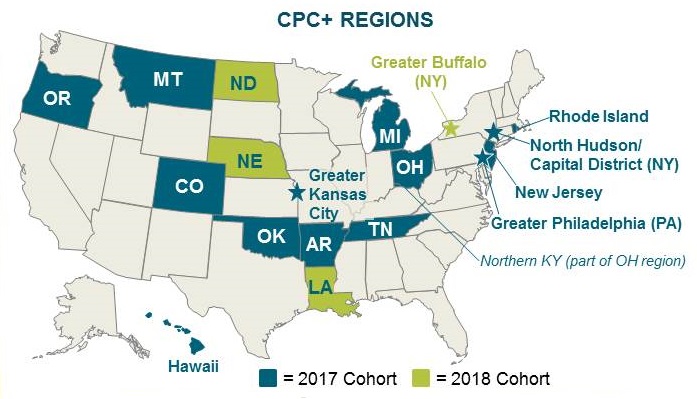
Comprehensive Primary Care Plus
| America's largest-ever initiative to transform primary care |
|---|
 |
|
CPC+ Logic Model
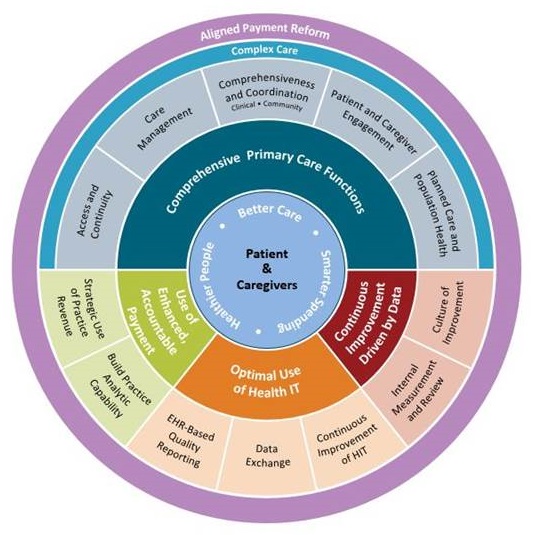 |
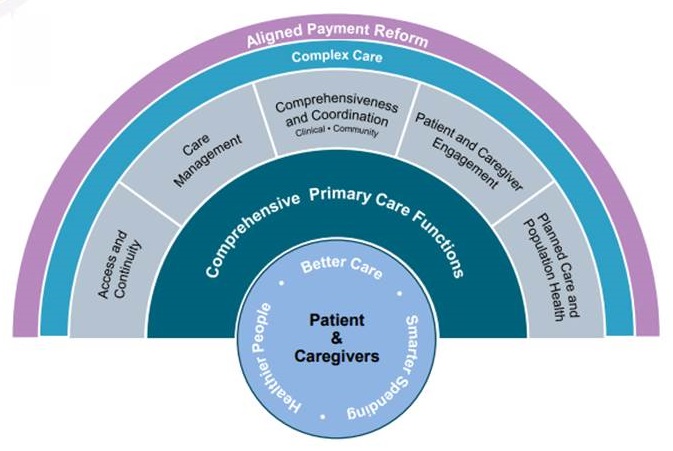
Five functions guide CPC+ care delivery transformation
 |
| Online Resources: Care Delivery Transformation Brief, Video, and Practice Requirements |
CPC+ Practices Enhance Care Delivery Capabilities Each Program Year
| <---------- | ------------Track---> | |
|---|---|---|
| <---Track 1---> | ||
| Access and Continuity | 24/7 patient access Empanelment Organize care for continuity Measure continuity of care |
Care delivered outside of traditional visits Empanelment  |
| Care Management | Risk stratify patient Two-step risk stratification Care management ED and hospital follow-up |
Two-step risk stratification Care plans |
| Comprehensiveness and Coordination | Identify specialists Collaborative care agreements EDs and hospitals information transfer Behavioral health integration |
Collaborative care agreements  Behavioral health integration Social service linkages Develop capabilities for complex patients Psychosocial assessment Address psychosocial needs Comprehensive medication management |
| Patient and Caregiver Engagement | Annual PFAC Biannual PFAC Assess self-management capabilities Self-management support |
Biannual PFAC Quarterly PFAC Self-management support Advance care planning |
| Planned Care and Population Health | Improve population health with data | Data-driven improvement by care teams |
| Year 1 requirements Year 2 requirements Integrated with enhanced Health IT for Track 2 |
||
Beneficiaries Attributed to the Complex Tier in Q1 2018
- 1,535 practices in Track 2
- 1,081,158 total attributed Medicare FFS beneficiaries
- 141,355 beneficiaries attributed to the complex tier (13.1%)
| Among 141,355 beneficiaries in the complex tier: |
|---|
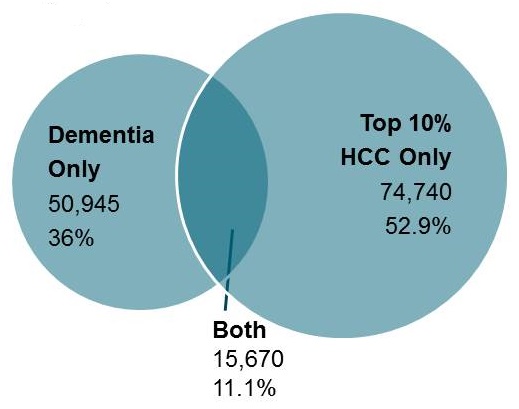 |
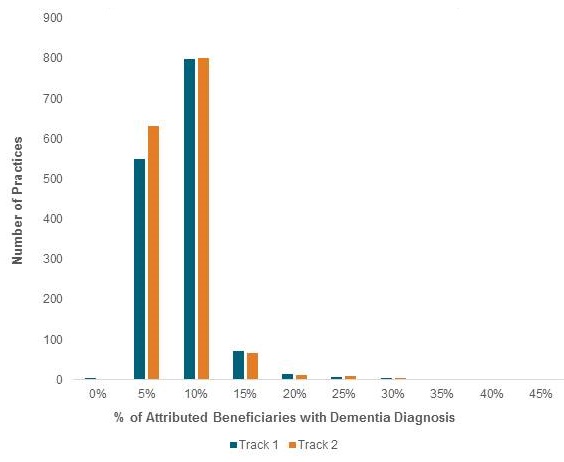
Nearly All Practices Treat Beneficiaries with Dementia, in Both Tracks
- On average, 6% of attributed beneficiaries have dementia flag
- Despite differences in CPC+ payment, Track 1 and 2 practices have roughly the same distribution
- Handful of practices have <1% or >45% of attributed beneficiaries with dementia
| Distribution of % of Beneficiaries with Dementia |
|---|
 |
CPC+ Quality Goals
- Incentive based on quality, patient experience, and utilization
- Improve quality performance as measured by electronic clinical quality measures (eCQMs)*
- * eCQM practice site reports must use 2015 Edition (c)(4) health IT
- Improve patient experience as measured by Consumer Assessment of Healthcare Providers and Systems (CAHPS) survey
- Decrease unnecessary utilization of care as measured by claims
- Patient reported outcome-based performance measure (PRO-PM) under development for Track 2 Only
- Improve quality performance as measured by electronic clinical quality measures (eCQMs)*
2018 CPC+ Quality Measure Set
- Outcome Measures (Report Both)
- Controlling High Blood Pressure
- Diabetes: Hemoglobin A1c Poor Control
- Other Measures (Choose 7 to Report)
- Breast Cancer Screening
- Cervical Cancer Screening
- Colorectal Cancer Screening
- Diabetes: Eye Exam
- Diabetes: Medical Attention for Nephropathy
- Closing the Referral Loop: Receipt of Specialist Report
- Use of High Risk Medications in the Elderly
- Preventive Care and Screening: Screening for Depression & Follow-Up Plan
- Depression Utilization of the PHQ-9 Tool
- Dementia: Cognitive Assessment
- Tobacco Use: Screening and Cessation Intervention
- Initiation & Engagement of Alcohol & Other Drug Dependence Treatment
- Falls: Screening for Future Falls Risk
- Influenza Immunization
- Pneumococcal Vaccination Status for Older Adults
- Ischemic Vascular Disease (IVD): Use of Aspirin or Another Antiplatelet
- Statin Therapy for the Prevention & Treatment of Cardiovascular Disease
CPC+ Data Feedback Approach
- Attribution/Payment Data
- Quarterly list of Medicare FFS beneficiaries attributed, by risk tier
- Quarterly financial support amounts
- Quality and Care Delivery Data
- Performance on Electronic Clinical Quality Measures and CAHPS surveys
- Quarterly report on care delivery requirements
- Data Sharing Levers
- Cost and Utilization Data
- Expenditures: professional services, inpatient, outpatient, SNFs, etc.
- Utilization: inpatient, 30-day readmission, ED utilization
- Multi-Payer Aggregation
- Aligned report with multi-payer data
- Allows clinicians to view entire patient population
- Reduces burden; enhances care coordination and population health
- Cost and Utilization Data
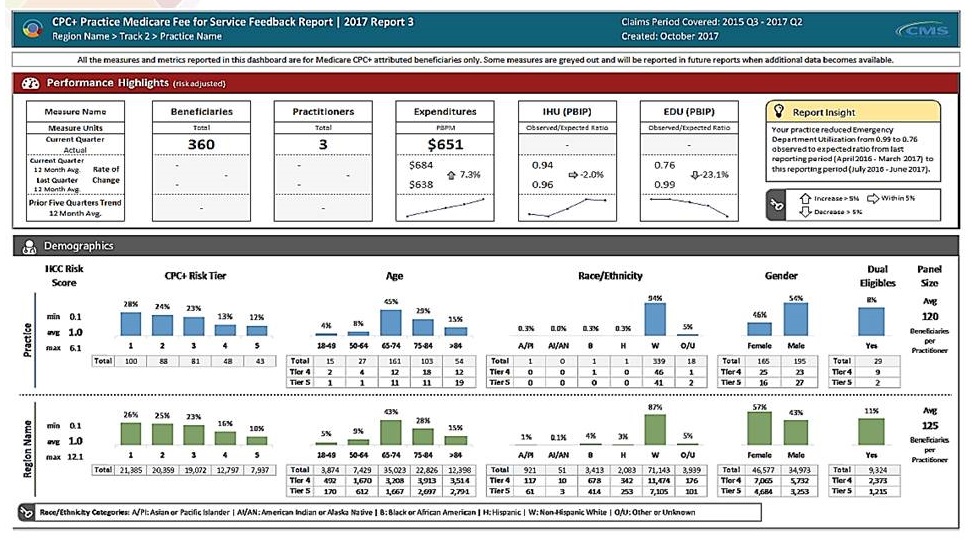
Practice Performance & Demographics (Dummy Data)
 |
Many Opportunities for Learning, Collaboration, and Support
- Building the CPC+ community
- Live & On-Demand Events:
- Onboarding webinar series
- Groups for similar practices
- Local Collaboratives:
- In-person learning sessions
- CPC+ Connect
- Online collaboration tool and knowledge sharing platform
- Live & On-Demand Events:
- Targeted supports
- Regional outreach for practices in need
- Written Guidance:
- Implementation Guide and Operational How-To
- Biweekly FAQs & weekly newsletter
- CPC+ Support available for programmatic questions
Interested in CPC+?
- Visit https://innovation.cms.gov/initiatives/Comprehensive-Primary-Care-Plus
- Email CPCplus@cms.hhs.gov
Extra Slides
Collaborative Care Agreements
- By the end of the first year, many practices enacted collaborative care agreements with specialists especially important for dementia population
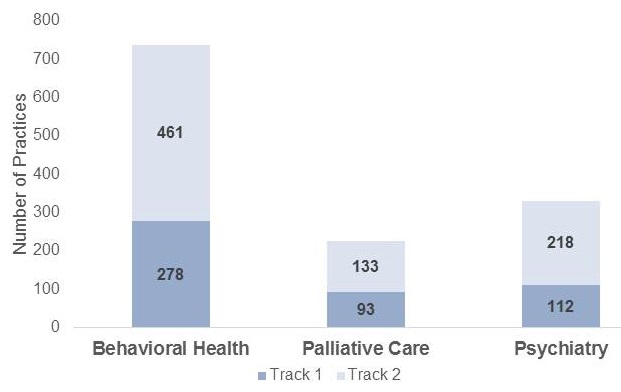 |
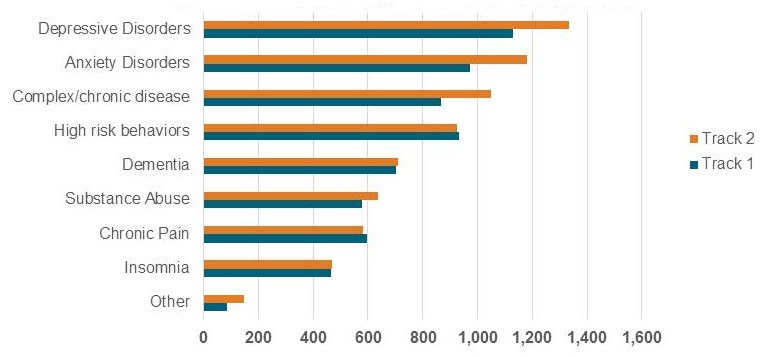
Behavioral Health Integration
- Half of all CPC+ practices indicate that dementia is a targeted mental health condition for their behavioral health strategy
 |
Social Service Linkages
- Practices screening patients for unmet social needs increased over year one
| Percentage of Practices Screening Patients |
|---|
 |
Multi-Payer Partnership Supports Comprehensive Primary Care Reform
- Payer Partnership Framework
- Enhanced, non-fee-for-service support for Track 1 and 2 practices to meet the aims of the care delivery model
- Performance-based incentive payments for Track 1 and 2 practices
- Change in cash flow mechanism from fee-for-service to at a least a partial alternative payment methodology for Track 2 practices
- Practice and member-level cost and utilization data at regular intervals for all practices
- Aligned quality and patient experience measures with Medicare FFS and other payers in the region
Health IT Vendor Partnership for CPC+ Track 2 Advanced Functionalities
- Vendor Partnership Framework
- Work closely with Track 2 practices to develop and optimize advanced health IT capabilities.
- Designate a CPC+-specific point of contact for available to practices.
- Designate an executive contact responsible for overseeing the partnership with CMS.
- Participate in monthly conference calls with CMS, and yearly capability re-attestation.
- Participate in CPC+ national and regional learning events on advanced health IT capabilities and the CPC+ care delivery model.
Three Payment Innovations Support CPC+ Practice Transformation
| Care Management Fee (PBPM) | Payment Structure Redesign | Performance-Based Incentive Payment (PBPM) | |
|---|---|---|---|
| Objective | Support augmented staffing and training for delivering comprehensive primary care | Reduce dependence on visit-based fee-for-service to offer flexibility in care setting | Reward practice performance on utilization and quality of care |
| Track 1 | $15 average (ranges from $6 to $30) | N/A (Medicare FFS) | $2.50 opportunity |
| Track 2 | $28 average (ranges from $9 to $100) | Hybrid Payment: a combination of upfront "Comprehensive Primary Care Payment" and reduced FFS claims | $4.00 opportunity |
| CPC+ practices also in the Medicare Shared Savings Program participate in their ACO's shared savings/loss arrangement INSTEAD of receiving CPC+ incentive payments. | |||
A Closer Look: Care Management Fee
| CMS uses CMS-HCC scores: Hierarchical Condition Categories |
|---|
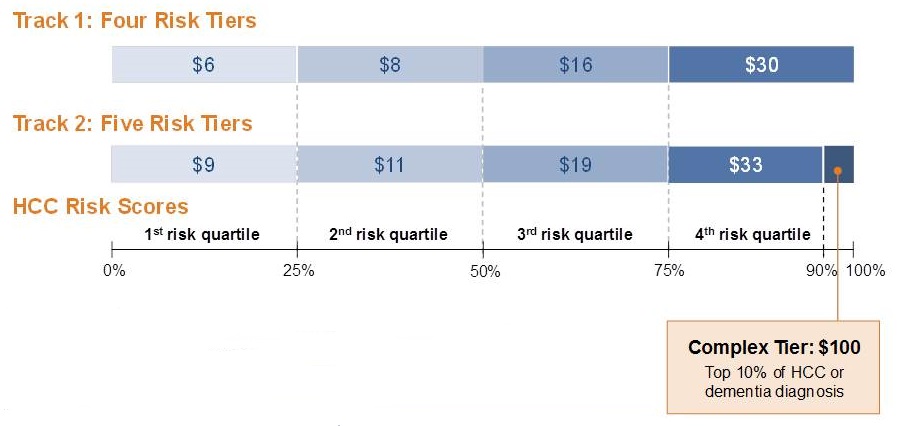 |
| Total CMF Medicare Payments by Track for 2017 |
|---|
 |
Track 2 Reimbursement Redesign Offers Flexibility in Care Delivery
- Designed to promote care delivery beyond office visits
- Practices receive enhanced fees with roughly half of expected FFS payments upfront and subsequent FFS billings reduced by the prepaid amount
- CPCP reduces incentive to bring patients into the office for a visit but maintenance of some FFS allows for flexibility to treat patients in accordance with their preferences
- Practices select the pace at which they will progress towards one of two hybrid payment options (both roughly 50/50) by 2019
| Hybrid of FFS and Upfront "Comprehensive Primary Care Payment" (CPCP) for Evaluation & Management |
|---|
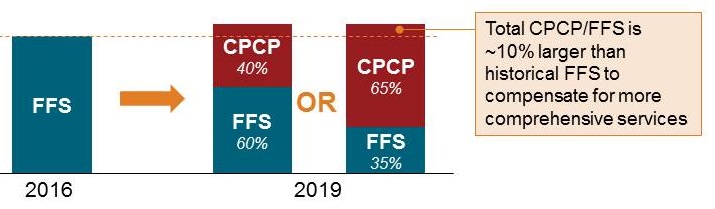 |
2017: Track 2 Practices by Hybrid Payment Choice
 |
| Figures based on data from the first quarter of CPC+ (Jan - Mar 2017). These figures do not represent an evaluation of this work or CPC+ itself. For more information, visit: https://innovation.cms.gov/initiatives/comprehensive-primary-care-plus |
Performance-Based Incentive Payment
| Based on performance on CAHPS, eCQMs, and Utilization metrics |
|---|
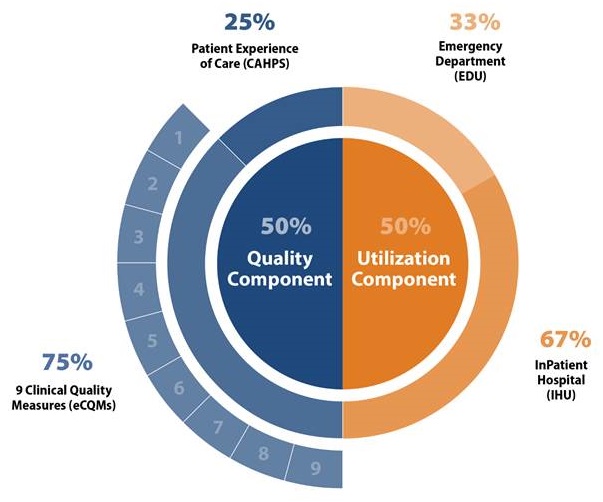 |
Overview of the CPC+ Evaluation
- Providing an independent, rigorous evaluation with rapid, actionable feedback
- Implementation Study
- Who participates in Comprehensive Primary Care Plus (CPC+)?
- What payments, data feedback, learning, and health IT supports does CPC+ provide?
- How do CPC+ practices transform care delivery?
- What are the barriers and facilitators to implementation of the model?
- Impact Study
- What are the effects of CPC+ on Medicare fee-for-service (FFS) (and in some regions Medicaid) cost, service use, and quality of care? Beneficiaries' experience of care? Practitioner and staff experience?
- Compare the change over time among CPC+ practices and comparison practices that were similar before CPC+ began.
- Synthesis of Findings
- Links changes in how practices deliver care with changes in outcomes
- Describes lessons learned for scalability and spread
- Implementation Study
April 27, 2018 -- Advisory Council Meeting #28
The meeting was held on Friday, April 27, 2018, in Washington, DC. During the meeting, the Clinical Care Subcommittee took charge of the theme, focusing on advancing consensus on dementia care elements to guide new outcomes measurement. The Council heard speakers in two sessions, one focused on developing consensus about dementia care elements, and the second on models that are informing outcomes measurement. The meeting also included updates on work from the previous meetings, a presentation on the final report from the October 2017 Care Summit, and federal workgroup updates. Material available from this meeting is listed below or at https://aspe.hhs.gov/advisory-council-alzheimers-research-care-and-services-meetings#Apr2018.
Comments and questions, or alerts to broken links, should be sent to napa@hhs.gov.
General Information
-
Agenda -- [HTML Version] [PDF Version]
-
Meeting Announcement -- [HTML Version] [PDF Version]
-
Meeting Summary -- [HTML Version] [PDF Version]
-
Public Comments -- [HTML Version]
Handouts
-
Main Summit Recommendations -- [HTML Version] [PDF Version]
-
National Research Summit on Care, Services, and Supports for Persons with Dementia and Their Caregivers: Report to the National Advisory Council on Alzheimer's Research, Care, and Services -- [HTML Version] [PDF Version]
Presentation Slides
-
Age-Friendly Health Systems -- [HTML Version] [PDF Version]
-
Alzheimer's Disease and Related Dementias Research Update -- [HTML Version] [PDF Version]
-
Care Planning and Health Information Technology: How to Aid Dementia Quality Care -- [HTML Version] [PDF Version]
-
Clinical Care Subcommittee Agenda: Advancing Consensus on Dementia Care Elements to Guide New Outcomes Measurement -- [HTML Version] [PDF Version]
-
Clinical Subcommittee Update -- [HTML Version] [PDF Version]
-
Defining Quality Dementia Care -- [HTML Version] [PDF Version]
-
Final Report to the NAPA Advisory Council -- [HTML Version] [PDF Version]
-
Long-Term Services and Supports Committee Update -- [HTML Version] [PDF Version]
-
Quality Care from the Perspectives of People Living with Dementia -- [HTML Version] [PDF Version]
-
Research Summit on Dementia Care: Building Evidence for Services and Supports Process Report -- [HTML Version] [PDF Version]
-
Testing the Promise of Primary Care: Comprehensive Primary Care Plus (CPC+) -- [HTML Version] [PDF Version]
-
Updates and Follow-Up from January Meeting -- [HTML Version] [PDF Version]