
U.S. Department of Health and Human Services
Use of the 1989 National Long-Term Care Survey for Examining Cognitive Impairment Eligibility Criteria
Mary Elizabeth Jackson, The MEDSTAT Group
Pamela Doty, U.S. Department of Health and Human Services
July 1995
This report was prepared under contract between HHS's DALTCP and the MEDSTAT Group. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the office at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. The e-mail address is: webmaster.DALTCP@hhs.gov. The Project Officer was Pamela Doty.
Presented at the 25th Public Health Conference on Records and Statistics and the National Committee on Vital and Health Statistics 45th Anniversary Symposium, July 17-19, 1995, Mayflower Hotel, Washington, D.C. Published in "Data Needs in an Era of Health Reform," Proceedings of the Public Health Conference on Records and Statistics, U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Center for Health Statistics, Rockville, MD, 1995.
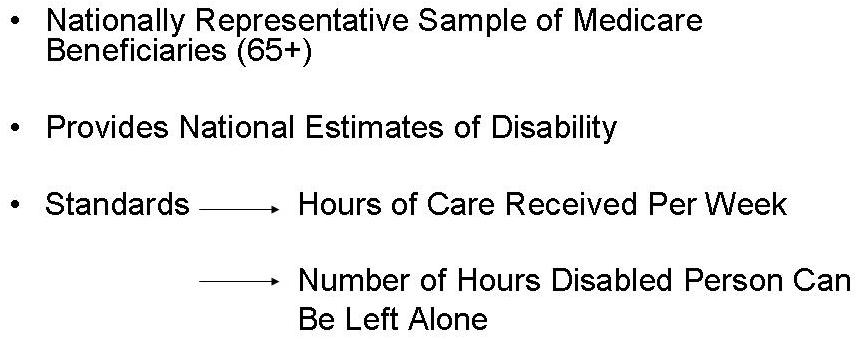
Analyses of the 1989 National Long-Term Care Survey (NLTCS) and its companion Informal Caregiver Survey (ICS) were used to examine the comparability of the cognitive impairment eligibility criteria to the 3+ ADL criteria in the Clinton Administration's long-term care health reform proposal from the Health Security Act. Also addressed by these analyses is the extent to which functional indicators, i.e. ADLs, by themselves, are sufficient for identifying both the physically disabled and severely cognitively impaired population. The NLTCS was used because it provides a nationally representative sample of Medicare beneficiaries age 65+ in 1989 that allows for the generation of national estimates on this population.
The Criteria. The Health Security Act (HSA) specified that a person would be eligible for long-term care benefits outlined in the plan if s/he was disabled in 3 or more ADLs out of five (bathing, dressing, toileting, transferring, eating) or experienced a comparable level of severe cognitive impairment. The bill stated that eligibility based on severe cognitive impairment was to be indicated by a standard mental status protocol(s) indicating severe cognitive impairment, PLUS one of the following: 1 or more ADLs out of the core five (bathing, dressing, toileting, transferring, eating); a serious behavior problem(s) that creates the need for supervision to prevent harm to the individual or others; or an IADL indicating some cognitive impairment.
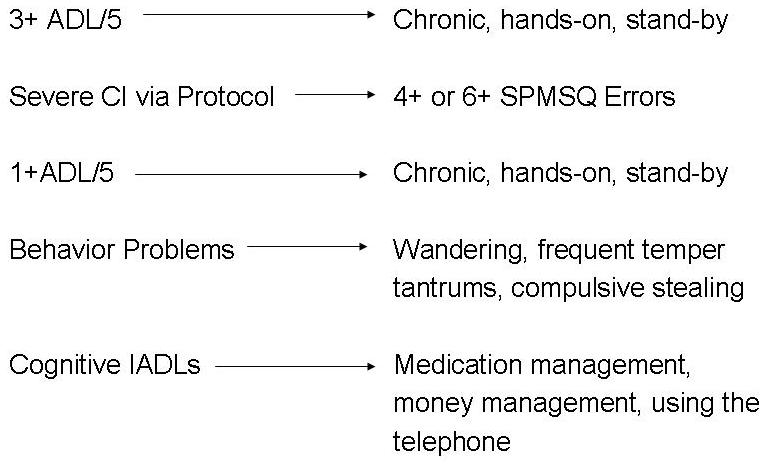
Operationalizing the Criteria. First, we attempted to operationalize these eligibility criteria using the data items available in the 1989 NLTCS and ICS. The five ADLs specified in the Health Security Act are available in the data set; disability in each ADL was defined as chronic, i.e., having lasted three months or longer and requiring either hands-on or stand-by assistance for performance.
Cognitive impairment eligibility criteria were operationalized using the variant of the Short Portable Mental Status Questionnaire (SPMSQ) available in the 1989 NLTCS. This battery contains 10 items, 9 of which are identical to the SPMSQ. The one item that differs from the SPMSQ is a slightly less difficult item than appears in the original version of the instrument; as such we accept a score of 4 or more errors (rather than 5), to indicate moderate/severe impairment and a score of 6 or more to indicate severe impairment.
We were also able to operationalize the additional criteria that the HSA stipulates must be met for evidence of cognitive impairment. As previously mentioned, ADL items are readily available in the data set (for operationalizing the additional criteria of 1+ ADLs in the CI criteria). The behavior problem items available in the NLTCS are: wandering, frequent temper tantrums, and compulsive stealing. Although these items may not be those one would choose, they were the only proxies available in the dataset, and thus were used to operationalize and behavior problem criteria. And finally, the cognitive IADLs were operationalized with the medication management, money management, and telephoning items.
Comparison Standards. In order to assess whether the cognitive impairment eligibility criteria is comparable to the 3+ ADL criteria a standard of comparison must be used that in some way indicates the level of disability or impairment, other than the eligibility criteria. The NLTCS provides two sources of standards. First, is the number of hours of care per week an individual receives from all sources--from informal sources (family and friends) who are unpaid and from persons who are paid to provide care. The second measure chosen to be used as a standard is an item in ICS which asks the caregiver how many hours the disabled person can safely be left alone.
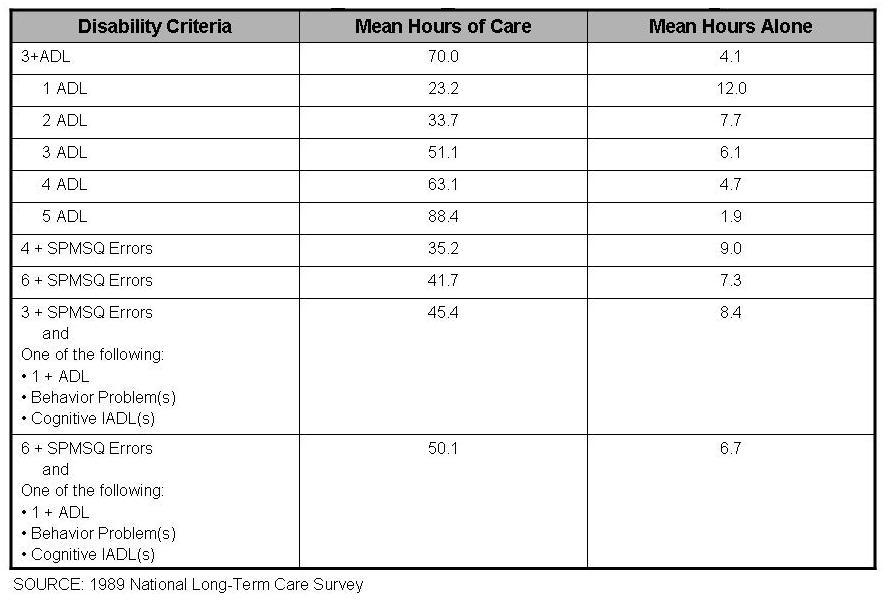
Results. Table 1 shows that persons meeting the eligibility criteria of 3 or more ADLs receive 70 hours of care per week, on average. However, this estimate includes persons with 4 and 5 ADL disabilities; because such individuals have more needs and therefore receive more hours of care, the average number of hours is somewhat inflated. In order to compare to the CI criteria a fairer approach is to use the number of hours associated with persons having 3 ADLs, which is 51.1 hours per week.
Table 1 also shows that regardless of how CI is operationalized, more loosely or more stringently, the number of hours that those with cognitive impairment receive is always less than the number of hours those with 3 or more ADL disabilities receive. The measure that comes the closest to being comparable is the one that combines behavioral evidence for the need for care/oversight with 6 or more errors on the SPMSQ. This CI measure is the most stringent as it requires evidence of more severity on the mental status protocol.
It should also be noted that the SPMSQ as a stand-alone criteria yields the poorest comparison. But when the protocol is combined with some manifestation for the need for care, comparability is enhanced.
Similar results are obtained when the comparison standard is the number of hours an individual can safely be left alone. Those with 3 ADL disabilities can be left alone for 6.1 hours, on average whereas those with 6+ MSQ errors and some evidence of the need for care can be left alone for 6.7 hours, on average.
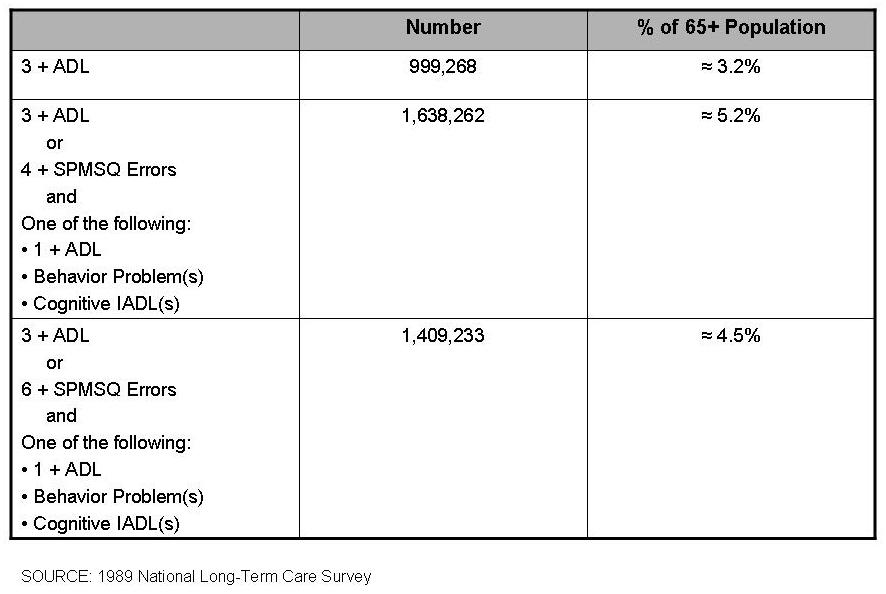
Table 2 displays the population estimates associated with the 3+ ADL disability criteria and operationalized HSA cognitive impairment criteria in conjunction with the 3+ ADL criteria. The estimates are for the 1989 aged 65 and older population. They indicate that close to one million elders (or 3.2% of the 65+ population) would be eligible for benefits if the sole criteria were 3+ ADL disabilities. When the cognitive impairment criteria are added, an additional 1.3 to 2.0 percent of the population would be eligible, depending upon the exact definition of cognitive impairment.
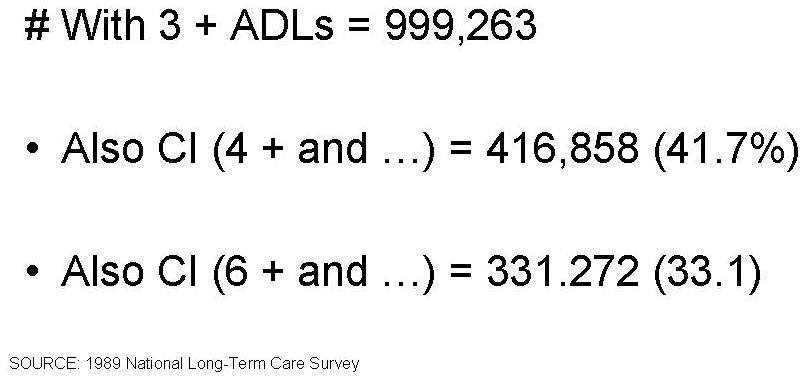
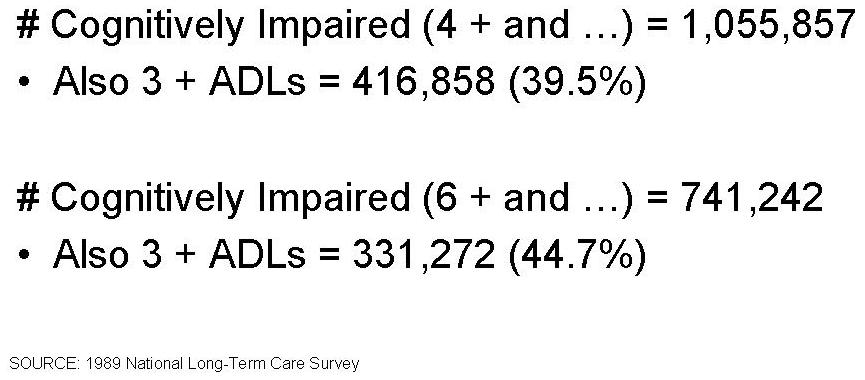
There are obviously some individuals who will meet both the 3+ ADL and CI eligibility criteria. Of those with 3 or more ADL disabilities, between one-third (33.1%) and two-fifths (41.7%) are also cognitively impaired, depending upon how CI is operationalized. And of those who meet CI criteria, approximately 2/5 are also disabled in 3 or more ADLs.
In order to examine whether ADLs might suffice as a stand-alone criteria for identifying both the physically disabled and cognitively impaired, two multiple regression analyses were conducted, one with the dependent variable being total hours of care, and the other hours the person could safely be left alone. The number of ADLs and the combined CI measures were entered as independent variables along with several control variables that are known/suspected to affect how much care a person receives. The control variables included the care recipient's age, sex and race; the primary caregiver's age, sex and relationship to the care recipient, i.e., spouse or not.
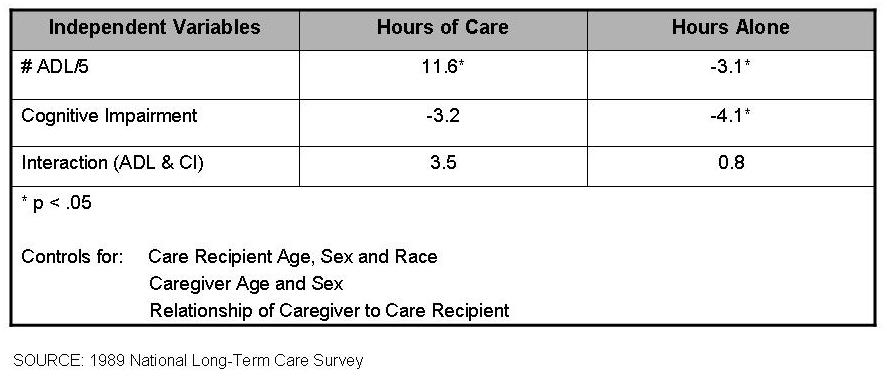
Table 3 presents the regression coefficients associated with the two key independent variables, i.e., ADLs and cognitive impairment. (Coefficients for the control variables are not shown.) These coefficients can be interpreted as the number of hours of care (or hours the care recipient can be left alone) associated with each measure. Results indicate that for each additional ADL disability there is an increase of 11.6 hours of care. Cognitive impairment, on the other hand, is associated with a decrease of 3.2 hours.
An interaction term was also included in the model. It reflects the number of hours a person who is both cognitively impaired and ADL disabled receives. The results indicate those who are cognitively impaired received 3.5 additional hours of care for each additional ADL disability.
Note that the ADL coefficient is the only one that is statistically significant. Cognitive impairment, once ADLs are taken into account, does not add significantly to the hours of care, and neither does the interaction term. ADLs are clearly the strongest predictors of the need for care.
However, the results are somewhat different when the outcome is the hours alone variable. Interestingly, each additional ADL is associated with a person being able to be left alone for 3.1 fewer hours, but cognitive impairment is associated with 4.1 fewer hours. And coefficients for both the ADL and cognitive impairment variables are statistically significant, suggesting that ADL criteria alone is not sufficient for predicting level of care need.
Discussion. The results of these analyses indicate that it may be possible to develop reasonable cognitive impairment criteria comparable to the 3+ ADL criteria, particularly if the cognitive impairment criteria are based upon indicators that reflect true need for care and/or oversight as manifested by functional and/or behavioral factors. Nevertheless, the results also suggest that ADL criteria alone are not sufficient for identifying the severely cognitively impaired, even when disability in an ADL is defined to include stand-by assistance and supervision (in addition to hands-on assistance). However, other function-based measures (e.g., some combination of ADLs and IADLs) may prove effective in identifying this population.
Finally, one must remember that these analyses were based on survey data, and that several of the items used to operationalize the eligibility criteria are proxies for indicators that would be employing in determining program eligibility. Moreover, even if there were a one-to-one correspondence between the survey items and eligibility criteria items, one would still have to offer the caveat that even the most valid criteria can identify an unintended population--in this instance the less than severely cognitively impaired--if not reliably administered, or administered as intended.
TABLES
| TABLE 1: TOTAL HOURS/WEEK OF CARE AND HOURS ALONE BY VARIOUS DISABILITY CRITERIA | ||
| Disability Criteria | Mean Hours of Care | Mean Hours Alone |
| 3+ ADL | 70.0 | 4.1 |
| 1 ADL | 23.2 | 12.0 |
| 2 ADL | 33.7 | 7.7 |
| 3 ADL | 51.1 | 6.1 |
| 4 ADL | 63.1 | 4.7 |
| 5 ADL | 88.4 | 1.9 |
| 4+ SPMSQ Errors | 35.2 | 9.0 |
| 6+ SPMSQ Errors | 41.7 | 7.3 |
| 4+ SPMSQ Errors and One of the Following:
| 45.4 | 8.4 |
| 6+ SPMSQ Errors and One of the Following:
| 50.1 | 6.7 |
| TABLE 2: NUMBER AND PERCENT OF AGED 65+ MEETING VARIOUS ELIGIBILITY CRITERIA | ||
| Criteria | Population Estimate | % of 65+ Population |
| 3+ ADL | 999,263 | ~ 3.2 |
| 4+ SPMSQ Errors and One of the Following:
| 1,638,262 | ~ 5.2 |
| 6+ SPMSQ Errors and One of the Following:
| 1,409,233 | ~ 4.5 |
| TABLE 3: PREDICTORS OF TOTAL HOURS OF HELP AND HOURS PERSON CAN BE LEFT ALONE | ||
| Independent Variables | Hours of Care | Hours Alone |
| # ADL/5 | 11.6* | -3.1* |
| Cognitive Impairment | -3.2 | -4.1* |
| Interaction | 3.5 | 0.8 |
| * p or = .05 | ||
PRESENTATION
Information taken from the presentation slides used at the Conference/Symposium.
| Eligibility Criteria |
 |
| Operalization of Eligibility Criteria |
 |
| 1989 National Long-Term Care Survey |
 |
| Number and Percent of 65+ Meeting Various Criteria |
 |
| Total Hours/Weeks of Care (All Sources) and Hours Person Can Be Left Alone by Various Disability Criteria |
 |
| Predictors of Total Hours of Help and Hours Person Can Be Left Alone |
 |
| Number and Percent of 3+ ADLers With Cognitive Impairment |
 |
| Number and Percent of Cognitively Impaired With 3 or More ADL Disabilities |
 |