
U.S. Department of Health and Human Services
U.S. Department of Health and Human Services
Office of the Assistant Secretary for Planning and Evaluation
January 2006
This report was prepared by the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP), in collaboration with other federal agencies. For additional information about the study, you may visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, John Drabek, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, SW, Washington, DC 20201. His e-mail address is: John.Drabek@hhs.gov.
This report was prepared by staff from the Department of Health and Human Services' Office of the Assistant Secretary for Planning and Evaluation, in consultation with the Administration on Developmental Disabilities, the Office of Disability, the Center for Medicare and Medicaid Services; the Department of Labor's Employment and Training Administration; and the Department of Education's National Institute on Disability and Rehabilitation Research.
Amy Hewitt, Charlie Lakin, and Sheryl Larson of the Research and Training Center on Community Living, Institute on Community Integration of the University of Minnesota contributed extensively to this report.
TABLE OF CONTENTS
- I. CHANGING PATTERNS OF LTSS FOR PERSONS WITH ID/DD
- A. Changing Settings of LTSS
- B. Changing Expectations of LTSS
- C. Changing Roles and Responsibilities of DSPs
- II. CURRENT AND PROJECTED SUPPLY AND DEMAND FOR DSPs
- A. Overview of Supply and Demand for DSPs
- B. Factors Associated with Demand for DSPs
- C. Translating Current and Projected LTSS Demand into DSP Demand
- D. Supporting the Continuing Essential Roles of Informal Caregivers
- E. Uncertainties in Long-Term Projections of LTSS and DSP Demand
- F. DSP Demand and Supply and Relative Contributions of Recruitment and Retention
- III. FACTORS ASSOCIATED WITH THE RECRUITMENT AND RETENTION OF DSPs TO MEET CURRENT AND PROJECTED FUTURE DEMAND
- A. Organizational Factors
- B. DSP Characteristics
- C. Results of Turnover Challenges for Organizations
- IV. IMPLICATIONS OF FAILING TO MEET CURRENT AND PROJECTED FUTURE DEMAND FOR A SUFFICIENT NUMBERS OF QUALIFIED DSPs
- A. Current Service Recipients
- B. Families
- C. Future Service Recipients
- V. INITIATIVES AND INNOVATIONS UNDERWAY TO RESPOND TO THE CURRENT AND PROJECTED FUTURE DEMAND FOR SUFFICIENT NUMBERS OF QUALIFIED DSPs
- A. Federal Agencies
- Department of Health and Human Services (HHS)
- Department of Labor (DOL)
- Department of Education (DoE)
- B. State and Local Agencies
- Kansas
- Illinois
- Ohio
- West Virginia
- Wyoming
- C. Other Promising Practices
- SPIN
- National Alliance for Direct Support Professionals
- APPENDIX A. INTERVENTION STUDIES
- A. Recruitment and Selection
- B. Orientation and Training
- C. Supervision and Management
- D. Appendix Notes
- LIST OF FIGURES AND TABLES
- FIGURE 1: Adults with Intellectual Disability and/or Developmental Disability
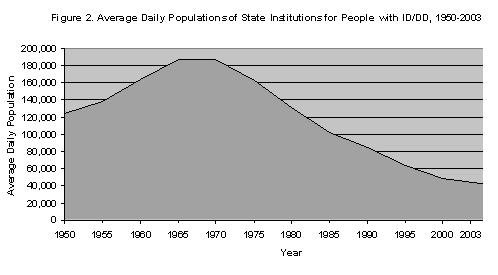
- FIGURE 2: Average Daily Populations of State Institutions for People with ID/DD, 1950-2003
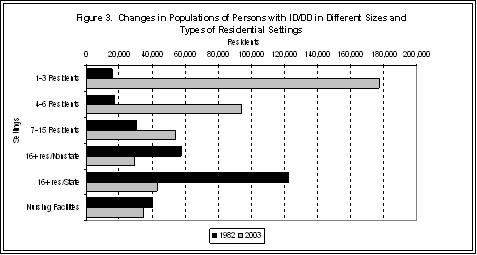
- FIGURE 3: Changes in Populations of Persons with ID/DD in Different Sizes and Types of Residential Settings
- FIGURE 4: Estimated Number of Children and Adults Identified with ID/DD Living with Families or Receiving Out of Family Home Residential or Nursing Services
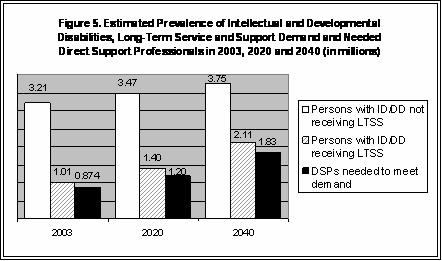
- FIGURE 5: Estimated Prevalence of Intellectual and Developmental Disabilities, Long-Term Service and Support Demand and Needed Direct Support Professionals in 2003, 2020 and 2040
- FIGURE 6: Demand for DSP Recruits to Meet Projected Demand for LTSS, 2005-2020 at Current 50% Turnover and with Annual Reductions by 2% until Reaching and Stabilizing at 30%
- TABLE 1: Current and Projected Demand for LTSS for Persons with ID/DD
- TABLE 2: Current and Projected Demand for DSPs for Persons with ID/DD
- TABLE 3: DSP Turnover in Residential/In-Home and Vocational/Day Services, 1998-2003
- TABLE 4: Factors Associated with Turnover from Correlation and Multivariate Studies Conducted in LTSS for Persons with ID/DD
- TABLE 5: DSP Wages and Turnover Differences for Community vs. Institutional LTSS
- TABLE 6: Factors Associated with Turnover Across Industries from Turnover Models and Meta-analytic Studies
- TABLE A-1: Training Needs for DSPs in LTSS for Persons with ID/DD
PREFACE
In 2004, Congress requested that the Department of Health and Human Services (HHS) conduct a study on the shortage of direct support professionals (DSPs) supporting persons with intellectual disabilities and other developmental disabilities (ID/DD), including an examination of the root causes associated with high vacancy and turnover rates, and an examination of the impact this shortage may be having on services for people with ID/DD. This report is a product of collaboration between many offices within HHS in response to the request from Congress. Staff throughout the Department worked collaboratively to share information and data pertaining to DSPs. The results of these efforts are presented in this unified Report to Congress. In addition, HHS included information from the following activities:
- HHS phone conversations with state and local experts in long-term services and supports (LTSS) for individuals with ID/DD, and the DSP workforce that is central to their delivery.
- Data collection by federal and state agencies on the status and trends in LTSS, and in the recruitment and retention of the DSP workforce needed to meet current and future demands.
- A review of the research and evaluation relevant to the recruitment, training and retention of a DSP workforce sufficient to meet the current and future needs of individuals with ID/DD, their families and the public and private agencies engaged in providing needs services and supports to them.
- A synthesis of Departmental efforts related to developing services and supports for individuals with ID/DD in home and community-based settings provided by a DSP workforce of sufficient size and quality to deliver those services and supports as designed.
EXECUTIVE SUMMARY
One of the challenges facing the U.S. in the 21st century will be to ensure that individuals of all ages receive, throughout their lives, the health and social support services they need to live with dignity as fully included members of our society. For the estimated 4.3 million Americans of all ages with intellectual disabilities and/or developmental disabilities (ID/DD) living in residential settings, their own homes or with members of their families, ensuring access to and quality of direct support professionals (DSPs) is key to realizing national goals established in the Americans with Disabilities Act, the Developmental Disabilities Assistance and Bill of Rights Act, and other statements of national purpose with regard to the full citizenship and inclusion of individuals with ID/DD.
In June 2003 there were an estimated 874,000 full-time equivalent (FTE)* DSPs assisting individuals with ID/DD in group residential settings, family homes, their own homes, community jobs, vocational and day training settings, and other service settings. In all such settings DSPs help persons with ID/DD with basic health and self-care needs, but also play a central role in assisting them to gain skills, participate in community life, develop social relationships, make decisions and judgments, and become more independent. DSPs may also be referred to as direct care staff, aides, home health assistants, respite care providers, personal care attendants and by numerous other terms, but whatever their title, they share the distinction of being essential to the quality of life, health and safety of more than 1 million Americans with ID/DD who are in need of long-term services and supports (LTSS).
The Department of Health and Human Services (HHS) estimates that by 2020, the number of DSPs needed to meet LTSS demand will grow to approximately 1.2 million FTEs providing an estimated 1.4 million individuals with ID/DD with needed residential, vocational and other supports. Between 2003 and 2020 HHS anticipates that the number of DSPs needed to provide for the growth of LTSS for individuals with ID/DD will increase by about 323,000 jobs, or roughly 37%. This increase will be largely due to population increases, increases in life expectancy among persons with ID/DD, aging of family caregivers, and expansion of home and community-based services. This increase in demand will be occurring at a time when the labor supply of adults age 18-39 years, who traditionally have filled these jobs is expected to increase only by 7%.
These projections indicate that meeting the future demand for DSPs will be extremely difficult to achieve through enhanced recruitment alone. It will be critically important to improve also the retention of existing DSPs along with efforts to attract new ones. Since many industries will be competing for the supply of direct care workers, including the much more rapidly growing LTSS systems for aging persons with disabilities, compensation, working conditions, career opportunities and job design will play a key role in retaining current DSPs and in attracting new workers to assure the supply of DSPs needed to provide LTSS. Providing adequate levels of high quality, committed and stable direct support will require sustained effort by many actors. In such efforts it will be essential to work across federal, state and local governments, education and training institutions, workforce investment systems, faith-based organizations, service provider organizations and DSPs themselves in shaping DSP roles into ones that offer those who enter them with sufficient opportunity and respect to consider it as a viable career decision.
Section Note
| * | An FTE refers to the number of hours of required DSP work equal to standard full-time employment (usually 40 hours). In practice about one-third of all DSPs work part-time so that two or more DSPs might work to equal one FTE. |
INTRODUCTION
DEFINING "DIRECT SUPPORT PROFESSIONAL" (DSP)
For the purposes of this Report to Congress, "direct support professional" (DSP) for persons with intellectual disabilities and other developmental disabilities (ID/DD) is defined in a manner consistent with the Congressional definition contained in the 2003 Direct Support Professional Recognition Resolution (S. Con. Res. 21/H. Con. Res. 94). Specifically, DSPs are individuals who receive monetary compensation to "provide a wide range of supportive services to individuals with intellectual and developmental disabilities on a day-to-day basis, including habilitation, health needs, personal care and hygiene, employment, transportation, recreation, and housekeeping and other home management-related supports and services so that these individuals can live and work in their communities" and "lead self-directed, community and social lives" (Congressional Record, November 4, 2003, p. H10301). DSPs for individuals with ID/DD work in a range of settings, including family homes, intermediate care facilities, small community residential settings, vocational and day training programs and others. They include full and part-time employees.
One of the challenges facing the U.S. in the 21st century will be to ensure that Americans who incur disability at any age have access to the health and social support services they need to become or remain integrated and valued members of their communities. For the 4.3 million individuals with intellectual disabilities and other developmental disabilities (ID/DD), assuring such supports and obtaining such outcomes, often depends on the adequacy and availability of direct support professionals (DSPs). Five factors are propelling increasing the demand for DSPs for individuals with ID/DD: (1) the growing U.S. population; (2) the increasing life expectancy of people with ID/DD; (3) increased prevalence of ID/DD; (4) the aging of family caregivers; and (5) the national commitment to, and steady expansion, of community and in-home services and supports for people with ID/DD.
Persons with ID/DD incur substantial and lasting disability at birth or in childhood. Assuring them of the support they need to enjoy health, safety and general well-being will depend in large part on there being sufficient numbers of paid DSPs, including full and part-time residential support providers, day training and vocational support workers, home health assistants, respite care providers, job coaches, and personal care attendants, as well as unpaid family members, neighbors and volunteers to provide the care needed. Already the nation is facing strains in finding a sufficient number of DSPs. Vacancy rates average 10-11% across the country, and reports are increasingly common of service providers who refuse requests to expand services to meet growing demand because of inability to recruit and retain the workforce needed to do so.
The national need for DSPs is not simply one of securing sufficient numbers of DSPs to fill available positions in residential, vocational, in-home supports and other support settings. DSPs need high levels of skill, knowledge, commitment and ethical foundation to fulfill the growing levels of responsibility given to them. This requires work environments that provide respect, support and opportunity for DSPs.
Providing adequate levels and quality of long-term services and supports (LTSS) will require sustained, concerted effort by many actors. The Federal Government has an important role to play, in promoting and supporting efforts of state and local government entities, of current and new disability service organizations, of emerging DSP worker associations, of education and training institutions, of workforce investment systems, of faith-based organizations, of advocacy organizations, and of families and persons with disabilities to develop informed commitments and provide effective responses to the challenges of assuring a DSP workforce of sufficient size and quality to meet the growing need for LTSS among Americans with ID/DD.
This report is an attempt to provide a comprehensive view of the supply and demand for DSPs for people with ID/DD. It is organized into the following sections:
- Section I -- Provides a brief overview of ID/DD and of the changing patterns in LTSS available to them. It describes the rapid shift from predominance of institutional settings to a system that is overwhelmingly focused on community and in-home supports. It also describes the changing expectations for services and the changing roles of DSPs as part of the changes.
- Section II -- Provides an overview of the current and projected demand for and supply of the DSP workforce for individuals with ID/DD. It identifies factors associated with future demand and associated difficulties in developing estimates of DSP shortages using available data. It examines the role of DSP turnover in present and future supply of DSPs. It describes the significance of unpaid informal caregiving to individuals with ID/DD, and how emerging support and financing models may affect demand for DSPs.
- Section III -- Summarizes research and describes factors that have been found to be important to the recruitment and retention of DSPs. It examines the potential effects on areas of important focus in anticipating and responding to potential imbalances between the supply and demand for DSPs in responding to the LTSS needs of persons with ID/DD.
- Section IV -- Explores the potential impact of failing to respond effectively to potential labor force imbalances, continuing high turnover, and/or insufficient recruitment of DSPs. It examines these potential effects on persons with ID/DD, family members, LTSS provider agencies and on DSPs themselves.
- Section V -- Provides descriptions of the Department of Health and Human Services (HHS) and other federal initiatives focused on supporting and developing an adequate and available labor force of DSPs. It also identifies promising practices being implemented by state and local governments and by service providing agencies to respond to the challenges of assuring that people with ID/DD have access to sufficient numbers of well-prepared DSPs to meet their LTSS needs.
ID/DD are different, but related concepts. They have certain shared features that cause them to overlap in the individuals they describe and in their popular use. Intellectual disability (or "mental retardation") is defined by current demonstration of: (a) significantly sub-average intellectual performance (as evidenced by an I.Q. of about 70 or lower), (b) substantial limitations in age appropriate performance in at least two major life areas related to independent living; and (c) manifested while still in the developmental period. Developmental disability is defined in part by substantial functional limitations in at least three of seven major life areas related to independent living. Developmental disability may be attributable to sub-average intellectual performance, but may also derive from physical impairments or from a combination of impairments. Like intellectual disabilities, developmental disabilities are first manifested in "the developmental period" (before age 22 years). ID/DD are frequently used interchangeably. Many state agencies that were once designated as "mental retardation" agencies are today state agencies on developmental disabilities. A major factor in this shift has been the federal Medicaid program with two primary programs of LTSS to persons with ID/DD: intermediate care facilities (ICFs/MR) and home and community-based services (HCBS). These programs are specifically designed for persons with "mental retardation" (intellectual disability) and "related conditions." Although the Medicaid definition of "related conditions" is not precisely the federal definition for "developmental disabilities," it is very similar. Still despite this, the terms intellectual disability (or "mental retardation") and developmental disability are not congruent. Figure 1 combines national household survey data and national data on out-of-family supervised residential programs to estimate the distribution of adults with ID/DD into "DD, not ID;" "ID, not DD;" and "ID and DD" groupings (children and youth are excluded because of complex definitional and social/educational issues make such distinctions difficult). According to these national studies there are an estimated 1.9 million adults, 18 years or older with ID/DD. Of these, just over half (51.5%) are estimated to have both intellectual and developmental disabilities; about 21.5% are estimated to be identified as having intellectual disability, but not developmental disability; about 27% are estimated to have developmental disability but not intellectual disability.1

I. CHANGING PATTERNS OF LTSS AND PERSONS WITH ID/DD
A. Changing Settings of LTSS
For nearly 40 years, the U.S. as a nation, and to varying degrees and on differing timelines all of the individual states, have embraced a commitment to reducing institutional placement of persons with ID/DD and to creating community alternatives for providing them with needed LTSS. As shown in Figure 2, between 1967 and 2003, the average daily population of persons with ID/DD in state institutions for persons with ID/DD decreased drastically from 194,650 to 42,385 (78.0%). As part of this process, there has been a growing commitment to state institution closures. In the 15 years between 1988 and 2003, there were on average, 8.3 state institution closures per year (133 in all).2
These trends are also evident in privately-operated (but virtually entirely government-financed) services. Between June 1982 and June 2003 persons with ID/DD living in private residential settings with 16 or more residents decreased by 48.4% (to 29,639); nursing facility residents with ID/DD decreased by an estimated 15.8% (to 35,008). LTSS for persons with ID/DD has been largely transformed into a system of home and community-based supports. In June 2003, of the estimated 437,289 persons with ID/DD receiving residential and nursing facility services and supports, 329,807 of them (75.4%) received LTSS in community living arrangements of 15 or fewer residents; 83.5% of whom (275,461) lived in settings of six or fewer residents, and 53.7% of whom (177,260) lived in settings of three or fewer residents.2Figure 3 summarizes the changing patterns in LTSS in the U.S. between 1982 and 2003.2 These statistics do not include the estimated 500,004 persons with ID/DD who received LTSS while living in the homes of birth or adoptive family members, or the estimated 38,000 children and youth with ID/DD in generic, child welfare/social service agency-administered foster care homes.3
The changes evident in Figure 3 have been supported and encouraged by formal national commitments. They include the Americans with Disabilities Act (ADA) of 1990 and its interpretation by the Supreme Court decision in Olmstead et al. v L.C. et al. (1999), an Executive Order of President Bush and the accompanying New Freedom Initiative, the Developmental Disabilities Assistance and Bill of Rights Act (DD Act) of 2000, and in a range of other legislation, judicial decisions and administrative policies. The financing of these changes has largely depended on the Medicaid for HCBS ("waiver") program. Beginning in the early 1990s, the states were allowed much greater access to federal cost-share for community services through the Medicaid HCBS waiver option, enabling them to claim federal cost-share for both newly developed services and for services previously financed entirely with state monies. A visible effect of this new access to Medicaid was that between 1992 and 2003 the combined ICF/MR and HCBS recipients with ID/DD increased from 208,689 (62,429 in HCBS) to 509,503 (402,438 in HCBS); and total Medicaid expenditures increased from $10.485 billion ($1.655 billion in HCBS) to $25.596 billion ($14.123 billion in HCBS).2 In 1992, 49.7% of combined ICF/MR and HCBS recipients lived in community settings; in 2003, 87%.2
Despite these commitments and the resulting expansion of LTSS, many people continue to wait for access to out-of-home services. In June 2003, it was estimated, based on the reports of 36 states maintaining such data, that an estimated 75,300 individuals with ID/DD were waiting for LTSS outside their family home.2 Access to services has been for some time a major challenge in LTSS management, but increasingly LTSS access is being reframed as a legal issue. The lack of access to services with "reasonable promptness" as required by Medicaid law is a primary complaint in a growing number of federal court cases.4 The role and commitment of states to assure an adequate workforce of DSPs to meet service demand of eligible and needy individuals is a growing aspect of these cases. Circumstances alleged to limit the ability to recruit and retain a sufficient workforce to meet the demand for community-based LTSS was a central aspect in Bell et al. v Biedess et al.5 In Bell, in August 2004, a U.S. District Court in Arizona ruled that Arizona was required to raise wages of DSPs because without doing so the plaintiffs would not receive the services to which they were entitled for want of DSPs to provide them. The growth in community LTSS, the increasing demand for community supports, and the challenges faced by states and service providing agencies, and by individuals and families, in recruiting and retaining sufficient numbers of qualified DSPs is becoming a significant policy challenge.
B. Changing Expectations in LTSS
Congress has addressed the needs of people with ID/DD in a variety of laws, including the ADA, the DD Act, the Rehabilitation Act, and other legislation. The first finding of the DD Act acknowledges "the right of individuals with developmental disabilities to live independently, to exert control and choice over their own lives, and to fully participate and contribute to their communities through full integration and inclusion in the economic, political, social, cultural and educational mainstream of the United States" (42 USC 15001 (a)(14)).
Realizing such rights with individuals who by definition have substantial functional limitations in the physical, social and/or cognitive skills of daily living often requires services and supports that compensate for and assist in overcoming the barriers to "full integration and inclusion." As Congress further noted in the DD Act, "there is an increasing need for a well trained workforce that is able to provide the services, supports and other forms of assistance required to enable the individuals to carry out these activities" (42 USC 15001 (a)(14)).
C. Changing Roles and Responsibilities in LTSS
The effects of LTSS system decentralization have been felt most directly in the increased responsibility, autonomy and required skills of DSPs. In 1982 there were a total of 15,700 different residential settings (excluding homes shared with family members) in which people with ID/DD were receiving LTSS from licensed or certified service providers, with an average 16 people with ID/DD per setting.6 In 2003, states reported 145,600 different residential settings (excluding homes shared with family members) in which people with ID/DD were receiving LTSS from licensed or certified service providers, with an average three people with ID/DD per setting.2 Similar changes have occurred in other supports, including, for example, substantial growth in the number of people with ID/DD who receive assistance to work in integrated jobs in typical work settings in the community. This decentralization of community support services has greatly increased the challenges faced by DSPs in fulfilling their roles. Increasing use of in-home services, supported living arrangements, and small group homes require much greater skill, judgment and personal accountability on the part of DSPs. DSPs must practice those skills with far less direct supervision and access to on-site consultation from professionals with advanced training in health services, psychology or other relevant disciplines than when DSPs worked predominantly in congregate care settings.7 This shift has produced roles with greater autonomy and responsibility, and increasingly this autonomy and responsibility is applied in support of persons with greater levels of intellectual, behavioral, health and functional impairments. As a result DSPs today are called on to provide medication supports, implement behavioral plans, teach new self-care skills, design and implement augmentative communication systems, and provide a wide range of other sophisticated supports that require substantial skills on the part of DSPs.
These demanding responsibilities are given primarily to paraprofessionals, that is, people without college degrees in a discipline relevant to their specific work responsibilities. The National Skills Standards Act of 1994 (Public Law 103-227) established an initiative to identify and establish national skills standards for 22 industries that were emerging as producers of major job growth for which higher education was not an essential aspect of job entry and success. The National Skills Standards for Direct Support Workers in Human Services were developed through an in-depth analysis of the knowledge, skills and attitudes needed by DSPs.8 The process confirmed that minimally competent DSP performance involved mastery of dozens of specific skills areas ranging from supporting people in understanding and realizing their basic rights to responding effectively to complex behavioral crises. A major challenge in assuring an adequate supply of DSPs to meet the growing demand will involve simultaneous attention to assuring that the supply of DSPs is not only sufficient in number, but also sufficient in skill and experience to meet the complex support needs of persons with ID/DD.
II. CURRENT AND PROJECTED SUPPLY OF AND DEMAND FOR DSPS
A. Overview of Supply of and Demand for DSPs
Current and projected number of persons with ID/DD needing LTSS. The demand for services and supports for individuals with ID/DD will drive the future demand for DSPs. The total number of individuals with ID/DD in need of residential, in-home and day supports (excluding special education), is expected to rise from an estimated 1,015,000 in 2003 to 1,400,000 in 2020, an increase of about 38%.9 The most significant predictable factors increasing demand for services and supports will be growth in the U.S. population; the effects of increased life expectancy of people with ID/DD and related survival rates of low and very low birth weight infants; and the aging of family caregivers with whom hundreds of thousands of adults with ID/DD currently live. Less predictable effects may include changes in public funding for LTSS, changes in entitlement and eligibility for LTSS, and/or changes in the nature (and attractiveness) of LTSS options. It should be noted, however, that within any conceivable scenario the rate of growth in demand for LTSS for persons with ID/DD will be substantially less dramatic than the increasing demand for LTSS among persons who are aged and disabled, because the growth in demand for LTSS among persons with ID/DD is much less linked to a particular age cohort (i.e., persons 80+ years old).
B. Factors Associated with Demand for DSPs
1. Family caregiving and DSP demand. It must be noted first that above all other potential factors, the unpaid "informal" caregiving of parents and other family members (and to a much smaller but often important extent, neighbors and friends) has an enormously important effect on demand for LTSS in the U.S. As they always have been, family members are currently the primary source of needed support to individuals with ID/DD. As Figure 4 shows, in 2003, there were an estimated 4.3 million individuals with ID/DD (about 1.5% of the U.S. population).10 Approximately 475,000 of these individuals were in residential support arrangements outside of homes shared with natural or adoptive family members (residential settings for persons with ID/DD, nursing facilities, foster homes). This includes an estimated 63,000 children and youth (17 years or younger) in residential and foster care settings, and 412,000 adults in residential settings, including 35,000 in nursing facilities. In contrast to the 475,000 persons with ID/DD receiving paid residential supports outside of family homes, there were an estimated 3,849,000 living with parents or other relatives, or in their own homes without ID/DD agency services (97.4% of all children; 78.4% of all adults). The large number of children identified with ID/DD might appear to suggest major impending demand for LTSS by 2020 (i.e., if they used LTSS at the same rates as currently identified adults (about 21.6%), there would be an additional 517,000 persons added to the LTSS systems). However, the substantial differences between children and adults in the estimated prevalence of ID/DD (3.3% and 0.9%, respectively) do not reflect a future "disability bubble" of significance in LTSS demand. The difference derives primarily from: (a) different definitions that Congress established for developmental disability among children and among adults that causes a much higher rate of children to fit the definition of developmental disability; and (b) the role that schools play in identifying large numbers of children as having intellectual disability during the school years for the purposes of providing supplemental special education, but whose labels disappear in adulthood as they are able to live without formal supports or recognition of disability.
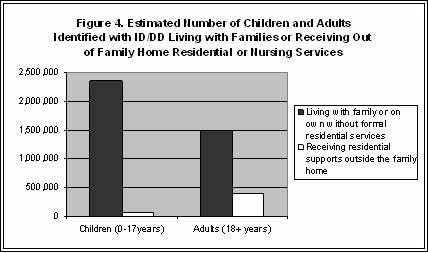
Figure 4 makes clear the importance of family caregiving to the sustainability of the national LTSS system, especially among those families that provide continuing support of adult family members.11 Neither should the demands accepted by these families be minimized. It is estimated that of the 1,043,000 adults with ID/DD who continue to reside with family members as adults,12 about half are unable to be left unsupervised for 2 or more hours at a time.13 The number of DSPs who would be needed to provide the ongoing and intermittent support required by these adults can only be roughly approximated, but the number of DSPs who would be required for those individuals who cannot be left unsupervised for more than 2 hours if they were not living with family members, could be conservatively estimated at nearly 600,000 full-time equivalent (FTE)* DSPs.14 It is more difficult to assess the impact of family caregiving in reducing LTSS need for children with ID/DD. Children today are relatively rarely placed outside the family home (an estimated 97.5% living with family).15 This tendency is much stronger today than in generations past (e.g., in 1965, U.S. public institutions housed 95,000 children and youth with ID/DD).16 It is largely a product of special education in local schools, Supplemental Security Income (SSI) and Medicaid for poor families, and a growing array of in-home supports for parents. Despite growing recognition of the value of family care for persons with ID/DD, notable changes in family support services would likely be associated with changes in LTSS demand.
2. Demographic and health related factors. Even assuming a continuing significant commitment of families to primary caregiving roles for persons with ID/DD, there will be a steadily increasing demand for LTSS between 2003 and 2020. LTSS demand will be affected by increasing life expectancy and, therefore, increased service years per individual with ID/DD. Data shows that for individuals with Down syndrome, spina bifida, and other conditions associated with ID/DD, recent medical advances and improved access to high quality, community medical treatment has resulted in notable, sometimes dramatic increases, in longevity. As an example, researchers from the Centers for Disease Control and Prevention using death certificates of nearly 18,000 persons with Down syndrome computed that, between 1983 and 1997, the average age at death of persons with Down syndrome increased from 25 years to 49 years.17 Each year of increased average lifespan for persons with ID/DD translates roughly to a 2.4% increase in demand for DSPs because of the associated increase in service years they will require (i.e., if the current average number of service years of persons with ID/DD is increased from 42 to 43, the corresponding increase in DSP demand will be 2.4%).18
The growing number and increasing survival rates of low birth weight infants will also affect LTSS demand by 2020. Survival rates of low and very low birth weight ("premature") children have been increasing since the 1980s as have been the total number of such births. There is a substantial association between low birth weight and cognitive and physical impairments, with children weighing less than 3.5 pounds at birth being about three times more likely to experience neuro-developmental impairments. Although these impairments are to some extent mitigated by access to good quality early intervention and education, the trend to increasing numbers of low birth weight children surviving into adulthood will have long-term effects on LTSS demand.19, 20
There are other factors that may have countervailing effects on LTSS demand by 2020. These derive from improved public health practices, such as reduced lead exposure or dietary supplementation. (Effects on childhood incidence are not generally felt on LTSS demand until the children reach adulthood.) There is, however, evidence that the introduction of folic acid supplements to the food supply has resulted in notable reductions in neural tube defects (a 31-34% reduction in spina bifida-affected pregnancies according to two studies)21 that will affect LTSS demand by about 2020. Advances in genetic screening and related parental decisions have the potential of affecting the prevalence of ID/DD in the future as well. Finally it is still unclear whether the growing identification of certain conditions, most notably autism, represents new levels of incidence, or less significantly, changing practices in diagnosis. If the former, there are obvious implications for prevalence of ID/DD and the related future demand for LTSS.
3. Social and administrative factors. Social and administrative factors could also have a notable effect on LTSS demand by 2020. In the early and mid-1970s Congress instituted a number of programs of enormous significance to children with ID/DD and their families (e.g., SSI, Medicaid health and long-term care services, special education entitlement). Along with these important benefits a growing range of state and local family support services were developed, as was an increased appreciation by health and social service professionals of the benefits of family life for persons with ID/DD. These new supports and improved understandings led to major decreases in the number of children and youth (0-21 years) with ID/DD living outside of family homes. The number of children and youth receiving residential supports outside natural, adoptive or foster family decreased from an estimated 90,942 in 1977 (36.8% of all residential service recipients) to an estimated 25,842 in 1997 (7.6% of all residential service recipients).15 The implications for LTSS demand are notable, but are linked to the family and community supports that allowed people with ID/DD to remain at home and family members to live more typical lives when they did. There are also currently great variations among states in the amounts and types of LTSS available to persons with ID/DD (e.g., states provide out-of-home residential supports across a range from 60.3 persons with ID/DD per 100,000 of total state population to 301.0 per 100,000).2 Because it is unlikely that such variations relate strictly to actual differences in prevalence of ID/DD in the various states, federal or court impositions of expectations for particular levels of LTSS access in all states could lead to increased LTSS development in certain states. On the other hand, in the absence of such requirements to access, fiscal difficulties could cause some states to reduce current levels of LTSS or redefine persons eligible for them. In other words, there are numerous other factors than need that could affect supply and demand of LTSS.
4. Summary of estimated changes in demand for LTSS. Despite the variety and ambiguity of factors potentially affecting LTSS demand by 2020, based on information currently available and assuming that current tendencies and trends will not be altered in major ways, HHS estimates that there will be approximately 1.4 million persons with ID/DD needing LTSS in 2020. These estimations of current and projected demand are shown in Table 1 according to LTSS service setting.
| TABLE 1. Current (2003) and Projected (2020) Demand for LTSS for Persons with ID/DD | ||
| Service Setting | Persons Needing Each Specific Service | |
| 2003 | 2004 | |
| State Institutions | 42,834 | 19,3091 |
| Residential in Private/Community Settings | 359,446 | 687,9382 |
| Nursing Facility | 35,005 | 02 |
| Waiting | 75,288 | 02 |
| Supports in Family Home | 500,004 | 690,0053 |
| Vocational/Day Services | 465,000 | 641,7004 |
|
||
C. Translating Current and Projected LTSS Demand into DSP Demand
The 2003 distribution of LTSS recipients by service types, the projected growth and redistribution of LTSS recipients, and the current and assumed stable staffing ratios for service types have been used to estimate the 2020 demand for DSPs. Because this report focuses on the supply of DSPs needed to meet demand, estimates of "demand" include persons waiting for services. Current DSP staffing ratios for individuals with ID/DD yield an estimate of 463,573 FTE DSP positions in residential services in June 2003 with another 85,089 needed for persons waiting for services. In anticipation of movement to the ID/DD community service system, community service staffing ratios were applied to the 35,005 persons with ID/DD in nursing facilities yielding an additional 39,556 DSPs. (These were not added to the total of vocational/day service recipients because it was assumed, as required in the OBRA 1987 nursing home reforms, that nursing facility residents with ID/DD are already receiving appropriate day services within the ID/DD system.) It is estimated that there are currently 160,890 DSPs supporting 465,000 vocational and day program participants. It is estimated that there are 125,001 DSPs providing in-home family supports to 500,004 individual with ID/DD and their families. In total, an estimated 874,095 FTEs of direct support are currently needed to meet the demand for DSPs for persons with ID/DD.22
| TABLE 2. Current (2003) and Projected (2020) Demand for DSPs for Persons with ID/DD | ||||||
| Service Type | 2003 | 2020 | ||||
| Current | Ratio1 | DSPs | Current | Ratio | DSPs | |
| State Institutions | 42,835 | 1.34 | 57,399 | 19,309 | 1.34 | 25,874 |
| Private/Community | 359,446 | 1.13 | 406,174 | 687,938 | 1.13 | 777,370 |
| Persons Waiting | 75,288 | (1.13) | (85,075) | 0 | 02 | |
| Persons on NFs | 35,005 | (1.13) | (39,556) | 0 | 02 | |
| In-Home Family | 500,004 | 0.25 | 125,001 | 690,005 | 0.25 | 172,501 |
| Vocational/Day | 465,000 | 0.346 | 160,890 | 641,700 | 0.345 | 221,387 |
| Total | 874,095 | 1,197,132 | ||||
|
||||||
As shown in Table 2, an increase of 323,037 FTEs of DSP positions (about 37%) is projected between 2003 and 2020. This projected growth rate of DSPs is slightly less than the projected growth rate in LTSS demand (38%) based on the assumption of continued reductions in institutionalized populations. The projected 38% growth rate in LTSS demand between 2003 and 2020 is actually less than the actual rates of LTSS growth in the recent past. For example, between 1987 and 2003 recipients of residential supports outside their family homes, the service generating most DSP demand, grew by 48%,2 reflecting a rapid rate of deinstitutionalization that is not likely to occur in the future. Although the projected 37% growth in DSP demand through 2020 is projected to be relatively modest, it will be occurring at a time, as Congress noted in Title III of the DD Act of 2000, when the supply of workers who have traditionally filled DSP roles, mostly young adults, is expected to increase only slightly. During that period persons 20-39 years old are expected to grow by 7.2%, while the number of needed DSPs is expected to grow by 37%.23
The demand for DSPs will likely accelerate somewhat after 2020, as the baby boom generation approaches an age where their caregivers are very elderly, and as beneficiaries of medical advances of the past generation move into and through adulthood when LTSS demand steadily grows. This increase in DSP demand is likely to be substantially exacerbated by the beginning of a substantial growth in DSP demand to meet the LTSS needs of the baby boom itself, the leading edge of which will reach 80 years in about 2025. The projected increase of 37% in DSP demand through 2020 increases to a projected 1,832,612 DSPs in 2040, an increase of about 110% more than in 2003.24 This reflects an increase of 51% in the estimated growth in out-of-family residential supports needs due to the projected 112% increase between 2020 and 2040 (based on Census estimates of the U.S. population) of parents of adults with ID/DD who have reached (or exceeded) 80 years, and the estimate that 20% of established rates of growth in residential service demand is associated with aging family caregivers.
D. Supporting the Continuing Essential Roles of Informal Caregivers
Even as the demand for DSPs grows, so too will the number of family members engaged in providing informal supports to individuals with ID/DD. Economic and social circumstances permit families to sustain the current level of caregiving,25 if the social, medical and administrative factors that cause and define ID/DD remain relatively constant, the proportional distribution of children and adults within the LTSS systems in 2020 should remain quite similar to 2003. It should be expected, however, that all of the factors above held relatively constant, there should be a notable increase between 2020 and 2040 in LTSS and DSP demand among persons with ID/DD. This will reflect the aging of the population of both caregivers and service users. With greater proportions of the ID/DD population moving through adulthood and growing proportions of family caregivers reaching advanced ages, increased LTSS and DSP demand will follow.
Figure 5 shows how the estimates of persons with ID/DD receiving LTSS, and the numbers of DSPs estimated to be needed to meet that demand, increase over time the total LTSS recipients and assumptions summarized above (i.e., the absence of major social, medical or policy changes). The number of DSPs will rise modestly, more rapidly than the projected numbers of persons with ID/DD. However, it is essential to recognize that the number of informal caregivers will continue to grow as well. Under current conditions and expectations, the estimated number of persons with ID/DD supported only by informal caregivers (i.e., those with ID/DD who are neither receiving nor awaiting formal LTSS) will grow from 3.21 million in 2003 to 3.47 million in 2020 to 3.75 million by 2040. It is further expected that approximately half of all persons with ID/DD who receive LTSS will do so while sharing a home with a family member. Without question the roles played by family members and other "informal" support providers in assisting persons with ID/DD who are not receiving formal services or who are receiving LTSS while living with family members are of the highest importance to sustaining the current system of LTSS for persons with ID/DD.
E. Uncertainties in Long-Term Projections of LTSS and DSP Demand
Because the uncertainties in predicting the occurrence and significance to LTSS demand of important economic, social and medical factors, such as the sustained engagement of informal unpaid caregivers, it is difficult to project with confidence estimates of potential demand for DSP workers in distant future decades. Many factors add to the uncertainty to such long-term projections. These include:
1. Continued commitment to developing and financing HCBS. In recent years there has been a concerted movement to ensure that individuals with ID/DD have opportunities for supported home and community lives. The Supreme Court's Olmstead decision recognized a national commitment to assure that individuals who can be supported in the community should be given the choice to live and receive LTSS in a community setting appropriate to the individual as state funds permit. President Bush's New Freedom Initiative further recognized a right to full and open access to community life. As community options grow so too does demand. This Report has assumed that demand and "need" will be viewed as essentially equal; that is, in the future, waiting lists will not be a predominant feature of LTSS systems. This may or may not bear out.
2. Changes in public funds available for LTSS. Growth in access to LTSS in the past decade has been largely fueled by increased Medicaid funding. Between FY 1991 and FY 2000, combined state and federal real dollar expenditures for LTSS for persons with ID/DD increased by 45% from $20.3 billion to $29.3 billion (in 2000 dollars). Of this total, state expenditures (in 2000 dollars) increased from $12.7 billion to $14.7 billion (15.9%), while federal expenditures increased from $7.6 billion to $14.8 billion (93.5%).26 Most states are now largely dependent on new state allocations for Medicaid-financed services to obtain federal matching funds. Depending on growth in LTSS funding, assumptions about the expansion of services to meet demand, stability in staffing ratios, and so forth, DSP demand well vary. At the same time, individuals with ID/DD and the LTSS they need have generally been more often protected in budget difficulties than many other expenditures. Any changes in state or federal Medicaid policies could potentially affect LTSS and related DSP demand.
3. Changing approaches to providing LTSS. In the estimates contained in this Report, it has been assumed that models of support and the mixes of out-of-home, in-home and informal supports currently needed (provided and awaited) will remain generally stable, with adjustments for variation associated with age. There are evolving models of LTSS that could affect DSP demand. Consumer-directed support models in which individuals with ID/DD and/or their family members control the funding that has been allocated to meet their needs, and use those funds to purchase the supports they want and need from individuals or organizations of their choice. Often the supports purchased by individuals with ID/DD and family are provided by friends, neighbors, family members and others who are known to the individual and family. Such approaches offer freedom to consumers. Under certain conditions their growth could increase significantly and the effects on DSP demand could be significant.
4. Changes in the regulation and expectations in LTSS. DSP demand is largely established by the expectations of the number of persons needed to provide the amount of needed LTSS at an acceptable level of quality. In recent years there have been questions raised in a number of forums, including Congressional hearings (Wyden, 1993), GAO reports (2003), and newspaper exposés throughout the U.S. about whether services as presently organized and delivered are of adequate quality and quantity to assure the basic health and safety of persons with ID/DD.27 Continuing concern about the quality of services could affect demand for a supply of DSPs.
5. Changes in prevalence of ID/DD. The assumptions made in this Report to Congress regarding the prevalence of ID/DD, as it relates to modest increases in longevity of persons with ID/DD, in the occurrence and survival of low birth weight/very low birth weight, in access to and decisions made based on genetic screening advances, in the effects of dietary supplements, reduced exposures to environmental toxins, and so forth are, of course, assumptions. The longer the period of projection, the less accurate these are likely to be.
F. DSP Demand and Supply and the Relative Contributions of Recruitment and Retention
1. Growth in FTEs needed is a small part of meeting DSP demand. To this point, this Report has focused on the projected growth in LTSS demand and the growing number of FTE DSP positions needed to meet that demand. It has been estimated that on average about 19,000 additional FTEs of direct support will need to be added each year to meet growing demand. In reality, recruiting an average of 19,000 DSPs each year to provide for the growth in LTSS demand is a very small part of the total number of DSPs who will need to be recruited each year. Given the current national average annual DSP turnover rate of approximately 50%, the estimated 19,000 DSPs who will need to be recruited on average each year to accommodate growth in demand will make up only 4% of the total required DSP recruitment. At current rates of turnover, 96% of all DSPs hired between 2003 and 2020 will be hired to replace DSPs who leave existing positions (and the people with ID/DD they were supporting).
2. Rates of DSP turnover in LTSS. There have been no national studies of DSP turnover during the past decade, but there have been many smaller scale state and local studies. Twenty-six studies of DSP turnover conducted in 1998 or later were identified for this Report. These studies computed DSP turnover for residential/in-home community services; vocational and/or day services; or for combined residential/in-home and vocational/day service.28 These studies and their findings are summarized in Table 3.
| TABLE 3. DSP Turnover in Residential/In-Home and Vocational/Day Services, 1998-2003 | ||
| Setting Type | Number of Studies | Average Rate |
| Residential/In-home | 11 | 53.6% |
| Vocational/Day | 6 | 46.0% |
| Both | 9 | 48.1% |
| Combined Average | 26 | 50.0% |
3. Retention is a key component to meeting increased DSP demand. In terms of meeting the growing demand for DSPs, many argue that it is important to consider first how to respond to the problem of retention than to focus initially on ways to expand recruitment beyond current levels. The reasons for doing so are not simply limited to assuring sufficient numbers of DSPs, although studies in six states and a survey of the membership of the American Network of Community Options and Resources (ANCOR) indicate national DSP vacancy rates of about 10-11%.29 Staff turnover, as will be explained subsequently, has negative effects on the lives of people with ID/DD. Although challenging, it seems important to note that if DSP turnover in LTSS were reduced from 50% to 35%, growth in LTSS demand could be met over the next decade with current patterns of recruitment. It is, in fact, extremely important given the existing challenges in recruiting sufficient numbers of DSPs to look to ways of making small reductions in current average rates of turnovers along with efforts to recruit new DSPs each year. Retention efforts will contribute to maintaining the skills and experience that are essential to DSP performance. Such a focus will be especially important given that the number of persons in the age group from which DSPs have been traditionally drawn, young adults of 18-39 years, will grow by about 7% between the present and 2020 as compared with about 37% increases in demand for DSPs.
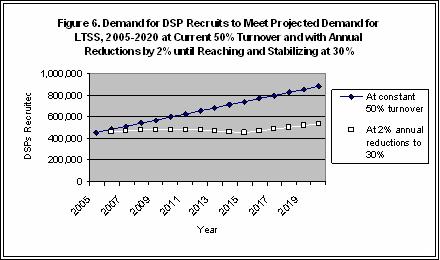
Figure 6 shows the relative effects on needed recruitment to meet projected DSP demand at the current 50% annual rate of DSP turnover and with a 2% annual reduction in DSP turnover over the next 10 years, and then maintenance at an annual average of 30% (i.e., 50% in 2005, 48% in 2006, reaching 30% in 2015 and then remaining at 30% through 2020).
The effects of such an accomplishment are notable. Meeting projected demand for DSPs in 2005 at current 50% turnover rates will require an estimated 456,000 new recruits. By 2015, an estimated 741,000 new DSPs will need to be recruited to meet growing service demand, but primarily to replace DSPs leaving their jobs. Relatively modest, but not simple, accomplishments in improved DSP retention could make enormous differences in the capacity to meet the future demand for direct support. As Figure 6 shows, by gradually reducing the current 50% rate of DSP turnover by 2% a year, the rates of DSP recruitment to meet current needs would be very nearly sufficient to meet the projected needs through 2020.30 By 2015, when the nation's demand more LTSS begins to crescendo as the baby boomers reach 70 years, new recruits for DSPs for persons with ID/DD would be nearly 289,000 fewer than under current patterns; by 2020, about 346,000 fewer. Although achieving such levels of reduced DSP turnover represents a significant challenge, given the demographics of an aging society in the absence of such improvements, the challenges of meeting the projected future demand for DSPs through recruitment alone will be even greater.
Section Note
| * | An FTE refers to the number of hours of required DSP work equal to standard full-time employment (usually 40 hours). In practice about one-third of all DSPs work part-time so that two or more DSPs might work to equal one FTE. |
III. FACTORS ASSOCIATED WITH THE RECRUITMENT AND RETENTION OF DSPS TO MEET CURRENT AND PROJECTED FUTURE DEMAND
Staff turnover is a significant driver of demand for DSPs in LTSS. Understanding the factors associated with turnover is essential because reducing turnover can substantially reduce the demand for DSPs for LTSS in coming years (see previous section). This section reviews what is known about those factors and about interventions that could be shared with organizations and individual employers to reduce recruitment and retention challenges.
A. Organizational Factors
Researchers studying turnover in LTSS for persons with ID/DD have focused on factors that drive turnover at an organizational level. Early studies reported that higher turnover was associated with having younger employees, less tenured employees, lower wages, less favorable staff ratios, programs that are newer, programs supporting individuals with more intensive needs, and programs with fewer staff members per site (see Table 4). Turnover tended to be higher in urban areas and in areas with lower unemployment rates (because employees could more easily find other jobs). While these early studies were helpful, they did not examine turnover in the context of more than one factor at a time.
Recent studies have used more sophisticated methods to study factors associated with turnover. Five statewide and three national studies investigated turnover in community LTSS for persons with ID/DD looking at multiple factors at the same time. DSP turnover was associated with pay (appearing in five of the eight studies), support needs of individuals (four studies), facility size, number of DSPs or ratios of DSPs to people supported (four studies), ICF/MR certification (two studies), urban versus rural location (two studies), how long the site had been open (two studies), and eligibility for paid leave or health benefits (two studies). Other factors associated with turnover were age of people supported, public versus private operation, supervisor tenure, unionization, hours of training provided, and the use of shift versus live in employees.
| TABLE 4. Factors Associated with Turnover from Correlation and Multivariate Studies Conducted in LTSS for Persons with ID/DD | ||
| Category | Correlations1 | Multiple Regression Analyses2 |
| Staff Characteristics |
|
|
| Job Experience |
|
|
| Conditions of Employment |
|
|
| Characteristics of People Supported |
|
|
| Service Model Characteristics |
|
|
| Employment Context |
|
|
|
||
Several studies have identified a number of factors associated with staff turnover among DSPs: (1) As deinstitutionalization continues, the wage gap between institutional (mostly state employed) DSPs and community (mostly privately employed) DSPs has been associated with substantially higher turnover rates in community settings (see Table 5); (2) Community settings were opened much more recently than institutional settings (newer programs experience higher turnover); (3) eligibility for and attractiveness of benefits (turnover is higher in settings that provide benefits to fewer employees); (4) the small size of the community homes (turnover is higher in smaller sites); and (5) the less favorable staff ratios in community homes (turnover is higher in settings with less favorable staff ratios).
| TABLE 5. DSP Wages and Turnover Differences for Community vs. Institutional LTSS | ||
| Public Institution | Community Services | |
| 1979 Starting wage1 | $4.01 | $3.49 |
| 1990 Average wage2 | $8.72 | $5.97 |
| 1998-2002 Average wage3 | $11.67 | $8.68 |
| 2002 Average turnover | 28%4 | 50%5 |
|
||
B. Employee Characteristics and Work Attitudes
Researchers have developed sophisticated models that describe factors associated with whether an employee will choose to stay or leave an organization, and to learn whether the factors identified in various models actually help explain why employees leave. Table 6 summarizes the factors that have received the most study. Unlike the ID/DD literature, which focuses on facility characteristics associated with turnover, these studies primarily describe factors associated with turnover for individual employees. As was true in the ID/DD research, this research documents the association between low wages and higher turnover. It also shows that certain employee characteristics (e.g., age, education and number of dependents), employee intent to leave, employee tenure, and employment context (unemployment rate and perceptions of the availability of other jobs) are associated with turnover. More importantly, however, these studies identify employee attitudes that predict turnover (e.g., having unmet expectations about the job, commitment to the organization and its mission, satisfaction with various job characteristics, and satisfaction with supervisors). These employee attitudes can be changed by using more effective human resource practices. The next section describes strategies employers can use to reduce turnover and improve recruitment success by addressing the factors that contribute to improving employee experiences. A major barrier to using those effective strategies is that frontline supervisors, organizations and individual employers often do not know about the strategies or know how to implement them.
C. Results of Recruitment and Retention Challenges For Organizations
DSP turnover and associated recruitment challenges have far reaching negative impacts on organizations. The majority of administrators in community LTSS for persons with ID/DD experience significant difficulty in finding DSPs to fill vacant positions.40 Recruitment problems can result in increased overtime of existing staff. For example, in Alaska, organizations reported spending $353.33 per DSP position per year on overtime.41 In Minnesota, the average in 2000 was $300.80 per DSP position per year.42 In Kansas, the average per DSP position per year was $476 in 2003.43 Another cost of recruitment is advertising expenses. Annual advertising costs ranged from $68.64 per DSP in Alaska to $496.83 per DSP in Minnesota.44 Besides the cost of recruiting new workers, high turnover also results in higher training costs.45
High turnover can also have a negative impact on DSPs. If replacement workers are not found quickly for those who have left, the remaining DSPs will experience an increased workload. While this is not troublesome on an occasional basis, the chronic vacancy rates reported by many providers suggest that DSPs are working under increased pressure most of the time. This can cause remaining DSPs to become frustrated and contribute to job burnout, further contributing to the retention challenge.46
| TABLE 6. Factors Associated with Turnover Across Industries from Turnover Models and Meta-analytic Studies | ||
| Category | Turnover Models1 | Meta-Analyses2 |
| Employee Characteristics |
|
|
| Employee Attitudes |
|
|
| Intent to leave |
|
|
| Job Experience |
|
|
| Job Characteristics |
|
|
| Employment Context |
|
|
|
||
IV. IMPLICATIONS OF FAILING TO MEET CURRENT AND PROJECTED FUTURE DEMAND FOR A SUFFICIENT NUMBERS OF QUALIFIED DSPS47
A. For Current Service Recipients
It is not possible to consider the quality of community services for people with ID/DD without attending to the status of the direct support workforce providing those supports. The quality and stability of DSPs are of fundamental importance to the well-being of people with ID/DD. As the U.S. Secretary of Labor, Elaine Chao, observed on September 24, 2002, "The paraprofessional long-term care workforce is the cornerstone of America's long-term care system . The fundamental, long-term challenge is how to develop a committed, stable pool of employees who are willing, able and skilled to provide quality care."48
The challenge is evident in a survey of administrators in Pennsylvania in which 79% reported duties and responsibilities of DSPs had increased, 75% said the medical fragility of people served increased, and 70% said behavioral problems of people served had increased over the past 10 years.49 However, only 14% said the quality of the DSP applicant pool had increased, while 30% said it had stayed the same, and 56% said it had decreased. The discrepancy between the increasing difficulties of DSP roles and declines in the quality of the applicant pool from which DSPs are drawn may have been a factor in creating the conditions that have led to reports and exposés on abuse and neglect from regulatory agencies and newspapers around the U.S.50
Perhaps the most detrimental workforce challenge is the high turnover of DSPs, which hinders the development and maintenance of relationships, the development of mutual respect between DSPs and individuals who receive support and their family members, and the development of trust between supported individuals and every new DSP that enters their life. High vacancy rates, an increased use of overtime, and DSP turnover rates averaging 50% or more have negative effects on the quality of supports provided.47 Without DSP continuity, quality, commitment, and competence, the opportunity for persons with ID/DD to become full citizens and active community members is greatly diminished. The nature of the current workforce crises makes it difficult for organizations to provide even basic support such as help with self-care and medical support. In a 2002 review of 50 years of research on DSP turnover and factors associated with it, Hall and Hall summarized five studies that showed that DSP performance had direct affects on challenging behavior, communication, treatment success, and successful placement in community residential settings.51 Turnover produces a continuing loss of people trusted for basic and often intimate assistance. People receiving supports become more vulnerable because the people caring for them do not know their unique needs and vulnerabilities. A 1999 report by the California State Auditor concluded that staff disruptions from high turnover and from difficulty replacing DSPs lead to consumers receiving "less-than-optimal" services to facilitate their inclusion into the community.52
Vacancies are causing families with members with ID/DD in the family home to do without basic family support services (personal assistance, respite care, etc.) as available DSPs are first allocated to residential and vocational programs for which there are no alternative care providers.42 Families caring for members with ID/DD in their home have reported more stress, income and job loss, and severe financial problems than other families.53 As the California State Auditor observed, "Lengthy job vacancies create further disruptions in services. Providers need almost 3 months to fill openings and new direct care staff require time to get to know the consumers and learn their needs. Continually establishing new relationships affects consumers as well; they regularly experience the loss of continuity in their services as well as the personal loss of familiar staff who assist them"(p. 2).52
A broad based study of HCBS services in Minnesota reported many impacts of workforce challenges on individuals with ID/DD and their families.54 While service coordinators rated residential or in-home services and the protection of basic rights and dignity as the highest quality components of the Minnesota system, they rated the availability of sufficient numbers of DSPs, the skills of DSPs, and the information sharing practices regarding quality assurance as the lowest quality components. They also reported that reducing staff turnover was needed to improve services in residential or in-home service settings (29%), and that reducing staff turnover would help improve the quality of services (38%). Similarly, 36% reported that reducing staff turnover was needed for individuals receiving vocational supports. In a separate survey of service coordinators, the three most serious problems for Minnesota's HCBS waiver program were: (a) the high number of DSPs in the lives of consumers (45% said the problem was "extremely serious"), (b) recruiting family foster care providers (46% said it was "extremely serious"), and (c) recruiting residential and in-home staff (35% said it was "extremely serious"). In this study, overall quality of life as rated by service coordinators was higher for individuals receiving services in sites with lower vacancy rates and in settings that paid higher DSP wages. In residential settings, individual quality of life was higher for people who had less severe intellectual disability. Almost all county HCBS administrators interviewed reported concern about a decline in the quality and quantity of staff hired. Recruitment problems were cited as affecting the development of sufficient community service programs to fully meet service demand. Individuals with ID/DD who worked in vocational settings with lower vacancy rates were more satisfied with their services.47
B. For Families
Overall 50% of families in the Minnesota HCBS Waiver Evaluation study with members receiving residential services reported turnover in the residential setting was a problem; 48% of families receiving in-home supports said turnover was a problem as did 35% of respite services recipients. Twenty-nine percent of responding families said turnover was a problem in vocational settings. Families related a number of personal experiences behind these statistics (58 in all, 34 of which were negative). Among the "negatives" were, "If I need 15 days of care provided for my son in a month I'm lucky to get 2 or 3 days covered;" "My biggest concern is getting good/caring staff. Pay is poor, turnover great. Training of staff and follow-up [is] sometimes weak;" and "As a single mother I have lost three jobs due to missing hours and work because I cannot find PCA care or they call in and don't show up." Among the more positive comments were, "Staff make the difference. When staff is good, life is good for my son;" "He has had some excellent, consistent direct care staff;" and "The relief obtained from having someone to take over a few hours a day enables us to keep refreshed and relieved."47
Families also responded to a series of questions regarding access to needed supports and services. Regarding aspects of service access, families were asked whether a statement was true most of the time, sometimes or rarely. Among families receiving respite services, only 54% said the supports met their needs (46% said the services met their needs only sometimes or rarely); only 46% reported they received the hours of service they were authorized to receive; and only 46% said supports were available when they needed them most of the time. Among families who received in-home supports, 70% said the supports met their needs; and 56% said supports were available when they were needed (44% reported that needed supports were available only sometimes or rarely). Among families whose family member received vocational supports, 82% said the supports were available when needed. The percent of families reporting that supports were available most of the time or when needed in time of crisis was substantially lower for family support recipients than for other service types. These differences support the observation that in times of insufficient staffing for the service system as a whole, the first to experience support limitations are the families who care for family members at home. Families were more satisfied with information and communication when their family member worked in larger vocational sites, in sites with lower vacancy rates, and in sites that paid higher wages to the DSPs. Family satisfaction with DSP quality was higher in vocational sites that had lower vacancy rates.
C. For Future Service Recipients
In some communities, organizations are pulling back from developing much-needed new support services due to the lack of skilled applicants to fill DSP positions.43 If the numbers of families and individuals with ID/DD needing LTSS continues to grow, as suggested earlier in this Report, having providers cut back on services will cause substantial problems. This inability to create new and timely services results in people who need support services remaining on waiting lists, to the detriment of those individuals and their families. Industry stakeholders acknowledge that this lack of qualified employees is a significant barrier to person-centered support services and that a high-quality workforce is essential in creating a system that provides high-quality support to everyone.55 There is also concern that the increasingly complex needs of people who receive supports in home and community-based settings cannot be met by the people who are currently being recruited and employed in the field.56
V. INITIATIVES AND INNOVATIONS UNDERWAY TO RESPOND TO THE CURRENT AND PROJECTED FUTURE DEMAND FOR QUALIFIED DSPS
There are numerous initiatives currently underway at the federal, state and local levels that respond to the current and projected future demand for sufficient numbers of qualified DSPs to support individuals with ID/DD. This section of the Report provides a brief description of many of these initiatives and activities. Those reported specifically focus on community human service organizations that provide services to people with ID/DD.
A. Federal Agencies
HHS and a number of other federal agencies have several initiatives underway to address the challenges of the community direct support workforce. Progress is already being made in a few states to address issues such as wages and benefits, training, and career development. In this section, there is a focus on federally initiated activities already underway that are aimed at developing a committed and qualified pool of DSPs in the range of community human service settings providing services specifically to ID/DD. These activities are grouped by agency/office and provide a brief description of each activity.
1. Department of Health and Human Services (HHS). HHS has embarked on a number of important initiatives.
Centers for Medicare and Medicaid Services (CMS)
Demonstration to Improve Direct Service Workforce Grants -- CMS has awarded ten demonstration grants aimed at helping states, regions or local partnerships demonstrate effective recruitment, training and retention activities for direct service workers who provide personal assistance to people with disabilities who need help with activities of daily living. Several of the grants seek to test offering health insurance benefits to workers to determine whether health benefits will improve worker retention. Others are developing educational materials, training of service workers, mentorship programs and other activities. Almost all of these long-term care projects are being carried out in services to the aging population and people with disabilities who utilize personal care and home health services. Only a few of these projects specifically target activities concerning DSPs who work in community settings with persons who have developmental disabilities.
Administration on Developmental Disabilities (ADD)
Projects of National Significance (PNS) -- Through its PNSs, ADD provided seed funding for two national internet-based curricula designed to improve DSP competence and to support more effective recruitment and retention of DSPs. One funded project developed the introductory courses for the College of Direct Support (CDS). The CDS is a multi-media internet-based curriculum that is designed to train DSPs throughout the U.S. Each course in the CDS is nationally validated and reviewed by a panel of content and training experts. The electronic platform is constructed to allow states and organizations to annotate each page as a means of customizing the curriculum content to reflect state and organizational policies. The project, initiated with ADD funding, is a partnership between the University of Minnesota's Research and Training Center on Community Living, MC Strategies, Inc., and the Sertoma Center. Revenues from curriculum sales now sustain dissemination, expansion and updating of this curriculum. Another ADD PNS resulted in the development of the College of Frontline Supervision (CFS). The CFS is an internet-based training curriculum designed to train Frontline Supervisors of DSPs how to most effectively recruit, train and retain DSPs. This curriculum is delivered on the same platform as the CDS.
Commissioners National Conference on Quality -- ADD sponsored a national conference in 2003 on quality in community human services for people with developmental disabilities. An entire track within this national conference was devoted to addressing the challenges of finding, keeping and adequately training DSPs. This was the first national conference with a distinct focus on the connection between a stable and competent DSP workforce and the quality of community human services provided to persons with ID/DD.
University Centers on Excellence in Developmental Disabilities -- ADD funds University Centers for Excellence in Developmental Disabilities throughout the U.S. These centers are designed to provide outreach training, technical assistance and research in the area of developmental disabilities. Each center has interdisciplinary training programs in the area of developmental disabilities. Many centers target some of their training activities and curriculum development toward DSPs who work in community human services.
Governor's Planning Councils on Developmental Disabilities -- Governor's Planning Councils on Developmental Disabilities are funded in each state. These councils are designed to provide policy guidance and support to state governments regarding persons with ID/DD. While not all councils embark on initiatives to address DSP issues, many councils do support training and technical assistance projects that target DSPs designed to improve DSP skills or to address issues such as recruitment and retention difficulties at the state level. Such councils have provided significant leadership in funding projects to assist in understanding the challenges of DSP competence, recruitment and retention as well as trying to identify successful interventions to address these challenges.
2. Department of Labor (DoL).
Community Support Skill Standards (CSSS) -- The DoL created an initiative in the mid-1990's to develop skill standards for emerging fields where there were high numbers of entry level positions. One industry targeted for this initiative was the community human services industry. In 1996, the CSSS were developed. These skill standards were derived from a comprehensive job analysis that was nationally validated. Since their development, the CSSS have served as a tool to create curriculum and career paths in many states (e.g., California, Ohio, Tennessee) and organizations (e.g., ACR/NCR in Maryland, SPIN in Pennsylvania). The CSSS also serve as a foundation for the targeted skill development in the CDS.
Direct Support Specialist Apprenticeship Standards -- DoL administers a national system for registered apprenticeship training programs that consist of structured on-the-job training and related academic, theoretical instruction tailored to industry requirements. Primarily individual employers, employer associations, or partnerships between businesses and labor unions, with involvement of education providers, such as community colleges, operate the programs. DoL has recently certified several Direct Support Specialist Apprenticeship programs including the Mid-Hudson Coalition in New York, Wyoming WINS program and the Ohio Paths program throughout Ohio.
DoL Workforce Development Network/ANCOR Pilot Programs -- In May 2004, DoL and ANCOR embarked on pilot programs to respond to the national crisis in providing a sufficient and qualified workforce of DSPs for persons with developmental disabilities. The pilot programs are attempting to develop an effective program model that will provide screened and trained direct support candidates to private providers of community services by integrating components of the DoL public workforce development network (One Stop Career Centers, Job Corps, etc.) with prospective employers in community service organizations. The initial four states in the pilot programs are Kentucky, Maine, Arizona and New York. ANCOR, DoL's partner in these programs, represents more than 800 providers of services and supports to nearly 400,000 persons with disabilities.
3. Department of Education (DoE).
National Institute on Disability Rehabilitation Research (NIDRR)
Research and Training Center on Community Living (RTC/CL) -- RTC/CL supports a long standing research, training and technical assistance program targeted at DSP career development and tenure. Current projects funded by RTC/CL include: (1) identifying national norms for DSP turnover, satisfaction and intent to stay on the job at 90 days; (2) a comparative analysis of the direct support turnover, vacancy and training issues between traditional provider driven services and individually directed services where the person and his/her family direct their own budgets; (3) Realistic Job Preview (RJP) effectiveness study which looks at how effective the use of RJPs is at reducing early turnover (within 90 days) at the organizational level; (4) best practice identification case studies -- uncovers and studies similarities and differences in emerging and effective practices designed to improve DSP retention and competence; (5) exploration of selection tools which can be used to screen potential DSPs who are applying for positions; and on-going analyses of secondary data sets related to DSP workforce trends and issues. In addition to these research projects the RTC/CL also provides technical assistance and outreach to states and others regarding DSP issues.
Workforce Research Studies -- The National Training Institute For Frontline Supervisors and Technical Assistance Project (NTIFFS) is a 3 year grant program designed to improve recruitment and retention across the country of DSPs, who are competent and confident in the skills needed to provide quality supports and services to individuals with developmental and other disabilities. This project is funded to refine, test and deliver a NTIFFS using a "Train-the-Trainer" model and a Technical Assistance and Consulting model to assist community human service employers, families and consumers from across the country to recruit, retain, and train DSPs and frontline supervisors. The project assists five agencies, organizations or coalition participants in identifying and managing their personnel and workforce challenges. Organizations participating in the project are developing and refining skills and intervention strategies in supporting and training frontline supervisors to maintain highly effective workforce development approaches.
B. State and Local
Many states have leveraged state resources or combined state resource with federal dollars to develop projects, grants, programs and systemic change efforts designed to address the direct support workforce shortage and turnover problems. Below is a description of many of these statewide initiatives.
1. Kansas. The Kansas Mobilizing for Direct Support Workforce Change project of the Kansas Council on Developmental Disabilities is designed to make systematic, long-term changes in the retention and recruitment of DSPs who support people with developmental disabilities in Kansas. The project assists 14 employers of DSPs (including individuals or families who directly hire DSPs) to put into action proven methods to find and keep high quality employees. In return, the employers contributed time and people willing to learn new skills, share their expertise, implement changes, and provide feedback to a project advisory committee on how to make these changes work best in Kansas. Each employer is expected to end the project with measurable improvements in their ability to find and/or retain high quality DSPs. The work of the project has been done through participation in six affinity groups, each focused on one type of intervention. Affinity groups include: (1) capacity building, (2) supervisor training, (3) technical assistance, (4) DSP training, (5) credentialing and apprenticeship, and (6) recruitment and marketing. Many tools and resources have been developed in this project including: a marketing and recruitment toolkit and a realistic job preview video and DVD.
2. Illinois. The Illinois Workforce Development Initiative to Achieve Improved Individual Outcomes for Citizens with Developmental Disabilities project of the Illinois Council on Developmental Disabilities (ICDD) is a 3 year workforce systems change initiative designed to improve recruitment and retention of DSPs in Illinois. The goal of this project is to develop long-lasting changes in Illinois so that people start applying for DSP positions and those who are hired stay in positions longer. The project will assist 15 community human service employers (14 organizations and ten individual and family employers) of DSPs to put into action proven methods to find and keep high quality employees who are competent and confident in the skills needed to provide high quality supports.
3. Ohio. The Ohio PATHS is an Initiative of the Ohio Alliance for Direct Support Professionals. In response to the direct support workforce shortage, organizations in Ohio have created a career path by building a DSP credentialing pathway -- PATHS (Professional Achievement through Training and Education in Human Services). PATHS incorporates the Community Support Skills Standards, the NADSP Code of Ethics and the Minnesota Front Line Supervisor Standards. Participants work with a skills mentor as they complete training and prepare portfolios to document their skills. Voluntary credentials are earned at four levels: Registration level, Certificate of Initial Proficiency (CIP), Certificate of Advanced Proficiency (CAP), and the Certificate of Specialized Skill and Knowledge. The PATHS credential is linked with DOL's Direct Support Specialist apprenticeship standards. PATHS has worked closely with and received grant support from the Ohio State Apprenticeship Council. PATHS was begun by the Ohio Private Resource Association (OPRA) working with the Ohio Alliance for Direct Support Professionals. The project was implemented in January 2003 with pilots in Cincinnati, Cleveland, and Toledo. Expansion to a fourth pilot region will begin in January 2005. By 2006, the voluntary credential will be established throughout Ohio. A Statewide Council oversees the project and approves candidates for credentialing. Regional Councils oversee local training and implementation. As of July 2004, 65 DSPs have received the CIP, and 44 Skills Mentors have received the CAP. Thirty-two agencies and two family advocates have participated.
4. West Virginia. The Human Service Research Institute (HSRI) is leading stakeholders in West Virginia through several interventions to strengthen the direct support workforce in that state. The group is building a policy document that examines the direct support workforce conditions to offer a pragmatic plan for addressing current challenges and to build and pilot a DSP skills certificate framework and curriculum. The model that has been designed and endorsed by the stakeholder group combines self-directed learning methods with instruction in employer based learning workshops. These workshops includes a series of carefully designed instructor led coaching sessions that wrap around specific courses offered in the CDS (a computer-based, multi-media learning environment). This model helps learners to solidify their self-directed learning through discussion, critical thinking and other constructivist learning processes. This model also facilitates a career view of direct support work by connecting direct support practitioners with their peers within the agency and from other community agencies to build their identity as DSPs and understand the career path within direct support and to other roles in human services.
5. Wyoming. The State of Wyoming established a DSP statewide wage increase following recommendations made in a legislatively authorized study regarding DSP wages and turnover. The wages of direct service staff working in adult services to people with developmental disabilities were increased in 2003 to an average wage of $10.23. A new minimum beginning wage of $7.50 was increased statewide to $8.00 after the employee had 12 months of experience. Wages reached a $10.21 average for staff members with one-year experience by October 2003. Fringe benefits increased 8.5%. Staff turnover was reduced statewide in one year by more than 15% (a one-third reduction in the rate of turnover).
C. Other Promising Practices
While government initiatives have been implemented and are useful in effecting policy and practice, much change occurs at the organizational level and through effective policy and practice advocacy. The descriptions below highlight some successful practices at the organization and policy advocacy levels.
1. Special People In Northeast, Inc. (SPIN). SPIN has a newly implemented program in place for DSP career development and tenure called Excellence in Direct Support Professional Training, Leadership Development and Career Development. SPIN is a non-profit human service organization founded in 1970. To help staff obtain the new skills necessary to become DSPs, SPIN developed a curriculum of six new training courses. Between September 1999 and May 2000, all habilitation instructors and coordinators and managers completed the courses. In July 2000, 300 habilitation instructors were recognized as DSPs in a celebration ceremony. While education was highly valued by SPIN, in 1998 only seven DSPs had college degrees or were currently enrolled despite the tuition reimbursement benefit. To improve this SPIN created several new educational opportunities in collaboration with post secondary educational institutes in the communities in which they employed DSPs. As a result, now, 56 SPIN DSPs have Bachelor's or Associate's degrees, and 19 are enrolled in college. Other recruitment, retention and training initiatives within this organization include: (1) Creating cross-functional quality council groups for staff, consumers and families to develop, initiate and implement change; (2) Participating in a five county, 60 organization image marketing campaign to attract DSPs and to improve their status; (3) Creating "SPIN Traditions" -- an orientation training that integrates the mission, values, and expectations at SPIN with personal stories from families, consumers, and staff, field experiences and a focus on welcoming new staff members; (4) Creating a Leadership Path that gives exemplary DSPs an opportunity to earn enhanced pay for taking increased responsibilities in staff recruitment and development. Roles include ambassador, strengths development peer, team leader (for new staff orientation and socialization), and traditions presenter; (5) Creating a "right-fit" philosophy that is used in the hiring and pre-service training to ensure that new employees share SPIN's values and mission, and can meet expectations; (6) Developing a recruitment and retention plan that provides increased pay for positions, longevity bonuses, recruitment bonuses and leadership opportunities at all levels; and (7) Implementing staff recognition efforts such as rewards for achieving tenure benchmarks starting at one year.
2. National Alliance for Direct Support Professionals (NADSP). The NADSP is a coalition of organizations and individuals committed to strengthening the quality of human service support by strengthening the direct support workforce. The group has representatives from the fields of mental health, developmental disabilities, child welfare, education, and many others in the human services community. The NADSP has developed a national agenda to address conditions chronicled for 25 years that are harmful to people who rely on human services. These conditions include high staff turnover, low social status, insufficient training, limited educational and career opportunities, and poor wages. These undermine the commitment of the DSPs, and have made it very difficult to recruit and train qualified and committed individuals in direct support roles in every area of human services. The NADSP believes that service participants and DSPs are partners in the move towards a self-determined life, and in complimenting and facilitating growth of natural supports. The organization recognizes that people needing support are more likely to fulfill their life dreams if they have well-trained, experienced, and motivated people at their side in long-term, stable, compatible support relationships. It also recognizes that well-planned workforce development strategies are needed to strengthen our workforce. The NADSP has developed a national Code of Ethics for community human service DSPs and has created the Moving Mountains Guiding Principles for employers of DSPs. The NADSP sponsors a quarterly magazine for DSPs called Frontline Initiative.
VI. CONCLUSIONS
One of the most important accomplishments of the nation's health and long-term care system has been the dramatic improvement in the care of persons with ID/DD over the past decades. The result is increased longevity and better integration of persons with ID/DD with the community. Today, over four million persons with ID/DD are cared for by their families, friends, and over one million DSPs. Even more DSPs will be needed in the future as the population of persons with ID/DD increases, in part because many of them will outlive their family caregivers.
The increased need for DSPs will occur at a time when the labor force is expected to grow much more slowly than in the past. There will be increased competition for people to work not only as DSPs, but as health and long-term care workers in general, as well as all of the other occupations that need workers of comparable education and skill levels. Making DSP jobs as attractive as possible will improve the likelihood that people will choose those jobs.
Numerous organizations are working to further improve the care of persons with ID/DD. Several departments of the Federal Government are involved in providing the services needed (e.g., through the Medicaid home and community-based services waivers, by improving the infrastructure through systems change grants, and by increasing education and training opportunities both for persons with ID/DD and for their DSPs). Further, at the state and local level, many governmental agencies and non-profit organizations are developing innovative programs to support DSPs.
VII. REPORT NOTES
-
Estimate for individuals in non-supervised residential settings are from Larson, S., Lakin, K.C., Anderson, L., Kwak, N., Lee, J., & Anderson, D. (2000). "Prevalence of mental retardation and/or developmental disabilities: Analysis of the 1994/1995 NHIS-D." DD Data Brief, 2(1), whole issue. Minneapolis, MN: University of Minnesota, Research and Training Center on Community Living. Estimate for persons with ID and/or DD in supervised residential settings are from Prouty, R., Smith, G., & Lakin, K.C. (Eds.) (2004). Residential services for persons with developmental disabilities: Status and trends through 2003. Minneapolis, MN: University of Minnesota, Research and Training Center on Community Living/Institute on Community Integration (on the web at http://rtc.umn.edu). Relative distribution of persons with ID/DD into ID, DD and ID and DD based on distributions computed in Lakin, K.C., Hill, B., Chen, T., & Stephens, S. (1989). Persons with mental retardation and related conditions in mental retardation facilities: Selected findings from the 1987 National Medical Expenditure Survey. Minneapolis, MN: University of Minnesota, Research and Training Center on Community Living (on the web at http://aspe.hhs.gov/daltcp/reports/mrperses.htm).
-
Prouty, R., Smith, G., & Lakin, K.C. (Eds.) (2004). Residential services for persons with developmental disabilities: Status and trends through 2003. Minneapolis, MN: University of Minnesota, Research and Training Center on Community Living/Institute on Community Integration (on the web at http://rtc.umn.edu).
-
Residential, family support and nursing services for persons with ID/DD are from: Prouty, R., Smith, G., & Lakin, K.C. (Eds.) (2004). Residential services for persons with developmental disabilities: Status and trends through 2003. Minneapolis, MN: University of Minnesota, Research and Training Center on Community Living/Institute on Community Integration (on the web at http://rtc.umn.edu). Statistics about persons with ID/DD in generic child welfare/social services foster care arrangements are less certain. Leslie, L., Hurlbert, M., Landverk, J., Rolls, J., Wood, P., & Kelleher, K. (2003). "Comprehensive assessments for children entering foster care: A national perspective." Pediatrics, 112(1), 134-142. The article reported that, "Over 40% of PSUs (child welfare agencies) had no public policy to identify children with mental health and/or developmental problems on entry into out-of-home care (p. 138). Based on less than ideal data we estimated that about 38,000 children and youth with ID/DD are in generic foster care settings. This estimate is educated by the National Health Interview survey-disability supplement which estimated 32,200 children and youth with ID/DD living in non-specialized homes with non-relatives. Assuming (based on a 1986 ASPE-funded survey of states [Hill, B.K. et al., 1987]) that the number of children and youth in foster placements with relatives other than parents equals about 17.5% of the number living with non-relatives, would yield an estimated 38,000 children and youth with ID/DD in foster care. This seems a reasonable estimated based on the Hill et al., 1987 study in which it was estimated that there were 13,900 children and youth with ID and 4,400 with physical disabilities (the numbers reported by states with a 65.4% increase to adjust for the foster care populations in states that could not report the disability statistics). This combined total estimate (18,300) was 7.0% of all children and youth in generic foster care settings in 1985. Applying that percentage to the 2003 reported number of 535,000 children and youth in generic foster care settings, yields an estimated 37,500 children and youth with ID/DD.
-
Smith, G. (2004). Status report: Litigation concerning home and community based services for persons with disabilities. Tualatin, OR: Human Services Research Institute (on the web at http://www.hsri.org).
-
Ball et al. v. Biedess et al. U.S. District Court, Arizona.
-
Lakin, K.C., Hill, B.K., & Bruininks, R. (1985). An analysis of Medicaid's Intermediate Care Facility for the Mentally Retarded program. Minneapolis, MN: University of Minnesota, Research and Training Center on Community Living.
-
Larson, S., Lakin, K.C., & Hewitt, A. (2002). "Direct support professionals." In Schalock, R., Baker, P., & Croser, D. (Eds.), Embarking on a new century: Mental retardation at the end of the 20th century. Washington, DC: American Association on Mental Retardation.
-
This process and outcome is described in Taylor, M., Bradley, V., & Warren, J. (1996). The community support skill standards: Skill standards for direct service workers in the human services. Cambridge, MA: Human Services Research Institute.
-
Statistics on persons currently needing residential, in home and other services come from the state reports in Prouty, R., Smith, G., & Lakin, K.C. (Eds.) (2004). Residential services for persons with developmental disabilities: Status and trends through 2003. Minneapolis, MN: University of Minnesota, Research and Training Center on Community Living/Institute on Community Integration (on the web at http://rtc.umn.edu). The estimate is made by combining the number of persons with ID/DD currently receiving LTSS while living in staffed residential settings, receiving support in their own homes and homes they share with family members (500,004), as well as 75,300 persons estimated to be waiting for services. The estimated 35,005 currently in nursing facilities and an estimated 38,000 children in foster care are added to this total with the assumption that they will also be part of the LTSS system for persons with ID/DD in 2020. To this total of about 1,050,600 individuals requiring residential or in-home supports there will be increases in demand for LTSS for persons with ID/DD that may be assumed to grow proportionately with the 15.9% projected population growth, bringing the estimated 2020 total of those needing such supports to 1,217,000. At the same time there will be commensurate growth in the demand for day and vocational support services from the estimated 2003 number of 465,000 service recipients. These day and vocational services are provided to people already included in the residential and in-home service recipients counts above, the of DSPs needed to provide those day and vocational services is in addition to the growth in residential and in-home supports, as will be the growth in the number of DSPs needed in the future. We have also assumed an increase in life expectancy of 2.5 years over the 17 year period between 2003 and 2020 (as has occurred in each of the previous two 17-year periods prior to 2003. This 2.5 year increase times the associated 2.4% increase in service years will increase service recipients to an estimated 1,291,000. The aging of parents who are currently 55 years or older who are now the primary caregivers to individuals with ID/DD and who have exceptional care needs (i.e., cannot be left alone for more than 2 hours at a time) will add an estimated 60,000 individuals to the LTSS system (although we do not well understand the likelihood of other family members accepting primary care roles). Changing prevalence of certain disabilities (e.g., autism); increasing (or decreasing) demand for services accompanying the increasing flexibility and community orientation of LTSS; broadening (or narrowing) of eligibility standards for ID/DD services nationally and/or within the states; better (or worse) state finances and LTSS financing commitments; changing federal policies that affect current federal-state cost-sharing and other factors are likely to be important, but without established patterns with which to make projections.
-
The total estimated prevalence of persons with ID/DD and breakdowns by type of residence is based on the estimate of the number of persons with ID/DD in the "non-institutionalized" population as provided in Larson, S., Lakin, K.C., Anderson, L., Kwak, N., Lee, J., & Anderson, D. (2000). "Prevalence of mental retardation and/or developmental disabilities: Analysis of the 1994/1995 NHIS-D." DD Data Brief, 2(1), whole issue. Minneapolis, MN: University of Minnesota, Research and Training Center on Community Living. The total estimated prevalence for persons with ID/DD and breakdowns by type of residence is based on the estimate of the number of persons with ID/DD in the "institutionalized" population (i.e., persons in staffed residences) from Prouty, R., Smith, G., & Lakin, K.C. (Eds.) (2004). Residential services for persons with developmental disabilities: Status and trends through 2003. Minneapolis, MN: University of Minnesota, Research and Training Center on Community Living/Institute on Community Integration (on the web at http://rtc.umn.edu). For foster care estimate see Hill, B.K., Lakin, K.C., Novak, A.R. & White, C.C. (1987). Foster care for children and adults with handicaps: Child welfare and adult social services. Washington, DC: HHS Office of the Assistant Secretary for Planning and Evaluation (on the web at http://aspe.hhs.gov/daltcp/reports/fosteres.htm.
-
The estimated number of children and adults in the family homes are based on the estimates of the National Health Interview Survey-Disability supplement. The estimates of children and adults receiving residential supports in out-of-family setting is from Prouty, R., Smith, G., & Lakin, K.C. (Eds.) (2004). Residential services for persons with developmental disabilities: Status and trends through 2003. Minneapolis, MN: University of Minnesota, Research and Training Center on Community Living/Institute on Community Integration (on the web at http://rtc.umn.edu). Estimates of children within the total residential population are from Lakin, K.C., Anderson, L. & Prouty, R. "Decreases continue in out-of-home residential placements of children and youth with mental retardation." Mental Retardation, 36(2), 165-167. The number of children with ID/DD in foster care was estimated from the proportion of all children in foster care with ID/DD computer in a 1987 ASPE-sponsored study with the proportion applied to the HHS Administration of Children and Families estimate of 560,000 children in foster care at the beginning of 1999. The ASPE study was Hill, B.K., Lakin, K.C., Novak, A.R. & White, C.C. (1987). Foster care for children and adults with handicaps: Child welfare and adult social services. Washington, DC: HHS Office of the Assistant Secretary for Planning and Evaluation (on the web at http://aspe.hhs.gov/daltcp/reports/fosteres.htm.
-
Larson, S., Lakin, K.C., Anderson, L., & Kwak, N. (2001). "Characteristics and service use by persons with MR/DD living in their own homes or with family members: NHIS-D analysis." DD Data Brief, 3(1), whole issue. Minneapolis, MN: University of Minnesota, Research and Training Center on Community Living.
-
Larson, S., Lakin, K.C., Anderson, L., & Kwak, N. (2001). "Demographic characteristics of persons with MR/DD living on their own or with family members: NHIS-D analysis." DD Data Brief, 3(2), whole issue. Minneapolis, MN: University of Minnesota, Research and Training Center on Community Living.
-
Estimates of the need for DSPs who would be needed to provide support to adults with ID/DD is based on the estimates of persons with ID/DD living with family members, the estimated level of paid support provided on average to adults living with family members and the difference in paid support provide to persons in out-of-home vs. in-home settings.
-
Lakin, K.C., Anderson, L. & Prouty, R. "Decreases continue in out-of-home residential placements of children and youth with mental retardation." Mental Retardation, 36(2), 165-167.
-
National Institute on Mental Health. (1966). Patients in mental hospitals, 1965. Washington, DC: U.S. Government Printing Office.
-
Yang, Q., Rasmussen, S.A., & Freedman, J.M. "Mortality associated with Down syndrome in the USA from 1983 to 1997: A population-based study." The Lancet, 359, 1019-1025.
-
Studies in Finland and Australia show substantial consistency in life expectancy of persons with different levels of intellectual disability and generally represent societies that make comparable types and qualities of services available to persons with ID. The Finnish study (Patja et al., 2000) showed that an average life expectancy of persons with mild or moderate ID was 70 years; the Australian study (Bittles et al., 2002) 71 years. The Finnish study reported an average life span of 56 years for persons with severe or profound ID; the Australian study 58 years. Based on these studies and a proximate 50-50% split in state LTSS system between persons with mild/moderate and severe/profound ID, an average longevity of 64 years may be expected of persons with ID/DD. Because of the relatively small percentage of DSPs supporting children, it may be assumed that an age of 64 represents approximately 64 years minus 22 years (the age of entering LTSS) or an average of about 42 service years. Therefore, each year of increased average longevity represents approximately a 2.4% in demand for DSPs. Sources: Patja, K., Iivanainen, M., Vesala, H., Oksanen, H., & Ruoppila, I. (2000). "Life expectancy of people with intellectual disability: A 35-year follow-up study." Journal of Intellectual Disability Research, 44(5), 591-599. Bittles, A, Petterson, B., Sullivan, S., Hussain, R., Glasson, E. & Montgomery, P. (2002). "The influence of intellectual disability on life expectancy." The Journals of Gerontology Series A: Biological Science and Medical Science, 57(7), 470-472.
-
Lewitt, E., Baker, L. Corman, H., & Shiono. P. (1995). "The direct cost of low birth weight." The Futures of Children, 5(1), 35-56.
-
Halsey, C., Collin, M., & Anderson, C. (1993). "Extremely low birth weight children and their peers: A comparison of preschool performances." Pediatrics, 91, 807-811.
-
Studies of the effects of the mandatory folic acid fortification of cereal grain products include: Williams, L.J., Mai, C.T., Edmonds, L., Shaw, G., Kirby, R., Hobbs, C., Seuer, L., Miller, L., Meaney, F., & Levitt, M. (2002). "Prevalence of spina bifida and anencephaly during the transition of mandatory folic acid fortification in the United States." Teratology, 66, 33-39. Mersereau, M., Kilker, K., Carter, A., Fasett, E., Williams, J., Flores, A., Prue, C., Willams, L., Mai, C., & Mulinare, J. (2004). "Spina bifida and anencephaly before and after folic acid mandate -- United States, 1995-1996 and 1999-2000." MMWR Weekly, 53(17), 362-365.
-
The estimates of current and projected DSPs are based on the following sources and computations: Every two years the "Residential services Status and trends" report (cited in full below) includes a survey of all operating state institutions (to which 99.5% responded in 2002-the last year of a fully completed survey. From that survey it was computed that nationally the average ratio of DSPs to persons with ID/DD in those settings was 1.34:1. [N.B. It takes 4.2 FTEs to cover a full 168 hour week with 40 hours shifts.]. This 1.34 ratio was applied to the 6/2003 number of residents of state institutions to obtain the estimated number of DSP FTEs.
Five surveys were identified of samples of community residential service settings for persons with ID/DD (including large private residential settings) conducted/ distributed since 1998 that have included statistics that allow computation of the ratios of persons served to full-time equivalent DSPs (California, Kansas, Minnesota, Washington and Wyoming). These surveys in the order appearing in the table below include: Wheeler, B. (2001). A three-year evaluation of the impact of WIC Section 4681.4 (rate increase) on direct support staff turnover in California's community care facilities for people with developmental disabilities: Year 1 results, 1999-2000. Los Angeles, CA: University of Southern California, USC University Affiliated Program. Fullager, C., Smalley, K., Flanagan, J., Walker, L., Downey, R., Bloomquist, L., Bratsberg, V., Shanteau, J., & Pickett, L. (1998). Community service provider direct care staff turnover study. Manhattan, KS: Institute for Social and Behavioral Research. Larson, S., Lakin, K.C., & Bruininks, R. (1998). Staff recruitment and retention: Study results and intervention strategies. Washington, DC: American Association on Mental Retardation. Start, S.L., & Cook, C. (1998). Stabilizing our residential programs and workforce. Seattle, WA: Community Residential Services Association. Heinlein, K. (2001). Report to the Joint Appropriations Committee on the study of nonprofessional direct care staff recruitment, retention and wages. Cheyenne, WY: Department of Health, Developmental Disabilities Division. Although these states are not necessarily representative, there is a fair level of stability of the estimates which yields a fair level of confidence about them.
The obtained estimated are listed below. Aggregating these estimates without weighting for state size, the computed average ratio of DSP FTEs per community service recipient was 1.13. This estimate is then applied to national statistics on community/private residential services and persons waiting for residential services as obtained in Prouty, R., Smith, G., & Lakin, K.C. (Eds.) (2004). Residential services for persons with developmental disabilities: Status and trends through 2003. Minneapolis, MN: University of Minnesota, Research and Training Center on Community Living/Institute on Community Integration (on the web at http://rtc.umn.edu). These are summarized below:
State FTEs/Service Recipient CaliforniaKansasMinnesotaWashington Wyoming 1.081.051.191.151.19 Average 1.13 The estimated number of vocational and day program recipients comes from the bi-annual State of the States survey: Rizzolo, M.K., Hemp, R., Braddock, D. & Pomeranz-Essley. (2004). The state of the states in developmental disabilities. Boulder, CO: University of Colorado, Coleman Institute on Cognitive Disabilities. The estimate of the number of DSPs per person in day training and vocational support programs is derived from preliminary data obtained from a national survey of 125 vocational and day service provider agencies. Those 125 agencies employed 7009 FTE DSPs to provide vocational/day services to 20,284 individuals. The resulting computation of DSPs to service recipients was .346 (preliminary data from Butterworth, J. (August 11, 2004). Personal communication. University of Massachusetts-Boston, Institute on Community Inclusion).
We do not have statistics on the number of DSPs who provide in-home supports (respite care providers, PCAs, home health attendants, CNAs, etc.) to people with developmental disabilities living with family members. If we assume that each of these individuals receives an average of 10 hours of support per week, then the ratio of support providers would be .25 FTEs per each of the 500,004 in-home support recipients are reported in "Residential services Status and trends through 2003".
Using these estimates and the available statistics on service recipients, we could compute that:
Service Setting Served Ratio DSPs State institution residents (6/03) = 42,835 X 1.34 = 57,399; Community settings and large private settings (6/03) = 359,446 X 1.13 = 406,174; Persons waiting for residential services (6/03) = 75,288 X 1.13 = 85,075; *Vocational and day programs (2002) = 465,000 X 0.346 = 160,890; Family/in-home supports (6/03) = 500,004 X 0.25 = 125,001; *Estimated Total DSP FTEs = 1,442,573 X = 834,553 * These are not all individual service recipients; notably the vocational and day program recipients will almost all be included in one of the residential or in-home categories. No adjustments have been made for part-time DSPs although various studies have indicated that part-time DSPs range from 25% to 35% of all DSP employees. Let me return to the NMES data and the estimates that would derive from the state institution and community settings statistics above. If we were to apply the NMES average DSP-to-resident ratio from 1987 to the 2003 resident counts, it would yield an estimated 426,420 FTE DSPs. If we were to use the 2002 ratios for state institutions and community residential settings, in combination they would yield an estimated 463,573 DSP FTEs. That is a notable difference, but it seems pretty reasonable as the use of large congregate care settings decreases.
-
Statistics on the 2002 and projected 2020 populations of persons in the U.S. between the ages of 20 and 39 years are from the U.S. Bureau of the Census, Statistical Abstract of the United States, Tables 11 and 12.
-
The estimates for 2040 are based on continuation of the trend of the average of 2.25 annual increase between 2003 and 2020 with an adjustment to reflect the impact of aging among parents of persons with ID/DD during the 2020 to 2040 period. During the period the US Census Bureau estimates a 112% growth in the number of US residents who are 80 or older. Among these individuals will be large numbers of parents of persons with ID/DD who will be unable because of disability or death among one or both parents to continue to be the primary support of adult children with ID/DD. The estimate of the associated increased demand for DSPs reflects an assumption that 25% of persons admitted to residential services from family settings with aging caregivers. A corresponding adjustment in the projected growth in LTSS demand (2.25% per year) was made to reflect the substantial growth in family caregivers (i.e., a 0.4% growth per year) based on these trends.
-
According to the National Health Interview Survey's Disability Supplement of 1994/1995 family's of children with intellectual disabilities (ID)/ and/or developmental disabilities (DD) or other disabilities have experience the following impacts as a result of their caregiving role.
IMPACT OF CHILD'S DISABILITY ON FAMILY Due to child's health, someone in the family has: DD not ID ID not DD ID and DD Other Disabilities Total ID, DD, or Other X2 Not taken job 20.7% 10.3% 36.1% 12.3% 16.1% 41.82** Changed work hours 19.1% 11.1% 28.5% 14.0% 16.1% 20.11** Worked fewer hours 17.7% 11.5% 25.8% 8.4% 14.7% 18.37** Quit Working 14.8% 8.5% 16.7% 8.6% 10.6% 13.63** Changed sleep patterns 13.2% 6.2% 15.9% 6.6% 8.8% 19.70** Turned down better job 9.2% 5.0% 16.9% 7.7% 8.6% 17.73** Changed jobs 12.1% 3.3% 17.3% 6.6% 8.2% 25.78** Had severe financial problems 9.8% 3.7% 9.1% 4.8% 6.0% 13.80** Reported one or more accommodations 38.4% 23.6% 52.7% 23.1% 30.9% 49.17** ** p < .01 This table was taken from Anderson, L., Larson, S., Lakin, K.C., & Kwak, N. (2002). "Children with disabilities: Social roles and family impacts in the NHIS-D." DD Data Brief, (1), whole issue. Minneapolis, MN: University of Minnesota, Research and Training Center on Community Living.
-
Data were gathered as part of the bi-annual State of the States survey on financing of services for persons with ID/DD, conducted at the University of Colorado, Coleman Institute on Cognitive Disabilities, David Braddock, Principal Investigator (funded by the Administration on Developmental Disabilities. Unpublished data were provided for this specific analysis and were published in Lakin, K.C., & Prouty, R. (2003). "Medicaid home and community based services: The first 20 years." Policy Research Brief, 14(3), whole issue. Minneapolis, MN: University of Minnesota, Research and Training Center on Community Living.
-
Among the numerous reports raising doubts about the adequacy of direct support as presently provided in community LTSS programs are a House Hearing 1993; R. Wyden (Chair), Growth in small residential living programs for the mentally retarded and developmentally disabled (Serial No. 103-8). The General Accounting Office in June 2003 released a report entitled: Federal oversight in growing Medicaid Home and Community Based waivers should be strengthened (GAO-03-03-576). Newspaper accounts of poor quality in community LTSS systems include: Hartford Courant. (December 2, 2001). "The toll: Suffocation, drowning, choking, burns." Oregon Statesman Journal. (March 12, 2000). "A rash of deaths, inquirers find neglect a factor." Boo, K. (March 14, 1999). "Forest Haven is gone, but the agony remains." The Washington Post, p. A1. The Washington Post. (March 15, 1999). "Residents languish; profiteers flourish." Atlanta Journal Constitution. (December 2, 2001). "Dying in darkness". The American Prospect. "Neglect for sale".
-
The studies summarized in Table 5 are drawn from two sources: (1) Larson, S., Hewitt, A., & Knobloch, B. (in press). "Recruitment retention and training challenges in community human service: Review of literature." In Larson, S. & Hewitt, A. (Eds). Staff recruitment, retention and training for community human services organizations. Baltimore, MD: Paul H. Brookes; and (2) from unpublished summaries of facility surveys gathered within states participating in the National Core Indicators program, co-sponsored by the National Association of State Directors of Developmental Disabilities Services and the Human Services Research Institute.
-
Statistics on DSP vacancy rates among community service providers include: [to be added]
-
Computations were first made for DSP demand based on projected growth in DSPs between 2004 and 2020. Computations included replacing 50% of current year's DSPs plus adding the average annual increase of 19,000 new DSPs. Computations of DSPs, needed at reduced turnover rates, began with the estimate of DSPs needed at the 50% turnover rate. It subtracted the 19,000 new additions, reduced the number of replacements by the proportional reduction in turnover for year (.96 [.48/.50], .92, .88, etc. to .60 and then maintained at .60). The estimated average number of new positions (19,000) was then added back in to yield the estimate number of DSPs needed at the reduced rate.
-
This column includes factors studied specifically in LTSS settings for persons with ID/DD. Fourteen of 73 factors examined in eight studies had been included in more than one investigation. This table shows the ten factors for which statistically significant findings were consistently in the same direction. This analysis was originally published in Lakin, K.C., & Larson, S.A. (1992). "Satisfaction and stability of direct-care personnel in community-based residential services." In Jacobson, J.W., Burchard, S.N., & Carling, P.J. (Eds.). Clinical services, social adjustment, and work life in community living. Baltimore, MD: Johns Hopkins University Press, pp. 244-262.
-
Five statewide and three national studies used multiple regression procedures to examine variables associated with turnover in community LTSS for people with DD. This column lists the variables associated with turnover in those studies. Studies include: Department of Employee Relations. (1989). Study of employee wages, benefits and turnover in Minnesota direct care facilities serving persons with developmental disabilities. St. Paul, MN: Minnesota Department of Employee Relations for the Department of Human Services. George, M.J., & Baumeister, A.A. (1981). "Employee withdrawal and job satisfaction in community residential facilities for mentally retarded persons." American Journal of Mental Deficiency, 85, 639-647. Larson, S.A., Hewitt, A.S., & Lakin, K.C. (2004). "A multi-perspective analysis of the effects of recruitment and retention challenges on outcomes for persons with intellectual and developmental disabilities and their families." American Journal on Mental Retardation, 109, 481-500. Jacobson, J.W., & Ackerman, L.J. (1992). "Factors associated with staff tenure in group homes serving people with developmental disabilities." Adult Residential Care Journal, 6, 45-60. Larson, S.A., & Lakin, K.C. (1999). "A longitudinal study of recruitment and retention in small community homes supporting persons with developmental disabilities." Mental Retardation, 178-191. Braddock, D., & Mitchell, D. (1992). Residential services and developmental disabilities in the United States: A national survey of staff compensation, turnover and related issues. Washington, DC: American Association on Mental Retardation. Lakin, K.C., & Bruininks, R.H. (1981). Occupational stability of direct-care staff of residential facilities for mentally retarded people. Minneapolis, MN: University of Minnesota, Center on Residential and Community Services. Larson, S.A., & Lakin, K.C. (1992). "Direct care staff stability in a national sample of small group homes." Mental Retardation, 30, 13-22. Detailed findings are in the table below:
MULTIPLE REGRESSION STUDIES OF FACILITY LEVEL TURNOVER AMONG DSPS IN COMMUNITY SETTINGS SUPPORTING INDIVIDUALS WITH ID/DD1 Authors Subjects % of variability accounted for Variables associaetd with turnover Single State Studies Department of Employee Relations, 1989 252 MN Facilities (group homes, day programs, semi-independent living services and rehabilitation facilities) 16% - Average hourly pay
- ICF-MR certification
- Urban vs. rural location
George & Baumeister, 1981 12 small TN agencies (Mean = 6.4 residents), 26 large TN agencies (Mean = 12.6 residents) 34% - Length of unit operation
- Age of residents
- N with severe challenging behavior
- Community skills of residents
Larson, Hewitt & Lakin, 2004 170 MN small HCBS group homes (Mean = 5.45 residents) and vocational settings (Mean = 28.8 participants) 12% - Average DSP wage
- Urban vs. rural location
Jacobson & Ackerman, 1992 38 NY group homes (Mean = 7 residents) 22% - Public vs. private operation
- Resident disability level
Larson & Lakin, 1999 110 small MN group homes (6 or fewer residents) 26% - Severity of disability and support need
- Starting pay
- Supervisor tenure in home
- % DSP eligible for paid leave
Natinoal Studies Braddock & Mitchell, 1992 618 private agencies (Mean = 15 residents) 8%c - Average wage
- Starting wage
- Health benefits
- Direct care ratio
- Per diem
- Level of mental retardation
- Unionization
- Facility size
- Facility age
- ICF-MR certification
- Hours of in service training
Lakin & Bruininks, 1981 73 small private residences (1 to 64 persons) 9% - Starting salary (indexed by per capita income)
- # of DSPs in facility
Larson & Lakin, 1992 101 small group homes (6 or fewer residents) 7% - # of DSPs
- Using shift vs. live-in workers
-
Lakin, K.C. (1981). Occupational stability of direct-care staff of residential facilities for mentally retarded people. Doctoral Dissertation. Minneapolis, MN: University of Minnesota.
-
Braddock, D., & Mitchell, D. (1992). Residential services and developmental disabilities in the United States: A national survey of staff compensation, turnover and related issues. Washington, DC: American Association on Mental Retardation.
-
Polister, B. Lakin KC, and Prouty R. (2003). "Wages of direct support professionals serving individuals with intellectual and developmental disabilities: a survey of state agencies and private residential provider trade associations. Policy Research Brief, 14(2). Minneapolis, MN: University of Minnesota, Institute on Community Integration).
-
Larson, S.A., Coucouvanis, K., & Prouty, R. (2003). "Staffing patterns, characteristics and outcomes in large state-operated residential facilities in 2002." In Prouty, R., Smith, G., & Lakin, K.C. (Eds.) (2004). Residential services for persons with developmental disabilities: Status and trends through 2003. Minneapolis, MN: University of Minnesota, Research and Training Center on Community Living/Institute on Community Integration (on the web at http://rtc.umn.edu).
-
Larson, S., Hewitt, A., & Knobloch, B. (in press). "Recruitment retention and training challenges in community human service: Review of literature." In Larson, S. & Hewitt, A. (Eds). Staff recruitment, retention and training for community human services organizations. Baltimore, MD: Paul H. Brookes. Unpublished summaries of facility surveys gathered within states participating in the National Core Indicators program, co-sponsored by the National Association of State Directors of Developmental Disabilities Services and the Human Services Research Institute.
-
A 1997 literature review noted that between 1973 and 1995, many models of turnover had been proposed identifying 65 different factors that explain turnover. Larson, S., Lakin, K.C., & Bruininks, R. (1998). Staff recruitment and retention: Study results and intervention strategies. Washington, DC: American Association on Mental Retardation. This table lists the factors that appeared across three or more of the following models. Arnold, H.J., & Feldman, D.C. (1982). "A multi-variate analysis of the determinants of job turnover." Journal of Applied Psychology, 67, 350-360. Bluedorn, A.C. (1982). "The theories of turnover: Causes, effects, and meaning." Research in the Sociology of Organizations, 1, 75-128. Hom, P.W., & Griffeth, R.W. (1991). "Structural equations modeling test of a turnover theory: Cross-sectional and longitudinal analyses." Journal of Applied Psychology, 76, 350-366. Jackofsky, E.F. (1984). "Turnover and job performance: An integrated process model." Academy of Management Review, 9, 74-83. Michaels, C.E., & Spector, P.E. (1982). "Causes of employee turnover: A test of the Mobley, Griffeth, Hand, and Meglino model." Journal of Applied Psychology, 67, 53-59. Mobley, W.H., Griffeth, R.W., Hand, H.H., & Meglino, B.M. (1979). "Review and conceptual analysis of the employee turnover process." Psychological Bulletin, 86, 493-522. Mobley, W.H., Horner, S.O., & Hollingsworth, A.T. (1978). "An evaluation of precursors of hospital employee turnover." Journal of Applied Psychology, 63, 408-414. Muchinsky, P.M., & Morrow, P.C. (1980). "A multi-disciplinary model of voluntary employee turnover." Journal of Vocational Behavior, 17, 263-290. Price, J.L. (1977). The study of turnover. Ames, IA: Iowa State University Press. Price, J.L., & Mueller, C.W. (1986). Absenteeism and turnover of hospital employees. Greenwich, CT: JAI Press, Inc. Saks, A.M. (1994). "A psychological process investigation for the effects of recruitment source and organization information on job survival." Journal of Organizational Behavior, 15, 225-244. Steers, R.M., & Mowday, R.T. (1981). "Employee turnover and post-decision accommodation processes." Research in Organizational Behavior, 3, 235-281. Stumpf, S.A., & Hartman, K. (1984). "Individual exploration to organizational commitment or withdrawal." Academy of Management Journal, 27, 308-329.
-
Fourteen meta-analytical studies have been conducted since 1984 looking across studies at combinations of variables that predict whether a staff member will stay or leave. This column summarizes variables found to be associated with turnover across studies. Data sources include: Bycio, P., Hackett, R.D., & Alvares, K.M. (1990). "Job performance and turnover: A review and meta-analysis." Applied Psychology: An International Review, 39, 47-76. Carston, J.M., & Spector, P.E. (1987). "Unemployment, job satisfaction, and employee turnover: A meta-analytic test of the Muchinsky model." Journal of Applied Psychology, 72, 374-381. Cohen, A. (1993). "Organizational commitment and turnover: A meta-analysis." Academy of Management Journal, 36, 1140-1157. Cotton, J.L., & Tuttle, J.M. (1986). "Employee turnover: A meta-analysis and review with implications for research." Academy of Management Review, 11, 55-70. Hom, P.W., Caranikas-Walker, F., Prussia, G.E., & Griffeth, R.W. (1992). "A meta-analytic structural equations analysis of a model of employee turnover." Journal of Applied Psychology, 77, 890-909. Irvine, D.M., & Evans, M.G. (1995). "Job satisfaction and turnover among nurses: Integrating research findings across studies." Nursing Research, 44, 246-253. Mathieu, J.E., & Zajac, D.M. (1990). "A review and meta-analysis of the antecedents, correlates, and consequences of organizational commitment." Psychological Bulletin, 108, 171-194. McEvoy, G.M., & Cascio, W.F. (1987). "Do good or poor performers leave? A meta-analysis of the relationship between performance and turnover." Academy of Management Journal, 30, 744-762. Mitra, A., Jenkins, G.D., & Gupta, N. (1992). "A meta-analytic review of the relationship between absence and turnover." Journal of Applied Psychology, 77, 879-889. Randall, D.M. (1990). "The consequences of organizational commitment: Methodological investigation." Journal of Organizational Behavior, 11, 361-378. Steel, R.P., & Ovalle, N.K. 2d. (1984). "A review and meta-analysis of research on the relationship between behavioral intentions and employee turnover." Journal of Applied Psychology, 69, 673-686. Tett, R.P., & Meyer, J.P. (1993). "Job satisfaction, organizational commitment, turnover intention, and turnover: Path analyses based on meta-analytic findings." Personnel Psychology, 46, 259-293. Wanous, J.P., Poland, T.D., Premack, S.L., & Dawis, K.S. (1992). "The effects of met expectations on newcomer attitudes and behaviors: A review and meta-analysis." Journal of Applied Psychology, 77, 288-297. Williams, C.R., & Livingstone, L.P. (1994). "Another look at the relationship between performance and voluntary turnover." Academy of Management Journal, 37, 269-298.
-
Test, D., Solow, J., & Flowers, C. (1999). North Carolina direct support professionals study: Final report. Charlotte, NC: University of North Carolina at Charlotte. Developmental Disabilities Service Division. (2000). Direct support staff turnover reduction plan: Annual report to residential providers. Oklahoma City, OK: Oklahoma Department of Human Services, Developmental Disabilities Service Division. Barry Associates. (1999). The Ohio Provider Resource Association 1999 salary and benefits survey. Kokomo, IN: Author. Cohen, A. (2000). Focus on the front line: Perceptions of workforce issues among direct support workers and their supervisors. A staff report. Boston, MA: Governor's Commission on Mental Retardation. (on the web at http://www.state.ma.us/gcmr/pdf/Focus_on_Frontlines_032000.pdf). Hewitt, A., Larson, S.A., & Lakin, K.C. (2000). An independent evaluation of the quality of services and system performance of Minnesota's Medicaid home and community based services for persons with mental retardation and related conditions. Minneapolis, MN: University of Minnesota, Institute on Community Integration, Research and Training Center on Community Living. Larson, S.A., Prouty, R.W., & Polister, B. (2003). "Staffing patterns, characteristics and outcomes in large state-operated residential facilities in 2002." In Prouty, R.W., Smith, G. & Lakin, K.C. (Eds.). Residential services for persons with developmental disabilities: Status and trends through 2000. Minneapolis, MN: University of Minnesota, Center on Residential Services and Community Living/Institute on Community Integration (on the web at http://rtc.umn.edu).
-
Johnston, K. (1998). Developmental disabilities provider direct service worker study: Results and findings. Anchorage, AK: Governor's Council on Disabilities and Special Education.
-
Hewitt, A., Larson, S.A., & Lakin, K.C. (2000). An independent evaluation of the quality of services and system performance of Minnesota's Medicaid home and community based services for persons with mental retardation and related conditions. Minneapolis, MN: University of Minnesota, Institute on Community Integration, Research and Training Center on Community Living.
-
Kansans Mobilizing for Workforce Change Stakeholder Advisory Group. (2004). Kansans mobilizing for change: A statewide workforce development plan to resolve the direct support workforce crisis. Topeka, KS: Kansas Council on Developmental Disabilities.
-
Hewitt, A., Larson, S.A., & Lakin, K.C. (2000). An independent evaluation of the quality of services and system performance of Minnesota's Medicaid home and community based services for persons with mental retardation and related conditions. Minneapolis, MN: University of Minnesota, Institute on Community Integration, Research and Training Center on Community Living. Johnston, K. (1998). Developmental disabilities provider direct service worker study: Results and findings. Anchorage, AK: Governor's Council on Disabilities and Special Education. Larson, S.A., Hewitt, A., & Anderson, L. (1999). "Staff recruitment challenges and interventions in agencies supporting people with developmental disabilities." Mental Retardation, 37, 36-46.
-
Employment Policy Foundation. (2002). "Employment Turnover -- A critical human resource benchmark." 2002 HR Benchmarks: Contemporary Issues in Employment and Workplace Policy (on the web at http://www.epf.org/pubs/newsletters/2002/hb20021203.pdf).
-
Hewitt, A., & Lakin, K.C. (2001). Issues in the direct support workforce and their connections to the growth, sustainability and quality of community supports. Minneapolis, MN: University of Minnesota, Research and Training Center on Community Living.
-
This section draws heavily from S.A., Hewitt, A.S., & Lakin, K.C. (2004). "A multi-perspective analysis of the effects of recruitment and retention challenges on outcomes for persons with intellectual and developmental disabilities and their families." American Journal on Mental Retardation, 109, 481-500.
-
The speech on the web at http://www.dol.gov/sec/media/speeches/sec648_9252002.htm.
-
Legislative Budget and Finance Committee. (1999). Salary levels and their impact on the quality of care for client contact employees in community-based MH/MR programs. A report in response to House Resolution 450. Harrisburg, PA: Author.
-
Boo, K. (March 14, 1999). "Forest haven is gone, but the agony remains." The Washington Post, p. A1. Corcoran, K., & Fahy, J. (June 18, 2000). Painful lessons: Lives hung in the balance as firm moved mentally disabled into communities. As problems grew, the state failed to intervene. Indianapolis Star. McEnroe, P. (October 25, 2001). Part 1: The system swallows up a boy "as good as gold." Star Tribune, Voiceless and Vulnerable Series (on the web at http://www.startribune.com, accessed November 6, 2001).
-
Hall, P.S., & Hall, N.D. (2002). Hiring and retaining direct-care staff: After fifty years of research, what do we know? Mental Retardation, 40, 201-211.
-
California State Auditor. (1999). Department of Developmental Services: Without sufficient state funding, it cannot furnish optimal services to developmentally disabled adults. Sacramento, CA: Bureau of State Audits, Author.
-
Anderson, L., Larson, S.A., Lakin, K.C., & Kwak, N. (2002). "Children with disabilities and social roles: An analysis of the 94/95 NHIS-D." DD Data Brief, 4(1). Minneapolis, MN: University of Minnesota, Research and Training Center on Community Living.
-
The 2000 Minnesota Home and Community Based Waiver Evaluation included interviews with 372 adult service recipients and 20 county DD managers, and surveys of 183 families, 520 county service coordinators, 228 direct support professionals, and 184 residential and 82 vocational managers. Larson, S.A., Hewitt, A.S., & Lakin, K.C. (2004). "A multi-perspective analysis of the effects of recruitment and retention challenges on outcomes for persons with intellectual and developmental disabilities and their families." American Journal on Mental Retardation, 109, 481-500.
-
National Association of State Directors of Developmental Disabilities Services & Human Services Research Institute. (2002). Provider survey: Summary report of staff stability and board representation data reported in CIP Phases II, III, and IV. Alexandria, VA & Cambridge, MA: Authors.
-
Greene, A. (2000). Barriers to self-determination -- what's next?: A service coordinator and point of entry perspective. In Measure for measure: Person-centered quality assurance. Wingspread conference proceedings, Racine, WI.
APPENDIX A. IMPACT OF INTERVENTIONS ON WORKFORCE CHALLENGES
A. Recruitment and Selection Best Practices
Finding and hiring adequate numbers of direct support professionals (DSPs) who have or who can readily learn the knowledge, skills and attitudes required in community long-term services and supports (LTSS) has been difficult for decades.1 In several recent studies more than 70% of administrators have reported having trouble finding people to fill DSP positions.2 Serious problems have been reported due to lack of qualified applicants (reported by 69% of administrators), inadequate pay or compensation (67%), challenging hours (evenings, nights, weekends, holidays; 55%), and applicants who do not demonstrate adequate work ethic (52%).3 In Minnesota, county service coordinators noted that recruiting foster families and residential and in-home staff were serious problems.4 These challenges have resulted in the vacancy rates of 8% or higher as reported earlier. DSP positions that have been funded remain vacant between 2.8 weeks and 10.5 weeks at a time when a DSP leaves the organization.5 Frontline supervisors report offering positions to as many as 53% of all applicants (indicating they had very limited choice in whom to hire).6
Several strategies have been used successfully in LTSS for persons with intellectual disabilities and other developmental disabilities (ID/DD) to improve recruitment and selection success. One strategy is to shift attention away from recruiting DSPs from impersonal sources such as newspaper advertisements, and toward hiring people who hear about the job from a current employee or someone affiliated with the employer. Research in both ID/DD settings and in general business settings has demonstrated that people who hear about the job from an inside source are significantly more likely to stay for at least 6 to 12 months after hire.7
A second strategy is called Realistic Job Previews (RJPs). RJPs inform potential employees about details of the job they are unlikely to know in an attempt to reduce their unmet expectations should they accept a position in the organization. RJPs describe both the positive and negative features of the job with the goal of assisting potential new hires to make an informed decision about a job offer. RJPs have been studied extensively and have been found to reduce turnover of new employees and to increase retention rates when they are used.8
A third strategy that can increase the success organizations have in hiring people who are a good match for the organization is the use of structured behavioral interviews. Valid and reliable selection practices can help organizations to reduce turnover and improve performance.9 Unlike the unstructured interviews commonly used in LTSS, structured interviews are based on an assessment of critical features that distinguish good and poor performers, ask all applicants the same set of questions, and score answers based on a set of predetermined scoring guidelines. Research on structured interviews has reported that they are among the most effective, if not the most effective selection tool currently available.10
B. Orientation and Training Strategies
Socialization is helping new employees understand "how things work around here." It includes getting to know the routines, the co-workers and the individuals a DSP will be working with. It also includes developing an understanding of the mission, vision and values of the organization. When current employees intentionally work to assist newcomers with this process, the new employees stay longer than when currently employees ignore or exclude new employees.11 New employees who have mentors are able to learn more about organizational issues and practices than those who do not have a mentor during their early organizational socialization.12
To be effective, DSPs must have a wide variety of complex skills and be able to implement them without benefit of on-site supervision.13 Many employees admit to not having these skills, and they point to their own lack of competence and that of their co-workers and supervisors as negatively affecting job satisfaction or causing them to want to leave their jobs.14 While there is some overlap, these skills are not the same as for DSPs in health care settings. There are important differences between people with ID/DD and adults with significant disabilities that first occurred in adulthood or old age.15 Adults with ID/DD are substantially more likely to have substantial limitations in economic self-sufficiency and managing finances (88% for adults with ID/DD vs. 45% for adults with substantial disabilities first occurring in adulthood), learning (88% vs. 10%), self-direction and independent decision making (52% vs. 15%); and expressive and receptive communication (40% vs. 13%). The two groups have similar rates substantial limitations with independent living skills such as cooking and shopping (57% vs. 62%), and personal care (20% vs. 14%). Adults with ID/DD are substantially less likely to have a limitation in mobility (18% vs. 31%). Recruits from long-term care settings serving people with disabilities other than ID/DD, and recruits with no experience have extensive training needs to learn how to provide community supports to people with ID/DD.
DSPs in community LTSS for persons with ID/DD need to perform adequately in the 12 competency areas identified in the Community Support Skill Standards (CSSS), and those in residential settings need to satisfy the Community Residential Core Competencies.16 The most pressing training needs for DSPs reported by frontline supervisors and DSPs in a recent five state study were in the areas of communication, documentation, consumer empowerment, health and wellness, and community and service networking.17 The highest rated needs within those categories are reported on Table A-1. The diversity of these topics shows the extensive scope of the role of DSPs supporting individuals with ID/DD.
| TABLE A-1. Training Needs for DSPs in LTSS for Persons with ID/DD | |
| Highest Rated DSP Training Needs | Other Training Needs |
Communication
|
|
Documentation
|
|
Consumer empowerment
|
|
Health and wellness
|
|
Community and service networking
|
|
Many resources are emerging to assist organizations and individual employers improve the effectiveness of the training provided to DSPs.18 Effective training is competency based.19 Competency-based training programs are based on specific, precisely stated outcomes usually called competencies or tasks that have been recently verified as essential for successful employment and includes the following components:
- Identifying what employees need to know (job analysis, mission and vision development).
- Clarifying expectations (job descriptions, performance reviews).
- Understanding current (individual) employee skill gaps (needs assessment/pre-test).
- Setting individual employee goals based on most critical needs (training goals, "just-in-time").
- Identifying training methods and topics (training).
- Providing opportunities to demonstrate and establish learning (post-assessment, skill demonstration, immediate and sustained use of new skills).20
In community LTSS for persons with ID/DD, validated competency standards include the CSSS and the Community Residential Core Competencies.21 Effective training practices take adult learning principles and learning styles into account, use just-in-time training, and create development opportunities for DSPs.22 Training resources such as the College of Direct Support (described in the section V) take these principles into account and develop training around validated competency areas. One Ohio project demonstrated that providing competency based training to DSPs who are seeking a credential increased their job satisfaction and the quality of the supports they provided.
C. Management and Supervision Strategies
Frontline supervisors have a tremendous impact on the work environment and on recruitment and retention success for DSPs. Supervisor tenure was a significant predictor of DSP turnover rate in community residential settings supporting individuals with ID/DD.6 A summary of 18 studies reported that supervisors and managers influence factors such as insufficient orientation, lack of career ladders, lack of recognition, inadequate training, job satisfaction, lack of opportunities for professional growth, minimal support from supervisors, little opportunity for input, a poor understanding of the organization's mission, and lack of clarity about job demands that are associated with DSP turnover.23 This suggests that addressing the problems of supply and demand for DSPs must be done with an understanding that stabilizing the position of frontline supervisor is a critical component of intervention work.
Across several recent studies, annual turnover rates for supervisors of DSPs averaged 21.4% and median vacancy rates were 6%.24 This is important because DSP turnover is higher in settings where the frontline supervisor has changed.6 Many frontline supervisors entered their jobs from a direct support position. Many supervisors report that they taught themselves how to do their job because no orientation or training to their new role had been provided.25 They reported being thrown into their positions with little support or help. Those who had received training reported that mentoring relationships with other supervisors or managers and networking opportunities were the most helpful. Addressing workforce issues for DSPs must include providing better support to frontline supervisors so that they will stay in their positions and implement effective management practices in their work.
To address the challenge of providing competency based training to frontline supervisors in LTSS for persons with ID/DD, a comprehensive job analysis was completed in Minnesota and validated in five other states.26 The resulting competency areas included (a) enhancing staff relations; (b) providing and modeling direct support; (c) facilitating and supporting consumer support networks; (d) planning and monitoring programs; (e) managing personnel; (f) leading training and staff development activities; (g) promoting public relations; (h) maintaining homes, vehicles, and property; (i) protecting health and safety; (j) managing finances; (k) maintaining staff schedules and payroll; (l) coordinating vocational supports; (m) coordinating policies, procedures, and rule compliance; and (n) performing general office work.27
Providing training to frontline supervisors on strategies to reduce recruitment and retention challenges has been effective in at least two demonstration projects. In Kansas, turnover for supervisors declined from 26.8% to 19.2%, and vacancy rates for supervisors declined from 3.2% to 2.6% after training and technical assistance had been provided.24 In a similar project in Minnesota, ten of 13 organizations reported declines in turnover and six of eight reported declines in vacancy rates within 18 to 24 months of receiving training and technical assistance.28 The average decline in turnover was 33%, with nine of the organizations reporting a decline of at least 20%. The average decline in vacancy rate was 28% with five organizations reporting declines of at least 25%.
D. Appendix Notes
-
Bruininks, R.H., Kudla, M.J., Wieck, C.A., & Hauber, F.A. (1980). "Management problems in community residential facilities." Mental Retardation, 18, 125-130.
-
In North Carolina, 70% of administrators reported having problems finding new DSPs. Test, D., Solow, J., & Flowers, C. (1999). North Carolina direct support professionals study: Final report. Charlotte, NC: University of North Carolina at Charlotte. In Alaska, 82% of administrators reported major problems finding qualified direct support employees. Johnston, K. (1998). Developmental disabilities provider direct service worker study: Results and findings. Anchorage, AK: Governor's Council on Disabilities and Special Education. In Minnesota, the proportion of administrators reporting problems finding qualified employees increased from 57% in 1995 to 75% in 1999. Hewitt, A., Larson, S.A., & Lakin, K.C. (2000). An independent evaluation of the quality of services and system performance of Minnesota's Medicaid home and community based services for persons with mental retardation and related conditions. Minneapolis, MN: University of Minnesota, Institute on Community Integration, Research and Training Center on Community Living. Larson, S., Lakin, K.C., & Bruininks, R. (1998). Staff recruitment and retention: Study results and intervention strategies. Washington, DC: American Association on Mental Retardation.
-
Larson, S.A. (1997). Recruitment issues for Minnesota agencies serving people with developmental disabilities or severe and persistent mental illness: Final Report. Minneapolis, MN: Center on Residential Services and Community Living, Institute on Community Integration, University of Minnesota.
-
Hewitt, A., Larson, S.A., & Lakin, K.C. (2000). An independent evaluation of the quality of services and system performance of Minnesota's Medicaid home and community based services for persons with mental retardation and related conditions. Minneapolis, MN: University of Minnesota, Institute on Community Integration, Research and Training Center on Community Living.
-
Positions were vacant an average of 2.8 weeks in Minnesota. Larson, S.A., & Lakin, K.C. (1999). "A longitudinal study of recruitment and retention in small community homes supporting persons with developmental disabilities." Mental Retardation, 178-191. An average of 4.0 weeks in Alaska. Johnston, K. (1998). Developmental disabilities provider direct service worker study: Results and findings. Anchorage, AK: Governor's Council on Disabilities and Special Education. An average of 4.3 weeks in Minnesota HCBS waiver settings. Hewitt, A., Larson, S.A., & Lakin, K.C. (2000). An independent evaluation of the quality of services and system performance of Minnesota's Medicaid home and community based services for persons with mental retardation and related conditions. Minneapolis, MN: University of Minnesota, Institute on Community Integration, Research and Training Center on Community Living. An average of 10.5 weeks in New York. NYSARC. (2000). Staff recruitment and retention: Report on turnover and vacancies. Study and analysis. Delmar, NY: Author.
-
Larson, S., Lakin, K.C., & Bruininks, R. (1998). Staff recruitment and retention: Study results and intervention strategies. Washington, DC: American Association on Mental Retardation.
-
One study followed 124 newly hired DSPs recruited from 110 small group homes supporting individuals with ID/DD. Larson, S., Lakin, K.C., & Bruininks, R. (1998). Staff recruitment and retention: Study results and intervention strategies. Washington, DC: American Association on Mental Retardation. In that study, new employees who heard about their job from a currently employee or another inside source were significantly more likely to remain in their jobs for 12 months than new employees who heard about the job from a newspaper advertisement or another outside source. A total of 33% of newly hired staff remained in their position for 12 months after hire while 14% moved to a different position in the same organization, 38% left the organization voluntarily and 15% were fired. New hires who were more committed to the organization 30 days after hire, those whose expectations about the job were better met and individuals who felt there were few job options were significantly more likely to stay than were other new hires. In a summary of 12 studies, job survival (the number of months a new hire stays in the organization) was 24% higher for employees recruited using inside sources than for employees using outside sources. Wanous, J.P. (1992). Organizational entry: Recruitment, selection, orientation and socialization of newcomers (2nd Edition). New York, NY: Addison Wesley. The benefit was greater among organizations that had high turnover rates. Another study found that employees who heard about the job through multiple informal sources, those who were rehired, and those who learned about the company through a clinical rotation had the most prehire knowledge, whereas those recruited through walking in or advertisements had the least prehire knowledge. Increased prehire knowledge was associated with lower turnover among 234 nursing applicants. Williams, C.R., Labig, C.E., & Stone, T.H. (1993). "Recruitment sources and posthire outcomes for job applicants and new hires: A test of two hypotheses." Journal of Applied Psychology, 78, 163-172. Other studies have confirmed the benefits of using inside recruitment sources in increasing information about and commitment to the job, improving the extent to which prehire expectations are met, and improving job survival. Saks, A.M. (1994). "A psychological process investigation for the effects of recruitment source and organization information on job survival." Journal of Organizational Behavior, 15, 225-244. Taylor, G.S. (1994). "The relationship between sources of new employees and attitudes toward the job." Journal of Social Psychology, 134, 99-110. Zottoli, M.A., & Wanous, J.P. (2000). "Recruitment source research: Current status and future directions." Human Resource Management Review, 10, 353-382. The Saks study showed that both recruitment source and information provided by the organization were significant contributors to job survival.
-
Several meta-analyses that compared the findings of many studies have reported that providing RJPs to reduce unmet expectations can be effective in reducing turnover. For example, one meta-analysis found that RJPs improved retention rates by 9-17%. McEvoy, G.M., & Cascio, W.F. (1985). "Strategies for reducing employee turnover: A meta-analysis." Journal of Applied Psychology, 70, 342-353. Another meta-analysis found that RJPs increased retention of employees 12% for organizations with annual retention rates of 50% and 24% for organizations with annual retention rates of 20%. Premack, S.L., & Wanous, J.P. (1985). "A meta-analysis of realistic job preview experiments." Journal of Applied Psychology, 70, 706-719. These studies, some of which included research conducted in organizations that support individuals with disabilities, suggest that RJPs have a positive effect and that this effect is larger for organizations with higher turnover rates.
-
Thomas, M., & Brull, H. (1993). "Tests improve hiring decisions at Franciscan Health System." Personnel Journal, 72(11), 89-92. Workforce Management. (December 21, 1998). "How to decrease turnover." (on the web at http://www.workforce.com/archive/article/21/97/93.php.)
-
Several high quality studies have confirmed the effectiveness of structured interviews. Hermelin, E., & Robertson, I.T. (2001). "A critique and standardization of meta-analytic validity coefficients in personnel selection." Journal of Occupational and Organizational Psychology, 74, 253-277. Buckley, M.R., & Russell, C.J. (1999). "Validity evidence." In Eder, R.W., & Harris, M.M. (Eds.). The employment interview handbook. Thousand Oaks, CA: Sage Publications, pp. 35-48. Cortina, J.M., Goldstein, N.B., Payne, S.C., Davison, H.K., & Gilliland, S.W. (2000). "The incremental validity of interview scores over and above cognitive ability and conscientiousness scores." Personnel Psychology, 53, 324-351. A book chapter that will be published by the end of 2004 reviews these strategies and provides guidance to employees of LTSS for persons with ID/DD on how to implement them. Larson, S.A., & Hewitt, A.S. (in press). "Selection strategies." In Larson, S. & Hewitt, A. (Eds). Staff recruitment, retention and training for community human services organizations. Baltimore, MD: Paul H. Brookes.
-
New employees often find it is difficult to get to know the routines, traits, and behaviors of their co-workers and the people to whom they provide supports and to learn and complete their job duties and routines of their daily work. Larson, S., Lakin, K.C., & Bruininks, R. (1998). Staff recruitment and retention: Study results and intervention strategies. Washington, DC: American Association on Mental Retardation. Support from co-workers is important. A study of newly hired DSPs found that DSPs who were supported by their co-workers were more likely to stay than those who were not. Bachelder, L., & Braddock, D. (1994). Socialization practices and staff turnover in community homes for people with developmental disabilities. Chicago, IL: University of Illinois at Chicago, Institute on Disability and Human Development, College of Associated Health Professions. Co-workers were reported in another study to be the most available source of socialization information and the most helpful. Louis, M.R., Posner, B.Z., & Powell, G.N. (1983). "The availability and helpfulness of socialization practices." Personnel Psychology, 36, 857-866.
-
Ostroff, C., & Kozlowski, S.W.J. (1993). "The role of mentoring in the information gathering processes of newcomers during early organizational socialization." Journal of Vocational Behavior, 42, 170-183.
-
Hewitt, A. (1998). Identification of competencies and effective training practices for direct support staff working in community residential service for persons with developmental disabilities. Minneapolis, MN: University of Minnesota. Taylor, M., Bradley, V., & Warren, R., Jr. (1996). The community support skill standards: Tools for managing change and achieving outcomes. Cambridge, MA: Human Services Research Institute.
-
Hewitt, A., Larson, S.A., & Lakin, K.C. (2000). An independent evaluation of the quality of services and system performance of Minnesota's Medicaid home and community based services for persons with mental retardation and related conditions. Minneapolis, MN: University of Minnesota, Institute on Community Integration, Research and Training Center on Community Living. Larson, S., Lakin, K.C., & Bruininks, R. (1998). Staff recruitment and retention: Study results and intervention strategies. Washington, DC: American Association on Mental Retardation.
-
Larson, S.A., Lakin, K.C., Kwak, N., & Anderson, L. (2001). "Functional limitations of adults in the US Non-Institutionalized Population: An NHIS-D Analysis." MR/DD Data Brief, 3(3). Minneapolis, MN: University of Minnesota, Research and Training Center on Community Living. Larson, S., Lakin, K.C., Anderson, L., & Kwak, N. (2001). "Characteristics and service use by persons with MR/DD living in their own homes or with family members: NHIS-D analysis." DD Data Brief, 3(1), whole issue. Minneapolis, MN: University of Minnesota, Research and Training Center on Community Living.
-
Hewitt, A. (1998). Identification of competencies and effective training practices for direct support staff working in community residential service for persons with developmental disabilities. Minneapolis, MN: University of Minnesota. Taylor, M., Bradley, V., & Warren, R., Jr. (1996). The community support skill standards: Tools for managing change and achieving outcomes. Cambridge, MA: Human Services Research Institute.
-
Doljanac, R., Larson, S.A., Hewitt, A., & Salmi, P. (unpublished manuscript). National validation study of competencies and training for front line supervisors and direct support professionals. Minneapolis, MN: University of Minnesota, Research and Training Center on Community Living.
-
Hewitt, A.S., Larson, S.A., O'Nell, & Sauer, J. (In press). "Orientation, socialization, networking and professionalization." In Larson, S. & Hewitt, A. (Eds). Staff recruitment, retention and training for community human services organizations. Baltimore, MD: Paul H. Brookes.
-
Blank, W.E. (1982). Competency-based training. Upper Saddle River, NJ: Prentice-Hall. Goldstein, I.L. (1993). Progress in organizational needs assessment, development, and education (3rd ed.). Pacific Grove, CA: Brookes/Cole.
-
O'Nell, S., & Hewitt, A.S. (In press). "Linking training and performance through competency-based training." In Larson, S. & Hewitt, A. (Eds). Staff recruitment, retention and training for community human services organizations. Baltimore, MD: Paul H. Brookes.
-
Hewitt, A. (1998). Identification of competencies and effective training practices for direct support staff working in community residential service for persons with developmental disabilities. Minneapolis, MN: University of Minnesota. Taylor, M., Bradley, V., & Warren, R., Jr. (1996). The community support skill standards: Tools for managing change and achieving outcomes. Cambridge, MA: Human Services Research Institute.
-
O'Nell, S., Hewitt, A.S., & Sauer. (In press). "Out of the classroom and on to employee training programs that work." In Larson, S. & Hewitt, A. (Eds). Staff recruitment, retention and training for community human services organizations. Baltimore, MD: Paul H. Brookes.
-
Hall, P.S., & Hall, N.D. (2002). Hiring and retaining direct-care staff: After fifty years of research, what do we know? Mental Retardation, 40, 201-211.
-
Kansans Mobilizing for Workforce Change Stakeholder Advisory Group. (2004). Kansans mobilizing for change: A statewide workforce development plan to resolve the direct support workforce crisis. Topeka, KS: Kansas Council on Developmental Disabilities.
-
Larson, S.A., Sauer, J., Hewitt, A., O'Nell, S., & Sedlezky, L. (1998). SOS training and technical assistance project for direct support professionals, trainers and frontline supervisors: Executive Summary. Minneapolis, MN: Research and Training Center on Community Living, Institute on Community Integration, University of Minnesota.
-
Hewitt, A.S., Larson, S.A., Lakin, K.C., Sauer, J., O'Nell, S. & Sedlezky, L. (2004). "The Roles and Essential Competencies of the Frontline Supervisors of Direct Support Professionals in Community Services." Mental Retardation, 42, 122-135. Doljanac, R., Larson, S.A., Hewitt, A., & Salmi, P. (unpublished manuscript). National validation study of competencies and training for front line supervisors and direct support professionals. Minneapolis, MN: University of Minnesota, Research and Training Center on Community Living.
-
Hewitt, A.S., Larson, S.A., Lakin, K.C., Sauer, J., O'Nell, S. & Sedlezky, L. (2004). "The Roles and Essential Competencies of the Frontline Supervisors of Direct Support Professionals in Community Services." Mental Retardation, 42, 122-135.
-
Hewitt, A., Larson, S., Sauer, J., Anderson, L., & O'Nell, S. (2001). Partnerships for Success: Retaining Incumbent Community Support Human Service Workers by Upgrading their Skills and Strengthening Partnerships among Workforce Centers, Educational Programs, and Private Businesses. University of Minnesota Subcontract Final Report. Minneapolis, MN: University of Minnesota, Research and Training Center, Institute on Community Integration.