
Friday, October 19, 2018
Printer Friendly Version in PDF Format (12 PDF pages)
Clinical Services Federal Update
Ellen Blackwell MSW
National Partnership to Improve Dementia Care in Nursing Homes
- The National Partnership to Improve Dementia Care in Nursing Homes is committed to improving the quality of care for individuals with dementia living in nursing homes with a mission to deliver health care that is person-centered, comprehensive and interdisciplinary with a specific focus on protecting residents from being prescribed antipsychotic medications unless there is a valid, clinical indication and a systematic process to evaluate each individual's need
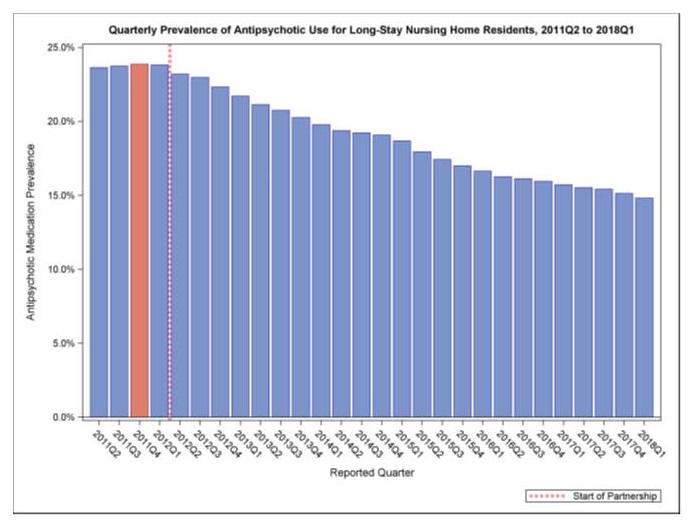
- CMS is tracking the progress of the National Partnership by reviewing publicly reported measures -- the official measure of the Partnership is the percentage of long-stay nursing home residents who are receiving an antipsychotic medication, excluding those residents diagnosed with schizophrenia, Huntington's Disease or Tourette's Syndrome
- Information at: https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/SurveyCertificationGenInfo/National-Partnership-to-Improve-Dementia-Care-in-Nursing-Homes.html
Strategy 2.D
2019 Goals
- Nursing homes with low rates of antipsychotic medication use are encouraged to continue their efforts and maintain their success
- Nursing homes with high rates of use are to work to decrease antipsychotic medication use by 15 percent, for long-stay residents, by the end of 2019
- These nursing homes are identified as "late adopters"
- https://www.cms.gov/newsroom/fact-sheets/data-show-national-partnership-improve-dementia-care-achieves-goals-reduce-unnecessary-antipsychotic
National Data
 |
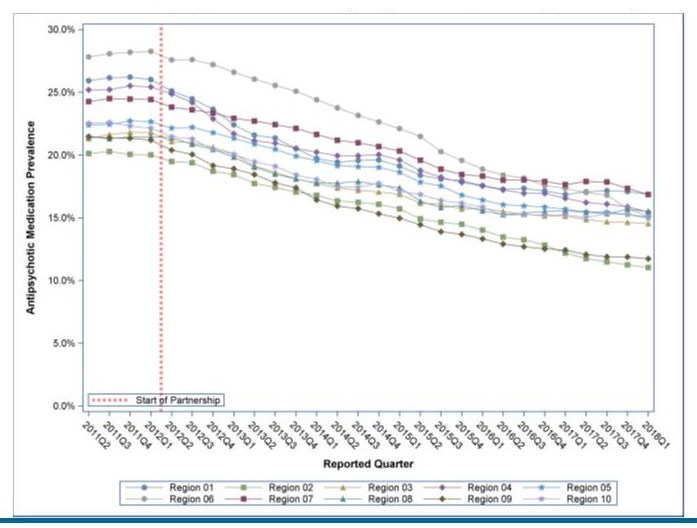
Regional Data
| Quarterly Prevalence of Antipsychotic Use for Long-Stay Residents, CMS Regions 2011Q2 to 2018Q1 |
|---|
 |
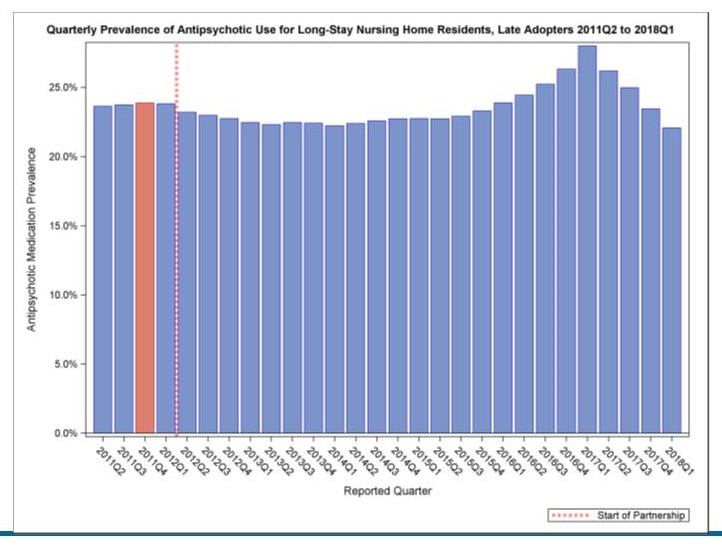
Late Adopters
- Nursing homes were identified as late adopters, based upon 2017Q1 data
- Continued to have a high rate of antipsychotic medication use
- percentage of change from 2011Q4 to 2017Q1 increased or decreased very little
- remained above the national average in 2017Q1
Late Adopter National Data
 |
Hand in Hand: A Training Series for Nursing Homes
- The updated Hand in Hand: A Training Series for Nursing Homes is now available on CMS's Integrated Surveyor Training Website (ISTW). Hand in Hand is available as a self-paced training as well as an instructor-led course
- The training focuses on caring for residents with dementia and abuse prevention
- The Hand in Hand training is available as a self-paced, online training and also available to download for use as an instructor-led course
- Federal law requires that nurse aides complete in-service training on dementia management and resident abuse prevention and that facilities furnish dementia management and resident abuse prevention training to all facility staff
- For more information on the surveyor training see: https://surveyortraining.cms.hhs.gov/pubs/ClassInformation.aspx?cid=0CMSHIH_ONL
Strategy 2.D
Medicare Supplemental Benefits -- 2018 Guidance
- Historically, CMS has defined a mandatory or optional supplemental health care benefit in Chapter 4 of the Medicare Managed Care Manual as an item or service (1) not covered by Original Medicare, (2) that is primarily health related, and (3) for which the plan must incur a non-zero direct medical cost
- An item or service that meets all three conditions may be proposed as a supplemental benefit in a plan's plan benefit package and the final determination of benefit status is made by CMS during the annual benefit package review
- Beginning in 2019, CMS is expanding the definition of "primarily health related" to consider an item or service as primarily health related if it is used to diagnose, compensate for physical impairments, acts to ameliorate the functional/psychological impact of injuries or health conditions, or reduces avoidable emergency and healthcare utilization, and also changing uniformity requirements
- A supplemental benefit is not primarily health related under the previous or new definition if it is an item or service that is solely or primarily used for cosmetic, comfort, general use, or social determinant purposes
Strategy 2.G
In 2019
- Due to these new flexibilities, nearly 270 Medicare Advantage plans will be providing an estimated 1.5 million enrollees new types of supplemental benefits
- They include reduced cost sharing and additional benefits for enrollees with certain conditions, such diabetes and congestive heart failure due to the agency's reinterpretation of uniformity requirements
- CMS expects continued growth in 2020, as plans take advantage of these new flexibilities
- On average Medicare Advantage premiums will decline, and Medicare Advantage enrollment is projected to reach a new all-time high with more than 36 percent of Medicare beneficiaries projected to be enrolled in Medicare Advantage in 2019
Patients Over Paperwork
- CMS has set up an agency-wide process to evaluate and streamline regulations and operations with the goal to reduce unnecessary burden, increase efficiencies and improve the customer experience
- Formal Requests for Information
- Customer Centered Work groups -- nursing homes, other provider types
- Human-Centered Design
- Meaningful Measurement Framework
- Health IT
- Promoting Interoperability
- Engaging Stakeholders
Patients Over Paperwork - FFS Clinician Journey Map
- Clinician
- Decide to become an enrolled Medicare provider.
- Enrollment & Eligibility
- Complete enrollment process to:
- gain access to the MAC Portal
- submit clains electronically
- obtain identity management (user IDs)
- participate in CMS models
- Outreach to R.O.s, providers, webinars, in-person, etc.
- Technical assistance (e.g. QIOs)
- Eligible to participate in Medicare
- Decide participating vs non-participating
- Choose to disenroll/opt-out
- CMS model ends
- Remove due to termination from program
- Complete enrollment process to:
- Beneficiary Eligibility
- Check beneficiary eligibility.
- Work with billing office staff to document clearly what services the patient is authorized to receive.
- Delivery of Healthcare
- Services (e.g. Professional services) and delivery of healthcare (e.g. infrastructure, ancillary services, etc.)
- Coordination of Care
- Compliance within our own practices or facilities
- Supervise Physician Extenders (e.g. NP, PA) & review their notes, x-rays, etc.
- Education & Outreach
- Includes the following:
- CMS.gov
- A/B MAC Jurisdiction
- Help Desk
- Medicare Learning Network
- Technical Assistance (e.g. QIOs)
- CMS Quality Payment Program (QPP)
- QPP for Solo, Small and Rural practices
- Technical Assistance Resource Guide
- Office of the National Coordinator for Health IT Resources
- ONC website
- ONC Certified Health Product List
- Health IT Playbook
- Includes the following:
- Billing
- Ensure documentation supports services accurately.
- Work with billing office staff to choose correct CPT/HCPCS & ICD-10 codes.
- Ensure billing only of services that were rpe-authorized (where applicable).
- Determine other insurances (coordinate benefits).
- Quality Reporting
- Work with EHR vendor, registries, QCDRs, billing & survey vendors to attest/submit quality measures
- Data validation before publication
- Review performance feedback reports (issued to clinician before payment)
- Physician Compare
- Claims Payment, Denial, Rejection & Repayment
- Work with billing office staff to:
- receive payment, denial, & remittance advice,
- receive medical documentation request,
- check claim status,
- review denied claims,
- resubmit corrected claims
- Submit 1st level appeal.
- Recoupment (auto or payment plan).
- Coordinate benefits to recoup.
- Suspend payment.
- Work with billing office staff to:
- Oversight & Compliance
- Chosen for an audit/investigation.
- Attach any medical documentation that was requested.
- Work with reporting entity to submit necessary documentation.
- Submit documentation to RAC/MAC & UPICS/ZPICS for medical review.
- Receive audit (review result findings letter).
- Receive overpayment demand letter.
- Education.
- Reconciliation & Appeals
- Participate in appeal hearing (3rd level).
Patients Over Paperwork
- On the Website now:
- E & M code reforms
- Simplifying office visit documentation
- Sharing the 2019 PFS proposed rule presentation
- Mapping the nursing home experience
- Implementing MACRA
- Cutting documentation requirements
- Making the medical review process clearer
- Meaningful Measures
- For more information visit: https://www.cms.gov/About-CMS/story-page/patients-over-paperwork.html
- Sign up for the newsletter here: https://public.govdelivery.com/accounts/USCMS/subscriber/new?topic_id=USCMS_12350
- Read past newsletters here: https://www.cms.gov/Outreach-and-Education/Outreach/Partnerships/PatientsOverPaperwork.html
2019 CMS Quality Conference
- The website link for the 2019 CMS Quality Conference is: https://www.cmsqualityconference.com
- The landing page provides a link to pre-register for the conference and to request your email address be added to the conference distribution list for additional notifications
 |
U.S. Dept. Veterans Affairs Updates
Federal Clinical Subgroup
Marianne Shaughnessy, PhD, CRNP
Susan G. Cooley, PhD
VA Geriatric Scholars Program
- A workforce development program to integrate geriatrics into primary care practices
- Longitudinal, multi-modal continuing education program for healthcare professions:
- Intensive education, clinical practicum experiences, self-paced learning through webinars and on-line learning communities, demonstration of knowledge through quality improvement projects
- Focus on rural VA clinics; outreach to rural Indian Health Service clinics
- Funded by VA Offices of Rural Health and Geriatrics/Extended Care
- Collaboration of 12 Geriatric Research, Education and Clinical Centers (GRECC), in partnership with VA Employee Education System (EES), academic affiliates and HRSA-funded Geriatric Workforce Education Programs (GWEP)
- Dementia Education Toolkits:
- Dementia http://www.gerischolars.org/course/view.php?id=29
- Cognitive Impairment, Memory Loss and Dementia http://www.gerischolars.org/course/view.php?id=2
FY18Q4 VA Geriatric Scholars Dementia Education and Resources
- Geriatric Scholars Program core course in geriatric medicine and gerontology
- Los Angeles, September 12-15, 2018
- New York, September 25-28, 2018
- Geriatric Scholars Program Clinical Practicum with focus on dementia at the following GRECCs:
- Madison GRECC, July 9-13, 2018; July 30-August 3, 2018; September 24-28, 2018
- Geriatric Scholars Program Rural Interdisciplinary Team Training in care of older Veterans
- On-site training for all clinic staff on teamwork in care of older adults; recognition of geriatric syndromes, "red flags," functional impairments including dementia . All trainings have been updated to include the Rural Caregiver Resource Center and opportunities for REACH training.
- Hot Springs AR July 13, 2018
- Zanesville, OH, July 18, 2018
- Newark, OH, July 19, 2018
- Conway, AR, August 17, 2018
- McClellan, CA, September 13, 2018
- Altoona, PA, September 17, 2018
- Butler, PA, September 18, 2018
- For IHS and Tribal partners
- Norton Sound Health Corporation September 24, 25, 2018
- On-site training for all clinic staff on teamwork in care of older adults; recognition of geriatric syndromes, "red flags," functional impairments including dementia . All trainings have been updated to include the Rural Caregiver Resource Center and opportunities for REACH training.
- GRECC Connect Webinars for VA Staff with specific focus on cognitive impairment, dementia:
- Strategies for Adapting Care for Patients with Dementia (Lauren Moo) September 18, 2018
REACH-VA Caregiver Support Intervention Updates
- National Program to Provide REACH VA to Caregivers of Veterans
- Funded by VA Office of Rural Health and Caregiver Support Program
- Pilot enhancement to curriculum: REACH training, June-Sept, 2018
- The Caregiver Center, funded by the Caregiver Support Program, is being included in the VA Geriatric Scholars Program Rural Interdisciplinary Team Training (RITT) training. The goal is to identify, train, and certify staff from rural facilities to deliver the REACH (Resources for Enhancing All Caregivers Health) and Telephone Support Group programs. The Caregiver Center will provide all materials for staff and Caregivers.
- September 2018, received list of RITT attendees interested in the REACH VA training.
- For Indian Health Service:
- REACH into Indian Country, a three year project funded by the Rx Foundation to implement the REACH caregiver support intervention across Indian Country has reached the initial goal of having a Program Coach trained and certified in at least 50 Tribal communities by February 2018.
- At the end of funding, July 2018, 191 staff have been trained and 80 have been certified with 56 of the 50 proposed communities now having a Program Coach who is trained and certified and could deliver the Program.
- Going forward, there is a mechanism in place for ongoing training through the UTHSC Caregiver Center. Additional Reach into Indian Country Caregiver Notebooks are available.
VA Office of Rural Health (ORH)Dementia-Related/Dementia-Relevant Projects
- ORH Enterprise Wide Initiatives
- Advanced Care Planning via Group Visits
- GRECC Connect
- Geriatric Scholars
- Gerofit, Geriatric Fitness Program
- Medical Foster Home
- State Veterans Homes (VSH) Telehealth Initiative
- https://www.ruralhealth.va.gov/providers/Enterprise_Wide_Initiatives.asp
- ORH National Promising Practice Disseminations
- Geriatric Scholars
- Geriatric Scholars Rural Interdisciplinary Team Training (RITT)
- Resources for Enhancing All Caregivers Health (REACH) and Telephone Support Group Caregiver Support Intervention
- GRECC Connect-Connecting Rural Providers with Geriatric Specialists Through Telemedicine
- https://www.ruralhealth.va.gov/providers/promising_practices.asp
- ORH Veterans Rural Health Resource Center -- Salt Lake City
- Dementia Caregiver Video Series https://www.ruralhealth.va.gov/vets/resources.asp#dem
- www.ruralhealth.va.gov
Caring for Older Adults & Caregivers at Home (COACH)
- Caring for Older Adults and Caregivers at Home (COACH) is a home-based dementia care program that assists Veterans with moderate to severe dementia living at home with a caregiver. The program provides support; education on dementia and behavioral management; referrals and assistance with resources; recommendations to address safety in the home. The COACH program respects caregivers' wishes to keep their loved ones living at home for as long as possible while improving the quality of life of the Veteran/caregiver dyad.
- The COACH home based dementia care program was awarded Gold Status by The VHA Office of Organizational Excellence in the 2018 VHA "Shark Tank" Competition.
- COACH was initiated at Durham VA Medical Facility by the Durham VA Geriatric Research, Education and Clinical Center (GRECC) in Fiscal Year (FY) 2010 with Geriatrics and Extended Care (GEC) Non Institutional Long Term Care (NILTC) innovation funding.
- COACH was expanded to Richmond VA Medical Facility in FY2018 through a Mentoring Partnership with Durham and GEC implementation funding. The Richmond program began enrolling Veterans in the COACH program June 11, 2018.
- Louisville VA Medical Facility will implement COACH in FY2019 with GEC funding and a mentoring partnership with Durham.
- COACH also expanded to rural areas in North Carolina with VA Office of Rural Health (ORH) funding from FY2014 to FY2016. It is listed as a Promising Practice by ORH.
- https://www.ruralhealth.va.gov/docs/promise/COACHModelOnepager_EMH.pdf
STAR-VA Training Program
- STAR-VA, adapted from Dr. Linda Teri's Staff Training in Assisted Living Residences (STAR) program, is an interdisciplinary, behavioral approach for understanding and managing distressed behaviors among Veterans Health Administration (VHA) Community Living Center (CLC; i.e., nursing home) residents with dementia.
- Between May and October 2018, 17 additional VHA CLC teams participated in STAR-VA training; between 2013 and 2018, 92 of 134 CLC teams nationally have participated in training.
- Veterans enrolled during the competency-based training program experience decreased frequency and severity of target behaviors and decreased symptoms of anxiety and depression over the course of the intervention.
- A VA Quality Enhancement Research Initiative (QUERI) Partnered Evaluation project, collaborating with VHA Offices of Geriatrics and Extended Care and Mental Health and Suicide Prevention, is working to evaluate the impact of STAR-VA on distressed/disruptive behaviors, psychotropic prescribing, staff injuries, and to determine facilitators and barriers to program sustainability.
Behavioral Recovery Outreach (BRO) Team Training
- The BRO Team program, developed at the Des Moines VA Medical Center, facilitates the transition of Veterans with complex problems (i.e., co-morbid medical, mental health/substance use, and/or neurocognitive conditions with distressed behaviors that can be disruptive to care) from VA CLCs to more appropriate, and less costly, community care settings (e.g., community nursing homes).
- BRO builds upon the STAR-VA intervention, focusing largely on Veterans with dementia and related distressed behaviors.
- With promising local outcomes -- including reductions in length of stay, behavioral readmission rates, and costs -- the BRO Team program has been disseminated this past year in the VA Midwest Healthcare Network (VISN 23).
- The VHA Care for Patients with Complex Problems (CP)2 Program partnered with VISN 23 BRO leaders in a 1.5-day virtual training to launch a national BRO dissemination with three inaugural partner sites (VISNs, 6, 7, 8) on September 13-14, 2018. Evaluation of this promising practice will continue.