
Monday, July 29, 2019
Printer Friendly Version in PDF Format (7 PDF pages)
Reflections
Laura Gitlin
Advising role -- Opportunities and Limitations
- We operate within a space between opportunities and limitations imposed by legislative rules/regulations guiding activities
- Understanding this space is particularly challenging for new members
- Within this space, the Advisory Council serves a very critical role and has achieved significant progress
- Four Key Goals for 2 year Chair appointment
- Enhance engagement of all members and more responsibility of subcommittee chairs/members
- Link recommendations/activities to five goals/strategies/actions of Plan
- Identify ways to be more impactful
- Examine ways to systematically evaluate accomplishments and identify future directions
Primary accomplishments per goal
- Goal: Enhance engagement of all members and more responsibility of subcommittee chairs/members
- Subcommittee chairs plan one meeting a year on a topic relevant to their respective NAPA Goals and recommendations
- Goal: Link recommendations/activities to five goals/strategies/actions of Plan
- Presentations and federal report outs tied to goals/strategies
- Goal: Identify ways to be more impactful
- Executive summary of recommendations as talking points for nonfederal members to use to engage with state and federal legislators
- Elevation of NAPA goals (esp. #2,3, 4) with the First National Resaerch Summit on Care and Services
- that will now be sustained as part of the NIA infrastructure for research milestone development
- Understanding of dementia across trajectory from prevention to end of life, as complex, requiring multi-sector, multidimensional, coordinated actions
- Goal: Examine ways to systematically evaluate accomplishments and identify future directions
- Driver Diagram
- Indicators of progress (how do we know we are moving forward; how will we know when goals are accomplished)
- Moonshot and 4-D approach
Recommendations moving forward
- Expand reach of Advisory Council meetings:
- Increase social media presence and concerted outreach to the public to tune in
- Sponsor meetings/pre-conferences at major meetings (AAIC, GSA etc)
- Chairs/subcommittee chairs - Formulate clear goals for what to accomplish; clearly link meetings/speakers to evolving recommendations
- Prepare for 2025:
- Evaluate what has been accomplished
- Evaluate what needs to be accomplished
- Provide strong rationale for continuing Advisory Council
Key Area Needing Immediate Attention
- Advance an infrastructure for treatment delivery
- Projected capacity insufficient to handle expected case load for treatments
- Key constraint - limited capacity of dementia specialists for diagnosis, limited access to infusion centers to deliver treatment
- Addressing capacity constraints needs to involve payment policy, regulatory requirements, workforce considerations, and capacity planning at national and local levels as well as ground awareness; development of quality indicators etc
 |
| https://www.rand.org/pubs/research_reports/RR2272.html |
Pragmatic Trials offers the science to help advance an infrastructure
- We have some evidence
- It often does not fit health systems
- Takes time, effort and frustration to fit
- In fitting, we may damage the peg
What is the MoonShot to improve Quality of Life Now?
- Ideas grounded in evidence that are:
- Ambitious, but not unattainable
- Can make a real difference
- Possible to accomplish in next few years.
- May change, influence recommendations, legislation, policy, practice, research
- Multi-sectorial (not one action)
- Focus on dementia care to improve quality of life
Moonshot has to be multi-sectorial and coordinated
- Improve Quality of Life
- Quality indicators
- Ground awareness
- Workforce prep
- Reimbursements for evidence-based programs
- Measurement of progress
The 4 Disciplines of Execution (4DX)" to Achieve our "Wildly Important Goal"
- Discipline 1: Focus on the Wildly Important
- Define crucial goals and narrow the team's focus to those goals.
- Discipline 2: Act on Lead Measures
- Consistently carry out and track results on those high-leverage activities that will lead to the achievement of WIGs.
- Discipline 3: Keep a Compelling Scoreboard
- Visibly track key success measures on a goal.
- Discipline 4: Create a Cadence of Accountability
- Regularly and frequently plan and report on activities intended to move the measures on the WIG scoreboard.
Act on Lead Measures
- Lag Measure: the historical measure of a goal or WIG achievement expressed in terms of from X to Y by when
- Ex: Increase annual water production from 175 million liters to 185 million liters by end of year
- Lead Measure: the measure of an action planned and taken as a means to achieving a WIG
- Predictive: if the lead measure changes, the lag measure will also change
- Influence-able by the team
- Ex: Increase the percentage of shifts with full crews from 80 to 95 percent.
Example of a Wildly Important Goal
- By 2025, increase by 25% the average length of time after diagnosis that a person with dementia can remain a community-dwelling adult
- Lag measures
- Reduced number of admissions to LTC
- Reduction of caregiver burden
- Lead measures
- Increase of support services
- Increased caregiver education
- Lag measures
Questions/Issues
- How do we measure preferred environment"
- How to we ask people with advanced dementia (in nursing homes, potentially) if they are in their preferred environment
- Preferred environment may change with disease trajectory and how to account for?.
- How to assure caregivers have training and resources they need to manage behavioral symptoms and other clinical symptoms?
- How to account for time of diagnosis and time of LTC -- what administrative data sets are available?
- Is LTC defined as facility-based placement (MDS data source for non-SNF stays; doable), use of long-term home-based services (data source?) or both?
- Is there a way to build in goals of care discussion (which is a Medicare service with a billing code -- ACP) into this?
- Consider as a lead measure % of people with a diagnosis of dementia who have a care plan.
- What is current % - i.e. baseline?
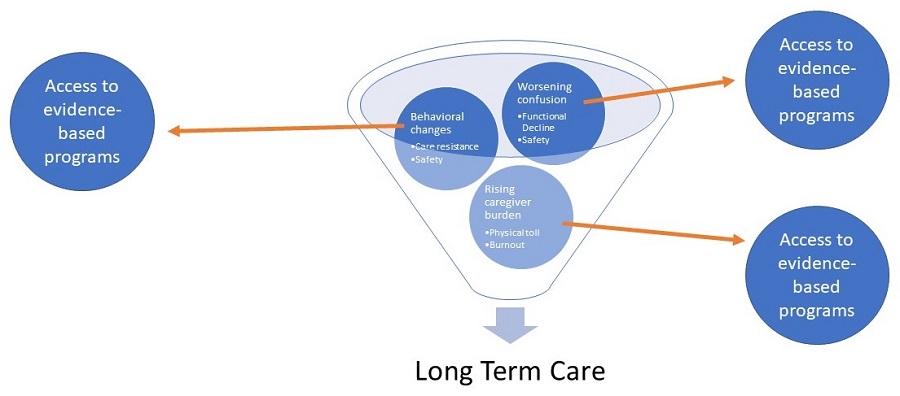
What drives placement to long term care?
 |
What is the impact of a transition to long term care?
- Positive aspects
- Expanded team for caregiving/reduced burden on family caregiver
- Increased social interactions for the person with dementia
- Negative aspects
- Loss of familiar environment/homesickness/confusion during transition
- Reduced person-centered care
- Major financial burden