
Functional Trajectories at the End of Life for Individuals with Dementia Issue Brief
Ila H. Broyles, PhD; Amy Huebeler, BS; Ira Dave, MS; Emily Graf, BA; Qinghua Li, PhD; Lauren Palmer, PhD; Zhanlian Feng, PhD; and Sarita L. Karon, PhD
RTI International
January 2020
Printer Friendly Version in PDF Format (4 PDF pages)
ABSTRACT
Dementia, including Alzheimer’s disease and related disorders, is a neurocognitive disease affecting an individual’s cognitive function and behavior. Dementia is a leading cause of death and is particularly prevalent at the end of life (EOL) in older adults. However, there is limited knowledge regarding the patterns of decline for adults with dementia, who may also have comorbid terminal conditions. This knowledge gap may prevent providers from offering palliative and hospice services, because they may not be able to identify when a dementia patient has entered the terminal phase of illness. It may also limit patients’ and families’ ability and willingness to access palliative services that can improve and complement EOL care.
For this project, we used a sample of decedents from the 2000-2012 Health and Retirement Study to understand the trajectories of functional decline of older adults with dementia near the EOL, and how these trajectories differ from those of people without dementia. In addition, we examined whether and how these trajectories vary by other patient characteristics such as demographics, comorbidities, and access to caregiving. Overall, the findings from the point-in-time analyses indicated that people with dementia have significantly higher levels of functional impairments than do people without dementia up until the last year of life. However, the functional impairment of people with dementia at 2-4 years before death may look similar to people without dementia in the last 6-12 months before death, after controlling for other characteristics.
This brief was prepared by RTI International under contract #HHSP23320160001I with the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Disability, Aging and Long-Term Care Policy. For additional information about this subject, visit the DALTCP home page at https://aspe.hhs.gov/office-disability-aging-and-long-term-care-policy-daltcp or contact ASPE Project Officers at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201,
Helen.Lamont@hhs.gov, Judith.Dey@hhs.gov, Iara.Oliveira@hhs.gov.
.
DISCLAIMER: The opinions and views expressed in this report are those of the authors. They do not reflect the views of the Department of Health and Human Services, the contractor or any other funding organization. This report was completed and submitted on June 2019.
BACKGROUND
Dementia, a terminal condition marked by cognitive impairment, affects at least 5.5 million Americans. Palliative care offers integrated care for patients with terminal illnesses including dementia, with a focus on improving quality of life through symptom management. One way Medicare beneficiaries can access palliative care is through the hospice benefit, which provides a comprehensive and holistic approach to treatment for patients who are terminally ill with a life expectancy of 6 months or less. Despite the potential benefits, health providers may be slow to offer the hospice benefit, and patients may be slow to opt for it until they are too near the end of life (EOL) to take full advantage of this type of care. For dementia patients, uncertainty around how long they may survive with their disease further complicates the difficult decision regarding when to focus on symptom relief rather than treatment.
One marker of approaching the EOL is a person's functional decline, as measured by a person's difficulty with the actions involved in daily self-care and mobility activities (also known as activities of daily living, or ADLs). There is growing evidence that functional decline near the EOL may differ depending on diagnosis and comorbidities. A better understanding of how functional decline may be different for people with dementia could help providers and policymakers assess whether existing models of care meet the needs of terminally ill people with dementia. We sought to understand whether the trajectories of functional status are different for older adults with and without dementia near the EOL and whether these trajectories vary by other patient characteristics like their comorbidities.
STUDY METHODS
We used data from the 2000-2012 Health and Retirement Study (HRS), a nationally representative, longitudinal panel study that interviews participants or their proxy every 2 years. Our sample included 5,853 people over the age of 65 who died ("decedents") during this time. We used the last two HRS surveys in decedents' lives to estimate the effect of dementia on functional status in each month in the last 4 years of life.
We measured a person's level of functional impairment by adding together the number of ADLs that the participant reported were difficult to perform (ranging from 0-6). ADLs included bathing, dressing, eating, bed transfer, toileting, and continence. An increasing number of ADL impairments from one time to the next indicates a person is experiencing a decline in his or her functional status. Using survey data, each decedents' number of ADL impairments was calculated in each of the last two surveys before death. We then constructed models to predict ADL impairments in each month in the last 4 years of life if patients did or did not have dementia, controlling for other patient characteristics such as demographics, socioeconomic status, residential setting, caregiving use, and comorbidities.
FINDINGS
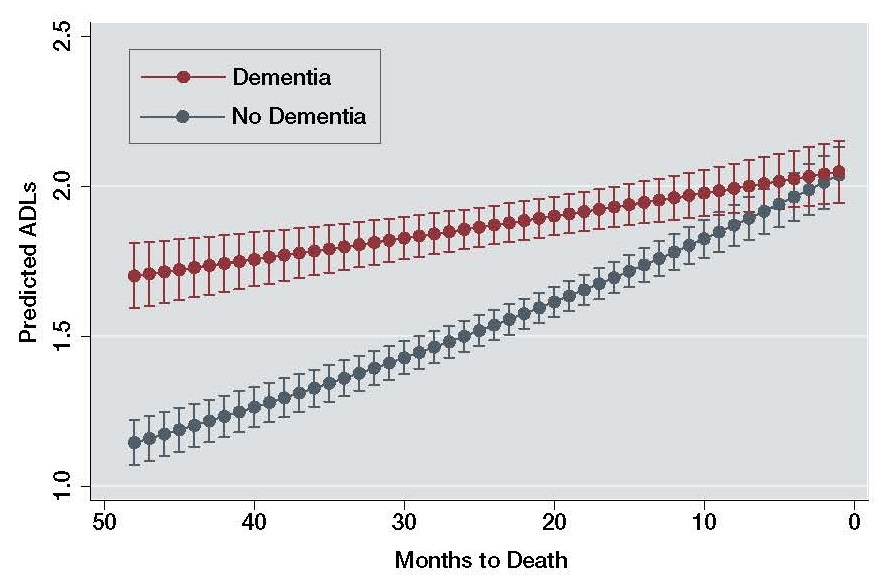
| FIGURE 1. Predicted ADL Impairments by Dementia Status |
|---|
 |
-
People with dementia had notably higher and sustained levels of predicted ADL impairment for longer periods of time before death compared to people without dementia. The predicted levels of ADLs for people with dementia 1-4 years before death were as high as predicted levels of ADLs for people without dementia only 6 months before death. In other words, people with dementia experience higher levels of difficulty with ADLs sooner and for more years in their EOL trajectory than people without dementia.
-
Dementia was associated with a slower and more gradual increase in ADL impairments in the last 4 years of life, after adjusting for demographic characteristics, comorbidities, and use of long-term services and supports.
-
After controlling for comorbidities (including cancer, stroke, obesity, etc.) and other characteristics, the adjusted functional status in the last 6 months of life was not significantly different between those with or without dementia.
-
Using this model, we found similar predicted ADL impairment (1.9 impairments) at 17 months before death for those with dementia, and 6 months before death for those with no dementia.
IMPLICATIONS
People with dementia have high and sustained levels of functional impairment several years before the end of their life, whereas people without dementia have comparably high functional impairment only at the very end of their life (last 6 months). In addition, people with dementia do not show a sharp functional decline in the last year of life as observed in patients without dementia. Without a clear functional change in the last year of life, accurately forecasting the remaining survival time for people with dementia may be challenging for providers, family members, and caregivers. Mischaracterizing the EOL timing of patients with dementia based on their functional decline alone may fail to recognize the specific care needs and treatments for this population in their last years of life. This might include adult day care, home care, and other services that people with dementia and their families could benefit from using.
| People with dementia do not show a sharp functional decline in the last year of life as observed in patients without dementia. |
Misinterpreting functional decline in patients with dementia may also affect how providers treat patients who have additional comorbidities. Because functional decline in the last months of life may be more marked for other terminal conditions, clinicians treating patients with a mix of diagnoses, like both cancer and dementia, may be tempted to look at functional status as a marker for the last months of life across clinical groups. These findings suggest that functional status change alone may not be a good indicator for determining the final phase of illness for people with dementia and comorbid conditions.
| People with dementia may need a longer period of sustained caregiving and more tailored care for their specific needs. |
Given these findings, existing models of EOL care may be insufficient and inappropriate to serve the longer period of decline typically observed in people with dementia. Multi-year periods of functional impairment in patients with dementia look similar to the last months of life for many other disease cohorts, highlighting that people with dementia may need a longer period of sustained caregiving and more tailored care for their specific needs. Models that offer palliative and supportive care at EOL but focus only on the last few months of life may be more effective with modifications to support people with dementia and their families.
Functional Trajectories at the End of Life for Individuals with Dementias
This brief was prepared by RTI International under contract #HHSP23320160001I with the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Disability, Aging and Long-Term Care Policy. For additional information about this subject, visit the DALTCP home page at https://aspe.hhs.gov/office-disability-aging-and-long-term-care-policy-daltcp or contact ASPE Project Officers at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201, Helen.Lamont@hhs.gov.
Reports Available
Functional Trajectories at the End of Life for Individuals with Dementia Issue Brief
- HTML version: https://aspe.hhs.gov/basic-report/functional-trajectories-end-life-individuals-dementia-issue-brief
- PDF version: https://aspe.hhs.gov/pdf-report/functional-trajectories-end-life-individuals-dementia-issue-brief
Functional Trajectories at the End of Life for Individuals with Dementia: Final Report