
U.S. Department of Health and Human Services
Work, Welfare, and the Burden of Disability: Caring for Special Needs of Children in Poor Families
Marcia K. Meyers, Anna Lukemeyer and Timothy M. Smeeding
Syracuse University, Maxwell School of Citizenship and Public Affairs, Center for Policy Research
April 1996
PDF Version: http://aspe.hhs.gov/daltcp/reports/wrkwlfes.pdf (53 PDF pages)
This report was prepared under grant #94ASPE263A between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and Syracuse University. For additional information about the study, you may visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the office at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. The e-mail address is: webmaster.DALTCP@hhs.gov. The Project Officer was Michele Adler.
The research is based on data collected by the University of California Data Archive and Technical Assistance, Berkeley, California under contract #21093 with the California Department of Social Services, Sacramento, California--Henry E. Brady, Principal Investigator. Interviews were conducted by the Survey Research Center, Berkeley, CA. The authors are grateful to Karin DAgostino for creative assistance with charts and tables, and to Douglas A. Wolf for econometric advice and assistance with statistical analyses. The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS
- BACKGROUND
- Prevalence and Severity of Childhood Disabilities
- Cash Assistance Programs for Families with Disabled Children
- Do Families with Disabled Children Incur Special Costs?
- Disabilities, Welfare "Dependence" and Work
- METHODS
- Data
- Sample Limitations
- Analysis
- RESULTS
- Characteristics and Program Participation
- Economic Well-Being
- Special Expenses
- Labor Force Participation
- APPENDICES
- APPENDIX A: Measures of Variables
- APPENDIX B
- LIST OF FIGURES
- FIGURE 1: Chronic Health Conditions and Disabilities: California Families Receiving AFDC in 1993
- FIGURE 2: Poverty Levels by Number of Disabled Children: Impact of Out of Pocket Expenditures on Poverty Level
- FIGURE 3: Poverty Levels by Number of Disabled Children and SSI Receipt: Income Adjusted for Expenditures
- LIST OF TABLES
- TABLE 1: Child's Disability or Chronic Condition, California Families Receiving AFDC in November 1992
- TABLE 2: Child's Disability by Severity and Supplemental Security Income Receipt: California Families Receiving Aid for Dependent Children in November 1992
- TABLE 3: Adult Caretaker and Family Characteristics by Presence and Severity of Child Disabilities: California Families Receiving AFDC in November 1992
- TABLE 4: Family Income and Welfare Use by Presence and Severity of Child Disabilities: California Families Receiving AFDC in November 1992
- TABLE 5: Family Hardship by Presence and Severity of Child Disabilities: California Families Receiving AFDC in November 1992
- TABLE 6: Out-of-Pocket Expenses in Prior Month for Special Needs of Disabled Child(ren), Families with One or More Disabled Children: California Families Receiving AFDC in November 1992
- TABLE 7: Out-of-Pocket Expenses in Prior Month for Special Needs of Disabled Child(ren) by Presence and Severity of Child's Disabilities: California Families Receiving AFDC in November 1992
- TABLE 7A: Out-of-Pocket Expenses in Prior Month for Special Needs of Disabled Child(ren) by Presence and Severity of Child's Disabilities: California Families Receiving AFDC in November 1992
- TABLE 8: Poverty Status with Adjustments for Out-of-Pocket Expenditures for Special Needs
- TABLE 8A: Poverty Status with Adjustments for Out-of-Pocket Expenditures for pecial-Needs Families at Different Poverty Levels
- TABLE 9: Labor Market Participation by Presence and Severity of Child Disabilities: California Families Receiving AFDC in November 1992
- TABLE 10: Variables in Logit Regression Means and Standard Deviations
- TABLE 11: Logistic Regression Results Coefficients
- TABLE A1: Coding of Severity: Children's Health Conditions and Disabilities
- TABLE B1: Control Variables
ABSTRACT
This paper addresses issues which arise at the juncture of welfare and disability policies. Using preliminary data from a recent survey of current and recent AFDC recipients in California, we find that disabilities and chronic health problems affect the mothers or children in 43 percent of all households in the AFDC system. The presence of one or more children with disabilities or chronic illnesses is found to have an impact on the economic well-being of families, with increased levels of direct hardship reported by families caring for one or more severely impaired children. Potential causes of higher levels of hardship are examined by considering the impact of direct expenses associated with the care of the child(ren) and reductions in the mother's probability of paid employment. SSI receipt is found to have a modest antipoverty effect for families with special needs children, reducing the prevalence of poverty and extreme poverty for families even after the additional direct costs of caring for these children are considered.
INTRODUCTION
Means-tested cash transfer programs are the focus of continuing controversy in state and federal welfare "reform" efforts. Two programs that benefit poor children have become particularly prominent targets of public and political controversy: Aid to Families with Dependent Children (AFDC) and Supplemental Security Income (SSI). Both programs provide means-tested cash assistance for children in poor families. AFDC, the federal/state cash entitlement program for families, has been the target of nearly continuous reform efforts since its rapid expansion in the 1970s. SSI, the federal cash assistance program for disabled individuals, has been, until recently, a relatively small and uncontroversial program. Growth in the number of child claimants in the past six years has propelled this program into the political spotlight and motivated a variety of "reform" proposals.
One group of potential claimants will be particularly affected by AFDC and SSI reforms: low-income families that care for disabled and chronically ill children. Depending on their income and disability status, these families may participate in one or both programs. Dual program participation and the special needs of disabled children create complexities with important implications for welfare policies. Families eligible for benefits under either program, for example, have incentives to pursue higher benefits through SSI; this appears to have consequences for state welfare and SSI caseloads. Those who care for seriously impaired children often incur higher medical and other costs; the frequency and size of these costs has implications for benefit levels and equity between the programs. These same parents may face special barriers to employment, self-sufficiency and participation in work preparation activities arising from the extra care needed by their disabled children; this has implications for work tests, time limits and other welfare reform policies. Additional complexities arise if parents in these families are themselves disabled or in poor health.
Although child and adult disabilities have obvious relevance to welfare policies, we still know relatively little about the extent and impact of disabilities and chronic health problems among welfare recipients. We lack good data on the prevalence of physical disabilities in the welfare population. Estimates of the prevalence of other, less easily measured limitations such as cognitive limitations, substance abuse and behavioral dysfunctions are even more limited. We also lack detailed analyses of the impact of these limitations on families' economic well-being. There are few studies of the impact of disabilities on women's employment; research is particularly scarce on disabilities in the population of single, low-income mothers who constitute the majority of welfare recipients. Estimates of the cost of caring for children with disabilities, in terms of direct expenditures and foregone earnings, are even less well developed.
This paper steps into this vacuum by addressing questions about individual functioning which arise at the junction of welfare and disability policies. Using preliminary data from a survey of current and recent AFDC recipients in California, we examine the prevalence and economic impact of children's health conditions and disabilities on poor families. First, we review the outstanding policy issues and current research related to these issues. Next, we pose the research questions. We then describe the data and methodology and present the results. Finally, we draw guarded conclusions and discuss their relevance to outstanding policy questions.
BACKGROUND
Defining childhood disabilities, and estimating their prevalence and impact on families' economic well-being are critical first steps in the design, delivery, and evaluation of public assistance programs for families who care for children with special needs.1 But these tasks are complicated by difficulties associated with the early identification of disabilities, ambiguities in program eligibility criteria, and disagreements about reporting-categories, definitions, and survey methodologies. In the following sections we review some of the outstanding controversies mi income assistance programs for poor families with special needs children, and what is currently known about the prevalence and impact of their special needs.
Prevalence and Severity of Childhood Disabilities
Estimates of the prevalence of childhood chronic illness and disability vary widely, depending on the data source, the researcher, and the population. Drawing on the 1988 National Health Interview Survey (NHIS), for instance, Newacheck and Taylor (1992) estimate that 30 percent of children under age 18 suffer from chronic illnesses when relatively mild conditions with little functional impact, such as mild allergies, are included. They estimate that only 9 percent of children suffer from moderately severe chronic conditions and 2 percent suffer from severe chronic illnesses. From that same data, Aday (1992) concludes that 15 percent of children have chronic illnesses causing major limitations in activities or serious pain or discomfort. Both Aday's and Newacheck and Taylor's estimates are based on data that exclude cancer and mental health problems. Using data from the 1990 and 1991 panels of the Survey of Income and Program Participation (SIPP), which does include mental health conditions but has fewer measures of mild health conditions, McNeil (1993) estimates that approximately 5 percent of United States children under age 15 suffer from disabilities and 1 percent have a severe disability.
The relative prevalence of disability also varies according to the researcher's definition of disabling conditions and the data collection methods. Using the NHIS data, Newacheck and Taylor report respiratory allergies as the most prevalent condition (afflicting about 10 percent of all children), followed by chronic ear infections, asthma, eczema and skin allergies, hearing or visual impairments, and speech defects. Drawing on the SIPP data, which included questions to elicit information about both physical and mental disabilities, McNeil concludes that learning disabilities are the most common disability, followed by speech problems, mental retardation, asthma, and mental or emotional disorders. Children with learning disabilities accounted for 29 percent of the total number of disabled children in McNeil's study. About 13 percent reported speech disorders, followed by mental retardation (7 percent), asthma (6 percent), and mental or emotional disorders (6 percent).
In general, disabilities increase with age, and, among children, disabilities are more common among boys (Newacheck and Taylor 1992; McNeil 1993). Children in low-income families are also more likely to suffer chronic illnesses and disabilities (Newacheck and McManus 1988; McNeil 1993). Newacheck (1988) estimates that children in low-income families face a 40 percent higher risk of being disabled. The causes of this higher prevalence are presumed to be multiple and interacting. Children in low-income families are more likely to five in poor neighborhoods where they are exposed to heightened environmental risks. They are more likely to be low birth weight and to suffer other complications associated with poor maternal nutrition, health behaviors, and health care. Children in poor families are also less likely to receive the adequate early nutrition, housing, and health care that might help prevent the development of serious disabilities and health conditions.
Cash Assistance Programs for Families with Disabled Children
Although estimates vary, both national prevalence studies and program data indicate that a substantial fraction of low-income families care for one or more children with special needs. The needs of these families for income support, medical care, and special services are at the center of national policy debates. In particular, poor families with disabled children may qualify for benefits from two different cash assistance programs which have become lightening rods for political controversy: Aid to Families with Dependent Children (AFDC) and the Supplemental Security Income (SSI).
The primary source of continuing income assistance available to low-income families with children is AFDC. Through AFDC, eligible families receive monthly cash payments and access to Medicaid benefits. The federal government pays a portion of the administrative expenses and benefit costs, but the states administer the AFDC program and set payment standards. Although it is not targeted to low-income families with disabled children, the AFDC program represents a major potential source of cash and medical assistance to these families.
Established by 1972 amendments to the Social Security Act, the federal Supplemental Security Income (SSI) program provides monthly cash benefits to individuals who are aged, blind, or disabled. In most states, the program also provides access to Medicaid benefits. Although the SSI program is primarily directed to adults, children who meet the income and disability requirements can receive SSI benefits.
The SSI program, and particularly its benefits for children, has become the target of extensive public and political concern in recent years. Two concerns have been paramount in the public debate: program growth and equity in benefits between the SSI and AFDC programs.
The dramatic recent growth in the number of children receiving SSI benefits has done the most to push the program to the forefront in policy debates. In December 1974, shortly after it was first implemented, the program provided benefits to 70,849 children, who made up 2 percent of total SSI beneficiaries. By December 1993, SSI provided benefits to 770,501 children--13 percent of total beneficiaries and more than twice the number of children receiving benefits in 1989 (Social Security Administration 1993). Since April 1992, SSI has paid more in federal benefits to disabled children than it has paid to aged beneficiaries, with this difference growing each year (Smeeding 1994).
The sources of this growth are multiple. A period of dramatic growth followed the Supreme Court's 1990 decision in Sullivan v. Zebley, which modified eligibility determination procedures to allow a functional, individual assessment of children's disabilities. Other factors may have also contributed to program growth. These include an increase in the numbers of disabled children in the underlying population, the impact of the Zebley decision in calling attention to a more comprehensive definition of disability for children, and SSI outreach activities undertaken since 1989 in response to Congressional mandates (U.S. General Accounting Office 1995). There is also anecdotal evidence that the declining benefits available through the AFDC and local general assistance programs have created incentives, for families and for state and local welfare workers, to qualify children for the relatively more generous SSI program (Committee on Childhood Disability 1995).
The growth in the SSI program for children has fueled debate about equity in the treatment of economically disadvantaged families eligible for the AFDC or SSI programs. Low-income families with disabled children have two potential sources of cash assistance: AFDC and SSI. A single individual may not receive benefits from both programs, but a family with a disabled child can combine benefits from both. The disabled child can receive SSI benefits while the rest of the household receives AFDC (U.S. House of Representatives 1993). If a child is eligible for either AFDC or SSI benefits, the child's family is frequently better off if the child receives SSI benefits and the rest of the household receives AFDC.2 For example, in 1993 a child eligible for the full federal SSI benefit would have received $434 per month. In most states, this amount was significantly greater than the marginal increase in AFDC benefits that would have resulted from including the child in the AFDC family unit. In the median state, the maximum monthly AFDC benefit in 1993 increased by $96 when family size increased from one to two and by $57 when family size increased from two to three. In California, a high benefit state, the monthly increases in benefits were $197 and $120 respectively (U.S. House of Representatives 1993).3
The basis for this difference in cash aid is now under considerable scrutiny. The legislative history of Public Law 92-603, which created the SSI program, suggests that Congress enacted this benefit structure because it accepted the argument that the needs of low-income families with disabled children were greater than the needs of other low-income families. Benefits for children were added to the SSI program in a political compromise. The House Ways and Means Committee initially added these benefits, explaining that disabled children living in low-income households were among the most disadvantaged of Americans, that they had greater needs than other children, and that, therefore, they were deserving of special help.4 The Senate at first rejected this view, but benefits for children were ultimately accepted in a House-Senate conference.5 These needs may include direct expenditures for transportation to distant hospitals or sources of medical care, extra laundry, babysitting, special child care, and respite care, home modifications, and other medical expenses not paid by public or private insurance (see Consortium for Children with Disabilities 1994; Hippolitus 1985; Stein and Jessop 1985). Families with disabled children may also suffer economically through the loss of employment income resulting from the need to take care of the disabled child (Hobbs, Perrin and Ireys 1985; Lansky et al. 1979).
Do Families with Disabled Children Incur Special Costs?
Information about the additional costs faced by families with disabled children is central to policy decisions for AFDC and SSI. A small literature on the out-of-pocket expenses associated with care of a disabled child suggests that some fraction of families with special needs children do incur direct costs caring for these children. For some, these costs are quite high. However, both the probability of any expenses and the average expenditures have been found to vary substantially.
Analyzing data from the 1980 Medical Care Utilization and Expenditure Study, Newacheck and McManus (1988) report that disabled children on average used more medical and health care services and incurred higher health care expenditures than non-disabled children. They also found that families with disabled children experienced uncovered, out-of-pocket expenses substantially higher than those of families with no disabled children. Out-of-pocket expenditures, like medical expenditures in general, were low or non-existent for many disabled children but very high for a minority. Out-of-pocket expenses were lower for low-income disabled children, reflecting perhaps the more comprehensive coverage provided by Medicaid (Newacheck and McManus 1988) and/or budget constraints in these families.
Jacobs and McDermott (1989) reviewed six studies of the costs associated with caring for children with specific diseases or disabling conditions. Looking at home costs, travel costs, and equipment costs, these studies reported average annual expenditures ranging from $334 for children with cystic fibrosis to $4,012 for children with cancer. Urban Systems Research and Engineering (1979) investigated extra expenditures incurred by families with SSI children and found that SSI families averaged $27.69 per month ($332.28 annually) in out-of-pocket expenses related to the child's disability in 1978. The most commonly reported categories of additional costs were transportation, clothes, and medical care items and services not covered by Medicaid. Again, these costs were not evenly distributed across families; some families experienced no costs while others experienced substantial costs.
Disabilities, Welfare "Dependence" and Work
Benefit differentials between the SSI and AFDC programs may also be justified on the basis of the indirect costs and economic impact, in reduced employment and earnings, associated with the care of disabled children. Reductions in work to care for children, if widespread, also have important implications for the AFDC program. Since the mid-1980s, the focus of welfare reforms has shifted decisively toward the reduction of welfare dependence and increased work tests for recipients. Welfare policies aimed at reducing "dependence" on public assistance are complicated by the fact that parents who are the policy targets have both caretaking and economic responsibilities for their children. Welfare policies that limit aid and impose rigorous work requirements raise even more complicated issues in the case of families who care for disabled children and may face heightened caretaking demands associated with their children's special needs.
A number of analysts have examined the dynamics of welfare use, the heterogeneity of households participating in various welfare programs, and individual and family factors that predict the duration of welfare receipt and probability of earnings exits (Bane and Ellwood 1983; Plotnick 1983; O'Neill, Bassi and Wolf 1987; Blank 1986a, 1989; Blank and Ruggles 1993; Gottschalk and Moffitt 1994; Hoynes and MaCurdy 1994). Other researchers have explored the prevalence of work and of work-related exits from welfare (Pavetti 1992; Harris 1992; Spalter- Roth et al. 1992).
This body of research suggests that both welfare receipt and work attachment are volatile for low-income parents. A majority of welfare recipients leave welfare for work, or combine welfare with work during some portion of their spells on welfare. Spells of work, like welfare, are often short, however. And several individual and family characteristics are consistent predictors of longer spells on AFDC and lower prospects for work-related exits: younger, less-educated women, women with more children, those eligible for higher AFDC benefits and those facing higher unemployment rates are the most at risk. None of these studies have specifically examined or considered families with severely disabled children.
Blank (1989b) has also shown that, among female-headed households with children, the health status of the head affects AFDC participation. A woman who reports limits on physical activity is more likely to participate in an AFDC program. Spalter-Roth et al. (1992) and others have documented lower labor force participation among AFDC recipients with disabilities and poor health, and among those with more children.
Research on the impact of disabled children on parents' work effort is less complete. A few small surveys of families with severely disabled children suggest that parents of these children report both additional time spent in care giving and lost employment income as a result of their children' disabilities. Leonard et al. (1992) report that primary care givers spent from 0 to 20 hours per day caring for severely disabled children, with a median of 4 hours and 42 minutes. They found that caregiving time varied positively with out-of-pocket expenses and negatively with the caregiver's hours worked. In a study of children receiving cancer treatment, Lansky et al. (1979) found that 16 of 32 families reported lost wages due to the child's condition, with a median loss of $68.94 in weekly income.
Studies using larger, nationally representatives samples have not always demonstrated that additional caretaking burdens result in lower labor force participation among women. In related research on the effect of caring for an elderly parent, a number of these studies show that such caretaking responsibilities cause no reduction in hours worked or employment (Wolf and Soldo 1994; Couch et al. 1995; but see Ettner 1995). Researchers examining care for disabled children have also reached ambiguous conclusions. Using data from the 1972 National Health Interview Study, Salkever (1982) found that a disabled child had a significantly negative effect on women's labor force participation only among white, two-parent families. In a 1995 study, Wolfe and Hill examined labor force participation among a sample of single mothers from the 1984 panel of the SIPP. They looked at the impact of a variety of health-related factors on the mother's decision whether or not to work. Two of their models found that the presence of a disabled child significantly reduced the probability of employment.6
In one of the few studies to directly examine the relationship between children's disabilities and work and welfare receipt, Acs, and Loprest (1994) use data from the 1990 SIPP to estimate the impact of children's disabilities on parents' probability of exiting welfare by any means, exiting welfare through work, or combining work with welfare. They find that "compared to women with healthy children, women with disabled children are more likely to exit AFDC within a year, more likely to work while on welfare and less likely to leave AFDC through work." None of these results is statistically significant, however. In a second model, Acs and Loprest look at each of three age-related categories of functional limitation. They report a patchwork of results with only one statistically significant finding: women whose children are limited in their school work are more likely to be employed while on welfare than women with healthy children.
RESEARCH QUESTIONS
Public assistance for families with disabled children has come under scrutiny in the larger political debate about welfare reform. Current proposals suggest reforms for SSI which range from virtual elimination of cash benefits for children to protection of the entitlement for both cash assistance and health insurance. Proposals for reforming AFDC consistently call for reductions in benefits and imposition of more stringent time limits and work tests. These reforms have significant implications for low-income families who care for children with chronic health problems and disabilities. National incidence studies suggest that these conditions are more common in poor families. High levels of disability have also been noted among parents in the AFDC program.
Unfortunately, the additional knowledge that would be needed for careful scrutiny of these proposals is both incomplete and dated. Estimates of the prevalence and severity of childhood disabilities and illnesses vary widely depending on the analyst, definitions, and data source. Estimates of the economic impact of children's special needs on families is even more problematic. Information about the additional costs faced by families with disabled children is critical. While we know that some families incur costs, the direct out-of-pocket costs associated with childhood disabilities appear to vary widely across types of disabilities and types of families affected, and the best studies for measuring these costs are now more than 15 years old. We also lack good estimates of the impact of caring for children on families' earnings: the indirect costs of foregone earnings if parents stay home to care for their special needs children and the direct costs of substitute child care if parents go to work outside the home.
In this paper we raise some of the questions which arise at the intersection of these welfare, disability, and poverty issues. We then present preliminary findings from a recent survey of current and recent AFDC recipients in California, and we use these data to address three sets of questions.
-
First what is the prevalence of chronic health conditions and disabilities among families in the AFDC program? How many families participate in the AFDC and SSI programs?
-
Second, how do families with affected children fare in comparison to other AFDC families? How does receipt of SSI affect families' economic well-being?
-
Finally, what are the direct costs (in out-of-pocket expenditures) and indirect costs (through reductions in labor market activity) associated with the care of children with health conditions and disabilities? How do these affect poverty status?
METHODS
Data
This paper analyzes preliminary data from Wave II of the (California) AFDC Household Survey. This is one of several databases constructed through the joint effort of the Department of Social Services of the State of California and the University of California Data Archive and Technical Assistance program. Respondents for the AFDC Household Survey were selected from the California Assistance Payment Demonstration Project (APDP) sample. The APDP sample is a stratified random sample of 15,000 AFDC recipient households selected from four California counties (Los Angeles, Alameda, San Joaquin, and San Bernardino) in November 1992.7 The sample included both single-parent households and two-parent households qualifying for benefits through the AFDC-UP program.8 Two-parent households were deliberately oversampled to increase the number of such cases available for analysis.
The data analyzed here are preliminary data from Wave II of a telephone survey of a subsample of 2,250 English and Spanish speaking households randomly selected from the APDP sample to receive telephone interviews.9 The AFDC Household Survey is a panel survey. Initial (Wave I) interviews began in October 1993; a follow-up interview was fielded, beginning in late spring 1995. In both waves, the adult female caretaker for AFDC child(ren) was asked detailed questions about family and household composition, parents' labor market activities, household income, and use of social services. Wave II of the survey also includes a set of questions to identify families with chronically ill or disabled children. These data are designed to allow researchers to assess the type and severity of the child's disabilities, to measure expenses associated with the child's condition, to identify children participating in the SSI program, and to examine the impact of the child's condition on a parent's labor market participation and the family's financial well-being.
In this paper we present data from the first 1,320 Wave II interviews completed as of December 1995.10 These interviews are still in progress, so the findings presented here are preliminary and subject to change after data collection is completed. Data are weighted in this analysis to adjust for differences in sampling fractions by strata and for survey completion rates.
Sample Limitations
Several important limitations in the generalizability of this sample should be noted. The sample for this study was designed to represent the AFDC population in four counties in California. While we believe this generalizes well to the welfare population in that state, it may not represent families in the AFDC system elsewhere in the country. Because important groups were not included in this round of surveys, notably recent immigrants, caution must be used even in drawing conclusions about California. The sample has another important limitation. As a point in time sample, it "samples the flow" of all welfare cases. These findings may represent the experiences of families who were receiving welfare at a point in time. As substantial research in this field has demonstrated, however, their experience will not represent all families who ever enter the welfare system. In particular, we would expect this point in time sample to represent the experiences of long-term, more highly disadvantaged welfare recipients (who dominate AFDC caseloads at a point in time), and to underrepresent the larger number of short-term, relatively more advantaged families who cycle through the welfare system more quickly.
It is also important to note that this sample represents the experience of only a fraction of SSI recipient families. Although the SSI program, like AFDC, is means-tested, its income tests and benefit reduction rates are considerably more generous. The sample of families represented here, those poor enough to qualify for both AFDC and SSI, are thus a small and especially disadvantaged subset of all families who receive SSI for disabled children.
Analysis
The first stage of analysis reported below is descriptive. Of the 1,320 cases available for analysis, we exclude 53 families who were no longer caring for AFDC recipient children at the Wave II contact. For the remaining 1,267, we describe the frequency and severity of children's conditions, their participation in the SSI program, and the incidence of chronic illnesses and disabilities among adults and children on the household level. To answer the question of relative economic well-being, we compare household income, access to health insurance, and several measures of economic well-being across households assumed to have different "caretaking burden" associated with children's special needs: households with no special-needs children versus those with one or more than one such child, and households with no special-needs children versus those with moderately or severely impaired child(ren). Variable measures and definitions are described in detail in Appendix A.
We then turn our attention to two possible sources of economic disadvantage for families with special-needs children. We consider out-of-pocket expenditures relating to children's health or disabling conditions, first by category of expenditure and then in terms of their impact on family economic status.
The final step in the analysis examines reductions in labor force participation among women with special-needs children. We use logistic regression to estimate the impact of the number and severity of children's special needs, and the impact of the receipt of SSI, on a dichotomous measure of labor force participation (currently working at a regular job). Our model is the reduced form specification of the standard static labor supply model (Killingsworth 1983; Wolfe and Hill 1995). (We discuss our specification in more detail in Appendix B.) Coefficients can be interpreted as changes in the log-odds that mothers worked, given a one unit change in the predictor variable. Taking the natural anti-log of the coefficient allows a more intuitive interpretation as an estimate of the change in the odds of working relative to one (at the sample mean).
The presence of a special-needs child is expected to reduce mothers' odds of working through at least two routes: first, by imposing an additional caretaking burden, and second, by increasing transfer income through SSI. We use two separate models to estimate the caretaking burden associated with the related but distinct dimensions of the number of affected children and severity of need. Model one measures the caretaking burden associated with the number of affected children by including two dummy variables for the presence of (1) only one child or (2) two or more children with chronic illnesses or disabilities. Model two measures burden by the severity of the child(ren)'s condition, including two dummy variables for the presence of (1) only moderately impaired child(ren) or (2) at least one severely disabled child. In an effort to separate the impact of the caretaking burden from the income effect of SSI, we use nested hierarchical models to first estimate the probability of work without controlling for SSI receipt, and then to re-estimate each model adding a dummy variable for receipt of SSI by any family member other than the respondent. In each specification we control for respondent's demographic and human capital characteristics, and other family income. (See Appendix B for further discussion of the estimation issues and variables.)
RESULTS
Characteristics and Program Participation
Prevalence of Conditions. Chronic health problems and disabilities were frequent in this sample of AFDC recipient families: over 40 percent of households had either a disabled mother and/or at least one child with special needs.
As Figure 1 shows, 391 (31 percent) adult female caretakers reported that they had a physical or mental disability that limited their ability to work. Women in 267 households (21 percent) reported the presence of at least one child with a chronic health problem or disability. One hundred ninety-eight (16 percent) reported one special needs child in the household, and 69 (5 percent) reported more than one.
When adult disabilities and children's special needs are considered together, 43 percent of households were affected: 145 households (11 percent) had a nondisabled mother and at least one child with a special need, 269 (21 percent) were headed by a disabled mother with no disabled children, and 122 households (10 percent) had both a disabled caretaker and a child with a chronic health condition or disability.
The prevalence of any limiting conditions for children (21 percent of households) and adults (31 percent), is much higher in this sample than the recent estimates by Acs and Loprest (1994). Using 32 months of SIPP data, they report that 8 percent of households that received AFDC had a child with a limiting condition and 18 percent had a disabled mother. Differences in the estimates may reflect differences in sample construction (longitudinal SIPP data versus point-in-time California data) and differences in the definition of limiting conditions. These may represent upper and lower bound estimates of the true prevalence of serious limitations in AFDC households.
The category of the first disabling condition for all children identified with special needs11 is summarized in Table 1, which also compares the incidence in this sample to estimates from nationally representative samples of children. Asthma and other respiratory diseases were the most common chronic condition for children in AFDC recipient families, affecting 6 percent of children. Behavior and learning disorders together formed the next most common category, involving 2 percent of children. Approximately 1 percent of children were affected by other physical or health impairments (cancer, epilepsy, heart problems and cerebral palsy), and 1 percent had mental retardation or developmental delays (including autism). Other categories of impairment each involved 1 percent of children or less. (An additional 2 percent of children were identified as having special needs but their conditions were not coded at the time of this writing.)
Comparison of these figures with those from nationally representative surveys is difficult, given widely different categories, methodologies, and conditions. In comparison to the 1988 National Health Interview Survey (Newacheck and Taylor 1992), which collected data on chronic health conditions affecting children under age 18, asthma was reported slightly more often in this sampl6 of low-income families; visual and hearing impairments and other physical or health conditions were reported less frequently in the AFDC Household Survey. (The 1988 NHIS did not collect information on mental conditions.) In comparison to the 1992 Survey of Income and Program Participation (McNeil 1993), physical disabilities were more frequently reported in our sample and mental conditions were less frequently reported.12 A much greater proportion of our respondents reported asthma as a disabling condition, and a substantially smaller proportion reported behavior and learning disorders and speech impairments.
Severity of Conditions. Although disabilities and chronic illnesses were common, the majority were mild to moderate by our definition of severity. Children's conditions by the severity of impairment are profiled in Table 2. Overall, 44 percent of children's conditions were coded as "severe" because the child required substantial additional help with daily activities, the condition interfered substantially with the child's attendance at school, or the child received SSI Severe impairment was most common in visual and hearing impairments (67 percent), other physical or health conditions (66 percent), mental retardation (89 percent), and mental illness (53 percent). Another 44 percent of children were coded as moderately impaired because they required some additional help with daily activities, were limited in usual activities or mobility, attended special education, or missed some school due to the condition. The majority of behavior and learning disorders (52 percent) and respiratory diseases (54 percent) fell into the moderate category. A final 12 percent of children were coded as mildly impaired; they met the conditions of the initial screen for chronic illnesses and/or disabling conditions, but parents did not report additional functional impairments. The category most frequently coded as mildly disabling was speech problems (41 percent).
Considered on the household level, 134 (11 percent) of all families cared for at least one child with a severe disability or illness. Disabilities were also common among adult caretakers and significantly correlated with the presence of a special-needs child. Overall, 391 adult caretakers (31 percent) reported that they had a chronic condition that limited or precluded employment. As shown in Table 3, adult disabilities were significantly more common in households with one or more special needs children.
SSI Program Participation. Although chronic health problems and disabilities were common in this sample of disadvantaged families, participation in the SSI program was relatively uncommon. Overall, 87 families were receiving SSI for their children, representing 7 percent of all families and 24 percent of families with special-needs children. Even among children coded as severely impaired by our measures, less than half were current SSI recipients.
Children's participation in the SSI program is summarized in Table 2. SSI was received by more than half of children in only two categories of special needs: mental retardation and developmental delays (69 percent of children) and vision and hearing impairments (67 percent); 46 percent of children with other physical and health conditions were SSI recipients. SSI receipt was relatively rare for children with conditions which were less frequently coded as severely impairing: only 16 percent of those with asthma and 16 percent of those with speech impairments were SSI recipients. Although frequently meeting our criteria for severely impaired, only 23 percent of those with behavioral and learning disabilities, and 15 percent of those with a mental illness received SSI.13
Parent and Family Characteristics. As Table 3 shows, women with special-needs children differed significantly from the other women in our sample on some but not all demographic. The average respondent in the AFDC Household Survey was 35 years old, with less than a high school education and 2.17 children. Thirty-three percent (33 percent) of respondents were African American, 37 percent were Latino, and 25 percent were white/European American.14 One quarter of all women were currently living with a spouse or partner.
Differences between those with and without special-needs children were generally nonsignificant for respondents' age, age of first AFDC receipt, marital and cohabitation status. Women with special-needs children did differ significantly from women without such children with respect to their own health characteristics. As discussed above, women with special-needs children were more likely to rate their health as poor, and they were more likely to report that they personally had a disability watch limited or prevented work. The proportion reporting poor health or a disability was highest among those with more than one disabled child.
Women with disabled children also had on average more children; not surprisingly, parents with more than one disabled child also had more total children. The probability of having disabled children in the family differed significantly by race and ethnicity. African American families were more likely to have one or more special-needs children, and to have moderately or severely impaired children. Both Latino and European American families were under-represented in all categories of families with disabled children.
Economic Well-Being
Families with special-needs children were more likely to rely on welfare and appeared to fare worse than other families on several measures of material hardship. Participation in the SSI program helps explain higher incomes in some families. Even with relatively more generous SSI benefits, however, families with special-needs children did not move far from poverty, and they continue to report more hardship than families with healthy children.
Overall, the families in this sample were very poor. Average family income, including Food Stamps, was $1,125.11 in the prior month. This is $38.00 below the federal poverty line for a family of four. Table 4 compares average family incomes, standardized for family size, among families with and without special-needs children.15 Incomes differed for families with one or more children who had special needs, although differences never achieved statistical significance. Families with no disabled children and those with one special-needs child had similar incomes, after adjusting for family size; those with more than one special-needs child had less income per family member. Income differences were small and nonsignificant when families were compared by the severity of the child's condition.
Welfare Use. All families in this sample received AFDC for at least one child when the sample was drawn at the end of 1992. By the time of the Wave II contact in 1995, families were beginning to leave the AFDC system. Overall, 72 percent of families had received AFDC in the month prior to the interview and 69 percent had received Food Stamps.
Participation in means-tested welfare programs was significantly higher for those families caring for disabled and ill children, and participation increased with the number and severity of special needs. Eighty-three percent of families with one affected child, and 95 percent of those with two or more, were still receiving AFDC. The fraction of families in the AFDC system was slightly higher than the sample mean for those families with mild to moderately affected children (78 percent), and substantially higher for those with severely impaired children (93 percent). Trends were similar although less dramatic for receipt of Food Stamps.
Families caring for disabled and ill children were also more likely than other families to live in subsidized housing and to have Medi-Cal or Medicare coverage. While slightly less than one-quarter of all families lived in subsidized housing or received housing vouchers, from 35 to 39 percent of those with one or more than one disabled child, respectively, had housing assistance. The probability of receiving subsidies increased to 31 percent for those with moderately disabled children and 41 percent for those with any severely impaired children. Since enrollment in Medi-Cal (or in some instances, Medicare) is automatic for individuals in the AFDC and SSI programs, it was not surprising to find that health insurance coverage was much more common for both adults and children in families that included special-needs children.16 Overall, 70 percent of adults and 77 percent of children had public or private health insurance. If there was at least one disabled child in the house, 85 to 93 percent of children and 79 to 82 percent of adults were covered. If any children were severely impaired, coverage rates increased to 96 percent for children and 91 percent for adults.
Material Hardship. Regardless of welfare status, most of the families in this sample were poor, and indicators of economic hardship were common. Overall, nearly two-thirds had incomes at or below the poverty line; just over three-quarters were living at or below 125 percent of poverty.
Table 5 describes several measures of direct hardship. In 19 percent of all families children had gone hungry in the time since the Wave I interview, and in 25 percent adults had gone without food due to a lack of money. Depending on subsidy status, 5 to 7 percent of families had faced eviction, 18 to 21 percent had been late with their rent on two or more occasions, and 2 to 3 percent had at least one experience of homelessness. As noted earlier, many parents reported poor health. Health problems and use of emergency medical care were frequent among children also. Nearly one-third of families had taken a child to the emergency room, 6 percent had children hospitalized, and 8 percent reported that children went without needed medical care.17
In comparison to families with no disabled children, those with special-needs children fared even worse on these measures of hardship. The fraction of families reporting that children went hungry in prior months more than doubled for those with special-needs child(ren); reports of adults going hungry were 16 to 24 percentage points higher. There was some evidence that families with disabled children had more evictions, utility shutoffs, and homelessness, although differences here were inconsistent. Families with any special-needs children were also much more likely to report health problems and unmet health care needs among their children: two to four times as many reported at least one overnight hospitalization and three to four times as many reported that their child had gone without needed medical care. On most indicators, material hardship increased with the number of special-needs children in the family and with the severity of the child(ren)'s chronic health problem or disability.
Special Expenses
Measures of economic well-being suggest a paradox: families with special-needs children appear to do no worse than other families in terms of income and access to health insurance. By direct measures of hardship, however, they fare worse than other families. One source of economic hardship for families with special-needs children not taken into account in measuring poverty status may be the direct cost of caring for these children such as special diets and clothing, medical and other equipment, medications, therapies, and transportation to special services. We would expect that these costs, if not covered by health insurance or other forms of assistance, place a particular burden on low-income families.
In fact, a recent National Research Council (NRC) study (Citro and Michael 1995) on measuring poverty recommends that out-of-pocket health care expenses be taken into account by subtracting them from income when determining poverty status. The NRC did not, however, go so far as to recommend that other health-related expenses be taken into account. We estimate that health care costs are only half of the extra costs of caring for a disabled child.
Table 6 shows the frequency and amount of out-of-pocket expenses reported by families with special-needs children. About half of families with one or more special-needs child(ren) reported out-of-pocket expenses associated with a child's disability or illness in the month preceding the interview. Expenses ranged from $6.00 to $665.00, with an average of $130.98 across those families who incurred any costs.18 As would be expected, families with more than one disabled child reported higher expenditures (an average of $155), as did families with a severely disabled child or children (averaging $163) (Table 7).
SSI receipt did not increase the probability that families would report out-of-pocket costs, but it did increase the dollar amount of these expenditures (Table 7A). Among families with one special-needs child, 47 percent of those without SSI and 43 percent of those with SSI reported costs; for families with more than one such child, about 65 percent reported expenditures. Average monthly expenditures, for families who reported costs were $26 higher for those who received SSI for one special-needs child ($139) than for those who did not, and $248 higher for those with more than one special-needs child, at least one of whom received SSI (from $74 to $322).
Across all families with disabled or chronically ill children, the most common category of expense was unreimbursed medical care and medications, for which 26 percent of families incurred expenses averaging $43.19 (among those with any expenses; see Table 6). Other frequently reported expenses were for special child care arrangements (20 percent) and special food (16 percent).
These results are consistent with the results of earlier studies by Urban Systems Research and Engineering, Inc. (1979) and Newacheck and McManus (1988). They suggest that a substantial proportion of families with disabled children incur disability-related expenses in any given month, and for some families these expenses are very high. Given the constrained economic circumstances of the families in this sample, out-of-pocket expenditures might be most usefully understood in relation to family resources. For those with any costs, the extra expenses related to caring for special needs children consumed 10 to 12 percent of total family income (cash and Food Stamps) for families with one and more than one involved child, respectively.
Table 8, Figure 2 and Figure 3 suggest the impact of those expenses on family poverty, by comparing poverty rates for families with special-needs children, adjusted for the out-of-pocket expenses directly associated with their children's conditions. For families with mild to moderately involved child, the fraction of families living at or below the poverty line increased from 67 percent to 69 percent after expenses were considered; for families with severely involved child(ren), an additional 15 percent of families had incomes at or below poverty line when direct expenditures for children's special needs were considered (from 44 percent to 59 percent).
The impact of out-of-pocket expenses seemed most dramatic for the poorest families. About one-quarter of families with healthy children lived at or below 75 percent of the poverty line. When expenditures were considered, the fraction of families with moderately involved children living in extreme poverty increased from 29 percent to 43 percent; the fraction of those with severely involved children who were this poor rose from 18 percent to 29 percent.
The extent to which these expenses were offset by SSI, particularly for the poorest families, is also notable (see Table 8A). In families with only healthy children, 66 percent were living at or below the poverty line. Among those with special needs children and no SSI, 68 percent to 88 percent were living at or below poverty after expenditures were considered (depending on the number of involved children). For those did receive SSI for their disabled children, in contrast, only 36 percent of those with one involved child and 57 percent of those with two or more were at or below poverty after adjusting for expenditures. Again, the impact was particularly evident among the poorest families: the percentage of families with special needs children who were extremely poor (living below 75 percent of the poverty line) dropped from between 47 percent and 66 percent, among those without SSI, to less than 30 percent among those whose children were SSI recipients.
As would be expected for a means-tested program, the effect of SSI receipt was modest for relatively better off families. Even with SSI, families did not move far from poverty and economic insecurity. Once expenditures were considered, 78 percent to 90 percent of families without SSI, and 77 percent to 83 percent of those in the SSI program, still had incomes at or below 125 percent of poverty.
Labor Force Participation
Parents' labor force activities and earnings are a second important factor in families' economic well-being that may be affected by children's special needs. Bivariate comparisons of labor force participation (Table 9) suggest that the presence of children with special needs considerably depressed parents' labor force activity, particularly among mothers.
Employment. The proportion of women holding a regular job and the proportion who worked at all in the previous month were significantly and substantially related to the number of disabled children in the family. Thirty-one percent of all mothers were working in a regular job when contacted, and 34 percent reported some paid work in the prior month. In contrast, only 26 percent of mothers reporting one child with a health problem or disability, and 4 percent of those with two or more affected children, were currently working in a regular job. Labor force participation also declined along with the severity of children's special needs: 27 percent of those whose children were mildly to moderately limited were working, but only 14 percent of those whose child(ren) had severe impairments were in the labor force. Trends were similar although less pronounced for spouses and partners of those respondents who were currently cohabitating. Overall, 60 percent of men had regular jobs at the Wave II interview. Employment declined slightly for those in families with one (58 percent) and substantially with more than one (39 percent) special-needs child; employment was also lower among men in families with moderately (58 percent) and severely (45 percent) involved children.
Reduced labor market activities translated in much smaller contributions of earnings to family income. Twenty-seven percent of income in all families came from the earnings of the respondent (mother) or her spouse or partner. In families with special needs children, earnings accounted for 7 to 20 percent of income (depending on the number of children). In families with one or more severely limited children, only 9 percent of family income came from adults' earnings.
Murtivariate Analysis. The reduction in parents' labor force activities may be directly related to the extra burden of caring for children with special needs and to problems relating to the availability and cost of special needs child care. The reduction may also result wholly or in part from other individual or family factors. Mothers who report having special needs children may differ in other ways that reduce their propensity to work--for example, they may have lower human capital or poorer health themselves. We would also predict a reduction in paid labor, regardless of caretaking burden, in response to the income effect of additional transfer income through the SSI program, which is available only to those families with disabilities.
Table 11 reports the results of multivariate analyses of mothers' employment as a function of her human capital and family characteristics, transfer income, and the special needs of her children. (Means and standard deviations are provided in Table 10). We use nested logistic regressions to estimate the total impact of having special-needs children in the family (models 1a and 2a), and the marginal impact of the caretaking burden after controlling for the effect of SSI (models 1b and 2b). Models are described more fully in Appendix B.
In all specifications, mothers' human capital characteristics were significant in expected directions. The odds of paid employment increased significantly with years of education. Mothers who reported their health as poor and those with children under the age of six were significantly less likely to be in paid employment. Latina women were significantly more likely to be working (with European Americans as excluded category). AFDC benefit rules favoring work had a significant positive impact in all four estimations. Other controls for household composition, marital status, and race were nonsignificant.
In the first step of the nested models, measures of caretaking burden were significant in expected directions. Before controlling for SSI receipt (model 1a), the odds of working were reduced by approximately one-third (OR=.644, p.07) for mothers with one special-needs child, and by more than 90 percent for women with more than one child with special needs (OR=.096, p.01). When a dummy for receipt of SSI by anyone in the family other than the mother was added in model 1b, the coefficient was large in the expected direction (negative) but nonsignificant. After controlling for the income effect of SSI, the dummy for having more than one special needs child continued to predict a nearly 90 percent reduction in the odds of working (OR=.111, P.01). The coefficient for having only one such child remained negative, but was much smaller in magnitude and statistically nonsignificant in this specification.
Similar although less robust results were observed in the second set of models, which measured caretaking burden in terms of the severity of the child's disability. When estimated without controlling for SSI (model 2a), the coefficient for the presence of a moderately limited child or children was negative but nonsignificant. The presence of one or more severely involved children significantly reduced the odds of working by about two-thirds (OR=.357, p.05). When the dummy for SSI was added in model 2b, it was large but nonsignificant and the explanatory power of the disability variables was reduced.19 The presence of a severely impaired child was seen to reduce the odds of working by about half (OR=.446, p.08). The coefficient for the presence of a moderately impaired child or children was both smaller in magnitude and nonsignificant.
These findings suggest that the presence of chronically ill and disabled children has a significant negative impact on mothers' labor force participation, even after controlling for differences in women's human capital characteristics, household configuration, and other income. The number of children with special needs and the severity of those needs were significant in explaining reductions in work, SSI receipt also had the expected negative impact on mothers' labor force participation, although the measure was not statistically significant. Because the receipt of SSI is contingent on the presence and severity of family members' disabilities (children or partners), the SSI variable may also pick up a portion of the reduction in labor force participation related to the extra care of a chronically ill or disabled child. These estimations thus provide upper and lower bound estimates of the true impact of the caretaking burden associated with special-needs children on women's participation in any regular job. It should also be noted that these are estimates of the most dramatic impact of special-needs children on mothers' paid employment More limited adjustments--in the form of reductions in the hours of regular work among those who were employed or intermittent absences from work due to children's needs--are not reflected in this measure.
CONCLUSIONS
Data from this survey of current and recent AFDC recipients in California suggest four initial conclusions about chronic illness and disabilities in this population and their impact on families' economic well-being.
First, in this sample of highly disadvantaged families, chronic health conditions and disabilities were common. Just over 20 percent of households reported caring for at least one child with special needs. When conditions affecting mothers and children were considered, over 43 percent of households were found to have a child with special needs, to be headed by a disabled mother, or both. Since this sample can be expected to overrepresent longer term AFDC recipients, this may represent an upper bound estimate of special needs among welfare participants.
Chronic conditions were defined broadly in this survey, and the special needs of children and associated caretaking burdens for parents can be expected to vary substantially even among families with affected children. Two categories stood out in our analyses: 5 percent of families were caring for more than one child with chronic difficulties, and nearly 11 percent of families had at least one child who met our criteria for a severe disability that substantially interfered with the child's regular activities.
Health and disabling conditions affected a substantial fraction of children in this sample; many fewer participated in the SSI program. Barely 7 percent of all children, and about one quarter of those with identified disabilities or chronic illnesses, were receiving SSI. This suggests that a considerable proportion of potential SSI recipients are not yet enrolled in the program and raises the possibility of additional demand for program benefits.
The second notable finding is that families with special-needs children were much more likely to rely on public welfare and appeared to fare worse than other families on several measures of material hardship, despite having similar per capita family incomes and better access to health insurance. Overall, the families in this sample were quite poor, with average incomes (including transfers and in-kind benefits) that did not reach the poverty line for a family of four. Economic hardship was frequent, in the form of hunger, housing problems, and limited access to health care. Families with special-needs children were more likely to report hardship on these measures, and hardship increased with the number of affected children and with the severity of children's impairments.
These findings suggest something of a paradox: families with special-needs children had about the same income, on average, as other families. But these same families seemed to be doing worse on direct measures of well-being. Our third major finding concerns the possible source of this hardship in actual expenses incurred caring for disabled children and reductions in earnings associated with their care.
Half of families reported out-of-pocket expenditures in the prior month for the care of chronically ill and disabled children. Most commonly, they paid for medical care and medications that were not covered by insurance; other frequently reported expenses included special child care arrangements and special food and diets. Among families who did incur special costs, expenditures averaged $132 overall, and $155 to $163 for those with more than one ill or impaired child or any severely impaired children. Because this sample was restricted to current and recent AFDC recipients, and the survey questions probed for the marginal, extra expenses associated specifically with the child's special needs, we consider these figures to be conservative measures of the costs of caring for ill and disabled children. Even as a lower-bound estimate, $132 or more may represent a substantial financial burden for low-income families.
The magnitude of burden is seen in the impact of these expenses on poverty status. Out-of-pocket expenses for special-needs children increased the fraction of families with income at or below the poverty line as much as 15 percentage points, depending on the number of children and severity of their needs. The impact of expenses was particularly evident among the poorest families. About one-quarter of families with healthy children were living at or below 75 percent of the poverty line. Twenty-nine to 43 percent of families with special needs children were this poor once the extra costs of caring for a special needs child were considered.
Mothers in families with special-needs children were also less likely to be working. When background and income factors were controlled, the presence of special-needs children was associated with a 36 percent to 90 percent reduction in the odds that mothers worked (depending on the number of affected children); the presence of severely involved children depressed the odds of work by 64 percent. The receipt of SSI appeared to explain part of this reduction in work effort. But mothers with multiple special-needs children, and those caring for severely impaired children, continued to have a 55 percent to 90 percent reduction in the odds of regular employment even after the income effect of SSI was controlled. This estimation captures the most dramatic impact on labor force participation. The 15 percent to 27 percent of mothers with special-needs children who did hold regular jobs may also have reduced the hours they worked in response to the special needs of their children.
A fourth conclusion to be drawn from these analyses is that SSI appears to be reasonably well targeted and moderately effective in reducing poverty for families with disabled children. Less than one-quarter of children with any identified disabilities or chronic illnesses were receiving SSI, and receipt was highest among children with conditions that appeared most disabling. When family incomes were adjusted to reflect out-of-pocket costs of caring for special-needs children, the fares who received SSI for their children were much less likely to be poor and extremely poor than similar families who did not receive SSI. Although SSI reduced poverty for a portion of these families, the impact was still modest and concentrated on the poorest families. Three-quarters of families with .SSI still had incomes at or below 125 percent of poverty.
DISCUSSION AND POLICY IMPLICATIONS
The conclusions from this study provide some insight on issues in welfare, SSI and disability policy. Some important limitations must be noted. As noted earlier, this sample can be strictly generalized only to four counties in California. Even more importantly, it represents a particularly disadvantaged subset of families in the AFDC and SSI programs. Because it is a point-in-time sample of AFDC cases, it can be expected to overrepresent long-term and more highly disadvantaged welfare recipients. And because families must be quite poor to qualify for AFDC, the families in this sample who also receive SSI for their special needs children represent the most highly disadvantaged families in the SSI program more generally.
These point-in-time data also cannot isolate the causal relationships connecting disabilities and economic hardship. In some cases, children's illnesses and disabilities probably represent an exogenous shock to families' economic well-being. The financial costs and caretaking burdens associated with children's conditions may compromise the economic well-being of families already struggling at the margins of economic stability.
A second possibility is that children's impairments have a more complex, multidirectional association with poverty. The prevalence of illnesses and disabilities in this sample of current and recent AFDC recipient households suggests that these conditions are not entirely exogenous to families' economic situation. Children growing up in poor families may be at greater risk for contracting illnesses associated with environmental conditions (e.g., asthma and cancer), for incurring disabilities associated with poor health care and health behaviors (e.g., low birth weights and Fetal Alcohol Syndrome), and for developmental disabilities associated with early life experiences. The presence of special needs children may thus be both cause and consequence of economic hardship.
A third and related possibility is that our indicators of children's special needs reflect underlying problems in families which are expressed in both poor economic status and poor health and developmental outcomes for children. The consistently worse status of families with more than one involved child, and those with both a disabled mother and one or more special needs children, might signal the interaction of health, functional, economic and social problems.
With these cautions in mind, we would offer the following comments on current policy issues which arise at the intersection of the AFDC and SSI programs.
First, extra assistance appears warranted for at least some of the families who care for children with special needs. On average, these families were doing worse than others on several direct measures of economic well-being. Many were incurring expenses associated specifically with their children's illnesses and disabilities. There was evidence that mothers were also less likely to work and thereby contribute earnings to the family.
The SSI program appears to have a modestly beneficial anti-poverty impact for families with disabled children. Families with disabled children who received SSI had higher incomes and were less likely to have incomes below the poverty line. This assistance benefited this group of families in relation to other poor families in our sample, particularly the poorest families. It was rarely a windfall, however; even with SSI benefits, the large majority of families were still hovering near the poverty line. And families with special-needs children continued to report high levels of direct economic hardship.
This study also supports efforts to target SSI assistance. Although chronic health problems and disabilities affected a substantial fraction of all families, the impact was consistently more dramatic for the smaller subset of families who faced more substantial caretaking demands. In this study, we measured these demands rather crudely by comparing families with more affected children and those with more severely impaired children. Even using this rough proxy of need, these families fared the worst on indicators of hardship, had the highest out-of-pocket expenses, and showed the most dramatic reductions in work.
A final policy concern, in both the SSI and AFDC programs, is that of "dependency" or long- term reliance on welfare assistance. The reduction in labor force participation among mothers in this sample suggests that participation in welfare programs may indeed be long-term for many families caring for children with special needs. It is not at all clear, however, from this or other research, that this reflects welfare dependence. To the extent that mothers in these families cope with additional caretaking responsibilities which make them less available for outside employment, it may be unrealistic to expect rapid transitions from welfare to self-sufficiency. There is no evidence in these data that there were strong incentives for families to choose continued welfare receipt over work, or that participation in the AFDC and SSI programs was financially rewarding for these families. They continue to be poor, and to experience more hardship than other families. Policies which indiscriminately reduce or eliminate assistance, without careful regard for the direct and indirect costs of caring for ill and disabled children, are likely to fail to have the intended impact on self-sufficiency and may greatly exacerbate hardship for an especially disadvantaged group of children.
REFERENCES
Acs, G. and P. Loprest. 1994. Do Disabilities Inhibit Exits from AFDC? Washington, DC: The Urban Institute.
Aday, L.A. 1992. "Health Insurance and Utilization of Medical Care for Chronically III Children with Special Needs: Health of Our Nation's Children, United States, 1988," Advance Data from Vital and Health Statistics, No. 215. Hyattsville, MD: National Center for Health Statistics.
Adler, M. n.d. Disability among Women on AFDC: An Issue Revisited. Washington, DC: Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. [http://aspe.hhs.gov/daltcp/reports/afdcwomn.htm]
Bane, M.J. and D. Ellwood. 1986. "Slipping Into and Out of Poverty: The Dynamics of Spells," Journal of Human Resources, 21:1-23.
Bane, M.J. and D. Ellwood (eds.). 1994. Welfare Realities. Cambridge, MA: Harvard University Press.
Blank, R.M. 1989a. "Analyzing the Length of Welfare Spells," Journal of Public Economics, 39:245-73.
____. 1989b. "The Effect of Medical Need and Medicaid on AFDC Participation," The Journal of Human Resources, XXIV: 54-87.
Blank, R.M. and P. Ruggles. 1993. "When Do Women Use AFDC and Food Stamps? The Dynamics of Eligibility vs. Participation," Working Paper No. 93-16. Northwestern University: Center for Urban Affairs and Policy Research.
Buhmann, B., L. Rainwater, G. Schmaus, and T.M. Smeeding. 1988. "Equivalence Scales, Well-Being, Inequality, and Poverty: Sensitivity Estimates across Ten Countries Using the Luxembourg Income Study (LIS) Database," Review of Income and Wealth, 34:11542.
Burke, V.J. 1974. Nixon's Good Deed: Welfare Reform. New York: Columbia University Press.
Citro, C. and R. Michael (eds.). 1995. Measuring Poverty: A New Approach. Washington, DC: National Academy of Science Press.
Committee on Childhood Disability. 1995. Restructuring the SSI Disability Program for Children and Adolescents. Washington, DC: National Academy of Social Insurance.
Consortium for Citizens with Disabilities. 1994. May 31, 1994, Memorandum Re: Children's SSI Program. Washington, DC: Bazelon Center for Mental Health.
Couch, K., M.C. Daly, and D. Wolf. 1995. "Time? Money" Both" Modeling the Decision to Care for an Elderly Parent." Paper prepared for the 1995 Population Association Meetings, March 1995.
Ellwood, M.R. and B. Burwell. 1990. "Access to Medicaid and Medicare by the Low-Income Disabled," Health Care Financing Review, 1990 Annual Supplement: 133-48.
Enberg, J., P. Gottschalk, and D. Wolf 1990. "A Random-Effects Logit Model of Work-Welfare Transitions," Journal of Econometrics, 43:63-75.
Ettner, S.L. 1995. "The Impact of 'Parent Care' on Female Labor Supply Decisions," Demography, 32:63-80.
Gottschalk, P. and R.A. Moffitt. 1994. "Welfare Dependence: Concepts, Measures, and Trends," The American Economic Review, 84(2):38-42.
Harris, K.M. 1992. "Work and Welfare among Single Mothers in Poverty." Paper presented at the APPAM Annual Research Conference, October 29, 1992 in Denver, CO.
Hippolitus, P. 1985. "Employment Opportunities and Services for Youth with Chronic Illness." In N. Hobbs and J. Perrin (eds.). Issues in the Care of Children with Chronic Illnesses. San Francisco: Jossey-Bass Publishers.
Hobbs, N., J. Perrin, and H. Ireys. 1985. Chronically Ill Children and Their Families. San Francisco: Jossey-Bass; Publishers.
Hoynes, H. and T. MaCurdy. 1994. "Has the Decline in Benefits Shortened Welfare Spells?" The American Economic Review, 84(2):43-48.
Jacobs, P. and S. McDermott. 1989. "Family Caregiver Costs of Chronically Ill and Handicapped Children: Method and Literature Review," Public Health Reports, 104:158-163.
Killingsworth, M.R. 1983. Labor Supply. Cambridge: Cambridge University Press.
Lansky, S., N. Cairns, G. Clark, J. Lowman, L. Miller, and R. Trueworthy. 1979. "Childhood Cancer: Nonmedical Costs of the Illness," Cancer, 43:403-408.
Leonard, B., J.D. Brust, and J.J. Sapienza. 1992. "Financial and Time Costs to Parents of Severely Disabled Children," Public Health Reports, 107:302-312.
Manski, C.F. and S.R. Lerman. 1977. "The Estimation of Choice Probabilities from Choice Based Samples," Econometrica, 45:1977-1988.
McNeil, J.M. 1993. "Americans with Disabilities, 1991-92," Current Population Reports, No. P70-33. Washington, DC: U.S. Bureau of the Census.
Newacheck, P. 1988. "Testimony before the Senate Finance Committee U.S. Congress," Children's Health Care Issues: Hearings before the Senate Committee on Finance. Washington, DC: U.S. Government Printing Office.
Newacheck, P. and M. McManus. 1988. "Financing Health Care for Disabled Children," Pediatrics, 81:385-94.
Newacheck, P. and W.R. Taylor. 1992. "Childhood Chronic Illness: Prevalence, Severity, and Impact," American Journal of Public Health, 82:364-71.
O'Neill, J.A., L.J. Bassi, and D.A. Wolf. 1987. "The Duration of Welfare Spells," The Review of Economics and Statistics, 69:241-248.
O'Neill, J.A., D.A. Wolf, L.J. Bassi, and M.T. Hannan. 1984. An Analysis of Time on Welfare. Washington, DC: The Urban Institute.
Pavetti, L.A. 1992. "The Dynamics of Welfare and Work: Exploring the Process by Which Young Women Work Their Way Off Welfare." Paper presented at the APPAM Annual Research Conference, October 29, 1992, Denver.
Plotnick, R. 1983. "Turnover in the AFDC Population: An Event History Analysis," The Journal of Human Resources, XVIII(1):65-8 1.
Salkever, D.S. 1982. "Children's Health Problems and Maternal Work Status," Journal of Human Resources, 17:94-109.
Smeeding, T.M. 1994. "Improving Supplemental Security Income." In R. Friedland., L. Etheredge, and B. Vladeck (eds.). Social Welfare Policy at the Crossroads. Washington, DC: National Academy of Social Insurance.
Social Security Administration. 1993. Children Receiving SSI. Baltimore, MD: Social Security Administration.
Spalter-Roth, R.M., H.I. Hartmann, and L. Andrews. 1992. Combining Work and Welfare: An Alternative Anti-Poverty Strategy. Washington, DC: Institute for Women's Policy Research.
Stein, R. and D. Jessop. 1985. "Delivery of Care to Inner-City Children with Chronic Conditions." In N. Hobbs and J. Perrin (eds.), Issues in the Care of Children with Chronic Illnesses. San Francisco: Jossey-Bass Publishers.
U.S. General Accounting Office. 1995. Supplemental Security Income: Growth and Changes in Recipient Population Call for Re-examining Program. Washington, DC: United States General Accounting Office.
U.S. House of Representatives, Committee on Ways and Means. 1993. Overview of Entitlement Programs. Washington, DC: U.S. Government Printing Office.
Urban Systems Research and Engineering, Inc. 1979. Survey of Blind and Disabled Children Receiving Supplemental Security Income Benefits. Baltimore, MD: Social Security Administration.
Weishaupt., R. and R. Rains. 1991. "Sullivan v. Zebley: New Disability Standards for Indigent Children to Obtain Government Benefits," Saint Louis University Law Journal, 35:539-96.
Wolf, D.A. and B.J. Soldo. 1994. Married Women's Allocation of Time to Employment and Care of Elderly Parents," The Journal of Human Resources, XXIX:1259-76.
Wolfe, B. and S. Hill. 1995. "The Effect of Health on the Work Effort of Single Mothers," The Journal of Human Resources, 30:42-62.
Woodward, B. and B. Weiser. 1994. "Costs Soar for Children's Disability Program," The Washington Post, February 4,1994, pp.A1.
| TABLE 1. Child's Disability or Chronic Condition, California Families Receiving AFDC in November 1992(2,133 children, weighted) | |||||||
| n | AFDC Household Survey | 1991-92 SIPPa | 1988 NHISb | ||||
| Percent of Disabled Children | Percent of All Children | Percent of Disabled Children | Percent of All Children | Percent of Disabled Children | Percent of All Children | ||
| PHYSICAL (non-mental) | 200 | 54.9 | 6.8 | 27.9 | na | ||
| Asthma | 167 | 45.9 | 5.7 | 2.0 | na | 13.7 | 4.2 |
| Vision, Hearing Impairments | 11 | 3.1 | 0.4 | 5.4 | na | 9.1 | 2.8 |
| Other Physical/Health Impairmentsc | 21 | 5.9 | 0.7 | 15.5 | na | 6.5d | 2.0 |
| MENTAL DISORDERS | 105 | 28.9 | 3.6 | 56.7 | na | ||
| Behavior/Learning Disorderse | 58 | 16.0 | 2.0 | 29.5 | na | na | na |
| Mental Retardation/ Developmental Delay | 24 | 6.6 | 0.8 | 7.8 | na | na | na |
| Mental/Emotional Illness | 19 | 5.1 | 0.6 | 6.3 | na | na | na |
| Speech Impairment | 5 | 1.3 | 0.2 | 13.1 | na | 8.5 | 2.6 |
| ALL CODED | 305 | 83.8 | 10.4 | na | |||
| NOT YET CODED | 59 | 16.2 | 2.0 | na | |||
| OTHER | na | 13.4 | na | ||||
| TOTAL | 364 | 100.0 | 12.4 | 100.0 | na | na | 30.7 |
| |||||||
| TABLE 2. Child's Disability by Severity and Supplemental Security Income Receipt: California Families Receiving Aid for Dependent Children in November 1992(2,133 children, weighted) | |||||||||||
| n | By Severity | By Supplemental Security Receipt | |||||||||
| Mild | Moderate | Severe | Yes | No | |||||||
| n | Percenta | n | Percenta | n | Percenta | n | Percenta | n | Percenta | ||
| PHYSICAL (non-mental) | 200 | 22 | 11.0 | 91 | 48.8 | 80 | 40.2 | 43 | 21.8 | 156 | 78.2 |
| Asthma | 167 | 18 | 10.8 | 90 | 54.1 | 59 | 35.1 | 26 | 15.6 | 141 | 84.4 |
| Vision, Hearing Impairments | 11 | 1 | 4.6 | 3 | 28.5 | 8 | 66.9 | 8 | 66.9 | 4 | 33.1 |
| Other Physical/Health Impairmentsb | 21 | 3 | 15.6 | 4 | 18.5 | 14 | 66.0 | 10 | 46.1 | 12 | 53.9 |
| MENTAL DISORDERS | 105 | 9 | 8.3 | 42 | 39.6 | 55 | 52.1 | 30 | 30.0 | 70 | 70.1 |
| Behavior/Learning Disordersc | 58 | 5 | 8.3 | 30 | 52.2 | 23 | 39.5 | 13 | 23.2 | 45 | 76.8 |
| Mental Retardation/ Developmental Delay | 24 | 0 | 0.0 | 3 | 11.5 | 21 | 88.6 | 13 | 69.5 | 6 | 30.5 |
| Mental/Emotional Illness | 19 | 2 | 11.3 | 7 | 35.6 | 10 | 53.1 | 3 | 15.4 | 16 | 84.6 |
| Speech Impairment | 5 | 2 | 40.7 | 2 | 43.5 | 1 | 15.8 | 1 | 15.8 | 4 | 84.2 |
| ALL CODED | 305 | 31 | 10.1 | 139 | 45.6 | 135 | 44.3 | 74 | 24.5 | 226 | 75.5 |
| NOT YET CODED | 59 | 12 | 19.7 | 22 | 36.8 | 26 | 43.5 | 13 | 22.5 | 46 | 77.6 |
| TOTAL | 364 | 42 | 11.6 | 161 | 44.2 | 161 | 44.2 | 87 | 24.2 | 271 | 75.8 |
SOURCE: California AFDC Household Survey, Wave II
| |||||||||||
| TABLE 3. Adult Caretaker and Family Characteristics by Presence and Severity of Child Disabilities: California Families Receiving AFDC in November 1992(1,320 weighted cases) | |||||||
| Sample Meana | All Families by Number of Disabled Children | All Families by Severity of Child(ren)'s Disability | |||||
| None | One | Greater Than 1 | None | Mild to Moderate | Severe | ||
| TOTAL FAMILIES | 1320 | n=1004 | n=198 | n=69 | n=1004 | n=133 | n=134 |
| Education (years) | 11.3 | 11.2 | 11.5 | 11.7 | 11.2 | 11.6 | 11.5 |
| Age (years) | 34.9 | 34.3 | 34.4 | 36.2 | 34.3 | 34.7 | 35.0 |
| Age First AFDC (years) | 24.9 | 24.9 | 24.1 | 23.3 | 24.9* | 24.9* | 22.8* |
| Currently Married (percent) | 18.0 | 18.3 | 14.1 | 21.1 | 18.3 | 19.7 | 12.1 |
| Living with Partner (percent) | 24.4 | 25.7 | 23.2 | 25.2 | 25.7 | 27.9 | 19.6 |
| Age Youngest Child (years) | 6.1 | 6.0 | 6.5 | 5.5 | 6.0 | 6.7 | 5.9 |
| Number of Children (number) | 2.2 | 2.2* | 2.3* | 3.1* | 2.2* | 2.4* | 2.6* |
| Disability Limits Work (percent) | 19.3 | 16.5* | 18.9* | 45.0* | 16.5* | 26.2* | 25.2* |
| Disability Prevents Work (percent) | 11.0 | 8.3* | 14.6* | 27.4* | 8.3* | 25.2* | 18.4* |
| Poor Health (percent) | 12.6 | 10.2* | 17.3* | 26.1* | 10.2* | 19.2* | 19.9* |
| African American (percent) | 33.3 | 29.1* | 47.5* | 52.8* | 29.1* | 44.6* | 53.1* |
| Latino (percent) | 36.8 | 40.2* | 25.7* | 31.2* | 40.2* | 29.0* | 25.2* |
| European American (percent) | 25.4 | 26.3* | 22.0* | 9.5* | 26.3* | 19.5* | 18.2* |
SOURCE: California AFDC Household Survey, Wave II. * p 0.05.
| |||||||
| TABLE 4. Family Income and Welfare Use by Presence and Severity of Child Disabilities: California Families Receiving AFDC in November 1992(1,320 weighted cases) | |||||||
| Sample Mean | All Families by Number of Disabled Children | All Families by Severity of Child(ren)'s Disability | |||||
| None | One | Greater Than 1 | None | Mild to Moderate | Severe | ||
| TOTAL FAMILIES | 1320 | n=1004 | n=198 | n=69 | n=1004 | n=133 | n=134 |
| INCOME | |||||||
| Family income for prior month (dollars) | 1,225.11 | 1,227.86 | 1,226.69 | 1,273.98 | 1,227.86 | 1,228.41 | 1,249.45 |
| Standardized for family sizeb (dollars) | 682.89 | 677.55 | 675.20 | 622.99 | 677.55 | 650.76 | 672.27 |
| Family income as percent of poverty (percent) | 110.5 | 110.0 | 108.0 | 97.6 | 110.0 | 104.2 | 119.8 |
| WELFARE USE | |||||||
| Received AFDC this month (percent) | 71.7 | 70.7* | 82.7* | 94.6* | 70.7* | 78.3* | 93.2* |
| Received Food Stamps prior month (percent) | 69.2 | 69.5* | 73.5* | 86.0* | 69.5* | 69.7* | 83.6* |
| Subsidized housing (percent) | 23.4 | 20.3* | 34.8* | 38.7* | 20.3* | 30.9* | 40.7* |
| Health insurance (adult) (percent) | 70.5 | 69.3* | 81.6* | 78.6* | 69.3* | 70.3* | 91.3* |
| Health insurance (child)c (percent) | 77.3 | 74.8* | 84.5* | 92.9* | 74.8* | 77.3* | 96.0* |
SOURCE: California AFDC Household Survey, Wave II. * p 0.05.
| |||||||
| TABLE 5. Family Hardship by Presence and Severity of Child Disabilities: California Families Receiving AFDC in November 1992(1,320 weighted cases) (in percent) | |||||||
| Sample Meana | All Families by Number of Disabled Children | All Families by Severity of Child(ren)'s Disability | |||||
| None | One | Greater Than 1 | None | Mild to Moderate | Severe | ||
| TOTAL FAMILIES | 1320 | n=1004 | n=198 | n=69 | n=1004 | n=133 | n=134 |
| HUNGER | |||||||
| Child went hungry (since Wave I) | 18.8 | 14.9* | 29.9* | 44.2* | 14.9* | 33.0* | 34.3* |
| Adults went hungry (since Wave I) | 25.0 | 19.9* | 36.6* | 54.0* | 19.9* | 39.0* | 43.2* |
| HOUSING ADEQUACYb | |||||||
| Subsidized | |||||||
| Eviction (since Wave I) | 5.0 | 4.4 | 8.1 | 2.3 | 4.4* | 13.5* | 1.2* |
| Utility shut off (since Wave I)c | 18.4 | 18.1 | 15.9 | 26.7 | 18.1 | 11.1 | 25.1 |
| Late rent (since Wave I) | 17.5 | 16.8 | 14.2 | 36.3 | 16.7 | 25.0 | 16.5 |
| Homeless (since Wave I) | 3.3 | 1.1* | 9.4* | 4.9* | 1.1* | 3.7* | 11.6* |
| Not Subsidized | |||||||
| Eviction (since Wave I) | 7.4 | 6.5* | 11.1* | 15.6* | 6.5* | 14.7* | 9.3* |
| Utility shut off (since Wave I)c | 14.8 | 13.3 | 17.7 | 26.9 | 13.3 | 15.8 | 23.9 |
| Late rent (since Wave I) | 20.8 | 21.2 | 16.8 | 22.0 | 21.2 | 15.5 | 21.1 |
| Homeless (since Wave I) | 2.0 | 1.8 | 4.0 | 0.3 | 1.8* | 5.3* | 0.5* |
| HEALTH AND HEALTH CARE | |||||||
| Randomly Selected Child | |||||||
| Any overnight hospitalizations (since Wave I) | 5.8 | 3.4* | 16.8* | 7.9* | 3.4* | 8.9* | 20.0* |
| Used emergency room (since Wave I) | 32.3 | 27.6* | 51.1* | 46.7* | 27.6* | 44.4* | 55.4* |
| Went without medical care (since Wave I) | 8.1 | 5.5* | 16.6* | 20.7* | 5.5* | 17.1* | 18.2* |
SOURCE: California AFDC Household Survey, Wave II. * p 0.05.
| |||||||
| TABLE 6. Out-of-Pocket Expenses in Prior Month for Special Needs of Disabled Children, Families with One or More Disabled Children: California Families Receiving AFDC in November 1992(267 weighted cases) | ||
| Percent with Any Expenses | Mean Expenditure(in dollars) | |
| Food | 15.8 | 78.05 |
| Clothing | 9.8 | 79.44 |
| Transportation | 8.8 | 73.09 |
| Child Care | 19.6 | 80.97 |
| Medical Care/Medicine | 26.1 | 43.19 |
| Other | 10.0 | 61.19 |
| Any Expenses | 49.8 | 130.98 |
| SOURCE: California AFDC Household Survey, Wave II. | ||
| TABLE 7. Out-of-Pocket Expenses in Prior Month for Special Needs of Disabled Child(ren) by Presence and Severity of Child's Disabilities: California Families Receiving AFDC in November 1992(265 weighted cases) | |||
| Percent with Any Expenses | Mean Total Expenses(dollars) | ||
| Of All Families with Disabled Children | Of Families Who Incurred Costsa | ||
| SAMPLE MEANb | |||
| ALL FAMILIES BY NUMBER OF DISABLED CHILDREN | |||
| None | na | na | na |
| One | 44.2 | 52.93 | 119.75 |
| Greater than one | 65.7 | 101.97 | 155.23 |
| ALL FAMILIES BY SEVERITY OF CHILD(REN)'S DISABILITY | |||
| None | na | na | na |
| Mild to Moderate | 49.1 | 48.79 | 99.42 |
| Severe | 50.5 | 65.53 | 163.39 |
SOURCE: California AFDC Household Survey, Wave II.
| |||
| TABLE 7A. Out-of-Pocket Expenses in Prior Month for Special Needs of Disabled Child(ren) by Supplemental Security Income Participation: California Families Receiving AFDC in November 1992(1,320 weighted cases) | |||
| Percent with Any Expenses | Mean Total Expenses(dollars) | ||
| Of All Families with Disabled Children | Of Families Who Incurred Costsa | ||
| SAMPLE MEANb | 49.3 | 65.69 | 130.98 |
| ALL FAMILIES WITH DISABLED CHILD(REN) BY NUMBER OF DISABLED CHILDREN AND SSI RECEIPT | |||
| One disabled child with SSI | 46.6 | 64.56 | 138.52 |
| One disabled child without SSI | 43.4 | 48.86 | 112.68 |
| More than one disabled child with SSI | 64.9 | 208.88 | 321.65 |
| More than one disabled child without SSI | 66.1 | 48.77 | 73.83 |
SOURCE: California AFDC Household Survey, Wave II.
| |||
| TABLE 8. Poverty Status with Adjustments of Out-of-Pocket Expenditures for Special Needs(1,320 weighted cases) (in percents) | ||||||||
| Sample Mean | All Families by Number of Disabled Children | All Families by Severity of Child(ren)'s Disability | ||||||
| None | One | Greater than one | None | Mild to Moderate | Severe | |||
| TOTAL FAMILIES | 1,320 | n=1004 | n=198 | n=69 | n=1,004 | n=133 | n=134 | |
| PERCENTAGE OF POVERTY LINE | ||||||||
| Less than 76 percent | All Income | 26.3 | 28 | 23 | 31 | 27 | 29 | 18 |
| Adjusted | 29.3 | 28 | 36 | 55 | 27 | 43 | 29 | |
| 76 to 100 percent | All Income | 37.2 | 38 | 31 | 35 | 39 | 37 | 26 |
| Adjusted | 36.3 | 38 | 23 | 23 | 39 | 26 | 30 | |
| 101 to 125 percent | All Income | 1.9 | 12 | 22 | 15 | 11 | 13 | 32 |
| Adjusted | 12.8 | 12 | 21 | 8 | 11 | 11 | 23 | |
| 126 to 150 percent | All Income | 8.0 | 7 | 13 | 7 | 7 | 6 | 16 |
| Adjusted | 7.6 | 7 | 11 | 3 | 7 | 8 | 12 | |
| Greater than 150 percent | All Income | 14.6 | 15 | 11 | 12 | 15 | 15 | 8 |
| Adjusted | 13.9 | 15 | 9 | 11 | 15 | 11 | 6 | |
| SOURCE: California AFDC Household Survey, Wave II. | ||||||||
| TABLE 8A. Poverty Status with Adjustments for Out-of-Pocket Expenditures for Special-Needs Families at Different Poverty Levels(1,320 weighted cases) (in percents) | |||||
| Percent of Poverty Line | Families with Disabled Children by Number and Supplemental Security Receipt | ||||
| One Disabled | Greater Than One Disabled | ||||
| SSI (yes) | SSI (no) | SSI (yes) | SSI (no) | ||
| Less than 76 percent | All Income | 5 | 32 | 0 | 45 |
| Adjusted | 5 | 47 | 29 | 66 | |
| 76 to 100 percent | All Income | 16 | 35 | 24 | 40 |
| Adjusted | 31 | 21 | 28 | 22 | |
| 101 to 125 percent | All Income | 54 | 11 | 36 | 5 |
| Adjusted | 47 | 11 | 19 | 2 | |
| 126 to 150 percent | All Income | 20 | 9 | 22 | 1 |
| Adjusted | 13 | 10 | 6 | 2 | |
| Greater than 150 percent | All Income | 5 | 13 | 18 | 9 |
| Adjusted | 4 | 11 | 17 | 8 | |
| SOURCE: California AFDC Household Survey, Wave II. | |||||
| TABLE 9. Labor Market Participation by Presence and Severity of Child Disabilities: California Families Receiving AFDC in November 1992(1,320 weighted cases) (in percents) | |||||||
| Sample Mean | All Families by Number of Disabled Children | All Families by Severity of Child(ren)'s Disability | |||||
| None | One | Greater than one | None | Mild to Moderate | Severe | ||
| TOTAL FAMILIES | 1,320 | n=1,004 | n=198 | n=69 | n=1,004 | n=133 | n=134 |
| Respondents with a regular jobb | 31.0 | 33.9 | 26.4 | 3.5 | 33.9 | 26.6 | 14.4 |
| Respondents worked at least one hourc | 33.6 | 35.9 | 29.9 | 7.1 | 35.9 | 32.4 | 15.7 |
| Partner with a regular job now | 60.2 | 61.7 | 57.8 | 39.0 | 61.7 | 58.3 | 45.1 |
| Partner worked at least one hour | 64.6 | 64.9 | 66.5 | 40.9 | 64.8 | 63.6 | 56.7 |
| Income from earnings | 27.0 | 29.0 | 20.2 | 7.0 | 29.0 | 24.5 | 9.0 |
SOURCE: California AFDC Household Survey, Wave II.
| |||||||
| TABLE 10. Variables in Logit Regression Means and Standard Deviations(1,116 weighted cases) | ||
| Variable | Mean | Standard Deviation |
| Years Education | 11.75 | 1.83 |
| Mother's Health Poor (percent) | 0.10 | 0.31 |
| Any Child Less than Age 6 (percent) | 0.53 | 0.50 |
| Mother's Age (years) | 33.64 | 8.92 |
| Mother's Age Squared | 1,210.91 | 702.42 |
| African-American (percent) | 0.31 | 0.46 |
| Latino (percent) | 0.27 | 0.44 |
| Never Married (percent) | 0.37 | 0.48 |
| Partner/Spouse Present (percent) | 0.34 | 0.48 |
| Number Other Adults | 0.43 | 0.86 |
| Other Income (dollars) | 356.09 | 712.26 |
| Number AFDC Eligible Children | 2.28 | 1.24 |
| Experimental Subject (percent) | 0.63 | 0.48 |
| Unemployment Rate (percent) | 0.08 | 0.10 |
| One Special Needs Child (percent) | 0.19 | 0.39 |
| More than One Special Needs Child (percent) | 0.06 | 0.23 |
| Child(ren) Moderately Impaired (percent) | 0.11 | 0.31 |
| Child(ren) Severely Impaired (percent) | 0.70 | 0.32 |
| SSI Receipt (percent) | 0.07 | 0.26 |
| TABLE 11. Logistic Regression Results Coefficients(1,116 weighted cases) | ||||||||
| Variable | Model 1a | Model 1b | Model 2a | Model 2b | ||||
| Coefficient | Standard Error | Coefficient | Standard Error | Coefficient | Standard Error | Coefficient | Standard Error | |
| Constant | -5.54 | 1.72 | -5.47 | 1.71 | -5.59 | 1.70 | -5.58 | 1.70 |
| Years Education | 0.32 | 0.07* | 0.31* | 0.07* | 0.31* | 0.07* | 0.31* | 0.07* |
| Mother's Health Poor | -0.76* | 0.40* | -0.75* | 0.40* | -0.84* | 0.40* | -0.82* | 0.39* |
| Any Children Less than Age 6 | -0.80* | 0.24* | -0.77* | 0.24* | -0.79* | 0.24* | -0.77* | 0.24* |
| Mother's Age | 0.09 | 0.07 | 0.09 | 0.07 | 0.09 | 0.07 | 0.09 | 0.07 |
| Mother's Age Squared | -0.001** | 0.00** | -0.001** | 0.00** | -0.001** | 0.00** | -0.001** | 0.00** |
| African American | -0.09 | 0.24 | -0.08 | 0.24 | -0.10 | 0.24 | -0.09 | 0.24 |
| Latino | 0.50* | 0.25* | 0.50* | 0.25* | 0.49* | 0.25* | 0.49* | 0.25* |
| Never Married | -0.04 | 0.24* | -0.04 | 0.24 | -0.05 | 0.24 | -0.04 | 0.24 |
| Partner/Spouse Present | 0.11 | 0.26 | 0.12 | 0.26 | 0.06 | 0.26 | 0.08 | 0.26 |
| Number of Other Adults | -0.01 | 0.11 | -0.01 | 0.11 | -0.03 | 0.11 | -0.02 | 0.11 |
| Other Income | -0.01** | 0.00** | -0.01** | 0.00** | -0.01** | 0.00** | -0.01** | 0.00** |
| Number of AFDC Eligible Children | -0.09 | 0.10 | -0.09 | 0.10 | -0.11 | 0.10 | -0.11 | 0.11 |
| Experimental Subject | 0.37* | 0.15* | 0.38* | 0.21* | 0.38* | 0.20* | 0.39* | 0.20* |
| Unemployment Rate | 0.01 | 0.08 | 0.01 | 0.08 | 0.02 | 0.08 | 0.02 | 0.08 |
| One Special Needs Child | -0.44** | 0.29** | -0.29 | 0.22 | - | - | - | - |
| More than One Special-Needs Child | -2.34* | 0.62* | -2.20* | 0.63* | - | - | - | - |
| Child(ren) Moderately Impaired | - | - | - | - | -0.38 | 0.33 | 0.38 | 0.33 |
| Child(ren) Severely Impaired | - | - | - | - | -1.03* | 0.46* | -0.81** | 0.55** |
| SSI Receipt | - | - | -0.75 | 0.66 | - | - | -0.48 | 0.75 |
| * p.05. ** p.10. | ||||||||
| FIGURE 1. Chronic Health Conditions and Disabilities: California Families Receiving AFDC in 1993(n=1267) |
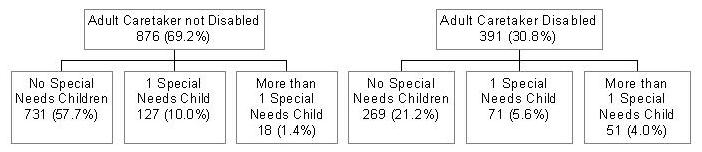 |
| FIGURE 2. Poverty Levels by Number of Disabled Children: Impact of Out of Pocket Expenditures on Poverty Levels |
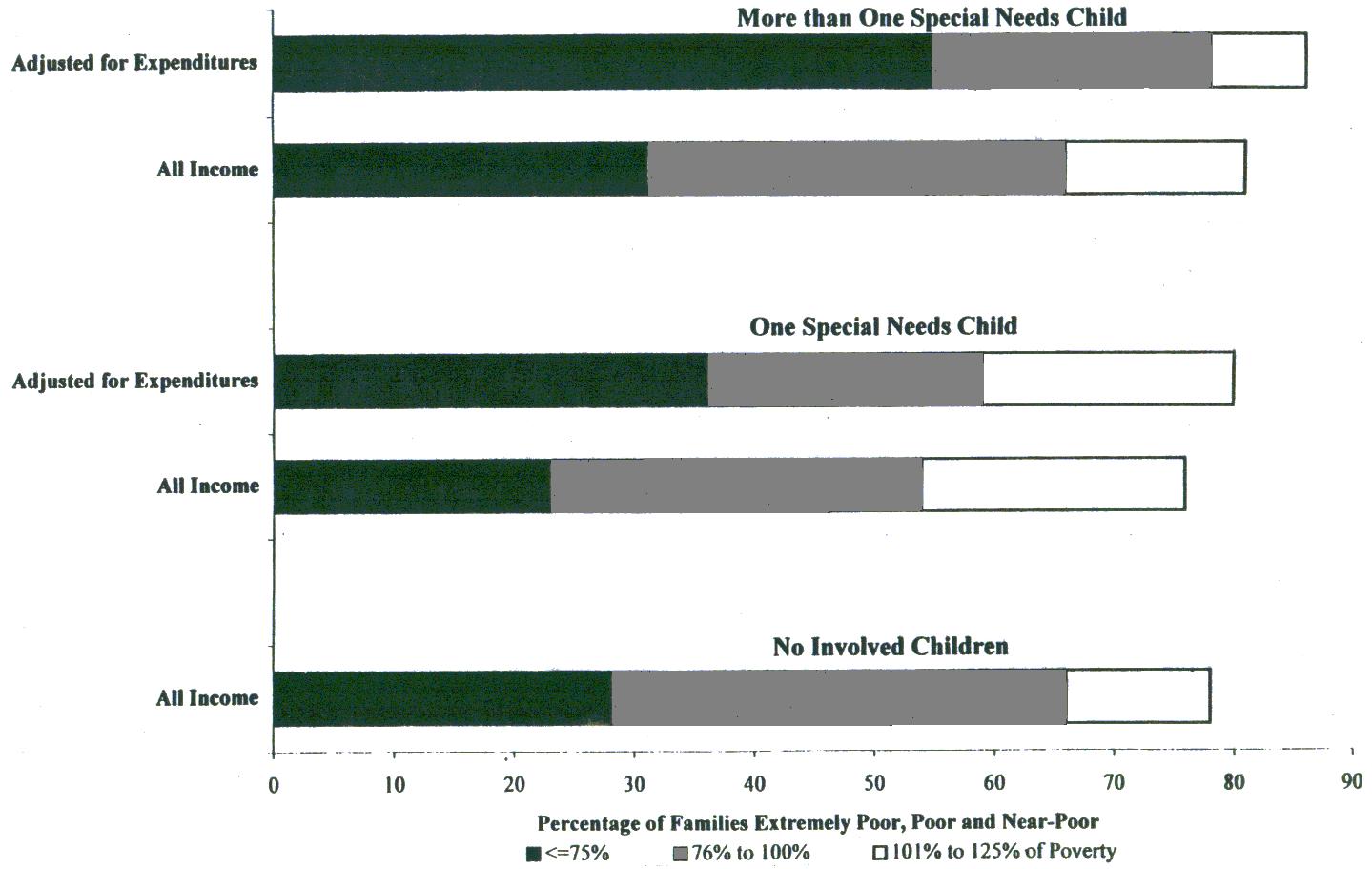 |
| FIGURE 3. Poverty Levels by Number of Disabled Children and SSI Receipt: Income Adjusted for Expenditures |
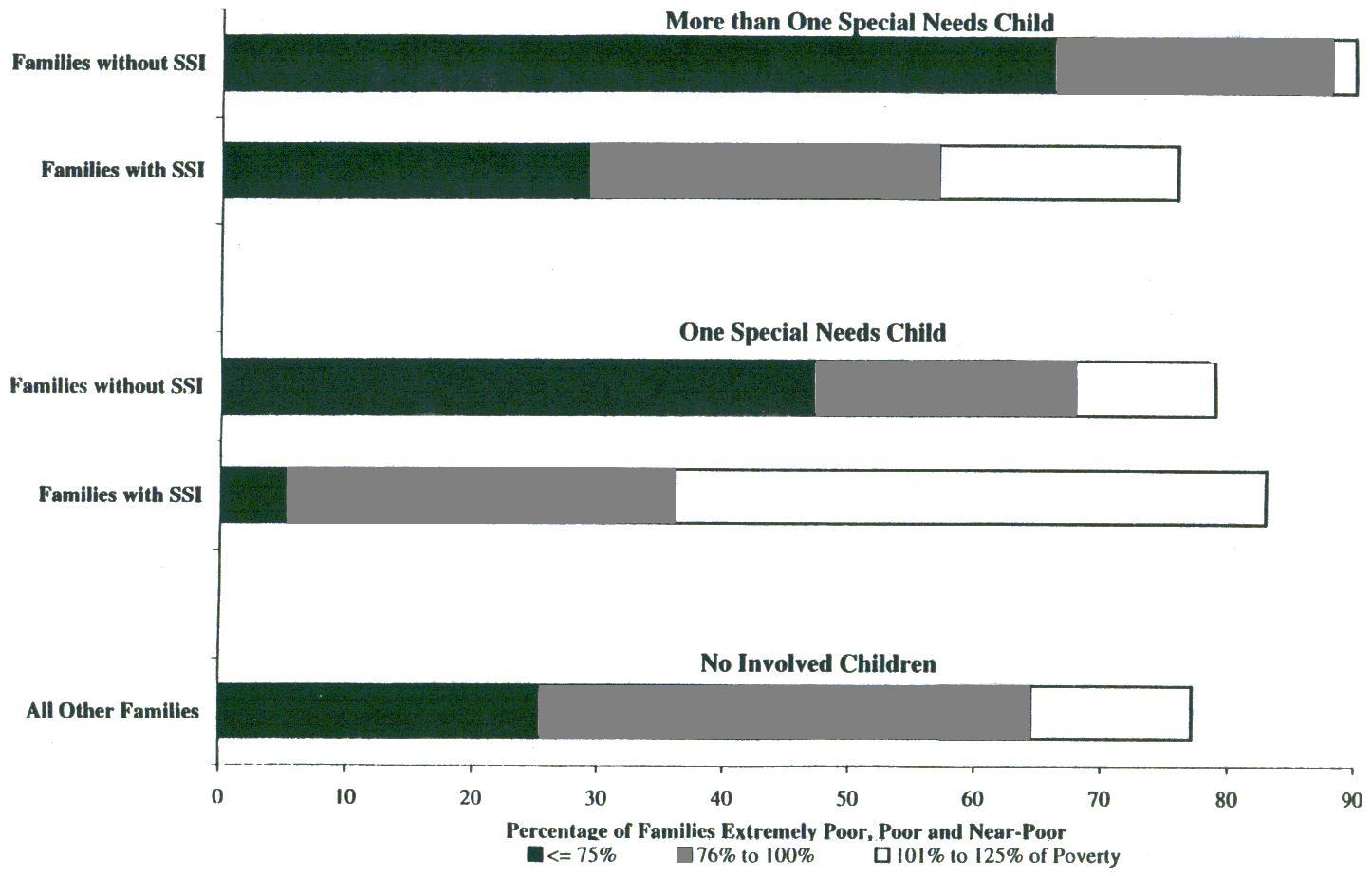 |
APPENDIX A: MEASURES OF VARIABLES
Chronic Health Conditions and Disabilities
Wave II of the AFDC Household survey included questions designed both to identify children with chronic health conditions and disabilities, and to measure the caretaking burdens which these conditions might have imposed on adults. We defined children's special needs broadly, to identify chronic health impairments, physical and mental disabilities. We considered "caretaking burden" along two related dimensions: the number of children in the family with chronic problems, and the severity of those problems.
Children with chronic health problems and disabilities were identified by asking respondents whether any of their children.20 (1) had a chronic health problem--physical, emotional, or mental--that limited the amount or kinds of things that he or she could do; (2) had a disability or handicapping condition that limited the amount or kind of things he or she could do; or (3) received SSI benefits. We identified a household as including a child or children with chronic conditions if the respondent answered yes to any of these three screening questions. Thus, we screened broadly to include activity-limiting chronic illnesses, and emotional, mental, and physical conditions which could produce a moderate to severe functional limitation.
For each child identified as having a chronic illness or disabling condition, respondents were asked to identify up to two specific conditions (diagnoses) causing the child's impairments. To measure the extent of limitation, and associated caretaking burden, respondents were also asked a series of questions regarding functional limitations and use of special health and educational services. These questions were based on questions in the 1992 National Health Interview Survey, the topical module on children's disability designed for the Survey of Income and Program Participation, and a 1978 survey of households with SSI children undertaken by Urban Systems Research and Engineering Inc. Appendix Table A1 summarizes our categorization of the severity of children's conditions as mild, moderate, or severe, based on functional limitations.
Economic Well-Being
Family income was measured for the prior month. Family was defined to include the respondent, her resident spouse or partner, and children for whom she had economic responsibility: resident biological children, step children, or children for whom she received AFDC. Income included earnings (respondent's pre-tax earnings and respondent's spouse or partner's pre-tax earnings), public cash transfers (AFDC payments, unemployment insurance payments, SSI benefits), private cash transfers (child support payments, money from friends, relatives or other sources), and in-kind public transfers (food stamps). The same total family income can produce very different standards of living depending on family size due to intra-family transfers and economies of scale (see Buhmann et al. 1988). Because we were interested in income as a measure of comparative well-being across family groups, we standardized income for family size by dividing total monthly income by the square root of family size (see Buhmann et al. 1988).
The survey also probed for direct indicators of economic well-being. Respondents were asked whether there had been times (since Wave I interview) when children had not gotten enough to eat or when the respondent (and her spouse or partner) had not gotten enough to eat. With respect to housing, respondents were asked if they had been late with rent or mortgage payments more than twice, or had experienced an eviction, a utility shut-off, or a period of homelessness, since their Wave I interview. The survey also collected information about health, health insurance, and use of medical care for the respondent and one randomly selected child in each family. Respondents were asked whether adults and child(ren) were currently covered through private or public health insurance (Medicaid or Medicare). They were also asked a series of questions about use of medical care (by adults and children) in the period since the first interview: whether they had sought care in an emergency room, spent one or more nights in the hospital, or gone without needed care entirely.
Disability-Related Expenditures
To measure the direct financial impact of caring for children with special needs, the survey included a series of questions about out-of-pocket expenditures for the additional or special needs of child(ren) with chronic problems. Questions were adapted primarily from Urban Systems Research and Engineering, Inc.'s 1978 survey of households with SSI children. We were particularly interested in expenditures which were not covered by health insurance or public programs.
Respondents were asked whether they had experienced direct out-of-pocket expenses related directly to their children's special needs in the month preceding the interview and, if they had experienced costs, the amount. We measured costs by summing expenditures reported for special clothes or shoes, special transportation, health care, and medicine not covered by Medicaid or insurance, special child-care or babysitting, and any other special expenses.21
It should be noted did measurement in this area is problematic for several reasons. Survey respondents may not be able to remember or accurately report all expenditures. This is particularly true in surveys such as this which ask for only a portion of expenditures, and probe for the marginal additional expenditures which are related to children's special needs. For this low-income sample, measurement may be compromised further by families' financial constraints. Actual out-of-pocket expenditures will reflect both children's needs and families' limited ability to meet those needs. For these reasons, we assume the estimates from this study will be conservative. The expenditures reported by these low-income families should be interpreted cautiously as indicators of spending under conditions of financial constraint.
Labor Force Participation
Survey questions probed for several indicators of parents' labor force participation. Respondents were asked whether they were currently employed in a "regular" job. Because the labor market attachments of low-income parents and those with young children are often volatile, the survey included questions about any work (at "odd jobs") in the prior month, and any paid work in each of the months since the Wave I interview. Respondents were also asked to report on the labor market activities of their resident spouses or partners. Earnings from all adult family members were included in questions about family income for the prior month.
| TABLE A1. Coding of Severity: Children's Health Conditions and Disabilities |
| ModerateChild meets one or more of the following conditions |
| Needs "a little" more help than other children with his/her age with daily activities (e.g., eating, bathing, dressing, or getting around the house). |
| Unable to take part in usual activities for child of his/her age. |
| Attends special classes or receives special education services due to condition. |
| Misses "some" days of school due to condition. |
| Limited in ability to crawl, walk, run, or use stairs. |
| SevereChild meets one or more of the following conditions |
| Child needs "a lot" more help than other children his/her age with daily activities (e.g., eating, bathing, dressing, or getting around the house). |
| Misses "a lot" of days of school due to condition. |
| Prevented from going to school at all by condition. |
| Receives Supplemental Security Income (SSI). |
APPENDIX B
The Model
Economist's standard, static labor supply model forms the conceptual underpinnings of our analysis of labor force participation. In this model, individuals choose the combination of market work and non-market activities which allows them maximum utility with respect to their consumption of goods and leisure (Killingsworth 1983). Women's labor force choices are affected by factors such as available market work and wages; availability of income from other sources (husband's earnings, property or other unearned income); productivity of time spent in other work; and household tastes (Salkever 1982). We estimate a reduced form specification of this model in which mother's labor force participation is a function of structural, demographic, and human capital variables identified in studies of AFDC recipients and their labor force participation. The model presented here adds variables designed to capture the effects of the presence of a disabled child or children and of different characteristics of these children.
We estimate the effect of having a disabled or chronically ill child on mother's labor force participation, measured as a dichotomous variable with a value of 1 if the respondent was currently working at a regular job for pay at the time of the Wave II interview and 0 otherwise. We use four dummy variables to measure the presence of one or more disabled children in the family and the severity of their disabling conditions. These are designed to capture the differences in caretaking burden that are associated with children's special needs and to proxy the associated barriers to employment outside the home for mothers of chronically ill and disabled children. Mothers' labor force participation is hypothesized to decrease as the number of affected children increases from none to one or more than one, and to decrease as the severity of their functional impairments increases from moderate to severe. Because these represent distinct but not entirely orthogonal dimensions of caretaking burden, we estimate separate models with dummy variables for the number of affected children (the presence of one or more than one disabled or chronically ill child) and for the severity of child(ren)'s conditions (the presence of any children with moderate or severe conditions). Details on the operationalization of control variables are provided in Appendix Table B1.
We control for structural, demographic and human capital factors using measures which previous researchers have identified as affecting AFDC and employment. We include variables for respondent's race, education, health, age, and age squared. Because women's labor market choices are sensitive to the presence and earnings of partners/spouses, we include a variable for current cohabitation status. Based on empirical research suggesting that work and welfare behaviors differ for women who are ever married, we also control for respondents' marital status (as ever or never married). We include other variables measuring household characteristics that facilitate or inhibit the woman's employment: the number of children and the presence of any children under age six (both assumed to reduce labor force participation) and the presence of adults in the household other than respondent and her spouse or partner (hypothesized to increase labor force participation by increasing the number of adults available for child care).
Our models also include structural economic variables that are hypothesized to affect the woman's employment choices. We include variables for the level of AFDC and SSI benefits available to the woman, and other nonmeans-tested income available to the family. All are expected to have an income effect which depresses mother's labor market activities. As a measure of local employment opportunities, we include county unemployment rates.
Methodological Issues
In this section, we discuss some methodological issues that we encountered in estimating the impact of children's disabilities on AFDC recipient's labor force participation and our attempts to resolve them.
Respondent's Health. Wolfe and Hill (1995), among others, suggest that a woman's health and disability status is an important determinant of her labor market participation. Our survey data presented two potential measures of these variables: the respondent's assessment of her health as excellent, good, fair, or poor, and the respondent's self-report of whether she had a disability that limited her ability to work. Self-reports of this type are arguably endogenous variables in a model of labor force participation. Nevertheless, similar measures have been used productively in models of low-income women's labor force participation (Wolf and Hill 1995; Spalter-Roth et al. 1992). We used the health rating rather than the disability rating for our estimation because the endogeneity problems seemed smaller with respect to this variable.
Respondent's Potential Wage. An important variable in the static economic model of labor force participation is the wage that the woman can command if she works. Determining and measuring this wage, particularly for those not working, raises complex econometric issues (Killingsworth 1983). Rather than inserting a direct measure of this wage in our model, we have attempted to include in our model those human capital variables which have been shown to affect the woman's potential wage: education, age, race, and marital status.
AFDC and SSI Benefits. The standard labor model suggests that the amount of AFDC, SSI, and other unearned income available to a woman will have an income effect which lowers her hours of employment. Her employment income also affects the amount of her AFDC, SSI, and other means-tested benefits, however, raising problems of endogeneity. For this reason, we do not simply include in our model the amount of AFDC and SSI payments received by the family. Instead, we include variables designed to capture the maximum AFDC benefit available to the family when that family has no earned income. We used two variables to capture the AFDC benefit amount. Since, AFDC benefits depend on household size, we use one variable to measure the number of the respondent's biological/step/AFDC children in the household. California has reduced maximum benefits available for some families in a policy experiment. The second variable measures whether the respondent's family is in the experimental group that receives lower benefits. In this way, we hope to capture the incentive effects of the AFDC policy in California with a variable that is not directly affected by the woman's labor force choices.
SSI benefits present a similar and more vexing problem for this estimation. SSI is expected to have an income effect for those families which receive benefits; benefits are also contingent on the presence of a disability--in the respondent, her partner or her children--which is expected to further reduce labor force participation. We are interested in estimating the independent effects of the caretaking burden and the SSI receipt for families with disabled children. We address the problem of the endogeneity on this measure by creating a dummy variable for the receipt of SSI by any household member other than the respondent (including children and spouse/partners). This gives us a measure of SSI which is not completely correlated with children's disabilities, and allows us to estimate the impact of SSI separately from that of other transfer income. We use nested logistic regression estimations to measure the impact of children's special needs with and without controlling for the receipt of SSI by any family members.
| TABLE B1. Control Variables | |
| African American | 1 = Respondent is African American; 0 otherwise. |
| Latino | 1 = Respondent is Latino; 0 otherwise. |
| Never Married | 1 = Respondent has never married; 0 otherwise. |
| Partner/Spouse Present | 1 = Respondent currently lives with spouse or partner; 0 otherwise. |
| Mother's Age | Respondent's age in years. |
| Mother's Age Squared | Respondent's age squared. |
| Number of Other Adults | Number of adults present in household other than respondent and respondent's spouse or partner. |
| Years Education | Respondent's schooling, in years.a |
| Mother's Health Poor | 1 = Respondent rates her health as poor; 0 otherwise. |
| Any Children Less than Age 6 | 1 = Respondent has at least on child under 6 years. |
| Other Income | Amount of non-means-tested income received by respondent's family in the previous month, excluding respondent's earnings. |
| Number of AFDC Eligible Children | Number of AFDC eligible children in respondent's family. |
| Experimental Subject | 1 = Respondent is in an experimental group receiving lower AFDC benefits than other families of comparable circumstances. |
| SSI Receipt | Respondent's spouse, partner or child received SSI benefits in the previous month. |
| Unemployment Rate | County or most applicable unemployment rate available for month before interview. |
| |
NOTES
-
We use the term "special needs" throughout the paper to refer to the constellation of chronic illnesses, childhood diseases, and physical, sensory, and mental disabilities that can produce functional limitations for children, extra caretaking burdens for parents, and eligibility for various public programs.
-
The SSI child is omitted from the AFDC family unit for purposes of determining eligibility and benefit levels. Thus, a mother with a single child who receives SSI will be ineligible for AFDC.
-
Benefits from the Food Stamp program and other means-tested programs usually add to the incomes of both AFDC and SSI families with disabled children.
-
See H.R. Rep. No. 231, 92nd Cong., 2d Sess., reprinted in 1972 U.S. Code Cong. and Admin. News 4989, 5015.
-
Urban Systems Research and Engineering (1979) outlines the Congressional debate in Survey of Blind and Disabled Children Receiving Supplemental Security Income (SSI) Benefits, as do Weishaupt and Rains (1991). Because SSI legislation was enacted within the context of sweeping welfare reforms proposed by the Nixon administration, Congress paid comparatively little attention to the issue of SSI benefits for children (Burke 1974; Woodward and Weiser 1994). Woodward and Weiser (1994) and Burke (1974) describe the political context.
-
Wolfe and Hill (1995) defined a disabled child as any child with a long-lasting physical condition that limits walking, running, or playing, or a long-lasting mental or emotional problem that limits school work or learning.
-
Together, these four California counties account for nearly one-half of the AFDC caseload in California.
-
The sample includes a small number of male respondents, but respondents were overwhelmingly women.
-
The AFDC Household Survey also conducted interviews with a subsample of 1,100 Laotian, Vietnamese, Armenian, and Cambodian speaking households. Data from this subsample are not included in our analysis.
-
Fifty-three households who were no longer caring for AFDC recipient children are excluded from most analyses.
-
This includes 364 children (out of a total of 2,133) in 267 households (out of a total of 1,320).
-
Currently, 16 percent of the children's conditions remain to be coded. The relative proportion of specific conditions in our sample may change as these responses are coded.
-
Only the first reported condition was coded for this analysis. It is possible that children received SSI on the basis of a second or third condition which was not coded.
-
An additional 4 percent identified themselves as another race or ethnicity.
-
Total family income was standardized for family size by dividing all cash income (plus food stamps) in the prior month by the square root of the number of adults and children in the family. See Buhmann et al. (1988).
-
Health insurance for one randomly selected child in each family.
-
Health and health care measures are based on one randomly selected child per family.
-
The average expenditure across all families with special-needs children, whether they experienced costs or not, was $65.69 (Table 7A).
-
Data for all analyses in this paper are weighted to adjust for sampling strata and survey completion rates. Because initial stratification was quite extreme, weighted data are also used for the logistic regression. Standard statistical software fails to produce correct standard errors for weighted data; in this analysis we used an expression for the covariance matrix of parameters estimated using weighted maximum likelihood found in Manski and Lerman (1977).
-
Respondents were asked screening questions with respect to their biological and step children. A few families were headed by a "caretaker relative" who was not the biological or step parent of the AFDC children. Caretaker relatives were asked the screening questions with respect to their AFDC children.
-
The special amount spent was recorded in each category for amounts under $100. We top-coded amounts greater than $100 as $100. Because of this, the expenses reported in this paper are likely to be underestimates.
To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human ServicesOffice of Disability, Aging and Long-Term Care PolicyRoom 424E, H.H. Humphrey Building200 Independence Avenue, S.W.Washington, D.C. 20201FAX: 202-401-7733Email: webmaster.DALTCP@hhs.gov
RETURN TO:
Office of Disability, Aging and Long-Term Care Policy (DALTCP) Home [http://aspe.hhs.gov/_/office_specific/daltcp.cfm]Assistant Secretary for Planning and Evaluation (ASPE) Home [http://aspe.hhs.gov]U.S. Department of Health and Human Services Home [http://www.hhs.gov]