
Friday, July 28, 2017
Printer Friendly Version in PDF Format (8 PDF pages)
Managing chronic conditions in people living with dementia
Deirdre Johnston, MB BCh
Assistant Professor, Department of Psychiatry and Behavioral Sciences
Co-Investigator and Clinical Intervention Director, MIND at Home
Disclosures
- National Institute on Aging (grant)
- National Institute of Mental Health (grant)
- Centers for Medicare & Medicaid Services (grant)
- The Associated (grant)
- The Hoffberger Family Philanthropies (grant)
- Richman Philanthropies (grant)
- Broadmead Retirement Community (consultant)
- Co-founder, MIND at Home Halo
Objectives
- Briefly describe impact of dementia on chronic conditions, outcomes and costs
- Provide overview of baseline comorbidities of MIND at Home enrollees
- Brief comment on implications for practice
Chronic disease self-management
- Dementia: progressive, irreversible, impairment of cognitive and executive function
- Capacity to self-manage is progressively lost
- Early intervention and caregiver education needed to prevent medication errors and complications
- Commonly heard in clinic: "I don&'t want to take his/her independence away."
Multimorbidity in dementia
- The average person with dementia has four comorbid chronic conditions. (Guthrie et al, BMJ 2012)
- Clinical guidelines focus on one disorder
- Fragmented care is the norm
Multimorbidity and polypharmacy
- Older adults with dementia see
- multiple providers
- for multiple chronic conditions
- in different settings (Callahan et al, 2014)
- Each comorbid condition may have its own treatment protocol
- including one or more medications
Most Frequent Co-morbid Conditions of MIND at Home Participants at Baseline
(CMS and NIA)
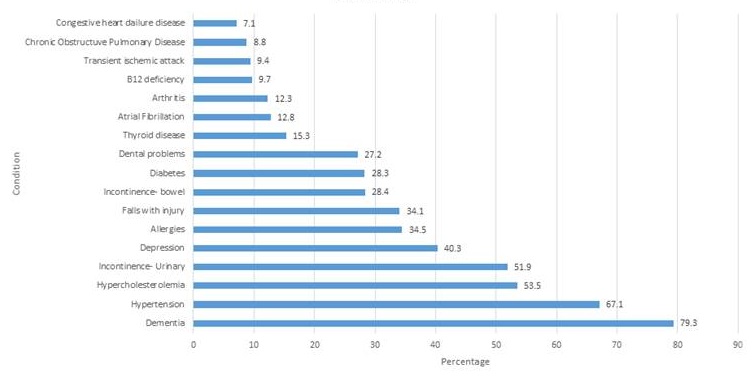 |
| All participants in CMMI MIND at Home demonstration project plus NIA randomized controlled trial (N=647) |
Dementia Diagnosis at Baseline
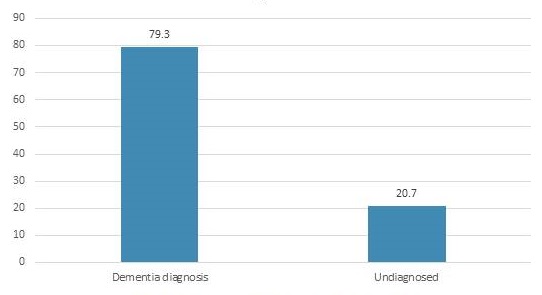 |
| MIND at Home RCT and HCIA, pooled data (N= 647) |
Number of Medications at baseline
- Participants:
- 8.23
- Caregivers:
- 5.07
Dementia is underdiagnosed
- Cognitive impairment is under-recognized and under-documented (Brodaty et al., 1994; Callahan et al., 1995; Eefsting et al., 1996; Bush et al., 1997; Lo¨ppo¨nen et al., 2003)
- Physicians' reasons for not diagnosing/documenting:
- time constraints
- cost
- stigma
- futility (Martin et al., BMC 2015)
Medications
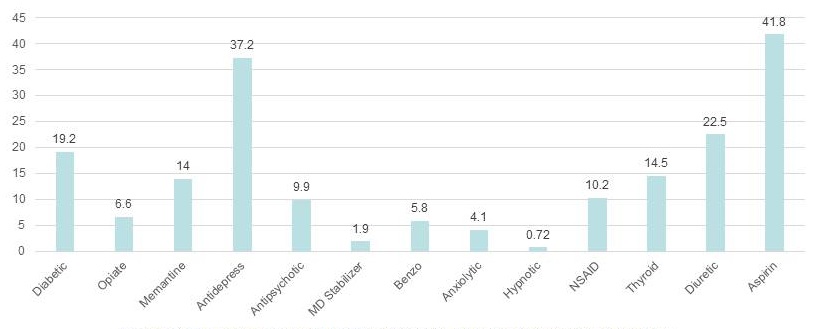 |
| Figure 1: The percentage of MIND participants on some commonly prescribed medications at baseline. 43% had medication use and adherence needs |
Cost implications of unmanaged chronic disease in dementia
- Most care costs for acute in-patient and institutional/long stay care (Gitlin et al., 2007)
- 25% of Medicare beneficiaries' costs are incurred in the last year of life (Hogan et al, Med Care, 2013)
- People with dementia have 80% higher rates of potentially avoidable hospitalizations (Phelan et al, 2012)
- Dementia diagnosis associated with higher costs of anti-dementia drug treatment, but with lower total medical care costs (Michalowsky et al., Int Psychogeriatr 2016)
Impact of dementia on co-existing chronic conditions
- Loss of ability to self-manage chronic conditions
- Associated with lower continuity of care, higher utilization:
- ED visits
- hospitalizations
- testing
- costs (Amjad et al, JAMA 2016).
- Early diagnosis and pro-active management of chronic conditions needed
- Caregiver education and support necessary
Reasons to screen and diagnose
- To treat and manage dementia
- Educate and support caregiver
- Address and manage comorbid conditions by:
- Eliminating unnecessary medications
- Helping caregiver cope
- Educating caregiver on managing the dementia and the comorbidities
- Reducing caregiver burden
- E.g, Some CGs make multiple trips to pharmacy per month
Summary and recommendations
- Dementia can be treated and managed
- Management of dementia includes managing the comorbidities
- Caregiver education
- Identification of high risk dyads
- Support and coaching
- Adaptation of care plan to changing needs
- Provider education/awareness to increase detection and treatment
- Workforce adaptation (e.g., Memory Care Coordinators)
- Attention to diversity and sensitivity to end of life care needs
July 28, 2017 -- Advisory Council Meeting #25
The meeting was held on Friday, January 26, 2018, in Washington, DC. The Research Subcommittee took charge of this meeting's theme, focusing on the process from targets to treatments. The Council heard speakers on the preclinical pipeline, the clinical trial pipeline, and the industry perspective. The meeting also included discussion of a driver diagram to guide the Council's future work, updates and a report from the October Care Summit, and federal workgroup updates. Material available from this meeting is listed below and is also available at https://aspe.hhs.gov/advisory-council-alzheimers-research-care-and-services-meetings#Jan2018.
Comments and questions, or alerts to broken links, should be sent to napa@hhs.gov.
General Information
-
Agenda -- [HTML Version] [PDF Version]
-
Meeting Announcement -- [HTML Version] [PDF Version]
-
Meeting Summary -- [HTML Version] [PDF Version]
-
Public Comments -- [HTML Version]
Presentation Slides
-
2017 National Plan Update and Non-Federal Recommendations -- [HTML Version] [PDF Version]
-
Clinical Services Subcommittee Federal Update -- [HTML Version] [PDF Version]
-
CommunityRx for Community-Residing People with Dementia and Their Caregivers -- [HTML Version] [PDF Version]
-
Dementia Caregiving in the U.S. -- [HTML Version] [PDF Version]
-
Development of the FY 19 NIH Bypass Budget for Alzheimer's Disease and Related Dementias -- [HTML Version] [PDF Version]
-
Implications of a Biologically Based Definition of Alzheimer's Disease -- [HTML Version] [PDF Version]
-
Increasing Opportunities for Choice and Control for Persons with Dementia -- [HTML Version] [PDF Version]
-
Interventions to Prevent or Slow Cognitive Decline, MCI and Dementia in Individuals without Dementia -- [HTML Version] [PDF Version]
-
Living Alone With Dementia -- [HTML Version] [PDF Version]
-
Long-Term Services and Supports Committee Update -- [HTML Version] [PDF Version]
-
Managing Chronic Conditions in People Living with Dementia -- [HTML Version] [PDF Version]
-
Preventing Cognitive Decline and Dementia -- [HTML Version] [PDF Version]
-
Research Summit on Dementia Care -- [HTML Version] [PDF Version]
-
The Many Challenges of Alzheimer's Disease -- [HTML Version] [PDF Version]