
SUPPORT AND SERVICES AT HOME (SASH) EVALUATION: SASH EVALUATION FINDINGS, 2010-2016
Amy Kandilov, Vincent Keyes, Noëlle Siegfried, Kevin Smith, Patrick Edwards, Jenna Brophy, Aubrey Collins, and Martijn Van Hasselt
RTI International
Alisha Sanders and Robyn Stone
LeadingAge Center for Applied Research
July 2019
Printer Friendly Version in PDF Format (32 PDF pages)
ABSTRACT
This document provides highlights of the evaluation of the Support and Services at Home (SASH) program for the first years of the program (2010-2016). The SASH program in Vermont is a promising approach to providing support services and care coordination to older adults and individuals with disabilities, using affordable housing properties as a platform for service delivery. Under contract from HHS and HUD, RTI International conducted a mixed-methods evaluation of the SASH program.
This report was prepared under contract #HHSP23337006T between the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Disability, Aging and Long-Term Care Policy and RTI International. For additional information about this subject, visit the DALTCP home page at https://aspe.hhs.gov/office-disability-aging-and-long-term-care-policy-daltcp or contact the Project Officer at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201, Emily.Rosenoff@hhs.gov.
DISCLAIMER: The opinions and views expressed in this report are those of the authors. They do not reflect the views of the Department of Health and Human Services, the contractor or any other funding organization. This report was completed and submitted on October 2018.
TABLE OF CONTENTS
1. OVERVIEW
1.1. Introduction
1.2. Health Needs among Low-Income Households Receiving Housing Assistance
2. SUPPORT AND SERVICES AT HOME PROGRAM
2.1. Design and Development of the SASH Program
2.2. SASH-Housing Sites and SASH Participants: Who Enrolled in the SASH Program?
3. FINDINGS
3.1. Medicare Expenditures
3.2. Medicaid Expenditures
3.3. Managing Multiple Medications
3.4. Perspectives on Property Management at SASH-Housing Sites
4. SUMMARY
4.1. Lessons for Replication
4.2. Conclusions
LIST OF FIGURES
- FIGURE 1: Total SASH Participants and SASH Participants Included in the Quantitative Analysis
- FIGURE 2: Panel Characteristics of Site-Based SASH Participants in the Analysis Sample
- FIGURE 3: Percentage of Respondents Who Had Difficulty Performing Medication-Related Tasks
LIST OF TABLES
- TABLE 1: Characteristics of Housing Properties Hosting the SASH Program
- TABLE 2: Average Baseline Demographic Characteristics and Health Status for Site-based and Community Participants in the SASH Program
- TABLE 3: DID Estimates for 8 Categories of Medicare Expenditures, Comparing SASH Program Participants to Non-SASH Comparison Beneficiaries
- TABLE 4: DID Estimates for 3 Categories of Medicaid Expenditures, Comparing Dually-Eligible SASH Program Participants to Dually-Eligible Non-SASH Comparison Beneficiaries
ACRONYMS
The following acronyms are mentioned in this report.
| BMQ | Brief Medication Questionnaire |
|---|---|
| CHT | Community Health Team |
| CSC | Cathedral Square Corporation |
| DID | Difference-In-Differences |
| DRHO | Designated Regional Housing Organization |
| ER | Emergency Room |
| FFS | Fee-For-Service |
| HCBS | Home and Community-Based Services |
| HCC | Hierarchical Condition Category |
| HHS | U.S. Department of Health and Human Services |
| HUD | U.S. Department of Housing and Urban Development |
| LIHTC | Low Income Housing Tax Credit |
| PBPM | Per-Beneficiary Per-Month |
| PIC | Public and Indian housing information Center |
| RTI | Research Triangle Institute |
| SASH | Support And Services at Home |
| TRACS | Tenant Rental Assistance Certification System |
| VNA | Visiting Nurse Association |
1. OVERVIEW
1.1. Introduction
This report provides highlights of the evaluation of the Support and Services at Home (SASH) program. The SASH program in Vermont is a promising approach to providing support services and care coordination to older adults and individuals with disabilities, using affordable housing properties as a platform for service delivery. Under contract from the U.S. Department of Health and Human Services (HHS) and the Department of Housing and Urban Development (HUD), RTI International and the LeadingAge Center for Applied Research have conducted a mixed-methods evaluation of the SASH program. To better understand the design and implementation of the SASH program, the team collected primary data from in-person and phone interviews with SASH program staff, property managers, and representatives of SASH community partners such as councils on aging, community health teams (CHTs), and visiting nurse associations (VNAs). To determine the impact of the SASH program on participant outcomes, we fielded a mail survey that asked participants and a comparison group about their health status and medication-management. We also analyzed data from Medicare and Medicaid claims to explore the impact of the SASH program on health care costs and utilization. Full SASH evaluation results for years 2011 to 2016 are available from the HHS Office of the Assistant Secretary for Planning and Evaluation.[1]
In the next section, we present the larger policy context of the SASH program by discussing the health needs of low-income households. In Section 2.1, we provide an overview of the design and development of the SASH program; and in Section 2.2, we describe the participants who enrolled in the SASH program and the affordable housing properties involved. In the next four sections, we highlight selected findings from the larger evaluation report--the impacts of the SASH program on Medicare expenditures (Section 3.1), on Medicaid expenditures (Section 3.2), on participants' management of their medications (Section 3.3), and on property management issues (Section 3.4). We summarize some of the challenges for the SASH program that emerged from our evaluation in Section 4.1, where we discuss lessons learned for replication of this housing-with-services model. The final Section 4.2 concludes with a summary and discussion of the findings reported in this report.
1.2. Health Needs among Low-Income Households Receiving Housing Assistance
Older adults prefer to live independently in their own homes and communities as long as possible. Advancing age, however, increases the likelihood of chronic illness, frailty, and disability, and consequently places some older adults in greater need of health and long-term services and supports (AARP, 2009; Redford & Cook, 2001). To continue to live independently, older adults may need access to in-home support services and housing that can be adapted to their growing needs (Lawton, 1976).
Living independently as they age may be particularly difficult for lower-income older adults; they may have fewer resources for support service and greater health care needs. In particular, older adults who qualify for housing assistance may require greater levels of assistance and support. As shown in a recent descriptive analysis comparing HUD-assisted Medicare beneficiaries dually enrolled in Medicaid to similar beneficiaries without HUD assistance, those assisted by HUD programs are more likely to have five or more chronic conditions, use health care such as visits to an emergency room at higher rates, and generate higher Medicare and Medicaid expenditures (Lewin Group, 2014). Even when controlling for geographic region and person-level confounding variables, HUD-assisted Medicare beneficiaries dually enrolled in Medicaid had higher utilization of health care services covered by Medicaid and higher Medicaid expenditures (Lewin Group, 2016). Medicare beneficiaries with HUD-assistance also had higher rates of health care utilization for hospital stays, skilled nursing facility stays, and emergency room visits (Lewin Group, 2016).
One approach to help lower-income older adults address their health and functional challenges involves capitalizing on publicly-assisted, multi-unit rental properties housing low-income seniors. Organizing a system of health care and long-term services and supports around this type of housing has the potential to improve health care outcomes and reduce health care costs. Economies of scale can be achieved in organizing, delivering, and purchasing services. Publicly-assisted service-enriched housing also enables on-site staff to observe and respond to residents' health and supportive services needs as they arise. Previous research shows that older residents living in housing with on-site service coordinators had significantly lower hospitalization rates than residents in housing without service coordinators (Sanders et al., 2014). Models such as the SASH program could provide strategies for helping to meet the health and long-term services and supports needs of lower-income older adults, while improving health care outcomes and reducing health care costs. The goal of our evaluation of the SASH program was to identify the impact of the SASH program on health care costs (Medicare and Medicaid expenditures) and to examine which aspects of the SASH program contributed to any favorable results.
2. SUPPORT AND SERVICES AT HOME PROGRAM
2.1. Design and Development of the SASH Program
The SASH program is designed to promote greater care coordination for a population of older adults and individuals with disabilities who live in affordable housing properties and who have high health care costs. The program's unique contribution is its use of teams embedded in affordable housing properties to connect residents to health services and social supports. The services provided by the SASH program are centered around a panel of participants; each panel has a core staff of a full-time SASH coordinator and a quarter-time SASH wellness nurse who serve approximately 100 participants. The SASH program officially launched in July 2011 and expanded into non-profit affordable housing properties throughout Vermont; as of December 2016, the SASH program had 54 panels with 6,064 participants who had been in the program for at least 3 months.
When a participant first enrolls in a SASH panel, the SASH coordinator completes a comprehensive assessment on health conditions, medications, and support services currently used or needed; this assessment is updated annually and helps the SASH coordinator identify the health and service needs of the individual and target group programming to the needs in the panel. To connect participants to resources in the community, the SASH coordinator and wellness nurse partner with local service provider organizations, such as home health agencies, councils on aging or area agencies on aging, and community mental health organizations, which together create the SASH Team. SASH coordinators and wellness nurses are expected to communicate and meet with participating service providers on the SASH Team regularly (at least once a month) to discuss specific participant cases and group wellness approaches.
When individuals enroll in the SASH program, they consent to the sharing of health care information between the SASH staff, community partners, and health care providers. With this consent, SASH staff work with the participants' health care providers to ensure proper medication usage, successful hospital discharges, and overall coordination and continuity of care. The SASH program provides a continuum of support and services that meets participants' needs, whether they are extremely healthy and looking for minimal supports or are very frail and in need of more robust support from the full SASH Team. Individuals who do not consent to share their health information but live in properties hosting SASH can still receive limited assistance from the SASH coordinator and wellness nurse and participate in SASH programming. However, without consent to share their information, staff cannot serve these individuals as intensively.[2]
The SASH program is a Vermont-wide initiative coordinated at the state, regional, and local levels. The non-profit housing provider Cathedral Square Corporation (CSC), which developed the SASH program, oversees the program at the state level and is responsible for defining and implementing the programmatic elements along with coordinating program expansion and training. At the regional level, six Designated Regional Housing Organizations (DRHOs) are responsible for planning the roll-out of the SASH program across their geographic regions; CSC serves as one of these six DRHOs. The program is delivered at the community level through the SASH panels, which are operated by housing host organizations.
There are more than 20 affordable housing organizations in Vermont that host the SASH program by operating one or more SASH panels in their properties.[3] These hosts are required to be non-profits, and they receive assistance or support from HUD, the Low-Income Housing Tax Credit (LIHTC) program, the U.S. Department of Agriculture Rural Development, and/or the State of Vermont. Housing hosts also include a few mobile home parks. We refer to the properties hosting the SASH panels as SASH sites.
While SASH was originally created to help meet the needs of residents in affordable housing sites (site-based participants), the program is available to any Medicare beneficiary living in surrounding communities (community participants). Most individuals become eligible for Medicare by turning 65 or by having a qualifying disability or health condition. SASH panels that primarily serve residents in affordable housing sites are called site-based panels. As the SASH program expanded statewide, some panels based in affordable housing sites were created to serve a mixture of site-based and community participants (mixed-panels), and a few panels were created solely for community participants (community panels).
2.2. SASH-Housing Sites and SASH Participants: Who Enrolled in the SASH Program?
The housing host sites are essential partners in the implementation of the SASH program. The SASH coordinators and wellness nurses typically operate out of space provided by the housing host. Across the 54 SASH panels, we identified 116 properties that were hosting the SASH program; on average, there are two properties in each SASH panel.[4] In Table 1, we present characteristics for properties that hosted the SASH program, using property data from 2012 through 2016. The housing properties that host the SASH program and that are included in our analysis are federally assisted housing properties, including public housing, privately owned assisted housing, and affordable housing built with LIHTC.
| TABLE 1. Characteristics of Housing Properties Hosting the SASH Program | |
|---|---|
| Property Characteristics | SASH Host Properties |
| Number of properties | 116 |
| Mean number of units per property | 79 |
| Mean occupancy length (years) | 6.8 |
| Mean household size | 1.6 |
| Mean household income of residents | $16,541 |
| Mean tenant rent | $360 |
| Residents aged 65 years and older (%) | 59.7 |
| Metropolitan (%) | 30.4 |
| Micropolitan (%) | 32.9 |
| Rural (%) | 36.6 |
| Median household income (by county) | $51,756 |
| Average annual Medicare expenditures | $7,765 |
| NOTE: Data from 2012-2016 TRACS and PIC data bases and 2012-2015 LIHTC data bases. Occupancy length could not be determined from the LIHTC data base. | |
There were 79 units on average in the properties hosting the SASH program. Residents of these properties had an average occupancy of 6.8 years. The mean household size was 1.6 person, the mean household income was $16,541, and the mean rent was $360. Almost 60% of residents in these properties were aged 65 or older. About one-third of properties were in metropolitan, micropolitan, and rural areas. County median household income ($52,756) and average annual Medicare expenditures ($7,765) is provided for reference.
| Medicare FFS is the traditional Medicare program offered directly through the Federal Government. The other option, Medicare Advantage, consists of private plans that contract with the government to provide Medicare benefits. Medicare FFS covers over 93% of Vermont's Medicare population. |
As of December 2016, there were 54 active SASH panels; and 6,064 individuals had participated in the program for at least 3 months. In Figure 1, we show how many participants are living in HUD-assisted and LIHTC housing versus how many are living in the community, as well as what proportion of SASH participants are Medicare fee-for-service (FFS) beneficiaries. In our examination of the impact of the SASH program on Medicare expenditures, the analysis sample is limited to the 2,973 participants who were Medicare FFS beneficiaries and who were living in HUD-assisted or LIHTC housing properties that hosted the SASH program.
| FIGURE1. Total SASH Participants and SASH Participants Included in the Quantitative Analysis |
|---|
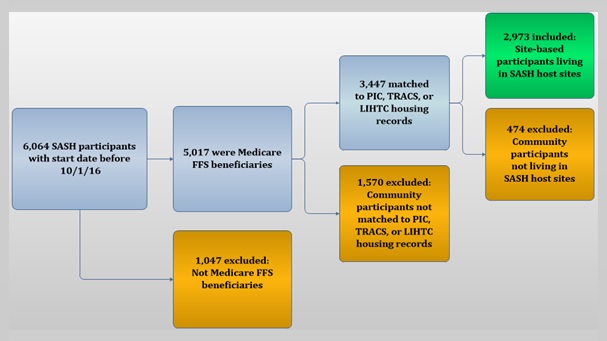 |
Table 2 presents the average demographic and health status characteristics for the SASH participants in the sample and the unweighted averages for the non-SASH comparison group beneficiaries. These characteristics are reported during the baseline year prior to the start of the SASH program (July 2010-June 2011). Statistically significant results in the table are denoted by asterisks (*).
Similar proportions of site-based SASH participants and the comparison group beneficiaries were White and female. Among both SASH participants and the comparison group, about half had Medicaid coverage in addition to Medicare. Mean household income was also similar between the SASH participants and the comparison group. However, there were significant differences between the SASH participants and the comparison group in all the remaining characteristics. SASH program participants were older on average than the comparison group beneficiaries (mean age, 69.2 vs. 65.7), were less likely to have originally qualified for Medicare because of disability, and were residing in smaller households.
We examined two measures of health status among SASH participants, the Hierarchical Condition Category (HCC) risk score and the Charlson comorbidity index (both are created using diagnosis codes on claims in the year before the start of the SASH program). The HCC risk score is interpreted as the predicted health care costs relative to the average Medicare FFS beneficiary. SASH participants have an HCC risk score of 1.06, meaning that their predicted health care costs are 6% more than the average, while the comparison group has an HCC risk score of 0.97, meaning that their predicted health care costs are 3% less than the average. The Charlson comorbidity index is a mortality predictor that sums across a list of 18 chronic conditions, each of which receives a score between one and six, depending on the probability of mortality. SASH participants have a higher average value of the Charlson index score (0.74 vs. 0.61) than the comparison group, meaning that they have more chronic conditions on average.
| TABLE 2. Average Baseline Demographic Characteristics and Health Status for Site-based and Community Participants in the SASH Program | ||
|---|---|---|
| Demographic and Health Status Characteristics | Site-Based Participantsa | Comparison Groupb |
| Total beneficiaries | 2,973 | 2,614 |
| Demographics | ||
| Mean age | 69.2 | 65.7* |
| Age = 64 (%) | 32.9 | 44.1* |
| Age 65-74 (%) | 29.9 | 25.1* |
| Age >=75 (%) | 37.3 | 30.8* |
| White (%) | 97 | 97 |
| Female (%) | 68 | 66 |
| Originally qualified for Medicare because of disability (%) | 42 | 48* |
| 52 | 51 | |
| Health status | ||
| Mean HCC Score | 1.06 | 0.97* |
| Mean Charlson Comorbidity Index | 0.74 | 0.61* |
NOTE: Standardized differences comparing SASH program beneficiaries to non-SASH comparison beneficiaries that are greater than or equal to the absolute value of 0.10 are noted with an "*".
| ||
Because the comparison group differs from the intervention group baseline characteristics which may affect the outcomes of interest, our regression analyses use weights derived from propensity-scores. Propensity-score matching attempts to balance the intervention and comparison groups with respect to baseline characteristics to reduce the potential for bias in the estimate of the intervention effect. After matching, all the statistically significant differences disappeared, indicating that matching was able to sufficiently balance demographic characteristics and health status between the SASH participants and the comparison group.
3. FINDINGS
3.1. Medicare Expenditures
SASH coordinators and wellness nurses emphasize prevention, nutrition, and healthy living in their work with SASH participants. Blood pressure clinics and foot clinics provided by the SASH staff help identify health problems before they lead to costly adverse health events. SASH staff partner with primary care practices and hospitals to promote better care coordination and discharge planning for participants who have been in the hospital. We would expect that these efforts could result in relative reductions in the growth of Medicare expenditures, when SASH participants are compared to a similar group of non-participants who are not receiving SASH services.
| A negative estimate indicates that the average change in Medicare expenditure outcomes among SASH program participants was lower by the reported amount, relative to the comparison group. |
In this section, we estimate the impact of the SASH program on the Medicare expenditures of SASH participants, compared to similar non-participants. In this analysis, we limit the treatment group to SASH participants who are Medicare FFS beneficiaries living in HUD-assisted or LIHTC housing properties that host the SASH program. Participants who are not covered by Medicare FFS and community participants living outside of the properties hosting the SASH program are excluded, leaving a sample of 2,973 site-based participants (see Figure 1). The demographic characteristics of the site-based SASH participants and the comparison group of non-participants were previously described in Table 2. The comparison beneficiaries are weighted so that their demographic characteristics are like those of the site-based SASH participants. We use Medicare claims data from January 2006 through December 2016 to examine the impact of the SASH program on the Medicare expenditures of SASH participants.
The quantitative analysis estimates the impact of the SASH program on expenditure outcomes using regression methods. We use a linear version of the difference-in-differences (DID) model, which allows us to compare the Medicare expenditures before and after the participants enrolled in the SASH program to the Medicare expenditures for comparison group beneficiaries during the same time periods. For each SASH participant, the baseline period spans from January 2006 through the date of SASH enrollment; the intervention period spans from the date of SASH enrollment through December 2016.
In our first report evaluating the SASH program (RTI International, 2014), we discovered that "early" SASH panels, the ones that began operation within the first 9 months of the SASH program, saw significantly slower growth in Medicare expenditures, while the panels that started later were not affected. Our hypothesis was that the intensive panel start-up activities (recruiting, initial participant assessments, etc.) might make it difficult for the SASH program to have a favorable impact on the health care expenditures of participants within a panel's first year. We anticipated that, as time progressed and as the start-up activities were completed, those later panels would also see favorable impacts. However, in subsequent reports (Kandilov et al., 2016) our analysis revealed that the favorable impact for the early panels persisted while the later panels did not see a favorable impact, even after they had been in operation for a few years.
| FIGURE 2. Panel Characteristics of Site-Based SASH Participants in the Analysis Sample |
|---|
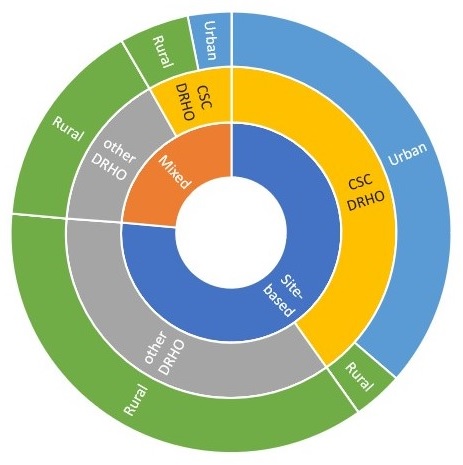 |
In the evaluation of the first 4 years of the SASH program (Kandilov et al., 2017), we identified other characteristics of panels that could contribute to the favorable results for Medicare expenditures, and we explored whether SASH had a different impact on panels with and without those characteristics. Most of the early panels were site-based panels; in site-based panels, more than 50% of participants are living in a HUD-assisted or LIHTC housing property that is hosting the SASH program. Results for the site-based panels are compared to the results for mixed-panels, where more than 50% of participants are living in the community. Participants in site-based panels may experience a more favorable impact from the SASH program, since most of the participants are easily accessible to the SASH staff in the host property. Note, even in the mixed-panels, the SASH participants included in the analysis are the ones living in the HUD-assisted or LIHTC host property, not the community participants. From Figure 2, note that about three-quarters of the analysis sample of site-based participants are in site-based panels. Participants in both site-based and mixed-panels are compared to the entire comparison group, since there is no way to designate the comparison properties as site-based or mixed.
Six different DRHOs are responsible for planning the roll-out of the SASH program across their geographic regions. CSC, the statewide administrator for the SASH program, was one of the six DRHOs; almost half (48%) of the SASH participants in our sample were in panels that were administered by the CSC DRHO. There were some differences between the operations of the CSC DRHO and the other five DRHOs during our analysis period, as well as some differences in participant demographics, so we compare the results for these two types of panels to determine if these differences were associated with favorable impacts of the SASH program. In Figure 2, we graphically represent the overlap between the site-based panels and the CSC DRHO panels. Most of the participants in CSC DRHO panels are also in site-based panels, but a small proportion are in mixed-panels. Participants in both CSC DRHO and other DRHO panels are compared to the entire comparison group.
Most of the early panels were in Chittenden County, which was the one urban county in Vermont. The rural panels are those in all other counties. Urban panels may perform better, since urban areas tend to have more community resources that can be tapped to aid the SASH participants and since the SASH staff do not have to travel long distances in rural areas to reach their participants. As shown in Figure 2, the urban panels are a subset of the CSC DRHO panels, and most of the sample in urban panels are in site-based panels. Participants in urban and rural panels are compared to the entire comparison group.
We used these three panel characteristics to conduct subgroup analyses, to explore which, if any, of these panel characteristics might be contributing to the favorable results found for the early panels. We compared each subgroup of panels to the entire comparison group.
In Table 3 we present the Medicare results for all SASH participants (column 1), for those in site-based panels (column 2) or mixed-panels (column 3), for those in CSC DRHO panels (column 4) or all other DRHO panels (column 5), and for those in urban (Chittenden County) panels (column 6) or rural panels (column 7). Positive coefficients in the table indicate that the growth in expenditures was faster among the SASH participants relative to the comparison group. Negative coefficients indicate that the growth in expenditures was slower among SASH participants and signal that the SASH program was successful in reducing the growth of these expenditures. Statistically significant results in the table are denoted by asterisks (*). The estimates in this table are the DID estimates for the per-beneficiary per-month (PBPM) change in Medicare expenditures. We calculate PBPM amounts by summing Medicare expenditures within each calendar quarter (i.e., January 1, 2012-March 31, 2012) and dividing by 3. Multiplying the PBPM estimates by 12 will produce the annual impact of the SASH program on the change in Medicare expenditures.
| TABLE 3. DID Estimates for 8 Categories of Medicare Expenditures, Comparing SASH Program Participants to Non-SASH Comparison Beneficiaries | |||||||
|---|---|---|---|---|---|---|---|
| Expenditure Type | (1) All SASH Participants (n=2,973) | (2) Site-Based Panels (n=2,271) | (3) Mixed Panels (n=702) | (4) CSC DRHO Panels (n=1,440) | (5) Other DRHO Panels (n=1,533) | (6) Urban Panels (n=1,179) | (7) Rural Panels (n=1,794) |
| Total Medicare | 12.72 (42.56) | -17.32 (46.61) | 22.31 (75.16) | -91.59** (46.37) | 59.95 (50.49) | -122.24** (48.74) | 63.35 (47.51) |
| Acute hospital care | -2.82 (22.06) | -23.01 (23.56) | 15.08 (47.89) | -56.63** (23.60) | 21.82 (28.20) | -70.64*** (24.91) | 21.40 (26.27) |
| Post-acute care | 16.79 (12.34) | 12.07 (13.78) | 17.43 (20.54) | -8.78 (13.29) | 31.71** (14.88) | -16.81 (13.81) | 32.10** (13.92) |
| ER | -3.67 (3.70) | -5.04 (4.04) | -3.93 (5.14) | -9.84** (4.32) | -0.87 (4.39) | -12.48*** (4.37) | 0.03 (4.22) |
| Outpatient department | -8.68 (7.85) | -5.77 (8.45) | -20.90 (13.30) | -8.51 (10.09) | -9.97 (9.71) | -7.71 (11.43) | -9.96 (8.94) |
| Primary care physician | 2.29 (1.48) | 2.10 (1.73) | 1.75 (2.38) | 1.65 (1.36) | 2.14 (2.41) | 1.54 (1.51) | 2.27 (2.14) |
| Specialist physician | -3.34 (2.24) | -4.48 (2.48) | -3.66 (3.69) | -6.83** (2.79) | -1.92 (2.67) | -6.70** (2.99) | -2.55 (2.60) |
| Hospice care | -0.25 (3.61) | -0.90 (3.75) | -2.24 (6.21) | 4.19 (4.56) | -6.50 (4.37) | 4.29 (4.64) | -4.84 (4.23) |
| * p 0.10; ** p 0.05; *** p 0.01; standard errors are in parentheses. NOTES: Medicare Part A and Part B claims data from January 2006 through December 2016. The SASH program began in July 2011. Baseline data for each beneficiary looks back to January 2006, if available. Site-based panels have greater than 50% of participants living in HUD-assisted or LIHTC housing. Mixed-panels have greater than 50% of participants living in the community. Urban panels are those located in Chittenden County; rural panels are those located in all other Vermont counties. | |||||||
Total Medicare expenditures: For the CSC DRHO panels, the SASH program reduced the growth in total Medicare expenditures by $91.59 PBPM, or approximately $1,100 per beneficiary per year. For the participants in the urban panels (a subset of the CSC DRHO panels), Medicare growth is slower by $122.24 PBPM, or more than $1,400 per beneficiary per year. Neither rural DRHO panels nor all other DRHO panels exhibit significant reductions in total Medicare expenditure growth. Among all SASH participants, there is no significant reduction in the growth of total Medicare expenditures, relative to the comparison group; similarly, when we separate the site-based panels from the mixed-panels, there is no significant reduction in the growth of total Medicare expenditures.
Acute hospital care expenditures: Medicare costs for stays in acute care hospitals are measured in the category of acute hospital care expenditures; this is the largest health care expense category for this population. SASH participants in the CSC DRHO panels have significantly slower growth in acute hospital care expenditures; Medicare expenditure growth in this category is $56.63 PBPM lower among SASH participants. This amount accounts for more than half of the slower total Medicare expenditure growth. Additionally, the subset of panels in urban areas have slower growth in expenditures for acute hospital care of $70.64 PBPM, which is the largest contributor to the slower total Medicare growth for participants in these panels. We find no impact of the SASH program on acute hospital care expenditures in the first 5.5 years of the program, for all SASH participants relative to the comparison group, or for participants in any of the other subsets of SASH panels.
Post-acute care expenditures: Post-acute care expenditures include stays in a skilled nursing facility or an inpatient rehabilitation facility which occur after a hospital stay. In our analysis, we find that participants in non-CSC DRHO panels and rural panels have significantly faster growth in post-acute care expenditures.
Emergency room expenditures: The growth rate in emergency room expenditures is $9.84 PBPM lower for the SASH participants in the CSC DRHO panels than for the comparison group and $12.48 PBPM lower for the SASH participants in the urban panels, but all other subsets of SASH participants do not have a significant difference in emergency room expenditure growth, nor does the entire sample of SASH participants.
Hospital outpatient expenditures: When we examine hospital outpatient expenditures, we do not find any significant differences between all SASH participants and the comparison group, or between any of the subsets of SASH participants and the comparison group.
Primary care physician expenditures: Among all SASH participants, there is no significant impact of the SASH program on the growth of primary care physician expenditures, relative to the comparison group. Also, no subset of SASH panels exhibits significantly higher or lower expenditure growth for primary care physicians.
Specialist physician expenditures: For the panels in the CSC DRHO, the SASH program reduced the growth in specialist physician expenditures by $6.83 PBPM; and for panels in the urban areas, the SASH program reduces the expenditure growth by $6.70 PBPM. No other subset of SASH panels exhibits significant reductions in specialist physician expenditure growth.
Hospice care expenditures: Hospice care is palliative care provided to end-of-life patients. When we compare all SASH participants to the comparison group, we find no impact of the SASH program on expenditures for hospice care. There is no impact when comparing any of the subsets of SASH participants to the comparison group.
Based on the results in Table 3, we find that the SASH program had no statistically significant impact on the growth of any of the examined Medicare expenditure measures for the entire population of SASH participants in the sample, across the first 5.5 years of the SASH program. When we report the results for the CSC DRHO panels and for the urban panels (subset of the CSC DRHO panels), we do find significantly slower PBPM growth in total Medicare expenditures, acute hospital care expenditures, emergency room expenditures, and specialist physician expenditures.
There are a few important limitations to the analysis of Medicare expenditures. One-third of SASH participants were living in the community and so were not included in the analysis due to the challenge of finding a suitable comparison group. Another 17% of participants were excluded because they were not Medicare FFS beneficiaries and thus had no claims data. The impacts of the SASH program on these participants may be different from the impacts observed for Medicare FFS beneficiaries living in HUD-assisted or LIHTC housing. Also, there could be positive spillover effects of the SASH program onto residents of the SASH properties who had not consented to share their health care information with the SASH Team, but we were unable to include these effects in our analysis.
3.2. Medicaid Expenditures
One goal of the SASH program is to help older adults age in place--live safely in their homes as they age and delay or prevent the need for long-term institutional care. Long-term institutional care can be expensive for state Medicaid programs, and it is not covered by Medicare. As presented in Table 2, approximately one half of the site-based SASH participants were dually-eligible for Medicare and Medicaid. For these participants, we can examine the impact of the SASH program on Medicaid expenditures and particularly on expenditures for home and community-based services (HCBS) and for long-term institutional care.
| Dually-eligible = individual who is enrolled in both Medicare and Medicaid. For these individuals, Medicare is the primary payer for health care services, while Medicaid pays for services not covered by Medicare (such as long-term institutional care). |
In this analysis, both SASH participants and individuals in the comparison group are dually-eligible Medicare FFS beneficiaries living in HUD-assisted or LIHTC housing who were at least 65 years old when the SASH program began; we limit the sample to older adults since the use of long-term care services is very low among the younger SASH participants. We answer the research question using Medicaid claims data from 2007 through 2016.
The quantitative analysis is like the approach described in the previous section; we use a linear version of the DID model to compare the Medicaid expenditures before and after the participants enrolled in the SASH program to the Medicaid expenditures for comparison group beneficiaries during the same time periods. For each SASH participant, the baseline period spans from January 2007 through the date of SASH enrollment; the intervention period spans from the date of SASH enrollment through December 2016.
In Table 4 we present the Medicaid results for all dually-eligible SASH participants (column 1), for those in site-based panels (column 2) or mixed-panels (column 3), for those in CSC DRHO panels (column 4) or non-CSC DRHO panels (column 5), and for those in urban (Chittenden County) panels (column 6) or rural panels (column 7). Positive coefficients in the table indicate that the growth in expenditures was faster among the dually-eligible SASH participants relative to the comparison group. Negative coefficients indicate that the growth in expenditures was slower among dually-eligible SASH participants and signal that the SASH program was successful in reducing the growth of these expenditures. Statistically significant results in the table are denoted by asterisks (*). The estimates in this table are the DID estimates for the PBPM change in Medicaid expenditures.
| TABLE 4. DID Estimates for 3 Categories of Medicaid Expenditures, Comparing Dually-Eligible SASH Program Participants to Dually-Eligible Non-SASH Comparison Beneficiaries | |||||||
|---|---|---|---|---|---|---|---|
| Expenditure Type | (1) All Dually-Eligible SASH Participants (n=1,052) | (2) Site-Based Panels (n=737) | (3) Mixed Panels (n=315) | (4) CSC DRHO Panels (n=482) | (5) CSC DRHO Panels (n=507) | (6) Urban Panels (n=381) | (7) Rural Panels (n=671) |
| Total Medicaid | -9.14 (25.90) | -20.76 (26.75) | 13.24 (37.77) | -7.31 (29.99) | -13.67 (29.02) | -14.35 (30.54) | -8.10 (28.55) |
| HCBS | 20.42 (15.78) | 17.78 (16.44) | 25.66 (18.40) | 17.12 (17.61) | 22.17 (17.60) | 5.38 (16.65) | 28.86 (17.65) |
| Long-term institutional care | -25.76 (19.72) | -33.40* (19.76) | -12.25 (28.59) | -20.57 (22.98) | -31.55 (21.04) | -13.88 (24.25) | -34.07* (20.61) |
| * p 0.10; ** p 0.05; *** p 0.01; standard errors are in parentheses. NOTES: Vermont Medicaid claims data from January 2007 through December 2016. The SASH program began in July 2011. Baseline data for each beneficiary looks back to January 2007, if available. Site-based panels have greater than 50% of participants living in HUD-assisted or LIHTC housing. Mixed-panels have greater than 50% of participants living in the community. Urban panels are those located in Chittenden County; rural panels are those located in all other Vermont counties. | |||||||
Total Medicaid expenditures: Among all dually-eligible SASH participants, there was no statistically significant difference in the growth of total Medicaid expenditures, relative to the comparison group. Also, there was difference in the growth of total Medicaid expenditures for any subset of SASH panels.
Expenditures for HCBS: There was no difference in HBCS expenditures in the first 5.5 years of the program, for all dually-eligible SASH participants relative to the comparison group, or for any subset of SASH panels. While the positive trends reported for all types of panels would be consistent with the idea that SASH staff are helping to connect participants to needed services, none of these trends are statistically significant.
Expenditures for long-term institutional care: Across all SASH participants, there was no statistically significant impact on expenditures for long-term institutional care. For participants in the site-based panels, the growth in expenditures for long-term institutional care was slower by $33.40 PBPM; and for participants in rural panels, the growth in these Medicaid expenditures was slower by $34.07 PBPM. To get an annual estimate, we multiplied the PBPM estimate by 12. This gives us an annual impact of about $400 per dually-eligible SASH participant over the age of 65.
| The growth in Medicaid expenditures for institutional long-term care was about $400 slower per year among SASH participants in both site-based panels and rural panels. |
In summary, across our entire sample of dually-eligible SASH participants over the age of 65, there was no statistically significant impact of the SASH program on any of the examined Medicaid expenditure outcomes. However, we did see favorable impacts of the SASH program on the institutional long-term care expenditures of participants in the site-based panels (70% of sample) and on participants in the rural panels (64% of sample).
3.3. Managing Multiple Medications
Many SASH participants are managing one or more chronic illness, as well as the multiple medications that accompany chronic illness. Therefore, medication self-management is an important component of the SASH program. Through site visit interviews, our evaluation team explored how the SASH coordinators and wellness nurses address medication-management issues with participants. The interviews with SASH staff highlighted ways that the SASH Team collaborates with participants' health care providers to ensure proper medication usage and teaches participants to properly manage their medications on their own.
When a participant first enrolls in a SASH panel, the SASH coordinator completes a comprehensive assessment to gather information on health conditions, medications, and support services currently used or needed; this assessment is updated annually and helps to identify participants who may have problems with their medications or need assistance with managing them.
| SASH participants reported less difficulty with common medication-management tasks, such as remembering to take all pills and getting refills on time. |
SASH staff provide a helpful front-line for identifying medication problems early and preventing issues caused by medication mismanagement, according to site visit interviewees. Wellness nurses are the key resource in this area because of their medical backgrounds, reminding participants to take all medications, training participants in how to fill their weekly pill boxes, or reaching out to participants' providers on medication usage. The emphasis in any medication-related support is on teaching SASH participants better self-management of their prescription drugs. However, wellness nurses' ability to provide support and training around medication-management is limited by the 10 hours per week they are available for each panel.
To further evaluate the impact of the SASH program on participants' medication-management, we conducted a mail survey of Medicare FFS beneficiaries who were living in HUD-assisted or LIHTC housing, surveying random samples of SASH participants and non-participants. In the survey, respondents were asked about the difficulties they had with common medication-management tasks, using items from the Brief Medication Questionnaire (BMQ) (Svarstad et al., 1999). The BMQ asked respondents about how difficult it was to open or close the medication bottle, read the print on the bottle, remember to take all the pills, get refills in time, and take many pills at the same time. As shown in Figure 3, SASH respondents indicated less difficulty with each of the five medication tasks relative to the comparison group of Medicare FFS beneficiaries in HUD-assisted or LIHTC housing where SASH was not available. Most notably, SASH participants had much less difficulty getting their refills in time and taking multiple pills at the same time.
| FIGURE 3. Percentage of Respondents Who Had Difficulty Performing Medication-Related Tasks |
|---|
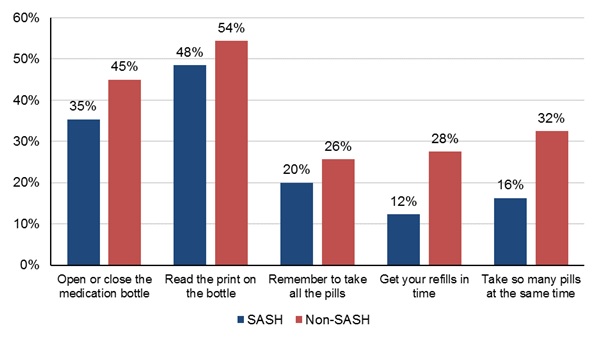 |
| NOTE: Unweighted responses from 2015 SASH beneficiary survey. |
Answers from the BMQ survey questions were combined into a single outcome measure. Our regression analysis of this medication measure, using propensity-score weights to balance the health and demographic characteristics of the SASH participants and the comparison group beneficiaries, revealed that SASH participants had fewer problems with medication-related tasks relative to comparison group members; the magnitude of this effect was moderate and statistically significant. Although the survey results are limited by the fact that we do not have baseline information on medication-management for the SASH participants and the comparison group to know how their scores compared prior to the start of the SASH program, the results are consistent with the efforts that SASH staff are taking to help participants better manage their medications. Thus, there is evidence from our analysis of the mail survey responses that SASH participants experienced fewer problems with medication-related tasks relative to a comparison group of Medicare beneficiaries living in HUD-assisted or LIHTC housing where the SASH program was not available.
3.4. Perspectives on Property Management at SASH-Housing Sites
The SASH program was initially designed to serve the needs of older adults and individuals with disabilities living in affordable housing properties and to help these residents age in place. Although the program expanded to include Medicare beneficiaries who were living in the community, about two-thirds of SASH participants were residents of HUD-assisted or LIHTC housing properties that hosted the SASH program.
The SASH program has the potential to have a positive impact on the participating properties and property management. Our evaluation examined the effect of the SASH program on the host properties by conducting in-person interviews with three property managers, eight SASH coordinators, and seven wellness nurses during the site visit in 2015; these site visit interviews were supplemented by one-on-one telephone interviews with property managers from four additional housing organizations hosting the SASH program.
| Property managers reported that the SASH program helped provide residents with services and resources to remain safely in their homes and to avoid eviction. |
During our interviews, property managers discussed the impacts the SASH program had on operations, property administration, and their own workload. Property managers who had not formerly had support services in place before the SASH program felt that they were better able to perform their primary function because the SASH coordinator and wellness nurse could address the health and wellness issues of participants. One property manager expressed concern that aging residents with unmet needs presented financial risk to their portfolios, such as physical property damages and property legal liabilities. For this reason, they felt the SASH program could reduce costs for the housing properties. Furthermore, SASH staff and property managers felt that SASH activities help create a better community within the properties. In addition to providing opportunities for social engagement, the program helps address tenant conflicts and complaints, such as conflicts surrounding lifestyle differences between long-term older residents and younger residents with disabilities, which can be disruptive to the community.
Property managers spoke of working with the SASH staff to identify resources and supports to address issues that arose. Almost all the property managers interviewed have regular engagement with the SASH staff, most often with the SASH coordinator. They mentioned meeting as needed, sometimes as frequently as weekly, or daily communication via phone and e-mail. At these meetings, property managers and SASH coordinators discuss many issues, including delinquent tenants who are not paying rent or not obeying property policies (e.g., smoking areas, hoarding, or other unsanitary conditions), mobility challenges that make it difficult for residents to get around and to keep their apartments safe and well maintained, and other medical-related needs of residents. Property managers and SASH staff also conduct joint welfare checks on residents.
Mental health issues can be a challenge among this population. The SASH program provides training to help the SASH coordinator and wellness nurse recognize and respond to mental health issues, and the SASH sites are required to partner with the local mental health agencies. This enhanced mental health capacity is an asset to property managers as well as residents. As one property manager noted, mental health issues can create challenges, and property managers are not trained to handle these issues. This manager had seen had several residents with mental illness at a previous property she operated, many of whom ended up being evicted; however, properties she now manages with the SASH program have had no evictions due to mental health issues, because SASH connects these residents with the needed resources and services.
Several SASH staff and property managers believe that a notable success has been the program's ability to help participants remain in their homes, both in terms of aging in place as their health and functional needs increase and in terms of helping participants avoid eviction. SASH staff help ensure that participants have the services and resources needed to be safe in their apartments and uphold their tenancy obligations.
4. SUMMARY
4.1. Lessons for Replication
Through the evaluation's interviews with SASH program staff, property managers, and representatives of SASH community partners such as councils on aging, CHTs, and VNAs, we were able to identify successes and challenges to consider when implementing similar housing-with-services programs.
Availability of staff time and other resources can be a significant help or hindrance to housing-with-services programs. Across all the SASH panels, site visit interviewees emphasized the limited number of wellness nurse hours as one of the primary challenges in the SASH program. The greater travel time in rural areas and in panels with a large proportion of community participants reduced the amount of time that wellness nurses could spend with SASH participants. Increasing the wellness nurse hours could result in a larger impact on participants.
The availability of additional resources may have contributed to the favorable impacts on Medicare expenditures in the CSC DRHO panels and the urban panels. The CSC DRHO panels benefited from having an additional level of support and management, called SASH Team Leaders. While this Team Leader role has now been implemented throughout the SASH program, during much of the analysis period only the CSC DRHO panels benefited from this additional support and management role. Our interviews also revealed that the urban panels (in Chittenden County) had access to more health care and social support services than those in rural areas. This could also contribute to the favorable impact of SASH among urban panels.
Population differences may affect the impact of housing-with-services programs. The SASH staff interviewed in the non-CSC DRHO panels indicated that their participant populations had a higher proportion of younger participants with disabilities, often with mental illness or substance use disorders. Additional quantitative analyses confirmed that the CSC DRHO panels had a larger proportion of older participants and fewer who originally qualified for Medicare due to disability. The SASH program may have more favorable impacts on health care costs among panels with a larger proportion of older adults.
Another population difference that became more important as the SASH program expanded throughout the State of Vermont was the difference between the site-based participants and the community participants. The expansion of the SASH program beyond the housing sites and into the community presented many challenges. SASH staff noted that participants living in the community had greater health and support needs and fewer resources to obtain the supports they required. Our claims data analysis confirmed that SASH participants in the community are older and in poorer health relative to the site-based participants. Future housing-with-services programs seeking to serve a widely dispersed population in the community should be aware that the needs of the community participants could require additional resources.
Education and communication are key to successful implementation of housing-with-services programs. The implementation of the comprehensive SASH training program was identified as an operational success by many interviewees. A training program for new staff, as well as ongoing training for existing SASH staff, ensures that staff maintain the necessary knowledge and skills to best serve SASH participants.
A focus of the SASH program is building relationships and fostering greater collaboration across community organizations, which in turn can help connect SASH participants to a variety of needed services and resources. While some partner agencies perceived that SASH activities are a duplication of services already being provided, others felt that the relationship with the core SASH staff was collaborative and that the SASH program complemented their own services. Other entities seeking to implement SASH-like programs should plan to spend time educating partner agencies and clearly delineating roles and responsibilities across organizations and programs, to avoid any real or perceived duplication of services and to foster good relationships.
4.2. Conclusions
In this report, we summarized notable successes observed during the first 5.5 years of the SASH program. We also outlined important lessons learned for future housing-with-services programs. For further details on the SASH program implementation, complete methodology of the evaluation, and additional findings from the interviews, beneficiary survey, and Medicare and Medicaid claims data analysis, we refer the reader to the previous SASH evaluation reports.[5]
The SASH program had a favorable impact on the Medicare expenditures for site-based participants in the CSC DRHO panels and in the urban (Chittenden County) panels. The impact of the SASH program on the growth of Medicare expenditures varied across different types of panels. Site-based participants in the CSC DRHO panels--representing 48% of the sample of site-based SASH participants who were Medicare FFS beneficiaries--experienced significantly slower growth in Medicare expenditures relative to a comparison group of similar Medicare beneficiaries; for these participants, growth in annual Medicare expenditures was lower by an estimated $1,100 per beneficiary per year. Also, the participants in urban panels experienced growth in Medicare expenditures that were slower by $1,400 per beneficiary per year; these panels were a subset of the CSC DRHO panels. These impacts on total Medicare expenditures were driven by statistically significant slower growth in Medicare expenditures for hospital stays, emergency room visits, and specialist physicians, which is consistent with the SASH program goal of preventing unnecessary high-cost care. The early adoption of the Team Leader role in the CSC DRHO panels and the greater availability of resources in Chittenden County may help to explain why there is a significant impact of the SASH program among these panels but not across all panels.
Growth in average annual Medicaid expenditures for long-term institutional care was $400 slower for dually-eligible SASH participants in site-based panels and in rural panels. One goal of the SASH program is to prevent or delay the need for long-term institutional care among older adults by providing the supports they need to live and age safely in their homes. Our analysis of Medicaid claims data indicates that the SASH program had a favorable impact on Medicaid expenditures for long-term institutional care for dually-eligible SASH participants over the age of 65. Dually-eligible participants in site-based panels and in rural panels experienced statistically significant slower growth in these Medicaid expenditures that averaged about $400 per beneficiary per year. Particularly for the participants in rural panels, SASH may be filling a gap in geographic areas where there are fewer community resources to support residents in their homes. Positive trends in Medicaid expenditures for HBCS, though not significant, are consistent with the SASH program goal of connecting participants to the health care and services they need.
SASH participants reported less difficulty with common medication-management tasks. Based on our analysis of responses from a mail survey, we find that SASH participants reported significantly less difficulty with tasks such as remembering to take all pills and getting refills on time, relative to a comparison group of Medicare beneficiaries who were not participating in SASH. Medication-management support is provided by the SASH staff, who focus on identifying medication-related issues and teaching participants to better manage their multiple medications on their own.
Property managers reported that the SASH program helps provide residents with the support they need to remain in their homes and to avoid eviction. Through both in-person and telephone discussion, property managers in SASH sites indicated that the SASH staff were valued assets in their properties. These property managers appreciated how the SASH coordinators and wellness nurses aided residents with physical and mental health concerns and provided connections with health care and support services.
The lessons for a replication of SASH-like models in other areas include ensuring adequacy of wellness nursing hours and understanding the additional challenges of serving participants in rural areas. Clear communication and delineation of roles among partner organizations could help prevent duplication or perceptions of duplication in services.
The SASH program is designed to promote greater care coordination for a high-cost population of older adults and individuals with disabilities living in affordable housing properties. The program's unique contribution is its use of teams embedded in affordable housing properties to connect residents to health services and social supports. Our highlighted findings suggest that the SASH program has the potential to reduce the growth of Medicare and Medicaid expenditures for some participants, improve self-management of multiple medications, and enable a population of older adults and disabled residents living in affordable congregate housing to remain safely in their homes as they age.
REFERENCES
AARP. (2009). Beyond 50.09 chronic care: A call to action for health care reform. Washington, DC: AARP Public Policy Institute.
Kandilov, A., Keyes, V., Siegfried, N., Edwards, P., Larsen, A., Smith, K., Eicheldinger, C., McCall, N., Van Hasselt, M., Raedar, D., Sanders, A., & Stone, R. (2016). Support and Services at Home (SASH) evaluation: Second annual report. Washington, DC: Office of the Assistant Secretary for Planning and Evaluation. https://aspe.hhs.gov/pdf-report/support-and-services-home-sash-evaluation-second-annual-report.
Kandilov, A., Keyes, V., Siegfried, N., Smith, K., Edwards, P., Brophy, J., Larsen, A., Van Hasselt, M., Sanders, A., & Stone, R. (2017). Evaluation of the first four years of the Support and Services at Home (SASH) program. Washington, DC: Assistant Secretary for Planning and Evaluation. https://aspe.hhs.gov/basic-report/support-and-services-home-sash-evaluation-highlights-first-four-years-research-summary.
Lawton, M.P. (1976). The relative impact of congregate and traditional housing on elderly tenants. Gerontologist, 16, 237-242.
Lewin Group. (2014). Picture of housing and health: Medicare and Medicaid use among older adults in HUD-assisted Housing. Washington, DC: Office of the Assistant Secretary for Planning and Evaluation. https://aspe.hhs.gov/basic-report/picture-housing-and-health-medicare-and-medicaid-use-among-older-adults-hud-assisted-housing.
Lewin Group. (2016). Picture of housing and health part 2: Medicare and Medicaid use among older adults in HUD-assisted housing, controlling for confounding factors. Washington, DC: Office of the Assistant Secretary for Planning and Evaluation. https://aspe.hhs.gov/pdf-report/picture-housing-and-health-part-2-medicare-and-medicaid-use-among-older-adults-hud-assisted-housing-controlling-confounding-factors.
Redford, L., & Cook, D. (2001). Rural health care in transition: The role of technology.Public Policy and Aging Report, National Academy on an Aging Society, Gerontological Society of America, 12(1).
RTI International & LeadingAge. (2014). Support and Services at Home (SASH) evaluation: First annual report. Washington, DC: Office of the Assistant Secretary for Planning and Evaluation. https://aspe.hhs.gov/report/support-and-services-home-sash-evaluation-first-annual-report.
Sanders, A. Smathers, K., Patterson, T., Stone, R., Kahn, J., Marshall, J., & Alecxih, L. (2014). Affordable senior housing plus services: What's the value? Washington, DC: LeadingAge Center for Housing Plus Services.
Svarstad, B.L., Chewning, B.A., Sleath, B.L., & Claesson, C. (1999). The Brief Medication Questionnaire: A tool for screening patient adherence and barriers to adherence. Patient Education and Counseling, 37(2), 113-124. dx.doi.org/10.1016/S0738-3991(98)00107-4.
NOTES
-
Full reports available at https://aspe.hhs.gov/.
-
Full example, if a SASH participant is admitted to the hospital, that participant's physicians have permission to involve the SASH coordinator and wellness nurse in discharge planning for the participant. For an individual who does not consent, his or her physicians would not be able to involve the SASH Team in discharge planning, or even alert them to the hospitalization.
-
A complete list of housing organizations participating in SASH is available at http://sashvt.org/admin/.
-
Note that 2.5 of the SASH panels were community panels, and therefore had no housing host and operated out of a centralized location in the community, such as a senior center.
-
Full reports available at https://aspe.hhs.gov/.
Support And Services at Home (SASH) Evaluation
This Research Summary describes the primary features of the SASH program, and summarizes the main findings of the evaluation to date. Authors include: Amy Kandilov, Vincent Keyes, Noëlle Siegfried, Kevin Smith, Patrick Edwards, Jenna Brophy, Aubrey Collins, Ann Larsen, and Martijn Van Hasselt from RTI International; and Alisha Sanders and Robyn Stone from LeadingAge Center for Applied Research.
This paper was prepared under contract #HHSP23337006T between the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Disability, Aging and Long-Term Care Policy and RTI International. For additional information about this subject, visit the DALTCP home page at https://aspe.hhs.gov/office-disability-aging-and-long-term-care-policy-daltcp or contact the Project Officer at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201, Emily.Rosenoff@hhs.gov.
Reports Available
Support And Services at Home (SASH) Evaluation: First Annual Report
- HTML https://aspe.hhs.gov/report/support-and-services-home-sash-evaluation-first-annual-report
- PDF https://aspe.hhs.gov/pdf-report/support-and-services-home-sash-evaluation-first-annual-report
Support And Services at Home (SASH) Evaluation: Second Annual Report
- HTML https://aspe.hhs.gov/basic-report/support-and-services-home-sash-evaluation-second-annual-report
- PDF https://aspe.hhs.gov/pdf-report/support-and-services-home-sash-evaluation-second-annual-report
Support And Services at Home (SASH) Evaluation: Highlights from the First Four Years
- HTML https://aspe.hhs.gov/basic-report/support-and-services-home-sash-evaluation-highlights-first-four-years-research-summary
- PDF https://aspe.hhs.gov/pdf-report/support-and-services-home-sash-evaluation-highlights-first-four-years-research-summary
Support And Services at Home (SASH) Evaluation: Evaluation of the First Four Years
- HTML https://aspe.hhs.gov/basic-report/support-and-services-home-sash-evaluation-evaluation-first-four-years
- PDF https://aspe.hhs.gov/pdf-report/support-and-services-home-sash-evaluation-evaluation-first-four-years
Support And Services at Home (SASH) Evaluation: Highlights from the Evaluation of Program Outcomes from 2010 to 2016
- HTML https://aspe.hhs.gov/basic-report/support-and-services-home-sash-evaluation-highlights-evaluation-program-outcomes-2010-2016
- PDF https://aspe.hhs.gov/pdf-report/support-and-services-home-sash-evaluation-highlights-evaluation-program-outcomes-2010-2016
Support And Services at Home (SASH) Evaluation: SASH Evaluation Findings, 2010-2016