
Link to Printer Friendly Version in PDF Format (5 PDF pages)
ABSTRACT: The COVID-19 pandemic has affected home care agencies--including home health agencies--and their staff in several important ways. Some of the challenges encountered were entirely new and resulted directly from the pandemic. In other cases, the pandemic worsened long-standing challenges in the industry. States and the federal government addressed some of these issues through changes to policies, regulations, and guidance. Home care agencies also responded with changes to their own policies and practices. The purpose of this study was to understand the challenges faced by home care (including home health) agencies due to the COVID-19 pandemic and the policies and practices put into place by the federal government, state governments, and home care agencies themselves to mitigate these challenges through a 50-state scan and interviews with stakeholders. This brief summarizes findings related to state and federal policy changes implemented due to COVID.
This report was prepared under contract #HHSP233201500039I between HHS's ASPE/BHDAP and RTI International. For additional information about this subject, you can visit the BHDAP home page at https://aspe.hhs.gov/bhdap or contact the ASPE Project Officers, at HHS/ASPE/BHDAP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201; Judith.Dey@hhs.gov, William.Haltermann@hhs.gov, Iara.Oliveira@hhs.gov, Marie.Squillace@hhs.gov.
DISCLAIMER: The opinions and views expressed in this report are those of the authors. They do not reflect the views of the Department of Health and Human Services, the contractor or any other funding organization. This report was completed and submitted on March 2, 2021.
BACKGROUND
Home care (including home health) agencies and their staff have experienced many challenges during the COVID-19 pandemic. These agencies provide services and supports that help individuals remain safely in their homes. The pandemic initially decreased access to these services because clients were hesitant to have workers in their homes and workers were fearful of either contracting or spreading the infection. New temporary federal and state policies implemented during the pandemic were intended to protect workers from infection by increasing available funds for personal protective equipment (PPE), increasing remote access to services, and compensating workers who were most at risk of contracting COVID-19. This brief explores the key policy changes affecting home care agency workers identified by a 50-state scan and interviews with stakeholders.
FINDINGS
Disaster relief funding. Advocates and providers highlighted the federal assistance provided by disaster relief funding such as the Paycheck Protection Program (PPP) and the Families First Coronavirus Response Act, which went directly to agencies and enabled them to pay workers bonuses, pay for childcare, and provide leave when needed. However, several advocates -- representing a large number of agencies -- noted that some providers were wary to use the funds because of shifting federal and state guidelines. Private-pay only agencies and larger agencies (i.e., >500 employees) did not qualify for provider relief funds. Further, as one advocate explained, "those dollars were very slow to flow," and some agencies had yet to receive their funds from the second distribution at the time of our interviews in December 2020 and January 2021.
|
Key challenges policy changes were meant to address:
|
Increased payment rates. States and home care agencies took advantage of increased pay rates to retain and preserve their workforce, although they varied in their approaches to incentivizing workers. Hazard pay and retainer payments were available across states through federal disaster relief funding such as the Coronavirus Aid, Relief, and Economic Security Act and PPP. Our scan identified 21 states with increased agency or provider pay rates. According to our interviews and policy scan, some increased rates were to be used for multiple purposes, including the purchase of PPE or cleaning supplies. Some advocates remarked that rate increases that went directly to agencies did not always translate to increased pay for workers. Our scan further revealed 19 states with hazard pay or "add-on" hourly payments that were a direct increase of a worker's hourly wage (Figure 1). Some state policy changes specified the amount of the increase and detailed the type of staff it covered, while others indicated the increase was specific to a certain Medicaid waiver service.
Twenty-seven states adopted retainer payments to stabilize the workforce (Figure 1). However, very few government officials, advocates, or agencies described how this benefit maintained their workforce. Some agencies implemented other benefits such as paid sick leave or childcare, but these were generally not a result of federal or state policy changes our scan found.
| Figure 1. State Policy Changes Related to Increase Medicaid Payment Rates to Home Care Agencies or Workers |
|---|
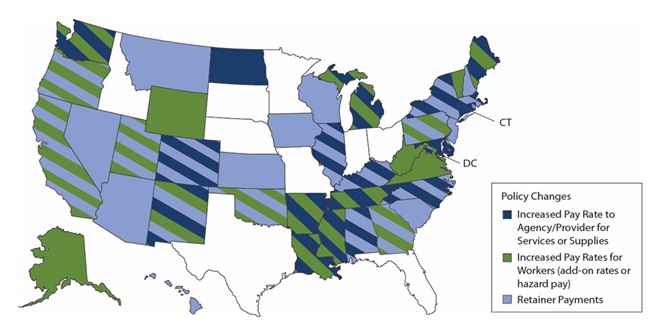 |
| NOTES: This figure was created from multiple secondary sources. The timeframe of the review was limited to March 1, 2020, through December 18, 2020. Some states used federal disaster funding outside of temporary changes to their Medicaid policy. This figure does not account for those uses of disaster relief funding. |
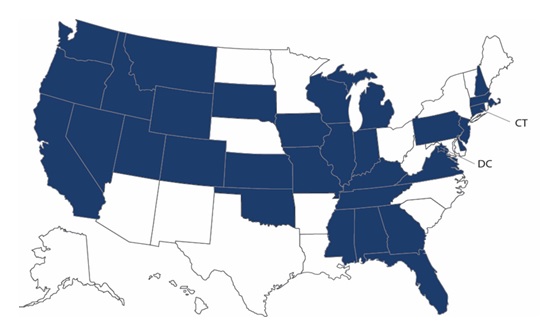
Changes to staff training, qualifications, or duties. Thirty-two states temporarily modified policies related to staff training, qualifications, or duties, including delaying some pre-employment requirements (Figure 2). These changes also expanded agencies' ability to provide training virtually to staff rather than in-person. Some states also expanded the roles of some types of agency staff, such as care managers, to provide direct care when staffing shortages occurred.
Electronic communications. Our scan found that every state expanded the use of telehealth, specifically among Medicaid waiver providers. Agencies and advocates agreed this change was helpful for delivering some services remotely (e.g., medication management), but countered that the lack of state guidance continued to cause challenges with reimbursement. Advocates commented that in most cases, home health agencies (HHAs) cannot be reimbursed for services provided via telehealth because the March 26, 2020 Centers for Medicare & Medicaid Services Interim Final Rule reaffirmed that remote visits made through telecommunications are not equivalent to in-person visits.[1] Advocates added that this guidance steered HHAs away from offering remote service delivery, risking the safety of staff and clients. Although telehealth and telecommunications have assisted home care agencies and HHAs, advocates report reimbursement is still lacking for both.
| Figure 2. State Policy Changes Related to Employment Requirements and Qualifications for Home Care Workers |
|---|
 |
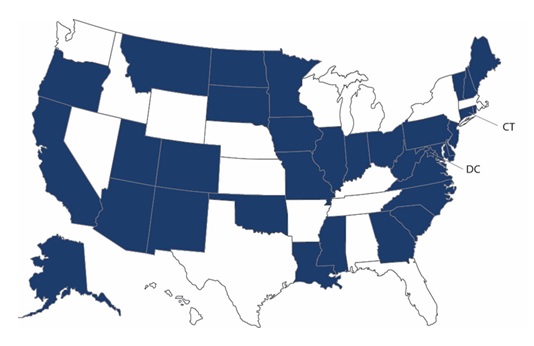
Paying family caregivers. Thirty-four states expanded payments to family caregivers (Figure 3). Stakeholders and some state and federal officials commented that this change was important to not only prompt the post-pandemic expansion of this benefit in the future, but also to help alleviate some workforce shortages that occurred because of the pandemic.
| Figure 3. State Policy Changes Allowing Payment (or Increased Payments) to Family Caregivers |
|---|
 |
Ordering of services by non-physician practitioners. Almost all stakeholders agreed that this policy change was important for supporting the home care workforce both during and beyond the pandemic. Advocates and agencies reported this change helped to maintain agency operations by expanding the ordering of home health or home care services by nurse practitioners or physicians' assistants. This change also helped to maintain a consistent client base and staff hours. Almost all states adopted this temporary policy change, and one state official commented on her agency's desire to make it a permanent policy change beyond the pandemic.
REMAINING CHALLENGES
The COVID-19 pandemic has brought many challenges to the provision of home care and home health throughout most of 2020 and continuing into 2021. Although some policies have been implemented to address these challenges, stakeholders agree that gaps still remain. Policies that deserve continued discussion and legislative action, according to all stakeholders, include:
-
Permanent pay rate increases for home care workers.
-
Allowable HHA reimbursement for telehealth visits.
-
Designation of home care workers as "essential workers" in all states, thus heightening awareness of their important role in the long-term services and supports sector, and prioritizing their access to PPE, testing, and vaccines.
ENDNOTES
RELATED PAPERS
COVID-19 Intensifies Home Care Workforce Challenges
https://aspe.hhs.gov/covid-home-care-workforce-challenges
COVID-19 Intensifies Home Care Workforce Challenges: Agency Perspectives Issue Brief
https://aspe.hhs.gov/covid-home-care-agency-perspectives
COVID-19 Intensifies Home Care Workforce Challenges: Policy Perspectives Issue Brief
https://aspe.hhs.gov/covid-home-care-policy-perspectives
HHS OFFICE OF THE ASSISTANT SECRETARY FOR PLANNING AND EVALUATION
SUGGESTED CITATION
Porter, K., Hunter, M., Mulmule, N., & Tyler, D. COVID-19 Intensifies Home Care Workforce Challenges: Policy Perspectives (Issue Brief). Washington, DC: Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services. June 1, 2021.
COPYRIGHT INFORMATION
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
___________________________________
Subscribe to ASPE mailing list to receive email updates on new publications: aspe.hhs.gov/join-mailing-list
For general questions or general information about ASPE: aspe.hhs.gov/about