
U.S. Department of Health and Human Services
An Analysis of Federal and State Policies Affecting Services to Mentally Retarded and other Developmentally Disabled Persons: State Perspectives Final Report
Tecla Jaskulski and Rebecca Weader
Macro Systems, Inc.
July 1987
PDF Version (156 PDF pages)
This report was prepared under contract #HHS-100-84-0035 between the Department of Health and Human Services's Office of Social Services Policy (now known as the Office of Disability, Aging and Long-Term Care Policy) and Macro Systems, Inc. For additional information about the study, you may visit the DALTCP home page at http://aspe.hhs.gov/daltcp/home.htm or contact the office at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, SW, Washington, DC 20201. The e-mail address is: webmaster.DALTCP@hhs.gov. The DALTCP Project Officer was Margaret Porter.
The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS
- I. OVERVIEW OF STUDY
- 1. Background
- 2. Study Objectives
- 3. The Approach
- II. SUMMARY OF STATE PROFILES
- 1. How High-Low CBS-Emphasis States Differ
- 2. State Characteristics
- 3. Major Influences on Community Service System Development
- 4. MR/DD System Goals
- III. FEDERAL POLICY PERSPECTIVES
- 1. State Perspectives on Federal Policy Influences
- 2. Implications for Federal Policy
- IV. GLOSSARY
- APPENDICES
- APPENDIX A: State Profiles
- APPENDIX B: Knowledgeable Individuals Consulted
- APPENDIX C: Bibliography
- APPENDIX D: Discussion Guide
- LIST OF TABLES
- EXHIBIT II-1: State MR/DD Systems
- EXHIBIT II-2: Virginia Service Delivery System
- EXHIBIT II-3: National and Selected State MR/DD Expenditures: 1977-1986
- EXHIBIT II-4: State Total MR/DD Expenditures and Community Expenditures: 1977-1986
- EXHIBIT II-5: National and State Per Capita MR/DD Expenditures: 1977-1982
- EXHIBIT II-6: State MR/DD Population in ICFs-MR Per 100,000 General Population
- EXHIBIT A-1: Colorado MR/DD Service Delivery System
- EXHIBIT A-2: Illinois Service Delivery System
- EXHIBIT A-3: Michigan Service Delivery System
- EXHIBIT A-4: Nebraska Service Delivery System
- EXHIBIT A-5: Texas Service Delivery System
- EXHIBIT A-6: Virginia Service Delivery System
ACKNOWLEDGEMENTS
The authors are indebted to a number of persons who helped in the preparation of this report. The Government Project Officer, Ms. Margaret Porter, provided invaluable guidance and support throughout the project. Other ASPE staff and members of the Working Group on MR/DD Policies also made valuable contributions.
Special thanks are due to the contacts in each state, without whose cooperation and assistance this study would not have been possible.
EXECUTIVE SUMMARY
1. Purpose of the Study
The Developmental Disabilities Act of 1984 required the Department of Health and Human Services (HHS) to submit a report to Congress on improving services to mentally retarded and other developmentally disabled (MR/DD) persons. That report, prepared by the Assistant Secretary for Planning and Evaluation (ASPE), Office of Social Services Policy, recommended the establishment of an intradepartmental Working Group to develop cost effective Federal policy options for enhancing independence, productivity, and community integration for MR/DD people.
The purpose of this study is to provide information to the Working Group on the impact of Federal programs and policies on state policies regarding community-based services (CBS) for MR/DD people. The objective of the investigation and analysis was to develop an understanding of the factors which influence state policy choices and the environment that is created for implementing Federal policies and programs at the state level. The study identifies those factors, especially those relevant to Federal policy, which either encourage or inhibit the development of services that promote autonomy and integration for MR/DD people and minimize inappropriate institutionalization.
2. Methodology
This report presents the results of an in-depth review of six state MR/DD service systems. To obtain an understanding of the elements which play a critical role in state policy, decisions regarding the degree of emphasis to be placed on CBS, it was decided to focus on the two ends of the CBS "continuum." Colorado, Michigan, and Nebraska (hereafter referred to as high-CBS emphasis states) were selected as states which have developed extensive CBS systems. Illinois, Texas, and Virginia (low-CBS emphasis states) provide the perspectives of states which continue to rely heavily on institutional services. Factors used to classify states in relation to their relative emphasis on CBS included: the distribution of expenditures between CBS and large public residential facilities (PRFs); the population in PRFs and small (15 beds or less) community residential facilities (CRFs); and trends in the reduction of the population in PRFs. State characteristics, such as population size and geographic location, also were considered in the state selection process.
Data collection and analysis emphasized discussions with key policy makers and program operators in each of the six states, as well as a review of relevant documents and reports supplied by the state informants. A profile of each state system was developed to serve as the primary instrument of analysis for a cross-state comparison.
3. Major Determinants of State Policies
The analysis of state MR/DD service systems reveals that state policy decisions and the state's overall emphasis on CBS are the results of the interaction between a complex array of factors specific to individual state's political and MR/DD service systems and the requirements and incentives imposed by Federal programs and policies. Although Federal policy is not the primary influence on state policy decisions, it does play a fundamental role in the financing and delivery of MR/DD services on the state level.
Colorado, Nebraska, and Michigan demonstrate a strong philosophical commitment to CBS, and have translated that philosophy into concrete policy. Michigan's orientation toward CBS reflects, in part, a traditionally strong commitment to human services. Advocates for CBS in Nebraska and Colorado were able to articulate the importance of CBS in terms of their states' conservative political values which emphasize individualism, independence, and local control. The high level of philosophical commitment in these three states created an environment conducive to CBS development. The three high-CBS emphasis states also benefited from the presence of strong, well-organized advocacy for community services. Several respondents in the low-CBS emphasis states cited the lack of effective advocacy as barrier to the development of CBS.
Although a political commitment to CBS and the presence of able and dedicated individuals are essential to the development of CBS, these factors are not sufficient for such development. A variety of other internal and external factors also appear to influence whether and how CBS develops in a particular state. For example, although community-level service delivery systems and a high degree of community involvement appear to be crucial to CBS implementation, their presence does not guarantee CBS development.
The health of a state's economy also is an important factor affecting state support for MR/DD services, especially in the Initial stages of the move toward an emphasis on CBS. Respondents in two of the three high-CBS states reported that the major expansion of CBS coincided with periods of economic prosperity in the state. Economic difficulties can have one of two effects on CBS development: scarcity of resources may encourage a state to consider less costly alternatives to institutional care; and, conversely, a shortage of funds may prevent a state from developing new services. Financial issues are a major concern, especially for the low-CBS-emphasis states which are struggling with pressures to expand CBS while maintaining service quality in large PRFs.
Federal policy has been critical to the development of CBS, but factors internal to individual states shape the nature and degree of Federal influence. For example, the ability to use Federal funds to finance CBS was an enabling factor for the three high CBS states--the availability of Title XIX funds and the Title XX Social Services Block Grant made CBS development possible. However, faced with the same alternatives, other states chose to continue to rely on institutional services. States' responses to the original Medicaid Intermediate Care Facility for the Mentally Retarded (ICF-MR) regulations illustrate another aspect of Federal influence: in two of the three high-CBS states, the regulations were explicitly cited as an additional impetus for the depopulation of PRFs; in the three low-CBS states, the investments in PRFs associated with complying to Federal standards are seen as an important barrier to CBS development.
4. Implications for Federal Policy
State perspectives on the impact of Federal policy focused on: the limited availability of funding; the relative inflexibility of federally funded programs; ambiguities and inconsistencies across the myriad of Federal programs serving the MR/DD population; and the perceived absence of clear and consistent policy and leadership on the Federal level. In general, state respondents were likely to describe Federal policies and programs, with the exception of the Home and Community Based Care waiver, as barriers to the development of individualized, integrated, nonmedical service models. This tendency is partially due to the heavy dependence among five of the six states examined on the ICF-MR program and other Medicaid funding to finance MR/DD services. Respondents in all of the states supported CBS objectives, such as increasing independence and productivity for MR/DD people, but felt that overall Federal policy and programs (especially ICF-MR) are oriented toward facility-based, medical/institutional models.
State responses to specific Federal policy changes are difficult to predict. However, several themes emerge from respondents' perceptions of current Federal programs and suggestions for future policy changes:
- States would be receptive to changes which would increase their flexibility to use Federal dollars for CBS, but would be reluctant to accept reduced Federal financial participation (FFP) in exchange for increased flexibility.
- A combination of the various Federal-funding streams would probably be attractive to states, although interagency turf battles at the state level might develop.
- Some type of preferential funding for CBS would probably be favorably received if such changes incorporate incentives for future expansion of CBS rather than penalties for choices made in the past.
The potential for Federal policy to encourage a greater emphasis on CBS, as well as the development of service models which facilitate community integration and independence for MR/DD individuals, is significant. State respondents repeatedly stressed the need for a clear, unequivocal Federal commitment to CBS, accompanied by programmatic guidelines and funding mechanisms which are consistent with that philosophical commitment.
Federal policy changes can perhaps make the greatest impact in states such as Virginia, Illinois, and Texas. These states want to expand CBS and have already begun to do so, but the size of their institutional populations and their relative lack of CBS experience will hinder expansion efforts. Federal involvement in technical assistance and service system development, in addition to financial assistance and strong leadership could be highly effective in increasing community service options for MR/DD people.
I. OVERVIEW OF STUDY
The analysis of Federal and state policies affecting services to mentally retarded and other developmentally disabled (MR/DD) persons recently conducted by Macro Systems, Inc. (Macro), and its subcontractor, Systemetrics, was designed to assist the Office of the Assistant Secretary for Planning and Evaluation (ASPE) in chairing the Working Group on Policies Affecting MR/DD Persons. The background, objectives, and methodology of this study are described in this chapter.
1. Background
The Developmental Disabilities Act of 1984 called for a Report to Congress on Policies for Improving Services to Mentally Retarded and Other Developmentally Disabled Persons Under Title XIX of the Social Security Act. The Office of Social Services Policy, ASPE, prepared the report in consultation with other departmental agencies, including the Office of Human Development Services (HDS) and the Health Care Financing Administration (HCFA), as well as two other Federal agencies: the Office of Special Education and Rehabilitative Services, Department of Education, and the National Council on the Handicapped. The report was transmitted to Congress on January 21, 1986.
The report identified four goals for increasing the independence, integration, and productivity of this population: (1) increasing incentives for community living; (2) improving standards for the Medicare Intermediate Care Facilities for the Mentally Retarded (ICFs-MR); (3) meeting the needs of adults; and (4) improving coordination and cooperation. In an effort to address these goals, the Department of Health and Human Services (HHS) said it would examine options which reduce incentives toward inappropriate institutionalization and provide states with greater flexibility to provide a continuum of services while establishing workable cost controls.
ASPE recommended the establishment of an intra-agency Working Group to conduct a systematic examination of policies related to mentally retarded and other developmentally disabled people and to develop cost-effective policy options. Areas to be addressed by this Working Group included the high cost of the ICF-MR program and its medical and institutional orientation; the shift to smaller facilities and the use of Medicaid home and community-based service waivers; concern about health and safety and enforcement of standards; controversy over support for educational and vocational services; and various options for restructuring the financing of services.
The Secretary concurred with the recommendation and a Working Group, chaired by ASPE, was established. The Working Group is conducting a systematic examination of policies related to this population and is developing policy options for the Secretary. Specifically, the Working Group is considering cost-effective options which will enhance the productivity, independence, and integration of developmentally disabled people. Emphasis is being placed on policies which could enhance self-sufficiency and encourage access to community living arrangements.
2. Study Objectives
The overall goal of this study is to provide information to ASPE and the Working Group to assist them in the delineation and assessment of policy options being considered for recommendation to the Secretary. One component, conducted primarily by Systemetrics and reported in other documents, focused on the analysis of existing data on the impact of current Federal policy with respect to the major Federal programs financing services to the MR/DD population, in particular the Medicaid program. This component has attempted to provide the Working Group with an overview of the relationship between the structure of these financing programs, the manner in which services are delivered, and how much they cost, as well as an analysis of programmatic and cost implications of alternative financing and delivery systems.
The component conducted by Macro focused on state perspectives regarding organizational, political, regulatory, and other factors which encourage or inhibit community-based services (CBS) for MR/DD individuals. State perceptions about the influence of Federal policy on state development of CBS received particular attention. The study was not limited to a review of Federal policy influence, however, but rather was designed to gain a better understanding of the bases for states' MR/DD policy decisions and the context in which Federal programs and policies operate. The analysis of state perspectives is being provided to ASPE and the Working Group to assist them in their assessment of proposed policy options, including the projected impact on state policies in further development of CBS for MR/DD people, especially services that meet Federal policy goals of promoting the population's independence, integration, and productivity.
The analysis of state perspectives is summarized in this report. Detailed information on the six states visited in developing this analysis is presented in the Appendix volume which accompanies this report.
3. The Approach
The approach to our analysis of state perspectives entailed four components:
- Review of national trends in state MR/DD systems
- Consultation with knowledgeable individuals
- Selection of six states for in-depth review
- Plan for data collection and analysis
Our activities in these areas are highlighted in this section.
(1) Review Of National Trends
Literature with information on state MR/DD systems was reviewed to identify national trends in such key areas as expenditures for MR/DD services; use of the ICF-MR Program; use of the Medicaid Home and Community-Based Care (HCB) Waiver; and overall community service configurations. Three sources were particularly helpful:
- An Analysis of Medicaid's Intermediate Care Facility for the Mentally Retarded (ICF-MR) Program (Lakin, et al., 1985)
- Persons with Mental Retardation in State-Operated Residential Facilities: Years Ending June 30, 1984 and June 30, 1985 with Longitudinal Trends from 1950 to 1985 (Lakin, et al., 1986)
- Public Expenditures for Mental Retardation and Developmental Disabilities in the United States: State Profiles (Second Edition) (Braddock, et al., 1986)
A copy of our general bibliography may be found in the Appendix. Additional information was obtained from review of such "fugitive" literature as technical assistance reports of the National Association of State Mental Retardation Program Directors and an informal survey on state use of the ICF-MR program, which included the following: public and private sponsorship; numbers of clients and numbers of facilities with more than 15 beds vs. 15 beds or less; and projected reaction to the proposed Community and Family Living Amendments (CFLA), then being considered by the 99th Congress.
(2) Consultation With Knowledgeable Individuals
Early in the study, we consulted with several knowledgeable individuals to obtain guidance in the development of the plan for data collection and analysis. In addition to the ASPE Work Group and fellow investigators Brian Burwell (Systemetrics) and Charlie Lakin (University of Minnesota), we consulted with representatives of major interest groups, including the National Association of State Developmental Disability Councils, the National Association of State Mental Retardation Program Directors, the National Association of State Mental Health Program Directors, the American Public Welfare Association/State Medicaid Directors, and the National Association of Private Residential Facilities for the Mentally Retarded. We also consulted with Federal officials knowledgeable about state programs and the states' response to Federal policies, in particular representatives of the Administration on Developmental Disabilities (ADD) and HC FA.
The discussions with knowledgeable individuals focused on four areas:
- Data sources for national trends and state-specific information
- Criteria for selecting the six states for in-depth review
- Suggested states
- Data collection strategies
Their guidance was of considerable value in the development of recommendations on states to be visited and the plan for data collection and analysis. The prior consultation with some of the national organization representatives also may have been helpful in gaining access to some of the key informants at the state level.
(3) State Selection
The approach to analysis of state perspectives included in-depth review of MR/DD systems in six states and the influences on CBS development. To focus more sharply on the understanding of state choices in CBS development, it was decided to divide the reviews evenly between states with extensive CBS emphasis and states which continued to rely more on services in large institutions and had relatively little CBS emphasis. Factors used to identify states in relation to their emphasis on CBS included: proportionate expenditures for CBS vs. (usually large) public residential facilities (PRFs); trends in reduction in PRF population; and relative numbers of small (15 beds or less) community residential facilities (CRFs).
Although CBS emphasis was the primary selection criterion, a variety of additional factors were considered as follows:
- Population--A range in total size of state population was considered; however, states with extremely large and extremely low populations were avoided.
- Geographic Region--A mix in geographic regions of the United States was sought.
- Use Of The HCB Waiver--Both waiver and nonwaiver states were included.
- MR/DD State Authority--A mix in state approaches to administration of its MR/DD system was sought, in particular the use of substate MR/DD authorities vs. a centralized system.
The study team's knowledge of current trends in state MR/DD systems and observations from knowledgeable individuals were used to assess ways in which states under consideration were representative of the overall nationwide mix. The six states selected in consultation with ASPE as a result of this assessment were:
- High CBS Emphasis: Colorado, Michigan, and Nebraska
- Low CBS Emphasis: Illinois, Texas, and Virginia
It should be emphasized that these designations are relative; i.e., this is not to say that Illinois, Texas, and Virginia are without CBS for their MR/DD citizens or that they are not moving to place more emphasis on CBS. As described in the following chapter, it is clear that these three states are actively pursuing strategies to develop an expanded community service system. Relatively speaking, however, they currently rely more extensively on large congregate institutions for MR/DD care than do Colorado, Michigan, Nebraska, and other strong CBS emphasis states.
(4) The Plan For Data Collection And Analysis
The plan for data collection was to gain understanding of state MR/DD system influences and state perspectives on Federal MR/DD policy through review of descriptive reports and documents, for example, state MR/DD budgets, and discussions with key informants. The informants included people in the following positions, or their designees, as appropriate to the individual states:
- MR/DD state agency director
- State mental health (MH) agency director where MR/DD is part of combined MH/MR department
- Director of special education services
- Director of state Medicaid agency or coordinator of Medicaid long-term care program
- Director of vocational rehabilitation services and/or supported employment program
- Director of the state Developmental Disabilities Council
- Director of the state DD Protection and Advocacy agency
- Representative(s) of the substate MR/DD authorities
- Director of the state Association for Retarded Citizens
- Director of the association of parents and other advocates for the maintenance of PRFs
- Representative(s) of the private providers
The study team's discussions with the informants were generally held person-to-person, as planned; telephone consultation was used for followup and to talk with those we were unable to meet with during our site visit. We also were fortunate in having Peg Porter, the ASPE delivery order officer, accompany us on two of the six visits.
The discussions were tailored to reflect the individuals' responsibilities in the state's MR/DD system. To obtain perspectives on the overall influences, however, and the degree of consensus on Federal policy perspectives, we attempted to cover the following topics with virtually all informants:
- Characterization of the state's degree of emphasis on community-based vs. state institution services
- Operational definition of community-based services
- Range of state-supported services available in the community, both residential and nonresidential (e.g., case management and off-site habilitation programs)
- Service administration responsibilities, including relevant interagency agreements
- Characteristics of MR/DD clients participating in CBS, and any significant differences between the CBS and PRF client populations
- Gaps in the CBS system
- Financing mechanisms for CBS, including use (if any) of the Medicaid HCB waiver and service development funding
- Financing of state PRFs and other system costs
- Major influences on MR/DD expenditures
- Cost controls on CBS programs
- Quality assurance mechanisms affecting CBS
- Factors which have contributed to the expansion of CBS; barriers to CBS development and how they might be overcome
- Short- and long-term goals for CBS and factors affecting their implementation
- Federal policy changes that would assist the state in achieving these objectives
The key informants who provided information on these topics in each state are listed as part of the state profiles found in the separate Appendix, as well as the state-specific documents used. The full text of the discussion guide also is included in the Appendix.
Information from the key informants and the documents provided by the informants were used to prepare a profile of each state's MR/DD system and a synthesis of perspectives on Federal policy and other influences on the state's development of community services for MR/DD individuals. The draft profile was sent to each key informant in the respective state for review and comment. Their clarifications, and, in some cases, additional information, are reflected in the state profiles found in the Appendix and in the discussion of state perspectives in this report.
The Plan For Analysis
The approach to our analysis of state perspectives focused on the need to provide information to ASPE and the Working Group that would be useful in the development and assessment of cost-effective policy options. The four major areas selected for analysis are as follows:
- Characteristics which differentiate high-CBS from low-CBS states
- Major influences on state CBS emphasis/how CBS has developed
- Influence of Federal policies on CBS development to date
- Probable state responses to the kinds of changes in Federal MR/DD policy being discussed by the Working Group
The influence of Federal Medicaid policies--policies either real or perceived--was, understandably, a major focus, along with the potential response to changes in the Medicaid program, given its dominance in financing MR/DD services. Perspectives on other Federal programs were included. However, less information was generally available to the study team on programs other than Medicaid, especially those that are generally administered at the local level (e.g., use of HUD 202/Section 8 funds in combination with client (SSI) payments).
The descriptions of the policy options being developed by the Working Group include coverage of five areas: (1) organization and administration; (2) client eligibility implications; (3) service array and delivery systems; (4) the financing approach, including potential cost-sharing; and (5) quality assurance strategies. Our analysis of possible state reactions to changes in Federal policy is designed to address these same areas, as well as an assessment of the likely effect on states' overall movement toward the goal of enhanced productivity, independence, and community integration of MR/DD individuals.
II. SUMMARY OF STATE PROFILES
The six states selected for the study exhibit significant variation with regard to the degree of emphasis on CBS, the range of services provided at the community level, the structure for service delivery, and the financing of CBS. Exhibit II-1, following this page, illustrates several features which describe the states' service systems:
- Size of the MR/DD population residing in various living arrangements (e.g., PRFs, small CRFs, etc.)
- Definition of CBS
- Use of the ICF-MR program to finance CBS
- Use of the Section 2176 HCB Waiver and other Title XIX options
- Activity in supported employment and family support services
- Existence of a community-level MR/DD authority
- Extent of private sector involvement
These features are discussed throughout this chapter in relation to current MR/DD service systems, influences on the development of current systems, and goals for future CBS development.
1. How High-Low CBS-Emphasis States Differ
The three high-CBS emphasis states appear to share at least the following characteristics:
- A strong philosophical commitment to CBS, with an emphasis on maximum integration and independence for the MR/DD individual
- Broad-based support for the expansion of CBS
- Extensive CBS already developed
- Investment in CBS and depopulation of PRFs rather than major capital investments in PRF improvements
The low-CBS emphasis states generally illustrated the converse of these characteristics, as follows:
- Lack of coherent support for CBS
- Considerable investment in PRFs
- Strong and organized support for congregate care
- Relatively few CBS alternatives
Despite the presence of a community service network in two of the three low CBS states--both Texas and Virginia have a statewide system providing services at the local level--their relative degree of CBS development and emphasis on CBS vs. large congregate care facilities is noticeably less than that found in the high-CBS emphasis states.
| EXHIBIT II-1: State MR/DD Systems | ||||||
| Colorado | Michigan | Nebraska | Illinois | Texas | Virginia | |
| Population | 3.2 million | 9 million | 1.6 million | 11 million | 16.4 million | 5.7 million |
| Population in PRFs |
|
|
|
|
|
|
| Population in CBS |
|
|
|
|
|
|
| Definition of CBS |
|
|
|
|
|
|
| ICF-MR >15 |
|
|
|
|
|
|
| HCBC Waiver |
|
|
|
|
|
|
| Other T19 Waiver | N/A |
| N/A | N/A |
|
|
| Case Management T19 Coverage | No |
| No |
|
| No |
| Private Sector Involvement |
|
|
|
|
|
|
| Local MR/DD Authority |
|
|
|
|
|
|
| ICF-MR 16 |
|
|
|
|
|
|
| Other CRF |
|
|
|
|
|
|
| Family Support |
|
|
|
|
|
|
| Supported Employment |
|
|
|
|
|
|
| 94-142 Age Range | 5 - 21 | 0 - 26 |
| 3 - 21 | 5 - 21 | 2 - 21 |
| Abbreviations Used PRF: Public Residential Facility CRF: Community Residential Facility | ||||||
There were other factors which we had speculated were likely to differentiate the high and low states, but which did not appear to do so in our sample:
- Strong employee unions--Strong employee unions are not necessarily associated with resistance to CBS. For example, Michigan has closed three PRFs and significantly reduced its total PRF population, yet has highly organized and vocal state employee unions. In contrast, Texas and Virginia employee unions are not considered particularly strong.
- Litigation--Litigation apparently is not necessarily associated with strong CBS development. Texas has had major litigation regarding PRF conditions and the need for CBS alternatives, while Nebraska's was generally considered not to be a significant factor in its CBS growth. It seems more likely that the absence of litigation reflects the lack of strong advocacy for deinstitutionalization and CBS development, as in Illinois and Virginia.
- Use of the ICF-MR program--As can be seen in the exhibit on state MR/DD system characteristics, there are different patterns across the six states. (For example, Nebraska has not used the ICF-MR program for small CRFs at all, while Michigan has used it extensively.) In general, however, the low-CBS states use the ICF-MR program for larger facilities and place more overall reliance on the ICF-MR program than the high-CBS states.
- Use of the HCB waiver--Involvement in the HCB Waiver opportunities is not necessarily correlated with high interest in CBS. The waiver has not been used by Michigan and Nebraska, and has been used by Illinois and Texas.
Examples of specific state characteristics are highlighted in the following section.
2. State Characteristics
(1) MR/DD System Administration
The lead agency in each state's MR/DD system is considered to be the state MR/DD agency. In none of the six states is this agency a cabinet-level department. In four states, the MR/DD authority is part of a department encompassing mental health and mental retardation, with MR/DD programs administered by a separate entity within the department; in Colorado and Nebraska, the MR/DD program agency is located within a department of institutions. These configurations are typical of states nationwide.
The six states are similar to each other and to other states in the complex division of responsibility among various state and substate agencies for various components of the MR/DD system. For example, the Virginia system includes the following major actors:
- Department of Mental Health and Mental Retardation (DMHMR)
- Administration of the PRFs
- Planning, policy-setting, and budget development
- Funding and performance agreements with 40 local Community Services Boards (CSBs)
- Payment of non-Federal share of ICF-MR costs from its budget
- Community Service Boards
- Provide six core services (emergency case, in- and outpatient services, residential care, day support, and prevention/intervention) to mentally ill, MR/DD, and substance abusing individuals
- Provide minimum of 10 percent of program costs (primarily done through contributions of county and other local governments from local tax dollars)
- Plan and design services to be operated directly or contracted Quality assurance
- Other services/functions as locally determined
- Department of Medical Assistance and Services (State Medicaid Agency)
- Administration of the ICF-MR program
- Monitoring of the ICF-IMR program, including annual inspection of care and utilization review for each resident in each facility
- Authority to decertify individual clients and deny payment for services
- Training and technical assistance for DMHMR personnel and ICFMR operators
- Department of Health--Licenses and inspects the ICFs-MR
- Department of Education and Local School Districts
- Operates special education programs for DD children ages 2-21 years
- Developing new initiative for transition from special education to vocational programs
- Department of Rehabilitative Services
- Administers traditional vocational rehabilitation services program, including services to some MR/DD individuals
- Collaborating with DMHMR and a state university to demonstrate supported employment (an Office of Special Education and Rehabilitation Services (OSERS) grant)
- Virginia Council on Development Disabilities
- Prepares state plan for services to the DD population, Federal DD definition
- Stimulates development of program strategies
- Department for Rights of the Disabled
- Designated DD Protection and Advocacy agency
- Also advocates for needs of disabled citizens who do not meet Federal DD definition (e.g., people becoming disabled after age 22)
- Administrative agency where the Council on Developmental Disabilities is found
A chart illustrating the Virginia system follows this page as Exhibit II-2. At the state as well as the Federal level, it is clear that developing and maintaining a coherent community service system presents major challenges in philosophical and political leadership, blending disparate funding streams, and coordinating programs which cut across multiple authorities.
Decentralized Authority
Further contributing to the complexity is the role of substate MR/DD authorities in all of the states visited except for Illinois. The responsibilities for these local authorities are generally similar to those described above for the CSBs in Virginia. With the exception of Colorado's Community Centered Boards (CCBs), local authorities which are independent private 501C3 corporations, the substate authorities are related in varying degrees to local governments, usually counties. Members of the governing boards of local MR/DD authorities are usually appointed by county or other local government officials. In addition, local governments are frequently required to contribute to local program budgets.
| EXHIBIT II-2: Virginia Service Delivery System |
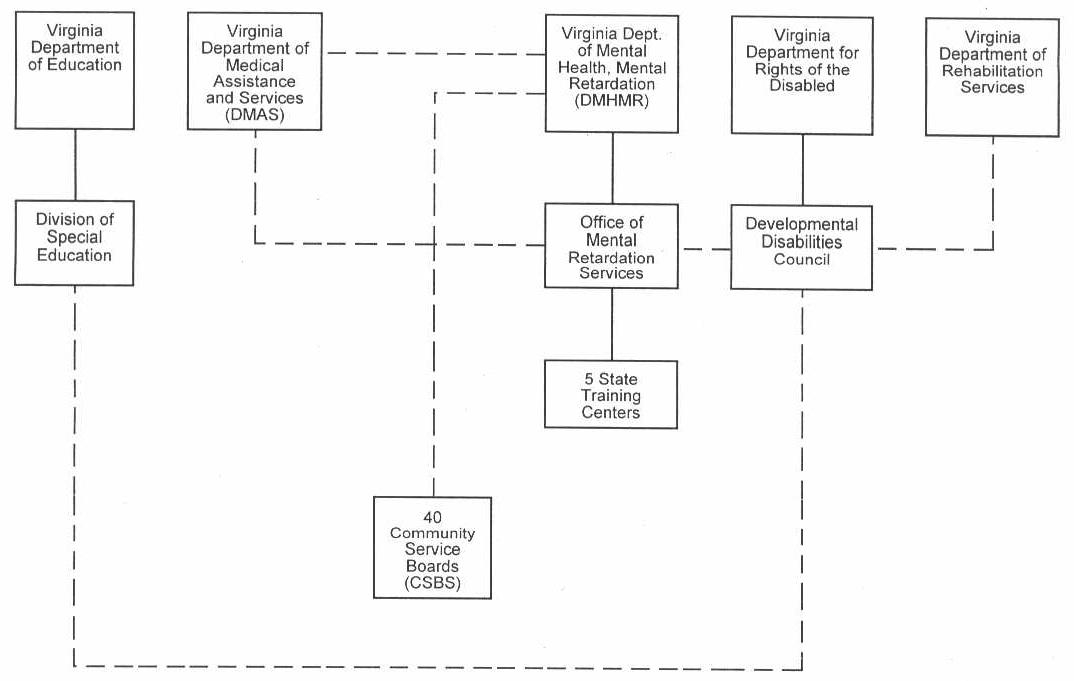 |
| Solid lines represent direct authority and oversight Broken lines represent coordination, communication, or indirect or limited authority |
In all five states with local authorities, it was agreed that there is tremendous variety among areas as to the array of available services, program priorities, clients served, local financial support, and program quality, even when statewide guidelines are in place. State MR/DD agencies in both Colorado and Michigan are attempting to exercise more control over local authorities, primarily through fiscal measures. Respondents in Nebraska, Texas, and Virginia did not report significant challenges to local authority. In all five, however, it is apparent that the state's ability to influence CBS development is limited by the degree of autonomy available to the local MR/DD authorities responsible for CBS programs.
Mental Retardation vs. MR/DD
Throughout this report, we have referred to the MR/DD population and service system--i.e., services to people with mental retardation and/or other developmental disabilities, with diagnoses such as autism, cerebral palsy, and epilepsy. Based on the current Federal definition of developmental disabilities, the MR/DD population also includes children with a wide array of conditions affecting their development such as ventilator- and other technology-dependent children, and children who have experienced head or spinal cord trauma. The central concept of the Federal definition is that it is based on the person's functional level rather than on his or her diagnosis:
The term "developmental disability," as defined in the Developmental Disabilities Act (P.L.98-527), means a severe, chronic disability of a person which--
- is attributable to a mental or physical impairment or combination of mental and physical impairments;
- is manifested before the person attains age 22;
- is likely to continue indefinitely;
- results in substantial functional imitations in three or more of the following areas of major life activities:
- self-care,
- receptive and expressive language,
- learning,
- mobility,
- self-direction,
- capacity for independent living,
- economic sufficiency; and
- reflects the person's need for a combination and sequence of special, interdisciplinary, or generic care, treatment, or other services which of lifelong or extended duration and are individually planned and coordinated.
With the exception of the federally-funded state DD Councils and state DD Protection and Advocacy Programs, however, few state agencies use the Federal DD definition for service eligibility; in fact, none of the six states visited used the Federal definition. In four of the six states--Michigan, Nebraska, Texas, and Virginia--the lead state agency is specifically the mental retardation authority, and its responsibility does not extend to other developmental disabilities. Similar limits are in place at the community level in those states as well, with services to people with other developmental disabilities the exception rather than the rule--at least for services administered by the local MR authority (i.e., services that are available to people with other developmental disabilities are generally provided through special education, crippled children's services, Medical Assistance, etc.).
The implication of limiting service eligibility to those who are mentally retarded is that people who have other developmental disabilities may receive a less comprehensive range of services.
Definitions used for determining ICF-MR eligibility also differ from both the Federal DD definition governing state DD planning and the Protection and Advocacy requirements. Still other definitions are used in classifying the special education population and in determining eligibility for vocational rehabilitation programs. The key difference between the state and Federal levels, however, appears to be that of MR vs. MR/DD, as well as the common policy of states and local authorities to include in the service system mildly retarded people who would not necessarily meet the Federal DD definition, especially with its emphasis on severity. It also is our understanding that such differences between Federal and state population eligibility are commonly found throughout the MR/DD system.
(2) Expenditures
The six states visited, like most states across the country, have increased their expenditures for MR/DD services and have increased the proportion of total MR/DD expenditures that support CBS as shown in Exhibit II-3 and Exhibit II-4. Nationwide, public expenditures (adjusted for inflation) rose 46 percent from 1977 to 1986, from $3.32 billion to $4.83 billion, not including local government funds. Expenditures for community services during this period rose 141 percent in constant dollars, while institutional expenditures rose only 14 percent. Although community expenditures in 1986 were still below 50 percent of total MR/DD expenditures, this percentage rose from 25 percent to over 41 percent between 1977 and 1986, despite the major expansion of the ICF-MR program for services in PRFs.
| EXHIBIT II-3: National and Selected State MR/DD Expenditures: 1977-19861,2 | ||||||||||||
| Total Expenditures($ in millions) | Institutional Expenditures3($ in millions) | Community Expenditures($ in millions) | Community Expenditures: % of Total($ in millions) | |||||||||
| 1977 | 1986 | % Change | 1977 | 1986 | % Change | 1977 | 1986 | % Change | 1977 | 1986 | % Change | |
| U.S. Total | 3,320.00 | 4,830.00 | 45.48 | 2,490.00 | 2,830.00 | 13.65 | 830.00 | 2,000.00 | 140.96 | 25.00 | 41.41 | 65.63 |
| Colorado | 43.75 | 51.00 | 16.57 | 25.00 | 25.00 | 0.00 | 18.75 | 26.00 | 38.67 | 42.86 | 50.98 | 18.95 |
| Nebraska | 27.47 | 30.42 | 10.74 | 14.15 | 15.00 | 6.01 | 13.32 | 15.42 | 15.77 | 48.49 | 50.69 | 4.54 |
| Michigan | 139.50 | 207.00 | 48.39 | 117.00 | 60.00 | -48.72 | 22.50 | 147.00 | 553.33 | 16.13 | 71.01 | 340.29 |
| Illinois | 180.00 | 197.50 | 9.72 | 137.50 | 122.50 | -10.91 | 42.50 | 75.00 | 76.47 | 23.61 | 37.97 | 60.83 |
| Texas | 160.0 | 184.50 | 15.31 | 135.00 | 152.00 | 12.59 | 25.00 | 32.50 | 30.00 | 15.63 | 17.62 | 12.74 |
| Virginia | 66.00 | 81.25 | 23.11 | 56.00 | 63.75 | 13.84 | 10.00 | 17.50 | 75.00 | 15.15 | 21.54 | 42.15 |
SOURCE: Braddock, D.; Hemp, R.; and Fujiura, G. Public Expenditures for Mental Retardation and Developmental Disabilities in the United States: State Profiles. Public Policy Monograph Series No. 29. Chicago: University of Illinois at Chicago, 1986.
| ||||||||||||
Expenditures in the six states illustrate the differences in MR/DID funding patterns between high CBS and low CBS states, as shown in Exhibit II-3 and Exhibit II-4 preceding this page. Although the three low states have increased CBS expenditures significantly from 1977-1986, as well as increasing the proportion of total MR/DD expenditures used to support community services, this proportion in all three was still below the national average of 41.4 percent: Illinois with 38.0 percent of expenditures going to CBS; Virginia - 21.5 percent, and Texas - 17.6 percent. In contrast, more than 50 percent of the public MR/DD expenditures in all three of the high-CBS emphasis states were for community services.
It should be noted that these totals generally do not include local government and other community-level expenditures as noted in Braddock (1986) from which these exhibits are adapted. (Such data are not routinely collected and reported by state MR/DD agencies.) Estimates from knowledgeable informants in Colorado were that CCBs, local governments, and other local funds provide 27 percent of the: resources for community services. Extensive local support is not necessarily correlated with high-CBS emphasis. For example, counties and other local governments in Virginia provide a minimum of 10 percent and as much as 50 percent of local CSB budgets for MR and other community mental health services. County governments in Nebraska and Michigan also are responsible for a portion of the costs of services to county residents in PRFs, although this is not common throughout the nation. Concerns about any potential increases in local government contributions for MR/DD services were raised by several informants because of the recent loss of the General Revenue Sharing program.
| EXHIBIT II-4: State Total MR/DD Expenditures and Community Expenditures: 1977-19861 |
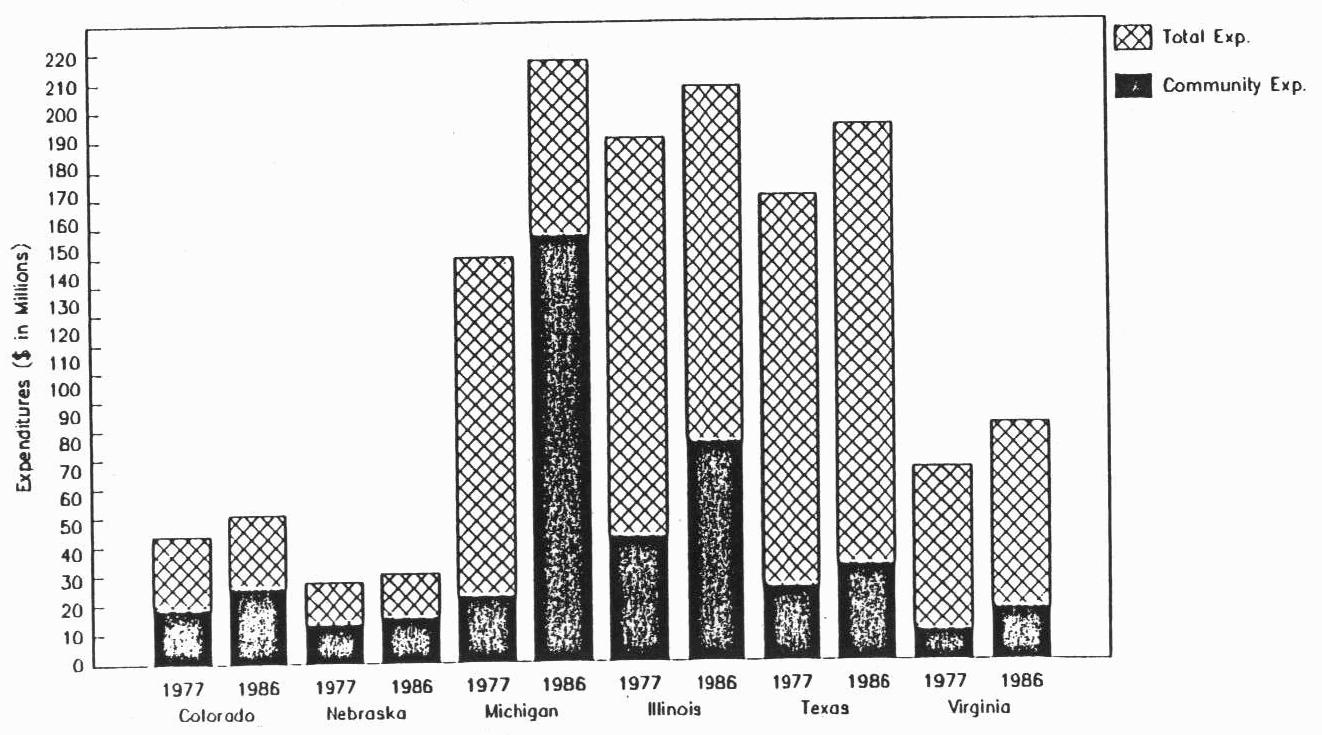 |
SOURCE: Braddock, D.; Hemp, R.; and Fujirua, G. Public Expenditures for Mental Retardation and Developmental Disabilities in the United States: State Profiles. Public Policy Monograph Series, No. 29. Chicago: University of Illinois of Chicago, 1986.
|
Trends in per capita MR/DD expenditures further illustrate differences between high- and low-CBS emphasis states, as shown in Exhibit II-5. Although all six states have increased per capita expenditures for community services, the three low-CBS emphasis states were well below the national community per capita expenditure average of $8.34, $6.50 (Illinois), $3.07 (Virginia), and $1.98 (Texas), while only one of the three high-emphasis states, Colorado, is below the national average at $8.05--possibly reflecting the additional 30 percent provided by CCBs and other local sources not included in the total.
| EXHIBIT II-5: National and State Per Capita MR/DD Expenditures: 1977-19821 | |||||||||
| Total Per Capita Expenditures | Institutional Per Capita Expenditures | Community Per Capita Expenditures | |||||||
| 19772 | 1982 | % Change | 19772 | 1982 | % Change | 19772 | 1982 | % Change | |
| U.S. Total | 14.66 | 20.11 | +38.0 | 10.99 | 11.85 | 7.8 | 3.67 | 8.34 | +12.76 |
| Colorado | 15.14 | 15.79 | +4.3 | 8.60 | 7.74 | (10.0) | 6.54 | 8.05 | +23.0 |
| Nebraska | 17.50 | 18.89 | +7.9 | 9.01 | 9.32 | +3.4 | 8.49 | 9.57 | +12.7 |
| Michigan | 15.07 | 22.77 | +51.0 | 12.64 | 6.60 | (48.0) | 2.43 | 16.17 | +565.0 |
| Illinois | 15.76 | 17.11 | +8.6 | 12.04 | 10.61 | (11.9) | 3.72 | 6.50 | +74.7 |
| Texas | 11.25 | 11.27 | +0.18 | 9.49 | 9.29 | (2.1) | 1.76 | 1.98 | +12.5 |
| Virginia | 12.35 | 14.23 | +15.29 | 10.47 | 11.16 | +6.6 | 1.88 | 3.07 | +63.3 |
| |||||||||
The ICF-MR Program
All six states participate in the ICF-MR program, as do nearly all states nationwide. The significant differences between the high- and low-CBS emphasis states are in their use of the ICF-MR program for medium and large (more than 15 beds) and small (15 beds or less) facilities, as illustrated in Exhibit II-6. Neither Colorado nor Nebraska uses the 15-bed or less ICF-MR program because policymakers in these two states feel that the ICF-MR model, even in a small setting, is too institutional. Michigan has used the program extensively for its AISMR residences, but plans to convert many to non-ICF-MR residences under the HCB waiver program. Michigan's use of the Alternative Intermediate Services (AIS)-MR model has been targeted to seriously disabled MR individuals. The three low-CBS states have not used the small ICF-MR program extensively; unlike the Colorado and Nebraska examples, the relative lack of small ICFs-MR in Texas, Virginia, and Illinois does not reflect the development of non-ICF-MR community residences or philosophical opposition to the "medical" model. However, officials in these three states indicated that the 15-bed or less ICF-MR program will probably be the area of fastest growth in community residential programs in the immediate future.
| EXHIBIT II-6: State MR/DD Population in ICFs-MR Per 100,000 General Population | |||||||
| State | State Population1 | Residents of ICFs-MR >15 beds2,3 | Residents of IFC-MR >15 per 100,000 General Population | Residents of ICF-MR 15 beds3 | ICF-MR 15 per 100,000 | Total ICF-MR | Total ICF-MR per 100,000 |
| Colorado | 3.2 million | 1,250 | 39.06 | 0 | -- | 1,250 | 39.06 |
| Michigan | 9.0 million | 1,650 | 18.33 | 1,800 | 20.00 | 3,450 | 38.33 |
| Nebraska | 1.6 million | 840 | 52.50 | 0 | -- | 840 | 52.50 |
| Illinois | 11.5 million | 8,7004 | 75.65 | 400 | 3.47 | 9,100 | 79.12 |
| Texas | 16.4 million | 10,500 | 64.02 | 800 | 4.87 | 11,300 | 68.90 |
| Virginia | 5.7 million | 3,060 | 53.68 | 200 | 3.50 | 3,260 | 57.19 |
| |||||||
The use of the ICF-MR program for larger facilities also varies between the high- and low-CBS states, with placements averaging 36.6 per 100,000 in Colorado, Michigan, and Nebraska vs. an average of 64.5 per 100,000 in Illinois, Texas, and Virginia. The greater use of the ICF-MR program for large facilities in the low-CBS states also is reflected in the higher per 100,000 population averages in the ICF-MR program overall, with an average of 43.3 ICF-MR residents per 100,000 in the high-CBS states vs. 68.4 per 100,000 average in the low-CBS states. It should be noted that these data do not include MR/DD people in non-ICF-MR Medicaid-certified nursing homes, a significant factor in states like Illinois where 3,000 such people have been identified.
(3) Services
A comprehensive array of services to MR/DD individuals cuts across many agencies and responsibilities. The six states we visited, although varying considerably with each other and within the states themselves as to the degree of CBS development and availability, all included the following services.
- Residential
- Large congregate care institutions
- Small-medium congregate care facilities
- Small family-sized CRFs
- Semi-independent living units (i.e., some supervision provided)
- Mix of public and private ownership, and mix of for-profit and not-for-profit among the private providers
- Habilitation Programs
- As part of residential services (daytime, evening, or both)
- Offsite day programs for people living in residential facilities or in their own homes
- Prevocational programs (May be considered part of vocational or educational services)
- Adult activity programs (May be considered part of vocational or educational services)
- Offsite programs generally provided by public or private not-for-profit agencies
- Vocational Services
- Assessment and counseling (through state Vocational Rehabilitation (VR) services or MR/DD)
- Vocational training (general preparation or specific) preparation for competitive employment
- Sheltered employment--All but moderately/mildly disabled persons are still likely to be limited to sheltered workshops and work activity programs, even in more progressive states
- Various models of supported employment
- Mix of public and private not-for-profit providers, mostly private
- Education
- Special education services for various age ranges and with mixed levels of integration of more severely involved students
- Relatively limited adult education
- Widespread use of early intervention/infant stimulation in most states, either through education or local MR/DD service system
- Supports to Families
- Home training for family members/parents
- Respite care (limited availability)
- Some subsidies available
- Information and referral
- Most commonly provided by local MR/DD authorities or their contract agencies
- Case Management
- Available to both families and individual clients
- Generally a mandated service or nearly so
- Usually the responsibility of the local MR/DD authority
- May also be some additional case management by individual providers
- Other
- Medicaid coverage (general health care, acute care, ICF-MR, and other long-term care services)
- State SSI supplement (40 states)
- Advocacy
The tremendous growth in MR/DD services, especially at the community level, has been associated with families abilities to work with local and state officials to develop opportunities for MR/DD young people. In many cases, families initiated community programs to provide alternatives to placement in state institutions. Since most MR/DD individuals never were placed in state facilities, however, the real impact of CBS growth has been in the promotion of the development of each individual's potential for independence.
How Service Configurations Vary Among States
Services in the three high-CBS states are different from those found in the low-CBS states as follows:
| Issue | High CBS Emphasis (CO, MI, NE) | Low-CBS Emphasis (IL, TX, VA) |
| Availability | More CBS available across the board/more served | Less CBS available/fewer served |
| Size/Type of Residential Services | Higher percentage of small and noncongregate options | More reliance on large and medium congregate care facilities, even in community |
| Client Disability | More CBS available to severely and multiply disabled clients/relatively less difference between CBS and PRF populations | Major gaps in CBS especially for severely and multiply disabled/CBS population generally much less disabled than PRF population |
| Deinstitutionalization | Early commitment to reduce PRF population | Relatively late in efforts to reduce PRF population |
The emphasis on CBS in-service programs is illustrated by Colorado's plans to expand options that are considered even more likely to promote individual development than the present system. The community residential system serves approximately 2,000 people in a variety of settings: follow-along supervision, minimum and moderate supervision group homes, intensive developmental group homes, social/emotional group homes, and behavior management group homes. Under the HCB Waiver, Colorado is adding Personal Care Alternatives (PCAs) to this repertoire. The objective of the PCA program is to allow the DD individuals to establish a home in the community rather than having to move as they "progress" through a series of facilities. Three models are being used, with staffing and support varied to meet individual needs. The host home model employs a family to have a DD person live in their home. In the peer companion and independent apartment models, the client lives with a disabled or nondisabled person and receives the necessary degree of support services. The PCA program is available to clients with a wide range of disability levels, including the severely and multiply handicapped. Simultaneously, the state Division of Developmental Disabilities is working with other agencies and the local MR/DD authorities for significant expansion of supported employment programs. In contrast, the low-CBS states are still thinking primarily in terms of large (8-15 person) group homes as the way to meet CBS objectives, although Texas has implemented policies limiting ICF-MR development to six-bed facilities.
High-CBS states also differ from low-CBS states in their use of the Medicaid program for CBS overall; Nebraska has chosen not to use Medicaid for CBS, while Michigan has used It extensively to expand community services, and Colorado has used the waiver to maintain growth in its CBS. In contrast, the low-CBS states have primarily used the ICF-MR program, and have focused on funding larger congregate facilities as illustrated in Exhibit II-1 above.
Other service system characteristics, however, are found to a varying degree among the six states regardless of CBS emphasis. All are placing increased emphasis on supports to families and supported employment initiatives. There also is no general correlation between CBS emphasis and private sector involvement, with the exception of the influence of large congregate care providers in the low-CBS states.
Major Service Caps
There also was considerable uniformity across the six states in their identification of gaps in the MR/DD service system. The major gaps mentioned include the following:
- Services for youth requiring special education, especially day programs/supported employment
- Services in rural areas
- Services for more challenging clients (even where some are available, more are needed)
- Programs to enable technology-dependent children to remain in their own homes (model waiver not sufficient to meet demand)
- Age-appropriate programs for elderly DD people
- In the four MR (i.e., not MR/DD) states; services for people with other developmental disabilities
The primary difference between high- and low-CBS states was that most informants in Illinois, Texas, and Virginia described across-the-board gaps in community services, as well as gaps in relation to particular population subgroups.
(4) Quality Assurance
Responsibilities for quality assurance in the state MR/DD system are typically divided among several agencies, reflecting the diverse responsibilities for the administration of service programs. For example, in Texas, quality assurance responsibilities involve the following actors:
- Texas Department of Mental Health and Mental Retardation (TDMHMR)
- Oversight of local community MH/MR program
- Monitoring and quality assurance in the state schools and community programs
- Monitoring of non-ICF-MR residential facilities
- Community Mental Health and Mental Retardation Centers
- Oversight of service provided at the local level based on performance contract with TDMHMR
- Governance provided by Center Boards of Directors
- Monitoring of individual client programs by case managers (also provided by case managers in state PRF outreach programs in areas without a center)
- Department of Human Services
- Promulgating regulations for the ICF-MR program
- Application of financial sanctions against ICF-MR providers
- Texas Department of Health
- Certification of state PRFs and licensing of all non-PRF ICFs-MR
- Inspections of care for residents of PRFs/all ICFs-MR
- Texas Planning Council for Developmental Disabilities--Service Evaluation
- Texas Rehabilitation Commission
- Oversight of vocational rehabilitation services
- Quality controls in administration of the Supplemental Security Income (SSI) and Social Security Disability Income (SSDI) programs
- Texas Education Agency--Oversight of special education services provided by the Independent School Districts
- Early Childhood Intervention Program--Oversight is provided by a parent representative and representatives from four state agencies: TDMHMR, Department of Health, Texas Education Agency, and Department of Human Services
- Advocacy, Inc. (Designated DD Protection and Advocacy Agency)
- Legal and protective advocacy services for individuals
- System advocacy
Additional oversight is provided by the judicial system in ongoing monitoring of the implementation of the consent decree of the Lelsz V. Kavanaugh suit mandating deinstitutionalization of three Texas PRFs; Association of Retarded Citizens (ARC)Texas has been involved actively in the litigation, and attempts to monitor Its compliance as well as to call the state's attention to other quality issues.
The Texas quality assurance profile is fairly typical of states in general as well as the six states visited, although states vary in specific divisions of responsibility among agencies and in mechanisms for monitoring non-ICF-MR community residences, with relatively few states having a comprehensive system of formal licensure of non-ICF-MR group homes. In many states, some DD people also live in "foster homes"--more accurately described as board and care homes, usually operating on a proprietary basis and housing several mentally disabled individuals--which are licensed and monitored by the public social services agency. As required by the Keyes Amendment, states specifically must provide assurances of systematic monitoring of board and care homes with more than one SSI recipient who have designated the operator/proprietor as representative payee.
The Case Management Debate
In Texas and two other states, issues were raised regarding the effectiveness of case management in quality assurance. Typically, a case manager's responsibilities include the monitoring of program services to be sure that: the individual client is receiving needed services as have been arranged (and presumably tailored to meet individual program goals); services are meeting basic standards of quality; and changes in providers are made as appropriate to respond to changing needs of the individual, or when It appears that a current provider is unable to meet those needs. The issue that has arisen is the question of conflict of interest when the case management is provided by the same local MR/DD authority that provides or administers the services. Informants in Texas, Nebraska, and Colorado noted pressure on the state to separate case management functions from the local CBS agencies, based on the premise that client interests cannot be adequately protected by case managers who work for and with the providers whose interests may conflict with the client's--for example, retaining a higher functioning person in a more sheltered setting than necessary because he/she is easier to work with (and therefore also less costly) than more disabled clients. Illinois officials indicated that they plan to move to an independent case management system, rather than continuing to contract for case management with providers of other services. Advocates for the present system, however, argue that case management responsibilities to the individual are kept paramount and that their being part of the overall agency benefits the clients by having better case manager access to and influence on program services. The resolution of this issue was noted as a factor likely to affect future CBS development by several respondents.
A related issue in quality assurance through case management is the ability to control provider reimbursement. Case managers have relatively little ability to determine reimbursements in the states visited or in states in general, especially in systems where the local case manager is not defined as the single point of entry to publicly supported services. For example, in most of the states visited, individual families can place DD relatives in private Medicaid facilities (generally large congregate care facilities) without going through the local assessment and case management system. In three of the states visited there were tensions between administrators of these facilities and the local MR/DD authority as to oversight responsibilities, with the large facilities tending to recognize only the traditional Medicaid quality assurance mechanism.
3. Major Influences on Community Service System Development
Informants in all six states described an array of factors which had influenced CBS development--both incentives and barriers--in their respective states. There also were extensive consensus within individual states as to which factors had been significant and what their influence had been. For example, although many of the key informants in Nebraska placed themselves at the forefront of the move to develop community services beginning in the late 1960s, there was strong consensus that the following factors contributed to Nebraska's leadership in CBS development:
- Involvement of parents and community members in the early stages of CBS development
- A strong, well-organized Association for Retarded Citizens
- Leaders in the field of community services, both theory and practice, who are involved in Nebraska
- Support from elected officials on both the state and local levels
- Ability to articulate a value-based statement of what mental retardation services should be
- Structural factors:
- Small state population
- Simple political system (unicameral legislature)
- Small financial investment in the institutional system
- Availability of funding for CBS development
- Title XX funds
- State funding of startup costs
- Strong and widespread philosophical commitment to CBS
A lawsuit filed in the early 1970s was considered to have made some contribution to CBS development, but informants noted that the litigation came after Nebraska had made a commitment to CBS and had developed a framework for financing and delivering those services through the 1969 inter-local Agreement Act. The only major factor identified as a barrier to CBS expansion was the state's recent economic difficulties. Despite these problems, however, support for CBS is strong enough that the mental retardation services budget received a slight increase in the last legislative session even as budgets for nearly all other state services were cut.
Not surprisingly, informants' descriptions of major influences in low-CBS emphasis states tended to focus more on inhibiting factors along with incentives. Although resource constraints were identified as an issue, many of the factors cited by informants as having inhibited CBS development had more to do with philosophical commitment and the state's political environment. For example, there was general consensus among the Texas informants that the following factors had been barriers to significant growth in CBS services:
- The legislature has been reluctant to fund human services and for MR/DD services; available resources have not been adequate to fund both institutional and community services.
- Several respondents cited the conservative political ideology which emphasizes independence, family privacy, and limited government as a major barrier to community services.
- The low level of public awareness has been an obstacle. Because there is little experience with community services In Texas, the public and many members of the legislature do not believe community services will work.
- Opposition from state school superintendents who have influence with the legislature and from Parents Associated for the Retarded of Texas (PART), the pro-institution parent group.
- Fears that reducing the size of state schools will mean lost jobs for state employees, with severe economic consequences in areas where the state school is a major employer.
- Several respondents commented that the institutional bias of the ICF-MR program continues to encourage Texas to emphasize institutional services.
- The absence of a reliable Federal funding stream for community-based, nonresidential programs.
Federal Program And Policy Influences
Nearly all informants described Federal programs and policies, along with other factors, as important influences in the development of the state's MR/DD system. The Medicaid program, particularly the ICF-MR component, was the most frequently mentioned influence, reflecting the extensive use of the program to support residential and related services. The significant variety in the ways the six states have used the Medicaid program to finance MR/DD services reflects the individual state's approach to MR/DD services and the Medicaid program in general, rather than program designs dictated at the Federal level. Differing rates of use for large facilities illustrate this trend. It also should be noted that although the Federal financial participation (FFP) in Medicaid is attractive to states, and candidly cited by several informants as a major factor in program design, states have not chosen to take advantage of all the Medicaid funding that is already available, such as funding for small community residences or for day programs under the clinic services option. A few informants specifically noted concerns about the Medicaid program's open-ended feature in relation to expanded obligation of state resources for the non-Federal share.
The major influences of the ICF-MR program included the following:
- Program requirements for PRFs forced states to raise standards, lower staffing ratios, and improve physical plants. High-CBS states tended to use depopulation and CBS development as part of these initiatives, while low-CBS states were likely to have focused more on PRF improvements.
- Existing private facilities were converted to ICFs-MR, especially large congregate care facilities in the low-CBS states of Illinois and Texas. (Although some smaller CRFs were converted in Michigan, Illinois, and Texas, this was not done on a major scale as has occurred in a few other states, most notably New York and Pennsylvania).
- Recent influence of the "look behinds" appeared to refocus attention on the need to maintain standards or risk loss of FFP. Even though the "look behinds" were sometimes painful for state officials, and led to some concern that required investments in PRFs and other large facilities would divert resources from CBS expansion, nearly all key informants described them as a positive influence.
The Section 2176 HCB Waiver was considered to have been a major influence in three of the six states, cutting across the CBS continuum. In Colorado, the Waiver was credited with having preserved the CBS expansion momentum at a point when the state's economy was in recession; as noted above, Colorado has used the Waiver to develop its PCAs model and to convert small ICFs-MR to non-ICF-MR CRFs. (Michigan plans to use its proposed Waiver similarly.) Illinois and Texas officials indicated that despite their inability to implement the Waiver at the full level approved, it has been instrumental in stimulating CBS development and in demonstrating the effectiveness of CBS. It should be noted that the three remaining states all plan to use the Waiver in the future, specifically to expand CBS availability.
Only one of the states has used other options of the Medicaid program extensively in its CBS system. Michigan covers some offsite day programs under the clinic services option, is developing coverage for case management as a discrete service, and has worked with the community mental health services system to ensure that these local MR/DD authorities are certified as Medicaid providers (all but one of the 55 local authorities are so certified). Michigan, along with Texas, also has obtained a model, or "Katie Beckett" waiver for services to severely disabled children; however, this was not considered a major influence.
The availability of client SSI funds was not mentioned frequently, but was identified by some informants in high-CBS states as a factor in CBS development. This was particularly the case in the high-CBS states, where SSI contributions from clients have been used in combination with Section 8 rental subsidies to finance non-ICF-MR alternatives. The Title XX/Social Services Block Grant (SSBG) program was a major .influence on the development of the Nebraska CBS system because of the availability of financing that could be used flexibly to meet needs defined at the local (Regional Governing Board) level. Title XX/SSBG also was used in Illinois and Texas (low-CBS states) to expand CBS in the late 1970s early 1980s. For example, Illinois spent an average of over $25 million in SSBG funds per year on MR/DD community services for the three years 1979-1981. Currently, however, all three states have reduced their use of Title XX/SSBG, and its influence is minimal.
The Developmental Disabilities Act
All six states have active Councils on Developmental Disabilities, funded through the Federal DD Act grant program. Informants reported varying degrees of involvement of the Councils in promoting CBS and advocating for more integrated and individualized services. Requirements for inter-agency cooperation in DD planning were noted in providing information on the strengths of Council activities, but not singled out as having had a major influence. It was clear that the Federal DD definition requirements for the Council and State Protection and Advocacy Agency had not been a major influence in the four states which focus on mental retardation rather than MR/DD. Some DD Council representatives in low-CBS states noted the political-reality limitations on their ability to push for major changes such as the reforms contained in the community and Family Living Amendments (CFLA). An informant in one state reported that the DD Council's endorsement of the CFLA proposed in the 98th Congress was deeply resented by a major private provider of MR/DD congregate care services who opposed CFLA and was able to generate thousands of letters to the governor protesting the Council's action.
Programs Not Administered By HHS
Informants in all six states noted the impact of P.L. 94-142, the Education for All Handicapped Children Act, in the expansion of community services. Although implementation of P.L. 94-142 has not always meant the degree of integration or "mainstreaming" that some had envisioned, there was general consensus that the program has led to expanded opportunities for MR/DD children and young adults, as well as preventing institutionalization. There also was consensus across the states that the success of P.L. 94-142 was placing major strains on the adult MR/DD service system, as young adults "age out" of special education and find no programs available. Waiting lists of "aging out" students were noted as a major issue in all six states.
There was lack of consensus on the influence of federally supported VR programs in CBS development. VR agency representatives tended to describe programs as reaching significant numbers of MR/DD people in the community, while most other informants indicated that VR programs seldom served more severely handicapped MR/DD clients (one VR agency representative presented this perspective in consonance with other informants in the state). The influence of the Independent Living program was noted by officials in only two states, perhaps because it was seen as serving the non-MR disabled population in systems where the primary focus is on mental retardation.
The Federal supported employment initiative was noted by several informants in each state. Four of the six states--two of three in each category--have grants from OSERS to develop supported employment services, as noted in Exhibit II-1 on state characteristics. Interest in supported employment was also expressed in Nebraska and Texas, the two states without OSERS grants, especially by representatives of the Association for Retarded citizens. Federal leadership from the Administration on Developmental Disabilities and OSERS in promoting supported employment seemed to be helpful to states in developing initiatives at the state level. On the other hand, some informants, and other MR/DD system representatives, expressed considerable skepticism regarding the feasibility of supported employment as a major vocational service objective despite its attractiveness. The major questions involved responsibility for long-term costs, recruitment of employers in rural areas or areas of high unemployment and declining economy, and program effectiveness for severely and multiply disabled individuals.
Other Influences On State MR/DD System
The primary influence on the development of CBS cited by informants in the high-CBS states was the broad-based support and philosophical commitment to community services. Virtually all informants in the three states believed this support and commitment to have resulted in state legislative appropriations for CBS, significant depopulation of PRFs, pro-CBS litigation, and widespread CBS development that was generally supported the community level. Informants in all three high-CBS states identified an informal coalition of parents, advocacy organizations, political leaders, and CBS providers who, along with policymakers in the state MR/DD agency, had helped shape the MR/DD system.
In contrast, the lack of such coalitions or their relative weakness was noted by informants in the three low-CBS states as a major factor in the relative lack of CBS development. At the same time, informants in these states reported that there continues to be strong political support for large MR/DD institutions, both PRFs and large private facilities. In Texas, for example, several of the PRFs, or "State Schools," are located in rural areas where they are a primary source of employment and support for the local economy; state legislators representing these areas understandably resist efforts that could lead to PRF closure. Private providers have also wielded considerable influence. For example, private providers and the nursing home lobby in Texas were successful in persuading the legislature to pass a law mandating that HCB rates be limited to a rate that is less than the average reimbursement rate for community ICF-MR providers; some informants felt this had hampered implementation of the Waiver.
Informants across all six states cited the states' economy as a major factor in shaping their MR/DD systems. Five of the six states--all but Virginia--reported significant economic problems which have increased the difficulties of financing CBS development. Informants noted various ways that this influence is felt, including pressures to obtain maximum FFP, (conversely) to limit FFP in order to avoid state match demands, to defer new initiatives, and to avoid demonstration program grants which are seen by some as likely to leave the state with an obligation to continue the support when the demonstration funds cease. The negative effect of the state's economic difficulties on CBS development was clearly stronger in the low-CBS states, where political strength is still developing, and less influential in the high-CBS states. As noted above, despite extreme problems in the economy, Nebraska's appropriations for CBS have continued to increase even as most other programs have been cut back.
The availability of resources for new service development was cited as a significant factor in most states. Some high-CBS states found ways to help substate MR/DD authorities and local providers develop services, for example, by appropriating special funds to cover startup costs (Nebraska), or by making additional funds available to local authorities. Texas has developed a major capacity-building initiative through its "Prospective Payment System" which makes $55.60 per day available to the local mental retardation authority for each client who returns to the area from a state PRF. Overall, however, the lack of startup funds was more frequently reported as a barrier, especially in low-CBS states. Several informants expressed concerns regarding their state's ability to maintain quality care in PRFs while simultaneously developing major expansions in community services.
The relationship between the state Medicaid and MR/DD agency was noted as a factor in all six states as well. Information in the three high-CBS states reported generally good working relationships and an overall consensus on Medicaid program objectives in relation to MR/DD individuals. For example, respondents in Michigan reported that the Department of Mental Health (the lead state MR agency) and the state Medicaid agency have worked together effectively on developing Medicaid-financed MR services. Moreover, views in the two agencies about appropriate goals for MR/DD services appeared to be compatible. Similar relations and a growing consensus had reportedly developed recently in one of the three low-CBS states. Informants identified this as having contributed to such activities as small ICF-MR development and effective use of waivers to expand CBS. In the other two low-CBS states, informants noted disagreements between the MR/DD and Medicaid agencies regarding areas such as target population, degree of medical orientation, and use of the Waiver. For example, in one state, the ICF-MR target population considered appropriate by the Medicaid agency was MR/DD individuals with significant health care needs, while several other Informants saw the need to serve a wide range of MR/DD individuals in the ICF-MR program, emphasizing habilitation rather than medical care.
Finally, informants in all six states reported several examples of intrastate variety that Influences their respective MR/DD systems. Many informants noted that rural areas have particular difficulties in meeting CBS development objectives, even when support is not the issue, due to lack of financial and programmatic resources. In contrast, community services in metropolitan areas and/or around universities were reported to be much more extensive and progressive, in both high- and low-CBS states. All states reported major differences in the availability of financial support from local governments and other local sources; where minimum local match is required, political support and commitment has meant contributions well above the minimum in some areas, and correspondingly better services.
In all but Illinois the considerable autonomy of local MR/DD authorities also has contributed to significant variation within states regarding CBS design and availability. Not surprisingly, several informants reported tensions between states and local MR/DD authorities, and in some cases with local governments, regarding state control vs. local autonomy. Another local autonomy issue cited as a factor in two of the three low-CBS states was local zoning authority. Several informants in these states reported that in the absence of legislation at the state level that restricts local zoning practices which discriminate against CRFs, community opposition was strong enough to use restrictive zoning rules to keep CRFs out.
4. MR/DD System Goals
There was general consensus within individual states and across the six states on goals for their MR/DD systems, regardless of where they are currently:
- Expanded development of community services, especially in integrated, normalizing settings
- Significant increases in supports to families and avoidance of out-of-home placement
- Continued reduction of PRF populations
- Development of supported employment programs
- Improvements in quality assurance efforts
The objectives for implementation of these goals varied, however, in relation to the state's efforts to date. Informants in high-CBS states tended to identify objectives such as closure of state PRFs and total or nearly-total PRF depopulation; small noninstitutional community alternatives for severely and multiply-handicapped MR/DD individuals or people with "challenging behaviors;" preference for non-ICF-MR models for community residences, such as Colorado's PCAs; and supported employment as a significant alternative to sheltered employment. Informants in the low-CBS states, especially Illinois and Texas, were more apt to describe such objectives as expanded group home and small ICF-MR development, gradual PRF depopulation, and meeting widespread needs for vocational and day programs. Although some informants in these states advocate the same kinds of objectives as those described in the high-CBS states, these views tended to be in the minority, with the exception of supported employment. There also was a greater tendency in low-CBS states for informants to see congregate care as a desirable alternative for more severely disabled individuals, with the more integrated services targeted primarily to individuals with mild or moderate disabilities. In addition, informants in high-CBS states were more apt to focus on client-based service development, while informants in low-CBS states tended to identify facility development needs.
There was considerable emphasis in all six states on cost-effectiveness as a major objective in MR/DD services. From the state perspective, this sometimes included pressures to seek FFP to support services, in particular through the Medicaid program. Several informants, however, including state officials, expressed the hope that states could work with the Federal Government to use the Medicaid program cost effectively to tailor services to meet individual needs and to avoid expensive out-of-home placements. Representatives in all six' states noted that state MR/DD budgets are scrutinized in detail by both the executive agencies and the legislature for cost containment strategies.
There also was a sense of optimism in three low-CBS states regarding their CBS development goals. State agency representatives and other informants in these states described an assessment of the current situation as "the time being ripe" for support to develop an expanded CBS system. These assessments were generally based on such factors as support from the governor, improvements in relations among involved agencies, and a sense that it is MR/DD's "turn" for attention and support in the legislature.
It should be noted that there were a range of opinions in all six states as to the appropriate MR/DD system goals and the strategies by which goals should be implemented. Each of the six states has an association of pro-PRF parents and advocates who object to plans that would include total PRF depopulation. Each state has some large facility private providers who advocate continued support for congregate care and sheltered workshop providers who feel threatened by pressure to convert services to supported employment. Tensions between advocates for noninstitutional, integrated services for MR/DD individuals and those who see a major continuing need for institutions and other traditional service models were expected to continue in all the states visited. The primary difference between the high- vs. low-CBS states was the relative strength of the two perspectives.
III. FEDERAL POLICY PERSPECTIVES
Most of the informants had perspectives to offer on Federal policy. Their comments focused on two areas: (1) how Federal policy influences or has influenced their state's MR/DD system; and (2) what changes in Federal policy would be helpful to the state in expanding CBS development. In this chapter, a summary of these perspectives are followed by a brief analysis of how states might be expected to respond to changes in Federal policy of the kind being considered by the Working Group.
1. State Perspectives on Federal Policy Influences
Federal policies were seen by state informants as one of several influences on MR/DD systems. This section presents a summary of views on Federal policy influence in promoting an overall orientation toward community MR/DD services, and influence on the system's administration, client eligibility, services, financing, and quality assurance.
(1) Influence On CBS Orientation
To date, Federal policy appears to have had minimal influence in promoting an emphasis on community services. The notable exception has been the Medicaid HCB Waiver program, which was cited by several states as significant in their CBS development and expansion efforts. The small ICF-MR program had been a major factor in support of CBS development in three of the states. However, two of the three, both high-CBS states, are in the process of reducing the use of the program through the Waiver, Colorado has in fact completed its conversion of small ICFs-MR to non-Medicaid facilities. The influence of the Developmental Disabilities Act and other Federal programs in promoting greater emphasis on CBS is unclear. Although several examples of pro-CBS activities of DD Councils were cited, it was not clear to what extent these activities had been shaped by Federal program requirements or in turn had been a major influence on state MR/DD systems, as DD Council influence was not cited as a factor in CBS development by the informants.
Several aspects of the ICF-MR program and the availability of FFP were primarily perceived to have discouraged CBS. For example:
- The original ICF-MR standards and the more recent "look-behind" effort encouraged large investments in capital improvements in PRFs and subsequent pressure to continue using PRFs.
- Pressure to maximize FFP encourages use of ICFs-MR even if other residential programs would be more appropriate for clients when the alternatives would require 100 percent state financing.
- ICF-MR regulations promote the use of large facilities because of economics of scale--some physical plant and staffing requirements make small ICFs-MR economically infeasible.
The Individual context of each state, however, appears to have been a major factor in determining response to FFP. For example, all three of the high-CBS states chose to depopulate PRFs and develop CBS as a major strategy for meeting ICF-MR standards and retaining FFP for their PRFs; the three low-CBS states, given the same options, chose to emphasize investments in PRFs.
Federal policies In special education, in particular the implementation of P.L. 94-142, also were seen as having promoted CBS orientation, although several informants noted differences in the degree to which MR/DD students, especially those with multiple handicaps, were Integrated with their nondisabled peers. There also were noticeable differences among the states regarding age ranges covered through the education system and services provided, given the latitude provided to the states in designing their approach to P.L. 94-142 implementation. The primary impact cited across the six states was the growing pressure to expand community services to meet the needs of special education students leaving school, and the increased activism of parents whose expectations have been raised regarding alternatives to institutionalization or total dependency on family members for activities and assistance.
The Supported Employment initiative was seen as promoting CBS development as well. The demonstration, training, and technical assistance opportunities were generally regarded as helpful in enhancing CBS orientation. It should be noted, however, that interest in supported employment was tempered in most of the states by observers who questioned its feasibility on a large scale.
(2) Influence On Service Organization And Administration
Federal policy was not considered a significant influence on the states' service organization and administration. Two exceptions noted were in the restriction of program responsibilities to the designated state Medicaid agency, and the difficulties in some states in developing consensus between the MR/DD and Medicaid agencies on how the Medicaid program can best be used for services to MR/DD individuals.
It should be noted that there are no Federal policies with extensive requirements for MR/DD service organizations and administration comparable to, for example, requirements in the Older Americans Act for both State Units on Aging (SUAs) and area agencies in aging (AAAs). The DD Act requirements for state DD Council composition and related state plan requirements, however, are somewhat analogous to the policies governing SUAs. As noted above, however, the Council's influence on the state system as a result of these policies is unclear.
(3) Influence On Client Eligibility
The primary Federal policy on client eligibility that was cited repeatedly was the requirement under the Medicaid program that limits eligibility to people in institutions, either because of parent-deemed income provisions or because needed services could only be reimbursed by Medicaid if provided as part of an ICF-MR program. Informants in all six states noted that families who wanted to keep even severely disabled relatives at home were frequently unable to do so because of the lack of resources and the ineligibility for Medicaid. It should be remembered that only two of the states have used the Medicaid Clinic services option to support habilitation services, with MR/DD adults in the other four states therefore having essentially no access to Medicaid services other than covered physical health care, unless they live in an ICF-MR or are served under the HCB Waiver.
The Federal DD definition appears to have had little effect on client eligibility. The primary service system in four of the six states is a mental retardation rather than a MR/DD system. In addition, it was clear from discussions with state informants that many of the mentally retarded people--primarily adults--who are already in the service system are mildly retarded individuals who may or may not meet the Federal DD definition.
Eligibility issues were raised by some informants regarding the interpretation of "need for active treatment" and of criteria for the SSI and the SSDI programs. The questions raised were generally focused on consistency in interpretation and the need to understand the relevant Federal policies rather than the impact of the policies themselves. Informants indicated that it was still too early to see if eligibility problems in the disability review process have been addressed with the recent changes. Finally, it should be noted that states have different eligibility criteria for different components of their MR/DD systems, with some components being more strongly influenced by Federal policy than others. For example, despite some differences among state agencies' administration of the Federal SSI and SSDI disability review programs, the eligibility for these programs is strongly influenced by Federal policy. In contrast, there are many MR/DD programs run by state agencies with little or no FFP, in which states set eligibility criteria virtually without Federal policy influence. The overall MR/DD service system includes many components with minimal Federal funding or regulation, such as the Michigan Family Support subsidy program. Even where Federal eligibility criteria exist, latitude in their interpretation frequently contributes to differences among, and even within, states as to who is served.
(4) Influence On Services
The ICF-MR program is the primary influence on the services being provided to MR/DD individuals. The emphasis on active treatment and the definitions of covered services were given mixed reviews by the states. On the positive side, most informants felt the concept of active treatment (as opposed to custodial care) was helpful in designing services, as is the emphasis on individual program planning. Restrictions against coverage of educational and vocational program services, especially when narrowly interpreted, were seen as having a negative effect on services design. Several respondents also noted the current confusion over the definition of active treatment. The policies permitting optional standards for ICFsMR under 16 beds were not mentioned as significant in shaping services.
The Federal policy Influence on who provides services appears to be minimal. Although Medicaid requires freedom of choice and that providers meet various standards to be certified, current policies do not seem to have affected the mix of public and private providers, for-profit and not-for-profit providers, or the level of competition; the extent and nature of private sector involvement has been shaped primarily by the individual state's policies and regulatory environment. For example, in three of the states, concerns were expressed that the state Medicaid agency's certification of large for-profit congregate care facilities was in conflict with goals for integrated community services.
(5) Influence On Financing
The primary Federal policy influence on financing has been the availability of FFP. It was clear that FFP is a factor in how states finance their MR/DD system, but clearly not the only factor or even necessarily the major factor. Even when Federal income maintenance funds provided to individuals are included, Federal funds represented less than 54 percent of MR/DD public expenditures--not including special education--in four of the six states. When SSI and SSDI are excluded, all six states fall below 50 percent use of FFP for their MR/DD system.
The Federal policy influence in rate-setting methodologies, primarily relevant to the Medicaid programs, was not explored. Concern was raised in general that some Medicaid policies increase program costs, as noted above. The HCB and model waivers were generally seen as more cost effective ways to finance services, although some informants noted financing constraints within the waiver regarding the interpretation of cost comparison formulas.
(6) Influence On Quality
Federal policy was widely considered to have a strong influence on program quality in the ICF-MR program, especially with the "look-behind" surveys. State ICF-MR review processes also influenced quality. However, the "look-behinds" also were a source of tension in some states over interpretations of Federal policy. Other Medicaid quality assurance efforts were mentioned by some informants such as the activities of the Regional Office (Region V) in reviews of skilled nursing facilities (SNFs) and Intermediate Care Facilities (ICFs) in Illinois which led to the identification of 2,800 to 3,000 inappropriately placed DD nursing home residents.
Other Federal policy influences on program quality and quality assurance mechanisms were not identified, although undoubtedly the DD Protection and Advocacy program, Section 504, P.L. 94-142, and other civil rights protections are a factor. States vary in the divisions of responsibility for quality assurance seemingly without regard to Federal policy requirements, with the exceptions of the state Medicaid agency designation.
2. Implications for Federal Policy
The analysis of state perspectives on the factors which influence their MR/DD systems and their implementation of CBS development objectives revealed various implications for Federal policy. Informants in all six states were forthcoming in their discussions of Federal policy influences, changes in Federal policy that were considered helpful to CBS development, and policies that they thought would inhibit such development. There was considerable consensus on these perspectives within individual states and across the six states. Although the description of the potential state responses to changes in Federal policy is, of necessity, speculative in nature, the relative degree of consensus on policy perspectives may indicate that the projected responses summarized at the end of this section are on target.
(1) Federal Policy Perspectives
Informants across the six states, including advocates for institutional and congregate care within the services continuum, were interested in Federal policy changes that would help their state expand its community services system. Most informants were particularly interested in policies that would promote the following: services which emphasize natural homes or homelike residences well integrated into the community; supports to families; and a full range of habilitation, education, developmental, and vocational services. There was widespread support for the following principles:
- Increased flexibility to states in the ways Medicaid can be used to support community services
- In-home services to severely disabled children that would not be dependent on model waiver procedures
- Coverage of appropriate educational and vocational program services (e.g., supported employment)
- HCB Waiver either continued indefinitely or made a regular optional program (although some informants were concerned that fiscally conservative policymakers would be less likely to pursue the HCB approach If It was for an optional program)
- Maintain or expand FFP
- Expand FFP availability for low-CBS states needing to develop services, at least over a short-term transitional period
- Stabilize FFP/increase state's ability to predict how much FFP will be available
- Some support for Medicaid "cap" in exchange for significant Increases in flexibility, despite opposition from advocacy groups to loss of entitlement and open-ended funding
- Some support for lower FFP rates for PRFs and other large facilities, support not limited to CBS advocacy groups, especially in low CBS states, as a necessary Incentive to shift emphasis to CBS
- Federal leadership
- Clarification/strengthening of support for CBS, especially in the Medicaid program
- Articulation of CBS goals and philosophy across Federal programs
- Clarification throughout the Federal-state Medicaid partnership network regarding the ICF-MR program and ways in which it differs from other long-term care services under Medicaid
- Shift from facility basis to client basis
- Reduction of conflicting program requirements/eligibility criteria between such programs as SSI/SSDI, vocational rehabilitation, special education, and Medicaid
- Support for services through the VR program that are more responsive to the needs of MR/DD individuals
- Continuing strong Federal presence in quality assurance
- Consistency among Regional Offices in program monitoring and interpretation of Federal policy
- Administrative consolidation within HCFA for MR/DD programs and policies
- Greater emphasis on cost-effective support to families that help avoid unnecessary institutionalization
- Technical assistance
- "State-of-the-art" services
- Manpower training in new technologies
- Training for surveyors and quality assurance program administrators
The Federal policy features accorded the strongest support and broadest consensus were increased flexibility and support for noninstitutional community alternatives, increased emphasis on help to families, strong Federal leadership, and maintenance/expansion of FFP.
Policies That Could Inhibit CBS Development
Informants in both high- and low-CBS states were generally optimistic that the kinds of Federal policy changes under consideration could be helpful in promoting CBS goals. Informants cited changes, however, which they considered likely to have a negative effect on CBS expansion. These included the following:
- Capped FFP--Although some informants expressed willingness to consider a cap in exchange for greater flexibility, others expressed concern that capped FFP for MR/DD programs could result in declining FFP over time, as has happened with Title XX/Social Services Block Grant funding.
- Reduced FFP--Informants in all six states expressed concern that FFP for MR/DD services should not be reduced, especially given the precarious position of the state economies.
- Elimination Of The HCB Waiver--All six states are in support of the kinds of flexibility offered by the HCB Waiver and are concerned that its elimination would impede further CBS development.
- Increased Fragmentation--Some informants recommended that policies which target services to specific population subgroups be avoided.
- Condemnation Of Congregate Care--Informants in low-CBS states, where large congregate care providers and/or PRFs have considerable political support, were concerned that policies which seem to condemn large MR/DD facilities would increase resistance to CBS development. Others in these states, however, indicated that the evidence on the merits of community services in smaller integrated settings required policy approaches that clearly favor this approach.
The Informants' primary concern was that trends toward increased flexibility and Individualized programming be continued without loss of Federal support.
(2) How States May Be Expected To Respond To Changes In Federal Policy
The analysis of state perspectives, in particular of the observations of informants in the low-CBS states, provided some indication as to how states may respond to changes in Federal policies affecting MR/DD service systems. Perhaps the most significant point emerging from the review of state perspectives is the following:
There was a strong general consensus that merely "tinkering" with Federal MR/DD policies will have little effect on states' ability to expand community-based services and to promote models that emphasize integration, productivity, and independence.
State responses to the kinds of changes in Federal policy under consideration by the Working Group that were further suggested by the analysis are summarized in the following.
- Overall emphasis on community services
- States will welcome Federal actions that facilitate expanded CBS with state policymakers, including philosophical direction, FFP, and technical assistance.
- Low-CBS states in particular would be able to use Federal leadership in promoting CBS growth by:
- Giving CBS supporters more "ammunition" (Federal standards, Federal policy statements, FFP that was available for CBS, etc.)
- Direct assistance in CBS development (demonstrations, technical assistance, fiscal incentives, support for CBS system development, etc.)
- It is not clear, however, if even radical changes in Federal policy would "turn around" a state which was determined to cling to large PRFs and other large congregate facilities (i.e., more determined than the low-CBS states visited for this study).
- Administration
- Effects on MR/DD system administration--overall division of responsibility and centralization vs. decentralization--are likely to be minimal unless new policies prescribed particular structures. Since there is considerable variety among states, as well as considerable history, prescriptive requirements would not be well received.
- States would generally support increased discretion in the governor's ability to delegate authority for some MR/DD aspects of the state's Medicaid program. This option would be particularly helpful to states in which the Medicaid long-term care program is .predominantly oriented to the needs of the frail elderly.
- States would welcome changes that brought more consistency in goals, target population, and specific requirements across such Federal programs as Medicaid, SSI and SSDI, Developmental Disabilities, Vocational Rehabilitation, Special Education, and Adult Basic Education. These efforts could be useful to states and communities In planning and monitoring their CBS systems and in developing more cost-effective service strategies.
- Client Eligibility
- The effect of Federal policy changes on client eligibility would depend on the use of mandatory client populations as well as the particular criteria selected. In states which do not generally include services to people with developmentally disabilities other than mental retardation, at least through the primary MR system, Federal mandates to include the full range of developmental disabilities would present significant problems in financing and system development.
- States are currently serving many mentally retarded people in their service systems, primarily adults, who may not meet DD definitions that focus on severity and/or inability to achieve gainful employment. If such clients were no longer eligible for services supported by FFP, many states could be expected to raise objections. This would be a particular problem in low-CBS states in which most of the people currently in their CBS system are higher functioning individuals; a major cutback in available FFP for these clients would mean other state resources would have to be used for this population rather than for new services for the moderately and severely disabled clients still in the PRFs.
- Most states also are already providing some services to families, including parent training, infant stimulation, respite care, Information and referral, and subsidy payments. Although some FFP Is being used, primarily through the HCB Waiver and P.L. 94-142 programs, most of these efforts are supported by state and local funds. A change in Federal program eligibility would therefore have more effect on the financing of services to DD people in their own homes, rather than change the overall scope of the population being served.
- Expenditures
- State's expenditures on their MR/DD systems are likely to be much more influenced by the state's economy than by Federal policy.
- Even if considerable new FFP were available, It Is unreasonable to assume that states will automatically increase their overall MR/DD expenditures or necessarily jump at FFP (although a few might be expected to do so). Most states are concerned about match requirements, open-ended obligations, and building up constituency expectations beyond what the state can afford in a period of economic difficulty. This is borne out by the observation that many states have not used Medicaid options for MR/DD services that are already available.
- Low-CBS states, especially those with troubled economies, may be unable to expand CBS and maintain quality PRF services simultaneously without short-term transitional assistance.
- Demonstration project funding may be helpful in supporting CBS innovations that can then be used as models throughout the MR/DD systems. Low-CBS states in particular may benefit from programs that validate community service models, such as small CRFs and vocational programs that integrate severely disabled adults into the community.
- Short-term demonstration project funding may be unattractive to some states if policymakers fear it establishes a level of support that the state will be unable to maintain after the demonstration funding is over. Demonstration funds that can be used for capacity building and system development might be useful to low-CBS states where key officials object to the usual kinds of demonstration grants.
- Many states are likely to use the HCB Waiver to expand CBS and alternatives to ICFs-MR. Changes in the HCB Waiver program, such as simplification of procedures and time-limited short-term developmental cost increases, would make the waiver even more useful, especially to low-CBS states.
- State SSI supplements are a major component of state-expenditures for CBS, especially in states which use non-Medicaid alternatives for community residences. States may be expected to raise this issue in response to policies which would pressure states to shift to non-Medicaid CRFs.
- State reactions to cost-sharing requirements will probably be mixed. Many states provide nearly all MR/DD services at no cost to participants, including family members, regardless of ability to pay.1 This is particularly true for families of adult MR/DD individuals whose freedom from financial responsibility for PRF and other service costs has been won in several states through the courts and hard-fought lobbying efforts. If cost-sharing were optional, states might be faced with difficult political battles with parents and other advocates. Mandatory cost-sharing provisions might be implemented with less political difficulty at the state level; however, the mechanics of cost-sharing and its monitoring would be seen as extremely difficult administratively in most states. Nevertheless, there is some state interest in cost-sharing as an appropriate strategy in financing community services.
- Services
- States could be influenced to raise the portion of MR/DD resources devoted to community services, especially if Federal policy changes are significant in shifting emphasis and support to CBS. Low-CBS states will probably require additional resources during the transition period to accomplish this, however, as they generally lack the CBS "infrastructure" to build on.
- Reductions in PRF population can be accelerated somewhat in low-CBS states, especially through combination of CBS growth and PRF depopulation incentives and help with system development. Some low-CBS states, however, are likely to continue their focus on expanded CBS for those who have never been in the institutions, especially in the absence of litigation on other strong pressures to deinstitutionalize.
- Services to families are likely to continue to expand, with or without major Federal policy changes. Federal policy will be significant in the extent to which states are able to expand family support more rapidly, and in their ability to capture FFP for these programs.
- States will be more likely to develop small non-ICF-MR CRFs if provisions like those currently found in the HCB Waiver are in place.
- Significant growth in the availability of vocational services and adult education programs is likely if reimbursement for these services under Medicaid extends beyond those covered by the COBRA amendments. Implementation also may present states with major turf battles as the MR/DD, Medicaid, VR, and education agencies sort out fiscal and administrative responsibilities.
- Increased emphasis/FFP availability could result in more providers being Involved and more choices available to consumers and payors. Because of the differences among states in their regulatory environment and degree of public vs. private dominance of the MR/DD system, however, the effects on provider makeup can be expected to vary considerably from state to state.
- States will welcome increased flexibility in the use of FFP, and can be expected to use this flexibility for more cost-effective services. At the same time, increased state flexibility could mean that some states will pursue goals other than those preferred by Federal policymakers.
- Quality assurance
- Most states can be expected to welcome strong Federal leadership in community services policy and to use it to gain support for CBS initiatives.
- States generally can be expected to support a continuing strong Federal presence in quality control, as in the "look-behinds," provided that quality assurance standards are clearly defined and communicated throughout the system on a timely basis.
- Major increases in state oversight requirements (for example, mandatory licensing of all providers receiving FFP under an HCB-like approach) would require extensive changes in many state systems, and also could increase costs significantly.
- Requirements that permitted only a single quality assurance (QA) organizational structure would cause difficulties in states with other models. For example, a mandatory separation of case management from service provision and administration would require extensive changes in states that currently require local MR/DD authorities to provide case management. At the same time, recognition of the issue of separation of oversight from services responsibilities might be useful to states in meeting appropriate goals for quality assurance, for example, if states were required to include independent program monitoring as a part of their QA system.
* * * *
Based on our analysis of influences on state MR/DD systems, it is clear that no single Federal policy approach will automatically lead to implementation of policy objectives for optimal productivity, independence, and integration of developmentally disabled people in their respective communities. States with relatively little CBS emphasis to date and with strong support for congregate care in large MR/DD facilities are likely to need considerable assistance--Federal leadership in the articulation of policy goals, FFP incentives for community services expansion, and technology transfer of cost-effective CBS program design--if their MR/DD systems are to progress significantly toward CBS policy goals. Federal policy also is one of several factors influencing state MR/DD systems. Although its influence can be considerable, it will continue to be limited in relation to the states overall policymaking context. It also is unlikely that current Federal policy approaches emphasizing devolution of authority to the states will be reversed in favor of prescriptive requirements for MR/DD service systems. Finally, it should be noted that state MR/DD policies are not implemented uniformly across the respective states; the influence of Federal policy on MR/DD services is further limited by the constraints on state-level control of its system at the community level, especially in states with decentralized MR/DD authority. Within these recognized limitations, however, Federal policy and programs can make a major contribution in CBS development. The six states reviewed in this analysis of MR/DD perspectives were clearly supportive of Federal leadership in MR/DD policy, and of an improved Federal-state partnership in cost-effective service systems. Their appreciation of being consulted by the Working Group through the activities of this study was indicative of the potential for a collaborative approach to implementation of MR/DD Federal policy goals.
IV. GLOSSARY
| CBS | - | Community-Based Services |
| CRF | - | Community Residential Facility |
| DD | - | Developmental Disability/Developmentally Disabled |
| FFP | - | Federal Financial Participation |
| HCB | - | Home and Community Based Care Waiver |
| HCFA | - | Health Care Financing Administration |
| HHS | - | Department of Health and Human Services |
| OSERS | - | Office of Special Education and Rehabilitation Services |
| ICF | - | Intermediate Care Facility |
| ICF-MR | - | Intermediate Care Facility for the Mentally Retarded |
| MR | - | Mental Retardation/Mentally Retarded |
| PRF | - | Public Residential Facility |
| SNF | - | Skilled Nursing Facility |
| SSI | - | Supplemental Security Income |
| SSDI | - | Social Security Disability Insurance |
| Title XIX | - | Title XIX of the Social Security Act--Medicaid |
| QA | - | Quality Assurance |
| CFLAs | - | Community and Family Living Amendments |
| CCBs | - | Community Centered Boards |
| ARC | - | Associated for Retarded Citizens |
| ASAs | - | Approved Service Agencies |
| PCAs | - | Personal Care Alternatives |
APPENDIX A: STATE PROFILES
COLORADO MR/DD SERVICE SYSTEM
I. Overview
Background
Colorado has a population of 3.2 million. There is a large urban concentration in the Denver area, but the state also has many isolated rural areas. Colorado has recently had significant economic and population growth, but is currently experiencing severe economic problems. The state has traditionally been politically conservative.
System Characteristics
Colorado's MR/DD service system places strong emphasis on community based services. The statement of philosophy of the lead state agency for DD services cites normalization, integration, personal autonomy, and individualization as guiding principals. The general consensus among respondents was that Colorado has made substantial progress in deinstitutionalizing the DD population and in establishing community-based services.
Colorado's service delivery system is characterized by a high degree of decentralization and local autonomy. Most services are funded through the state Division for Developmental Disabilities, but are developed and administered by local service entities--the Community Centered Boards (CCBs).
Colorado uses Title XIX extensively for both institutional and community services. However, ICF-MR supports only the PRFs and six large private facilities. All other Medicaid-supported DD services are financed through the HCB Waiver.
Issues in Community Service Development
Although Colorado's MR/DD service system is oriented toward community services, there are number of issues to be resolved for the further expansion of community-based services. The major issues include:
- An overall lack of resources at both the state and local levels
- Conflict about the appropriate roles of the various actors in the system
- Inadequate community services for hard to serve clients
- Inadequate family support
Federal Policy Perspectives
Most recommendations for Federal policy changes focused on Medicaid reform:
- Nearly all respondents expressed strong support for CFLAs
- Several respondents suggested making waiver services optional services under the state Medicaid plan
- In general, respondents want Medicaid to be more flexible in meeting individual needs
II. Service System Profile
Major Actors in the MR/DD Service System
Division For Developmental Disabilities (DDD)
DDD, located within the Department of Institutions, is responsible for the operation of the 3 state PRFs (Regional Centers), planning and policy development, and funding of the CCBs--the local service entities. The agency performs annual quality assurance reviews of CCBs and must designate providers as "Approved Service Agencies" (ASAs) before they can receive state funds. DDD also contracts directly for a limited number of community-based programs.
Developmental Disabilities Planning Council
The DD Council, also located in the Department of Institutions, is responsible for developing the state DD plan, analysis of issues and programs affecting DD services, and fostering interagency cooperation and coordination. In addition, the DD Council provides some seed money for innovative projects, but does not concentrate on funding or providing direct services.
Department Of Education--Special Education Services
Colorado requires the public school system to provide special education services to all handicapped children ages 5 to 21. The state Special Education Services Division oversees local school districts' special education programs, provides technical assistance and funding, and develops policy. Special Education Services also is involved in interdepartmental efforts to expand supported employment initiatives and to improve support services for the transition from special education to adult life.
Department Of Social Services (DSS)
The Bureau of Medical Programs within DSS is responsible for administration of the private ICF-MR program and rate-setting for the PRFs (which are ICF-MR certified). DSS also administers other programs such as foster care that affect DD individuals.
Division Of Rehabilitation
The Division of Rehabilitation, within the Department of Social Services, provides rehabilitation and vocational services for handicapped individuals, including the MR/DD population. Rehabilitation is placing increasing emphasis on serving severely disabled individuals. The Division also is heavily involved in supported employment initiatives.
Department Of Health
The Department of Health surveys and licenses all residential programs for the MR/DD population--PRFs, ICFs-MR, nursing homes, and community residential facilities--on an annual basis. DDD and the Department of Health conduct joint surveys of community residential programs.
Community Centered Boards (CCBs)
The 22 CCBs are nonprofit, quasi-governmental bodies responsible for providing services to the MR/DD population. CCBs are the single point of entry into the DD system. State law in essence gives CCBs a "franchise" to provide services in individual catchment areas and requires them to do planning and provide case management. Most also provide services directly, in addition to contracting with private sector providers. The balance between direct contract services varies greatly among CCBs. There also are no uniform requirements as to their board composition and governance structure; each is an independent 501C3 corporation. CCBs are responsible for monitoring and quality assurance of their own and contracted programs.
Interagency Cooperation
Nearly all respondents reported that cooperation at the division level is excellent; most attributed this to strong leadership from division directors. For example, DDD, the DD Planning Council, the Division of Rehabilitation, and Special Education have worked closely together to develop the Rocky Mountain Training Institute which will train providers to develop supported employment initiatives. However, some respondents indicated that cooperation between DDD and the CCBs, and between CCBs and private providers, is not as effective.
Association for Retarded Citizens (ARC) - Colorado
The ARC in Colorado acts as an advocate for mentally retarded individuals on both the local and state level. Local ARC chapters are not extensively involved in service delivery, but have chosen to concentrate on advocacy activities.
Institutional Services
- DDD operates 3 Regional Centers for DD individuals:
- All are ICF-MR certified.
- Current census is 923 (5/5/87).
- Population in the Regional Centers has declined from approximately 1,600 in 1976
- DDD plans to reduce the Regional Center population to 835 by September 1987.
- Six private ICFs-M R:
- Approximately 346 DD people reside in private ICFs-MR.
- Average size is 58 beds, with a range of 40-87 beds.
- Providers are both for-profit and non-profit.
- Private ICFs-MR contract directly with DSS and are licensed by the Department of Health.
- Nursing homes:
- In 1986, 510 DD people resided in general purpose nursing homes.
- A 1984 DDD study found that approximately 68 percent of DD people in nursing homes were inappropriately placed.
- Most respondents agreed that clients served in institutional settings are generally those considered harder to serve than those served in the community:
- Approximately 88 percent of clients in PRFs have multiple handicaps. In comparison, only 33 percent of CCB program clients have multiple handicaps.
- Residents of the PRFs are more likely than community DD residents to have medical problems or emotional/behavioral disorders.
Community Services
Most community-based services are provided through CCBs, either directly or by contract with other ASAs. DDD also contracts directly with some providers for community services.
Community Residential Programs
The community residential system serves approximately 2000 people in a variety of settings: follow-along supervision, minimum and moderate supervision group homes, intensive developmental group homes, social/emotional group homes, and behavior management group homes.
Personal Care Alternatives (PCAs) are waiver-financed residential services. The objective of the PCA program is to allow DD individuals to establish homes in the community rather than having them "progress" through a series of facilities. There are three PCA residential models, with staffing varied to meet individual needs. The host home model employs a family to have a DD person live in its home. In the peer companion and independent apartment models, the client lives with a disabled or nondisabled person, and receives the necessary degree of support services.
Foster Care
- Approximately 130 DD children live in DDD-funded foster homes.
- Approximately 415 DD children live in DSS-funded foster care. This number includes both voluntary and court-ordered placements. DDD and DSS would prefer not to serve DD children in the regular foster care system.
Non-Residential Services
Respite Care
- Respite care services include short-term living arrangements to deal with family or provider crises, as well as periodic family relief.
- Several respondents reported that respite services are limited.
Case Management
- Recent legislation designated case management as an entitlement for all DD people.
- CCBs are the designated case management provider and must provide a determination of eligibility and development of an Individual Habilitation Plan.
- Case management services are funded by DDD, but CCBs claim that they provide case management to more people than they are funded for.
Supported Employment
- Supported employment is currently the major priority for vocational programs for MR/DD people. DDD has set a statewide objective that 25 percent of the persons served in adult day services be served in supported employment by January 1988.
- DDD, the DD Council, Special Education Services, and the Division of Rehabilitative Services have worked together to develop the Rocky Mountain Training Institute. Initially funded through Rehabilitation and DDD, the Institute will train providers, educators, and employers to expand supported employment services. Colorado has been approved for an OSERS grant to continue the project.
Early Childhood Intervention
- The Department of Education oversees services to more than 3000 preschool-aged handicapped children and their families.
- In FY 1985, 640 children participated in the infant stimulation program, and 1035 DD children participated in the preschool program. DDD currently funds the early childhood program (services are provided through CCBs), but the Governor has designated the Department of Education as the lead agency to implement P.L. 99-457. DDD expects to transfer authority for the early childhood program to the Department of Education next year.
Family Support
Respondents indicated that in-home services and other supports to families are very weak. Family support is currently limited to a project which includes 50 families.
General Financing and Service Development Issues
Financing Of Community Services
Federal Funds
- Medicaid is the major source of Federal funding for MR/DD services. Medicaid funds community based services through the HCB Waiver.
- SSI payments and other Federal income transfer payments provide an average of approximately 21 percent of program costs for community residential programs.
State Funds
- DDD's FY 86 budget devoted approximately 65 percent to community services.
- FY 86 combined state and Federal expenditures for community services were approximately $51.7 million.
- State expenditures for community services were $38 million in FY86.
- Between FY 1977 and FY 1986, Federal and state expenditures for community services increased by 57 percent in constant dollars.
Local/CCB Funds
- The CCB match requirement for state funds is 5 percent. However, on a statewide basis, CCB and local funds provide approximately 27 percent of funds for community services.
- Some CCBs receive county or municipal funds, and also may supplement state dollars with fundraising, foundation grants, United Way funds, etc. There is tremendous variety among CCBs in funding sources and percentage of local vs. state funds.
ICF-MR Program
In FY 1985, approximately 1000 clients resided in ICF-MR facilities (including the three Regional Centers). State and Federal ICF-MR expenditures were approximately $47 million. Colorado does not use the ICF-MR program to finance small community residences.
Home And Community Based Care Waiver (HCB)
Colorado has pursued the waiver aggressively. Several respondents reported that the initial effect was the refinancing of small ICFs-MR, which were converted to Waiverfinanced facilities. Services financed under the Waiver include case management, habilitative day and residential programs, respite care, personal care, and non-medical alternatives. DDD reports that it will soon "reach the limit" with the Waiver; further expansion of Waiver-financed services will be limited to people leaving the Regional Centers. The state will no longer be able to use the Waiver to address the needs of people on community waiting lists.
CBS Development Costs
DDD does not provide initial capital funds, so CCBs or private providers must usually find money to cover startup costs. However, capital costs are usually factored into the reimbursement rate. One respondent suggested that funding development costs would tend to encourage dependence on segregated, facility-based service models.
III. Experience With and Development of CBS
Development of CBS in Colorado
Community services and the CCBs originally started during the 1960s as alternative schools for DD children and sheltered workshops for DD adults. The CCBs developed expertise in serving the MR/DD population and were available to develop new services when Colorado began to deinstitutionalize DD people from the Regional Centers. In addition, services available through the CCB network enabled the majority of DD people to remain in their home communities.
In response to the 1975 ICF-MR regulations, DDD chose to reduce the size of the Regional Centers' population rather than invest all resources in the institutions. The current array of community services was expanded to meet the needs of clients coming out of institutions. However, extensive physical plant improvements were required to bring the Regional Centers into compliance with the regulations.
Several factors played an important role in encouraging the development of community services in Colorado. The state's conservative political ideology, emphasizing ideals of individualism, family strength and independence, and local autonomy, complemented the move to CBS. Community service advocates have been able to effectively connect the goals of community services for MR/DD people with the state's broader value system. The favorable economic circumstances of the 1970s also contributed to the development of CBS. The economic climate has worsened, but respondents felt that the need to develop low-cost alternatives will continue to encourage community services.
Current Emphasis on CBS
The consensus among respondents was that Colorado has made significant progress in developing and operating community services. Client and budget data support these perceptions. Although Colorado has developed a wide array of community-based services, interviewees did point out areas where improvement is needed, including:
- There are waiting lists for residential services in all areas of the state.
- Young adults who have left special education programs have difficulty gaining access to services.
- Most respondents agreed that appropriate community services for medically fragile clients are inadequate. Several respondents expressed concern about the adequacy of backup services and medical care for severely disabled clients in community settings.
- Many community providers, to date, do not have personnel who are trained to deal with behaviorally disturbed clients. People with challenging behaviors are the major source of requests foe admission to the state operated Regional Centers.
- Several respondents noted that respite care and family support services are "in their infancy."
- The quality and comprehensiveness of services varies greatly throughout the state.
Goals for CBS/Issues to be Resolved
Nearly all respondents cited similar objectives for the further development of community-based services in Colorado. The state will continue to reduce the population in the regional centers, with a long-term goal of phasing out the Regional Centers. Most respondents agreed that future development should emphasize nonfacility-based services such as personal care alternatives, supported employment, and family support services. Support for nonfacility-based services was based on both programmatic and fiscal interests. Avoiding capital investments in facilities and promoting the use of generic services may reduce program costs. Developing services which are tied to client needs rather than to facilities will allow greater flexibility and individualization of services. Cost containment and individualization of services were both cited as important goals.
Although most respondents were in agreement about the major goals for Colorado's MR/DD system, there was some debate about the most appropriate methods for implementing the goals, as well as about the appropriate roles and responsibilities of the various actors involved in the system. For example, several respondents questioned the independence and effectiveness of CCB-provided case management because of CCBs' major role in direct service delivery. There also seems to be tension between private providers and CCBs (e.g., over CCB control of admissions to private facilities).
IV. Federal Policy Perspectives
Incentives and Barriers
Colorado has been successful in using Title XIX funds to develop and operate community-based services. The availability of the HCB Waiver enabled and encouraged the state to expand community residential programs. By using the waiver so extensively, Colorado has avoided some of the problems other states have experienced in using ICF-MR to fund small residential programs. However, respondents cited a number of Federal policy problems which act as barriers to community services, including:
- Current Medicaid policy offers families financial incentives for out-of-home, institutional placements.
- Medicaid does not have an overall MR/DD policy: ICF-MR program requirements do not reflect the true service needs of the population.
- One official noted that the "guerilla warfare" between HCFA and the states is unproductive and does not offer a good environment for planning or delivering services.
Policy Recommendations
Many suggestions for Federal policy changes focused on reform to make Medicaid funding for MR/DD services more flexible and oriented toward Individual needs. For example:
- Nearly all respondents expressed qualified support for the CFLAs as a means to correct the institutional bias in the ICF-MR program.
- Several respondents suggested creating a unit in HCFA specific to DD and community services.
- A few respondents would favor a block-grant approach to funding MR/DD services. However, support for this approach was tempered by concerns about the possibility of future budget cuts.
- Several respondents suggested making the services that are available through the HCB Waiver optional services under the state Medicaid plan. This suggestion is motivated by concerns about the temporary nature of the Waiver.
In addition to suggesting changes in the Medicaid program, respondents also commented on broader policy issues which require a strong Federal role. For example:
- Consistency in eligibility, service definitions, and program standards across all programs is needed.
- Federal attention to the broader issues of health insurance coverage for disabled people will be helpful.
- Respondents also emphasized the need for national policies on disability issues and in support of community integration for DD people.
V. Summary
General Observations
Colorado clearly has made a definite commitment to community services: all respondents were in accord with the ideals of community integration for DD people. The development of community services was greatly aided by the ability of advocates to link their cause with the state's political value system.
The degree of decentralization and high level of local autonomy have been important features of Colorado's MR/DD system. The current trend appears to be toward a greater degree of central control. DDD has become more directive, as well as more stringent with the monitoring process, and seems to be attempting to ensure consistency of goals and service quality throughout the state. However, CCBs' resistance to central control may be increasing, particularly regarding the separation of case management from service delivery. CCBs want to continue to provide services directly and do not wish to serve as a planning or case management agency.
Federal Policy Implications
Colorado's extensive use of Title XIX to fund community services presents opportunities for Federal policy to influence the future development of the community services system. Because Colorado's policy and, to a great extent, actual programs are consistent with the objective of community integration and independence for MR/DD people, the influence of Federal policy could be to encourage Colorado to continue in the direction it has already taken and to stimulate the development of those community services (e.g. respite care and family support) which are not in place. However, the independence and diversity of the CCBs could limit the ability of Federal policy to influence actual community-level program implementation in Colorado.
| EXHIBIT A-1: Colorado MR/DD Service Delivery System |
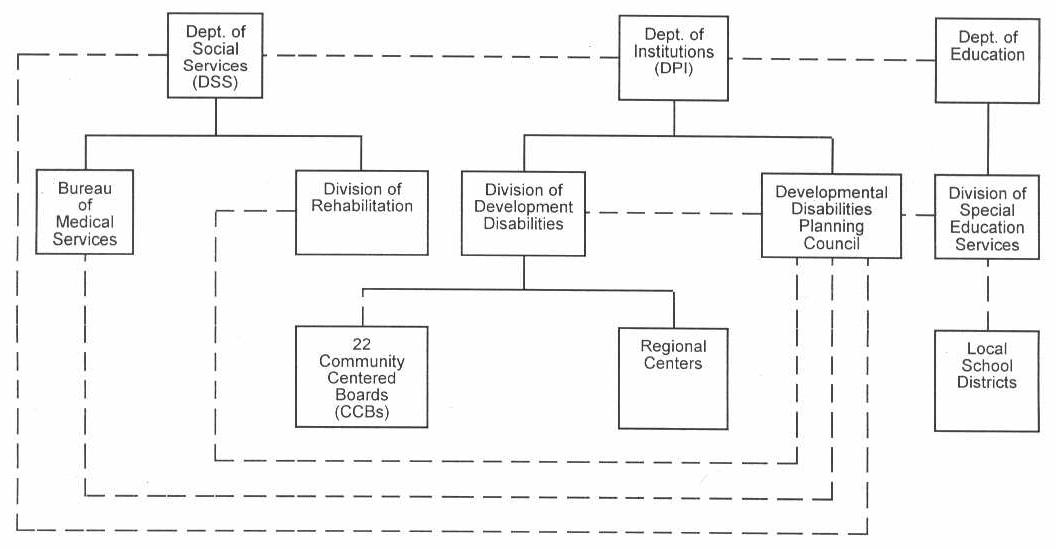 |
State Agency Representatives on DD Council:
Solid lines represent direct authority and oversight Broken lines represent coordination, communication, or indirect or limited authority |
Colorado Site Visit - Interviews
Gary Smith Deputy Director, Division for Developmental Disabilities
Jeff Strully Executive Director, ARC - Colorado
Brian McNulty Director of Special Education, Colorado Department of Education
Anthony Francavilla Rehabilitation Administrator, Division of Rehabilitation
Jane Covode Executive Director, Colorado Association of Community Centered Boards
William Gorman Director, Colorado Developmental Disabilities Planning Council
Margaret Stauder Good Shepard Lutheran Home
Charlie Allinson Executive Director, Community Options, Inc.
Source Documents
Colorado Department of Institutions, Division for Developmental Disabilities. 1986 - 1987 State Plan.
Colorado Department of Institutions, Division for Developmental Disabilities. Rules and Regulations, 2CCR 503-1.
Colorado Department of Institutions, Division for Developmental Disabilities.
Colorado Department of Institutions, Division for Developmental Disabilities. FY 1988 Budget Request and Summary.
Colorado Developmental Disabilities Council. Three-Year State Plan, 1987-1989.
Colorado State Board of Education. Status of K-12 Public Education in Colorado, 1986.
ILLINOIS MR/DD SERVICE SYSTEM
I. Overview
Background
Illinois has a population of 11.4 million with large urban areas surrounding Chicago and St. Louis, MO. The state has major industrial development, but a large part of the state is rural. Illinois economy has been adversely affected by both the farm crisis and the decline of the industrial base.
Major System Characteristics
Illinois MR/DD system places strong emphasis on congregate care--large public residential facilities, large private ICFs-MR, and nursing homes. Illinois uses Title XIX to finance the majority of residential services through ICF-MR and, to a lesser extent, the Waiver.
The service delivery system is centralized; there is no statewide local service entity or MR/DD authority. Regional offices of the state MR/DD agency have been closed as part of the agencys austerity program. Private providers, both non-profit and proprietary, play a key role in service delivery.
Issues in Community Service Development
Respondents agreed that the major problem in Illinois MR/DD system is an overall lack of appropriate community-based services, including all types of services and for all types of clients. There are several major barriers to the development of a more extensive network of community-based services: the high level of investment in large residential facilities; the political influence of private providers and nursing home operators; and the institutional bias of the ICF-MR program. The availability of the Waiver has provided some incentives for community services development, but Illinois has not used it extensively.
Recommended Policy Changes/Federal Policy Implications
The majority of policy recommendations and observations focused on Medicaid reform to encourage the development of community-based services. Respondents most often suggested using ICF-MR reform as an incentive for states to increase community services rather than as a punishment for states who have not already done so.
There is potential for Federal policy changes to have an effect in Illinois because of the centralized decision making structure and the state's dependence on the ICF-MR program to fund services.
II. Service System Profile
Major Actors in the MR/DD Service System
Department Of Mental Health And Developmental Disabilities (DMHDD)
DMHDD is responsible for the administration and operation of the nine state-owned institutions for the developmentally disabled. DMHDD also manages the contracts for all privately-operated, DMHDD-funded programs, including residential and day programs. The Department recently eliminated regional offices which were previously responsible for contract administration and case management for some clients; DMHDD's central office has assumed these responsibilities. Policy development, budget preparation, and overall quality assurance also occur at the state level within DMHDD.
Governor's Planning Council On Developmental Disabilities
The DD Council is administratively located within DMHDD, but is effectively independent and relates primarily to the governor's office. The Council includes representatives from: the general public; DMHDD; the Departments of Public Aid, Public Health, and Rehabilitative Services; Children and Family Services, the State Board of Education; and the Division of Services to Crippled Children. DDPC is primarily responsible for policy analysis, advocacy, and interagency coordination around issues such as supported employment and transition for young adults aging out of special education. The Council also is actively involved in providing technical assistance to DD providers regarding preparation for HCFA look-behinds.
Department Of Public Aid (DPA)
DPA administers a variety of programs affecting MR/DD people. DPA's Bureau of Long-Term Care is responsible for rate-setting and Inspection of Care for all ICFs-DD (Illinois' term for ICFs-MR), ICFs, and SNFs. (The Department of Public Health is responsible for licensing of all ICFs-DD and SNFs/ICFs.) DPA also administers services that are not specifically directed toward the DD population, but which are important programs for MR/DD people (e.g. SSI).
Department Of Rehabilitative Services (DORS)
DORS provides rehabilitation services to the entire disabled population based on the degree of functional impairment and the potential for independent employment. DORS is the administering agency for Federal Vocational Rehabilitation (VR) funds. However, vocational rehabilitation is only one component of DORS programs and VR funds make up only about one-third of the agency budget. Other divisions include Home Services, Services to Children, and Services to the Blind. DORS works with public school special education programs, beginning with students at about age 15, to provide independent living training and work experiences. DORS also is involved in the supported employment initiative.
Other State Agencies
The Department of Children and Family Services (DCFS) and the Division of services to Crippled Children (DSCC) also provide services relevant to the MR/DD population--licensing of residential facilities, foster care, and medical services.
Local Government Involvement
There are three possible mechanisms through which county governments may become involved in MR/DD services: "377 Boards" for public health services; "553 Boards" for services for "mental deficiency;" and 708 Boards for community mental health services. Formation and funding of these boards is optional. From a statewide perspective, the role of the county service boards is very limited. However, county service boards are significant in some areas of the state, especially in the southern, rural counties. The local government role in direct service provision is limited by requirements that a county service board "spin-off" programs to other providers after the startup period.
Interagency Cooperation
Respondents reported that the various state departments and agencies are involved in many joint projects and planning processes. For example:
- DORS and DMHDD are working together on supported employment, and also are working to clarify responsibilities regarding vocational services.
- DMHDD, DORS, and the State Board of Education are cooperating to improve transition services for students graduating from specially education.
- DDPC and DPA provide joint technical assistance services for DD facility operators.
- DDPC, DMHDD, and the State Board of Education operate pilot early intervention projects for DD children younger than 3 years.
- Respondents indicated that DPA's goals for the ICF-MR program are not always consistent with other agencies goals (e.g., regarding community Integration and least restrictive environment)
Private Sector Involvement
Private sector providers--both proprietary and non-profit--are an integral part of the Illinois' MR/DD service system. Nearly all services outside the PRFs are provided through private facilities and agencies. Local ARC chapters are frequently involved in service operation and ARC-Illinois often is perceived as a provider representative rather than primarily as a client advocacy organization.
Institutional Services
DMHDD operates nine public residential facilities which range in size from 100 to 800 beds. The state-operated institutions serve a total of approximately 4,500 clients. All beds are either ICF-MR or SNF certified. In addition to the 9 PRFs, approximately 4,200 clients reside in large private ICFs-DD. Most PRF beds are ICF-MR certified, but several facilities, both public and private, were temporarily decertified on look-behinds. DMHDD decertified one PRF voluntarily. (The Department of Public Health is responsible for licensing and certification of ICFs-DD and nursing homes. DPA conducts Inspections of Care.)
Approximately 3,000 DD people live in SNFs and ICFs. According to the DDPC, approximately 2,800 of these nursing home residents are inappropriately placed and are not receiving the necessary habilitative services. SNF-Pediatric facilities serve 1,000 clients, some of whom are over the age of 22. Severely disabled children also reside in Child Care Institutions which range in size from 50 to 100 beds. Approximately 600 DD children live in these facilities, which are licensed by DCFS and funded by DMHDD.
Most respondents indicated that residents of both public and private institutions are generally hard to serve clients with severe mental retardation, multiple handicaps, behavior disorders, or dual diagnosis of mental illness and mental retardation. However, some severely disabled and hard to serve clients are participating in community programs, and several respondents noted that many institutional residents could be served in the community. Although Illinois has not yet been able to significantly reduce the population in large institutions, DMHDD personnel pointed out that they have been able in recent years to prevent admission of children to the state operated facilities.
Community Services
Residential Services
Although Illinois has developed a range of residential and non-residential services on the community level, the emphasis--in terms of both expenditures and client placements--is clearly on institutional settings.
The range of options and number of clients residing in less restrictive community settings has increased significantly over the past decade. Community residential programs funded by DMHDD include:
- Home Individual Programs (HIPs) serve no more than 2 clients in each program. In FY 1987, approximately 160 clients resided in HIPs.
- Community Residential Alternatives (CRAs) are group homes for no more than 8 adults. CRAs serve approximately 700 clients.
- Community Living Facilities (CLFs) are large group homes which serve an average of 20 adult clients. CLFs serve a total of approximately 700 clients.
- Childrens Group Homes, facilities of 5 to 10 beds, serve approximately 100 DD children.
- Supported Living Arrangements serve more than 1,000 DD people.
- Special Home Placements--foster care homes for adults and children serve approximately 100 DD people. One of the fastest growing areas is ICFs-DD for 15 or fewer people. Approximately 400 clients currently reside in small ICFs-DD. DMHDD personnel reported that 400 new beds in the ICF-MR 15 category are under construction and another 200 are awaiting Certificate of Need approval.
Non-Residential Services
Case Management/Case Coordination
DMHDD funds case management services for approximately 8,600 clients through 72 provider agencies throughout the state. With the exception of only one agency, all case management providers operate other services for DD people as well. DMHDD plans call for movement toward an independent case management system.
Day Programs
- Developmental Training I and II programs (DT I and DT II) provide training in functional skills for daily living, and also provide functional skills training. DT I and DT II are funded by DMHDD, DPA, and local education agencies, and serve more than 1,200 DD clients.
- Vocational Development programs involve time-limited services directed toward placing clients in competitive employment. Vocational Development, funded by DMHDD and DORS, serves approximately 2,400 DD people.
- Regular Work programs offer sheltered employment for clients who are judged to require a high degree of supervision. DMHDD and DORS fund Regular Work programs for approximately 6000 clients.
- The supported employment demonstration project funded through DORS serves approximately 300 adults throughout the state. DMHDD also funds supported employment projects.
Home Services
DORS administers a Home Services program for people with disabilities, including some MR/DD people. Services include personal care aides, home health aides, nurses, and respite care. The program serves disabled people from birth to age 60 with the objective of allowing people to remain in their own homes. State general revenue funds support the Home Services program.
Respite Care
DMHDD funds approximately $4 million In respite care services through general funds and the Medicaid waiver.
Family Support
DMHDD funds client and family support services for approximately 7,000 DD people and their families.
Early Intervention
DMHDD, the DD Council, and the State Board of Education operate early intervention programs for 6,500 DD children from birth to age 3.
General Financing Service Development Issues
ICF-MR Program
Illinois depends heavily on Title XIX for funding residential services. ICF-MR funds PRFs, large/medium sized private ICFs-DD, and small private ICFs-DD. Illinois ICF-MR, ICF, and SNF rates are among the lowest in the nation. HCFA look-behinds have found significant deficiencies, particularly in regard to lack of active treatment, in Illinois facilities--both public and private. However, most respondents described the look-behinds as "the best thing that could have happened." After HCFA personnel identified areas and facilities with serious deficiencies, the possibility of decertification and loss of Federal funds spurred the legislature to appropriate the funds needed to correct the deficiencies.
Waiver Experience
Illinois implemented its HCS Waiver in FY 1985. The primary purpose of the Waiver was to begin to reduce the population in state operated institutions. Illinois has been unable to use its Waiver to the extent anticipated; the Waiver was approved for 1,500 people but currently serves only 648 people. Respondents offered several explanations:
- Zoning problems at the local level
- Public resistance to community residential programs
- Lack of startup funds and technical assistance
Services provided under the Waiver:
- DT I and DT II
- Case management
- Respite care
- A variety of residential options: Special Home Placements, CLFs, CRAs, and HIPs
- Habilitation services
Although the Waiver has not been used to the fullest possible extent, respondents from DMHDD felt that it has been beneficial:
- Some people have moved out of the institutions.
- Providers have gained experience serving more disabled clients.
Illinois has applied for a renewal of its Waiver. The new Waiver will provide case coordination, deinstitutionalization, and relocation of people in SNFs and ICFs. DD people living in their family homes also will be eligible.
One respondent commented that it will be difficult to get people out of SNFs, ICFs, and large ICFs-DD with the Waiver because the reimbursement rates in these facilities are so low that the cost of community services for these clients would be higher than costs in ICFs-DD and nursing homes, and the Waiver requires cost saving or cost neutrality on an individual basis.
The Division of Services to Crippled Children administers a waiver for medically fragile, technology dependent children. This waiver provides home health and other services as an alternative to hospital or SNF care for approximately 60 severely disabled children.
CBS Development Costs
In general, DMHDD and Title XIX do not cover initial capital costs, so potential providers must finance initial startup costs through other means (e. g. bank loans). However, reimbursement rates do include the costs of repayment of such loans.
III. Experience with/Development of CBS
Development of CBS in Illinois
All respondents characterized Illinois as a "congregate care state" and agreed that Illinois has not made significant progress in establishing a comprehensive and extensive network of community-based services for MR/DD people. Most of the development that has occurred has been limited to a few areas of the state. However, the HCB Waiver did provide some impetus and a framework for CBS development:
Respondents attributed Illinois' failure to develop CBS to a variety of factors:
- Lack of a strong philosophical commitment to community services at either the state or community level
- Lack of unified, grassroots advocacy for community services--families have not pushed for community services
- No Federal court involvement (although the ARC and other advocates are now considering a possible class action suit)
- Strong opposition from pro-institution parents, unions, communities
- Influence of a very strong and effective provider lobby
- Absence of a local delivery system, and no tradition of local government involvement in human services
- General lack of resources--budgetary priorities have been in other areas
Most respondents felt that some of these problems were beginning to lessen, creating a better environment for expanding community services. For example, the leadership at DMHDD is committed to the development of more community services.
Gaps in CBS
The general consensus among respondents was that the major gap is an overall lack of appropriate community services for the MR/DD population, rather than any particular services. Several respondents noted that even when an array of services is available at the community level, gaining access to services is difficult because there is no single point of entry into the system. Specific problem areas mentioned include:
- Residential options of all kinds
- Case management/coordination
- Day programs--especially for young adults exiting special education
- Programs for hard-to-serve clients (e.g. behaviorally impaired and dually diagnosed)
- Great variation throughout the state in quality and availability of services
- DMHDD and DPA eligibility criteria do not all include all nonmentally retarded DD individuals
Goals for CBS/Issues to be Resolved
Most respondents agreed that the major goals for the future development of CBS include:
- Implementation of a service model with independent case management as the core
- Expansion of case management services
- Expansion and improvement of supported employment, family support services, and transition from school to work
- Relocation of MR/DD people in SNFs and ICFs
- Compliance with Federal ICF-MR standards
Factors that will affect the achievement of these goals include:
- The ability of advocates to broaden the base of public support
- Obtaining necessary resources, in particular the legislature's support for CBS appropriations and initiatives
- Ability of agencies to work together
- A state legislative mandate for community services
- The state's economy
IV. Federal Policy Perspectives
Incentives and Barriers
Several respondent's expressed the view that ICF-MR's bias toward institutional settings (e.g., restrictive standards for small facilities) has encouraged Illinois to continue to rely on large public and private facilities. The degree to which the institutional nature of the Illinois ICF-MR program results from Federal requirements or DPA interpretations of those requirements was unclear. The expenditures required to meet ICF-MR standards and implement plans of correction, as well as the high level of financial and emotional investment in congregate care facilities, act as a barrier to developing community services. In addition, the political strength of the provider and nursing home lobby has discouraged Illinois from expanding community-based services. Respondents felt that the waiver has been helpful in providing an incentive for community services.
Policy Recommendations
Most suggestions for Federal policy changes pertained to Medicaid reform:
- Nearly all respondents acknowledged that supporting CFLA or any other option that would reduce money spent on institutional care would be politically difficult because of the high level of investment in institutions and the strength of the provider and nursing home lobby.
- Most respondents suggested establishing some type of differential reimbursement for community services, creating an incentive to expand community services.
- Several people stressed that Federal policies which are punitive or state that congregate care is wrong would only succeed in mobilizing opposition to community services.
- Several respondents would support separation of MR/DD services from the rest of Medicaid.
- DMHDD and DPA personnel suggested that HCFA finalize the new ICF-MR standards and make a clear statement supporting the use of Title XIX for small facilities. Another interviewee suggested that habilitation be defined to include vocational services.
Other comments on Federal policy included:
- Eligibility definitions should be more consistent across programs and should be clarified.
- Programs should not be separated by disability--this only creates competition for limited resources among disability groups.
- Long-term planning for programs with any amount of Federal financial participation is often difficult because state agencies do not know what their appropriation will be from year to year. The official who made this comment suggested that the level of FFP be guaranteed when programs are authorized.
V. Summary
General Observations
- Illinois' dependence on large institutions and the political strength of community service opponents will continue to slow the development of community services. Significant change is unlikely to occur without some external encouragement.
- Although Illinois has long-standing emphasis on large facilities, the system has started to move toward community services. All respondents were very supportive of the concepts of community integration, individualized services, etc. With the exception of the supported employment initiative, interest seems to be focused on facility-based services and the ICF-MR program.
- The centralized nature of the service delivery system may increase the state's opportunities to implement major policy changes.
Federal Policy Implications
- The heavy use of Medicaid provides opportunities for Federal policy to influence change in Illinois. The absence of a strong local government role is problematic: Federal policy decisions would not be diluted by another level of implementation/interpretation, but the lack of local community input into and ownership of programs could impede effective service delivery.
- Federal policy changes which threaten to reduce FFP, or explicitly or implicitly condemn the choices Illinois has made, will probably not be helpful, and will only succeed in raising opposition.
- The strong support for HCFA look-behinds underlines the importance of an effective Federal "watchdog" role.
| EXHIBIT A-2: Illinois Service Delivery System |
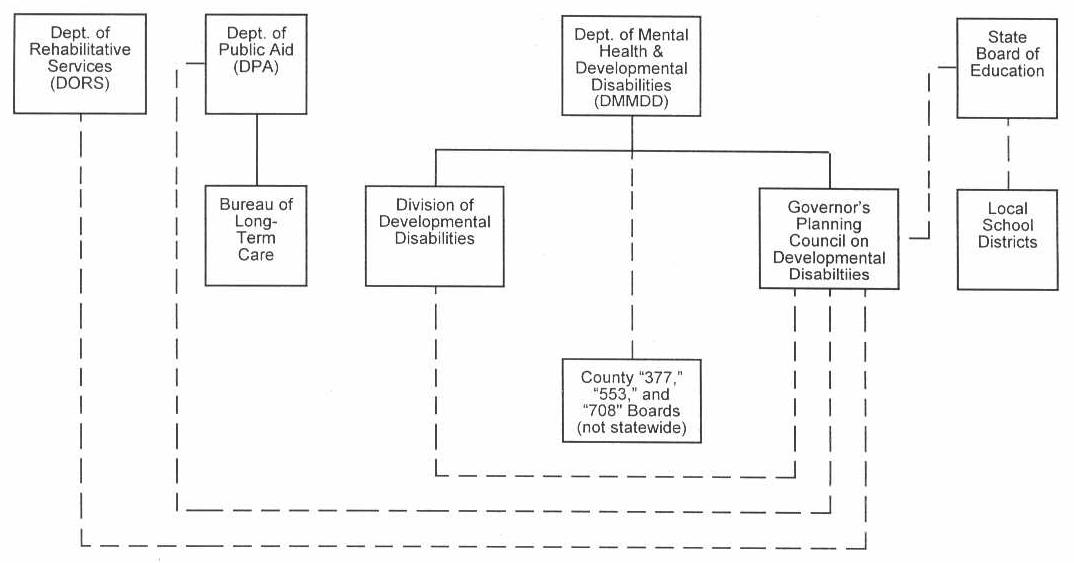 |
State Agency Representatives on DD Council:
Solid lines represent direct authority and oversight Broken lines represent coordination, communication, or indirect or limited authority |
Illinois Site Visit - Interviews
William Murphy Associate Director for Developmental Disabilities Illinois Department of Mental Health and Developmental Disabilities
Lynn Handy Budget and Planning, Division of Developmental Disabilities Illinois Department of Mental Health and Developmental Disabilities
Kay Scrogin Deputy Associate Director for Developmental DisabilitiesDivision of Developmental Disabilities Illinois Department of Mental Health and Developmental Disabilities
Carl Suter Executive Director Developmental Disabilities Planning Council
Marva Arnold Division of Long Term Care Illinois Department of Public Aid
Jerry Morrison Administrator, Division of Field Services Illinois Department of Rehabilitative Services
Rene Christensen Consultant - Special Education Illinois State Board of Education
Jess McDonald Governor's Office
David Brooks Assistant Director ARC - Illinois
Source Documents
Illinois Department of Mental Health and Developmental Disabilities. Illinois Mental Health Statistics, FY86.
_____. FY 1987 DD Service System, April 18, 1986.
_____. FY87 Medical Waiver. Program Cost Projection Report.
_____. FY87 DD Purchase Care. Department Cost Projection Summary.
Illinois Department of Rehabilitation Services. Annual Report '85.
Illinois Governor's Planning Council on Developmental Disabilities. Report to the Illinois General Assembly on Public Act 84-569, Vol. 1: Descriptive Information for the Preparation of A Housing Needs Assessment of Persons with Disabilities, May 1986.
Illinois Governor's Planning Council on Developmental Disabilities. Illinois Transition Project: Transition Plan Development for Special Education Students in Illinois Public Schools.
Taylor Institute. An Analysis of the Regulatory Environment of Illinois Long Term Care Settings Serving Persons with Developmental Disabilities, 1986.
Taylor Institute. Evaluation and Service Identification Project for Developmentally Disabled Residents of Intermediate Care and Skilled Nursing Facilities.
MICHIGAN MR/DD SYSTEM
I. Overview
Background
Michigan has a population of approximately 9 million with a large urban concentration around Detroit. The state has significant rural and agricultural areas, but also Is heavily industrialized. Michigan's economy was severely affected by the recession of the early 1980s and has not completely recovered.
Major System Characteristics
Michigan's MR/DD system is frequently described as a national leader in the area of CBS. The state has reduced the population of DD Institutions from 12,000 to approximately 1,650 since the late 1960's. State policy supports service delivery in the least restrictive setting and Michigan has undertaken innovative, state-funded efforts to assist families with members who have disabilities.
Although the Michigan system is characterized by a high degree of decentralization--most community services are provided by county-level mental health authorities, the lead state agency the Department of Mental Health (DMH) plays a strong role in guiding the development and implementation of community service policy.
Medicaid is crucial to Michigan's CBS system, providing funding for the remaining large public residential facilities and a network of small ICFs-MR, and through the clinical services program (part of the state plan) for day programming. Michigan has two model waivers and has applied for a HBC Waiver which will finance MR/DD services not available under the current state Medicaid plan.
Issues in Community Service Development
Although Michigan has been a leader in developing an extensive system of CBS, most respondents agreed that the system must be expanded to provide adequate and appropriate services to all MR/DD people in need. Moving toward a greater emphasis on integrated settings and individualized services is a major goal. The state's ability to obtain a HBC Waiver and to maintain the current level of financial support will be the major issues for community services in Michigan.
Federal Policy Recommendations
The majority of respondent's suggestions for Federal policy changes concerned Medicaid reform and efforts to alter the institutional bias of Medicaid long-term care funding. Informants also commented that a greater degree of Federal leadership on issues such as housing, transportation, and income maintenance for people with disabilities, and improved coordination of services and policymaking among various state and Federal agencies, would be helpful.
II. Service System Profile
Major Actors in the MR/DD Service System
Department of Mental Health (DMH)
DMH is the lead state' agency providing services to persons with mental illness, mental retardation, and some developmental disabilities. DMH's primary responsibilities include:
- Administration and operation of the eight Regional Centers for Developmental Disabilities (CDDs)
- Policy and budget development
- Funding and oversight of community mental health programs
- Monitoring of ICF-MR certified facilities
- Ensuring protection of client rights through the Office of Recipient Rights (ORR)
Community Mental Health Boards (CMHBs)
The 55 local CMHBs operate services for persons with mental illness and developmental disabilities who live in their home communities. Local CMHBs may encompass a single- or multi-county area. Members are appointed by county commissioners and must include a variety of community representatives as well as county commissioners.
- Most CMHBs serve as the single point of entry into the DMH-funded MR/DD service system.
- In general, DMH provides 90 percent of funding for CMHB services. County contributions and private fund-raising make up the remainder; however, some residential services are completely funded by DMH.
- DMH must approve new CMHB services prior to funding.
- The quality and level of MR/DD service varies among CMHBs and depends heavily on individual counties' ability and willingness to provide the local match. CMHBs can only receive the amount of state funds they can match.
- Currently not all CMHBs receive 10 percent of their funding from the counties. However, all CMHBs are moving toward a funding structure of a minimum of 10 percent local match funds. In addition, some CMHBs contribute more to the gross program than the 10 percent match. The "excess" local funding is usually used for local priority programs.
Department Of Social Services (DSS)
DSS is involved in the MR/DD service system through the administration of a variety of entitlement programs which benefit DD individuals (e.g., the state SSI supplement program, AFDC, General Assistance, foster care for adults and children, and adult community placement for people who are not DMH/CMHB clients). DSS plays a key role in the community service system through the Adult Foster Care (AFC) program. Licensure standards for AFDC homes provide the statutory base for the community residential system. DSS also is the single state Medicaid agency, administering Title XIX funds through the Medical Services Administration (MSA). MSA's activities related to MR/DD services Include:
- Development and administration of Medicaid waivers
- Administration of the state Medicaid plan, including the Mental Health Clinic Services Program, which pays for nonresidential community services for DD people
Developmental Disabilities Council
The DD Council is administratively located in DMH. Its membership is appointed by the Governor and includes persons with developmental disabilities, relatives or guardians of DD people; representatives from DMH, DSS, Michigan Rehabilitative Services (MRS), the Department of Public Health (DPH), the Department of Education, and the Department of Management and Budget, and representatives of local agencies and nongovernmental organizations. The DD Council's major responsibilities include:
- Advocacy with state agencies, the legislature, and the Governor. The DD Council focuses on systems advocacy rather than individual client representation.
- Funding of innovative service development through grants. For example, the Council funded demonstration grants for family support services projects form which practice experience and data were drawn to create the state family support services and family support subsidy programs.
- Analysis and policy development also are necessary activities.
The. DD Council also has Regional Interagency Coordinating Committees on Developmental Disabilities (RICCs) which provide input to the Council and work toward service coordination and problem resolution on the local level.
Department Of Education--Special Education Services
Michigan law requires special education services for all handicapped individuals from birth through age 25. The primary functions of Special Education Services are funding and setting and enforcing standards. Local school districts provide services, either directly or through contact with neighboring school districts or the Intermediate School District (ISD). The 57 ISDs, which are combinations of several local school districts, are primarily responsible for the development of a plan for the delivery of special education services within their boundaries. The ISD also is responsible for monitoring and data collection, and may provide direct services.
Michigan Rehabilitative Services (MRS)
MRS is located in the Department of Education and is the state administering agency for Federal VR funds. MRS has emphasized rehabilitation, training, and placement of disabled people in competitive employment, but also now is providing leadership for supported employment initiatives as the recipient of an OSERS-supported employment grant.
Michigan Protection And Advocacy Service (P and A)
P and A is an independent advocate, responsible for ensuring the rights of DD and MI people in Michigan. The agency plays a key role in quality assurance and monitoring of the MR/DD service system, receiving enough state general fund support to make this a viable function. P and A activities include:
- Continuous service monitoring--P and A can resort to administrative action and litigation to resolve service inadequacies and protect the rights of disabled people.
- Acting as a catalyst for legislative and administrative action, and interagency coordination. For example, P and A investigations and Involvement were critical in the development of a DMH/DSS policy preventing the admission of disabled children to nursing homes without going through the Community Mental Health (CMH) system for assessment and evaluation, and exploration of alternative services.
- Conducting training and technical assistance for judges and attorneys regarding guardianship laws and alternative sentencing for DD juveniles.
Interagency Cooperation
Respondents gave mixed reports about the effectiveness of interagency coordination. Cooperation between DMH and DSS/MSA (the state Medicaid agency) has reportedly been highly successful and instrumental in the development of the current array of services. Informants also cited the Michigan Interagency Task Force on Disability, DSS/DPH interagency agreements on nursing home inspection, licensure, and accreditation, and joint DMH and Department of Education efforts on supported employment as examples of interagency cooperation. However, a few respondents indicated that there is conflict between DMH and the Department of Education regarding the use of segregated special education facilities. Relationships between DMH and some CMHBs are periodically strained by disagreement over the degree to which DMH should be involved in the actual implementation of services at the community level. In addition, there is frequently conflict between CMHBs and their county funding sources.
Private Sector Involvement
Private non-profit agencies are involved in the MR/DD service system throughout the state, operating day, vocational, and residential programs. DMH, policy prevents residential facilities from being owned and operated by the same agency. Private sector providers also are involved outside the DMH/CMH system through DSS foster care and voluntary programs, and through non-profit vocational services programs which provide employment.
ARC Michigan
The Michigan chapter of ARC has played an important role in the development of the state's CSB system. Local ARC chapters have operated community programs; however, most chapters are reducing their involvement in direct service delivery in an effort to strengthen their roles in advocacy and monitoring. The ARC obtained a grant from DMH to train parents and other family members of MR/DD people to monitor community-based programs. Local ARC chapters and the state chapter also have been major participants in SS1/DI training, supported employment initiatives, and community integration projects.
Institutional Services
DMH operates eight Regional CDDs which currently serve approximately 1,650 residents. The CDD census has declined from more than 12,000 at its peak in the late 1960's.
- All CDDs are ICF-MR certified.
- The DPH is responsible for licensing and certification of CDDs.
- DMH is responsible for monitoring and inspection of care.
Nursing Homes
- Private providers operate six SNF-MR facilities with an average size of 25 to 150 beds. These facilities are regulated by DMH, and admissions must be approved by DMH on the basis of functional assessment criteria developed by DPH.
- Five nursing homes have closed since 1980. The population in SNF-MR facilities has declined from 1,400 in 1980 to approximately 600 in 1987.
- DMH plans call for phasing out SNF/MR facilities and moving residents to less restrictive settings.
- DMH and DSS have developed an interagency policy which prohibits the admission of children to nursing homes without going through CMHB assessment and placement process.
Most respondents were in agreement that clients remaining in the PRFs are not significantly different from those living in the community. One informant commented that clients in the CDDs, for the most part, are there because "their turn hasn't come up yet." DD people in nursing homes--and some client in CDDs--were acknowledged to have intense medical needs, but respondents pointed out that many community programs are serving clients with high medical needs successfully. DMH has been able in recent years to prevent the admission of children to CDDs.
Community Services
Residential Services
CMHBs and DMH operate a variety of community residential options for DD individuals ranging from scattered site, semi-independent living arrangements to intensive supervision group homes. Many residential programs are contracted by DMH to private sector providers and, in a few cases, to CMHBs. Other residential programs are contracted or operated by CMHBs. All residential programs which were initiated after 1981 are supported by 100 percent state funds. Community residential programs which were in operation before 1981 are supported by 90 percent state funds and 20 percent local funds. DMH funds residential programs at four levels:
- Level I: Semi-independent living arrangements
- Level II: Group homes for clients who need a higher degree of supervision, with an emphasis on daily living skills and social skills for independence
- Level Ill: Residential facilities for client with a greater degree of impairment--1,000 beds
- Level IV: Residential programs for clients who are multiply handicapped or severely impaired, and require a high degree of personal care assistance
- The DMH/CMH community residential system also includes specialized residential programs such as programs for autistic children and clients with behavior disorders.
- The community residential system has a capacity of approximately 4,600 beds.
Alternative Intermediate Services (AIS) are ICF-MR certified facilities of four to eight beds which are licensed by the DPH as ICFs-MR and by DSS as child care institutions or adult small group foster homes. AIS homes were originally developed for placement of clients being moved out of institutions. Residents are adults and children who are severely disabled.
- AIS homes are privately owned. DMH holds a long-term lease and usually contracts the operation of the program to a non-profit agency other than the home's owner.
- AIS home contracts are administered through CDDs. DMH plans to transfer this responsibility to CMHBs which are capable of administering the AIS programs in their service areas.
- There are approximately 1800 AIS beds.
DSS Residential Services
The community residential services provided through DSS (the state Social Service agency) and the community-based mental health system are based on an adult foster care licensure statute which was enacted in the early 1970's and has been amended occasionally since that time. All community residential programs must be licensed as foster care homes. Licensure, inspection, and monitoring are all handled by state regulatory staff housed in DSS, separate from the Adult Community Placement Program which handles placement, case management, and protective services for adults in permanent placement who are not DMH/CMH clients. Residential placements for DD adults are frequently made in Adult Foster Care homes which provide room, board, and a low level of supervision. AFC home residents also may participate in CMHB day programs. AFC homes are financed through client SSI payments.
Non-Residential Services
Case Management
- Case management services are mandated only for those clients in DMH or CMH supported residential placements. DSS requires quarterly contact with Adult Community Placement workers for SSI recipients.
- CMHBs may provide case management for clients in all their programs, not just residential facilities.
- DMH is responsible for case management for people in CDDs and AIS homes.
- Michigan plans to add case management to the state Medicaid plan. Medicaid coverage for case management should increase its availability.
Medicaid Mental Health Clinic Services
- The program includes almost all adult day treatment, habilitative training, and work activity programs for DD and mentally ill clients in those CMHBs which are certified Medicaid providers. (Only one is not.)
- Services for DD people include: diagnosis and evaluation; interdisciplinary treatment planning; psychological testing occupational and physical therapy; day programs; speech, language, and hearing therapy; individual and group therapy; crisis intervention; health services; transportation; and medication review.
- Services must be provided under the clinical supervision of a Medicaid billable professional (e.g., physician or occupational therapist).
- The Mental Health Clinic Services program was originally financed under the Medicaid waiver, but the state Medicaid plan was amended in 1986 to include these services.
Supported Employment
- Michigan has an OSERS grant for supported employment which involves DMH, MRS, Special Education, and the DD Council. The agencies estimate total annual expenditures of $2.6 million for supported employment.
- The DD Council also is awarding grants to public and private non-profit agencies to set up supported employment projects and has committed approximately one-third of its supported employment allocation to assist the state interagency initiation.
- A report by Western Michigan University estimated that approximately 840 people are currently involved in supported employment.
Vocational Rehabilitation Services
- MRS estimates that about 5,000 DD people were placed in competitive employment last year. Many of these people are young adults leaving special education programs.
- MRS has tended to focus on time-limited services oriented toward competitive employment, but is now increasing its emphasis on supported employment and services to the severely disabled population.
- In FY 1986 MRS was not able to spend its entire Federal VR appropriation because, among other factors, funds needed for the state match were not available.
Family Support
In 1983, Michigan initiated the Family Support Subsidy program which provides nonmeans-tested cash payments to families with disabled children (severely multiply impaired, severely mentally impaired, or autistic) under the age of 18. Families with an annual income less than $60,000 are eligible to receive the subsidy which is based on the level of Federal SSI payments. There are no restrictions on how the money is spent.
- As of January 1987, approximately 2,700 families were eligible for and receiving the subsidy.
- Annual expenditures for the subsidy program are approximately $8 million.
- State dollars provide 100 percent of the funding for the program.
In 1983, following a series of family support demonstration projects, DMH allocated $2 million to CMHBs for the statewide expansion of family support services to assist in the preservation of families and to delay or prevent out-of-home placements. Age and disability are not restricted as in the Family Support Subsidy program. Currently family support services are financed by more than $4 million in state general funds.
In addition, nine Independent Living Centers are currently operating in Michigan. Services offered to adults with handicaps include information and referral, peer counseling, independent living skills training, and self-advocacy skills training. However, the Independent Living Centers are not a major resource for the mentally retarded population, mainly serving DD people who are not mentally retarded and people with later on-set physical handicaps.
General Financing and Service Development Issues
ICF-MR Program
CDDs are ICF-MR certified
- There are eight CDDs with a total of approximately 1,650 beds
Alternative Intermediate Services
- Michigan uses ICF-MR extensively to support community residential facilities, especially for the more severely impaired population.
- AIS program was developed as a result of the decision to reduce the population in CODs.
- DMH is now dissatisfied with the model. At the time it was developed. the AIS model was progressive, but DMH officials now feel that it is too restrictive and too medical in nature.
- DMH and MSA respondents did not report any current problems with look-behinds.
Waiver Experience
- Michigan originally applied for and had approved the 1915(b) Medicaid case management waiver, including clinic services for the mentally ill and MR/DD populations. Application for the waiver was in part motivated by the need to retain as much Federal funding as possible for people coming out of the institutions.
- After the initial waiver period, HCFA did not approve a renewal because of issues related to demonstration of cost-effectiveness and coverage of habilitation services for DD people. HCFA agreed to allow clinic services as an amendment to the state Medicaid plan.
- Michigan has applied for a HCB Waiver which, if approved, will cover additional DD services not included in the Clinic Services program. If the application is approved, DMH plans to decertify a number of AIS facilities and fund them through the Waiver.
- DMH, DSS, and DPH also have model waivers--"Katie Beckett" waivers limited to 50 clients--to serve severely disabled clients and technology-dependent children.
Overall, Michigan is very dependent on Title XIX for funding community services and has been extremely successful in making Medicaid and ICF-MR work in the community. This success can be at least partially attributed to effective cooperation between DMH and DSS.
III. Experience with/Development of CBS
Development of CBS in Michigan
Michigan began to reduce the population in its large institutions in the early 1970's. The Plymouth Center class action lawsuit led to a far-reaching consent decree mandating deinstitutionalization. Michigan also established the CMHB system in 1964, creating a local level service delivery system. Also, Michigan's response to the 1976 ICF-MR regulations was the decision to develop the AIS program and to reduce the population in CDDs, rather than upgrade the CDDs.
Informants listed several factors which contributed to Michigan's development of CBS:
- Michigan has traditionally been very progressive in human services. One respondent described the state as "people-oriented."
- Advocacy for community services by families, the ARC, and other advocacy organizations has been strong and effective.
- One respondent commented that the effort to establish community services occurred when the state had the economic resources to support the effort. Michigan experienced a severe recession in the late 1970s and early 1980s, but was able to maintain the commitment to community services because service systems had already been established.
- Leadership from DMH, the governor, and legislature played a key role. Informants cited examples of a "forward-thinking" DMH director during the 1960s, a supportive governor who was in office for 14 years, and the current governor, now in his second term.
- Although unions are powerful in Michigan, public employee opposition to reducing the population of the PRFs has not been a major barrier. This may be partially the result of the state's efforts to offer other state employment and retraining to dislocated workers.
Current Emphasis on Community Services
Michigan has made a clear policy commitment to CBS. Serving DD people in their home communities is assumed to be the standard, not an extraordinary situation. Most out-of-home, residential placements are made-in non-institutional settings, although residential programs may not always achieve ideals of community integration. Currently state policy is trying to move toward a greater emphasis on individualized services and support to families.
Gaps in Community Services
The consensus among respondents was that although Michigan has been successful in developing a wide range of community services for MR/DD people and moving people out of institutions, the system does not serve everyone in need adequately and appropriately. For example, approximately 1,700 DD people remain in CDDs; DMH personnel pointed out that the community-based system does not yet have the capacity to serve all DD people who have never been in Institutions, much less those who are still there. In addition, the level and quality of services available varies tremendously throughout the state, depending on Individual CMHBs interest in DD services and counties' ability and willingness to fund services.
Specific problem areas include:
- Residential services for adults living with aging parents, as well as adults living at home for whom greater independence is appropriate
- Services for young children with high health care needs
- Age-appropriate services to young adults who have left school
- Respite care--one informant commented that improvements in respite care could be the most important service for families
- Case management
- Supported employment and vocational services
- Family support services
- Lack of public transportation--a major barrier to community integration and community employment
- Access to general health care and health insurance
Goals for CBS/Issues to be Resolved
In general, respondents agreed on the service goals and policy directions Michigan should pursue. The most important long-range objectives are to develop the capacity to provide adequate and appropriate service to all DD individuals in need, to improve cooperation and coordination in the service system, and to equalize the level and quality of service across the state. Specific goals include:
- Expanding supported employment to offer the opportunity to all DD people who want to participate
- Expand residential services, but not using the AIS model
- Improve interagency coordination around the transition issue
- Expand family support services, especially respite care
- Reduce the use of segregated special education facilities
- Maintain an ongoing effort to prevent institutionalization
- Improve the scope and quality of services in those geographic areas which have not been progressive or lack resources
- Broaden the base of public support and coordinate advocacy activities among interest groups
- Develop services aimed at improving social skills for community integration and skills for independent living
- Increase the role of clients and their families in monitoring and planning future program models.
IV. Federal Policy Perspectives
Incentives/Barriers
State agency personnel commented that although there are some problems with Medicaid, Michigan has generally been able to use Title XIX funds to pursue its goals. Michigan's success in using Medicaid to support community services was partially attributed to good relationships between DMH and MSA and with HCFA regional office personnel. However, respondents did state that Federal Medicaid policy does impose some barriers to expansion and improvement of CBS:
- ICE-MR focuses on facilities--"bricks and mortar"--not individual service needs.
- Medicaid does not always allow reimbursement for services in the community that are paid for If the client is in an institution.
- Medicaid does not readily fund less intrusive services.
- Use of Title XIX funds adds to the administrative burden and imposes an unnecessary medical/professional bias on some services.
Regarding Federal policy In general, respondents noted that the majority of Federal funds for disabled people focuses on maintaining dependence rather than fostering Independence.
Policy Recommendations
The majority of respondents' suggestions for changes in Federal policy focused on Medicaid funding; comments dealt with general Medicaid reform issues and regulatory issues:
- Nearly all respondents expressed strong support for CFLA.
- Several Informants suggested that ICF-MR should change to a habilitative rather than health care model and that HCFA should establish an office to focus on habilitation and community services, perhaps for all disability groups.
- Several respondents recommended that discussions regarding Medicaid reform should not focus on the institutional model as the reference point in terms of service and cost comparisons.
- Informants also commented that Medicaid reform along the lines of CFLA should recognize the differences among states--i.e., that some states have not yet developed an extensive system of community services and will need more time and financial and technical assistance to do so.
- DMH personnel suggested that Medicaid reform proposals should not assume that greater state flexibility will automatically lead to cost increases. These respondents pointed out that some states do not take advantage of the flexibility that is already available.
- Respondents wanted more consistency among regulations, HCFA central and regional offices, and program auditors.
- DMH personnel opposed regulations requiring small ICFs-MR to comply with the same staffing requirements as large facilities, as well as requirements for a minimum of 4 people living together to receive Title XIX long term care funding.
Other suggestions:
- Create SSDI work incentive paralleling changes for SSI.
- Improve enforcement of P.L. 94-142 standards.
- Strengthen Federal role regarding standards and availability for housing and transportation.
- Increase Federal encouragement of coordination among state agencies (e.g., similar to the requirements for supported employment grants).
- Increase Federal support for maternal and child health services-primary prevention.
- Clarify Federal regulations for Adult Basic Education (ABE) to emphasize that severely disabled people are eligible for ABE services. Respondents felt that states have sometimes interpreted the ABE program too narrowly.
- One informant commented that vigorous Federal and state oversight will be especially important for CBS because the population and services will be dispersed and difficult to monitor.
- One respondent suggested that HHS and the Department of Education should combine services for the handicapped because current programs and policies are too fragmented.
- Several informants noted that clear policy direction and strong Federal leadership do help to "move the system" (e.g., Supported Employment Initiatives).
V. Summary
General Observations
An overall view of Michigan's MR/DD system shows the state's commitment to CBS. State policy supports clearly the concept of service delivery in the least restricted setting: most residential placements are made in noninstitutional settings; state funds are used in the Family Support Services and Subsidy programs to enable families to keep disabled children at home; and the CMHB system provides a mechanism for local level service delivery.
However, actual implementation does not always achieve stated policy goals: more than 1,600 clients remain in the DD institutional system; education services for severely disabled children are provided in segregated settings; and a DD person's access to adequate and appropriate service depends heavily on where he/she lives.
Although respondents concurred with the assessment of Michigan's MR/DD system as progressive, they readily offered criticisms and pointed out gaps in the service system. For example, several respondents expressed dissatisfaction with the AIS/MR model, and nearly all informants commented that Michigan needs to begin to develop more individualized community services and options for supported independence.
Implications for Federal Policy
Michigan's extensive use of Title XIX funds to support CBS offers opportunities for Federal policy to influence future developments in MR/DD services. Michigan does not need Federal encouragement or the threat of Federal penalties to emphasize community services. However, the state's need to increase Federal financial participation in ASR/DD services would allow Federal policy changes to accelerate the Michigan system's move toward goals of community integration and individualized services.
| EXHIBIT A-3: Michigan Service Delivery System |
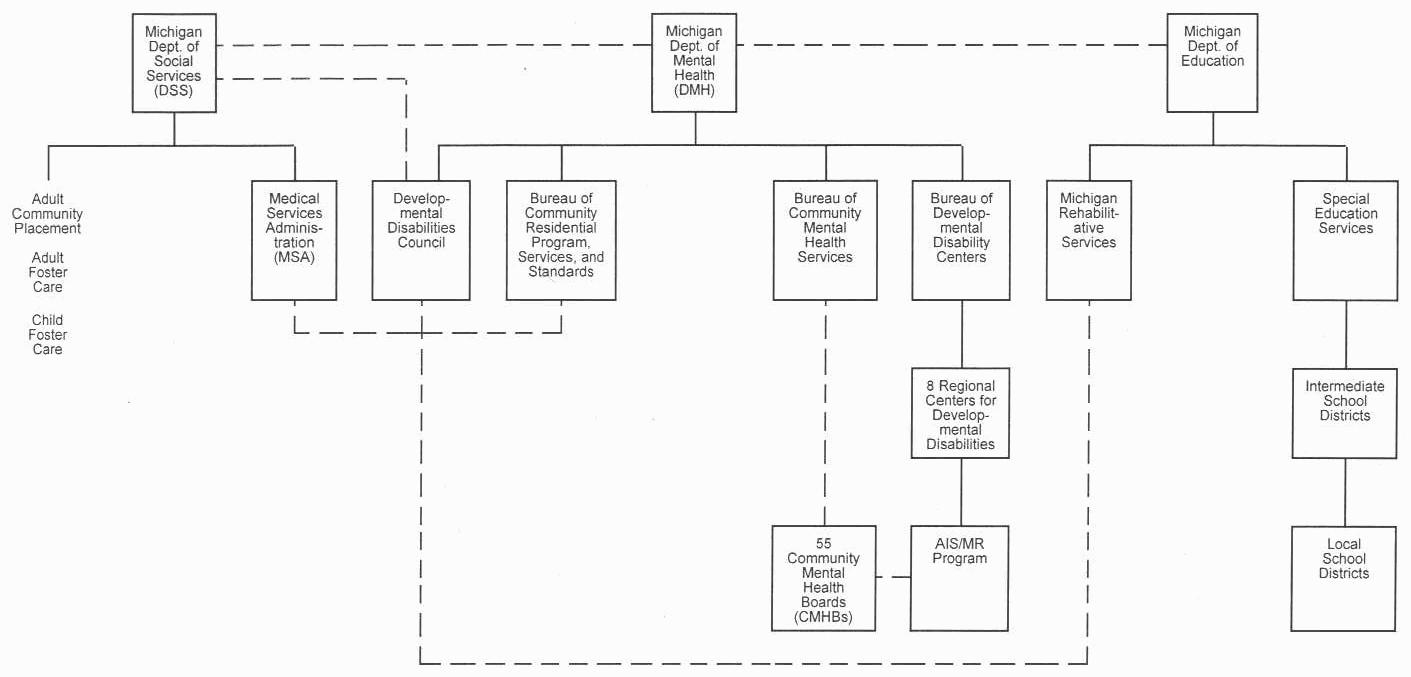 |
State Agency Representatives on DD Council:
Solid lines represent direct authority and oversight Broken lines represent coordination, communication, or indirect or limited authority |
Michigan Site Visit - Interviews
Elizabeth Ferguson Executive Director Michigan Developmental Disabilities Council
Jim Barclay Community Services for Developmental Disabilities
Peter Griswold Michigan Rehabilitation Services
Kevin Magin Special Education Services
Ron Eggleston Medical Services Administration Michigan Department of Social Services
Tom Watkins Acting Director Michigan Department of Mental Health
Annette Abrams Michigan Department of Mental Health
Ben Censoni Deputy Director Bureau of Community Residential Services Programs
Elizabeth Bauer Director Michigan Protection and Advocacy Services
Marjorie Mitchell President, ARC - Michigan
Mary Wagner Community Living Center
Source Documents
Michigan Department of Management and Budget. Report of Residential Contracts/Administrative Rate Study, 1986.
Michigan Department of Mental Health. Baseline Study on Family Support Services in the State of Michigan, September 1984.
Michigan Department of Mental Health. Budget Request Submitted to House Appropriations Subcommittee on Mental Health, March 9, 1987.
_____. Fact Sheets: Resident Population Centers for Developmental Disabilities, FY 1960-1986; Resident Population State Psychiatric Hospitals, FY 1960-1986; Operating Appropriations: Michigan Department of Mental Health, 1980-1987; Patients and Residents in State Facilities, Number of Employees, 1955-1986; and Michigan Zoning Laws.
_____. News Briefs, March 1987.
_____. Report on Family Support Subsidy Program, FY84-85.
_____. Report on Family Support Subsidy Program, FY85-86.
_____. Request for Special Targeted Home and Community-Based Waiver, January 1987
Michigan Department of Social Services. Biennial Report FY85-86.
_____. Proposed Amendment to State Medicaid Plan.
Michigan Developmental Disabilities Council Developmental Disabilities Three-Year State Plan, FY 1987-1989.
_____. Report of Task Force on Community Placement Issues, February 1984.
_____. Supported Employment in Michigan Status Report: Fall, 1986.
Michigan Interagency Task Force on Disability, Work: The Real Social Security, 1985.
Western Michigan University. Baseline Report: The Delivery of Supported Employment Services in Michigan, 1987.
_____. The Evaluation Center and the Center for Human Services. Student Transition to Adult Life: A Preliminary Assessment of Michigan Practices and Alternate Approaches, 1986.
NEBRASKA MR/DD SERVICE SYSTEM
I. Overview
Background
Nebraska has a population of approximately 1.6 million. There is a large urban concentration around Omaha in the Eastern part of the state. The overall character of the state is rural, with some very isolated areas. The economy is heavily dependent on agriculture and has suffered from the crisis in the farm economy. Nebraska has a unicameral legislature with only 49 members. The state has traditionally been fiscally and politically conservative.
The Office of Mental Retardation (OMR) estimates that approximately 12,600 people in Nebraska meet the clinical definition for mental retardation. This figure does not accurately reflect the size of the population in need of services; not all individuals who would meet the clinical definition of mental retardation are in need of specialized services. In addition, the OMR estimate does not include the nonretarded, developmentally disabled population. Current data Indicate that approximately 4,600 people in Nebraska receive specialized mental retardation services.
Major System Characteristics
Nebraska's MR/DD system is characterized by a strong degree of emphasis on CBS. Deinstitutionalization and the development of CBS began in Nebraska in the late 1960's--much earlier than in other states. Unlike many other states which have been progressive in establishing CBS, Nebraska does not use ICF-MR for small residential facilities and has not implemented its HCB Waiver. The Nebraska system also is distinguished by its almost exclusive use of public sector providers.
Issues in Community Service Development
Although Nebraska has succeeded in developing an extensive system of CBS, several major issues will affect further progress:
- Ability to maintain the current level of funding in light of the state's poor economy
- Dissension regarding the need for changes in the current service delivery structure
- Efforts to establish a stronger emphasis on family support and Individualized services
- Expansion of eligibility criteria to include the nonmentally retarded, developmentally disabled
Federal Policy Perspectives
Most respondents' comments regarding Federal policy centered on Medicaid reform and the problems with the current ICF-MR program. Suggestions for Medicaid reform focused on the need for more flexibility and an individualized service orientation, rather than a facility orientation.
II. Service System Profile
Major Actors in the MR/DD Service System
Department Of Public Institutions (DPI)
DPI is responsible for the provision of services to mentally retarded and developmentally disabled individuals, mentally ill people, alcohol and drug abusers, ill and aged veterans, and visually impaired individuals. Services specific to mentally retarded individuals include the operation of Beatrice State Developmental Center and administrative oversight of the OMR.
Office Of Mental Retardation (OMR)
OMR is located within the Department of Public Institutions. Its primary mission is to coordinate and oversee the community mental retardation services system. Within that capacity, OMR carries out the following tasks:
- Development of systems plan, outlining long-term policy issues
- Development of strategic plans, identifying goals and formulating plans for achieving those goals
- Development of budget proposal for legislature
- Budget/program approval and funding of regional programs
- Quality assurance and monitoring of regional programs
- Limited degree of direct contracting for CBS
Regional Governing Boards (RGB)
The six RGBs for mental retardation services are composed of county commissioner representatives from each of the counties contained in the region. The regions are responsible for the administration and operation of CBS for mentally retarded people in their regions. RGBs do not have taxing authority; budget requests are approved by the participating counties. Responsibilities of the regional programs include:
- Planning, policy setting, and budget development for community services
- Administration and operation of local programs
- Monitoring and quality assurance
- Although OMR nominally reviews and must approve regional budgets, plans, and programs, the regions have considerable autonomy in program design and implementation. Regions lobby the legislature directly for budget approval and appropriations are made specifically for regional and local area programs.
Department Of Social Services (DSS)
DSS's major role is the administration and operation of a number of entitlement programs which affect the MR/DD population. DSS also supervises a number of social programs which are not specifically directed toward the MR/DD population, but do serve MR/DD individuals. Specific responsibilities include:
- Administration of the ICF-MR program (the Department of Health is responsible for licensure and certification of ICFs-MR)
- Administration of Title XX funds
- Licensing and monitoring of Adult Family Homes for mentally retarded adults and foster homes for some mentally retarded children
- Administration of the state SSI supplement program
Governor's Planning Council On Developmental Disabilities
The Developmental Disabilities (DD) Council is located within the Department of Health. Its major functions are planning, systems advocacy, and service monitoring. The DD Council has volunteer advisory councils in each of the six regions which assist with planning, local advocacy, and grant evaluation. Other responsibilities include:
- Development of the DD plan which tries to identify areas of high unmet need and devise innovative strategies for dealing with problem areas
- Monitoring of legislative and regulatory changes which affect people with disabilities
- Funding of special projects
Advocacy Group Involvement
ARC-Nebraska was instrumental in the initial development of CBS in Nebraska. The ARC remains a strong influence on policy decision in the state. The Mental Retardation Association of Nebraska favors maintaining Beatrice State Developmental Center and the ICFs-MR.
Institutional Services
Although Nebraska has developed a comprehensive network of CBS, more than 800 mentally retarded people reside in large, congregate care settings, which include:
- DPI operates the Beatrice State Developmental Center, an ICF-MR certified facility serving approximately 470 residents.
- Private ICF-MR providers:
- Martin Luther Home Society operates one 146 bed ICF-MR.
- Bethphage Mission operates two ICFs-MR with a total of 208 residents.
- Omaha Developmental Center is a 49 bed ICF-MR.
- A total of 840 clients are ICF-MR residents.
- A small number of mentally retarded people are served at the Nebraska Psychiatric Institute.
Respondents indicated that although there may be a higher proportion of severely disabled clients in the ICFs-MR, the community programs also serve many severely disabled individuals. A few respondents indicated that the institutional programs serve those people community programs are unable or unwilling to serve, such as:
- An increasing number of children are entering ICFs-MR because most regional programs emphasize adults.
- The regions serve mentally retarded individuals, not the overall developmentally disabled population.
Community Services
Residential Services
The overwhelming majority of community-based program are operated by the regions. The array of services varies from region to region, but programs fall into the following categories.
Supported Community Living
- Extended family homes include Adult Family Homes for mentally retarded adults and foster homes for mentally retarded children. These homes are licensed and monitored by DSS. Approximately 100 mentally retarded people reside in extended family homes.
- Semi-independent living arrangements serve approximately 360 clients who need minimal supervision, but require some help with living skills.
- Family support is provided to help maintain mentally retarded individuals in their own homes.
Assisted Residential Living
- Group homes for 10 or fewer people provide 24-hour care and supervision.
- Approximately 768 mentally retarded individuals live in 174 group homes.
- Nebraska does not use ICF-MR to fund small community-based facilities services.
Non-Residential Services
Vocational Services
- Approximately 1500 mentally retarded people over the age of 16 participate in sheltered workshops.
- Approximately 100 people are employed in work stations in industry.
- Approximately 1000 clients are employed in work training.
Family Support
- In-home support services such as assistance and training with medical equipment and personal care assistance
- Respite care
Case Management
- Regions employ case managers for all mentally retarded individuals who request services; case managers are responsible for coordinating all needed services.
- Several respondents indicated interest in developing an independent case management system.
Education Services
- Nebraska requires local school districts to provide special education services to all handicapped children from the date of diagnosis to age 21.
- Local school districts bear most of the responsibility for serving the school age population, regional programs tend to emphasize adult services.
- The Department of Education operates the Family Home Care program for handicapped children who must be moved out of their home school districts for educational reasons. The project locates and trains "foster" parents for children who must attend school away from home. The Department of Education pays for the residential costs once the home school district pay for educational costs.
Community Service Providers
Although RGBS are permitted to provide services through contract, only Region VI uses the private sector extensively. (OMR contracts with several community service providers directly.) Respondents attributed Nebraska's decision to not to encourage private sector development to concerns that private providers would not put client interests ahead of business interests.
General Financing and Service Development Issues
Financing Of Community Services
Federal funds supply approximately 34 percent of expenditures:
- Title XX/Social Services Block Grant is the major source of Federal funding for community services
- Other Federal funds include SSI payments to individuals; education funds, DD grants, Medicare payments for some individuals in hospital-certified beds in Beatrice, and Medicaid payments for Medicaid-eligible MR/DD individuals
State funds supply approximately 45 percent of expenditures:
- State match for Title XIX funds is 43 percent
- In FY84-85, state expenditures of approximately $10.2 million for IC Fs-M R
- State match for DD grant
- State funds to private community providers
State funding of regional mental retardation services:
- The legislature appropriates funds individually to regions and counties.
- Regional budget requests are based on a model which estimates program costs on the basis of how much it costs to service high-, medium-, and low-need clients.
- In FY 84-85, state payments to regions were $19.6 million.
County and local funds make up approximately 7 percent of total expenditures:
- Counties must make a contribution for residents in Beatrice.
- County contributions to regional programs have decreased as a percentage of total expenditures.
- County contributions vary widely across the state.
- County/local contributions are raised primarily through the property tax.
- Most regional programs charge fees on a sliding scale.
ICF-MR Program
Nebraska has chosen not to use ICF-MR to finance small, community-based residential facilities primarily because of perceptions that the ICF-MR medical model of care was inappropriate for CBS. Therefore, Title XIX is not a significant funding source for CBS.
Waiver Experience
Nebraska applied for and received a Medicaid 2176 waiver for services to the mentally retarded population in 1984. However, the state never implemented the waiver. Respondents suggested two major reasons for the decision not to implement the waiver:
- Concern about obligating the state to higher Medicaid expenditures
- Administration concerns about the absence of effective state control over regional programs
Several respondents indicated that they would like to see the state develop a new waiver so that Medicaid funds can support community programs.
Community Service Development Costs
During the initial phase of community services development, the legislature appropriated special funds to cover startup costs. These funds are no longer available.
III. Experience with/Development of CBS
Development of CBS in Nebraska
Advocates and parents of mentally retarded people were responsible for Nebraska's development of CBS in the late 1960's. Nebraska was one of the first states to develop an extensive system of CBS. In 1969, the Nebraska legislature passed the Interlocal Agreement Act, establishing the current regional system and laying the ground work for state funding of CBS.
The Horacek v. Exon law suit, filed in the early 1970's, also contributed to the development of community services. The suit was dismissed in 1984 on the grounds of the state's compliance with the consent decree. However, the lawsuit came along after Nebraska had made a commitment to CBS and a framework for delivering those services.
Respondents cited a variety of factors which contributed to Nebraska's progress and shaped policy directions:
- Involvement of parents and community people in the early stages of development
- Presence of a strong, well-organized ARC
- Leaders In the field of community services were involved in Nebraska
- Support from elected officials on both the state and local levels
- The ability to articulate a value-based statement of what MR services should be
- Structure of the State
- Small population
- Simple political system (unicameral legislature)
- Small financial investment in the institutional system
- Availability of funding for the development of CBS
- Title XX funds
- State fund for start-up costs
- Strong philosophical commitment
Current Emphasis on CBS
The consensus among respondents was that Nebraska has made a strong, lasting commitment to CBS for the mentally retarded population. The commitment is reflected in both expenditures and client placements:
- Expenditures for community services are significantly higher than for Institutional services.
- Approximately 840 clients are in institutional settings; 2,400 are served by community programs.
Nebraska has maintained the level of funding for community services in spite of state economic problems. In the last legislative session, the mental retardation services budget received a slight increase; budgets for nearly all other state services were cut.
Gaps in Community-Based Services
Although all respondents agreed that Nebraska has made great strides in developing CBS, they also cited a variety of deficiencies in the service system, in terms of both service gaps and structural problems.
Service gaps:
- Waiting lists for residential and vocational services
- Family support and respite care
- Work training
- Community integration services
Some groups of individuals among the MR/DD population are not being served well:
- Multiply handicapped adults
- Mentally retarded individuals with behavior problems
- The elderly MR/DD people
- Autistic individuals
- Aging out population
Several respondents cited problems with the current regional structure:
- The regional structure has become "Institutionalized."
- The current system does not allow for meaningful monitoring and oversight from the state level.
- The types and quality of service and the population served vary among the regions.
- Several respondents felt that the lack of competition--the absence of a strong private sector role--may reduce the quality of service.
Goals for Community-Based Services/Issues to be Resolved
Respondents generally agreed that the primary challenge for Nebraska in the immediate future will be to develop services which are responsive to individual needs and provide support to families:
- Improve family support services
- Develop services to help people with mental retardation participate more fully in community
- Improve case management (i.e., several respondents suggested that case management should be separated from service provision)
- Serve everyone in need in the most appropriate setting
- Improve services to the severely disabled
Nebraska's community service system was described by several respondents as "mature," but in need of some structural changes.
- The state has a high level of investment in the current system which, according to some, inhibits its ability to respond to changing needs and implement Innovative service approaches.
- Some respondents felt that the current system does not focus on the individual, and does not provide adequate support to families.
- Accountability: ultimate responsibility for providing services is not clearly articulated in statute.
- The absence of a competitive private sector role gives RGBs a "monopoly" on providing services.
- OMR and the regional programs are mandated to provide services only to the mentally retarded. There has been some discussion about expanding eligibility to include all developmental disabilities.
- A Medicaid waiver must be implemented.
IV. Perspectives on Federal Policy
Incentives/Barriers
Some respondents expressed the view that the current ICF-MR program encourages the state to continue to support institutional care. Nebraska chose not use ICF-MR in the community because of the perception of the inappropriateness of the medical model.
Several respondents were dissatisfied with the HCFA look behind surveys. While supportive of the effort to ensure quality services, they offered criticisms:
- HCFA's attitude is not one of cooperating with state to improve services, but is confrontational.
- Active treatment requirements are unclear.
Policy Recommendations
Although Nebraska does not use Title XIX for community services, many suggested Federal policy changes focused on Medicaid reform:
- Build more flexibility Into Medicaid so that Title XIX can be spent in the community without the restrictiveness of the ICF-MR program
- Make waiver services permanent optional service under the state Medicaid plan
- Create an MR/DD authority within Title XIX
- Focus Title XIX on services rather than institutions/facilities
- Pass CFLAs (a representative of MRAN opposed this)
- Cover startup costs of community services
A number of suggestions focused on vocational services and programs:
- Make definitions of disability consistent across Federal programs
- Make VR serve the MR/DD population
- Bring OSERS and VR regulations closer together, possibly make VR the primary referral agency for exiting special education students
V. Summary
In general, Nebraska is very progressive; maintaining MR/DD people in the community is the rule rather than the exception. Although there is strong loyalty to the current system, people do seem willing to examine structural problems and do not appear to be complacent or satisfied with what they are doing. The Nebraska example demonstrates that the development of CBS is an ongoing process. However, the potential of extending the lessons of the Nebraska example are limited by the state's small size and homogeneity.
In addition to having one of the most decentralized MR/DD systems, Nebraska also has a system in which almost all services are in the public sector.
Implications For Federal Policy
Major changes in MR/DD services funded under Medicaid that would support innovative and nonmedical model services could be useful in enhancing the Nebraska system. Minor changes would probably have little effect.
The current system's emphasis on local (regional) autonomy and control limits the state's ability to ensure outcomes at the community level. OMR is also a very small agency, with less than 10 staff members.
| EXHIBIT A-4: Nebraska Service Delivery System |
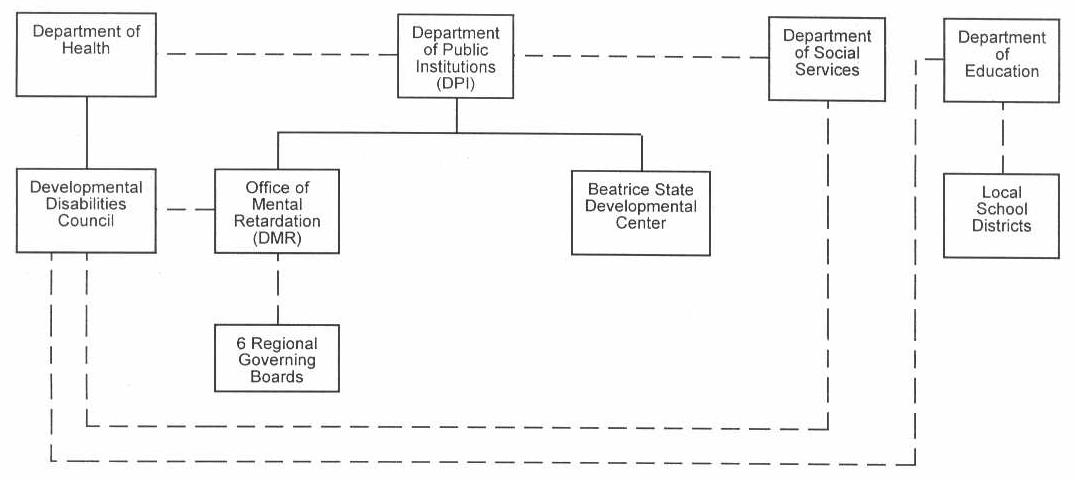 |
| Solid lines represent direct authority and oversight Broken lines represent coordination, communication, or indirect or limited authority |
Nebraska Site Visit - Interviews
Dave Evans Director, Office of Mental Retardation Nebraska Department of Public Institutions
Don Anderson Director of Compliance Nebraska Department of Education
Dave Powell Executive Director, ARC-Nebraska
Robert Seiffert Department of Social Services
Eric Evans Executive Director Developmental Disabilities Council
Dee Everett Past President, ARC-US
Delores Bangert Chair, Nebraska Association of Private Residential Facilities for the Mentally Retarded
Don Moray Director, Region VI Mental Retardation Services
Lyn Rucker Director, Region V Mental Retardation Services
Pat Crawford Mental Retardation Association of Nebraska
Sources Documents
Nebraska Department of Public Institutions. Nebraska Mental Retardation System Plan, May 1986.
_____. Regulations for Organizing and Implementing Mental Retardation Services, January 1985.
_____. Report on the Design and Assembling of A Standard Cost Model for the Nebraska Community-Based Mental Retardation Programs, October 1984.
_____. Two-Year Strategic Plan: Operations Year July 1, 1986 - June 30, 1987 and Budget Request Year July 1, 1987 - June 30, 1988.
Region V Mental Retardation Services. Annual Report 1985-86.
TEXAS MR/DD SYSTEM
I. Overview
Background
Texas is one of the nation's largest, most populous states, with a population of approximately 14 million. Approximately half the state's residents live in one of several large urban areas (Dallas, Fort Worth, Houston, and San Antonio). The state also has isolated rural areas, and population centers are separated by long distances.
Texas has traditionally been politically conservative, favoring limited government involvement in and expenditure for human services. In the past decade, the state experienced significant population and economic growth, but the economy has suffered from the recent slump in oil prices.
Major System Characteristics
The Texas MR system has relied heavily on large institutions and funding has not significantly emphasized CBS. Approximately 8,000 mentally retarded individuals are served in the 13 state schools (PRFs), while the community residential system, which includes private ICFs-MR of up to 200 beds, has a capacity of approximately 4,000 beds. Texas began to place greater emphasis on community services during the late 1970's, and this trend has been accelerated the past 3 years, partly as a result of the settlement of a major class action lawsuit against the Department of Mental Health and Mental Retardation (TDMFMR). Actual delivery of CBS is decentralized. Community Mental Health and Mental Retardation Centers, the local service authorities in most areas, contract with the state Department of Mental Health and Mental Retardation to provide services on the community level.
The ICF-MR program provides the bulk of funding for residential services, both institutional and community based. In addition, Texas has a HCB Waiver, which will provide services for 450 clients.
Issues for Community Service Development
Texas' long standing dependence on large congregate care facilities acts as a major barrier to the expansion of community services. The high level of investment in the state school system and the rising costs of operating that system divert available resources from the development of new services at the community level. One respondent also suggested that because Texas has not had extensive experience with CBS, public opposition to community services for MR/DD people is a barrier. Legislators and members of the public may not be convinced that community-based MR/DD services will be safe and effective.
The state's traditionally low tax rates (there is neither a personal nor corporate income tax) and the current fiscal crisis limit the resources available for community services. Any decision regarding the development of CBS will be at least partially influenced by Texas' need to maximize FFP. The need to comply with the consent decree settling the Lelsz V. Kavanaugh class-action suit against DMHMR will also affect the development of CBS in Texas.
Federal Policy Perspectives
Most respondents' suggestions for Federal policy changes focused on Medicaid reform to alter the institutional bias-of the ICF-MR program. Informants commented that Texas will need both incentives for developing community services and disincentives for emphasizing institutional services to make significant changes in the way MR/DD services are developed. Several people also stressed that any major restructuring of .Medicaid long-term care funding (e.g., CFLA) should recognize that change in states like Texas will take time, and also should recognize that costs will be higher during the transition period. Other comments regarding Federal policy stressed the need for stronger Federal leadership and commitment to community services.
II. Service System Profile
Major Actors in the MMR/DD System
Department Of Mental Health And Mental Retardation (TDMHMR)
TDMHMR has primary responsibility for providing services to citizens with mental illness and mental retardation. The Department's authorizing legislation directs the agency to give priority to the most severely disabled population, particularly those at risk of institutionalization, and to emphasize alternatives to treatment in congregate care facilities. TDMHMR's activities and services for the MR population include:
- Administration and operation of the 13 state schools for the mentally retarded
- Administration of five state centers for the mentally retarded
- Planning and policy development, including the development of ICF-MR program policy in conjunction with the Texas Department of Human Services
- Preparation of strategic plans and statewide goals and objectives
- Funding and oversight of local community MH/MR programs
- Monitoring and quality assurance in the state schools and community programs (MRAs)
- Monitoring of non-ICF-MR residential facilities operated by local Mental Retardation Authorities
Community Mental Health And Mental Retardation Centers (CMHMR Centers)
The 31 CMHMR Centers are quasi-governmental bodies which provide community-based mental health and mental retardation services throughout Texas. TDMHMR has divided the state into 60 local service areas. Each local service area has a MRA which is either the local CMHMR Center or, in areas without a Center, an outreach program of one of the state schools. CMHMR Centers sign performance contracts with TDMHMR and provide services within the goals of TDMHMR plans, but they are accountable to their own boards.
- CMHMR Centers must provide a set of core services: case management, diagnosis and evaluation, family support, and respite care.
- TDMHMR provides most of the funding for CMHMR services; county, municipal, and private funds make up the remainder.
Department Of Human Services (TDHS)
TDHS is involved in the MR/DD service system through the administration of a wide range of social service programs which benefit MR/DD individuals. TDHS is the single state Medicaid agency and jointly administers the ICF-MR program with TDMHMR. Responsibilities include:
- Setting reimbursement rates for ICFs-MR
- Promulgating regulations in conjunction with TDMHMR for the ICF-MR program
- Administration of general social service programs such as income assistance and services to families and children
- Application of financial sanctions against ICF-MR providers
Texas Planning Council For Developmental Disabilities
The DD Planning Council is located in the Texas Rehabilitation Commission (TRC). The Council does not provide services directly; its role is to facilitate the development of a comprehensive service delivery system for DD people. Primary responsibilities include:
- Public education about developmental disabilities
- Advocacy with state agencies and the legislature
- Policy development and analysis
- Service evaluation
- Facilitation of interagency coordination on issues of material interest and agreement
- Funding of research and demonstration projects, emphasizing residential services and unemployment-related services.
Texas Rehabilitation Commission (TRC)
TRC is the administering agency for both Federal VR funds and the DD Planning Council. Although the emphasis of TRC's VR-funded programs has been on time-limited services leading to competitive employment, the agency has also made efforts to emphasize services to the severely disabled population. Specific services relevant to the MR/DD population include:
- Extended Rehabilitation Services (ERS) for disabled people who cannot be competitively employed
- Independent Living Program
- Deaf-Blind Program
- Comprehensive Medical Rehabilitation Services for people with brain and spinal cord injuries
- Administration and processing of SSI and SSDI programs in Texas (there Is no state supplement)
Texas Education Agency (TEA)
Texas law requires special education services for handicapped children from age 3 through 21 (blind, deaf, and deaf-blind are eligible from birth through age 21). The local Independent School Districts (ISDs) provide direct special education services. TEA is responsible for oversight and monitoring, allocation of Federal funds, and providing technical assistance.
Texas Department Of Health (TDH)
TDH provides personal health care services through the Bureau of Maternal and Child Health and the Crippled Children's Bureau. The agency also is responsible for licensing, certification, and inspection of care for the state schools and all ICFs-MR.
Other Agencies
- Advocacy, Inc. is the state's DD protection and advocacy agency mandated by the DD Act of 1984. Its responsibilities include legal and protective advocacy services, system advocacy, and a Client Assistance Program.
- The Health and Human Services Coordinating Council's mission is to serve as the primary agency for planning and coordinating health and human services. Its responsibilities include research and policy analysis, maintenance of a centralized data base on health and human services in Texas, and information and referral sources.
- The Council on Disabilities is responsible for developing a long-range plan for all persons with disabilities and promoting the development of statewide policies on disabilities.
Interagency Cooperation
Respondents reported that state agencies concerned with the DD population are involved in a variety of interagency efforts to Improve and coordinate services:
- TDMHMR, TRC, and TEA have a legislatively mandated interagency agreement for cooperation in services for transition from special education to adult services.
- TEA has a separate Interagency Coordination Office created specifically to work with the state schools and ISDs on the deinstitutionalization of school-age children.
- TDH, TDHS, TDMHMR, and TEA participate in the Early Childhood Intervention Council which develops a state plan for early childhood intervention and provides grants for direct services.
Advocacy Organization Involvement
The ARC-Texas is one of the primary advocates for community-based MR/DD services in Texas. The ARC has been actively involved in the Lelsz V. Kavanaugh case which is directed toward improving services in the state school system and has been an important factor in efforts to move people out of the state schools.
Parents Associated for the Retarded of Texas (PART) split off from the ARC and represents the pro-institution point of view. Most members are parents of state school residents. PART has been an effective advocate for the maintenance of the state school system.
Private Sector Involvement
Private sector providers play an important role in the nonstate school residential services systems. More than three-quarters of ICF-MR beds (outside the state schools) are operated and owned by private providers, including small non-profit organizations as well as large health services chains. The Texas Association of Private ICF-MR Providers (TAPP) is the primary representative for private ICF-MR facilities. Private sector involvement also includes charitable and private-pay facilities such as The Brown School and Mary Lee Schools. Many non-ICF-MR small group homes also are privately owned and operated.
Institutional Services
State Schools For The Mentally Retarded Operated By The TDMHMR
- Thirteen state schools range in size from approximately 350 to 1,000 beds.
- Approximately 9,600 clients lived in the state schools in FY 1986.
- Nearly all beds are ICF-MR certified.
- The resolution and settlement of the Lelsz V. Kavanaugh suit mandated a census reduction in three of the state schools.
Private Sector
- Private providers own and operate several large ICFs-MR which range in size from 30 to 200 beds.
- Two proprietary chain providers (Beverly and ARA Services) operate large ICFs-MR.
Client Population
Several respondents commented that, in comparison with earlier years, the residents of the state schools are older and more severely impaired. Children and individuals functioning in the mild to moderate range have been priorities for deinstitutionalization. In general, children who are severely impaired are being cared for at home or in ICFs-MR. Approximately 250 people are on the waiting list for the state schools, but TDMHMR is not admitting new residents.
Community Services
Most CBS are provided through the 60 local service areas' MRAs, either CMHMR Centers or state school outreach programs. If a local MRA cannot provide needed services, TDMHMR may contract with another local agency or private provider. The range of services available at the community level has expanded in the last 3 to 4 years, partly In response to the Federal court-mandated deinstitutionalization effort.
In response to both the court case and the need to improve services in the state schools, the legislature appropriated funds for reducing client-to-staff ratios in the state schools. TDMHMR has used these funds to implement a program of financial incentives for CMHMR Centers--the Prospective Payment System.
- MRAs receive $55.60 per day for each client who returns to the local service area from one of the state schools.
- The payment does not have to be spent for services for deinstitutionalized individual, but can be used to support the development and operation of the MRAs' services In general. However, all services required in the individual's program plan must first be provided.
- The availability of these funds has stimulated the development of services for both former state school residents and community residents who are mentally retarded.
Residential Services
Community-Based ICF-MR Program
- TDMHMR and TDHS designate all non-PRF school ICF-MR facilities as part of the community ICF-MR program.
- There are a total of approximately 4,400 ICF-MR beds in the community program; about 3,800 beds are privately provided.
- The facilities range In size from less than 6 beds to more than 200 beds.
- Since 1981, TDHS regulations have prohibited development of any ICFMR with more than six beds. All growth In the ICF-MR program has been in this category, although providers and TDHS agree that the model is not cost-permissive at current reimbursement rates (i.e., providers cannot break even at current rates).
Non-ICF-MR Residential Facilities
- There are approximately 2,000 beds in non-Title XIX financed group homes, operated by MRAs.
- Group homes have been developed by CMHMR Centers, local ARC chapters, and other private providers.
Nonresidential Services
Case Management
- Case management is a core service which MRAs are required to provide for all mentally retarded clients returning from state schools in their local service areas.
- TDMHMR representatives commented that case management has Improved in the last 2 years.
Vocational Services
- Most CMHMR Centers operate their own vocational programs.
- TRC operates the Extended Rehabilitative Services (ERS) program for severely disabled individuals who can work but need continuous training and supervision. The ERS program provides sheltered employment, transportation, medical services, and assistive devices such as hearing aids and wheelchairs. In some eases, ERS arranges community-based residential services. TRC operates ERS programs in 11 cities throughout the state, including some services to MR/DD people.
- Supported employment has not yet been developed extensively.
Family Support
- Family support is a core service required of CMHMR Centers.
- A bill pending in the legislature would provide a $3,600 annual subsidy for families with disabled children.
Education Services
- Special education is required for children ages 3-21; direct services are provided by local ISDs.
- Early Childhood Intervention Program (ECI):
- The program was created in 1981 by the legislature to identify and provide services to children from birth to age 6 who are developmentally delayed or who are at risk of a developmental delay.
- The ECI program is overseen by representatives from TDMHMR, TDH, TDHS, and TEA, as well as parent representative.
- ECI programs are funded by grants awarded by the ECI Council; programs must provide educational programming, therapeutic treatment, case management, and parent counseling.
- Sixty-two programs were funded in FY 1986.
General Financing and Service Development Issues
ICF-MR Program
- Texas has used ICF-MR extensively for small facilities.
- ICF-MR facilities and clients are categorized by levels of care which are based on an individual's 1.Q., ABL, health status, and ambulatory status:
- Level I--Clients are mildly to moderately retarded.
- Level V--Clients are moderately to severely retarded.
- Level VI--Clients are severely to profoundly retarded.
- TDHS establishes payment rates for the community ICF-MR program on a cost-based prospective reimbursement system. The reimbursement rate is based on the median cost level reported by all facilities in previous years.
- Reimbursement rates vary by level of care. Current rates:
- Level I facilities: $55.62 per day per client
- Level V facilities: $46.56 per day per client
- Level VI: $55.84 per day per client
- Payment rates do not reflect differences in facility size or location. Although regulations only allow development of facilities smaller than six beds, the reimbursement rate does not account for the higher cost of operating a small facility.
- Reimbursement rates for state schools are much higher than rates for the community program:
- Level I: $74.76 per day per client
- Level V: $93.83 per day per client
- Level VI: $103.57 per day per client
Waiver Experience
- Texas' 1915(c) HCB Waiver was approved in 1985. The Waiver was developed jointly by TDMHMR and TDHS.
- The Waiver finances the Intermediate Community Services program which operates on a cluster model which includes:
- A core home which provides initial evaluation and respite and administrative services for all clients in the cluster.
- In-home services to MR clients living in their own homes. Services Include case management, homemaker services, respite care habilitation, social services, nursing, psychological services, and rehabilitation.
- Alternative residences for clients who live outside their family homes.
- Services are provided through 10 project sites with five more to be announced In June 1987.
- The Waiver was originally projected for 450 clients, but TDMHMR and TDHS personnel do not expect to reach capacity within the initial 3-year Waiver period.
- Services are reimbursed at a rate of $45.90/day. Private providers and the nursing home lobby helped to pass a law which limits the rate to less than the average rate for community ICF-MR providers.
- Texas also has model waiver for severely disabled people which currently serves only 27 clients.
Community Service Development Costs
- TDMHMR has made some development funds available, but this is not an ongoing effort.
- The prospective payment program has contributed to expansion of CBS.
- The prospective payment program has caused some tension between private providers and CMHMR Centers.
III. Experience with and Development of Community Services
Development of Community Services in Texas
The consensus among respondents was that Texas has not yet made adequate progress in establishing a comprehensive network of community services. However, one informant commented that the state has "turned the corner" toward emphasizing community services as the primary source of care. Respondents listed a variety of factors which contributed to Texas' traditional orientation toward institutional care:
- The legislature has been reluctant to fund human services and for MR/DD services available resources have not been adequate to fund both Institutional and community services.
- Several respondents cited the conservative political ideology which emphasizes independence, family privacy, and limited government as a major barrier to community services.
- The low level of public awareness has been an obstacle. Because there is little experience with community services in Texas, the public and many members of the legislature do not believe community services will work.
- Opposition from state school superintendents who have influence with the legislature and from PART, the pro-institution parent group.
- Fears that closure or downsizing of state schools will have a negative effect on local economies.
- Several respondents commented that the institutional bias of the ICF-MR program continues to encourage Texas to emphasize institutional services.
- The absence of a reliable Federal funding stream for community-based, nonresidential programs.
Current Emphasis on Community Services
Most informants agreed that Texas is in a period of transition to a community service system. All respondents supported the ideals of normalization and community integration for the MR/DD population. Official policy statements now express a preference for service in the home community. A number of elements have precipitated this change and will continue to influence policy decisions in Texas:
- The Lelsz V. Kavanaugh case
- TDMHMR Board policies which support community services
- Availability of the Waiver, and the ability to use Federal funds in the community
- Advocacy and public education to reduce opposition to community services.
Gaps in Community Services
Respondents agreed that the most significant gap is a general lack of adequate and appropriate community services, rather than the absence of any specific services. Many mentally retarded people do not receive the services they need; TDMHMR has identified 1,600 people who are at risk of institutionalization and in desperate need of services. Although a general improvement in quantity and quality of services is the primary need, respondents did identify several areas of special need:
- DD individuals who do not meet the definition of mental retardation are not eligible for TDMHMR services.
- There is a lack of community settings for the severely handicapped.
- Day programs for MR/DD people in the community are needed.
- Young adults completing special education programs have difficulty gaining access to appropriate community services.
- Quantity and quality of services is uneven throughout the state.
Goals for CBS/Issues to be Resolved
The most frequently mentioned goal for community services was the improvement and expansion of CBS at all levels. Most respondents agreed that Texas should and will continue to reduce the population in the state schools. Specific goals include:
- Reduce the population of the state schools by 1,800 by FY 1991 (TD MHM R Strategic Plan)
- Develop 3,300 new community residential placements and an array of nonresidential services by FY 1991 (TDMHMR Strategic Plan)
- Develop services that emphasize community integration, support to families, and the use of generic community resources
- Improve vocational services, Including supported employment
- Improve services for the transition from special education to adult community life
- Increase the Integration of special education programs into regular education
A number of issues must be resolved to implement these goals:
- Texas must find ways other than ICF-MR to use Medicaid funds to support community services. Several respondents pointed out that the legislature sees maximizing Federal funding as a major goal and Title XIX as the only stable Federal funding stream for MR/DD services.
- TDMHMR and the Texas Council of CMHMR Centers are working to develop a methodology for equalizing state funding of CMHMR Centers.
- One respondent commented that this is a "watershed year" for human services in the state: if legislative support for community MR/DD services can at least be maintained during the current fiscal crisis, this will indicate that Texas has made a real commitment to community services.
IV. Federal Policy Perspectives
Incentives/Barriers
Informants noted that Federal policy has had a significant influence on the development of Texas' MR/DD service system:
- The institutional orientation of ICF-MR and the availability of Federal funds for institutional services has encouraged Texas to continue with PRFs.
- Availability of ICF-MR funding for small facilities has contributed to the level of community residential service that has developed.
- The categorical focus of Federal disability programs is an obstacle to coordination of services and promotes the "turf battles" between state agencies.
Policy Recommendations
Many respondents' suggestions for Federal policy changes focused on the need to restructure the ICF-MR program to redirect resources to CBS. Several informants also commented on the need for stronger Federal leadership and oversight.
Medicaid Reform
- Respondents stated that some change in the institutional orientation of the ICF-MR program is needed, but this change should be gradual and should include funding of a transition period. State personnel stressed that the transition to community services will take time and will require greater financial resources for the initial startup period.
- One informant suggested greater state flexibility with Title XIX: states need to find a way to get beyond the entitlement concept so that they can stay within fiscal restraints. A state should have the option to cap its own program; this would be the only way Texas could take advantage of Medicaid options currently available.
- Another respondent commented that the legislature will probably be unwilling to modify the state Medicaid plan (e.g., by adding case management or services currently financed under the Waiver) without estimates of increased eligibility and costs, and without some guarantees of cost controls.
- ICF-MR funding should "debundle" services and shift to providing the least intensive, least intrusive level of service appropriate to client needs.
- Clarify who should be eligible for ICF-MR, possibly make it time-limited for higher functioning clients.
- Clarify Title XIX regulations regarding vocational services and active treatment. State personnel commented that even an unfavorable clarification would be better than the current uncertainty about HCFA's recent interpretations.
General Policy Suggestions
- A stronger political commitment on the Federal level would be helpful in persuading people in Texas that development of community MR/DD services would be worthwhile.
- Better enforcement of P.L. 94-142 is required.
- A Federal mandate requiring states to look at disability globally would help to encourage continuity and coordination.
- Technical assistance should be provided to states to implement new technologies; for example, complex medical or assistive devices.
- Funding for training of personnel, particularly special education teachers, should be expended.
- One respondent commented that Federal leadership and guidance is very helpful--when policy issues (this informant cited transition services for special education students and programs for the deaf-blind) are emphasized at the he Federal level, those issues get more attention at the state level.
V. Summary
General Observations
Based on current observations of client placements and expenditures, Texas does not adequately emphasize community services. Although noninstitutional placements and in-home services are becoming more viable options for MR/DD people living in their home communities, 8,000 people continue to reside in the state schools. Deinstitutionalization will continue, but, given the large number of people in state schools and large ICFs-MR, combined with the low level of community alternatives, it will be a slow process.
Although the high level of investment in the state school system and the state's fiscal conservation regarding human services are major obstacles, Texas appears to be moving toward an emphasis on community services. For example, TDMHMR's Strategic Plan calls for a 20 percent reduction in the state school population by 1991; state law explicitly supports service In the least restrictive, most normalized setting possible; and all respondents expressed support for the concepts of community integration and individualized services. In addition, the existence of local MRAs and CMHMR Centers provides a framework for service delivery at the community level.
Federal Policy Implications
Texas is unlikely to be able to make major changes in Its MR/DD service system without external encouragement and financial and technical assistance. The state's heavy use of Medicaid to support both institutional and community services indicates that restructuring of the ICF-MR program to increase incentives for community services could be effective in accelerating the move toward a community-based system.
Respondents seem receptive to the idea of increased Federal influence in the development of community services, provided that Federal policy changes recognize the obstacles to Texas' development of community services and do not punish the state for choices made in the past.
| EXHIBIT A-5: Texas Service Delivery System |
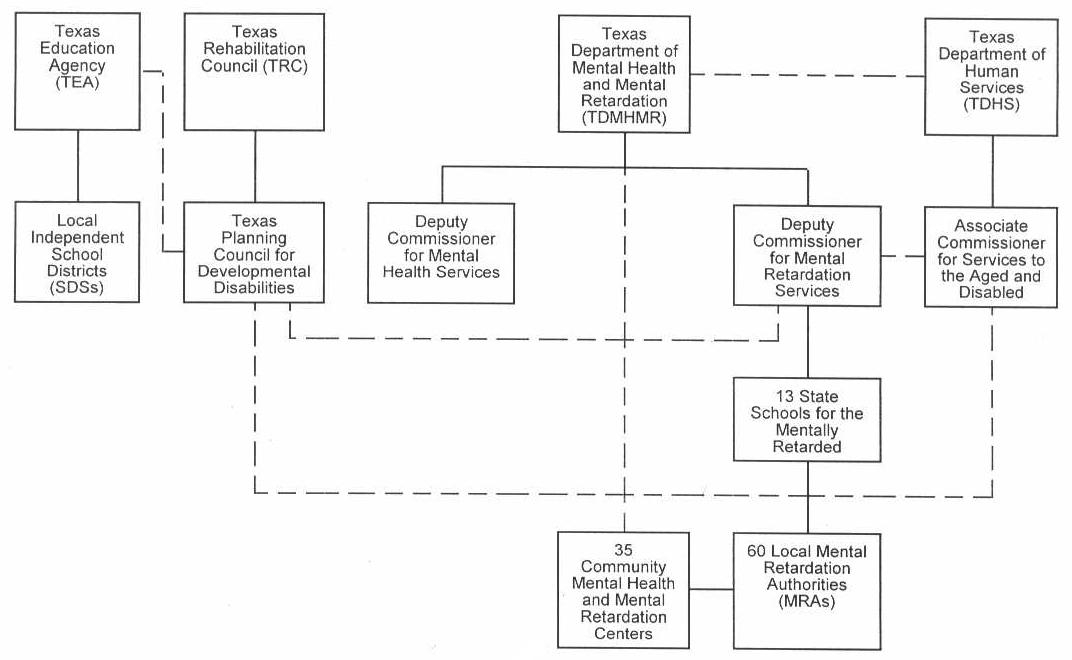 |
State Agency Representatives on DD Council:
Solid lines represent direct authority and oversight Broken lines represent coordination, communication, or indirect or limited authority |
Texas Site Visit - Interviews
David Rollins Assistant Deputy Commissioner for MR Services Texas Department of Mental Health and Mental Retardation
Carmen Quesada Executive Director ARC - Texas
Janice Caldwell Associate Commissioner for Services to the Aged and Disabled Texas Department of Human Services
Spencer McClure Executive Director Texas Council for Community MHMR Centers
Dick Johnson Executive Director Texas Association of Private ICF-MR Providers (TAPP)
Rober Webb Executive Director Texas Planning Council for Developmental Disabilities
Ann Smisko Texas Education Agency
Source Documents
Association for Retarded Citizens/Texas. Legislative Platform.
Texas Association of Private ICF-MR Providers. Comments on Proposed Rule: Medicaid Program Standards for ICFs/MR BERC-226-P., May 1, 1986.
_____. Community-Based ICF-MR Program Issues. March 16, 1987.
_____. Recommendations to the Sunset Advisory Commission, July 15, 1986.
Texas Department of Mental Health and Mental Retardation. Executive Fact Book, FY 1986.
_____. Initial Strategic Plan, 1986 - 1991.
_____. Intermediate Community Services Program Overview.
Texas Department of Mental Health and Mental Retardation and Texas Department of Human Services. Corrective Action Plan for Waiver Oversight Review.
Texas Rehabilitation Commission. Programs and Budget Request, 1988 - 1989 Biennion.
Texas Rehabilitation Commission and Texas Planning Council for Developmental Disabilities. State Plan for Texans with Developmental Disabilities, FY 1987-89.
VIRGINIA MR/DD SERVICE SYSTEM
I. Overview
Background
Virginia has a population of approximately 5.9 million. Although Northern Virginia belongs to the metropolitan Washington area, the state does have a significant rural population. The Virginia Department of Mental Health and Mental Retardation estimates the base population in need of services at approximately 11,000. This figure does not include the nonretarded, developmentally disabled population.
Major System Characteristics
Virginia's MR/DD system relies heavily on institutional care and has not yet developed a comprehensive array of CBS. The system is characterized by a high level of decentralization; Community Service Boards (CSBs)--the local MR/DD service authority--are responsible for nearly all community-level services.
Issues for Community Service Development
The major barriers to expansion of CBS have been:
- The high level of investment in the institutional system
- The absence of unified, effective advocacy for community services
- Opposition from parents of institutional clients and the general public
Virginia's ability to expand the CBS system will largely depend on the level of public awareness and legislative support. Most respondents expressed optimism about the changes for increasing support and funding for community MR/DD services.
Federal Policy Perspectives
Most respondents' suggestions for Federal policy reform reflected Virginia's need to meet rising institutional costs while also trying to establish and operate community services.
Specific observations included:
- ICF-MR's bias toward large facilities
- The need for incentives, rather than threats for devveloping community services
II. Service System Profile
Major Actors in the Service System
The major agencies involved in providing services to the MR/DD population include the Department of Mental Health and Mental Retardation (DMHMR), the Department of Medical Assistance and Services (DMAS), and the 40 local CSBs.
DMHMR Responsibilities
- Administration and operation of the state's large public residential facilities (PRFs) for the mentally retarded
- Planning, policysetting, and budget development
- Monitoring and quality assurance
- Funding of the 40 CSBs (although DMHMR and the local CSBs sign annual performance agreements, DMHMR has no line authority over the CSBs)
Community Service Board (CSB) Responsibilities
- CSBs provide six core services defined by statute (emergency care, in/out patient services, residential care, day support, and prevention/intervention services) to mentally ill and MR/DD individuals, and substance abusers. Only emergency services are mandated.
- The state provides funds which range from 37 percent to 90 percent of individual CSB budgets.
- The local share of CSB budgets is raised from a mix of local property taxes, client fees, and other contributions.
- Individual CSBs have significant autonomy in planning, policy setting, and service delivery. A local CSB can choose the services to be provided, the method of service delivery, and, to a limited extent, the population to be served. The CSB may either provide services directly or through contract.
- Monitoring and quality assurance also are CSB responsibilities.
DMAS Responsibilities
- Administration of the ICF-MR program; DMHMR pays the non-Federal match.
- Monitoring of the ICF-MR program: the Department of Health licenses the ICFs-MR; DMAS conducts an annual inspection of care and utilization review for each facility and each resident, checking for active treatment and client eligibility for ICF-MR; and DMAS can decertify Individual clients and deny payment for services.
- DMAS provides training and technical assistance for DMHMR personnel and ICF-MR operators.
Other important actors in the MR/DD service system include: the Department for Rights of the Disabled; the Department of Education; local school districts; the Department of Rehabilitative Services (DRS); ARC-Virginia; and Parents and Associates of the Institutionalized Retarded (P.A.LR.), a pro-institution advocacy group.
Interagency Cooperation
- DMHMR has formal interagency agreements on both the state and local levels with DMAS and the DRS
- Respondents from both DMHMR and DMAS reported that, in addition to formal agreements, the actual working relationship between the two agencies has improved in recent years.
- One respondent described the status of interagency cooperation as "working toward working together." He cited a new interagency agreement involving 11 human service agencies which will enable the individual agencies to understand more clearly what the other agencies do.
Institutional Services
Virginia operates five state training centers for the mentally retarded with a total capacity of 3,000 beds. (The current census is slightly under capacity.) All beds are ICFMR or SNF certified. HCFA "look-behind" surveys recently forced the state to make large capital investments and staffing increases in the state facilities to comply with physical plant and active treatment requirements.
Community Services
Nearly all CBS are operated through the CSB system. As a result, services vary greatly throughout the state. CSBs have the option of contracting with the private sector, but respondents indicated that the use of private providers is limited.
Residential Services
CSBs operate more than 100 group homes for 12 or fewer people. CSBs also operate or contract for small ICFs-MR with a total capacity of 200 beds. The Department of Social Services operates "adult homes"--similar to foster homes--for mentally retarded adults.
Non-Residential Services
Non-residential CBS provided by CSBs Include case management, vocational training and supported employment, day treatment programs, and emergency services. Three CSBs are developing family support and respite care as pilot projects.
Approximately 3000 children participate in the infant stimulation program.
The DRS, DMHMR, and the Rehabilitation Research and Training Center at Virginia Commonwealth University are working together on a major supported employment project that is made up of the following:
- The project is funded through a 5-year grant from OSERS in the U.S. Department of Education.
- The emphasis of the supported employment programs is assisting severely disabled people who have not previously been successful in competitive employment.
- The program uses a variety of models of supported employment including the use of job coaches, placement of small groups of disabled people in established industry, and the use of mobile work crews.
Virginia requires local school districts to provide special education services for all handicapped children aged 2 to 21. Virginia's requirement for special education preceded P.L. 94-142.
The Department of Education has recently initiated a program to address the needs of handicapped students exiting special education. This program involves vocational assessments for students in the years prior to their leaving school in an attempt to prepare for transition to appropriate vocational programs.
Client Population
Approximately 7,500 people with mental retardation receive community services. The majority of people with mental retardation and developmental disabilities who are being served in community programs have never been in the large state facilities, and, in general, are less disabled than those in the state training centers. CSBs have traditionally regarded the residents of the training centers as a state responsibility, and MR/DD people living in local communities as CSB responsibilities. CSB representatives did not report any significant pressure from the state to serve people who are being de institutionalized.
General Financing and Service Development Issues
DMHMR reports that expenditures for institutional and community services total approximately $126 million. Of this total, $105 million supports the state-operated training centers. State funding for community services is $21 million.
ICF-MR Program
Most state facility beds are ICF-MR certified (the rest are SNF certified). There is one privately operated 60 person ICF-MR, and approximately 12 CSB-operated ICFs-MR for 16 or fewer people.
Clients are admitted to ICFs-MR on the basis of financial eligibility and a functional assessment. One respondent noted that financial eligibility criteria do not serve as a restraint on admissions to ICFs-MR; those who qualify on the basis of the functional assessment can nearly always qualify financially. Expenditures for the ICF-MR program total approximately $97 million.
Waiver Experience
Virginia submitted a Waiver proposal in 1985, but HCFA did not approve the application. Respondents suggested several reasons for HCFA's disapproval and the state's decision not to pursue revisions:
- The high cost of the services proposed
- The proposal became too complicated and was prepared under a great deal of publicity--"it tried to be all things to all people"
- Lack of effective cooperation between DMHMR and DMAS
- Concern about the instability of the Waiver
DMHMR and DMAS officials and other respondents indicated that some of the problems which plagued the development of the first Waiver proposal have been resolved. Virginia plans to submit a new Waiver proposal in 1987 or 1988.
Community Service Development Costs
The costs of developing community services are usually financed through CSB operating or capital budgets. Although the state has provided some startup funds--usually allotted through an RFP process--DMHMR officials report that the level of state investment in community services is relatively low in comparison to investment in institutions.
III. Experience With and Development of CBS
Development of CBS in Virginia
Virginia established the framework for the delivery of CBS with the establishment of the CSB. The creation of the CSB system committed the state to a decentralized approach to the development of community services for the MR/DD population. The population of the large PRFs has declined from approximately 4,500 to 3,000 over the past 10 years. Although the training centers currently admit clients, the overall census continues to decline.
Unlike many other states, Virginia has not had the impetus of either a major class action lawsuit or a strong network of pro-CBS advocates to expedite the development of community services. Virginia's limited progress in developing an extensive and comprehensive network of CBS was attributed to:
- The absence of a strong pro-CBS advocacy group
- The high level of financial and emotional investment in the state training centers
- The influence of P.A.I.R.
- A general lack of resources
Current Emphasis on CBS
The consensus among respondents seemed to be that although Virginia is in a period of transition to a stronger emphasis on CBS, the state continues to rely heavily on large PRFs:
- DMHMR officials estimate that approximately 80 percent of state MR/DD expenditures are for institutional services
- Several respondents indicated that although the state has voiced a commitment to community services, financial support has not followed yet. DMHMR officials and several other respondents are optimistic about the legislature's willingness to increase support for MR/DD services.
Gaps in CBS
Interviewees reported that significant gaps remain in the community service system:
- Nearly all respondents cited the lack of affordable housing for the MR/DD population as a major problem.
- Case management, vocational services, and day treatment programs are reportedly inadequate especially for the "aging out" population.
- Respondents also indicated that children, dually diagnosed, medically fragile and severely disabled clients, and autistic people are not served well.
- Some rural areas of the state lack the resources necessary to provide all needed services.
Goals for CBS/Issues to be Resolved
Future progress will be affected by:
- The level of public awareness of the needs of MR/DD people
- The effectiveness of advocacy groups
- The decentralized nature of the community service delivery system
- Legislative willingness to expand funding for MR/DD services
- State of the economy
Goals for community services:
- Meet the needs of MR/DD people who are not being served adequately
- Expand the range and level of services available in the community
- Improve services for severely handicapped individuals
- Improve services for those in transition from special education to adult life
- Obtain a workable Title XIX waiver
Issues to be resolved:
- Equitable allocation of state funds among CSBs
- Shifting resources from operating budgets of state PRFs to development and operation of community services through CSBs
IV. Perspectives on Federal Policy
Incentives/Barriers
Respondents indicated that Federal policies impose several major barriers to community service expansion:
- The difficulty of using Medicaid funds to support community services impedes progress in developing those services. Specifically, respondents cited the regulatory bias toward large facilities and the inability to "make the dollars follow the client" from institution to community.
- The high cost of complying with Federal ICF-MR regulations limits the resources available for community services. This is especially true of the costs associated with complying with the results of the look-behind surveys.
- Complex Federal wage and hour laws pose problems for some, less-sophisticated community providers.
Policy Recommendations
The majority of suggestions about Federal policy changes focused on Medicaid reform:
- Offer incentives for increasing CBS rather than penalties for not doing so. For example, one respondent suggested establishing higher Federal matching rates for community services.
- Modify regulations to correct ICF-MR's institutional bias.
- Allow Medicaid funds to focus on the client and individual service instead of on facilities.
- Create a separate MR/DD authority within Medicaid.
- Remove ICF-MR from Medicaid.
- Change waiver requirements to cover the temporarily higher costs of operating a dual institutional/community system.
Other suggestions included:
- A tax incentive for parents of an MR/DD person to set aside money to meet the future needs of their child
- Federal efforts to help alleviate the shortage of affordable housing
Nearly all respondents stressed the need for the Federal Government to take a stronger leadership role in promoting community services for the MR/DD population.
V. Summary
General Observations
If judged on the basis of expenditures and available services, Virginia does not emphasize CBS for the MR/DD population. However, all respondents displayed strong interest in expanding the range of services available in the community. The major obstacles appear to be the heavy investment in institutions, and the difficulty of meeting rising institutional costs while trying to develop and operate community services.
The decentralized nature of the community service delivery system limits the state's ability to implement policy decisions.
Federal Policy Implications
Because Virginia has not used Title XIX to support CBS, minor changes in the ICF/MR program are unlikely to have a major effect on the array and availability of program services.
The reorientation of Title XIX to CBS, including reduced incentives to fund PRFs, has the potential to promote expanded resources to the CSBs for community services. A permanent HCB Waiver might be helpful in addressing concerns that the state would have to pick up Federal costs should the Waiver demonstration end.
The state is committed to the CSB system; however, the state's lack of control over the CSBs' decisions means that Federal policy changes which affect state incentives will not necessarily be translated into expanded/improved community MR/DD services.
| EXHIBIT A-6: Virginia Service Delivery System |
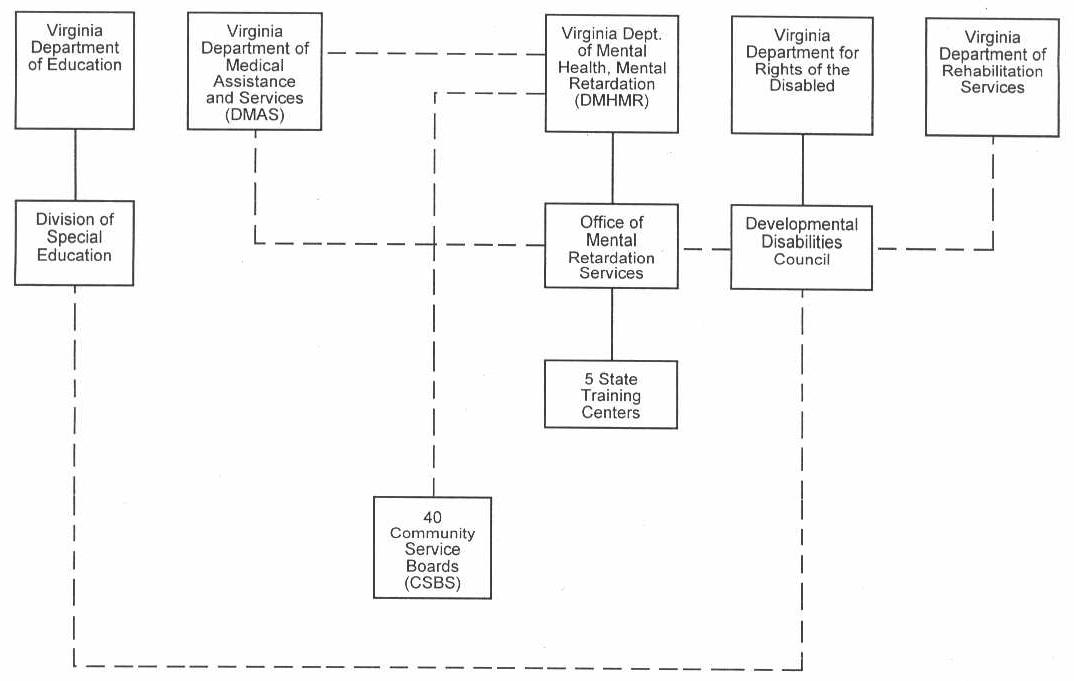 |
| Solid lines represent direct authority and oversight Broken lines represent coordination, communication, or indirect or limited authority |
Virginia Site Visit - Interviews
James C. Bumpas Assistant Commissioner, Program Support Virginia Department of Mental health and Mental Retardation
Stanley J. Butkus Director, Office of Mental Retardation Services Virginia Department of Mental Health and Mental Retardation
Ann Cook Virginia Department of Medical Assistance and Services
Susan Spielberg Acting Director Virginia Department for Rights of the Disabled
Jim Rothrock Director Board of Rights of the Disabled
Austin T. Tuning Director Division of Special Education Administration and Finance Virginia Department of Education
J.T. Paciocco Director of Special Projects Virginia Department of Rehabilitative Services
Grant Revell State Program Supervisor for Supported Employment Virginia Department of Rehabilitative Services
Janet Hill Virginia Department of Mental Health and Mental Retardation
Martha Wingfield Henrico Area Mental Health and Mental Retardation Services
Shelba Murphy President Association for Retarded Citizens - Virginia
LeRoy A. Aarons Parents and Associates of the Institutionalized of Virginia, Inc.
APPENDIX B: KNOWLEDGEABLE INDIVIDUALS CONSULTED
Robert Gettings, Executive Director, National Association of State Mental Retardation Program Directors
Ruth Katz, National Association of State Mental Retardation Program Directors
Susan Ames-Zierman, Executive Director, National Association of Developmental Disabilities Councils
Marty Ford, ARC - U.S.
Joni Fritz, National Association of Private Residential Facilities for the Mentally Retarded
Richard Jensen, American Public Welfare Association
Brian Burwell, Systemetrics
Charlie Lakin, Center for Residential and Community Services, University of Minnesota
Wayne Smith, HHS, HCFA
Kris Rogge, HHS, Administration on Developmental Disabilities
APPENDIX C: BIBLIOGRAPHY
Allard, Marcy and Toff, Gail. Current and Future Development of Intermediate Care Facilities for the Mentally Retarded. Intergovernmental Health Policy Project, August 1980.
Braddock, D. and Hemp, R. "Governmental Spending for Mental Retardation and Developmental Disabilities, 1977-1984." Hospital and Community Psychiatry, Vol. 37, No. 7. July 1986.
Braddock, D.; Hemp, R.; and Fijura, G. Public Expenditures for Mental Retardation and Developmental Disabilities in the United States: State Profiles, 2nd Edition: FY 1977-86, September 1986.
Braddock, D.; Howes, R.; and Hemp, R. A Summary of Mental Retardation and Developmental Disabilities Expenditures in the United States: FY 1977 - 1984. (Preliminary Working Data), July 1984.
_____. Public Expenditures for Mental Retardation and Developmental Disabilities in the United States: Analytical Summary.
City of New York, Human Resources Administration. The Management of Publicly Financed Home Care. November 1984.
Cohen, Joel (The Urban Institute). Public Programs Financing Long-Term Care. January 1983.
Human Services Research Institute. Longitudinal Study of the Court-Ordered Deinstitutionalization of Pennhurst Residents: Comparative Analysis of the Cost of Residential, Day and Other Programs Within Institutional and Community Settings. August 1984.
Intergovernmental Health Policy Project. Focus on...Nursing Home Reimbursement Under Medicaid, February 1986.
Lakin, K.C.; Hill, B.K.; and Bruininks, R.H. (Eds.). An Analysis of Medicaid's Intermediate Care Facility for the Mentally Retarded (ICF-MR) Program. Minneapolis: University of Minnesota, Department of Educational Psychology, 1985.
Lakin, K.C.; Hill, B.K.; Street, H.; and Bruininks, R.H. Persons with Mental Retardation in State-Operated Residential Facilities: Years Ending June 30, 1984 and June 30. 1985 with Longitudinal Trends from 1950 to 1985. Minneapolis: University of Minnesota, Department of Educational Psychology, 1986.
Long-Term Care Policy Coordinating Council. Long-Term Care Financing in New York State: 1985-2010. September 1985.
Macro Systems, Inc. Synthesis of Cost Studies on the Long-Term Care of HealthImpaired Elderly and Other Disabled Persons. September 1985. [http://aspe.hhs.gov/daltcp/reports/syncost1.htm]
Mathematica Policy Research, Inc. A Study of the Early Implementation Experience of the Wisconsin Community Options Program. January 1984.
Menninger, Heather (Intern, U.S. DHHS, Health Care Financing Administration). Issues in the Development, Programming, and Administration of Community Residential Facilities for Developmentally Disabled Persons. October 1980.
National Association of State Directors of Special Education. Severely Handicapped Youth Existing Public Education: Issues and Concerns. 1986.
National Association of State Mental Retardation Program Directors. Trends in Capital Expenditures for Mental Retardation Facilities: A State-by-State Survey, June 1980.
_____. Selected State Policies Governing the Operation of Community ICF-MR Facilities. April 1984.
_____. The Federal Look Behind Initiative: Impact on the States. February 1986.
National Governors' Association, Center for Policy Research. State Reimbursement Policies for Privately Operated Intermediate Care Facilities for the Mentally Retarded: 1984.
New York State Commission on the Quality of Care for the Mentally Disabled. Willowbrook: From Institution to the Community: A Fiscal and Programmatic Review of Selected Community Residents in New York City. August 1982.
Petronko, Michael; Nezo, Arthur; and Pos, Aaltje. Natural Setting Therapeutic Management (NSTM) Asian Alternative to Institutionalization for the Severely Mentally Retarded. 1982.
Rymer, Marilyn; Burwell, Brian; Madigan, Denise; and Adler, Gerald. Short-Term Evaluation of Medicaid: Selected Issues. January 1984.
State of Washington, Department of Social and Health Services. Community-Based Care, Systems for the Functionally Disabled: A Project in Independent Living.
State of Wisconsin Department of Health and Social Services, Bureau of Evaluation, Division of Policy and Budget. Interim Evaluation of the Community Integration Program. July 1985.
Temple University Developmental Disabilities Center. A Matched Comparison Study of Cost Effectiveness: Institutionalized and Deinstitutionalized Clients.
Temple University Developmental Disabilities Center and Human Services research Institute. The Pennhurst Longitudinal Study: Combined Report of Five Years of Research and Analysis. 1985. [http://aspe.hhs.gov/daltcp/reports/5yrpenn.htm]
Texas Tech University Research and Training Center in Mental Retardation. Comparative Costs of Public Residential and Community Residential Facilities for the Mentally Retarded. Working Paper W-50. 1983.
Touche Ross and Company. Cost Study of the Community-Based Mental Retardation Regions and Beatrice State Developmental Center. (Unpublished Study for Nebraska Department of Public Institutions and Public Welfare). August 1980.
U.S. Department of Health and Human Services, Assistant Secretary for Planning and Evaluation. Policies for Improving Services for Mentally Retarded and Other Developmentally Disabled Persons Served Under Title XIX of the Social Security Act. January 1986.
U.S. Department of Health and Human Services, Health Care Financing Administration. Grants and Contracts Report: Short-Term Evaluation of Medicaid, Selected Issues. October 1984.
_____. Studies Evaluating Medicaid Home and Community-Based Care Waivers. December 1984.
_____. Study of the Skilled Nursing Facility Benefit Under Medicare. January 1984.
U.S. Department of Health and Human Services, Office of the Inspector General. Board and Care Homes: A Study of Federal and State Actions to Guard the Health and Safety of Board and Care Home Residents. April 1982.
U.S. General Accounting Office, Human Resources Division. Financing Health and Education Services for Handicapped Children (GAO/HRD-86-62BR). July 1986.
Wisconsin Department of Health and Social Services. Report on Health Care Coverage for Working-Age Persons with Physical Disabilities.
APPENDIX D: DISCUSSION GUIDE
Name, Title: Agency/Organization: Address: Telephone: Interviewed By: Date:
1. How would you characterize the (name of state) MR/DD system in relation to:
(1) Degree of emphasis on community-based vs. state institution services? (2) Involvement of private providers? (3) Supports to families? (4) How do you define community-based services?
2. What is your agencys (organizations) role in providing services to the MR/DD population? Other roles?
3. A. Describe the range of state-supported services available on the community level, beginning with the residential programs:
Probes: (1) ICFs/MR >15 (2) ICFs/MR 15 (3) Non-ICF/MR community residential facilities (4) Foster homes (adult? children?) (5) Specialized facilities (For what populations?) (6) Nursing homes (SNF? ICF?) (7) Respite care (8) Other?
3. B. Non-residential services:
Probes: (1) Case management (2) Vocational training programs (3) Day treatment (4) Supported employment (5) Family support (6) Other?
3. C. Services administration responsibilities:
Probes: (1) Planning and priority-setting (2) Services development (3) Selection of providers (4) Oversight of providers (5) Other?
4. What populations participate in community-based services?
Probes: (1) Deinstitutionalized vs. never in institutions: (2) Number in community programs vs. number in state facilities: (3) Percent in relation to level of functioning, multiple disabilities:
5. What gaps remain in the community-based service system?
Probes: (1) By type of service or type of client? (2) By geographic area? (3) Other?
6. A. How are community-based services financed?
Probes: (1) Federal funds: Medicaid, SSBG, HUD 202/Section 8, SSI, Medicare, SSDI, other? (2) State funds: non-Federal Medicaid share, general funds, dedicated funds, other? (3) Local funds: local government general funds, local government dedicated funds, other? (4) Individual client and/or family payments? (5) Other?
6. B. How has (name of state) used the Medicaid waivers?
Probes: (1) Home and community-based care waiver experience? (2) Other? (3) If not, why not?
6. C. How are community service development costs financed?
6. D. How are state institution costs financed?
Probes: (1) Program services? (2) Capital improvements/ICF/MR plans of correction/new construction?
6. E. Other MR/DD system costs?
6. F. What are the major influences on MR/DD expenditures?
Probes: (1) State budget allocations? (2) Other state expenditures/revenue sources? (3) Local government? (4) Other?
7. How are costs for community-based services being controlled? By whom?
Probes: (1) Reimbursement limits (2) Eligibility restrictions (3) Case management (4) Competitive bidding (5) Other
8. What type of quality assurance mechanisms are in place for clients in community-based services?
Probes: (1) Where is the primary responsibility for quality assurance? (2) How closely are services generally monitored? (3) What sanctions are available? How often used? (4) How is client outcome considered vs. process indicators?
9. How does (the MR/DD agency) work with other agencies involved in the MR/DD service system?
Probes: (1) Interagency agreements (2) Coordination/cooperation at the community level (3) Between the state and local level
10. What factors have contributed to the expansion of community-based services? Why?
Probes: (1) Philosophical commitment? Whose? (2) Court actions (3) Medicaid waivers (4) Other
11. What are/have been the barriers to community-based services?
Probe: How could have they been overcome?
12. What are the short-term goals for community-based services? Long-term?
Probes: (1) Plans for achieving those goals? (2) Factors most likely to affect the implementation of these plans? (3) Are there other goals/strategies that might be preferable? In what ways?
13. A. What Federal policy/program changes would be most helpful in achieving those objectives? Why?
13. B. What changes in Federal policies/Federal programs would be least helpful? Why?
14. What else is it important to understand in looking at the (name of state) MR/DD system?
Probes: (1) Any other people we should be sure to talk to? Phone number? (2) Any reports, budget documents, etc., we should have? (3) Anything else youd like to add?
NOTES
-
This is unlike the public mental health system , which frequently charges for services based on ability to pay, but which serves primarily a low-income population without access to the private sector. The public MR/DD system in most states is the primary service system to people of all but the highest income levels.