
U.S. Department of Health and Human Services
Why Do They Stay? Job Tenure Among Certified Nursing Assistants in Nursing Homes
Joshua M. Wiener, Ph.D., Marie R. Squillace, Ph.D., Wayne L. Anderson, Ph.D., and Galina Khatutsky, M.S.
April 10, 2009
PDF Version: http://aspe.hhs.gov/daltcp/reports/2009/whystay.pdf (33 PDF pages)
This article appeared in The Gerontologist (2009, 49(2):198-210; doi:10.1093/geront/gnp027). It was prepared under contract #HHS-100-03-0025 between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and the the Research Triangle Institute. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, Marie Squillace, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. Her e-mail address is: Marie.Squillace@hhs.gov.
The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS
- INTRODUCTION
- Wages and Benefits
- Training and Career Opportunities
- Organizational Culture
- Recruiting Certain Types of Workers
- Other Variables Affecting Job Tenure
- Purpose
- LIST OF EXHIBITS
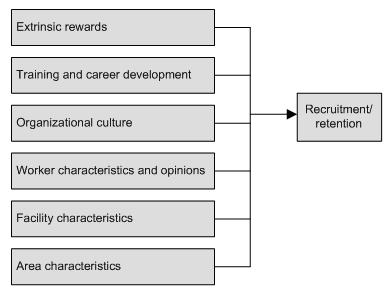
- EXHIBIT 1: Factors Affecting Job Tenure of CNAs in Nursing Homes
- LIST OF TABLES
- TABLE 1: Descriptive Statistics
- TABLE 2: OLS on Logged Number of Months in Facility
- TABLE 3: Change in Variables With Statistically Significant Results in Multivariate Analysis Ordinary Least Squares on Number of Months in Facility
ACKNOWLEDGEMENT
Funding for this study was provided by the Office of Disability, Aging, and Long-Term Care Policy, Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services, through Contract Number HHS-100-03-0025, Task Order HHSP23300007T. The authors wish to thank Christine Bishop and Peter Kemper for useful comments on earlier drafts. We are grateful to Valentina Akhmerova and Dhuly Chowdhury for research support. The opinions expressed in this study represent the views of the authors and are not those of the U.S. Department of Health and Human Services or RTI International.
AUTHORS
Joshua M. Wiener, Ph.D., Aging, Disability, and Long-Term Care Program, RTI International, Washington, D.C.
Marie R. Squillace, Ph.D., Office of Disability, Aging, and Long-Term Care Policy, Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services, Washington, D.C.
Wayne L. Anderson, Ph.D., Aging, Disability, and Long-Term Care Program, RTI International, Research Triangle Park, North Carolina.
Galina Khatutsky, M.S., Aging, Disability, and Long-Term Care Program, RTI International, Waltham, Massachusetts.
Address correspondence to Joshua M. Wiener, PhD, Aging, Disability, and Long-Term Care Program, RTI International, 701 13th Street, Northwest, Suite 750, Washington, DC 20005. E-mail: jwiener@rti.org
ABSTRACT
Purpose: This study identifies factors related to job tenure among certified nursing assistants (CNAs) working in nursing homes.
Design and Methods: The study uses 2004 data from the National Nursing Home Survey, the National Nursing Assistant Survey, and the Area Resource File. OLS regression analyses were conducted with length of job tenure as the dependent variable. Tenure of CNAs was hypothesized to be motivated by the extrinsic rewards of their job; initial training and mentoring; reasons for being a CNA; organizational culture; and personal, facility, and market characteristics. Separate analyses were conducted for the overall sample and for CNAs who worked for the facility for more than 1 year.
Results: Among policy-relevant domains, extrinsic rewards had the largest number of significant variables (four). Only one training and one organizational culture variable significantly affected CNA job tenure. Significant variables in domains not readily influenced by policy (e.g., personal characteristics and characteristics of the facility and surrounding market area) were often significant in both regressions.
Implications: This study underscores the importance of the basic economics of job choice by low-income workers. Wages, fringe benefits, job security, and alternative choices of employment are important determinants of job tenure that should be addressed, in addition to training and organizational culture.
Key Words: CNAs, Direct care workers, Long-term care, Nursing homes, Job tenure, Turnover
INTRODUCTION
Long-term care workers, such as certified nursing assistants, are the backbone of the formal long-term care delivery system, providing the majority of paid assistance to people with disabilities (Anderson, Wiener, Greene, & OKeeffe, 2004; Harris-Kojetin, Lipson, Fielding, Kiefer, & Stone, 2004; National Commission on Nursing Workforce for Long-Term Care, 2005; Stone & Wiener, 2001). Over 700,000 certified nursing assistants provided personal assistance to residents in nursing homes in 2004 (Squillace, Remsburg, & Bercovitz, 2006). These frontline nursing home workers primarily help people by assisting with activities of daily living (such as eating, bathing, and dressing) and some instrumental activities such as using the telephone. The central role of these workers in providing hands on services makes them the key factor in determining the quality of paid long-term care.
Certified nursing assistants in nursing homes are difficult to recruit and retain in nursing homes (Decker, Dollard, & Kraditor, 2001). Nationally, turnover rates for certified nursing assistants in nursing homes were estimated to be 71% per year in 2002 (American Health Care Association, 2003). Annual turnover rates among these workers are significantly higher than for other service workers (U.S. General Accounting Office [GAO], 2001). Vacancy rates for certified nursing assistants are also high, reaching 8.5% for certified nursing assistants in 2002 (American Health Care Association, 2003). Of particular concern is that high annual turnover rates and vacant positions may compromise the continuity of resident care and care quality (Castle & Engberg, 2006; Centers for Medicare & Medicaid Services, 2002; Harrington et al., 2000; Kramer, Eilertsen, Lin, & Hutt, 2000; U.S. GAO, 2001).
High turnover effectively reduces staffing levels and may mean that staff do not have time to get to know the needs and preferences of individual residents. Workers who provide care in understaffed environments may experience high levels of stress and frustration and low levels of satisfaction, which may lead to poor quality of care and further contribute to high turnover rates. As a result of high turnover and vacancy rates, providers incur substantial recruitment and training costs (Leon, Marainen, & Marcotte, 2001; Seavey & Salter, 2006). At least 36 states consider certified nursing assistant vacancies and turnover to be a serious issue and many are currently pursuing public policy actions to improve the adequacy and stability of the direct care workforce (Harmuth & Dyson, 2005).
The current worker shortage is likely to be exacerbated by the increased demand for long-term care workers as a result of the aging population. The number of older Americans in need of long-term care is predicted to more than double, from 10.0 million in 2000 to 20.9 million in 2040 (Johnson, Toomey, & Wiener, 2007). A number of factors will contribute to this growth; chief among them is the increase in the size of the elderly population aged 85 and older. As a result of demographic shifts, there will be a need for 325,000 additional nursing aides, orderlies, and attendants by 2014, an increase of 22% from 2004 (Hecker, 2005). Implementing effective recruitment and retention strategies, therefore, will be critical to filling these new positions and those left vacant by turnover.
A large number of policy initiatives have been proposed to address the problem of high turnover by certified nursing assistants in nursing homes. These strategies can be grouped into four broad categories--improving wages and benefits, upgrading training programs and career ladders, improving organizational culture, and recruitment strategies (Institute of Medicine [IOM], 2001; Stone & Wiener, 2001; U.S. GAO, 2001). The purpose of this study is to assess these strategies and other factors that may increase certified nursing assistant job tenure in nursing homes.
Wages and Benefits
Certified nursing assistants have low wages and often lack fringe benefits. The median hourly wage of certified nursing assistants in nursing homes was only $10.04 in 2004 (Squillace , Harris-Kojetin, Rosenoff, Han, & Remsburg, 2007). A recent analysis of certified nursing assistants suggests that among those likely to leave their job in the next year, one in three workers cited pay as a reason they would leave their job (Squillace, Bercovitz, Remsburg, & Rosenoff, 2007). In addition to having low wages, an estimated 16% of certified nursing assistants do not have health insurance (Squillace, Harris-Kojetin, et al., 2007).
Proposals to improve extrinsic benefits of the job, such as wages and fringe benefits, make a straightforward economic case. Workers are more likely to stay on the job when they are well paid, especially relative to other employment opportunities. The argument is also that better worker compensation packages could help draw marginal workers into the labor force. In addition, increases in the compensation of long-term care staff relative to other low-wage positions could reallocate the available low-wage workforce to long-term care (Holzer, 2001). Elasticity of labor supply across occupations with few education and training requirements is relatively high (Ehrenberg & Smith, 1997). To implement this approach, just over half the states funded wage pass-throughs for direct care workers in recent years and over 40% of wage pass-throughs have been for workers in nursing facilities (Seavey & Salter, 2006). In these initiatives, Medicaid or other public payment rate increases are earmarked to raise wages for long-term care staff. Although consistent with economic theory, there is little evidence as to whether wage pass-throughs affect recruitment and retention of workers; the wage increases are often small and enforcement and accountability mechanisms for the pass-throughs are often lacking (Seavey & Salter, 2006). In a rare study of the effects of wage increases, a near doubling of wages of home care workers in San Francisco County, California, increased the retention rate over a 52-month period from 39% to 74% (Howes, 2005).
The importance of health benefits has gained greater attention in the past few years and may play a stronger role in reducing turnover and increasing retention than wages alone (Howes, 2006). About a dozen states have public and private sector initiatives to achieve broader health insurance coverage for these workers (Seavey & Salter, 2006).
Training and Career Opportunities
The low education levels and inadequacy of training of certified nursing assistants also may adversely affect job tenure and quality of care. Approximately three quarters of certified nursing assistants in nursing homes had only a high school education or less in 2004 (Squillace, Harris-Kojetin, et al., 2007). These direct care occupations are often considered dead-end jobs because of the lack of additional training and opportunity for advancement.
Increased entry-level or continuing training may be important in helping workers improve competency, skills, and confidence and may improve the recruitment and retention of direct care workers (American Association of Homes and Services for the Aging, 2007; Castle, Engberg, Anderson, & Men, 2007; Institute for the Future of Aging Services & the Paraprofessional Healthcare Institute, 2005). In a review of literature on the impact of training on recruitment and retention, researchers found that higher levels of training helped employers find and keep nurse aides, although the effect was notably stronger on retention than on recruitment (Leon, Marainen, & Marcotte, 2001). Similarly, studies that tested the effects of enhanced educational programs have observed reductions in nurse aide turnover (McCallion, Toseland, Lacey & Banks, 1999; Noel, Pearce, & Metcalf, 2000). Evaluations also suggest that combining training with organizational culture change or payment incentives may result in reductions in turnover, increased satisfaction, and improved care quality (Hollinger-Smith, 2002; Konrad & Morgan, 2004; Stone et al., 2002).
On the other hand, certified nursing assistants may leave their job if they lack time management skills and experience in prioritizing competing demands (Pillemer, 1996), if they received little guidance during their orientation on how to respond to job demands (Bowers & Becker, 1992), or if their training did not realistically match the demands of the job (Atchley, 1996; Castle et al., 2007; Schirm & Garland, 1997). Although workers who provide care to an older, more acute population of residents in nursing homes will require additional training and supervision, they often lack the funds and time to participate in additional training or advancement opportunities (Dawson, 2007). Nonetheless, about half the states require more hours of training for certified nursing assistants than the federally mandated 75-hour minimum (IOM, 2001).
Organizational Culture
Initiatives to improve the organizational culture of nursing homes focus on the values that determine organizations behavior, the relationships between internal and external stakeholders, traditions, what is rewarded and punished in the organization, and the norms of behavior (Bowers, 2001). While extrinsic rewards may draw individuals into an organization to work, the satisfaction that they receive while on the job (e.g., from the organizational culture) contributes to longer job tenure (Bowers, 2001; Walsh, Abrahams, & Capitman, 1994). Productive relationships with supervisors and coworkers, opportunities for teamwork, and respect have been identified as potentially important intrinsic factors that would improve job tenure (Dawson, 2007; Stone & Wiener, 2001).
A number of nursing homes are attempting to change their organizational culture by involving workers in decisions, empowering workers, and providing more feedback, autonomy, and respect (Eaton, 2001; McGuire, Houser, Jarrar, Moy, & Wall, 2003). Many of these initiatives (such as the Eden Alternative, the Wellspring Model, the Pioneer Network, and Green House homes) focus mainly on improving quality of care, but these approaches have important spillover effects on the workforce (Anderson et al., 2004; Barba, Tesh, & Courts, 2002; Kane, Lum, Cutler, Degenholtz, & Tu, 2007; National Commission on Nursing Workforce for Long-Term Care, 2005; Thomas & Stermer, 1999). Although primarily a provider initiative, some states have provided financial incentives for nursing homes to replicate these models (Stone & Wiener, 2001). North Carolina has implemented a state licensure program to reward providers that meet higher standards for workplace culture and performance goals in areas of training, supportive workplaces, career development opportunities, and balanced workloads; the vision is to link the voluntary license to higher reimbursement (American Association of Homes and Services for the Aging, 2007).
Recruiting Certain Types of Workers
In many parts of the country, a significant portion of the candidates for direct care work are new immigrants, minorities, women transitioning from welfare to work, and others facing significant barriers to employment (U.S. GAO, 2001). Currently, we know little about what attracts workers to the long-term care field, other than the fact that many are drawn by their desire to help people (Bowers, 2001; Pindus, Dyer, Ratcliffe, Trutko, & Isl, 1997; Squillace, Bercovitz, et al., 2007). Determining effective recruitment strategies is important given high worker replacement costs (Seavey & Salter, 2006). States are experimenting with several strategies, such as conducting broad educational and marketing initiatives to reach populations from whom workers are traditionally drawn, and developing worker registries to provide providers and consumers with a centralized list of qualified and screened workers (Harmuth & Dyson, 2005). In addition, recent evidence suggests that tapping nontraditional worker pools, such as men, students, and older people, may help alleviate the worker shortage (Kirby, Pavetti, Max, & Gregory, 2005).
Other Variables Affecting Job Tenure
The research literature suggests that there may be other variables that affect job tenure and turnover, including facility and local labor market characteristics (Castle, 2006; Grau, Chandler, Burton, & Kolditz, 1991; Gray & Phillips, 1996; Kash, Castle, Naufal, & Hawes, 2006). In terms of facility characteristics, some advocates argue that nonprofit nursing facilities are more mission driven than for-profit facilities and have higher staffing and other characteristics that may increase job tenure (Harrington, Wollhandler, Mullan, Carillo, & Himmelstein, 2001; Hillmer, Wodchis, Gill, Anderson, & Rochon, 2005). Similarly, facilities with higher staffing ratios are associated with higher quality of care, which may increase job tenure among certified nursing assistants (IOM, 2001, 2003). By a similar logic, facilities with a high proportion of private pay and Medicare residents may have more resources to spend on resident care and on certified nursing assistants, which may lead to longer job tenure among certified nursing assistants.
At the local labor market level, certified nursing assistants make choices among the employment options available to them (Kash et al., 2006). Thus, geographic areas with high unemployment rates may have longer job tenure among certified nursing assistants because there are not other employment options available. Similarly, geographic areas with a high supply of nursing homes and home care agencies may have lower job tenure in each facility because certified nursing assistants have other options for similar employment if they become dissatisfied with their current job (Gray & Phillips, 1996; Kash et al., 2006).
Purpose
The purpose of this study is to assess factors that may increase job tenure of CNAs in nursing homes. This study focuses on wages and benefits, training, and organizational culture as policy interventions that may increase the supply and job tenure of CNAs. We use multivariate regression to analyze data that merge information on nursing homes, CNAs, and local market conditions. The major advance of this research over other studies is its use of a nationally representative sample of CNAs within a nationally representative sample of nursing homes. All previous studies have been of local or regional samples that were not representative of the country as a whole. In brief, among other variables, increasing wages and benefits has a consistently positive impact on job tenure.
CONCEPTUAL FRAMEWORK
A number of conceptual models have been proposed to examine job tenure and turnover (Lok & Crawford, 2001; Mathieu & Zajac, 1990; Price, 2000; and, Tett & Meyer, 1993). In this paper, we hypothesize that job tenure of CNAs is influenced by (1) extrinsic rewards of their job (e.g., wages and fringe benefits); (2) training and career development (e.g., initial training and mentoring); (3) organizational culture (e.g., ability to work in teams); (4) reasons for being a CNA; and (5) demographic/personal, facility, and market characteristics (Exhibit 1). The analysis focuses heavily on the policy levers available to government decisionmakers and providers, such as wages and benefits, organizational culture, and training. Demographic, facility, and market characteristics are primarily control variables in the analysis. For example, whether the facility is located in an area with high unemployment is not a factor that health care policymakers can affect.
| EXHIBIT 1: Factors Affecting Job Tenure of CNAs in Nursing Homes |
 |
DATA AND METHODS
Data Sources. This study linked 2004 data from the National Nursing Home Survey (NNHS), the National Nursing Assistant Survey (NNAS), and the Area Resource File (ARF). We used the NNHS, which serves as the sampling frame for the NNAS, to obtain facility-level data about the organizations for which the CNAs worked. The NNHS is a national probability survey of nursing facilities conducted periodically by the National Center for Health Statistics (U.S. NCHS, 2007). The sample included 1,500 nursing facilities selected using systematic sampling with probability proportional to their bed size.
We used the NNAS to obtain information on the characteristics of CNAs, their compensation, and their view of the work environment. The NNAS, sponsored by the U.S. Department of Health and Human Services Office of the Assistant Secretary for Planning and Evaluation and conducted in partnership with the National Center for Health Statistics, is the first national survey of CNAs working in nursing homes (Squillace et al., 2006). The survey provides information on CNAs personal characteristics, work experience, reasons for entering the field, job characteristics and rewards, working conditions, job satisfaction, and why they leave the field.
The NNAS sample used a two-stage probability design. In the first stage, a randomly selected subsample of 790 of the 1,500 nursing homes in the NNHS sample were selected to participate in the NNAS. Of these, 208 facilities were deleted from the sample for ineligibility or nonparticipation in the NNHS or NNAS. The remaining 582 facilities provided a list of CNAs for sampling, yielding a facility response rate of 76 percent.
In the second stage, a sample of CNAs was selected randomly from each of the 582 facilities. A total of 4,542 CNAs were selected to participate in the NNAS. Of those selected, 4,274 were eligible and 3,017 completed an interview, yielding a response rate among those eligible of 70.6%, and a combined NNHS/NNAS response rate of 53%. Data were collected through telephone interviews between September 2004 and January 2005. The sample of 3,017 respondents, when weighted, represents 702,500 CNAs.
We obtained data on market characteristics of each nursing facility from the 2004 ARF to control for differences across areas. These data included each areas unemployment rate, health care resource supply factors proportionate to the respective populations served, and whether an area was metropolitan.
Dependent Variable. Most studies addressing continuity of employment use a measure of job turnover--usually a percentage of staff who leave their employer during a year (Castle, 2006). In contrast, since the NNAS is a cross-sectional survey of individuals rather than facilities, this study uses a measure of job tenure, which examines length of time in a job. An OLS regression model was estimated on the number of months a certified nursing assistant had their current job using a variable derived from the NNAS. This model was estimated for the total sample (n=2,221), and for the subgroup of respondents with at least 1 year of job tenure at their nursing home (n=1,312). CNAs with a year or more of tenure have successfully completed any initial probationary period and may be more committed to the facility and to the field. CNAs with less than a year of tenure may decide that their job was not a good fit and leave, or supervisory facility staff may decide to terminate the employment relationship.
Independent Variables. Tenure of CNAs was hypothesized to be motivated by the extrinsic rewards of their job, initial training and mentoring, reasons for being a certified nursing assistant, organizational culture, personal characteristics, facility characteristics, and the market characteristics of the area in which the facility is located. Extrinsic rewards, such as wages and benefits offered, provide the concrete rewards of employment. Initial training and mentoring and the reasons for becoming a certified nursing assistant could affect job performance as well as attitudes about the job and the employer. Organizational culture factors, such as workers relationships with their supervisors and the responsibilities of the job, also potentially affect decisions about job tenure. Personal characteristics, such as immigration status or whether workers care for dependent children or elders, also may affect job tenure. Facility characteristics, such as ownership type and the percentage of Medicaid residents (possibly a proxy for lower resident reimbursement or for chronic care residents), may affect the quantity and quality of resources available for performing their job and, therefore, affect tenure. Characteristics of the geographic area, such as whether the facility is in a rural area and the availability of similar types of jobs, also may affect job tenure.
Statistical Issues. We estimated the descriptive statistics and regressions for the sample using the NNAS probability weights and survey design adjustments in SAS. Respondents used in the total sample for regressions numbered 2,221 of the original 3,017. Most of the 796 observations excluded from the sample were missing data on various extrinsic reward and organization culture variables, with few data missing on personal characteristics. There were no significant differences in the length of tenure, the dependent variable, for respondents with missing vs. non-missing data in either the whole sample, or among respondents with one year of tenure or more. The dependent variable in the analysis, the number of months worked in the current job, ranged from 1 month to 300 months. This variable was not normally distributed, with few CNAs having long lengths of tenure; as a consequence, the regression was estimated using the log transformation of the variable to reduce skewness.
To retransform the logged estimates of the number of months of tenure back to the normal (unlogged) scale, we applied Duans (1983) smearing factor to obtain an unbiased estimate of the number of months of tenure. A smearing factor, which is the mean squared error resulting when retransforming coefficients from the logged to the normal scale, was applied to each regression coefficient to correctly calculate the magnitude of the effect, which otherwise would be too small.
RESULTS
In descriptive statistics, job tenure in the current facility differed for the total sample (26.0 months) and for the subgroup with at least a year of tenure (54.2 months) (Table 1). These two groups differed little on variables relating to extrinsic rewards, training, organizational culture, reasons for being a certified nursing assistant, and characteristics of their facility and area. Notably, the average hourly wage rate between the two groups differed by only 35 cents ($10.34 for the total sample versus $10.69 for those with at least 1 year of tenure). In terms of personal characteristics, CNAs in the total sample, when compared to the longer job tenure subgroup, were more likely to be younger, never married, and to receive any public benefits, such as Food Stamps.
Table 2 presents the logged regression results for the total sample and for the subgroup with at least 1 year of tenure by substantive domain. Table 3 presents the unlogged smeared regression coefficients for the same regressions for only the variables significant at p0.05. This table shows the magnitude of the effect of each variable.
Overall, all domains of interest had at least one, and in some cases several, variables that were statistically associated with tenure. The R-square value ranged from 0.314 to 0.329. The degrees of freedom ranged between 436 and 450. However, several of the hypothesized variables did not have the expected effect, and the overall effect size of the significant variables was modest. All significant variables had an effect on job tenure of less than 3 months.
Among the domains that can be directly influenced by policy makers, extrinsic rewards had the largest number of significant variables (four). Only one training and one organizational culture variable significantly affected job tenure. Significant variables in domains not readily influenced by policy (such as personal characteristics and characteristics of the facility and surrounding market area) were often significant in both regressions.
Extrinsic Rewards. Overall, the variables in this domain, such as higher wages, paid time off, and availability of a pension, have a consistently positive effect on job tenure in both regressions. For example, for the total sample, a $1 increase in wages is associated with 2.1 additional months of tenure and 1.5 additional months for the longer job-tenure subgroup. However, a $1 increase in wages would require a large increase in labor costs.
Receiving paid personal or vacation days and paid holidays as part of the benefit package has a significant effect on tenure for the total sample, but did not affect tenure for the subgroup with at least 1 year of tenure. However, receiving a pension benefit has a significant effect in both regressions. Each of these benefits independently produces about 2 additional months of employment in the facility. Surprisingly, health insurance coverage was not significant in either regression.
Training, Organizational Culture, and Reasons for Becoming a Certified Nurse Assistant. In terms of training, having a mentor in their first (not necessarily the current) job was a significant predictor of job tenure, adding about 2 months in the total sample and 1.6 months for the subgroup of respondents. However, a self-reported assessment of how well their initial training prepared them for their job was not significant.
Variables denoting positive aspects of organizational culture, such as respect received, working in teams, and the potential for deciding how to do their work, were not significant in any of the models. Unexpectedly, the variable working in a facility that valued the work of CNAs either very much or somewhat was negatively significant in the total sample, resulting in 2 months less tenure than those who reported no such positive attitude in their facility.
Among several reasons for choosing work as a certified nursing assistant, in the total sample, those who entered the field for job security were predicted to stay about 2 months longer than those who chose the work because they liked to help others. CNAs whose primary reason for entering the field was a desire to work in health care did not differ in tenure from those who entered the field because they wanted to help others.
Personal Characteristic of CNAs. Several personal characteristics of CNAs were significant predictors of job tenure. Nursing assistants younger than 30 and males had shorter tenure in both the total sample and the longer job-tenure subgroup. In the total sample, CNAs with more than a high school education or GED had shorter job tenure, while in the subgroup, immigrants had shorter job tenure. The size of these effects ranged from roughly 2 to 3 months. CNAs aged 45 and older had longer job tenure, but this may be related to older persons having had the opportunity to work for a longer period than younger persons.
Facility Characteristics. Two facility-level variables were associated with increased tenure. First, and unexpectedly, the percentage of nursing home residents covered by Medicaid had a positive and significant effect on job tenure of almost 2 additional months. Second, the presence of special units in the facility, such as programs for palliative care, continence management, dementia or Alzheimers disease, had a significant and positive effect of 2 additional months of employment for the total sample only. These programs may signify a more sophisticated organization with dedication to providing better quality care and to training its employees. On the other hand, the three variables representing hours of care per resident day for CNAs, registered nurses, and licensed practical nurses were not significantly associated with longer tenure.
Market Characteristics. Three market characteristics positively affected job tenure. The county unemployment rate was positively associated with longer tenure; a 1 percentage point increase in the unemployment rate increased tenure between 1.4 and 1.7 months for the subgroup and total sample of respondents, respectively. The supply of certified nursing home beds per 1,000 older people increased tenure between 1.3 and 1.7 months for the subgroup and total sample of respondents, respectively. Moreover, the supply of home health agencies per 1,000 older people also increased tenure by 1.7 months for the subgroup and 2.2 months for the total sample of respondents. Home health agencies presumably offer a competing opportunity for employment, although home health aides are generally less well paid and receive fewer fringe benefits (Montgomery, Holley, Deichert, & Koloski, 2005).
| TABLE 1. Descriptive Statistics | |||||
| Category | Variable | Total Samplen=2,221 | Tenure >1 Yearn=1,312 | ||
| Mean | Std Error | Mean | Std Error | ||
| Tenure | Number of months employed in current facility | 25.96 | 1.04 | 54.21 | 1.03 |
| Extrinsic Rewards | Hours worked per week | 36.85 | 0.23 | 37.22 | 0.28 |
| Wage rate | 10.34 | 0.11 | 10.69 | 0.11 | |
| Sick leave benefit | 0.70 | 0.02 | 0.72 | 0.02 | |
| Paid holidays off | 0.72 | 0.02 | 0.76 | 0.02 | |
| Paid personal/vacation days | 0.85 | 0.01 | 0.89 | 0.01 | |
| Pension benefit available | 0.62 | 0.02 | 0.65 | 0.02 | |
| Paid bonuses available | 0.37 | 0.02 | 0.37 | 0.02 | |
| Enhanced package of benefits (childcare/transport/assistance) | 0.38 | 0.03 | 0.39 | 0.03 | |
| Health insurance partially paid for CNA only | 0.79 | 0.02 | 0.80 | 0.02 | |
| Health insurance fully paid for CNA only | 0.12 | 0.02 | 0.12 | 0.02 | |
| Health insurance not paid for CNA only | 0.09 | 0.01 | 0.08 | 0.01 | |
| Health insurance partially paid for CNA & family | 0.64 | 0.03 | 0.65 | 0.03 | |
| Health insurance fully paid for CNA & family | 0.04 | 0.02 | 0.05 | 0.02 | |
| Health insurance not paid for CNA & family only | 0.32 | 0.02 | 0.70 | 0.02 | |
| Training | Assigned a mentor for first job | 0.81 | 0.01 | 0.81 | 0.01 |
| Initial training prepared well (omitted) | 0.66 | 0.01 | 0.66 | 0.02 | |
| Initial training prepared somewhat well | 0.31 | 0.01 | 0.31 | 0.02 | |
| Initial training prepared not at all well | 0.03 | 0.00 | 0.03 | 0.01 | |
| Organizational Culture | Supervisor a reason to work there | 0.62 | 0.01 | 0.63 | 0.02 |
| Coworkers a reason to work there | 0.78 | 0.01 | 0.78 | 0.02 | |
| Respected/rewarded for their work | 0.70 | 0.01 | 0.70 | 0.02 | |
| Respected by supervisor as part of team | 0.95 | 0.01 | 0.95 | 0.01 | |
| Supervisor supports NA working in teams | 0.84 | 0.01 | 0.85 | 0.01 | |
| NA can decide how to do their work | 0.90 | 0.01 | 0.91 | 0.01 | |
| NA is involved in challenging work | 0.92 | 0.01 | 0.92 | 0.01 | |
| Organization values their work as NA | 0.93 | 0.01 | 0.93 | 0.01 | |
| Reason for Being NA | Society values their work as an NA | 0.88 | 0.01 | 0.88 | 0.01 |
| Imp reason for being NA--helping others (omitted) | 0.63 | 0.01 | 0.62 | 0.02 | |
| Imp reason for being NA--work in health care | 0.08 | 0.01 | 0.07 | 0.01 | |
| Imp reason for being NA--job security | 0.08 | 0.01 | 0.09 | 0.01 | |
| Imp reason for being NA--other reason | 0.21 | 0.01 | 0.22 | 0.01 | |
| Worker Characteristics | Age under 30 | 0.30 | 0.01 | 0.22 | 0.01 |
| Age 30-45 (omitted) | 0.36 | 0.01 | 0.37 | 0.02 | |
| Age over 45 | 0.33 | 0.01 | 0.40 | 0.02 | |
| Male gender | 0.08 | 0.01 | 0.07 | 0.01 | |
| Minority race | 0.44 | 0.02 | 0.45 | 0.02 | |
| Hispanic | 0.10 | 0.01 | 0.09 | 0.01 | |
| Less than high school | 0.13 | 0.01 | 0.13 | 0.01 | |
| High school degree or GED (omitted) | 0.61 | 0.01 | 0.62 | 0.02 | |
| More than high school or GED | 0.26 | 0.01 | 0.24 | 0.02 | |
| Married (omitted) | 0.52 | 0.02 | 0.54 | 0.02 | |
| Widowed or divorced/separated | 0.22 | 0.01 | 0.24 | 0.02 | |
| Never married | 0.26 | 0.01 | 0.22 | 0.01 | |
| Immigrant | 0.19 | 0.02 | 0.21 | 0.02 | |
| Main language not English | 0.11 | 0.01 | 0.11 | 0.01 | |
| Any public benefits | 0.31 | 0.01 | 0.28 | 0.01 | |
| Care for dependent child or elder | 0.40 | 0.02 | 0.39 | 0.02 | |
| Facility Characteristics | For-profit status | 0.58 | 0.03 | 0.58 | 0.03 |
| More than 100 beds in facility | 0.65 | 0.01 | 0.65 | 0.02 | |
| CNA hours per patient per day | 2.06 | 0.03 | 2.06 | 0.03 | |
| RN hours per patient per day | 0.39 | 0.01 | 0.40 | 0.01 | |
| LPN hours per patient per day | 0.63 | 0.02 | 0.62 | 0.02 | |
| Percent of residents primarily paid for by Medicaid | 0.69 | 0.06 | 0.71 | 0.09 | |
| Any special units in facility | 1.15 | 0.02 | 1.16 | 0.02 | |
| Administrator with special certification | 1.74 | 0.03 | 1.73 | 0.03 | |
| CNAs with special training | 1.52 | 0.03 | 1.53 | 0.03 | |
| Area Characteristics | Nonmetropolitan area | 0.15 | 0.01 | 0.14 | 0.01 |
| Unemployment rate | 5.59 | 0.11 | 5.58 | 0.10 | |
| Number of certified beds per 1,000 elderly | 54.82 | 1.01 | 55.00 | 1.01 | |
| Number of home health agencies per 1,000 elderly | 0.23 | 0.01 | 0.22 | 0.01 | |
| Number of hospital beds per 1,000 population | 3.46 | 0.12 | 3.44 | 0.12 | |
| SOURCE: Authors analysis of merged 2004 National Nursing Home Survey, National Nursing Assistant Survey and Area Resource File. | |||||
| TABLE 2: OLS on Logged Number of Months in Facility | |||||
| Category | Variable | Whole Samplen=2,221 | Tenure >1 Yearn=1,312 | ||
| Coefficient | Std Error | Coefficient | Std Error | ||
| Extrinsic Rewards | Hours worked per week | 0.00 | 0.00 | 0.00 | 0.00 |
| Wage rate | 0.23 | 0.02* | 0.15 | 0.01* | |
| Sick leave benefit | -0.06 | 0.08 | 0.07 | 0.07 | |
| Paid holidays off | 0.21 | 0.07* | 0.09 | 0.06 | |
| Paid personal/vacation days | 0.32 | 0.10* | -0.05 | 0.08 | |
| Pension benefit available | 0.26 | 0.07* | 0.18 | 0.07* | |
| Paid bonuses available | 0.03 | 0.07 | -0.02 | 0.06 | |
| Enhanced package of benefits (childcare/transport/assistance) | -0.07 | 0.07 | -0.05 | 0.06 | |
| Health insurance partially paid for CNA only | 0.02 | 0.11 | -0.10 | 0.09 | |
| Health insurance fully paid for CNA only | 0.00 | 0.14 | -0.12 | 0.10 | |
| Health insurance partially paid for CNA & family | -0.05 | 0.08 | -0.07 | 0.06 | |
| Health insurance fully paid for CNA & family | -0.39 | 0.27 | -0.14 | 0.16 | |
| Training | Assigned a mentor for first job | 0.18 | 0.08* | 0.18 | 0.07* |
| Initial training prepared well (omitted) | --- | --- | --- | --- | |
| Initial training prepared somewhat well | 0.02 | 0.07 | 0.02 | 0.06 | |
| Initial training prepared not at all well | -0.03 | 0.16 | 0.00 | 0.14 | |
| Organizational Culture | Supervisor a reason to work there | -0.02 | 0.08 | -0.04 | 0.07 |
| Coworkers a reason to work there | 0.07 | 0.09 | 0.09 | 0.07 | |
| Respected/rewarded for their work | -0.05 | 0.08 | 0.11 | 0.07 | |
| Respected by supervisor as part of team | -0.03 | 0.18 | -0.19 | 0.14 | |
| Supervisor supports NA working in teams | 0.09 | 0.09 | -0.03 | 0.09 | |
| NA can decide how to do their work | 0.15 | 0.10 | 0.10 | 0.09 | |
| NA is involved in challenging work | 0.04 | 0.12 | 0.11 | 0.11 | |
| Organization values their work as NA | -0.29 | 0.12* | -0.01 | 0.12 | |
| Reason for Being NA | Society values their work as an NA | 0.17 | 0.10 | 0.11 | 0.10 |
| Important reason for being NA--helping others (omitted) | --- | --- | --- | --- | |
| Important reason for being NA--work in health care | -0.14 | 0.12 | -0.04 | 0.10 | |
| Important reason for being NA--Job security | 0.19 | 0.09* | 0.07 | 0.08 | |
| Important reason for being NA--other reason | 0.03 | 0.08 | -0.05 | 0.07 | |
| Worker Characteristics | Age under 30 | -0.44 | 0.10* | -0.41 | 0.07* |
| Age 30-45 (omitted) | --- | --- | --- | --- | |
| Age over 45 | 0.53 | 0.09* | 0.34 | 0.07* | |
| Male gender | -0.41 | 0.12* | -0.31 | 0.10* | |
| Minority race | 0.11 | 0.08 | 0.11 | 0.06 | |
| Hispanic | -0.11 | 0.12 | -0.02 | 0.11 | |
| Less than high school | 0.08 | 0.10 | 0.08 | 0.09 | |
| High school degree or GED (omitted) | --- | --- | --- | --- | |
| More than high school or GED | -0.22 | 0.09* | -0.12 | 0.07 | |
| Married (omitted) | --- | --- | --- | --- | |
| Widowed or divorced/separated | -0.03 | 0.09 | -0.03 | 0.07 | |
| Never married | -0.09 | 0.08 | -0.01 | 0.07 | |
| Immigrant | -0.01 | 0.12 | -0.21 | 0.08* | |
| Main language not English | -0.04 | 0.15 | 0.09 | 0.12 | |
| Any public benefits | -0.08 | 0.07 | -0.01 | 0.06 | |
| Care for dependent child or elder | -0.09 | 0.06 | -0.05 | 0.06 | |
| Facility Characteristics | For profit status | 0.04 | 0.07 | -0.01 | 0.06 |
| More than 100 beds in facility | 0.09 | 0.07 | 0.07 | 0.06 | |
| CNA hours per patient per day | 0.06 | 0.06 | 0.06 | 0.05 | |
| RN hours per patient per day | -0.23 | 0.15 | -0.11 | 0.12 | |
| LPN hours per patient per day | 0.06 | 0.12 | 0.03 | 0.10 | |
| Percent of residents primarily paid for by Medicaid | 0.04 | 0.01* | 0.02 | 0.01* | |
| Any special units in facility | 0.23 | 0.10* | 0.13 | 0.09 | |
| Administrator with special certification | 0.00 | 0.07 | 0.05 | 0.07 | |
| CNAs with special training | 0.11 | 0.07 | 0.08 | 0.06 | |
| Area Characteristics | Nonmetropolitan area | 0.03 | 0.07 | 0.08 | 0.06 |
| Unemployment rate | 0.04 | 0.02* | 0.03 | 0.01* | |
| Number of certified beds per 1,000 elderly | 0.00 | 0.00* | 0.00 | 0.00* | |
| Number of home health agencies per 1,000 elderly | 0.26 | 0.12* | 0.25 | 0.12* | |
| Number of hospital beds per 1,000 population | 0.00 | 0.01 | 0.00 | 0.01 | |
| Constant | -1.01 | 0.47* | 1.20 | 0.36* | |
| R-square | 0.31 | 0.33 | |||
| SOURCE: Authors analysis of merged 2004 National Nursing Home Survey, National Nursing Assistant Survey and Area Resource File. p0.05* | |||||
| TABLE 3: Change in Variables With Statistically Significant Results in Multivariate Analysis Ordinary Least Squares on Number of Months in Facility | ||
| Change in Months | ||
| Total Sample (n = 2,221) | Tenure >1 Year (n = 1,312) | |
| Extrinsic rewards | ||
| Wage rate | 2.1 | 1.5 |
| Paid holidays off | 2.1 | |
| Paid personal/vacation days | 2.3 | |
| Pension benefit available | 2.2 | 1.6 |
| Training | ||
| Assigned a mentor for first job | 2.0 | 1.6 |
| Organizational culture | ||
| Organization values their work as CNA | -2.2 | |
| Reason for being CNA | ||
| Important reason for being CNA--job security | 2.0 | |
| Worker characteristics | ||
| Younger than 30 | -2.6 | -2.0 |
| Older than 45 | 2.8 | 1.9 |
| Male gender | -2.5 | -1.8 |
| More than high school or GED | -2.1 | |
| Immigrant | -1.6 | |
| Facility characteristics | ||
| Percent of residents paid for primarily by Medicaid | 1.7 | 1.4 |
| Any special units in facility | 2.1 | |
| Area characteristics | ||
| Unemployment rate | 1.7 | 1.4 |
| Number of certified beds per 1,000 elderly people | 1.7 | 1.3 |
| Number of home health agencies per 1,000 elderly people | 2.2 | 1.7 |
| SOURCE: Authors analysis of merged 2004 National Nursing Home Survey, National Nursing Assistant Survey, and Area Resource File. NOTE: CNA = certified nursing assistant; GED = General Equivalency Diploma. | ||
DISCUSSION
This study uses the NNHS, the NNAS, and the ARF to analyze the determinants of job tenure using multivariate analyses. Our findings suggest that extrinsic rewards appear to be the most consistent determinants of job tenure, although some elements of job training and organizational culture, the personal characteristics of CNAs, and other characteristics of nursing homes and the local market area are also factors. In general, this study of job tenure finds fewer significant variables than studies that analyze turnover rates (Bostick et al., 2006; Brannon, Zinn, Mor, & Davis, 2002; Castle, 2006; Castle & Engberg, 2007; Kash et al., 2006).
Individual variables that were statistically significant in increasing job tenure had an effect size of 1-3 months. While the additional job tenure resulting from any single predictor variable does not seem large, an individual CNA might have several factors that increase job tenure because they work for a facility or have personal characteristics that increase job tenure. Therefore, some CNAs might have their job tenure increase by 6 months or more as a result of having this constellation of factors. For example, nursing assistants who worked for facilities that provide paid days off and a pension plan and paid $1 more per hour than the average CNA, and were assigned mentors in their first job might have job tenure about six months higher than CNAs who work for nursing homes that do not provide these extrinsic rewards. CNA respondents without these four factors are likely to have less than the average job tenure (26 months), so the effect of these four factors on job tenure for people without them would be to potentially increase their job tenure by 25 percent. Given the high proportion of nursing assistants with short tenure, if more CNAs had several of these job tenure-increasing factors, then overall length of time on the job might increase substantially.
Especially because CNAs tend to have low incomes (two thirds of NNAS respondents report family income under $30,000) (Squillace, Harris-Kojetin, et al., 2007), it is not surprising that extrinsic rewards, such as wages, time off, and pensions, are important determinants of job tenure. An adequate wage is important for workers facing financial hardship and many other low-paying service jobs offer few fringe benefits. Employer health insurance was not a significant variable, which may reflect participation in Medicaid and the State Childrens Health Insurance Program. In addition, the significant effect of the unemployment rate in both regressions underlines that CNAs make choices among their available options, and when jobless rates are higher, they are more likely to stay at their jobs because other employment may be unavailable. The finding that entering the field for job security had longer job tenure relative to entering the field primarily to help others is consistent with this finding.
These findings fit with economic theory and are technically easy to address. For example, nursing homes know how to implement wage increases and increase time off. However, someone must pay for higher wages and benefits, and doing so will be costly, both to providers and the government. In particular, Medicare and Medicaid pay for the care of 78% of nursing home residents (American Health Care Association, 2007), so wage increases and more fringe benefits for CNAs will most likely require higher reimbursement levels from the two public programs. Given competing national priorities, obtaining those funds will be difficult.
Some observers have argued that higher wages and better fringe benefits may be necessary to recruit direct care workers, but once employed, workers want to feel valued by the organization and society. In order to feel competent and needed, these employees may need more and better training as well as nursing homes that have a more responsive and empowering organizational culture. Contrary to our expectations, relatively few of our organizational culture and training variables were statistically significant. Among the training variables, only having a mentor in the first job as a certified nursing assistant was statistically significant. Among the organizational culture variables, the organization values their work as a nursing assistant was significant but unexpectedly negative for the whole sample, and not significant for persons with at least 1 year of tenure. These results may reflect the relative weakness of the organizational culture movement in nursing homes in 2004, the time of the survey.
Although not readily changeable, several personal characteristics of CNAs were statistically significant, including age, gender, education, and immigration status. The negative effect of more than a high school education on job tenure suggests that more educated CNAs may view these jobs as temporary entry-level employment before moving on to either more education or jobs with more potential for advancement. While being an immigrant did not greatly affect the length of job tenure, it was a significant negative variable for the long-stay CNAs. Other analyses of the NNAS suggest that immigrant CNAs are more highly educated than native-born CNAs (Khatutsky, Squillace, Anderson, & Wiener, 2007). It is possible that, like more educated CNAs, immigrants use these jobs as a transition to better opportunities. Strategies to increase the supply of direct care workers through higher immigration rates may result in workers with shorter job tenure.
Some facility characteristics, such as the degree of dependence on Medicaid and whether there were any type of special care units or programs, also significantly affect job tenure, but staffing levels were not significant. Given that understaffing is a common critique of nursing homes (U.S. Health Care Financing Administration, 2000; Wiener, Freiman and Brown, 2007) that directly affects the day-to-day life of direct care workers, it was expected that staffing levels would be associated with job tenure.
The finding that CNAs who work in facilities with a higher percentage of Medicaid residents have longer tenure was not expected, since it is often argued that these facilities have lower quality (Harrington et al., 2001). This variable, however, may be correlated with case mix in that Medicaid patients may have less intensive medical care needs and may be easier to care for. Another possible explanation is that staff develop stronger attachments to the long-stay, chronic care residents in high-percentage Medicaid facilities, providing satisfaction that leads them to stay on the job.
Finally, the market area in which CNAs work also has an effect on job tenure. Beyond the unemployment rate, both the number of certified nursing home beds and number of home health agencies per 1,000 older people were positively related to job tenure. We expected the direction would be negative; the more providers in the area, the more likely that CNAs would leave their job if dissatisfied and find work in another facility or home health agency.
The major advance of this study over other studies of tenure and turnover is its use of a nationally representative sample of CNAs within a nationally representative sample of nursing homes. All previous studies have been of local or regional samples that were not representative of the country as a whole (e.g., Brannon et al., 2002; Castle, 2005; Harrington & Swan, 2003). Nonetheless, this study has three limitations. First, this is a study of job tenure derived from a cross sectional survey rather than a study of job turnover. By definition, the length of job tenure at the time of the survey is not complete and persons with short job tenure are underrepresented in the sample. A cohort study would provide additional valuable insights about how and why CNAs remain in their particular positions and is highly recommended when longitudinal data become available.
Second, the level and type of disability of residents may have an important impact on job tenure but the NNHS is not designed to produce facility-level estimates of resident disability, so those variables are absent from our equations. Third, the motivating interest in job tenure and turnover comes from the widely held belief that turnover and job tenure have an impact on quality of care in nursing homes, but the lack of quality measures on the two surveys does not allow for the direct testing of that relationship in this paper.
In conclusion, the care of the 1.5 million persons in nursing homes in the United States is largely in the hands of CNAs. In the current system, turnover is high, which may adversely affect residents. This study underscores the importance of the basic economics of job choice by low-income workers. Wages, fringe benefits, job security, and alternative choices of employment are important determinants of job tenure that need to be addressed, in addition to improvements in training and organizational culture.
REFERENCES
American Association of Homes and Services for the Aging. (2007). Better jobs better care: Building a valued, committed workforce. Washington, DC: Author.
American Health Care Association. (2003). Results of the 2002 AHCA survey of nursing staff vacancy and turnover in nursing homes. Washington, DC: Author.
American Health Care Association. (2007). Nursing facility patients by payor--number of patients, CMS OSCAR data current surveys, June 2007. Washington, DC: Author. Available at: http://www.ahcancal.org/research_data/oscar_data/NursingFacilityPatientC... .
Anderson, W. L., Wiener, J. M., Greene, A. M. & OKeeffe, J. (2004). Direct service workforce activities of the Systems Change grantees. Report prepared for the Centers for Medicare and Medicaid Services. Research Triangle Park, NC: RTI International.
Atchley, R. C. (1996). Frontline workers in long-term care recruitment, retention and turnover: Issues in an era of rapid growth. Oxford, OH: Scripps Gerontology Center.
Barba, B., Tesh, A. & Courts, N. (2002). Promoting thriving in nursing homes: The Eden Alternative. Journal of Gerontological Nursing, 28, 7-13.
Bostick, J. E., Rantz, M. J., et al. (2006). Systematic review of studies of staffing and quality in nursing homes. Journal of the American Medical Directors Association, 7, 366-376.
Bowers, B. (2001). Organizational change and workforce development in long-term care. Paper prepared for the Urban-Institute and Institute for the Future of Aging Services Technical Expert Panel on Organizational Culture Change. Madison, WI: University of Wisconsin.
Bowers, B. J., & Becker, M. (1992). Nursing assistants in nursing homes: The relationship between organization and quality. The Gerontologist, 32, 360-366.
Brannon, D., Zinn, J. S., Mor, V., & Davis, J. (2002). An explanation of job, organizational, and environmental factors associated with high and low nursing assistant turnover. The Gerontologist, 42, 159-168.
Castle, N. G. (2005). Turnover begets turnover. The Gerontologist, 45, 186-195.
Castle, N. G. (2006). Measuring staff turnover in nursing homes. The Gerontologist, 46, 210-219.
Castle, N. G., & Engberg, J. (2006). Organizational characteristics associated with staff turnover in nursing homes. The Gerontologist, 46, 62-73.
Castle, N. G., & Engberg, J. (2007). The influence of staffing characteristics on quality of care in nursing homes. Health Services Research, 42, 1822-1847.
Castle, N. G., Engberg, J., Anderson, R., & Men, A. (2007). Job satisfaction of nurse aides in nursing homes: Intent to leave and turnover. The Gerontologist, 47, 193-204.
Castle, N., Engberg, J., and Men, A. (2007). Nursing home staff turnover: Impact on Nursing Home Compare quality measures. The Gerontologist, 47, 650-661.
Centers for Medicare & Medicaid Services. (2002). Appropriateness of minimum staffing ratios in nursing homes. Baltimore, MD: Author.
Dawson, S. (2007). Recruitment and retention of paraprofessionals. A presentation to the Institute of Medicines Committee on the Future Health Care Workforce for Older Americans. Bronx, NY: Paraprofessional Health Care Institute.
Decker, F. H., Dollard, K., & Kraditor, K. (2001). Staffing of nursing services in nursing homes: Present issues and prospects for the future. Seniors Housing & Care Journal, 9, 3-26.
Duan, N. (1983). Smearing Estimate: A nonparametric retransformation method. Journal of the American Statistical Association, 78, 605-610.
Eaton, S. (2001). What a difference management makes! Nursing staff turnover variation within a single labor market. Chapter 5 in Centers for Medicare and Medicaid Services, Report to Congress: Appropriateness of Minimum Nurse Staffing Ratios in Nursing Homes Phase II Final Report. Baltimore: Centers for Medicare & Medicaid Services.
Ehrenberg, R. & Smith, R. (1997). Modern labor economics: Theory and public policy. New York: Addison Wesley.
Grau, L., Chandler, B., Burton, B. & Kolditz, D. (1991). Institutional loyalty and job satisfaction among nurse aides in nursing homes. Journal of Aging and Health, 3, 47-65.
Gray, A. M. & Phillips, V. L. (1996). Labour turnover in the British National Health Service: A local labour market analysis. Health Policy, 36, 273-289.
Harmuth, S., & Dyson, S. (2005). Results of the 2005 national survey of state initiatives on the long-term care direct-care workforce. Brooklyn, NY: Paraprofessional Healthcare Institute.
Harrington, C., Kovner, C., Mezey, M., Kayser-Jones, J., Burger, S., Mohler, M., et al. (2000). Experts recommend minimum nurse staffing standards for nursing facilities in the United States. The Gerontologist, 40, 5-16.
Harrington, C., & Swan, J. H. (2003). Nursing home staffing, turnover, and case mix. Medical Care Research and Review, 60, 366-392.
Harrington, C., Woolhandler, S., Mullan, J., Carrillo, H., & Himmelstein, D. U. (2001). Does investor ownership of nursing homes compromise the quality of care? American Journal of Public Health, 91(9), 1452-1455.
Harris-Kojetin, L., Lipson, D., Fielding, J., Kiefer, K. & Stone, R. (2004). Recent findings on frontline long-term care workers: A research synthesis 1999-2003. Washington, DC: Office of the Assistant Secretary for Planning & Evaluation, U.S. Department of Health and Human Services. Available at: http://aspe.hhs.gov/daltcp/reports/insight.htm .
Hecker, D. E. (2005). Occupational employment projections to 2014. Monthly Labor Review, 128 , 70-101.
Hillmer, M. P., Wodchis, W. P., Gill, S. S., Anderson, G. M., & Rochon, P. A. (2005). Nursing home profit status and quality of care. Medical Care Research and Review, 62, 139-166.
Hollinger-Smith, L. (2002). Evaluation of the LEAP replication study. Evanston, IL: Mather Institute on Aging.
Holzer, H. (2001). Long-term care workers and the low-wage labor market: Current characteristics and future trends. Washington, DC: The Urban Institute and the Institute for the Future of Aging Services.
Howes, C. (2005). Living Wages and Retention of Homecare Workers in San Francisco. Industrial Relations, 44, 139-63.
Howes, C. (2006). Wages, benefits and flexibility matter: Building a high quality home care workforce. Better Jobs, Better Care. Washington, DC: American Association of Homes and Services for the Aging.
Institute for the Future of Aging Services. (2007). The long-term care workforce: Can the crisis be fixed. Washington, DC: National Commission for Quality Long-Term Care.
Institute for the Future of Aging Services & the Paraprofessional Healthcare Institute. (2005). Workforce strategies No. 3. The role of training in improving the recruitment and retention of direct care workers in long-term care. Washington DC: Author.
Institute of Medicine. (2001). Improving the quality of care in nursing homes. Washington, DC: National Academy Press.
Institute of Medicine. (2003). Keeping patients safe: Transforming the work environment of nurses. Washington, DC: National Academy Press.
Johnson, R. W., Toomey, D., and Wiener, J. M. (2007). Meeting the long-term care needs of the Baby Boomers: How changing families will affect paid helpers and institutions. Washington, DC: The Urban Institute. Available at: http://www.urban.org/UploadedPDF/311451_Meeting_Care.pdf .
Kane, R. A., Lum, T. Y., Cutler, L. J., Degenholtz, H. B. & Tu, T.-C. (2007). Resident outcomes in small-house nursing homes: A longitudinal evaluation of the initial Green House program. Journal of the American Geriatrics Society, 55, 832-839.
Kash, B. A., Castle, N. G., Naufal, G. S., & Hawes, C. (2006). Effect of staff turnover on staffing: A closer look at registered nurses, licensed vocational nurses, and certified nursing assistants. The Gerontologist, 46(5), 609-619.
Khatutsky, G., Squillace, M. R., Anderson, W. L., & Wiener, J. M. (2007). Personal characteristics and the work environment. Presented at the Gerontological Society of American Annual Meetings, San Francisco, CA, November 19.
Kirby, G., Pavetti, L., Max, J., & Gregory, J. (2005). TANF recipients as potential long-term care workers: An assessment of the prospects in the District of Columbia, Illinois, Maryland and South Carolina. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. Available at: http://aspe.hhs.gov/daltcp/reports/TANFltc.htm .
Konrad, T. R. & Morgan, J. C. (2004). Workforce improvement for nursing assistants: Supporting training, education, and payment for upgrading performance. Chapel, NC: University of North Carolina Institute on Aging.
Kramer, A., Eilertsen, T., Lin, M., & Hutt, E. (2000). Effects of nurse staffing on hospital transfer quality measures for new admissions. In Health Care Financing Administration Report to Congress: Appropriateness of Minimum Nurse Staffing Ratios In Nursing Homes. Baltimore, MD: Health Care Financing Administration.
Leon, J., Marainen, J., & Marcotte, J. (2001). Pennsylvanias frontline workers in long term care: The provider perspective. A Report to the Intergovernmental Council on Long-term Care. Philadelphia, PA: Polisher Research Institute at the Philadelphia Geriatric Center.
McCallion, P., Toseland, R. W., Lacey, D., & Banks, S. (1999). Educating nursing assistants to communicate more effectively with nursing home residents with dementia. The Gerontologist, 39, 546-558.
McGuire, M., Houser, J., Jarrar, T., Moy, W. & Wall, M. (2003). Retention: Its all about respect. Health Care Manager, 22, 38-44.
Montgomery, R. J. V., Holley, L., Deichert, J., & Koloski, K. (2005). A profile of home care workers from the 2000 Census: How it changes what we know. The Gerontologist, 45, 493-600.
National Commission on Nursing Workforce for Long-Term Care. (2005). Act now for your tomorrow: Final report of the National Commission on Nursing Workforce for Long-Term Care. Washington, DC: American Health Care Association.
Noel, M., Pearce, G., & Metcalf (2000). The effect of educational and staffing interventions on the CNA workforce. Journal of the American Medical Directors Association, 1, 241-247.
Pillemer, K. (1996). Solving the frontline crisis in long-term care. Cambridge, MA: Frontline Publishing Company.
Pindus, N. M., Dyer, D., Ratcliffe, C., Trutko, J., and Isl, K. (1997). Industry and cross-industry mobility: Experiences, trends and opportunities for low-wage workers in health, hospitality and child care. Washington, DC: The Urban Institute. Available at: http://www.urban.org/publications/407375.html .
Seavey, D., & Salter, V. (2006). Paying for quality care: State and local strategies for improving wages and benefits for personal care assistants. Washington, DC: AARP.
Schirm, V., & Garland, T. (1997). Nurses perceptions of the role of nurse assistants in delivery of quality care in the nursing home. Presented at the annual meeting of the Midwest Sociological Society, Des Moines, IA, April 3-6.
Squillace, M., Bercovitz, A., Remsburg, R., & Rosenoff, E. (2007). Nurse aide retention: What do the workers say? Working Paper. Washington, DC: Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services.
Squillace, M., Harris-Kojetin, L., Rosenoff, E., Han, B., & Remsburg, R. (2007). A national profile of certified nursing assistants working in U.S. nursing homes: Results from the 2004 National Nursing Assistant Survey. Working Paper. Washington, DC: Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services.
Squillace, M., Remsburg, R., & Bercovitz, A. (2006). An introduction to the National Nursing Assistant Survey. Washington, DC: The U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. Available at: http://aspe.hhs.gov/daltcp/reports/2006/NNASintro.htm .
Stone, R., Reinhard, S. C., Bowers, B., Zimmerman, D., Phillips, C. D., Hawes, C., et al. (2002). Evaluation of the Wellspring Model for improving nursing home quality. New York: The Commonwealth Fund.
Stone, R., & Wiener, J.M. (2001). Who will care for us? Addressing the long-term care workforce crisis. Washington, DC: The Urban Institute and the Institute for the Future of Aging Services. Available at: http://aspe.hhs.gov/daltcp/reports/ltcwf.htm .
Thomas, W., & Stermer, M. (1999). Eden Alternative principles hold promise for the future of long-term care. Balance, 3, 14-17.
U.S. General Accounting Office. (2001). Nursing workforce recruitment and retention of nurses and nurse aides is a growing concern. Testimony before the Committee on Health, Education, Labor and Pensions, U.S. Senate. Washington, DC: U.S. General Accounting Office.
U.S. Health Care Financing Administration. (2000). Report to Congress: Appropriateness of minimum nurse staffing ratios in nursing homes. Baltimore: U.S. Department of Health and Human Services.
U.S. National Center for Health Statistics. (2007). National Nursing Home Survey: Public-use data files. Hyattsville, MD: Author. Available at: http://www.cdc.gov/nchs/products/elec_prods/subject/nnhs.htm .
Walsh, E. G., Abrahams, R., & Capitman, J. (1994). Recruitment and retention of paraprofessional home care workers: The effects of agency type and working conditions. Waltham, MA: Brandeis University.
Wiener, J. M., Freiman, M. P., & Brown, D. (2007). Nursing home care quality: Twenty years after the Omnibus Budget Reconciliation Act of 1987. Washington, DC: Henry J. Kaiser Family Foundation. Available at: http://www.kff.org/medicare/upload/7717.pdf .
To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human ServicesOffice of Disability, Aging and Long-Term Care PolicyRoom 424E, H.H. Humphrey Building200 Independence Avenue, S.W.Washington, D.C. 20201FAX: 202-401-7733Email: webmaster.DALTCP@hhs.gov
RETURN TO:
Office of Disability, Aging and Long-Term Care Policy (DALTCP) Home [http://aspe.hhs.gov/_/office_specific/daltcp.cfm]Assistant Secretary for Planning and Evaluation (ASPE) Home [http://aspe.hhs.gov]U.S. Department of Health and Human Services Home [http://www.hhs.gov]