
U.S. Department of Health and Human Services
Office of the Assistant Secretary for Planning and Evaluation
December 2020
Link to Printer Friendly Version in PDF Format (6 PDF pages)
ABSTRACT: This brief examines utilization of mental health services among infants with Neonatal Abstinence Syndrome (NAS) who have a mental health condition when they reach the age of five.
This brief was prepared through intramural research by the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Behavioral Health, Disability, and Aging Policy. For additional information about this subject, you can visit the BHDAP home page at https://aspe.hhs.gov/bhdap or contact the authors at HHS/ASPE/BHDAP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201, Mir.Ali@hhs.gov, Emma.Nye@hhs.gov, Kristina.West@hhs.gov.
DISCLAIMER: The opinions and views expressed in this brief are those of the authors. They do not reflect the views of the Department of Health and Human Services, the contractor or any other funding organization. This brief was completed and submitted in March 2020.
|
HIGHLIGHTS This paper examines utilization of mental health services among infants with NAS who have a mental health condition when they reach the age of five. Key findings include the following:
|
Introduction
Rates of Neonatal Abstinence Syndrome (NAS) have increased during the past decade in the United States (Wahlen et al., 2019). As a result, there has emerged a significant policy focus on the impact of the opioid epidemic on children (Wachman and Schiff, 2018). In addition to experiencing longer hospital stays, higher rates of readmission, and higher treatment costs (Winkelman et al., 2018), children with NAS also have lower language scores and cognition (Beckwith and Bruke, 2015), lower verbal and mathematic ability (Ornoy et al., 2001), and problems with working memory and inhibitory control (Levine and Woodward, 2018). In addition, recent literature has documented evidence showing that more than half of infants with NAS are diagnosed with a mental health condition by the time they reach the age of five (Sherman et al., 2018). This age is an important milestone in terms of school readiness and developmental outcomes; thus close attention to impacts of NAS by this age is critical. Despite the high incidence of mental health conditions among children with NAS, there is a lack of longitudinal data regarding mental health treatment utilization among them. This study examines mental health treatment utilization among infants with NAS with a mental health condition by the time they reach the age of five.
Significant Proportion of Infants Born with NAS are Diagnosed with a Mental Health Condition, but Very Few Receive Any Treatment
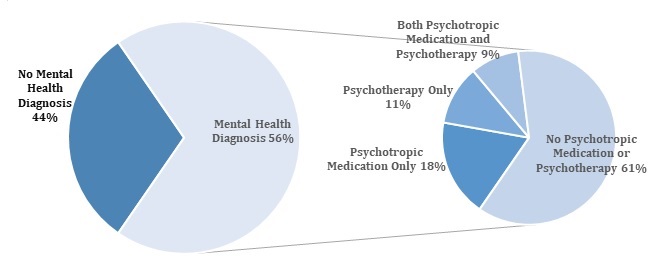
Figure 1 shows that 56% of children born with NAS during birth are diagnosed with a mental health condition by the time they reach the age of five. Among those children with NAS and a mental health diagnosis, over half of them did not receive any mental health treatment (61%). Among children with NAS and a mental health condition, 18% received a psychotropic medication only, 11% received psychotherapy only, and 9% received a combination of psychotropic medication and psychotherapy for their mental health condition.
| FIGURE 1. Utilization of Mental Health Treatment among School-Aged Ready Children Born with NAS |
|---|
 |
Discussion
Over 50% of children born with NAS were diagnosed with a mental health condition by the time they turned five years old. However, more than 60% of these children did not receive any mental health treatment. Furthermore, of those who did receive treatment, few received any behavioral interventions or psychotherapy in tandem with a psychiatric prescription. The rate of mental health conditions and lack of treatment utilization is much higher in the NAS population compared to the rates observed in the general population of young children as documented in the literature (Ali et al., 2018). These findings raise potential concerns about the lack of mental health treatment utilization among children with NAS and a mental health condition, given that evidence-based practices indicate that combined treatment with psychiatric medications and psychotherapy may be appropriate for the most common mental disorders among children (Olfson et al., 2015). It also highlights the need for broader implementation of evidence-based practices, and the need for a more integrated and comprehensive approach in treating children with NAS.
Caution must be exercised when interpreting these data, particularly when making inferences about causality, as there are likely environmental and other confounders that impact mental health and treatment utilization. The sample is not nationally representative nor does it cover all states, and the majority of children with NAS did not have five years of continuous enrollment in Medicaid. Lastly, the data used here do not capture treatment paid for by sources other than Medicaid insurance, and treatment for which no claims were submitted or insurance claims were denied.
These findings have implications for early screening, preventative interventions, psychosocial support, and treatment for children and families of this population. They further imply challenges for school readiness and highlight the need for continued, comprehensive care of children born with NAS.
References
Ali MM, Teich JL, Lynch S, Mutter R. (2018). Utilization of mental health services by preschool children with private insurance coverage. Administration & Policy in Mental Health & Mental Health Services Research; 45(5): 731-740.
Beckwith AM, Burke SA. (2015). Identification of early developmental deficits in infants with prenatal heroin, methadone, and other opioid exposure. Clinical Pediatrics; 54(4): 328-335.
Levine TA, Woodward LJ. (2018). Early inhibitory control and working memory abilities of children prenatally exposed to methadone. Early Human Development; 116: 68-75.
Olfson M, Druss BG, Marcus SC. (2015). Trends in mental health care among children and adolescents. New England Journal of Medicine; 372: 2029-2038.
Ornoy A, Segal J, Bar-Hamburger R, Greenbaum C. (2001). Developmental outcome of school-age children born to mothers with heroin dependency: Importance of environmental factors. Developmental Medicine & Child Neurology; 43(10): 668-75.
Sherman LJ, Ali MM, Mutter R, Larson J. (2019). Mental disorders among children born with Neonatal Abstinence Syndrome. Psychiatric Services; 70(2): 151.
Wachman EM, Schiff DM, Silverstein M. (2018). Neonatal abstinence syndrome. JAMA; 319(13): 1362-74.
Wahlen BL, Holmes AV, Blythe S. (2019). Models of care for neonatal abstinence syndrome: What works? Seminars in Fetal & Neonatal Medicine; 24(2): 121-132.
Winkelman TA, Villapiano N, Kozhimannil KB, Davis MM, Patrick S. (2018). Incidence and costs of Neonatal Abstinence Syndrome among infants with Medicaid: 2004-2014. Pediatrics; 141(4): e20173520.
Appendix 1: Methodology
The study used IBM Watson Health MarketScan Multi-State Medicaid claims database (2008-2017). The sample of the analysis includes 3,075 infants diagnosed with NAS at birth (ICD-9 code 779.5) between 2008 and 2012 and continuously enrolled in the database till they reached the age of five (as far forward as 2017). Mental health diagnosis was measured by whether the child had any of the following diagnoses (ICD-9 codes: 290-319; ICD-10 codes: F20-F99): adjustment disorder; attention deficit/hyperactivity disorder; anxiety disorder; behavioral and emotional disorder with childhood onset; bipolar disorder; depression or mood disorder, not otherwise specified; disruptive behavior disorder; neurotic, stress related disorder; schizophrenia and other psychoses; and other mental disorders (full list of ICD-9 and ICD-10 codes provided in Table 1).
| TABLE 1. ICD-9/10 Codes Used to Define Mental Health Disorder Diagnostic Groups | |
|---|---|
| Mental Health Disorder Diagnostic | ICD-9 Codes |
| Adjustment Disorder | 308.0-308.2, 308.4, 308.9, 309.0-309.4, 309.82, 309.83, 309.89, 309.9 |
| Attention Deficit/Hyperactivity Disorder | 314 |
| Anxiety Disorder | 293.84, 300.0, 300.2, 300.3, 308.3, 309.21, 309.81, 313.0, 313.2, 313.89 |
| Bipolar Disorder | 296.0, 296.1, 296.4-296.8, 301.13 |
| Communication and Learning Disorder | 307.0, 307.9, 315.0-315.2, 315.31, 315.32, 315.39, 315.9 |
| Depression or Mood Disorder, not otherwise specified | 293.83, 296.2, 296.3, 296.9, 298.0, 300.4, 311 |
| Disruptive Behavior Disorders | 312.0-312.4, 312.81, 312.82, 312.89, 312.9, 313.81 |
| Pervasive Developmental Disorder or Mental Retardation | 299, 317-319 |
| Schizophrenia and Other Psychoses | 295, 297-298 |
| Other Mental Disorder | 290-319, not listed above |
| Mental Health Disorder Diagnostic | ICD-10 Codes |
| Schizophrenia, Schizotypal and Delusional Disorders | F20-F29 |
| Mood [affective] Disorders | F30-F39 |
| Neurotic, Stress-Related and Somatoform Disorders | F40-F48 |
| Behavioral Syndromes Associated with Physiological Disturbances and Physical Factors | F50, F51, F54, F59 |
| Behavioral and Emotional Disorders with Onset Usually Occurring in Childhood and Adolescence | F90-F98 |
| Unspecified Mental Disorder | F99 |
The mental health treatment indicator is a categorical variable with four mutually exclusive categories: psychotropic prescription medication filled only; psychotherapy only; both psychotropic prescription medication filled and psychotherapy; and no mental health treatment. Psychotropic prescription medication use was defined by using the pharmacy claims file as having filled one or more psychotropic drug prescriptions. The following therapeutic classes, which are commonly used to treat behavioral disorders, were included to indicate usage of psychotropic medication: antidepressants, antipsychotics, anticonvulsants, antimanic agents, antiparkinsonian agents, anxiolytics/sedatives, hypnotics, benzodiazepines, barbiturates, central nervous system (CNS) agents--miscellaneous (CNS miscellaneous), and stimulants (full list available from the authors upon request). Psychotherapy was defined by using the following Current Procedural Terminology codes: 90804-90819, 90821-90824, 90826-90829, 90832-90834, 90836-90840, 90845-90847, 90849, 90853, 90857, 90862, 90875, 90876, and 99605. Children with claims for neither psychotropic medication nor psychotherapy were categorized as receiving no mental health treatment.
Neonatal Abstinence Syndrome
This brief was prepared through intramural research by the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Behavioral Health, Disability, and Aging Policy. For additional information about this subject, you can visit the BHDAP home page at https://aspe.hhs.gov/bhdap or contact the authors at HHS/ASPE/BHDAP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201, Mir.Ali@hhs.gov, Emma.Nye@hhs.gov, Kristina.West@hhs.gov.
Reports Available
Trends in Hospital Readmission and Emergency Department Visit among Infants Born with Neonatal Abstinence Syndrome Issue Brief
- HTML version: https://aspe.hhs.gov/basic-report/trends-hospital-readmission-and-emergency-department-visit-among-infants-born-neonatal-abstinence-syndrome-issue-brief
- PDF version: https://aspe.hhs.gov/pdf-report/trends-hospital-readmission-and-emergency-department-visit-among-infants-born-neonatal-abstinence-syndrome-issue-brief
Use of Outpatient Pharmacological Treatment Among Infants Born with Neonatal Abstinence Syndrome: Medicaid 2008-2017 Issue Brief
- HTML version: https://aspe.hhs.gov/basic-report/use-outpatient-pharmacological-treatment-among-infants-born-neonatal-abstinence-syndrome-medicaid-2008-2017-issue-brief
- PDF version: https://aspe.hhs.gov/pdf-report/use-outpatient-pharmacological-treatment-among-infants-born-neonatal-abstinence-syndrome-medicaid-2008-2017-issue-brief
Utilization of Mental Health Services among Children Diagnosed with Neonatal Abstinence Syndrome at Birth Issue Brief
- HTML version: https://aspe.hhs.gov/basic-report/utilization-mental-health-services-among-children-diagnosed-neonatal-abstinence-syndrome-birth-issue-brief
- PDF version: https://aspe.hhs.gov/pdf-report/utilization-mental-health-services-among-children-diagnosed-neonatal-abstinence-syndrome-birth-issue-brief