
Informal Caregiver Supply and Demographic Changes: Review of the Literature
Brenda C. Spillman, Eva H. Allen, and Melissa Favreault
Urban Institute
December 2020
Link to Printer Friendly Version in PDF Format (55 PDF pages)
ABSTRACT: There is a concern in the United States about the possibility of an impending “care gap” between the number of these traditional spouse and child informal caregivers available and the number of baby boomers requiring assistance as they age. This literature review examines: (1) the recent prevalence of care needs among older Americans and the informal supports available to meet them, (2) compensatory strategies used when traditional supports are not available, and (3) outcomes related to lack of care and use of compensatory strategies. And looks at projections of future gap between needs and key demographic and other trends that may affect projections.
This report was prepared under contract #HHSP233201600024I between HHS's ASPE/BHDAP and Urban Institute. For additional information about this subject, you can visit the BHDAP home page at https://aspe.hhs.gov/bhdap or contact the ASPE Project Officers, at HHS/ASPE/BHDAP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C., 20201; Judith.Dey@hhs.gov.
DISCLAIMER: The opinions and views expressed in this report are those of the authors. They do not reflect the views of the Department of Health and Human Services, the contractor or any other funding organization. This report was completed and submitted on February 12, 2019.
TABLE OF CONTENTS
NEED FOR CARE AND INFORMAL CARE AVAILABILITY
- Disability and Care Needs
- Informal Care Availability
- Assistive Device Use
- Paid Assistance
- Residential Alternatives
- Unmet Need for Assistance
- Reliance on Medicaid for Paid Assistance
EXISTING PROJECTIONS/FORECASTS
KEY TRENDS THAT MAY AFFECT PROJECTIONS
- Rising Educational Attainment
- Longer Working Years
- Increased Female Labor Force Participation
- Fertility, Family Structure, and Social Arrangements
- Increasing Diversity in the Older Population
- Geographic Dispersion of Families
- Changes in the Long-Term Care Delivery System
- Long-Term Care Costs and Workforce
- Technology Change
LIST OF FIGURES AND TABLES
- FIGURE 1: Need for Assistance with Routine Activities, NHATS 2001 and MCBS 2013
- FIGURE 2: Older Adults Meeting HIPAA Criteria
- TABLE 1: Concepts/Search Terms for Literature Review
ACRONYMS
The following acronyms are mentioned in this report.
| ADL | Activity of Daily Living |
|---|---|
| CAPABLE | Community Aging in Place--Advancing Better Living for Elders |
| HCAOA | Home Care Association of America |
| HCBS | Home and Community-Based Services |
| HIPAA | Health Insurance Portability and Accountability Act |
| HRS | Health and Retirement Study |
| IADL | Instrumental Activity of Daily Living |
| LTSS | Long-Term Services and Supports |
| MCBS | Medicare Current Beneficiary Survey |
| NHATS | National Health and Aging Trends Study |
| NLTCS | National Long-Term Care Survey |
| SSA | Social Security Administration |
INTRODUCTION
For decades, analysts have anticipated that aging of the large baby boom cohort would profoundly shape the use and cost of health and long-term care in the United States and other Western countries. Initially a primary focus was on the sheer number of baby boomers (birth years 1946-64) and the implications for demands on the health and long-term care systems (Knickman and Snell 2002; de Meijer, et al., 2013), with a few exceptions that also focused on implications for caregiving (Spillman and Pezzin 2000; Johnson, Toohey, and Wiener 2007).
Recently attention has shifted to potential effects of lower childbearing and other demographic factors on the future supply of spouses and children, traditionally the main source of informal caregiving. The concern in the United States and elsewhere is the possibility of an impending "care gap" between the number of these traditional spouse and child informal caregivers available and the number of baby boomers requiring assistance as they age, with implications for both recipients and family caregivers (Keefe, Légaré, and Carrière 2007; Pickard 2008, 2015; de Meijer, et al. 2013; Redfoot, Feinberg, and Houser 2013).
In this review, we first examine what is known about the following issues:
-
The recent prevalence of care needs among older Americans and the informal supports available to meet them.
-
Compensatory strategies used when sufficient traditional supports are not available.
-
Outcomes related to lack of care and use of compensatory strategies.
We then turn to existing projections or forecasts of future need for care and the gap between needs and informal care resources, methodologies used in projections, significant predictors, and key demographic and other trends that may affect projections
METHOD
To inform our review, we conducted a web-based literature search of relevant peer-reviewed and gray literature (e.g., reports produced for governmental agencies, foundations, or advocacy organizations). We limited the search primarily to work produced since 2010 because of dramatic changes in the long-term care delivery system and environment in recent years, but we include selected high-quality earlier works where appropriate. The search started with a core set of pertinent materials identified through prior work and search terms designed to address the research questions (Table 1). We augmented the initial terms with key words or concepts from particularly useful sources, and drew on sources cited in relevant studies only to a limited degree, because sources necessarily predate the studies in which they are cited.
| TABLE 1. Concepts/Search Terms for Literature Review |
|---|
| Basic Search Qualifiers |
| Aging, aged, late life, old-age, Medicare elderly or aged, older people/population, baby boom |
| Search Concepts/Terms |
| Prevalence |
| Disability and Care |
| Compensatory Strategies |
| Key Outcomes |
| Projections/Forecasts and Methodology |
| Key Trends Affecting Relationships and Projections |
NEED FOR CARE AND INFORMAL CARE AVAILABILITY
Only the earliest tier of the baby boom, born from 1946 to 1953, has reached age 65, and it will be 15-20 years before they reach ages when the risk of needing care is highest. National data sources on needs of the older population so far include at most the first few baby boom birth years. As a result, the best information available primarily reflects care needs, the relationship between key characteristics and disability rates, and informal care for the older population born before 1946 that is provided largely by the baby boom generation. Compiling estimates across sources is complicated by different data collection protocols used in national data sources that can lead to differences in estimates of ostensibly the same measure. We focus on two measures relevant to the aims of this project that are designed to capture, respectively, the overall prevalence of disability and the prevalence of severe disability.
Disability and Care Needs
Disability can be measured broadly to encompass impairment of body function or structure; activity limitation, or difficulty encountered performing routine activities; and restrictions in participation in life situations that result from the interaction of health and the physical and social environment at any age (World Health Organization 2018).
The definition of old-age disability most commonly used in the United States is narrower, however, focused on having difficulty or receiving help with specified routine activities of two types. The first type is self-care (bathing, dressing, toileting, and eating) or mobility activities, such as getting in or out of bed or chair and moving around inside, collectively termed as activities of daily living (ADLs), and associated with more serious disability (Katz 1969). The second type of activities include household and related activities, such as meal preparation, shopping, and money management, collectively termed instrumental activities of daily living (IADLs) (Lawton and Brody 1969). Although limitation in IADLs alone is associated with less severe or earlier stages of functional decline, it is highly relevant for the ability to live independently and may occur with or without ADL limitations. Including older adults experiencing difficulty doing activities without help is useful in characterizing the population who may be at risk of needing help--or unmet need when help is not available.
The most recent nationally representative published estimates for the Medicare population age 65 or older using this definition are from the National Health and Aging Trends Study (NHATS), which began data collection in 2011, and the 2013 Medicare Current Beneficiary Survey (MCBS). Because the sample for the 2011 NHATS was drawn in 2010, the survey includes only Medicare beneficiaries born in 1945 or earlier, just before the first baby boomers reached age 65. The population age 65 or older in the 2013 MCBS includes at most those born in the first three baby boom years (1946-48).
The NHATS estimates indicate that nearly half (48 percent) of the Medicare population age 65 or older in 2011 either received assistance with ADLs or IADLs or received no help but had difficulty performing one or more these activities even with any assistive devices they used. Such difficulty may be a precursor to the onset of help or an indicator of unmet need for help. (Freedman and Spillman 2014a). Almost 30 percent were receiving help, 2.9 percent in nursing homes and 25.8 percent in other settings, including traditional residences and supportive care settings, such as assisted living. The remaining half of older Medicare beneficiaries either had no limitations (21.7 percent) or were able to accommodate limitations by doing activities less often or by independent use of assistive devices (30 percent). Consistent with prior research, rates of disability requiring help were higher for women, unmarried persons, and African Americans, and Hispanics (Freedman and Spillman 2014a).
Estimates from the 2013 MCBS indicated that 44 percent of beneficiaries age 65 or older had difficulty or were unable to perform ADLs or IADLs (Federal Interagency Forum on Aging Statistics 2016), including 4 percent living in nursing homes or other long-term care facilities. Although the MCBS nursing home estimate is higher than the NHATS estimate of 2.9 percent, the MCBS definition may include a portion of respondents who were living in supportive settings other than nursing homes that would not be classified as nursing home residents in the NHATS (Freedman and Spillman 2014b).
| FIGURE 1. Need for Assistance with Routine Activities, NHATS 2011 and MCBS 2013 |
|---|
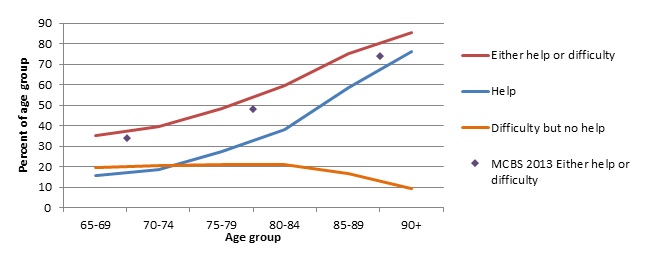 |
As seen in Figure 1, the proportion of older adults with difficulty or help rises steadily with age, which is the single strongest predictor of disability. NHATS estimates rise from 35 percent of those ages 65-69 to 85 percent of those age 90 or older. The proportion receiving help rose at an increasing rate with age, while the proportion experiencing difficulty who manage without help was essentially stable at 20 percent until age 85 and then fell to about 10 percent for those age 90+. The MCBS 2013 prevalence of difficulty or help by age (indicated by diamond markers in Figure 1) rose from 34 percent of those ages 65-74 to 74 percent of those age 85 or older and is similar to the 2011 NHATS estimates, although somewhat lower at higher ages.
A second, more narrow measure of old-age disability is survey-based approximation of the "benefit triggers" for tax-advantaged long-term care insurance policies specified in the Health Insurance Portability and Accountability Act (HIPAA) of 1996 (Drabek and Marton 2015). These HIPAA-based criteria focus on more severe disability, identifying people with chronic need for help with two or more ADLs, including incontinence, and adding severe cognitive impairment as a separate criterion. Besides establishing a benchmark for private insurance, the measure has become more common for approximating high-need for long-term care services generally and eligibility for Medicaid services specifically, although considerable variation across state programs remains (Drabek and Marton 2015; Willink, Davis, Mulcahy, and Wolff 2017). The criteria are approximated in survey data as receiving help for at least 90 days with two or more of six specified activities (eating, bathing, dressing, toileting, transferring to or from bed or chair, and incontinence), requiring substantial supervision because of severe cognitive impairment, or living in a nursing home (Drabek and Marton 2015).
| FIGURE 2. Older Adults Meeting HIPAA Criteria |
|---|
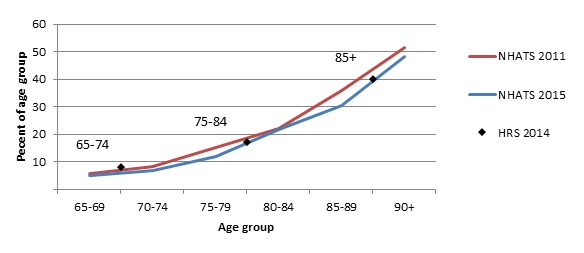 |
Figure 2 maps estimates of the population meeting HIPAA criteria available from the 2011 and 2015 NHATS and the 2014 Health and Retirement Study (HRS) (Spillman 2017; Johnson 2017). Estimates from the NHATS 2011 indicate that nearly 16 percent of the population age 65 or older meet the HIPAA criteria, rising with age from just under 6 percent of those ages 65-69 to about half of those age 90 or older. NHATS 2015 estimates, which include the first four baby boom birth years (1946-49), indicate a slightly lower percentage meeting HIPAA criteria through most of the age range, rising from just over 5 percent of those age 65-69 to just under half of those age 85 or older, and track well with the HRS 2014 estimates.
A further distinction of interest for considering both the demand for caregivers and the use of compensatory measures is IADL versus ADL limitations. Limitation only in IADLs, such as shopping and managing money, which are generally more amenable than ADLs to changes affecting the general population (e.g., direct deposit of Social Security checks, automatic bill paying, increasing availability of microwave ovens and pre-packaged meals, and telephone or online ordering of groceries and other supplies), largely drove overall declines in disability requiring assistance during the 1980s and 1990s (Spillman 2004). Declines in ADL limitations, indicating more severe needs and greater frailty, were far smaller and occurred only in the 1990s (Freedman, et al. 2004). A more recent study found evidence across five national data sources that declines did not continue into the early 2000s for either IADLs or ADLs for those ages 65-84, but may have continued for those age 85 or older (Freedman, et al. 2013). The study also found evidence of modest increases in the very low prevalence of disability among those approaching age 65 (ages 55-64), a finding that has been explored in other studies, expanding the period studied or the definition of limitation (Martin and Schoeni 2014; Chen and Sloan 2015).
Generally, for both older and younger people, protective effects of rising educational attainment and negative effects of obesity and related conditions, such as diabetes and cardiovascular disease, have been found to be at least partially offsetting, and the role of increased survival among people with disability onset earlier in life is unknown (Martin and Schoeni 2014). For the older population, the period from the early 1980s to the early 2000s has been associated with both medical and social trends that affect disability rates (Schoeni, Freedman, and Martin 2008). These include improved medical interventions for cardiovascular disease; increases in cataract surgery and knee and joint replacements; other pharmaceutical innovations for potentially disabling condition, such as arthritis; greater educational attainment; related reductions in poverty; and increased male longevity and associated declines in widowhood.
Informal Care Availability
Informal care networks are the primary source of long-term care for the older population in the United States. These networks are instrumental to older people's ability to remain in the community. Supporting community living has been a major focus of federal and state Medicaid policy in recent years. About 90 percent or more of older community-dwelling people receiving help with routine personal care or household tasks because of functional decline receive some informal care, and about two-thirds receive only informal care (Freedman and Spillman 2014a; Kaye, Harrington, and LaPlante 2010; Spillman 2009; Spillman and Black 2005). Collectively, informal caregivers provide 75-80 percent of total care hours for these older Americans, indicating the substantial amount of care that would have to be provided otherwise in their absence (Spillman 2009; Johnson and Wiener 2006). Research also has uniformly found that spouses and children are the main source of informal assistance, followed by other relatives, neighbors, or friends, although individual experiences differ, depending on the potential caregivers available and the strength of traditional relationships (Spillman and Pezzin 2000; Wolff and Kasper 2006; Freedman and Spillman 2014a).
Data from the NHATS and the companion National Study of Caregiving indicate that in 2011, 18 million informal caregivers provided 1.3 billion hours of care monthly to more than 9 million older adults receiving informal assistance at home or in supportive care settings other than nursing homes (Spillman, et al. 2014).
These older adults living in settings other than nursing homes had on average four potential network members, approximated by spouses, children, other household members, and social network members identified by respondents (Freedman and Spillman 2014a). About 1 percent of those receiving no assistance with IADLs or ADLs, 2.5 percent of those receiving assistance, and 8.7 percent of those living in supportive care settings had no potential network members.[1] The average actual care network size, including about 10 percent of caregivers who were paid non-relatives but excluding staff in supportive care settings, was 2.2 among those receiving assistance with ADLs and/or IADLs, rising with disability level, and 1.7 for those living in supportive care settings. Among residents in supportive care settings, 12.5 percent reported no helpers other than staff. About one in five actual caregivers were spouses or partners, just under half were children, 22 percent were other relatives, and about 9 percent were unpaid non-relatives (Spillman, et al. 2014).
Estimates in Spillman et al. (2014) indicate that informal caregivers for older adults provided an average of 75 hours a month of assistance, ranging from an average 110 hours for spouses to 35 hours for non-relatives. About a third of informal caregivers were age 65 or older, 51 percent were ages 45-64, and 17 percent were under age 45. Women were 62 percent of caregivers and provided an average 81 hours a month versus 65 monthly hours for men. Among caregivers other than spouses, about 30 percent lived with the care recipient providing an average of 114 hours of care monthly versus 45 hours for non-resident caregivers. The 42 percent of non-spouse caregivers who were unmarried provided an average 90 hours monthly versus 48 hours for married caregivers, and the 49 percent who were not working provided 81 hours of care monthly, versus an average 50 hours for workers. Only about 20 percent of non-spouse caregivers had children under age 18, and both they and those without minor children provided about 65 hours of care a month. For all caregivers, the presence of ADLs and, especially, dementia was associated with both substantially higher average hours of care and experiencing greater negative aspects of caregiving.
Despite the dominant role of informal care, research indicates that informal caregiving has evolved over the last few decades, in response to policy and demographic changes. A study using the National Long-Term Care Survey (NLTCS), the precursor to the NHATS, examined informal care from spouses and children, between 1984 and 1994, a period when the baby boomers' age range rose from 20-38 to 30-48 (Spillman and Pezzin 2000).[2] The study found a large increase in use of paid care consistent with Medicare program changes in the late 1980s and early 1990s that temporarily generated dramatic increases in Medicare home health use and spending for older adults with disabilities (Komisar 2002; McCall, et al. 2001; Murtaugh, et al. 2003)[3] as well as an increase in the proportions of spouses and children who were both working full-time and providing care, contemporaneous with increases in female labor force participation.
Spillman and Pezzin (2000) found that over the 1984-94 period the share of older adults receiving help with ADLs or IADLs decreased, primarily at lower care levels, accompanied by a decline in the prevalence of help from spouses and children, while the use of paid care increased, consistent with the increase in Medicare home health use. Spouses and children continued to be the dominant potential source of care, but as a group, they were less likely to be active caregivers in 1994 and more likely to be the primary caregiver if they were providing care. Thus, the reduction in informal caregiving was among family caregivers playing a secondary role, which may reflect substitution of paid care for secondary caregivers, but also may imply an increasing concentration of care among fewer family caregivers.
The study also found that full-time labor force participation among wives and daughters with a spouse or parent with disabilities rose from 43 percent in 1984 to nearly 48 percent in 1994. The proportion of full-time workers rose from 23 percent to nearly 28 percent among wives and daughters who were primary caregivers and from 53 percent to 56 percent for those who were secondary caregivers. The proportion of husband and son caregivers who were employed full-time also rose among primary caregivers but fell for secondary caregivers from about 69 percent to about 63 percent (Spillman and Pezzin 2000).
Perhaps because traditional family caregivers were plentiful, little literature has examined caregiving when spouses and children are not available. Analysis of the 1999 NLTCS found that about 15 percent of all older adults with chronic disabilities had neither a spouse nor child (Spillman and Black 2005). Among the 12 percent of community residents who lacked these traditional caregivers, one-third managed their disabilities with assistive devices and no help, about half received informal care provided by other relatives or non-relatives (27 percent only informal care, and 20 percent informal and paid care), and about one-fifth received only paid care. Use of only assistive devices was fairly invariant to whether a spouse or child was available, but among the 88 percent who had a spouse or child, nearly 70 percent received informal care and fewer than 5 percent received only formal care.
COMPENSATORY STRATEGIES
Dramatic changes have occurred over the last three decades in compensatory strategies to either substitute for or supplement care, despite relatively plentiful family care resources. Chief among compensatory strategies are increasing use of assistive devices, including home modifications; use of paid assistance; co-residence with relatives or others or moves to more accommodative housing; and use of residential care settings, including nursing homes and alternative supportive settings.
Assistive Device Use
Use of assistive devices as a compensatory strategy is an important factor that underlies but has not been addressed empirically in most previous studies of changes in old age disability discussed above. An innovation of the NHATS data collection protocol is the ability to identify additional older adults in the general population of Medicare beneficiaries who use devices to fully accommodate limitations. These beneficiaries, who report neither difficulty nor help with activities, are excluded in disability measures based on difficulty or help. Previous data sources conditioned device use questions either on having reported difficulty with activities or having been identified with chronic limitations in a screening instrument (Cornman, Freedman, and Agree 2005). Arguably, identification of a substantial proportion of the population with limitations missed by previous data collection protocols and examination of their characteristics is of particular interest for projecting future demand for caregiving.
Estimates from the 2011 NHATS indicate that 25 percent of older Medicare beneficiaries manage their limitations by using assistive devices and report no help and no difficulty performing related activities when they use their devices (Freedman, Spillman, and Kasper 2017). Adjusted models in a longitudinal analysis of 2011 NHATS participants who survived to 2012, the first follow-up year for the 2011 cohort, indicated that both initiation of and continuing successful accommodation of limitations with only assistive devices were more common for those ages 80-89, those with more children, and those living in homes with supportive environmental features, such as grab bars and bath seats. The authors speculate that the finding about children suggests that adult children may play an important role in identifying and encouraging parents to incorporate assistive devices into their daily lives. Further analysis found that relative to participants who were fully able in all activities, successful accommodation was associated with similar levels of well-being and only slightly lower ability to participate in valued activities (Freedman, Spillman, and Kasper 2017).
Spillman (2005) examined independent device use reported in the NLTCS, in which assistive device questions are asked only of people preidentified as having difficulty in a screening interview or previous survey rounds. Analysis using data for the period from 1984 to 1999 found that as disability managed with help declined, the use of assistive devices rose steadily within the population with chronic disabilities, driven primarily by independent use of devices. Over the 15-year period, the prevalence of device use among community residents with disabilities rose from 72 percent to 86 percent, and the prevalence of device use with no assistance rose from 13 percent to 25 percent.
A subsequent update indicated a continued increase in device use to 90 percent of community residents with disabilities between 1999 and 2004. But, contrary to the earlier period, the increase occurred entirely among older adults also using help, while independent device use with no assistance remained constant (Spillman 2014b). The devices that were most common and saw the largest increases were simple aids for mobility, bathing, and toileting (walkers, canes and crutches, tub or shower seats, and raised toilet seats), and the proportion using multiple types of devices increased by 2.5 percent a year between 1994 and 2004.
Exploratory cross-sectional multivariate analysis indicated that among those using both help and devices, independent use of devices with at least one activity was associated with reduced hours of informal and formal assistance, but not with increased unmet need. A supplemental analysis incorporating the presence of supportive environmental features in the home found that having such features was not associated with reduced unmet need, but that respondent identification of desirable features not present in the home was associated with higher unmet need (Spillman 2014b). Two other studies--Hoenig, Taylor, & Sloan (2003) using the 1994 NLTCS and Anderson and Wiener (2015) using the 2004 data--also estimated multivariate models and found an association between device use and reduced total hours and reduced informal care hours, respectively, although sample selection, disability measures, and methods differed across the three studies.
Paid Assistance
Data from the 2011 NHATS indicate that only 5 percent of older adults with disabilities living in settings other than nursing homes received only paid care, but about 33 percent received some care from paid non-relatives. This proportion has been stable since the mid-1980s, except for the dramatic temporary increase during the late 1980s and early 1990s associated with Medicare home health (Spillman 2009). In an analysis of data from the 2005 Survey of Income and Program Participation, Kaye et al. (2010) found that 18 percent of people age 65 or older living in households received paid care. Analysis of self-reported payment source data from the 2005 and 2006 Medical Expenditure Panel Survey indicated that older care recipients or family members were the primary (22 percent) or secondary (6 percent) payer for formal assistance; 24 percent reported at least some Medicaid payment, and 45 percent reported some Medicare payment.[4]
Research indicates that many retirees have not saved enough for retirement, let alone for potential long-term care costs, and in many cases, may misjudge their risks with respect to long-term care or income sufficiency (Society of Actuaries 2016; Munnell, Hou, and Sanzenbacher 2017; Wiener, et al. 2015). The median hourly rate in 2016 for unskilled homemaker services and personal assistance from home health aides was $20, and the median daily rate for adult day care was $68 (Genworth 2016). Assuming a moderate 24 hours a week of home care or three days a week of adult day care, those prices imply a median cost of between $900 and $2,000 a month (not taking into account fairly substantial geographic variation in rates) or roughly $11,000-$25,000 a year. In 2015, median total retirement income was about $55,000 for married couples and $21,000 for unmarried people, and Social Security represented 90 percent or more of retirement income for about a third of retirees (SSA 2017).[5] The average monthly benefit for new retirees in 2016 was about $1,400 a month or $17,000 a year. Overall, 8.8 percent of beneficiaries were poor (income below the federal poverty threshold), with far larger proportions among those who were unmarried (especially women) and those who were not non-Hispanic Whites. These estimates suggest that privately paid care at home is unlikely to be sustainable for long periods for many retirees, particularly for unmarried people and minorities, all of whom tend to have higher rates of disability requiring assistance (Freedman and Spillman 2014a). As a result, many of those with low income and assets who lack sufficient informal care resources may have to turn, as a last resort, to public support, specifically to Medicaid, the largest public payer for long-term services and supports (LTSS).[6]
Nursing home care is the only mandated Medicaid long-term care service, but a major thrust of federal and state Medicaid policy in recent years has been increasing community-based options for Medicaid LTSS. State programs can exercise a number of options, including various waiver programs and state plan benefits for low income older adults and others with disabilities. The proportion of total Medicaid LTSS spending for home and community-based services (HCBS) for older adults and people with physical disabilities increased from less than 20 percent in fiscal year 2000 to 45 percent in fiscal year 2016 (Eiken, et al. 2018). Both access to and the scope and quantity of services available, however, vary widely across states. The proportion of Medicaid LTSS spending that went for HCBS in fiscal year 2016 ranged from 13 percent in Kentucky to 80 percent in Oregon. Moreover, in many cases, income and asset allowances for Medicaid enrollees are too low to cover community living expenses (Johnson and Lindner 2016), and low reimbursements or program rules may further limit access to some providers. Thus, some older people eligible for Medicaid may defer enrollment as long as possible in order to remain at home, or enter nursing homes if functional or health declines make continued community residence infeasible. This may be particularly true for those who are unmarried or married couples in states where spousal impoverishment protections are available for HCBS recipients.
Residential Alternatives
Moves to explicit residential care settings and moves by older adults or their potential informal caregivers (primarily children) may be prompted by or in anticipation of declining health or function, particularly if a spouse is not present. On the other hand, recent trends toward increased intergenerational residence, particularly among millennials, may be driven by the needs or situation of children or for mutual economic or other support, rather than by parental care needs (Dettling and Hsu 2018; Zhang, Engelman and Agree 2013; Choi 2003). Moves also may be to settings such as retirement communities or senior housing, either near or far from family members, or to apartments or condominiums in areas where transportation, shopping, health care and other amenities are more accessible.
Intergenerational Households
For most of the 20th century, co-residence with children declined at an increasing rate for people age 65 or older, reaching a low point of 13 percent for older Whites in 1990 and 22 percent for older Blacks in 1970 before rising modestly, largely driven between 1950 and 2000 by increased income and education in the younger population (Ruggles 2007). Recent estimates based on Census data indicate a rebound in intergenerational households during and after the Great Recession from 12 percent in 1980 to 20 percent in 2016, with millennials most likely to live in multigeneration situations (Cohn and Passel 2018). Although intergenerational living was more common in both periods among all groups other than non-Hispanic Whites, the increases occurred for all races and ethnicities. The highest prevalence in 2016 was among Asian Americans (an increase to 29 percent from 26 percent) and the lowest among non-Hispanic Whites (an increase to 16 percent from 13 percent). A quarter of those age 85 or older, previously the most common age group, were living in multigenerational households in 2016, compared with a third of those ages 25-29.
A combination of widowhood, feasibility of residential options, and preferences may contribute to differences by age and sex in living arrangements. According to Current Population Survey data, three-quarters of men and nearly three-fifths of women ages 65-75 were living with a spouse or partner in 2018, compared with two-thirds of men and only one-third of women age 75 or older (Census Bureau 2019). A higher proportion of men and women in both age groups lived alone than with other relatives, but the proportion living with other relatives was higher in the older age group, 7 percent versus 5 percent for younger men and 20 percent versus 14 percent for younger women, possibly related to declining health or functioning. As seen in Figure 1 and Figure 2 above, only about 33 percent of older adults in the younger age group had difficulty or help with ADLs or IADLs, compared with 45-85 percent for the older age group, and fewer than 10 percent had severe disability, compared with 17-48 percent in the older age group.
We found only one study assessing how preferences or planning for future residential situations may differ for baby boomers. In a one-state (Connecticut) study Robison et al. (2014) examined expectations for living arrangement changes for baby boomers (born 1946-65) and older adults (born before 1946). Findings indicated that, relative to the older adults, baby boomers were significantly more likely to plan to move to an apartment, live in a retirement community or assisted living, or live with an adult child. For baby boomers and older adults combined, higher education was associated with plans for all alternative living situations except living with a child, and having potential caregivers[7] was associated with a higher expectation of living with an adult child and a lower expectation for other alternatives, including nursing home residence. Having experience as a caregiver was not associated with any of the potential residential plans, and having a current disability[8] was associated only with a lower expectation of moving to an apartment and a higher likelihood of assisted living or nursing home residence.
Choi et al. (2014) analyzed a sample of people who had at least one child at baseline and experienced the onset of ADL limitations over a two-year period. The authors found that, controlling for morbidity, age, and sex, those with lower socioeconomic status[9] were more likely to have children nearby or co-resident, less likely to have a non-disabled spouse, and more likely to have no spouse present. After further controlling for the number and prior work status of children, the authors found that having nearby or co-resident children was associated with higher probability of continued community residence with ADL assistance (26 percent and 32 percent versus 21 percent for those with no nearby children), and, within the group receiving ADL assistance, a lower probability of formal care. In a separate analysis Cho et al. (2015) found evidence that older adults' major health events may prompt moves by either a child or the parent experiencing the event to be closer or co-reside, particularly for unmarried older adults and those with a daughter.
Alternative Residential Settings and Use of Nursing Homes
The rise of alternative supportive care settings, such as assisted living, and the decline in nursing home use since the mid-1980s has been an important trend in the care options available to older adults with declining health or disabilities. Evidence from the NHATS indicates that in 2011, about 12 percent of older Medicare beneficiaries (4.5 million) lived in community settings other than traditional housing, and about 3 percent (1.1 million) lived in nursing homes. Among the 4.5 million in alternative community settings, 2.5 million were in retirement or senior housing communities, nearly 1 million were in independent living settings, and 1 million were in assisted living settings, the latter nearly on a par with the number living in nursing homes (Freedman and Spillman 2014b). For comparison, estimates from the 2002 MCBS and 1999 NLTCS found that 4.2 percent of the population age 65 or older were living in nursing homes and only 2.2 percent were in alternative residential care (Spillman and Black 2006).
Not surprisingly, both at the end of the 20th century and in 2011, relative to older people remaining in traditional community housing, larger proportions of those living in residential care alternatives to nursing homes were receiving help with ADLs, denoting more severe disability, or had Alzheimer's disease or other dementias; the proportions were even larger for those in nursing homes (Spillman and Black 2006; Freedman and Spillman 2014b). Larger proportions were women; unmarried, primarily because of widowhood; and low income relative to older adults living in traditional housing. Only the MCBS estimates indicated that older people living in residential care alternatives to nursing homes were also more likely to have income above $40,000 than people in all other types of residence. All three studies found that non-Hispanic Whites were overrepresented in alternative residential care settings and underrepresented in nursing homes.[10]
KEY POLICY OUTCOMES
The two central policy concerns related to a potential shortfall of informal care and use of compensatory strategies are that: (1) those without sufficient informal resources will experience a high rate of unmet need for care, which may lead to greater hardship and public costs because of further health and functional decline or adverse events such as falls, burns, inadequate nutrition, incontinence, missed physician appointments, depression, hospitalization, and emergency room visits; and (2) a combination of insufficient informal care and a lack of economic resources to pay privately for compensating supports and services will increase pressure on state and federal Medicaid spending to fill the gap. A further collateral policy concern is the possibility of increased Medicare spending, not only as the result of unmet needs for IADL or ADL care but also because of the critical role family caregivers play in the health and health care of older adults, particularly those with disabilities and/or dementia (Spillman, et al. 2014; Wolff and Spillman 2014).
Unmet Need for Assistance
Recent evidence regarding the prevalence and correlates of unmet need for assistance suggests that it is prevalent and is strongly associated with economic disadvantage, and specifically with the older population already enrolled in Medicaid.
NHATS assessed unmet among the 47 percent of older adults living in settings other than nursing homes who reported either difficulty performing ADL or IADL activities without help or receiving help. Unmet need was defined as having experienced one or more adverse consequences when help was not available, such as toileting accidents, medication errors, and going without clean clothes, groceries, or personal items (Freedman and Spillman 2014a). Nearly a third of older adults with difficulty or help reported at least one adverse consequence, the most common being toileting accidents (43 percent), not being able to go outside the home or building (30 percent) or places inside the home or building (26 percent), and medication errors (20 percent).
Adverse consequences were more common for minorities, widowed or unmarried people, and those in the lowest income quartile, and rose dramatically with the level of assistance, from 15 percent of those with difficulty but no help, to nearly three-quarters of those receiving help with three or more ADLs. Unmet need was particularly common--nearly 60 percent--for those receiving paid help in the community, relative to those receiving only informal care (42 percent) or living in residential care settings, combining independent and assisted living (36 percent).
Freedman and Spillman (2014b) examined how assistance and unmet need varied across a more detailed residential continuum from traditional housing to retirement housing, independent living, and assisted living and found that the prevalence of assistance was higher and physical and cognitive capacity lower in each successive setting. Unmet needs were common in traditional community housing (31 percent) but most prevalent in retirement or senior settings (37 percent) and assisted living settings (42 percent). Differences across settings in individual demographic, health, and functioning characteristics largely explained the elevated prevalence of unmet needs in assisted living, but not in retirement settings, where the odds of having an unmet need were twice that for residents in traditional housing for getting out of bed, getting cleaned up, shopping, laundry, and preparing hot meals. Further analysis indicated that the higher unmet need was associated only with the subset of persons in public housing for seniors.
Allen, Piette, and Mor (2014) examined differences in unmet need between those who are dually eligible for Medicaid and other Medicare beneficiaries. They found larger proportions of those who were dually eligible were female, minority race/ethnicity, unmarried, lived alone and had less than a high school education and three or more health conditions. They also were at least twice as likely to need assistance with multiple self-care or mobility activities (ADLs) and household activities (IADLs), and they were more likely to experience six of 11 adverse consequences included in the study.
Reliance on Medicaid for Paid Assistance
A study undertaken for Office of the Assistant Secretary for Planning and Evaluation using the NLTCS 2004 and linked Medicaid and other administrative data found that about 14 percent of Medicare beneficiaries age 65 or older in 2004 were eligible for Medicaid, and another nearly 5 percent had enrolled within four years of interview (Spillman and Waidmann 2014).[11] Baseline rates of enrollment were higher for women than men (17 percent versus 10 percent) and rose with age, from 12 percent for those ages 65-74 to 20 percent for those age 85 or older. Enrollment was lowest (10-13 percent) among who had no disabilities or managed their chronic disabilities without help, and rose with the level of disability, from 21 percent of those receiving help with only IADLs to 33 percent of those receiving help with at least three ADLs. The highest rates of baseline enrollment were 38 percent for those with cognitive impairment, which may be present at any level of assistance, and 63 percent for those living in institutional settings.
Among community residents not enrolled at baseline, the rate of transition to Medicaid was higher for those living alone, with someone other than a spouse, or in retirement settings. The highest rates of transition were for those living in community residential care settings, such as assisted living. Bivariate analysis found no difference in transition between those who had a daughter who was co-resident or lived nearby (as a proxy for access to informal care) and those who did not. Transition was strongly associated, however, with lower socioeconomic status (lower income, less than high school education, renters, and homeowners with low-value homes) and transition. Most transitions (56 percent) occurred among those still living in community settings, 10 percent occurred at nursing home admission, reflecting the generally less stringent financial eligibility for those who meet functional criteria for nursing home care, and a third transitioned by "spending down" assets an average of nine months after nursing home admission.
Multivariate results controlling for baseline characteristics indicated that long-stay nursing home entry in a given month was by far the largest predictor of transition during the four-year follow-up period, increasing the likelihood of transition 30-fold, but having events associated with potentially high out-of-pocket Medicare costs also were important. Short-stay nursing home use increased the likelihood of transition nearly fivefold, and inpatient and outpatient hospital use each increased the likelihood by 60 percent. The most important baseline characteristics were economic factors (low income, not owning a home), non-Hispanic Black race, and cognitive impairment. State policies were also important: living in a state with a high commitment to HCBS and/or extending spousal impoverishment protections to HCBS recipients each roughly doubled the likelihood of transition.
EXISTING PROJECTIONS/FORECASTS
Over the past several decades, various researchers have tried to quantify the risks that older adults now face of needing LTSS and how these risks are likely to evolve. Some of these studies build in the potential effects of demographic change--like change in the distributions of educational attainment, race-ethnicity, and presence of surviving spouses and children--in deep ways. Others focus on the most recent past experience and speculate about future implications. Some of these studies focus on a particular type of care use or need, such as nursing home needs (Hurd, Michaud, and Rohwedder 2013).
In one of the more recent studies, which uses dynamic microsimulation methods and data from a wide range of longitudinal sources, Favreault and Dey (2015) project that just over half of all early baby boomers turning 65 in 2015-2019 will need LTSS, and a quarter will have at least two years of need. Projections differ, however, by income and sex. A projected 31 percent of those in the lowest income quintile will need LTSS for at least two years versus 22 percent of those in the highest quintile, and 30 percent of women versus 20 percent of men will need at least two years of care, in part because women were projected to maintain their historical life expectancy advantage over men. Like Favreault and Dey (2015), Kemper, Komisar, and Alecxih (2005/2006) use a microsimulation model that is grounded in historic data and find large differences in men's and women's future projected LTSS needs. They project that the average spell of LTSS needs for women is about 70 percent longer than those for men: 3.7 years compared with 2.2 years.
Using a simulation approach geared at estimating economic and demographic differences across states, Redfoot, Feinberg, and Houser (2013) project how care gaps might evolve in coming decades. They begin by defining a caregiver support ratio--the ratio of the population ages 45-64 to the population ages 80 and older. The rationale for the choice is that recent studies have revealed that caregivers for older adults with disabilities are concentrated in their 40s and 50s. Their projections reveal that the caregiver support ratio should drop rapidly and steadily over the next 20 years, potentially leaving a large care gap and many seniors with unmet care needs. Although the simplicity of the approach holds considerable appeal, it also has some limitations. The age ranges are somewhat arbitrary, and with improvements in longevity, many people in their late sixties, their seventies, and even their eighties may be well positioned to provide care to family and friends with LTSS needs. Similarly, younger family members often provide care. Reductions in male mortality is leading to shorter average periods of widowhood, and thus lengthier periods when spouses can support one another. So even if one can glean important insights about future pressures through indices like these, more detail may be appropriate for developing more granular policy interventions.
In an earlier study using similar methods to Favreault and Dey (2015), Johnson, Toohey, and Wiener (2007) consider how sensitive projections of LTSS needs would be to alternative disability rates. They find a wide range in their projections of future needs. They also project that demand for formal care may increase more rapidly than the provision of informal care, in large part due to declines in family size and improvements in women's earnings prospects. These findings highlight the potential that families will find ways to adapt as informal care becomes costlier to provide.
A separate literature attempts to project future prevalence of older adults with dementia or cognitive impairment--an important subset of people with LTSS needs (Schoeni, Freedman, and Langa 2018). Studies relying primarily on the substantial correlation between advanced age and dementia, have projected that the global number of people with dementia could triple, barring delays in onset or treatment breakthroughs (Prince, et al. 2015). Recent studies examining dementia trends, however, suggest offsetting factors may moderate increases, and studies in higher income countries have found declines in dementia (Langa 2015; Wu, et al. 2017). Many studies in this area find large differences in prevalence and duration of severe cognitive impairment by sex and education. Those with the least education are more likely to be impaired at every age, and both their absolute and percentage time impaired are estimated to be longer (Crimmins, et al. 2018).
KEY TRENDS THAT MAY AFFECT PROJECTIONS
Several trends other than life expectancy and disability rates, will affect future caregiving demand and supply. These include demographic shifts and continuing evolution in options for LTSS. Important demographic trends include increasing educational attainment, delayed retirement, increased workforce participation among women, lower and/or delayed rates of childbearing, and changes in family structure. In addition, increasing racial and ethnic diversity and growing geographical dispersion of families are associated with changing cultural norms and attitudes about old-age and caregiving, and could affect the ways in which care needs are met. Ongoing changes in the long-term care delivery system, including shifts in the mode and cost of services, the direct-care labor supply, and reliance on technology to complement or substitute for traditional caregiving, also will affect both the demand for and supply of informal care.
Rising Educational Attainment
Higher educational attainment in the United States has been associated with better health, greater life expectancy, delayed onset of functional impairments, and lower care needs in older age (National Research Council 2012; National Academies of Sciences, Engineering, and Medicine 2015; Kasper 2017). The proportion of people age 65 or older who have more than a high school education has been increasing steadily since 1985, a trend that is projected to continue (Martin, Schoeni and Andreski 2010). Tabulations of Census Bureau data indicate that an increasing proportion of Americans reaching retirement age have completed more years of formal education: about 84 percent of people age 65 or older had a high school education or more, and about 27 percent had at least a bachelor's degree in 2014, up from 78 percent and 21 percent, respectively, in 2010, consistent with changes observed in the NHATS data between 2011 and 2015 (Kasper 2017). Thus, increased educational attainment among aging baby boomers implies the potential for reduced care needs as they age. However, recent studies indicating stable old-age disability in the 2000s and modest increases among baby boomers nearing retirement age raise doubts that these returns to education will persist (Freedman, et al. 2011; National Research Council 2012). Badley et al. (2015) found that increased obesity and associated disease burden among baby boomers have almost completely offset expected effects of their higher educational attainment. Uncertainty about future health and functioning in the baby boomer generation also is increased by other countervailing trends, such as increased opioid use-related mortality, which has occurred disproportionately in the baby boom generation (Huang, Keyes, and Li 2018).
Longer Working Years
Higher educational attainment also contributes to greater labor productivity, and, along with other prevailing trends such as increased longevity and improved health, increases potential for longer working years among older people (National Research Council 2012). From the worker's perspective, more highly paid, more fulfilling, and less physically demanding jobs associated with higher educational attainment make work at older ages more valuable and feasible. SSA policies raising the full retirement age discourage early retirement, and elimination of penalties for deferring benefits past full retirement age have reduced disincentives for continuing work (Maestas and Zissimopoulos 2010). Other secular trends also may contribute to later retirement. These include the decline of defined benefit pensions and rise of defined contribution retirement savings, declining availability of retiree health benefits, widespread elimination of mandatory retirement, lingering financial losses and debt from the Great Recession, and the increasing availability of part-time positions (Population Reference Bureau 2018).
In 2016, there were four working-age adults to each adult age 65 or older. With continued population aging, the ratio is expected to fall to 2.8 by 2030 when all baby boomers have passed age 65, and continue to decline thereafter as subsequent generations reach retirement ages (Census Bureau 2017). This trend may further support labor force opportunities for older adults who are willing and able to continue working. In 2011, 15 percent of men and 8 percent of women over the age of 70 years old were still in the labor force (National Research Council 2012). Almost a third of retirees in a 2017 survey of older adults reported working (Williams and Brown 2017). Most said they continued to work after retirement because they wanted to stay active, but the survey also found substantial levels of stress and concern among workers and retirees about their ability to afford LTSS in late life. Other research also indicates a changing retirement path, with half of retirees either working reduced hours after retirement or returning to work, in most cases based on pre-retirement intentions to do so (Maestas 2010).
Changing attitudes and expectations, discussed in more detail below, also indicate an increasing desire among older adults to provide for their own care as they age and avoid being a burden to their children and families. Such considerations could motivate more adults to remain in the labor force past conventional retirement ages and have beneficial impacts on lifetime earnings, retirement savings, and ability to afford paid caregiving if needed. An important factor, however, is differential health and disability trends for workers with lower education and earnings. Decisions to leave the labor force earlier could increase the need to rely on Medicaid and other public assistance if long-term care is needed, particularly if earlier retirement is related to health. Uncertainty about how older people will consider trade-offs between retirement and working longer complicates predictions of future care needs.
Increased Female Labor Force Participation
Changing social norms and strong economic growth have had a dramatic impact on female labor force participation. Between 1995 and 2000, the participation of women in the workforce rose from less than 40 percent to almost 80 percent before declining slightly (National Research Council 2012). Although women age 55 and older participate in the workforce at lower rates than younger women, their labor participation has been steadily growing since the mid-1990s and is projected to continue increasing as the overall United States population ages (National Research Council 2012). Because women are more likely to be primary caregivers for family members who are ill or have disabilities, increased female labor force participation has implications for availability of informal caregivers as well as their economic well-being. Literature on the relationships between caregiving responsibilities and labor force participation found that female caregivers, particularly those who live in the same household with the care recipient or who provide high level of care, were more likely than male caregivers and non-caregivers to be out of labor force, to retire, to earn less, to work fewer hours or make other adjustments to their work schedules to accommodate caregiving (Lilly, Laporte, and Coyte 2007; Van Houtven, Coe, and Skira 2013). Baby boomers are the majority of current caregivers for older adults. Therefore, negative effects of caregiving on lifetime earnings and retirement savings could reduce their ability to pay for their own care in the future and ultimately result in an increased demand for Medicaid LTSS. The absence of widespread paid leave policies, particularly for low income workers, is likely to exacerbate such effects (Feinberg 2018; National Academies of Sciences, Engineering, and Medicine 2016).
Fertility, Family Structure, and Social Arrangements
Next to spouses, children tend be the default informal caregivers to aging parents, so declines in fertility increase the potential for unmet need and greater need for formal care. Although fertility rates in the United States have not declined as much as in other industrial countries (National Research Council 2012), they dropped from an average of three children per family for the silent generation (born between the mid-1920s and mid-1940s) to an average of two children per baby boom family (Munnell, Chen, and Sanzenbacher 2018; Wettstein and Zulkarnain 2018). They reached their lowest level since the mid-1970s in 2017, when the total fertility rate was just 1,765.5 births per 1,000 women (Martin, et al. 2018). Increased education levels and female labor force participation among baby boomers have been associated with delayed childbearing, particularly for women with higher levels of education and higher-paying employment (Heck, et al. 1997; Budig and Hodges 2010). Fertility rate declines and delayed childbearing have persisted in the post¬-baby boom generations, implying the potential for a care gap in subsequent generations (Wettstein and Zulkarnain 2018). One countervailing trend to reduced access to children as caregivers is increasing life expectancy among men, reflected in increasing proportions of women living with spouses at older ages. Current Population Survey estimates indicate that the proportion of women living with a spouse or partner increased from 45 percent in 1970 to 59 percent in 2019 for women age 65-74, and from 21 percent to 35 percent for women age 75 or older (Census Bureau 2019).
Other changes in family structure, such as greater rates of divorce, cohabitation, and childlessness in the baby boom and subsequent generations have further implications for availability of informal caregivers and increased risk for unmet need (King and Scott 2005; Brown and Lin 2012; Stepler 2017; Brown and Wright 2017). Furthermore, data from the HRS indicate that the share of retirees with extended family and social networks, defined as having relatives and good friends living nearby and attending church regularly, has also been declining since 1994 (U.S. Congress Joint Economic Committee 2019). One study estimated that about one in five older adults are "elder orphans" at risk of aging alone with no or limited family and social support systems (Carney, et al. 2016). On the other hand, increasing educational attainment, higher labor participation among women, as well as potential for longer years of working may improve access to formal paid caregiving among older adults who lack informal caregiving (Span 2011).
In addition to independent living and age-restricted senior or retirement housing, where about 9 percent of older Medicare beneficiaries lived in 2011, other "grassroots" community-based models exist that are providing social and sometimes other supports for older adults who lack informal care. These include, for example, Age Friendly Communities, intergenerational co-housing, Villages, and Naturally Occurring Retirement Communities, all of which provide some degree of social and sometimes supportive services (Accius 2010; Greenfield, et al. 2013; Gonyea and Hudson 2015; Vladeck and Altman 2015; Davitt, et al. 2015). These and other such models often appear to be neither uniform enough in structure or composition for evaluation nor prevalent enough to quantify as a widespread solution for the older population (Koss and Almeida 2016). Common issues are whether they are equipped to allow aging-in-place as support needs increase, whether they are suitable or feasible for residents across a range of income levels, and the need for ongoing public or private financial and policy support to be sustainable over time (Golant 2014).
Increasing Diversity in the Older Population
The Census Bureau projects that America will become more racially and ethnically diverse over the next two decades, with minority groups outnumbering non-Hispanic Whites in 2043 (Ortman, Velkhoff, and Hogan 2014). This diversity will affect racial and ethnic composition of older population, with nearly 40 percent of older people expected to be of minority origin by 2050 (Ortman, Velkhoff, and Hogan 2014; Houser, Fox-Grage, and Ujvari 2018). Hispanics and Asians will represent the largest share of older minorities, fueled by growing share of immigrants coming to the United States from Latin America and East and South Asia today (Lopez, Bialik, and Radford 2018). Race/ethnicity and immigration are associated with different attitudes toward family responsibilities and may result in very different patterns of caregiving.
Research has found that foreign-born and second-generation populations tend to have stronger cultural preferences for "taking care of their own" and may be less likely to seek formal care than native-born White Americans (Anderson and Turner 2010; Chapleski, Sobeck, and Fisher 2003; Guo, et al. 2015; Jervis, Boland, and Fickenscher 2010; Min and Barrio 2009; Montenegro 2014; Silverstein and Wang 2015). Racial and ethnic cultural norms around filial obligations are changing, however, and may be weakening as a result of cultural assimilation (Silverstein and Wang 2015). For instance, some African Americans expressed preference for institutional care if they thought a high level of care was needed (Anderson and Turner 2010; Guo, et al. 2015), Japanese Americans are more likely than non-Japanese Americans to prefer care that would minimize dependence and burden on their families (Iwasaki, et al. 2015), and Korean Americans are willing to consider nursing home if their perceived health status is poor (Jang, et al. 2008). Other research suggests that immigrants may have smaller family and social networks than native-born Americans, which could mean lower access to informal caregiving in older years (Seltzer and Yahirun 2013).
Race, ethnicity, and gender differences are also evident in income and other socioeconomic characteristics of older Americans. Older Whites are three times as wealthy as older Hispanics and African Americans and also less likely to be poor. Older women of all racial backgrounds and ethnicities are more likely to be poor than older men (Seltzer and Yahirun 2013). Disparities in education and wealth affect life expectancy, with better-educated and higher income people living longer on average (National Academies of Sciences, Engineering, and Medicine 2015). A study examining active life expectancy--the number of years spent without disabilities--among older people between 1982 and 2011 found that active life expectancy increased for Whites but not for Blacks, particularly Black women (Freedman and Spillman 2016). Another study found that among baby boomers, Hispanics had worse health and lower incomes and educational attainment than non-Hispanic Whites (Villa, et al. 2012). Given these differences in socioeconomic characteristics and health, increasing racial diversity and income inequality in the United States alone may be associated with higher rates of disability and a greater need to rely on public assistance if informal supports are insufficient.
Geographic Dispersion of Families
Contrary to popular belief, the United States is not an increasingly mobile society. An analysis of the Census Bureau data found that overall mobility rates have declined since 1950 (Wolf and Longino 2005). Today's young adults are less likely to move than prior generations of young people (Fry 2017). While concerns that the growing geographic dispersion of families will reduce the future availability of informal caregivers may be slightly overstated, parents and adult children may not live close enough to provide informal care, particularly if the care requires day-to-day presence. A study examining differences in availability of informal caregivers among generational cohorts estimated that baby boomers may have lower likelihood of having adult children living within ten miles than previous generations (Ryan, et al. 2012). Indeed, an analysis of HRS data found that share of retirees with children who lived within ten miles fell from 68 percent in 1994 to 55 percent in 2014, driven in part by declining fertility in the same time period (U.S. Congress Joint Economic Committee 2019). Compton and Pollak (2015) found that the median distance between married couples and their mothers is less than 25 miles, although adult children with a college degree were less likely to live near their mothers. Given that educational attainment in the United States is rising, this finding could imply that more adult children will live far from their aging mothers in the future.
On the other hand, expansion of telework and work from home employment options could increase opportunities for adult children to move closer to their parents, including providing more flexibility to combine work and caregiving responsibilities for adult children who already live with or near aging and frail parents (Chokshi 2017; Radu 2018; Gohringer 2017; Office of Personnel Management 2015). In cases when relocation to care for elderly parents is not feasible or desirable, geographic dispersion of adult children may imply a lower supply of proximate informal care, but also may support long-distance informal caregivers who rely more on arranging and managing paid caregivers or use of supportive residential care settings or technology (Cagle and Munn 2012).
Changes in the Long-Term Care Delivery System
Recent trends in the long-term care delivery system reflect the general preference for "aging-in-place" among older adults and especially baby boomers (Brown 2015; HCAOA 2016; Johnson and Appold 2017). Although not always the case, care delivered at home may be less costly than facility-based care. One estimate indicates that the median cost of paid caregiving to older people who live at home is about $45,000 a year, similar to the cost of assisted living, while the cost of a private room in a nursing home is more than $90,000 a year (HCAOA 2016; Houser, Fox-Grage, and Ujvari 2018). Other options, such as adult day care may reduce both the cost of care and stress on family caregivers, particularly dementia caregivers (Zarit, et al. 2011; Harris-Kojetin, et al. 2013).
The preference for aging at home is reflected in the increased proportion of state and federal Medicaid LTSS spending that goes for HCBS. States are also moving to integrated, managed care models to better serve people with LTSS needs (Kaye 2014). Other health-related and LTSS-related innovations, such as federal, state, and local attention to social determinants of health, including access to housing and transportation for vulnerable populations, have expanded in part because of state concerns about the effects of the baby boomers on public costs (Spillman, Leopold, Allen, and Blumenthal 2017; Wallace 2014/2015). The aging of baby boomers also is likely to support continued growth in private market solutions, such as advances in assistive technology to support independent living and private pay home care services that can substitute for or supplement informal caregiving (HCAOA 2016).
Long-Term Care Costs and Workforce
Studies that examined the impact of the aging population on health care costs found modest effects overall, but large increases in the cost of long-term care for older people and people with disabilities (de Meijer, et al. 2013; Hagen 2013; Redfoot and Favreault 2018). Favreault and Dey (2015) estimated that on average, long-term care services will cost $138,100 per person, with more than half ($72,200) paid out-of-pocket. LTSS prices have been rising faster on average for institutional care than prices for HCBS services (Hagen 2013). In 2017, median annual costs were nearly $100,000 for a private nursing home, $45,000 for assisted living, $33,540 for a home health aide, and $18,200 for adult day services (Houser, Fox-Grage, and Ujvari 2018). The annual median cost of these services increased an average of 3 percent between 2017 and 2018 (Genworth 2018). Increases in the cost of these services outstripped the 2.1 percent overall inflation rate between 2017 and 2018. The five-year compounded average growth rate was about 3.5 percent for nursing facility care, 3 percent for assisted living, and more than 2.5 percent for home care and 2 percent for adult day care. Given these costs, formal long-term care over an extended period is unaffordable for many older Americans and becoming less affordable over time, suggesting that a growing proportion of older adults with long-term care needs will have to rely on Medicaid (Hagen 2013; Houser, Fox-Grage, and Ujvari 2018). The Congressional Budget Office found that between 2001 and 2010, on average about two-thirds of nursing facility residents were enrolled in Medicaid (Hagen 2013).
Private long-term care insurance holds little promise for helping most baby boomers bridge potential care gaps. Robison et al. (2013) found that about a quarter of older adults and 40 percent of baby boomers had no plans or did not know how they would pay for long-term care, about 40 percent planned to use savings or investments, about 22 percent expected to sell their homes, and about 20 percent overall and slightly smaller proportion of baby boomers expected to use long-term care insurance. The market for traditional stand-alone long-term care insurance reached its peak in 2002 and continues to shrink, although purchase of policies that combine long-term-care coverage with life insurance or annuities has increased somewhat (Gleckman 2017). Only 5 percent of Americans older than 40 years and 13 percent of those age 65 or older own insurance policies (Houser, Fox-Grage, and Ujvari 2018; Hagen 2013). Premiums for long-term care insurance are based on an applicant's health status and likelihood of disability and underwriting excludes a significant portion of would-be buyers, so that purchase generally makes economic sense only earlier in life (Hagen 2013). Research has shown that people who have children or other potential sources of informal care are significantly less likely to have long-term care insurance than people who lack access to informal care (Mommaerts 2016).
Rising long-term care costs are driven primarily by the shortage of qualified workers and increasing need for more specialized care (Genworth 2018). The number and qualifications of the direct workers needed in the future will depend on health and disability in the older population and personal preferences for types of care, which will be influenced by increasing diversity of older adults as well as federal and state policies with respect to Medicaid coverage and benefit design of long-term care services (Spetz, et al. 2015). The Bureau of Labor Statistics estimates faster job growth in home care than in other sectors over the next several years reflecting recent shifts from institutional care toward HCBS services (HCAOA 2016). Spetz et al. (2015) project that shifts from institutional to home care will increase the number of entry level positions. However, finding enough workers willing to take and continue in these low-wage positions may be difficult barring improvements, such as increasing the wage or adding benefits, such as health insurance (Kaye 2014; Houser, Fox-Grage, and Ujvari 2018). United States immigration policy could also affect the supply of workers willing to take on caregiving jobs.
Technological Change
Technology permeates nearly every aspect of life today, including health and caregiving. Disability declines in the 1980s and 1990s happened in the context of proliferation of everyday conveniences. The ability of current and future older adults to age in place and live more independently when physical and cognitive functioning declines may be enhanced by rapidly evolving technologies designed to address health and disability management (e.g., improved assistive devices, electronic access to personal and general health information, home monitoring) and development and dispersion of more general technologies relating to communication, transportation, and daily activities (e.g., smart phones, smart houses, digital assistants, ride-sharing, and adaptive software) (Bruce 2011; Jacelon and Hanson 2013; Liu, et al. 2016; Nam, Han, and Gilligan 2019; Gaugler, et al. 2019).
The baby boom generation came to adulthood and are maturing contemporaneously with major advances in information and other technology, and they also are the primary source of care for their aging parents. Thus, baby boomers as a group are comfortable with evolving productivity and other technologies, experienced and knowledgeable caregivers, a large consumer group with the capacity to shape market solutions, and an important constituency for long-term care policy changes (Lee, et al. 2019; Putnam 2008). They also are less resistant to rapidly new and evolving technologies that can both support greater independence and reduce the demands on their caregivers (Peek, et al. 2014; AARP Project Catalyst 2016). Examples of such technologies are online portals for monitoring health care and communicating with health care providers and in-home electronic monitoring of health and functioning with real-time transmission of information to health care providers and caregivers (Bruce 2011). Such advances could reduce the need for adult children to leave the labor force, reduce their work hours, or relocate to provide or manage care for the older parents. Children of the baby boomers, particularly millennials, are likely to be even more technology-focused caregivers (Flinn 2018; Coughlin 2018). On the other hand, research examining use of health-related technology among those age 54 or older indicates a continuing "digital divide" for racial and ethnic minorities relative to Whites, possibly tracing to effects of lower socioeconomic status (Mitchell, et al. 2019).
Just as advances in medical treatment were associated with the declines in old-age disability in the 1980s and 1990s, new medical discoveries and technologies, including genomics, artificial intelligence, and even robotics have the potential to enhance independence among baby boomers as they begin to reach ages when disability risks are highest, and ease the anticipated burdens on family caregivers, the health system, and public programs (Mattick, et al. 2014; Sanford Medicine 2018; Bolotnikova 2017).
Less flashy, but possibly more important, is continued growth of care models tailored to the needs of people with chronic conditions and functional deficits, and designed in some cases to improve functioning by addressing environmental and other factors. These care models include Community Aging in Place--Advancing Better Living for Elders (CAPABLE), an extension of an existing multicomponent person-directed approach to improve quality of life and physical functioning and reduce mortality through occupational therapy, physical therapy, and home modifications (Gitlin, et al. 2006, 2009). CAPABLE tested the effects of adding management of pain, medications, and depressive symptoms; communication with primary care practitioners; and home repair for a sample of low income community residents with disabilities, randomly assigned to treatment and control groups (Szanton, et al. 2019). After five months in the program, treatment group participants' ADL disability scores were 30 percent lower, and they were significantly more likely than the control group to report that the program made life easier, helped them with self-care, and increased their confidence.
CONCLUSION
Our review has included a wide range of literature and projections, based on current knowledge. These studies provide a solid starting place for projecting caregiving supply and demand for the baby boomers and later generations but also highlight areas of substantial uncertainty. Expansion of LTSS options and major demographic and societal trends will affect future caregiving demand and supply and outcomes, such as unmet need for care and reliance on Medicaid assistance. The size, endurance, and ultimate importance of these trends as the baby boom generation enters retirement ages is largely unknown at present. Among the most important areas of uncertainty identified in our review are the following:
-
Rising educational attainment has been associated with better health, increased longevity, lower care needs in older age, and the potential for greater economic security if better-educated older adults can work longer or return to the labor force. Yet, some studies suggest these returns to education may not persist if there is an education threshold for gains, or because of countervailing health-related trends, such as rising obesity.
-
Caregivers are disproportionately women, so their increased labor force participation has implications for the availability of caregivers and, in the absence of generally available paid leave, their economic well-being if they must reduce hours or quit working to take care of their frail family members.
-
Increasing diversity in the ethnicity, race, and nativity of the older population are associated with different attitudes toward family responsibilities and may result in very different caregiving patterns.
-
Expanding options for telework and work from home could improve flexibility to combine work and caregiving responsibilities but are not feasible or available for all types of employment, particularly low-wage jobs.
-
Rising long-term care costs, driven primarily by the shortage of qualified workers, make privately paid long-term care unaffordable for many low and middle income Americans and may increase the need to rely on Medicaid.
-
Effects of advances in technology are a large area of uncertainty that may have overarching implications for the demand and supply of caregivers. The ability to live more independently with functional decline can be enhanced by improved technology specific to disability and caregiving technologies, but also by generally applicable technology that reduces the physical and cognitive load of performing everyday activities, such as smart houses and widespread Internet access for activities such as shopping and communicating with health professionals.
Our review identified a number of other relevant uncertainties, such as various co-housing options and community-level initiatives for which no solid evidence on prevalence or trend is currently available. In contrast, for the areas of uncertainty highlighted above, sufficient information exists to at least develop sensitivity parameters for modeling their effects on caregiver demand, supply, and outcomes in terms of unmet need and reliance on Medicaid for the baby boomers
REFERENCES
AARP Project Catalyst. (2016). Caregivers and Technology. Washington, DC: AARP. Retrieved from https://www.aarp.org/content/dam/aarp/home-and-family/personal-technolo….
Accius, J.C. (2010). The Village: A Growing Option for Aging in Place. Washington, DC: AARP Public Policy Institute. Retrieved from https://assets.aarp.org/rgcenter/ppi/liv-com/fs177-village.pdf.
Allen, S.M., Piette, E., & Mor, V. (2014). The adverse consequences of unmet need among older persons living in the community: Dual-eligible versus Medicare-only beneficiaries. Journals of Gerontology, Series B: Psychological Sciences & Social Sciences, 69(7), S51-S58. doi: 10.1093/geronb/gbu124.
Anderson, J.R., & Turner, W.L. (2010). When caregivers are in need of care: African-American caregivers' preferences for their own later life care. Journal of Aging Studies, 24(1), 65-73. doi: 10.1016/j.jaging.2008.06.002.
Badley, E.M., Canizares, M., Perruccio, A.V., Hogg-Johnson, S., & Gignac, M.A. (2015). Benefits gained, benefits lost: Comparing baby boomers to other generations in a longitudinal cohort study of self-rated health. Milbank Quarterly, 93(1), 40-72. doi: 10.1111/1468-0009.12105.
Bee, A., & Mitchell, J. (2017). Do Older Americans have More Income than We Think? SESHD Working Paper #2017-39. Washington, DC: Census Bureau. Retrieved from https://www.census.gov/content/dam/Census/library/working-papers/2017/demo/SEHSD-WP2017-39.pdf.
Berman, C. (2014). What aging parents want from their kids. Atlantic. Retrieved from https://www.theatlantic.com/health/archive/2016/03/when-youre-the-aging-parent/472290/.
Bolotnikova, M.N. (2017). Anti-aging approaches. Harvard Magazine. Retrieved from https://harvardmagazine.com/2017/09/anti-aging-breakthrough.
Brown, K. (2015). Federal Strategy Needed to Help Ensure Efficient and Effective Delivery of Home and Community-Based Services and Supports. Washington, DC: Government Accountability Office. Retrieved from https://www.gao.gov/products/GAO-15-190.
Brown, S.L., & Lin, I.F. (2012). The gray divorce revolution: Rising divorce among middle-aged and older adults, 1990-2010. Journals of Gerontology Series B: Psychological Sciences & Social Sciences, 67(6), 731-741. doi: 10.1093/geronb/gbs089.
Brown, S.L., & Wright, M.R. (2017). Marriage, cohabitation, and divorce in later life. Innovation in Aging, 1(2), 1-11. doi:10.1093/geroni/igx015
Bruce, C.R. (2011). Informed decision making for in-home use of motion sensor-based monitoring technologies. Gerontologist, 52(3), 317-324. doi: 10.1093/geront/gnr124.
Budig, M.J., & Hodges, M.J. (2010). Differences in disadvantage: Variation in the motherhood penalty across White women's earnings distribution. American Sociological Review, 75(5), 1-24. doi: 10.1177/0003122410381593.
Cagle, J.G., & Munn, J.C. (2012). Long distance caregiving: A systematic review of the literature. Journal of Gerontological Social Work, 55(8), 682-707. doi: 10.1080/01634372.2012.703763.
Carney, M.T., Fujiwara, J., Emmert Jr. B.E., Liberman, T.A., & Paris, B. (2016). Elder orphans hiding in plain sight: A growing vulnerable population. Current Gerontology & Geriatrics Research, article ID 4723250, 11 pages. doi: 10.1155/2016/4723250.
Chapleski, E.E., Sobeck, J., & Fisher, C. (2003). Long-term care preferences and attitudes among Great Lakes American Indian families: Cultural context matters. Care Management Journals, 4(2), 94-100.
Chen, Y., & Sloan, F.A. (2015). Explaining disability trends in the U.S. elderly and near-elderly population. Health Services Research, 50(5), 1528-1549. doi: 10.1111/1475-6773.1 2284.
Choi, N.G. (2003). Coresidence between unmarried aging parents and their adult children. Who moved in with whom and why? Research on Aging, 25(4), 384-404.
Choi, H., Schoeni, R.F., Langa, K.M., & Heisler, M.M. (2015). Older adults' residential proximity to their children: Changes after cardiovascular events. Journals of Gerontology Series B: Psychological Sciences & Social Sciences, 70(6), 995-1004. doi: 10.1093/geronb/gbu076.
Choi, H.J., Schoeni, R.F., Langa, K.M., & Heisler, M.M. (2014). Spouse and child availability for newly disabled older adults: Socioeconomic differences and potential role of residential proximity. Journals of Gerontology, Series B: Psychological Sciences & Social Sciences, 70(3), 462-469, doi:10.1093/geronb/gbu015.
Chokshi, N. (2017). Out of the office: More people are working remotely, survey finds. New York Times. Retrieved from https://www.nytimes.com/2017/02/15/us/remote-workers-work-from-home.html.
Coe, N.B., Skira, M.M., & Larson, E.B. (2018). A comprehensive measure of the costs of caring for a parent: Differences according to functional status. Journal of the American Geriatrics Society, 66(10), 2003-2008. doi: 10.1111/jgs.15552.
Cohn, D., & Passel, J.S. (2018). A Record 64 million Americans Live in Multigenerational Households. Washington, DC: Pew Research Center. Retrieved from http://www.pewresearch.org/fact-tank/2018/04/05/a-record-64-million-americans-live-in-multigenerational-households/.
Compton, J., & Pollak, R.A. (2015). Proximity and co-residence of adult children and their parents in the United States: Descriptions and correlates. Annals of Economics and Statistics, Special Issue on the Economics of Gender (117/118), 91-114. doi: 10.15609/annaeconstat2009.117-118.91.
Cornman, J.G., Freedman, V.A., & Agree, E.M. (2005). Measurement of assistive device use: Implications for estimates of device use and disability in late life. Gerontologist, 45(3), 347-358. doi: 10.1093/geront/45.3.347.
Coughlin, J. (2018) Caregiver crunch? No problem, this is how tech-savvy millennials will care for aging baby boomers. Forbes. Retrieved from https://www.forbes.com/sites/josephcoughlin/2018/05/21/caregiver-crunch-no-problem-this-is-how-tech-savvy-millennials-will-care-for-aging-baby-boomers/#6ca822902034.
Crimmins, E.M., Saito, Y., Kim, J.K., Zhang, Y.S., Sasson, I., & Hayward, M.D. (2018). Educational differences in the prevalence of dementia and life expectancy with dementia: Changes from 2000 to 2010. Journals of Gerontology: Social Sciences, 73(S1): S20-S28. doi: 10.1093/geronb/gbx135.
Davitt, J.K., Lehning, A.J., Scharlach, A., & Greenfield, E.A. (2015). Sociopolitical and cultural contexts of community-based models in aging: The village initiative. Public Policy & Aging Report, 25, 15-19. doi: 10.1093/ppar/pru055.
de Meijer, C., Wouterse, B., Polder, J., & Koopmanscap, M. (2013). The effect of population aging on health expenditure growth: A critical review. European Journal of Ageing, 10(4), 353-361. doi: 10.1007/s10433-013-0280-x.
Dettling, L.J., & Hsu, J.W. (2018). Returning to the nest: Debt and parental co-residence among young adults. Labour Economics, 54, 225-236. doi: 10.1016/j.labeco.2017.12.006.
Drabek, J., & Marton, W. (2015). Measuring the Need for Long-Term Services and Supports. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. Retrieved from https://aspe.hhs.gov/basic-report/measuring-need-long-term-services-and-supports-research-brief.
Eiken, S., Sredl, K., Burwell, B., & Amos, A. (2018). Medicaid Expenditures for Long-Term Services and Supports in FY 2016. Medicaid Innovation Accelerator Program, IBM Watson Health. Retrieved from https://www.medicaid.gov/medicaid/ltss/downloads/reports-and-evaluation….
Fabius, C.D., & Thomas, K.S. (2018). Examining black-white disparities among Medicare beneficiaries in assisted living settings in 2014. Journal of the American Medical Directors Association, Epublication ahead of print. doi:10.1016/j.jamda.2018.09.032.
Favreault, M., & Dey, J. (2015). Long-Term Services and Supports for Older Americans: Risks and Financing. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. Retrieved from http://aspe.hhs.gov/basic-report/long-term-services-and-supports-older-americans-risks-and-financing-research-brief.
Favreault, M., & Johnson, R. (2017). Projections of Risk of Needing Long-Term Services and Supports at Ages 65 and Older. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation.
Feinberg, L.F. (2018). Breaking New Ground: Supporting Employed Family Caregivers with Workplace Leave Policies. Washington, DC: AARP Public Policy Institute. Retrieved from https://www.aarp.org/content/dam/aarp/ppi/2018/08/breaking-new-ground-supporting-employed-family-caregivers-with-workplace-leave-policies.pdf.
Flinn, B. (2018). Millenials: The Emerging Generation of Family Caregivers. Washington, DC: AARP Public Policy Institute. Retrieved from https://www.aarp.org/ppi/info-2018/millennial-family-caregiving.html.
Freedman, V.A., & Spillman, B.C. (2014a). Disability and care needs of older Americans. Milbank Quarterly, 92(3), 509-541. doi: 10.1111/1468-0009.12076.
Freedman, V.A., & Spillman, B.C. (2014b). The residential continuum from home to nursing home: Size, characteristics, and unmet needs of older adults. Journal of Gerontology: Social Sciences, 69 (1), S42-S50. doi: 10.1093/geronb/gbu120.
Freedman, V.A., & Spillman, B.C. (2016). Active life expectancy in the older US population, 1982-2011: Differences between Blacks and Whites persisted. Health Affairs, 35(8), 1351-1358. doi: 10.1377/hlthaff.2015.1247.
Freedman, V.A., Spillman, B.C., Andreski, P.M., Cornman, J.C., Crimmins, E.M., Kramarow, E., Lubitz, J., Martin, L.G., Merkin, S.S., Schoeni, R.F., Seeman, T.E., & Waidmann, T.A. (2013). Trends in late-life activity limitations in the United States: An update from five national surveys. Demography, 50(2), 661-671. doi: 10.1007/s13524-012-0167-z.
Freedman, V.A., Spillman B.C., & Kasper, J.D. (2017). Successful aging through successful accommodation with assistive devices. Journals of Gerontology Series B: Psychological Sciences & Social Sciences, 72(2), 300-309. doi: 10.1093/geronb/gbw102.
Freedman, V.A., Wolf, D.A., & Spillman, B.C. (2016). Disability-free life expectancy over 30 years: A growing female disadvantage in the U.S. population. American Journal of Public Health, 106(6), 1079-1085. doi: 10.2105/AJPH.2016.303089.
Fry, R. (2017). Americans are Moving at Historically Low Rates, in Part because Millennials are Staying Put. Washington, DC: Pew Research Center. Retrieved from http://www.pewresearch.org/fact-tank/2017/02/13/americans-are-moving-at-historically-low-rates-in-part-because-millennials-are-staying-put/.
Gaugler, J.E., Zmora, R., Mitchell, L.L., Finlay, J.M., Peterson, C.M., McCarron, H., & Jutkowitz, E. (2019). Six-month effectiveness of remote activity monitoring for persons living with dementia and their family caregivers: An experimental mixed methods study. Gerontologist, 59(1), 78-89. doi:10.1093/geront/gny078.
Geerts, J., Willemé, P., & Mot, E. (eds). (2012). Long-Term Care Use and Supply in Europe: Projections for Germany, the Netherlands, Spain and Poland. ENEPRI Research Report No. 116.
Genworth. (2016). 13th Annual Cost of Care Survey: Summary of 2016 Survey Findings. Retrieved from https://www.genworth.com/dam/Americas/US/PDFs/Consumer/corporate/131168_050516.pdf.
Genworth. (2018). 15th Annual Cost of Care Survey. Retrieved from http://investor.genworth.com/investors/news-releases/archive/archive/2018/Genworths-15th-Annual-Cost-of-Care-Survey-Shows-Continuing-Rise-in-Long-Term-Care-Costs/default.aspx.
Gitlin L.N., Hauck W.W., Dennis M.P., Winter L., Hodgson N., & Schinfeld S. (2009). Long-term effect on mortality of a home intervention that reduces functional difficulties in older adults: Results from a randomized trial. Journal of the American Geriatric Society, 57, 476-481. doi:10.1111/j.1532-5415.2008.02147.x.
Gitlin L.N., Winter L., Dennis M.P., Corcoran M., Schinfeld S., & Hauck W.W. (2006). A randomized trial of a multicomponent home intervention to reduce functional difficulties in older adults. Journal of the American Geriatric Society, 54, 809-816. doi:10.1111/j.1532-5415.2006.
Gleckman, H. (2017). The traditional long-term care insurance market crumbles. Forbes. Retrieved from https://www.forbes.com/sites/howardgleckman/2017/09/08/the-traditional-long-term-care-insurance-market-crumbles/#7e3975dc3ec3.
Golant, S.M. (2014). Age-friendly communities: Are we expecting too much? IRPP Insight, 5, 13-14. Retrieved from http://irpp.org/wp-content/uploads/assets/research/faces-of-aging/age-friendly/golant-feb-2014.pdf.
Gonyea, J.G., & Hudson, R.B. (2015). Emerging models of age-friendly communities: A framework for understanding inclusion. Public Policy & Aging Report, 25(1), 9-14, https://doi.org/10.1093/ppar/pru056.
Gohringer, K. (2017). Telecommuting and dependent care: Work solutions for caregivers. Virtual Vocations. Retrieved from https://www.virtualvocations.com/blog/telecommuting-survival/telecommuting-dependent-care-solutions/.
Greenfield, E.A., Scharlach, A.E., Lehning, A.J., Davitt, J.K., & Graham, C.L. (2013). A tale of two community initiatives for promoting aging in place: Similarities and differences in the national implementation of NORC programs and villages. Gerontologist, 53(6), 928-938. doi: 10.1093/geront/gnt035.
Guo, J., Konetzka, R.T., Magett, E., & Dale, W. (2015). Quantifying long-term care preferences. Medical Decision Making, 35(1), 106-113. doi: 10.1177/0272989X14551641.
Hagen, S. (2013). Rising Demand for Long-Term Services and Supports for Elderly People. Washington, DC: Congressional Budget Office. Retrieved from https://www.cbo.gov/sites/default/files/113th-congress-2013-2014/reports/44363-ltc.pdf.
Harris-Kojetin, L., Sengupta, M., Park-Lee, E., & Valverde, R. (2013). Long-term care services in the United States: 2013 overview. Rockville, MD: National Center for Health Statistics. Vital & Health Statistics, 3(37).
Heck, K.E., Shoendorf, K.C., Ventura, S.J., & Kiely, J.L. (1997). Delayed childbearing by education level in the United States, 1969-1994. Maternal & Child Health Journal, 1(2), 81-88.
Hoenig, H., Taylor D.H., & Sloan, F.A. (2003). Does assistive technology substitute for personal assistance among the disabled? American Journal of Public Health, 93(2), 330-337.
Home Care Association of America (HCAOA). (2016). Caring for America's Seniors: The Value of Home Care. Global Coalition on Aging. Retrieved from http://www.hcaoa.org/assets/1/27/Value_of_Home_Care___SECURED.pdf.
Houser, A., Fox-Grage, W., & Ujvari, K. (2012). Across the States: Profiles of Long-Term Services and Supports. Washington, DC: AARP Public Policy Institute. Retrieved from https://www.aarp.org/content/dam/aarp/research/public_policy_institute/ltc/2012/across-the-states-2012-full-report-AARP-ppi-ltc.pdf.
Houser, A., Fox-Grage, W., & Ujvari, K. (2018). Across the States: Profiles of Long-Term Services and Supports. Washington, DC: AARP Public Policy Institute. Retrieved from https://www.aarp.org/content/dam/aarp/ppi/2018/08/across-the-states-profiles-of-long-term-services-and-supports-full-report.pdf.
Huang, X., Keyes, K.M., & Li, G. (2018). Increasing prescription opioid and heroin overdose mortality in the United States, 1999-2014: An age-period-cohort analysis. American Journal of Public Health, 108(1), 131-136. doi: 10.2105/AJPH.2017.304142.
Hurd, M., Michaud, P.C., & Rohwedder, S. (2013). The lifetime risk of nursing home use. In D.A. Wise (ed.), Discoveries in the Economics of Aging, Chicago, IL: University of Chicago Press.
Iwasaki, M., Pierson, M.E., Madison, D., & McCurry, S.M. (2015). Long-term care planning and preferences among Japanese American baby boomers: Comparison with non-Japanese Americans. Geriatrics & Gerontology International, 16(9), 1074-1084. doi: 10.1111/ggi.12601.
Jacelon, C. S., & Hanson, A. (2013). Older adults' participation in the development of smart environments: An integrated review of the literature. Geriatric Nursing, 34, 116-121. doi: 10.1016/j.gerinurse.2012.11.001.
Jang, Y., Kim, G., Chiriboga, D.A., & Cho, S. 2008. Willingness to use a nursing home: A study of Korean American elders. Journal of Applied Gerontology, 27(1), 110-117.
Jervis, L.L., Boland, M.E., & Fickenscher, A. (2010). American Indian family caregivers' experiences with helping elders. Journal of Cross-Cultural Gerontology, 25(4), 355-369.
Johnson Jr., J.H., & Appold, S.J. (2017). U.S. Older Adults: Demographics, Living Arrangements, and Barriers to Aging in Place. Kenan Institute White Paper. Retrieved from http://www.kenaninstitute.unc.edu/wp-content/uploads/2017/06/AgingInPlace_06092017.pdf.
Johnson, R.W. (2017). What is the Lifetime Risk of Needing and Receiving Long-Term Services and Supports? Washington, DC: Urban Institute. Forthcoming 2019.
Johnson, R.W., & Lindner, S. (2016). Older Adults' Living Expenses and the Adequacy of Income Allowances for Medicaid Home and Community-Based Services. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. Retrieved from https://aspe.hhs.gov/basic-report/older-adults-living-expenses-and-adequacy-income-allowances-medicaid-home-and-community-based-services.
Johnson, R.W., Toohey, D., & Wiener, J.M. (2007). Meeting the Long-Term Care Needs of the Baby Boomers: How Changing Families will Affect Paid Helpers and Institutions. Washington, DC: Urban Institute. Retrieved from https://www.urban.org/research/publication/meeting-long-term-care-needs-baby-boomers.
Johnson, R.W., & Wiener, J.M. (2006). A Profile of Frail Older Americans and Their Caregivers. Washington, DC: Urban Institute. Retrieved from https://www.urban.org/research/publication/profile-frail-older-americans-and-their-caregivers.
Kahana, E., & Kahana, B. (2014). Baby Boomers' expectations of health and medicine. Virtual Mentor, 16(5), 380-384. doi: 10.1001/virtualmentor.2014.16.05.msoc2-1405.
Kasper, J.D. (2017). HIPAA estimates using the 2011 and 2015 NHATS. Memo to William Marton, Director, Division of Disability and Aging Policy. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation.
Kaye, H.S. (2014). Toward a model long-term services and supports system: State policy elements. Gerontologist, 54(5), 754-761. doi: 10.1093/geront/gnu01.
Kaye, H., Harrington, C., & LaPlante, M. (2010). Long-term care: Who gets it, who provides it, who pays, and how much? Health Affairs, 29 (1), 11-21. doi: 10.1377/hlthaff.2009.0535.
Keefe, J., Legare J., & Carriere, Y. (2005). Developing new strategies to support future caregivers of the aged in Canada: Projections of need and their policy implications. Canadian Public Policy, 33 (Supplemental 1), 1-16.
Kemper, P., Komisar, H.L., & Alecxih, L. (2005/2006). Long-term care over an uncertain future: What can current retirees expect? Inquiry, 42(4), 335-50. doi: 10.5034/inquiryjrnl_42.4.335.
King, V., & Scott, M.E. (2005). A comparison of cohabiting relationships among older and younger adults. Journal of Marriage & Family, 67(2), 271-285. doi:10.1111/j.0022-2445.2005.00115.x.
Koss, S., & Almeida, B. (2016). Community-Based Models for Aging in Place. Washington, DC: American Institutes for Research. Retrieved from https://www.air.org/sites/default/files/private/downloads/report/Community-Based-Models-for-Aging-in-Place-Nov-2016.pdf.
Knickman, J.R., & Snell, E.K. (2002). The 2030 problem: Caring for aging baby boomers. Health Services Research, 37(4), 849-884. doi: 10.1034/j.1600-0560.2002.56.x.
Langa, K.M. (2015). Is the risk of Alzheimer's disease and dementia declining? Alzheimer's Research & Therapy, 7, 34. doi:10.1186/s13195-015-0118-1.
Lee, C.C., Czaja, S.J., Moxley, J.H., Sharit, J., Boot, W.R., Charness, N., & Rogers, W.A. (2019). Attitudes toward computers across adulthood from 1994 to 2013. Gerontologist, 59 (1), 22-33. doi: 10.1093/geront/gny081.
Lilly, M.B., Laporte, A., & Coyte, P.C. (2007). Labor market work and home care's unpaid caregivers: A systematic review of labor force participation rates, predictors of labor market withdrawal, and hours of work. Milbank Quarterly, 85(4), 641-90. doi: 10.1111/j.1468-0009.2007.00504.x.
Liu, L., Stroulia, E., Nikolaidis, I., Miguel-Cruza, A., & Rincon, A.R. (2016). Smart homes and home health monitoring technologies for older adults: A systematic review. International Journal of Medical Informatics, 91, 44-59. doi: 10.1016/j.ijmedinf.2016.04.007
Lopez, G., Bialik, K., & Radford, J. (2018). Key Findings about U.S. Immigrants. Washington, DC: Pew Research Center. Retrieved from http://www.pewresearch.org/fact-tank/2018/11/30/key-findings-about-u-s-immigrants/.
Maestas, N., & Zissimopoulos, J. (2010). How longer work lives ease the crunch of population aging. Journal of Economic Perspectives: A Journal of the American Economic Association, 24(1), 139-160. doi: 10.1257/jep.24.1.139.
Martin, L.G., Freedman, V.A., Schoeni, R.F., & Andreski, P.M. (2009). Health and functioning among baby boomers approaching 60. Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 64(3), 369-377. doi: 10.1093/geronb/gbn040.
Martin, L.G., Schoeni, R.F., & Andreski, P.M. (2010). Trends in health of older adults in the United States: Past, present, future. Demography, 47(Supplement), S17-S40.
Mattick, J.S., Dziadek, M.A., Terrill, B.N., Kaplan, W., Spigelman, A.D., Bowling, F.G., & Dinger, M. E. (2017). The impact of genomics on the future of medicine and health. Medical Journal of Australia, 201(1), 17-20. doi: 10.5694/mja13.10920.
McCall, N., Komisar, H.L., Petersons, A., & Moore, S. (2001). Medicare home health before and after the BBA. Health Affairs, 20(3), 189-198.
Miller, A.R. (2011). The effects of motherhood timing on career path. Journal of Population Economics, 24, 1071-1100.
Miller, A.M. (2015). No spouse, no kids, no caregiver: How to prepare to age alone. U.S. News & World Report. Retrieved from https://health.usnews.com/health-news/health-wellness/articles/2015/10/26/no-spouse-no-kids-no-caregiver-how-to-prepare-to-age-alone.
Min, J.W., & Barrio, C. (2009). Cultural values and caregiver preference for Mexican-American and non-Latino White elders. Journal of Cross-cultural Gerontology, 24(3), 225-239. doi: 10.1007/s10823-008-9088-0.
Mitchell, U.A., Chebli, P.G., Ruggiero, L., & Muramatsu, N. (2019). The digital divide in health-related technology use: The significance of race/ethnicity. Gerontologist, 59(1), 6-14. doi: 10.1093/geront/gny138.
Mommaerts, C. (2016). Long-Term Care Insurance and the Family. https://drive.google.com/file/d/0By9dlLrSuqrXREdldHYzUWN0MTQ/view.
Montenegro, X. (2014). Caregiving Among Asian Americans and Pacific Islanders Age 50+. Washington, DC: AARP Research. doi: org/10.26419/res.00092.001.
More students than homes available for home share program. (2014). CBS News. Retrieved from https://www.cbc.ca/news/canada/newfoundland-labrador/more-students-than-homes-available-for-home-share-program-1.2751327.
Muir, T. (2017). Measuring Social Protection for Long-Term Care. OECD Health Working Papers, No. 93. Paris: OECD Publishing. doi: 10.1787/a411500a-en.
Munnell, A.H., Chen, A., & Sanzenbacher, G.T. (2018). Is the Drop in Fertility Temporary or Permanent? Chestnut Hill, MA: Boston College, Center for Retirement Research. Retrieved from http://crr.bc.edu/wp-content/uploads/2018/07/ib18-14-1.pdf.
Munnell, A.H., Hou, W., & Sanzenbacher, G.T. (2017). Do Households have a Good Sense of Their Retirement Preparedness? Chestnut Hill, MA: Boston College, Center for Retirement Research. Retrieved from http://crr.bc.edu/wp-content/uploads/2017/02/IB_17-4.pdf.
Murphy, S.L., Xu, J., Kochanek, K.D., & Arias, E. (2018). Mortality in the United States, 2017. NCHS Data Brief, No. 328. Hyattsville, MD: National Center for Health Statistics. Retrieved from https://www.cdc.gov/nchs/products/databriefs/db328.htm.
Murtaugh, C.M., McCall, N., Moore, S., & Meadow, A. (2003). Trends in Medicare home health care use: 1997-2001 the Balanced Budget Act has been successful at reining in the use of the home health benefit and shifting it toward skilled services. Health Affairs, 22(5): 146-156.
National Academies of Sciences, Engineering, and Medicine. (2015). The Growing Gap in Life Expectancy by Income: Implications for Federal Programs and Policy Responses. Washington, DC: National Academies Press. doi: 10.17226/19015.
National Academies of Sciences, Engineering, and Medicine. (2016). Families Caring for an Aging America. Washington, DC: National Academies Press. doi: 10.17226/23606.
National Research Council. (2012). Aging and the Macroeconomy: Long-Term Implications of an Older Population. Washington, DC: National Academies Press. doi: 10.17226/13465.
Ortman, J.M., Velkhoff, V.A., & Hogan, H. (2014). An Aging Nation: The Older Population in the United States. Washington, DC: Census Bureau. Retrieved from https://www.census.gov/prod/2014pubs/p25-1140.pdf.
Peek S.T.M., Wouters E.J.M., Van Hoof, J., Luijkx K.G., Boeije H.R., & Vrijhoef H.J.M. (2014). Factors influencing acceptance of technology for aging in place: A systematic review. International Journal of Medical Informatics, 83(4), 235-248. doi: 10.1016/j.ijmedinf.2014.01.004.
Pickard, L. (2008) Informal Care for Older People Provided by Their Adult Children: Projections of Supply and Demand to 2041. PSSRU discussion paper, 2515. London, UK: Personal Social Services Research Unit.
Pickard, L. (2015). A growing care gap? The supply of unpaid care for older people by their adult children in England to 2032. Ageing & Society, 35(1), 96-123. doi: 10.1017/S0144686X13000512.
Pickard, L., Wittenberg, R., Comas-Herrera, A., King, D., & Malley, J. (2012). Mapping the future of family care: Receipt of informal care by older people with disabilities in England to 2032. Social Policy and Society, 11(4), 533-545. doi:10.1017/S1474746412000346
Pope, E.H. (2012). Baby boomers set up as healthcare volunteers. New York Times. Retrieved from https://www.nytimes.com/2012/03/08/business/retirementspecial/baby-boomers-step-up-as-health-care-volunteers.html?_r=0.
Population Reference Bureau. (2018). Health and Working Past Traditional Retirement Ages. Today's Research on Aging, Program and Policy Implications No. 37. Retrieved from https://www.prb.org/wp-content/uploads/2018/04/TRA_37_Health_and_Working_Past_Traditional_Retirement_Ages.pdf.
Prince, M., Wimo, A., Guerchet, M., Ali, G., Wu, Y., & Prina, M. (2015). The global impact of dementia: An analysis of prevalence, incidence, cost and trends. World Alzheimer Report. London, UK: Alzheimer's Disease International. Retrieved from https://www.alz.co.uk/research/WorldAlzheimerReport2015.pdf.
Purington, K., & Williams, N. (2018). Case Study: How Indiana Addresses its Health Care Workforce Challenges. National Academy for State Health Policy (NASHP). Retrieved from https://nashp.org/wp-content/uploads/2018/11/IN-Workforce-Case-Study.pdf.
Radu, S. (2018). How soon will you be working from home? Telecommuting might not just be a company perk in the next decade. U.S. News & World Report. Retrieved from https://www.usnews.com/news/best-countries/articles/2018-02-16/telecommuting-is-growing-but-still-not-unanimously-embraced.
Redfoot, D., & Favreault, M. (2018). Population aging: A poor predictor of Medicaid expenditures. Public Policy & Aging Report, 28(2), 48-55. doi: 10.1093/ppar/pry012.
Redfoot, D., Feinberg, L., & Houser, A. (2013). The Aging of the Baby Boom and the Growing Care Gap: A Look at Future Declines in the Availability of Family Caregivers. Washington, DC: AARP Public Policy Institute. Retrieved from https://www.aarp.org/home-family/caregiving/info-08-2013/the-aging-of-the-baby-boom-and-the-growing-care-gap-AARP-ppi-ltc.html.
Reynolds, K. (2018). Lessons from Germany's Shared Housing Models: Expanding Ownership Opportunities and Improving the Built Environment. Retrieved from https://howhousingmatters.org/articles/lessons-germanys-shared-housing-models-expanding-ownership-opportunities-improving-built-environment/.
Robison, J., Shugrue, N., Fortinsky, R.H., & Gruman, C. (2013). Long-term supports and services planning for the future: Implications from a statewide survey of baby boomers and older adults. Gerontologist, 54(2), 297-313. doi: 10.1093/geront/gnt094.
Ruggles, S. (2007). The decline of intergenerational coresidence in the United States, 1850 to 2000. American Sociological Review, 72(6), 964-989. doi: 10.1177/000312240707200606.
Ruggles, S. (2011). Intergenerational coresidence and family transitions in the United States, 1850-1880. Journal of Marriage and the Family, 73(1), 138-148. doi: 10.1111/j.1741-3737.2010.00794.x.
Ryan L.H., Smith, J., Antonucci, T.C., & Jackson, J.S. (2012). Cohort differences in the availability of informal caregivers: Are the boomers at risk? Gerontologist, 52(2), 177-188. doi: 10.1093/geront/GNR142.
Scharlach, A., Graham, C., & Lehning, A. (2012). The "village" model: A consumer-driven approach for aging in place. Gerontologist, 52(3), 418-427. doi: 10.1093/geront/gnr083.
Schoeni, R.F., Freedman, V.A., & Langa, K.M. (2018). Introduction to a Supplement on Population Level Trends in Dementia: Causes, Disparities, and Projections. Journals of Gerontology, Series B: Psychological Sciences & Social Sciences, 73(S1), S1-S9. doi: 10.1093/geronb/gby007.
Seltzer, J.A., & Friedman, E.M. (2014). Widowed mothers' coresidence with adult children. Journals of Gerontology, Series B: Psychological Sciences & Social Sciences, 69(1), 63-74. doi: 10.1093/geronb/gbt072.
Seltzer, J.A., & Yahirun, J.J. (2013). Diversity in Old Age: The Elderly in Changing Economic and Family Contexts. California Center for Population Working Papers. Retrieved from http://papers.ccpr.ucla.edu/index.php/pwp/article/view/PWP-CCPR-2013-012.
Silverstein, M., & Giarrusso, R. (2010). Aging and family life: A decade review. Journal of Marriage & the Family, 72(5), 1039-1058. doi: 10.1111/j.1741-3737.2010.00749.x.
Silverstein, M., & Wang, R. (2015). Does familism inhibit demand for long-term care? Public policy implications of growing ethnic diversity in the United States. Public Policy & Aging Report, 25(3), 83-87. doi: 10.1093/ppar/prv016.
Smith, K.E., Scheuren, F., & Berk, J. (2001). Adding Historical Earnings to the Survey of Income and Program Participation (SIPP). Statistical Computing Section, American Statistical Association.
Social Security Administration (2017). Fast Facts & Figures About Social Security, 2017. SSA Publication No. 13-11785.
Solé-Auró, A., & Crimmins, E.M. (2012). Who cares? A comparison of informal and formal care provision in Spain, England and the USA. Ageing & society, 34(3), 495-517. doi: 10.1017/S0144686X12001134.
Sonnega, A., Faul, J.D., Ofstedal, M.B., Langa, K.M., Phillips, J.W., & Weir, D.R. (2014). Cohort profile: The health and retirement study (HRS). International Journal of Epidemiology, 43(2), 576-585. doi: 10.1093/ije/dyu067.
Span, P. (2009). When the Time Comes: Families with Aging Parents Share Their Struggles and Solutions. London: Springboard.
Span, P. (2011). Aging without children. New York Times. Retrieved from https://newoldage.blogs.nytimes.com/2011/03/25/aging-without-children/.
Spetz, J., Trupin, L., Bates, T., & Coffman, J.M. Future demand for Long-term care workers will be influenced by demographic and utilization changes. Health Affairs, 34(6), 936-945. doi: 10.1377/hlthaff.2015.0005.
Spillman, B.C. (2009). Policy Analyses Using the 2004 National Long-Term Care Survey. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation.
Spillman, B.C. (2014a). Updated Analyses of Trends in Use of Assistive Devices. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. Retrieved from https://aspe.hhs.gov/report/updated-analyses-trends-use-assistive-devices.
Spillman, B.C. (2014b). Why do elders receiving informal home care transition to long stay nursing home residency? Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. Retrieved from https://aspe.hhs.gov/basic-report/why-do-elders-receiving-informal-home-care-transition-long-stay-nursing-home-residency.
Spillman, B.C., & Black, K.J. (2005). Staying the Course: Trends in Family Caregiving. Washington, DC: AARP Public Policy Institute, Issue Paper #2005-17. Retrieved from https://pdfs.semanticscholar.org/47df/4fa1ca1ed6544a874a17a62c2b61b7bb15ed.pdf.
Spillman, B.C., & Black, K.J. (2006). The Size and Characteristics of the Residential Care Population: Evidence from Three National Surveys. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. Retrieved from https://aspe.hhs.gov/basic-report/size-and-characteristics-residential-care-population-evidence-three-national-surveys.
Spillman, B.C., Leopold, J., Allen, E.H., & Blumenthal, P. (2017). Developing Housing and Health Collaborations: Opportunities and Challenges. Washington, DC: Urban Institute. Retrieved from https://www.urban.org/research/publication/developing-housing-and-health-collaborations-opportunities-and-challenges.
Spillman, B.C., & Long, S.K. (2009). Does high caregiver stress predict nursing home entry? Inquiry: Journal of Health Care Organization, Provision, and Financing, 46(2), 140-161. doi: 10.5034/inquiryjrnl_46.02.140.
Spillman, B.C., & Pezzin, L.E. (2000). Potential and active family caregivers: Changing networks and the "sandwich" generation. Milbank Quarterly, 78(3), 347-374. doi: 10.1111/1468-0009.00177.
Spillman, B.C., & Waidmann, T.A. (2014). Rates and Timing of Medicaid Enrollment among Older Americans. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. Retrieved from https://aspe.hhs.gov/basic-report/rates-and-timing-medicaid-enrollment-among-older-americans.
Spillman, B.C., Wolff J.L., Freedman, V.A., & Kasper, J.D. (2014). Informal Caregiving for Older Americans: An Analysis of the 2011 National Study of Caregiving. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. Retrieved from https://aspe.hhs.gov/report/informal-caregiving-older-americans-analysis-2011-national-study-caregiving.
Stagg, B.C., Choi, H., Woodward, M.A., & Ehrlich, J.R. (2018). Association of social support network size with receipt of cataract surgery in older adults. JAMA Ophthalmology, 136(4), 423-427. doi: 10.1001/jamaophthalmol.2018.0244.
Stallard, E. (2011). Estimates of the incidence, prevalence, duration, intensity and cost of chronic disability among the U.S. elderly. North American Actuarial Journal, 15(1), 32-58. doi: 10.1080/10920277.2011.10597608.
Stallard, E., & Yashin, A.I. (2016). Long Term Care Morbidity Improvement Study: Estimates for the Non-insured U.S. Elderly Population Based on the National Long-Term Care Survey 1984-2004. Society of Actuaries.
Stampfl, N.S. (2015). Multigenerational Houses under One Roof. Goethe Institute. Retrieved from https://www.goethe.de/en/kul/mol/20537209.html.
Stanford Medicine. (2018). The democratization of health care. 2018 Health Trends Report. Palo Alto, CA: Stanford Medicine. Retrieved from https://med.stanford.edu/content/dam/sm/school/documents/Health-Trends-Report/Stanford-Medicine-Health-Trends-Report-2018.pdf.
Stepler, R. (2016). Smaller Share of Women Ages 65 and Older are Living Alone. Washington, DC: Pew Research Center. Retrieved from http://www.pewsocialtrends.org/2016/02/18/smaller-share-of-women-ages-65-and-older-are-living-alone/.
Stepler, R. (2017). Led by Baby Boomers, Divorce Rates Climb for America's 50+ Population. Washington, DC: Pew Research Center. Retrieved from http://www.pewresearch.org/fact-tank/2017/03/09/led-by-baby-boomers-divorce-rates-climb-for-americas-50-population/.
Stepler, R. (2017). Number of U.S. Adults Cohabiting with a Partner continues to Rise, Especially among Those 50 and Older. Washington, DC: Pew Research Center. Retrieved from http://www.pewresearch.org/fact-tank/2017/04/06/number-of-u-s-adults-cohabiting-with-a-partner-continues-to-rise-especially-among-those-50-and-older/.
Suitor, J.J., Gilligan, M., Pillemer, K., Fingerman, K.L., Kim, K., Silverstein, M., & Bengtson. V.L. (2018). Applying within-family differences approaches to enhance understanding of the complexity of intergenerational relations. Journals of Gerontology: Series B, 73(1), 40-53. doi: 10.1093/geronb/gbx037.
Super, N. (2002). Who will be There to Care? The Growing Gap between Caregiver Supply and Demand. National Health Policy Forum Background Paper. Washington, DC; National Health Policy Forum & George Washington University. Retrieved from http://uwiuaxj.nhpf.org/library/background-papers/BP_Caregivers_1-02.pdf.
Szanton, S.L., Xue, Q-L., Leff, B., Guralnik, J., Wolff, J.L., Tanner, E.K., Boyd, C., Thorpe Jr., R.J., Bishai, D., & Gitlin, L.N. (2019). Effect of a Biobehavioral Environmental Approach on Disability Among Low-Income Older Adults A Randomized Clinical Trial. JAMA Internal Medicine, 179(2), 204-211. doi:10.1001/jamainternmed.2018.6026.
Tomassini C., Glaser, K., Wolf, D.A., Van Groenou. B.M.I., & Grundy, E. (2004). Living arrangements among older people: An overview of trends in Europe and the USA. Population Trends, Spring(115), 24-34.
Truffer, C.J., Wolfe C.J., & Rennie, K.E. (2016). 2016 Actuarial Report on the Financial Outlook for Medicaid. Washington, DC: Report to the Office of the Actuary, Centers for Medicare & Medicaid Services, U.S. Department of Health & Human Services.
U.S. Census Bureau. (2019). Historical Living Arrangements of Adults. Retrieved from https://www.census.gov/data/tables/time-series/demo/families/adults.html.
U.S. Census Bureau. (2018). Older People Projected to Outnumber Children for First Time in U.S. History. Washington, DC: Census Bureau, National Population Projections, Release Number CB18-41. Retrieved from https://www.census.gov/newsroom/press-releases/2018/cb18-41-population-projections.html.
U.S. Census Bureau. (2017). 2017 national population projections tables, Table 2. Projected age groups and sex composition of the population. Retrieved from https://www.census.gov/data/tables/2017/demo/popproj/2017-summary-tables.html.
U.S. Congress Joint Economic Committee. (2019). An Invisible Tsunami: "Aging Alone" and Its Effect on Older Americans, Families, and Taxpayers. Retrieved from https://www.jec.senate.gov/public/index.cfm/republicans/analysis?ID=2A6AFA60-B7F1-4083-B445-79E0C2979BC4.
U.S. Office of Personnel Management. (2015). Handbook on Workplace Flexibilities and Work-Life Programs for Elder Care. Washington, DC: Office of Personnel Management. Retrieved from https://www.opm.gov/policy-data-oversight/pay-leave/leave-administration/fact-sheets/handbook-on-workplace-flexibilities-and-work-life-programs-for-elder-care.pdf.
Van Houtven, C.H., Coe, N.B., & Skira, M.M. (2013). The effect of informal care on work and wages. Journal of Health Economics, 32(1), 240-252. doi: 10.1016/j.jhealeco.2012.10.006.
Vasunilashorn, S., Steinman, B.A., Liebig, P.S., & Pynoos, J. (2012). Aging in place: Evolution of a research topic whose time has come. Journal of Aging Research, 2012, Article ID 120952, 6 pages. doi: 10.1155/2012/120952.
Villa V.M., Wallace S.P., Bagdasaryan S., & Aranda, M.P. (2012). Hispanic baby boomers: Health inequities likely to persist in old age. Gerontologist, 52(2), 166-176. doi: 10.1093/geront/GNS002.
Vladeck, F., & Altman, A. (2015). The future of the NORC-supportive service program model. Public Policy & Aging Report, 25, 20-22. doi:10.1093/ppar/pru050.
Wallace, S.P. (2014/2015). Equity and Social Determinants of Health among Older Aadults. San Francisco, CA: American Society on Aging. Retrieved from https://www.asaging.org/blog/equity-and-social-determinants-health-amon….
Wettstein, G., & Zulkarnain, A. (2017). How Much Long-Term Care do Adult Children Provide? Chestnut Hill, MA: Center for Retirement Research at Boston College, Report 17-11.
Wettstein, G., & Zulkarnain, A. (2018). Will Fewer Children Boost Demand for Formal Long-Term Care? Chestnut Hill, MA: Center for Retirement Research at Boston College.
Williams, A.R., & Brown, S.K. (2017). 2017 Retirement Confidence Survey: A Secondary Analysis of the Findings from Respondents Age 50+. Washington, DC: AARP Research. doi: 10.26419/res.00174.001.
Willink, A., Davis, K., Mulcahy, J., & Wolff, J.L. (2017). Use of Paid and Unpaid Personal Help by Medicare Beneficiaries Needing Long-Term Services and Supports. Washington, DC: An Issue Brief of the Commonwealth Fund.
Wittenberg, R., Pickard, L., Malley, J., King, D., Comas-Herrera, A., & Darton, R. (2008). Future Demand for Social Care, 2005 to 2041: Projections of Demand for Social Care for Older People in England. PSSRU Discussion Paper 2514. Personal Social Services Research Unit. Retrieved from https://www.pssru.ac.uk/pub/dp2514.pdf.
Wolf, D.A., & Longino, C.F. (2005). Our increasingly mobile society? The curious persistence of a false belief. Gerontologist, 45(1), 5-11. doi: 10.1093/geront/45.1.5.
Wolff, J.L., & Kasper, J.D. (2006). Caregivers of frail elders: Updating a national profile. Gerontologist, 46(3), 344-356. doi: 10.1093/geront/46.3.344.
Wolff, J.L., & Spillman, B.C. (2014). Older adults receiving health care assistance and their family caregivers: Prevalence, characteristics, and hours of care. Journals of Gerontology, Series B: Psychological Sciences & Social Sciences, 69 (Suppl 1), S65-S72. doi: 10.1093/geronb/gbu119.
World Health Organization. (2018). Disability and Health. Retrieved from https://www.who.int/news-room/fact-sheets/detail/disability-and-health.
Wu, Y.T., Beiser, A.S., Breteler, M.M.B., Fratiglioni, L., Helmer, C., Hendrie, H.C., Honda, H., Ikram, M.A., Langa, K.M., Lobo, A., Matthews, F.E., Ohara, T., Pérès, K., Qui, C., Seshadi, S., Sjölund, B-M., Skoog, I., &Brayne, C. (2017). The changing prevalence and incidence of dementia over time--Current evidence. Nature Reviews Neurology, 13, 327-339. doi:10.1038/nrneurol.2017.63.
Zarit, S.H., Kim, K., Femia, E.E., Almeida, D.M., Savla, J., & Molenaar, P.C.M. (2011). Effects of adult day care on daily stress of caregivers: a within-person approach. Journals of Gerontology, Series B: Psychological Sciences & Social Sciences, 66(5), 538–546. doi:10.1093/geronb/gbr030.
Zhang, Y., Engelman, M., & Agree, E.M. (2013). Moving considerations: A longitudinal analysis of parent-child residential proximity for older Americans. Research on Aging, 35(6), 663-687. doi: 10.1177/0164027512457787.
NOTES
-
In practice, it is impossible to identify all people who might become caregivers if the need arises. The NHATS inclusion of social network members is an advance over previous measures, but a limitation is that social network members were not identified for NHATS participants who had a proxy respondent. This limitation may account for some of the participants with no potential caregivers reported.
-
Informal care prevalence estimates included all caregivers, but caregiver-level analyses were limited to spouses and children because the survey collected detailed information on work and family only for spouses and children.
-
In a subsequent study, Spillman and Black (2005) found that the increase in paid care had virtually disappeared by 1999, after implementation of the first stage of prospective payment designed to curb the rapid rise in use and spending for Medicare home health.
-
Because of the limitations on Medicare's payment for supportive services, the Medicare reports may reflect confusion between Medicare and Medicaid and/or imprecise identification of services by survey respondents.
-
The Social Security Administration (SSA) did not provide income statistics in the most recent Fast Facts, citing concern that the Current Population Survey data underlying them understate income. See Bee and Mitchell (2017).
-
Benefits also may be available to older adults, including some with higher incomes, and their caregivers through the U.S. Department of Veterans Affairs, Administration for Community Living programs, including Aging and Disability Resource Centers, Area Agencies on Aging, and the National Family Caregiver Support Program, and through local and state programs, although these programs are small relative to Medicaid in both the populations served and the range and quantity of direct supports.
-
Relatives or friends who could help them with daily activities.
-
A specific physical, intellectual/cognitive, mood, or sensory impairment, or needed help with ADLs.
-
Measured by less than some college education.
-
The underrepresentation of minorities may not hold for younger Medicare beneficiaries with disabilities. Fabius et al. (2018) examined racial patterns using Medicare administrative data and found that relative to whites, black beneficiaries were disproportionally represented in assistive living settings and more often were younger, disabled, and dually eligible for Medicare and Medicaid.
-
The 5 percent estimate of transitions to Medicaid is roughly consistent an estimate in Wiener et al. (2013) using data from 1996/1998 to 2008 HRS that 13 percent of Medicare beneficiaries age 65 or older not initially covered by Medicaid enrolled over a 10-year to 12-year period.
Informal Caregiver Supply and Demographic Changes
This brief was prepared under contract #HHSP233201600024I between the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Behavioral Health, Disability, and Aging Policy and RTI International. For additional information about this subject, you can visit the BHDAP home page at https://aspe.hhs.gov/bhdap or contact the ASPE Project Officers at HHS/ASPE/BHDAP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201; Judith.Dey@hhs.gov.
Reports Available
Family Structures and Support Strategies in the Older Population: Implications for Baby Boomers Issue Brief
- HTML version: https://aspe.hhs.gov/basic-report/family-structures-and-support-strategies-older-population-implications-baby-boomers-issue-brief
- PDF version: https://aspe.hhs.gov/pdf-report/family-structures-and-support-strategies-older-population-implications-baby-boomers-issue-brief
Informal Caregiver Supply and Demographic Changes: Review of the Literature