
Friday, July 28, 2017
Printer Friendly Version in PDF Format (7 PDF pages)
Increasing Opportunities for Choice and Control for Persons with Dementia
Today's Conversation
- Introduction to Self Direction
- The philosophy and practice of self direction
- Importance of the role of a representative
- Why self-direction is right for some
- Research Findings
- How is Self-Directing faring?
- Basic Assumptions of Self-Direction
- Other Interesting Tid-bits
- Questions
Defining Self Direction
- Person Decides
- What
- When
- Who
- How
- Those who provide supports and services are accountable to the individual and/or representative.
- The freedom for one to plan his/her own life.
- Flexibility based on personal preferences.
Representatives
- May be used if a person is apprehensive about self-directing
- May be used if a person lacks the cognition or ability to make decisions
- Must reflect a strong personal relationship with the person
- Must express knowledge about the persons needs, wishes, and personal goals and make decisions based on those preferences
- Must agree to accept responsibility for self-directing
- Agree to a face-to-face interview routinely
- May not be paid to be a representative
- May not be paid to be a hired worker for the person
- May not have a history of abuse, neglect or exploitation
- Must participate in the person-centered planning process
- About 40% of elderly have designated a representative
Why Self Direction is Right for Many
- Allows greater access to services in rural areas.
- Expands labor force by creating new opportunities for caregiver employment.
- Honors cultural uniqueness of individuals with workers.
- Allows participants to be served by individuals they know and trust. Continuity is critical particularly for those with dementia.
- Preferences may change over time.
- Cost is same or less that traditional personal care services.
- Facilitates easier access to services on nights and weekends.
- Flexible budgets allow for persons to have greater access to community activities.
Research Findings
- Health and welfare
- Display better health outcomes
- Very few incidents of reported abuse, neglect or exploitation
- Service use
- Modest increase in obtaining personal care and equipment
- Individuals more likely to obtain services they need
- When needs are met, use of higher-cost services is reduced
- Caregiver reaction
- More satisfied with care arrangement
- Expressed less emotional strain
- Most felt well-trained to perform duties
- Positive influence on the quality of life
- Increased satisfaction
- Enhanced feeling of safety
- Continuity of care
- Improves access to services
- Participants receive necessary services
- Significantly reduces unmet needs
- Promotes life in the community
- Shown to reduce nursing facility placements even more than traditional services
How is Self-Direction Going?
- How Many People Self-Direct?
- Over one million are self-directing
- Medicaid is the largest funder of services
- Medicaid programs down to 252 due to consolidation
- Serves all ages, across all disability populations
- Other Interesting Facts
- CA and MA have used self-direction since mid-1980s
- Significant take-up with Managed Care Health Plans
- Scotland and England have used self-direction with a focus on individuals with dementia for years
- Australia s implementing a nationwide system using self-direction
- Challenges Reported
- Case management lack of interest in self-direction
- Enrollment labor-intensive
- Some apprehensive to be an employer
- Perception of fraud, abuse and misuse of program funds
- Fair Labor Standards Act compliance
Majority of States have 1000 - 5000 Participants
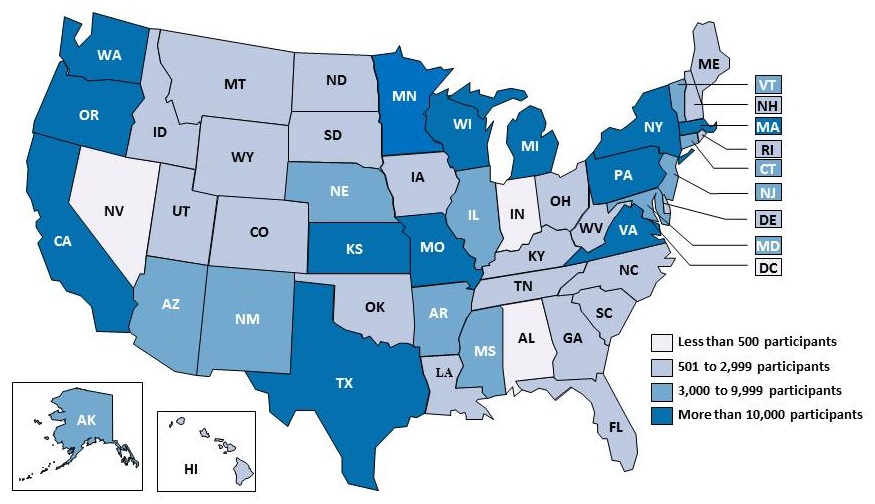 |
ALT TEXT:
|
Assumptions of Self Direction
- Persons with cognitive limitations should have the option to self-direct
- Participants/Representatives are experts when it comes to their own lives
- Participants prefer to make their own decisions related to their needs and preferences
- Some participants will choose to take a more active role in meeting their needs and preferences
- Supports must be available including counseling and assistance with payroll, employer/employee obligations, and managing a budget
- Participants will exercise their choices and spend money wisely
- PD may save money. When people receive the basic services they need, there is less reliance on hospitalizations, ER visits, and admissions to nursing homes.
This May Surprise You
- Twenty four percent of people of all ages who receive Medicaid and Medicare home health have moderate to severe cognitive impairments.*
- Budgets can be used to purchase items designed for safety.
- For example, wondering devices, video monitoring systems, exit sensors, and bed occupancy notifications, reminding devices, medication management systems, GPS locators and tracking devices, and picture phones.
- Many Medicaid Waivers include special services for persons with dementia.
- These include additional training for health care workers, dementia coaching, and crisis intervention.
- Many Medicaid programs permit payment for advanced training for caregivers, in-home and out-of-home respite, payment for conferences and workshops, and unique learning opportunities.
* http://www.KFF.org/Medicaid/issue-brief/medicaids-role-for-people-with-dementia/
Closing Remarks
- Self-directing is growing in the Medicaid and Managed Care markets.
- There is attention to private pay and long-term health insurance companies to adopt self direction.
- The penetration rate for self-directed Medicaid programs remains low in most areas ( between 5 % and 20%).
- Training varies among programs from none to 40 hours of intensive training prior to hire.
- Cost studies have not been definitive.
- Financial Management Services has become more sophisticated ( mobile applications for timesheet submissions, electronic service plans allowing for immediate changes, real-time view of budgets on line, and electronic voice verification systems (a requirement in 2019) to verify worker/participant/location/tasks of service.
What kind of programs do you want available to you?
Questions
PUBLIC CONSULTING GROUP
http://www.publicconsultinggroup.com
July 28, 2017 -- Advisory Council Meeting #25
The meeting was held on Friday, January 26, 2018, in Washington, DC. The Research Subcommittee took charge of this meeting's theme, focusing on the process from targets to treatments. The Council heard speakers on the preclinical pipeline, the clinical trial pipeline, and the industry perspective. The meeting also included discussion of a driver diagram to guide the Council's future work, updates and a report from the October Care Summit, and federal workgroup updates. Material available from this meeting is listed below and is also available at https://aspe.hhs.gov/advisory-council-alzheimers-research-care-and-services-meetings#Jan2018.
Comments and questions, or alerts to broken links, should be sent to napa@hhs.gov.
General Information
-
Agenda -- [HTML Version] [PDF Version]
-
Meeting Announcement -- [HTML Version] [PDF Version]
-
Meeting Summary -- [HTML Version] [PDF Version]
-
Public Comments -- [HTML Version]
Presentation Slides
-
2017 National Plan Update and Non-Federal Recommendations -- [HTML Version] [PDF Version]
-
Clinical Services Subcommittee Federal Update -- [HTML Version] [PDF Version]
-
CommunityRx for Community-Residing People with Dementia and Their Caregivers -- [HTML Version] [PDF Version]
-
Dementia Caregiving in the U.S. -- [HTML Version] [PDF Version]
-
Development of the FY 19 NIH Bypass Budget for Alzheimer's Disease and Related Dementias -- [HTML Version] [PDF Version]
-
Implications of a Biologically Based Definition of Alzheimer's Disease -- [HTML Version] [PDF Version]
-
Increasing Opportunities for Choice and Control for Persons with Dementia -- [HTML Version] [PDF Version]
-
Interventions to Prevent or Slow Cognitive Decline, MCI and Dementia in Individuals without Dementia -- [HTML Version] [PDF Version]
-
Living Alone With Dementia -- [HTML Version] [PDF Version]
-
Long-Term Services and Supports Committee Update -- [HTML Version] [PDF Version]
-
Managing Chronic Conditions in People Living with Dementia -- [HTML Version] [PDF Version]
-
Preventing Cognitive Decline and Dementia -- [HTML Version] [PDF Version]
-
Research Summit on Dementia Care -- [HTML Version] [PDF Version]
-
The Many Challenges of Alzheimer's Disease -- [HTML Version] [PDF Version]
Videos
-
Welcome thru Clinical Care -- [Video]
-
LTSS Research -- [Video]
-
Public Comments thru Federal Workgroup Updates -- [Video]
-
Recommendations thru Adjourn -- [Video]