
Friday, February 3, 2017
Printer Friendly Version in PDF Format (7 PDF pages)
Clinical Services Subcommittee Federal Update
Shari Ling, M.D.
2016 Veterans Health Administration Dementia Steering Committee Recommendations
- U.S. Dept. Veterans Affairs (VA) Veterans Health Administration (VHA) Dementia Steering Committee Recommendations - updated Sept. 2016
- Guidance to improve health/well-being of Veterans - increasing access to best practices in care for Veterans suffering from dementia and their families/carers
- Interdisciplinary, VA-specific, comprehensive
- Combine published evidence with VA experts' experience
- Address dementia recognition, diagnosis, treatment at different stages, care coordination, administrative matters, research, education
- Not VHA policy or mandates
- Now posted on VHA Office of Geriatrics & Extended Care Internet web site: https://www.va.gov/geriatrics/GEC_Data_Reports.asp
2016 VHA Clinician Fact Sheet: Detection of Cognitive Impairment
- U.S. Dept. Veterans Affairs (VA) Veterans Health Administration (VHA) National Center for Health Promotion and Disease Prevention (NCP) Clinician Fact Sheet "Detection of Cognitive Impairment" - updated Dec. 2016
- VHA does not recommend screening for cognitive impairment in asymptomatic older adults (those presenting with no signs or symptoms of cognitive impairment)
- VHA Primary Care clinicians should be alert to early signs or symptoms of cognitive impairment and evaluate as approrpriate
- Fact Sheet includes lists of warning signs that clinicians may notice or that patients and caregivers may report, plus elements of a structured diagnostic evaluation if warning signs are present.
- Now posted on VHA NCP Internet web site: http://www.prevention.va.gov/docs/NCP_CPS_Factsheet_Cognitive_Impairment.pdf
New Medicare-Medicaid Accountable Care Organization Model
- In December CMS announced a new model that builds on the Medicare Shared Savings Program, where Medicare ACOs that hit spending and quality targets are able to share in savings with CMS
- This model will consider Medicaid savings, as the enrollees will be dually eligible for Medicare and Medicaid
- It will potentially include a broad range of long-term care services
- CMS intends to enter agreements with as many as six states
(Strategy 2.E)
Information at: https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2016-Fact-sheets-items/2016-12-15-2.html
Improved Care Planning in the 2017 Physician Fee Schedule is Underway
- Primary Care and Care Coordination: CMS covers enhanced payment for chronic care management, including payment for new codes and for extra care management furnished following the initiating visit for patients with multiple chronic conditions
- Mental and Behavioral Health: CMS pays for specific behavioral health services and other approaches to behavioral health integration including the "Collaborative Care Model," and team care
- Cognitive Impairment Care Assessment and Planning: A new code pays for cognitive and functional assessment and care planning for beneficiaries with cognitive impairment (e.g. Alzheimer's disease)
(Strategy 2.F)
Medicare Payment for Behavioral Health Integration
- The 2017 Physician Fee Schedule includes notable behavioral health enhancements: CMS will pay for specific benehavioral health services and other approaches to behavioral health integration including the "Collaborative Care Model," and team care; a new code describes cognitive and functional assessment and care planning for beneficiaries with cognitive impairment (e.g. Alzheimer's disease)
- In December Patrick Conway, CMS's Acting Administrator, and other CMS staff published an article in the New England Journal of Medicine on this important topic: http://www.nejm.org/doi/full/10.1056/NEJMp1614134?af=R&rss=currentIssue&
(Strategy 2.G)
PACE Innovation Act Request for Information
- In December CMS issued a RFI on a new proposed 5-year PACE model for dually eligible beneficiaries: age 21 and older, with disabilities that impair mobility, who are at nursing home "level of care," and meet other eligibility criteria
- The model is called "Person-Centered Community Care" (P3C)
- CMS is also seeking information from stakeholders on additional populations who could benefit from enrollment in PACE-like models, and information on how PACE can be adapted to better serve the needs of these new groups and the currently eligible PACE group
- The comment period closes February 10
(Strategy 2.G)
Information at: https://www.cms.gov/Medicare-Medicaid-Coordination/Medicare-and-Medicaid-Coordination/Medicare-Medicaid-Coordination-Office/PACEInnovationAct.html
Socioeconomic Status and Fair and Equitable Care
- Consumer-focused care acknowledges the role social risk factors such as income, education, race and ethnicity play in a person's health
- Value-based payment can drive improvements in care and reduce disparities by creating balanced accountability for the care provided to people with social risk factors
- In December the Secretary's office, in association with CMS, issued a report on the effect of socioeconomic status on Medicare quality and resource use measures
(Strategy 3.A)
Information at: https://aspe.hhs.gov/pdf-report/report-congress-social-risk-factors-and-performance-under-medicares-value-based-purchasing-programs
Person and Family Engagement Strategy
- Issued in November, the Strategy seeks to enhance person and family engagement across CMS
- It establishes definitions and consistency for frequently used terms to help people engage more fully in their healthcare
- It serves as a guide to support meaningful, intentional application of person and family engagement principles to all policies and programs addressing health and wellbeing
- The Strategy creates a foundation for expanding awareness and enhance person and family engagement
(Strategy 3.D)
Information at: https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/QualityInitiativesGenInfo/Person-and-Family-Engagement.html
Beneficiary Engagement Models
- Beneficiary engagement broadly refers to the actions and choices of individuals with regard to their health and health care, and these decisions impact cost, quality, and patient/consumer satisfaction and outcomes
- CMS's new Beneficiary Engagement and Incentives (BEI) Models are the Shared Decision Making Model and the Direct Decision Support Model
- The models target "preference-sensitive conditions" for which the clinical evidence does not clearly support one treatment option, and the appropriate course of treatment depends on the values or preferences of the beneficiary regarding the benefits, harms, and scientific evidence for each treatment option
(Strategy 3.D)
Information at: https://innovation.cms.gov/initiatives/Beneficiary-Engagement-DDS/index.html and https://innovation.cms.gov/initiatives/beneficiary-engagement-sdm/
National Partnership to Improve Dementia Care in Nursing Homes
- The December Medicare Learning Network (MLN) Connects® call on the National Partnership to Improve Dementia Care and Quality Assurance and Performance Improvement focused on aspects of the recent Long-Term Care Facility fule that impact behavioral healthcare
- Section 483.40 Behavioral Health Services: Dementia includes a requirement that residents who display or are diagnosed with dementia receive the appropriate treatment to attain or maintain his or her highest practicable physical, mental, and psychosocial well-being
- Rehabilitative Services, Medically-Related Social Services, and pharmacy must also be addressed
- The call also addressed aspects of collaborative care to reduce antipsychotic use
- The audio recording and transcript are at: https://www.cms.gov/Outreach-and-Education/Outreach/NPC/National-Provider-Calls-and-Events.html
(Strategy 3.D)
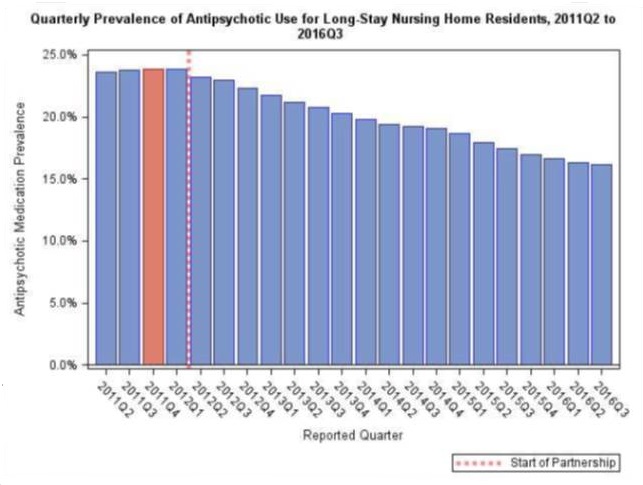
National Partnership to Improve Dementia Care in Nursing Homes Antipsychotic Medication Use Trend Update
- In 2011 Quarter 4, 23.9 percent of long-stay nursing home residents were receiving an antipsychotic medication; since then there has been a decrease of 32.4 percent to a national prevalence of 16.1 percent in 2016 Quarter 3
- Success has varied by state and CMS region, with some states and regions having seen a reduction of greater than 30 percent
 |
Measures Under Consideration List for Pre-Rulemaking
- CMS has been publishing a list of quality and cost measures under consideration for certain Medicare quality and value-based purchasing programs annually, collaborating with the National Quality Forum (NQF) to gain input from stakeholders
- The "MUC" List for 2017 was finalized in November
- It includes MUC 16-317, Safety Concern Screening and Follow-Up for Patients with Dementia: Percentage of patients with dementis or their caregiver(s) for whom there was a documented safety screening * in two domains of risk: dangerousness to self or others and environmental risks; and if screening was positive in the last 12 months, there was documentation of mitigation recommendations, including but not limited to referral to other resources
(Strategy 5.A)
Information at: https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/QualityMeasures/CMS-Measures-Inventory.html
QUESTIONS?
February 3, 2017 -- Advisory Council Meeting #23
The meeting was held on Friday, February 3, 2017, in Washington, DC. The theme of this Advisory Council meeting was clinical trials for Alzheimer's disease and related dementias and recruitment challenges. Additional afternoon presentations included updates on progress towards a Care and Services Summit, federal workgroup updates, and preparation for the Advisory Council's 2017 Recommendations, due in April 2017. Material available from this meeting is listed below and is also available at https://aspe.hhs.gov/advisory-council-alzheimers-research-care-and-services-meetings#Feb2017.
Comments and questions, or alerts to broken links, should be sent to napa@hhs.gov.
General Information
-
Agenda -- [HTML Version] [PDF Version]
-
Meeting Announcement -- [HTML Version] [PDF Version]
-
Meeting Summary -- [HTML Version] [PDF Version]
-
Public Comments -- [HTML Version]
Handouts
-
Panelist Bios -- [HTML Version] [PDF Version]
Presentation Slides
-
2017 Recommendations -- [HTML Version] [PDF Version]
-
Alzheimer's Association TrialMatch -- [HTML Version] [PDF Version]
-
Clinical Services Subcommittee Federal Update -- [HTML Version] [PDF Version]
-
Clinical Studies Recruitment Strategy -- [HTML Version] [PDF Version]
-
Development and Use of Registries to Accelerate Enrollment into Alzhiemer's Trials -- [HTML Version] [PDF Version]
-
Long-Term Services and Supports Committee Update -- [HTML Version] [PDF Version]
-
National Recruitment Strategy -- [HTML Version] [PDF Version]
-
NINDS Update -- [HTML Version] [PDF Version]
-
Randomized Controlled Trials for Alzheimer's Disease -- [HTML Version] [PDF Version]
-
Strategies to Facilitate Recruitment and Screening for Alzheimer's Clinical Trials -- [HTML Version] [PDF Version]
-
Transforming AD Therapy Development -- [HTML Version] [PDF Version]
-
Update National Research Summit on Care, Services and Supports for Persons with Dementia and Their Caregivers -- [HTML Version] [PDF Version]