
Friday, April 27, 2018
Printer Friendly Version in PDF Format (13 PDF pages)
Age-Friendly Health Systems
Amy Berman, Kedar Mate
Institute for Healthcare Improvement
The John A. Hartford Foundation
Agenda
- Age-Friendly Health System
- Brief Review of Other Initiatives Related to Dementia
AFHS: Situation and background
- "Triple Threat"
- Demography
- Utilization
- Disutility
- Counties Included in Data Set:
- Livingston
- Macomb
- Monroe
- Oakland
- Washtenaw
- Wayne
| Population Growth by Age Group 2010-2040 |
|---|
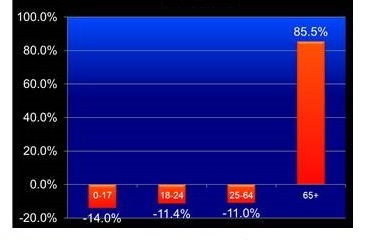 |
Know-do gap
- We have lots of evidence-based geriatric-care models of care that have proven very effective
- Yet, most reach only a portion of those who could benefit
- Difficult to disseminate and scale
- Difficult to reproduce in settings with less resources
- Most do not apply across settings of care (e.g. hospital and home)
- The portion programs are reaching today is about 4 million of our 46 million older adults
Improving the Health of Older Adults
- $565,000,000
- Amount invested in aging and health since 1982
- Age-Friendly Health Systems
- Family Caregiving
- Serious Illness and End-of-Life
What is an Age-Friendly Health System?
- A system in which every older adult 65+:
- Gets the best care possible;
- Experiences no healthcare-related harms;
- Is satisfied with the health care; and
- Realizes optimal value.
AIM
- By 2020, we will reach older adults cared for in 20% of US health care facilities
Deriving the Evidence-based interventions
- Reviewed 17 evidence-based models and programs serving older adults:
- What population is served?
- What outcomes were achieved?
- What are the core features of the model?
July - August 2016
- 90 discrete core features identified by model experts in pre-work
- Redundant/similar concepts removed and 13 core features synthesized by IHI team
- Expert Meeting led to the selection of the "vital few": the 4Ms
The Four M's
- What Matters: Knowing and acting on each patient's specific health goals and care preferences
- Medication: Optimizing medication use to reduce harm and burden, focused on medications affecting mobility, mentation, and what matters
- Mentation: Identifying and managing depression, dementia and delirium across care settings
- Mobility: Maintaining mobility and function and preventing complications of immobility
Evidence-base
- What Matters:
- Asking what matters and developing an integrated systems to address it lowers inpatient utilization (54% dec), ICU stays (80% dec), while increasing hospice use (47.2%) and pt satisfaction (AHRQ 2013)
- Medications:
- Older adults suffering an adverse drug event have higher rates of morbidity, hospital admission and costs (Field 2005)
- 1500 hospitals in HEN 2.0 reduced 15,611 adverse drug events saving $78m across 34 states (HRET 2017)
- Mentation:
- Depression in ambulatory care doubles cost of care across the board (Unutzer 2009)
- 16:1 ROI on delirium detection and treatment programs (Rubin 2013)
- Mobility:
- Older adults who sustain a serious fall-related injury required an additional $13,316 in hospital operating cost and had an increased LOS of 6.3 days compared to controls (Wong 2011)
- 30+% reduction in direct, indirect, and total hospital costs among patients who receive care to improve mobility (Klein 2015)
References at end of slides
Affiliates
- The John A. Hartford Foundation
- Institute for Healthcare Improvement
- Trinity Health
- Kaiser Permanente
- Scension
- Providence St. Joseph Health
- Anne Arundel Medical Center
- Catholic Health Association of the United States
- The Joint Commission
- American Hospital Association
A sample of tests being run by our health system teams
- Glacier Hills: Moving to single document, work flow, documentation of What Matters conversation
- Glacier Hills: Education of providers about asking What Matters questions using Being Mortal film
- St. Alphonsus: What Matters Most to You flyer
- St. Alphonsus: Testing Serious Illness Conversation Guide questions
- St. Alphonsus: Asking What Matters questions in Assessment Bundle
- St. Alphonsus: Moving advance care planning documents/ advanced directives to the next level/site of care or provider at discharge
- St. Mary Mercy: Integrate What Matters questions into geriatrics assessment
- Providence: Testing Scotland What Matters questions
- KP: Knowing older adults through "My Care My Life" binder
- Ascension: Assessing caregiver burden with caregivers and patients
- Ascension: Information on website about services and to enable self-referral
- Ascension: Streamlined patient access Referral and intact process
- St. Alphonsus: Bring home med containers to AWV for better med rec
- St. Alphonsus: Checking home meds with provider profile in EMR with every admit
- St. Alphonsus: Obtaining med list from pharmacy to review for deprescribing
- St. Alphonsus: Education guide based on Med Rec Guide
- St. Mary Mercy: Medication review for pill burden and sending deprescribing recommendations to pharmacy
- Providence: PharmD reviews med list for high risk meds and recommends de-prescribing to PCP
- PACE: Pharmacovigilance review with ER/hospital utilization review
- Anne Arundel: Established an Age-Friendly prescribing "culture"; Looking for opportunities to scale-up to other units
- KP: Patients encouraged to bring personal items to hospital to create a "Just like home" environment
- KP: Coaching for staff to develop personal relationship with pts
- KP: Educate providers re medication issues for deprescribing and treatment of delirium
- KP: Self-care plan for high-risk patients, case manager creates plan to include hydration and nutrition
- Glacier Hills: Screening (bCAM), standard intervention for delirium
- St. Alphonsus: Assessment with mini-cog and PHQ2
- St. Mary Mercy: Communication re 3D delirium assessment
- St. Mary Mercy: Assessment with family member involvement
- Anne Arundel: Hydration- geriatric cups
- Glacier Hills: Assessment tool with what matters most about mobility
- Glacier Hills: Workflow, PT referral to wellness center, education
- St. Alphonsus: Timed Get Up and Go assessment
- St. Mary Mercy: Matter of balance, check your risk for falling (CDC) plus meds
- St. Mary Mercy: Story book, shorts, What Matters document, thank you letters, MOVE (mobility optimizes virtually everything)
- Providence: STEADI results at annual wellness visit, patient who has fallen or with specific STEADI score has follow up visit with RN to address risk factors
- Providence: Measure mobility with STEADI scores at AWV year-over-year
- Providence: Patient who has fallen or with specific STEADI score participate in a shared medical appointment; PharmD reviews med list for high risk meds and recommends deprescribing to PCP
- KP: Patient-initiated patient mobilization, MD's provide 1-page prompt with exercises (includes exercises for patients in bed and wheelchair)
- Anne Arundel: Mobility/quality tech
- Anne Arundel: 6-clicks, refer to PT
How will we reach more older adults and when can health systems get involved?
 |
Results from prototyping units
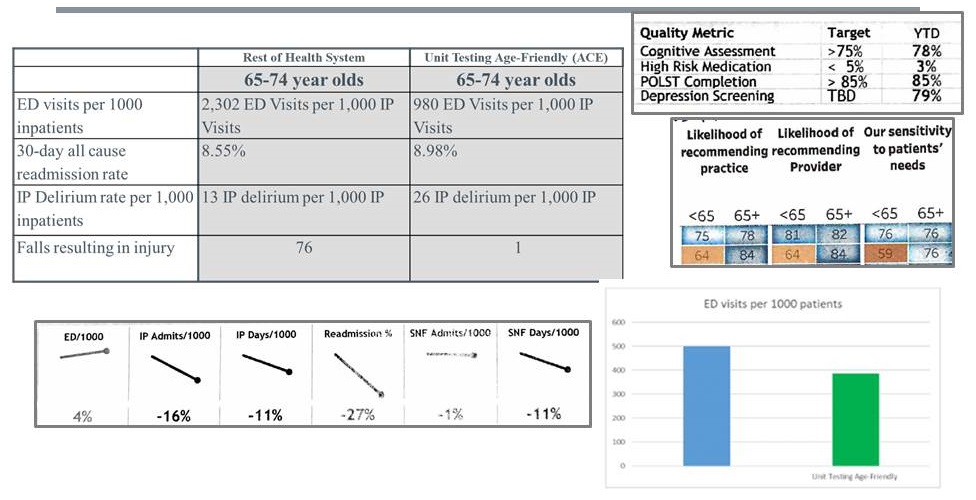 |
What matters protocol
| Clinical Steps | Content/Intent/Hints | Suggested Questions/Steps/Actions: |
|---|---|---|
| 1. Set Up: |
|
Consider what will help you have a successful conversation. This includes things such as hearing, language, eye contact, body language, patient history, spiritual beliefs, etc. |
2. Invite the patient to the conversation:
|
Taking time to let the patient know why you are asking these questions can help the patient understand why you want to know what is important to them. This explanation can be personalized for each patient or situation. |
"Our team here at Providence believes that knowing what is important to you will help us better understand how to help you meet your goals. Is it okay if I ask you a few questions?" Open ended questions to consider: 1. What makes you happy? 2. What worries you? |
| 3. Ask the question: |
|
Please use following questions in the following order: 3. What are your biggest concerns about your health when you think about the future? |
| 4. Summarize + Action Planning: |
|
4. What steps can we take to help you get there? 5. What else would you like us to know about you? (optional) Summaries + Action Planning may be something like:
|
| 5. New Steps |
|
|
| 6. Document: |
|
EPIC dot phrase -- .pcc |
Documentation
 |
Creating Age-Friendly Health Systems: A National View of Progress
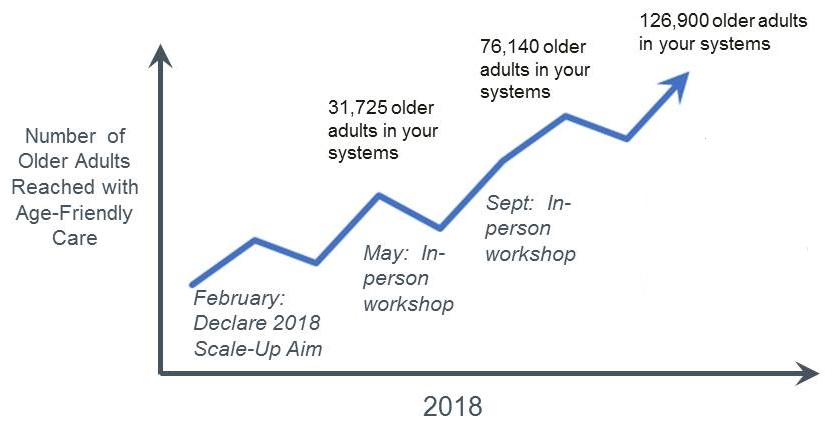 |
Changes to become Age-Friendly system-wide
- Support front-line teams to adopt 4Ms of Age-Friendly Health system
- Board and C-suite commitment to AFHS
- Routine board agenda item
- Executive compensation incentive
- Letter of commitment
- Integration into strategic plan & executive dashboard measures
- Appears in 2019 strategic plan
- Resourcing plan for AFHS
- Primary pt outcome & system quality measures stratified by age
- Evidence-based clinical changes (4Ms) integrated into front-line clinical practice
- Develop awareness & skills in 4Ms
- EHR integration of 4Ms
- Workflow integration of 4Ms
- Job role integration of 4Ms
- Major care pathways include 4Ms
- Patient, family & caregiver participation in governance and relevant committees
- Older adult representation in Board committee
- Older adult, family, caregiver engagement in practices committees & clinical governance
- Formal partnership with community organizations
- Clear service navigation partners identified by system
- Preferred partnerships with social service providers for older adults
- Board and C-suite commitment to AFHS
Age-Friendly Health System What Really Matters Advisory Committee
- "Nobody ever asks 'what matters to you?' They ask 'what pain level do you have?' 'What's your problem today?' But what really matters just never came up. That has been a failing. I applaud you for coming forward with this. I think It will really improve the patient experience and their health. And as an older person I am looking forward to it."
What's next?
- This is our moment. It is time for an Age-Friendly system of care that touches every single older adult in this country.
- First 5 systems, scaling up across their systems
- This summer we will launch 4 mini-collaboratives to engage other institutions around the country
- Formalizing the business case, a "What Matters" starter kit, EHR guidance, policy guidance.
Achieving Measurable Impact with Grantee Partners
- UCLA Alzheimer's and Dementia Care Program: uses NP dementia care managers to assess health, offer treatment, develop care plans, make referrals to community-based services for patient and family caregiver support.
- CMMI Health Care Innovation Award (2012), current JAHF grantee preparing for dissemination
- Model shows1
- Reductions in:
- hospitalizations due to ambulatory care sensitive conditions (7/1,000 pts)
- 30-day readmissions (41/1,000 pts)
- nursing home placement (25% lower rate)
- cost ($605 less per pt per quarter)
- Improvements in:
- understanding and mgmt of dementia
- self-care among caregivers
- access to community-based support
- Branand, B., et al. "HCIA Disease-Specific Evaluation: Third Annual Report." NORC, 2017
- Reductions in:
- Moving and Scaling Home-Based Primary Care (HBPC): 3-part initiative (data registry, workforce development, payment policy) to improve health for most frail older adults living in the community.
- Independence at Home demo1:
- $25 m in Medicare savings in 1st year
- $3,070 per beneficiary
- VA HBPC Program2:
- Reductions in:
- hospital days (89%)
- nursing home days (59%)
- 30-day readmissions (21%)
- $9,000 savings per veteran
- Reductions in:
- CMS, "Affordable Care Act payment model saves more than $25 million in first performance year," June 2015
- Edes, T. et al. (2014), Better access, quality, and cost for clinically complex veterans with home-based primary care J Am Geriatr Soc, 62: 1954-1961
- Independence at Home demo1:
- Benjamin Rose Institute on Aging & Family Caregiver Alliance: Online Resource to Compare Dementia Caregiving Programs
- Web-based resource aims to help health and social service organizations compare, select and implement evidence-based programs for dementia caregiving
- These evidence-based programs for dementia caregiving improve caregiving skills, reduce caregiver stress, mitigate negative affects on physical and emotional health, finances and family relationships.
- There are approximately 50 evidence-based programs that address the needs of family caregivers of people living with dementia.
- PACE 2.0 (National PACE Assoc.): Adapting and expanding access to Programs of All-Inclusive Care for the Elderly.
- Model provides all needed preventive, primary, acute and long term care services for nursing home eligible patients
- PACE participants report being healthier, happier and more independent than counterparts in other care settings1
- Next phase builds on PACE Innovation Act, will identify:
- underserved subpopulations currently eligible to enroll
- new unserved populations, such as younger adults with physical or mental challenges
- Leavitt, M., Secretary of Health and Human Services. (2009). Interim report to Congress. The quality and cost of the Program of All-Inclusive Care for the Elderly
April 27, 2018 -- Advisory Council Meeting #28
The meeting was held on Friday, April 27, 2018, in Washington, DC. During the meeting, the Clinical Care Subcommittee took charge of the theme, focusing on advancing consensus on dementia care elements to guide new outcomes measurement. The Council heard speakers in two sessions, one focused on developing consensus about dementia care elements, and the second on models that are informing outcomes measurement. The meeting also included updates on work from the previous meetings, a presentation on the final report from the October 2017 Care Summit, and federal workgroup updates. Material available from this meeting is listed below or at https://aspe.hhs.gov/advisory-council-alzheimers-research-care-and-services-meetings#Apr2018.
Comments and questions, or alerts to broken links, should be sent to napa@hhs.gov.
General Information
-
Agenda -- [HTML Version] [PDF Version]
-
Meeting Announcement -- [HTML Version] [PDF Version]
-
Meeting Summary -- [HTML Version] [PDF Version]
-
Public Comments -- [HTML Version]
Handouts
-
Main Summit Recommendations -- [HTML Version] [PDF Version]
-
National Research Summit on Care, Services, and Supports for Persons with Dementia and Their Caregivers: Report to the National Advisory Council on Alzheimer's Research, Care, and Services -- [HTML Version] [PDF Version]
Presentation Slides
-
Age-Friendly Health Systems -- [HTML Version] [PDF Version]
-
Alzheimer's Disease and Related Dementias Research Update -- [HTML Version] [PDF Version]
-
Care Planning and Health Information Technology: How to Aid Dementia Quality Care -- [HTML Version] [PDF Version]
-
Clinical Care Subcommittee Agenda: Advancing Consensus on Dementia Care Elements to Guide New Outcomes Measurement -- [HTML Version] [PDF Version]
-
Clinical Subcommittee Update -- [HTML Version] [PDF Version]
-
Defining Quality Dementia Care -- [HTML Version] [PDF Version]
-
Final Report to the NAPA Advisory Council -- [HTML Version] [PDF Version]
-
Long-Term Services and Supports Committee Update -- [HTML Version] [PDF Version]
-
Quality Care from the Perspectives of People Living with Dementia -- [HTML Version] [PDF Version]
-
Research Summit on Dementia Care: Building Evidence for Services and Supports Process Report -- [HTML Version] [PDF Version]
-
Testing the Promise of Primary Care: Comprehensive Primary Care Plus (CPC+) -- [HTML Version] [PDF Version]
-
Updates and Follow-Up from January Meeting -- [HTML Version] [PDF Version]