Monday, October 21, 2019
Printer Friendly Version in PDF Format (9 PDF pages)
Risks and Costs of Dementia at Older Ages
Melissa Favreault and Richard W. Johnson
Urban Institute
Judith Dey, Helen Lamont, William Marton
ASPE
Research Questions
- How many older adults in the US will develop dementia in coming decades?
- How does this vary by other characteristics (race/ethnicity, socio-economic status, gender, etc.)?
- How does the risk of developing dementia change with age?
- For how long will people with dementia need care?
- For less than one year, more than one year, more than five years, etc.?
- What are the expected costs of caring for people with dementia?
- Who will pay for this care?
- How costly is care in nursing homes for people with dementia compared to other settings?
Dynamic Simulation of Income Model
- Projects the size, characteristics of the US population for the next 75 years
- Starts with representative sample of individuals and families and ages them year by year
- Marriage
- Children
- Employment
- Disability (including dementia)
- Death
- Use aging algorithms from high-quality data sources
- Compute eligibility, benefits, and taxes using calculators
- Use Social Security and Medicare trustees assumptions
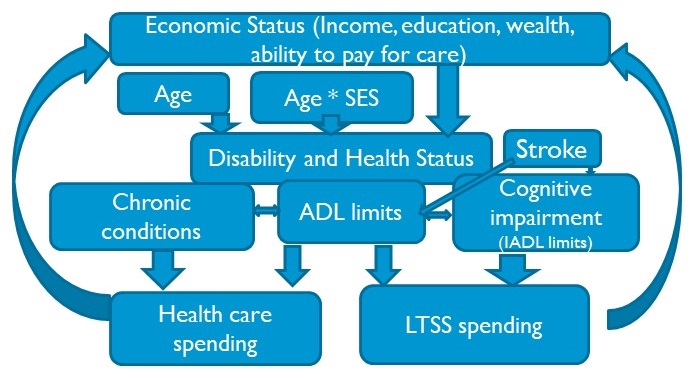
Modeling Overview
Number of People with Dementia Will Nearly Double by 2055
| Number of people with Dementia, by Age |
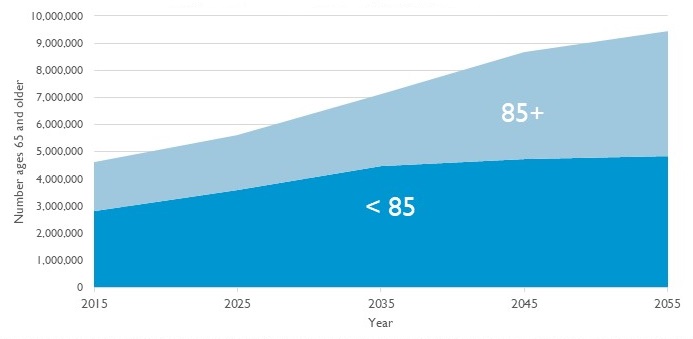 |
| Source: DYNASIM. Compare to Alzheimer’s Association (2015), Brookmeyer et al (2018), Herbert et al (2013), Matthews et al. (2018), and Zissimopoulos et al. (2018). |
This Occurs Despite Modest Projected Decline in Dementia Prevalence at Older Ages
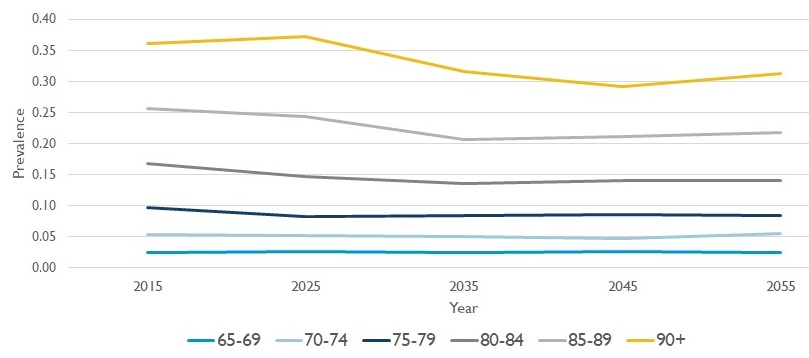 |
| Source: DYNASIM. Compare to Brookmeyer et al. (2011), Freedman et al. (2018), Herbert et al (2013), Hudomiet, Hurd, and Rohwedder (2018), Li et al. (2017), Matthews et al. (2018), Stallard and Yashin (2016), and Zissimopoulos et al. (2018) |
Americans who Survive to Age 65 Face a Three in Ten Chance of Developing Dementia
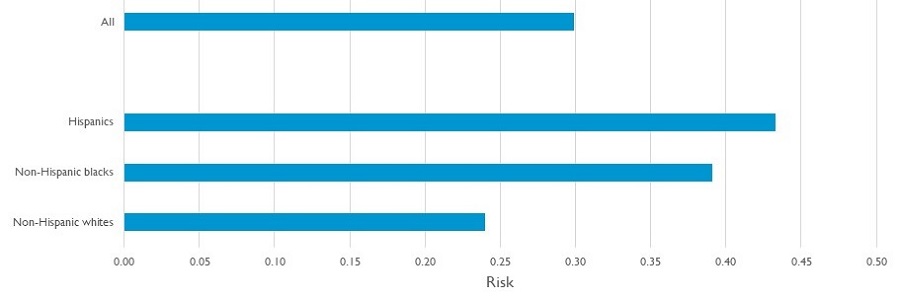 |
| Source: DYNASIM., 1963-1967 birth cohort. Compare to Mayeda et al. (2016), Murtaugh et al. (2011), Yang and Levey (2015), and Zissimopoulos et al. (2018). |
Chances of Dementia Differ Significantly by Education and Gender
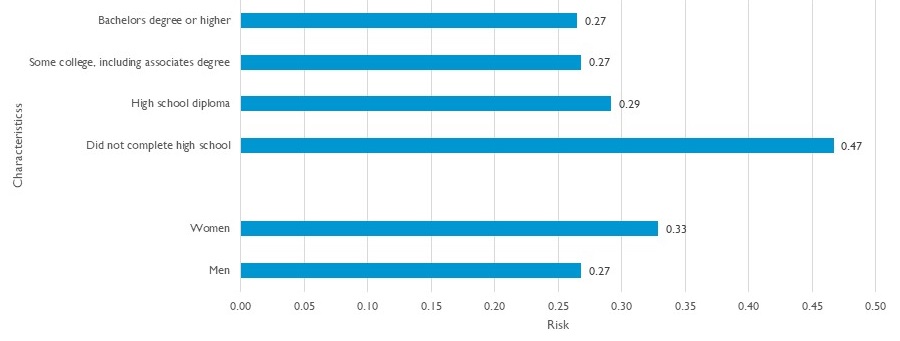 |
| Source: DYNASIM, 1963-67 birth cohorts |
The Median Duration of Dementia is Lengthy
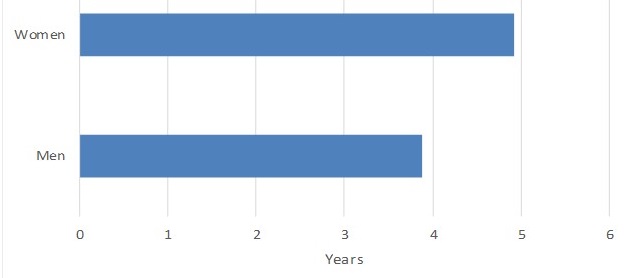 |
| Source: DYNASIM , 1973-1977 birth cohorts |
Costs are Largely Borne Out-of-Pocket by Families and by Medicaid
| Present value of average LTSS costs due to dementia (2019$), by payer |
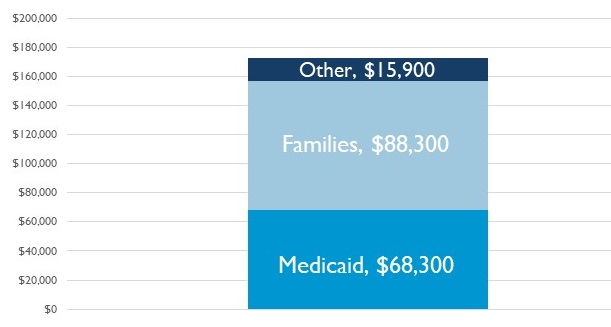 |
| Source: DYNASIM, 1953-57 birth cohorts. Note: Payer composition differs from calculations based on NHEA, as many NHEA computations include post-acute care, exclude many private transactions, and exclude some assisted living/residential care. |
Dementia Care Costs so Much Because Much is Delivered in Costly Institutional Settings
| Present value of care for people with dementia (2019$), by setting |
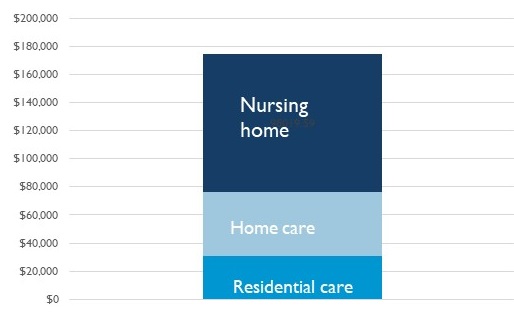 |
| Source: DYNASIM, 1953-57 birth cohorts. |
Families are a Vital Support to People with Dementia, Providing Care that Exceeds Value of Paid Care
| Present value of care for people with dementia (2019$), by source of care |
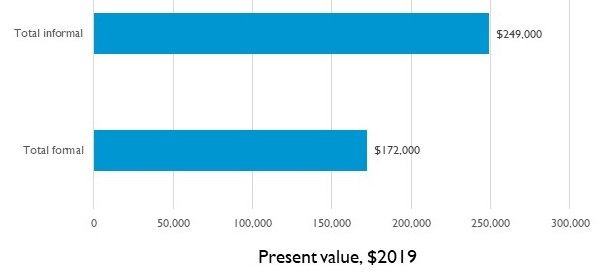 |
| Source: DYNASIM, 1953-57 cohorts. Compare, for example, to Jutkowitz, Kane, et al. (2017). |
Averages Mask the Risk that Families Face of Long Spells with High Financial and Personal Costs
| Present value of care for people with dementia (2019$), by source of care |
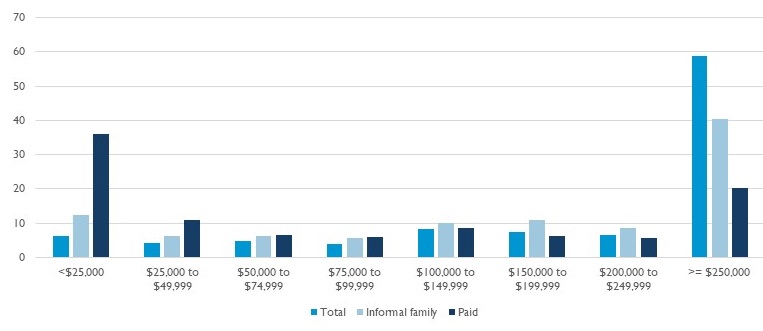 |
| Source: DYNASIM, people born 1953-1957 |
Conclusions
- The number of older adults in the US with dementia is expected to nearly double by 2055
- Burden of the disease affects different populations disproportionately
- Among those who develop dementia, roughly half will have it for four or more years
- The average present value of care for people with dementia is over $170,000
- Families and Medicaid cover most care costs
- Families face the double burden of paying for formal care and providing informal care--the value of informal care exceeds the formal costs
- Nursing home care is the most costly, but the value of informal care is even more significant
Thank you
This research and presentation was made possible by the US Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. The statements made and views expressed are solely the responsibility of the authors, and not HHS/ASPE, the Urban Institute, its Board, or sponsors.
Caveats
- Cognitive impairment is difficult to measure, sensitive to definitions and thresholds
- Can change throughout the year; we use a high-quality survey, but it only asks questions every two years
- Important to use exit interview, proxy responses
- First symptoms vs. diagnosis vs. study entry vs. passed a severity threshold (Brodaty, Seeher, Gibson 2012)
- Our aims are descriptive, so we do not address many questions
- Our costs focus on LTSS costs, not added acute health care costs
- Challenging to forecast when patterns change, literature is inconsistent
- We must monitor the research, especially longitudinal aspects
Valuing Care
- Formal care: Literature divided between gross and net costs
- Informal care: Use an hourly cost based on median state care costs (Genworth) and projected care hours (HRS data)
- Foregone wages is an alternative from the literature
- Higher for some, lower for others (caregivers who no longer work)
- Use present discounted value
- Lump sum amount (in today’s dollars) families need to set aside to cover the stream of costs required to meet care needs through time of death
- Accounts for interest the lump sum accrues until it is used