
Human Services Research Institute
September 2019
Printer Friendly Version in PDF Format (105 PDF pages)
ABSTRACT
This project evaluated needs assessment methodologies for substance use disorder treatment capacity, highlighting best practices and identifying gaps and opportunities for improvement. This Environment Scan became Appendix C for the Final Report, available at https://aspe.hhs.gov/basic-report/needs-assessment-methodologies-determining-treatment-capacity-substance-use-disorders-final-report.
This report was prepared under contract #HHSP233201600015I between HHS's ASPE/DALTCP and the Human Services Research Institute. For additional information about this subject, you can visit the DALTCP home page at https://aspe.hhs.gov/office-disability-aging-and-long-term-care-policy-daltcp or contact the ASPE Project Officer, Judith Dey, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. Her e-mail address is: Judith.Dey@hhs.gov.
DISCLAIMER: The opinions and views expressed in this report are those of the authors. They do not reflect the views of the Department of Health and Human Services, the contractor or any other funding organization. This report was completed and submitted on July 13, 2018.
"
ACRONYMS
The following acronyms are mentioned in this report and/or appendices.
| ACA | Affordable Care Act |
|---|---|
| ACF | HHS Administration for Children and Families |
| AIDS | Acquired Immune Deficiency Syndrome |
| ASAM | American Society for Addiction Medicine |
| ASPE | HHS Office of the Assistant Secretary for Planning and Evaluation |
| BHSIS | Behavioral Health Services Information System |
| BLS | Bureau of Labor Statistics |
| BRFSS | Behavioral Risk Factor Surveillance System |
| CAPT | SAMHSA Center for the Application of Prevention Technologies |
| CAST | Calculating for an Adequate System Tool |
| CDC | HHS Centers for Disease Control and Prevention |
| CFR | Code of Federal Regulations |
| CHA | Community Health Assessment |
| CHI | Community Health Improvement |
| CHNA | Community Health Needs Assessment |
| CMS | HHS Centers for Medicare & Medicaid Services |
| CNA | Community Needs Assessment |
| COD | Co-Occurring Disorder |
| COR | Contracting Office Representative |
| DAWN | Drug Abuse Warning Network |
| DHCS | California Department of Health Care Services |
| DHHS | North Carolina Department of Health and Human Services |
| DSM-IV | Diagnostic and Statistical Manual of Mental Disorders, 4th edition |
| DSRIP | Delivery System Reform Incentive Program |
| EBP | Evidence-Based Practice |
| FPL | Federal Poverty Level |
| FTE | Full-Time Equivalent |
| FY | Fiscal Year |
| GAO | U.S. Government Accountability Office |
| HHS | U.S. Department of Health and Human Services |
| HIV | Human Immunodeficiency Virus |
| HPSA | Health Professional Shortage Area |
| HRSA | HHS Health Resources and Services Administration |
| HUD | U.S. Department of Housing and Urban Development |
| ICF | International Classification of Functioning, Disability and Health |
| IMU | Index of Medical Underservice1 |
| IOM | Institute of Medicine |
| IRB | Institutional Review Board |
| IRS | Internal Revenue Service |
| LGBT | Lesbian, Gay, Bisexual, Transgender |
| LGBTQ | Lesbian, Gay, Bisexual, Transgender, Queer and/or Questioning |
| LME-MCO | Local Management Entity-Managed Care Organization |
| MAT | Medication-Assisted Treatment |
| MCO | Managed Care Organization |
| MeSH | Medical Subject Headings |
| MHBG | Community Mental Health Services Block Grant |
| MIS | Management Information System |
| MUA/P | Medically Underserved Areas/Populations |
| N-MHSS | SAMHSA National Mental Health Services Survey |
| N-SSATS | SAMHSA National Survey of Substance Abuse Treatment Services |
| NACCHO | National Association of County and City Health Officials |
| NACT | Network Adequacy Certification Tool |
| NAPHD | National Association of Public Health Directors |
| NCHS | HHS National Center for Health Statistics |
| NHCS | CDC National Hospital Care Survey |
| NPHAB | National Public Health Accreditation Board |
| NSDUH | HHS National Survey on Drug Use and Health |
| NY CNA | New York Community Needs Assessment |
| Opioid STR | State Targeted Response to the Opioid Crisis Grant |
| OTP | Opioid Treatment Program |
| PHAB | Public Health Accreditation Board |
| PPS | Performing Provider Systems |
| RSA | Rehabilitation Services Administration |
| SAMHSA | HHS Substance Abuse and Mental Health Services Administration |
| SAPTBG | Substance Abuse Prevention and Treatment Block Grant |
| SIG | State Incentive Grant |
| SOW | Statement of Work |
| SPF | Strategic Prevention Framework |
| SSR | State Sampling Region |
| SUD | Substance Use Disorder |
| TAG | Technical Advisory Group |
| TEDS | Treatment Episode Data Set |
| VA | U.S. Department of Veterans Affairs |
| YRBSS | Youth Risk Behavior Surveillance System |
EXECUTIVE SUMMARY
Introduction and Background
Project Overview
In September 2017, the Office of the Assistant Secretary for Planning and Evaluation contracted with the Human Services Research Institute to evaluate needs assessment methodologies for substance use disorder (SUD) treatment capacity. The overarching aim of the project is to enhance the effectiveness of needs assessment to promote organization and system change, addressing gaps in the existing data and promoting the implementation of evidence-based practices (EBPs), peer supports, and innovative technologies. The project was advised by a Technical Advisory Group (TAG) composed of nine non-government experts and three government experts.
Need for Effective SUD Treatment Capacity Needs Assessment
According to the Substance Abuse and Mental Health Services Administration (SAMHSA, 2017), in 2016:
-
An estimated 28.6 million people (10.6% of the population aged 12 and older) had used an illicit drug in the month before the survey.
-
An estimated 16.3 million people aged 12 and over were heavy alcohol users.
-
An estimated 15.1 million people aged 12 or older met Diagnostic and Statistical Manual of Mental Disorders (4th edition) criteria for alcohol dependence or abuse.
-
An estimated 21.0 million people aged 12 or older, about one in 13, needed substance use treatment.
-
Approximately 3.8 million people, 1.4% of all people aged 12 or over and 10.6% of those needing treatment, received any substance use treatment in the past year.
According to SAMHSA data for 2015, of the adults who needed substance use treatment but did not receive specialty treatment, only 4.8% (863,000) felt that they needed treatment for their use of alcohol or illicit drugs. About 1.7% of this group made an effort to obtain treatment, and 3.7% felt they needed treatment but did not make an effort to obtain it (SAMHSA, 2016).
Approach and Methods
We reviewed literature on needs assessment specific to SUD treatment capacity and recent literature on needs assessment methodology generally to formulate an operational definition of SUD "treatment system needs." We then developed a protocol for retrieving and systematically reviewing a sample of SUD needs assessment reports to examine:
-
Questions addressed.
-
Populations addressed.
-
Workforce categories addressed.
-
Settings incorporated.
-
Levels of care incorporated.
-
Data sources/methods used.
-
Best practices identified.
-
Method validation (if any).
The protocol also included criteria for rating the quality of needs assessments, based on the approach of systematic literature reviews.
We conducted a systematic search of SUD needs assessment in the grey and published literature, resulting in a convenience sample for review, consisting of two categories: "mandated" needs assessments (usually those produced in response to some funding requirement, which address SUD among other public health issues) and "locally initiated" needs assessments, typically one-time studies conducted in connection with a state or county SUD policy initiative. We reviewed these two categories separately, with a summary overview of mandated reports and a more fine-grained analysis of the locally initiated reports. Two additional research questions were addressed by separate scans, examining how states operationalize network capacity and whether there are needs assessments of other provider types that might be adapted to SUD.
Definition of Needs Assessment. Based on the literature review, needs assessment was operationally defined for purposes of the search and analysis as consisting of four components: (1) a measurement of the current condition ("what is"), (2) a specification of the optimal state ("what should be"); (3) a measurement of the gap between the current and optimal states; and (4) recommendations, ideally prioritized, for actions to address the gap.
Results
The search produced a convenience sample of 40 reports, seven mandated and 33 locally initiated, selected to be diverse in geographical area, type of substance abuse, and populations.
Mandated Needs Assessments
There are at least 14 types of nationally required needs assessments that typically address SUD among other public health issues topics addressed. Compared to locally initiated needs assessments, these are fairly generic in their approach because they are required to follow specific guidelines; we therefore subjected these to a more general overview rather than the detailed data extraction applied to locally initiated assessments, focusing on three types: (1) those required by SAMHSA including the Substance Abuse Block Grant and Mental Health Services Block Grant programs, Strategic Prevention Framework State Incentive Grants, and State Targeted Response to the Opioid Crisis Grants; (2) Community Health Needs Assessments (CHNAs), which are required of all non-profit hospitals; and (3) Community Health Assessments (CHAs), which are conducted by local public health agencies for accreditation by the National Association of Public Health Directors (NAPHD).
SAMHSA Grant Programs. Requirements for SAMHSA needs assessments mainly consist of a set of questions to be addressed, with little guidance or requirements related to methodology. The major strengths of the SAMHSA-mandated reports are in addressing the "what is" component of a needs assessment: describing the existing service system, utilization patterns, and consumer characteristics. The greatest limitations are in the approach to measuring need, which typically consists of no more than prevalence figures from national data sources such as National Survey on Drug Use and Health (NSDUH) compared to utilization statistics.
Community Health Needs Assessments. CHNAs benefit from requirements added by the Affordable Care Act to the original Internal Revenue Service requirements that include broad community representation and an accompanying Community Health Improvement Plan detailing activities to be conducted by the hospital to promote public health and address issues identified in the CHNA--the "what should be" component of a needs assessment.
Community Health Assessments. CHAs benefit from initial support provided by the Robert Wood Johnson Foundation and very detailed requirements by the NAPHD for areas and topics to be addressed. Methodology is enhanced by the availability of a framework for conducting the needs assessment known as Mobilizing for Action through Planning and Partnerships, which was developed jointly by the National Association of County and City Health Officials and the Centers for Disease Control and Prevention. Also, many state public health agencies provide additional guidance and support for local agencies.
Locally Initiated Needs Assessments
The following is a summary of results of the review of locally initiated needs assessment, organized according to the research questions.
What questions are addressed?
Approximately 40 different issues and topics were identified, with the largest number, as expected, related to prevalence, utilization, and unmet need. Estimated demand (services likely to be requested in response to certain initiatives) was addressed by 17 of the 33 reports.
Some important topics received relatively limited attention; for example, only a handful of reports addressed network assets and strengths, a topic recommended in the recent methodology literature. Only one report addressed law enforcement, disparities, benefit design, peer involvement, technology, and EBPs, despite the importance of these topics in the field of SUD treatment.
Aspects of quality addressed most frequently were access and availability of services; relatively few reports examined the use of evidence-based treatments, outcomes measurement, and patient satisfaction.
What populations are addressed?
The older reports we reviewed tended to assess need for the general population, whereas more recent reports drilled down to examine availability and accessibility of services for a wide range of specific subgroups, such as demographic subpopulations and persons in a particular status (such as homelessness and incarceration), and users of specific substances.
What workers are incorporated?
Overall, the reports incorporated a wide variety of workforce categories, although individual reports tended to address only a few general categories, and few addressed peers as an aspect of workforce capacity.
What settings (geographic areas/regions) are addressed?
Most reports focused on a specific state, county, or city; only a few focused on urban, rural, or frontier regions/boundaries of the state or county. One focused on a tribal community within the northern portion of a state.
What levels of care are addressed?
We reviewed how the needs assessments addressed levels of care in connection with service capacity--that is, what kind of services are required to meet the individual-level needs of a population, with specific reference to the use of the American Society for Addiction Medicine (ASAM) Levels of Care Criteria. This important feature of needs assessment was relatively neglected, with many reports simply providing data for utilization of existing services without discussion of service gaps and few referencing ASAM Criteria.
What data sources and methods are used?
Most reports combined qualitative and quantitative data. Qualitative data included stakeholder interviews, surveys, focus groups, and public meetings, as well as review of documents. Quantitative usually consisted of national data sets (mostly NSDUH) and local administrative data such as service utilization; a few (mainly academic studies) used social indicators. While a number of the mandated needs assessments (e.g., SAMHSA block grant applications) used the National Survey of Substance Abuse Treatment Services and Treatment Episode Data Set, few of the locally initiated reports drew upon these sources. Notably, none used data from Healthy People 2020 and the National Directory of Drug and Alcohol Treatment Facilities. Need was usually estimated simplistically as the gap between treated and untreated prevalence. Recommendations were seldom data-based; instead, they were presented as expert opinion.
Are there best practices identified?
Our assessment is that the field of SUD treatment needs assessment is not yet sufficiently developed to identify formal best practices, but we were able to identify a number of exemplary and promising approaches, such as techniques to improve the precision of estimates and methods for enhancing the utility of results for planning.
Have any methods been validated?
Only three of the reports described validation of any aspects of methodology.
Quality of SUD Needs Assessment Reports
We rated the quality of the reports using an approach adapted from systematic literature reviews, whereby the quality of studies are rated based on clarity and transparency of the information presented about various aspects of the methodology, in this case the methodology related to the research questions and to needs assessment generally.
Quality ratings for the reports as a whole varied considerably depending on the measure. For example, most reports rated highly on measures related to settings, populations, data methods and limitations, treatment needs and recommendations. On the other hand, few clearly defined the selection criteria for workers and only about half provided clear definitions of levels of care. Few offered more than a brief explanation of need or described validations of any aspects of methodology. About half referenced a model of "what should be," such as the ASAM Level of Care or the SAMHSA Good and Modern Behavioral Health System.
Needs Assessment from Other Provider Types
A separate environmental scan was conducted to identify needs assessments for other provider types that may be adapted for SUD. We examined Health Professional Shortage Areas (HPSA) and Delivery System Reform Incentive Program (DSRIP).
HPSA assessments, which are conducted by primary care clinics applying for Health Resources and Services Administration funding, address provider shortages in primary care, dental care, and mental health. Determination of eligibility for funding is based on a scoring algorithm that is specific to each of the three provider types. Features relevant to SUD needs assessment are: determination of need based on three types of shortage (geographic, population, facilities), scoring based on weights for a set of social indicators, and detailed definitions of components. As a model for SUD treatment capacity needs assessments, the HPSA approach has one primary limitation: it is a method for allocating resources to localities where the shortages are greatest but is not a method for planning at the system level (i.e., allocating resources within areas, such as how many psychiatrists, nurses, social workers, etc., should be provided in a particular area).
DSRIP is a type of Centers for Medicare & Medicaid Services (CMS) Section 1115 Waiver that allows Medicaid funding to be used to create incentives for providers to pursue a wide range of system reforms. States require eligible entities (e.g., health care systems) to submit a plan describing projects and metrics they intend to implement, features of which could provide models for smaller-scale SUD needs assessments. We reviewed one example of a DSRIP report, the Capital Region, Mohawk and Hudson Valley DSRIP Community Needs Assessment (CNA) conducted by the Albany Medical Center and Ellis Performing Provider Systems (Albany Medical Center PPS & Ellis PPS, 2014). Some features of this report that offer models for SUD treatment needs assessments include: engagement with a diverse group of organizations in developing the CNA, diverse methods of data collection designed to fill gaps in any one source, detailed information about providers from the state's Provider Network Data System, distribution of behavioral health providers in local areas (square miles by neighborhood), and summary of system assets and resources.
How States Operationalize Network Adequacy Standards
We also reviewed procedures and policies related to network adequacy standards in selected states (California and North Carolina). Network adequacy standards established by the states reflect the "what should be" condition in a needs assessment as defined (at least implicitly) at the level of state policy making.
CMS regulations require states to develop and assess standards for certain specialty services including behavioral health. These changes aimed to align Medicaid managed care regulations with requirements of other major sources of coverage. There are three parts of the Managed Care Rule that comprise the majority of network adequacy standards:
Time and Distance
States are required to develop time and distance standards for adult and pediatric behavioral health providers (that is, the number of minutes it takes a beneficiary to travel from their residence to the nearest provider site, and the number of miles a beneficiary must travel from their residence to the nearest provider site). Plans are required to meet the standards for time or distance.
Timely Access
Plans are required to meet state standards for timely access to care and services, taking into account the urgency of the need for services. Timely access standards refer to the number of days in which a plan must make an appointment available.
Network Certification
Plans are required to demonstrate that they offer an appropriate range of services that is adequate for the anticipated number of beneficiaries for the service area and that they maintain a network of providers adequate to meet the needs of the anticipated number of beneficiaries.
Some states are using newer approaches to determine if they have sufficient capacity to meet the needs of beneficiaries with SUD.
California
The California Department of Health Care Services (DHCS) has developed a Network Adequacy Certification Tool (NACT) for plans to collect information on location, current capacity, and projected capacity of SUD providers. Using the information from the NACT, the Plan must submit to DHCS geo-access maps of all the network providers in the Plan's service area, which plot the time and distance for all SUD network providers, stratified by service type and geographic location.
North Carolina
The North Carolina Department of Health and Human Services (DHHS) has developed network adequacy standards for plans, but requests that the plans use this information to identify the gaps in network adequacy and accessibility as well as strategies to address the identified gaps. DHHS has developed a tool that set forth requirements for Managed Care Organizations (MCOs) to conduct a Community Behavioral Health Service Needs, Providers and Gaps Analysis and requires MCOs to develop a strategic plan to address gaps for Medicaid and non-Medicaid beneficiaries.
Recommendations and Conclusions
The final report will focus on the research questions that call for recommendations, drawing upon input from the TAG and issues identified in the reviews of literature and needs assessments reports described above. The following are areas identified in the environmental scan that call for recommendations in the final report:
-
Data and methods for gauging treatment needs and gaps.
-
Questions that should be answered in needs assessments.
-
Incorporating best staffing practices, telehealth policies and peer supports into needs assessments.
-
Supplying key pieces of missing data.
-
Validating needs assessment methods.
-
Approaches for making needs assessments more uniform.
-
Increasing the effectiveness of needs assessment in promoting organizational and system change.
Conclusions
The SUD-specific assessments that we reviewed mostly share certain features such as mixed methods of data collection (surveys, key informant interviews, focus groups, services utilization data, etc.) but with considerable variability in the scope and level of detail provided. Some areas of variability include:
-
Extent to which recommendation priorities, feasibility, and strategies are presented.
-
Extent to which resources/assets/strengths are identified.
- Extent to which system capacity needs are broken out by levels of care.
-
Extent to which system redundancy/efficiency is addressed.
Other important aspects of treatment capacity were addressed by only a few of the needs assessments. These included peer involvement, the functions of law enforcement, estimates of changes in demand resulting from system reforms, treatment completion/adherence as an aspect of utilization, and the extent of EBPs.
It is evident from our review that SUD treatment presents some unique challenges for needs assessment, mainly in the considerable variability in how SUD treatment systems are structured and in the relative lack of uniformity in defining aspects of systems (such as workforce designations, service categories, provider types and levels of care) compared to health care and even mental health.
INTRODUCTION
Project Overview
In September 2017, the Office of the Assistant Secretary for Planning and Evaluation (ASPE) contracted with the Human Services Research Institute to evaluate needs assessment methodologies for substance use disorder (SUD) treatment capacity. The overarching aim of the project is to enhance the effectiveness of needs assessment to promote organization and system change, addressing gaps in the existing data and promoting the implementation of evidence-based practices (EBPs), peer supports, and innovative technologies.
Technical Advisory Group (TAG)
ASPE requested the project be advised by a TAG. The group is composed of nine non-government experts and three government experts. It was first convened during a conference call in February 2018, during which the group members provided valuable feedback on the project's research questions as well as the approach and design of the environmental scan. The TAG plays an important role in the project and will continue to provide guidance throughout the project, including guiding the development of recommended best practices in SUD system capacity needs assessment and identifying data improvements for future assessments. This guidance will help form the final report for the project.
The project will result in:
-
A reference library of SUD needs assessments from the peer reviewed and grey literature as well as needs assessments from other fields (e.g., physical health or other specialty health conditions) with direct relevance for SUD service needs assessments.
-
A summary of best practices in various aspects of needs assessment methodology, including specific data sources and data analytic techniques to project capacity needs (by level of treatment, staffing type, and staffing patterns) with a focus on EBPs, recovery supports, and telehealth.
-
An overview of current practices in SUD needs assessments--along with recommendations to address the limitations of existing methods.
Extent of the Problem
The need for an effective needs assessment method for SUD treatment is evident. According to the Substance Abuse and Mental Health Services Administration (SAMHSA, 2017), in 2016:
-
An estimated 28.6 million people (10.6% of the population aged 12 and older) had used an illicit drug in the month before the survey.
-
An estimated 16.3 million people aged 12 and over were heavy alcohol users.
-
An estimated 15.1 million people aged 12 or older met Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) criteria for alcohol dependence or abuse.
-
An estimated 21.0 million people aged 12 or older, about one in 13, needed substance use treatment.
-
Approximately 3.8 million people, 1.4% of all people aged 12 or over and 10.6% of those needing treatment, received any substance use treatment in the past year.
According to SAMHSA data for 2015, of the adults who needed substance use treatment but did not receive specialty treatment, only 4.8% (863,000) felt that they needed treatment for their use of alcohol or illicit drugs. About 1.7% of this group made an effort to obtain treatment, and 3.7% felt they needed treatment but did not make an effort to obtain it (SAMHSA, 2016).
It is evident from these statistics that increasing the number of people recognizing their need for treatment is a major public health issue with important implications for assessing system capacity. Increasing our understanding of how to conduct SUD treatment needs assessment may help communities, states, and the Federal Government ensure that we have adequate treatment capacity.
Research Questions
The project is guided by the following research questions regarding current methods and practices in the field of SUD treatment needs assessment, as specified in the Statement of Work (SOW), with several questions suggested by the project team.
-
How have needs assessments with respect to SUD treatment capacity been conducted in the past? Which populations, workers, settings, and levels of care have been incorporated into the assessments? What data sources and methods have been used? What questions were the assessments meant to answer?
-
Are there needs assessments from other provider types (for example, primary care physicians) that could be applied to the SUD treatment workforce? What are the differences between other workforces and the SUD workforce that might make such application difficult? How could these difficulties be overcome?
-
Are there best practices with respect to these needs assessments? What data and methods most effectively gauge treatment needs and current gaps? What questions should be answered in conducting these needs assessments?
-
How does American Society for Addiction Medicine (ASAM) Levels of Care relate to capacity needs (both in workforce and setting)? How can best staffing practices, telehealth policies, and peer supports be incorporated into needs assessments?
-
What are the key pieces of missing data that would improve these needs assessments, including one-time data collection efforts and potential federal efforts?
-
Have any of these needs assessments methods been validated? If not, how can these needs assessment methods be validated?
-
How can needs assessment approaches be made more uniform while remaining adaptable to local conditions and stakeholder priorities?
-
How can assessments become more effective at promoting organizational and system change to address, rather than simply identify, system gaps?
-
How do states and managed care plans operationalize network adequacy standards?
Approach of the Environmental Scan
Steps in the environmental scan were:
-
Developing a Workplan, reviewed by the Contracting Office Representative (COR) and TAG, specifying tasks and research questions (six from the SOW, with an additional two presented by our team and one added during the Post-Award meeting).
-
Developing a Protocol, also reviewed by the COR and TAG, for retrieving and systematically reviewing a sample of SUD needs assessment reports based on the subset of research questions related to content and practices in the field.
-
Reviewing recent literature on general needs assessment methodology and selected articles on needs assessment specific to SUD treatment capacity as background for reviewing SUD needs assessment reports.
-
Formulating an operational definition of "SUD network capacity" based on the methodology literature and incorporating feedback from the TAG.
-
Conducting a search of SUD needs assessment in the grey and published literature using the search strategy according to the protocol and described in in the Methods section of this report.
-
Scanning needs assessment reports identified according to the search strategy to determine eligibility for inclusion and retrieving those meeting inclusion criteria to create a convenience sample for review.
-
Sorting retrieved reports into two categories defined post-hoc based on the results of the search: "mandated" needs assessments (usually those produced in response to some funding requirement, which address SUD among other public health issues) and "locally initiated" needs assessments, typically one-time studies conducted in connection with a state or county SUD policy initiative.
-
Conducting an overview of the reports and various sources of guidance within the sample of mandated needs assessments to identify typical features and methods.
-
Conducting a fine-grained analysis of the sample of locally initiated needs assessments reports to identify content and quality, using the data extraction tool based on the research questions and presented in the Protocol.
-
Synthesizing findings from the review of locally initiated reports in tabular and narrative form.
-
Conducting a separate scan addressing the research question related to how states operationalize network capacity (added in the Post-Award meeting).
-
Identifying examples to address the research question about how needs assessments from other provider types might be adapted to SUD treatment.
-
Producing this report incorporating the above steps.
Organization of this Report
The report is generally organized according to the research questions from the SOW. These address a diverse array of topics that generally consist of two types: questions related to current practices in the field (e.g., "What data sources and methods have been used?") and questions that call for recommendations (e.g., "Are there needs assessments from other provider types that could be applied to the SUD treatment workforce?"). This report on the environmental scan focuses primarily on the research questions related to practices; however, it includes a preliminary discussion of recommendations. A more detailed discussion of recommendations will be provided in the final report.
The first section of this report consists of a background section with a review of the literature on needs assessment methodology in general and the literature specific to methodology of SUD needs assessment. This is not intended to be a systematic review of literature in the field but rather to clarify the concepts of "needs assessment" and "network capacity" as a framework for addressing the research questions.
The review of needs assessment methodology is followed by a review of a set of SUD treatment needs assessment reports retrieved from the published and grey literature utilizing modified methods of systematic literature reviews. Two types of reports are reviewed. The first, termed "mandated" reports, are those which are conducted by states as a requirement of various federal grant programs or by public health agencies for purposes of accreditation. These generally address SUD among a range of other public health issues. For this type, we provide a general overview of the content and methodology. The second type, termed "locally initiated," are needs assessments specific to SUD conducted on an ad hoc basis--usually in connection with some policy initiative. We review these in more detail, using a protocol for data extraction based on the research questions. Information thus obtained is presented in tabular and narrative form. The protocol is provided in Appendix E.
Next, we address the research question, "How do states and managed care operationalize network adequacy?" which was conducted as a separate scan using different information sources (primarily policy documents).
The next section addresses another single research question, about whether needs assessments for other provider types might be adapted to SUD treatment, by discussing several examples. This discussion will be expanded in the final report.
Finally, we provide a preliminary response to questions that call for recommendations, which will be expanded in the final report, with input from the TAG and the COR.
BACKGROUND
Review of Selected Needs Assessment Methodology Literature
The following section provides a brief review of needs assessments methodology literature, focusing on aspects most relevant to SUD treatment capacity, as a framework for clarifying the concepts of needs assessment and capacity. This is followed by a review of selected articles on needs assessment methodology specific to SUD treatment.
What is a Needs Assessment?
Needs assessment emerged as a distinct branch of program evaluation in the 1970s and has evolved to address a broad scope of social issues.
Despite this broad application, the field has generally settled on a fairly standard definition of what constitutes a needs assessment as distinct from other types of evaluation and research. This definition begins with what White & Altschuld (2012) describe as "the classic definition of need: the discrepancy between the normative or 'current' condition and the optimal or 'what should be' state"--a formulation that is often condensed to the gap between "what is" and "what should be." In addition to these three components--a definition of what is, a specification of what should be, and a measurement of the gap between them--there is an essential fourth component: "Needs assessment also includes making judgments with regard to needs and putting them into prioritized order to guide decisions about what to do next" (Altschuld & Watkins, 2014).
This orientation to action is emphasized by a statement of the needs assessment.com website: "Needs Assessments are used to identify strategic priorities, define results to be accomplished, guide decisions related to appropriate actions to be taken, establish evaluation criteria for making judgments of success, and inform the continual improvement of activities within organizations" and it is this feature that primarily distinguishes needs assessment from other forms of evaluation and social science research (Kaufman, 1986). It is worth examining each of the four components of a needs assessment in some detail with reference to the methodological literature, as they are more complex than they may initially appear.
Describing "What Is" and "What Should Be"
These two elements present several challenges that must be addressed in conducting a needs assessment. In the first place, there are often (as in the case of SUD treatment needs assessment) two dimensions to what is and what should be: the population of people with SUD and the services to provide treatment for them. The definition of each requires different sources of data and methods of analysis, which then must be reconciled to assess their interrelationship --for example, the relationship between the predominance of a specific type of SUD in a local area and the types of services available in that area (McAuliffe & Dunn, 2004b).
A second challenge is related to obtaining input from multiple stakeholders to represent a broad range of perspectives, which has now become a standard and essential method of needs assessment data collection (Stefaniak et al., 2015).
Analysis of data obtained by stakeholder input also presents challenges. Lee & Altschuld (2007b) discuss these in the framework of "discrepancy analysis"--that is, analyzing the difference between what respondents indicate what is and what should be. Challenges for analysis include the following:
-
Differentiating between discrepancies derived from wants versus needs.
-
Determining the size and nature of a discrepancy.
-
Developing discrepancies from multiple sources or methods.
-
Qualitative data (focus group interviews, individual interviews) may not directly lead to discrepancies.
-
Understanding the value of "Not Applicable" responses.
-
Understanding missing data for one or both scales.
-
Deciding whether discrepancies can be determined using total group means for an item or only from the subgroup of individuals completing both scales.
-
Determining whether different needs indices produce similar results.
-
When there is variation of the number of responses for different items.
White & Altschuld (2012) also address this issue in the context of surveys that produce "importance scores"--that is, ratings of what respondents consider most important with respect to both the what is and what should be. The problem is that responses of stakeholder groups may not be equivalent and therefore not comparable due to various factors such as differences in the availability of information. The authors recommend various methods of survey design to minimize these issues to enhance the comparability of different perspectives.
These methodological issues related to discrepancy analysis and importance scores are relevant to the methodology of SUD needs assessments, which often utilize surveys of a wide variety of stakeholders with varying amounts and types of knowledge--for example, members of the general public, who may have limited knowledge of the SUD treatment system but many concerns; providers, who possess a vast store of one kind knowledge; and consumers, who possess extensive knowledge of a different kind. A well-designed survey can minimize the variance that is due to variations in knowledge by designing questions that are based on knowledge available to all (for example, by providing an introductory explanation of the issue), thereby obtaining equivalent opinions from diverse stakeholder groups about what is and what should be.
Defining a Need--Measuring the Gap Between What Is and What Should Be
Once the what is and what should be conditions are properly specified, the next step is to measure the gap between, which constitutes the need. Of the four components of a needs assessment, it is the way in which a need is defined that has the greatest effect in determining the course and outcomes. According to Watkins & Kavele (2014): "How you define needs: (a) clarifies the goals of your assessment; (b) influences how you design your assessment; (c) determines what you measure, and therefore how you measure; and (d) influences what you report, to whom, and in what format," and there is a considerable body of literature addressing the question of how to define need. The authors provide a list of common categories with subtypes of meanings of the term "need" with references to sources: object-focused definitions (e.g., things without which it is impossible to live); goals (e.g., basic drives); deficiencies; gaps (in results, conditions, etc.) human condition (necessities for a full life); and physical or psychological needs. Given this variability, there is considerable potential for ambiguity in practice, the most common of which in needs assessment is a failure to distinguish between need and solutions, whereby need properly defined is the gap between two conditions which may be addressed by a diversity of solutions. Clarity in this distinction is an important consideration for SUD treatment needs assessment methodology.
Providing Recommendations and Setting Priorities
Of the four components of a needs assessment, this may be the most challenging, for two reasons: first, because it requires choosing what in most cases will be a multitude of possible solutions for addressing a need; and second, because a needs assessment typically involves input from multiple stakeholders with diverse perspectives, values, and interests, which must be taken into consideration in offering recommendations and priorities. The following considers these challenges, particularly in reference to SUD treatment capacity needs assessment.
Prioritization is especially critical in SUD needs assessment because the gap between treated and untreated prevalence is large. In the United States, fewer than 20% of individuals with drug use disorders and 10% with alcohol use disorders receive treatment (SAMHSA, 2013). A major reason for this gap is that a large proportion of those with a disorder do not perceive a need for treatment or are skeptical about its effectiveness; a logical recommendation, therefore, would be to initiate a public education campaign or an outreach program. As Edlund et al. (2009) point out, however, if eight out of nine individuals currently do not perceive a need for treatment, then if efforts to increase perceived need were successful for only one out of eight individuals, the overall number of people receiving SUD services could almost double, an increase that would likely overwhelm the capacity of the SUD treatment system. Shepard et al. (2005) estimate that to provide services to all those identified in surveys as needing services would require an increase of 5-10 times current services levels.
Another problem with untreated prevalence as a measure of need for treatment that has been widely debated in the literature since the first national epidemiological surveys in the 1990s is that prevalence as estimated by diagnostic criteria in national surveys may not correspond to need for treatment--either because informal supports are adequate for many individuals' level of distress or because their condition is transitory (Spitzer, 1998). Analyzing data from a nationally representative longitudinal study, the National Epidemiologic Survey of Alcohol and Related Conditions, Sareen et al. (2013) found that 49.8% of those with a diagnosis who did not receive treatment had remitted after three years.
Experts therefore generally indicate that for recommendations to be feasible they must incorporate some form of prioritization. As noted by Ciarlo & Tweed in reference to mental health planning "to permit effective planning, policy makers must decide exactly which needy group(s) of persons are likely targets for their...services. Only then can the selection and implementation of an appropriate indirect needs assessment model to estimate those needs logically follow" (1992). McAuliffe, for example, suggests that data obtained from population surveys that define need for treatment according to diagnostic criteria should be supplemented with measures of clinical significance to prioritize treatment for subgroups of the SUD population that have the greatest need--especially as he notes, a significant proportion of those identified as having a SUD at a point-in-time may not need treatment at all (due to spontaneous recovery) or at least not in a specialty setting (as opposed to routine primary care, 12-step programs, etc.).
There are many other ways of prioritizing, however, and the process of choosing among them is likely to be complex and frequently politicized. In the first place, prioritization may focus on the population (subgroups with greatest need) or on the service system (filling gaps in the continuum of care). Second, stakeholders may differ in their priorities depending on their perspective: law enforcement may prioritize individuals at risk of incarceration, neighborhood associations may prioritize public intoxication, advocacy groups may prioritize the homeless or racial/ethnic groups, policy makers may prioritize the uninsured, etc. Third, prioritization of population subgroups is likely also to require prioritization of components of the service system, as subgroups will vary in the type of service appropriate for each.
Review of Selected Substance Use Disorder Treatment Needs Assessment Methodology Literature
Technical reports on methodology for SUD services needs assessment are relatively limited in number, and most are several decades old. The number is somewhat larger if mental health needs assessment methodology is included, but the time frame for these is similar. An additional limitation, especially in the more recent literature, is that most of these reports focus on techniques for measuring treated and untreated prevalence, but few (with the exception of several discussed below) discuss methods for determining the appropriate number and capacity of service systems--for example, how many inpatient beds, outpatient slots, workforce categories, etc.
A key set of papers on SUD needs assessment are those by McAuliffe & colleagues in the 1990s and early 2000s (McAuliffe, 1978; McAuliffe, 1990; McAuliffe, Breer et al., 1991; Breer, McAuliffe et al., 1996; McAuliffe, LaBrie et al., 1999; McAuliffe, Woodworth et al., 2002; McAuliffe, Labrie et al., 2003; McAuliffe, 2004a; McAuliffe & Dunn, 2004b). The earliest of the reports (McAuliffe, Breer et al., 1991), one of several on a needs assessment project in Rhode Island, is also among the most rigorous of those identified in the environmental scan. Conducted prior to the widespread availability of national prevalence surveys such as the National Survey on Drug Use and Health (NSDUH), which many later reports rely upon, McAuliffe & colleagues developed estimates of treated and untreated prevalence in the Rhode Island population by conducting a telephone survey of Rhode Island residents, which they tested for reliability and validity. They also estimated the number of additional treatment slots needed and how these should be distributed across treatment modalities and geographical areas by reviewing drug use patterns of those who said they wanted treatment, by interviewing providers and agency officials to identify system gaps, and by examining areas' social indicators. Finally, they calculated the relative cost-effectiveness of different treatments.
More recently, Balenko & Peugh (2005) conducted a study of treatment needs of prison inmates in which they used a framework for estimating treatment needs derived from the ASAM Patient Placement Criteria and other client matching protocols that assessed drug use severity, drug-related behavioral consequences, and other social and health problems. The results indicated high levels of drug involvement, but considerable variation in severity/recency of use and health and social consequences, consistent with the suggestion by McAuliffe cited above, that many persons with SUD diagnoses may require little or no treatment.
Defining "Network Capacity" in the Context of SUD Treatment
Network capacity may be defined in a variety of ways depending on the context, but the methodological literature provides a framework for an operational definition specific to needs assessment. This formulation guides the review of SUD needs assessment reports presented in this report.
Essential to a determination of what is and what should be is an understanding of what is meant by network capacity (used here synonymously with "system capacity"), which may be defined narrowly or more broadly. The narrow definition refers to the number of available treatment slots, such as hospital beds, workforce size, number of clinics. Measurement of capacity in this definition consists of an inventory or census, conducted within a defined geographic boundary. An example of an inventory, with the United States as the boundary, is the SAMHSA National Survey of Substance Abuse Treatment Services (N-SSATS). This report assumes a broader definition of network capacity, one that takes into consideration two other aspects of a service system besides the supply: continuity and quality.
Continuity refers to a balanced continuum of care such as represented by the ASAM Criteria or the SAMHSA Good and Modern Behavioral Health System. ASAM's criteria is a system for individualized treatment planning that represents SUD treatment as a continuum marked by four broad levels of service and an early intervention level. Within the five broad levels of care, decimal numbers are used to further express gradations of intensity of services. These levels of care provide a standard scale representing the continuum of recovery-oriented addiction services.[1] The SAMHSA Continuum of Care[2] is a structure consisting of four components, Promotion, Prevention, Treatment and Recovery, each of which includes a set of interventions or services.
Quality is a multi-dimensional construct that expands the definition of network capacity. An example of a framework for assessing capacity in terms of quality is the Institute of Medicine's (IOM's) "Six Aims" (IOM, 2011) for a system in which there is not only an adequate supply of services but those services also have the attributes of being Safe, Effective, Patient-centered, Timely, Efficient, and Equitable. Examples of how each of the six aims might be addressed in SUD treatment needs assessments are:
-
Safe: Is the workforce adequately trained to deal with emergencies?
-
Effective: Does the system include a full complement of evidence-based services?
-
Patient-centered: Is there leadership and a management structure that can support a culture of patient-centeredness?
-
Timely: Are programs adequately staffed such that long waiting times are avoided?
-
Efficient: Is there an adequate data infrastructure in place to monitor utilization and resource allocation?
-
Equitable: Are there adequate quality improvement processes in place to identify and address disparities?
These are only a few of many aspects of capacity related to the six aims that a needs assessment might address. Few, if any, needs assessments address all six aims, but our review identifies which of these dimensions they do address and describes approaches and best practices in the context of the project's research questions.
Defining "Needs Assessment" in the Context of SUD Treatment
The "what is" condition: Based on the four components of needs assessment, specification of "what is" calls for measures of current system capacity as described above--an inventory of existing services, available slots, number of people receiving services, number and configuration of staffing, etc.--as represented, for example, by the N-SSATS and also a count of the number of people with met and unmet treatment needs as represented by the NSDUH.
The "what should be" condition: The second component, "What should be" implies specification of some goal or standard for those factors included under "what is." It is this component that distinguishes a needs assessment from other types of research and reports (epidemiological studies, for example) which include only the first component, a measurement of "what is."
The specification of "what should be," though essential for a needs assessment, may be more formal and quantifiable or less formal and qualitative, as shown in the SUD needs assessments we review. Examples of more formal definitions are the standards represented by the ASAM Criteria or the SAMHSA Continuum of Care described above. Less formal specifications, which are more typical of the needs assessments reviewed, generally involve some combination of stakeholder input, comparison with national statistics, expert opinion and the like. The less formal approach of SUD needs assessment is explained to some extent by the fact that the SUD treatment system is less formally organized than, for example, health care, for which the Health Resources and Services Administration (HRSA) is able to develop research-based formulas for the number of patients that can be served by specific practitioner types as discussed below.
Measurement of the gap: This component of a SUD needs assessment also may be more or less formal. An example of a very formal approach is the HRSA method of designating Health Professional Shortage Areas (HPSA) and Medically Underserved Areas/Populations (MUA/P), as determined by the Index of Medical Underservice (IMU), the calculation of which is based on four weighted criteria (population-to-provider ratio; percent of population below the federal poverty level (FPL); percent of the population over age 65; infant mortality rate). IMU can range from zero to 100, where zero represents the completely underserved and 100 represents completely served. MUA/Ps are those with an IMU of 62.0 or less. In this example, a standard of "what should be" is set by setting an ideal standard of number of specific workforce professionals to the population levels, adjusted for poverty, age, and infant mortality. Notably, however, the ideal of the population being completely served is then adjusted downward by the 62.0 cut-off score, representing what is practical to achieve. This is analogous to the case of SUD treatment, where the ideal of treatment for all with a diagnosed disorder is neither feasible nor necessary, as discussed in the Background section of this report.
Guidance for decision making: The formality of the HRSA method of gap measurement is not always possible or even necessary for purposes of guiding policy decisions related to SUD treatment, and in many cases the standard is more subjective or ad hoc. A major challenge in decision making with respect to SUD treatment needs is the very large gap between those who need treatment (based on most definitions of need) and those who receive it. As noted in the Background section, fewer than 8% of those with alcohol abuse or dependence receive treatment. Reducing this gap by even a few percentage points would require an enormous expansion of capacity and a corresponding commitment of resources beyond that which is feasible in most circumstances. For this reason, prioritization of recommendations is especially important in needs assessment for SUD treatment. Few of the needs assessments that we reviewed included anything more than the most cursory process of prioritizing recommendations. We suggest that methods of doing so would be an important target for improvement of SUD needs assessment methodology, and that the methods would be prime candidates for designation as best practices, a topic we will address in more detail in the final report with input from the TAG.
Challenges in Defining NeedThe challenge of defining need for SUD treatment was addressed at length by the TAG in the June 11, 2018, meeting. Key points include:
|
METHODS
Following the review of selected literature on needs assessment methodology, we conducted three activities to address the research questions (separated primarily because they address different types of questions that draw on different data sources): (1) retrieval and review of a convenience sample of SUD treatment capacity needs assessment reports, to address questions related to content and practices in the field; (2) description of some needs assessments from other fields that might be used as models for SUD treatment, to address the research question, "Are there needs assessments from other provider types...that could be applied to the SUD treatment workforce?"; and (3) a separate scan, based on a review of state policy documents, to address the research question, "How do states and managed care organizations operationalize network capacity."
Methods for Review of Substance Use Disorder Needs Assessment Reports
Search Strategy
The scan of SUD treatment capacity needs assessments utilizes modified methods of systematic literature review to locate representative examples of SUD treatment needs assessment reports in the published and gray literature to address the research questions related to practices in the field. Systematic reviews require careful search strategies to ensure that all relevant reports are identified, and they typically entail methods for rating the quality of individual reports (primarily the degree to which they minimize the risk of bias) to assess the overall strength of the evidence summarized from the reports.
A challenge of this approach is that a majority of SUD needs assessment reports are not published in peer reviewed journals and therefore do not adhere to the consistent standards of format and quality that apply to the peer reviewed reports that are the typical source for systematic reviews in the health care field. Moreover, accessibility of unpublished needs assessment, especially those produced less recently (prior to widespread use of the Internet) is limited. Though we believe that the convenience sample of SUD network capacity needs assessments that we were able to retrieve, given the resources for this project, is representative of current practice in the field, it is undoubtedly a small portion of those produced over the years.
White and Altschuld (2012) comment on this challenge:
The lack of sources is not surprising since many assessments are never circulated beyond the organization, probably because they are used for internal purposes with no thought to publishing. Sharing them with the evaluation community would go a long way to help practitioners as well as build the body of professional knowledge. Toward that end more needs assessment research should be disseminated. This starts with greater emphasis on writing and publication by university students, professional associations, practitioners, and those supporting needs assessments.
We have addressed these limitations of the systematic review approach in two ways--first by using more flexible inclusion/exclusion criteria and second by using a more complex data extraction process.
Inclusion/Exclusion Criteria
Our inclusion/exclusion criteria are based on the concept of needs assessment derived from the methodological literature as described previously. That is, to be included a study of SUD must include: (1) a description of "what is" at both the population and system level (for example, prevalence of a disorder and an inventory of available services); (2) some operational definition of what should be (for example, the numbers and characteristics of individuals who should receive treatment) and some model of services necessary to treat the identified population; (3) some measure of the gap between what is and what should be (for example, a reduction in the number or percent of individuals with an unmet need, or the cost of additional services required to address the need).
We initially considered a fourth requirement, consistent with the definition of needs assessment: that the report include specific recommendations or priorities for action. Without knowing in advance how many reports this might exclude, we decided on a more relaxed standard--to include any report that: (a) is self-identified as a needs assessment; (b) meets the other three criteria; and (c) at least provides information suitable for informing policy and decision making, whether or not in the form of explicit recommendations. To assess the utility of reports for this purpose, however, we rated each as to whether it includes: (1) suggestions or recommendations for narrowing the gap; (2) prioritized recommendations; (3) strategies for acting on the recommendations; and (4) the feasibility of accomplishing recommended actions.
Excluded Reports: An example of a report that would be excluded based on these criteria is an epidemiological study providing estimates of treated and untreated prevalence--that is, a measure of need--but without some measure of existing or desired system capacity. Another example would be a description of a service system that may identify areas for needed expansion or improvement but does not include information about the characteristics and size of the population served by the system.
Sources and Search Terms
We initially cast a wide net, testing various sources (e.g., databases including PubMed, Webofscience, Google Scholar, relevant journals such as the Journal of Substance Abuse, etc.) and a variety of search terms. We were quickly able to narrow this strategy down to a few sources and search terms as we found that any more added very little to sensitivity (identifying a larger number of relevant reports) or specificity (excluding non-relevant reports). Accordingly, we adopted two strategies with search terms: one for unpublished reports and the other for published (peer reviewed) articles. For unpublished reports we simply entered Google search terms "[state] needs assessment" with the name of each state. This typically produced reports in the range of 150-200 per state. We then scanned the summary description in the Google entry to determine whether it merited closer review to determine eligibility for inclusion. We did not establish a time frame for two reasons: (1) because the availability of information on the Internet is self-limiting to the past 10-15 years; and (2) because the focus of the environmental scan is primarily current, rather than historical, practice.
For peer reviewed literature we used PubMed; after testing various combinations of Medical Subject Headings (MeSH) search terms, we settled on "Substance-Related Disorders/therapy"[MeSH] AND "Health Services Needs and Demand"[MeSH] as providing the best balance between specificity and sensitivity. (We found that the MeSH term "needs assessment" was not useful in that it resulted primarily in articles related to instruments for assessing the health care of individuals.)
| FIGURE 1. Flow Diagram, Adapted from PRISMA |
|---|
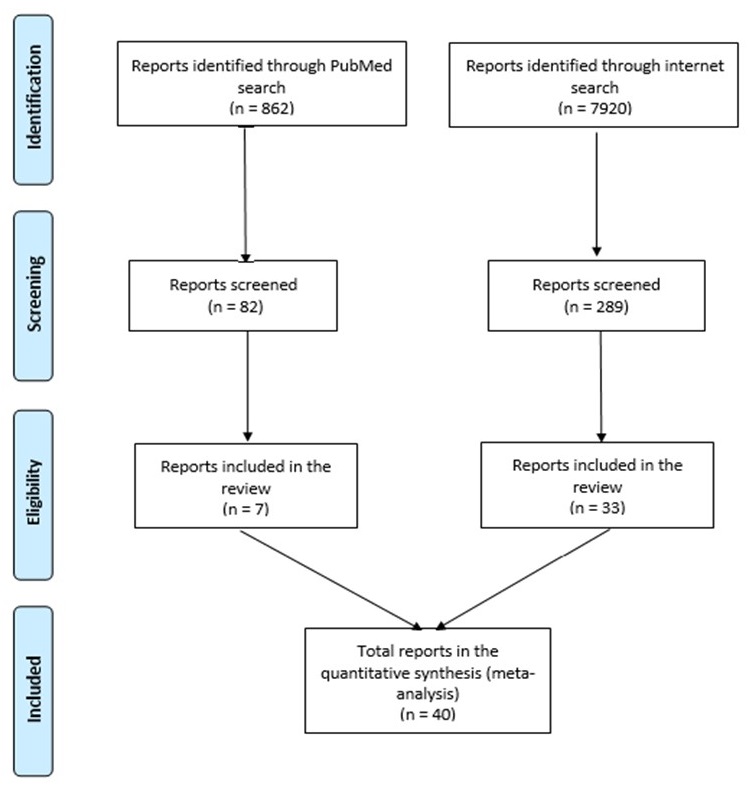 |
| SOURCE: Moher, Liberati, Tetzlaff & Altman, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med, 6(7): e1000097. doi:10.1371/journal.pmed1000097. For more information, visit http://www.prisma-statement.org/. |
For published articles, we reviewed abstracts of those identified initially by the search terms, and for those that seemed appropriate we reviewed the entire article. For those identified in the Internet search, we reviewed the document and retrieved any that addressed SUD, including those that also addressed mental health.
After screening out studies that did not meet the inclusion criteria, we classified those that were included into two categories: "mandated" and "locally initiated" needs assessments. Mandated needs assessments, described in detail below, are those conducted to meet requirements of various broader programs, such as federal grants to the states. Locally initiated needs assessments, on the other hand, are typically standalone initiatives conducted for a specific policy purpose or single research project that meet the inclusion criteria.
Using this search strategy, for locally initiated needs assessments we obtained a purposeful convenience sample of 33 reports from the grey literature (Internet) and seven from the peer-reviewed literature that reflect a diverse range of factors of interest for the environmental scan: geographical diversity (a range of states, and both rural and urban areas), scale (national, state, local areas) methodological variety (complex statistical models as well as basic approaches using available data), and a variety of topic areas (e.g., both general and vulnerable populations, general capacity issues as well as specific areas such as workforce capacity, various type of substance use).
The flow diagram above, adapted from the PRISMA recommendations for reporting of systematic reviews, presents the number of reports screened and included.
For the mandated reports, given their more generic nature, we did not aim for a specific sample but instead scanned a number of them in each category using the review approach described below.
Review Methods for Mandated and Locally Initiated Needs Assessments
We adopted different strategies for reviewing these two categories of needs assessments. For the mandated needs assessments, we provide a general overview of the methodologies and content based on review of a sample of each type and review of the guidance or requirements provided by the relevant authorizing organization. For the locally initiated needs assessment we conducted a more detailed analysis with data extraction based on the research questions presented above.
This differential approach is based on three considerations about the mandated reports--first because the sheer number would exceed the resources of this project to analyze individually, second their generic nature in being conducted according to specified requirements thereby limits the value in reviewing large numbers of them, and third because they are less focused on specific policy questions related to system capacity and therefore provide less knowledge relevant to the research questions that would contribute to the advance of SUD needs assessment methodology.
Procedures for Extracting Information to Address Research Questions Related to SUD Needs Assessment Practices and Methods
Content and Methods: Each of the research questions was broken down into a set of individual items. In this context, we use the term methods in the broad sense of approaches taken in conducting the needs assessment (e.g., how data were collected, how levels of care were defined, how the service system was defined, etc.). Using a coding instrument based on the research questions listed in the introduction, we extracted information related to the content and methods of the reports and to the quality based on a set of criteria. Questions related to content and methods are addressed in the review are presented in abbreviated form in Figure 2. The protocol (Needs Assessment Data Extraction Form), with questions in full and individual items may be found in Appendix E. The remaining research questions listed in the introduction involve recommendations that will be addressed in the final report.
| FIGURE 2. Abbreviated Review Questions Related to Content and Practices |
|---|
|
Using the number of responses to each item we were then able to quantify this information in order to provide an overview of practices in the field as represented by this sample of needs assessments.
It should be emphasized that the research questions focus more on the issues addressed by SUD needs assessments and the method employed, rather than specifics of the findings. That is, we were not attempting to summarize data about, for example, prevalence or numbers of people receiving services as in a systematic review of research literature, but rather were extracting information about the kinds of data that were presented and how they were obtained and analyzed in order to assess current practices in the field.
Quality Ratings: In addition to extracting information about the content and practices of SUD needs assessment, the protocol included criteria for rating the quality of needs assessment. This approach is adapted from the methods of systematic reviews, where quality is a matter of the extent to which the reader is able to assess the strengths and weaknesses of the study based on the relative clarity and transparency of information provided about how the study was conducted (Moher, et al., 2009). In this framework, quality is assessed based on the extent of information provided in the reports about the methods employed: for example, if a survey was conducted, does the report indicate whether it had been tested, how the sample was defined, etc. Questions related to quality are presented in abbreviated form in Figure 3 and are presented in their entirety in the protocol (Appendix E).
| FIGURE 3. Abbreviated Review Questions Related to Quality |
|---|
|
The purpose of the quality assessment is not to judge the quality of individual studies but rather to gain a sense of current practices in SUD capacity needs assessment overall. The criteria are based on some of the research questions and are generally designed to indicate how successfully reports represent the essential components of a needs assessment: defining "what is" and "what should be" with sufficient clarity and specificity that that the gap between them is measurable and providing guidance for decision making and priority-setting. Thus, the focus of the quality ratings is upon utility--to what extent does a needs assessment provide the information necessary to serve as a guide for decision making?
In the following sections these questions are addressed as a general overview of the mandated needs assessments and then in a more detailed way, using the Data Extraction Form, for the locally initiated SUD-specific needs assessment reports.
RESULTS I: REVIEW OF NEEDS ASSESSMENT REPORTS
Overview of Mandated Needs Assessments
As discussed in the Methods section, mandated needs assessments are those carried out in connection with requirements for various Federal and, in some cases, State programs, one of the two types of reports that we reviewed. They are conducted according to specific guidelines of the program and therefore tend to be more generic than the locally initiated reports, the other type reviewed. The mandated reports are also much more numerous and usually address SUD as one among other types of public health issues. Accordingly, we reviewed a representative selection of several dozen, with a less rigorous approach than for the locally initiated reports, primarily summarizing characteristics of methods and content. The major programs that require this type of needs assessment are identified in Figure 4, on the following page.
| FIGURE 4. Federal Programs Requiring Needs Assessments | ||
|---|---|---|
| Program Title | Program Administration | Organization |
| Substance Abuse Prevention and Treatment Block Grant | SAMHSA[1] | States |
| Community Mental Health Services Block Grant (MHBG) | SAMHSA | States |
| Strategic Prevention Framework (SPF) State Incentive Grant (SIG) | SAMHSA | States |
| State Targeted Response to the Opioid Crisis Grant (Opioid STR) | SAMHSA | States |
| Community Health Needs Assessments (CHNAs) | IRS[2] | Non-profit hospitals |
| Community Needs Assessments (CNAs) | NPHAB[3] | Public health agencies |
| Delivery System Reform Incentive Payment (DSRIP) | CMS[4] | States |
| Community Services Block Grants | ACF[5] | States |
| Community Development Block Grants | HUD[6] | States |
| Comprehensive State-wide Needs Assessments | RSA[7] | States |
| Maternal and Child Health Services Title V Block Grants | HRSA[8] | States |
| Primary Care Services Grant Program | HRSA | States |
| Ryan White HIV/AIDS | HRSA | States |
|
||
With the exception of needs assessments conducted for the Substance Abuse Prevention and Treatment Block Grant (SAPTBG) program, those in the above list generally address a wide range of issues and service types, with SUD being discussed to a very limited extent. Here we provide an overview of those that are more likely to contain at least some discussion of SUD treatment needs.
Substance Abuse Prevention and Treatment Block Grant (SAPTBG) and Community Mental Health Services Block Grant (MHBG )
The FY 2018-2019 combined application for the SAPTBG and MHBG requires applicants to conduct a behavioral health needs assessment and plan that focuses on "the strengths, needs, and service gaps for specific populations."[3] The assessment step in this process requires the applicant to "Identify the unmet service needs and critical gaps within the current system" and recommends for that purpose the use of SAMHSA's various data sets (NSDUH, Treatment Episode Data Set [TEDS], etc.). The strengths of this approach are: (1) it requires a data-driven analysis of existing service system capacity; (2) it directs attention to the needs of various subpopulations who often experience disparities in care; and (3) it calls for a detailed plan for how funding will be used to enhance the existing system. However, it lacks some of the features that would result in a needs assessment of the highest quality as described in the Background section on needs assessment methodology.
The major limitation is that these requirements do not provide a definition of need as called for in the literature. Consequently, there is a tendency for applicants to rely on the simple and less useful definition of "unmet need" as the gap between untreated and treated prevalence. Descriptions of gaps in the service system are therefore often very general--for example, this statement from one state application: "There is a need for more services which provide various levels of treatment and which extend to women in underserved areas of the state." Another application from a large state has only a single reference to gaps, citing a task force report on Youth SUD treatment needs that identified three main gaps--standardized assessments, workforce development, and access to care--without further discussion.
A second limitation of the block grant approach is that it does not set out a standard for a description of an optimal service system against which applicants can measure gaps in the capacity of their service system. The application does, however, request--but not require--applicants to provide detailed information in the form of checklists about whether they provide a long list of services, described as "key focus areas that are critical to implementation of provisions related to improving the quality of life for individuals with behavioral health disorders."
Strategic Prevention Framework (SPF) State Incentive Grants (SIGs)
As of January 2017, all 50 states, eight jurisdictions, and 19 tribes have received SPF SIG/TIG funding. SPF SIG grant funding has been used to support a wide range of prevention initiatives such as prescriber education, coordination with law enforcement, production of educational videos, naloxone training, and many others.
Needs assessment for the SPF SIG is the first of the five steps of the SPF (SAMHSA, 2018):
-
Step 1: Assess Needs: What is the problem, and how can I learn more?
-
Step 2: Build Capacity: What do I have to work with?
-
Step 3: Plan: What should I do and how should I do it?
-
Step 4: Implement: How can I put my plan into action?
-
Step 5: Evaluate: Is my plan succeeding?
The website for SAMHSA's Center for the Application of Prevention Technologies (CAPT) provides some very general guidance on conducting needs assessments; this guidance focuses on collecting data to address four questions that are primarily epidemiological, with examples provided for each: What substance use problems and related behaviors are occurring in your community? How often are these problems and related behaviors occurring? Where are these substance use problems and related behaviors occurring? Who is experiencing more of these substance use issues and related behaviors?
As demonstrated by a sample of SPF SIG reports that we reviewed, the SPF approach for conducting needs assessments differs in certain respects from the model that we have utilized in this report. While the SPF emphasizes the collection and analysis of data, the type of data is primarily related to prevalence and patterns of substance use with little attention to analyzing existing service capacity and gaps. Instead, there is an emphasis on assessing a community's "readiness for change," which generally refers to attitudes about substance use and prevention, for which CAPT provides a variety of measurement tools such as stakeholder interview guides.
State Targeted Response to the Opioid Crisis Grants (Opioid STR)
According to the Funding Opportunity Announcement, the purpose of the Opioid STR program is "to address the opioid crisis by increasing access to treatment, reducing unmet treatment need, and reducing opioid overdose related deaths through the provision of prevention, treatment and recovery activities for opioid use disorder." Award amount is determined by a formula based on unmet need for opioid use disorder treatment and drug poisoning deaths. Funding is intended, in part, to "support a comprehensive response to the opioid epidemic using a strategic planning process to conduct needs and capacity assessments." The requirements for the needs assessment are to identify the following:
-
Areas where opioid misuse and related harms are most prevalent.
-
The number and location of opioid treatment providers in the state, including providers that offer opioid use disorder services.
-
All existing activities and their funding sources in the state that address opioid use prevention, treatment, and recovery activities and remaining gaps in these activities.
The state needs assessments follow a prescribed format that calls for a variety of epidemiological and treatment system information, but a limited requirement for specifying gaps and need. With regard to prevention services, for example, grantees are asked simply to "identify any strengths or gaps in services." To estimate treatment needs, grantees are suggested to use the SAMHSA data sources (NSDUH, etc.) without further refinement such as anticipated demand, etc.
Community Health Needs Assessments (CHNAs)
CHNAs originated as a requirement by the Internal Revenue Service (IRS) that non-profit hospitals be able to demonstrate a "community benefit" beyond simply delivering standard medical care. Subsequently, a number of states implemented their own community benefit statutes. This requirement was greatly expanded by the Affordable Care Act (ACA), which added the requirement that non-profit hospitals conduct a needs assessment every three years. With nearly 3,000 non-profit hospitals in the nation,[4] the number of CHNAs that have been produced far exceeds the resources for any practical systematic review. However, we have reviewed a sample of these reports to identify the manner and extent to which they address SUD capacity and gaps.
The basic principles and requirements for a CHNA are described by Rosenbaum (2013). Key features of the requirements are:
-
Involvement by people who represent the "broad interests" of the communities served by non-profit hospitals, including people with "special knowledge of or expertise in public health."
-
A definition of community that encompasses both a significant enough area to allow for population-wide interventions and measurable results and includes a targeted focus to address disparities among subpopulations.
-
Development of an accompanying Community Health Improvement (CHI) Plan detailing activities to be conducted by the hospital to promote public health and address issues identified in the CHNA.
-
An emphasis on transparency, for example a requirement that the report be made widely available to the public, by posting on a hospital organization website or the facility's website.
Community Health Assessments (CHAs)
CHAs are similar to CHNAs but are conducted by different types of organizations for different purposes and with different requirements; whereas CHNAs are conducted by non-profit hospitals to satisfy requirements of the IRS and the ACA, under direction of the Centers for Medicare & Medicaid Services (CMS), CHAs are conducted by county public health boards for purposes of accreditation by the National Association of Public Health Directors (NAPHD), established in 2007 with support from the Robert Wood Johnson Foundation. The IRS and NAPHD have coordinated to encourage hospitals and public health departments to collaborate in producing a single combined CHNA-CHA that satisfies both sets of requirements, and a number of them have done so. Several of these have been conducted by collaborations between hospitals and public health agencies.
NAPHD has very detailed requirements for CHAs, which address the following components:
-
Various sources of data.
-
Population demographics.
-
Health issues identified.
-
Special populations with health issues.
-
Contributing causes of health issues.
-
Description of assets to address health issues.
-
Documented input from stakeholders.
Many of these reports utilize a framework known as Mobilizing for Action through Planning and Partnerships, which was developed jointly by the National Association of County and City Health Officials (NACCHO) and the CDC. The needs assessment component is embedded in the third of six phases, entitled Collecting and Analyzing Data, which involves four types of assessments: Community Themes and Strengths, Local Public Health System, Community Health Status, and Forces of Change. The NACCHO website provides an array of tools and training materials for conducting each of these assessments.
A review of a sample of 58 CHAs that extracted health status indicators reported in the plans identified a total of 1,524 indicators with an average of 29 indicators per health department (Bender, 2017). Categories of indicators included nutrition, physical activity, and obesity; access to health services; maternal, infant, and child health; tobacco prevention and control; social determinants/health equity; injury and violence; substance abuse; mental health; clinical preventive services; chronic disease; environmental quality; reproductive and sexual health; oral health; data; overall health and well-being; organizational capacity; and emergency preparedness.
RELEVANCE OF CHNAS AND CHAS FOR SUD TREATMENT CAPACITY NEEDS ASSESSMENT
CHNAs and CHAs provide a wealth of information that has the potential for uses beyond the primary function of meeting organizational requirements, a potential that is greatly enhanced by their accessibility (particularly in contrast to locally produced needs assessments, which are often not disseminated beyond the agency that produced them). With respect to the issue of SUD needs assessments specifically, a striking finding of our review of a sample of CHNAs and Community Needs Assessments (CNAs) is that substance abuse is almost invariably at or near the top of the list of community concerns. As a basis for the utility aspect of needs assessment--providing guidance for policy making and priority-setting--these reports have both limitations and benefits. The limitation is that with so many areas of public health being addressed, the degree of detail is inevitably constrained. The main benefit is that these reports provide an understanding of where substance use fits in with the broader range of public health problems and resources. While they are not a substitute for a needs assessment that focuses exclusively on substance use treatment capacity, they offer a useful starting point for collecting more granular information.
Review of Locally Initiated Needs Assessments
In this section we provide a narrative and tabular summary of needs assessments that were initiated locally (e.g., at the city, county, or state-level) for specific policy initiatives rather than those that are federally mandated for ongoing policy purposes or for public health accreditation, a total of 40 reports (see Appendix B for a list of the reports). The summary is based on, and organized according to, the research questions that guide this project.
What Questions are Addressed?
| TABLE 1. Topic Areas: Supply and Demand | |
|---|---|
| Number of Reports | |
| Prevalence/frequency related to: | |
| General substance use | 22 |
| Alcohol | 15 |
| Opioids | 9 |
| Heroin | 8 |
| Methamphetamine | 2 |
| Marijuana | 3 |
| Cocaine | 5 |
| Depression | 2 |
| Suicide | 2 |
| Overdose | 5 |
| Co-Occurring Disorder (COD) | 6 |
| Medical Co-morbidity | 4 |
| Other prevalence/frequency described | 23 |
| Unmet need (other than prevalence) | 9 |
| Provider organization supply/capacity | 6 |
| Utilization/penetration | 17 |
| High utilizers | 5 |
| Demand (services likely to be requested) | 17 |
| Referrals | 7 |
| Means of obtainment (how drugs are obtained) | 5 |
| Risk factors | 4 |
| Expenditures/costs/cost benefit | 9 |
| Benefit design/coverage | 4 |
| Funding sources | 8 |
| Policy changes affecting supply or demand | 4 |
| Law enforcement | 1 |
We operationalized this research broadly, as "What topics were addressed by the locally initiated needs assessments?" Tables 1-5 report the results, organized into categories of topics: supply and demand, populations, quality issues, use of technology, and barriers and limitations. We identified approximately 40 different issues and topics addressed by the reports we reviewed, with most addressing multiple topics--that is, individual reports may have addressed more than one of the items in each category. Notably, there were some topics that received relatively limited attention. Whereas recent literature on needs assessment methodology emphasizes the importance of collecting information about network assets and strengths, we identified only a handful that addressed this topic. Only one of the reports addressed law enforcement as a factor affecting service utilization. Other topics that are of current interest in the field but receive less attention in the needs assessments that we reviewed are benefit design, peer involvement, technology, and EBPs. Table 1 presents the number of reports that address topics related to supply and demand including prevalence, utilization, risk factors and issues related to costs.
Table 2 represents questions that were addressed related to issues of diversity and disparities as an aspect of system capacity, indicating that this has not been considered a central issue in the field despite the widespread attention in health care policy.
| TABLE 2. Populations | |
|---|---|
| Number of Reports | |
| Special populations | 3 |
| Disparities | 7 |
| Diagnostic group differences | 3 |
| Regional variation | 5 |
| Demographic trends | 8 |
| Cultural competency | 6 |
Table 3 identifies questions related to quality that were addressed. It is noteworthy than only a few included measures of clinical quality (outcomes, adherence, and perception of care), as an element in the broader conception of system capacity; however, a number did include qualitative information from service users obtained through focus groups and interviews.
| TABLE 3. Quality Issues | |
|---|---|
| Number of Reports | |
| Access (wait-times, available slots, etc.) | 19 |
| Availability of services/network adequacy | 16 |
| Outpatient follow-up | 7 |
| Outcomes | 5 |
| Treatment completion/adherence | 1 |
| Satisfaction/perception of care | 4 |
| Quality/performance measurement systems | 2 |
| Collaboration | 10 |
| Leadership | 3 |
| Evidence-Based Practices (EBPs) | 4 |
| Benchmarks for future progress | 3 |
| Transitions by functional level | 8 |
| Behavioral health integration | 4 |
| System assets/strengths | 7 |
| Other quality | 3 |
Table 4 indicates the number of needs assessments that addressed questions related to the use of technology. This category also provides background for the research question about how telehealth policies can be incorporated into needs assessments, which will be addressed in the final report recommendations, for which there is a clear need as only a very few reports address this increasingly important aspect of system capacity.
| TABLE 4. Use of Technology | |
|---|---|
| Number of Reports | |
| Data systems | 4 |
| Use of Health Information Technology | 3 |
| Use of Electronic Medical Records | 2 |
| Use of Telehealth | 4 |
| Use of e-prescribing | 3 |
| Interoperability among provider organizations | 1 |
| Interoperability among public agencies | 2 |
| Other technology issues | 2 |
The reports address a wide variety of questions related to barriers and limitations, including many that that are not included in the already extensive list in the protocol, with nearly all the reports (n=39) identifying at least one other barrier or limitation that was not on the list (Table 5). Notably, many more reports identified policies--an area where change may be achieved relatively easily in that additional resources are not required--compared to other barriers such as provide reimbursement that would require additional resources to address.
| TABLE 5. Barriers/Limitations | |
|---|---|
| Number of Reports | |
| Policies | 19 |
| Mental health (MH)/SUD bifurcation | 4 |
| Agency silos | 3 |
| Decentralized (e.g., county) systems | 4 |
| Service locations | 3 |
| Lack of services | 9 |
| Service costs | 2 |
| Lack of access (not specified) | 5 |
| Lack of qualified workforce | 9 |
| Provider reimbursement limitations | 9 |
| Stigma | 7 |
| Privacy/confidentiality issues | 2 |
| Other barriers/limitations | 39 |
What Populations are Addressed?
This section addresses the research question regarding the populations addressed in needs assessment. Whereas earlier SUD treatment needs assessments tended to address the general population, one of the hallmarks of more recent needs assessments, which are largely represented in the reports obtained through Internet searches, is that they drill down to examine availability and accessibility of services for a wide range of specific subgroups, such as demographic subpopulations including age, gender, racial/ethnic and sexual orientation, and persons in a particular status (such as homelessness and incarceration) as shown in Table 6. More recent needs assessments also tend more to focus on users and service capacity of specific substances--particularly opioids. These results are in contrast to the relatively little attention given to issues of disparities indicated in Table 2. As a general explanation for this discrepancy, needs assessments focusing on specific subpopulations generally do not draw comparisons among subgroups but focus only on the capacity issues related to the group of interest.
| TABLE 6. Populations/Groups of Focus | |
|---|---|
| Number of Reports | |
| Substance use disorder (SUD) | |
| Substance unspecified | 8 |
| Alcohol | 7 |
| Poly drug use | 2 |
| Needle use | 1 |
| Opioids | 10 |
| Prescription drugs | 7 |
| Heroin | 5 |
| Methamphetamines | 2 |
| Mental health | 11 |
| Co-occurring disorders (CODs) | 10 |
| HIV/AIDS | 0 |
| Children/adolescents | 21 |
| Transition-age youth | 6 |
| Adults | 19 |
| Older adults | 2 |
| Racial/ethnic groups | 1 |
| LGBT/LGBTQA | 4 |
| Gender | 5 |
| Income | 5 |
| Marital status | 0 |
| Homeless | 7 |
| Veterans | 1 |
| Adults criminal justice system | 10 |
| Youth juvenile justice system | 1 |
| Child/youth child welfare | 0 |
| Other population or group of focus specified | 14 |
| Not described/specified | 0 |
What Workers are Incorporated?
As shown in Table 7, needs assessment reports incorporated a wide variety of workforce categories, although any single category was addressed by only a few reports. Consistent with the findings in relation to other research questions, only a few reports (n=4) address peers as an aspect of workforce capacity. This requires further investigation, however, as a large proportion of the SUD treatment workforce consists of people in recovery; it may be a matter of nomenclature where the term peer is applied differently in SUD than in mental health. This is a question that will be explored with the TAG and addressed in the final report.
| TABLE 7. Workforce Categories | |
|---|---|
| Number of Reports | |
| Psychiatrists | 11 |
| Addiction | 2 |
| Other psychiatrists | 2 |
| Physicians (non-psychiatrist) | 8 |
| Licensed buprenorphine physicians | 6 |
| Other physicians | 3 |
| Nurses | 7 |
| Licensed Practical Nurses/Licensed Vocational Nurses | 1 |
| Registered Nurse (Diploma, Associate's, and Baccalaureate) | 3 |
| Psychiatric and Mental Health Nurses | 1 |
| Advanced Practice Registered Nurses (Master's and Doctoral) | 2 |
| Nurse Practitioner | 2 |
| Physician Assistant | 2 |
| Psychologists | 9 |
| Social Workers | 10 |
| Associate's and Baccalaureate | 1 |
| Master's | 2 |
| Clinical | 3 |
| Counselors | 12 |
| Rehabilitation Counseling | 3 |
| Addiction Counseling | 4 |
| Clinical Mental Health Counseling | 1 |
| Other counselors | 4 |
| Peers | 4 |
| Other workforce category | 1 |
Needs assessments most frequently examined the workforce in a specific geographic boundary or characteristics related to training, certification, and licensing. Although SUD treatment workforce salaries are frequently cited as a contributing factor to workforce shortages, this was addressed by a negligible number of reports.
| TABLE 8. Workforce Distribution, Characteristics and Funding of Salaries | |
|---|---|
| Number of Reports | |
| Workforce geographic distribution | |
| By state | 3 |
| By county across the state | 3 |
| By urban/rural | 3 |
| Other geographical classification | 9 |
| Workforce characteristics | |
| Racial/ethnic composition | 2 |
| Competencies/training | 7 |
| Certification | 5 |
| Licensing | 5 |
| Other workforce characteristics | 5 |
| Sources of funding for workforce salaries | |
| Medicaid | 4 |
| Medicare | 1 |
| Private insurance | 1 |
| State funds | 1 |
| Charity/free care | 1 |
| Self-pay | 1 |
What Settings (geographic areas/regions) are Addressed?
In the locally initiated needs assessments reports we have reviewed to date, most have focused on specific states or specific counties and cities. Most have focused on the entire state or county, while only a few have focused on urban, rural, or frontier regions/boundaries of the state or county. One focused on a tribal community within the northern portion of a state.
What Levels of Care are Addressed?
We reviewed how the needs assessments addressed levels of care in connection with service capacity--that is, what kind of services are required to meet the individual-level needs of a population. This is another issue that has been discussed since the 1980s (Ford & Luckey, 1983; Rush, 1990). To assess how it was addressed, we looked for evidence of some standard for a comprehensive mental health system--such as the ASAM levels of care or the SAMHSA Good and Modern Behavioral Health System standards--and included a question about how need was defined in the quality rating section. As with the reporting on treatment needs, this important feature of needs assessment was relatively neglected. Instead, many reports simply provided utilization data of existing services. Especially in the mandated needs assessment, often there was also a list of service gaps but without any discussion as to how these were identified.
What Data Sources and Methods are Used?
Methods in needs assessments consist of three types of activity: (1) methods of data collection; (2) methods of data analysis; and (3) methods for formulating recommendations. The following sections discuss how these activities were conducted in the needs assessments we reviewed. This section also provides an introduction to the question, "What are key pieces of missing data?"--which will be addressed in more detail with recommendations from the TAG in the final report.
METHODS OF DATA COLLECTION
Data collection consists of obtaining information about the "what is" and "what should be" conditions--characteristics of the population, prevalence of the disorder, and characteristics of the service system (number and types of services and workforce, etc.). The most common means of data collection are: obtaining stakeholder perspectives by means of surveys, conducting focus groups and interviews, and holding public meetings; utilizing secondary data such as national data sets (most NSDUH) or administrative data such as claims, and reviewing documents (previous reports, policies, program descriptions, etc.). Most assessments combined stakeholder perspectives with national data sets to estimate prevalence and combined SAMHSA data sets with local health information to estimate capacity/utilization. Sources of data used in the reports are enumerated in Table 9 and Table 10.
Table 9 enumerates the various federal data sources used in the needs assessments. Notably, none used data from Healthy People 2020 and the National Directory of Drug and Alcohol Treatment Facilities. Reasons for this and recommendations for how these sources might be utilized more frequently will be provided in the final report.
| TABLE 9. Federal Data Sources | |
|---|---|
| Number of Reports | |
| SAMHSA National Survey on Drug Use and Health (NSDUH) | 12 |
| Behavioral Risk Factor Surveillance System (BRFSS) | 4 |
| Youth Risk Behavior Surveillance System (YRBSS) | 5 |
| SAMHSA Treatment Episode Data Set (TEDS) | 5 |
| SAMHSA Behavioral Health Barometer | 1 |
| SAMHSA Buprenorphine Treatment Practitioner Locator | 2 |
| SAMHSA National Survey of Substance Abuse Treatment Services (N-SSATS)[a] | 1 |
| U.S. Census Bureau Data | 13 |
| Bureau of Labor Statistics (BLS) | 3 |
| Centers for Disease Control and Prevention (CDC) Data | 2 |
| Healthy People 2020 | 0 |
| National Directory of Drug and Alcohol Treatment Facilities | 0 |
| SAMHSA Emergency Department Data | 0 |
| SAMHSA National Mental Health Services Survey (N-MHSS) | 0 |
Table 10 presents the number using various types of secondary state-level data. Notably, although Medicaid and to a lesser extent Medicare claims are widely used in services research, they are not widely utilized for needs assessment despite their potential for assessing service utilization. We will discuss this issue and provide recommendations for how these sources may be incorporated into SUD needs assessment.
| TABLE 10. State and Local Secondary Data | |
|---|---|
| Number of Reports | |
| State Management Information System (MIS) | 7 |
| State health database (including Medicaid enrollment) | 12 |
| Licensing boards | 4 |
| County/City Management Information System (MIS) | 1 |
| County/City health database | 1 |
| Provider Management Information System (MIS) | 1 |
| Medical record/Electronic health record | 2 |
| Medicaid claims | 2 |
| Existing reports/studies | 13 |
| Document review | 2 |
| Other data source or method | 14 |
| Medicare claims | 0 |
| Healthy People 2020 | 0 |
Tables 11-15 present sources of information obtained from various groups by means of surveys, focus groups, key informant interviews, meetings and steering committees. It is notable that peer organizations are not included in any form, in contrast to mental health needs assessments, in which this very common. A possible explanation is that peer organizations have not developed in the SUD treatment system to the extent that they have in mental health. We will discuss this issue with the TAG. Also notable is that very few (n=4) needs assessments utilized steering committees, though it is likely that many were guided by collaborations of various kinds that were not identified as steering committees.
| TABLE 11. Surveys | |
|---|---|
| Number of Reports | |
| Any surveys | 19 |
| State/local agency leadership/staff | 3 |
| Legislators | 0 |
| Provider organization leadership | 13 |
| Practitioner/workers | 6 |
| Peer organizations | 0 |
| Advocacy organizations | 0 |
| Consumers/patients | 6 |
| Family members | 2 |
| General public | 4 |
| Other groups | 7 |
| TABLE 12. Focus Groups | |
|---|---|
| Number of Reports | |
| Any focus groups | 8 |
| State/local agency leadership/staff | 1 |
| Legislators | 0 |
| Provider organization leadership | 4 |
| Practitioner/workers | 0 |
| Peer organizations | 0 |
| Advocacy organizations | 2 |
| Consumers/patients | 5 |
| Family members | 3 |
| Other groups | 4 |
| TABLE 13. Key Informant Interviews | |
|---|---|
| Number of Reports | |
| Any key informant interviews | 19 |
| State/local agency leadership/staff | 11 |
| Legislators | 0 |
| Provider organization leadership | 12 |
| Practitioner/workers | 5 |
| Peer organizations | 0 |
| Advocacy organizations | 3 |
| Consumers/patients | 4 |
| Family members | 3 |
| Other groups | 15 |
| TABLE 14. Meetings | |
|---|---|
| Number of Reports | |
| Any meetings | 4 |
| Community/public | 2 |
| State/local agency leadership/staff | 3 |
| Legislators | 0 |
| Provider organization leadership | 3 |
| Practitioner/workers | 1 |
| Peer organizations | 0 |
| Advocacy organizations | 2 |
| Consumers/patients | 2 |
| Family members | 2 |
| TABLE 15. Steering Committees | |
|---|---|
| Number of Reports | |
| Any steering committee | 4 |
| State/local agency leadership/staff | 1 |
| Legislators | 0 |
| Provider organization leadership | 1 |
| Practitioner/workers | 1 |
| Peer organizations | 0 |
| Advocacy organizations | 0 |
| Consumers/patients | 1 |
| Family members | 1 |
METHODS OF DATA ANALYSIS
After data collection, the second methodological activity involves analysis of the data. As discussed in the Background section, data analysis in the context of SUD treatment needs assessment primarily involves measuring the gap between what is and what should be--the need for additional service capacity, additional types of services, elimination of redundant or ineffective services, and additional population subgroups served. The simplest approach for measuring the population need for services is prevalence. Similarly, the simplest approach for measuring the supply of services is to conduct an inventory of the existing service system, measuring how many people are served. Though some needs assessments we reviewed go no further than this, these are not very useful for the function of needs assessments to serve as guides for decision making, for several reasons. First, as noted above, there is not a one-to-one correspondence between prevalence of a disorder and need for services. Second, this method does not take into account different treatment needs and types of treatment (for example, residential treatment versus outpatient treatment). Third, it provides little information about the inputs to treatment capacity--for example, specific types of staff or programs that would be necessary to provide adequate treatment.
Most of the reports we reviewed used some combination of quantitative and qualitative data in their analysis of need, going beyond the simplest approach but falling short of a more robust approach. An example is New Jersey's needs assessment for child behavioral health (New Jersey Department of Children and Families, 2016), which draws upon several management information systems (MIS) used for tracking and identifying patterns of service utilization combined with county-based planning and advisory groups established by statute to "identify service and resource gaps and priorities for resource development" and to advise the Department of Children and Families on "the development and maintenance of a responsive, accessible, and integrated system of care." The limitation of utilization data for measuring need is that the population of individuals with unmet need are likely to differ from those who are receiving services--and therefore to require different types of services. Additionally, utilization data do not identify inappropriate use (services received by individuals who do not have a need) unless covariates such as clinical status are examined. In short, this approach does not serve the third form of data analysis: to identify solutions.
METHODS FOR FORMULATING RECOMMENDATIONS AND PRIORITIES
Once the needs assessment has collected data and analyzed it to define the gap between what is and what should be, the final step is to specify and prioritize what is usually a considerable number of possible solutions. Few of the unpublished reports that we reviewed used techniques of planning models, such as those proposed by Green at al. (2016) that use mathematical formulas to estimate a population's service need based on social indicators correlated with substance abuse.
As noted in the background discussion of methodology, planning models of this type that use formulas to estimate capacity needs have received limited attention in recent years, with the exception of some use of simulation models and the Calculating for an Adequate System Tool (CAST) model developed by Green et al. (2016). Where this does take place, however, is with studies that focus on contingency planning related to anticipated policy changes, for example a needs assessment conducted in anticipation of California Medicaid expansion (California DHCS, 2012). For this assessment, researchers developed a complex algorithm that estimated the size and characteristics of the potential expansion population, with upper and lower bounds based on various assumptions, then estimated service utilization for various subgroups of this population, based on comparison with the current Medicaid population adjusted for differences between the two groups. Although this analysis did not attempt to estimate the need for particular categories of services, it did offer recommendations for addressing various gaps and shortcomings in the current system to accommodate the expansion population, as well as to improve the service system for all.
Optimally, needs assessments not only offer recommendations but also prioritization of recommendations to guide decision making. Only a fraction of those we reviewed did so, but one of the most effective means employed by those that did, primarily academic centers, was to provide a cost analysis, as in the report by Shepard et al. (2005). After estimating the number of persons with a clinically significant SUD, they calculated that providing substance abuse treatment and outreach services to them would require an additional cost of approximately $109 million ($17 per capita), of which the state Bureau of Substance Abuse Services would need to fund $31 million ($5 per capita), representing an increase of 42% over its current spending. While the authors acknowledge that this increase is formidable, they suggest that it could be manageable if spread over a period of five years, and that the increase for other payer sources would be proportionately smaller.
EXAMPLE OF DATA SOURCES AND METHODS
The Wisconsin Community Mental Health Needs Assessment stands as an example of an assessment that collected data from a wide range of sources. These included secondary data (LIFE Study reports, Behavioral Risk Factor Surveys, Youth Risk Behavior Surveys, data from the Centers for Disease Control and Prevention (CDC), hospital health assessments, and administrative data from organizations that serve mental health consumers); focus groups with diverse stakeholders including the general public, providers, and referral agents; surveys designed based on focus group feedback including a telephone survey with a sample of the general public, online surveys of providers and referral sources, and in-person surveys with a convenience sample of consumers recruited through provider organizations. While this represents a broader range of sources and a more rigorous methodology than most of the reports we reviewed, it demonstrates the possibilities for SUD treatment data collection. Several reports refer to "data triangulation," but there is little indication that this is done in any systematic way.
Data collected by a variety of federal agencies and made readily available electronically have become a primary source of information for both mandated and locally initiated needs assessment. This includes data related to prevalence, utilization, provider supply, and population characteristics. Given the central role these sources play in current needs assessment methodology, it is important to understand their strengths and limitations. As background for recommendations to address data gaps that will be provided in the final report, the following reviews the strengths and limitations of these sources for purposes of SUD treatment needs assessment.
Are there Best Practices Identified?
This section addresses the research question, "Are there best practices with respect to these needs assessments?" While it may be premature to identify best practices in SUD treatment needs assessment as there are not yet formal criteria to evaluate what constitutes best practice, in the review of needs assessment reports we identified a number of innovative and exemplary practices that might be candidates for these criteria.
Over the years, there have been articles recommending refinements in SUD treatment needs assessment. The aforementioned articles by McAuliffe et al. (2004) propose an improved method of measuring need; Rowan-Szal et al. (2007) discuss an instrument for assessing treatment staff training needs known at the Texas Christian University Program Training Needs; and most recently Green at al. (2016) present a sophisticated research-based methodology for assessing treatment needs and system capacity on a broad scale.
In our review of a sample of needs assessment, we identified practices, methods and approaches (typically more focused than those cited above) that we considered would contribute to the field if adopted more widely. These are discussed briefly below. We will discuss these practices in more detail in the Final Report.[5]
INNOVATIVE AND EXEMPLARY PRACTICES
As part of our quality review, we flagged practices that were innovative or exemplary in some respect and worthy of adoption in the field. In general, these are practices that add to the precision or the utility of a needs assessment. Among the exemplary practices were reports that went beyond offering recommendations to explain the rationale, feasibility, cost or barriers for acting on the recommendations. For example, one report identified various political, social, and demographic factors likely to affect capacity in the future, thus adding to the utility for planning purposes. We also flagged studies that presented more detail about the methods they employed as this helps users of the report to assess the reliability and applicability to a particular situation.
Other practices serve to improve the precision or level of detail in the measurement of need or availability of services, for example by adding a measure of clinical significance, which has been a major challenge in SUD needs assessment. Likewise, several studies adopted strategies for drilling down into data to obtain a fuller understanding, for example by conducting follow-up interviews with survey respondents or obtaining workforce capacity information that included not only numbers but caseload size. We flagged one study that used a simulated patient approach, calling agencies as though a potential client to inquire about availability of special services for special populations (LBGT). This "secret shopper" method has been used by CMS to test network adequacy, and in this case, the method demonstrated inaccuracies in the self-report information represented in N-SSATS.
Practices that enhance utility:
-
Identified forces that affect capacity at multiple (federal, state, county, systems, and organization) levels.
-
Along with strategies for recommendations, also included "rationale" for each strategy with examples from other states and "implementation steps" serving the purpose of the needs assessments as a tool for decision making.
-
Added clinical significance to prevalence estimates in measuring need.
-
Revised service definitions to clarify gaps identified in a previous-year needs assessment.
-
Estimated how new treatment slots should be distributed geographically.
-
Developed a code of ethics to guide the project and explain why IRB approval was not required.
-
Used the Robert Wood Johnson Social Determinants of Health (a set of social and behavioral factors that affect health and health disparities) as an organizing framework.
-
Utilized data visualization software to map clinics and organizations to reveal possible gaps in treatment provision across different regions.
-
Compared the state's needs to those of other comparable states.
-
Provided estimates of additional spending required for a "good" and an "ideal" system of care.
-
Reviewed policy changes that impact behavioral health services with graphic representation of impacts.
Practices that enhance precision or level of detail:
-
Identified comparable states for comparing rates (vs. simply using national averages).
-
Population density and number of overdoses by zip code were used to highlight underserved areas.
-
Created online inventory of inpatient, outpatient, and in-state residential behavioral health services for children and electronic bed tracking system for quantifying usage and determining service needs.
-
Survey asked workers for number of clients per week.
-
Followed up on publicly-available information about providers by contacting them to confirm and elaborate.
-
Described interviewer training and quality control.
-
Described the selection and training of bilingual surveyors (bilingual Navajo speakers) including project goals, concepts, interviewing skills and confidentiality, and how concepts and items could be interpreted into Navajo language.
-
Conducted follow-up interviews with a sub-sample of survey respondents to explore discrepancies between positive clinical screening and perceived need.
Have Any Methods been Validated?
The only needs assessments that provided any information about validation methods were the several academic research reports, which addressed, for example, validity of social indicators in estimating prevalence.
Quality of Substance Use Disorder Needs Assessment Reports
As discussed in the Methods section, we rated the quality of reports based on the clarity and transparency of the information presented about the methods utilized in the needs assessment. Here we summarize the results of the quality ratings. A table showing the ratings by number of reports in each category of quality is provided in Appendix D. The number of reports varies for each quality criteria. This is because we added items as we identified issues in the review process. For the Final Report we will include the entire sample of reports.[6]
Are the Purpose or Questions Clearly Defined and Addressed?
We assessed whether the assessment report clearly specified the research questions the assessment intended to address. As shown in Appendix D, most of the reports (24 out of 29) were judged to have clearly defined and addressed the purpose.
Are Populations Defined Clearly?
Of 33 reports, 26 provided clear explanations for how the population was defined for the purposes of needs assessment, and five provided partial or imprecise explanations.
Is Treatment Need Fully Defined?
As discussed in the section on methodology, defining treatment need is one of the most critical components of a needs assessment; it was also the most problematic aspect of the reports we reviewed. Given the importance, we approached this issue from several perspectives, examining how it was addressed in items on questions and populations and, for a sub-sample of reports, a question in the quality section about how need was defined.
Despite the attention to this complex issue in the literature on SUD needs assessment methodology as far back as the early 1980s (Maddock, et al., 1988; Rush, 1990), very few of the reports we reviewed offer more than a brief explanation of need. In many cases, the extent was limited to survey questions about unmet needs or an estimate of unmet needs defined as untreated prevalence, drawn from data sources such as NSDUH. In the quality ratings, eight of the 16 reports rated on this criterion provided what we judged to be an adequate definition of need, three defined (unmet) need simply as the gap between prevalence and service utilization, and the remaining reports provided no definition. As discussed above, this is inadequate for the purpose of needs assessments to serve as a guide for planning and decision making. We will discuss this issue in more detail in the final report, with recommendations and examples of best practices for how it may be addressed.
Is the Setting Clearly Specified?
Nearly all (n=28) of the reports rated on this criterion (n=32) provided clear definitions of the setting, while four provided partial or less precise explanations.
Are Levels of Care Defined?
Rating on this criterion was mixed: 16 rated as providing clear definitions of levels of care, whereas six were rated as providing less complete definitions and nine as not defining levels of care. Consistent with other findings related to levels of care, this is clearly an area for improvement and will be addressed with recommendations in the final report.
Are Data Methods Described?
This category includes criteria related to survey methodology (when applicable, whether random sampling was employed, whether testing of the instrument was reported), whether statistical methods were described, whether stratification was used in the analysis if applicable, whether data limitations were reported and whether validation of the methodology was reported. Of 24 reports using surveys, six reported random sampling, while it was unclear for seven. Only three reported on whether the instrument had been tested. Statistical methods were described by 15 of 27 reports. Stratification was reported in three of the 15 reports reviewed on this criterion. Limitations related to data were reported by 22 of 31 reports. Related to the research question about whether any needs assessment methods have been validated, only three of 30 reports described validation of any aspects of methodology. Recommendations for improvement in this area will be addressed in the final report, with input from the TAG.
Was a Model System for Gap Comparison Presented?
This criterion is related to the "what should be" condition of a needs assessment. Model system refers to some template such as the ASAM Levels of Care or the SAMHSA Good and Modern Behavioral Health System. Exactly half of 30 reports did reference such a model.
Is there Guidance for Policy Decisions?
This important criterion is related to the fourth essential component of a needs assessment, that it serves the purpose of supporting decision making. Of 34 reports, 28 offered recommendations, and 20 of those addressed priorities, feasibility, and/or strategies for acting on the recommendations.
How is Capacity Measured?
How capacity is measured is a fundamental aspect of needs assessment. We rated methods of measuring capacity based on the reliability of the data source, with the most reliable being an inventory such as number of providers, beds, slots, etc. (provided in eight reports), followed in order of decreasing reliability (due to the relative potential for missing data, selection bias, subjectivity, or imperfect knowledge) by utilization data such as administrative data, claims, etc. (four reports), consumer self-report regarding access, availability, etc. (three reports), key informants (six reports), surveys (four reports).
A number of reports identified the challenge of measuring capacity. While there are various sources of information about the number of different types of facilities and provider organizations, such as SAMHSA's N-SSATS database, and sources of utilization data, such as TEDS, they do not provide readily available information about the actual capacity of a system--how many people it is able to serve. In addition to a lack of data, capacity is challenging to measure because it involves multiple factors--workforce characteristics, available resources, location of services, etc.
Assessing the workforce component of capacity is especially challenging for a variety of reasons: the nomenclature and scope of practice for different occupational categories in the substance use treatment field vary widely from one location to another, and it is difficult to determine the job functions in a particular organization--for example, is a nurse an administrator or a direct care provider? This issue arises especially frequently in connection with Medication-Assisted Treatment (MAT) capacity as there are numerous reports that authorized prescribers and treatment facilities do not operate at full capacity, but the extent of the gap and the reasons for it are unclear. A recent U.S. Government Accountability Office (GAO) report has emphasized the importance of measuring progress and understanding barriers in increasing MAT capacity, which the U.S. Department of Health and Human Services is now actively evaluating (GAO, 2017). The results of these evaluation activities will be informative in understanding issues related to SUD treatment capacity generally.
With respect to workforce capacity it should be noted that a number of reports focus on this topic exclusively, whereas others took a more global approach to measuring capacity and need and did not address it all. We allowed for both when determining which assessments to include in our review--on the grounds that this difference depended on the intended scope of the needs assessment. In the quality ratings we assess whether this scope was adequately defined.
Are Ethical Issues/IRB Approval Addressed?
This quality question was prompted by a needs assessment involving substance use by a vulnerable population, which referenced an earlier study in the 1970s that is regarded as having violated human subjects protection. Five of 32 reports indicated having received IRB approval. We flag this as a topic for discussion: whether locally initiated needs assessments should be subject to the same requirements as research studies and, if so, what the implication of this burden would be and whether there might be less burdensome ways of addressing ethical issues.
Our quality assessment was designed to provide an overview of how effectively the sample of needs assessment reports fulfilled the primary functions of a needs assessment, with an emphasis on the utility. Thus, we did not attempt to judge the appropriateness of the methodology as much as the level of detail that was provided, such that a user of the report would be able to judge the extent to which they might rely on it for a particular purpose. In addition, we included several criteria, such as the question of ethical issues and IRB approval, that are not widely met, but which are present in a few exemplary cases.
Population, Workforce, Setting, and Levels of Care
Clear and appropriate definitions of these components of a treatment system are critically important for the reliability and utility of a needs assessment. A majority, but not all, reports were adequate in these areas. Few needs assessments utilized the ASAM Criteria for defining levels of care; this is a particularly challenging aspect of SUD needs assessment because definitions of levels of care vary so extensively from one locale to another and are often not clearly defined for the service system, making it difficult for a needs assessment to do the same.
Data Collection and Analysis
We examined reports for several aspects of methodology, including the use of surveys and analytic methods. Our focus was less on whether the methodology was appropriate but rather whether it was reported. Needs assessments vary widely in methodological sophistication, which has important implications for how they are used.
Validation
In our quality ratings, we looked specifically for any mention of validation and found only three of the unpublished reports that referenced any type of validation.
Need and Capacity
We examined how need and capacity are defined and measured. In particular, we were interested in how many reports go beyond an estimate of the difference between treated and untreated prevalence as a measure of need, which has limited utility for planning purposes. We extracted this information from a subset of 16 reports; of these five provided no operational definition of need, three defined need simply as estimated untreated prevalence, and eight provided definition based various other sources such as published literature and standard clinical assessments. Only one study estimated the number with a diagnosis that would not need treatment. One study, which focused on accessibility of services for people with disabilities, used the requirements of the Americans for Disabilities Act as a definition of the "what should be" condition.
RESULTS II: NEEDS ASSESSMENTS FROM OTHER PROVIDER TYPES
This section provides an introduction to the research question that asks, in part, "Are there needs assessments from other provider types (for example, primary care physicians) that could be applied to the SUD treatment workforce?" Two models are discussed: general health care and the Medicaid 1115 Waiver Delivery System Reform Incentive Program (DSRIP). The final report will address the additional components of the question that call for recommendations: "What are the differences between other workforces and the SUD workforce that might make such application difficult, and how could these difficulties be overcome?".
General Health Care
The most obvious place to identify approaches in other provider types of systems that might serve as a model for SUD needs assessment is in the general health care field. Two types of health care needs assessment that are particularly promising methodological models are the HRSA's designation of HPSA and the needs assessments conducted in preparation for CMS DSRIP applications. While these are conducted at a scale and complexity of methodology that is beyond the scope of most locally conducted SUD needs assessments, they merit review as models of best practices.
Health Professional Shortage Areas (HPSA)
HPSA assessments, which are conducted by primary care clinics applying for HRSA funding, address provider shortages in primary care, dental care, and mental health. Determination of eligibility for funding is based on a scoring algorithm that is specific to each of the three provider types. Several features of the HPSA determination process are relevant to SUD needs assessment, particularly in methods for addressing the complexities of assessing capacity as discussed above. Briefly, these include:
-
Determinations made on the basis of three types of shortage: geographic (shortages affecting the entire population of a specified area), population (affecting specific subgroups such as low income), or facilities (specific types of health care facilities).
-
Scoring based on weights for a set of several components: for mental health these are population-to-provider ratio, percent poverty, ratio of elderly and youth to the general population, prevalence of alcohol and substance abuse, and travel time to care facility.
-
Detailed definitions for components, for example how to calculate and count full time equivalent (FTE) psychiatrists.
These methods provide for quantitative comparison of needs across geographical areas and across different types of needs within an area, thus serving the function of needs assessment in providing guidance for priority-setting and decision making--in this case, for allocation of resources to areas with the greatest need.
As models for SUD treatment capacity needs assessments, the HPSA approach has one primary limitation: it is a method for relative allocation of resources across areas--directing resources to localities where the shortages are greatest--but is not a method for planning at the system level. That is, it does provide an indication of how allocations should be made within areas: how many psychiatrists, nurses, social workers etc. should be provided in a particular area. In this respect, the HPSA methodology is similar to the SAMHSA block grant formulas, which also use social indicators to determine the size of the allocation to individual states but not how the state's allocation should be used. To adapt this methodology for SUD treatment system capacity needs assessment, it would be necessary to combine it with the "what should be" component to determine how the workforce should be distributed in a balanced system of care. An example is McAuliffe's Rhode Island needs assessment, which determined the appropriate location of treatment facilities based on local area social indicators. The IMU on which the Health Provider Shortage Area designation is based would need to be quite different for SUD. The IMU score is based on four weighted factors: providers-population ratio, percent at 100% of the FPL, percent aged 65 and over, and the infant mortality rate. The indicators suggested by Green et al. (2016) would be better suited to SUD. Finally, the designation of medically underserved area is determined by a cut-off IMU score of 62 or below (out of a possible 100). An appropriate cut-off score for SUD would need to be developed.
Delivery System Reform Incentive Program (DSRIP)
DSRIP is a type of CMS Section 1115 Waiver created by the ACA that allows Medicaid funding to be used to create incentives for providers to pursue a wide range of system reforms. (The Kaiser Family Foundation website provides an overview of DSRIP waivers.[7]) States typically require eligible entities to submit a plan for approval that outlines the specific projects and metrics they intend to implement, features of which could provide models for smaller-scale SUD needs assessments. An example of a DSRIP report is the Capital Region, Mohawk and Hudson Valley DSRIP Community Needs Assessment (NY CNA) conducted by the Albany Medical Center and Ellis Performing Provider Systems (PPS) (Albany Medical Center PPS & Ellis PPS, 2014).
The NY CNA presents a huge amount of information about health care resources and utilization, as well as the health needs for the general population, Medicaid insured, and uninsured populations for 11 counties. Some features of this report that offer models for SUD treatment needs assessments include:
-
Engagement with a diverse group of organizations in developing the CNA including community health centers; health plans; local business; philanthropy; colleges/universities; school districts; faith-based; housing; mental/behavioral health; transportation; social services; and media.
-
Diverse methods of data collection designed to fill gaps in any one source. These included a provider survey, a community-based organization survey, a consumer survey, focus groups with Medicaid members and the uninsured concentrated on three groups (chronic disease, mental health and substance abuse), and listening sessions held with providers, including physicians, members and the general community.
-
Detailed information about providers from the state's Provider Network Data System, which the authors considered, based on research reports, to be more reliable than the widely used Area Health Resources Files.
-
The distribution of behavioral health providers in local areas (square miles by neighborhood) in relationship to the density of beneficiaries with behavioral health conditions.
-
A summary of systems assets and resources identified and quantified through the collaborative process of developing the CNA.
Locally conducted SUD treatment needs assessments are unlikely to have the resources that were available for the NY CNA, and this group also benefitted from New York's exceptionally rich health information systems. However, the practices identified in the points above could be readily adapted for use on a smaller-scale.
RESULTS III: HOW STATES OPERATIONALIZE NETWORK ADEQUACY STANDARDS
This section presents information obtained through a separate process in the environmental scan, reviewing procedures and policies related to network adequacy standards in selected states. Network adequacy standards established by the states reflect the "what should be" condition in a needs assessment as defined (at least implicitly) at the level of state policy making.
On May 6, 2016, CMS published the Medicaid and Children's Health Insurance Program Managed Care Final Rule (Managed Care Rule) which revised Title 42 of the Code of Federal Regulations (CFR) to include language that required states to develop network adequacy standards and ensure adequate provider capacity for their Medicaid program. Specific language in these regulations requires states to develop and assess standards for certain specialty services including behavioral health (mental health and SUD services). These changes aimed to align Medicaid managed care regulations with requirements of other major sources of coverage. There are three parts of the Managed Care Rule that comprise the majority of network adequacy standards: Title 42 of the CFR Part 438.68 Network adequacy standards, Part 438.206 Availability of services, and Part 438.207 Assurances of adequate capacity and services. Each of these parts is described below.
Network Adequacy Standards--Time and Distance
Part 438.68, Network adequacy standards, requires states to develop time and distance standards for adult and pediatric behavioral health (mental health and SUD treatment) providers. Time means the number of minutes it takes a beneficiary to travel from the beneficiary's residence to the nearest provider site. Distance means the number of miles a beneficiary must travel from the beneficiary's residence to the nearest provider site. While states are required to establish time and distance standards, Plans are required to meet the standards for time or distance. For example, some states require that SUD services must be within 15 miles from the beneficiary's residence or within a 30-minute drive from the beneficiary's residence.
Network Adequacy Standards--Timely Access
Part 438.206, Availability of services, requires the Plans to meet state standards for timely access to care and services, taking into account the urgency of the need for services. Timely access standards refer to the number of business days in which a Plan must make an appointment available to a beneficiary from the date the beneficiary, or a provider acting on behalf of the beneficiary, requests a medically necessary service.
Network Certification Requirements
Part 438.207, Assurances of adequate capacity and services, requires each Plan to submit documentation to the state Medicaid agency to demonstrate that it complies with the following requirements:
-
Offers an appropriate range of services that is adequate for the anticipated number of beneficiaries for the service area (i.e., as defined by the state).
-
Maintains a network of providers, operating within the scope of practice under state law, that is sufficient in number, mix, and geographic distribution to meet the needs of the anticipated number of beneficiaries in the services area.
Some states are using newer approaches to determine if they have sufficient capacity to meet the needs of beneficiaries with SUD; California and North Carolina are described below. The North Carolina example illustrates how the state required Plans to use the assessment to identify service gaps and strategies for addressing these gaps.
California
The California Department of Health Care Services (DHCS) has developed and will be putting into place (in July 2018) a process to implement the federal managed care regulations regarding time, distance, and timely access to SUD services included in the Drug Medi-Cal program. This includes that SUD managed care plans document that it meets the federal network adequacy requirements. DHCS also incorporated state legislation from the fall of 2017 that codified the federal managed care requirements for Medi-Cal including the Drug Medi-Cal program.
DHCS has developed a tool for counties (who are the state's Drug Medi-Cal Plans) to assess the adequacy of the SUD provider network against the needs of Medi-Cal beneficiaries with an SUD. Specifically, the state has developed a Network Adequacy Certification Tool (NACT) for Plans to collect information on location, current capacity, and projected capacity of SUD providers. The NACT collects information on:
-
The site (physical location) of each organization that renders SUD services--this includes county owned and operated facilities and other contracted network provider sites.
-
The type of SUD provider that renders the service (individual practitioners, outpatient clinics, intensive outpatient programs, residential programs, and opioid treatment programs).
-
The age group served, hours of operation, FTE of practitioners, licensed capacity for Opioid Treatment Programs (OTPs), distance between site and closest public transportation, telehealth capabilities, and language capacities.
-
Current number of Medi-Cal beneficiaries served by the provider and the maximum number of Medi-Cal beneficiaries the provider will accept. It also collects information regarding the projected utilization of Drug Medi-Cal services for the following year.
The NACT also requires the Drug Medi-Cal Plan to summarize the provider count for the geographic areas they serve (by provider type and age group) as well as provide the expected utilization for the following modalities: outpatient SUD clinics, intensive outpatient program and OTPs. Information regarding the NACT will be included in the Final Report.[8]
Using the information from the NACT, the Plan must submit to DHCS geo-access maps of all the network providers in the Plan's service area. The map must plot the time and distance for all SUD network providers, stratified by service type, and geographic location using beneficiary addresses, provider addresses and time (minutes)/distance (miles) standards set forth by the state. The Plan also has to provide information on the number and percent of Medi-Cal beneficiaries with SUD that were without access to SUD services. The state has established the following time and distance standards for SUD services:
-
Outpatient services (three tiers)--for more populated counties the standard is up to 15 miles or 30 minutes from a beneficiary's place of residence; for less populated counties the standard is 30 miles or 60 minutes from a beneficiary's place of residence; for sparsely populated counties the standard is 60 miles or 90 minutes. The time and distance standards identify which counties fall into which of the three tiers.
-
OTPs (four tiers)--same tiers the state has developed for outpatient services, but between the second and third tier this is another tier that has an access requirement of 45 miles or 75 minutes. The time and distance standards identify which counties fall into which of the four tiers.
Access standards for outpatient SUD services are appointments within ten days from the request for services; for OTPs, the standard is within three days from request to appointment. The distance and time variance for OTPs is based on the beneficiaries need in an OTP to receive their medication daily, since imminent withdrawal will occur without such medication.
North Carolina
Similar to California, the North Carolina Department of Health and Human Services (DHHS) has developed network adequacy and access requirements for its behavioral health managed care plans that are based on standards reflected in the final federal Medicaid rule. However, North Carolina requests that the plans use this information to identify the gaps in network adequacy and accessibility as well as strategies to address the identified gaps. DHHS has developed a tool that set forth requirements for Local Management Entities-Managed Care Organizations (LME-MCOs) to conduct a Community Behavioral Health Service Needs, Providers and Gaps Analysis. The Division of Mental Health, Developmental Disabilities and Substance Abuse Services and the Division of Medical Assistance--both Divisions within DHHS --have contracts with LME-MCOs containing requirements for assessments of community need, availability of providers, and gaps in services. DHHS requires LME-MCOs to develop a strategic plan to address gaps for Medicaid and non-Medicaid beneficiaries. The tool is used to collect and analyze information across both mental health and SUD services using five categories: outpatient services (including individual practitioners), location-based services (e.g., IOP, OTPs), community/mobile service (mobile crisis and employment services for SUD), site-based crisis services including detoxification, inpatient services, and specialized services (SUD residential treatment). The tool collects information on:
-
Number of providers that are accepting new consumers (Medicaid and non-Medicaid).
-
Number of consumers (Medicaid and non-Medicaid) with choice of two providers within 30 miles/45 minutes.
-
Medicaid and non-Medicaid beneficiaries' (individuals with low income served with state general revenue and federal block grant funds) access to services.
Each LME-MCO must provide geo-maps for each Medicaid-funded service listed in the requirements. The LMEs-MCOs are also required to provide additional information for the Gaps/Needs Analysis, including the size/geographic location/distribution of specific cultural and special populations. The plan must describe the obstacles and barriers to serving these populations and the gaps they experience in accessing SUD services.
The LMEs-MCOs are required to discuss the gaps they find from the administration of the tool with local leaders, staff, and consumers of SUD organizations. This includes:
-
A description of methods used to get input from consumers and family members regarding service needs, gaps and strategies, including efforts to achieve geographic and disability-specific representation.
-
The service gaps in the SUD service system that were identified by consumers and family members.
-
The methods used to get input from stakeholders other than consumers and family members regarding service needs, gaps and strategies and the SUD service gaps were identified by other stakeholders.
A copy of the 2018 North Carolina Network Adequacy and Accessibility Analysis Requirements Tool will be included in the Final Report.[9]
PRELIMINARY RECOMMENDATIONS AND CONCLUSIONS
The final report will focus on the research questions that call for recommendations, drawing upon input from the TAG and issues identified in the reviews of literature and needs assessments reports described above. Specifically, these questions are:
-
What data and methods most effectively gauge treatment needs and current gaps?
-
What questions should be answered in conducting these needs assessments?
-
How does ASAM Levels of Care relate to capacity needs (both in workforce and setting)?
-
How can best staffing practices, telehealth policies and peer supports be incorporated into needs assessments?
-
What are the key pieces of missing data that would improve these needs assessments, including one-time data collection efforts and potential federal efforts?
-
How can needs assessment methods be validated?
-
How can needs assessment approaches be made more uniform while remaining adaptable to local conditions and stakeholder priorities?
-
How can assessments become more effective at promoting organizational and system change to address, rather than simply identify, system gaps?
Here we provide some background information based on the environmental scan for more detailed discussion on specific recommendations to be provided in the Final Report.
Data and Methods for Gauging Treatment Needs and Gaps
Although the review of methodology literature describes a variety of methods and types of data for assessing treatment needs of varying complexity, most of the needs assessment reports reviewed, with a few exceptions, use relatively simple approaches, combining quantitative data from secondary sources such as national surveys and local administrative data with qualitative information obtained from stakeholders. Some considerations for recommendations are: development and use of more systematic methods for combining qualitative and quantitative information (data triangulation), federal action to address current gaps in data sources, and better methods for measuring clinical significance in addition to diagnosis.
Questions that Should be Answered in Needs Assessments
Some of the recommendations in this area should address the questions of how to define and measure continuity and continuum of care, what are the specific types of services required by different subgroups defined by severity, chronicity etc., how to identify redundant and ineffective services, how to incorporate measurement of assets with measurement of needs.
Relation of ASAM Levels of Care to Capacity Needs
The review of needs assessment reports identified very few that drew upon the ASAM Criteria as a framework. The final report, with input from the TAG, will provide a detailed discussion about how ASAM Criteria may be incorporated in needs assessment as a formulation for the "what should be" conditions.
Incorporating Best Staffing Practices, Telehealth Policies and Peer Supports into Needs Assessments
While information on these topics was relatively sparse in the needs assessments we reviewed, there were some examples that would serve as recommendations for the field. The question of peer supports requires further investigation. Only four of the reports indicated that they included peers in their assessment of workforce categories. It may be that this is a question of nomenclature, however, as a considerable portion of the SUD treatment workforce are persons in recovery. The final report will include these as well as other recommendations suggested by the TAG and other sources such as the research and policy literature.
Supplying Key Pieces of Missing Data
The description of commonly utilized federal data sources in the previous section identifies a number of limitations for purposes of SUD needs assessment. Members of the TAG have expertise in this area, which the final report will draw upon to recommend options for addressing these gaps.
Validating Needs Assessment Methods
While validation of tools for needs assessment at the individual level is commonplace, there was virtually no mention of validation in the reviewed needs assessment reports. However, several articles in the methodology literature, including some by members of the TAG, do report on methods of validation, which will be included in the final report.
Approaches for Making Needs Assessments More Uniform
Because SUD treatment systems vary extensively from one locale to another, locally conducted needs assessments have the advantage of being attuned to the issues and characteristics unique to the region. A drawback of the variability in design, methods and quality, however, is that it limits the possibility of another potential use of these reports for some form of "meta-assessment" to investigate regional variations and consistencies of SUD treatment systems. The review of needs assessment reports, especially those in the federally mandated category, as well as the methodology literature review suggested possibilities for this purpose.
One strategy that would aid in making SUD treatment needs assessments more uniform and also support improvements in quality would be to emulate the many federal, state, and private organization guidelines and tools that are available for conducting CHNAs and CHAs. At the federal level the CDC provides the web-based CHI (CHI) Navigator,[10] which provides tools for conducting CHNAs, with an emphasis on promoting collaboration among various types of organizations such as health care systems, public health agencies, and community-based organizations. A number of state public health agencies have developed guides for local agencies to develop CHAs for purposes of accreditation by the Public Health Accreditation Board (PHAB). For example, the Iowa Department of Public Health provides an online guide with detailed information for each of the steps in developing a CHA keyed to the requirements of the PHAB.[11]
A private non-profit organization, Community Commons, has developed a free web-based platform "designed to assist hospitals (with particular attention to critical access and other smaller facilities), non-profit organizations, state and local health departments, financial institutions, and other organizations seeking to better understand the needs and assets of their communities, and to collaborate to make measurable improvements in community health and well-being."
Tools modeled on these examples but designed specifically for SUD treatment, with options to accommodate local variations, would be an important contribution the enhancing uniformity. Tools of this kind could also serve to enhance the quality of needs assessments by establishing quality criteria and offering guidance on methodology.
Another promising approach for enhancing uniformity as well as quality is the research-based methodology of CAST, a tool designed to provide practitioners and policy makers with guidelines on the number of programs, practitioners, and interventions that are needed in the local substance abuse treatment system (Green, et al., 2016). This methodology is described in more detail in the review of SUD needs assessment methodology literature.
Increasing the Effectiveness of Needs Assessment in Promoting Organizational and System Change
This topic primarily concerns the recommendations and prioritization component of needs assessment, the extent and quality of which varied considerably among the reviewed needs assessment reports. The final report will draw upon best practices from the reports to provide recommendations for enhancing this function. Additionally, there are several recent reports on the potential, as yet largely unrealized, of leveraging the information from CHNAs and CHA for system change, for example Bender (2017), which we will summarize for recommendations.
Conclusions
Overall, we found that the SUD-specific assessments that we reviewed share certain features such as mixed methods of data collection (surveys, key informant interviews, focus groups, services utilization data, etc.) but with considerable variability in the scope and level of detail that is provided.
-
Recommendation priorities, feasibility, and strategies: As discussed in the introductory section on needs assessment methodology, a key function of a needs assessment is to serve as a guide for decision making and/or priority-setting. A comprehensive needs assessment, therefore, will go beyond documenting gaps in a treatment system or unmet needs in a population, but will additionally provide at least guidance on ways in which needs and gaps may be addressed, and--optimally--information about the feasibility, challenges, costs, and opportunities for implementing recommendations. Appendix D, which presents our quality assessments, indicates that only about half of those reviewed provide this key function.
-
Resources/assets/strengths: As emphasized in the more recent literature on needs assessment methodology, documentation is an important component for serving the function of planning and priority-setting--not only documentation of system gaps and limitations but also of strengths on which to build. This was addressed by only a handful of the reports we reviewed (n=7).
-
Levels of care: One of the questions in our review was about reporting on levels of care, including whether ASAM Criteria were employed. We found that ASAM Criteria were used only in a few cases, and that generally there was a great deal inconsistency about how levels of care were specified. Few of the reports asked the direct question, "What is the capacity of different levels of care in the system?"
-
System redundancy/efficiency: None of the reports that we reviewed measured the extent to which there was redundancy, underutilized capacity, and inefficient service delivery that might provide opportunities for system reform without additional resource demands.
Some important aspects of treatment capacity were addressed by only a few of the needs assessments. These included peer involvement, the functions of law enforcement, estimates of changes in demand resulting from system reforms, treatment completion/adherence as an aspect of utilization, and the extent of EBPs.
The most likely reasons for many of these omissions are limitations in currently available data, which will be addressed in the final report.
It is evident from our review that SUD treatment presents some unique challenges for needs assessment, mainly in the considerable variability in how SUD treatment systems are structured and in the relative lack of uniformity in defining aspects of systems (such as workforce designations, service categories, provider types and levels of care) compared to health care and even mental health. A framework to address these challenges, known as CAST, developed by Green et al. (2016) is now being tested in several sites. It will be interesting to see how this approach will be disseminated and the extent to which it influences SUD treatment needs assessment.
APPENDIX A: REFERENCES
Abelson, J. (2009). "Opportunities and challenges in the use of public deliberation to inform public health policies." Am J Bioeth, 9(11): 24-25.
Albany Medical Center PPS & Ellis Performing Provider Systems (2014). Capital Region, Mohawk and Hudson Valley DSRIP Community Needs Assessment, Albany Medical Center PPS, Ellis PPS.
Altschuld, J.W., and R. Watkins (2014). "A primer on needs assessment: More than 40 years of research and practice." New Directions for Evaluation, 144: 5-18.
Altschuld, J.W., and A.C. Watkins (Eds.) (2014). Needs Assessment: Trends and a View Toward the Future. New Directions for Evaluation.
Aoun, S., D. Pennebaker, and C. Wood (2004). "Assessing population need for mental health care: A review of approaches and predictors." Mental Health Services Research, 6(1): 33-46.
Armstrong M.I., K.A. Blasé, B. Caldwell, W. Holt, T. King-Miller, A. Kuppinger, C. Obrochta, D.N. Policella, and F. Wallace (2006). Final Report: Independent Assessment of the New Jersey's Children's Behavioral Health Care System. Tampa, FL: University of South Florida, Louis de la Parte Florida Mental Health Institute.
Batsche, C.J., and S. Reader (2012). "Using GIS to enhance programs serving emancipated youth leaving foster care." Eval Program Plann, 35(1): 25-33.
Beck, A.J., P.M. Singer, J. Buche, R.W. Manderscheid, P. Buerhaus, C.M. Tuohy, and M.L. Boulton (2016). A Minimum Data Set for the Behavioral Health Workforce. Behavioral Health Workforce Research Center.
Belenko, S., and J. Peugh (2005). "Estimating drug treatment needs among state prison inmates." Drug Alcohol Depend, 77(3): 269-281.
Bender, K. (2017). "Knowing your community: Community health assessment as a powerful tool. Journal of Public Health Management & Practice, 23(4) Supp.
Bopp, M., E.A. Fallon, D.J. Bolton, A.T. Kaczynski, S. Lukwago, and A. Brooks (2012). "Conducting a Hispanic health needs assessment in rural Kansas: Building the foundation for community action." Evaluation & Program Planning, 35(4): 453-460.
Bradshaw, J. (1972). Taxonomy of Social Need. Problems and Progress in Medical Care: Essays on Current Research, 7th series. G. McLachlan. London: Oxford University Press, 71-82.
Breer, P., W.E. McAuliffe, and E.B. Levine (1996). "Statewide substance abuse prevention planning." Eval Rev, 20(5): 596-618.
Burnam, M.A., P.H. Reuter, J.L. Adams, A. Palmer, K. Model, J.E. Rolph, J. Heilbrunn, G.N. Marshall, D.F. McCaffrey, S.L. Wenzel, and R.C. Kessler (1997). Review and Evaluation of the Substance Abuse and Mental Health Services Block Grant Allotment Formula. Santa Monica, CA: RAND Corporation.
California Department of Community Services and Development (2016). 2016-2017 Community Action Plan.
California Department of Health Care Services (DHCS) (2012). California Mental Health and Substance Use System Needs Assessment, Technical Assistance Collaborative/Human Services Research Institute.
Center for Evidence Based Management (2014). Critical Appraisal Checklist for a Case Study. https://www.cebma.org.
Chung, Y., L. Salvador-Carulla, J.A. Salinas-Perez, J.J. Uriarte-Uriarte, A. Iruin-Sanz, and C.R. Garcia-Alonso (2018). "Use of the self-organising map network (SOMNet) as a decision support system for regional mental health planning." Health Research Policy and Systems, 16(1): 35
Ciarlo, J.A., and D.L. Tweed (1992). "Implementing indirect needs-assessment models for planning state mental health and substance abuse services." Evaluation and Program Planning, 15(2): 195-210.
Community Action Partnership (n.d.). COE DEVELOPED CSBG ORGANIZATIONAL STANDARDS: Category 3 Community Assessment.
Conley, A.M., S.A. Vagi, and J. Horney (2014). "Use of the community assessment for public health emergency response to conduct community health assessments for public health accreditation." Journal of Public Health Management & Practice, 20(5): 490-497.
Dewit, D.J., and B. Rush (1996). "Assessing the need for substance abuse services: A critical review of needs assessment models." Evaluation & Program Planning, 19(1): 41-64.
Doessel, D.P., R.F. Williams, and H. Whiteford (2010). "Structural imbalance and resource shortage in the Australian mental health sector." J Ment Health Policy Econ, 13(1): 3-12.
Dworkis, D.A., L.A. Taylor, D.A. Peak, and B. Bearnot (2017). "Geospatial analysis of emergency department visits for targeting community-based responses to the opioid epidemic." PLoS ONE.
Edlund, M.J., B.M. Booth, and Z.L. Feldman (2009). "Perceived need for treatment for alcohol use disorders: Results from two national surveys." Psychiatr Serv, 60(12): 1618-1628.
Federal Register (2014). Additional Requirements for Charitable Hospitals; Community Health Needs Assessments for Charitable Hospitals; Requirement of a Section 4959 Excise Tax Return and Time for Filing the Return. Internal Revenue Service.
Ford, W.E., and J.W. Luckey (1983). "Planning alcoholism services: A technique for projecting specific service needs." Int J Addict, 18(3): 319-331.
Gaber, J. (2000). "Meta-needs assessment." Evaluation & Program Planning, 23(2): 139-147.
Georgia Watch Health Access Program. Nonprofit Hospital Community Health Needs Assessments in Georgia.
Green B., R. Lyerla, D.F. Stroup, A. Azofeifa, and P.M. High (2016). "A tool for assessing a community's capacity for substance abuse care." Prev Chronic Dis, 13: 1-10.
Hser, Y.I., C. Teruya, A.H. Brown, D. Huang, E. Evans, and M.D. Anglin (2007). "Impact of California's Proposition 36 on the drug treatment system: Treatment capacity and displacement." Am J Public Health, 97(1): 104-109.
Institute of Medicine (IOM) (2001). Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press.
Jarman, B., S. Hirsch, P. White and R. Driscoll (1992). "Predicting psychiatric admission rates." British Medical Journal, 304(6835): 1146-1151.
Kaufman, R. (1986). "Obtaining functional results: Relating needs assessment needs analysis, and objectives." Educational Technology, 26(1), 24-26.
Kessler, R.C., K.A. McGonagle, S. Zhao, C.B. Nelson, M. Hughes, S. Eshleman, H.U. Wittchen, and K.S. Kendler (1994). "Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: Results from the National Comorbidity Survey." Archives of General Psychiatry, 51(1): 8-9.
Kwan, K., V. Do-Reynoso, G. Zarate-Gonzalez, and S. Goldman-Mellor (2018). "Development and implementation of a community health survey for public health accreditation: Case study from a rural county in California." Eval Program Plann, 67: 47-52.
Lavey, W.G. (2017). "Underutilized community health needs assessments: Four environmental actions for hospitals that improve community health." Health Matrix, 27(1): 229-261.
Lee, Y.F., J.W. Altschuld, and J.L. White (2007a). "Effects of multiple stakeholders in identifying and interpreting perceived needs." Evaluation & Program Planning, 30(1): 1-9.
Lee, Y.F., J.W. Altschuld, and J.L. White (2007b). "Problems in needs assessment data: Discrepancy analysis." Evaluation & Program Planning, 30(3): 258-266.
Maddock, J.M., D. Daley, and H.B. Moss (1988). "A practical approach to needs assessment for chemical dependency programs." Journal of Substance Abuse Treatment, 5(2): 105-111.
Marr B (2015). "How big data is changing healthcare." Forbes. https://www.forbes.com/sites/bernardmarr/2015/04/21/how-big-data-is-changing-healthcare/#6523b7b42873.
Marshall, D., T. Pyron, J. Jimenez, J. Coffman, J. Pearsol, and D. Koester (2014). "Improving public health through state health improvement planning: A framework for action." J Public Health Manag Pract, 20(1): 23-28.
McAuliffe, W.E. (1978). "On the statistical validity of standards used in profile monitoring of health care." Am J Public Health, 68(7): 645-651.
McAuliffe, W.E. (1990). "Health care policy issues in the drug abuser treatment field." J Health Polit Policy Law, 15(2): 357-385.
McAuliffe, W.E. (2004a). "Measuring treatment needs: A reply to Gfroerer, Epstein, and Wright." Addiction, 99: 1219-1220.
McAuliffe, W.E., and R. Dunn (2004b). "Substance abuse treatment needs and access in the USA: Interstate variations." Addiction, 99(8): 999-1014.
McAuliffe, W.E., P. Breer, N.W. Ahmadifar, and C. Spino (1991). "Assessment of drug abuser treatment needs in Rhode Island." American Journal of Public Health, 81(3): 365-371.
McAuliffe, W.E., R. LaBrie, N. Lomuto, R. Betjemann, and E. Fournier (1999). "Measuring interstate variations in drug problems." Drug Alcohol Depend, 53(2): 125-145.
McAuliffe, W.E., R. Labrie, R. Woodworth, C. Zhang, and R.P. Dunn (2003). "State substance abuse treatment gaps." American Journal on Addictions, 12(2): 101-121.
McAuliffe, W.E., R. Woodworth, C. Zhang, and R.P. Dunn (2002). "Identifying substance abuse treatment gaps in substate areas." Journal of Substance Abuse Treatment, 23(3): 199-208.
Moher, D., A. Liberati, J. Tetzlaff, D.G. Altman, and the PRISMA Group (2009). "Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement."PLoS Med, 6(7): e1000097. doi.org/10.1371/journal.pmed.1000097.
Mullan, F., R.L. Phillips Jr., and E.L. Kinman (2004). "Geographic retrofitting: A method of community definition in community-oriented primary care practices." Fam Med, 36(6): 440-446.
National Association for State Community Services Programs (2011). A Community Action Guide to Comprehensive Community Needs Assessments.
N.E.W. Mental Health Connection (2015). Community Mental Health Needs Assessment. D. Wegge and L. Warner. Fox Cities Wisconsin, St. Norbert College Strategic Research Institute.
New Jersey Department of Children and Families (2016). Inventory and Need Assessment for New Jersey Children's Behavioral Health.
Nolin, J., S.T. Wilburn, K.T. Wilburn, and D. Weaver (2006). "Health and social service needs of older adults: Implementing a community-based needs assessment." Evaluation & Program Planning, 29(3): 217-226.
Ontario Centre of Excellence for Child and Youth Mental Health (2013). Conducting a Community Needs Assessment. http://www.excellenceforchildandyouth.ca/sites/default/files/resource/EIS_Community_Needs_Assessment.pdf.
Regier, D.A., W.E. Narrow, D.S. Rae, R.W. Manderscheid, B.Z. Locke, and F.K. Goodwin (1993). "The de facto us mental and addictive disorders service system: Epidemiologic catchment area prospective 1-year prevalence rates of disorders and services." Archives of General Psychiatry, 50(2): 85-94.
Rosenbaum, S. (2013). Principles to Consider for the Implementation of a Community Health Needs Assessment Process. George Washington University, Department of Health Policy School of Public Health and Health Services. http://nnphi.org/wp-content/uploads/2015/08/PrinciplesToConsiderForTheImplementationOfACHNAProcess_GWU_20130604.pdf.
Rowan-Szal, G.A., J.M. Greener, G.W. Joe, and D.D. Simpson (2007). "Assessing program needs and planning change." Journal of Substance Abuse Treatment, 33(2), 121-129.
Rush, B. (1990). "A systems approach to estimating the required capacity of alcohol treatment services." British Journal of Addiction, 85(1): 49-59.
Sareen, J., C.A. Henriksen, M.B. Stein, T.O. Afifi, L.M. Lix, and M.W. Enns (2013). "Common mental disorder diagnosis and need for treatment are not the same: Findings from a population-based longitudinal survey." Psychological Medicine, 43(9): 1941-1951.
Shepard, D.S., G.K. Strickler, W.E. McAuliffe, A. Beaston-Blaakman, M. Rahman, and T.E. Anderson (2005). "Unmet need for substance abuse treatment of adults in Massachusetts." Adm Policy Ment Health, 32(4): 403-426.
Skewes, M.C., and J.P. Lewis (2016). "Sobriety and alcohol use among rural Alaska Native elders." Int J Circumpolar Health, 75: 30476.
Spence, R. (2003). "Analysis model for planning chemical dependence treatment systems." Journal of Substance Abuse Treatment, 24(3): 175-181.
Spitzer, R.L. (1998). "Diagnosis and need for treatment are not the same." Archives of General Psychiatry, 55(2): 120-120.
Stefaniak, J.E., M. Mi, and N. Afonso (2015). "Triangulating perspectives: A needs assessment to develop an outreach program for vulnerable and underserved populations."Performance Improvement Quarterly, 28(1): 49-68.
Substance Abuse and Mental Health Services Administration (SAMHSA) (2013). Results from the 2012 National Survey on Drug Use and Health: Summary of National Findings. NSDUH Series H-46, HHS Publication No. (SMA) 13-4795. Rockville, MD: Substance Abuse and Mental Health Services Administration.
Substance Abuse and Mental Health Services Administration (SAMHSA) (2015). Behavioral Health Barometer: United States, 2015. HHS Publication No. SMA-16. Rockville, MD: Substance Abuse and Mental Health Services Administration.
Substance Abuse and Mental Health Services Administration (SAMHSA) (2016). Receipt of Services for Substance Use and Mental Health Issues among Adults: Results from the 2015 National Survey on Drug Use and Health. NSDUH Data Review. https://www.samhsa.gov/data/sites/default/files/NSDUH-ServiceUseAdult-2015/NSDUH-ServiceUseAdult-2015/NSDUH-ServiceUseAdult-2015.htm.
Substance Abuse and Mental Health Services Administration (SAMHSA) (2017). Key Substance Use and Mental Health Indicators in the United States: Results from the 2016 National Survey on Drug Use and Health. Rockville, MD: Center for Behavioral Health Statistics and Quality. https://www.samhsa.gov/data/.
Substance Abuse and Mental Health Services Administration (SAMHSA). (2018). Applying the Strategic Prevention Framework (SPF).
Torres, J.M., J. Lawlor, J.D. Colvin, M.R. Sills, J.L. Bettenhausen, A. Davidson, G.J. Cutler, M. Hall, and L.M. Gottlieb (2017). "ICD social codes: An underutilized resource for tracking social needs." Med Care, 55(9): 810-816.
Tweed, D.L., J.A. Ciarlo, L.A. Kirkpatrick, and D.L. Shern (1992). "V. Empirical validity of indirect mental health needs-assessment models in Colorado." Evaluation & Program Planning, 15(2): 181-194.
U.S. Government Accountability Office (GAO) (2017). OPIOID USE DISORDERS: HHS Needs Measures to Assess the Effectiveness of Efforts to Expand Access to Medication Assisted Treatment.
Watkins, R., and J.W. Altschuld (2014). "A final note about improving needs assessment research and practice." New Directions for Evaluation, (144): 105-114.
Watkins, R., and J. Kavale (2014). "Needs: Defining what you are assessing." New Directions for Evaluation, 144: 19-31.
Watkins, R., M. West Meiers, Y.L. Visser (2012). A Guide to Assessing Needs: Essential Tools for Collecting Information, Making Decisions, and Achieving Development Results. World Bank. https://openknowledge.worldbank.org/handle/10986/2231.
White, J.L., and J.W. Altschuld (2012). "Understanding the 'what should be condition' in needs assessment data." Evaluation & Program Planning, 35(1): 124-132.
WHO World Mental Health Survey Consortium (2004). "Prevalence, severity, and unmet need for treatment of mental disorders in the World Health Organization World Mental Health Surveys." JAMA, 291(21): 2581-2590.
APPENDIX B: LIST OF NEEDS ASSESSMENTS REVIEWED
Locally Initiated Needs Assessments
We reviewed the following locally initiated needs assessments:
Alaska Mental Health Trust Authority (2015). Southeast Alaska Youth Behavioral Health Gaps and Needs Assessment. Bartlett Regional Hospital service area, McDowell Group.
Alcohol Drug and Mental Health Board of Franklin County (2015).Preparing for the Future: Policy Landscape and Needs Assessment for Mental Health and Addiction Services in Franklin County. Franklin County, Ohio, Health Policy Institute of Ohio and Community Research Partners.
Bauman, M., R. Bhatta, K. Kierulf-Vieira, E. Kuller, P. Wendt, and M.Y. Yu (2017). Staten Island Needs Assessment: Opioid Addiction Prevention and Treatment Systems of Care Capstone Research Report. Columbia University, School of International and Public Affairs, Staten Island, New York.
Beck Consulting and Hornby Zeller Associates (2016). Alaska Behavioral Health Systems Assessment Final Report. Alaska Mental Health Trust Authority, Alaska Native Tribal Health Consortium, MAT-SU Health Foundation, Alaska Division of Behavioral Health, Alaska Mental Health Board, Advisory Board on Alcoholism and Drug Abuse.
California Department of Health Care Services (DHCS) (2012). California Mental Health and Substance Use System Needs Assessment, Technical Assistance Collaborative/Human Services Research Institute.
CDC Prescription Drug Overdose: Data-Driven Prevention Initiative Planning Grant (2017). South Dakota Opioid Abuse Needs Assessment, Sage Project Consultants.
Chesapeake Integrated Behavioral Healthcare (2016). Community Substance Use Needs Assessment. City of Chesapeake, Planning Council.
Chester, B., P. Mahalish, and J. Davis (2008). "Mental health needs assessment of off-reservation American Indian People in Northern Arizona." American Indian & Alaska Native Mental Health Research, 8(3): 25-40. Arizona, Native Americans for Community Action, Arizona Department of Health and Human Services.
Chontos, S. (2017). South Dakota Opioid Abuse Needs Assessment. South Dakota, Sage Consultants, South Dakota Department of Health.
Christopher, M.C., M. Jones, G. Baldwin, and E. McCance-Katz (2015). National and State Treatment Need and Capacity for Opioid Agonist Medication-Assisted Treatment. FDA, SAMHSA, et al. National and state.
City of Issaquah (2017). Community Needs Assessment for Health and Wellbeing Equity in Issaquah: A Social Determinants of Health Assessment. Issaquah, Washington, Health Resources in Action.
Cochran, B.N., K.M. Peavy, and J.S. Robohm (2007). "Do specialized services exist for LGBT individuals seeking treatment for substance misuse? A study of available treatment programs." Subst Use Misuse, 42(1): 161-176. National, University of Montana.
Delaware Department of Justice (2017). Prescription Opioid and Heroin Addiction Treatment Needs Assessment Final Report. Delaware, Hornby Zeller Associates .
Dillon, N. (n.d.). Mental Health and Substance Abuse Workforce Needs. Minnesota, Governors' Health Reform Task Force Workforce Work Group, Minnesota Department of Human Services.
District of Columbia Children and Youth Investment Trust Corporation (2011). Needs and Assets Assessment of Washington, DC Youth Executive Summary. C. B. Amanda Asgeirsson, Kristina Beall, Ninma Idowu-Fearon, Christine Iverson, Nakita Kanu, Janice Llanos-Velazquez, Reena Mathew, Briana Nord, Chelsi Stevens, Nicole Vij, Ghada Khan, Yasir Shah, John Wedeles. Washington D.C., George Washington University School of Public Health and Health Services.
Dolkar, T. (2014). Latinos in Minnesota: A Mental Health Needs Assessment. Minnesota, University of Minnesota, School of Social Work.
Englander, H., M. Weimer, R. Solotaroff, C. Nicolaidis, B. Chan, C. Velez, A. Noice, T. Hartnett, E. Blackburn, P. Barnes, P.T. Korthuis (2017). Planning and Designing the Improving Addiction Care Team (IMPACT) for Hospitalized Adults with Substance Use Disorder. Oregon regional "coordinated care organization", Oregon Health and Science University.
Greenfield, B.L., M.D. Owens, and D. Ley (2014). "Opioid use in Albuquerque, New Mexico: a needs assessment of recent changes and treatment availability." Addiction Science & Clinical Practice, 9(1): 10. Albuquerque, New Mexico, Department of Psychology and Center on Alcoholism, Substance Abuse, and Addictions, University of New Mexico.
Han, B., W.M. Compton, C. Blanco and L.J. Colpe (2017). Prevalence, Treatment, and Unmet Treatment Needs of US Adults With Mental Health and Substance Use Disorders. National, Substance Abuse Mental Health Services Administration, NIDA, et al.
Healthy Voices Healthy Choices Coalition (2017).Prescription Opioid Misuse and Heroin Use Among Youth and Young Adults in Anchorage, Alaska, Needs Assessment. Alaska, Alaska Injury Prevention Center.
Jones, E., L. Ku, S. Smith, and M. Lardiere (2014). County Workforce, Reimbursement, and Organizational Factors Associated with Behavioral Health Capacity in Health Centers. Department of Health and Human Services, Office of Economic Analysis Evaluation and Modeling, George Washington University, School of Public Health and Health Services Department of Health Policy, et al. National.
Keystone Policy Center (2017). Bridging The Divide: Addressing Colorado's Substance Use Disorder Needs. Colorado, Keystone Policy Center.
Massachusetts Department of Public Health Bureau of Substance Abuse Services (2010). The Substance Use and Addictions Workforce and Organizational Development Strategic Plan: Year 1 Results and Update. Massachusetts, DMA Health Strategies.
McAuliffe, W.E. (2004a). "Measuring treatment needs: A reply to Gfroerer, Epstein, and Wright." Addiction, 99: 1219-1220.
McAuliffe, W.E., and R. Dunn (2004b). "Substance abuse treatment needs and access in the USA: Interstate variations." Addiction, 99(8): 999-1014.
McAuliffe, W.E., P. Breer, N.W. Ahmadifar, and C. Spino (1991). "Assessment of drug abuser treatment needs in Rhode Island." American Journal of Public Health, 81(3): 365-371. Rhode Island, North Charles Foundation Department of Psychiatry, Harvard Medical School at Cambridge Hospital.
McAuliffe, W.E., R. LaBrie, N. Lomuto, R. Betjemann, and E. Fournier (1999). "Measuring interstate variations in drug problems." Drug Alcohol Depend, 53(2): 125-145.
McAuliffe, W.E., R. Labrie, R. Woodworth, C. Zhang, and R.P. Dunn (2003). "State substance abuse treatment gaps." American Journal on Addictions, 12(2): 101-121. National, Substance Abuse and Mental Health Services Administration, National Technical Center for Substance Abuse Needs Assessment, North Charles Research and Planning Group, Cambridge, Massachusetts.
McAuliffe, W.E., R. Woodworth, C. Zhang, and R.P. Dunn (2002). "Identifying substance abuse treatment gaps in substate areas." Journal of Substance Abuse Treatment, 23(3): 199-208.
N.E.W. Mental Health Connection (2015). Community Mental Health Needs Assessment. D. Wegge and L. Warner. Fox Cities Wisconsin, St. Norbert College Strategic Research Institute.
New Hampshire Bureau of Drug and Alcohol Services (2014). Substance Use Disorder Treatment and Other Service Capacity in New Hampshire. New Hampshire, New Hampshire Center for Excellence.
New Jersey Department of Children and Families (2016). Inventory and Need Assessment for New Jersey Children's Behavioral Health.
New Mexico Department of Health (n.d.). Behavioral Health Needs and Gaps in New Mexico. C. Lovelace, Presbyterian MCOs, New Mexico state-wide, Technical Assistance Collaborative, Health Services Research Institute.
North Carolina Department of Health and Human Services (DHHS) (2017). Community Needs Assessment and Gaps Analysis. Alliance Behavioral Healthcare.
North Dakota Department of Human Services, Behavioral Health Division (2016). NORTH DAKOTA Behavioral Health Assessment Gaps and Recommendations. North Dakota.
Oklahoma Department of Mental Health and Substance Abuse Services (1999). Oklahoma State Treatment Needs Assessment Studies, Alcohol and Other Drugs Study #3: Survey of Inmates, Probationers, and Parolees in the Oklahoma State Department of Corrections. Oklahoma Corrections.
Padwa, H., and B. Oeser (2013). White Paper on California Substance Use Disorder Treatment Workforce Development. UCLA Integrated Substance Abuse Programs, California Department of Health Care Services.
Rural Healthcare Program of The Leona M. and Harry B. Helmsley Charitable Trust (2015). Focus on South Dakota--A Picture of Health. South Dakota, Oregon Health & Science University (K.J. McConnell, M.M. Davis, M. Spurlock, T. Meath, D. McCarty), N. Knight-Richardson, Providence Center for Outcomes Research and Education (B. Wright, K. Dulacki, H.G. Li), North Dakota State University (D. Warne).
Saloner, B., N. Carson, B. Lê Cook (2014). Explaining Racial/Ethnic Differences in Adolescent Substance Abuse Treatment Completion in the United States. United States, Robert Wood Johnson Foundation Health and Society Scholars Program, National Institute of Mental Health.
Schumacher, A., and P. Berenbaum (2015). Local Determinants of Health in Addison County. Middlebury College Community Engagement Program, Addison County, Vermont, Middlebury College.
Shasta Health Assessment and Redesign Collaborative (2015). Behavioral Health Needs Assessment and Gap Analysis Report. Health Alliance of Northern California.
Shepard, D.S., G.K. Strickler, W.E. McAuliffe, A. Beaston-Blaakman, M. Rahman, and T.E. Anderson (2005). "Unmet need for substance abuse treatment of adults in Massachusetts." Adm Policy Ment Health, 32(4): 403-426. Massachusetts, Heller School for Social Policy and Management, Department of Psychiatry at Harvard Medical School, Massachusetts Department of Public Health.
Siskiyou Health Care Collaborative (2015). Siskiyou County Behavioral Health Needs and Community Capacity Assessment With Implementation Plan. County, Siskiyou Health Care Collaborative Behavioral Health Task Group.
Substance Abuse Mental Health Services Administration (2009). Needs Assessment and Resource Inventory. Missouri Institute of Mental Health, Mental Health Transformation State Incentive Grant (MHT-SIG) Missouri.
Utah Division of Substance Abuse and Mental Health (n.d.). Utah Prevention by Design Needs Assessment. Utah, National Alliance on Mental Health Utah.
Virginia Commonwealth University, Department of Rehabilitation Counseling (2007). The Accessibility of Substance Abuse Treatment Facilities in the United States for Persons with Disabilities. S.L. West. National.
Washington/Baltimore High Intensity Drug Trafficking Area (2015). Heroin Treatment Needs Assessment for Berkeley County, West Virginia. Berkely Countyy, West Virginia.
West, S.L. (2007). "The accessibility of substance abuse treatment facilities in the United States for persons with disabilities." J Subst Abuse Treat, 33(1): 1-5.
APPENDIX C: FEDERAL DATA SOURCES
Because of the widespread use of federal data sources in SUD needs assessment, it is important to have an understanding of their characteristics and limitations. The following is an overview of the most frequently used data sources.
Substance Abuse and Mental Health Services Administration Data Sources
SAMHSA has several resources that are widely utilized in needs assessments. These include the NSDUH, the N-SSATS, the National Mental Health Services Survey (N-MHSS), the TEDS, Behavioral Health Barometer, Behavioral Health Treatment Services Locator, Buprenorphine Treatment Practitioner Locator, OTP Directory, and the Emergency Department Data.
Many of these data sources are maintained by the Center for Behavioral Health Statistics and Quality as part of the Behavioral Health Services Information System (BHSIS), though data collection for some of these data sources is contracted out (e.g., NSDUH is contracted to RTI International). The purpose of BHSIS, which was formerly known as the Drug and Alcohol Services Information System, is the operation of an integrated statistical data system that provides information at the national, state, and local levels on the facilities and services available for substance abuse and mental health treatment in the United States, and the characteristics of the people admitted to the treatment facilities.
The National Survey on Drug Use and Health (NSDUH), which has been conducted since 1971, is considered the primary data source of information on the prevalence, patterns, and consequences of alcohol, tobacco, and illegal drug use and abuse and mental disorders in the United States civilian, non-institutionalized population, age 12 and older. Data is collected from persons who are residing in households, non-institutionalized group quarters (e.g., shelters, rooming houses, and dormitories) and civilians living on military bases. The annual survey generates estimates at the national, state, and sub-state levels.
The NSDUH utilizes a stratified multi-stage area probability sample that is designed to be representative of the United States and each of the 50 states and the District of Columbia. It is implemented using a coordinated sample design that is state-based, with an independent, multi-stage area probability sample within each state and the District of Columbia. As a result, states are viewed as the first level of stratification and as a variable for reporting estimates; then each state is stratified into approximately equally populated state sampling regions (SSRs) and selected within each SSRs are census block groups, dwelling units and within dwelling units up to two residents for the interviews. Results of the NSDUH are available as the Published NSDUH, which provides estimates at the state and sub-state levels produced using small area estimation methods and by pooling multiple years of data.[12] For state-level estimates, two years of data are combined; for sub-state estimates, three years of data are combined.
The NSDUH has several limitations for purposes of needs assessment:
-
The design and methodology of the NSDUH have been modified in various ways over the years, which may impact the comparability of estimates from surveys collected in different time periods.
-
NSDUH is a household survey that relies on the sampled respondents to provide accurate and honest reports of their substance use and substance use treatment experiences.
-
The sample excludes active duty military members and persons who do not live in households (homeless persons not in shelters and persons in institutions such as jails or prisons, hospitals, or residential treatment facilities) during most of the quarter of the year in which they were interviewed.
-
To protect confidentiality, the Public Use Files of the NSDUH do not include geographic identifier; therefore, these files cannot be utilized to provide estimates at the region, state or sub-state levels or to produce related analyses. Estimates also cannot be obtained for variables that were stripped due to disclosure reasons.
The National Survey of Substance Abuse Treatment Services (N-SSATS) is an annual census of all public and private substance abuse treatment facilities in the United States. Participation in the N-SSATS is voluntary but the incentive for participation is the opportunity to be included in SAMHSA's online Behavioral Health Treatment Services Locator (discussed below). The information is collected at the site of delivery of services rather than from administrative entities such as licensing boards.
The N-SSATS collects data on: (1) characteristics of individual facilities such as services offered and types of treatment provided, and payment options; (2) client count information such as counts of clients served by service; (3) information regarding hospital and residential capacity, the number of treatment admissions in the past 12 months and a single-day client census; (4) the number of facilities that provide medication-assisted treatment (MAT) with methadone, buprenorphine, and/or naltrexone and the number of clients that receive these medications; and (5) general information such as licensure, certification, or accreditation and facility website availability. Information is collected from all 50 states, the District of Columbia, Puerto Rico, the Federated States of Micronesia, Guam, Palau, and the Virgin Islands.
Primary limitations of the N-SSATS for purposes of SUD treatment needs assessments are that it does not include data from private physicians who are not affiliated with a substance abuse treatment program or facility, and it excludes jails, prisons, or other correctional facilities that exclusively treat incarcerated clients.
The National Mental Health Services Survey (N-MHSS) is an annual survey of all known public and private mental health treatment facilities in the United States. Data is collected from facilities within the 50 states, the District of Columbia, and the U.S. territories. The surveys are forwarded to facilities included in the Behavioral Health Treatment Services Locator.
The annual surveys collect statistical information on the numbers and characteristics of known mental health treatment facilities. Beginning in 2014, every other year, data is also collected on the number and demographic characteristics of persons served in the treatment facilities as of specified survey reference date. The N-MHSS includes: public psychiatric hospitals; private psychiatric hospitals, non-federal general hospitals with separate psychiatric units; U.S. Department of Veterans Affairs (VA) medical centers; residential treatment centers for children; residential treatment centers for adults; outpatient or day treatment or partial hospitalization mental health facilities; and multi-setting (non-hospital) mental health facilities.
Like the N-SSATS, participation in the survey is voluntary and provides the opportunity to be included in the Behavioral Health Treatment Services Locator (discussed below). Data is collected via a secure web-based questionnaire, a paper questionnaire sent by mail, and a computer-assisted telephone interviewing.
The N-MHSS has the following limitations:
-
It excludes U.S. Department of Defense military treatment facilities, individual private practitioners or small group practices not licensed as a mental health clinic or center, and jails or prisons.
-
It excludes facilities that only provide any of the following services: crisis intervention services, psychosocial rehabilitation, cognitive rehabilitation, intake, referral, mental health evaluation, health promotion, psychoeducational services, transportation services, respite services, consumer-run/peer support services, housing services, and legal advocacy.
-
It excludes residential facilities whose primary function is other than specialty mental health treatment services.
The Treatment Episode Data Set (TEDS) a cooperative program between SAMHSA and state substance abuse agencies to collect data on substance use treatment services. TEDS was developed as a response to the 1988 Comprehensive Alcohol Abuse, Drug Abuse, and Mental Health Amendments (P.L. 100-690), which established a revised SAPTBG and mandated federal data collection on clients receiving treatment for either alcohol or drug abuse.
TEDS collects data on the demographic and substance abuse characteristics of admissions to and discharges from substance abuse treatment for persons aged 12 and older. State laws require certain substance abuse treatment programs to report all their admissions and discharges to the state. In all states, treatment programs receiving any public funds are required to provide the data on both publicly and privately funded clients, and in some states, programs that do not receive public funds are required to provide data as well. Data are reported by approximately 10,000 facilities, programs, or administrative units in the 50 states, the District of Columbia, and Puerto Rico. Admission and discharge data are collected.
The following are limitations of the TEDS:
-
The facilities that report TEDS data are primarily those that receive State alcohol and/or drug agency funds for the provision of drug or alcohol services. Facilities that are often not included are those that do not receive funding through the Single State Authority, Indian Health Service facilities, or hospital-based programs.
-
VA and military treatment facilities are excluded.
-
Correctional facilities (state prisons and local jails) report TEDS data in some states but not in others.
-
There are state-level differences in the reporting of TEDS data. For example, some states only require facilities to report TEDS data for patients for whom treatment is publicly funded.
-
TEDS data represent admissions to or discharges from substance use treatment, not individuals. So, an individual admitted to treatment twice in a calendar year would be counted as two separate admissions. However, admission and discharge data from the TEDS can be combined using unique identifiers to estimate unique numbers of persons admitted to treatment.
-
Most of the data collected is self-reported by persons admitted for treatment; the recall of certain data (e.g., prior treatment or substances used) may be different depending on the saliency of the topic and the differences in the context within which the data are being collected.
The Behavioral Health Barometer provides state and national reports that provide a snapshot of behavioral health in the nation. Presented are data from SAMHSA data sources (NSDUH and N-SSATS) as well as other federal partners such as the CDC (the Youth Risk Behavior Surveillance System), and the National Institute on Drug Abuse (the Monitoring the Future survey). The reports also include data on the use of mental health and substance use treatment services by Medicare enrollees, as reported by the CMS.
The Behavioral Health Treatment Services Locator is updated annually using data from the N-SSATS and N-MHSS. The locator provides information for those seeking treatment facilities in the United States or U.S. territories for substance abuse/addiction and/or mental health problems. The locator is available at https://findtreatment.samhsa.gov/.
The Buprenorphine Treatment Practitioner Locator can be utilized to identify physicians who are certified to provide buprenorphine treatment to treat opioid addiction (e.g., heroin or prescription pain relievers) in a city, state, or zip code. The locator provides the provider's name, degree (i.e., medical doctor, nurse practitioner), and contact information (address and phone number). This locator is available at https://www.samhsa.gov/medication-assisted-treatment/physician-program-data/treatment-physician-locator.
The Opioid Treatment Program Directory can be used to find treatment programs that treat opioid addiction and dependence. The directory can be searched by state and provides the program names and contact information (address, phone and location on a map). This directory is located at http://dpt2.samhsa.gov/treatment/directory.aspx.
Emergency Department Data. Until 2011, SAMHSA collected data through the Drug Abuse Warning Network (DAWN), which was a public health surveillance system that monitored drug-related hospital emergency department visits to report on the impact of drug use, misuse, and abuse in metropolitan areas and across the nation. In its final year, DAWN collected data from metropolitan areas in 37 states (with complete coverage of 13 states) and covered one-third of the United States population. SAMHSA is re-establishing DAWN and data abstraction will begin in mid-2019.
DAWN produced annual estimates of drug-related visits to hospital emergency departments for the nation and for selected metropolitan areas. The 2011 data is available at https://www.samhsa.gov/data/emergency-department-data-dawn/reports.
SAMHSA is currently working with the National Center on Health Statistics on its new National Hospital Care Survey (NHCS). Through the NHCS, SAMHSA will receive data on drug-related emergency department visits and will publish them as SAMHSA's Emergency Department Surveillance System.
The primary limitation of the DAWN is that data from different times periods are not comparable due to changes in design and methodology.
Centers for Disease Control and Prevention Data Sources
CDC had several resources that are utilized in needs assessments. Two sources widely used in SUD needs assessments are the Behavioral Risk Factor Surveillance System (BRFSS) and the National Center for Health Statistics (NCHS).
The Behavioral Risk Factor Surveillance System (BRFSS) is a telephone survey that collects state-level data about United States residents regarding their health-related risk behaviors, chronic health conditions, and use of preventive services. The BRFSS was established in 1984 and now collects data in all 50 states, the District of Columbia and three U.S. territories. BRFSS completes more than 400,000 adult interviews per year. The BRFSS is considered a powerful tool for targeting and building health promotion activities.
The BRFSS is conducted by state health departments, who either use in-house interviewers or contract with telephone call centers or universities to administer the surveys continuously through the year. The states use a standardized core questionnaire, optional modules, and state-added questions. Annual BRFSS data can be downloaded at https://www.cdc.gov/brfss/annual_data/annual_data.htm. BRFSS prevalence data and topic specific data can be viewed at: https://www.cdc.gov/brfss/brfssprevalence/index.html.
National Center for Health Statistics (NCHS)
NCHS is the principal health statistics agency in the United States. Its mission is to provide statistical information that will guide actions and policies to improve the health of the American people. NCHS addresses the full spectrum of concerns in the health field from birth to death, including overall health status, lifestyle and exposure to unhealthful influences, the onset and diagnosis of illness and disability, and the use and financing of health care and rehabilitation services.
The NCHS provides data from various sources including population surveys (e.g., National Health Interview Survey), vital statistics (e.g., National Vital Statistics System), provider surveys, and historical surveys.[13] The NCHS website provides publicly-available data that can be downloaded for analysis.
U.S. Census Bureau
Many needs assessments utilize data that is available from the U.S. Census Bureau such as the 2010 Census Data or the American Community Survey to describe population within states, census tracks or other and in some cases to compare that community to populations in other communities or states.
Bureau of Labor Statistics (BLS)
BLS data are widely used by needs assessments, especially those that address workforce issues. While the BLS is the primary source for estimates of future workforce demands, it is limited for purposes of SUD treatment needs assessments by the fact that it is occupational categories do not correspond well to classifications of the SUD workforce in sources such as licensing boards and scope of practice policies that are used for assessing current capacity.
Healthy People 2020
For the last three decades, Healthy People has provided ten-year national objectives for improving the health of all Americans. Healthy People 2020 was launched in December 2010 and has over 1,200 objectives to monitor and improve the health of Americans over the decade. The objectives are organized into 42 topic areas. DATA 2020 is an interactive tool that is available within the Office of Disease Prevention and Health Promotion which allows users to explore data and technical information related to Healthy People 2020 objectives. Many data sources are included within Data 2020 and can be explored at http://www.healthypeople.gov/2020/data-search/Data-Sources.
Data 2020 can be searched by topic (e.g., access to health services, health-related quality of life and well-being, mental health and mental disorders, substance abuse) and data source, and several of the needs assessments reviewed utilize this resource.
APPENDIX D: QUALITY RATING TABLES
| Quality Assessment Areas | Number of Reports |
|---|---|
| Questions (purposes) specified | |
| Yes | 29 |
| Partial | 2 |
| No | 2 |
| Questions clearly addressed | |
| Yes | 24 |
| Partial | 5 |
| No | 0 |
| Methods for defining the population described | |
| Yes | 26 |
| Partial | 5 |
| No | 2 |
| Selection criteria for workers specified | |
| Yes | 9 |
| Partial | 1 |
| No | 6 |
| Not applicable | 6 |
| Setting well defined | |
| Yes | 28 |
| Partial | 4 |
| No | 0 |
| Levels of care identified | |
| Yes | 16 |
| Partial | 6 |
| No | 9 |
| Survey: Random sampling | |
| Yes | 6 |
| No | 11 |
| Unknown/unclear | 7 |
| Survey: Instrument reliability and validity reported | |
| Yes | 3 |
| No | 18 |
| Survey: Pilot testing of the instrument reported | |
| Yes | 3 |
| No | 17 |
| Statistical methods described | |
| Yes | 15 |
| No | 12 |
| Unknown/unclear | 4 |
| Stratification used in the analysis | |
| Yes | 3 |
| No | 7 |
| Unknown/unclear | 5 |
| Limitations due to data unavailability or quality reported | |
| Yes | 22 |
| No | 9 |
| Validation of the methodology reported | |
| Yes | 3 |
| No | 27 |
| Model system for gap comparison presented | |
| Yes | 15 |
| No | 15 |
| Recommendations offered | |
| Yes | 29 |
| No | 5 |
| Recommendation feasibility, priorities or strategies | |
| Yes | 20 |
| No | 10 |
| Not Applicable (no recommendations offered) | 4 |
| Ethical issues addressed | |
| Yes | 5 |
| No | 27 |
| IRB approved | |
| Yes | 5 |
| No | 7 |
| Unknown/unclear | 19 |
| How capacity was measured | |
| Inventory (number of providers, beds, slots, etc.) | 8 |
| Utilization data | 4 |
| Consumer self-report (access, availability) | 3 |
| Key informants | 6 |
| Surveys | 4 |
| Unknown/unclear | 1 |
| Operational definition of "need" provided | |
| Yes prevalence-unmet need gap | 3 |
| Yes-other describe: | 8 |
| No | 5 |
| Partial | 0 |
APPENDIX E: DATA EXTRACTION FORM
ASPE Network Capacity for Substance Use Disorder Needs Assessment Data Extraction Form
Coder:
Date Completed:
Module A: Coding of Content
Section A: Document Information
- Document Title: (e.g., Report Title or Article Title)
- Source Title: (e.g., Journal title or Book Title)
- Document Publication Year:
- Contractor(s) Conducting Needs Assessment:
- Funder(s) of Needs Assessment:
Purpose/Focus of Report: (include a short description)
NOTES:
Section A: Questions/Issues Explored
-
What topics are explored in the questions/issues? (Check all that are applicable) Note: Should include only items that are included in the assessment of the current system, not things that are discussed in a general way, such as in the background section. For example, "Research has demonstrated significant health disparities for individuals with mental illness and substance use and there is growing evidence of shortened lifespans" we would not check "disparities" unless disparities were assessed in the current system.
___Prevalence/frequency related to: (Check all that are applicable)
___General substance use
___Alcohol
___Opioids
___Heroin
___Methamphetamine
___Marijuana
___Cocaine
___Depression
___Suicide
___Overdose
___Co-Occurring Disorders (CODs)
___Medical Co-morbidity
___Other prevalence/frequency, describe:
___Other prevalence/frequency, describe:
___Unmet need (other than prevalence)
___Utilization/Penetration
___Demand (services likely to be requested)
___Referrals
___Means of Obtainment (how drugs are obtained)
___Risk Factors
___Expenditures/costs/cost benefit
___Funding sources
___Workforce supply
___Workforce competency/training
___Workforce licensing/certification
___Peer involvement
___Provider organization supply/capacity
___Collaboration
___Law enforcement
___Leadership
___Special populations
___Disparities
___Diagnostic group differences
___Regional variation
___Demographic trends
___Cultural competency
___Benchmarks for future progress
___Behavioral health integration
___High utilizers
___Quality (Check all that are applicable)
___Access (capacity, wait-times, etc.)
___Availability/Network adequacy (existence of services)
___Outpatient follow-up
___Outcomes
___Treatment completion/adherence
___Satisfaction/perception of care
___Other quality describe:
___Other quality describe:
___Evidence-Based Practices (EBPs)
___Stigma
___Transitions by functional level
___Benefit design/coverage
___Policy changes
___Technology (Check all that are applicable)
___Data systems
___Use of HIT
___Use of EMRs
___Use of Telehealth
___Use of e-prescribing
___Interoperability among provider organizations
___Interoperability among public agencies
___Privacy/confidentiality issues
___Other technology issue describe:
___Other technology issue describe:
___Barriers/limitations (Check all that are applicable)
___Policies
___MH/SUD bifurcation
___Other agency silos
___Decentralized (e.g., county) systems
___Service locations
___Service costs
___Lack of access, NOS
___Qualified workforce
___Provider reimbursement limitations
___Stigma
___Other barriers/limitations, describe:
___Other barriers/limitations, describe:
___Quality/performance measurement systems
___System assets/strengths
___Other, describe:
___Other, describe:
___Not specified/identified
NOTES:
Section B: Location
-
What is the geographical boundary? (Choose only one)
___United States (U.S.)
___County/countries outside of U.S. (If yes, specify):
___Region(s) (If yes, specify):
___State(s) (If yes, specify):
___County(ies) within state(s) (If yes, specify):
___City(ies) (If yes, specify):
___Zip Code(s) (If yes, specify):
___Tribe(s)/Tribal Community(ies) (If yes, specify):
___Other, describe:
___Other, describe:
___Not specified/identified
NOTES:
-
Is there a focus on a specific type of region? (Choose only one)
___Urban
___Suburban
___Rural
___Frontier
___No specific regional focus (e.g., focused on a county or state)
___Not specified/identified
NOTES:
Section C: Data Sources/Methods
-
What data sources/methods were utilized? (Check all that are applicable)
___SAMHSA National Directory of Drug and Alcohol Abuse Treatment Facilities
___SAMHSA NSDUH
___BRFSS
___Youth Risk Behavior Surveillance System (YRBSS)
___SAMHSA TEDS
___SAMHSA Behavioral Health Barometer
___SAMHSA Buprenorphine Treatment Practitioner Locator
___SAMHSA N-SSATS
___SAMHSA N-MHSS
___SAMHSA Emergency Department Data
___U.S. Census Data
___Bureau of Labor Statistics (BLS)
___Centers for Disease Control and Prevention (CDC) Data
___State Management Information System (MIS)
___State health database (including Medicaid enrollment)
___Licensing boards
___Healthy People 2020
___County/City MIS
___County/City Health database
___Provider MIS
___Medical Record/EHR
___Medicaid claims
___Medicare claims
___Existing reports/studies
___Surveys with: (Check all that are applicable)
___State/local agency leadership/staff
___Legislators
___Provider organization leadership
___Practitioner/workers
___Peer organizations
___Advocacy organizations
___Consumers/patients
___Family members
___General Public
___Other surveys with, describe:
___Other surveys with, describe:
___Focus groups with: (Check all that are applicable)
___State/local agency leadership/staff
___Legislators
___Provider organization leadership
___Practitioner/workers
___Peer organizations
___Advocacy organizations
___Consumers/patients
___Family members
___Other focus groups with, describe:
___Other focus groups with, describe:
___Key informant interviews with: (Check all that are applicable)
___State/local agency leadership/staff
___Legislators
___Provider organization leadership
___Practitioner/workers
___Peer organizations
___Advocacy organizations
___Consumers/patients
___Family members
___Other key informant interviews with, describe:
___Other key informant interviews with, describe:
___Meetings
___Community/public
___State/local agency leadership/staff
___Legislators
___Provider organization leadership
___Practitioner/workers
___Peer organizations
___Advocacy organizations
___Consumers/patients
___Family members
___Steering committee
___State/local agency leadership/staff
___Legislators
___Provider organization leadership
___Practitioner/workers
___Peer organizations
___Advocacy organizations
___Consumers/patients
___Family members
___Other steering committee members, describe:
___Other steering committee members, describe:
___Document review
___Other, describe:
___Other, describe:
___Not specified/identified
NOTES:
Section D: Data Limitations Noted
-
What data limitations were noted? (Check all that are applicable)
___Claims: Emergency Department Utilization by non-Medicaid
___Other claims limitations
___Omitted persons not residing in households (e.g., unsheltered homeless)
___State system lack integration/common identifiers
___Providers reimbursed by multiple payers
___Non-billing services (drop in centers, warm lines, etc.)
___Other, describe:
___Other, describe:
___Not specified/identified
NOTES:
Section E: Populations/Groups
-
What are the populations/groups of focus? (Check all that are addressed)
___Substance use disorder (SUD) (Please specify)
___Substance use unspecified
___Alcohol
___Poly drug use
___Needle use
___Opioids
___Prescription drugs
___Heroin
___Methamphetamines
___Marijuana
___Cocaine
___Hallucinogens
___Other substance use disorder, specify:
___Other substance use disorder, specify:
___Mental health
___Co-occurring disorders (CODs) (mental illness and substance use disorders)
___HIV/AIDS
___Children/adolescents
___Transition-age youth
___Adults
___Older adults
___Racial/ethnic groups (If yes, specify groups):
___Lesbian, gay, bisexual, or transgender individuals, questioning and allies (LGBT/LGBTQA)
___Gender
___Income
___Marital Status
___Homeless
___Veterans
___Adults criminal justice system
___Youth juvenile justice system
___Child/youth child welfare
___Other (specify):
___Other (specify):
___Not described/specified
NOTES:
Section F: Workforce Characteristics and Supply
-
What are the workforce categories of focus? (Check all that are addressed)
___Psychiatrists (Check all that apply)
___Addiction
___Other psychiatrists, describe:
___Physicians (non-psychiatrist)
___Licensed buprenorphine physicians
___Other physicians, describe:
___Nurses (Check all that apply)
___Licensed Practical Nurses/Licensed Vocational Nurses
___Registered Nurse (Diploma, Associate's, and Baccalaureate)
___Psychiatric and Mental Health Nurses
___Advanced Practice Registered Nurses (Master's and Doctoral)
___Nurse Practitioner
___Other nurses, describe:
___Physician Assistant
___Psychologists
___Social Workers (Check all that apply)
___Associate's and Baccalaureate
___Masters
___Clinical
___Counselors (Check all that apply)
___Rehabilitation Counseling
___Addiction Counseling
___Clinical Mental Health Counseling
___Other counselors, describe:
___Peers
___Other, describe:
___Other, describe:
___Not specified/identified
NOTES:
-
Are workforce pay sources specified? (Check all that are addressed)
___Medicaid
___Medicare
___Private insurance
___State funds
___Charity/free care
___Other, describe:
___Other, describe:
___Not specified/identified
NOTES:
-
Is the geographic distribution of the workforce reported?
___By state
___By county across the state
___By urban/rural
___Other geographical classification describe:
___Not reported
NOTES:
-
What workforce characteristics are reported?
___Racial/ethnic composition
___Competencies/training
___Certification
___Licensing
___Other, describe:
___Other, describe:
___Not specified/identified
NOTES:
Section G: Provider Organization and Service Type
-
What types of facilities or organization types are addressed? (Check all that are addressed)
___Community Health Centers (CHC)
___Federally Qualified Health Centers (FQHC)
___Community Mental Health Center (CMHC)
___Health Care for the Homeless agency
___Hospital or Medical Center
___Private psychiatric hospital inpatient
___Private psychiatric hospital outpatient
___Public psychiatric hospital (acute care)
___Public psychiatric hospital (long term care)
___Academic Medical Center
___Substance use (only) agency
___Opioid Treatment Program (OTP)
___Mental health/substance use agency
___Veteran Administration (VA) agency or facility
___Accountable Care Organizations (ACO)
___Health Homes
___Primary care clinics
___Drug/mental health courts
___Social service agency
___Consumer-run agency
___Shelter or temporary housing resources (e.g., Sober Living, Halfway Homes, etc.).
___Other housing agencies
___Jail/Prison
___Private practice
___Other, describe:
___Other, describe:
___Not specified/identified
NOTES:
-
What types of service settings are addressed? (Check all that are addressed)
___Hospital (Check all that are addressed)
___General hospital
___Emergency room
___Veteran Administration (VA) hospital
___Hospital detoxification
___Psychiatric hospital
___Psychiatric unit within a general hospital
___Hospital outpatient
___Other hospital, describe:
___Outpatient (Check all that are addressed)
___Outpatient detoxification
___Outpatient SUD treatment
___Outpatient methadone/buprenorphine or naltrexone treatment
___Outpatient MH treatment
___Outpatient day treatment or partial hospitalization
___Intensive outpatient treatment
___Outpatient VA
___Other outpatient, describe:
___Residential
___Residential detoxification
___Residential SUD treatment
___Residential MH treatment
___Other residential, describe:
___Inpatient
___Inpatient detoxification
___Inpatient SUD treatment
___Inpatient MH treatment
___Other inpatient, describe:
___Other, describe:
___Other, describe:
___Not specified/identified
NOTES:
Section H: Services/Level of Care
-
Are ASAM levels specifically addressed?
___Yes
___No (skip to 3)
NOTES:
-
If yes, what ASAM Level are addressed? (Check all that are addressed)
___Level of Care 0.5: Early Intervention for Adults and Adolescents
___Level of Care 1: Outpatient Services for Adolescents and Adults
___Level of Care 2: Intensive Outpatient/Partial Hospitalization Services
___Level of Care 2.1: Intensive Outpatient Services for Adolescents and Adults
___Level of Care 2.5: Partial Hospitalizations for Adolescents and Adults
___Level of Care 3.1: Clinically Managed Low-Intensity Residential Services for Adolescents and Adults
___Level of Care 3.3: Clinically Managed Population-Specific High-Intensity Residential Services for Adults
___Level of Care 3.5: Clinically Managed Medium-Intensity Residential Services for Adolescents and Clinically Managed High-Intensity Residential Services for Adults
___Level of Care 3.7: Medically Monitored High-Intensity Inpatient Services for Adolescents and Medically Monitored Intensive Inpatient Services Withdrawal Management for Adults
___Level of Care 4: Medically Managed Intensive Inpatient Services for Adolescents and Adults
NOTES:
-
What services/treatment modalities are addressed? (Check all that are addressed)
___Substance abuse treatment services (Check all that apply)
___Inpatient treatment
___Outpatient treatment
___Individual treatment
___Group treatment
___Family treatment
___Residential treatment
___Day treatment
___Crisis/emergency services
___Support services
___Education/risk reduction/screening
___Prevention
___Medication-assisted treatment (e.g., methadone, buprenorphine, etc.)
___Detoxification
___Rehabilitation
___Intensive home based treatment (SAMHSA Good and modern)
___Consultation to caregivers (SAMHSA Good and modern)
___Outreach/engagement SAMHSA Good and modern)
___Aftercare (hospital, residential, outpatient, etc.)
___Self-help/faith-based
___Other substance abuse treatment services, describe:
___Mental health treatment services--check all that apply
___Psychotherapy/counseling
___Medication management
___Peer support/consumer operated services
___Psychosocial (e.g., supported employment, case management)
___School-based services
___General health services
___Housing
___Financial
___Transportation
___Legal
___Testing (e.g., Hep C, HIV, STD)
___Needle exchange
___Condoms
___Other, describe:
___Other, describe:
___Not specified/identified
NOTES:
Section I: Funding
-
What payor sources were included in the needs assessment? (Check all that are applicable)
___Medicaid
___Medicare
___Dually Eligible
___State financed insurance (other than Medicaid)
___Community Mental Health Service Block Grant (MHBG) Funds
___Substance Abuse Prevention or Treatment Block Grant (SAPTBG) Funds
___State Mental Health Agency (or Equivalent) Funds
___State Substance Abuse Agency (or Equivalent) Funds
___County or Local Government Funds
___Access to Recovery (ATR) vouchers
___Private Insurance/Fee for Pay
___Private Insurance/HMO
___Military Insurance (VA, TRICARE)
___Indian Health Services
___Uninsured
___Cash or self-payment
___Other, describe:
___Other, describe:
___None specified/included
NOTES:
Module B: Coding for Quality
-
Are the questions (purposes) of the needs assessment clearly specified? (Research Question 4 and 9)
___Yes
___Partial
___No
NOTES:
-
Are the methods for defining the population described? (Research Question 2a)
___Yes
___Partial
___No
NOTES:
-
Are the selection criteria for workers specified? (Research Question 2b)
___Yes
___Partial
___No
NOTES:
-
Is the setting (geographical area, service area) well defined for the purpose? (Research Question 2c)
___Yes
___Partial
___No
NOTES:
-
Are the levels of care identified in the utilization assessment? (Research Question 2d)
___Yes
___Partial
___No
NOTES:
-
[If surveys were conducted] Was random sampling used?
___Yes
___No
___Unknown/unclear
NOTES:
-
[If surveys were conducted] Is the instrument reliability and validity reported?
___Yes
___No
NOTES:
-
[If surveys were conducted] Is pilot testing of the instrument reported?
___Yes
___No
NOTES:
-
Were statistical methods described?
___Yes
___No
___Unknown/unclear
NOTES:
-
Are limitations due to data unavailability or quality reported? (Research Question 12)
___Yes
___No
NOTES:
-
Is validation of the methodology reported? (Research Question 13)
___Yes
___No
NOTES:
-
Does the report include a model system for gap comparison ("what should be")?
___Yes
___No
NOTES:
-
Does the report include recommendations?
___Yes
___No
NOTES:
-
Are recommendation feasibility, priorities or strategies discussed?
___Yes
___No
___Not Applicable (no recommendations offered)
NOTES:
-
Were ethical issues addressed in the needs assessment?
___Yes
___No
NOTES:
-
Was the needs assessment approved by an IRB?
___Yes
___No
___Unknown/unclear
-
How was capacity measured?
___Inventory (number of providers, beds, slots, etc.)
___Utilization data
___Consumer Self-report (access, availability)
___Key informants
___Unknown/unclear
NOTES:
-
Was stratification used in the analysis?
___Yes
___No
___Unknown/unclear
NOTES:
-
Is an operational definition of "need" provided?
___Yes Prevalence-unmeet need gap
___Yes-Other Describe:
___No
___Partial
NOTES:
Best Practices Notes:
Write notes on anything that looks good from the report.
NOTES
-
See https://www.samhsa.gov/sites/default/files/grants/fy18-19-block-grant-application.pdf.
-
See https://aspe.hhs.gov/basic-report/needs-assessment-methodologies-determining-treatment-capacity-substance-use-disorders-final-report.
-
See https://aspe.hhs.gov/basic-report/needs-assessment-methodologies-determining-treatment-capacity-substance-use-disorders-final-report.
-
See https://www.kff.org/report-section/an-overview-of-delivery-system-reform-incentive-payment-waivers-issue-brief/.
-
See https://aspe.hhs.gov/basic-report/needs-assessment-methodologies-determining-treatment-capacity-substance-use-disorders-final-report.
-
See https://aspe.hhs.gov/basic-report/needs-assessment-methodologies-determining-treatment-capacity-substance-use-disorders-final-report.
-
See https://www.samhsa.gov/data/population-data-nsduh/reports?tab=38.
PROJECT AND REPORT INFORMATION
Network Capacity for Substance Use Disorder Treatment
This report was prepared under contract #HHSP233201600015I between HHS's ASPE/DALTCP and the Human Services Research Institute. For additional information about this subject, you can visit the DALTCP home page at https://aspe.hhs.gov/office-disability-aging-and-long-term-care-policy-daltcp or contact the ASPE Project Officer, Judith Dey, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. Her e-mail address is: Judith.Dey@hhs.gov.
Reports Available
Needs Assessment Methodologies in Determining Treatment Capacity for Substance Use Disorders: Final Report
- HTML https://aspe.hhs.gov/basic-report/needs-assessment-methodologies-determining-treatment-capacity-substance-use-disorders-final-report
- PDF https://aspe.hhs.gov/pdf-report/needs-assessment-methodologies-determining-treatment-capacity-substance-use-disorders-final-report
Needs Assessment Methodologies in Determining Treatment Capacity for Substance Use Disorders: Environmental Scan Final Report
- HTML https://aspe.hhs.gov/report/needs-assessment-methodologies-determining-treatment-capacity-substance-use-disorders-environmental-scan-final-report
- PDF https://aspe.hhs.gov/pdf-report/needs-assessment-methodologies-determining-treatment-capacity-substance-use-disorders-environmental-scan-final-report