
CREDENTIALING, LICENSING, AND REIMBURSEMENT OF THE SUD WORKFORCE:
A REVIEW OF POLICIES AND PRACTICES ACROSS THE NATION
Nilufer Isvan, Rachael Gerber, David Hughes, Kristin Battis, and Evan Anderson
Human Services Research Institute
John O'Brien
Technical Assistance Collaborative
November 2019
Printer Friendly Version in PDF Format (134 PDF pages)
ABSTRACT
The main purpose of this study was to investigate the barriers to and facilitators of licensing, credentialing, and insurance reimbursement for substance use disorder (SUD) treatment providers across the nation. The study included an environmental scan of key issues, reviews of credentialing, licensing, and reimbursement policies in the 50 states and D.C., and in-depth case studies of four states that implemented innovative strategies to incentivize their SUD workforce.
The study identified as key barriers to entry to the field: (1) variability across (and in some cases, within) states in career ladders and certification/licensing requirements; (2) low education requirements for qualification, lack of education programs focusing on SUD treatment; (3) unavailability of licensure in 20 states; (4) Lack of pathways to independent practice; (5) lack of insurance coverage for SUD services; and (6) low reimbursement rates compared to other behavioral health professions. The results of this study suggest that state-level system redesign efforts are most effective when accompanied by initiatives to support providers in adapting their practices to the new environment. Establishing state licensure statutes is a strong facilitator of insurance reimbursement, especially if accompanied by workforce development efforts and grandfathering clauses for existing practitioner.
This report was prepared under contract #HHSP233201600015 between HHS's ASPE/DALTCP and the Human Services Research Institute. For additional information about this subject, you can visit the DALTCP home page at https://aspe.hhs.gov/office-disability-aging-and-long-term-care-policy-daltcp or contact the ASPE Project Officers, Judith Dey and Kristina West, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201; Judith.Dey@hhs.gov, Kristina.West@hhs.gov.
DISCLAIMER: The opinions and views expressed in this report are those of the authors. They do not reflect the views of the Department of Health and Human Services, the contractor or any other funding organization. This report was completed and submitted on February 2019.
"ACRONYMS
The following acronyms are mentioned in this report and/or appendices.
| AADC | Advanced Alcohol and Drug Counselor |
|---|---|
| ADC | Alcohol and Drug Counselor |
| ASAM | American Society of Addiction Medicine |
| ASPE | HHS Office of the Assistant Secretary for Planning and Evaluation |
| BHC | Behavioral Health Collaborative |
| BHWRC | University of Michigan Behavioral Health Workforce Research Center |
| CACREP | Council for Accreditation of Counseling and Related Educational Programs |
| CADC | Certified Alcohol and Drug Counselor |
| CADTP | California Association of DUI Treatment Programs |
| CASAC | Credentialed Alcoholism and Substance Abuse Counselor |
| CCAPP | California Consortium of Addiction Programs and Professionals |
| CCBHC | Certified Community Behavioral Health Clinic |
| CCS | Certified Clinical Supervisor |
| CHIP | Children's Health Insurance Program |
| CIBHS | California Institute for Behavioral Health Solutions |
| CMS | HHS Centers for Medicare & Medicaid Services |
| COD | Co-Occurring Disorder |
| COR | Contracting Office's Representative |
| CPS | Certified Prevention Specialist |
| CPT | Current Procedural Terminology |
| CRPA | Certified Recovery Peer Advocate |
| CS | Clinical Supervisor |
| CSAT | SAMHSA Center for Substance Abuse Treatment |
| CTAC | New York Community Technical Assistance Center |
| D.C. | District of Columbia (also known as Washington, D.C.) |
| DALTCP | ASPE Office of Disability, Aging and Long-Term Care Policy |
| DEA | Drug Enforcement Administration, U.S. Department of Justice |
| DHCS | California Department of Health Care Services |
| DHHS | North Carolina Department of Health and Human Services |
| DMC-ODS | Drug Medi-Cal Organized Delivery System |
| DSRIP | Delivery System Reform Incentive Payment |
| DUI | Driving Under the Influence |
| FFS | Fee-For-Service |
| FTE | Full-Time Equivalent |
| FY | Fiscal Year |
| HCPCS | Healthcare Common Procedure Coding System |
| HHS | U.S. Department of Health and Human Services |
| HHSC | Texas Health and Human Services Commission |
| HRSA | HHS Health Resources Services Administration |
| IC&RC | International Certification and Reciprocity Consortium |
| IMD | Institution for Mental Diseases |
| IOM | Institute of Medicine |
| LAC | Licensed Addiction Counselor |
| LADC | Licensed Alcohol and Drug Counselor |
| LADC-MH | Licensed Alcohol and Drug Counselor--Mental Health |
| LCDC | Licensed Chemical Dependency Counselor |
| LCDP | Licensed Chemical Dependency Professional |
| LCDS | Licensed Chemical Dependency Supervisor |
| LCSW | Licensed Clinical Social Worker |
| LICDC-CS | Licensed Independent Chemical Dependency Counselor--Clinical Supervisor |
| LME | Local Management Entity |
| LOCADTR | Level of Care for Alcohol and Drug Treatment Referral |
| LPC | Licensed Professional Counselor |
| MAC | Master Addiction Counselor |
| MACPAC | Medicaid and CHIP Payment and Access Commission |
| MAT | Medication-Assisted Treatment |
| MCO | Managed Care Organization |
| MCTAC | New York Managed Care Technical Assistance Center |
| MFT | Marriage and Family Therapist |
| MH | Mental Health |
| MHPAEA | Mental Health Parity and Addiction Equity Act |
| MLADC | Master Licensed Addiction and Drug Counselor |
| MMC | Medicaid Managed Care |
| MRT | Medicaid Redesign Team |
| N-SSATS | National Survey of Substance Abuse Treatment Services |
| NAADAC | National Association for Alcoholism and Drug Abuse Counselors (now the Association for Addiction Professionals) |
| NBCC | National Board for Certified Counselors |
| NCAC | National Certified Addiction Counselor |
| NCSAPPB | North Carolina Substance Abuse Professional Practice Board |
| NCSE | National Clinical Supervision Endorsement |
| NHBDAS | New Hampshire Bureau of Drug and Alcohol Services |
| NSDUH | National Survey on Drug Use and Health |
| OASAS | New York Office of Alcoholism and Substance Abuse Services |
| OMH | New York Office of Mental Health |
| ONDCP | Office of National Drug Control Policy, Executive Office of the President of the United States |
| PLADC | Provisional Licensed Alcohol and Drug Counselor |
| RHP | Regional Healthcare Partnership |
| RSS | Recovery Support Services |
| SAMHSA | HHS Substance Abuse and Mental Health Services Administration |
| SBIRT | Screening, Brief Intervention, and Referral to Treatment |
| SNP | Special Needs Plan |
| SOP | Score of Practice |
| SPA | State Plan Amendment |
| STR | State Targeted Response to the Opioid Crisis |
| SUD | Substance Use Disorder |
| SUPPORT | Substance Use Disorder Prevention that Promotes Opioid Recovery and Treatment (also known as SUPPORT for Patients and Communities Act of 2019) |
| TAP 21 | SAMHSA Technical Assistance Publication #21 |
| UCLA | University of California, Los Angeles |
| VA | U.S. Department of Veterans Affairs |
EXECUTIVE SUMMARY
Introduction
The United States is experiencing a workforce shortage in the substance use disorder (SUD) treatment field, an issue that has received increased attention from policymakers and health care professionals due to its centrality in addressing the nationwide opioid epidemic. Multiple factors--including limited insurance coverage for SUD services, low reimbursement rates, and low salaries for treatment professionals--have made the SUD treatment field a relatively unattractive specialization. And despite an expansion in insurance coverage for SUD services in recent years, barriers presented by insurance-based payment often limit providers' eligibility or discourage them from joining insurance networks, thereby preventing providers from using their full capacity to appropriately treat people.
In September 2018, the U.S. Department of Health and Human Services Office of the Assistant Secretary for Planning and Evaluation (ASPE) contracted with the Human Services Research Institute to conduct a study of licensing and credentialing policies for SUD treatment providers across the 50 states and the District of Columbia (D.C.) and to examine billing eligibility and reimbursement for SUD treatment services across Medicaid, Medicare, and commercial insurance plans. The purpose of the project is to examine state variation in policies and to investigate the barriers to and facilitators of increased treatment capacity and insurance reimbursement for SUD providers across the nation.
SUD treatment services are provided by a broad range of practitioners, including physicians, nurses, behavioral health counselors, social workers, psychologists, and many others. This study focuses on the SUD counselor segment of the workforce, as this segment is particularly impacted by licensing, credentialing, and reimbursement barriers due to the lack of standardization on qualifications and credentials.
Methods
The first phase of the project was an environmental scan to gather information about existing knowledge on this issue and to uncover knowledge gaps. The scan, which was conducted through a literature review and interviews with experts in the field, laid the foundation for a review of the various policies that regulate SUD provider credentialing, licensing, and reimbursement across the nation. Parallel to that review, we conducted in-depth case studies of four states that served as informative examples of innovative SUD workforce development strategies and efforts to incentivize provider participation in insurance networks.
Key Findings
Licensing and Credentialing Substance Use Disorder Counselors
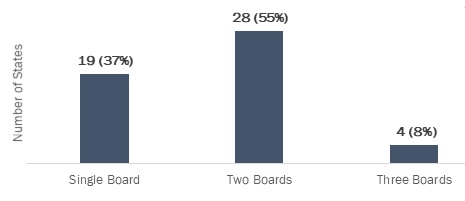
There are multiple credentialing bodies for the SUD counseling profession, both at the national level and within individual states. Nineteen (19) states (37%) have a single board that oversees licensure and/or certification for all SUD credentials within the state, and the rest (63%) have multiple boards offering different credentials, often with no state-level standards for minimum requirements.
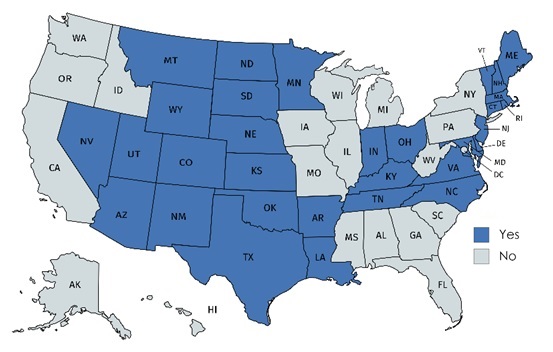
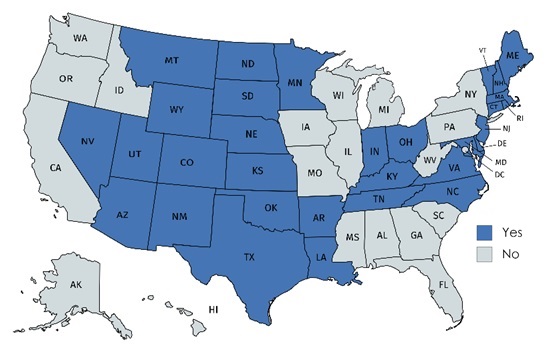
Thirty-one (31) states (61%) offer licensure for SUD counseling; the remaining 20 states (39%) offer certification only (Exhibit ES1).
| EXHIBIT ES1. States Offering Licensure for SUD Counseling |
|---|
 |
There is wide variation in states' respective career ladders for SUD counselors and in educational and practice requirements for these credentials. To obtain the highest SUD counseling credential available within the state, 37 states (73%) require a master's degree, six states (12%) require a bachelor's degree, four states (8%) require an associate degree, and three states (6%) require only a high school diploma or equivalent. One state currently has no minimum degree requirement. The minimum number of required practice hours ranges from 1,000 hours (equivalent to half a year) to 12,000 (6 years) for the states' highest SUD counseling credential.
Based on the environmental scan, state review, and case studies, we identified the following credentialing-related barriers to entering the field and examples of initiatives to facilitate entry:
| Barrier | Facilitator |
|---|---|
| #1. Lack of standard credentials and inaccessibility of qualification information |
|
| #2. Low and non-standard training and education requirements for practice |
|
Billing Eligibility and Reimbursement
The availability of state licensure regulations for SUD counselors facilitates their billing eligibility across public and private insurance plans. Our review identified only 11 states where an SUD counselor is eligible for direct reimbursement from the state's Medicaid plan as an independent billing provider; all of them offer licensure for SUD counseling. In states where they are not eligible to enroll as independent providers, SUD counselors must work in a facility/program that is reimbursed on their behalf. UnitedHealth/Optum, the nation's largest commercial health insurer, requires a license as a prerequisite for independent billing status. An SUD counselor is eligible in only 13 states (out of 50 states and D.C.) among Optum's commercial plans, all states with licensure. While licensure is a facilitator, it by no means guarantees billing eligibility across insurance plans.
The following are key barriers and facilitators related to billing eligibility and direct reimbursement of SUD counselors:
| Barrier | Facilitator |
|---|---|
| #1. Lack of insurance coverage for SUD services and low reimbursement rates |
|
| #2. Uneven availability of state-regulated licensure across the nation |
|
| #3. Legislative, administrative, and financial burdens of joining insurance networks and filing claims |
|
Conclusions
This study revealed that the SUD counseling profession faces multiple interconnected challenges associated with complex training, credentialing, and payment structures. Compared to other counseling professions like clinical social work and marriage/family therapy, addiction counseling is a less desirable specialty due to the difficulty in obtaining a credential or a license, low portability of credentials across state lines, relatively low earning potential, and multiple barriers to establishing an independent practice, joining insurance networks, and filing claims.
The absence of a clearly defined career ladder specific to SUD counseling, often vague and inconsistent requirements for advancing within the profession, low reimbursement, and relatively low earning potential have combined to make this an undesirable area of concentration in comparison to other behavioral health specialties. Despite the innovative initiatives to address these challenges and to facilitate entry into and advancement in the field described in this report, workforce shortages remain one of the key barriers to addressing the national opioid crisis.
Promising measures for addressing the workforce shortage include:
-
The adoption of common addiction education standards as a condition of providing SUD counseling.
-
Increased availability of degree programs offering standard curricula in SUD treatment.
-
Financial incentives including increased reimbursement, scholarships, and student loan repayment programs that incentivize students to pursue advanced degrees in SUD treatment.
An additional approach to enhancing the workforce would be to introduce addiction as a specialization track in behavioral health degree programs, with standards that address the required core competencies of addiction counseling. This would incentivize students in these programs to enter the SUD field, building on the education and internships they completed during their academic training. Such efforts would necessitate the collaboration of multiple credentialing bodies, state agencies, and institutions of higher education.
Systemic reform efforts that simultaneously address several interlinked barriers with participation from multiple state and national stakeholders hold the highest promise for the future of the workforce.
INTRODUCTION
Background
Substance use disorder (SUD) services have traditionally been underfunded, especially in comparison to other behavioral health services such as mental health treatment and family and marriage therapy. For example, spending on SUD treatment services constituted only 1.0% of total health care expenditures in 2014, less than one-fifth of the share of mental health expenditures (5.9%). Moreover, no substantial change is projected in these shares through 2020 (SAMHSA, 2014). In line with this difference in overall expenditures, earning potential of SUD counselors is also lower than counselors in other behavioral health professions: In 2017, the median salary for an SUD counselor was $41,070, compared to $46,890 for social workers and $49,170 for marriage and family therapists (MFTs) (U.S. Bureau of Labor Statistics, 2018). Low and spotty coverage by public and commercial insurance plans and comparatively lower salaries have made the SUD field a relatively unattractive specialization for counseling professionals, leading to a nationwide workforce shortage in the field (Ryan, Murphy, & Krom, 2012). This issue has received increasing attention from policymakers and health care professionals in recent years due to its centrality in addressing the nationwide opioid epidemic (Commission on Combating Drug Addiction & the Opioid Crisis, 2017; Beck, Manderscheid, & Buerhaus, 2018).
State and federal legislation during the past few decades, such as state parity rules, the 2008 Mental Health Parity and Addiction Equity Act (MHPAEA), and several health market reforms, have considerably expanded insurance coverage for SUD services. More recent policy initiatives by the Centers for Medicare & Medicaid Services (CMS)--most notably Medicaid Section 1115 waivers, which allow states to expand coverage for SUD services and to better integrate these services into their overall health care system--have further increased reimbursement options for these services.
To some extent, these policy changes encouraged SUD providers to join insurance networks. Data from the National Survey of Substance Abuse Treatment Services (NSSATS) indicate that the proportion of SUD facilities that accept Medicaid payments increased by 16.4% between 2010 and 2017. Acceptance of private insurance and Medicare payments also showed modest increases during this period--by 11.1% and 9.4%, respectively. However, a substantial number of SUD providers continue to operate outside of insurance networks. 2017 N-SSATS data show that 30% of provider facilities do not accept private insurance payments, 36% do not accept Medicaid, and 65% do not accept Medicare (SAMHSA, 2011; 2018a). The unmet need for treatment continues to be of concern: According to the National Survey on Drug Use and Health (NSDUH), an estimated 19.7 million people aged 12 or older in 2017 met the clinical criteria for an SUD, whereas only 2.5 million received treatment at a specialty facility. Inability to pay for treatment was a commonly reported reason for needing but not receiving treatment (SAMHSA, 2018b). These numbers indicate an urgent need to increase the number of providers that accept public and private insurance payments for SUD services.
Increased coverage of SUD services in recent years has been accompanied by sweeping changes in the SUD treatment delivery environment, driven by factors such as increased emphasis on quality metrics and service integration as requirements for joining insurance networks (Buck, 2011). Recent advances in SUD treatment approaches have contributed to this changing environment, adding new competency requirements for practitioners. Additionally, public and private insurance plans are increasingly requiring certification--and in many cases, state licensure--as a condition for joining their networks (Hagedorn, Culbreth, & Cashwell, 2012). On the other hand, certification requirements and related education programs in the addiction field have been falling behind emerging competency requirements for the past two decades (Mustaine, West, & Wyrick, 2003), resulting in an underqualified workforce facing barriers to joining insurance networks.
Although states are beginning to revise their certification and licensing policies for SUD providers to address these barriers in the long run (Boozang, Bachrach, & Detty, 2014), the short-term impact of these system redesign efforts has been an increase in SUD workforce shortages and continued barriers to joining insurance networks as the existing practitioners and new professionals catch up with network requirements (Andrews et al., 2015). The initial step in addressing these issues is to understand the barriers to developing an adequate SUD workforce and the credentialing, licensing, and reimbursement policies that prevent or discourage SUD service providers from joining insurance networks.
Study Overview
The main purpose of this study is to investigate the barriers to and facilitators of increased treatment capacity and insurance reimbursement for SUD providers across the nation. SUD treatment services are provided by a broad range of practitioners, including behavioral health counselors, recovery specialists, social workers, psychiatrists, psychologists, primary care and emergency physicians, nurse practitioners, pediatricians, and obstetricians. This study focuses on the sector of this workforce most impacted by the certification, licensing, and reimbursement barriers mentioned above: addiction counselors. In the rest of this report, we refer to this workforce segment as the "SUD treatment" or "SUD counselor" workforce, while acknowledging that it is a specific sector of the broader group of professionals who provide addiction-related treatment services. Although substance use prevention workers constitute a separate career ladder, there are points of intersection between the two such that it is possible to move to the treatment ladder from some rungs of the prevention ladder. We therefore included the prevention workforce in our state review of credentialing and licensing policies.
The first phase of the project involved an environmental scan, which consisted of a literature review and interviews with experts in the field, to gather information about existing knowledge on this issue and to uncover knowledge gaps. The environmental scan laid the foundations for a review of the policies that regulate SUD-specific provider credentialing, licensing, and reimbursement in 50 states and the District of Columbia (D.C.).
Parallel to that review, we conducted in-depth case studies of four states that provide informative examples of SUD workforce development strategies and efforts to incentivize provider reimbursement through health plans.
Research Questions
The study was structured around the following research questions:
- How do insurers reimburse providers for SUD treatment?
- What requirements do states have for licensing and credentialing of SUD providers?
- What additional requirements do state Medicaid plans impose for determining which providers may bill Medicaid? Which services may they bill?
- How do reimbursable services and eligible providers differ between Medicare and Medicaid?
- Do private insurers impose additional requirements in terms of which SUD treatment providers may bill and for which services they may bill?
- How do reimbursement policies impact participation in insurance networks?
- What are the major incentives and disincentives to receiving reimbursement through insurance plans and Medicaid programs?
- What efforts have states made to increase the number of SUD treatment providers that accept insurance?
Organization of the Report
The remaining sections of this report are organized into the following sections:
-
Methodology. This section briefly describes our methods for each of the study's research tasks: (1) the environmental scan; (2) state-level review of licensing and credentialing requirements for SUD treatment providers; (3) state-level review of billing eligibility and reimbursement across insurance types; and (4) in-depth case studies with four states. Further detail about our methods for each of these tasks is contained in Appendices C-F.
-
State Approaches to Licensing and Credentialing SUD Treatment Providers. This section presents findings from our state-level review of licensing/credentialing policies, including states' respective career ladders for the SUD workforce, licensure vs. certification, affiliation with state and national credentialing bodies, and variation in credentialing requirements for the highest level of SUD counselor in each state. Detailed tables on requirements for all SUD credentials compiled for this review are in Appendix A. The section concludes with a discussion of barriers and facilitators associated with licensing and credentialing based on the results of the state-level review, environmental scan, and case studies.
-
Billing Eligibility and Reimbursement. This section begins with a brief overview of how providers submit claims to insurance companies for reimbursement. The subsections that follow present the results of our review of billing eligibility and reimbursement for the SUD workforce across Medicaid, Medicare Advantage, and commercial insurance plans. Due to limited documentation available online on billing/reimbursement policies for Medicare Advantage and commercial insurance plans, the subsections on these plans are relatively brief, with the bulk of our findings and discussion focused on Medicaid. The section concludes with a discussion of key barriers and facilitators associated with reimbursement for the SUD workforce based on the results of the state-level review, environmental scan, and case studies.
-
Conclusions and Implications. This section synthesizes the main findings and policy implications of the study.
-
Appendices A-G. Much of the detailed data compiled for this report, and the technical details of the study's methodology, are contained in the appendices. Detailed tables on licensing/credentialing requirements are in Appendix A; a detailed table on reimbursement codes by state is in Appendix B; Appendices C-F contain detailed descriptions of our methodology; Appendix G contains summaries of the four case studies.
METHODOLOGY
Environmental Scan
The environmental scan consisted of a comprehensive literature review and in-depth, semi-structured interviews with nine key informants with expertise in the areas of licensing and credentialing and/or insurance reimbursement for SUD services.
Literature Review
We scanned the peer-reviewed published literature, as well as grey literature, to gather information on the barriers and facilitators to licensing and credentialing and insurance reimbursement for SUD providers. For journal articles, we used PubMed and Google Scholar to scan for articles published in the past 10 years using search terms relevant to the research questions of the study. To complement the database searches, we scanned the past 10 years' worth of issues for a predetermined list of journals. The journal list is provided in Appendix C. For the grey literature scan, we searched the publications of a predetermined list of agencies and organizations for reports, policy briefs, white papers, or guidelines issued during the past 10 years related to SUD provider licensing and credentialing and insurance reimbursement. The list of agencies and organizations is provided in Appendix C.
Expert Interviews
In January and early February 2018, we conducted semi-structured interviews with nine key informants to provide insight into SUD provider licensing and credentialing and billing for SUD services. Key informants were selected to represent a range of expertise, including knowledge of licensing and credentialing regulations, Medicaid and Medicare policies, and commercial insurance reimbursement for SUD treatment services. First, we generated a list of potential key informants based on information gathered from the literature review and discussions with the U.S. Department of Health and Human Services (HHS) Office of the Assistant Secretary for Planning and Evaluation (ASPE) contracting office's representatives (CORs). We identified individuals who either authored key articles or reports and/or published multiple recent articles central to our research questions. In consultation with the CORs, we selected nine key informants from an initial list of 15 and invited them to participate in the study. All nine agreed to be interviewed.
In collaboration with the CORs, we developed an interview guide that consisted of 17 questions and prompts based on the research questions of the study. Prior to each interview, we customized the guide to the informant's area of expertise and shared it with them. The interviews were conducted via telephone and lasted approximately one hour. Key informants were informed that their names would not be used in the reports resulting from this study.
Review of State Approaches to Licensing and Credentialing Substance Use Disorder Treatment Providers
The SUD treatment workforce is diverse and multidisciplinary, consisting of counselors, social workers, psychologists, physicians, nurses, and others. The focus of this review is on the SUD counseling workforce. The broad variation across states in available titles and credentials for this segment of the workforce required an analysis and reporting method that would allow for cross-state comparisons from a relatively standard slate of practitioner categories. The classification framework we used for this purpose was based on the national career ladder proposed by the Substance Abuse and Mental Health Services Administration (SAMHSA), which describes five levels of SUD counselor with increasing expertise and responsibility--ranging from entry-level SUD technician to a master's level independent clinical SUD counselor (SAMHSA, 2011). We added two categories to the five that constitute this model career ladder: peer recovery specialist and prevention specialist.
A data collection template was developed in Excel to define the data elements to be extracted for every SUD counseling and peer recovery credential available within each state. The elements included information about the board that oversees licensure or certification and specific requirements for education, minimum degree, practice hours, examinations, supervision, and other factors related to licensing/credentialing. These data elements are described in detail in Appendix D.
The review was conducted between March and June 2018. A single analyst searched for information from states' addiction counseling regulatory licensing and/or credentialing websites. At the time data were extracted to the template, the analyst classified all credentials for each state into one of the seven categories. We based the classification primarily on the minimum degree required, but also considered the structure of the state's career ladder and where in that structure a title is situated, as well as whether independent practice without supervision is authorized for the credential. A more detailed description of our methods is provided in Appendix D. A second analyst reviewed all data extracted to the template against the source websites for accuracy.
We supplemented these data with information on addiction counselor scopes of practice (SOPs) collected and made available online by the Behavioral Health Workforce Research Center (BHWRC) at the University of Michigan.[1]
Review of Billing Eligibility and Reimbursement
Provider Type
Like the review of licensing and credentialing, our review of billing eligibility and reimbursement focused on the SUD counseling workforce. The environmental scan revealed that most other types of providers who treat people for SUD--such as psychologists, clinical social workers, professional counselors, physicians, and nurses--are typically eligible for insurance reimbursement, the one exception being that professional counselors are not eligible for reimbursement under Medicare. In contrast to these other professions, states' approaches to licensing and credentialing of SUD counselors vary widely, suggesting a corresponding level of variability across states in billing eligibility. In this report, therefore, we focused on the SUD counseling workforce, which we defined as practitioners who are licensed or certified in SUD counseling and who do not hold an additional credential in another discipline, such as clinical psychology, social work, or professional counseling.
Billing Codes
Our review was guided by eight billing codes for SUD services. Multiple coding systems are used to identify services for reimbursement, the most common being the Current Procedural Terminology (CPT) and the Healthcare Common Procedure Coding System (HCPCS). We focused on outpatient services that can be billed by individual-level practitioners rather than services billed by facilities, such as residential or inpatient treatment. A subset of HCPCS codes are specific to SUD treatment services, while their equivalent CPT codes are applicable to both mental health and SUD services. This review therefore focused on SUD-specific HCPCS codes. Exhibit 1 displays these codes and the corresponding level of care as defined by the American Society of Addiction Medicine (ASAM) as follows:
- 0.5: Early intervention.
- 1.0: Outpatient services.
- 2.1: Intensive outpatient services.
| EXHIBIT 1. Billing Codes used in Review of Reimbursement Policies | ||
|---|---|---|
| ASAM Level | Billing Code | Billing Code Description |
| 0.5 | H0001 | Alcohol and/or drug assessment |
| 0.5 | H0049 | Alcohol and/or drug screening |
| 0.5 | H0050 | Alcohol and/or drug services, brief intervention, per 15 minutes |
| 1 | H0004 | Behavioral health counseling and therapy, per 15 minutes |
| 1 | H0038 | Self-help/peer services, per 15 minutes |
| 1, 2.1 | H0006 | Alcohol and/or drug services; case management |
| 1, 2.1 | H0007 | Alcohol and/or drug services; crisis intervention |
| 2.1 | H0015 | Alcohol and/or drug services; intensive outpatient |
| SOURCE: HCPCS H-Codes, https://hcpcs.codes/h-codes/. | ||
Higher levels of ASAM's continuum of care involve hospitalization and residential care and are subject to certification, licensing, and reimbursement requirements of facilities rather than individual practitioners; they are, therefore, outside the scope of this study. Data on Medicaid coverage of the entire ASAM continuum of care by state are available in the report to Congress by the Medicaid and CHIP Payment and Access Commission (MACPAC, 2018).
Billing codes are known to vary across states and payers; therefore, our methodology incorporated an approach to searching for comparable billing codes in cases where one of these eight codes is not in use in a given state. Appendix E provides further detail about the use of alternate billing codes in this review.
Search Domain and Strategy
The search domain for this review was documentation of billing eligibility and reimbursement that is within the public domain and available online from state Medicaid, Medicare Advantage, and commercial insurance plans. There is broad variability across states and payers in the level of available detail on billing policies, and the format and location of that information. Medicaid plans, since they are publicly funded, make more detail available than do commercial plans, which typically consider their billing and reimbursement policies proprietary.
For Medicaid, we went to each state's official Medicaid website and searched for three types of documentation: (1) provider and/or billing manuals; (2) fee schedules; and (3) provider enrollment resources. These resources were typically for fee-for-service (FFS) plans. As a rule, we reviewed whatever billing documentation was linked directly from state Medicaid websites; if the state has an FFS plan, we used that plan; if the state does not have an FFS plan, we searched for documentation from each of the managed care plans listed on the state's website.
We reviewed these resources to determine the following:
-
If SUD counseling professionals at any level are eligible to enroll as an independent "billing provider" (someone who can be reimbursed directly by Medicaid) or whether they are required to work in a facility, such as an SUD treatment program, that is reimbursed on their behalf.
-
If each of the eight billing codes selected for this review are used to bill for services, and if not, whether comparable alternate codes are used.
-
If SUD counselors are eligible to be reimbursed for each of the billing codes.
All information was recorded into an Excel template designed to standardize data across states for analysis. Appendix E provides further detail about our data extraction and data coding methods.
Commercial plans and Medicare Advantage plans, we quickly found, do not typically make billing documentation available to the public. UnitedHealth/Optum was the only nationwide commercial insurer that had state-by-state billing information in the public domain. For our analysis of commercial insurance, we therefore relied on billing eligibility information from UnitedHealth/Optum's Provider Express portal.[2] These methods are described further in Appendix E.
The review and data extraction were conducted between July and October 2018.
Case Studies
We selected four states for in-depth case studies; they were selected on the basis that they had implemented various strategies to incentivize providers to join provider networks and accept insurance reimbursement. To develop an initial list of candidate states, we relied on the results of our environmental scan. We polled our key informants and supplemented their suggestions with our findings from the literature review to arrive at a list of 12 candidate states. We then examined the relevant epidemiological and socioeconomic characteristics of the candidate states to develop a final list of states that varied in terms of these characteristics. California, New York, North Carolina, and Texas were selected for in-depth study. Appendix F provides summary information on these states' characteristics and sources of data used in the selection process.
We contacted the agency responsible for SUD services in the selected states to provide information about the study and to request an interview with the appropriate senior staff member. During the initial interview, we solicited recommendations for other individuals in the state who could provide us with insights about the SUD workforce from both the administrator and provider points of view. At least two informants were interviewed in each state. The interview findings were supplemented with background research on the state's health care system and recent policy initiatives relevant to behavioral health service delivery and provider incentives. Draft case summaries of each state were submitted to the informants for review and revised based on their feedback before being reviewed by ASPE. Summary results of the case studies are provided in Appendix G.
STATE APPROACHES TO LICENSING AND CREDENTIALING SUBSTANCE USE DISORDER TREATMENT PROVIDERS
Career Ladder for the Substance Use Disorder Treatment Workforce
In 2010, SAMHSA convened a stakeholder group to develop a career ladder and model SOPs for the SUD counseling workforce (SAMHSA, 2011). Exhibit 2 shows the five categories defined by the stakeholder group and a brief description of the educational attainment and supervision requirements envisioned for each.
| EXHIBIT 2. SAMHSA's Model Career Ladder and SOPs for the SUD Treatment Workforce | ||
|---|---|---|
| SAMHSA Category | SAMHSA Category Title | Brief Description |
| Category 4 | Independent Clinical SUD Treatment Counselor/Supervisor | Typically has a master's degree and is licensed to practice independently |
| Category 3 | Clinical SUD Counselor | Typically has a master's degree and either has not yet attained a license or the license is restricted to practice under supervision |
| Category 2 | SUD Counselor | Has a bachelor's degree and provides services under clinical supervision |
| Category 1 | Associate SUD Counselor | Has an associate degree and can provide services under supervision |
| SUD Technician | SUD Technician | Has a high school diploma or equivalent and works under supervision |
We categorized the findings from our review of states' licensing and credentialing requirements into this framework, adding a sixth category for "peer recovery specialist." We separated credentials for supervision (e.g., Certified Clinical Supervisor or CCS) into their own category because their requirements (focused mostly on supervision skills) are typically overlays to the requirements for another underlying credential. We also classified Prevention Specialists into their own category because SAMHSA's career ladder is focused on SUD treatment.
Exhibit 3 shows the number of states with at least one credential for each of SAMHSA's five categories, plus peer recovery specialist.
| EXHIBIT 3. Number of States with at Least 1 SUD Treatment Credential, by Category (SAMHSA's 5 categories plus peer recovery) |
|---|
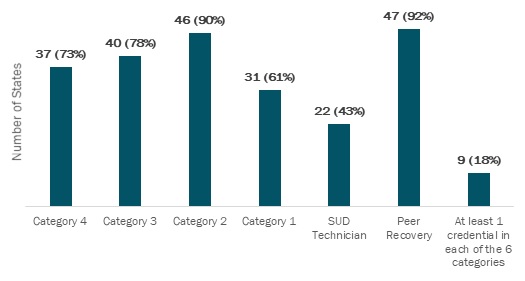 |
In all, 37 states (73%) have a credential equivalent to SAMHSA's Category 4 that allows for independent practice without supervision. We included a non-licensed, certified credential in this category if it was the terminal (highest) available SUD credential in the state and came with an authorization to practice independently without supervision.[3] A total of 40 states (78%) have a credential in Category 3 and 46 (90%) have a credential equivalent to SAMHSA's Category 2.
Credentials at the lower rungs of SAMHSA's career ladder were less frequent, identified in 31 states (61%) for Category 1 and 22 states (43%) for entry-level SUD technician. A greater number of states (47, or 92%) have a credential for peer recovery specialist. Nine states (18%) have at least one credential in each of the six categories.
Exhibit 4 on the following page summarizes the number of SUD treatment credentials we identified for each category by state. The number of available credentials ranged from three to 16 per state. On one hand, a greater number of credentials can signify more entry points into the field for individuals with varying levels of education and experience; on the other hand, numerous and often overlapping credentials can create confusion and burden to those seeking to enter the field and those pursuing advancement within it.
The title of every credential by category and by state is in Exhibit A1. Requirements for each credential (discussed in a later subsection on state variations) are also provided as detailed tables in Appendix A.
| EXHIBIT 4. Number of SUD Treatment Credentials by SAMHSA Category and Total SUD Treatment Credentials, by State | ||||||||
|---|---|---|---|---|---|---|---|---|
| State | Cat 4 | Cat 3 | Cat 2 | Cat 1 | Tech | Peer | Superv | Total |
| Alabama | 1 | 1 | 4 | 1 | 1 | 1 | 9 | |
| Alaska | 1 | 2 | 2 | 2 | 1 | 8 | ||
| Arizona | 1 | 1 | 2 | 1 | 1 | 1 | 1 | 8 |
| Arkansas | 1 | 1 | 2 | 1 | 1 | 1 | 7 | |
| California | 2 | 1 | 2 | 1 | 1 | 3 | 10 | |
| Colorado | 1 | 1 | 1 | 1 | 1 | 5 | ||
| Connecticut | 1 | 1 | 1 | 1 | 1 | 1 | 6 | |
| Delaware | 1 | 1 | 1 | 1 | 1 | 5 | ||
| D.C. | 2 | 2 | 1 | 1 | 6 | |||
| Florida | 1 | 1 | 1 | 1 | 1 | 5 | ||
| Georgia | 1 | 2 | 2 | 1 | 2 | 1 | 1 | 10 |
| Hawaii | 1 | 1 | 1 | 3 | ||||
| Idaho | 1 | 1 | 1 | 1 | 1 | 5 | ||
| Illinois | 2 | 1 | 1 | 1 | 1 | 1 | 7 | |
| Indiana | 1 | 3 | 4 | 3 | 2 | 2 | 1 | 16 |
| Iowa | 1 | 1 | 2 | 1 | 1 | 1 | 7 | |
| Kansas | 1 | 1 | 1 | 1 | 4 | |||
| Kentucky | 1 | 1 | 1 | 1 | 4 | |||
| Louisiana | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Maine | 1 | 1 | 1 | 1 | 4 | |||
| Maryland | 1 | 1 | 3 | 1 | 1 | 1 | 8 | |
| Massachusetts | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Michigan | 1 | 1 | 1 | 1 | 4 | |||
| Minnesota | 1 | 1 | 1 | 1 | 2 | 2 | 8 | |
| Mississippi | 2 | 2 | 1 | 1 | 1 | 1 | 1 | 9 |
| Missouri | 1 | 3 | 3 | 2 | 1 | 10 | ||
| Montana | 1 | 1 | 1 | 3 | ||||
| Nebraska | 1 | 1 | 1 | 3 | ||||
| Nevada | 1 | 1 | 1 | 1 | 1 | 1 | 6 | |
| New Hampshire | 1 | 1 | 1 | 1 | 4 | |||
| New Jersey | 1 | 1 | 1 | 1 | 1 | 5 | ||
| New Mexico | 1 | 1 | 1 | 1 | 1 | 5 | ||
| New York | 1 | 2 | 1 | 1 | 2 | 7 | ||
| North Carolina | 1 | 1 | 1 | 1 | 4 | |||
| North Dakota | 1 | 1 | 1 | 1 | 4 | |||
| Ohio | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Oklahoma | 1 | 1 | 1 | 3 | ||||
| Oregon | 1 | 1 | 1 | 1 | 4 | |||
| Pennsylvania | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 8 |
| Rhode Island | 1 | 3 | 1 | 1 | 1 | 1 | 8 | |
| South Carolina | 1 | 1 | 1 | 1 | 4 | |||
| South Dakota | 1 | 1 | 1 | 3 | ||||
| Tennessee | 1 | 1 | 1 | 1 | 4 | |||
| Texas | 2 | 1 | 1 | 1 | 1 | 1 | 7 | |
| Utah | 2 | 2 | 3 | 1 | 1 | 1 | 10 | |
| Vermont | 1 | 1 | 1 | 1 | 4 | |||
| Virginia | 1 | 1 | 2 | 2 | 1 | 1 | 8 | |
| Washington | 1 | 1 | 1 | 3 | ||||
| West Virginia | 1 | 1 | 1 | 1 | 4 | |||
| Wisconsin | 1 | 1 | 1 | 1 | 1 | 5 | ||
| Wyoming | 1 | 1 | 1 | 1 | 1 | 5 | ||
Licensure vs. Certification
A license is a state's grant of legal authority to practice within a designated scope of practice (IC&RC, 2018). Certification is similar in that it represents achievement of professional competency for a defined SOP, but it can be overseen by a non-governmental board and is considered weaker than licensure in terms of title protection. "Title protection" is statutory language mandating that only individuals with the credential can use the title; it is a formal, legal acknowledgement of professional qualification. The SOP for a credential can be identical whether it is licensed or certified, but licensure typically establishes a legal title and practice protection whereas certification does not. For example, a 2016 review of SOPs for addiction counselors found that title protection was included in 84% of the licensed addiction counselor (LAC) SOPs but only 19% of the certified alcohol and drug counselor (CADC) SOPs (Page et al., 2017).
As of November 2018, 31 states (61%) offer licensure for SUD counseling and 20 states (39%) offer certification only. The states offering licensure for SUD counseling are shown in Exhibit 5. Many states with licensure also offer certification. The ways in which licensure and certification relate to each other varies by state. For example, in some states, certification is a required step on the path to licensure. In some others, there are separate tracks for licensure and certification, where certification is typically pursued by professionals already licensed in another counseling field who wish to include SUD counseling in their practice--such as professional counselors or clinical social workers.
| EXHIBIT 5. States Offering Licensure for SUD Counseling |
|---|
 |
State and National Credentialing Bodies
There are multiple credentialing bodies for the SUD profession, both at the national level and within individual states. As shown in Exhibit 6, 19 states (37%) have a single board that oversees licensure and/or certification for all SUD credentials (treatment and prevention) within the state; the rest have multiple boards offering credentials at different levels, often with no state-level standards for minimum requirements.
| EXHIBIT 6. Variation across States in the Number of Credentialing Boards |
|---|
 |
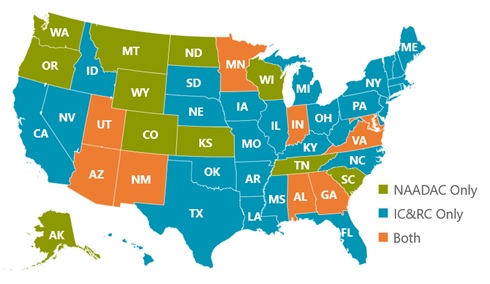
The main national credentialing bodies for the SUD profession are the International Certification and Reciprocity Consortium (IC&RC) and the Association for Addiction Professionals (NAADAC, formerly known as the National Association for Alcoholism and Drug Abuse Counselors). Both IC&RC and NAADAC define competencies required for practice and have standard tests for measuring competencies required at various levels of practice. NAADAC standards are national whereas IC&RC standards vary by state. On the other hand, professionals are required to meet the standards set forth by their state in order to apply for NAADAC certification, which infuses NAADAC certification with a level of variability by state as well. Although the standard credentials of the two national organizations (listed in Exhibit 7) have some overlap, they are by no means identical in scope or in minimum requirements.
| EXHIBIT 7. Credentials Offered by the 2 National Certification Bodies | |
|---|---|
| IC&RC | NAADAC |
|
|
Most SUD credentials available in a state are adapted from those issued by one of the two national organizations, and credentials that require a qualifying examination typically recognize standard tests developed by one of these two national organizations. Exhibit 8 shows variation across states in their affiliation with the two national credentialing bodies. In 30 states (59%), an IC&RC test is used for all credentials that are contingent on passing an examination; in 11 states (22%), only NAADAC tests are used. In the remaining ten states (20%), some credentials are linked to IC&RC and some to NAADAC tests. As mentioned earlier, both national bodies make room for state-level modifications to their credentialing requirements. Thus, a credential affiliated with the same national body in two different states does not necessarily have identical requirements, although reciprocity or endorsement between the two states is more likely than if they were affiliated with different credentialing organizations.
| EXHIBIT 8. Variation across States in Affiliation with National Credentialing Bodies |
|---|
 |
State Variation in Licensing/Credentialing Requirements
We reviewed and extracted data on licensing and certification requirements for over 400 SUD practitioner credentials across the 50 states and D.C. These data are presented in Appendix A, organized by the five categories in SAMHSA's career ladder with additional categories for clinical supervisor, peer recovery specialist, and prevention specialist.
The data show wide variability across states' respective career ladders for SUD professionals and across educational and practice requirements for these credentials. This variation is especially informative as it applies to the highest level in each state's SUD career ladder (the state's "terminal" credential), because this level is the most impacted by reimbursement policies. Exhibit 9 and Exhibit 10 on the following page show the variation across states in the minimum degree and minimum practice hours required to attain the state's terminal SUD counseling credential.
| EXHIBIT 9. Minimum Degree Required to Attain the Highest Level of the SUD Counseling Career Ladder |
|---|
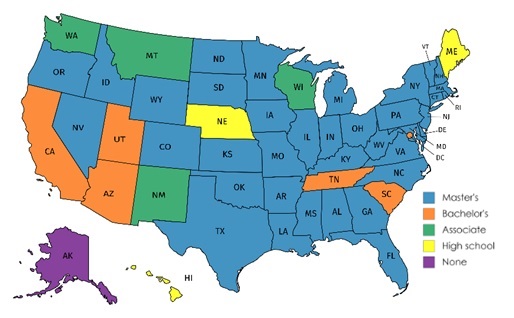 |
Thirty-seven states (73%) require a master's degree to attain the highest SUD counseling credential in the state; six states including D.C. (12%) require a bachelor's degree, four states (8%) require an associate degree, and three states (6%) require only a high school diploma or equivalent. One state, Alaska, currently has no minimum degree requirement but reduces the number of required practice hours for individuals who hold a degree. Similarly, in other states, higher education can often be substituted for some practice requirements.
| EXHIBIT 10. Minimum Practice Hours Required to Attain the Highest Level of the SUD Counseling Career Ladder |
|---|
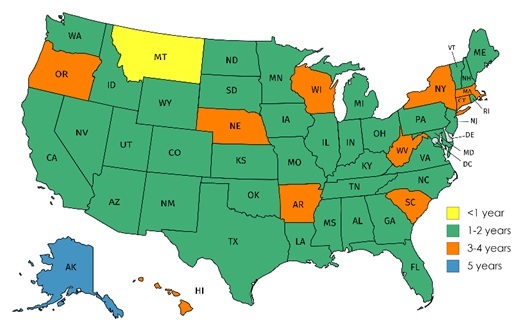 |
The minimum number of practice hours required to attain the highest SUD counseling credential within each state (Exhibit 10) ranged from 1,000 (equivalent to half a year) to 12,000 (6 years). Most states (38 states, 76%) require between 2,000 and 4,000 hours (1-2 years). Comparing the two maps on the following page (Exhibit 9 and Exhibit 10), we find that states with lower minimum degree requirements often require more practice hours. The substitution of practice experience for education hours is often referred to as the "apprentice model," in contrast to the "professional model" for credentialing typical of most other clinical practices. In most states that require less than a master's degree, a portion of the required practice hours can be substituted by a higher degree. This is the case in Alaska, where an individual with no degree is required to have 12,000 practice hours (6 years) to attain the highest credential, but the requirement is reduced to 10,000 hours (5 years) if the applicant has a degree.
Discussion of Credentialing Policies: Barriers and Facilitators
Based on the environmental scan, state review, and case studies, we identified two key credentialing-related barriers to entering the SUD counseling field:
-
Lack of standard credentials and inaccessibility of qualification information.
-
Low and non-standard training and educational requirements for practice.
The rest of this chapter is organized into separate sections discussing each of these two barriers. Examples of efforts and initiatives to address each barrier, as identified through the environmental scan and case studies, are also included in the relevant sections under subsection headings labeled as "facilitators."
Barrier 1: Lack of Standard Credentials and Difficulty Obtaining Information on Practice Requirements
As the preceding discussion demonstrates, the SUD treatment workforce is regulated by a wide range of credentials, credentialing bodies, and minimum requirements. The high degree of variation within and across states in credentialing requirements poses a serious barrier to professionals considering careers in this area. All but 19 states have multiple credentialing boards offering different but in many instances overlapping credentials with differing requirements. This creates a complex environment to navigate for students and early-career professionals interested in an SUD treatment specialty. For example, as part of a 2016 study of assets and gaps in New Hampshire's SUD service continuum, researchers surveyed and interviewed stakeholders throughout the state and found that "complex, unclear, and cumbersome" licensing procedures were the most frequently cited barrier to addressing the state's SUD workforce shortages (NHBDAS, 2016). This view was reiterated by most of our key informants when commenting on nationwide SUD workforce barriers. Other studies focusing on these barriers also reached similar conclusions (Alagoz, Hartje, & Fitsgerald, 2017). In addition to the lack of clarity in and complexity of the credentialing process, variation across states in certification and licensure regulations limits the portability of SUD credentials, constituting a barrier to career mobility; this is an additional disincentive to entering the field.
There was consensus among the experts interviewed for this study that uniform standards for competency requirements and credentialing of SUD counselors is a high national priority; this position is backed up by the published literature (Miller et al., 2010). An Institute of Medicine (IOM) report on the quality of behavioral health care (IOM, 2006) noted the differences between states in credentialing and licensing standards for mental health and SUD providers and recommended measures to reduce, and ideally, eliminate these differences, guided by core competencies included in education programs nationwide. This call for uniform standards was reiterated in a more recent report (IOM, 2011) within the broader context of the nation's public health policies: "national accreditation holds promise as a conduit in aiding governmental public health agencies to demonstrate minimum structural and quality process capabilities" (p. 6). This is especially relevant for SUD counseling, one of the least standardized clinical practices in the nation and a crucial one in addressing the current opioid crisis. Establishing uniform credentials, however, poses many challenges and requires collaboration among multiple stakeholders, such as the federal and state health agencies, credentialing boards, and advocacy groups representing behavioral health and counseling professionals. There are, however, initiatives to establish consensus and/or facilitate collaboration among these stakeholders and to otherwise reduce the barriers associated with licensing and certification.
Facilitator 1.1: Efforts to Establish National Credentials
In 2005, SAMHSA issued a mandate calling for the two main credentialing entities--NAADAC and IC&RC--to work together to find common standards for credentialing the SUD workforce. In accordance with the mandate, the two bodies met on and off for several years to explore alternatives for a joint set of credentials, without concrete results. There was another wave of joint action in 2013 with a "softer" approach to collaboration than all-out merger, involving a joint workgroup to coordinate unified efforts in areas such as workforce advocacy, reimbursement, licensure, and certification. However, we learned from a key informant who was intimately familiar with these efforts that the collaboration effort gradually lost momentum; currently there are no active efforts in place that we are aware of. Resuming this or a similar initiative would be a step toward national standardization, given our finding that almost all the credentials we reviewed nationwide were to some degree aligned with the credentials defined by one of these two national organizations.
Facilitator 1.2: Within-State Consolidation of Certification Boards
As mentioned earlier, 19 states have a single certification board for the SUD profession. This reduces the variability within states in the career pathways available to SUD practitioners and the requirements for obtaining credentials (Morgen, Miller, & Stretch, 2012). As our North Carolina case study revealed, consolidation of multiple boards into a single board with a shared mission, values, and practice standards greatly facilitates SUD practitioners' entry into the state's SUD workforce, both in the case of new graduates and established professionals seeking endorsement for credentials received from other states. The consolidation process, however, is usually challenging; it involves moving against the inertia of established practices and professional identities.
| Case in point |
|---|
| North Carolina Substance Abuse Professional Practice Board (NCSAPPB) is the state's sole certification board for addiction counselors. It is also the sole accreditation entity for education programs that provide training for SUD counselors. A member of the Board interviewed for this study described it as "a quasi-state agency that operates independently." The board director reports directly to the legislature, the governor's office, and the state auditor. Although the Board operates autonomously from the North Carolina Department of Health and Human Services (DHHS), it closely collaborates with that agency. One of the strengths of the Board is the degree of autonomy it allows its staff, resulting in quicker decisions than would be the case in a government agency. NCSAPPB was established in the 1980s through the merger of two boards that separately CADCs. The merger was a contentious process with both groups of professionals initially resisting a single practice definition comprising both. With time, however, it has become the valuable resource incentivizing the SUD workforce that it is today. |
Facilitator 1.3: Centralized Information Dissemination and Technical Assistance to Providers
One of the negative consequences of multiple credentials and credentialing boards is the difficulty that students and early-career professionals face in obtaining detailed and unambiguous information about the SUD counseling career ladder and qualifications for practice in their state. Some states have addressed this barrier by establishing centralized training and technical assistance resources for the SUD workforce to help them navigate this complex information environment.
| Case in point |
|---|
| New York's Office of Alcoholism and Substance Abuse Services (OASAS) partners with the Community Technical Assistance Center (CTAC) and Managed Care Technical Assistance Center (MCTAC) to maintain a "one-stop shop" to meet behavioral health providers' need for practice information. In addition to providing in-person and online training and technical assistance to providers, CTAC/MCTAC maintains a portal with information on credentialing, within-state variation on regulations, establishing and maintaining a practice in the changing environment of system redesign, working with the regional managed care organizations (MCOs), and best clinical practices. An important resource developed through a partnership between OASAS and CTAC is the Level of Care for Alcohol and Drug Treatment Referral (LOCADTR) tool, a web-based application that guides providers in determining the most appropriate levels of care for a given SUD. The state strongly encourages all insurers and providers to use the tool in determining the appropriate level of care for their enrollees and clients, and Medicaid MCOs are required to use it. CTAC/MCTAC also maintains an email helpline to respond to questions from individuals and agencies. Over 5,000 messages arrive daily and receive responses within 24 hours, on average. These services are all offered free of charge and funded by the state. Close communication with OASAS keeps CTAC/MCTAC informed of new and upcoming policy developments and provides OASAS with timely feedback from the field to aid in policy decisions. |
Barrier 2: Low and Non-Standard Educational Requirements
Although this study focuses on the portion of the counseling workforce with SUD-related credentials, it is useful to consider the entire SUD counseling workforce in discussing training requirements. A survey of specialty SUD treatment facilities across the nation found that 42% of the staff working in these facilities were counselors, and 19% were medical staff (e.g., physicians, pharmacists, nurses, mid-level professionals). The rest were evenly divided among administrative staff and patient support staff (e.g., peer support specialists, care managers, patient navigators). Less than a third of the non-administration staff were certified in addiction treatment and certification was inversely correlated with education level: 59% of the counselors with an associate degree were certified in addiction compared with 40% of those with a master's and 34% of those with a doctoral degree (Bouchery, 2017). These figures suggest hat even though the majority of the counseling staff in SUD specialty facilities had at least a master's degree (57%), their advanced education does not necessarily translate into enhanced knowledge of addiction treatment (Bouchery & Dey, 2018). These findings give us a rough snapshot of workforce composition.
The following comment by Kirk Bowden, made at a time when he was NAADAC's president, is very telling with respect to low and uneven education requirements for SUD counseling:
I hold two behavioral health licenses in my state. Both of my licenses grant me the authority to independently practice psychotherapy with clients whose primary diagnosis is an addiction and/or substance use disorder. Neither license required me to complete a single hour of course work in addiction counseling. (Bowden, 2015)
Education requirements for SUD-specific credentials are also lower than those of other counseling professions. For example, a 50-state review of training requirements for counselors found that requirements for mental health counselors were generally structured around formal education whereas addiction counselors' qualifications were typically structured around hours of supervised work (Kerwin, Walker-Smith, & Kirby, 2006). The majority of content experts and state officials interviewed for this study reiterated that unless education and training in addiction treatment is made a requirement for providing SUD services, professionals interested in practicing in this area will prefer to specialize in behavioral health fields with better career advancement prospects, income, and clearer credentialing requirements, such as clinical social work or mental health counseling.
To a large extent, low educational requirements have their roots in the historical development of addiction treatment as an area of knowledge best acquired through lived experience and on-the-job training, in contrast to other clinical specialties where skill acquisition is tightly linked to nationally accredited academic programs. This apprenticeship model of training may be effective in trades with high levels of predictability and a narrowly defined set of tasks, but it might not be as suitable for professions with rapid knowledge development, rigorous research on best practices, and an ever-changing landscape of risk and protective factors. Training of the latter type of professionals typically involves standard curricula that are frequently updated to address new knowledge and practice models, and a standard credentialing system linked to education and professional development in order to bridge the gap between research and practice (Lamb, Greenlick, & McCarty, 1998; Bowden, 2015). There is increasing emphasis on research-based practices in the SUD treatment field that requires the rapid diffusion of new research findings within the profession. Low and varying education requirements in the field will likely delay the adoption of best practices and the discontinuation of discredited treatment models in response to new research findings (Glasner-Edwards & Rawson, 2010).
Our review of minimum education and practice hour requirements (Exhibit 9 and Exhibit 10) revealed that in some states, SUD treatment can be provided without an academic degree or with a minimum of a high school education whereas no state has a minimum practice requirement under 1,000 hours. This suggests that the apprenticeship model still has a hold in parts of the nation, reinforcing the perception that addiction treatment is more a trade than a profession. This is further disincentive to selecting this field as an academic specialty (Morgen et al., 2012). As one of our key informants put it, "Why waste education hours and money if it is not required?" The perception that addiction treatment does not require as much academic training as other behavioral health professions, although no longer an accurate representation of the field, also plays into lower salaries and reimbursement rates for SUD treatment providers; this barrier is discussed in detail later in this report (the section on billing eligibility and reimbursement).
Facilitator 2.1: State Licensure Statutes and Title/Practice Protections
States can address this barrier by regulating the SUD treatment profession: imposing minimum educational requirements for certification and licensure and making it illegal to use an SUD counseling title without certification (title protection) and ultimately, legally requiring clearly defined credentials in order to provide SUD services (practice protection). Legislative actions in this direction are lengthy processes requiring a carefully forged collaboration and consensus among multiple stakeholders in the state, such as state health officials, legislators, professional associations representing the entire range of behavioral health professionals, institutions of higher education, practicing behavioral health providers, individuals with lived experience, and the public at large. Drafting of the legislation is typically preceded by a comprehensive review of the profession, often called a "sunrise review," that specifies clearly demarcated professional boundaries, a career ladder, SOPs, and competency requirements. These factors are all subject to opposition from multiple stakeholders potentially affected by changes to the status quo, underscoring the importance of consensus building in preparation for bringing the statutes to the state's legislature. Two common reasons for such legislation to fail are: (1) opposition from counseling professionals with established practices to newly imposed professional boundaries and competency requirements; and (2) the absence of a corresponding academic career ladder in the state's higher education system.
| Case in point |
|---|
| After several failed attempts, the Indiana Addiction Counselor Licensure bill was signed into law in 2009. The law includes both title and practice protection for addiction counselors. The successful effort had several factors based on lessons learned from previous failures: A professional mediator with legal and legislative experience assisted in establishing consensus among stakeholders previously opposed to the legislation; the SOP was clearly defined, with collaboration from state and national professional associations in counseling professions; an academic career ladder in line with qualifications required for practice was established through collaboration with the state's community college system and a private university; and grandfathering options were included in the legislation to offer "soft" transition options for practicing providers. This legislative effort has come to be referred to as the "Indiana Model," and is cited as a roadmap for other states (Turner-Bull, 2011; Osborn, 2015). |
There are guidelines and roadmaps for establishing clearly defined professional titles and credentials for the SUD profession. SAMHSA's (2011) model career ladder and SOPs, used in the present study to classify the over 300 credentials we found across the nation into categories comparable across states, is one such guideline that states can use to set up and regulate a multi-tiered career ladder. Another example is NAADAC's (2011) model legislative language to regulate the profession.
Facilitator 2.2: Efforts to Establish Standardized Core Competencies and Link SUD Credentials to Academic Programs
Establishing and enforcing standard training requirements for addiction counselor credentials will require standard educational curricula, which, in turn, depends on consensus among multiple national state and local stakeholders around a set of core competencies (Bowden, 2015). An early effort to identify and define core competencies for the profession was funded by the National Institute on Alcohol Abuse and Alcoholism in 1984 (Birch & Davis Associates, 1984). This work laid the foundations for subsequent work in this area. Currently, the most commonly recognized professional standards are those developed by the Center for Substance Abuse Treatment in 2006 (CSAT, 2006); these have been regularly updated since their first publication. Commonly referred to as TAP 21, the CSAT standards facilitate the development and accreditation of degree programs for addiction counseling.
The Council for Accreditation of Counseling and Related Educational Programs (CACREP) that accredits educational programs in counseling has established standards for addiction counseling (CACREP, 2016). While these standards provide guidelines for counseling programs that choose to offer addiction as a specialization, they do not necessarily correspond to the credentialing requirements of the SUD field, which developed separately from the professional counseling field. A move toward state licensing/credentialing requirements that link to degree programs with uniform accreditation standards will, therefore, involve a reconsideration of the entire counseling field (Morgen et al., 2012), requiring collaboration among multiple credentialing and accreditation bodies.
Our study also identified some state-level efforts to link educational and credentialing standards for the profession.
| Case in point |
|---|
| North Carolina's Substance Abuse Professional Practice Board (NCSAPPB), the state's single certification body for addiction counselors, also provides accreditation for educational programs in the state (and a few other states) with curricula that align with their certification requirements. The NCSAPPB website maintains a list of these accredited programs as a resource for SUD professionals, and members of the board pay visits to colleges with accredited programs to provide the students with information about the field. These visits also function as efforts to raise interest in the profession and to encourage new students to specialize in this area. |
One training gap mentioned by multiple expert informants and state officials is the lack of cross-training between addiction and other behavioral health fields. Given the co-occurring nature of these disorders, this training gap has created a competency gap in the behavioral health workforce. Coordination between state certification bodies and institutions of higher education would be needed to develop training resources required for qualification.
| Case in point |
|---|
| A senior member of the California County Behavioral Health Directors Association interviewed for this study observed that any qualified counselor can provide SUD treatment, regardless of their background in addiction-specific education and practice. The SUD-specific credentials that require addiction training and practice hours, while obtainable from either of the two certification boards in the state, are voluntary. Thus, there is no incentive for a licensed counselor to further specialize in SUD treatment that requires additional education and practice hours beyond what they have already completed to obtain their professional counseling license. On the other hand, the state is in the process of transforming its SUD services, moving toward an integrated delivery system with strict quality controls. One of the requirements for an SUD treatment program to receive funding from the state--through the state's Medicaid waiver demonstration--is to have a licensed counselor on staff. In the absence of state-level practice protections banning the provision of SUD counseling without demonstrating core competencies needed for the practice, the presence of a licensed counselor in an SUD treatment facility will fall short of ensuring service quality. Addressing this issue will require the collaboration of multiple professional associations, the state, and institutions of higher education in an effort establish minimum addiction-specific educational standards for the entire SUD workforce and provide the training resources needed to meet those standards. A step in the right direction was taken when a bill was introduced during the 2017-2018 session of the State Assembly (AS-2804) to develop the state's SUD treatment workforce. The bill combined mandates for certifying organizations to formalize a career ladder for addiction professionals and requires that the California State University system, the University of California, and the California Community College system develop goals and plans to provide the necessary training resources. The bill also included appropriations for scholarships, grants, and loan forgiveness programs for completing SUD-related courses. Although the bill failed during the last session, a member of the California Consortium of Addiction Programs and Professionals (CCAPP) indicated that a similar SUD licensure bill is being drafted for submission to the Assembly in January 2019 |
In line with the increasing need for integrated mental health and SUD treatment, there are ongoing efforts to develop cross-training curricula with positive outcomes (Wendler & Murdock, 2006). Programs that incorporate addiction-related material into a broader range of clinical disciplines would help ensure that the entire SUD workforce--Licensed Clinical Social Workers (LCSWs), licensed professional counselors (LPCs), clinical psychologists, and other addiction service providers as well as practitioners with SUD-specific credentials--has the skills and knowledge to implement best practices. In fact, a fully-integrated health care delivery system can best be supported with broader interdisciplinary cross-training, including professions that do not routinely treat SUDs but encounter these symptoms in their practice, such as primary care providers, psychiatrists, pediatricians, and obstetricians (Broyles, Conley, & Harding, 2013; Das & Roberts, 2016).
Facilitator 2.3: Student Loan Repayment Programs
Student loan repayment is an effective strategy for attracting new professionals into a specialty field, and it is widely used across the nation to address workforce shortages. These programs partially or fully repay the student loans of qualified individuals, either as a grant or a one-time payment, in return for a commitment to work for a specified period of time in a specialty field and/or geographic area that is experiencing workforce shortages. In addition to addressing workforce shortages, these programs incentivize professionals to further their education in the specified field. Until recently, these funding opportunities were not available to addiction counselors, perhaps because the field was perceived as depending more on supervised practice than on formal education. Some states now include SUD practitioners among their eligibility criteria for loan repayment programs. For example, Texas passed a law in 2018 to provide loan repayment of up to $10,000 for Licensed Chemical Dependency Counselors (LCDC) willing to work in underserved areas or with underserved populations.
The opioid crisis has also sparked interest in loan forgiveness and other career support programs at the federal level. In March 2018, the U.S. Department of Labor announced up to $21 million out of its National Health Emergency demonstration grant projects to provide career support (including training and education support) for new entrants or incumbent workers in the SUD treatment workforce in areas impacted by opioid use, addiction, and overdose. This was followed by the signing into law of the SUPPORT for Patients and Communities Act in 2019. Section 7071 of the act provides forgiveness for student loans of up to $250,000 in federal funds for SUD treatment professionals. The law requires the recipient to work in a full-time substance use treatment position for up to 6 years in a geographical area with a workforce shortage.
Loan repayment programs, grants, and scholarships are powerful incentives to pursue degrees in SUD treatment. It is important, however, to ensure that such programs do not reinforce existing assumptions about the low educational requirements of the profession. An example of such an assumption is the Texas program, where the repayment scale for LCDCs stops at an associate degree whereas LCSWs, professional counselors, and MFTs are eligible for loan repayments of up to $40,000--and up to $80,000 if they earn a doctorate.
One factor that may limit the effectiveness of loan repayment and scholarship programs in addressing the SUD workforce shortage are the large practice hour requirements that graduates need to fulfill to get certified or licensed in SUD counseling. This period increases the time between graduation and the onset of independent practice by several years in some states. Morgen et al. (2012) point out that in many states, the long practice hour requirements are a carryover from an earlier era when most SUD counselors had no more than a high school diploma. The authors suggest that as the profession transitions from the early "apprenticeship model" to the newly emerging professional model with advanced degree requirements, practice hour requirements need to be recalibrated accordingly. In addition to streamlining SUD-specific credentialing requirements, they point out, such a recalibration will facilitate entry into the profession from individuals already qualified in other counseling professions.
BILLING ELIGIBILITY AND REIMBURSEMENT
The Reimbursement Process
Two types of universal claim forms are used by providers to submit claims to insurance companies for reimbursement of services:
-
The CMS-1500 is used by non-institutional providers, such as individual-level practitioners in private or group practice. It is accepted by most insurance plans, including Medicaid, Medicare Part B, and private insurance.
-
The UB-04 (also known as CMS-1450) is similar to the CMS-1500 but is used by institutional/facility providers, such as hospitals and treatment centers.
Both claim forms are used to record information about a patient's demographics and insurance coverage, diagnoses, services received, and information about the billing provider, including the National Provider Identifier number, a unique 10-digit number issued to providers (individuals and institutions) by CMS.
Insurance plans can vary in their requirements for how these claims forms must be filled out. For example, on the UB-04, some plans require that the rendering practitioner (the individual who performed the service) be identified on the claim, while other plans do not have this requirement. This variability has important implications for our findings: In states where the billing entity for SUD services is restricted to institutions/facilities, the documentation in billing manuals--our source of data on reimbursement--was especially limited with regard to the practitioner types that can render reimbursable services associated with specific billing codes.
In the rest of this section, we present the findings of our review of billing eligibility across Medicaid, Medicare, and commercial insurance. We defined "billing eligibility" as the ability to enroll in the insurance plan as an independent provider type (e.g., a "billing provider") authorized to submit claims and receive reimbursement directly. In states where an SUD counselor is not eligible to enroll as a billing provider, the facility/institution is the entity billing and reimbursed on the counselor's behalf.
Billing Eligibility Under Medicare
Federal Medicare rules define the practitioner types authorized to provide services under Medicare Part B (outpatient services). The list includes physicians, clinical psychologists, clinical social workers, clinical nurse specialists, nurse practitioners, certified nurse anesthetists, physician's assistants, and certified nurse midwives. These are the only practitioner types authorized to provide SUD services.[4] SUD services rendered by professional counselors are not eligible for reimbursement.
Medicare Advantage plans are administered by private companies that contract with Medicare and may offer additional benefits in some cases. Although our initial plan was to review billing eligibility and reimbursement documentation from a sample of Medicare Advantage plans in each state, we found that commercial companies typically do not make this information publicly available. An SUD coverage policy document from UnitedHealthcare,[5] a leading administrator of Medicare Advantage plans, suggests that it adheres to Original Medicare (federal Medicare FFS) policies for coverage of SUD services but leaves room for the possibility of expanded benefits with language deferring to plan-specific documentation over its general Medicare Advantage Policy Guidelines.
As with many commercial insurance plans, there are several types of Medicare Advantage plans, including Health Maintenance Organization, Preferred Provider Organization, and Special Needs Plans (SNPs). SNPs are Medicare Advantage plans that are specifically designed to provide targeted care to special needs individuals, including those in institutional settings, those dually eligible for Medicare and Medicaid, and those with chronic disabling conditions. Dual Eligible SNPs are for dual eligible individuals and offer the opportunity for expanded benefits by combining those available from Medicare and the state's Medicaid plan. Similarly, Fully-Integrated Dual Eligible SNPs were established to promote the full integration and coordination of Medicare and Medicaid benefits for dual eligible beneficiaries and offer a promising avenue for expanded service coverage and reimbursement options.
Billing Eligibility Under Commercial Insurance Plans
Similarly, we were unable to systematically review billing eligibility for SUD counselors across commercial insurance plans because commercial companies do not typically make this information publicly available. However, we identified one company--UnitedHealth/Optum--that makes information on billing eligibility available online.
UnitedHealth Group, of which Optum is a subsidiary, is the nation's largest health insurer. Optum's Provider Express portal[6] lists the practitioner types eligible to enroll in its network as "individually-contracted" clinicians in each of the 50 states and D.C.
Exhibit 11 shows the 13 states in which an SUD counselor is eligible by Optum to be an individually-contracted clinician (i.e., billing provider) as of July 2018. Notably, only licensed SUD counselors are eligible for independent reimbursement in each of the 13 states (listed below the map). Optum's website explains that practitioner eligibility is based on geographic and specialty needs and requires an unrestricted, valid license from the state and authority to practice independently without supervision.
| EXHIBIT 11. SUD Counselors' Eligibility for Independent Billing Status under UnitedHealth/Optum Commercial Plans |
|---|
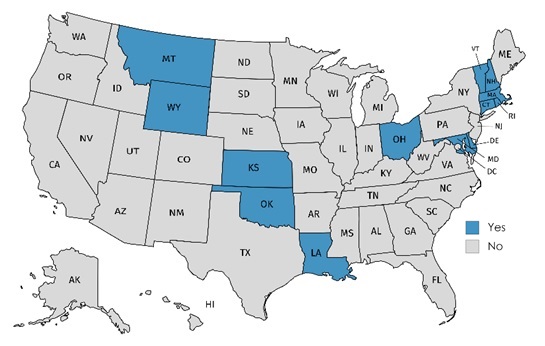 |
| SOURCE: Optum's Provider Express Portal, https://www.providerexpress.com/content/ope-provexpr/us/en/our-network/jon-states.html, accessed July 16, 2018. NOTE: In Nebraska, Licensed Alcohol and Drug Counselor (LADC) and Provisional Licensed Alcohol and Drug Counselor (PLADC) are eligible to be individually-contracted under Optum's Medicaid plans but not its commercial plans; we therefore did not include Nebraska in the map. We found no similar language distinguishing eligibility between Medicaid and commercial plans on Optum's website for other states. ELIGIBLE SUD COUNSELORS BY STATE:
|
Billing Eligibility and Reimbursement Under Medicaid
State Medicaid agencies typically make documentation on billing and reimbursement available to the public online. For this review, we searched the provider and billing manuals available through each state's official Medicaid agency website; they typically reflect FFS Medicaid plans, though in some states they also apply to managed care plans.
Federal rules do not define the practitioner types that are eligible for reimbursement under Medicaid. Instead, this is determined at the state-level and insurance plan-level based on multiple factors, including a practitioner's SOP, the setting in which services are delivered, and the specific contracts developed between insurance plans and service providers.
We identified 11 states in which an SUD counselor is eligible to enroll as an independent billing provider, shown below in Exhibit 12. In 32 states, an SUD counselor is not eligible to enroll as a billing provider. In eight states, we could not determine billing eligibility from the available online documentation.
| EXHIBIT 12. SUD Counselors' Eligibility for Independent Billing Status under Medicaid |
|---|
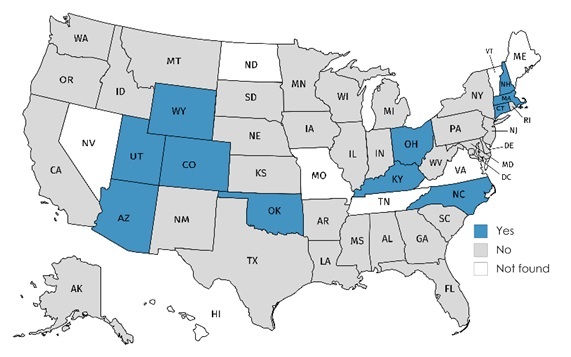 |
| NOTE: In Kansas, a Licensed Clinical Addiction Counselor (LCAC) is not eligible to enroll as an independent billing provider in the FFS plan but is eligible under managed care plans. |
Determining SUD counselors' eligibility for reimbursement for our set of predefined billing codes required a two-phase approach for data extraction and analysis:
-
Determine whether the insurance plan uses each of the eight predefined billing codes and if not, whether a comparable alternate code used.
-
Determine whether an SUD counselor is eligible to bill for or render the service
Exhibit 13 shows the number of states using the exact code, the number using a comparable alternate code, and the number for which the exact code or an alternate was not found. These data are presented at the state level in Appendix B.
| EXHIBIT 13. Number of States using Exact of Alternate Billing Codes among the 8 Billing Codes Examined in this Study (Medicaid) |
|---|
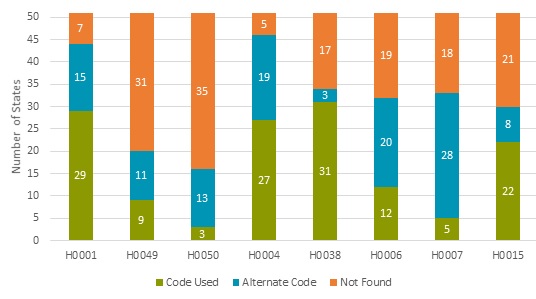 |
BILLING CODE DESCRIPTIONS:
|
In most states, the billing documentation available did not specify which individual practitioner types can be reimbursed for particular service codes; however, when that level of detail was available, SUD counselors were typically eligible to be reimbursed for the codes reviewed in this study
It is notable that H0049 and H0050--two codes used for billing for Screening, Brief Intervention, and Referral to Treatment (SBIRT) services--are not more widely used across state Medicaid plans. SBIRT is an evidence-based practice that is effective in early identification of SUD and is encouraged by SAMHSA. SAMHSA published guidance on coding for reimbursement for SBIRT services (SAMHSA, 2017), identifying H0049 and H0050 for billing under Medicaid and comparable codes used by commercial insurance (99408 and 99409) and Medicare (G0396 and G0397). We identified only nine states using H0049 and three states using H0050. A possible reason for these low numbers is that we reviewed billing documentation for behavioral health and not primary care settings where SBIRT services are often delivered. Another recent study (Hinde, Bray, Kaiser & Mallonee, 2017) also noted that activation of HCPCS or CPT codes for SBIRT is limited across states and examined possible reasons, including institutional constraints, federal block grant and SBIRT grant funding, priority given to SUD treatment in the state, and states' economic and political climates. The authors found that per-capita federal block grant (but not SBIRT grant) funding was associated with a decreased likelihood of SBIRT code activation, while the existence of state parity laws increased the likelihood of code activation.
Alignment of Licensure and Independent Billing Eligibility
One of the important findings of this review is that insurance reimbursement at the individual practitioner level is correlated with licensure. The Medicaid and commercial plans reviewed for this study restrict reimbursement eligibility to licensed providers; in that sense, practitioners in states that do not have licensure for SUD counselors are at a disadvantage. Exhibit 14 aligns licensure availability and Medicaid and Optum eligibility for independent billing for each state. These results show that unavailability of licensure is a serious barrier to independent billing status. On the other hand, while licensure is a facilitator, it by no means guarantees independent billing status.
| EXHIBIT 14. Licensure Availability and Eligibility for Independent Billing Status for SUD Counselors under Medicaid and Optum, by State | |||
|---|---|---|---|
| State | Licensure Available | Medicaid Eligible | Optum (comm.) Eligible |
| Alabama | No | No | No |
| Alaska | No | No | No |
| Arizona | Yes | Yes | No |
| Arkansas | Yes | No | No |
| California | No | No | No |
| Colorado | Yes | Yes | No |
| Connecticut | Yes | Yes | Yes |
| Delaware | Yes | No | Yes |
| District of Columbia | No | No | No |
| Florida | No | No | No |
| Georgia | No | No | No |
| Hawaii | No | Not stated | No |
| Idaho | No | No | No |
| Illinois | No | No | No |
| Indiana | Yes | No | No |
| Iowa | No | No | No |
| Kansas | Yes | No | Yes |
| Kentucky | Yes | Yes | No |
| Louisiana | Yes | No | Yes |
| Maine | Yes | Not stated | No |
| Maryland | Yes | No | Yes |
| Massachusetts | Yes | Yes | Yes |
| Michigan | No | No | No |
| Minnesota | Yes | No | No |
| Mississippi | No | No | No |
| Missouri | No | Not stated | No |
| Montana | Yes | No | Yes |
| Nebraska | Yes | No | No |
| Nevada | Yes | Not stated | No |
| New Hampshire | Yes | Yes | Yes |
| New Jersey | Yes | No | No |
| New Mexico | Yes | No | No |
| New York | No | No | No |
| North Carolina | Yes | Yes | No |
| North Dakota | Yes | Not stated | No |
| Ohio | Yes | Yes | Yes |
| Oklahoma | Yes | Yes | Yes |
| Oregon | No | No | No |
| Pennsylvania | No | No | No |
| Rhode Island | Yes | No | Yes |
| South Carolina | No | No | No |
| South Dakota | Yes | No | No |
| Tennessee | Yes | Not stated | No |
| Texas | Yes | No | No |
| Utah | Yes | Yes | No |
| Vermont | Yes | Not stated | Yes |
| Virginia | Yes | Not stated | No |
| Washington | No | No | No |
| West Virginia | No | No | No |
| Wisconsin | No | No | No |
| Wyoming | Yes | Yes | Yes |
Discussion of Billing Eligibility and Reimbursement: Barriers and Facilitators
Based on the environmental scan, state review, and case studies, we identified the following factors as key barriers to billing eligibility and direct reimbursement of SUD counselors:
-
Lack of insurance coverage for SUD services and low reimbursement rates.
-
Uneven availability of state-regulated licensure across the nation.
-
Legislative, administrative, and financial burdens of joining insurance networks and filing claims.
The rest of this chapter is organized into separate sections discussing each of these three factors. Examples of efforts and initiatives to address the barriers, as identified through the environmental scan and case studies, are also included in the relevant sections under subsections labeled as "facilitators."
Barrier 1: Lack of Insurance Coverage for SUD Services and Low Reimbursement Rates
Low funding levels for SUD services is cited as one of the largest disincentives to enter the SUD workforce. While recent health reform initiatives have greatly expanded insurance coverage for SUD services, coverage is by no means universal. A 2013 survey of state Medicaid programs collected data on coverage of seven SUD services across the four levels of care identified by ASAM and found that 26 states and D.C. covered at least one service in each of the four levels of care and only 13 states and D.C. covered all seven services. (Grogan et al., 2016). Similarly, a 2015 study by MACPAC reviewed SUD services covered under Medicaid state plans based on provider and billing manuals and fee schedules, similar to the sources used in the present study, and found that only 24 state plans covered psychotherapy for SUD, 25 covered case management/care coordination, 22 covered intensive outpatient care, and 14 covered peer support services (MACPAC, 2016).
There is little in the published literature on commercial insurance coverage of SUD services, though an expert interviewed for this study indicated that it has historically been better than Medicaid. This, however, is not consistently the case. For example, a 2016 study of reimbursement rates for SUD services from claims data in New Hampshire found that commercial reimbursement rates were substantially lower compared to Medicare and similar to the state's Medicaid rates (Compass Health Analytics Inc., 2016). Although plans that participate in the state and federal marketplaces are required to cover ten essential benefits of which SUD services is one, coverage for individual services is highly dependent on the plan as well as an individual's circumstances (e.g., prior experience in treatment programs, type of substance use, co-occurring mental health diagnoses). Even when a service is a covered benefit under a state's Medicaid plan, MCOs might not reimburse it under the provider's participation agreement (Falcone & Berke, 2018).
Reimbursement rates for SUD services are notoriously low throughout the nation, especially compared to other counseling professions. As one example of disparities in rates, our Texas case study found that in the state's Medicaid plan, 15 minutes of alcohol and/or drug counseling (H0004) is reimbursed at $14 compared to $44 for 30 minutes of psychotherapy. Low rates are an important disincentive to providers to join insurance networks. Data from the 2017 N-SSATS show that 30% of provider facilities do not accept private insurance payments, 36% do not accept Medicaid, and 65% do not accept Medicare (SAMHSA, 2018a).
Facilitator 1.1: Medicaid Waivers to Redesign Service Delivery and Reimbursement Systems
There are multiple initiatives across the nation to expand coverage of SUD services and to increase reimbursement rates. All of the experts interviewed for the study mentioned at least one of the following as an important vehicle for increasing the range of covered services and populations:
-
State plan amendments (SPAs) under Section 1915(i) of the Social Security Act.
-
Home and community-based services covered through Section 1915(c) waivers.
-
Section 1115 Medicaid demonstration waivers that allow broad changes in eligibility, benefits, cost sharing, and provider payment models.
These vehicles allow states to cover services that are not typically covered by Medicaid plans to specific populations defined by their age, severity of condition, and in some cases, geographical location (Musumeci, Rudowitz, Hinton, Antonisse, & Hall, 2018). We found no studies that explicitly assess the impact of these initiatives on providers' ability or willingness to join insurance networks. However, a national study that investigated the factors that drive providers' decisions to join networks (Andrews, 2014) provides valuable clues about how states' Medicaid coverage may motivate providers to accept public insurance plans. Using provider-level data from NSSATS in conjunction with a full review of state Medicaid programs, the study investigated how the state's Medicaid coverage influenced Medicaid acceptance. The study found that the number of SUD services covered and the number of optional eligibility expansions implemented by the state plan were the strongest state-level predictors of Medicaid acceptance by providers in the state.
| Case in point |
|---|
| In 2014, New York received CMS approval for a Medicaid 1115 waiver demonstration to redesign its health care delivery system. This initiative had a far-reaching impact on the SUD workforce. Whereas the state's Medicaid system had previously carved out mental health and SUD treatment services, full integration of health care within a managed care environment calls for a single care management organization to take on the responsibility of managing its members' complete needs--their physical and behavioral health service needs, both acute and long-term. The action plan further recommended that these reforms include safeguards to prevent "the 'medical model' of care from displacing community-based behavioral health service delivery." Additionally, New York is one of the initial eight demonstration states for the Certified Community Behavioral Health Clinics (CCBHCs) program that seeks to improve access to community mental health and addiction treatment services. As part of these efforts, New York uses federal matching funds to provide training and technical assistance to behavioral health providers in adapting their practices to the new policy environment, provide sign-on bonuses to attract new SUD workers, scholarships, and student loan forgiveness for training new professionals. For example, the newly-created Credentialed Alcoholism and Substance Abuse Counselor (CASAC) credential was supported by a scholarship program for peer workers, adding 750 certified peer workers to the workforce within 2 years. |
Facilitator 1.2: Medicaid Health Homes and Bundled Services
One specific type of SPA option relevant for the present project is a Medicaid health home, mentioned by several key informants as a reimbursement facilitator. Under this option, states may design health homes to provide comprehensive care coordination for Medicaid beneficiaries with chronic conditions, integrating physical and behavioral health services offered to beneficiaries. Health homes bring together a wide range of providers under one virtual roof, organized around an intaking entity; they also typically utilize alternative payment models such as partial or full capitation or bundled rates. Bundling together the full range of services (including recovery supports and wraparound services) under a single rate allows providers to be reimbursed for their services regardless of their insurance network membership. In many states, the establishment of health homes seems to have facilitated insurance coverage for services and service providers not previously covered by insurance plans.
As of the end of 2017, four states (Maine, Maryland, Rhode Island, Vermont) had Medicaid health homes specifically for SUD treatment. For example, Maine's SUD health homes bring together a clinical team lead, Medication Assisted Treatment prescriber, nurse care manager, opioid dependency clinical counselor, and peer recovery coach to coordinate their services (CMS, 2018). A SAMHSA report published in 2010 had indicated that addiction recovery support services (RSS) in Maine were financed solely through state appropriations with no federal funds, suggesting that the health home model adopted by the state in 2017 has expanded reimbursement options for recovery coaches by including Medicaid reimbursement. Similarly, the flexibility offered by the Vermont health home model allowed the state to expand Medicaid coverage to services (e.g., pediatric psychiatric consultation) and their providers not previously reimbursable through Medicaid (Johnson & Miller, 2016).
Alternatives to the FFS payment model, such as those adopted by health homes, help incentivize providers by opening up flexibility in the services and providers reimbursable through insurance plans and by reducing the administrative burden on individual providers. Models such as case-based or episode-based rates, capitated payment models, and bundled payments allow a single billing process for a predefined group of services and/or a team of providers (Mauri et al., 2017). In recognition of the growing interest in collaborative, team-based services for behavioral health, CMS recently introduced three new Medicare billing codes (G0502, G0503, and G0504) for a group of bundled services provided according to a coordinated treatment plan by a primary care team under the Collaborative Care Model (CMS, 2016).
Of particular interest for the present study is the Patient-Centered Opioid Addiction Treatment bundle of services proposed by ASAM for inclusion in Section 1115(a) waivers, to cover an array of integrated outpatient services including medication-assisted treatment (MAT). As mentioned earlier and also brought up by several key informants, MAT is an evidence-based SUD treatment model that is currently underused; even practitioners with prescription authorization shy away from taking on patients with MAT needs because they either do not have the infrastructure to provide the entire slate of services these patients need or because of the complex billing structure for MAT. The additional recordkeeping and reporting requirements imposed by the Drug Enforcement Administration (DEA), and the possibility of on-site inspections by DEA agents, often pose prohibitive administrative burdens. The proposed bundle offers a service delivery and payment model that "transforms inadequate and siloed provider reimbursement into a bundled payment structure that rewards highly qualified providers who deliver evidence-based treatment" (ASAM, 2017).
In line with the literature on the role of alternative payment models in facilitating provider reimbursement, a key informant intimately familiar with both public and private insurance plans indicated that provider categories that cannot bill to Medicaid as individual providers (e.g., peer recovery coaches in some states) are, in some cases, being reimbursed as part of an episode-based bundled payment model.
Facilitator 1.3: Expansion of Telepractice
Telepractice widens a provider's client base without adding commuting burden; the ability to bill insurance for these services is an additional facilitator for providers. A third related advantage of having telepractice as a reimbursable service option is that it facilitates the fulfilment of loan repayment requirements, which often involve practice in underserved areas and among underserved populations.
Several states have taken measures to facilitate telepractice in behavioral health. In New York, insurance plans are prohibited from distinguishing between in-person care and telepractice in reimbursing covered services. Our informants indicated that this has significantly helped expand SUD services to remote areas that are experiencing provider shortages. In North Carolina, CCSs are authorized to provide supervision through telepractice, enhancing access to supervision services for professionals seeking an SUD credential with supervised practice prerequisites. Finally, Texas's Delivery System Reform Incentive Payment (DSRIP) Program, funded through a Medicaid waiver and designed to incentivize innovative health service delivery mechanisms, currently funds 49 projects to expand behavioral health telehealth services. These projects will increase the need for behavioral health practitioners, including SUD counselors, thus opening new employment opportunities for this workforce
Barrier 2: Uneven Availability of Licensure
The results of our state review indicate that a practitioner's eligibility to receive insurance reimbursement (public or private) is limited in the absence of state licensure regulations. All of the states in which an SUD counselor is eligible for independent reimbursement under Medicaid or Optum also have licensure for SUD counselors (Exhibit 14). On the other hand, licensure for SUD counseling is unavailable in 20 (39%) states (Exhibit 5). In states that restrict billing eligibility to SUD facilities, absence of licensure also poses a barrier for the SUD profession because a facility's eligibility to join insurance networks is increasingly contingent on having a licensed professional on staff. In states without statutory title and practice protections for SUD counselors, this requirement is typically met by hiring licensed behavioral health counselors (e.g., licensed marriage and family counselors or mental health service providers) who may not have sufficient addiction training.
| Case in point |
|---|
| California currently has no licensure requirements for SUD professionals, an issue underscored by our key informants in the state as a serious barrier to reimbursement as well as to career advancement. Past legislative efforts to address this barrier failed due to opposition from several stakeholder groups. The CCAPP is currently conducting a full review of SOPs and competency requirements (a "sunrise review") and our key informants expressed optimism that the new version of the legislation based on this review will have better luck in the upcoming legislative session. In the meantime, California is implementing a Section 1115 waiver demonstration to redesign its behavioral health system to provide Medicaid coverage for all SUD levels of care, to transition to a managed care payment model with reporting requirements for quality measures, and to integrate behavioral and physical health care. The goal is to enhance the accessibility and quality of SUD services and the expectation is that, in the long run, career advancement and reimbursement opportunities for SUD professionals will improve. In the short term, however, the existing barriers due to lack of licensure are leading to new barriers. In counties that join the demonstration, availability of a licensed professional on staff is a billing eligibility requirement for SUD programs but SUD counselors cannot meet this requirement unless they are licensed in another counseling field such as clinical social work or marriage and family therapy. |
The California case demonstrates the urgent need for consistent licensure laws, not only to increase SUD practitioners' ability join insurance networks but also to ensure that system redesign efforts do not have unintended negative consequences during the transition and early stages. Legislative efforts in this direction were discussed in more detail in the previous section.
Barrier 3: Legislative, Administrative, and Financial Burdens
The administrative and financial burden associated with joining insurance networks is another barrier to providers' joining insurance networks. Filing insurance claims has historically been labor-intensive with often unclear requirements. In many cases, providers need to join multiple networks with differing filing and reimbursement structures to meet the needs of their client base, increasing the amount of paperwork required for reimbursement. Especially in the current environment of system transformations and rapidly changing policies, providers find it burdensome to adapt their practices in line with policy transformations. Small practices find these system changes more burdensome than do larger provider agencies with better administrative infrastructures.
In addition to this administrative burden, the process of expanding coverage by adding new provider types and billing codes eligible for reimbursement by state Medicaid systems can be expensive and cumbersome.
| Case in point |
|---|
| Until recently, peer RSS in Texas were funded through grants. A 2015 house bill to expand Medicaid coverage to peer services failed to pass. Two years later, the state legislature passed a revised version of the bill directing the Texas Health and Human Services Commission (HHSC) to create a Medicaid benefit for peer support services. In line with this mandate, HHSC assembled a stakeholder workgroup--composed of peer specialists, peer supervisors, and trainers of peer specialists--to provide input on Medicaid policies regulating the training, certification, scope of services, and supervision of Certified Peer Specialists and Recovery Coaches. The draft rules were presented for public comment during the summer of 2018. The 2018-19 General Appropriations Act provides funds for training and technical assistance to peer specialists and appropriated $834,600 (all funds) in FY18 and $2,375,100 (all funds) in FY19 to provide peer support services in the Medicaid program. However, the proposal to allow certified peer specialists to directly bill Medicaid for their services failed due to opposition from a variety of stakeholder groups. A senior member of the HHSC interviewed for this study mentioned this multi-year legislative effort as an example of the cost-intensity and resource-intensity of efforts to add a new provider category to a state's Medicaid program. |
Facilitator 3.1: Burden-Sharing through Pooling Resources
Examples of successful state efforts to incentivize providers to join insurance networks include efforts to streamline the claims process and the provision of resources to support providers in adapting to the changing policy environment.
| Case in point |
|---|
| Transition to a value-based payment model requires important changes to providers' existing business models, involving administrative and infrastructural adaptations that often require a substantial investment. The transition can, thus, pose important challenges to providers, and especially to small providers with limited resources. In January 2018, New York began making Medicaid funds available to support providers through this transition. Multiple mental health and addiction service providers can join together to form Behavioral Health Collaboratives (BHCs) to qualify for these funds. All members of the collaborative then share in the administrative functions created with these funds, instead of each provider separately investing in the new functions needed for practice transformation. So far, 19 such collaboratives have been awarded. For example, one such network, the South Central Behavioral Health Care Collaborative, was awarded $1.6 million over 3 years to bring together 33 providers in their region to "address identified gaps in services by seeking additional partners who offer those services and working with current partners to expand available services." |
Facilitator 3.2: State Supports for Providers in Contracting with MCOs
As mentioned previously, the transition to a managed care model brings with it a number of new challenges for providers. Although states impose certain parameters for MCOs, such as network adequacy standards and minimum quality reporting requirements, MCOs have some flexibility in selecting their network members and in setting the terms of provider contracts. For providers who need to join multiple MCO networks to establish a client base or to retain their existing clients, this often involves meeting multiple sets of criteria and administrative practices. One approach to addressing this barrier is for states to impose some regulations protective of providers on Medicaid MCOs, such as model contracting language (Falcone & Berke, 2018). This removes some of the barriers to joining insurance networks, especially because Medicaid is usually the largest payer in the state.
| Case in point |
|---|
In transitioning its Medicaid program from FFS to managed care, New York established some regulations on Medicaid MCOs to ease the challenges that providers encounter in joining networks. These include the following:
|
CHALLENGES AND LIMITATIONS
This study faced several challenges and limitations, notably the lack of publicly available documentation on billing eligibility and reimbursement from insurance plans. Where documentation was available, it often lacked sufficient detail to determine SUD practitioners' ability to be reimbursed for specific service codes.
In addition, variation across states and insurance plans in the billing codes used for SUD services presented a challenge to standardizing data across states. We attempted to identify comparable alternate billing codes when one of the study's eight predefined codes was not in use; however, some of the alternate codes we selected may not be entirely comparable. Additionally, insurance policies are frequently in flux, and while we relied on documentation linked directly from state's Medicaid websites, some of the information may be outdated as policies are updated.
Our review of Medicaid billing eligibility and reimbursement focused on Medicaid FFS plans for which documentation was more accessible than for managed care plans. The findings therefore do not reflect all Medicaid plans in a given state
In our review of states' licensing and certification requirements, standardizing data across states was challenging given the variability in the level of detail available from source documents. SAMHSA's model career ladder provided a useful framework with which to compare states' SUD credentials at varying levels; however, it also presented a challenge because classifying credentials into this framework required subjective determinations; moreover, credentials overseen by numerous boards were often overlapping, making their placement in the career ladder difficult. Our classifications were made primarily based on minimum degree requirements and the position of the credential within each state's own SUD career ladder. Our analysis did not distinguish between certification that is voluntary (only intended to acknowledge a specific level of knowledge/experience) and required (prerequisite for service provision) certification. We separated clinical supervisor credentials (e.g., CCS) into their own category because the requirements typically overlay the requirements for an underlying credential (e.g., LAC); however, in separating these credentials we might have inadvertently removed some standalone credentials that should have remained in one of SAMHSA's five categories.
Finally, the data compiled through the state-by-state review of credentialing and reimbursement policies were not verified by state officials. However, drafts of the case study summaries (Appendix G) were reviewed by our informants in each state, and their feedback was incorporated into the final versions.
CONCLUSIONS AND IMPLICATIONS
This study revealed that the SUD counseling profession faces multiple interconnected challenges associated with complex training, credentialing, and payment structures. Exhibit 15 summarizes some of the key factors that pose barriers and/or disincentives to entering this profession, developing one's career to its full potential, joining insurance networks, and receiving reimbursement.
| EXHIBIT 15. Interconnected Barriers Experienced by the SUD Counseling Workforce |
|---|
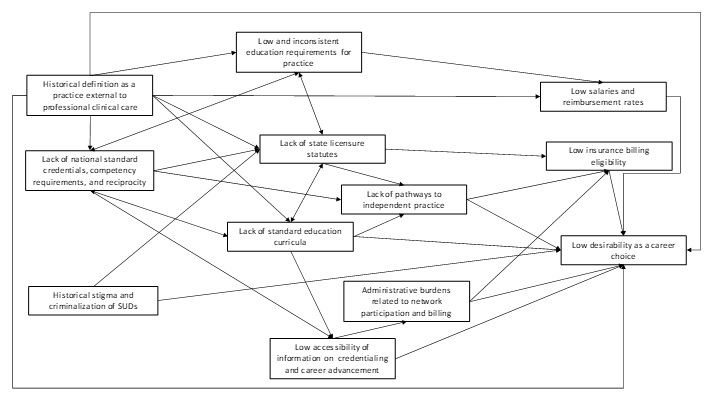 |
Compared to other counseling professions like clinical social work and marriage/family therapy, addiction counseling is a less desirable specialty due to the difficulty in obtaining a credential or a license, low portability of credentials across state lines, relatively low earning potential, and multiple barriers to establishing an independent practice, joining insurance networks, and filing claims. There are multiple credentialing bodies at the national and state levels with varying education and skill requirements, resulting in a proliferation of distinct but overlapping credentials across the nation. There is no standard, clearly defined career ladder specific to SUD counseling, and the requirements for advancing within the profession are often vague and inconsistent. The multiple education and practice requirements across the nation go hand-in-hand with lack of degree programs in this specialty and the absence of standard curricula on addiction treatment in colleges and universities.
Insurance coverage for SUD services and reimbursement rates also vary from state to state, and reimbursement rates are typically lower than those for comparable behavioral health services. In many states, SUD counselors are not eligible to join insurance networks as independent providers; they can only receive payment for their services by joining the staff of an accredited facility eligible for insurance reimbursement. Increasingly, insurance plans and MCOs require a state license for joining their networks as independent providers. This poses a barrier in the 19 states and D.C. that do not have licensure for SUD counselors. State licensure facilitates, though by no means guarantees, independent billing eligibility: Of the 25 states with licensure for addiction counselors and available information on network eligibility, 14 (56%) do not allow SUD counselors to independently bill Medicaid and 58% do not have a commercial Optum plan that accepts licensed SUD counselors as independent network enrollees. In light of the opioid crisis currently facing the nation, and the associated need for an adequate SUD counseling workforce, these factors have serious consequences.
Our study identified multiple initiatives that address these barriers. For example, Medicaid expansion and innovative Medicaid waiver demonstrations implemented by several states have increased the coverage of SUD treatment, in some cases including the full ASAM continuum of care. The health insurance reforms went a long way toward redefining SUD treatment as essential clinical care by requiring insurance plans to provide basic coverage for individuals with addiction-related conditions. State parity rules and health care integration efforts have also helped redefine the SUD counseling profession as a clinical practice comparable to others and helped address the stigma attached to individuals with SUDs and their care providers. Multiple states have or are in the process of establishing licensure for SUD counselors, thus facilitating independent practice and encouraging insurance network participation. Scholarships and student loan repayment programs have helped increase the desirability of the field, incentivizing students to specialize in SUD counseling.
The urgent need to establish uniform credentials, SOPs, and associated education programs has been addressed by efforts to establish consensus between the two main national credentialing organizations, NAADAC and IC&RC, and through consolidation and shared decisions on competency requirements among multiple certification boards within states. Some states, such as North Carolina and Indiana, have made efforts to establish degree programs linked to their certification and licensing requirements.
Despite these and other innovative initiatives to address the barriers, SUD workforce shortages and the resulting unmet need for treatment persist. According to the 2016 NSDUH, an estimated 17.7 million adults in the United States needed but did not receive specialty substance use treatment (Park-Lee et al., 2017). Based on the results of this survey, a study conducted by the Health Resources and Services Administration (HRSA) estimated a shortage of 17,570 full-time equivalents (FTEs) in the national addiction counselor workforce, with 38 states experiencing shortages at various levels (HRSA, 2018). The study projects that by 2030, the shortage could reach up to 35,000 FTEs with 45 states suffering from shortages. The interconnectedness of the factors underlying this unmet demand may be one of the barriers. For example, some states that are implementing Medicaid waivers to increase coverage and reimbursement rates for addiction treatment have witnessed unintended negative impacts on the workforce in the short term. By changing the policy environment, for example, they imposed new administrative and infrastructural burdens on providers as well as new competency requirements for joining insurance networks which the existing workforce found difficult to meet.
Promising measures for addressing the workforce shortage include:
-
The adoption of common standards for addiction education requirements as a condition of providing SUD counseling.
-
Increased availability of degree programs offering standard curricula in SUD treatment.
-
Financial incentives including increased reimbursement, scholarships, and student loan repayment programs that incentivize students to pursue advanced degrees in SUD treatment.
An additional approach to enhancing the qualified workforce is to offer addiction as a specialization track in degree programs such as social work, clinical psychology, and professional counseling, with standards that address the required core competencies of addiction counseling. This will incentivize students in these fields to start gaining education credits and practice hours in addiction services as part of their degree requirements, reducing the additional burden of qualifying for an SUD-specific credential. Some authors have pointed out that this pathway from other behavioral health fields into the SUD profession would be further facilitated if the practice hour requirements of SUD-specific credentials were recalibrated to take into consideration the advanced degrees of new graduates (Morgen et al., 2012). These measures would require collaboration and consensus among the credentialing bodies of multiple behavioral health professions as well as state behavioral health agencies. An important consideration in initiatives to revise states' current credentialing and licensing policies is supporting the existing workforce through the transition by incorporating grandfathering provisions into new policies.
So far, the most successful initiatives have been those that adopted a multi-faceted approach to addressing the barriers encountered by the SUD workforce, carefully developing a collaborative approach to secure the participation of and consensus among multiple stakeholders. In New York, for example, the first step in the Medicaid redesign effort was the establishment of a multi-stakeholder workgroup that identified service assets and gaps, studied other states' experiences with similar initiatives, and produced an action plan that included remedies for possible unintended consequences, such as providers' challenges in transforming their practices in line with the new regulatory environment. Likewise, Indiana's legislative efforts to establish licensure for an addiction counselor career ladder included collaboration among state health agencies, institutions of higher education, and representatives of the SUD profession. The resulting policies incorporated grandfathering clauses to ease the transition for the existing workforce and the establishment of degree programs to help the new workforce meet licensing and certification requirements. This type of systemic reform efforts with participation from multiple state and national stakeholders holds promise for the future of the workforce. It is further cause for optimism that the Office of National Drug Control Policy (ONDCP) has identified "increasing the size of the addiction service workforce, and treatment and recovery infrastructure" as one of the goals in its latest strategic plan (ONDCP, 2019).
REFERENCES
Alagoz, E., Hartje, J., & Fitsgerald, M. (2017). Strategies for Recruitment, Retention, and Development of the Substance Use Disorder Treatment and Recovery Services Workforce: A National Qualitative Report. Kansas City, MO: Addiction Technology Transfer Center National Office. Retrieved from https://attcnetwork.org/centers/network-coordinating-office/national-workforce-report-national-qualitative-report-september.
Andrews, C.M. (2014). The relationship of state Medicaid coverage to Medicaid acceptance among substance abuse providers in the United States. Journal of Behavioral Health Services & Research, 41(4), 460-472. doi: 10.1007/s11414-013-9387-2.
Andrews, C., Abraham, A., Grogan, C.M., Pollack, H.A., Bersamira, C., Humphreys, K., & Friedmann, P. (2015). Despite resources from the ACA, most states do little to help addiction treatment programs implement health care reform. Health Affairs, 34(5), 828-835. doi: 10.1377/hlthaff.2014.1330.
Andrews, C.M., Grogan, C.M., Westlake, M.A., Abraham, A.J., Pollack, H.A., D'Aunno, T.A., & Friedmann, P.D. (2018). Do benefits restrictions limit Medicaid acceptance in addiction treatment? Results from a national study. Journal of Substance Abuse Treatment, 87, 50-55. doi: org/10.1016/j.jsat.2018.01.010.
American Society of Addiction Medicine (ASAM). (2017). Response to a Request for Information issued by the Centers for Medicare and Medicaid Innovation. Retrieved from https://www.asam.org/advocacy/news/asam-advocacy-blog/2017/11/20/asam-comments-on-the-new-direction-for-the-centers-for-medicare-and-medicaid-innovation.
Association for Addiction Professionals (NAADAC). (2011). Licensing of Addiction Professionals in States. Alexandria, VA: National Association for Alcoholism and Drug Abuse Counselors. Retrieved from https://www.naadac.org/assets/2416/naadac_model_state_licensure_bill.pdf.
Beck, A.J., Manderscheid, R.W., & Buerhaus, P. (2018). The future of the behavioral health workforce: Optimism and opportunity. American Journal of Preventive Medicine, 54(6S3), S187-S189. Retrieved from https://www.sciencedirect.com/science/article/pii/S0749379718316271#s0005.
Birch & Davis Associates. (1984). Development of Model Professional Standards for Counselor Credentialing. Rockville, MD: U.S. Department of Health and Human Services, National Institute on Alcohol Abuse and Alcoholism. Retrieved from https://dp.la/item/c11d9f00465948895d7ed6cfe354d045.
Boozang, P., Bachrach, D., & Detty, A. (2014). Coverage and Delivery of Adult Substance Abuse Services in Medicaid Managed Care. Technical Assistance Brief #2. Centers for Medicare & Medicaid Services, Medicaid Managed Care Information Resource Center. Retrieved from https://www.medicaid.gov/medicaid/benefits/downloads/cms-adult-substance-abuse-services-coverage.pdf.
Bouchery, E. (2017). Examining Substance Use Disorder Treatment Demand and Provider Capacity in a Changing Health Care System: Final Report. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. Retrieved from https://aspe.hhs.gov/report/examining-substance-use-disorder-treatment-demand-and-provider-capacity-changing-health-care-system-final-report.
Bouchery, E., & Dey, J. (2018). Substance Use Disorder Workforce. Issue Brief. U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and valuation. Retrieved from https://aspe.hhs.gov/basic-report/substance-use-disorder-workforce-issue-brief.
Bowden, K. (2015). My Big Concern for the Addiction Counseling Profession. Advances in Addiction and Recovery, 3(1), 4. Retrieved from https://www.naadac.org/AAR-archive/.
Broyles, L.M., Conley, J.W., & Harding Jr., J.D. (2013). A scoping review of interdisciplinary collaboration in addiction education and training. Journal of Addictions Nursing, 24(1), 29-36. doi: 10.1097/JAN.0b013e318282751e.
Buck, J.A. (2011). The looming expansion and transformation of public substance abuse treatment under the Affordable Care Act. Health Affairs, 30(8), 1402-1410. Retrieved from doi: 10.1377/hlthaff.2011.0480.
Center for Substance Abuse Treatment (CSAT). (2006). Addiction Counseling Competencies: The Knowledge, Skills, and Attitudes of Professional Practice. Technical Assistance Publication (TAP) Series 21. HHS Publication No. (SMA) 15-4171. Rockville, MD: Substance Abuse and Mental Health Services Administration. Retrieved from https://store.samhsa.gov/sites/default/files/private/sma12-4171.pdf.
Centers for Medicare & Medicaid Services (CMS). (2016). CMS Expands Medicare Payment for Behavioral Health Services. Retrieved from https://mcdonaldhopkins.com/wapi/Pdf/View?url=https://mcdonaldhopkins.com/Insights/Alerts/2016/11/09/CMS-expands-Medicare-payment-for-behavioral-health-services.
Centers for Medicare & Medicaid Services (CMS). (2018). State-by-State Health Home State Plan Amendment Matrix. Retrieved from https://www.medicaid.gov/state-resource-center/medicaid-state-technical….
Commission on Combating Drug Addiction and the Opioid Crisis. (2017). Report of the President's Commission on Combating Drug Addiction and the Opioid Crisis. Washington, D.C. Retrieved from https://www.indexinvestor.com/resources/Research-Materials/Social/US_Opioid_Commission_Report.pdf.
Compass Health Analytics, Inc. (2016). Analysis of New Hampshire Commercial Insurance Claim Data Related to Substance Use Disorder: Reimbursement Rates. Retrieved from https://www.nh.gov/insurance/reports/documents/080516_nhid_analysis_of_claims_for_substance_use_disorder_pricing.pdf.
Council for Accreditation of Counseling and Related Education Programs (CACREP). (2016). CACREP Standards. Section 5-A. Retrieved from https://www.cacrep.org/for-programs/2016-cacrep-standards/.
Das, S., & Roberts, L.W. (2016). Addiction training: Striving to fill an unmet need. Academic Psychiatry, 40, 451-453. doi: 10.1007/s40596-016-0535-x.
Falcone, A., & Berke, D. (2018). Medicaid Managed Care Contracting. An Advocacy Guide for State Associations of Behavioral Health Providers. National Council for Behavioral Health. Retrieved from https://www.thenationalcouncil.org/wp-content/uploads/2018/08/Medicaid-Managed-Care-Contracting-Guide-for-State-Associations-FTLF-2018_Updated-8.8.2018.pdf.
Glasner-Edwards, S., & Rawson, R. (2010). Evidence-based practices in addiction treatment: Review and recommendations for public policy. Health Policy (Amsterdam, Netherlands), 97(2-3), 93-104. doi: 10.1016/j.healthpol.2010.05.013.
Gostin, L.O., Burris, S.C., & Lazzarini, Z. (1999). The law and the public's health: A study of infectious disease law in the United States. Columbia Law Review, 99(1), 59-128. doi: 10.2307/1123597. Retrieved from https://www.jstor.org/stable/i246982.
Grogan, C.M., Andrews, C., Abraham, A., Humphreys, K., Pollack, H.A., Smith, B.T., & Friedmann, P.D. (2016). Survey highlights differences in Medicaid coverage for substance use treatment and opioid use disorder medications. Health Affairs, 35(12), 2289-2296. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5304419/.
Hagedorn, W.B., Culbreth, J.R., & Cashwell, C.S. (2012). Addiction counseling accreditation: CACREP's role in solidifying the counseling profession. Professional Counselor, 2(2), 124-133. dio: org/10.15241/wbh.2.2.124.
Hinde, J., Bray, J., Kaiser, D., & Mallonee, E. (2017). The influence of state-level policy environments on the activation of the Medicaid SBIRT reimbursement codes. Addiction, 112 (Suppl. 2), 82-91. doi: 10.1111/add.13655.
Health Resources and Services Administration (HRSA). (2018). State-Level Projections of Supply and Demand for Behavioral Health Occupations: 2016-2030. Rockville, MD: U.S. Department of Health and Human Services, Health Resources and Services Administration, National Center for Health Workforce Analysis. Retrieved from https://bhw.hrsa.gov/sites/default/files/bhw/nchwa/projections/addiction-counselors-2018.pdf.
Institute of Medicine (IOM). (2006). Improving the Quality of Health Care for Mental and Substance-Use Conditions. Washington, DC: National Academies Press. Retrieved from https://www.nap.edu/catalog/11470/improving-the-quality-of-health-care-for-mental-and-substance-use-conditions.
Institute of Medicine (IOM). (2011). For the Public's Health: Revitalizing Law and Policy to Meet New Challenges. Washington, DC: National Academies Press.
International Certification & Reciprocity Consortium (IC&RC). (2018). Licensure vs. Certification. Retrieved from https://www.internationalcredentialing.org/lic-cert.
Johnson, J., & Miller, L. (2016). Report on Integration of Substance Abuse Payment and Care Coordination with Physical and Mental Health. Vermont Governor's Office. Retrieved from http://hcr.vermont.gov/sites/hcr/files/pdfs/Mental%20Health%20Integration%20Leg%20Report%201.15.16%20FINAL.pdf.
Kerwin, M.E., Walker-Smith, K., & Kirby, K.C. (2006). Comparative analysis of state requirements for the training of substance abuse and mental health counselors. Journal of Substance Abuse Treatment, 30, 173-181. doi: org/10.1016/j.jsat.2005.11.004.
Lamb, S., Greenlick, M.R., & McCarty, D. (1998). Bridging the Gap Between Practice and Research: Forging Partnerships with Community-based Drug and Alcohol Treatment. Washington, DC: National Academy Press.
Mauri, A., Harbin, H., Unützer, J., Carlo, A., Ferguson, R., & Schoenbaum, M. (2017). Payment Reform and Opportunities for Behavioral Health: Alternative Payment Model Examples. Scattergood Foundation, PEGS Foundation, and Kennedy Forum. Retrieved from http://www.scattergoodfoundation.org/sites/default/files/Scattergood_AP….
Medicaid and CHIP Payment and Access Commission (MACPAC). (2016). State Policies for Behavioral Health Services Covered under the State Plan. Retrieved from https://www.macpac.gov/publication/behavioral-health-state-plan-services/.
Medicaid and CHIP Payment and Access Commission (MACPAC). (2018). June 2018 Report to Congress on Medicaid and CHIP. Retrieved from https://www.macpac.gov/publication/june-2018-report-to-congress-on-medicaid-and-chip/.
Miller, G., Scarborough, J., Clark, C., Leonard, J., & Keziah, T. (2010). The need for national credentialing standards for addiction counselors. Journal of Addictions and Offender Counseling, 30(2), 50-57. doi: 10.1002/j.2161-1874.2010.tb00056.x.
Morgen, K., Miller, G., & Stretch, L.S. (2012). Addiction counseling licensure issues for licensed professional counselors. Professional Counselor, 2(1), 58-65. doi: 10.15241/kmm.2.1.58.
Mustaine, B., West, P., & Wyrick, B. (2003). Substance abuse counselor certification requirements: Is it time for a change? Journal of Addictions and Offender Counseling, 23(2), 99-107. doi: 10.1002/j.2161-1874.2003.tb00174.x.
Musumeci, M., Rudowitz, R., Hinton, E., Antonisse, L., & Hall, C. (2018). Section 1115 Medicaid Demonstration Waivers: The Current Landscape of Approved and Pending Waivers. Issue Brief. Washington, DC: Kaiser Family Foundation. Retrieved from http://files.kff.org/attachment/Issue-Brief-Section-1115-Medicaid-Demonstration-Waivers-The-Current-Landscape-of-Approved-and-Pending-Waivers.
New Hampshire Department of Health and Human Services (NHBDAS). (2016). New Hampshire's Substance Use Disorder Continuum of Care Assets and Gaps Assessment Results. New Hampshire Department of Health and Human Services, Bureau of Drug and Alcohol Services. Retrieved from https://www.dhhs.nh.gov/dcbcs/bdas/documents/coc-assests-gap.pdf.
Office of National Drug Control Policy (ONDCP). (2019). National Drug Control Strategy. Washington, DC: Executive Office of the President of the United States.
Osborn, D.P. (2015). Licensing the addiction profession in all 50 states: The process begins. Advances in Addiction and Recovery, 3(1), 20-23. Retrieved from https://www.naadac.org/AAR-archive/.
Page, C., Beck, A.J., Buche, J., Singer, P.M., Vazquez, C., & Perron, B. (2017). National Assessment of Scopes of Practice for the Behavioral Health Workforce. Retrieved from http://www.behavioralhealthworkforce.org/wp-content/uploads/2016/09/FA3_SOP_Full-Report-3.pdf.
Park-Lee, E., Lipari, R.N., Hedden, S.L., Kroutil, L.A., & Porter, J.D. (2017). Receipt of Services for Substance Use and Mental Health Issues among Adults: Results from the 2016 National Survey on Drug Use and Health. NSDUH Data Review. Rockville, MD: Substance Abuse and Mental Health Services Administration. Retrieved from https://www.samhsa.gov/data/.
Rieckmann, T., Farentinos, C., Tillotson, C.J., Kocarnik, J., & McCarty, D. (2011). The substance abuse counseling workforce: Education, preparation, and certification.Substance Abuse, 32(4), 180-90.
Ryan, O., Murphy, D., & Krom, L. (2012). Vital Signs: Taking the Pulse of the Addiction Treatment Workforce. A National Report, Version 1. Kansas City, MO: Addiction Technology Transfer Center. Retrieved from https://www.integration.samhsa.gov/workforce/VitalSignsReport.pdf.
Substance Abuse and Mental Health Services Administration (SAMHSA) (2011). National Survey of Substance Abuse Treatment Services (N-SSATS): 2010. Data on Substance Abuse Treatment Facilities. DASIS Series S-59, HHS Publication No. (SMA) 11-4665. Rockville, MD: Substance Abuse and Mental Health Services Administration. Retrieved from https://wwwdasis.samhsa.gov/dasis2/nssats/2010_nssats_rpt.pdf.
Substance Abuse and Mental Health Services Administration (SAMHSA). (2011). Scopes of Practice and Career Ladder for Substance Use Disorder Counseling. Rockville, MD: Substance Abuse and Mental Health Services Administration. Retrieved from http://atforum.com/documents/PEP11-SCOPES.pdf.
Substance Abuse and Mental Health Services Administration (SAMHSA). (2014). Projections of National Expenditures for Treatment of Mental and Substance Use Disorders, 2010-2020. HHS Publication No. SMA-14-4883. Rockville, MD: Substance Abuse and Mental Health Services Administration. Retrieved from https://store.samhsa.gov/sites/default/files/private/sma14-4883.pdf.
Substance Abuse and Mental Health Services Administration (SAMHSA). (2017). Coding for Screening and Brief Intervention Reimbursement. Rockville, MD: Substance Abuse and Mental Health Services Administration. Retrieved from https://www.samhsa.gov/sbirt/coding-reimbursement.
Substance Abuse and Mental Health Services Administration (SAMHSA). (2018a). National Survey of Substance Abuse Treatment Services (N-SSATS): 2017. Data on Substance Abuse Treatment Facilities. Rockville, MD: Substance Abuse and Mental Health Services Administration. Retrieved from https://www.samhsa.gov/data/sites/default/files/cbhsq-reports/2017_NSSATS.pdf.
Substance Abuse and Mental Health Services Administration (SAMHSA). (2018b). Key Substance Use and Mental Health Indicators in the United States: Results from the 2017 National Survey on Drug Use and Health. HHS Publication No. SMA 18-5068, NSDUH Series H-53. Rockville, MD: Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality. Retrieved from https://www.samhsa.gov/data/report/2017-nsduh-annual-national-report.
Turner-Bull, S. (2011). Moving to licensure. Addiction Professional, 9(2), 9-11. Retrieved from https://www.addictionpro.com/article/moving-licensure.
U.S. Bureau of Labor Statistics. (2018). Occupational Outlook Handbook, 2018-19 Edition. Lanham, MD: Bernan Press.
Wendler, A.M., & Murdock, T.B. (2006). Evaluation of a cross-training curriculum for mental health and addiction counselors. Journal of Teaching in the Addictions, 4(2), 63-78. doi: 10.1300/J188v04n02_04.
APPENDIX A: Licensing and Credentialing Detailed Tables
The following tables are contained in this section:
- EXHIBIT A1: SUD Treatment Career Ladder, by State
- EXHIBIT A2: Requirements: SAMHSA's Category 4--Independent SUD Counselor/Supervisor
- EXHIBIT A3: Requirements: SAMHSA's Category 3--Clinical SUD Counselor
- EXHIBIT A4: Requirements: SAMHSA's Category 2--SUD Counselor
- EXHIBIT A5: Requirements: SAMHSA's Category 1--Associate SUD Counselor
- EXHIBIT A6: Requirements: SAMHSA's SUD Technician Category
- EXHIBIT A7: Requirements: Clinical Supervisor
- EXHIBIT A8: Requirements: Peer Recovery Specialist
- EXHIBIT A9: Requirements: Prevention Specialist
EXHIBIT A1: SUD Treatment Career Ladder, by State
| EXHIBIT A1. SUD Treatment Career Ladder, by State | |||||||
|---|---|---|---|---|---|---|---|
| State Abbr. | SAMHSA's Category 4 | SAMHSA's Category 3 | SAMHSA's Category 2 | SAMHSA's Category 1 | SAMHSA's SUD Technician | Peer Recovery Specialist | Supervisor |
| AK | Advanced Behavioral Health Counselor | Behavioral Health Counselor II Chemical Dependency Counselor II |
Behavioral Health Counselor I Chemical Dependency Counselor I |
Chemical Dependency Counselor Technician Behavioral Health Technician |
Chemical Dependency Clinical Supervisor | ||
| AL | Advanced Alcohol & Drug Counselor | National Certified Addiction Counselor II | National Certified Addiction Counselor I State Certified Addiction Counselor Certified Adolescent Alcohol & Drug Abuse Professional Certified Alcohol & Drug Counselor |
Associate Addiction Professional | Certified Recovery Support Specialist | Certified Clinical Supervisor | |
| AR | Licensed Alcoholism & Drug Abuse Counselor | Advanced Certified Alcohol & Drug Counselor | Licensed Associate Alcoholism & Drug Abuse Counselor Alcohol & Drug Counselor |
Certified Alcoholism & Drug Abuse Technician | Peer Recovery Coach | Certified Clinical Supervisor | |
| AZ | Licensed Independent Substance Abuse Counselor | Advanced Alcohol & Drug Abuse Counselor | Licensed Associate Substance Abuse Counselor Certified Alcohol & Drug Abuse Counselor |
Certified Addiction Counselor | Licensed Substance Abuse Technician | Certified Peer Recovery Specialist | Certified Clinical Supervisor |
| CA | Licensed Advanced Alcohol Drug Counselor CADTP Alcohol/Other Drug Counselor-Advanced |
Certified Alcohol Drug Counselor II | Certified Alcohol Drug Counselor I CADTP Alcohol/Other Drug Counselor |
Registered Alcohol Drug Technician | Certified Peer Recovery Specialist | CADTP Alcohol/Other Drug Counselor-Clinical Supervisor CCAPP Certified Alcohol & Drug Counselor-Clinical Supervisor |
|
| CO | Licensed Addiction Counselor | Certified Addiction Counselor III | Certified Addiction Counselor II | Certified Addiction Counselor I | Colorado Peer & Family Specialist | ||
| CT | Licensed Alcohol & Drug Counselor | Certified Addiction Counselor | Certified Alcohol & Drug Counselor | Certified Addiction Counselor-Provisional | Certified Peer Recovery Specialist | Certified Clinical Supervisor | |
| DC | Advanced Certified Alcohol & Drug Counselor Certified Addiction Counselor II |
Certified Alcohol & Drug Counselor Certified Addiction Counselor I |
Certified Peer Specialist | Certified Clinical Supervisor | |||
| DE | Licensed Chemical Dependency Professional | Certified Advanced Alcohol & Drug Counselor | Certified Alcohol & Drug Counselor | Certified Peer Recovery Specialist | Certified Clinical Supervisor | ||
| FL | Certified Master's Level Addiction Professional | Certified Addiction Professional | Certified Addiction Counselor | Certified Behavioral Health Technician | Certified Recovery Support Specialist National Certified Peer Specialist Certified Recovery Peer Specialist |
||
| GA | Certified Advanced Alcohol & Drug Counselor | Certified Alcohol & Drug Counselor II Certified Addiction Counselor II |
Certified Alcohol & Drug Counselor I Certified Addiction Counselor I |
Electronic-Counseling Alcohol & Drug Counselor | Counselor-In-Training Certified Alcohol & Drug Counselor Trainee |
Certified Peer Recovery Coach | Certified Clinical Supervisor |
| HI | Certified Substance Abuse Counselor | Hawaii Certified Peer Specialist | Certified Clinical Supervisor | ||||
| IA | International Advanced Alcohol & Drug Counselor | International Alcohol & Drug Counselor | Certified Alcohol & Drug Counselor Certified Co-Occurring Disorders Professional |
Certified Treatment Assistant | Certified Peer Recovery Specialist | Certified Clinical Supervisor | |
| ID | Advanced Certified Alcohol/Drug Counselor | Certified Alcohol/Drug Counselor | Idaho Student of Addiction Studies | Certified Peer Recovery Coach | Certified Clinical Supervisor | ||
| IL | Certified Advanced Alcohol & Other Drug Counselor Certified Reciprocal Alcohol & Other Drug Abuse Counselor |
Certified Alcohol & Drug Counselor | Certified Assessment & Referral Specialist | Certified Associate Addictions Professional | Certified Peer Recovery Specialist | Certified Supervisor Alcohol & Other Drug Counselor | |
| IN | Licensed Clinical Addiction Counselor | Licensed Clinical Addiction Counselor Associate Certified Alcoholism & Drug Abuse Counselor IV Certified Co-Occurring Disorders Professional Diplomat |
Licensed Addiction Counselor Indiana Certified Addiction Counselor Level II Certified Co-Occurring Disorders Professional Certified Alcoholism & Drug Abuse Counselor II |
Licensed Addiction Counselor Associate Indiana Certified Addiction Counselor Level I Certified Alcoholism & Drug Abuse Counselor I |
Addiction Counselor in Training Addiction Professional in Training |
Certified Addiction Peer Recovery Coach II Certified Addiction Peer Recovery Coach I |
Certified Clinical Supervisor |
| KS | Licensed Clinical Addiction Counselor | Licensed Masters Addiction Counselor | Licensed Addiction Counselor | ||||
| KY | Licensed Clinical Alcohol & Drug Counselor | Licensed Clinical Alcohol & Drug Counselor Associate | Certified Alcohol & Drug Counselor | Registered Alcohol & Drug Peer Support Specialist | |||
| LA | Licensed Addiction Counselor | Certified Advanced Alcohol & Drug Counselor | Certified Addiction Counselor | Registered Addiction Counselor Counselor-in-Training |
Addiction Treatment Assistant | Peer Recovery Support Specialist | Certified Clinical Supervisor |
| MA | Licensed Alcohol & Drug Counselor I Certified Alcohol & Drug Counselor II |
Licensed Alcohol & Drug Counselor II | Certified Alcohol & Drug Counselor | Certified Alcoholism Counselor | Licensed Alcohol & Drug Counselor Assistant | Certified Addictions Recovery Coach | Certified Clinical Supervisor |
| MD | Licensed Clinical Alcohol & Drug Counselor | Licensed Graduate Alcohol & Drug Counselor | Certified Associate Counselor-Alcohol & Drug Certified Co-Occurring Disorders Professional Certified Chemical Dependency Counselor |
Certified Supervised Counselor-Alcohol & Drug | Certified Peer Recovery Specialist | Certified Clinical Supervisor | |
| ME | Licensed Alcohol & Drug Counselor | Certified Alcohol & Drug Counselor | Alcohol & Drug Counseling Aide | Certified Clinical Supervisor | |||
| MI | Certified Advanced Alcohol & Drug Counselor | Certified Alcohol & Drug Counselor | Certified Peer Recovery Mentor | Certified Clinical Supervisor | |||
| MN | Certified Advanced Alcohol & Drug Counselor | Licensed Alcohol & Drug Counselor | Certified Alcohol & Drug Counselor Reciprocal | Certified Alcohol & Drug Counselor | Certified Peer Recovery Specialist Reciprocal Certified Peer Recovery Specialist |
Licensed Alcohol & Drug Counselor Supervisor Certified Clinical Supervisor Reciprocal |
|
| MO | Certified Reciprocal Advanced Alcohol & Drug Counselor | Addiction Counselor III Certified Reciprocal Alcohol & Other Drug Counselor Certified Alcohol & Drug Counselor |
Addiction Counselor II Missouri Associate Alcohol Drug Counselor II Registered Alcohol Drug Counselor-Provisional |
Addiction Counselor I Missouri Associate Alcohol Drug Counselor I |
Certified Reciprocal Peer Recovery | ||
| MS | Certified Advanced Alcohol & Drug Counselor Certified Addictions Therapist |
Certified Alcohol & Drug Counselor II Provisionally Certified Addictions Therapist |
Certified Alcohol & Drug Counselor I | Certified Alcohol & Drug Counselor | Intern Counselor | Certified Peer Support Specialist Professional | Certified Clinical Supervisor |
| MT | Licensed Addiction Counselor | Addiction Counselor License Candidate | Behavioral Health Peer Support Specialist | ||||
| NC | Licensed Clinical Addiction Specialist | Certified Substance Abuse Counselor | Peer Support Specialist | Certified Clinical Supervisor | |||
| ND | Licensed Master Addiction Counselor | Licensed Clinical Addiction Counselor | Licensed Addiction Counselor | Registered Clinical Supervisor | |||
| NE | Licensed Alcohol & Drug Counselor | Provisionally Licensed Alcohol & Drug Counselor | Peer Support & Wellness Specialist | ||||
| NH | Master Licensed Alcohol & Drug Counselor | Licensed Alcohol & Drug Counselor | Certified Recovery Support Worker | Licensed Clinical Supervisor | |||
| NJ | Licensed Clinical Alcohol & Drug Counselor | Certified Alcohol & Drug Counselor | Chemical Dependence Associate | Certified Peer Recovery Specialist | Certified Clinical Supervisor | ||
| NM | Licensed Alcohol & Drug Abuse Counselor | Certified Alcohol & Drug Counselor | Licensed Substance Abuse Associate Counselor | Certified Peer Support Worker | Certified Clinical Supervisor | ||
| NV | Licensed Clinical Alcohol & Drug Abuse Counselor | Licensed Alcohol & Drug Abuse Counselor | Certified Alcohol & Drug Abuse Counselor | Provisional Alcohol & Drug Abuse Counselor | Certified Alcohol & Drug Abuse Counselor Intern | Peer Recovery & Support Specialist | |
| NY | Master Credentialed Alcoholism & Substance Abuse Counselor | Advanced Credentialed Alcoholism & Substance Abuse Counselor Credentialed Alcoholism & Substance Abuse Counselor II |
Credentialed Alcoholism & Substance Abuse Counselor | Credentialed Alcoholism & Substance Abuse Counselor Trainee | Certified Addiction Recovery Coach Certified Recovery Peer Advocate |
||
| OH | Licensed Independent Chemical Dependency Counselor | Licensed Chemical Dependency Counselor III | Licensed Chemical Dependency Counselor II | Chemical Dependency Counselor Assistant | Chemical Dependency Counselor Assistant Preliminary | Ohio Certified Peer Recovery Supporter | Licensed Independent Chemical Dependency Counselor-Clinical Supervisor |
| OK | Licensed Alcohol & Drug Counselor | Certified Alcohol & Drug Counselor | Certified Peer Recovery Support Specialist | ||||
| OR | Certified Alcohol Drug Counselor III | Certified Alcohol Drug Counselor II | Certified Alcohol Drug Counselor I | Certified Addiction Peer Recovery Counselor | |||
| PA | Certified Advanced Alcohol & Drug Counselor | Certified Alcohol & Drug Counselor | Certified Associate Addiction Counselor | Associate Addiction Counselor | Certified Allied Addiction Practitioner Certified Intervention Professional |
Certified Recovery Specialist | Certified Clinical Supervisor |
| RI | Licensed Chemical Dependency Clinical Supervisor | Licensed Chemical Dependency Professional Certified Advanced Alcohol & Drug Counselor Student Assistance Counselor |
Certified Alcohol & Drug Counselor | Provisional Alcohol & Drug Counselor | Certified Peer Recovery Specialist | Certified Clinical Supervisor | |
| SC | Certified Addictions Counselor II | Certified Addictions Counselor I | Certified Clinical Supervisor | ||||
| SD | Licensed Addiction Counselor | Certified Addiction Counselor | Addiction Counselor Trainee | ||||
| TN | Level II Licensed Alcohol & Drug Abuse Counselor | Level I Licensed Alcohol & Drug Abuse Counselor | Certified Peer Recovery Specialist | Certified Qualified Clinical Supervisor | |||
| TX | Advanced Alcohol & Drug Counselor Certified Chemical Dependency Specialist |
Licensed Chemical Dependency Counselor | Alcohol & Other Drug Abuse Counselor | Licensed Chemical Dependency Counselor Intern | Peer Recovery Support Specialist | Certified Clinical Supervisor | |
| UT | Licensed Advanced Substance Use Disorder Counselor Advanced Alcohol & Drug Counselor |
Alcohol & Drug Counselor Certified Advanced Substance Use Disorder Counselor |
Licensed Substance Use Disorder Counselor Certified Substance Use Disorder Counselor Certified Advanced Substance Use Disorder Counselor Intern |
Certified Substance Use Disorder Counselor Intern | Certified Peer Support Specialist | Certified Clinical Supervisor | |
| VA | Licensed Substance Abuse Treatment Practitioner | Certified Advanced Alcohol & Drug Counselor | Certified Substance Abuse Counselor Certified Alcohol & Drug Counselor |
Certified Substance Abuse Counselor Assistant Associate Addiction Counselor |
Certified Peer Recovery Specialist | Certified Clinical Supervisor | |
| VT | Licensed Alcohol & Drug Abuse Counselor | Certified Alcohol & Drug Abuse Counselor | Apprentice Addiction Professional | Vermont Certified Recovery Coach | |||
| WA | Chemical Dependency Professional | Chemical Dependency Professional Trainee | Certified Peer Counselor | ||||
| WI | Clinical Substance Abuse Counselor | Substance Abuse Counselor | Substance Abuse Counselor-in-Training | Certified Peer Specialist | Independent Clinical Supervisor | ||
| WV | Advanced Alcohol & Drug Counselor | Alcohol & Drug Counselor | Peer Recovery Support Specialist | Clinical Supervisor | |||
| WY | Licensed Addictions Therapist | Provisional Addictions Therapist | Certified Addictions Practitioner | Certified Addictions Practitioner Assistant | Certified Peer Specialist | ||
EXHIBIT A2: Requirements: SAMHSA's Category 4--Independent SUD Counselor/Supervisor
| EXHIBIT A2. Requirements: SAMHSA's Category 4--Independent SUD Counselor/Supervisor | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| State Abbr. | Credential Title | Minimum Degree | Education Hours | Practice Hours | Supervision Hours | Required Examination* | Annual Cont. Educ. Hours | Renewal Period (months) | Reciprocity |
| AK | Advanced Behavioral Health Counselor | None | With degree 70; without degree 548 | With degree 10k; without degree 12k | 100 | None | 40 | 24 | Yes |
| AR | Licensed Alcoholism & Drug Abuse Counselor | Master's | 270 | 6,000 | Not stated | Any nationally recognized exam | 40 | 24 | No |
| AZ | Licensed Independent Substance Abuse Counselor | Bachelor's | 24 semester credit hours | 300 | 100 | IC&RC AADC, NAADAC NCAC II or MAC, or NBCC Master Addiction Counselor | 30 | 24 | No |
| CO | Licensed Addiction Counselor | Master's | 168 | 3,000 | 2 per month | NAADAC MAC | 40 | 24 | Not stated |
| CT | Licensed Alcohol & Drug Counselor | Master's | 360 | 6,000 | 300 | IC&RC ADC | 20 | 12 | Yes |
| DE | Licensed Chemical Dependency Professional | Master's, & must be Certified Alcohol & Drug Counselor | 30 | 3,200 | 100 | IC&RC ADC | 40 | 24 | Yes |
| GA | Certified Advanced Alcohol & Drug Counselor | Master's | 300 | 4,000 | 300 | IC&RC AADC | 40 | 24 | Yes |
| IA | International Advanced Alcohol & Drug Counselor | Master's | 186 | 2,000 | 300 | IC&RC AADC | 40 | 24 | Yes |
| IN | Licensed Clinical Addiction Counselor | Master's | 27 semester hours | 4,000 | 200 | IC&RC AADC or NAADAC MAC | 40 | 24 | Yes |
| KS | Licensed Clinical Addiction Counselor | Master's | 27 semester hours | 6 semester hours | 150 | NAADAC NCAC II or MAC | 30 | 24 | Yes |
| KY | Licensed Clinical Alcohol & Drug Counselor | Master's | 180 | 2,000 | 300 | IC&RC AADC | 60 | 36 | Yes |
| LA | Licensed Addiction Counselor | Master's | 270 | 2,000 | 300 | IC&RC AADC | 48 | 24 | Not stated |
| MA | Licensed Alcohol & Drug Counselor I | Master's | 270 | 6,000 | 300 | IC&RC Exam (not specified) | 40 | 24 | Yes |
| Certified Alcohol & Drug Counselor II | Master's | 180 | 2,000 | 300 | IC&RC AADC | 40 | 24 | Yes | |
| MD | Licensed Clinical Alcohol & Drug Counselor | Master's | 48 semester credits | 2,000 | 100 | NAADAC MAC & Law Test | 40 | 24 | Yes |
| MN | Certified Advanced Alcohol & Drug Counselor | Master's | 180 | 2,000 | 300 | IC&RC AADC | 40 | 24 | Yes |
| MO | Certified Reciprocal Advanced Alcohol & Drug Counselor | Master's | 180 | 2,000 | 300 | IC&RC AADC | 20 | 24 | Yes |
| MS | Certified Advanced Alcohol & Drug Counselor | Master's | 270 | 4,000 | 300 | IC&RC AADC | 40 | 24 | Yes |
| Certified Addictions Therapist | Master's | Not stated | 4,000 | Not stated | Department of Mental Health Addictions Therapist Exam | 80 | 48 | Not stated | |
| MT | Licensed Addiction Counselor | Associate | 330 | 1,000 | Not stated | NAADAC NCAC I or NCAC II, Northwest Certification II, or Southwest Certification II | 20 | 12 | Yes |
| NC | Licensed Clinical Addiction Specialist | Master's | 180 | 4,000 | 300 | IC&RC AADC | 40 | 24 | Yes |
| ND | Licensed Master Addiction Counselor | Master's | 31 graduate-level credits | 2,700 | 120 | NAADAC MAC | 40 | 24 | Yes |
| NE | Licensed Alcohol & Drug Counselor | High school or equivalent | 270 | 6,000 | Not stated | IC&RC ADC & the Case Presentation Method Oral Exam | 40 | 24 | Yes |
| NH | Master Licensed Alcohol & Drug Counselor | Master's | 270 | 3,000 | 300 | IC&RC AADC | 48 | 24 | Yes |
| NJ | Licensed Clinical Alcohol & Drug Counselor | Master's | 270 | 3,000 | 300 | IC&RC AADC | 40 | 24 | Yes |
| NM | Licensed Alcohol & Drug Abuse Counselor | Associate | 276 | 3,000 | 200 | NAADAC NCAC I | 40 | 24 | Yes |
| NV | Licensed Clinical Alcohol & Drug Abuse Counselor | Master's | Not stated | 2,000 | Not stated | IC&RC AADC or National Clinical Mental Health Counseling Examination | 40 | 24 | Yes |
| OH | Licensed Independent Chemical Dependency Counselor | Master's | 650 | 2,000 | 400 | IC&RC ADC | 40 | 24 | Yes |
| OK | Licensed Alcohol & Drug Counselor | Master's | 630 | 2,000 | 52 | IC&RC AADC | 180 | 12 | Yes |
| OR | Certified Alcohol Drug Counselor III | Master's | 300 | 6,000 | Not stated | NAADAC MAC & written jurisprudence exam | 40 | 24 | Yes |
| PA | Certified Advanced Alcohol & Drug Counselor | Master's | 180 | 2,000 | 100 | IC&RC AADC | 40 | 24 | Yes |
| RI | Licensed Chemical Dependency Clinical Supervisor | Master's; must be Certified Advanced Alcohol & Drug Counselor | Not stated | 2,000 (Certified Advanced Alcohol & Drug Counselor) | Not stated | IC&RC AADC (for Certified Advanced Alcohol & Drug Counselor certification) | Not stated | 24 | Yes |
| SD | Licensed Addiction Counselor | Master's | 21 semester hours | 2,000 | 300 | IC&RC ADC | 40 | 24 | Yes |
| TN | Level II Licensed Alcohol & Drug Abuse Counselor | Bachelor's | 270 | 4,000 | 100 | NAADAC NCAC II or MAC & a jurisprudence exam | 30 | 24 | Yes |
| TX | Advanced Alcohol & Drug Counselor | Master's | 180 | 2,000 | Not stated | IC&RC AADC | 40 | 24 | Yes |
| Certified Chemical Dependency Specialist | Master's | 135 | 4,000 | Not stated | None | 40 | 24 | No | |
| VA | Licensed Substance Abuse Treatment Practitioner | Master's | 87 semester hours | 600 | 1 per week | NAADAC MAC | 20 | 24 | Yes |
| VT | Licensed Alcohol & Drug Abuse Counselor | Master's | 270 | 2,000 | 100 | IC&RC AADC | 40 | 24 | Yes |
| WV | Advanced Alcohol & Drug Counselor | Master's | 300 | 6,000 | 300 | IC&RC AADC | 40 | 24 | Yes |
| WY | Licensed Addictions Therapist | Master's | 27 | 3,000 | 100 | NAADAC MAC or NBCC Master Addiction Counselor | 45 | 24 | Yes |
*EXAM NAME ABBREVIATIONS:
|
|||||||||
EXHIBIT A3: Requirements: SAMHSA's Category 3--Clinical SUD Counselor
| EXHIBIT A3. Requirements: SAMHSA's Category 3--Clinical SUD Counselor | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| State Abbr. | Credential Title | Minimum Degree | Education Hours | Practice Hours | Supervision Hours | Required Exam* | Annual Cont. Educ. Hours | Renewal Period (months) | Reciprocity |
| AK | Behavioral Health Counselor II | None | With degree 40; without degree 382 | With degree 6k, without degree 8k | 100 | None | 40 | 24 | Yes |
| AK | Chemical Dependency Counselor II | None | With degree 48, without degree 176 | With degree 6k, without degree 8k | 200 | NAADAC NCAC I, NCAC II, or MAC | 40 | 24 | Yes |
| AL | Advanced Alcohol & Drug Counselor | Master's | 180 | 2,000 | 300 | IC&RC AADC | 20 | 12 | Yes |
| AR | Advanced Certified Alcohol & Drug Counselor | Master's | 180 | 2,000 | 300 | IC&RC AADC | 40 | 24 | Yes |
| AZ | Advanced Alcohol & Drug Abuse Counselor | Master's | 180 | 2,000 | Not stated | IC&RC AADC | 40 | 24 | Yes |
| CA | Licensed Advanced Alcohol Drug Counselor | Master's | 300 | 4,000 | Not stated | IC&RC AADC | 50 | 24 | Yes |
| CADTP Alcohol/Other Drug Counselor-Advanced | Not stated | 380 | 10,000 | Not stated | IC&RC Exam (not specified) | 40 | 24 | Yes | |
| CT | Certified Addiction Counselor | Not stated | 300 | 6,000 | 300 | IC&RC ADC | 20 | 12 | Yes |
| DC | Advanced Certified Alcohol & Drug Counselor | Not stated | Not stated | Not stated | Not stated | IC&RC AADC or National Certification Commission Exam (not specified) | Not stated | Not stated | Not stated |
| Certified Addiction Counselor II | Bachelor's | 42 | Not stated | 180 | NAADAC NCAC II & jurisprudence exam | 40 | 24 | Not stated | |
| DE | Certified Advanced Alcohol & Drug Counselor | Master's | 180 | 2,000 | 100 | IC&RC AADC | 40 | 24 | Yes |
| FL | Certified Master's Level Addiction Professional | Master's | 350 | 4,000 | 200 | Florida's Master's Level Certified Addiction Professional Exam; IC&RC AADC if seeking reciprocity | 20 | 12 | Yes |
| GA | Certified Addiction Counselor II | Bachelor's | 270 | 6,000 | 144 | NAADAC NCAC I or NCAC II | 40 | 24 | Yes |
| Certified Alcohol & Drug Counselor II | Bachelor's | 300 | 4,000 | 300 | IC&RC ADC | 40 | 24 | Yes | |
| HI | Certified Substance Abuse Counselor | High school or equivalent | 300 | 6,000 | 400 | IC&RC Exam (not specified) | 40 | 24 | Yes |
| IA | International Alcohol & Drug Counselor | High school or equivalent | 300 | 6,000 | 300 | IC&RC ADC | 40 | 24 | Yes |
| ID | Advanced Certified Alcohol/Drug Counselor | Master's | 180 | 2,000 | 33 | IC&RC AADC | 40 | 24 | Yes |
| IL | Certified Advanced Alcohol & Other Drug Counselor | Master's | 180 | 2,000 | 300 | IC&RC AADC | 40 | 24 | Yes |
| Certified Reciprocal Alcohol & Other Drug Abuse Counselor | High school or equivalent | 300 | 6,000 | 300 | IC&RC ADC | 40 | 24 | Yes | |
| IN | Licensed Clinical Addiction Counselor Associate | Master's | 27 semester hours | 700 | 105 | IC&RC AADC or NAADAC MAC | 40 | 24 | Yes |
| Certified Co-Occurring Disorders Professional Diplomat | Master's | 140 | 2,000 | 100 | IC&RC COD Professional Exam | 40 | 24 | Yes | |
| Certified Alcoholism & Drug Abuse Counselor IV | Bachelor's | 320 | 6,000 | 300 | IC&RC AADC | 40 | 24 | Yes | |
| KS | Licensed Masters Addiction Counselor | Master's | 27 semester hours | Not stated | Not stated | NAADAC MAC | 30 | 24 | Not stated |
| KY | Licensed Clinical Alcohol & Drug Counselor Associate | Master's | 180 | Not stated | Not stated | IC&RC AADC | 60 | 36 | Yes |
| LA | Certified Advanced Alcohol & Drug Counselor | Master's | 180 | 2,000 | 300 | IC&RC AADC | 40 | 24 | Yes |
| MA | Licensed Alcohol & Drug Counselor II | High school or equivalent | 270 | 6,000 | 300 | IC&RC Exam (not specified) | 40 | 24 | Yes |
| MD | Licensed Graduate Alcohol & Drug Counselor | Master's | 27 semester hours | Not stated | Not stated | NAADAC MAC & Law Test | 40 | 24 | No |
| ME | Licensed Alcohol & Drug Counselor | High school or equivalent | Not stated | 2,000 | 1 per every 20 hours of client contact | IC&RC AADC or ADC & Case Presentation Method Oral Exam | 36 hours every 2 years | 12 | Not stated |
| MI | Certified Advanced Alcohol & Drug Counselor | Master's | 186 | 2,000 | 100 | IC&RC AADC | 40 | 24 | Yes |
| MN | Licensed Alcohol & Drug Counselor | Bachelor's | 270 | 880 | Not stated | IC&RC Exam (not specified) or NAADAC NCAC II | 40 | 24 | Yes |
| MO | Addiction Counselor III | High school or equivalent | Not stated | 4,000 | Not stated | None | Not stated | Not stated | Not stated |
| Certified Alcohol & Drug Counselor | High school or equivalent | 180 | 4,000 | 300 | IC&RC ADC | 40 | 24 | No | |
| Certified Reciprocal Alcohol & Other Drug Counselor | High school or equivalent | 300 | 6,000 | 300 | IC&RC ADC | 40 | 24 | Yes | |
| MS | Certified Alcohol & Drug Counselor II | Master's | 270 | 10,000 | 300 | IC&RC ADC | 40 | 24 | Yes |
| Provisionally Certified Addictions Therapist | Master's | Not stated | Not stated | Not stated | None | 80 | 48 | Not stated | |
| ND | Licensed Clinical Addiction Counselor | Bachelor's | 32 credit hours | Not stated | Not stated | Not stated | 40 | 24 | Yes |
| NH | Licensed Alcohol & Drug Counselor | Associate | 270 | 6,000 | 300 | IC&RC ADC | 48 | 24 | Yes |
| NM | Certified Alcohol & Drug Counselor | Not stated | 270 | 6,000 | 300 | IC&RC ADC | 40 | 24 | Yes |
| NV | Licensed Alcohol & Drug Abuse Counselor | Master's | Not stated | 4,000 | Not stated | IC&RC ADC & oral boards | 40 | 24 | Yes |
| NY | Master Credentialed Alcoholism & Substance Abuse Counselor | Master's | 350 | 6,000 | 300 | IC&RC Exam (not specified) | 60 | 36 | Yes |
| OH | Licensed Chemical Dependency Counselor III | Bachelor's | 180 | 2,000 | Not stated | IC&RC ADC | 40 | 24 | Yes |
| PA | Certified Alcohol & Drug Counselor | Bachelor's | 300 | 4,000 | 200 | IC&RC ADC | 40 | 24 | Yes |
| RI | Licensed Chemical Dependency Professional | High school or equivalent (must be certified as a Certified Advanced Alcohol & Drug Counselor or Certified Alcohol & Drug Counselor) | Not stated | Not stated | Not stated | IC&RC AADC or ADC | Not stated | 24 | Yes |
| Certified Advanced Alcohol & Drug Counselor | Master's | 180 | 2,000 | 100 | IC&RC AADC | 40 | 24 | Yes | |
| Student Assistance Counselor | Master's | 60 | 1,350 | 70 | None | 40 | 24 | No | |
| SC | Certified Addictions Counselor II | Bachelor's | 450 | 8,000 | 150 | NAADAC NCAC II & oral exam | 40 | 24 | Yes |
| TX | Licensed Chemical Dependency Counselor | Associate | 270 | 4,000 | 300 | Not stated | 40 | 24 | Yes |
| UT | Licensed Advanced Substance Use Disorder Counselor | Bachelor's | 300 | 4,000 | 350 | NAADAC NCAC II or MAC, or IC&RC AADC | 40 | 24 | Yes |
| Advanced Alcohol & Drug Counselor | Master's | 180 | 2,000 | 300 | IC&RC AADC | 40 | 24 | Yes | |
| VA | Certified Advanced Alcohol & Drug Counselor | Master's | 180 | 2,000 | 100 | IC&RC AADC | 40 | 24 | Yes |
| WA | Chemical Dependency Professional | Associate | 30 semester credits | 2,500 | 50 | NAADAC NCAC II or MAC, or IC&RC AADC | 28 | 24 | Yes |
| WI | Clinical Substance Abuse Counselor | Associate | 366 | 5,000 | Not stated | NAADAC NCAC I & exam on Wisconsin statutes & admin codes | 40 | 24 | Yes |
| WY | Provisional Addictions Therapist | Master's | 420 | 3,000 | 100 | NAADAC MAC or NBCC Master Addiction Counselor | 45 | 24 | Yes |
*EXAM NAME ABBREVIATIONS:
|
|||||||||
EXHIBIT A4: Requirements: SAMHSA's Category 2--SUD Counselor
| EXHIBIT A4. Requirements: SAMHSA's Category 2--SUD Counselor | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| State Abbr. | Credential Title | Minimum Degree | Education Hours | Practice Hours | Supervision Hours | Required Examination* | Annual Cont. Educ. Hours | Renewal Period (months) | Reciprocity |
| AK | Behavioral Health Counselor I | None | With degree 36; without degree 286 | With degree 2k; without degree 4k | 100 | None | 40 | 24 | Yes |
| Chemical Dependency Counselor I | None | With degree 20; without degree 148 | With degree 2k; without degree 4k | 100 | None | 40 | 24 | Yes | |
| AL | National Certified Addiction Counselor II | Bachelor's | 450 | 10,000 | Not stated | NAADAC NCAC II | 50 | 24 | Yes |
| AR | Alcohol & Drug Counselor | Not stated | 300 | 6,000 | 300 | IC&RC ADC | 40 | 24 | Yes |
| Licensed Associate Alcoholism & Drug Abuse Counselor | Bachelor's | 270 | 6,000 | Not stated | Any nationally recognized exam | 40 | 24 | No | |
| AZ | Certified Alcohol & Drug Abuse Counselor | Bachelor's | 200 | 6,000 | Not stated | IC&RC ADC | 40 | 24 | Yes |
| Licensed Associate Substance Abuse Counselor | Bachelor's | 3 semester hours | 3,200 | 100 | IC&RC AADC, NAADAC NCAC II or MAC, or NBCC Master Addiction Counselor | 30 | 24 | No | |
| CA | Certified Alcohol Drug Counselor II | Bachelor's | 315 | 4,000 | Not stated | IC&RC ADC | 50 | 24 | Yes |
| CO | Certified Addiction Counselor III | Bachelor's | 56 | 2,000 | 2 per month | NAADAC NCAC II | 40 | 24 | Not stated |
| CT | Certified Alcohol & Drug Counselor | Not stated | 360 | 6,000 | 300 | IC&RC ADC | 20 | 12 | Yes |
| DC | Certified Addiction Counselor I | Associate | 30 | Not stated | 500 | NAADAC NCAC I & D.C. jurisprudence exam | 40 | 24 | Not stated |
| Certified Alcohol & Drug Counselor | Not stated | Not stated | Not stated | Not stated | IC&RC ADC or National Certification Commission Exam | Not stated | Not stated | Not stated | |
| DE | Certified Alcohol & Drug Counselor | Associate | 300 | 4,000 | 200 | IC&RC ADC | 40 | 24 | Yes |
| FL | Certified Addiction Professional | Bachelor's | 350 | 6,000 | 300 | Florida Certified Addiction Professional Exam. IC&RC ADC if seeking reciprocity | 20 | 12 | Yes |
| GA | Certified Addiction Counselor I | High school or equivalent | 180 | 4,000 | 96 | NAADAC NCAC I | 40 | 24 | Yes |
| Certified Alcohol & Drug Counselor I | High school or equivalent | 300 | 6,000 | 300 | IC&RC ADC | 40 | 24 | Yes | |
| IA | Certified Alcohol & Drug Counselor | High school or equivalent | 150 | 3,000 | 36 | IC&RC ADC | 40 | 24 | Yes |
| Certified Co-Occurring Disorders Professional | Bachelor's | 340 | 6,000 | 200 | IC&RC COD Professional Exam | 40 | 24 | Yes | |
| ID | Certified Alcohol/Drug Counselor | High school or equivalent | 270 | 6,000 | 300 | IC&RC ADC | 40 | 24 | Yes |
| IL | Certified Alcohol & Drug Counselor | High school or equivalent | 225 | 4,000 | 150 | Certified Alcohol & Drug Counselor Illinois Examination | 40 | 24 | No |
| IN | Licensed Addiction Counselor | Bachelor's | 40 semester hours | 4,000 | 150 | IC&RC ADC or NAADAC NCAC II | 40 | 24 | Yes |
| Certified Alcoholism & Drug Abuse Counselor II | None | 270 | 4,000 | 300 | IC&RC ADC | 40 | 24 | Yes | |
| Certified Co-Occurring Disorders Professional | Bachelor's | 200 | 6,000 | 200 | IC&RC COD Professional Exam | 40 | 24 | Yes | |
| Indiana Certified Addiction Counselor Level II | Bachelor's | 450 | 10,000 | 100 | NAADAC NCAC II | 40 | 24 | Yes | |
| KS | Licensed Addiction Counselor | Bachelor's | 30 semester hours | Not stated | Not stated | NAADAC NCAC II | 30 | 24 | Yes |
| KY | Certified Alcohol & Drug Counselor | Bachelor's | 270 | 6,000 | 300 | IC&RC ADC | 60 | 36 | Yes |
| LA | Certified Addiction Counselor | Bachelor's | 270 | 4,000 | 300 | IC&RC AADC | 48 | 24 | Not stated |
| MA | Certified Alcohol & Drug Counselor | High school or equivalent | 300 | 6,000 | 300 | IC&RC Exam (not specified) | 40 | 24 | Yes |
| MD | Certified Associate Counselor-Alcohol & Drug | Bachelor's | 33 semester hours unless degree in counseling | 2,000 | Not stated | NAADAC NCAC II & Maryland law exam | 40 | 24 | Yes |
| Certified Chemical Dependency Counselor | Bachelor's | 300 | 6,000 | 300 | IC&RC ADC | 40 | 24 | Yes | |
| Certified Co-Occurring Disorders Professional | Bachelor's | 200 | 6,000 | 200 | IC&RC COD Professional Exam | 40 | 24 | Yes | |
| ME | Certified Alcohol & Drug Counselor | High school or equivalent | Not stated | 4,000 | 1 per every 20 hours of client contact | IC&RC ADC | 24 every 2 years | 12 | Not stated |
| MI | Certified Alcohol & Drug Counselor | Not stated | 300 | 6,000 | 300 | IC&RC ADC or AADC | 40 | 24 | Yes |
| MN | Certified Alcohol & Drug Counselor Reciprocal | Not stated | 300 | 6,000 | 300 | IC&RC ADC | 40 | 24 | Yes |
| MO | Addiction Counselor II | High school or equivalent | Not stated | Not stated | Not stated | Not stated | Not stated | Not stated | Not stated |
| Missouri Associate Alcohol Drug Counselor II | High school or equivalent | 90 | 2,000 | 300 | Not stated | 20 | 24 | Not stated | |
| Registered Alcohol Drug Counselor-Provisional | Bachelor's | 3 hours of live ethics | 6,000 | Not stated | Not stated | Not stated | No renewal, expires after 2 years | Not stated | |
| MS | Certified Alcohol & Drug Counselor I | Bachelor's | 270 | 8,000 | 300 | IC&RC Exam (not specified) | 40 | 24 | Yes |
| NC | Certified Substance Abuse Counselor | High school or equivalent | 270 | 6,000 | 300 | IC&RC ADC | 60 | 24 | Yes |
| ND | Licensed Addiction Counselor | Bachelor's | 32 credit hours | 960 | 160 | NAADAC NCAC I or MAC | 40 | 24 | Yes |
| NE | Provisionally Licensed Alcohol & Drug Counselor | High school or equivalent | 270 | 300 | Not stated | None | 40 | 24 | No |
| NJ | Certified Alcohol & Drug Counselor | High school or equivalent | 270 | 3,000 | 300 | IC&RC ADC | 60 | 24 | Yes |
| NV | Certified Alcohol & Drug Abuse Counselor | Bachelor's | Not stated | 4,000 | Not stated | IC&RC ADC & state oral exam | 40 | 24 | Yes |
| NY | Advanced Credentialed Alcoholism & Substance Abuse Counselor | Bachelor's | 350 | 6,000 | 300 | IC&RC Exam (not specified) | 60 | 36 | Yes |
| Credentialed Alcoholism & Substance Abuse Counselor II | Associate | 350 | 6,000 | 300 | IC&RC ADC | 60 | 36 | Yes | |
| OH | Licensed Chemical Dependency Counselor II | Associate | 180 | 2,000 | Not stated | IC&RC ADC | 40 | 24 | Yes |
| OK | Certified Alcohol & Drug Counselor | Bachelor's | 45 | 4,000 | 104 | IC&RC ADC | 270 | 12 | Yes |
| OR | Certified Alcohol Drug Counselor II | Bachelor's | 300 | 4,000 | Not stated | NAADAC NCAC II & written jurisprudence exam | 40 | 24 | Yes |
| PA | Certified Associate Addiction Counselor | High school or equivalent | 300 | 6,000 | 300 | IC&RC ADC | 40 | 24 | Yes |
| RI | Certified Alcohol & Drug Counselor | High school or equivalent | 300 | 6,000 | 300 | IC&RC ADC | 40 | 24 | Yes |
| SC | Certified Addictions Counselor I | Bachelor's | 270 | 4,000 | 150 | NAADAC NCAC I & oral exam | |||
| SD | Certified Addiction Counselor | High school or equivalent | 27 semester hours | 8,000 | 300 | IC&RC ADC | 40 | 24 | Yes |
| TN | Level I Licensed Alcohol & Drug Abuse Counselor | High school or equivalent | 270 | 6,000 | 100 | NAADAC NCAC I or MAC & jurisprudence exam | 30 | 24 | Yes |
| TX | Alcohol & Other Drug Abuse Counselor | High school or equivalent | 300 | 6,000 | Not stated | IC&RC ADC | 40 | 24 | Yes |
| UT | Alcohol & Drug Counselor | High school or equivalent | 270 | 6,000 | 300 | IC&RC ADC | 40 | 24 | Yes |
| Certified Advanced Substance Use Disorder Counselor | Bachelor's | 300 | Not stated | 350 | IC&RC ADC, NADAAC NCAC II or MAC | 40 | 24 | Yes | |
| VA | Certified Alcohol & Drug Counselor | Bachelor's | 300 | 4,000 | 200 | IC&RC ADC | 40 | 24 | Yes |
| Certified Substance Abuse Counselor | Bachelor's | 400 | 2,000 | 100 | NAADAC NCAC I | None | 24 | No | |
| VT | Certified Alcohol & Drug Abuse Counselor | Bachelor's | 270 | 4,000 | Not stated | IC&RC ADC | 40 | 24 | Yes |
| WI | Substance Abuse Counselor | Not stated | 360 | 3,000 | Not stated | NAADAC NCAC I & online open-book exam on Wisconsin statutes & administrative code | 30 | 24 | Yes |
| WV | Alcohol & Drug Counselor | High school or equivalent | 300 | 12,000 | 300 | IC&RC ADC | 40 | 24 | Yes |
| WY | Certified Addictions Practitioner | Bachelor's | 27 | Not stated | Not stated | IC&RC ADC or NAADAC NCAC II | 45 | 24 | Yes |
*EXAM NAME ABBREVIATIONS:
|
|||||||||
EXHIBIT A5: Requirements: SAMHSA's Category 1--Associate SUD Counselor
| EXHIBIT A5. Requirements: SAMHSA's Category 1--Associate SUD Counselor | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| State Abbr. | Credential Title | Minimum Degree | Education Hours | Practice Hours | Supervision Hours | Required Examination* | Annual Cont. Educ. Hours | Renewal Period (months) | Reciprocity |
| AL | Certified Adolescent Alcohol & Drug Abuse Professional | Not stated | 270 | 6,000 | 300 | State exam | 20 | 12 | No |
| Certified Alcohol & Drug Counselor | High school or equivalent | 270 | 6,000 | 300 | IC&RC ADC | 20 | 12 | Yes | |
| National Certified Addiction Counselor I | Not stated | 270 | 6,000 | Not stated | NAADAC NCAC I | 50 | 12 | Yes | |
| State Certified Addiction Counselor | Not stated | 60 | 4,000 | Not stated | Not stated | 50 | 24 | Yes | |
| AZ | Certified Addiction Counselor | High school or equivalent | 200 | 4,000 | Not stated | Not stated | 40 | 24 | No |
| CA | CADTP Alcohol/Other Drug Counselor | Not stated | 315 | 2,080 | 160 | IC&RC ADC | 40 | 24 | Yes |
| Certified Alcohol Drug Counselor I | Associate | 315 | 2,080 | Not stated | IC&RC ADC | 50 | 24 | Yes | |
| CO | Certified Addiction Counselor II | High school or equivalent | 126 | 2,000 | 3 per month | NAADAC NCAC I | 40 | 24 | Not stated |
| CT | Certified Addiction Counselor-Provisional | Not stated | 300 | 2,000 | 300 | IC&RC ADC | None | Non-renewable | Yes |
| FL | Certified Addiction Counselor | High school or equivalent | 270 | 6,000 | 300 | IC&RC ADC | 20 | 12 | Yes |
| GA | Electronic-Counseling Alcohol & Drug Counselor | High school or equivalent | 18 | Not stated | Not stated | None | 6 | 24 | No |
| IL | Certified Assessment & Referral Specialist | High school or equivalent | 185 | 2,000 | 150 | Assessment/Referral Specialist Examination | 40 | 24 | No |
| IN | Indiana Certified Addiction Counselor Level I | Not stated | 270 | 6,000 | 50 | NAADAC NCAC I | 40 | 24 | Yes |
| Certified Alcoholism & Drug Abuse Counselor I | None | 180 | 2,000 | 220 | Not stated | 40 | 24 | No | |
| Licensed Addiction Counselor Associate | Bachelor's | 40 semester hours | 350 | Not stated | IC&RC ADC or NAADAC NCAC II | 40 | 24 | Yes | |
| LA | Counselor-in-Training | High school or equivalent | 180 | Not stated | Not stated | Not stated | 20 | 12 | Not stated |
| Registered Addiction Counselor | High school or equivalent | 270 | 6,000 | 300 | IC&RC AADC | 48 | 24 | Not stated | |
| MA | Certified Alcoholism Counselor | High school or equivalent | 180 | 4,000 | 120 | IC&RC Exam (not specified) | 40 | 24 | No |
| MD | Certified Supervised Counselor-Alcohol & Drug | Associate | 24 semester credits | 6 semester credit internship | Not stated | NAADAC NCAC I & the Maryland law exam | 40 | 24 | Yes |
| MN | Certified Alcohol & Drug Counselor | Not stated | 270 | None | 300 hours | IC&RC ADC | 40 | 24 | No |
| MO | Addiction Counselor I | Bachelor's | 15 credit hours | Not stated | Not stated | Not stated | Not stated | Not stated | Not stated |
| Missouri Associate Alcohol Drug Counselor I | High school or equivalent | 3 | 160 | Not stated | Not stated | 20 | 24 | Not stated | |
| MS | Certified Alcohol & Drug Counselor | High school or equivalent | 270 | 6,000 | 300 | IC&RC ADC | 40 | 24 | Yes |
| MT | Addiction Counselor License Candidate | Associate | None | None | None | None | 20 | 12 | No |
| NJ | Chemical Dependence Associate | Not stated | 54 | 1,500 | 200 | Not stated | 24 | 24 | Not stated |
| NM | Licensed Substance Abuse Associate Counselor | Associate | 90 | Not stated | Not stated | None | 40 | 24 | No |
| NV | Provisional Alcohol & Drug Abuse Counselor | Bachelor's | Not stated | 4,000 | Not stated | None | Not stated | Non-renewable | Not stated |
| NY | Credentialed Alcoholism & Substance Abuse Counselor | High school or equivalent | 350 | 6,000 | 300 | IC&RC ADC | 60 | 36 | Yes |
| OH | Chemical Dependency Counselor Assistant | High school or equivalent | 70 | Not stated | Not stated | None | 40 | 24 | No |
| OR | Certified Alcohol Drug Counselor I | Associate | 150 | 1,000 | Not stated | NAADAC NCAC I | 40 | 24 | Yes |
| PA | Associate Addiction Counselor | High school or equivalent | 100 | 2,000 | 100 | None | 40 | 24 | No |
| RI | Provisional Alcohol & Drug Counselor | High school or equivalent | 140 | 2,000 | 150 | None | None | Non-renewable | No |
| SD | Addiction Counselor Trainee | High school or equivalent | Not stated | Not stated | 8 per month | None | None | Non-renewable | Not stated |
| UT | Certified Substance Use Disorder Counselor | Associate | 200 | Not stated | 200 | IC&RC AADC or ADC, NAADAC NCAC I, II, or MAC | 40 | 24 | Yes |
| Licensed Substance Use Disorder Counselor | Associate | 200 | 2,000 | 200 | IC&RC AADC or ADC, NAADAC NCAC I, II, or MAC | 40 | 24 | Yes | |
| Certified Advanced Substance Use Disorder Counselor Intern | Bachelor's | 300 | Not stated | 350 | None | None | Non-renewable | No | |
| VA | Associate Addiction Counselor | High school or equivalent | 200 | 4,000 | 200 | None | 40 | 24 | No |
| Certified Substance Abuse Counselor Assistant | High school or equivalent | 300 | Not stated | 180 | VA State Constructed Certified, Substance Abuse Counselor Assistant Exam | None | 24 | No | |
| VT | Apprentice Addiction Professional | Bachelor's | 40 | Not stated | Not stated | Not stated | 40 | 24 | No |
| WA | Chemical Dependency Professional Trainee | Not stated | 4 | Not stated | 50 | None | None | 24 (renewable 4 times) | No |
| WI | Substance Abuse Counselor-In-Training | Not stated | 100 | None | Not stated | Online open-book exam on Wisconsin statutes & admin code | 30 | 24 | No |
| WY | Certified Addictions Practitioner Assistant | Associate or NCAC I | None with degree; 270 without | Not stated | Not stated | NAADAC NCAC I | 45 | 24 | Yes |
*EXAM NAME ABBREVIATIONS:
|
|||||||||
EXHIBIT A6: Requirements: SAMHSA's SUD Technician Category
| EXHIBIT A6. Requirements: SAMHSA's SUD Technician Category | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| State Abbr. | Credential Title | Minimum Degree | Education Hours | Practice Hours | Supervision Hours | Required Examination* | Annual Cont. Educ. Hours | Renewal Period (months) | Reciprocity |
| AK | Behavioral Health Technician | None | With degree 12; without degree 127 | With degree none; without 2k | 100 | None | 40 | 24 | Yes |
| Chemical Dependency Counselor Technician | None | With degree 20; without degree 84 | None | None | None | 40 | 24 | Yes | |
| AL | Associate Addiction Professional | Not stated | 140 | 2,000 | 150 | State exam | 20 | 12 | No |
| AR | Certified Alcoholism & Drug Abuse Technician | High school or equivalent | 270 | 6,000 | Not stated | Any nationally recognized exam | 40 | 24 | No |
| AZ | Licensed Substance Abuse Technician | Associate | 3 semester hours | None | None | IC&RC ADC or AADC, NAADAC NCAC I, II or MAC | 30 | 24 | No |
| CA | Registered Alcohol Drug Technician | Not stated | 9 | None | None | None | 3 | 12 | Not stated |
| CO | Certified Addiction Counselor I | High school or equivalent | 112 | 1,000 | 3 per month | None | None | 24 | Not stated |
| FL | Certified Behavioral Health Technician | High school or equivalent | 30 | 1,000 | 24 | Certified Behavioral Health Technician Exam | 10 | 12 | Yes |
| GA | Certified Alcohol & Drug Counselor Trainee | High school or equivalent | 300 | 300 | 40 | None | 20 | 12 | No |
| Counselor-In-Training | High school or equivalent | 20 | Not stated | 220 | None | 20 | 12 | No | |
| IA | Certified Treatment Assistant | Not stated | 40 | 500 | Not stated | None | 15 | 24 | No |
| ID | Idaho Student of Addiction Studies | Not stated | 315 | 300 | Not stated | Not stated | 60 | 24 | No |
| IL | Certified Associate Addictions Professional | High school or equivalent | Not stated | Not stated | Not stated | Certified Associate Addictions Professional Exam | 40 | 24 | No |
| IN | Addiction Counselor in Training | Not stated | 12 | Not stated | Not stated | None | 40 | 24 | No |
| Addiction Professional In Training | Not stated | 12 | 320 | Not stated | NAADAC NCAC I | 40 | 24 | Yes | |
| LA | Addiction Treatment Assistant | None | 6 | Not stated | Not stated | Not stated | 6 | 24 | Not stated |
| MA | Licensed Alcohol & Drug Counselor Assistant | High school or equivalent | 50 | 2,000 | None | IC&RC Exam (not specified) | 40 | 24 | Yes |
| ME | Alcohol & Drug Counseling Aide | High school or equivalent | Not stated | Not stated | Not stated | None | 12 hours every 2 years | 12 | Not stated |
| MS | Intern Counselor | High school or equivalent | 186 | Not stated | Not stated | Not stated | Not stated | Not stated | Not stated |
| NV | Certified Alcohol & Drug Abuse Counselor Intern | Not stated | 60 credit hours, plus 12 hours | Not stated | Not stated | None | Not stated | Not stated | Not stated |
| NY | Credentialed Alcoholism & Substance Abuse Counselor Trainee | Not stated | 350 | 4,000 | Not stated | Not stated | Not stated | Not stated | Not stated |
| OH | Chemical Dependency Counselor Assistant Preliminary | High school or equivalent | 40 | Not stated | Not stated | None | 40 | 24 | No |
| PA | Certified Allied Addiction Practitioner | High school or equivalent | 50 | 4,000 | 100 | IC&RC CAAP Exam | 25 | 24 | Yes |
| Certified Intervention Professional | High school or equivalent | 150 | 4,000 | 100 | None | 30 | 24 | No | |
| TX | Licensed Chemical Dependency Counselor Intern | High school or equivalent | 270 | 300 | Not stated | None | None, non-renewable but can be extended 3 years | Non-renewable | No |
| UT | Certified Substance Use Disorder Counselor Intern | Associate | 200 | Not stated | 200 | None | None, 6-month certification | Non-renewable | No |
*EXAM NAME ABBREVIATIONS:
|
|||||||||
EXHIBIT A7: Requirements: Clinical Supervisor
| EXHIBIT A7. Requirements: Clinical Supervisor | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| State Abbr. | Credential Title | Minimum Degree and/or Required Credential to Qualify* | Education Hours | Practice Hours | Supervision Hours | Required Examination^ | Annual Cont. Educ. Hours | Renewal Period (months) | Reciprocity |
| AK | Chemical Dependency Clinical Supervisor | None | With degree 78; without degree 206 | With degree 10k; without degree 12k | 300 | NAADAC NCAC II or MAC | 40 | 24 | Yes |
| AL | Certified Clinical Supervisor | Reciprocal IC&RC ADC, AADC or SUD credential in another field at master's level | Not stated | 10,000 | 200 | IC&RC CS Exam | Not stated | Not stated | Yes |
| AR | Certified Clinical Supervisor | Reciprocal IC&RC counselor credential | 36 | 10,000 | 200 | IC&RC CS Exam | 18 | 24 | Yes |
| AZ | Certified Clinical Supervisor | Not stated | Not stated | Not stated | Not stated | Not stated | 40 | 24 | Yes |
| CA | Licensed Advanced Alcohol Drug Counselor Supervisor | Master's | 345 | 4,000 | Not stated | IC&RC ADC | 50 | 24 | Yes |
| CADTP Alcohol/Other Drug Counselor-Clinical Supervisor | Not stated | 490 | 10,000 | Not stated | IC&RC Exam (not specified) | 46 | 24 | Yes | |
| CCAPP Certified Alcohol & Drug Counselor Clinical Supervisor | Certified Alcohol & Drug Counselor credential | Not stated | Not stated | Not stated | Not stated | Not stated | Not stated | Not stated | |
| CT | Certified Clinical Supervisor | Reciprocal Certified Addiction Counselor or Certified Co-Occurring Disorders Professional for at least 1 year | 30 | 10,000 | Not stated | IC&RC CS Exam | 3 | 12 | Yes |
| DC | Certified Clinical Supervisor | Not stated | Not stated | Not stated | Not stated | IC&RC CS Exam | Not stated | Not stated | Not stated |
| DE | Certified Clinical Supervisor | IC&RC reciprocal Certified Alcohol & Drug Counselor, Certified Advanced Alcohol & Drug Counselor, Certified Co-Occurring Disorders Professional, Certified Co-Occurring Disorders Professional-Diplomate or master's in behavioral science field | 30 | 10,000 | 200 | IC&RC CS Exam | 6 | 24 | Yes |
| GA | Certified Clinical Supervisor | Bachelor's | 30 | 10,000 | 300 | IC&RC CS Exam | 40 | 24 | Yes |
| HI | Certified Clinical Supervisor | IC&RC reciprocal CSAC, Certified Criminal Justice Addictions Professional, or Certified Co-Occurring Disorders Professional-Diplomate or SUD credential in another field at master's level | 30 | 10,000 | 200 | IC&RC CS Exam | 40 | 24 | Yes |
| IA | Certified Clinical Supervisor | IC&RC AADC, Certified Criminal Justice Addictions Professional, Co-Occurring Disorders Professional, Co-Occurring Disorders Professional-Diplomate or SUD credential in another field at master's level | 36 | 10,000 | 200 | IC&RC CS Exam | 6 | 24 | Yes |
| ID | Certified Clinical Supervisor | IC&RC reciprocal Certified Alcohol & Drug Counselor or Advanced Certified Alcohol & Drug Counselor or SUD credential in another field at master's level | 30 | 10,000 | 200 | IC&RC CS Exam | 15 | 24 | Yes |
| IL | Certified Supervisor Alcohol & Other Drug Counselor | Certified Reciprocal Alcohol & Other Drug Abuse Counselor credential | 350 | 10,000 | 300 | IC&RC ADC & CS Exam | 40 | 24 | Yes |
| IN | Certified Clinical Supervisor | IC&RC CADAC II or IV, Certified Criminal Justice Addictions Professional, Co-Occurring Disorders Professional or Co-Occurring Disorders Professional-Diplomate or SUD credential in another field at master's level | 30 | 10,000 | 200 | IC&RC CS Exam | 40 | 24 | Yes |
| LA | Certified Clinical Supervisor | LAC, Certified Addiction Counselor, Registered Addiction Counselor or other qualified MH professional credential | 90 | 10,000 | Not stated | IC&RC CS Exam | 48 | 24 | Not stated |
| MA | Certified Clinical Supervisor | Bachelor's & Certified Alcohol & Drug Counselor or Certified Alcohol & Drug Counselor II for at least 2 years | 30 | 10,000 | 200 | IC&RC CS Exam | 6 | 24 | Yes |
| MD | Certified Clinical Supervisor | Certified Chemical Dependency Counselor, Certified Criminal Justice Addictions Professional, or Co-Occurring Disorders Professional or SUD cred. in another field at master's level | 30 | 10,000 | 200 | IC&RC CS Exam | 6 | 24 | Yes |
| ME | Certified Clinical Supervisor | Must hold LADC credential | 30 | 4,000 | Not stated | IC&RC CS Exam | 12 hours every 2 years | 12 | Not stated |
| MI | Certified Clinical Supervisor | IC&RC reciprocal credential | 30 | 10,000 | 200 | IC&RC CS Exam | 6 | 24 | Yes |
| MN | Certified Clinical Supervisor Reciprocal | Alcohol & Drug Counselor Reciprocal, Certified Criminal Justice Addictions Professional Reciprocal, Co-Occurring Disorders Professional, Co-Occurring Disorders Professional-Diplomate or SUD credential in another field at master's level | 30 | 10,000 | 200 | IC&RC CS Exam | 6 | 24 | Yes |
| Licensed Alcohol & Drug Counselor Supervisor | LADC or other qualified professional as determined by the Board | 12 | 6,000 | Not stated | Not stated | 40 | 24 | Not stated | |
| MS | Certified Clinical Supervisor | Certified Alcohol & Drug Counselor, Certified Alcohol & Drug Counselor I, Certified Alcohol & Drug Counselor II or Certified Advanced Alcohol & Drug Counselor credential | 30 | Not stated | 200 | IC&RC CS Exam | 6 | 24 | Yes |
| NC | Certified Clinical Supervisor | Master's degree & Licensed Clinical Addiction Specialist | 30 | 4,000 | Not stated | IC&RC CS Exam | 15 | 24 | Yes |
| ND | Registered Clinical Supervisor | LAC credential | 20 | 6,000 | Not stated | Not stated | 8 | 24 | No |
| NH | Licensed Clinical Supervisor | MLADC or LADC credential | 30 | 10,000 | 200 | IC&RC CS Exam | 6 | 24 | Yes |
| NJ | Certified Clinical Supervisor | Licensed Clinical Alcohol & Drug Counselor, Certified Alcohol & Drug Counselor, or master's in related counseling field | 60 hours if not Licensed Clinical Alcohol & Drug Counselor or Certified Alcohol & Drug Counselor | 10,000 | Not stated | IC&RC CS Exam | 30 | 24 | Yes |
| NM | Certified Clinical Supervisor | IC&RC reciprocal Certified Alcohol & Drug Counselor/ADC or AADC or SUD credential in another field at master's level | 30 | 10,000 | 200 | IC&RC CS Exam | 6 | 24 | Yes |
| OH | Licensed Independent Chemical Dependency Counselor-Clinical Supervisor | Master's | 470 | 4,000 | 400 | IC&RC ADC & CS Exam | 40 | 24 | Yes |
| PA | Certified Clinical Supervisor | IC&RC reciprocal CAAC, Certified Alcohol & Drug Counselor, Certified Advanced Alcohol & Drug Counselor, Co-Occurring Disorders Professional, Co-Occurring Disorders Professional-Diplomate, Certified Criminal Justice Addictions Professional or master's in behavioral science | 30 | 10,000 | 200 | IC&RC CS Exam | 6 | 24 | Yes |
| RI | Certified Clinical Supervisor | IC&RC reciprocal CAAC, Certified Alcohol & Drug Counselor, Certified Advanced Alcohol & Drug Counselor, Co-Occurring Disorders Professional, Co-Occurring Disorders Professional-Diplomate, Certified Criminal Justice Addictions Professional or SUD cred. in other field at master's level | 30 | 10,000 | 200 | IC&RC CS Exam | 6 | 24 | Yes |
| SC | Certified Clinical Supervisor | Bachelor's & Certified Addiction Counselor II | 250 | 10,000 | Not stated | Oral exam | 40 | 24 | Yes |
| TN | Certified Qualified Clinical Supervisor | Licensed Alcoholism & Drug Abuse Counselor II for at least 5 years | 30 | 4,000 | 36 | Not stated | 10 | 14 | Not stated |
| TX | Certified Clinical Supervisor | IC&RC ADC, AADC, or Certified Criminal Justice Addictions Professional | 30 | 10,000 | 200 | IC&RC CS Exam | 40 | 24 | Yes |
| UT | Certified Clinical Supervisor | IC&RC reciprocal ADC, AADC, Certified Criminal Justice Addictions Professional, Co-Occurring Disorders Professional, Co-Occurring Disorders Professional-Diplomate or SUD credential in another field at master's level | 30 | 10,000 | 200 | IC&RC CS Exam | 6 | 24 | Yes |
| VA | Certified Clinical Supervisor | Master's or IC&RC Certified Alcohol & Drug Counselor, Certified Advanced Alcohol & Drug Counselor, Co-Occurring Disorders Professional, or Certified Criminal Justice Addictions Professional | 30 | 10,000 | 200 | IC&RC CS Exam | 6 | 24 | Yes |
| WI | Independent Clinical Supervisor | CSAC, Professional Counselor, Marriage & Family Therapist, or LCSW at master's level | 30 | 2,000 | Not stated | NAADAC NCSE Exam | 6 | 24 | Yes |
| WV | Clinical Supervisor | IC&RC reciprocal ADC, AADC, Certified Criminal Justice Addictions Professional | 30 | 10,000 | 200 | IC&RC CS Exam | 40 | 24 | Yes |
*EXAM NAME ABBREVIATIONS:
|
|||||||||
EXHIBIT A8: Requirements: Peer Recovery Specialist
| EXHIBIT A8. Requirements: Peer Recovery Specialist | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| State Abbr. | Credential Title | Focus* | Education Hours | Practice Hours | Supervision Hours | Required Examination | Annual Cont. Educ. Hours | Renewal Period (months) | Reciprocity |
| AL | Certified Recovery Support Specialist | SUD-specific | 40 | Not stated | Not stated | Certified Recovery Support Specialist Exam | 16 | 12 | Not stated |
| AR | Peer Recovery Coach | SUD-specific | 46 | 500 | 25 | IC&RC Peer Recovery Exam | 20 | 24 | Yes |
| AZ | Certified Peer Recovery Specialist | SUD-specific | Not stated | Not stated | Not stated | Certified Recovery Support Specialist Exam | Not stated | Not stated | Yes |
| CA | Certified Peer Recovery Specialist | SUD-specific | 100 | 500 | 25 | IC&RC Peer Recovery Exam | 20 | 24 | Yes |
| CO | Colorado Peer & Family Specialist | SUD-specific | 60 | 500 | 25 | IC&RC Peer Recovery Exam | 30 | 24 | Yes |
| CT | Certified Peer Recovery Specialist | SUD-specific | 50 | 500 | 25 | IC&RC Peer Recovery Exam | 10 | 12 | Yes |
| DC | Certified Peer Specialist | MH and/or SUD | 6-week course | 80 | Not stated | Not stated | Not stated | Not stated | Yes |
| DE | Certified Peer Recovery Specialist | SUD-specific | 46 | 1,000 | 25 | IC&RC Peer Recovery Exam | 20 | 24 | Not stated |
| FL | Certified Recovery Peer Specialist | MH and/or SUD | 40 | 500 | 500 | Florida Certified Recovery Peer Specialist Exam | 10 | 12 | Yes |
| GA | Certified Peer Recovery Coach | MH and/or SUD | 100 | 500 | 50 | Not stated | 40 | 24 | Yes |
| HI | Hawaii Certified Peer Specialist | MH or COD | Not stated | Not stated | Not stated | Not stated | 16 | 12 | Not stated |
| IA | Certified Peer Recovery Specialist | MH and/or SUD | 46 | 500 | 25 | IC&RC Peer Recovery Exam | 20 | 24 | Yes |
| ID | Certified Peer Recovery Coach | SUD-specific | 46 | 500 | 25 | Not stated | 20 | 24 | Yes |
| IL | Certified Peer Recovery Specialist | SUD-specific | 100 | 2,000 | 100 | IC&RC Peer Recovery Exam | 30 | 24 | Yes |
| IN | Certified Addiction Peer Recovery Coach I | SUD-specific | 30 | None | Not stated | IC&RC Peer Recovery Exam | 40 | 24 | Yes |
| Certified Addiction Peer Recovery Coach II | SUD-specific | 46 | 500 | 25 | IC&RC Peer Recovery Exam | 40 | 24 | Yes | |
| KY | Registered Alcohol & Drug Peer Support Specialist | SUD-specific | 60 | 500 | 25 | IC&RC Peer Recovery Exam | Not stated | 36 | Yes |
| LA | Peer Recovery Support Specialist | SUD-specific | 46 | 500 | 25 | IC&RC Peer Recovery Exam | 20 | 24 | Yes |
| MA | Certified Addictions Recovery Coach | SUD-specific | 60 | 500 | 35 | IC&RC Certified Addictions Recovery Coach Exam | 30 | 24 | Yes |
| MD | Certified Peer Recovery Specialist | SUD-specific | 46 | 500 | 25 | IC&RC Peer Recovery Exam | 20 | 24 | Yes |
| MI | Certified Peer Recovery Mentor | SUD-specific | 46 | 500 | 25 | IC&RC Peer Recovery Exam | 20 | 24 | Yes |
| MN | Certified Peer Recovery Specialist | SUD-specific | 40 | None | 1 per every 20 hours of service provision | IC&RC Peer Recovery Exam | 20 | 24 | No |
| Certified Peer Recovery Specialist Reciprocal | SUD-specific | 46 | 500 | 25 | IC&RC Peer Recovery Exam | 20 | 24 | Yes | |
| MO | Certified Reciprocal Peer Recovery | SUD-specific | 46 | 500 | 25 | IC&RC Peer Recovery Exam | 20 | 24 | Yes |
| MS | Certified Peer Support Specialist Professional | MH and/or SUD | Not stated | 250 | Not stated | Peer Support Specialist Professional Exam | 20 | 48 | Not stated |
| MT | Behavioral Health Peer Support Specialist | MH and/or SUD | 40 | Not stated | Not stated | Not stated | 20 | 12 | Yes |
| NC | Peer Support Specialist | MH and/or SUD | 60 | Not stated | Not stated | None | 20 | 24 | Not stated |
| NE | Peer Support & Wellness Specialist | MH and/or SUD | 40 | Not stated | Not stated | Not stated | 6 | 12 | Not stated |
| NH | Certified Recovery Support Worker | SUD-specific | 46 | 500 | 25 | IC&RC Peer Recovery Exam | 12 | 24 | Not stated |
| NJ | Certified Peer Recovery Specialist | SUD-specific | 46 | 500 | 25 | IC&RC Peer Recovery Exam | 20 | 24 | Yes |
| NM | Certified Peer Support Worker | MH and/or SUD | 40 | Not stated | Not stated | Certified Peer Support Worker Exam | 40 | 24 | No |
| NV | Peer Recovery & Support Specialist | SUD-specific | 46 | 500 | 25 | IC&RC Peer Recovery Exam | 20 | 24 | Yes |
| NY | Certified Addiction Recovery Coach | SUD-specific | 60 | None | None | None | 6 | 36 | Yes |
| Certified Recovery Peer Advocate | SUD-specific | 46 | 500 | 25 | IC&RC Peer Recovery Exam | 8 | 36 | Yes | |
| OH | Ohio Certified Peer Recovery Supporter | MH and/or SUD | 56 | None | Not stated | Ohio Peer Recovery Supporter Exam | 30 | 24 | No |
| OK | Certified Peer Recovery Support Specialist | MH and/or SUD | Not stated | Not stated | Not stated | Peer Recovery Support Specialist Exam | 12 | 12 | Not stated |
| OR | Certified Addiction Peer Recovery Counselor | SUD-specific | 80 | 500 | 25 | IC&RC Peer Recovery Exam | 20 | 24 | Yes |
| PA | Certified Recovery Specialist | SUD-specific | 54 | Not stated | Not stated | IC&RC Peer Recovery Exam | 30 | 24 | Yes |
| RI | Certified Peer Recovery Specialist | SUD-specific | 46 | 500 | 25 | IC&RC Peer Recovery Exam | 20 | 24 | Yes |
| TN | Certified Peer Recovery Specialist | MH and/or SUD | 40 | 75 | 3 | None | 10 | 12 | No |
| TX | Peer Recovery Support Specialist | SUD-specific | 46 | 500 | 25 | IC&RC Peer Recovery Exam | 20 | 24 | Yes |
| UT | Certified Peer Support Specialist | MH and/or SUD | 40 | Not stated | Not stated | Not stated | 20 | 24 | No |
| VA | Certified Peer Recovery Specialist | SUD-specific | 72 | 500 | 25 | IC&RC Peer Recovery Exam | 20 | 24 | Yes |
| VT | Vermont Certified Recovery Coach | SUD-specific | Not stated | Not stated | Not stated | None | 8 | 60 | No |
| WA | Certified Peer Counselor | MH and/or SUD | 40 | Not stated | Not stated | State Certified Peer Counselor Exam | Not stated | Not stated | No |
| WI | Certified Peer Specialist | MH and/or SUD | Not stated | Not stated | Not stated | Wisconsin Peer Specialist Certification Exam | 20 | 24 | No |
| WV | Peer Recovery Support Specialist | SUD-specific | 46 | 500 | 25 | IC&RC Peer Recovery Exam | 20 | 24 | Yes |
| WY | Certified Peer Specialist | MH and/or SUD | 36 | Not stated | Not stated | None | 19 | 24 | No |
*FOCUS REFERS TO THE FOLLOWING CATEGORIES:
|
|||||||||
EXHIBIT A9: Requirements: Prevention Specialist
| EXHIBIT A9. Requirements: Prevention Specialist | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| State Abbr. | Credential Title | Minimum Degree | Education Hours | Practice Hours | Supervision Hours | Required Examination | Annual Cont. Educ. Hours | Renewal Period (months) | Reciprocity |
| AL | Certified Prevention Manager | Bachelor's | 100 | 4,000 | 3 years managerial experience | IC&RC Prevention Specialist Exam | Not stated | Not stated | Yes |
| Certified Prevention Specialist | Bachelor's | 100 | 4,000 | Not stated | IC&RC Prevention Specialist Exam | Not stated | Not stated | Yes | |
| Associate Prevention Specialist | High school or equivalent | 75 | 2,000 | Not stated | Not stated | Not stated | Not stated | No | |
| AR | Certified Prevention Specialist | Not stated | 100 | Not stated | Not stated | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| Associate Preventionist | Not stated | Not stated | Not stated | None | None | 24 | 24 | Not stated | |
| AZ | Certified Prevention Specialist | Not stated | Not stated | Not stated | Not stated | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| CA | California Certified Prevention Specialist | Not stated | 120 | 2,000 | None | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| CO | Colorado Certified Prevention Specialist | Not stated | 120 | 2,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| CT | Certified Prevention Specialist | Not stated | 100 | 2,000 | 120 | IC&RC Prevention Specialist Exam | 20 | 12 | Yes |
| DC | Certified Prevention Specialist or Professional | Not stated | Not stated | Not stated | Not stated | IC&RC Prevention Specialist Exam | Not stated | Not stated | Not stated |
| DE | Certified Prevention Specialist | Bachelor's | 120 | 2,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| FL | Certified Prevention Professional | Bachelor's | 250 | 6,000 | 200 | IC&RC Prevention Specialist Exam | 20 | 12 | Yes |
| Certified Prevention Specialist | High school or equivalent | 120 | 2,000 | 120 | IC&RC Prevention Specialist Exam | 20 | 12 | Yes | |
| GA | Criteria Internationally Certified Prevention Specialist | Bachelor's | 150 | 4,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| HI | Certified Prevention Specialist | High school or equivalent | 120 | 2,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| IA | Advanced Certified Prevention Specialist | Bachelor's | 144 | 6,000 | Not stated | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| Certified Prevention Specialist | High school or equivalent | 168 | 2,000 | Not stated | IC&RC Prevention Specialist Exam | 40 | 24 | Yes | |
| ID | Certified Prevention Specialist | High school or equivalent | 120 | 2,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| IL | Certified Senior Prevention Specialist | High school or equivalent | 150 | 8,000 | 240 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| Certified Prevention Specialist | High school or equivalent | 120 | 2,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes | |
| IN | Certified Prevention Specialist | Not stated | 100 | 2,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| KS | Certified Prevention Professional | Bachelor's | 150 | 3,500 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| Certified Prevention Technician | High school or equivalent | 60 | 2,000 | 120 | None | 40 | 24 | No | |
| KY | Certified Prevention Specialist | Bachelor's | 150 | 2,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| LA | Certified Prevention Professional | Bachelor's | 100 | 4,000 | 120 | IC&RC Prevention Specialist Exam | 48 | 24 | Not stated |
| Prevention Specialist in Training | High school or equivalent | Not stated | Not stated | Not stated | Not stated | 20 | 12 | Not stated | |
| Registered Prevention Professional | High school or equivalent | 100 | 6,000 | 120 | IC&RC Prevention Specialist Exam | 48 | 24 | Not stated | |
| Licensed Prevention Professional | Master's | 100 | 2,000 | 120 | IC&RC Prevention Specialist Exam | 48 | 24 | Not stated | |
| MA | Certified Prevention Specialist | High school or equivalent | 200 | 2,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| MD | Certified Prevention Professional | Bachelor's | 200 | 4,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Not stated |
| Certified Prevention Specialist | High school or equivalent | 120 | 6,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Not stated | |
| Associate Prevention Specialist | High school or equivalent | 50 | 2,000 | 60 | None | 20 | 24 | Not stated | |
| ME | Certified Prevention Specialist | Not stated | 120 | 2,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| MI | Certified Prevention Consultant | Not stated | 240 | 8,000 | 240 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| Certified Prevention Specialist | Not stated | 120 | 2,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes | |
| MN | Certified Prevention Professional Advanced | High school or equivalent | 120 | 240 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | No |
| Certified Prevention Professional Reciprocal | High school or equivalent | 120 | 2,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes | |
| Certified Prevention Professional | High school or equivalent | Substance Abuse Prevention Skills Training course | None | None | None | 40 | 24 | No | |
| MO | Certified Reciprocal Prevention Specialist | High school or equivalent | 120 | 4,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| Missouri Advanced Prevention Specialist | High school or equivalent | Not stated | 10,000 | Not stated | None | 40 | 24 | Not stated | |
| Missouri Prevention Specialist | High school or equivalent | Not stated, includes 3 hours of ethics training | Not stated | Not stated | None | 5 | 24 | Not stated | |
| MS | Certified Prevention Specialist | Bachelor's | 150 | 4,000 | 120 | Not stated | 40 | 24 | Yes |
| Certified Prevention Specialist Manager | Bachelor's | 150 | 10,000 | 120 | Not stated | 40 | 24 | Yes | |
| Associate Prevention Specialist | Not stated | 75 | 2,000 | 120 | Not stated | 20 | 24 | Not stated | |
| NC | Certified Substance Abuse Prevention Consultant | High school or equivalent | 270 | 6,000 | 300 | IC&RC Prevention Specialist Exam | 60 | 24 | Yes |
| NH | Certified Prevention Specialist | Not stated | 240 | 4,000 | 240 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| NJ | Certified Prevention Specialist | Bachelor's | 120 | 4,000 | 120 | IC&RC Prevention Specialist Exam | 50 | 24 | Yes |
| Certified Associate Prevention Specialist | Not stated | Not stated | 2,000 | 200 | Not stated | 40 | 24 | Not stated | |
| NM | Senior Certified Prevention Specialist | Not stated. Must hold CPS credential at IC&RC reciprocal level | 120 | 10,000 | 144 | No further exam beyond IC&RC Prevention Specialist Exam needed to obtain CPS credential (see row below). | 40 | 24 | Yes |
| Certified Prevention Specialist | Not stated | 120 | 2,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes | |
| Certified Prevention Intern | High school or equivalent | 50 | 1,000 | 60 | None | 40 | 24 | No | |
| NV | Certified Prevention Specialist | High school or equivalent | 120 | 2,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| NY | Certified Prevention Professional, Credentialed Prevention Professional | Bachelor's | 250 | 4,000 | 12 | IC&RC Prevention Specialist Exam | 60 | 36 | Yes |
| Certified Prevention Specialist, Credentialed Prevention Specialist | High school or equivalent | 120 | 2,000 | 120 | IC&RC Prevention Specialist Exam | 60 | 36 | Yes | |
| OH | Ohio Certified Prevention Consultant | Bachelor's | 120 | 6,000 | Not stated | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| Ohio Certified Prevention Specialist | Associate's | 120 | 2,000 | Not stated | IC&RC Prevention Specialist Exam | 40 | 24 | Yes | |
| Ohio Certified Prevention Specialist Assistant | High school or equivalent | 45 | 100 | Not stated | None | 20 | 24 | No | |
| OK | Certified Prevention Specialist | Associate's | 256 | 2,000 | 120 | IC&RC Prevention Specialist Exam | 20 | 12 | Yes |
| Associate Prevention Specialist | Associate's | 256 | 2,000 | 120 | None | 20 | 12 | Not stated | |
| OR | Certified Prevention Specialist | Not stated | 150 | 2,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Not stated |
| PA | Certified Prevention Specialist | Bachelor's | 120 | 4,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| RI | Advanced Certified Prevention Specialist | Bachelor's | 270 | 6,000 | 170 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| Certified Prevention Specialist | High school or equivalent | 175 | 2,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes | |
| Associate Prevention Specialist | High school or equivalent | 48 | 200 | Not stated | None; must upgrade to CPS within 2 years | None | N/A | No | |
| SC | Certified Senior Prevention Specialist | High school or equivalent | 300 | 10,000 | 200 | IC&RC Prevention Specialist Exam | 50 | 24 | Yes |
| Certified Prevention Specialist | High school or equivalent | 150 | 2,000 | 750 | IC&RC Prevention Specialist Exam & an oral interview by the Certification Peer Review Committee | 50 | 24 | Yes | |
| SD | Certified Prevention Specialist | Bachelor's | 15 semester hours | 2,000 | 750 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| Prevention Specialist Trainee | Bachelor's | Not stated | Not stated | 8 hours per month | None | None; Trainee recognition is granted for up to 5 years | N/A | Not stated | |
| TN | Certified Prevention Specialist II | Bachelor's | 220 | 4,000 | 240 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| Certified Prevention Specialist I | High school or equivalent | 120 | 2,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes | |
| TX | Certified Prevention Specialist | Not stated | 120 | 2,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Not stated |
| Advanced Certified Prevention Specialist | Associate's | 200 | 10,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes | |
| Associate Prevention Specialist | High school or equivalent | 120 | 3,000 | 120 | None | 40 | 24 | Not stated | |
| UT | Certified Prevention Specialist | Not stated | 120 | 2,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| VA | Certified Prevention Specialist | Bachelor's | 120 | 4,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| Associate Prevention Specialist | High school or equivalent | 100 | 4,000 | 200 | None | 40 | 24 | No | |
| WA | Certified Prevention Professional | High school or equivalent | 120 | 2,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| Associate Prevention Professional | Not stated | 70 | 500 | Not stated | None | None, can be renewed once | 24 | No | |
| WI | Certified Prevention Specialist | Not stated | 120 | Not stated | Not stated | Online Open-Book Examination on the Wisconsin Statutes & Administrative Code | 40 | 24 | Yes |
| Certified Prevention Specialist In Training | Not stated | 40 | Not stated | Not stated | None | 25 | 24 | No | |
| WV | Certified Prevention Specialist II | Bachelor's | 270 | 12,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| Certified Prevention Specialist I | Not stated | 180 | 8,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes | |
| WY | Certified Prevention Specialist | Not stated | 150 | 8,000 | 120 | IC&RC Prevention Specialist Exam | 40 | 24 | Yes |
| NOTE: CPS = Certified Prevention Specialist | |||||||||
APPENDIX B: Reimbursement Detailed Table
| EXHIBIT B1. Exact and Alternative Reimbursement Codes by State | ||||||||
|---|---|---|---|---|---|---|---|---|
| H0001 | H0049 | H0050 | H0004 | H0038 | H0006 | H0007 | H0015 | |
| Alabama | 90791-HF | NF | NF | 90832 | Yes | Yes | H2011 | NF |
| Alaska | Yes | T1023 | 99408 | 90832 | Yes | T1016 | H2011 | NF |
| Arizona | Yes | H0002 | NF | Yes | Yes | T1016 | H2011 | Yes |
| Arkansas | Yes | NF | NF | 90832 | Yes | NF | H2011 | Yes |
| California* | Yes | Yes | NF | Yes | Yes | Yes | H2011 | NF |
| Colorado | Yes | S9445 | NF | Yes | Yes | Yes | NF | NF |
| Connecticut | 96127 | NF | NF | 90832 | NF | T1016 | S9484 | Yes |
| Delaware | Yes | NF | NF | Yes | Yes | NF | H2011 | Yes |
| D.C. | Yes | H0002 | 99408 | Yes | Yes | Yes | Yes | Yes |
| Florida | Yes | T1023 | NF | H2010 | NF | T1017 | NF | NF |
| Georgia | H0031 | NF | NF | 90832 | Yes | T1016 | H2011 | Yes |
| Hawaii | NF | NF | NF | NF | NF | NF | NF | NF |
| Idaho | 90791 | 99408 | 99408 | 90832 | NF | NF | 90839 | NF |
| Illinois | H2000 | NF | NF | Yes | NF | T1016 | H2011 | NF |
| Indiana | NF | NF | 99408 | Yes | Yes | NF | NF | Yes |
| Iowa | 90791 | Yes | 99408 | Yes | Yes | T1016 | Yes | Yes |
| Kansas | Yes | Yes | Yes | Yes | Yes | Yes | NF | Yes |
| Kentucky | Yes | H0002 | 99408 | 90832 | Yes | T2023 | H2011 | Yes |
| Louisiana | Yes | Yes | Yes | Yes | NF | NF | H2011 | Yes |
| Maine | NF | NF | NF | NF | NF | NF | NF | NF |
| Maryland | Yes | NF | NF | Yes | NF | NF | NF | Yes |
| Massachusetts | Yes | NF | NF | Yes | Yes | Yes | NF | H2012-HF |
| Michigan | Yes | NF | NF | Yes | Yes | H2035 | H2011-HF | Yes |
| Minnesota | Yes | NF | NF | NF | Yes | T1016 | NF | NF |
| Mississippi | NF | NF | NF | NF | Yes | NF | NF | NF |
| Missouri | Yes | NF | NF | Yes | NF | NF | NF | NF |
| Montana | Yes | NF | 99408 | Yes | NF | T1016 | NF | H0012 |
| Nebraska | Yes | NF | NF | 90832 | Yes | 90887 | 90839 | 90843 |
| Nevada | 96127 | Yes | NF | 90832 | Yes | T1016 | H2011 | S9480 |
| New Hampshire | Yes | Yes | 99408 | Yes | Yes | Yes | Yes | Yes |
| New Jersey | Yes | Yes | NF | Yes | H0036 | Yes | Yes | Yes |
| New Mexico | Yes | NF | NF | 90832 | Yes | NF | H2011 | Yes |
| New York | Yes | Yes | Yes | Yes | Yes | NF | NF | S9480 |
| North Carolina | 90791 | NF | NF | 90832 | NF | H0032 | H2011 | Yes |
| North Dakota | NF | NF | NF | 90832 | NF | NF | NF | NF |
| Ohio | 90791 | NF | G0396 | 90832 | Yes | Yes | 90839 | Yes |
| Oklahoma | Yes | H0002 | NF | Yes | H2015 | T1017 | H2011 | NF |
| Oregon | Yes | H0002 | NF | Yes | Yes | Yes | NF | Yes |
| Pennsylvania | NF | NF | NF | Yes | Yes | NF | NF | NF |
| Rhode Island | Yes | NF | NF | Yes | Yes | NF | H2011 | NF |
| South Carolina | 90791 | H0002 | NF | 90832 | Yes | NF | H2011 | NF |
| South Dakota | Yes | NF | NF | Yes | NF | NF | H2011 | Yes |
| Tennessee | NF | NF | NF | NF | NF | NF | NF | NF |
| Texas | Yes | Yes | 99408 | Yes | NF | T1017 | H2011 | H0004, H0005 |
| Utah | H0031 | NF | NF | H2019 | Yes | NF | 90839 | NF |
| Vermont | Yes | NF | NF | Yes | NF | Yes | Yes | Yes |
| Virginia | 90791 | NF | 99408 | 90832 | T1012 | Yes | H0036 | Yes |
| Washington | Yes | NF | NF | Yes | NF | T1017 | NF | NF |
| West Virginia | H0031 | T1023 | 90791, 90792, H0031 | Yes | Yes | T1017 | H2011 | H0004 |
| Wisconsin | 90791 | NF | H0022 | H0022 | Yes | T1017 | S9484 | H2012-HF |
| Wyoming | H0031 | NF | NF | H2019 | Yes | G9012 | T1017 | NF |
| *Data for California are from the Los Angeles Organized Delivery System (ODS) and do not represent the entire state. BILLING CODE DESCRIPTIONS:
|
||||||||
APPENDIX C: Sources Consulted for the Environmental Scan
In addition to database searches, the following journals were scanned for relevant articles published during the past 10 years:
-
Addiction
-
Administration and Policy in Mental Health and Mental Health Services Research
-
Advances in Alcohol and Substance Abuse
-
American Journal of Community Psychology
-
American Journal of Drug and Alcohol Abuse
-
American Journal of Psychiatry
-
Drug and Alcohol Review
-
Health Affairs
-
Health Services Research
-
Journal of Addiction
-
Journal of Addiction Nursing
-
Journal of Addiction Research and Therapy
-
Journal of Behavioral Health Services and Research
-
Journal of Drug Abuse
-
Journal of Studies on Alcohol and Drugs
-
Journal of Substance Abuse Treatment
-
Psychiatric Services
-
Substance Abuse Treatment, Prevention, and Policy
Reports, policy briefs, white papers, and guidelines published by the following agencies and organizations were scanned:
-
Agency for Healthcare Research and Quality
-
Alliance for Health Policy
-
Alliance of Community Health Plans
-
Altarum Institute
-
America's Health Insurance Plans
-
American College of Healthcare Executives
-
American Health Information Management Association
-
American Health Lawyers Association
-
American Hospital Association
-
Association for Behavioral Health and Wellness
-
Brookings Center for Health Policy
-
California Health Care Foundation
-
CATO Institute, Health Care and Welfare Division
-
Center for American Progress, Health Care Division
-
Commonwealth Foundation
-
Economic Policy Institute, Health Research Division
-
Health Access (CA)
-
Health Insurance Association of America
-
Healthcare Leadership Council
-
The Joint Commission
-
Kaiser Family Foundation
-
National Academies of Sciences, Health and Medicine Division
-
National Association for Alcoholism and Drug Abuse Counselors (NAADAC)
-
National Association for Children's Behavioral Health
-
National Association of Health Insurers
-
National Association of State Alcohol and Drug Abuse Directors (NASADAD)
-
National Center on Addiction and Substance Abuse at Columbia University
-
National Coalition on Healthcare
-
National Council for Behavioral Health
-
National Institute for Health Care Management
-
RAND Corporation, Health and Health Care Research
-
Robert Wood Johnson Foundation, Health Systems Research
-
Society of Insurance Research
-
Substance Abuse and Mental Health Services Administration (SAMHSA)
-
Trust for America's Health
-
UCLA Center for Health Policy Research
-
Urban Institute Health Policy Center
APPENDIX D: Detailed Methodology: Licensing/Credentialing Review
We reviewed states' licensing/credentialing board websites to identify requirements for every SUD counseling, SUD technician, peer recovery specialist, and SUD prevention specialist credential available within each state. At the time data were extracted, we classified each treatment credential either into one of the five categories defined in SAMHSA's model career ladder or the additional peer specialist category that is not included in that model. We based the classification primarily on the minimum degree required, but also considered how the state's career ladder is structured and where in that structure a title is situated, as well as whether independent practice without supervision is authorized under the credential. For example, if the highest available credential for SUD counselor in a state required only a bachelor's degree but authorized independent practice without supervision, we classified it in Category 4 even though SAMHSA's model ladder indicates a master's degree for this level. If authority for independent practice was not explicit in the information available on licensing/credentialing board websites, we reached out to the relevant board via email to clarify and used the information if it was provided. We also referred to a 2013 study[7] by the National Association of State Alcohol and Drug Abuse Directors (NASADAD) that similarly mapped SUD credentials to SAMHSA's career ladder; we used this study as a reference when making classification determinations, but our results are not identical.
The initial classification of counseling credentials was performed by a single analyst, then reviewed by a second analyst for agreement. Once data were compiled for all states, we again reviewed the classifications for comparability within categories and made some adjustments. It is important to note that we had SOPe information for only a limited set of credentials; therefore, our classifications are not definitive but instead were used as a guiding framework. In states with credentials overseen by multiple boards, classification was especially difficult as the career ladders within the state were often overlapping. The method therefore involved some degree of subjectivity, discussed in the Limitations section of this report.
We pulled clinical supervisor credentials (e.g., CCS) into a separate category because the requirements are typically overlays to the requirements for an underlying credential (e.g., Certified Addiction Counselor).
For peer recovery specialists, we included credentials focused on SUD, either alone or in conjunction with mental health. We did not include peer credentials if the description was limited to mental health with no mention of SUD. If a state had more than one peer specialist credential--for example, one specific to SUD recovery and another for mental health or co-occurring disorders--we selected the SUD-specific credential as the most relevant to the study's research questions.
Our search was conducted between April and June 2018. The data were compiled in an Excel spreadsheet. Due to space limitations, we could not fit all extracted data elements into the tables in this report. Elements not shown are: the name of the board that oversees the credential, the board type, URL to the website where data were obtained, and tasks allowable under the credential's SOP (only available for one credential per state from the University of Michigan's online tool[8]). The grid below shows the elements presented in this report along with a definition of each.
| Data Element | Definition | Where Displayed in This Report |
|---|---|---|
| State | State abbreviation. | Appendix A tables |
| Title | Credential title. | Appendix A tables |
| Affiliation | Whether the credential is affiliated with IC&RC, NAADAC, both, or neither. | Aggregated at the state-level, Exhibit 8 |
| Minimum Degree | Minimum degree required to obtain the credential. This field is not presented for peer recovery credentials as peer roles emphasize lived experience rather than educational achievement. | Appendix A tables |
| Education Hours | The required number of hours of education to obtain the credential, sometimes denoted in credit or semester hours. | Appendix A tables |
| Practice Hours | The number of required practice hours in the field to obtain the credential. | Appendix A tables |
| Exam Name | Name of the required examination, if any | Appendix A tables |
| Continuing Ed Hours | Number of hours of continuing education, per year (unless otherwise stated), required to maintain the credential. | Appendix A tables |
| Renewal Period | Period after which the credential is required to be renewed, in months. | Appendix A tables |
| Reciprocity | Yes/No whether a pathway for reciprocity was stated or confirmed via email by the board that oversees the credential. "Reciprocity" means the certification board would accept a similar credential from another state/jurisdiction if it meets certain requirements defined by the board. | Appendix A tables |
| Focus | For peer recovery credentials only, this field indicates whether the focus of the credential is: SUD-specific, mental health and/or SUD, or mental health and COD. | Exhibit A7 |
APPENDIX E: Detailed Methodology: Billing Eligibility and Reimbursement
Medicaid
The review of billing eligibility and reimbursement policies was conducted between July and October 2018. The main data source was state Medicaid FFS plans. The following search and data extraction methods were used in the review.
Search Domain and Strategy
The search domain was documentation of billing eligibility and reimbursement available online within the public domain. First, we identified each state's official Medicaid website. From there we looked for information for providers, following links with designations such as "For Providers" or "Provider Resources." Once there, we searched for three types of documentation:
-
Provider and/or billing manuals. An SUD-specific provider/billing manual would be the first resource to review if available. If an SUD-specific manual was not available, we reviewed manuals related to behavioral health. In the absence of behavioral health-related manuals, we searched general provider/billing manuals.
-
Fee schedules. If sufficient detail was not available from provider manuals, we searched SUD-specific or behavioral health-related fee schedules. In the absence of SUD-related or behavioral health-related fee schedules, we reviewed general fee schedules for the reimbursement codes selected for this study.
-
Provider enrollment resources. We searched these resources for relevant information on SUD practitioner eligibility to enroll in Medicaid as an independent provider type. If information was unavailable, we called the plan's "provider relations" line and used the information, if supplied. In some states, billing eligibility was inferred from information in the billing manuals.
Approach to Identifying Alternate Billing Codes
It was expected that different coding systems would be used across state plans. Although the review was guided by a set of eight HCPCS codes, we attempted to identify a comparable alternate code when one of those codes was not in use in a given state. For some codes, the closest alternative we selected is not an exact match, which is a limitation of this study. Below is our approach to identifying alternate codes.
| Original Code | Approach to Identifying Alternate Code |
|---|---|
| H0001 = Alcohol and/or drug assessment | In the absence of H0001 we looked for a code associated with assessment. If there was a choice between an assessment code that does not involve diagnostic evaluation and one that does, we chose the code without diagnostic evaluation to best align with H0001. However, if a diagnostic evaluation code was the only available replacement, we used it as an alternative (e.g., CPT code 90791). |
| H0049 = Alcohol and/or drug screening | We looked for codes associated with "screening" specifically. We did not use diagnostic evaluation codes in place of screening. |
| H0050 = Alcohol and/or drug services, brief intervention, per 15 minutes | We searched for any code associated with brief intervention (detail unspecified) or SBIRT specifically. |
| H0004 = Behavioral health counseling and therapy, per 15 minutes | We looked for individual counseling or psychotherapy codes. If the code description mentioned SUD specifically, we used it, if not, we used a general individual psychotherapy code, the most common of which was CPT code 90832--individual psychotherapy, per 30 minutes. We did not identify an equivalent CPT code for a 15-minute increment. |
| H0038 = Self-help/peer services, per 15 minutes | If H0038 was not used, we looked for any code related to peer services. |
| H0006 = Alcohol and/or drug services; case management | We looked for an alternate code containing a reference to case management in its description. |
| H0007 = Alcohol and/or drug services; crisis intervention | We looked for an alternate code containing a reference to crisis intervention in its description. |
| H0015 = Alcohol and/or drug services; intensive outpatient | In the absence of a code specifically designated for intensive outpatient services, we used a code for "day treatment," if available. |
Data were extracted into an Excel template for standardization and analysis.
Commercial Insurance
For commercial insurance, we used UnitedHealth/Optum's Provider Express portal[9] which lists the practitioner types eligible to enroll in Optum's network as "individually-contracted clinicians" in all 50 states and D.C. The data were compiled in July 2018. We searched for similar data on billing eligibility from other national commercial health insurers but did not find any information in the public domain.
APPENDIX F: Case Study Selection Methodology
| EXHIBIT F1. Characteristics of Case Study States in Relation to National Levels | ||||
|---|---|---|---|---|
| California | New York | Texas | North Carolina | |
| Unmet Need for SUD Treatment[1] | ↑ | ↔ | ↓ | ↓ |
| % Non-White[2] | ↑ | ↑ | ↓ | ↑ |
| % Urban[3] | ↑ | ↑ | ↑ | ↓ |
| % Under Poverty[4] | ↔ | ↔ | ↑ | ↑ |
| % No Health Coverage[4] | ↑ | ↓ | ↑ | ↑ |
| % Public Health Insurance Coverage[4] | ↑ | ↑ | ↓ | ↔ |
| Drug Overdose Deaths[5] | ↓ | ↓ | ↓ | ↔ |
| Medicaid SUD Restriction Level[6] | Low | Low | Medium | Medium |
| Medicaid Expansion[7] | Yes | Yes | No | No |
COMPARISON TO NATIONAL LEVELS:
|
||||
APPENDIX G: Case Studies
The following states are contained in this section:
California
California |
|---|
Agencies/Organizations Contacted
|
Background
California's SUD treatment services had developed over time as a siloed system of care, isolated from the rest of the health care system, with its own practice philosophy, regulatory structure, and funding streams.[10] Although the limited Medicaid coverage and reimbursement rates were regulated by the state, counties had the authority to organize their own service delivery systems. Throughout the past two decades, however, the state has been gradually integrating SUD treatment services with its health care system, and these activities accelerated in response to recent federal policy changes. The MHPAEA and the Affordable Care Act were key milestones in this integration process, followed by the approval of an amendment to the state's waiver authorized by Section 1115 of the Social Security Act. With the approval of this amendment in 2015, California became the first state to initiate a Section 1115 waiver demonstration specifically designed to transform its SUD service delivery system.
The state's Drug Medi-Cal Organized Delivery System (DMC-ODS) pilot program is the reform mechanism through which the waiver is being implemented.[11] DMC-ODS uses Medicaid funds to expand coverage for SUD services, structured around the American Society of Addiction Medicine (ASAM) criteria,[12] including a waiver of the restriction for treating SUD patients in institutions for mental diseases (the IMD exclusion). Participation in the DMC-ODS is voluntary for the state's 58 counties, in keeping with the relative autonomy that California counties have traditionally had in managing their publicly funded health systems. Counties that choose to opt-in are required to submit an implementation plan for approval by the state's Medicaid authority (Medi-Cal). As of June 2018, 40 counties had submitted plans, 11 had started implementing the DMC-ODS, and approximately 80% of the state's population resided in an "opt-in" county.
The DMC-ODS gives counties some flexibility to set reimbursement rates that align with county-specific cost of living parameters. Although the state will continue to set reimbursement rates, opt-in counties may propose higher or lower rates for all SUD services except those provided under the Narcotic Treatment Program that regulates medication assisted treatment. Counties are required to justify their proposed rates, if different from the statewide rates, and there is typically a negotiation process before state approval is obtained for implementing the rates with funding from the demonstration. This fiscal flexibility gives counties the ability to negotiate rates that align with county-specific cost of living parameters. Non-ODS counties continue to use reimbursement rates set by the state. Under the waiver, the DMC-ODS functions as the health plan for behavioral health for each of the opt-in counties and the counties operate as MCOs contracting with the state to create and maintain their own provider networks within the county. In sum, in addition to broadening the range of reimbursable SUD services and increasing reimbursement rates for existing services, DMC-ODS has enhanced counties' autonomy in the use of public funds for behavioral health services; this, in turn, has increased the variation in health systems across counties. Private health plans in opt-in counties are required to establish memoranda of understanding with the county and to abide by their county's DMC-ODS rules
Given the differences in DMC-ODS implementation across counties, this case study selected a single DMC-ODS county to investigate provider experiences under the waiver. We selected Los Angeles County because of its large population; with more than 10.2 million residents, LA County is the most populous in California and has almost three times the population of California's next largest county (San Diego, population 3.3 million).[13]
Barriers to Substance Use Disorder Workforce Development
California has historically experienced severe SUD provider shortages, especially in rural areas. According to the senior director of government affairs at the California Consortium of Addiction Programs and Professionals (CCAPP), the typical practitioner is over 40; and prior to the waiver, there were few incentives for entry into the field to replace retiring practitioners. The key barriers to developing this workforce were:
-
Lack of integration with the health care system.
-
Low salaries and insufficient reimbursement rates.
-
Low skill requirements.
-
Absence of a state-regulated licensure process for addiction counselors.
-
Lack of pathways to insurance reimbursement as an independent practitioner.
As mentioned in the previous section, the SUD field in California has been isolated from the rest of the health care system and developed within an altogether different landscape than the other counseling professions. This isolation had several implications for the workforce. First, SUD treatment professionals were paid considerably less than other health professionals. The range of services covered by public funds varied widely across the state, depending on each county's resources such as discretionary grants and county general funds. A related factor is that in several counties, the safety net for SUD treatment is reserved for the criminal justice-involved population and depended on the availability of funds from sources other than Medi-Cal.[14] This has been an impediment to system integration and to the development of a professional identity for SUD practitioners as health care professionals. For example, the Los Angeles county administrator pointed out:
"Our providers are more experienced interacting with courts, attorneys, the sheriff, and the Department of Child and Family Services than they would be with the primary care provider or with a dentist."
These factors constituted disincentives for new graduates with counseling degrees to specialize in addiction. The DMS-ODS Transformation brings the criminal justice-involved populations into the Medi-Cal safety net, thus weakening the link between SUD treatment and the criminal justice system
Related to the above factors, skill requirements for SUD practice have been, and continue to be substantially lower compared to other counseling services. The state has no prerequisites for practice in the field other than registering with one of the two state-accredited certification organizations, the California Association of DUI Treatment Programs (CADTP) that certifies Alcohol and Other Drug Abuse Counselors or the CCAPP that offers certification in three SUD counselor levels as well as two levels of SUD counseling license. None of these credentials, however, are required by the state for providing SUD services. There are no state-regulated training requirements for becoming a registrant, although the certification boards have reached a consensus decision to require a standard 9-hour orientation and ethics training for registration. Registrants have 5 years to work towards certification, during which time they are authorized by the state to provide counseling services. The CCAPP director we interviewed pointed out that most SUD practitioners use the 5 years as registrant to gain professional experience and work toward higher counseling credentials but given the low salaries of certified SUD counselors, most of them choose to pursue certification in a counseling field other than SUD. These factors combine to create an SUD workforce comprised mostly of registrants at the entry-level and higher-level counselors certified in non-SUD specialties at higher levels. It is worth noting here that the registrant position (Registered Alcohol and Drug Technician) comprises the lowest rung of the model career ladder for SUD professionals developed by SAMHSA.[15]
To get Medicaid reimbursement, practitioners need to work in certified provider organizations and there are very few commercial plans willing to reimburse independent SUD practitioners.
Our informant indicated that under the terms of the state's facility licensure, 30% of a provider organization's staff need to be certified counselors (not necessarily in the addiction field) with at least 155 hours of education. She pointed out that these are low education and staff certification standards. The certification boards in the state, through a consensus decision, now require 315 hours of education for certification as an addiction counselor. However, this has not increased the overall skill level of SUD practitioners by much: Given the low salaries for certified SUD counselors and the ability to work for 5 years as a registrant, early-career It practitioners do not have an incentive to SUD counseling over other, better paid, counseling credentials:
"Why would you use your education to study addiction treatment to become a certified addiction counselor who works for minimum wage when you can work for $75 per hour as a marriage and family therapist?... We are losing the best and the brightest--when they do get their master's degree they license with one of the licensing boards in CA and then leave the field because they can make more money elsewhere. It pays so poorly, and it [addiction counseling license] is not recognized by the state". Students are not choosing it and schools are not teaching to it because there is no license track at the end of the career ladder."
State licensure appears to be the key missing component in efforts to fully professionalize the SUD field and to incentivize professionals to qualify for SUD counseling credentials. Minimum skill requirements imposed by the state are likely to have a positive impact on salaries while at the same time defining and codifying a professional identity for practitioners in this field comparable to other counseling professions
Impact of System Transformation on Substance Use Disorder Professionals
The DMC-ODS currently being piloted is transforming the SUD landscape with implications for workforce development. The barriers discussed in the previous section are all addressed by the DMC-ODS to varying degrees.
System Integration and "Culture Change"
As mentioned previously, California's integration of SUD treatment services with mental and physical health predates the approval of the DMC-ODS waiver in 2015. Under the waiver, however, these efforts have gained additional institutional supports. One of the stated goals of the DMC-ODS is to facilitate coordination between SUD providers and the rest of the health care system. For example, one of the requirements for inclusion in the DMC-ODS is for the county to enter into a memorandum of understanding with all Medi-Cal managed care plans that enroll beneficiaries served by the DMC-ODS in the county, to establish, at a minimum, mutual referral protocols, coordinated case management, and medical information sharing. This requirement has helped move the state in the right direction in terms of integration: A survey of county administrators conducted before the implementation of the DMC-ODS and repeated 1 year after implementation found that the opt-in counties experienced increased communication across departments of their health care systems, whereas non-ODS counties reported no similar improvements. Notably, all of the opt-in counties reported improved communication between SUD and mental health services and 86% reported communication improvements between SUD and physical health services.[16]
These integration efforts are contributing to the "mainstreaming" of SUD treatment as part of the overall health care landscape;[17] this goes a long way toward strengthening the professional identity of practitioners as health care providers
Incentives for SUD Workforce Development
County systems participating in the waiver are required to comply with Medicaid Managed Care Regulations (42 CFR Part 438),[18] including requirements related to network adequacy and quality reporting. This, in conjunction with the expansion of covered services, has provided incentives for counties to develop the size and skill levels of their SUD workforce by increasing the number of provider organizations in their networks and by enhancing staff adequacy provisions in their provider contracts. In the long run, these developments are expected to benefit the SUD workforce. They do, however, pose some immediate challenges that are discussed in further detail in the section, "Remaining Challenges and Future Directions."
Increases in Reimbursement Rates
The ability of ODS counties to set their own reimbursement rates for SUD services is arguably the single most important workforce development facilitator. In addition to the ability to take local conditions into consideration in rate setting, the waiver gives counties the authority to establish rate parity between mental health and SUD services. While acknowledging this as a promising development in the long run, our informants stressed that SUD counselors will need qualifications comparable to mental health counselors in order to achieve comparable rates. That is, attracting qualified professionals into the SUD field is a prerequisite for this workforce to achieve full rate parity. We return to this point in the next section.
Development of a Peer Recovery Workforce
Peer recovery supports in non-ODS counties can only be billed through a certified facility; however, the state does not require peer recovery specialists to register with a certification board as a prerequisite for practice, and hence, they do not need to complete even the 9-hour training required by certification boards. In ODS counties, peers can bill as individuals for RSS (although not for other service modalities), and comparable to the mental health side, they can meet clients in the community, and in their home to provide wraparound supports. The DMC-ODS waiver includes a requirement to provide SUD peer supports as a component of recovery services funded through the waiver. Counties that choose to make use of this provision are required to submit an SUD Peer Support Training Plan[19] to the California Department of Health Care Services (DHCS) for approval. At a minimum, the training plan should address:
-
Development of a comprehensive, individualized client plan that includes specific goals.
-
Person-centered approaches that actively engage and empower clients and/or their designated proxies.
-
A formally defined supervision protocol for peer recovery support workers.
-
A well-defined process to ensure that peer support staff complete training and receive a county SUD Peer Support designation.
-
A methodology for assuring that SUD peer support staff obtain a basic set of competencies necessary to perform and document the peer support function.
-
A method to evaluate the peer's ability to support recovery from SUDs.
In other words, the county opt-in proposals that include reimbursement for peer services are required to also describe the county's proposed plan for training and qualifying peer specialists for approval by the DHCS, since there are currently no state-level training and qualification standards for these newly reimbursable services.
The DHCS provides training and technical assistance to counties in developing their peer-to-peer recovery workforce in line with the above criteria. Administrators of ODS counties often participate in these sessions to share their accomplishments and challenges in this area.[20]
In summary, the DMC-ODS waiver is promoting the development of core competencies, well-defined training programs, formal supervision protocols, and performance evaluation methods for peer recovery support workers in the state.
Training and Technical Assistance on System Transformation
The DMC-ODS constitutes a fundamental transformation of California's service delivery system for SUD treatment, introducing new regulatory, administrative, contracting, billing, assessment, service delivery, and performance reporting practices that county administrations and their provider networks need to adopt. This necessitates a comprehensive training and technical assistance infrastructure to support providers and administrators alike. To meet these needs, the California DHCS has contracted with the California Institute for Behavioral Health Solutions (CIBHS) to provide training to counties and providers in planning for, applying, and implementing the waiver.[21]
The county training plan developed for this purpose[22] covers the following areas:
-
Assessing the existing service system and the infrastructure development needed to integrate additional service modalities required by the waiver.
-
ASAM Criteria:
-
General overview.
-
Utilization of the criteria for appropriate patient placement.
-
Utilization of the criteria to determine the appropriate treatment plan based on level of care.
-
-
Developing a provider network in line with the waiver's standard terms and conditions:
-
Drafting provider Requests for Proposals.
-
Developing provider selection criteria and contracting terms.
-
-
Drafting quality assurance plans.
-
Overview of MAT.
-
Detailed review of each level of care covered by the waiver:
-
Included services.
-
Appropriate interaction between providers in transitioning patients within the continuum.
-
In addition to the above training areas, the CIBHS provides an online forum and blog and a resource library for counties and providers. Since each participating county has a different waiver implementation plan, they offer county-specific learning collaboratives and other training resources for providers and enrollees.[23]
Remaining Challenges and Future Directions
Recruiting a qualified workforce to meet the terms and conditions of the DMC-ODS remains one of the leading challenges for counties. Although the waiver has contributed to redefining the SUD field as a professional health care specialty with its own core competencies and career ladder, this "culture change" is still in its early stages. Some counties that attempt to impose new training and practice hour requirements meet with resistance from their existing workforce. For example, when the Division of Substance Abuse Prevention and Control in Los Angeles County tried to impose 90 hours of specialized course work and 3 months of supervised practice in addition to the basic 9-hour orientation for SUD counselors as a requirement for joining the county's provider network, provider organizations found it difficult to recruit qualified staff and existing staff found the new requirements too burdensome. Our informant from the county described these tensions as follows:
"We are in kind of a back and forth with providers about whether or not it's desirable for the county to have requirements above and beyond those of the state. Per the state, you can bill for all of these services as a registered counselor [with a 9-hour training], but we're trying to add some additional quality controls to that and some of our providers feel that we shouldn't be doing that."
In Los Angeles County, these tensions have resulted in some provider organizations discontinuing their contracts and some practitioners leaving the county. Although the Deputy Director of California County Behavioral Health Directors Association informed us that this type of "provider walkout" is not an overarching issue across all opt-in counties, it is still an important lesson learned about one of the "growing pains" of system transformation.
The need for state-level legislation that defines the field and regulates licensing and certification for different levels of SUD practice was mentioned by all of our informants as an important gap in professionalizing the field and attracting qualified practitioners; informants added that this legislative effort needs to be accompanied by state-level workforce development efforts that provide training, education, and incentives to attract qualified new practitioners to replace retiring practitioners.
Assembly Bill 2804 introduced during the last legislative session included provisions that addressed these barriers. The bill included provisions that the DHCS:
-
Conduct a quality assessment of addiction treatment, prevention, and integrated workforces that includes a sunrise review[24] of addiction counselors.
-
Require that approved certifying organizations formalize a career ladder for addiction professionals that encompasses registrants through master's level counselors.
-
Adopt standards for peer specialists and intervention specialists so that those specialists can be included in regulations for certifying organizations.
The bill also included funding for SUD training and incentives such as fee waivers and student loan forgiveness. All of our informants mentioned this legislative effort as an important step forward. The Assembly decided to send AB 2804 to its Health Committee but failed to advance any further before the end of the session. SUD workforce advocates are continuing their efforts on several fronts. An SUD licensure bill is in preparation for submission to the legislature in January 2019. Additionally, CCAPP has submitted a budget request for 1.5 million dollars to be added to the state's Health Workforce Education and Training budget for some of the SUD workforce development efforts that were part of the moribund AB 2804. The request indicates that,
"[t]he funding would help the [SUD] profession in the following ways:
-
Educational stipends for students and registered SUD counselors seeking certification
-
Development of a statewide SUD workforce needs assessment report
-
Development of a quality assessment for addiction treatment, prevention, and integrated workforces that includes a sunrise review for addiction counselors
-
Development of a Medication Assisted Treatment (MAT) Training to educate the SUD workforce about patient-centered MAT treatment modalities
-
Development of an LGBTQI+ Treatment Quality Assessment tool and trainings to allow providers to assess the quality of treatment they are providing to the LGBTQI+ community and to identify goals for improvement"[25]
CCAPP has already initiated a sunrise review for addiction counselors.
State officials are currently working on the 2020 renewal of the waiver with the goal of further institutionalizing DMC-ODS and expanding coverage to ASAM levels 3.7 and 4.0, which are not covered under the current waiver. Informants indicated that lessons learned from the initial years are guiding this work, which they view as further cause for optimism
Concluding Remarks
As the nation's trailblazer in developing an organized SUD service delivery system, California offers many lessons learned--both through its accomplishments and the challenges encountered by some of its counties. One important lesson that can be derived from this experience is that the success of a comprehensive service system with quality controls and performance monitoring is highly dependent on the preexisting practice landscape and "culture," and relatedly, on the availability of a regulated and skilled professional workforce. Increasing the demand for a skilled workforce and establishing service quality requirements is likely to pose challenges and tensions if there are workforce shortages and few incentives to attract new entries into the field. Legislative efforts currently under way will go a long way toward responding to these challenges as the DMC-ODS demonstration expands and eventually becomes institutionalized statewide.
North Carolina
North Carolina |
|---|
Agencies/Organizations Contacted
|
Background
North Carolina's behavioral health system is in the middle of far-reaching reforms. In response to a 2015 legislative directive from the North Carolina General Assembly, the system is in the process of transitioning from a FFS structure to a managed care structure. The state is also working to expand Medicaid coverage and to integrate behavioral health and physical health services. A 2017 amendment to the state's pending 1115 waiver demonstration application also includes a proposal to cover the entire ASAM continuum of care for SUD and to provide residential treatment for SUDs in institutions of mental diseases (IMDs); at the time of writing, CMS approval for the amended waiver application and state legislation approving the proposed Medicaid expansion were still pending.
Currently, the behavioral health and intellectual/developmental disability services in the state are administered by local management entities (LMEs)/MCOs through a "closed network" system. Providers are required to contract with the local LME/MCO in order to be reimbursed; LMEs/MCOs may impose contracting criteria above and beyond the state's credentialing and licensing regulations. Out-of-network services can only be reimbursed under limited conditions and through regulated agreements.[26]
Current Barriers Facing Substance Use Disorder Professionals
Like much of the rest of the nation, North Carolina has long experienced an SUD workforce shortage, especially in rural counties; however, the shortage has become an increasingly urgent issue in light of the opioid crisis. Recent system reforms that were designed to increase access to high-quality SUD care for the entire population have created some short-term challenges for providers during the transition.
The biggest of these barriers are the revisions to licensing rules and SOPs necessitated by the waiver demonstration requirements. To establish full alignment with ASAM criteria, the state's entire array of SUD services is currently under revision. Until the revisions are fully institutionalized, providers aiming to enter the profession are forced to navigate a system in flux.
North Carolina's closed network system poses an additional barrier: Currently, there is no centralized source of information about the varying contracting criteria of the state's seven LMEs/MCOs. As a result, providers are forced to consult the LMEs/MCOs one by one to find the network that best fits their credentials and practice goals. (The relative recency of the closed network system is one reason for the difficulty of obtaining this information.)
Both of these barriers are associated with the uncertainty that accompanies any system transformation. What is most relevant to the present study are the measures under way to address these transition-related challenges by providing effective workforce supports. North Carolina's Behavioral Health Strategic Plan (2018)[27] incorporates several measures, some of them already in progress, to alleviate the challenges that SUD providers are encountering as a result of the changing practice and reimbursement environment. Before describing these measures, it is useful to consider several points of strength the state already possesses and can build on.
Current Facilitators Supporting the Substance Use Disorder Profession
Centralized Credentialing System
All credentialing functions for SUD professionals are housed under a single roof, the North Carolina Substance Abuse Professional Practice Board (NCSAPPB), with the sole exception of peer support specialists, whose credentialing is provided by the University of North Carolina. NCSAPPB was established in the mid-1980s, when the certification body for alcohol counselors merged with its counterpart for drug counselors. The merger process was not an easy one, as would be expected when two professional disciplines work to establish a new profession that encompasses the practice standards and ethical codes of both. Once established, however, the consolidated Board streamlined the credentialing process and became an important asset for professionals interested in an SUD practice. NCSAPPB is not administratively linked to the DHHS but reports directly to the legislature, the state auditor, and the governor's office. Although it works closely with the DHHS, its administrative autonomy provides it with a degree of flexibility in its day-to-day operations.
Move from a Title Act to a Practice Act
Until 2005, NCSAPPB operated under a title act only. This type of legislation mandates that only individuals qualifying for an SUD counseling license can legally use the associated title. However, any professional with a counseling license (e.g., a mental health counselor) can provide SUD counseling services so long as they do not use the SUD counselor title. Starting in 2005, SUD licenses have been regulated by a practice act which prohibits the provision of SUD services without an SUD license. According to the executive director of NCSAPPB, this legislative move was a game-changer that "transformed the SUD landscape" and contributed to the growth of the SUD workforce. It constituted legal acknowledgement of the need for specialized training to provide SUD services, thus contributing to the professionalization of the field. It is important to note that the addition of a credential requirement to practice could easily have become a workforce barrier if the state had multiple credentialing entities with varying criteria, as is the case in many states.
Peer Support Specialists
North Carolina is one of the first states to introduce a peer support specialist credential. The certificate program is offered by the University of North Carolina's social work program and consists of 30 hours of dedicated training. Peer support specialists can count their practice hours toward credential requirements for more advanced positions. This gives them an incentive to advance within the SUD career ladder. On the other hand, peer support services are currently not reimbursable except as part of a bundled service. They are funded through other resources such as CURES Act funds. As part of the system reforms, the legislature is considering expanding service definitions to include peer support services as a reimbursable clinical category.
Centralized Credential Information, Academic Programs, and Active Recruitment
Ten universities and multiple community colleges in the state offer SUD-specific undergraduate and/or graduate degree programs, in addition to accredited training programs such as summer schools or online training courses. The NCSAPPB is responsible for the accreditation of all SUD-specific training programs in the state, facilitating the alignment of available training opportunities with credentialing criteria. One out-of-state degree program (East Tennessee State University's Master of Social Work, including SUD Certificate) is also accredited by the Board.
The NCSAPPB website[28] provides all the information that an SUD professional would need to practice in North Carolina, including certification and licensing requirements, SOPs, accredited academic programs, online and in-person training courses, and downloadable application forms. Centralized and easy access to these resources is, in and of itself, a facilitator for entering or advancing within the SUD workforce.
In addition to the outreach efforts of colleges and universities to attract students into these certification programs, members of the NCSAPPB engage in active workforce recruitment by visiting campuses to provide information about available professional opportunities in the SUD field.
Supervision and "Telesupervision"
The NCSAPPB offers a separate credential for clinical supervisors (Certified Clinical Supervisor, or CCS). This is not a standalone credential; Licensed Clinical Addiction Specialists interested in pursuing the supervision of persons providing can apply for the certificate which clearly defines supervision requirements and standardizes supervisor qualifications. This facilitates the credentialing process for positions requiring a certain number of supervised practice hours.
CCSs are allowed to provide supervision through telepractice. This enhances access to supervision services for professionals seeking an SUD credentials with supervised practice prerequisites.
Out-of-State Licenses
The state has a simplified licensing process for out-of-state professionals who are International Certification and Reciprocity Consortium (IC&RC) members. These individuals are required to complete a special application form and undergo a background check, but they can generally obtain their state license within 15-30 days. Out-of-state practitioners who are not members are expected to go through the full credentialing process; their existing credentials are reviewed on a case-by-case basis to assess equivalence and to determine further action required for endorsement, if any
Remaining Challenges and Future Directions
While the behavioral health system transition is still under way, the uncertainty about SUD service definition revisions, the changing benefit and reimbursement models, and the difficulty of joining insurance networks in the relatively new closed network system continue to pose challenges for the SUD workforce and for new practitioners. The DHHS's Behavioral Health Strategic Plan and the North Carolina Opioid Action Plan (2017-2021)[29] include measures to attract new behavioral health practitioners and to help the existing workforce navigate this changing landscape. In addition, the Department has recently issued a policy paper entitled Supporting Provider Transition to Medicaid Managed Care[30] with further details on the state's policies regarding workforce development and retention.
Credentialing and Reimbursement Supports
Although North Carolina's consolidated and centralized credentialing system has streamlined the credentialing process for SUD practitioners in past years, the managed care system has introduced some new complexities. To be reimbursed, providers are now required to join a network, and many providers need to contract with multiple networks to retain their existing patients. To meet their accreditation requirements, MCOs impose some prerequisites above and beyond the state's credentialing criteria, and these can vary by network. Thus, providers are forced to apply separately to multiple networks with different but overlapping contract requirements.
As part of the transition to managed care, the DHHS will develop an integrated Provider Data Management system and Credentials Verification Organization to centralize the credentialing and enrollment process. Until this system is fully operational, the current Medicaid enrollment process will remain in place and will be enhanced with additional features. Specifically, all prepaid health plans in the state will be given access to a centralized clearinghouse that combines verified provider enrollment data with managed care credentialing data. They will be prohibited from requesting additional information from providers for their contracting process, and providers will no longer be expected to give credentialing information separately to every plan with which they contract.
In a further effort to facilitate the network enrollment process for providers, DHHS will provide SUD practitioners with training and education on contracting strategies under managed care, changes to administrative and operational processes, changes to state systems, continuous quality improvement strategies, and evidence-based practice models.
Regional Provider Support Centers
As part of the system transition, DHHS is developing Regional Provider Support Centers. These will be organizations under contract with the department (through a competitive bid process) to support the workforce in their clinical transformation and care improvement efforts as well as electronic health record and health information exchange connectivity.
Payers' Council
As part of the North Carolina Opioid Action Plan, the state will convene a Payers' Council. The Council is currently being assembled with cooperation from the major health payers in the state. Although the main goal of the Council is to collaborate in regulating opioid prescription and dispensing practices across the state, the members will also partner in designing clinical benefits policies, treatment plans, and recovery supports. This collaboration will help reduce variability across plans in these policies and practices and reduce administrative burdens and reimbursement barriers experienced by providers.
Telemedicine
The behavioral health system reforms include a plan to enhance the infrastructure for telepractice and to encourage health plans to make use of this option. For example, health plans will be able to leverage their telemedicine capability to meet their network adequacy requirements. These measures will allow providers to expand their client base.
Concluding Remarks
North Carolina's centralized credentialing system, educational opportunities, and active recruitment of new professionals into the SUD field have been important factors facilitating the development and retention of the state's SUD workforce. The far-reaching system reforms currently in progress will, in the long run, benefit the SUD workforce in the form of improved reimbursement opportunities and streamlined enrollment processes. The transition period, however, has presented some challenges as providers try to adapt to the new system and to continue their practice within an environment in flux. These barriers are also common in other states implementing similar system reforms. The provider support measures that North Carolina has included in its strategic plans will provide useful examples for other states.
New York
New York |
|---|
Agencies/Organizations Contacted
|
Background
In 2011, New York Governor Andrew Cuomo established the Medicaid Redesign Team (MRT). Composed of stakeholders and experts from throughout the state, the team was tasked with working collaboratively to review and redesign New York's Medicaid system. The Action Plan they developed set forth a roadmap for a complete system overhaul, including, among other reforms, "ending the state's Medicaid FFS system and replacing it with a comprehensive, high-quality and integrated care management system."[31] To implement the full action plan, New York submitted an amendment to the state's existing Medicaid 1115 waiver demonstration. The finalized terms and conditions of the amendment were announced in 2014. The MRT was named a finalist for the 2015 Innovations in American Government Awards by Harvard University's Kennedy School of Government for its work, and especially for its "intensive stakeholder engagement process" in designing a health care delivery system with equal emphasis on cost and quality.[32]
This system redesign has a far-reaching impact on New York's behavioral health system. Whereas the state's Medicaid system had previously carved out mental health and SUD treatment services, full integration of health care within a managed care environment calls for a single care management organization to take on the responsibility of managing its members' complete needs--their physical and behavioral health service needs, both acute and long-term. The action plan further recommended that these reforms include safeguards to prevent "the 'medical model' of care from displacing community-based behavioral health service delivery."[33] The reforms were rolled out starting in October 2015; MRT expects the redesign approximately 5 years to be fully implemented.
Additionally, New York is one of eight demonstration states for the federal Excellence in Mental Health and Addiction Treatment Expansion Act (Excellence Act)[34] to improve access to community mental health and addiction treatment services. The Excellence Act defines and established criteria for Certified Community Behavioral Health Clinics (CCBHCs) that provide a set of required services, with an emphasis on crisis care, evidence-based practices, integration with physical health care, and care coordination. As part of the Excellence Act demonstration, 13 CCBHCs were established around New York State and began serving their communities in July 2017. This initiative dovetails with the MRT Action Plan's emphasis on avoiding hospitalization for behavioral health services that can be provided in a community setting. The chief counsel for the New York Office of Alcoholism and Substance Abuse Services (OASAS) expressed optimism about the contribution of the CCBHCs toward the state's goal of putting in place a comprehensive, integrated, and community-based behavioral health service delivery model; at the same time, he also pointed out that "this is still very much a work in progress."
These recent and currently unfolding reforms at the state level necessitate substantial practice transformation at the provider level. We next turn to New York's efforts to support the behavioral health workforce during this challenging transition.
Available Substance Use Disorder Workforce Supports
Training and Technical Assistance Resources
In planning and implementing the system overhaul, state officials were mindful of lessons learned from states that preceded New York in implementing similar structural reforms; in particular, they focused on the challenges that providers would face in adapting to the new system. In 2014, before the new system was rolled out, OASAS and the Office of Mental Health (OMH) contracted with Community Technical Assistance Center of New York (CTAC) and Managed Care Technical Assistance Center of New York (MCTAC) to work with behavioral health providers across the state in preparation for the transition. The co-director of CTAC/MCTAC summarized the role of their organization as "a bridge between system transformation and clinical or practice transformation." He added that in those states that transitioned their behavioral health systems from FFS to managed care without a similar "bridge," providers had difficulty adapting to the new system and some even went out of business, an eventuality that the New York redesign tried to avoid. In New York's Medicaid system, this transition was accompanied by a shift from a "carve-out" to a "carve-in" approach to behavioral health services and the introduction of a value-based payment environment, making the transition even more difficult for providers and adding urgency to the need for advance and ongoing training and technical assistance.
The partnership between OASAS and CTAC/MCTAC in supporting providers to weather the system overhaul has been successful in helping ease this transition. According to the CTAC/MCTAC co-director, one important factor that has helped is the "in-between" position of his organization. Given that CTAC/MCTAC is a non-government agency, providers feel encouraged to engage with them in a less guarded manner. Consequently, in the words of our informer, the agency gets "an unfiltered providers' view of what is actually going on." On the other hand, they are not a workforce advocacy organization either, which helps with their credibility in informing OASAS about the workforce barriers they witness in the field
The resources that CTAC/MCTAC offer the SUD workforce take into consideration the regional differences in delivery systems. This tailored approach helps providers distinguish between statewide and regional policies and practices. They offer group-format in-person trainings in every region, typically attended by 200-250 individuals. The trainings cover a broad range of topics--from administrative and infrastructure changes required by the new system to high-quality service provision, contracting, billing, and performance reporting. In addition to in-person events, the organization offers online trainings, including the Uniform Clinical Network Provider Training, which provides an overview of the expectations for providers under the new system. Since 2014, CTAC/MCTAC has made at least one in-person contact with about 85% of the approximately 900 behavioral health providers in New York; most have been contacted every year.
An important resource for SUD providers, developed through a partnership between OASAS and CTAC, is the LOCADTR tool.[35] LOCADTR is a web-based application that guides providers in determining the most appropriate levels of care for a given SUD. The state strongly encourages all insurers and providers to use the tool in determining the appropriate level of care for their enrollees and clients. Medicaid MCOs are required to use it.
One specific need that CTAC/MCTAC addresses is related to the state's requirement that MCOs provide a training program for their provider networks, to provide appropriate knowledge, skills, and expertise and offer technical assistance in fulfilling managed care requirements. These programs typically offer continuing clinical education and address topics such as co-occurring disorders, cultural competency, evidence-based practices, billing, coding, data interface, documentation requirements, claims submissions, and the service array available to Medicaid beneficiaries. MCOs can fulfil this requirement by having their providers take trainings offered by CTAC/MCTAC. Although the state requires MCOs to make trainings available, there is no requirement for providers to take the trainings; this helps the state provide resources without adding to the prerequisites for joining networks. Providers can also obtain continuing education credits and fulfil some certification requirements through these resources.
The CTAC/MCTAC website[36] archives their training events and makes recordings available for online access. The site also offers online tools, handouts, a list of acronyms, policy guidance documents, and instructional films. An email helpline is also available to respond to questions from individuals and agencies. Over 5,000 messages arrive daily and receive responses within 24 hours, on average. All of these services are offered free of charge and funded by the state.
There is a formal feedback mechanism between the state (OASAS and OMH) and CTAC/MCTAC. The email queries are shared with the state daily. Weekly communications allow the two sides to share policy updates and feedback from the provider side. To solicit input from providers, CTAC/MCTAC also conducts periodic focus groups and makes an annual presentation to state officials. This feedback mechanism allows the state to stay up-to-date on the impact of its policies on behavioral health practice and to respond to challenges in a timely fashion. It also allows CTAC/MCTAC to learn about new and upcoming policy initiatives and to make timely updates to its resource base to help the workforce keep up with a rapidly changing policy environment.
Contracting Safeguards
Managed care brings a new set of regulations governing insurance networks, including new contracting requirements and reimbursement schedules. These changes impose administrative and financial burdens on providers that were set up to operate within the old environment. One way in which New York has supported the workforce during the system redesign is through regulating MCOs. The state has a model contract[37] that all Medicaid MCOs are required to use in recruiting providers, including some important safeguards to reduce potential burden on their providers and to facilitate providers' network participation. These provisions can be summarized as follows:
-
One such requirement is standardized online communication between MCOs and providers. All Medicaid MCOs are required to set up web-based portals to communicate with their networks, eliminating the need for telephone or fax interactions that are more burdensome and not as readily conducive to standard recordkeeping. This requirement streamlines the application, contracting, and reimbursement processes for providers.
-
Reimbursement for SUD services. Network adequacy regulations include opioid treatment programs as essential services, and prior authorization cannot be required for SUD services. These regulations apply to commercial plans as well as Medicaid plans. All New York health plans now reimburse outpatient, inpatient, or residential SUD services.
A recent review of model MCO contracts from the providers' point of view[38] cites the New York model[39] for several additional "provider-friendly" features:
-
"Soft" transition in reimbursement rates. One of the challenges that providers face during the transition from a FFS to a managed care payment model is the lengthy process of adjusting their practice to new reimbursement rates. To ease this transition, New York requires its MCOs to pay outpatient behavioral health providers (licensed or certified) the Medicaid FFS rates for the first 2 years of their joining the MCO's network.
-
Medicaid MCO contracts restricted to use of Medicaid products. If a Medicaid MCO requires providers to accept pre-negotiated rates for services and supports not covered by Medicaid as a condition of participating in the MCO's Medicaid plans, providers find it difficult to join Medicaid networks. In New York, Medicaid MCOs are prohibited from including such requirements, called "All Products Clauses," in their agreements with providers.
-
Streamlined credentialing. In some states, MCOs may impose credentialing requirements above and beyond those required by the state, as part of their contracts. These may vary from one MCO to the next within the state, making it difficult for providers to join multiple networks. New York requires its MCOs to accept state licensure or certification as having met the MCO's contracting standards, easing the way for providers to join MCO networks.
-
Medical necessity and grievance decision facilitators. Obtaining a medical necessity ruling from MCOs can be a time-consuming process and may require several iterations to justify the need for a service. Likewise, providers may also find the grievance process burdensome and lengthy; as with the medical necessity ruling, this process may require several iterations to explain the context for the grievance, to have the grievance reviewed, and to have it acted upon. To facilitate these processes, New York requires that MCO staff involved in medical necessity or provider grievance decisions have clinical experience relevant to the case under consideration.
Strictly speaking, the use of the model contract is a requirement only for Medicaid MCOs; however, OASAS' chief counsel indicated that the state has been "aggressive in getting commercial plans to use state approved model contract language in commercial plans."
Support in Transitioning to a Value-Based Practice Model
Transition to a value-based payment model requires important changes to providers' existing business models, involving administrative and infrastructural adaptations that often require a substantial investment. The transition can, thus, pose important challenges to providers, and especially to small providers with limited resources. Starting in January 2018, the state is making Medicaid funds available to support providers through this transition.[40] Multiple mental health and addiction service providers can join together to form BHCs to qualify for these funds. All members of the collaborative then share in the administrative functions created with these funds, instead of each provider separately investing in the new functions needed for practice transformation. Regional collaboratives can use these funds to:
-
Identify gaps in the continuum of care they offer and make changes in the practice to offer better integrated care.
-
Develop new processes for monitoring treatment plans to preempt avoidable complications and avoid unnecessary costs.
-
Identify and implement opportunities for quality improvement and cost reduction.
-
Improve information technology capabilities and efficient data sharing mechanisms with multiple providers.
-
Develop quality improvement protocols to identify and address shortfalls when quality metrics do not meet their targets.
So far, 19 such collaboratives have been awarded. For example, one such network, the South Central Behavioral Health Care Collaborative, was awarded $1.6 million over 3 years to bring together 33 providers in their region to "address identified gaps in services by seeking additional partners who offer those services and working with current partners to expand available services."[41]
Incentives for Hiring New SUD Providers
With the help of funding from the State Targeted Response to the Opioid Crisis (STR), New York makes funds available to provider organizations for offering sign-on bonuses to recruit new SUD staff members. Combined with network adequacy requirements that require the availability of SUD services, these funds encourage networks to expand their SUD workforce capacity while at the same time providing incentives for professionals to enter the SUD field.
Funds available to the 13 CCBHCs in the state through the Excellence Act have also created new avenues for expanding the SUD workforce. A review of the early impact of this initiative by the National Council for Behavioral Health[42] found that gaining CCBHC status helped clinics offer enhanced salaries to hire new staff or to retain existing staff. For example, these newly available funds allow them to hire new prescribers for MAT and to provide peer support services to clients of all ages.
Training and Education Support for Counselors and Peer Specialists
Credentialed Alcoholism and Substance Abuse Counselors (CASACs) in New York are required to complete 60 hours of continuing education every 3 years. The state provides free online training to cover all 60 hours, so that once certified, a CASAC does not need to pay for any further education to be recertified. This is an incentive to join and remain in the SUD workforce.
During the past 2 years, OASAS has also offered scholarships for Certified Recovery Peer Advocates (CRPAs) to complete the required training and take the test for certification. This has had a large impact on the workforce: The OASAS general counsel indicated that the number of CRPAs in the state went from zero to 750 during that period. He added that OASAS is committed to continuing this program because they consider it "a really critical element in what we need to do moving forward."
The state department of health has a loan forgiveness program to encourage medical professionals to practice in high-need areas, with a few slots available for addiction and mental health providers.[43] Additional funds have recently become available through HRSA's National Service Corps to allow additional addiction treatment professionals to take advantage of loan forgiveness. The state is also exploring the option of setting aside some funds from its STR grant for this purpose.
Telepractice
Telemedicine widens a provider's client base without adding commuting burden; the ability to bill insurance for these services is an additional facilitator for providers. In New York, insurance plans are prohibited from distinguishing between in-person care and telepractice in reimbursing covered services. That is, all covered services are reimbursed even if provided through telepractice. Our informants indicated that this has significantly helped expand SUD services to remote areas experiencing provider shortages.
Remaining Challenges and Future Directions
The SUD field in New York is in the process of extensive transformation, opening new professional opportunities for practitioners at multiple levels. The new managed care and value-based payment models being instituted in the state, however, focus on provider organizations as the main actors. New York does not offer a license for SUD counseling, only a certification. It is still not possible for individual SUD professionals to establish independent practices and join insurance networks. SUD practitioners can only get insurance reimbursement for their services as staff members in a licensed facility. This may be a discouraging factor for a student or early-career professional at the stage of choosing a field of specialization. For many professionals, having independent practice at the end of their career ladder is an incentivizing factor. To the best of our knowledge, there are no current legislative efforts to define and regulate a role for independent providers of SUD services within the developing managed care environment. Such efforts may help further bolster the desirability of addiction counseling as a specialty.
Concluding Remarks
The key lesson learned from the successes that New York has had with its Medicaid redesign is the importance of providing support to providers in adapting their practices to the new system. Not only has the state provided supports and resources to providers in bridging the gap between existing business models and the requirements of the new system, it has done so in a timely fashion to preempt undue provider burden and workforce losses. This coordination between system redesign and provision of workforce supports has allowed the state to simultaneously expand coverage for behavioral health services, control costs, and improve service quality without suffering any workforce losses as has been the case in other states transitioning their behavioral health system from FFS to managed care. No doubt, the conscious efforts to learn from the experiences of other states during the planning stages were instrumental in making this a relatively smooth transition for the workforce.
Texas
Texas |
|---|
Agencies/Organizations Contacted
|
Background
During the past decade, Texas has undertaken a redesign of its entire health and human services system with important ramifications for behavioral health delivery. For example, behavioral health programs previously managed and regulated by multiple state agencies were moved under a single regulatory entity, to streamline funding and administrative functions. In 2011, Texas received approval for a 5year Section 1115 transformation waiver demonstration to expand its existing regional Medicaid managed care (MMC) services to the entire state, to reform its uncompensated care payment system, and to develop a Delivery System Reform Incentive Payment (DSRIP) pool to fund innovative strategies for improving health care delivery. The latest phase of the demonstration was recently approved to continue through September 2022.[44]
Through the DSRIP program, provider organizations can apply for funding for a broad range of innovative projects aimed at improving access to and the quality of health care while controlling costs. To participate in the DSRIP program, providers must be members of their local Regional Healthcare Partnership (RHP). There are 20 geographically distinct RHPs throughout the state through which the program is implemented. Of the approximately 1,500 DSRIP projects funded during the initial waiver period (2011-2017), more than a quarter (461) had a behavioral health focus and 56 specifically addressed SUD. The areas of focus for the funded SUD projects include:
-
Integrated physical and behavioral health treatment.
-
SUD workforce development.
-
Increased capacity to treat SUDs with co-occurring mental health disorders or intellectual disabilities.
-
Improved interventions to justice-involved individuals who also need substance use services.
-
Coordinated care among health systems.
The SUD-focused projects collectively received over $432 million in DSRIP funds over the first 6 years of the waiver demonstration.
Alongside the innovative strategies facilitated by this large-scale waiver demonstration, the Texas Health and Human Services Commission (HHSC) implemented several projects and initiatives to strengthen the state's behavioral health system, such as the RSS Program to incorporate recovery supports into the system of care and to develop the recovery and peer support workforce. This case study summarizes the impact of these recent system transformation efforts on the SUD workforce.
Impact of System Reforms on Substance Use Disorder Services and Workforce
Training and Technical Support during System Transition
The shift from a FFS model to a managed care reimbursement model typically brings with it workforce challenges (such as uncertainty in requirements) as well as the need for new administrative processes, infrastructure changes, and practice transformation measures. The 1115 waiver demonstration has also introduced changes in the practice and reimbursement environment, adding to providers' need for support in adapting to ongoing changes.
The HHSC proactively responded to these needs by creating shared learning structures. The 20 RHPs participating in the DSRIP program all have a lead organization (anchor) responsible for keeping its members informed of regulatory changes and offering training and technical assistance to the collaborating providers. Anchors are required to establish a regionwide learning collaborative and develop a training plan. The HHSC conducts bi-weekly calls with the anchors to provide information and receive provider feedback. The HHSC also conducts webinars and distributes reporting templates and guideline documents to providers, and it conducts an annual Learning Collaborative Summit to bring together the members of all participating RHPs.
Many of the topics addressed in regional learning collaborative meetings support SUD providers. Some examples are:
-
DSRIP project implementation, strategic planning, and/or reporting.
-
Patient and community engagement.
-
Behavioral health integration.
-
Selecting the right care in the right setting.
-
Care navigation.
-
Specialty care access.
-
Medical homes.
-
Measurement strategies.
-
Telehealth.
Providers interviewed by the demonstration evaluation team expressed overall satisfaction with these shared learning efforts.[45] Additionally, Texas has a rigorous training program for behavioral health peer recovery specialists (discussed in the next section).
Recovery and Peer Support Specialists
During the past decade, there were multiple efforts to regulate and develop the peer workforce within Texas's behavioral health system. A statewide peer specialist certification program was established in 2012. By 2015, there were 180 training vendors for SUD peer specialists and 460 certified peer providers.[46] In 2014, HHSC launched the RSS Program following a 3-year planning and stakeholder engagement period. The program funded 22 SUD provider organizations to embed peer-based recovery supports into their existing service mix. The program also included a rigorous training and technical assistance program for peer recovery specialists. Through webinars, technical assistance calls, and site visits, the training program addressed topics[47] such as:
-
Hiring and training recovery coaches.
-
Engaging and enrolling persons in recovery.
-
Collaboration of clinical and recovery support teams.
-
Defining target populations.
-
Promoting person-centered planning.
-
Conducting strength-based global assessments.
-
Determining appropriate level of engagement and intensity of services.
-
Developing Peer Advisory Leadership Councils.
-
Conducting assertive outreach and early reintervention.
-
Promoting employee role clarity.
-
Encouraging self-care for recovery coaches.
-
Aligning traditional policies and procedures with a recovery-orientation.
-
Promoting community integration.
-
The role of Medication Assisted Recovery.[48]
-
Changing the locus of services from the agency to the community.
Between 2014 and 2018, 255 new recovery coaches were hired by the provider organizations participating in the RSS program.
A recent article reviewing best practices in peer support practices3 selected Texas as one of the four states that lead the nation in peer provider workforce development efforts (along with Arizona, Georgia, and Pennsylvania). The authors report that, at $15.69, the average hourly wage for peer recovery support specialist in Texas was the highest among the four "model" states they studied.
Until recently, peer support services in Texas were funded through grants. In 2017, the 85th Legislature passed House Bill 1486, directing the HHSC to create a Medicaid benefit for peer support services. In line with this mandate, HHSC assembled a stakeholder workgroup--composed of peer specialists, peer supervisors, and trainers of peer specialists--to provide input on Medicaid policies regulating the training, certification, scope of services, and supervision of Certified Peer Specialists and Recovery Coaches.[49] The draft rules were presented for public comment during the summer of 2018. The 2018-19 General Appropriations Act provides $79,500 each fiscal year (FY) for training and technical assistance to peer specialists and appropriated $834,600 (all funds) in FY18 and $2,375,100 (all funds) in FY19 to provide peer support services in the Medicaid program. These developments will substantially strengthen the status of peer specialists as health care professionals and increase the availability of funding for their services. However, the proposal to allow certified peer specialists to directly bill Medicaid for their services failed in the prior legislative session due to opposition from a variety of stakeholder groups. A senior policymaker interviewed for this study pointed out that, in general, adding a new provider category to a state's Medicaid program is a time-consuming and expensive process and suggested that this may have been one of the barriers encountered in this legislative effort.
Loan Repayment
Student loan repayment is an effective strategy for attracting new professionals into a specialty field and is widely used across the nation to address workforce shortages. Until 2017, Licensed Chemical Dependency Counselors (LCDCs) in Texas did not qualify for the state's Loan Repayment Program for Mental Health Professionals. A 2017 house and senate bill (HB 3083/SB 1509) added LCDCs to the program, making them eligible for loan repayment up to $7,000 (up to $10,000 if they hold an associate degree). The goal of the legislation was to incentivize them to serve Medicaid or CHIP patients and incarcerated individuals and to practice in medically underserved areas.[50]
Expansion of Telehealth
As of May 2017, there were 81 DSRIP projects specifically related to telehealth; 49 of those specifically addressed expanding behavioral health services through improved telehealth infrastructure.[51] These projects will increase the need for behavioral health practitioners, including SUD counselors, thus opening new employment opportunities for this workforce. Additionally, employment in facilities with telehealth capacity will help professionals participating in the newly available loan repayment program fulfil the requirement to bring services to underserved areas without having to relocate.
Remaining Challenges and Future Directions
Disparity in Reimbursement Rates and Administrative Burden
Recent health care delivery reforms have helped support and further develop Texas's SUD workforce, especially by creating new employment and reimbursement opportunities. However, some barriers to reimbursement remain to be addressed. For example, as one of our key informants mentioned, the Medicaid reimbursement rates for SUD services are in critical need of updating, a process the state has begun for block grant-funded services and plans to begin for Medicaid-funded services next year. To illustrate the urgency of the need for this update, our informant cited the example of the SUD-specific billing category "15-minute alcohol and/or drug services," which is reimbursed by Medicaid at $14.50 whereas the rate for a similar mental health billing category, "30 minutes psychotherapy," is $44.66. The informant also expressed concern about the complexity and administrative burden of insurance reimbursement for providers, especially for dual eligible (Medicaid and Medicare) patients.
Disparity in Skill Requirements and Educational Incentives
The inclusion of LCDCs in the student loan repayment program is an important factor for incentivizing professionals to join the SUD field. However, as a statement by the Texas Hospital Association pointed out in their statement supporting the measure,[52] the loan ceilings are much lower for LCDCs than for other behavioral health professionals eligible for the program. For example, LCSWs, LPCs, and licensed MFTs without doctoral degrees are eligible for loan repayments up to $40,000 and can receive up to $80,000 if they hold a doctorate.[53] The repayment scale for LCDCs stops at an associate's degree as the highest degree eligible for repayment consideration; the implied assumption underlying the program's structure is that LCDCs will not seek a higher degree. In contrast, the program provides incentives for other behavioral health professionals to continue their education through a doctoral degree.
Remaining DSRIP Challenges Cited by Stakeholders
The 2017 evaluation of the waiver demonstration included semi-structured interviews with stakeholders, including providers. The key themes from a qualitative analysis of stakeholder concerns included the following recommendations:
-
Streamline the DSRIP and MMC processes.
-
Simplify DSRIP and timelines and payment schedules.
-
Eliminate frequent changes in DSRIP rules and regulations.
-
Recognize and address the unique implementation challenges of different types of providers in meeting DSRIP requirements.
-
Include more provider types in DSRIP and MMC that were previously excluded from participating.
Need for Sustainability Planning
Finally, sustainability of the positive changes brought about by DSRIP is an important concern expressed by stakeholders. The newly approved waiver extension includes mechanisms for annual decreases in federal matching funds; these funds will be completely eliminated by the end of the demonstration in 2021. Maintaining the expanded employment and reimbursement opportunities for the SUD workforce beyond the demonstration period will require careful sustainability planning.
NOTES
-
Behavioral Health Workforce Research Center. Scopes of Practice for Behavioral Health Professionals. Accessed November 2018 at http://www.behavioralhealthworkforce.org/practice-data-visualizations/.
-
See https://www.providerexpress.com/content/ope-provexpr/us/en/our-network/jon-states.html.
-
Authorization for independent practice is not uniformly documented; in some states, we made an inference from available documentation in the absence of direct evidence for this capability.
-
CMS, Medicare Coverage of Substance Abuse Services, https://www.cms.gov/outreach-and-education/medicare-learning-network-mln/mlnmattersarticles/downloads/se1604.pdf, accessed December 31, 2018. SUPPORT for Patients and Communities Act, 2018, https://www.congress.gov/bill/115th-congress/house-bill/6, accessed September 9, 2019.
-
See https://www.uhcprovider.com/content/dam/provider/docs/public/policies/medadv-guidelines/t/treatment-drug-abuse-chemical-dependency.pdf, accessed December 31, 2018.
-
Optum Provider Express, https://www.providerexpress.com/content/ope-provexpr/us/en/our-network/jon-states.html, accessed October 11, 2018.
-
National Association of State Alcohol and Drug Abuse Directors (NASADAD). (2013). State Regulations on Substance Use Disorder Programs and Counselors: An Overview. Retrieved from http://nasadad.org/wp-content/uploads/2010/12/State_Regulation_of_SUD_Programs_and_Counselors-7-26-13.pdf.
-
See http://www.behavioralhealthworkforce.org/practice-data-visualizations/.
-
See https://www.providerexpress.com/content/ope-provexpr/us/en/our-network/jon-states.html.
-
Padwa, H., & Oeser, B. (2013). White Paper on California Substance Use Disorder Treatment Workforce Development. Los Angeles, CA: UCLA Integrated Substance Abuse Programs.
-
For a description of this waiver opportunity, see the July 2015 letter from the Centers for Medicare & Medicaid Services to state Medicaid directors, available at https://www.medicaid.gov/federal-policy-guidance/downloads/smd15003.pdf.
-
ASAM levels 3.7 and 4.0 are currently not covered under the ODS. However, the state working to include these levels under the waiver.
-
U.S. Census Bureau, Population Division. (2018). Annual Estimates of the Resident Population: April 1, 2010 to July 1, 2017. Available at http://factfinder2.census.gov.
-
Wilhelm, P. (2016). DMC-ODS at the Starting Blocks: Insights from Phase I. A study for the California Senate Office of Research on the expansion of substance use treatment under California's Medi-Cal 2020 waiver. Berkeley, CA: University of California. Retrieved from https://sor.senate.ca.gov/sites/sor.senate.ca.gov/files/DMC-ODS%20Final%20Report%20Wilhelm%20Hyperlinked.pdf.
-
Substance Abuse and Mental Health Services Administration (SAMHSA). (2011). Scope of Practice and Career Ladder for Substance Use Disorder Counseling. Retrieved from http://atforum.com/documents/PEP11-SCOPES.pdf.
-
Urada, D., Antonini, V.P., Teruya, C., Tran, E., Huang, D., Padwa, H., Castro-Moino, K., Lee, A.B., & Grossman, J. (2017). California Drug Medi-Cal Organized Delivery System, FY 2016-2017 Evaluation Report. Los Angeles, CA: UCLA Integrated Substance Abuse Programs.
-
Brassil, M., Backstrom, C., & Jones, E. (2018). Medi-Cal moves addiction treatment into the mainstream: Early lessons from the Drug Medical Organized Delivery System pilots. Oakland, CA: California Health Care Foundation. Issue brief retrieved from https://www.chcf.org/publication/medi-cal-addiction-treatment-mainstream/.
-
See https://www.medicaid.gov/medicaid/managed-care/downloads/managed-care-regulations-42-cfr-part-438.pdf.
-
See https://www.dhcs.ca.gov/formsandpubs/Documents/MHSUDS%20IN_17-008.pdf and https://www.dhcs.ca.gov/formsandpubs/Documents/SUD_Peer_Support_Plan_Guide.pdf.
-
See, for example, https://www.dhcs.ca.gov/provgovpart/Documents/DMC_ODS_Peer_Support_Training_4.5.18.pdf.
-
See https://www.cibhs.org/sites/main/files/file-attachments/dmc-ods_waiver_training_plan.pdf.
-
See, for example, Los Angeles County's provider support resources at https://www.cibhs.org/la-county-learning-collaborative.
-
A sunrise review is a statutory process that investigates whether there is a need to regulate a previously unregulated profession.
-
We are grateful to Sherri Daly for sharing the text of the budget request with us.
-
See https://files.nc.gov/ncdhhs/documents/files/Joint-Communication-Bulletin-J195-Out-of-Network-Agreement.pdf.
-
See https://files.nc.gov/ncdma/documents/Reports/Legislative_Reports/SL2016-94-Sec12F-10-and-SL2017-57-Sect11F-6_2018_01.pdf.
-
See https://www.ncdhhs.gov/north-carolinas-opioid-action-plan.
-
See https://files.nc.gov/ncdhhs/documents/ProviderTransition_PolicyPaper_FINAL_20180518.pdf.
-
New York State Department of Health. (2014). A Plan to Transform the Empire State's Medicaid Program--Better Care, Better Health, Lower Costs: A Multi-Year Action Plan, p. 5 (emphasis in the original text). Retrieved from https://www.health.ny.gov/health_care/medicaid/redesign/docs/mrtfinalreport.pdf.
-
See https://www.innovations.harvard.edu/medicaid-redesign-team.
-
MRT Action Plan, p. 10.
-
See https://www.congress.gov/bill/115th-congress/house-bill/3931.
-
See https://www.oasas.ny.gov/treatment/health/locadtr/index.cfm.
-
See https://www.health.ny.gov/health_care/managed_care/docs/medicaid_managed_care_fhp_hiv-snp_model_contract.pdf.
-
Falcone, A.J., & Berke, D.M. (2018). Medicaid Managed Care Contracting: An Advocacy Guide for State Associations of Behavioral Health Providers. Report prepared for the National Council for Behavioral Health. Retrieved from https://www.thenationalcouncil.org/wp-content/uploads/2018/08/Medicaid-Managed-Care-Contracting-Guide-for-State-Associations-FTLF-2018_Updated-8.8.2018.pdf.
-
See https://www.health.ny.gov/health_care/managed_care/docs/medicaid_managed_care_fhp_hiv-snp_model_contract.pdf.
-
See https://mhanys.org/mh-update-1-4-18-governors-press-release-transformation-grant-awards/.
-
See https://fcscortland.org/SCBHCC+Receives+%241.6+Million+Award.
-
See https://www.thenationalcouncil.org/wp-content/uploads/2017/11/New-York-CCBHC-Impact-Summary-11-28-17.pdf.
-
See https://www.health.ny.gov/professionals/doctors/graduate_medical_education/doctors_across_ny/.
-
See https://hhs.texas.gov/sites/default/files//documents/laws-regulations/policies-rules/1115-waiver/waiver-renewal/1115renewal-cmsletter.pdf.
-
See https://hhs.texas.gov/sites/default/files/documents/laws-regulations/policies-rules/1115-docs/tool-guidelines/Evaluation-Texas-Demonstration-Waiver.pdf.
-
Chapman, S.A., Blash, L.K., Mayer, K., & Spetz, J. (2018). Emerging roles for peer providers in mental health and substance use disorders. American Journal of Preventive Medicine, 54(6-S3), S267-S274. Retrieved from https://www.sciencedirect.com/science/article/pii/S0749379718316052.
-
See https://socialwork.utexas.edu/dl/ari/recovery-support-services-report-2018.pdf.
-
This term is sometimes used in place of "medication-assisted treatment" to underscore the importance of combining medications with other recovery services such as counseling and peer supports.
-
See https://hhs.texas.gov/sites/default/files/documents/laws-regulations/reports-presentations/2018/hb-1486-primer-2-26-18.pdf.
-
See https://lrl.texas.gov/legis/BillSearch/BillDetails.cfm?billFileID=280329&from=advancedsearch&startrow=1&number=50&IDlist=&unclickList.
-
See https://hhs.texas.gov/sites/default/files/documents/laws-regulations/policies-rules/1115-docs/tool-guidelines/Evaluation-Texas-Demonstration-Waiver.pdf.
-
See https://dnnsymkuj.blob.core.windows.net/portals/0/Images/Issues/BehavioralHealth/LCDC_Workforce_OnePager_tn.jpg?sr=b&si=DNNFileManagerPolicy&sig=nnSnE2PGTx38po4cQD4eABVKr%2FCfatb23iw7CesWw9U%3D.
-
See http://www.hhloans.com/index.cfm?objectid=EC6C1C10-8982-11E5-A0840050560100A9.
{kind=link}
PROJECT AND REPORT INFORMATION
Substance Use Disorder Providers and Insurance Reimbursement
This brief was prepared by the Human Services Research Institute under contract #HHSP233201600015 with the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Disability, Aging and Long-Term Care Policy. For additional information about this subject, visit the DALTCP home page at https://aspe.hhs.gov/office-disability-aging-and-long-term-care-policy-daltcp or contact ASPE Project Officers at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201, Kristina.West@hhs.gov, Judith.Dey@hhs.gov.
Reports Available
Credentialing Substance Use Disorder Counselors: The Need for Uniform Standards Issue Brief
- HTML version: https://aspe.hhs.gov/basic-report/credentialing-substance-use-disorder-counselors-need-uniform-standards-issue-brief
- PDF version: https://aspe.hhs.gov/pdf-report/credentialing-substance-use-disorder-counselors-need-uniform-standards-issue-brief
State Licensure for Substance Use Disorder Counseling: Implications for Billing Eligibility Issue Brief
- HTML version: https://aspe.hhs.gov/basic-report/state-licensure-substance-use-disorder-counseling-implications-billing-eligibility
- PDF version: https://aspe.hhs.gov/pdf-report/state-licensure-substance-use-disorder-counseling-implications-billing-eligibility
Credentialing, Licensing, and Reimbursement of the SUD Workforce: A Review of Policies and Practices Across the Nation