
SUPPORT AND SERVICES AT HOME (SASH) EVALUATION:
HIGHLIGHTS FROM THE EVALUATION OF PROGRAM OUTCOMES FROM 2010 TO 2016
Amy Kandilov, Vincent Keyes, Noëlle Siegfried, Kevin Smith, Patrick Edwards, Jenna Brophy, Aubrey Collins, Ann Larsen, and Martijn Van Hasselt
RTI International
Alisha Sanders and Robyn Stone
LeadingAge Center for Applied Research
July 2019
Printer Friendly Version in PDF Format (6 PDF pages)
ABSTRACT
This paper describes the primary features of the SASH program and summarizes the main findings of the evaluation to date.
This paper was prepared under contract #HHSP23337006T between the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Disability, Aging and Long-Term Care Policy and RTI International. For additional information about this subject, visit the DALTCP home page at https://aspe.hhs.gov/office-disability-aging-and-long-term-care-policy-daltcp or contact the Project Officer at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201, Emily.Rosenoff@hhs.gov.
DISCLAIMER: The opinions and views expressed in this report are those of the authors. They do not reflect the views of the Department of Health and Human Services, the contractor or any other funding organization. This report was completed and submitted on August 2018.
The Support and Services at Home (SASH) program in Vermont was developed by the Cathedral Square Corporation (CSC) to connect older adults and individuals with disabilities, living in affordable housing properties or the surrounding communities, with support services and community-based health care services, in order to promote greater care coordination, improve health status, and slow the growth of health care expenditures. This housing-with-services model is delivered to panels of approximately 100 participants; each panel is served by a full-time SASH coordinator and a quarter-time wellness nurse. Most of the 54 SASH panels in 2016 were hosted by non-profit housing organizations and located in federally subsidized or other non-profit affordable housing properties. At the regional level, six Designated Regional Housing Organizations (DRHOs) are responsible for planning the roll-out of the SASH program across their geographic regions; CSC serves as one of these six DRHOs.
Under contract from the U.S. Department of Health and Human Services and the U.S. Department of Housing and Urban Development (HUD), RTI International and the LeadingAge Center for Applied Research conducted an evaluation of the SASH program using Medicare and Medicaid claims data, data collected from interviews with SASH staff and key stakeholders, and a mail survey of Medicare beneficiaries. The quantitative analysis compares the health outcomes and service utilization of SASH participants with those of Medicare beneficiaries living in HUD-assisted properties not participating in SASH; this report summarizes the principal findings of the evaluation's analysis of Medicare and Medicaid claims data.
Which SASH Participants are Included in the Analysis?
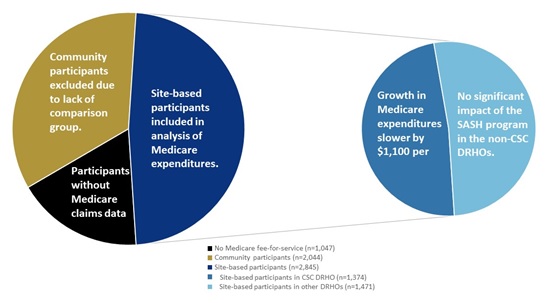
SASH was originally created to help meet the needs of older adults and individuals with disabilities living in affordable housing sites ("site-based participants"), but the program is also available to any Medicare beneficiary living in surrounding communities ("community participants"). About one-third of all SASH participants between 2011 and 2016 were community participants (see Exhibit 1). Community participants, who were typically referred into the program by their physicians or who sought out the program on their own, were excluded from the analysis of Medicare and Medicaid claims data due to the difficulty of identifying an appropriate comparison group. Another 18% of SASH participants were not Medicare fee-for-service (FFS) beneficiaries and so were excluded from the analyses due to lack of data on their health care expenditures and utilization. The remaining site-based participants with Medicare FFS coverage were included in the claims data analysis; for these participants, the SASH program became available in their housing properties, and so it is reasonable to compare them to similar residents of affordable housing properties which were not hosting the SASH program.
What Did the Evaluation Find?
-
Across the six DRHOs overseeing the SASH program at the regional level, participants in the CSC DRHO were least likely to be under the age of 65, while those in the Rural Edge DRHO were most likely to be under the age of 65. Participants in the CSC DRHO were also least likely to have originally qualitied for Medicare due to disability. The CSC and Rutland Housing Authority DRHOs have the highest proportion of participants aged 85 and older.
-
Medicare claims data also showed that, among the site-based SASH participants in the CSC DRHO panels, growth in annual Medicare expenditures was slower by an estimated $1,100 per beneficiary per year (see Exhibit 1). Participants in urban panels (i.e., those in Chittenden County) saw slower growth in Medicare expenditures of over $1,450 per beneficiary per year; the urban panels were a subset of the CSC DRHO panels. SASH participants in these panels also had slower rates of growth for hospital, emergency department, and specialty physician costs. However, there was no evidence that the SASH program decreased Medicare expenditures for the participants in the panels in the other five DRHOs.
-
The slower growth in Medicare expenditures among the CSC DRHO panels and the urban panels was driven by slower growth in Medicare expenditures among the dually-eligible SASH participants in those panels. Among participants in the CSC DRHO panels and the urban panels, about 45% were dually-eligible.
-
Analysis of Medicare claims data indicated that SASH participants in the urban panels had significantly lower rates of all-cause hospital admissions compared to non-participants.
-
Among dually-eligible SASH participants, growth in Medicaid expenditures for institutional long-term care was significantly slower for participants in the site-based panels and rural panels; the average impact was $400 per participant per year.
-
The SASH program had a favorable impact on the incidence of injuries (fractures, dislocations, and intracranial injuries) leading to an emergency department visit or hospitalization, among SASH participants over the age of 65. The increase in these injuries--often associated with falls--for the comparison beneficiaries was larger than the increase in injuries for the SASH participants.
What are the Lessons for Replication?
While we see slower growth in Medicare spending in the panels in the CSC DRHO, we do not see the same trend for panels in the other five DRHOs combined. We also estimated slower growth in Medicare spending for the panels in urban areas (Chittenden County), but not for panels in rural areas (all other counties). Note that the urban panels are a significant subset of the CSC DRHO panels.
In site visits, we identified possible differences that could help to explain these results. The CSC panels benefited from having an additional level of support and management, called SASH Team Leaders. While this Team Leader role has now been implemented throughout the SASH program, during much of the analysis period only the CSC panels benefited from this additional support and management role. Our interviews also revealed that the urban panels in Vermont had access to more health care and social support services than those in rural areas. This could also contribute to the favorable impact of SASH in urban panels.
Further, the SASH staff interviewed in the non-CSC DRHO panels indicated that their participant populations had a higher proportion of younger participants with disabilities, often behavioral health or substance abuse issues. Additional quantitative analyses confirmed that the CSC DRHO panels had a larger proportion of older participants and fewer who originally qualified for Medicare due to disability. The SASH program may have more favorable impacts on health care costs among panels with a larger proportion of older adults.
Conclusion
The SASH program is designed to promote greater care coordination for a population of older adults and individuals with disabilities who have high-cost health care needs and who are living in affordable housing properties and the surrounding communities. The program's unique contribution is its use of teams embedded in affordable housing properties as a platform to connect residents to health services and social supports. The evaluation identified slower growth in Medicare expenditures among SASH participants in CSC DRHO panels and the urban panels. Demographic differences between the DRHOs, the earlier presence of SASH Team Leaders in the CSC DRHO, and the greater availability of community resources in the urban areas may help to explain why the SASH program had a favorable impact for a large proportion of, but not all, SASH participants.
| EXHIBIT 1. SASH Evaluation Analysis Sample and the Impact of SASH on Medicare Expenditures on the Analysis Sample |
|---|
 |
Support And Services at Home (SASH) Evaluation
This Research Summary describes the primary features of the SASH program, and summarizes the main findings of the evaluation to date. Authors include: Amy Kandilov, Vincent Keyes, Noëlle Siegfried, Kevin Smith, Patrick Edwards, Jenna Brophy, Aubrey Collins, Ann Larsen, and Martijn Van Hasselt from RTI International; and Alisha Sanders and Robyn Stone from LeadingAge Center for Applied Research.
This paper was prepared under contract #HHSP23337006T between the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Disability, Aging and Long-Term Care Policy and RTI International. For additional information about this subject, visit the DALTCP home page at https://aspe.hhs.gov/office-disability-aging-and-long-term-care-policy-daltcp or contact the Project Officer at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201, Emily.Rosenoff@hhs.gov.
Reports Available
Support And Services at Home (SASH) Evaluation: First Annual Report
- HTML https://aspe.hhs.gov/report/support-and-services-home-sash-evaluation-first-annual-report
- PDF https://aspe.hhs.gov/pdf-report/support-and-services-home-sash-evaluation-first-annual-report
Support And Services at Home (SASH) Evaluation: Second Annual Report
- HTML https://aspe.hhs.gov/basic-report/support-and-services-home-sash-evaluation-second-annual-report
- PDF https://aspe.hhs.gov/pdf-report/support-and-services-home-sash-evaluation-second-annual-report
Support And Services at Home (SASH) Evaluation: Highlights from the First Four Years
- HTML https://aspe.hhs.gov/basic-report/support-and-services-home-sash-evaluation-highlights-first-four-years-research-summary
- PDF https://aspe.hhs.gov/pdf-report/support-and-services-home-sash-evaluation-highlights-first-four-years-research-summary
Support And Services at Home (SASH) Evaluation: Evaluation of the First Four Years
- HTML https://aspe.hhs.gov/basic-report/support-and-services-home-sash-evaluation-evaluation-first-four-years
- PDF https://aspe.hhs.gov/pdf-report/support-and-services-home-sash-evaluation-evaluation-first-four-years
Support And Services at Home (SASH) Evaluation: Highlights from the Evaluation of Program Outcomes from 2010 to 2016
- HTML https://aspe.hhs.gov/basic-report/support-and-services-home-sash-evaluation-highlights-evaluation-program-outcomes-2010-2016
- PDF https://aspe.hhs.gov/pdf-report/support-and-services-home-sash-evaluation-highlights-evaluation-program-outcomes-2010-2016
Support And Services at Home (SASH) Evaluation: SASH Evaluation Findings, 2010-2016