
Printer Friendly Version in PDF Format (50 PDF pages)
This paper is an attachment to the U.S. Department of Health and Human Services (HHS), Office of the Assistant Secretary for Planning and Evaluation (ASPE) report "Innovative Medicaid Managed Care Coordination Programs for Co-morbid Behavioral Health and Chronic Physical Health Conditions: Final Report". Available at: https://aspe.hhs.gov/basic-report/innovative-medicaid-managed-care-coordination-programs-co-morbid-behavioral-health-and-chronic-physical-health-conditions-final-report.
TABLE OF CONTENTS
- State Medicaid Innovations for the Coordination of Care for Individuals with Co-morbid Behavioral Health and Chronic Physical Conditions
- Managed Medicaid Health Plan Innovations for the Coordination of Care for Individuals with Co-morbid Behavioral Health and Chronic Physical Conditions
- Discussion
- Center for Medicare and Medicaid Innovations Grants
- State Innovation Models Initiative
- Four Major Types of Models of Care Coordination in Medicaid
- Summary and Conclusion
APPENDICES
- APPENDIX I: Search Methodology Report
- APPENDIX II: Key Informant Interviews
LIST OF FIGURES
- FIGURE 1: Continuum of ICM and Features
LIST OF TABLES
- TABLE 1: Integrated Care Models
- TABLE 2: Characteristics of Newly Eligible Medicaid Expansion Population
- TABLE 3: Health Measures of Adults
- TABLE 4: Health Status, Access to Care and Utilization for Adults Ator Below 133% FPL
- TABLE 5: Characteristics of Currently Uninsured Individuals Expected to be Income Eligible for Medicaid and Current Medicaid Enrollees, Both with Household Incomes Less than 138% of the FPL, by Substance Use Disorder Status
ACRONYMS
The following acronyms are mentioned in this report and/or appendices.
| ACA | Patient Protection and Affordable Care Act |
|---|---|
| ACO | Accountable Care Organization |
| ADHS | Arizona Department of Health Services |
| AHIP | America's Health Insurance Plans |
| AHRQ | Agency for Healthcare Research and Quality |
| CHCS | Center for Health Care Strategies |
| CHIP | Children's Health Insurance Program |
| CIHS | Center for Integrated Health Solutions |
| CMMI | Center for Medicare and Medicaid Innovations |
| CMS | Centers for Medicare and Medicaid Services |
| CMSA | Case Management Society of America |
| CYF | Department of Children, Youth, and Families |
| DBHS | Division of Behavioral Health Services |
| DIAMOND | Depression Improvement Across Minnesota, Offering a New Direction |
| EHR | Electronic Health Record |
| FFS | Fee-For-Service |
| FPL | Federal Poverty Level |
| GI | Gastro-Intestinal |
| HARP | Health and Recovery Plan |
| HBTP | Home-Based Therapy Program |
| HMO | Health Maintenance Organization |
| ICM | Integrated Care Model |
| IMPACT | Improving Mood - Promoting Access to Collaborative Treatment |
| KDADS | Kansas Department for Aging and Disability Services |
| KDHE | Kansas Department of Health and Environment |
| MBHP | Massachusetts Behavioral Health Partnership |
| MCO | Managed Care Organization |
| MEPS | Medical Expenditure Panel Survey |
| MRT | Medicaid Redesign Team |
| NASHP | National Academy for State Health Policy |
| NCQA | National Committee for Quality Assurance |
| NHANES | National Health and Nutritional Examination Survey |
| NHCHC | National Health Care for the Homeless Council |
| OB/GYN | Obstetrics and Gynecology |
| P4P | Pay For Performance |
| PCC | Primary Care Clinician |
| PCCM | Primary Care Case Management |
| PCMH | Patient-Centered Medical Home |
| PCP | Primary Care Provider |
| PHQ-9 | Patient Health Questionnaire-9 |
| RBHA | Regional Behavioral Health Authority |
| SIM | State Innovation Models |
| SMD | State Medicaid Director |
| SMI | Serious Mental Illness |
| SSI | Supplemental Security Income |
| UPMC | University of Pittsburgh Medical Center |
BACKGROUND AND INTRODUCTION
Medicaid currently provides health and long-term care coverage for over 9.5 million low-income beneficiaries (Smith, Gifford, Ellis, Rudowitz, & Snyder, 2013). This accounts for one in six dollars spent on all health care in the United States. Managed care and other care coordination programs are increasingly being used to improve care, manage costs, and improve quality.
The role of managed care plans in Medicaid has been expanding over recent years, and states are increasingly relying on these programs to provide quality health care to their beneficiaries. Between 2001 and 2011 the proportion of beneficiaries covered by Medicaid health plans expanded from 37 percent to 51 percent (America's Health Insurance Plans [AHIP] Center for Policy & Research, 2013). Additionally, Medicaid managed care plans have recognized that to care for this population effectively and efficiently, they need to address the day-to-day challenges that impede their members' ability to navigate health systems and maintain good health (National Association of Medicaid Directors, 2014). These include a wide array of social and health factors. Social impediments include financial resources for housing and safe living conditions, clothing, transportation, and other basic needs and social service issues. Health challenges include managing multiple chronic conditions, coordinating care for physical and behavioral health, navigating complex medical systems, limited health literacy, and access and engagement with ongoing care. A number of financing challenges also persist with the often different and disconnected contracting and reimbursement models for physical and behavioral health. Reviewing recent trends in how Medicaid managed care plans are striving to improve the outcomes of care and control costs can help provide guidance on best practices and evidence-based innovations.
This environmental scan reviews four key elements of care coordination for Medicaid recipients with physical and behavioral health conditions:
-
Evidence-based approaches to care coordination.
-
Innovative managed care programs that coordinate care for individuals with co-morbid behavioral health and chronic physical conditions.
-
State Medicaid program activities that promote care coordination for individuals with complex behavioral and physical disease profiles.
-
The likely characteristics of individuals who are newly eligible for Medicaid under the Patient Protection and Affordable Care Act (ACA).
The first section establishes a framework for the review, while the second addresses a key area of interest for this report -- innovations in managed care programs in coordinating care for individuals with both physical and behavioral health conditions. The third part of this review provides insights on state Medicaid programs that may have key policy implications for improved outcomes, and the fourth explores the opportunities for expanded care coordination programs for those newly eligible for Medicaid under the ACA. A comprehensive literature review of published and gray literature has informed this report. Search methods and process are detailed in Appendix I. A series of background interviews were also conducted as a part of this environmental scan. These are included in Appendix II and also reflected throughout the report.
A SUMMARY OF THE KEY COMPONENTS OF EVIDENCE-BASED APPROACHES TO CARE COORDINATION FOR INDIVIDUALS WITH CO-MORBID BEHAVIORAL HEALTH AND CHRONIC PHYSICAL HEALTH CONDITIONS
A comprehensive review of the literature on care coordination (McDonald et al., 2007) has identified more than 40 different definitions of care coordination. From these, five key components have been described: (1) numerous participants are typically involved in care coordination; (2) coordination is necessary when participants are dependent on each other to carry out disparate activities in a patient's care; (3) to carry out these activities in a coordinated way, participants need adequate knowledge about their own and others' roles and available resources; (4) to manage all required patient care activities, participants rely on an exchange of information; and (5) the integration of care activities has the goal of facilitating appropriate delivery of health care services.
Based on this comprehensive review, McDonald et al. (2007) developed a working definition of care coordination: "Care coordination is the deliberate organization of patient care activities between two or more participants (including the patient) involved in a patient's care to facilitate the appropriate delivery of health care services. Organizing care involves the marshalling of personnel and other resources needed to carry out all required patient care activities, and is often managed by the exchange of information among participants responsible for different aspects of care."
Organizations that have demonstrated an ability to effectively provide care management and chronic care coordination include medical practices, hospitals, integrated delivery systems, state/community organizations, and health plans (Berenson & Howell, 2009). Among these organizations, however, one size does not fit all, and the diversity of populations and organizations providing these services require multiple models. Consequently, the literature on evidence-based care coordination encompasses multiple terms and concepts that are used interchangeably to describe these services (McDonald et al., 2007). Some examples include collaboration, continuity of care, teamwork approaches, disease or care management, and patient navigators.
Care coordination activities and responsibilities are determined by a range of factors. In Medicaid, contracts are established between the state and their managed care vendors and determine the scope and requirements for these services (National Association of Medicaid Directors, 2014). These contracts represent opportunities for states to procure services that are focused on both financial and quality targets (Center for Health Care Strategies [CHCS], 2014). Contracts between states and managed care organizations (MCOs) can support development of innovations that improve the coordination of care for Medicaid beneficiaries (National Association of Medicaid Directors, 2014). Contracts that establish care coordination guidelines for MCOs support development of innovations in the scope and quality of services that are available in the community (Association for Behavioral Health and Wellness, 2014).
Several models of care coordination have been developed and deployed to improve outcomes of care for those with chronic physical and behavioral health conditions. There is a high co-morbidity for behavioral health conditions and chronic physical illnesses. For people with multiple chronic conditions and/or functional limitations, care coordination necessitates a link between medical and social support services (Berenson & Howell, 2009). Medicaid recipients, for example, frequently have complex health and social needs that require coordination of both medical and community services. Medicare and Medicaid funding requires the integration of care to address the coordination needs of the dually eligible population.
McDonald et al. (2007) identify a number of essential tasks and activities for care coordination. These include assessing the patient and determining likely challenges to coordination; developing a plan that identifies coordination challenges and organizes separate care plans; identifying the participants and specifying their roles and responsibilities for care coordination; communicating with the patient and all other participants to ensure the exchange of information on all aspects of care; executing a care plan and implementing the coordination interventions; monitoring and adjusting care to address coordination failures; and evaluating health outcomes, including identifying coordination problems that have impacted outcomes. The Case Management Society of America (CMSA) (Kathol, Parez, & Cohen, 2010) has developed a care coordination framework that assesses an individual's health risks and needs. Through an assessment of the biological, psychological, social, and health systems domains, the CMSA model examines the historical, current state, and future vulnerability of the individual. This framework helps identify candidates for care management and target interventions to improve health outcomes.
The opportunities and challenges for implementing care coordination differ among the organizations that provide these services. For example, Medicaid can mandate care coordination through its contractual arrangements but is limited in its ability to directly provide these services. MCOs are able to coordinate care within the plan or through delegated services at the provider level but may be limited by the information that is available to them. All MCOs have access to broad population-based claims and utilization data and to member data available through administrative sources. However, most do not have detailed clinical information on their covered beneficiaries and must aggregate other forms of patient information through direct contacts with providers. Health systems are able to coordinate care at the patient-level since they have access to health information through electronic records and sources that are directly linked to their systems of care. However, providers are sometimes challenged by a lack of robust health information technologies, and often restricted by the lack of information from outside their systems.
Information systems that provide direct access to patient-level information are a cornerstone of care coordination. Yet, there are limitations on what information is available to payers and providers and who has access to this data. MCOs have population-based enrollment information as well as individual and aggregated claims data. This is useful for the identification and stratification of high-risk patients but does not provide the necessary detail for full care coordination. For example, MCOs can identify through claims and encounter data that a covered beneficiary has a diagnosis of diabetes. From these sources they can also determine if that patient has had an annual eye exam, but they are not likely to have full access to the results of these tests. Providers have access to direct patient-level information through their clinical records, including electronic medical records, care registries, and fee-for-service billing records; however, they do not generally have access to the details of care provided outside of their practices. As an example, when a primary care physician refers a diabetic patient for an annual eye exam and the exam occurs outside the physician's practice, the physician is dependent on referral response letters and other forms of communications for the results.
Root causes for poor care coordination have been reported (Burton, 2012) and exist at both the provider and payer level. Generally, health systems and provider organizations have different electronic health records (EHRs) and technology platforms. This makes it difficult for hospitals to effectively transmit patient information to physician offices. While substantial progress has been made toward developing health information exchange systems to facilitate sharing health care data across provider systems, these efforts are still far from universal availability or widespread use (Dullabh et al., 2012). As a result, primary care providers (PCPs) often do not know that transitions in care have occurred, the results of specialty consultations and services, or changes made in their patient's medications or treatment plans. Care coordination is also difficult between payers and provider systems for many of the same reasons. Payers are also constrained by the timeliness of the encounter and claims data that they have access to.
Care coordination requires effective communication and transfer of health information between levels of care. A review of studies tracking the availability of hospital discharge data noted that only 12-34 percent of physicians reported having their patient's discharge information at their first post-discharge visit (Kripalani et al., 2007). Further, when the patient's health information was available, providers noted deficiencies and gaps, including follow-up plans, test results, and discharge information. Nevertheless, rapid advancements in electronic health information, meaningful use standards, health information exchanges, and technology incentive programs are helping to address these deficiencies and promote opportunities for improved care coordination. Also, although historically there have been few financial incentives or penalties for the failure to transmit information that would support effective care coordination (Burton, 2012), recent policy initiatives to reduce hospital reimbursements for short-term re-admissions are providing incentives for improved coordination of care.
Health care is provided in acute hospital facilities, outpatient offices and clinics, and long-term care settings, and in both general health care and across a broad range of specialist health care settings (e.g., cardiac, GI, dental, mental). This care is often fragmented, not well coordinated, and patients migrate across multiple systems of care based on clinical needs. As they do, their social needs and functional limitations travel with them and require variable levels of social support (Shier, Ginsburg, Howell, Volland, & Golden, 2013). To achieve quality health outcomes, uninterrupted attention to patient's health and social needs is required. Evidence supports the argument that coordinated efforts to identify and meet the social needs of patients will generate lower health care utilization and costs and result in better health outcomes. For Medicaid covered beneficiaries the availability of social and other safety-net services are key components of care coordination and improved health outcomes (National Association of Medicaid Directors, 2014; CHCS, 2014).
Care coordination can occur at both the provider and health plan (payer) level. In addition, community-based collaborations have been developed to include broad groups of stakeholders. Some of these have successfully addressed integrating care for physical and behavioral health conditions.
At the provider level there are a range of evidence-based care coordination programs that support improved health outcomes. The Chronic Care Model (Wagner, 1998) establishes the key roles of informed and active patients, and prepared and proactive practice teams that bring together the resources of health systems and community supports. Together this collaborative and team-based approach supports the integration of care across the continuum of physical and behavioral health. The application of this model to behavioral health conditions has also been expanded to include key elements of empowerment, recovery, and resiliency (Daniels, Adams, Carroll, & Beinecke, 2009).
Specific care coordination programs have been developed at the provider level for behavioral health care and the integration of primary care services. The Improving Mood - Promoting Access to Collaborative Treatment (IMPACT) model of care was developed in a national treatment trial focused on improved treatment outcomes for depression in older adults (Grypma, Little, Haverkamp, & Unützer, 2006). This framework has gained broad application across diverse populations and the five key elements of the IMPACT model are as follows:
-
Collaborative care, which is the cornerstone of the IMPACT model. The patient's PCP works with the patient and a care manager and develops and implements a treatment plan that includes medications and/or evidence-based psychotherapy. The care manager and the PCP work with a consulting psychiatrist to adapt the care plan as needed.
-
A central role for a depression care manager. This role can be provided by a range of professionals and supported by paraprofessionals. Key functions include educating patients about depression, supporting anti-depressant medications prescribed by the PCP, monitoring and tracking depression symptoms, coaching and activation support, brief problem-solving counseling, and relapse prevention.
-
A designated psychiatrist who serves as a consultant to the care manager, the PCP, and patient.
-
Outcome measurement that is monitored by the care manager. The IMPACT model is built around the use of the PHQ-9 to assess response to care but recognizes that there are other effective tools.
-
Stepped care, which adjusts treatment based on clinical outcomes on an evidence-based algorithm. If the patient does not experience significant improvement at 10-12 weeks, changes are made to the treatment plan, including changes in dosages or types of medications, addition of psychotherapy, or other modifications that are proposed by the team psychiatrist.
The results of the IMPACT trial found significant improvement for patients participating in this collaborative depression care model when compared to those receiving routine care. A meta-analysis of 37 randomized controlled trials (Gilbody, Bower, Fletcher, Richards, & Sutton, 2006) concluded that there was sufficient evidence to demonstrate the effectiveness of this collaborative care model when compared to routine care.
An initiative in Minnesota to implement a care model for depression deemed to be effective in the IMPACT trial was examined by Solberg et al. (2013). The Depression Improvement Across Minnesota, Offering a New Direction (DIAMOND) initiative, a community collaborative of stakeholders from clinical services, payers, employers, and others, was implemented in 75 primary care clinics. Based on the findings of the IMPACT trial, six key components of depression care were adopted:
-
The use of standard, reliable, and validated screening tools for the assessment and management of depression (for this project the PHQ-9 was utilized).
-
Systematic patient follow-up based on the use of the assessment tool (a patient registry was used to provide tracking of cases).
-
Evidence-based guidelines and a stepped care approach for treatment.
-
A care manager to provide education for staff, coordinate care, and troubleshoot services for patients with depression.
-
A relapse prevention plan for patients ready to move out of the care management program.
-
Psychiatric consultation available for all care.
In an approach to redesign systems of care, a care manager was made available to provide education and self-management support, promote stepped care, coordinate care across primary and behavioral health clinicians, and provide relapse prevention. Payment redesign was also a cornerstone of the DIAMOND program. This included directing payment and reimbursements for activities proven to lead to better outcomes, including care coordination and team-based care. Other redesign components included covering care manager and consulting psychiatrist costs, bundled services and a single billing code used at certified DIAMOND sites, and periodic payments to the medical group that were invisible to the patient. A review of the progress of this initiative across the 75 primary care clinics implementing the DIAMOND program demonstrated that outcomes are improved when primary care clinics are prepared with the necessary tools and resources to implement evidence-based care for depression and financial barriers are reduced (Solberg et al., 2013). However, it is also important to note that this program is available for commercially insured patients and generally not available to Medicaid recipients of care.
These examples demonstrate how care coordination for physical and behavioral health conditions can be provided at the provider, payer, and community collaborative levels. This includes the development and payment for resources that support care coordination, psychiatric consultation, and team-based care. Medicaid managed care offers opportunities and challenges for MCOs and providers to build innovative care coordination programs. Based on established principles described above, states, MCOs, and providers are working to improve the integration of care for those with chronic physical and behavioral health conditions.
A SUMMARY DESCRIPTION OF ANY INNOVATIVE MANAGED CARE PROGRAMS THAT COORDINATE CARE FOR INDIVIDUALS WITH CO-MORBID BEHAVIORAL HEALTH AND CHRONIC PHYSICAL CONDITIONS
Continually escalating costs are leading state Medicaid plans to increasingly consider managed care options. External factors are also influencing how health plans are able to care for covered beneficiaries (Silow-Carroll & Rodin, 2013). A review of four Medicaid managed care plans yielded three common goals: improve care coordination, access, and delivery; strengthen the community and safety-net infrastructure; and prevent illness and reduce disparities. These plans also used their covered population data as a source to identify gaps in care and help engage communities in designing interventions and resources to address the needs of beneficiaries. They also note that state Medicaid programs can be helpful in promoting goals, priorities, and guidelines that foster technical assistance and community engagement.
Medicaid managed care plans have been at the forefront of designing and implementing programs to improve care and outcomes for patients with chronic illnesses. These programs go well beyond those that have been developed in commercial plans, and have shown favorable results. Some of these plans are reported in AHIP Center for Policy and Research Capitol Hill briefing, Health Plan Innovations: Caring for Medicare and Medicaid Patients with Chronic Illnesses (2012). Representatives from four Medicaid health plans described innovative tools and techniques for helping patients manage chronic illnesses and avoid unnecessary hospitalizations, re-admissions, visits to emergency rooms, and care facility stays. Three main themes described in this report include the following:
-
Traditional models of care must be adjusted to meet the unique needs of patients with complex conditions, particularly those who are dually eligible for Medicare and Medicaid.
-
To achieve better health outcomes and avoid preventable hospitalizations among patients with chronic conditions, it is important to address not only individuals' medical needs but also other challenges -- such as transportation, affordable housing, hunger, health literacy, and home safety -- that affect patients' ability to manage their conditions.
-
Success in improving the health and well-being of patients with chronic illness requires careful coordination of services, regular follow-up with patients and physicians, and support from a multidisciplinary team of professionals and paraprofessionals that often includes one-on-one, in-person contacts.
State Medicaid Innovations for the Coordination of Care for Individuals with Co-morbid Behavioral Health and Chronic Physical Conditions
Care coordination is becoming a universal attribute across most state Medicaid programs (Smith et al., 2013). In a review of state plans for Medicaid transformation, the Kaiser Commission on Medicaid and the Uninsured's 50-state Medicaid budget survey for state fiscal years 2013 and 2014 found that 40 states reported new or enhanced care coordination activity or initiatives. Strategies for care coordination at either the MCO or provider levels are common, and principal goals include reducing fragmentation and improving coordination across behavioral and physical health care. States have a unique ability to leverage the type and focus of care coordination activities through their contracts with MCOs (National Association of Medicaid Directors, 2014).
The Kaiser survey reports that Medicaid is the single largest source of financing for behavioral health services. Among non-elderly adults, per beneficiary spending is significantly higher for those with a co-occurring mental health diagnosis than for those without. Further, an earlier Kaiser survey found that over 60 percent of non-elderly Medicaid covered adults with a diagnosed mental health condition also have a diagnosed chronic physical condition (Kaiser Family Foundation, 2010).
At the state level, contracting mechanisms represent the best opportunity for Medicaid to foster innovation with their MCO vendors (National Association of Medicaid Directors, 2014). For behavioral health, a range of carve-in and carve-out arrangements have been developed. In some cases these services have been carved out from the contracted Medicaid MCOs and provided by a statewide specialty vendor. Other states are fully integrating these services within a single health plan.
Recently, some states are following a strategy of eliminating existing carve-out of behavioral health programs (Kaiser Family Foundation, 2010). Other states are deploying strategies to use expanded behavioral health organization models. These programs are tasked with supporting the coordination of care across physical (acute and primary care) and behavioral health services (mental health and addictions) and monitoring outcomes on established metrics. Other state-based approaches include the implementation of administrative service organizations to manage behavioral health services. Health home models are also being developed to improve coordination of care for those with behavioral health conditions, including serious mental illness (SMI) and substance use conditions.
States are implementing different managed Medicaid innovations to promote the coordination of care for physical and behavioral health conditions (National Association of Medicaid Directors, 2014). At the state level, Medicaid is able to direct innovation in care coordination through system design and contracting mechanisms. State examples below provide an overview of the types of initiatives that are being developed.
Arizona
The Arizona Department of Health Services/Division of Behavioral Health Services (ADHS/DBHS) serves as the single state authority to provide coordination, planning, administration, regulation and monitoring of all facets of the state public behavioral health system. DBHS contracts with community-based organizations, known as Regional Behavioral Health Authorities (RBHAs), to administer behavioral health services. RBHAs operate much like a health maintenance organization (HMO), and each RBHA contracts with a network of service providers similar to health plans to deliver a range of behavioral health care services.
In March 2013, ADHS/DBHS awarded Mercy Maricopa Integrated Care a 3-year multibillion dollar contract to provide Maricopa County Medicaid beneficiaries with SMI with fully coordinated, integrated physical and behavioral health services. Mercy Maricopa Integrated Care is a partnership between Maricopa Integrated Health Services, the county's safety-net health care system, and Mercy Care Plan, a Phoenix-based non-profit that serves the county's low-income behavioral health patients.
Originally expected to begin operations on October 1, 2013, the start date has been delayed due to legal action by the county's current RBHA. Mercy Maricopa Integrated Care is currently preparing to undertake the role of the RBHA starting April 1, 2014.
This contract is Arizona's first for integrated health. Although it only affects one county, the state is exploring implementing managed integrated physical and behavioral health care statewide for Medicaid beneficiaries with SMI. On December 9, 2013, Arizona released a request for information seeking comment on the proposed statewide expansion and is currently examining the feasibility of contracting with additional MCOs for the other five counties.
Kansas
In January 2011, Governor Sam Brownback tasked his lieutenant governor and a working group of cabinet members to fundamentally reform the state's Medicaid system to improve patient outcomes and financial sustainability. In January 2013, Kansas introduced KanCare. KanCare delivers whole-person, integrated care to nearly all of the state's Medicaid beneficiaries.
KanCare has contracted with three MCOs: Amerigroup of Kansas, Inc.; Sunflower State Health Plan; and UnitedHealthcare Community Plan of Kansas. KanCare health plans are required to coordinate all care with the goal of improving health outcomes through preventative services and screenings and managing chronic conditions, while slowing the rate of cost growth over time. In July 2014, Kansas expects its health homes initiative to be operational. Kansas's health home model will focus on providing care to Medicaid beneficiaries with SMIs to prevent hospitalizations, emergency room visits, and other costly crises responses. Services provided by the health homes include comprehensive care management, individual and family supports, referral to social and community services, care coordination, comprehensive transitional care, and health promotion. The state's managed care contractors will work with the health homes and are expected to oversee the process and use their payment data to determine which Medicaid beneficiaries will require the most care coordination.
KanCare is administered by the Kansas Department of Health and Environment (KDHE) and the Kansas Department for Aging and Disability Services (KDADS). KDHE maintains financial management and contract oversight while KDADS administers the Medicaid waiver programs for disability services, mental health and substance abuse, and state hospitals and institutions.
New York
New York State Medicaid is transitioning from all behavioral health fee for services to specialized integrated managed care plans that provide physical health, behavioral health, pharmacy, long-term care, and health homes in 2014. The state anticipates implementing two types of integrated managed care plans with specialized behavioral health features that will provide integrated physical and behavioral health services for adults and children with SMI or addiction disorders.
As part of a total revamp of the state's Medicaid system, Governor Andrew Cuomo established the New York Medicaid Redesign Team (MRT), launched in 2010, to drive the transition. MRT initiated the first phase of the transition in 2011 and launched in 2012. Phase 1 entails behavioral health organizations interacting with provider organizations to review treatment and discharge aftercare plans for Medicaid fee-for-service admissions to inpatient mental health, detoxification, and substance use rehabilitation units.
Phase 2 consists of shifting all fee-for-service behavioral health services to managed care through two models: health and recovery plans (HARPs), and other specialized integrated behavioral health physical health plans (non-HARP entities). Enrollment in both programs is targeted for April 2014 in New York City. HARPs will enroll a subset of individuals with high use of intensive services and provide all Medicaid state plan services for physical health, behavioral health, pharmacy, long-term care, and health homes. HARPs will additionally manage new 1115 Medicaid waiver benefits for Home and Community-Based 1915(i) waiver-like services that are not currently offered in the state's Medicaid plan.
Florida
In June 2013 Magellan Health Services, Inc. announced its intention to launch the Magellan Complete Care plan in Florida. The plan is a new Medicaid HMO health plan that integrates primary and behavioral health care management and aims to support those with SMI with coordinated physical and mental health care through a care coordination team. Working with its members and their doctors, counselors, family, and caregivers, Magellan Complete Care focuses on establishing goals for a healthier mental and physical life.
Member enrollment in Magellan's Medicaid HMO plan began in June 2013 in Broward County, Florida. As part of its new Medicaid managed care program, the state in September 2013 awarded Magellan several contracts to launch the Magellan Complete Care plan in eight regions that include 40 of the state's 67 counties. Implementation is expected in some time this year.
Massachusetts
Massachusetts has initiated the integration of primary care and behavioral health services and currently offers a full-risk carve-out for behavioral health and managed fee-for-service for physical health. As an alternative to integrating care through MCOs, the state contracts with behavioral health organizations to provide both physical and behavioral health services for individuals with SMI or other behavioral health needs. As part of the state's mandate of mandatory health coverage, all non-dual eligible and non-institutionalized Medicaid beneficiaries are enrolled in the state's primary care case management (PCCM) program, known as the Primary Care Clinician (PCC) plan, or in one of five MCOs.
The state contracts with a single vendor to manage behavioral health services for PCC plan enrollees and to administer the PCC plan itself. In October 2012, the state selected the Massachusetts Behavioral Health Partnership (MBHP), a ValueOptions company, for a 5-year contract to provide integrated physical and behavioral health programs, management support services, and behavioral health specialty services for the PCC Plan.
MBHP aims to increase integration of medical and behavioral health care, thereby increasing integration of treatment for mental health and substance use disorders, and to implement a care management program to assist enrollees with complex medical and/or behavioral health needs in the coordination of care. MBHP's program includes an emphasis on engaging members in total health by promoting the integration of physical and behavioral health services. MBHP's program includes a new member engagement center, health needs assessment for members, a nurse advice line, an integrated care management program, and enhanced network management activities with providers of both primary care and behavioral health.
Managed Medicaid Health Plan Innovations for the Coordination of Care for Individuals with Co-morbid Behavioral Health and Chronic Physical Conditions
A recent study of innovation in managed care plans conducted by AHIP's Center for Policy and Research (2013) looks at interventions that improve the health and well-being of Medicaid beneficiaries. Seventeen health plan examples were reviewed around three principal areas: working with community partners; addressing obesity; and caring for people with complex needs. For the purpose of this review, the cited Medicaid health plan examples that address behavioral and physical health care integration are reviewed from the perspective of the problem, the intervention, and the results. The results are those that are presented by the plans in this AHIP review, and in many cases are self-reported outcomes.
UPMC Health Plan -- UPMC for you
Problem
"UPMC for you" is the Medicaid component of the University of Pittsburgh Medical Center (UPMC) Health Plan. One specific challenge for UPMC for you has been managing health care for children in foster care, since medical records of these children often are dispersed across a range of clinics and doctors' offices. To better coordinate care for its 400 Medicaid members in foster care, UPMC for you developed a program with two central goals: (1) to create an EHR for each child; and (2) provide county case workers with much-needed information, support, and resources to ensure that children are able to receive the care that they need.
Intervention
Working with the Department of Children, Youth, and Families (CYF), UPMC for you creates an EHR for each child that enters foster care. This EHR tracks all medical, dental, and behavioral care; the records are regularly shared with CYF and provide a resource for case workers, biological parents, foster parents, placement staff, and health care providers. Recognizing that CYF case workers are the hub of care coordination, UPMC for you establishes regular collaborative meetings and provides one-to-one support to help arrange care for these children. UPMC for you care managers (nurses and social workers) work with case workers to track necessary well visits, chronic care, dental care, and behavioral health care for each child. In cases of hospitalization for behavioral health care, the program also coordinates services with the CYF case workers and care managers to support community transitions.
Results
This program has successfully created EHRs for 100 percent of those enrolled. These new technology resources support a number of improvements in health outcomes and care coordination. The impact of the program has generated an increase in well child annual visits. Prior to the inception of the program (2007-2008), 53 percent of the population had well child visits, and following the programs conclusion (2009-2010) the rate increased to 78.5 percent. The rates of dental care for the children in foster care also increased 25 percent. A modest 3.5 percent increase was noted for those receiving needed behavioral health care within 60 days. Since the program began UPMC for you reports the implementation of a variety of improvements to support the tracking and access to behavioral health services for these children. CYF case workers also report high levels of satisfaction with the program.
UPMC for you has also participated in a community-based collaborative to promote the integration of physical and behavioral health (Beckjord et al., 2011). Participating with Gateway and Unison Health Plans and ten practice sites, the collaborative screened perinatal woman at high-risk for depression. The findings from this collaborative noted that the greatest barrier to successful integration of behavioral and physical health was sharing health information because of different information technology platforms used by provider and payer systems.
Affinity Health Plan -- Beacon Health Strategies
Problem
The Affinity Health Plan found that Medicaid beneficiaries who were discharged from psychiatric hospitals often had difficulty transitioning levels of care and engaging in ongoing treatment. Some of the challenges included inadequate transportation, difficulties with medications, and lack of awareness of community support resources. Partnering with the Affinity Health Plan's behavioral health provider, Beacon Health Strategies, a safety-net program was developed.
Intervention
The home-based therapy program (HBTP) was developed to better address the unmet needs of Medicaid beneficiaries. Early interventions were provided by social workers and psychiatrists to reach out to these beneficiaries and support community re-engagement and tenure. Upon admission to a psychiatric hospital, Medicaid members receive an enrollment letter from the HBTP. Those who agree to participate in the program meet with a HBTP social worker or psychiatrist while they are in the hospital. They begin formulating discharge and level of care transitions plans. Once the patient is discharged, the HBTP clinician meets with enrollees at their home and reviews the implementation of the treatment plan and medication adherence and addresses any questions or problems.
Results
Affinity Health Plan self-reports that the findings from this program support improved outcomes for those enrolled. The range of problems addressed include both behavioral health and other social and environmental challenges. Program staff successfully coordinated care between physical and behavioral health providers, social systems supports, and other community resources. Between 2009 and 2011 the numbers of beneficiaries referred to the program increased from 207 to 805.
Aetna -- Intensive Care Management
Problem
Aetna designed its intensive care management program to reach out to Medicaid members with tailored supports to meet their needs. Often Medicaid beneficiaries have relied on emergency rooms as their primary source of care for chronic medical and behavioral health conditions. Others who have been in good health may not have used any health care services and do not have a usual place for care when they need services. Matching services with individual needs is the goal of this program.
Intervention
Seeking the root cause of the problems that impede good health is at the core of the intensive care management program. In some cases this may include fears about health conditions; in others it may be challenges to safe housing, affordable nutrition and food, and behavioral health, including both mental health and substance use conditions. Intensive care management staff conduct in-depth interviews with members to determine their health-related goals, motivations, and priorities. Care managers work collaboratively to identify barriers and develop supportive resources to meet the individual's needs. They also work with a team of providers to coordinate services from PCPs, behavioral health clinicians, pharmacists, and others to address member's needs. For those beneficiaries with less acute needs, outreach staff provide assistance in identifying health resources, scheduling routine appointments and check-ups, and routine monitoring.
Results
Aetna self-reports that this intensive care management program has shown favorable results. As of March 2012 the program has enrolled 3,500 members in five states (Arizona, Delaware, Illinois, Texas, and Virginia). In 2013 the program will be expanded to include Medicaid covered beneficiaries in Florida, California, Missouri, and Ohio.
Discussion
The published literature in reviewed journals on how managed care plans coordinate care for Medicaid beneficiaries is scant. This is due in part to competition among plans and their core service missions. As a result, health plans have been less inclined to formally publish the results of their initiatives (AHIP, 2014). In instances where their care coordination efforts have been collaborative with service delivery systems, published results are more common.
There are several examples of innovations in care coordination among Medicaid managed care plans in the gray literature. These are provided by a range of public policy and trade associations. These examples are useful in their illustration of the scope of challenges and innovations addressed. However, they are somewhat limited in the rigor of the evaluation designs and focus on outcomes.
The process for disseminating information about innovation in Medicaid care management and coordination of care for behavioral and physical health is limited by inconsistent evaluation standards. Results are in part anecdotal, and it is difficult to compare outcomes across Medicaid plans and states. These challenges should not limit ongoing innovation, and it will be important to develop consistent evaluation standards.
Best practice examples can be identified and must serve as a framework for developing and testing new frameworks. Organizations that provide leadership and oversight for Medicaid plans should continue to challenge plans to share their results and promote comparative evaluation of new programs and innovations.
A SUMMARY OF STATE MEDICAID PROGRAM ACTIVITIES THAT PROMOTE CARE COORDINATION FOR INDIVIDUALS WITH COMPLEX BEHAVIORAL AND PHYSICAL DISEASE PROFILES, INCLUDING QUALITY MEASURES AND OUTCOME TRACKING SYSTEMS
This review has identified several models that states are using to coordinate care within their Medicaid programs and highlights four of the most popular models. The Centers for Medicare and Medicaid Services (CMS) has shown a great interest in these care coordination models and has communicated guidance to state Medicaid Directors (SMDs) on how to implement them. CMS is also providing financial support through grants and awards to states that are looking to coordinate care. Since the Medicaid program is run at the state level, there is no "one size fits all" model, so CMS is working with the interested states to find a model that best works within their current goals and infrastructure.
In July 2012, CMS initiated a series of "State Medicaid Director" letters aimed at promoting integrated care models (ICMs). CMS describes ICMs as "initiatives, which could include (but are not limited to) medical/health homes, accountable care organizations (ACOs), ACO-like models, and other arrangements that emphasize person-centered, continuous, coordinated, and comprehensive care" (CMS, 2012b). CMS characterizes these ICMs as "organized and accountable care delivery and payment methodologies aligned across payers and providers to ensure effective, seamless, and coordinated care" (CMS, 2012b). To date, four letters have been released, with the most recent sent on November 22, 2013. These letters aim to initiate "a series of communications intended to strengthen our [CMS] collaborations with states to facilitate achieving better care, better health, and reduced expenditures in Medicaid programs" (CMS, 2012b) with a focus on creating ICMs.
The first SMD letter explored policy considerations for states looking to implement ICMs. CMS recognizes that ICMs have long been in existence through managed care, and the focus of the first two SMD letters was on providing guidance to states with a fee-for-service system that are looking to implement ICMs. CMS has plans to send out separate letters regarding ICM implementation within risk-bearing managed care contracts at a later date. The first SMD letter in this series was intended to provide high-level observation on how states can best act to implement ICMS by utilizing new authorities offered to them by the ACA and the importance of health information technology and quality, accountability, and outcomes measures. CMS also stresses the importance of collaboration and that ICMs are only achieved if all stakeholders partner together. While the first SMD letter gave a broad overview, the second letter looked specifically at flexibility within the Medicaid statute that supports delivery system and payment reform in fee-for-service systems.
In the second letter, CMS provides guidance and options on how states can move away from a volume-based fee-for-service structure to an ICM with financial incentives to improve beneficiary health outcomes. States can move to ICMs through new initiatives or enhance existing efforts under a Medicaid state plan amendment or use demonstration or waiver authority (CMS, 2012c). Table 1 below highlights the different tools Medicaid agencies can utilize to implement ICMs in their states. Traditionally, some states have implemented PCCM programs in an effort to coordinate a Medicaid beneficiary's care while still paying a provider's fee for service (CMS, 2012c). Because these programs usually limit a beneficiary's "free choice of providers," the PCCM programs must be run under one of the Medicaid managed care authorities (ex. Section 1905(a)(25)) or through a waiver/demonstration authority under section 1115 of the Social Security Act (CMS, 2012c). After working with some states, CMS has decided the models that provide optional Medicaid state plan PCCM services utilizing Section 1905(t)(1) can be used to implement ICMs that align financial incentives such as care coordination payments and/or shared savings without restricting beneficiary free choice of providers (CMS, 2012c).
| TABLE 1. Integrated Care Models | |||
|---|---|---|---|
| Tool | Statutory Reference | Purpose | Policy Consideration |
| ICM State Plan Amendment |
|
Option to provide ICMs to all individuals under the state plan. Ability to incentivize quality and share savings. |
|
| PCCM Contract |
|
Utilizing existing PCCM contracts to reward quality. Limits providers eligible through contract. Ability to incentivize quality and share savings. |
|
| Selective Contract Waiver |
|
Limit the number of providers eligible to offer services within the model. |
|
| 1115 Demonstration |
|
Target populations, limit geographic scope, reach target populations. |
|
| SOURCE: CMS letter to SMDs, "Integrated Care Models," 2012c. | |||
In addition to state plan amendments, waiver authority might be used to implement ICMs. Depending on the chosen model, some states may need to use a combination of state plan and waiver authority (CMS, 2012c). Utilizing 1915(b) waivers states can selectively contract with a defined set of providers among a broader pool of qualified providers. Under 1115(a) waivers states can test ICMs in specific geographical areas, limit freedom of choice, and/or vary the amount, duration, and scope of services amongst different populations (CMS, 2012b). Additional options include Targeted Case Management and Health Homes under the ACA, which are options for states interested in implementing ICMs on a smaller scale before spreading statewide (CMS, 2012c). These programs can also be designed to promote the integration of primary and behavioral health services.
The third letter provides guidance on developing shared savings methodologies for Medicaid agencies looking to implement ICMs in their states. Shared savings programs originated in Medicare and the private health insurance market as an approach to reward through payment incentives providers who better coordinate care and improve quality. Some Medicaid agencies have taken notice of this program and have looked to implement it in their states. This is a new concept, and CMS plans to work with states and provide guidance in designing a program that best fits the state's Medicaid population. However, at this time, CMS is not interested in partnering with states on shared savings proposals that are based solely on cost savings and that do not improve quality and health outcomes or that limit access to eligible beneficiaries (CMS, 2013a). The letter provided information on key structural components of a shared savings payment methodology, including the essential concepts of shared savings, how to handle distribution of payments, conducting an actuarial analysis, developing risk and gain-sharing arrangements, and targeting specific providers and populations (CMS, 2013a).
The fourth letter provides an overview of quality considerations for Medicaid agencies implementing or developing ICMs in their states. This latest letter provides a framework for quality improvement and measurement that is consistent with CMS's and the U.S. Department of Health and Human Services' approaches in these areas (CMS, 2013b). CMS recognizes that to be successful, state Medicaid programs and CMS should have a common understanding of what it means to measure, monitor, and improve the quality of health care in value-based payment models (CMS, 2013b). In this letter, CMS outlines quality improvement strategies that include the following categories: goals, interventions, metrics, targets, and transparency and feedback. CMS notes that these components should be tied together as part of a cohesive plan in the context of what is happening related to quality in a state across purchasers (CMS, 2013b). If developed and implemented properly, this plan is intended to help states identify metrics such as which areas need targeted improvement or which indicators will help identify if improvement actually took place.
Center for Medicare and Medicaid Innovations Grants
CMS's Center for Medicare and Medicaid Innovations (CMMI) is leading an initiative under the ACA to develop new payment mechanisms that will improve the overall quality of care and advance the cost effectiveness of our health care system. CMMI announced the first group of awardees for the Health Care Innovation Awards in May 2012 and the second (final) group in June 2012. These organizations will implement projects in communities across the nation that aim to deliver better health, improved care, and lower costs to people enrolled in Medicare, Medicaid and the Children's Health Insurance Program (CHIP), particularly those with the highest health care needs. Funding for these projects is for 3 years.
State Innovation Models Initiative
In February 2103, the CMMI announced six model testing, three model pre-testing, and 16 model design awardees for the State Innovation Models (SIM) initiative. Nearly $300 million will be supplied by the SIM initiative to support the development of state-based models for multi-payer payment and health care delivery system transformation, and will be broad based and focus on the Medicare, Medicaid, and CHIP population. Nearly all of these awardees mention some form of care coordination in their program descriptions. A complete listing of awardees with program descriptions is available at http://innovation.cms.gov/initiatives/state-innovations/.
Four Major Types of Models of Care Coordination in Medicaid
Figure 1 provides a visual representation of the care models with the least amount of accountability for coordinated quality and cost outcomes (going from left to right) to those models with the most amount of accountability for quality and cost outcomes. In reviewing the literature, we have identified the four most common Medicaid models to review: (1) PCCM; (2) patient-centered medical homes (PCMHs); (3) health homes; and (4) ACOs.
| FIGURE 1. Continuum of ICMs and Features |
|---|
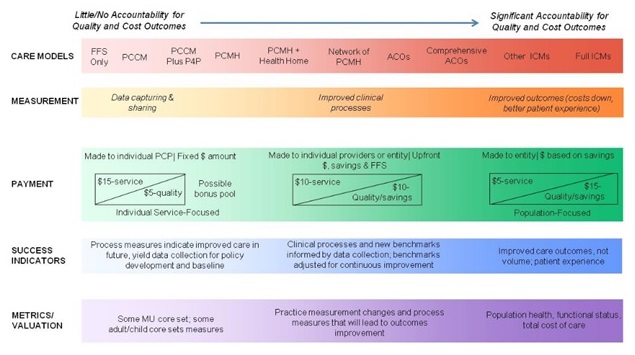 |
| SOURCE: CMS, "Continuum of New Integrated Care Models in Medicaid: Key Program Features, Medicaid and CHIP Learning Collaboratives," July 2012. |
Primary Care Case Management
Some state Medicaid programs are interested in care coordination models that do not require MCOs. PCCM programs serve this purpose and represent a combination of managed care and fee-for-services. PCCMs are designed to link Medicaid beneficiaries with PCPs, who for a flat case management fee are responsible for coordinating a limited range of care management activities. In a Technical Assistance Brief for CMS's Integrated Care Resource Center, authors Hamblin, Verdier, and Au (2011) have identified several mechanisms in which care coordination can be achieved, often in combination, including:
-
Paying PCPs enhanced fees to support care coordination/care management functions.
-
Supporting the development of community-based care teams to extend the reach of practice-based care.
-
Investing in health information technology to support electronic health exchange, population management, and performance measurement.
-
Developing incentives designed to promote integration.
PCCM programs have been used by state Medicaid agencies since the 1980s and have evolved to enhance basic PCCM programs with additional features, including more intensive case management and care coordination for high-need beneficiaries, improved financial and other incentives for PCPs, and increased use of performance and quality measures (Verdier, Byrd, Stone, & Mathematica Policy Research, 2009). Thirty-one states offer PCCM programs as of 2010 (Smith et al., 2013).
Verdier et al.'s study of five states with enhanced PCCMs concluded that enhanced PCCM programs may equal or exceed capitated MCO programs on measures of access, cost, and quality but only if states devote substantial resources to designing, implementing, managing, and funding enhancements. This is especially useful if some form of broader capitated payment is not feasible for states. There has also been a noticeable increase in states utilizing performance and quality measures such as Healthcare Effectiveness Data and Information Set, Consumer Assessment of Healthcare Providers and Systems, and similar measures (Verdier, 2009).
Medical Home and Patient-Centered Care
The concept of the medical home was developed by the American Academy of Pediatrics in the 1960s and further advanced in 2007 when four major physician groups agreed to a common view of the PCMH model (National Academy for State Health Policy [NASHP], 2013b). The Agency for Healthcare Research and Quality (AHRQ) defines medical homes as a model of the organization of primary care that delivers the core functions of primary care (AHRQ, 2013). These five core functions and attributes include comprehensive care, patient-centered, coordinated care, accessible services, and quality and safety. Similar to the payment models used in PCCM, PCMH models typically have care management fees added to standard fee-for-service payments to providers for office visits, tests, or procedures. In addition to the care management fees, providers may receive bonus payments for meeting or exceeding specified quality and efficiency targets. One key difference is that PCMH models are team-based and feature physician-led approaches to providing comprehensive, coordinated, and continuous care for all populations. As of April 2013, NASHP reports that 43 states have adopted policies and programs to advance medical homes (NASHP, 2013b). The National Committee for Quality Assurance (NCQA) has developed a set of standards and guidelines that define the attributes of a PCMH and has designated more than 5,700 primary care practices and 26,000 clinicians as medical homes (NCQA, 2013).
Health Homes
The Health Homes provision was included in the ACA as an opportunity to build a patient-centered system of care that achieves improved outcomes for Medicaid beneficiaries with chronic conditions and better services and value for state Medicaid programs (CMS, 2010). CMS expects providers to integrate and coordinate all primary, acute, behavioral health, and long-term services and supports to treat the "whole-person" (CMS, 2013d). Health Homes were developed specifically for Medicaid beneficiaries who at a minimum have two or more chronic conditions, have one chronic condition and are at risk for another, or have one serious and persistent mental health condition.
States have flexibility when determining eligible health home providers. CMS identifies health homes providers as: (1) a designated provider; (2) a team of health professionals; or (3) a health team. A designated provider can be a physician, clinical/group practice, rural health clinic, community health center, community mental health center, home health agency, pediatrician, OB/GYN, or other provider. A team of health professionals may include physicians, nurse care coordinators, nutritionists, social workers, and behavioral health professionals and can be free-standing, virtual, hospital-based, or a community mental health center. A health team must include medical specialists, nurses, pharmacists, nutritionists, dieticians, social workers, behavioral health providers, chiropractic's, and licensed complementary and alternative practitioners.
CMS recognizes that many states that are interested in developing health homes will want to coordinate with their existing medical home initiatives (CMS, 2010). CMS encourages states to compare their current medical home initiatives with the health homes requirements and design an option to complement one another. An important part of the reporting requirement of the health homes initiative is to report quality measures to the state and report utilization, expenditure and quality data for an interim survey and an independent evaluation. CMS has recommended eight health home core measures to assess individual level clinical outcomes and care processes (Center for Integrated Health Solutions [CIHS], 2013). As a financial incentive to develop Health Homes, states implementing health homes will be given 90 percent Federal Medical Assistance Percentages for the first eight fiscal quarters their initiative is in effect. As of July 2013, CMS had approved Medicaid health homes in 12 states (Alabama, Idaho, Iowa, Maine, Missouri, New York, North Carolina, Ohio, Oregon, Rhode Island, Washington, and Wisconsin) (CIHS, 2013).
Accountable Care Organizations
An ACO is a provider-run organization that utilizes a strong base of primary care and works with a network of doctors and hospitals, all of whom are accountable for coordinating across the full continuum of care with the hope of reducing overall costs while increasing quality of care. Another important feature of the ACO is the use of quality metrics that focus on patient-centered care, increased coordination of care, and incentives designed to reward performance (Kaiser Family Foundation, 2010). Beyond this standard definition of ACO, the ACO models tend to vary by state and local markets. ACOs were originally created in Medicare as a way to qualify for the Medicare shared savings program under the ACA (McClellan, McKethan, Lewis, Roski, & Fisher, 2010). Some Medicaid agencies have taken notice of the model and begun implementing them in their states as a way to coordinate care, increase quality, and save money.
Many of the Medicaid ACO initiatives are either in the early stages of implementation or have been operational for a short time. NASHP has been tracking the states' efforts to implement ACOs. As of November 2013, NASHP has identified 17 states that are contemplating (California, Hawaii, New York, North Carolina, and Washington), in the process of implementing (Alabama, Maine, Massachusetts, New Jersey, Texas, Vermont, Louisiana, and Utah), or currently operating (Arkansas, Colorado, Minnesota, and Oregon) ACOs within their Medicaid systems. Seven of these states (Maine, Massachusetts, Minnesota, New Jersey, Oregon, Texas, and Vermont) are part of a learning collaborative working with the CHCS to develop and implement ACOs in their states. Through this collaborative, CHCS has been sharing its findings throughout the process. These ACO initiatives are going to vary by state in their organizational structure (hybrid MCO/provider-led ACOs, provider-led ACOs, MCO-led ACOs), payment models (per member per month, global payment, shared savings), delivery systems (fee-for-service, managed care), scale (statewide, regional), and beneficiary population (all beneficiaries, certain populations excluded) (CHCS, 2012).
A study by the Kaiser Commission on Medicaid and Uninsured (2012) looked at the role of Medicaid on the emergence of Medicaid ACOs. The study found that because risk-based managed care is the predominant Medicaid delivery and payment system the relationship between ACOs and MCOs is an important consideration when states begin planning and implementing ACOs. In some states, MCOs coordinate with ACOs (Colorado, Minnesota) and in others, the MCOs act as ACOs (Utah), and the boundaries are difficult to discern. In states where there are minimal MCOs within the Medicaid program, a transition to an ACO may be more natural fit.
A SUMMARY OF THE LIKELY CHARACTERISTICS OF INDIVIDUALS NEWLY ELIGIBLE FOR MEDICAID UNDER THE AFFORDABLE CARE ACT
On June 28, 2012, the U.S. Supreme Court in National Federation of Independent Business v. Sebelius upheld the constitutionality of Congress' power to enact certain provisions of the ACA, marking the beginnings of nationwide health care reform, particularly to the Medicaid program (National Federation of Independent Business v. Sebelius, 2012). Prior to the ACA, the Medicaid program offers federal funding to states to assist pregnant women, children, needy families, the blind, the elderly and the disabled in obtaining medical care (42 U.S.C. §1396d(a)). Under the newly enacted ACA, beginning January 1, 2014, states have the option to expand their Medicaid program to non-disabled adults, ages 19-64, earning at or below 138 percent of the federal poverty level (FPL) ($15,586 per year for an individual in 2013) (National Health Care for the Homeless Council [NHCHC], 2012).
Medicaid currently provides health care coverage to more than 50 million Americans, including more than 20 million non-elderly adults (Chang & Davis, 2013). A state's decision on whether to expand its Medicaid coverage under the ACA affects an estimated 15.1 million uninsured adults who would become newly eligible under the ACA (Kenney et al., 2012). Of the 15.1 million, 11.5 million who have incomes below 100 percent of the FPL are at risk of not obtaining health insurance under the ACA, should their state not opt to exercise the option to expand (Kenney et al., 2012). Uninsured adults who have incomes above 100 percent and below 138 percent of the FPL and are living in states that opted not to expand Medicaid may qualify for subsidized private health plans that can be purchased in the Marketplace. Since the U.S. Supreme Court's decision, many state governors have delayed their decisions to expand Medicaid, as a significant amount of planning is required for a successful program) (NHCHC, 2012). As of January 2014, twenty-five states and the District of Columbia have exercised the option to expand Medicaid under the ACA (Urban Institute Health Policy Center, n.d.). Across these 25 states opting to expand Medicaid, an estimated 4.9 million poor and uninsured adults will become newly eligible under the ACA's expansion rules in January 2014 (Urban Institute Health Policy Center, n.d.).
Under the ACA, states have the opportunity to expand Medicaid coverage to millions of uninsured adults, thereby creating a critical need to gather information on the likely characteristics of the expansion population in order to prepare health care delivery systems for a potentially large influx of new patients (Chang & Davis, 2013). States opting to implement the Medicaid expansion would move Medicaid's traditional focus away from low-income pregnant women and children, low-income parents, and severely disabled individuals to new population groups (Decker, Kostova, Kenney, & Long, 2013). A better understanding of the likely characteristics of the newly eligible Medicaid population will enable states to design applicable benefit packages, allocate sufficient resources and develop enrollment strategies (Somers, Hamblin, Verdier, & Byrd, 2010). Despite the significance of such information, determining the likely health needs of the newly eligible Medicaid expansion population is difficult to ascertain given the fact that this population has not been systematically tracked (Somers et al., 2010). Nevertheless, several studies and institutions have begun to describe the likely characteristics of the newly eligible Medicaid expansion population.
| TABLE 2. Characteristics of Newly Eligible Medicaid Expansion Population | ||||
|---|---|---|---|---|
| Below 100% FPL | Below 138% FPL | |||
| Share | Number | Share | Number | |
| Total | 100.0% | 11,483 | 100.0% | 15,060 |
| Age | ||||
| 19-24 | 27.5% | 3,163 | 26.1% | 3,934 |
| 25-34 | 25.6% | 2,940 | 26.0% | 3,912 |
| 35-54 | 32.9% | 3,779 | 34.5% | 5,192 |
| 55-64 | 13.9% | 1,601 | 13.4% | 2,023 |
| Sex | ||||
| Male | 53.4% | 6,132 | 53.0% | 7,979 |
| Female | 46.6% | 5,351 | 47.0% | 7,081 |
| Age/Sex | ||||
| Men 19-44 | 39.2% | 4,502 | 38.7% | 5,833 |
| Women 19-44 | 29.7% | 3,414 | 30.3% | 4,556 |
| Men 45-64 | 14.2% | 1,630 | 14.3% | 2,147 |
| Women 45-64 | 16.9% | 1,937 | 16.8% | 2,525 |
| Parental Status | ||||
| Has a Dependent Child in Household | 13.4% | 1,538 | 17.6% | 2,650 |
| Does not have a Child in Household | 86.6% | 9,946 | 82.4% | 12,411 |
| Race/Ethnicity | ||||
| White Only | 55.1% | 6,323 | 54.9% | 8,270 |
| Hispanic | 18.0% | 2,071 | 19.4% | 2,924 |
| Black/African American | 19.8% | 2,274 | 18.7% | 2,809 |
| Other Multiple | 7.1% | 815 | 7.0% | 1,057 |
| Individual Citizenship Status | ||||
| U.S. Citizen | 94.7% | 10,879 | 93.9% | 14,143 |
| Legal Immigrant | 5.3% | 604 | 6.1% | 918 |
| SOURCE: Kenney et al. "Opting into the Medicaid Expansion under the ACA: Who Are the Uninsured Adults Who Could Gain Health Insurance Coverage?", 2012. | ||||
Using data from the 2010 American Community Survey, the Urban Institute found that with the implementation of the ACA, States may see a dramatic spike of patients who are non-disabled, non-pregnant parents with incomes up to 138 percent of the FPL. Previously, few states covered these groups and even fewer cover such without dependent children (Kenney et al., 2012). The brief finds that the newly eligible Medicaid expansion population of 15.1 million who could gain coverage under the ACA is a diverse group in terms of age, race and ethnicity, with about 26 percent between the ages 19-24; 26 percent between the ages 25-34; 35 percent between the ages 35-54; 13 percent between the ages 55-64; and nationwide, just over half White (55 percent) (Kenney et al., 2012). Moreover, the Urban Institute finds that 82 percent of the newly eligible are adults who are not living with dependent children, with the remaining 2.7 million being parents living with dependent children. Nationally, just over half of the newly eligible Medicaid population is male, with the remaining 47 percent being women, and of the 47 percent, 4.6 million women are in the reproductive ages 19-44 (Kenney et al., 2012). Table 2 summarizes the Urban Institute's findings.
The conclusions in a policy brief from the Kaiser Commission on Medicaid and the Uninsured published in August 2012 were similar to the Urban Institute's. While they did not make distinctions between the sexes, the Kaiser Commission also concluded that the newly eligible Medicaid expansion population is diverse in terms of race, ethnicity, and age and that most adults newly eligible are without dependent children, a group that has been historically excluded from coverage (Kaiser Commission on Medicaid and the Uninsured, 2012, August). Both the Kaiser Commission and the Urban Institute utilized data from the 2010 American Community Survey to identify the newly eligible Medicaid expansion population.
In terms of health status, literature suggests that the initial enrollment of the newly eligible Medicaid expansion population will be in poorer physical and mental health than those currently enrolled in Medicaid but that the newly eligible Medicaid expansion population overall is healthier in both categories than those already covered under Medicaid.
A policy brief published in August 2010 by the CHCS and Mathematica Policy Research, Inc. examined the experiences of ten existing state programs (Arizona, Indiana, Maine, Minnesota, New York, Oregon, Pennsylvania, Vermont, Washington, and Wisconsin) for low-income childless adults to estimate the characteristics of the new expansion population. The brief found that while the newly eligible expansion population includes a blend of healthy and chronically ill adults, several factors make it likely that the initial enrollment of the expansion population would be those with fairly high health care needs (Somers et al., 2010). The brief found that the low-income childless adults would have a higher burden of illness and more complex health care needs, including a higher prevalence of mental illness and substance abuse (Somers et al., 2010).
In a brief also published in August 2010, the Urban Institute, using data from the Medical Expenditure Panel Survey (MEPS) 2005-2006, found that the newly eligible expansion Medicaid population of low-income childless adults is healthier on average than those individuals who are currently enrolled in Medicaid (Holohan, Kenney, & Pelletier, 2010). The brief discredits the examination of state experiences to project the likely characteristics of the newly eligible expansion population due to the fact that these programs have a relatively low participation rate and considerable adverse selection (Holohan et al., 2010). The brief also agrees with the above research conducted by CHCS and Mathematica that those with more serious health problems will likely enroll first (Holohan et al., 2010).
To ascertain the likely health profile of the newly eligible Medicaid population, the Urban Institute looked to the population from which the newly eligible will be drawn (Holohan et al., 2010). Thus, the brief examined the characteristics of both parents and childless adults with incomes that were below 138 percent of the FPL (Holohan et al., 2010). The brief found that there is strong evidence that those who enroll under the Medicaid expansion under the ACA are likely to be healthier in both general and mental health, less likely to have two or more chronic conditions, and less likely to be limited in their ability to work than those who are currently covered under Medicaid, particularly after the initial start-up period (Holohan et al., 2010). The brief presents a number of caveats, however. It acknowledges that MEPS is self-reported information on health status, the presence of chronic health care problems, and substance abuse problems. It may be the case that the newly eligible expansion population is less likely to be aware of existing chronic health care problems and less likely to report substance abuse and mental health problems (Holohan et al., 2010).
A more recent study, published in June 2013, conducted by Drs. Sandra Decker and Deliana Kostova of the Centers for Disease Control and Prevention and Drs. Genevieve Kenney and Sharon Long of the Urban Institute, shares similar findings. The study documented the health care needs and risks of the newly eligible Medicaid expansion population. The study used data from the 2007-2010 National Health and Nutritional Examination Survey (NHANES) to analyze health conditions among uninsured adults ages 19-64 with income no more than 138 percent of the FPL and compared it with health conditions of those adults aged 19-64 currently enrolled in Medicaid. They found that compared with those adults currently enrolled in Medicaid, the newly eligible were less likely to have chronic conditions such as hypertension, diabetes, and hypercholesterolemia (Decker et al., 2013). However, they found that while only one-third of the newly eligible had one of the three conditions, they were also less likely to be aware that they had the condition or to have it under control. Thus, they suggest that although the newly eligible Medicaid expansion population is likely to have fewer chronic conditions, this population will have more undiagnosed or uncontrolled conditions (Decker et al., 2013). The study found that the newly eligible were likely to have fewer health risks such as obesity or a sedentary lifestyle, although the population is more likely to engage in binge drinking and smoking (Decker et al., 2013).
A study from the University of Michigan (Chang & Davis, 2013) found results similar to the ones described above. This was a cross-sectional study of 13.8 million people that also used the NHANES 2007-2010 data to identify and compare adult United States citizens who were newly eligible for Medicaid under the ACA with current adult Medicaid beneficiaries (Chang & Davis, 2013). The study compared characteristics such as age, sex, race/ethnicity, education and various health measures such as body mass index, blood sugar levels, blood pressure, depression, and alcohol and tobacco use (Chang & Davis, 2013). The study found that the newly eligible Medicaid expansion population are in significantly better health than current beneficiaries and are less likely to be obese or have depression, with no difference between diabetes or hypertension rates. The expansion population had a significantly higher proportion of those who reported smoking tobacco and moderate or heavy alcohol use, thereby exposing them to future chronic disease (Chang & Davis, 2013). Table 3 summarizes the study's findings.
| TABLE 3. Health Measures of Adults (ages 19-64) | |||
|---|---|---|---|
| Measure | Current Medicaid Beneficiaries % (95% CI) |
Potentially Eligible for Medicaid Under ACAa % (95% CI) |
P Valueb |
| Health status | <0.001 | ||
| Excellent/very good | 33.5 (28.8-38.6) | 34.8 (30.6-39.3) | |
| Good | 31.6 (28.6-34.7) | 40.4 (36.5-44.3) | |
| Fair/poor | 35.0 (30.6-39.5) | 24.8 (22.3-27.5) | |
| Body mass indexc | 0.008 | ||
| Normal weight | 24.6 (21.3-28.2) | 31.5 (28.1-35.1) | |
| Overweight | 29.9 (25.7-34.5) | 29.9 (27.2-32.8) | |
| Obese | 42.9 (37.8-48.3) | 34.5 (30.8-38.4) | |
| Diabetesd | 7.5 (5.7-9.9) | 5.2 (3.6-7.4) | 0.094 |
| Hypertensione | 9.9 (7.9-12.4) | 12.3 (10.2-14.7) | 0.15 |
| Depressionf | 22.3 (19.5-25.3) | 15.5 (12.8-18.8) | 0.003 |
| Smokingg | 0.002 | ||
| Never smoker | 44.8 (38.9-50.8) | 37.1 (32.6-42.0) | |
| Former smoker | 17.3 (13.6-21.7) | 13.7 (11.0-16.9) | |
| Current smoker | 38.0 (33.0-43.3) | 49.2 (43.8-54.6) | |
| Alcohol useh | <0.001 | ||
| Non-drinker | 17.7 (14.0-22.0) | 12.7 (9.9-16.0) | |
| Light drinker | 56.5 (50.5-62.2) | 49.2 (45.2-53.2) | |
| Moderate drinker | 16.0 (12.7-20.1) | 21.6 (17.5-26.5) | |
| Heavier drinker | 9.8 (8.0-12.0) | 16.5 (12.9-21.0) | |
SOURCE: Chang & Davis, "Potential Adult Medicaid Beneficiaries Under the Patient Protection and Affordable Care Act Compared With Current Adult Medicaid Beneficiaries," 2013.
|
|||
In summary, the majority of literature concedes that although healthier, the expansion population is less likely to be aware of chronic conditions. While overall the newly eligible Medicaid expansion population may be healthier than expected, those who have the chronic conditions will initially require more care than a comparable population already enrolled in Medicaid. A brief published in April 2010 by the Kaiser Family Foundation supports this contention. An analysis of the MEPS 2007 conducted by the Kaiser Commission on Medicaid and the Uninsured examined 17.1 million non-elderly uninsured adults who qualified under the ACA Medicaid expansion rules. The Kaiser Commission found that a third of this population have a diagnosed chronic condition that may worsen due to the lack of health insurance coverage. Moreover, about 60 percent of this population has considerably less access to care, thus making it less likely that they receive preventative care. Also, about a third of this population has not had their blood pressure checked (Kaiser Family Foundation, 2010). Table 4 summarizes the Commission's findings.
| TABLE 4. Health Status, Access to Care and Utilization for Adults (19-64) At or Below 133% FPL (2007) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Medicaid (non-SSI, non-dual) at or below 133% |
Uninsured At or Below 133% |
vs. Medicaid |
Uninsured Parents At or Below 133% |
vs. Medicaid |
Uninsured Childless Adults At or Below 133% |
vs. Medicaid |
|||||
| Population 4,378,994 |
% 100.0% |
Population 13,877,185 |
% 100.0% |
Population 4,918,518 |
% 100.0% |
Population 8,958,666 |
% 100.0% |
||||
| Health Status | |||||||||||
| General Health: % in Fair/Poor Health | 868,266 | 20.0% | 2,217,942 | 16.3% | 770,938 | 15.7% | 1,447,004 | 16.7% | |||
| Mental Health: % in Fair/Poor Health | 632,949 | 14.6% | 1,339,578 | 9.8% | * | 412,304 | 8.4% | * | 927,274 | 10.7% | |
| % with 0 Chronic Conditions | 2,163,566 | 49.4% | 9,462,890 | 68.2% | * | 3,518,581 | 71.5% | * | 5,944,309 | 66.4% | * |
| % with at least 1 Chronic Condition | 2,215,429 | 50.6% | 4,414,295 | 31.8% | * | 1,399,937 | 28.5% | * | 3,014,357 | 33.6% | * |
| % with only 1 Chronic Condition | 833,613 | 19.0% | 2,517,076 | 18.1% | 852,000 | 17.3% | 1,665,076 | 18.6% | |||
| % with 2 or more Chronic Conditions | 1,381,816 | 31.6% | 1,897,219 | 13.7% | * | 547,938 | 11.1% | * | 1,349,281 | 15.1% | * |
| % with Mental Chronic Condition only | 355,647 | 8.1% | 988,078 | 7.1% | 323,467 | 6.6% | 664,611 | 7.4% | |||
| % with both Mental and Physical Chronic Conditions | 632,399 | 14.4% | 657,833 | 4.7% | * | 176,542 | 3.6% | * | 481,290 | 5.4% | * |
| % Limited or Unable to Work | 544,188 | 12.4% | 873,953 | 6.3% | * | 181,868 | 3.7% | * | 692,086 | 7.7% | * |
| Access to Care | |||||||||||
| No Usual Source of Care | 887,037 | 20.4% | 8,078,295 | 60.5% | * | 2,807,554 | 58.0% | * | 5,270,741 | 62.0% | * |
| No Doctor Visit | 1,515,049 | 34.6% | 9,669,565 | 69.7% | * | 3,224,387 | 65.6% | * | 6,445,178 | 71.9% | * |
| Unable to Receive/Delayed Getting Medical Care | 229,923 | 5.3% | 1,835,257 | 13.5% | * | 543,617 | 11.1% | * | 1,291,640 | 14.8% | * |
| Unable to Receive/Delayed Getting Rx | 191,044 | 4.4% | 1,188,189 | 8.7% | * | 272,801 | 5.6% | 915,387 | 10.5% | * | |
| Access to Care among People with 1+ Chronic Conditions | |||||||||||
| No Usual Source of Care | 348,818 | 15.9% | 2,086,342 | 48.0% | * | 692,666 | 49.5% | * | 1,393,676 | 47.3% | * |
| No Doctor Visit | 390,890 | 17.6% | 1,862,959 | 42.2% | * | 604,196 | 43.2% | * | 1,258,763 | 41.8% | * |
| Unable/Delayed Getting Medical Care | 166,075 | 7.5% | 1,033,394 | 23.6% | * | 257,036 | 18.4% | * | 776,358 | 26.1% | * |
| Unable/Delayed Getting Rx | 133,496 | 6.0% | 873,416 | 20.0% | * | 204,710 | 14.7% | * | 668,706 | 22.5% | * |
| Prevalence Rates | |||||||||||
| Cancers, Leukemias, Other Malignancies | 104,792 | 2.4% | 135,715 | 1.0% | 59,471 | 1.2% | 76,244 | 0.9% | |||
| Diabetes Mellitus | 423,348 | 9.7% | 524,126 | 3.8% | * | 231,367 | 4.7% | * | 292,759 | 3.3% | * |
| Heart Conditions | 172,364 | 3.9% | 242,075 | 1.7% | * | 42,033 | 0.9% | * | 200,042 | 2.2% | |
| Hypertension | 685,263 | 15.6% | 1,051,090 | 7.6% | * | 346,861 | 7.1% | * | 704,229 | 7.9% | * |
| Hyperlipidemias | 377,009 | 8.6% | 526,491 | 3.8% | * | 130,821 | 2.7% | * | 395,670 | 4.4% | * |
| Chronic Pulmonary Conditions | 377,665 | 8.6% | 549,113 | 4.0% | * | 150,304 | 3.1% | * | 398,809 | 4.5% | * |
| Kidney Disorders | 31,460 | 0.7% | 15,449 | 0.1% | * | 4,633 | 0.1% | * | 10,816 | 0.1% | * |
| Vertebral Disc Problems | 100,023 | 2.3% | 312,883 | 2.3% | 122,543 | 2.5% | 190,340 | 2.1% | |||
| Psychoses | 177,887 | 4.1% | 149,662 | 1.1% | * | 67,849 | 1.4% | * | 81,813 | 0.9% | * |
| Depression | 715,647 | 16.3% | 1,109,038 | 8.0% | * | 266,661 | 5.4% | * | 842,378 | 9.4% | * |
| Use of Medical Care | |||||||||||
| No Medical Care in 2007 | 805,356 | 18.4% | 7,032,043 | 50.7% | * | 2,240,986 | 45.6% | * | 4,791,057 | 53.5% | * |
| Check-up in past 2 years | 3,200,336 | 76.4% | 5,974,150 | 46.8% | * | 2,276,690 | 48.4% | * | 3,697,460 | 45.9% | * |
| BP Check in past 2 years | 3,840,107 | 91.4% | 8,635,636 | 67.8% | * | 3,329,466 | 71.1% | * | 5,306,170 | 66.0% | * |
| Cholesterol Check in past 2 yrs (35+ M/ 45+ F) | 808,938 | 74.5% | 2,063,767 | 45.7% | * | 561,353 | 41.4% | * | 1,502,414 | 47.5% | * |
| Pap Smear in past 3 years (all Females) | 2,724,571 | 89.7% | 3,775,600 | 65.4% | * | 2,187,086 | 77.6% | * | 1,588,514 | 53.7% | * |
| Mammogram in past 2 years (Female 50+ yrs) | 234,829 | 71.7% | 525,226 | 44.5% | * | 108,945 | 58.9% | 416,280 | 41.8% | * | |
| SOURCE: KFF analysis of 2007 Medicaid Expenditure Panel Survey Data. SOURCE: Kaiser Family Foundation, "Expanding Medicaid Under Health Reform: A Look at Adults at or below 133 percent of Poverty," Focus on Health Reform, 2010. NOTE: All insurance categories are for full-year coverage. Individuals with part-year coverage were not included in this analysis. * Statistically significant difference from Medicaid (p<0.05). |
|||||||||||
| TABLE 5. Characteristics of Currently Uninsured Individuals Expected to be Income Eligible for Medicaid and Current Medicaid Enrollees, Both with Household Incomes Less than 138% of the FPL, by Substance Use Disorder Statusa | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Characteristics | Uninsured and Future Income Eligible | Currently Enrolled in Medicaidb | P for Comparison of Those with Substance Use Disorders |
||||||||
| Substance Use Disorderc |
No Substance Use Disorder |
P | Substance Use Disorderc |
No Substance Use Disorder |
P | ||||||
| N (N=837) |
% | N (N=4,212) |
% | N (N=496) |
% | N (N=3,313) |
% | ||||
| Age | <0.01 | .17 | 0.12 | ||||||||
| 20-25 | 568 | 29.1 | 2,309 | 19.6 | 268 | 23.5 | 1,792 | 20.4 | |||
| 26-34 | 139 | 27.6 | 807 | 24.9 | 123 | 33.5 | 704 | 28.9 | |||
| 35-49 | 112 | 32.3 | 867 | 36.3 | 89 | 32.5 | 639 | 34.6 | |||
| 50-64 | 18 | 11.0 | 229 | 19.2 | 16 | 10.5 | 178 | 16.2 | |||
| Female | 299 | 28.2 | 2,415 | 56.3 | <0.01 | 328 | 57.1 | 2,676 | 74.2 | <.01 | <0.01 |
| Childless | 564 | 60.1 | 2,205 | 51.8 | 0.03 | 189 | 45.7 | 870 | 33.0 | <.01 | <0.01 |
| Employed | 501 | 65.4 | 2,412 | 54.2 | <0.01 | 188 | 35.7 | 1,382 | 37.9 | .49 | <0.01 |
| Married | 145 | 29.9 | 1,350 | 41.9 | <0.01 | 78 | 16.6 | 836 | 30.5 | <.01 | 0.01 |
| Education | 0.15 | .97 | 0.32 | ||||||||
| Less than high school | 366 | 47.5 | 1,621 | 40.8 | 205 | 40.7 | 1,172 | 40.5 | |||
| High school | 251 | 29.4 | 1,476 | 34.9 | 175 | 36.1 | 1,405 | 36.8 | |||
| Some college | 220 | 23.1 | 1,115 | 24.3 | 116 | 23.2 | 736 | 22.6 | |||
| Fair or poor health status | 154 | 24.2 | 596 | 18.9 | 0.09 | 106 | 24.7 | 614 | 27.5 | .40 | 0.91 |
| Tobacco use in past month | 650 | 76.0 | 1,712 | 39.1 | <0.01 | 378 | 72.1 | 1,451 | 42.1 | <.01 | 0.50 |
| Substance dependenced | 520 | 63.4 | 0 | --- | 348 | 71.6 | 0 | --- | 0.08 | ||
| Substance abuse | 317 | 36.6 | 0 | --- | 148 | 28.4 | 0 | --- | |||
| Serious psychological distress | 291 | 28.8 | 615 | 11.5 | <0.01 | 217 | 41.1 | 675 | 21.9 | <.01 | <0.01 |
| Any emergency room use in past year | 369 | 42.2 | 1,481 | 33.6 | <0.01 | 279 | 56.3 | 1,679 | 50.8 | .18 | <0.01 |
| Any inpatient use in past year | 96 | 10.8 | 408 | 9.4 | 0.44 | 105 | 20.8 | 703 | 19.6 | .76 | <0.01 |
SOURCE: Busch et al., "Characteristics of Adults With Substance Use Disorders Expected to be Eligible for Medicaid Under the ACA," Psychiatric Service, 2013.
|
|||||||||||
Overall, data on the likely characteristics of the newly eligible Medicaid expansion population under the ACA is scarce (Busch, Meara, Huskamp, & Barry, 2013). While literature does suggest that the overall expansion population may be healthier, it is consistent with the suggestion that the expansion population may have a significant demand for substance abuse treatment (Busch et al., 2013). However, not much is known about the effect of the ACA on the expansion population with severe disorders (Garfield, Zuvekas, Lave, & Donohue, 2011).
In 2013, Drs. Busch, Meara, Huskamp, and Barry reported on a study they conducted on the need for substance use disorder treatment among the newly eligible Medicaid expansion population under the ACA. The study used data from the 2008-2009 National Survey on Drug Use and Health and compared 3,809 current low-income Medicaid enrollees with 5,049 currently uninsured individuals with incomes that may qualify for Medicaid under the expansion (Busch et al., 2013). They found that the rate of substance use disorders among currently uninsured income-eligible individuals was higher than the rate among current Medicaid enrollees (14.6 percent versus 11.5 percent, p=0.03). Their findings are summarized in Table 5.
In terms of mental health, the Substance Abuse and Mental Health Services Administration estimates that if all states were to expand Medicaid over 15 million adults would be eligible to enroll, and of that population, 7 percent have a SMI and 15 percent psychological distress (NHCHC, 2012). This finding may suggest an increase in the number of users who may utilize mental health services. A study conducted by the University of Pittsburgh examined data from MEPS 2004-2006 to estimate changes that may occur in the number of mental health service users after reform is fully implemented in 2019. The study found that adults who were self-identified with severe mental disorders, severe depression, or other psychological distress, were more likely than those without such conditions to be uninsured (21 percent compared with 16.5 percent) (Garfield et al., 2011). Thus, the authors estimate that the expansion of insurance coverage under the ACA will lead to 1.15 million new users of mental health services, which represents a 4.5 percent increase in mental health service users. The study additionally estimates an increase of 2.3 million users of mental health services in Medicaid (Garfield et al., 2011).
Understanding the characteristics of these individuals will be beneficial to states designing benefit packages, making funding and resource determinations, addressing workforce issues, and developing enrollment strategies as they weigh their decision to expand or to implement in 2014. While undoubtedly valuable to assess these characteristics, literature has noted that there are limitations when measuring these characteristics (Decker et al., 2013). It has noted that it is impossible to project conclusively the demand for health care among the newly eligible since it is possible that this population's care-seeking behavior and other unmeasured characteristics may differ from the current covered population's behavior (Decker et al., 2013). Moreover, the studies addressed above project the demographics and health care characteristics of the newly eligible in the entire nation. These types of data are entirely dependent upon which states decide to expand and the specific health profiles of those areas (Decker et al., 2013).
Summary and Conclusion
This report details four key areas related to the coordination of care for physical and behavioral health conditions by Medicaid managed care plans. These include: evidence-based approaches to care coordination; innovative managed care programs that coordinate care for individuals with co-morbid behavioral health and chronic physical conditions; state Medicaid program activities that promote care coordination for individuals with complex behavioral and physicals disease profiles; and the likely characteristics of individuals who are newly eligible for Medicaid under the ACA. A comprehensive literature review has served as the foundation of the report, and key informant interviews have been used to provide additional resources.
Based on the findings of this report core characteristics of care coordination in Medicaid managed care plans have been identified. Next steps include the identification of innovative Medicaid MCOs that can be reviewed for further elaboration of their principles for improving the coordination of care for complex behavioral health and chronic physical conditions.
REFERENCES
Agency for Healthcare Research and Quality (AHRQ). (2013). Patient Centered Medical Home Resource Center. Retrieved from http://pcmh.ahrq.gov.
America's Health Insurance Plans (AHIP). (2014). Personal Communication.
America's Health Insurance Plans, Center for Policy and Research. (2012). Health Plan Innovations: Caring for Medicare and Medicaid Patients with Chronic Illnesses. (Briefing Summary). Retrieved from https://www.ahip.org/AHIPResearch/AHIPBriefingJan2012/.
America's Health Insurance Plans, Center for Policy and Research. (2013). Innovations in Medicaid Managed Care: Highlights of Health Plans' Programs to Improve the Health and Well-being of Medicaid Beneficiaries. Retrieved from http://www.ahip.org/MedicaidInnovationsBook/.
Association for Behavioral Health and Wellness. (2014). Personal Communication.
Beckjord, E.B., Keyser, D.J., Schultz, D., Lovejoy, S., Firth, R., & Pincus, A.P. (2011). Potential Benefits of Health Information Technology for Integrating Physical and Behavioral Health Care: Perinatal Depression as a Case-in-Point. Translational Behavioral Medicine, 1, 89-92. doi: 10.1007/s13142-011-0020-8.
Berenson, R., & Howell, J. (2009). Structuring, Financing and Paying for Chronic Care Coordination. Retrieved from Families USA website: http://familiesusa2.org/assets/pdfs/health-system-reform/Care-Coordination.pdf.
Burton, R. (2012). Health Policy Brief: Care Transitions.Health Affairs. Retrieved from http://www.healthaffairs.org/healthpolicybriefs/brief.php?brief_id=76.
Busch, S.H., Meara, E., Huskamp, H.A., & Barry, C.L. (2013). Characteristics of Adults with Substance Use Disorders Expected to be Eligible for Medicaid under the ACA. Psychiatric Services, 64(6), 520-526. doi: 10.1176/appi.ps.201200011.
Center for Health Care Strategies, Inc. (CHCS). (2012). Seven States Join National Effort to Advance Medicaid Accountable Care Organizations.
Center for Health Care Strategies, Inc. (2014). Personal Communication.
Center for Integrated Health Solutions (CIHS). (2013). Financing and Policy Considerations for Medicaid Health Homes for Individuals with Behavioral Health Conditions: A Discussion of Selected States' Approaches. Retrieved from http://www.integration.samhsa.gov/integrated-care-models/Health_Homes_Financing_and_Policy_Considerations.pdf.
Centers for Medicare and Medicaid Services (CMS). (2010). Health Homes for Enrollees with Chronic Conditions. (Letter to state Medicaid directors) (SMDL# 10-024, ACA# 12). Retrieved from http://downloads.cms.gov/cmsgov/archived-downloads/SMDL/downloads/SMD10024.pdf.
Centers for Medicare and Medicaid Services. (2012a). Initial Core Set of Health Care Quality Measures for Medicaid-eligible Adults.
Centers for Medicare and Medicaid Services. (2012b). Integrated Care Models. (Letter to state Medicaid directors) (SMDL# 12-001, ICM# 1). Retrieved from http://www.medicaid.gov/Federal-Policy-Guidance/downloads/SMD-12-001.pdf.
Centers for Medicare and Medicaid Services. (2012c). Policy Considerations for Integrated Care Models. (Letter to state Medicaid directors) (SMDL# 12-002, ICM# 2). Retrieved from http://www.medicaid.gov/Federal-Policy-Guidance/Downloads/SMD-12-002.pdf.
Centers for Medicare and Medicaid Services. (2012d). Continuum of New Integrated Care Models in Medicaid: Key Program Features. Retrieved from http://www.medicaid.gov/State-Resource-Center/MAC-Learning-Collaboratives/Downloads/VBP_Continuum-Brief-July-2012.pdf.
Centers for Medicare and Medicaid Services. (2013a). Shared Savings Methodologies. (Letter to state Medicaid directors) (SMDL# 13-005, ICM# 3). Retrieved from http://www.medicaid.gov/Federal-Policy-Guidance/downloads/SMD-13-005.pdf.
Centers for Medicare and Medicaid Services. (2013b). Quality Consideration for Medicaid and CHIP Programs. (Letter to state Medicaid directors) (SMDL# 13-007, ICM# 4). Retrieved from http://medicaid.gov/Federal-Policy-Guidance/Downloads/SHO-13-007.pdf.
Centers for Medicare and Medicaid Services. (2013c). Fact Sheet: State Innovation Models Initiative. Retrieved from http://www.cms.gov/apps/media/press/factsheet.asp?Counter=4546&intNumPerPage=10&checkDate=&checkKey=&srchType=1&numDays=3500&srchOpt=0&srchData=&keywordType=All&chkNewsType=6&intPage=&showAll=&pYear=&year=&desc=&cboOrder=date.
Centers for Medicare and Medicaid Services. (2013d). Health Homes.
Chang, T., & Davis, M. (2013). Potential Adult Medicaid Beneficiaries under the Patient Protection and Affordable Care Act Compared with Current Adult Medicaid Beneficiaries. Annals of Family Medicine, 11(5), 406-411. Retrieved from http://www.annfammed.org/content/11/5/406.short.
Daniels, A.S., Adams, N., Carroll, C., & Beinecke, R.H. (2009). A Conceptual Model for Behavioral Health and Primary Care Integration: Emerging Challenges and Strategies for Improving International Mental Health Services.International Journal of Mental Health, 38(1), 100-112.
Decker, S.L., Kostova, D., Kenney, G.M., & Long, S.K. (2013). Health Status, Risk Factors, and Medical Conditions among Persons Enrolled in Medicaid vs Uninsured Low-income Adults Potentially Eligible for Medicaid under the Affordable Care Act. Journal of the American Medical Association, 309(24), 2579-2586. Retrieved from http://jama.jamanetwork.com/article.aspx?articleID=1699906.
Dullabh, P., Milstein, J.-A., Nye, C., Moiduddin, A., Virost, L.M., Babalola, E., Mahmud, A., Ashish, K. J. (2012). Evaluation of the State Health Information Exchange Cooperative Agreement Program: Early Findings from a Review of Twenty-seven States. Retrieved from the Office of the National Coordinator for Health Information Technology website: http://www.healthit.gov/sites/default/files/private/pdf/state-health-info-exchange-coop-program-evaluation.pdf.
Grypma, L., Little, S., Haverkamp, R., & Unützer, J. (2006). Taking an Evidence-based Model of Depression Care from Research to Practice: Making Lemonade Out of Depression. General Hospital Psychiatry, 28, 101-107.
Garfield, R.L., Zuvekas, S.H., Lave, J.R., & Donohue, J.M. (2011). The Impact of National Health Care Reform on Adults with Severe Mental Disorders. American Journal of Psychiatry, 168(5), 486-494.
Gilbody, S., Bower, P., Fletcher, J., Richards, D. & Sutton, A.J. (2006). Collaborative Care for Depression: A Cumulative Meta-analysis and Review of Longer-term Outcomes. Archives of Internal Medicine, 166(21), 2314-2321.
Hamblin, A., Verdier, J., & Au, M. (2011). State Options for Integrating Physical and Behavioral Health Care. (Integrated Care Resource Center Technical Assistance Brief). Retrieved from the SAMHSA-HRSA Center for Integrated Health Solutions website: http://www.integration.samhsa.gov/integrated-care-models/Integrated_Care_Briefing_Paper_models_of_integration_analysis_10-6-11.pdf.
Holohan, J., Kenney, G., & Pelletier, J. (2010). The Health Status of New Medicaid Enrollees under Health Reform. (Timely Analysis of Immediate Health Policy Issues). Retrieved from the Urban Institute website: http://www.urban.org/uploadedpdf/412206-health-status.pdf.
Kaiser Commission on Medicaid and the Uninsured. (2012). Emerging Medicaid Accountable Care Organizations: The Role of Managed Care. Retrieved from http://kaiserfamilyfoundation.files.wordpress.com/2013/01/8319.pdf.
Kaiser Commission on Medicaid and the Uninsured. (2012). Characteristics of Uninsured Low-income Adults. Retrieved from http://kaiserfamilyfoundation.files.wordpress.com/2013/01/8350.pdf.
Kaiser Commission on Medicaid and the Uninsured. (2012). The Role of Medicaid for People with Behavioral Health Conditions. Retrieved from http://kaiserfamilyfoundation.files.wordpress.com/2013/01/8383_bhc.pdf.
Kaiser Family Foundation. (2010). Expanding Medicaid under Health Reform: A Look at Adults At or Below 133% of Poverty. (Focus on Health Reform). Retrieved from http://kaiserfamilyfoundation.files.wordpress.com/2013/01/8052-02.pdf.
Kathol, R.G., Parez, R., & Cohen, J.S. (2010). The Integrated Case Management Manual: Assisting Complex Patients Regain Physical and Mental Health. New York, NY: Springer.
Kenney, G., Zuckerman, S., Dubay, L., Huntress, M., Lynch, V., Haley, J., & Anderson, N. (2012). Opting into the Medicaid Expansion under the ACA: Who are the Uninsured Adults Who could Gain Health Insurance Coverage. (Timely Analysis of Immediate Health Policy Issues). Retrieved from the Urban Institute website: http://www.urban.org/UploadedPDF/412630-opting-in-medicaid.pdf.
Kripalani, S., LeFevre, F., Phillips, C.O., Williams, M.V., Basaviah, P., & Baker, D.W. (2007). Deficits in Communication and Information Transfer between Hospital-based and Primary Care Physicians. Journal of the American Medical Association, 297(8), 831-841.
McClellan, M., McKethan, A.N., Lewis, J.L., Roski, J., & Fisher, E.S. (2010). A National Strategy to Put Accountable Care into Practice.Health Affairs, 29(5), 982-990. doi: 10.1377/hlthaff.2010.0194.
McDonald, K.M., Sundaram, V., Bravata, D.M., Lewis, R., Lin, N., Kraft, S.A., McKinnon, M., Paguntalan, H., & Owens, D.K. (2007). Definitions of Care Coordination and Related Terms. In Closing the Quality Gap: A Critical Analysis of Quality Improvement Strategies (Vol. 7: Care Coordination). (Technical Reviews, No. 9.7). Rockville, MD: Agency for Healthcare Research and Quality. Retrieved from http://www.ncbi.nlm.nih.gov/books/NBK44012/.
National Academy for State Health Policy (NASHP). (2013a). State "Accountable Care" Activity Map. Retrieved from http://nashp.org/state-accountable-care-activity-map.
National Academy for State Health Policy. (2013b). Medical Home and Patient-Centered Care. Retrieved from http://nashp.org/med-home-map.
National Association of Medicaid Directors. (2014). Personal Communication.
National Committee for Quality Assurance (NCQA). (2011). 2011 PCMH Standards and Guidelines.
National Committee for Quality Assurance. (2013). Public is Invited to Comment on Proposed Changes to Patient-Centered Medical Home Standards. (News Archives). Retrieved from http://www.ncqa.org/Newsroom/NewsArchive/2013NewsArchive/NewsReleaseJune172013.aspx.
National Federation of Independent Business v. Sebelius. (No. 11393) (S. Ct. June 28, 2012). Retrieved from http://www.supremecourt.gov/opinions/11pdf/11-393c3a2.pdf.
National Health Care for the Homeless Council (NHCHC). (2012). Medicaid Expansion and the ACA: Issues for the HCH Community. (Policy Brief). Retrieved from http://www.nhchc.org/wp-content/uploads/2011/10/PolicyBrief-MedicaidExpansion-Sept20121.pdf.
Shier, G., Ginsburg, M., Howell, J., Volland, P., and Golden, R. (2013). Strong Social Support Services, such as Transportation and Help for Caregivers, Can Lead to Lower Health Care Use and Costs. Health Affairs, 32(3), 544-551.
Silow-Carroll, S., & Rodin, D. (2013). Forging Community Partnerships to Improve Health Care: The Experience of Four Medicaid Managed Care Organizations. (Issue Brief, Vol. 19). Retrieved from The Commonwealth Fund website: http://www.commonwealthfund.org/Publications/Issue-Briefs/2013/Apr/Forging-Community-Partnerships-to-Improve-Care.aspx.
Smith, V., Gifford, K., Ellis, E., Rudowitz, R., & Snyder, L. (2013). Medicaid in a Historic Time of Transformation: Results from a 50-state Medicaid Budget Survey for State Fiscal Years 2013 and 2014. Retrieved from the Kaiser Family Foundation website: https://kaiserfamilyfoundation.files.wordpress.com/2013/10/8498-medicaid-in-a-historic-time-of-transformation.pdf.
Solberg, L.I., Crain, A.L., Jaeckels, N., Ohnsorg, K.A., Margolis, K.L., Beck, A., Whitebird, R.R., Rossom, R.C., Crabtree, B.F., & Van de Ven, A.H. (2013). The DIAMOND Initiative: Implementing Collaborative Care for Depression in 75 Primary Care Clinics. Implementation Science, 8, 135.
Somers, S.A., Hamblin, A., Verdier, J.M., & Byrd, V.L.H. (2010). Covering Low-income Childless Adults in Medicaid: Experiences from Selected States. (Policy Brief). Retrieved from the Center for Health Care Strategies, Inc. website: http://www.chcs.org/usr_doc/Medicaid_Expansion_Brief.pdf.
Urban Institute Health Policy Center. (n.d.). 11.5 million Poor Uninsured Americans could be Eligible for Medicaid if States Opt for ACA Expansion. Retrieved http://www.urban.org/health_policy/health_care_reform/map.cfm.
Verdier, J., Byrd, V., Stone, C., & Mathematica Policy Research, Inc. (2009). Enhanced Primary Care Case Management Programs in Medicaid: Issues and Options for States. Retrieved from the Center for Health Care Strategies, Inc. website: http://www.chcs.org/usr_doc/EPCCM_Full_Report.pdf.
Wagner, E.H. (1998). Chronic Disease Management: What will it Take to Improve Care for Chronic Illness? Effective Clinical Practice, 1(1), 2-4.
APPENDIX I. SEARCH METHODOLOGY REPORT
The research team consulted with Westat's Information Research Center's staff to develop a search methodology strategy. Below you will find the search terms used to conduct the literature search. After reviewing the results from the initial round of searching, the search terms were refined to identify more relevant results. The final round of searching relied primarily on searching the grey literature and interviewing key informants. The references found in the published literature were saved to RefMan database.
Round 1.
Project team prepared a list of search terms. The terms were categorized and edited by a librarian who then searched the terms in PubMed.
Terms in columns 1-4 were combined with AND. Terms in columns 5-8 were searched alone or in combination with terms in columns 1-4.
For example: (Medicaid AND chronic AND behavioral) AND ("managed care" OR "coordinated care")
Search results limited to last 10 years.
106 abstracts from PubMed were sent to the project team for review.
The project team requested that going forward the search strategy be more focused on finding relevant managed care coordination programs, preferably Medicaid programs.
Round 2.
Gray literature sources were searched to find examples of relevant programs.
These program names and a focused search strategy were searched in PubMed and PsycInfo.
| Medicaid | Chronic physical condition | Mental health | Co-morbid* | Managed care | Coordinated care | Quality measures | Bundled care |
|---|---|---|---|---|---|---|---|
| Chronic physical illness | Anxiety | Co-morbid* | MCO | Care coordination | Outcome measures | Capitated care | |
| Chronic illness | Behavioral medicine | Co-occurring | Managed behavioral health care organization | Collaborative care | Performance measures | Capitation | |
| Chronic conditions | Bipolar disorder | Co-management | Integrated care | Rating Rated |
Pharmacy benefit management | ||
| Physical disorders AND chronic | Depression | Case management | Shared care | Reproducibility of results | Fee-for-service | ||
| Diabetes | Depressive disorders | Disease management | Transitional care | Scales Subscales |
|||
| Asthma | Mental health services | Clinical monitoring | Synchronized care | Process evaluation | |||
| Heart disease | Psychotherapy | Stepped care | Interdisciplinary care | Outcome assessment methods | |||
| Obesity | Stress | Continuity of patient care | Model+ | ||||
| Substance related disorders | Patient-centered care | Pilot projects | |||||
| Patient care planning | Evidence-based | ||||||
| Integration | |||||||
| Medical home | |||||||
| Medical care home | |||||||
| Health home | |||||||
| Primary care home | |||||||
| Family centered care home | |||||||
| Team-based care | |||||||
| Navigation Navigator+ | |||||||
| Promotoras/ promatores |
This strategy includes:
-
"Health home+" AND Medicaid
-
"Health Home+" AND (names of states where Medicaid has health home programs)
-
"Medicaid managed care"
-
Medicaid AND "managed care" AND (comorbid* OR co-morbid* OR co-occur*
-
Medicaid AND "managed care" AND (coordinat* OR integrat*) AND (comorbid* OR co-morbid* OR co-occur*)
-
Medicaid AND "managed care" AND (coordinat* OR integrat*) AND (physical OR chronic) AND (behavioral OR mental)
-
Medicaid AND "collaborative care" AND (model+ OR program+)
Names of programs found in the gray literature search
13 hits were found in PubMed and PsycInfo.
The same strategy will be used to search in CINAHL, PILOTS, ASSIA, Sociological Abstracts and Social Services Abstracts.
Round 3.
Conduct more thorough grey literature searches and key informant interviews.
APPENDIX II. KEY INFORMANT INTERVIEWS
As part of the Environment Scan, the Westat research team interviewed several key informants from organizations that are very familiar with innovations currently taking place among the Medicaid managed care plans. The research team conducted interviews with the following:
-
America's Health Insurance Plans
- Barbara Lardy, M.P.H., Senior Vice President, Clinical Affairs and Strategic Partnerships
- Natalie Slaughter, M.S.P.P.M., Senior Health Research Associate
-
Association for Behavioral Health and Wellness
- Pamela Greenberg, M.P.P., President and CEO
- Pamela Greenberg, M.P.P., President and CEO
-
Center for Health Care Strategies, Inc.
- Allison Hamblin, M.S.P.H., Vice President for Strategic Planning
- Allison Hamblin, M.S.P.H., Vice President for Strategic Planning
-
Medicaid Health Plans of America
- Amy Ingham, Medicaid Policy Manager
- Liza Greenberg, R.N., M.P.H., Clinical Consultant
-
National Association of Medicaid Directors
- Matt Salo, Executive Director
- Andrea Maresca, M.P.H., Director of Federal Policy and Strategy
Innovative Medicaid Managed Care Coordination Programs for Co-morbid Behavioral Health and Chronic Physical Health Conditions
This report was prepared under contract #HHSP23320100026WI between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and Westat. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/office-disability-aging-and-long-term-care-policy-daltcp or contact the ASPE Project Officer, Joel Dubenitz, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. His e-mail addresses is: Joel.Dubenitz@hhs.gov.
Reports Available
Innovative Medicaid Managed Care Coordination Programs for Co-morbid Behavioral Health and Chronic Physical Health Conditions: Final Report (May 2015)
- Full HTML Version: https://aspe.hhs.gov/basic-report/innovative-medicaid-managed-care-coordination-programs-co-morbid-behavioral-health-and-chronic-physical-health-conditions-final-report
- Full PDF Version: https://aspe.hhs.gov/pdf-report/innovative-medicaid-managed-care-coordination-programs-co-morbid-behavioral-health-and-chronic-physical-health-conditions-final-report
Innovative Medicaid Managed Care Coordination Programs for Co-morbid Behavioral Health and Chronic Physical Health Conditions: Final Environmental Scan (March 2014)
- Full HTML Version: https://aspe.hhs.gov/basic-report/innovative-medicaid-managed-care-coordination-programs-co-morbid-behavioral-health-and-chronic-physical-health-conditions-final-environmental-scan
- Full PDF Version: https://aspe.hhs.gov/pdf-report/innovative-medicaid-managed-care-coordination-programs-co-morbid-behavioral-health-and-chronic-physical-health-conditions-final-environmental-scan