
Trends in Hospital Readmission and Emergency Department Visit among Infants Born with Neonatal Abstinence Syndrome
ASPE ISSUE BRIEF
Mir M. Ali, Emma Nye, and Kristina West
U.S. Department of Health and Human Services
Office of the Assistant Secretary for Planning and Evaluation
December 2020
Link to Printer Friendly Version in PDF Format (6 PDF pages)
ABSTRACT: This paper examines trends in hospital readmission and emergency department visits among infants with Neonatal Abstinence Syndrome (NAS) between 2008 and 2017 in the United States, using a multi-state Medicaid claims database.
This brief was prepared through intramural research by the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Behavioral Health, Disability, and Aging Policy. For additional information about this subject, you can visit the BHDAP home page at https://aspe.hhs.gov/bhdap or contact the authors at HHS/ASPE/BHDAP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201, Mir.Ali@hhs.gov, Emma.Nye@hhs.gov, Kristina.West@hhs.gov.
DISCLAIMER: The opinions and views expressed in this brief are those of the authors. They do not reflect the views of the Department of Health and Human Services, the contractor or any other funding organization. This brief was completed and submitted in March 2020.
| HIGHLIGHTS This paper examines trends in hospital readmission and emergency department visits among infants with NAS between 2008 and 2017 in the United States, using a multi-state Medicaid claims database. Key findings include the following:
|
Introduction
Over the past decade the rates of infants diagnosed with Neonatal Abstinence Syndrome (NAS) have increased rapidly, coinciding with the rise in opioid prescribing and opioid-related overdose deaths (Wahlen et al., 2019). Despite the recent increases in infants diagnosed with NAS and its associated health care services utilization, little is known about the trends in hospital readmissions rates or emergency department visits among NAS infants in the United States. Hospital readmissions rates are often used as both a quality measure to assess whether the initial hospital discharge protocol was safe and effective and a general evaluation of the effectiveness of the treatment regimen for infants with NAS (Patrick et al., 2015). In this report, a large Medicaid claims database is used to estimate the trends in hospital readmission rates and emergency department visits among NAS infants between 2008 and 2017.
Significant Proportion of Infants Born with NAS Experienced Hospital Readmission or Emergency Department Visit within 90 Days of Discharge
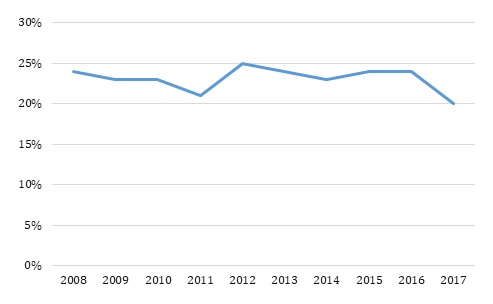
Close to a quarter of all NAS infants covered under Medicaid experienced a hospital readmission or emergency department visit within 90 days of their initial birth-related hospital discharge between 2008 and 2017 (Figure 1). This rate remained steady throughout the study period, with the highest rate (25%) occurring in 2012 and reaching the lowest (20%) in 2017. The primary reasons for hospital readmission and emergency department visit between 2008 and 2017 include conditions related to respiratory infections, fever, cough, and drug withdrawal syndrome (Table 1).
| FIGURE 1. Hospital Readmission/Emergency Department Visit among Medicaid NAS Infants within 3 Months of Birth Related Hospital Discharge |
|---|
 |
The study used IBM Watson Health MarketScan Multi-State Medicaid claims database (2008-2017). The sample includes all infants (ICD-9 livebirth codes V30-V39 and ICD-10 livebirth codes Z37-Z38) diagnosed with NAS (ICD-9 code 779.5 and ICD-10 code P961) born between 2008 and 2017. The sample size ranged from 989 NAS infants in 2008 to 5,027 NAS infants in 2017. Rates of hospital readmission or emergency department visit among NAS infants were measured by whether the infants had any inpatient hospitalization or had an emergency department encounter within 90 days of release from their birth hospitalization for each study year.
Discussion
Between 2008 and 2017, approximately a quarter of NAS infants covered under Medicaid experienced a hospital readmission or an emergency department visit within three months of their initial birth-related hospital discharge. This rate remained relatively steady throughout the study period and conditions related to drug withdrawal syndrome was one of the primary reasons for the hospital readmission or the emergency department visit.
The increase in the rates of infants diagnosed with NAS and the steady rate of hospital readmission in the midst of the opioid crisis underscores the public health significance of the issue. The first-line of treatment for NAS infants usually includes creating a quiet and soothing environment, rooming-in with the mother, breastfeeding and increased mother-infant bonding, protocols that require creating a supportive environment for both the infants and the substance-affected mothers. Thus, the relatively high rate of hospital readmissions and emergency department visits, especially for drug withdrawal symptoms, highlights the need of maybe providing more supportive services to this particularly vulnerable subset of families.
This study has several potential limitations. The number of Medicaid states represented in the MarketScan data varies from year to year and the trends in hospital readmission and emergency department visits observed in this study could be a function of that. Similarly, the MarketScan Medicaid database is not nationally representative, thus the rates observed in the study might not be generalizable to the entire population of infants diagnosed with NAS covered under Medicaid. However, this limitation is not unique to MarketScan, and is also applicable to other administrative claims databases.
Hospitalization and emergency department encounters appear to be common among NAS infants. Establishment of evidence-based protocols for both in-hospital and post-discharge treatment along with expansion of supportive resources for mothers and caregivers should be considered to reduce this risk. Future policy developments and activities targeted at NAS infants could potentially benefit from focusing on hospital readmissions rates.
References
Maalouf FI, Cooper WO, Slaughter JC, Dudley J, Patrick SW. (2018). Outpatient pharmacotherapy for Neonatal Abstinence Syndrome. Journal of Pediatrics; 199: 151-157.
Patrick SW, Burke JF, Biel TJ, Auger KA, Goyal NK, Cooper WO. (2015). Risk of hospital readmission among infants with Neonatal Abstinence Syndrome. Hospital Pediatrics; 5(10): 513-519.
Wahlen BL, Holmes AV, Blythe S. (2019). Models of care for neonatal abstinence syndrome: What works? Seminars in Fetal and Neonatal Medicine; 24(2): 121-132.
Winkelman TA, Villapiano N, Kozhimannil KB, Davis MM, Patrick S. (2018). Incidence and costs of Neonatal Abstinence Syndrome among infants with Medicaid: 2004-2014. Pediatrics; 141(4): e20173520.
| TABLE 1. Top 5 Frequent Reasons for Hospital Readmission or Emergency Department Visit among Medicaid NAS Infants: 2008-2017 | ||
|---|---|---|
| ICD-9/ICD-10 Code for Reasons for Hospitalization/Emergency Department Visit | N | Events |
| Year: 2008 | ||
| 465.9 Acute upper respiratory infections of unspecified site | 48 | 151 |
| 779.5 Drug withdrawal syndrome in newborn | 39 | 54 |
| 786.2 Cough | 35 | 61 |
| 779.89 Other specified conditions originating in the perinatal period | 28 | 34 |
| 780.60 Fever, unspecified | 25 | 62 |
| Year: 2009 | ||
| 780.60 Fever, unspecified | 68 | 275 |
| 465.9 Acute upper respiratory infections of unspecified site | 61 | 247 |
| 786.2 Cough | 58 | 123 |
| 779.5 Drug withdrawal syndrome in newborn | 49 | 67 |
| 079.99 Unspecified viral infection | 40 | 143 |
| Year: 2010 | ||
| 780.60 Fever, unspecified | 61 | 242 |
| 465.9 Acute upper respiratory infections of unspecified site | 59 | 270 |
| 530.81 Esophageal reflux | 41 | 90 |
| 787.03 Vomiting alone | 40 | 106 |
| 779.5 Drug withdrawal syndrome in newborn | 40 | 47 |
| Year: 2011 | ||
| 780.60 Fever, unspecified | 74 | 420 |
| 465.9 Acute upper respiratory infections of unspecified site | 67 | 230 |
| 786.2 Cough | 50 | 163 |
| 787.03 Vomiting alone | 47 | 142 |
| 779.5 Drug withdrawal syndrome in newborn | 41 | 42 |
| Year: 2012 | ||
| 786.2 Cough | 193 | 559 |
| 465.9 Acute upper respiratory infections of unspecified site | 192 | 711 |
| 780.60 Fever, unspecified | 158 | 757 |
| 478.19 Other disease of nasal cavity and sinuses | 125 | 404 |
| 779.5 Drug withdrawal syndrome in newborn | 103 | 155 |
| Year: 2013 | ||
| 786.2 Cough | 207 | 755 |
| 465.9 Acute upper respiratory infections of unspecified site | 194 | 854 |
| 780.60 Fever, unspecified | 175 | 714 |
| 478.19 Other disease of nasal cavity and sinuses | 137 | 491 |
| 779.5 Drug withdrawal syndrome in newborn | 122 | 230 |
| Year: 2014 | ||
| 465.9 Acute upper respiratory infections of unspecified site | 212 | 882 |
| 786.2 Cough | 202 | 508 |
| 780.60 Fever, unspecified | 194 | 779 |
| 787.03 Vomiting alone | 149 | 484 |
| 779.5 Drug withdrawal syndrome in newborn | 112 | 197 |
| Year: 2015 | ||
| R05 Cough | 77 | 212 |
| J069 Acute upper respiratory infection, unspecified | 74 | 263 |
| R0981 Nasal congestion | 56 | 194 |
| P961 Neonatal withdrawal symptoms from maternal use of drugs of addiction | 51 | 55 |
| R509 Fever, unspecified | 46 | 264 |
| 779.5 Drug withdrawal syndrome in newborn | 78 | 132 |
| 465.9 Acute upper respiratory infections of unspecified site | 69 | 272 |
| 780.60 Fever, unspecified | 56 | 222 |
| 779.89 Other specified conditions originating in the perinatal period | 52 | 106 |
| 786.2 Cough | 50 | 118 |
| Year: 2016 | ||
| R05 Cough | 171 | 418 |
| J069 Acute upper respiratory infection, unspecified | 150 | 591 |
| P961 Neonatal withdrawal symptoms from maternal use of drugs of addiction | 145 | 192 |
| R509 Fever, unspecified | 140 | 667 |
| R0981 Nasal congestion | 100 | 283 |
| Year: 2017 | ||
| J069 Acute upper respiratory infection, unspecified | 122 | 516 |
| R05 Cough | 116 | 284 |
| R509 Fever, unspecified | 82 | 580 |
| R0981 Nasal congestion | 74 | 207 |
| R1110 Vomiting, unspecified | 72 | 207 |
Neonatal Abstinence Syndrome
This brief was prepared through intramural research by the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Behavioral Health, Disability, and Aging Policy. For additional information about this subject, you can visit the BHDAP home page at https://aspe.hhs.gov/bhdap or contact the authors at HHS/ASPE/BHDAP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201, Mir.Ali@hhs.gov, Emma.Nye@hhs.gov, Kristina.West@hhs.gov.
Reports Available
Trends in Hospital Readmission and Emergency Department Visit among Infants Born with Neonatal Abstinence Syndrome Issue Brief
- HTML version: https://aspe.hhs.gov/basic-report/trends-hospital-readmission-and-emergency-department-visit-among-infants-born-neonatal-abstinence-syndrome-issue-brief
- PDF version: https://aspe.hhs.gov/pdf-report/trends-hospital-readmission-and-emergency-department-visit-among-infants-born-neonatal-abstinence-syndrome-issue-brief
Use of Outpatient Pharmacological Treatment Among Infants Born with Neonatal Abstinence Syndrome: Medicaid 2008-2017 Issue Brief
- HTML version: https://aspe.hhs.gov/basic-report/use-outpatient-pharmacological-treatment-among-infants-born-neonatal-abstinence-syndrome-medicaid-2008-2017-issue-brief
- PDF version: https://aspe.hhs.gov/pdf-report/use-outpatient-pharmacological-treatment-among-infants-born-neonatal-abstinence-syndrome-medicaid-2008-2017-issue-brief
Utilization of Mental Health Services among Children Diagnosed with Neonatal Abstinence Syndrome at Birth Issue Brief
- HTML version: https://aspe.hhs.gov/basic-report/utilization-mental-health-services-among-children-diagnosed-neonatal-abstinence-syndrome-birth-issue-brief
- PDF version: https://aspe.hhs.gov/pdf-report/utilization-mental-health-services-among-children-diagnosed-neonatal-abstinence-syndrome-birth-issue-brief