
ABSTRACT
Communicating necessary and timely information to providers across the continuum of care is central to providing coordinated care. This report focuses on the information exchange processes of integrated care models that provide care for populations with long-term service and support (LTSS) needs. Individuals with LTSS needs require a number of people to be involved to provide care and support, and all of these providers require specific information elements about each individual. Integrated care models' primary focus is on care coordination among a large range of provider types. Organizations providing integrated care have invested substantial effort in developing approaches that support information exchange among the continuum of providers.
To gather details on information exchange content and processes in integrated care models, RTI International conducted a comprehensive environmental scan, convened a technical advisory group (TAG), interviewed subject matter experts (SMEs), and conducted case studies of three established systems administering integrated care models. Findings from the project will help to identify areas for improvement as well as promising practices that may be useful to promote effective information exchange practices in integrated care models. The full report includes several appendices. Appendix A is the environmental scan describing a range of integrated care models throughout the United States. Appendices B, C, and D provide more detailed descriptions of the three case study sites and how information flows in those sites: Geisinger Health System in Pennsylvania; Minnesota Senior Health Options, Special Needs BasicCare, and HealthPartners in Minnesota; and Community Care, Inc. in Wisconsin.
DISCLAIMER: The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS
1. BACKGROUND
- 1.1. Project Goals
- 1.2. What is Integrated Care?
- 1.3. What is Health Information Exchange?
- 1.4. Project Methodology
2. THEMES FROM SITE VISITS AND SUBJECT MATTER EXPERT INTERVIEWS
- 2.1. How is Information Exchanged?
- 2.2. What Information Do Providers Want to Receive and Do They Receive It?
- 2.3. What Are the Remaining Gaps or Challenges to Exchanging Information?
3. CONCLUSION: FUTURE DIRECTIONS
APPENDICES
- APPENDIX A: Environmental Scan
- APPENDIX B: Integrated Care Models Overview--Geisinger Health System
- APPENDIX C: Minnesota Care Study
- APPENDIX D: Community Care
LIST OF FIGURES
- FIGURE B-1: Geisinger Information Flow
- FIGURE C-1: HealthPartners Information Flow
- FIGURE D-1: Community Care Information Flow
LIST OF TABLES
- TABLE ES-1: Summary of Information Providers Want to Receive, by Provider Type
- TABLE 1-1: Integrated Care Models
- TABLE 1-2: HIE Adoption as of 2013
- TABLE 2-1: Summary of Information Providers Want to Receive, by Provider Type
- TABLE A-1: Integrated Care Models
ACKNOWLEDGMENTS
The Office of the Assistant Secretary for Planning and Evaluation and RTI International would like to thank the participants of the Technical Advisory Group, subject matter expert interviews and site visits for their contributions to this project. They provided valuable guidance and insight into information exchange processes and integrated care models.
We would like to especially thank the participants of our site visits at Geisinger Health System; Minnesota Department of Human Services, Bluestone Physician Group, and HealthPartners; and Community Care, Inc. in Wisconsin. We are grateful for their time and willingness to assist us in reaching our project goals. They provided us with the indispensable and detailed information required to better understand how information is exchanged in their integrated care models.
ACRONYMS
The following acronyms are mentioned in this report and/or appendices.
| AAA | Area Agency on Aging |
|---|---|
| ACO | Accountable Care Organization |
| ADL | Activity of Daily Living |
| AHIMA | American Health Information Management Association |
| ASPE | HHS Office of the Assistant Secretary for Planning and Evaluation |
| C-SNP | Chronic Care Special Needs Plan |
| CAH | Critical Access Hospital |
| CAPABLE | Community Aging in Place, Advancing Better Living for Elders |
| CCD | Continuity of Care Document |
| CCI | Wisconsin Community Care, Inc. |
| CFR | Code of Federal Regulations |
| CMS | HHS Centers for Medicare and Medicaid Services |
| D-SNP | Dual Eligible Special Needs Plan |
| DHS | Minnesota Department of Human Services |
| EHR | Electronic Health Record |
| FIDE-SNP | Fully Integrated Dual Eligible Special Needs Plan |
| HCBS | Home and Community-Based Services |
| HCIA | Health Care Innovation Award |
| HHS | U.S. Department of Health and Human Services |
| HIE | Health Information Exchange |
| HIMSS | Healthcare Information and Management Systems Society |
| HIPAA | Health Insurance Portability and Accountability Act |
| HIT | Health Information Technology |
| HITECH | Health Information Technology for Economic and Clinical Health Act |
| I-SNP | Institutional Special Needs Plan |
| IADL | Instrumental Activity of Daily Living |
| KeyHIE | Keystone Health Information Exchange |
| LTSS | Long-Term Services and Supports |
| MDS | Minimum Data Set |
| MLTSS | Managed Long-Term Services and Supports |
| MnDHO | Minnesota Disability Health Options |
| MSHO | Minnesota Senior Health Options |
| OASIS | Outcome and Assessment Information Set |
| ONC | HHS Office of the National Coordinator for Health Information Technology |
| PACE | Providers of All-Inclusive Care for the Elderly |
| PCP | Primary Care Provider |
| PES | Provider Enterprise System |
| SASH | Support and Services at Home evaluation |
| SME | Subject Matter Expert |
| SNBC | Special Needs BasicCare |
| SNP | Special Needs Plan |
| SPA | State Plan Amendment |
| TAG | Technical Advisory Group |
| U.S.C. | United States Code |
| VHA | Veterans Health Administration |
| WHO | World Health Organization |
EXECUTIVE SUMMARY
Communicating necessary and timely information to providers across the continuum of care is central to providing coordinated care. This report focuses on the information exchange processes of integrated care models that provide care for populations with long-term services and supports (LTSS) needs. Individuals with LTSS needs require a number of people to be involved to provide care and support, and all of these providers require specific information elements about each individual. Integrated care models' primary focus is on care coordination among a large range of provider types. Organizations providing integrated care have invested substantial effort in developing approaches that support information exchange among the continuum of providers.
To gather details on information exchange content and processes in integrated care models, RTI International conducted a comprehensive environmental scan, convened a Technical Advisory Group, interviewed subject matter experts (SMEs), and conducted case studies of three established systems administering integrated care models. Findings from the project will help to identify areas for improvement as well as promising practices that may be useful to promote effective information exchange practices in integrated care models. The full report includes several appendices. Appendix A is the environmental scan describing a range of integrated care models throughout the United States. Appendices B, C, and D provide more detailed descriptions of the three case study sites and how information flows in those sites: Geisinger Health System in Pennsylvania; Minnesota Senior Health Options, Special Needs BasicCare, and HealthPartners in Minnesota; and Community Care, Inc. in Wisconsin.
|
Key Findings Efforts to better understand information exchange in integrated care models reflect the following key findings:
|
Themes from Interviews and Case Studies
The site visits and SME interviews helped specifically identify how information is exchanged among the various providers participating in integrated care models. Key themes emerged; we have divided these themes into three main research questions:
-
How is information exchanged?
-
What information do providers want to receive, and do they receive it?
-
What are the remaining gaps or challenges to exchanging information?
How is Information Exchanged?
-
We found that even in integrated care systems, personal relationships in information exchange processes related to care coordination are key. Care coordination and the supporting exchange of information are still high touch processes. Technology can be a valuable tool in facilitating communication and information exchange, but organizational trust and personal relationships between the providers is still foundational to successful care coordination.
-
The Office of the National Coordinator for Health Information Technology (ONC) 2014 Report to the Congress indicated that EHR adoption has increased significantly among acute care providers targeted for EHR incentives, although there is lower than desired sharing of electronic health information outside of providers' organizations. The absence of EHR incentives in settings such as post-acute care, LTSS, and behavioral health has also left adoption of health information technology as a lower priority among such setting providers (ONC, 2014; Dougherty, Williams, Millenson, & Harvell, 2013). This presents challenges for integrated care systems serving individuals using a range of medical services and LTSS.
-
The findings from our site visits were largely congruent with findings cited in the ONC Report to Congress, even in these integrated care systems, including: (1) high rates of EHR adoption by hospitals and eligible professionals receiving financial incentives; (2) low rates of sharing data electronically with providers outside of the organization; and (3) low adoption of EHRs and health information exchanges (HIEs) by long-term and post-acute care providers who did not receive financial incentives. There also are differences in EHR access between providers who are affiliated with an integrated care system, and external partners with whom they share cases.
-
Some providers have developed approaches to information sharing that do not require EHR/HIE:
-
Bluestone Physician Services, a physician-led model in Minnesota providing on-site primary care in residential settings, implemented a proprietary care coordination communication system to facilitate timely, electronic communication with their client facilities.
-
KeyHIE Transform™, a web-based subscription service, enables a nursing home or home health agency to contribute patient information to an HIE organization based on electronic assessment data the provider is required to submit to the Centers for Medicare and Medicaid Services. The process is Health Insurance Portability and Accountability Act (HIPAA) and protected health information compliant and works with or without an EHR system (ONC, 2013).
-
What Information Do Providers Want to Receive and Do They Receive It?
-
The information providers want to receive differs based on the provider type (Byrne & Dougherty, 2013). These differences were most apparent when comparing the preferences of acute care providers versus LTSS providers.
- Acute care providers prefer a clinical snapshot of the individual.
- LTSS providers want functional assessments and care plans of the individual, in addition to the clinical snapshot.
- Care coordinators want as much information about the individual as possible, including all health care and LTSS needs.
-
Across all provider types, the method of information exchange had a direct impact on whether desired information was received.
- When information exchange is supported by access into the EHR, the provider may have full access to all current and historical health information on the patient; however, such access will be determined by factors such as provider privileges, patient authorization, and organizational policy.
- When electronic information exchange is not available, information is conveyed by more manual methods such as phone, fax, or hardcopy. These methods can create information gaps.
-
No matter the amount of information provided, how information is displayed and made available to providers is key to successful information exchange. Providers need tailored views that are limited to the key elements of interest to them and easy to access.
| TABLE ES-1. Summary of Information Providers Want to Receive, by Provider Type | ||
|---|---|---|
| Provider Type | What Information Do Providers Want? | |
| Acute care providers (e.g., primary care providers [PCPs], hospital providers) |
|
|
| LTSS providers |
|
|
| Care coordinator/case manager |
|
|
What Are the Remaining Gaps or Challenges to Exchanging Information?
-
Existing EHRs do not meet the needs of integrated care models. Current EHRs focus on episodic care while integrated care models focus on continuity of care. Current EHRs do not have good templates for collecting LTSS and behavioral health information, so integrated care models are forced to use note sections of the EHR, which can be hard to navigate and can make the information less readily accessible.
-
Exchanged information needs to be presented in a format that is relevant to and consumable by the receiving provider. Our experts and sites reported challenges locating desired documents in the EHR, as well as issues with consuming the content (e.g., document format that is foreign to recipient, making it difficult or time-consuming to locate information; content that is too granular or not detailed enough for the receiving provider).
-
Providers view the high costs associated with establishing and maintaining EHR interfaces with electronic information exchange partners as a barrier to HIE.
-
LTSS providers tend to be outside of the integrated care models' administrative systems, creating challenges to information exchange in a timely manner and getting a comprehensive picture of the individual.
-
LTSS providers ineligible for meaningful use incentives, such as nursing homes and home health agencies, have experienced difficulty in receiving needed connectivity support (cooperation is often needed between niche market EHR vendors and large acute care EHR vendors).
-
Integrated care models raised several concerns about the challenges to meet privacy and care coordination regulatory requirements while simultaneously fostering the exchange of information among providers.
-
Misunderstandings and differences in provider interpretation of the HIPAA of 1996 (P.L. 104-91) privacy requirements caused inconsistent access to information. Varying interpretations of HIPAA requirements for a patient's authorization to release information were cited as a particular barrier to information flow among providers. Also, all integrated care models identified particular concerns for exchanging behavioral health information across providers as a challenge.
1. BACKGROUND
1.1. Project Goals
The purpose of this project was to describe the current practice of information exchange in integrated care models that include acute care and long-term services and supports (LTSS). We focused on these systems because integrated care models are designed to facilitate information exchange between providers responsible for different domains of patient care. Integrated care models' primary focus is on care coordination among a range of provider types and they have invested in developing information exchange approaches to support care coordination.
To gather details on the content and processes of information exchange, RTI International conducted a comprehensive environmental scan, convened a Technical Advisory Group (TAG), interviewed subject matter experts (SMEs), and conducted case studies of existing integrated care models. Findings from the project will help to identify areas for improvement as well as promising practices that may be useful to understanding information exchange practices in integrated care models. The findings will also provide needed information to the Office of the National Coordinator for Health Information Technology (ONC) about how LTSS and post-acute care providers use health information technology (HIT) and participate in electronic health information exchange (HIE).
Specifically, the project focused on the following research questions:
-
What information is being exchanged between LTSS and acute care providers in integrated care models?
-
What systems do integrated care arrangements use for HIE?
-
Which providers are using the information?
-
What information is most useful to providers in the acute and LTSS systems? How do acute care and LTSS providers organize care as a result of HIE?
-
Are there specific financial or policy barriers to efficient and timely information exchange in integrated care systems?
1.2. What is Integrated Care?
Integrated care broadly refers to the "bringing together of inputs, delivery, management and organization of services as a means [of] improving access, quality, patient outcomes, user satisfaction and efficiency" (Grone & Garcia-Barbero, 2001). Integrated care can apply to many different systems of care for many different populations. The value of integrated care models is particularly relevant to those populations who rely on the health care system the most, including those who have both medical and LTSS needs. Providing health care, social services, and related supports at the right time and place to such individuals can be very complex. Challenges may arise around obtaining needs assessments, putting together comprehensive service packages, coordinating multiple providers and services, ensuring continuity, monitoring health and functional status, responding to crises, supporting family caregivers, and performing all of these essential activities within existing funding and resource constraints (Kodner & Spreeuwenberg, 2002). An integrated care model can provide the organizational structure to support the coordination needed to provide quality care to these populations. This report focuses on such integrated care models that provide care for populations with LTSS needs.
Integrated care models have a primary goal of providing coordinated care based around the formal linkages of different types of providers, although the organizational elements of the integrated care systems can vary widely.
-
Providers. The provider arrangements of integrated care models can range from a model that includes a core team of providers that integrates medical, LTSS, and behavioral health services to a model that focuses on integrating a more limited set of services, such as an accountable care organization (ACO) that integrates different acute care providers (e.g., hospitals and primary care providers [PCPs]).
-
Financing. Integrated care models can also differ by the types of payers involved. For example, there are some systems that include the Medicaid and Medicare programs as the primary payers for services (e.g., fully integrated dual eligible special needs plans [FIDE-SNPs] or the Medicare-Medicaid Plans participating in the U.S. Department of Health and Human Services [HHS] Centers for Medicare and Medicaid Services [CMS] demonstrations under the Financial Alignment Initiative) while other systems focus on integration with just Medicare financing (e.g., shared savings ACOs).
-
Managing Organization. A variety of organizations manage integrated care models. Some of the more prominent systems are managed through health plans, while others are managed through provider-based organizations. In other cases, the integrated care model is managed through an organization that is both the health plan as well as provider of services for its members (e.g., Providers of All-Inclusive Care for the Elderly [PACE] programs, Geisinger Health System).
The organization of an integrated care model is reflected in how and what information is exchanged across the continuum of providers. Table 1-1 identifies a number of existing integrated care models that require information exchange across a variety of provider settings, including LTSS and post-acute care. The variety of integrated care models utilize different models of HIE that can foster coordination. Additional information about these models is provided in Appendix A, the Environmental Scan.
| TABLE 1-1. Integrated Care Models | |
|---|---|
| Integrated Care Model Type | Examples |
| Medicare-Managed Care SNPs | FIDE-SNPs:
C-SNPs and I-SNPs:
|
| Financial Alignment Demonstrations | To date, 11 states implemented demonstrations:
|
| Beacon Community Programs (2010-2014) |
|
| Health Homes |
|
| VHA |
|
| Medicaid MLTSS |
|
| Medicare ACOs |
|
It is important to note that no integrated care system has developed a perfect and seamless process for exchanging information. The care manager or care coordinator remains the key in bridging the informational gaps across the continuum of care; existing technologies can be useful tools in facilitating information exchange, but they are not the foundation.
However, these models each have important components that can inform how to best support the exchange of information among different providers across the continuum of care.
-
Integrated Care Models Function Within Localized Health Care Environments. The same model may not be transferable to another location, especially at the provider level. The fully integrated PACE program, for example, has not grown significantly and its processes may not be replicable in all regions, yet the program provides valuable lessons about information exchange and coordination that may be informative to other models of care.
-
Models Vary in the Degree of Integration or Range of Providers Included. Integrated care systems that include MLTSS, a growing model of care nationally, may be integrated well in some components but not in all components of the system. In some cases MLTSS programs have integrated the financing components but act just as a manager of vendor relationships in the other aspects of the care system.
-
Some Integrated Care Models Are Built around Unique Populations or Environments and Therefore May Not Be Transferrable to Other Populations. Although the Veterans Health Administration's (VHA) fully integrated care and comprehensive electronic medical record system is only relevant to the veteran population with its unique needs, the best practices developed by the VHA can be applicable to other populations who have high medical and LTSS needs.
1.3. What is Health Information Exchange?
Integrated care providers, including their partners, have a frequent need to exchange health information on behalf of their patients, who are among the most vulnerable and costly in our society. One of the key benefits of the use of HIT is the ability to exchange information to communicate and coordinate services on behalf of patients, and their physicians and entire care team who are often located in different geographic areas and practice settings (Dougherty, Williams, Millenson, & Harvell, 2013). This project examined both how information is exchanged (i.e., what methods or specific tools are used) as well as what types of information are exchanged among integrated care providers (i.e., what information providers find most useful).
1.3.1. Defining Health Information Exchange
The term "health information exchange" and its acronym "HIE" are often invoked in discussions about provider communication and information sharing, and they are used in both noun and verb forms. When used as a noun, HIE refers to the entities established to securely exchange health information (such as the Keystone Health Information Exchange [KeyHIE]). When used as a verb, HIE refers to the process of electronic exchange of health-related information and covers actions such as the electronic exchange of a physician prescription to a pharmacy or the electronic exchange of test results from a clinical laboratory to a primary care physician's electronic health record (EHR) (Karl, 2012; HIMSS, 2014). The concept of electronic exchange of health information (HIE) has been further described as the "capability to electronically move clinical information among disparate healthcare information systems, and maintain the meaning of the information being exchanged" (HIMSS, 2014). For purposes of this report, we will use the acronym HIE as a verb and will reference the noun form as HIE organization(s).
1.3.2. Health Information Exchange Adoption and Challenges
The ONC released the Report to Congress on Health IT Adoption and HIE in October 2014. The report highlighted metrics showing increased adoption of HIE by hospitals and physicians from the period prior to the Health Information Technology for Economic and Clinical Health (HITECH) Act and the most recent period for which adoption numbers were available. Adoption numbers for 2013 for various electronic information exchange activities are shown in Table 1-2. However, the report acknowledged that gaps and challenges remained for the widespread use of interoperable systems and HIE across the health care continuum, which are relevant to information exchange in integrated care systems, noting the following:
-
Post-acute and institutional LTSS, most behavioral health, and lab providers not eligible for EHR incentive payments have limited involvement in HIE.
-
Close to 40% of Medicare beneficiaries discharged from acute care hospitals go on to receive services in post-acute care settings such as skilled nursing facilities and rehabilitation hospitals; however, there is presently little capacity to support HIE across these settings.
-
HIE is problematic in rural areas where high-speed Internet service, the primary infrastructure for HIE, is not always readily available.
-
Despite increased data exchange among hospitals, communication deficits continue largely due to factors not related to technology, such as organizational culture and provider workflow.
In addition, the June 2015 report by NORC at the University of Chicago titled "Provider Experiences with HIE: Key Findings from a Six-State Review," also presented insights related to evolving expectations for HIE and the role of HIE in supporting care coordination (Dullabh, Hovey, & Ubri, 2015). The NORC report summarized findings from a data collection activity that is part of a multi-year evaluation of the effect of the ONC State HIE Program on HIE progress.
Citing increased provider focus on integrated, patient-centered care in support of new payment models, the report identified areas of HIE expansion. Prior emphasis on HIE to connect disparate systems and meet meaningful use exchange requirements (e.g., eprescribing, lab exchange) is evolving into looking to HIE as a means to provide actionable information from across the care continuum to improve care delivery and coordination. Highlighted needs for information exchange included:
-
Admission, discharge, transferalerts, to provide timely notification of patient encounters with hospitals and other care settings.
-
Care coordination across the care continuum, to facilitate communication and coordination between providers across care settings (including long-term care, home health and behavioral health).
-
Interstate and regional exchange, to support exchange of data across state lines for patients accessing out-of-state care, and to mitigate challenges such as differing state laws and requirements related to health information privacy and disclosure, consent models, and interoperability between systems.
| TABLE 1-2. HIE Adoption as of 2013 | ||
|---|---|---|
| Information Exchanged/Activity | HIE Among Hospitals, % |
HIE Among Physicians, % |
| Shared data electronically with physicians or hospitals outside of their organization | 62 | 14 |
| Radiology reports | 55 | --- |
| Laboratory results | 57 | --- |
| Clinical care summaries | 42 | --- |
| Medication lists | 37 | --- |
| Send and receive secure electronic messages containing patient health information | 41 | --- |
| Capability for providers to electronically query patient health information from sources outside of system | 51 | --- |
| Provide electronic notification to PCP when patient enters emergency department | 24 | --- |
| Sent prescriptions electronically via Surescripts (1 of the nation's largest e-prescribing networks) | --- | 70 |
| New and renewal prescriptions sent electronically | --- | 57 |
| Capability to order lab tests electronically | --- | 69 |
| View lab results electronically | --- | 77 |
| Provide patients the capability to view online, download, or transmit information from medical record | --- | 42 |
The report also discussed challenges and lessons learned related to HIE, including issues such as:
-
Services and Infrastructure. The study found that providers were primarily exchanging information through services that were not led by the state HIE program (such as internal HIE systems of large health systems where affiliated providers are given access to the system). While use of private exchange systems is currently a common process, providers did see potential value in community and statewide HIE systems.
-
High Cost of HIE Participation. Both hospitals and providers identified cost as a key barrier to establishing HIE connections. EHR vendor fees associated with connecting to outside systems can be substantial, with costs for even smaller practices estimated at $13,000-$22,000 to cover interface set-up, monthly service, and product upgrades associated with establishing cross-provider connectivity. Such fees can be burdensome and must be evaluated against other provider/organization priorities. Larger hospital systems with affiliated providers have found it worthwhile to address the cost burden issue by subsidizing connectivity associated fees for practices who cannot afford it on their own.
-
Limited Vendor Support for Providers Ineligible for Meaningful Use. Providers ineligible for meaningful use incentives (such as nursing homes and home health agencies) have experienced difficulty in receiving needed connectivity support from large commercial vendors who are often focused on implementing systems for hospitals and providers eligible for the EHR Incentive Program. In addition, many of these ineligible providers use niche market systems (e.g., software designed specifically for nursing homes or rehabilitation facilities), necessitating cooperation across vendors to enable electronic exchange of health information.
-
Lack of Interoperable Systems. Providers have noted difficulty in exchanging clinical care summary documents due to differences in how these documents are created in the various hospital and provider EHR systems. Various EHR vendors have interpreted and implemented the standards for summary documents differently, resulting in the inability of systems to incorporate information from the summary documents into the EHR and creating inefficiencies in information exchange as well as barriers to care coordination.
1.4. Project Methodology
We relied on several strategies to identify and understand information exchange processes used in integrated care models. We first conducted an environmental scan of existing integrated care models. We then held a TAG meeting with several experts in the areas of integrated care models and information exchange processes to discuss relevant issues and identify potential sites for case studies or to serve as SMEs. Based on the TAG's recommendations, we conducted SME interviews and three case studies to learn more about the specific processes used among various integrated care models in different areas of the country.
1.4.1. Environmental Scan
The RTI team conducted an environmental scan of integrated care models throughout the United States to provide background material for the TAG, to inform site selection for the case studies and identify key informants. We compiled a list of existing initiatives designed to fully integrate and coordinate acute care and LTSS. For each identified integrated care initiative, the team reviewed publicly available literature by conducting electronic searches of MEDLINE using PubMed, JSTOR, Google Scholar, and the Grey Literature Report as well as review programmatic web sites and project reports. Each model is described in detail with a general overview, including any particulars about its information exchange processes, followed by a list of resources and specific examples in states or communities throughout the United States (see Appendix A).
1.4.2. Technical Advisory Group
The purpose of the TAG meeting was to provide further refinement regarding the goals of the project, feedback on the environmental scan, recommendations for case study sites, and to review the site visit protocols. A list of possible TAG members was presented to the HHS Office of the Assistant Secretary for Planning and Evaluation (ASPE) and approved experts were invited to participate in the meeting. The TAG meeting was held in-person in Washington, DC on March 24, 2014, and included the following members:
- Michelle Dougherty, AHIMA Foundation (now with RTI International)
- Kathy Leitch, Health Management Associates (no longer with this organization)
- Cheryl Phillips, LeadingAge
- Carol Raphael, Manatt Health Solutions
- Tim Schwab, Tim Schwab Healthcare Solutions, Inc.
- Christine van Reenen, SNP Alliance
- Terrence O'Malley, Partners HealthCare System, Inc.
1.4.3. Subject Matter Expert Interviews
To supplement the findings of the environmental scan and site visits, RTI identified individuals with expertise in LTSS and acute care, information exchange, and care coordination and sought additional perspectives and information not covered by the TAG membership. RTI held five interviews with seven SMEs. The following SMEs were consulted for this project:
- Gary Jessee, Star PLUS Texas
- Pam Parker, SNP Alliance and Maureen Murray, South Country Health Alliance
- April Brenner, VHA Westwood
- Kathryn Cabell and Chris Stevens, Billings Clinic
- Cindy Burke, Atlanta Regional Community-Based Care Transition Program
1.4.4. Site Visits
RTI staff reviewed the TAG site selection recommendations and worked with ASPE staff to narrow the list of potential sites. Site selection criteria included choosing a variety of model types (e.g., ACO, MLTSS, or Medicare SNP), type and size of population served, scope of model, and program longevity. After extensive coordination efforts on the part of the sites and RTI, we conducted three site visits: Geisinger Health System, the Minnesota Senior Health Options (MSHO) program and HealthPartners, and Community Care, Inc. (CCI) of Wisconsin. Each site is described in more detail below and in Appendices B, C, and D. To gain an understanding of the information exchange processes from different perspectives involved with these integrated care systems, we developed interview protocols that focused on four stakeholder groups: program leadership, program staff (e.g., care managers or care coordinators, PCPs), HIT program staff, and external partners (e.g., community LTSS providers, nursing homes).
The case study sites represent an assortment of integrated care models, and each site represented more than one integrated care model. All three sites include systems that both deliver as well as manage the care for their beneficiaries.
Geisinger (ACO, Medicare Advantage Plan and Health System)
Geisinger is an integrated care model that delivers care through its health system and provides coverage through its health plans. The Geisinger health system participates in an ACO and has a Medicare Advantage Plan for its Medicare beneficiaries. The Geisinger health system also includes the Proven Wellness Neighborhood program, developed from Geisinger's Patient Centered Medical Home program "ProvenHealth Navigator." The Proven Wellness Neighborhood program targets individuals in the community who have high medical and support service needs and uses licensed social workers and community health assistants to connect individuals with needed community support services.
Minnesota: MSHO (FIDE-SNPs) and Special Needs BasicCare (Medicaid managed care), Bluestone Physician Services, and HealthPartners (FIDE-SNP and Health System)
Minnesota has developed several managed care options for their senior and persons with disabilities populations. MSHO is a FIDE-SNP that combines Medicare and Medicaid health programs and support systems into one health care package. It is for people aged 65 and older who are eligible for Medicaid and enrolled in Medicare Parts A and B. People can choose to join MSHO or stay in their current Medicare Advantage program. The Minnesota Special Needs BasicCare (SNBC) program is a voluntary managed care program for people with disabilities aged 18-64 who have Medicaid. SNBC enrollees may have a care coordinator or navigator to help them access health care and support services. Bluestone Physician Services is a physician-led model that provides on-site primary care in residential care settings as well care coordination services for seniors and persons with disabilities. HealthPartners is a non-profit integrated health care system that participates in the MSHO program as a participating FIDE-SNP.
Wisconsin Community Care, Inc. (PACE, FIDE-SNP, MLTSS)
Wisconsin's CCI includes a PACE program, the Partnership program (an FIDE-SNP) for Medicare-eligible and Medicaid-eligible older adults and adults with disabilities, as well as the Family Care program (a Medicaid MLTSS plan). The programs all rely on a model that uses interdisciplinary teams to provide individualized care, including acute and LTSS providers (e.g., home care).
2. THEMES FROM SITE VISITS AND SUBJECT MATTER EXPERT INTERVIEWS
Communicating necessary and timely information to providers across the continuum of care is central to providing coordinated care. Individuals with LTSS needs require a number of people to be involved to provide care and support, and all of these providers require specific information about each individual. A high level of care coordination and particular focus on exchanging information is required to ensure that all of the providers can understand the full picture of what the individual needs and provide the appropriate care and support.
The site visits and SME interviews helped specifically identify how information is exchanged among the various providers participating in integrated care arrangements. This section provides some key themes that emerged from our site visits and interviews with SMEs around information exchange. We have divided these themes into three main research questions:
-
How is information exchanged?
-
What information do providers want to receive, and do they receive it?
-
What are the remaining gaps or challenges to exchanging information?
2.1. How is Information Exchanged?
An important take-away from our site visits, SME interviews, and literature review was the importance of personal relationships in the information exchange processes related to care coordination--even in scenarios where access to electronic data is in play. Care coordination and the supporting exchange of information are still very high touch processes (Bates, 2015). Communication and developing relationships with community providers is key, particularly for providers external to the organization. Technology can be a valuable tool in facilitating communication and information exchange, but organizational trust and personal relationships between the providers is still foundational to successful care coordination. Personal communications and relationships foster an understanding of the role and information needed by the integrated care provider to coordinate timely, appropriate services for the patient.
As for electronic exchange of health information, EHR adoption, interoperability standards, and services to support HIE are all key factors to enabling this process. The ONC 2014 Report to Congress indicated that EHR adoption has increased significantly among acute care hospitals, critical access hospitals (CAHs) and professionals eligible for CMS EHR financial incentives authorized under the HITECH Act. June 2014 metrics showed 75% of the nation's eligible professionals and 92% of hospitals/CAHs had received the CMS EHR incentives (ONC, 2014). There has also been continued progress in establishing standards and services that support HIE. However, despite these advances, 2013 metrics also show that actual practice patterns are not following through on the promise of electronic exchange of information across organizational, vendor, and geographic confines. Only 14% of physicians electronically shared patient information outside of their organization, while 62% of hospitals engaged in external electronic information exchange (ONC, 2014).
Additionally, the absence of EHR incentives in settings such as post-acute care, LTSS and behavioral health has left adoption of HIT as a lower priority among setting providers. For example, a national study in 2012 found that EHRs were used in only 20% of residential care facilities (includes personal care homes, adult care homes, board and care homes, and adult foster care). Electronic exchange of information and care coordination activities among all providers could be advanced through better alignment of HIT capabilities across settings (ONC, 2014).
Our site visits were largely congruent with findings cited in the ONC Report to Congress, and our points of convergence are highlighted below:
-
Increased Adoption of EHRs among Providers Receiving Financial Incentives. EHRs were implemented in the hospital (Geisinger, HealthPartners) and physician practice (Geisinger, HealthPartners, CCI) settings--allowing the organizations to capture CMS EHR financial incentives. Organization providers and case managers have access to current and historical information on patient's seen in the health system/organization through the EHR. There is some use of internal EHR messaging functionality for care coordination purposes. In addition, affiliated providers (e.g., ACO partners, nursing homes and home health agencies owned by the health system) and case managers for health plans are provided access to EHR data, as authorized by the patient, through EHR web portals such as EPIC Care Everywhere.
-
Low Rates of Sharing Data Electronically with Providers Outside of the Organization. For patient's receiving care and services from providers external to the organization, electronic information exchange processes were varied, a secondary process, and included:
- secure e-mail (CCI);
- secure messaging through Direct (Billings);
- electronic transfer of continuity of care documents (CCDs) via Direct messaging (CCI); and
- information exchange through a formalized HIE organization (Geisinger).
However, while some electronic exchange of information did occur with providers outside of the organization, by and far the most common methods of information exchange with such providers remains phone, fax, and hardcopy (Geisinger, HealthPartners, CCI). Care managers from our visit sites reported continued reliance on more manual information exchange methods in relation to obtaining information from physician offices and hospitals external to the organization.
-
Low Adoption of EHRs/HIE by Long-Term and Post-Acute Care Providers (e.g., nursing homes, home health, and residential care) not Receiving Financial Incentives. Electronic exchange of information with this provider community is largely not occurring, with care coordinators or care managers reporting continued reliance on more manual information exchange methods (phone/fax/hardcopy) in relation to exchanging information with these providers. However, some promising practices that support electronic information exchange without requiring an EHR include:
-
Bluestone Physician Services, a physician-led model in Minnesota providing on-site primary care in residential settings, is a promising exemplar that has implemented a proprietary care coordination communication system to facilitate timely, electronic communication with their client facilities.
-
KeyHIE Transform™, a web-based subscription service, enables a nursing home or home health agency to contribute patient information to a HIE organization based on electronic assessment data the provider is required to submit to CMS. Data generated from a Minimum Data Set (MDS) system (nursing homes) or Outcome and Assessment Information Set (OASIS) system (home health) is then converted into a CCD containing the patient assessment information and made available to appropriate HIEs. The process is Health Insurance Portability and Accountability Act (HIPAA) and protected health information compliant and works with or without an EHR system.
-
2.2. What Information Do Providers Want to Receive and Do They Receive It?
Through our site visits, SME interviews, and literature review we learned that the information providers want to receive differs based on the provider type (Byrne & Dougherty, 2013). These differences, discussed below and presented in Table 2-1, were most apparent when comparing the preferences of acute care providers versus post-acute and LTSS providers. Consideration that not all providers want or find it useful to receive all information about an individual is key to supporting a system that can coordinate care and have providers easily and efficiently access the appropriate information to ensure quality care.
Across all provider types, we also noted that the method of information exchange had a direct impact on whether desired information was received. Primary examples include:
-
In situations where information exchange is supported by access into the EHR (such as by web portal), the provider may have full access to all current and historical health information on the patient, however such access will be determined by factors such as provider privileges, patient authorization, and organizational policy.
-
In situations where electronic information exchange or EHRs are not available, information is conveyed by more manual methods such as phone, fax, or hardcopy. These methods can create information gaps due to situations such as missed calls,incomplete information faxed or copied, or misrouted faxes.
2.2.1. Acute Care Providers
Acute care providers working in integrated care models, particularly PCPs, often preferred a clinically focused snapshot of the individual, including information that is directly related to the patient's visit such as the diagnosis list, medication list, allergy list, immunizations, and problem list. Even when caring for individuals with LTSS needs, many of the acute care providers interviewed did not find value in receiving information on the more global goals of the patients or their care plans. Providers maintained that if they needed more information on the patient, they would prefer to access the additional information through a different process than the exchange of the initial snapshot of immediate information. In our discussions with staff physicians at Geisinger, they often found that the amount of documentation and level of information exchanged was too much for a provider to handle at once. In the cases where they received LTSS and behavioral health information or a patient's LTSS or overall care plan, for example, the providers often just added this documentation to a growing pile of papers in their clinics that were rarely consulted, if ever.
2.2.2. Post-Acute, Long-Term Services and Supports, and Behavioral Health Providers
Post-acute and LTSS providers, on the other hand, generally wanted a more comprehensive picture of the individual compared to their acute care partners. In addition to the medically focused information that the acute care providers wanted, post-acute and LTSS providers also wanted the LTSS and behavioral health information about an individual, such as the information from an individual's functional and cognitive assessments and overall LTSS and medical care plans. The preferences for information depended on the LTSS or other community-based provider type. In some cases, information about an individual's care plan was necessary for state licensing requirements for certain community-based residential care facilities. Per state licensing requirements, residential care facilities in Minnesota and Wisconsin must have a care plan for each resident, so these providers wanted information from all other care plans that had been created for the individual. Although this project does not focus on behavioral health, we did interview some behavioral health providers participating in the integrated care models. These behavioral health providers wanted to make sure they had information on an individual's past medical and medication history, current medication list, any previous behavioral health diagnoses and how past providers arrived at those diagnoses, and past treatments that may have worked or not worked.
2.2.3. Care Coordinators or Care Managers
The care coordinators or care managers, who were used by all of the integrated care models we visited, were of the mindset that more is better, including details around all providers and support services the individual had accessed or had plans to access. For example, Area Agency on Aging (AAA) staff in Pennsylvania, which partners with Geisinger, administers and coordinates home and community-based services (HCBS) waiver services in the state for individuals age 65 or older, mentioned that any information on provider referrals was important to have. They also value information about individuals' living situations and whether an individual has transportation issues. Among the care coordinators for CCI members, the most important information elements about an individual included past medical history including hospitalizations, chronic conditions and baseline medical information, especially if the individual was newly enrolling in a CCI program. They also valued information about any behavioral health history.
| TABLE 2-1. Summary of Information Providers Want to Receive, by Provider Type | ||
|---|---|---|
| Provider Type | What Information Do Providers Want? | |
| Acute care providers (e.g., PCPs, hospital providers) |
|
|
| Post-acute and LTSS providers |
|
|
| Care coordinator/case manager |
|
|
2.2.4. Displaying Information by Provider Type
In addition to the importance of supporting the different information needs of various provider types, how the information is displayed when accessed by the provider is also important. This point was particularly relevant for providers working within an integrated care model that had EHRs, where there was an abundance of information. A family medicine provider may need access to certain data elements about a person as an easily accessible snapshot whereas a surgeon may need similar information but at a clinically different level that may require more extensive detail. When we spoke with staff from the Billings Clinic in Montana, they emphasized that more information is better because of the complexity of health care and because providers should have as much information as possible to provide quality care.They also emphasized how important it was for EHR systems to support customized views of exchanged information based on what is important to the specific provider type. When a provider accesses the EHR, for example, the first screen shot should have the information most relevant to that type of provider.
Several participants raised questions about whether all providers should have access to all information. There was not common agreement among the site visit participants and interviewees about the extent to which providers should have access to all information based on HIPAA requirements related to restricting patient information to the "minimum necessary" for the intended purpose. Some informants emphasized the necessity of restricting certain EHR content based on provider type. In their view, LTSS providers who were more tangential to providing care or support services to an individual would not need to see that person's entire medical record. On the other hand, the Billings Clinic in Montana, which is an ACO, emphasized that they make sure that their entire EHR is open to all of the providers employed or managed by their organization (e.g., hospitals, PCPs, nursing facility, and assisted living facility) and had worked hard to ensure that was so. This open access required "monumental legal work" to ensure that all of their providers were still compliant with HIPAA and any other regulatory provisions on privacy.
2.3. What Are the Remaining Gaps or Challenges to Exchanging Information?
The care systems we visited and spoke with also provided insight about remaining gaps and challenges to exchanging information even within a fully integrated care system. Barriers to optimal information exchange emerged in the conversations we had across all of the site visits. Some of the challenges were related to state or federal regulatory requirements. Other issues were related to the development of EHRs and their applicability to integrated care systems. And finally, LTSS providers were generally external partners to the integrated care systems and lacked EHRs, which contributed to challenges in the exchange of information.
2.3.1. Applicability of Existing Electronic Health Records for Integrated Care Systems
The use of EHR systems has become standard across most health systems, including hospitals and clinics. This trend also includes many integrated care systems with whom we met--all of the sites we visited had implemented an EHR. However, all of the systems mentioned that it was difficult to find an EHR that worked well for their integrated care focus. Providers in integrated care models must have the ability to document information regarding medical, LTSS, and behavioral health needs and services, yet most EHRs are only designed to support clinical aspects of care. Therefore, the LTSS and behavioral health information is entered into narrative notes in the EHR where it is harder to navigate and locate such information. In other instances, the integrated care model uses a separate case management system that is more appropriate for capturing the necessary non-medical information (such as contact, health plan, and LTSS and behavioral health information) needed for care management and coordination. The care managers at HealthPartners, for example, use the Care Partner case management system to track all their information about individuals receiving case management services. They then separately input select data from their system into the broader EPIC EHR system that is used by all of the HealthPartners providers. Geisinger case managers also mentioned using a separate case management system (Human Services Information Systems) to document similar LTSS and behavioral health information about a member.
Many of the existing EHR systems are not equipped to handle the number of patient encounters seen by an integrated care model that provides care to high needs populations. For example, CCI, which serves more than 10,000 enrollees and focuses on populations with high health care and LTSS needs, reported that they have roughly 90,000 encounters just in one month, which is much higher than the average practice in a health care system.
Site visit participants also discussed interoperability issues among different EHRs that created challenges for exchanging information with providers outside of their integrated care system. In many cases, the integrated care system staff had to rely on faxing and making phone calls to exchange information with other health care systems. Exchanging information through faxes and phone calls often affects the timeliness of the information being exchanged. Timing can be critical, for example, when information is needed to support transitions for high needs individuals from hospital to home to ensure appropriate home care services are in place. This was noted as one of the biggest issues for South County Health Alliance, whose staff reported difficulty in getting information about hospital discharges in a timely manner.
And as noted previously, the presentation of exchanged information in a format that is relevant and consumable by the receiving provider is critical. Our experts and site informants reported challenges regarding locating desired exchanged documents in the EHR, as well as issues with consuming the content (e.g., the document format is foreign to recipient, making it difficult or time-consuming to locate information; or content is too granular or not detailed enough for the receiving provider). Some site visit participants also indicated that they still needed to figure out how to standardize data within their own health care systems so that it could be exchanged across HIEs. Their efforts to exchange information uncovered a range of inconsistencies in how providers and external health systems capture data as well as inconsistencies in service definitions.
Providers also view the high costs of establishing and maintaining EHR interfaces with electronic information exchange partners as a barrier to information exchange. The EHR vendor fees associated with connecting to outside systems can be substantial and such fees can be burdensome. Providers and health systems must evaluate the need to electronically connect with outside systems against other organizational priorities. For example, CCI noted that they needed to consider costs when determining partnerships to pursue for HIE (e.g., external health systems, the state HIE). In addition to EHR vendor costs to establish connectivity to access the state HIE, CCI has to pay to be a member of the state HIE and subscribe to each component of the HIE that the organization would like to access for their providers and staff.
2.3.2. Long-Term Services and Supports Providers
Although all of the integrated health care systems served populations with LTSS needs and provided coverage for LTSS, a majority of the LTSS providers were not part of the integrated care system. This was particularly true among the HCBS providers who tended to be more isolated from the integrated care systems. HCBS waiver services were often administered through the county (Minnesota) or through a local agency (AAA in Pennsylvania) and therefore the providers of such services were not part of the integrated care systems. With few LTSS providers as part of the integrated care systems, few LTSS providers could access the integrated care systems EHRs or other information exchange tools. In some cases the LTSS providers continued to have a difficult time accessing necessary information about the beneficiaries. For example, one AAA mentioned that they often had to physically walk over to some of the nearby hospitals to get discharge information about individuals needing LTSS.
LTSS providers are ineligible for Meaningful Use incentives and therefore have experienced particular difficulties in receiving needed connectivity support from large commercial vendors who are often focused on implementing systems for hospitals and providers eligible for the EHR Incentive Program. Many LTSS providers also use EHR software designed specifically for their settings (e.g., nursing homes or rehabilitation facilities), which then requires cooperation across the larger acute care vendors to enable electronic exchange of health information.
2.3.3. Regulatory Concerns
At every site visit, we heard concerns about the challenges to meet regulatory requirements and foster the exchange of information among providers. Several staff mentioned how federal Health Insurance Portability and Accountability Act (HIPPA) regulations on exchanging personal health information contributed to gaps in the exchange of needed information among providers. Each of the integrated care systems we spoke with both delivered services and managed services for their members as a health plan. Many of the systems' staff reported that external providers (e.g., community physicians' offices) are sometimes confused about whether HIPAA allows a health plan's care coordinator or care manager to access or receive a member's personal health information. For example, CCI staff reported that some physician offices will not send a member's past medical history to the CCI team based on the physician's office interpretation of HIPAA rules.
The HIPAA requirements appeared to create a barrier even when a system had been developed to facilitate information exchange. The EPIC Care Everywhere portal was developed to help with information exchange with providers external to integrated care system, yet HealthPartners providers reported that they still find it challenging to get all the information they need for coordinated patient care. The Care Everywhere applications accessed by HealthPartners providers do not allow access to a patient's record through the portal unless a signed patient authorization is in place for that particular episode of care. For example, if a patient has three hospitalizations, separate patient authorizations for each hospitalization are needed for the provider to access all three records. According to some HealthPartners providers, system requirements implemented to support HIPAA and other privacy regulations are too rigid and lead to barriers in the seamless exchange of information and better care coordination.
In addition, concerns about privacy were particularly evident when speaking about behavioral health issues. Many of the care teams and PCPs indicated that they had a hard time accessing adequate behavioral health information about an individual. The behavioral health providers indicated that they could not share information with other providers due to HIPAA and other federal regulations around exchanging specific behavioral health information. When speaking with HealthPartners providers, we learned that these instances occurred even when the behavioral health provider was part of the same network as the other providers of the integrated care system. The federal confidentiality law and regulations (codified as 42 U.S.C. §290dd-2 and 42 CFR Part 2 ["Part 2"]), focuses on confidentiality of substance use disorder diagnoses and treatments specifically. Part 2 permits patient information to be disclosed to HIE systems; however, the regulation requires patient consent for disclosure of the information. These regulations, however, do not apply to mental health conditions, despite many behavioral health providers refraining from sharing any information with other providers also providing services to an individual.
In some cases, requirements for exchanging specific information between providers and federal and state agencies were viewed as burdensome and not conducive to supporting the provision of coordinated care. Care coordinators spoke about the disconnect between CMS requirements for documenting the care planning process and the information needed to develop a care plan. They perceived that the documentation requirements got in the way of the care planning process. For example, CMS regulations require SNPs to document a number of modelof care elements for each member, including individualized care plans. In Minnesota, the counties often found these Medicare SNP requirements to be burdensome with too much paperwork and often detrimental to developing comprehensive care plans for the individuals. The health plans also have certain requirements around documenting care plans. Some counties provide care coordination services for more than one health plan in Minnesota, so the health plans developed a collaborative care plan that was a standardized tool that all counties could use when documenting care plans. While helpful in addressing the documentation requirements, this tool was perceived as being only for auditing purposes rather than actually benefiting patient care.
2.3.4. Connectivity Challenges in Rural Regions
The 2014 ONC Report to Congress identified problematic high-speed Internet service in rural areas as one of the challenges in advancing HIE. As high-speed Internet service is the primary infrastructure for HIE, it is critical to rural providers that such service is always readily available (ONC, 2014). This HIE challenge was also identified in our Minnesota and Wisconsin site visits and SME interviews.
3. CONCLUSION: FUTURE DIRECTIONS
Fully integrated care models provide insights about how coordinated care is operationalized through information exchange, particularly for individuals with high health and LTSS needs. These systems have demonstrated that while technology and the use of EHRs has facilitated a more seamless process to communicate along the continuum of care--primarily within health care systems, yet less so with providers external to the health care system with whom they share patients--the technology has its limits. Fully integrated care models with extensive experience and highly developed activities to support coordination continue to rely on the individual care coordinator or care manager to be the primary conduit in which information is collected, exchanged, and used to provide coordinated care.
|
Key Findings Efforts to better understand information exchange in integrated care models reflect the following key findings:
|
Substantial challenges and barriers remain to having a seamless and efficient exchange of information, even within fully integrated care systems and particularly across acute and LTSS providers. Several of these challenges are external to the integrated care system itself, including certain regulatory requirements or the capacity of certain providers (e.g., home and community-based providers) to fully integrate themselves within a health care system. As policymakers focus on promoting coordinated care, it is important to consider that not even fully integrated care systems are able to establish a seamless information exchange process at this time.
-
The personal relationships established between providers and other care staff are foundational to seamless information exchange and successful care coordination. Technology can be a valuable tool in facilitating communication and information exchange, but organizational trust and personal relationships between the providers is still foundational to successful care coordination. Personal communications and relationships foster an understanding of the role and information needed by the integrated care provider to coordinate timely, appropriate services for the patient.
With this finding, policymakers may consider continued support of projects that encourage building relationships among community providers. For example, the Community-Based Care Transition Programs fosters relationships between hospital discharge planners and other community providers to avoid readmissions for high-risk Medicare beneficiaries.
-
Despite the technological advancements made in information exchange approaches in health care, existing EHRs are not adequate for integrated care models at this time. The personal communication and relationships required for successful information exchange and care coordination can be greatly facilitated by access to EHRs. However, most EHRs are primarily designed to support medical aspects of care and tend to be more focused on episodic, acute care, rather than capturing the continuity of medical, LTSS, and behavioral health needs and services that are critical to integrated care models. As EHRs and other tools for information exchange move forward, incorporating and supporting additional non-medical information, such as LTSS and behavioral health information, will be key to achieving more integrated provision of care.
Furthermore, how information is displayed and available to providers is keyto successful information exchange. Providers need tailored views that are limited to the key elements of interest to them and easy to access. And as noted previously, the presentation of exchanged information in a format that is relevant and consumable by the receiving provider is critical and often needed. Our experts and sites reported challenges regarding locating desired exchanged documents in the EHR, as well as issues with consuming the content (e.g., document format is foreign to recipient making it difficult or time-consuming to locate information; content is too granular or not detailed enough for the receiving provider).
Policymakers could consider how to encourage and support the development of EHRs that are more relevant to the range of services provided in integrated care systems. EHRs that would be more applicable to integrated care models would need to support capturing LTSS and behavioral information in a format that could be easily searched and accessed by the range of providers working within an integrated care model. EHR developers also need to consider supporting the customization of information display so that the receiving provider is able to access the information in a manner relevant to that provider type.
-
Our findings of low adoption of EHRs by LTSS providers (e.g., nursing homes, home health providers, residential care facilities) were congruent with other study results, such as the ONC 2014 Report to the Congress. The electronic exchange of information with this provider community is largely not occurring. Care coordinators and managers in the case study sites reported a continued reliance on manual information exchange methods such as phone, fax, or exchanging hardcopy documents when communicating and exchanging information with LTSS providers.
Because LTSS providers are currently not included in any Meaningful Use financial incentives for EHR adoption, policymakers might consider extending these incentives to LTSS providers. Policymakers might also consider identifying and supporting adoption of alternative technological approaches to information exchange such as the Bluestone Bridge communication portal or other community web-based portals.
-
Informants from all of the sites mentioned that misunderstandings and differences in HIPAA interpretation are key barriers to exchanging and accessing needed information about individuals. Particularly for integrated care systems that are also health plans, many of the systems' staff reported that external providers were sometimes confused about whether HIPAA allows a health plan's care coordinator or care manager to access or receive a member's personal health information. Furthermore, we heard from many informants that the lack of standard definitions and rules about how providers can connect with one another, particularly a provider from one system to a provider in another system, is another major challenge to efficient information exchange. As CCI staff noted, each hospital system that allows outside providers access to their EHR has different rules about who can access the EHR and what EHR information they can access.
Policymakers could consider increasing education and clarifying the interpretation of HIPAA privacy regulations. A clearer understanding of what personal, health, and LTSS information is legally allowed to be exchanged under HIPAA regulations would be valuable to health care systems trying to develop better information exchange practices. Furthermore, the increase in state-sponsored or supported HIEs is also forcing policymakers to determine what information can be exchanged and HIT administrators to figure out how to standardize data within their own health care systems. Efforts to exchange information have uncovered a range of inconsistencies in how providers and health systems capture data as well as inconsistencies in service definitions. In order to have a functional HIE, these inconsistencies would have to be addressed, which would also require addressing how staff collect and report the data.
REFERENCES
Bates, D. (2015). Health information technology and care coordination: The next big opportunity for informatics? International Medical Informatics Association Yearbook, 2014. http://dx.doi.org/10.15265/IY-2015-0020.
Byrne, C., Dougherty, M. (2013). Long-term and post-acute care providers engaged in health information exchange: Final report. Retrieved July 9, 2015, from http://aspe.hhs.gov/report/long-term-and-post-acute-care-providers-engaged-health-information-exchange-final-report.
Dougherty, M., Williams, M., Millenson, M., Harvell, J. (2013).EHR payment incentives for providers ineligible for payment incentives and other funding study. Retrieved June 26, 2015, from http://aspe.hhs.gov/basic-report/ehr-payment-incentives-providers-ineligible-payment-incentives-and-other-funding-study.
Dullabh, P., Hovey, L., Ubri, P. (2015). Provider experiences with HIE: Key findings from a six-state review. Retrieved June 25, 2015, from http://www.healthit.gov/sites/default/files/private/reports/provider_experiences_with_hie_june_2015.pdf.
Eoyang, G., Grossman, L. (2013). Minnesota Disability Health Options (MnDHO): Review and lessons learned. Circle Pines, MN: Human Systems Dynamics Institute for Minnesota Department of Human Services. Retrieved from https://edocs.dhs.state.mn.us/lfserver/Public/DHS-6817-ENG.
Gröne O., Garcia-Barbero M. (2001, June 1). Integrated care: A position paper of the WHO European Office for Integrated Health Care Services. International Journal of Integrated Care. Retrieved from: http://www.ijic.org/.
Healthcare Information and Management Systems Society (HIMSS).(2014). FAQ: Health information exchange. Retrieved from http://www.himss.org/library/health-information-exchange/FAQ.
Karl, E. (2012). What's in a name? Breaking down health information exchange, one definition at a time. Journal of AHIMA, 83(6), 62-63. Retrieved from http://www.ahima.org .
Kodner, D., Spreeuwenberg, C. (2002). Integrated care: Meaning, logic, applications, and implications--A discussion paper. International Journal of Integrated Care, Oct-Dec, 2, e2. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1480401/.
Lind A., Gore S. (2010). From the beneficiary perspective: Core elements to guide integrated care for dual eligible--Technical assistance brief. Center for Health Care Strategies. Retrieved from http://www.chcs.org/usr_doc/TCDE_Core_Elements_122010.pdf.
Office of the National Coordinator for Health Information Technology. (2013). Certification guidance for EHR technology developers serving health care providers ineligible for Medicare and Medicaid EHR incentive payments. Washington, DC. Retrieved from http://www.healthit.gov/sites/default/files/private/generalcertexchangeguidance_final_9-9-13.pdf.
Office of the National Coordinator for Health Information Technology (2013). Issue brief: Health IT in long-term and post acute care. Washington, DC. Retrieved from http://www.healthit.gov/sites/default/files/private/pdf/HIT_LTPAC_IssueBrief031513.pdf.
Office of the National Coordinator for Health Information Technology.(2014). Report to Congress: Update on the adoption of health information technology and related efforts to facilitate the electronic use and exchange of health information. Washington, DC. Retrieved from http://www.healthit.gov/sites/default/files/private/rtc_adoption_and_exchange9302014.pdf.
RTI International & Leading Age. (2014). Support and Services at Home (SASH) evaluation: First annual report. Retrieved from http://aspe.hhs.gov/report/support-and-services-home-sash-evaluation-first-annual-report.
APPENDIX A. ENVIRONMENT SCAN
A.1. Introduction
The purpose of this project is to describe the current practice of HIE in integrated care systems. To gather details on HIE, RTI International will conduct a comprehensive environmental scan, convene a TAG, interview SMEs, and conduct case studies of existing integrated plans. The goal of the project is to look inside the "black box" of existing integrated care systems to discover how they exchange information--one of the key characteristics of integrated care. Findings from the project will identify areas for improvement as well as promising practices that may be useful to understanding HIE practices, especially for managed care plans participating in the State Demonstrations to Integrate Care for Dual Eligible Individuals and other SNPs. The findings also will provide needed information to ONC about how LTSS and post-acute care providers use HIT and participate in electronic HIE.
Specifically, the project will address the following research questions:
-
What information is being exchanged between LTSS and acute care providers in integrated care arrangements?
-
What systems do integrated care arrangements use for HIE?
-
Which providers are using the information?
-
What information is most useful to providers in the acute and LTSS systems? How do acute care and LTSS providers organize care as a result of HIE?
-
Are there specific financing or policy barriers to efficient and timely information exchange in integrated care systems?
This document presents the environmental scan, which includes a number of existing integrated care models that offer information exchange across provider settings, including LTSS and post-acute care. Each model is described in detail with a general overview, followed by a list of resources and specific examples in states or communities throughout the United States. After the model descriptions, Table A-1 presents all of the discussed model types, including their definition, HIE relevance, and existing examples.
A.2. Integrated Care Models
A. Medicare Managed Care Special Needs Plans (SNPs)
|
Medicare Advantage Plans were developed in 1997 to provide Medicare Part A (hospital coverage) and Part B (provider coverage) through capitated managed care plans. As of 2003, most Medicare Advantage plans also include Medicare Part D (medication coverage). Because individuals may incur copayment costs and may have different rules set by a private insurer, Medicare Advantage plans function similarly to private insurance obtained through an employer; in this case, Medicare assumes the role of the employer in defraying some health insurance costs. Like other types of private coverage, Medicare Advantage plans may rely on preferred provider organizations, health maintenance organizations, or private fee-for-service.1, 2 SNPs are a type of Medicare Advantage plan that provides coverage for a specific group of individuals who share common traits, such as having the same chronic condition or disease, being dually eligible for Medicare and Medicaid, or requiring an institutional level of care. With the exception of FIDE-SNPs, Medicare Advantage plans are not responsible for LTSS, but they are responsible for coordinating the care of their enrollees. In addition, each type of SNP (i.e., FIDE-SNP, D-SNP, C-SNP, and I-SNP) serves beneficiaries that are likely to have LTSS needs.3, 4, 5 HIE Relevance: Since Medicare Advantage plans coordinate care across acute and post-acute care providers, there is a degree of HIE within all Medicare Advantage plans. In particular, FIDE-SNPs present an opportunity for HIE shared across both acute and LTSS providers. |
Dual Eligible Special Needs Plans (D-SNPs) and Fully Integrated Dual Eligible Special Needs Plans (FIDE-SNPs)
Created under the Medicare Modernization Act of 2003, Medicare Advantage SNPs offer targeted care to special needs populations, including those who: (a) are residing in institutions or are eligible for an institutional level of care and residing in the community; (b) are dually eligible for Medicare and Medicaid coverage; or (c) have severe chronic conditions.6 While Dual Eligible D-SNP enrollees may receive enhanced benefits beyond the basic Medicare benefit at the discretion of the plan, FIDE-SNPs combine Medicare and Medicaid funding and provide the full range of Medicare and Medicaid benefits coordinated by a single managed care organization. These organizations oversee the care process to align delivery of services, including LTSS, for each recipient as a means of reducing potential duplication or repetition of services and treatments. As of January 2014, CMS reported that 1.5 million individuals in the United States were enrolled in D-SNPs (including FIDE-SNPS).7
Examples
Some examples of FIDE-SNPs include the Wisconsin Family Care Partnership Plans, which offer integrated care to about 4,200 seniors and persons with disabilities located in 14 counties in the state.8 Similarly, Senior Care Options in Massachusetts operates through five health plans, such as the Commonwealth Care Alliance, and serves thousands of older adults throughout the state (except certain rural counties) through integrated service delivery.9MSHO provides integrated services to about 35,000 seniors.10
Chronic Condition Special Needs Plans (C-SNPs) and Institutional Special Needs Plans (I-SNPs)
C-SNPs and I-SNPs are specific types of Medicare Advantage plans that target special populations. C-SNPs restrict enrollment to those individuals with a diagnosis on the CMS-approved list of 15 chronic conditions, which includes conditions such as diabetes, heart failure, and cardiovascular disorders. C-SNPs coordinate care across provider types, including acute care and LTSS, although they are not required to provide services beyond the Medicare benefit. I-SNPs restrict enrollment to individuals residing in a nursing facility for at least 90 days, or who require facility-level care but reside in the community. Eligibility is based on a state's Level of Care assessment, but the underlying goal of reducing avoidable hospitalizations and maintaining high-quality care remains similar to other SNPs. Although I-SNPs enroll nursing home residents or those at the same level of care residing in the community, I-SNPs are only financially responsible for Medicare-covered services.11, 12
Example
Enrollment in C-SNPs and I-SNPs remains lower than D-SNP plans.13 However, CareMore's Reliance plan is one example of a C-SNP, serving older adults in the Greater Los Angeles metropolitan area. Evercare also manages I-SNP products available throughout the United States, through parent company United Healthcare.
B. Financial Alignment Demonstrations
|
The Financial Alignment Demonstrations are an opportunity provided by CMS for states to design new approaches to coordinate care for dual eligible individuals (also referred to as Medicare-Medicaid enrollees). These dual eligible persons qualify to receive both Medicare and Medicaid coverage and may include low-income older adults and persons with disabilities. Approximately 10 million people in the United States qualify as dually eligible beneficiaries.14 Dually eligible beneficiaries often have complex and costly health care needs, and the lack of coordination between Medicare and Medicaid exacerbates these concerns. To address these issues, CMS is entering into memoranda of understanding with several states to test models that align Medicare and Medicaid financing, while also integrating primary and acute care, behavioral health, and LTSS for dual eligible beneficiaries. States will implement one or both of the following types of models:15
The goal of the initiative is to raise the quality of care, while reducing costs in demonstration states. This initiative will identify and validate delivery system and payment coordination models that can be tested and replicated in other states.16 As of July 2015, 11 states have implemented demonstrations. HIE Relevance: Successful coordination of all services across Medicare and Medicaid for dually eligible persons, will require significant information exchange across provider types and will likely include a range of approaches to HIE. |
Examples
To date, 11 states have implemented have signed Memoranda of Understanding with CMS and begun implementing their demonstrations. The following are examples of some of the demonstrations being implemented:
-
Massachusetts is implementing a county-specific capitated model for full-benefit Medicare-Medicaid enrollees who are aged 21-64 at the time of enrollment.17
-
Washington is implementing a managed fee-for-service demonstration across most counties in the state (excluding King (Seattle) and Snohomish, for which Washington State is developing a capitated model demonstration). The initiative is open to full-benefit Medicare-Medicaid enrollees of all ages who are eligible for Medicaid health home services.18
-
Minnesota is implementing an Alternative model, intended to further strengthen integration of its existing Medicare Advantage SNPs and Medicaid managed care plans by testing administrative changes to better align the two programs. These initiatives are designed to integrate CMS and state oversight of the MSHO program; clarify and simplify enrollee information and processes; expand health care home purchasing arrangements; and make program administration more efficient for CMS, the state, and plans.
C. Program of All-inclusive Care for the Elderly (PACE)
|
First funded through grants in 1990, PACE provides coordinated acute and LTSS for frail, older adults (age 55 and older) who receive Medicaid and/or Medicare and who are eligible for nursing facility care based on the level of care criteria in each state. This special population typically has significant health needs, and PACE is designed to meet these needs while allowing participants to remain in their homes and communities. PACE organizations generally use an integrated staff model of primary care, rehabilitation services, nursing, social work, and LTSS delivered at adult day centers. Available services include adult day care; primary care; hospital care; nursing home care (5-15% of PACE enrollees move to nursing homes and remain enrolled in PACE); medication coverage; home care; counseling; dentistry; physical, occupational, and recreational therapy; and other services, including meals and transportation. PACE organizations are funded by risk-adjusted capitation payments from Medicare and Medicaid.19, 20 HIE Relevance: As the most fully, clinically integrated model of acute care and LTSS, PACE organizations provide an opportunity to learn what health information topics, modes of exchange, and formats primary care and LTSS providers find valuable. In addition, PACE plans contract with inpatient, post-acute care, and residential care providers, with whom they must engage in some form of HIE. |
Examples
There are 114 PACE programs operating in 32 states.20 Most programs are very small, but a few have larger enrollments, as shown below:
-
CenterLight Healthcare in New York is the nation's largest PACE program and has been operating since 1992. CenterLight Healthcare has 11 PACE centers and six alternative-care settings.21
-
InnovAge in Colorado, New Mexico, and California (based in Colorado) has been coordinating care for older adults and persons with disabilities at PACE centers since 1990. InnovAge has seven PACE centers and three alternative-care settings, as well as an additional center currently under construction.22
-
AltaMed in California has offered PACE services to older adults since 1996. AltaMed has six PACE centers, as well as 16 affiliated medical and dental clinics.23
-
On Lok Lifeways in California serves older adults in the greater San Francisco area and was the original PACE program (created in 1986 and first awarded PACE funding in 1990). They offer ten PACE centers, three of which are located within On Lok's affordable housing buildings.24
-
Providence ElderPlace in Oregon serves as the state's only PACE program, operating since 1990. Providence ElderPlace has seven PACE centers and three assisted living facilities.25
D. Medicaid Managed Long-Term Services and Supports (MLTSS)
|
Rather than charging based on a fee-for-service model in which each service is covered a la carte, Medicaid managed care plans employ care organizations to deliver bundled care services to Medicaid recipients. Medicaid MLTSS represent a type of Medicaid managed care plan that addresses specific LTSS needs, including delivery of HCBS and nursing home care. Some MLTSS models may be coordinated with a Medicare plan (e.g., as a FIDE-SNP or as part of Medicare-Medicaid plan under the Financial Alignment Initiative). The underlying goal of this model is supporting quality LTSS needs while working to keep the costs of services low. As of 2012, 16 states offered MLTSS programs, most of which target older adults (age 65 and older). While acute care is outside of the MLTSS benefit package, these programs have an incentive to coordinate with acute care providers.26, 27, 28, 29 HIE Relevance: As MLTSS present an opportunity for potential coordination between LTSS and acute care providers who serve Medicaid recipients, the type and volume of HIE may vary between state programs. This variation in HIE could enable comparisons between models to provide a better understanding of multiple modes of HIE. |
Examples
-
Minnesota's Senior Care Plus plan provides specific services to low-income seniors. Services include primary care and other physician services; LTSS; hospital stays; rehabilitation services; preventive care; and prescription drug coverage.30
-
Wisconsin's Family Care plan also offers LTSS and is available in 57 counties in Wisconsin.31
E. Medicare Accountable Care Organizations (ACOs)
|
Medicare ACOs are relatively new, with the first formal use of the term ACO appearing in the Affordable Care Act (2010). ACOs consist of hospitals, physicians, and other types of providers who work together voluntarily to ensure coordination of care for Medicare recipients. These organizations are intended to be more cost-effective because increased coordination and communication across providers helps reduce the chance of error and minimizes the incidence of duplicative testing or procedures. The three primary components of ACOs are strong provider communication with a focus on primary care; payment systems that reflect the links between providers; and performance measures to ensure quality of care and assess potential cost savings. As described below, Medicare ACOs are supported through three key payment structures: Shared Savings Programs, Advance Payment models, and Pioneer models. Despite the broad array of services coordinated through ACOs, many do not include LTSS.32, 33 HIE Relevance: ACOs may be promoting HIE across acute and post-acute care settings, including skilled nursing facilities and home health agencies. Theoretically, they would also be coordinating care with LTSS providers. |
There are three key types of ACOs:
-
Shared Savings Programs coordinate care, including coordination between hospitals and other providers, for Medicare fee-for-service beneficiaries, meaning that costs are reimbursed to providers after health services are provided. Shared Savings Programs are rewarded for containing costs while also meeting or exceeding high standards of quality care delivery. The care coordination process also requires accountability of providers and investment in infrastructure to support care goals.34, 35
-
The Advance Payment ACO Model offers a funding opportunity for small, rural, or physician-based providers who would like to coordinate care but who lack the financial resources to invest in care coordination. This model offers upfront monthly payments that are used toward improving local care infrastructures (e.g., electronic records systems) that will facilitate care coordination. This model is very new and is still being tested. The first Advance Payment ACOs were awarded funds in 2013.36
-
Pioneer ACOs allow providers with experience in care coordination, to move from Shared Savings model to a format more tailored to the specific populations they treat (i.e., population-based payment model). These ACOs are also intended to coordinate with private payers through alignment of incentives to improve quality of care and provide cost savings to Medicare, employers, and patients. This model provided the first awards in 2012.37
Relationship to LTSS
For nursing facilities who participate in a Shared Savings Program, Medicare and Medicaid payments for services provided to residents remain unchanged; however, these facilities are also eligible to receive a portion of the savings that was generated by the ACO. Nursing facilities cannot create ACOs of their own, but they can participate in ACOs with hospitals, health clinics, or physician offices. Participation also requires that certain patient care criteria be met in four key areas: patient-caregiver experience, care coordination and safety, preventive health, and care of at-risk populations. Non-profit facilities are also eligible to participate in ACOs without jeopardizing their status.
In December 2013, more than 100 new ACOs were approved by HHS. Some of these new models may also include more links to post-acute care settings and LTSS, but at this stage, it is difficult to determine how different types of organizations may interact under the new ACOs.
Although it is too soon to witness all the purported benefits of facility participation in the ACO model, the model has been lauded as a key step towards strengthening relationships between nursing facilities and hospitals and increasing provider communication across care settings. Some of these may also include LTSS, but the relationships are still developing.38
Example
Created in January 2013, Billings Clinic in Billings, Montana, is a Shared Savings ACO that includes a hospital, physician practices in Montana and Wyoming, and an assisted living and skilled nursing facility. Though LTSS are not mentioned explicitly, the organization seems to dominate the local health market, suggesting a strong possibility of communications across acute and LTSS providers, even if those partnerships have not been formalized. This example may be worth exploring in greater detail.39
F. Support and Services At Home (SASH)
|
The SASH model provides coordinated, LTSS and housing to facilitate care for Vermonters who are aging in place. Hallmarks of the model include care coordination across providers and between primary care and HCBS, as well as use of HIT to facilitate records management and provider communication. SASH also provides support for care transitions and education to self-manage chronic conditions through a team-based approach and volunteer engagement.40, 41 Key model details (from RTI study):
HIE Relevance: Given the focus on integrating primary care and LTSS, and inclusion of the AAAs, SASH presents a distinctive opportunity to explore HIE-specific to a given state and, perhaps, involving a broader array of providers than most other models. Achieving a better understanding of HIE content and processes within SASH can facilitate a broader understanding of how similar HIE could be achieved across other geographic settings. |
G. Beacon Community Programs
|
Beacon Community Programs are designed to use HIT to advance the HHS aims of better health and better healthcare at a lower cost. Seventeen communities were awarded 3-year Beacon grants in 2010 through the ONC within HHS. Beacon communities, with their unique populations and regional contexts, have pursued the following endeavors:
All sites address health needs and supports for populations with chronic conditions, including older adults.43, 44 HIE Relevance: With information exchange being a primary component of Beacon Community activities, programs that have targeted inclusion of older adults and/or persons with disabilities (see discussion of Geisinger and Bangor Beacon communities below) should provide a rich source of information for this study. |
Examples
-
Keystone Beacon Project (Geisinger partnership). This initiative received federal funding to partner physicians, hospitals, nursing homes, and LTSS (home health care organizations) with the KeyHIE and to promote exchange of critical patient health information. Geisinger also has developed a standard clinical summary document derived from Nursing Home MDS and Home Health OASIS data in the format required to meet Meaningful Use requirements. Since all partners have access to the same system, each one can access patient records to obtain key details, such as test results, medications, or diagnoses, and participating home health agency staff can receive real time alerts when patients are hospitalized. The system has specialized security (Transport Layer Security) to ensure HIPAA compliance, confidentiality, and patient safety. Although the program did not focus only on older adults or persons with disabilities, inclusion of nursing facilities and home health agencies made these populations significant components of the initiative.45, 46 The same system of case management and HIT access is continuing under Geisinger's current Keystone ACO, Patient Centered Medical Home, and the Geisinger health plan.
-
Bangor Beacon Community. This initiative employed an existing statewide HIT system (HealthInfoNet) and expanded use of the system to more providers. Prior to the grant, only the local hospital could access the HIT system to upload or review patient information, such as laboratory results or patient allergies. Through the grant, participation was extended to additional hospitals, physician practices, nursing facilities, counseling, and home health agencies. The target population for this effort was individuals with chronic conditions, such as diabetes, asthma, and congestive heart failure; many of these chronically ill individuals are also older adults.47
H. Health Homes
|
Created under the Affordable Care Act (2010) and first launched in 2011, Health Homes provide care management for primary care, behavioral health, and HCBS for eligible individuals with chronic health conditions. Children and adults are eligible if they have two or more chronic health conditions (e.g., asthma, diabetes, heart disease, obesity, substance abuse disorder); if they have one chronic condition and a risk for developing others; or if they have one or more serious mental health conditions. Health Homes are created under state Medicaid programs with additional federal support. The underlying goals of Health Homes are improving care by reducing redundancy in testing or treatment, while also reducing expenditures. Covered services include comprehensive care management, care coordination, health promotion, patient and family support, transitional care, and use of HIT. Health Homes may be physician's offices, health clinics, medical homes, or community health centers. To manage the matrix of caregivers a patient may see, a care manager oversees care provision to ensure that the patient's needs are met. Also, health records are shared across providers to keep all parties informed of progress and changes.48, 49, 50 HIE Relevance: This process of housing an individual's health management under one care manager's purview creates a virtual home for health care and health information (i.e., "health home"). Health Homes offer a unique opportunity to see how information is exchanged and used across providers, including acute and LTSS. |
Example
-
Health Homes in Washington are serving individuals with chronic conditions, and as of 2013, also serving Medicare-Medicaid dual eligible beneficiaries with LTSS and related services under the state's Financial Alignment Demonstration.51Iowa also provides Health Homes to individuals with chronic conditions in 29 of the state's 99 counties.52
I. Health Care Innovation Awards (HCIAs)
|
First awarded in 2012 and again in 2014, HCIAs are designed to improve health care and reduce costs for individuals on Medicare, Medicaid, or the Children's Health Insurance Program. Some models target workforce development; others focus on enhancing infrastructure, and still others propose new modes of health services delivery. A few models focus on care coordination and use of HIT, including efforts to reduce hospital emergency department use and hospital readmission and efforts to reach patients in rural settings. Some programs also target LTSS and potential care coordination between LTSS and acute providers through efforts to improve care for dual eligible patients and individuals with chronic conditions.53 HIE Relevance: While HCIAs vary significantly in their goals and target populations, programs that include possible HIE between acute and LTSS providers could present an opportunity to learn more about various methods of and formats for coordinating services across provider types. |
Examples
Some projects may include care integration for older adults and persons with disabilities but will need more investigation to clarify:54
-
Massachusetts. Beth Israel Deaconess Medical Center is reducing avoidable re-hospitalizations through care integration.
-
Virginia. Carilion New River Valley Medical Center provides rural care coordination and HIT for pharmacists to improve medication management and record keeping for patients with chronic disease.
-
Arizona and California. Pacific Business Group on Health provides care managers to individuals with multiple chronic conditions to help manage disease and prevent hospitalizations.
-
Oregon. The Providence Portland Medical Center is creating a Coordinated Care Organization to provide integrated care for dual eligibles, including a care coordination registry, to improve care and reduce emergency department use and hospital admissions.
-
Alabama, Connecticut, Florida, Georgia, Illinois, Indiana, Kansas, Kentucky, Massachusetts, Michigan, Mississippi, Nebraska, Oklahoma, West Virginia, Wisconsin. TransforMED, VHA-affiliated hospitals (formerly Voluntary Hospitals of America), will create "medical neighborhoods" to assess patient risk and improve care coordination and transitions, and reduce unnecessary treatment and testing.
-
Iowa. The University of Iowa is providing outreach to rural hospitals to improve care coordination and communication for patients with complex illness using telehealth.
-
Maryland. The Johns Hopkins School of Nursing's Community Aging in Place, Advancing Better Living for Elders (CAPABLE) program (awarded in 2012) pairs various types of LTSS, including home assistance with activities of daily living (ADLs), medication management, mobility, and other services. Occupational therapist, nurses, and other providers work together to develop a matrix of services for individual recipients to support ongoing residence in home settings. The goal of these efforts is to reduce hospitalization and nursing home admission, though the extent to which the CAPABLE staff communicate with participants' other providers (e.g., primary care physician) is unknown.
J. Veterans Health Administration (VHA)
|
VHA hires its own physicians and maintains its own facilities, including acute care and LTSS, and electronic medical records are used throughout the system. However, individuals eligible for VHA care are still permitted to seek health services outside the VHA system, which can result in the same lack of communication, potential duplication of services and redundancy of expenditures that occurs in systems that are not well coordinated. The primary reasons for veterans to seek non-VHA care are logistical (i.e., the nearest VHA providers are located far away). Programs like VHA Home-Based Primary Care provide care to older veterans and veterans with disabilities in their homes.55 HIE Relevance: The VHA employs electronic medical records and provides both acute and LTSS. As a result, it offers the opportunity to evaluate the content and format of HIE between acute and LTSS providers. |
Example
-
The VHA Home-Based Primary Care program supports older veterans and veterans with disabilities by providing primary care, skilled services, case management, and LTSS such as assistance with ADLs and instrumental activities of daily living (IADLs) in the home. As of October 2013, the VHA Home-Based Primary Care was in effect in multiple communities throughout the United States.56, 57
ENDNOTES
-
Centers for Medicare and Medicaid Services. (2013). Medicare Advantage plans. Retrieved from http://www.medicare.gov/sign-up-change-plans/medicare-health-plans/medicare-advantage-plans/medicare-advantage-plans.html.
-
Centers for Medicare and Medicaid Services. (2013). How do Medicare Advantage plans work. Retrieved from http://www.medicare.gov/sign-up-change-plans/medicare-health-plans/medicare-advantage-plans/how-medicare-advantage-plans-work.html.
-
National Association of States United for Aging and Disabilities. (2013). Leveraging options under Medicare, Medicaid, and the Affordable Care Act: Managed care in long term services and supports. Retrieved from http://www.cbrx.il.gov/aging/1athome/MarthaRoherty_NASUAD3.pdf.
-
Centers for Medicare and Medicaid Services. (2013). SNP comprehensive report. Retrieved from http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/MCRAdvPartDEnrolData/Special-Needs-Plan-SNP-Data-Items/SNP-Comprehensive-Report-2014-01.html?DLPage=1&DLSort=1&DLSortDir=descending.
-
Grabowski, D.C. (2009). Special needs plans and the coordination of benefits and services for dual eligibles. Health Affairs (Millwood), Jan-Feb, 28(1), 136-146.
-
Centers for Medicare and Medicaid Services. (2013). Dual eligible SNP. Retrieved from http://www.cms.gov/Medicare/Health-Plans/SpecialNeedsPlans/DualEligibleSNP.html.
-
Leading Age. (2013). Adult day services to provide services under Medicare via managed care contracts. Retrieved from http://www.leadingage.org/uploadedFiles/Content/Members/HCBS/Adult_Day/….
-
Wisconsin Department of Health Services. (2013). Family care partnership program. Retrieved from https://www.dhs.wisconsin.gov/familycare/fcp-overview.htm.
-
Massachusetts Department of Health and Human Services. (2015). Senior care options. Retrieved from http://www.mass.gov/eohhs/consumer/insurance/senior-care-options/.
-
Minnesota Department of Human Services. (2015). Minnesota health care programs managed care enrollment totals. Retrieved from http://www.dhs.state.mn.us/main/idcplg?IdcService=GET_FILE&RevisionSelectionMethod=LatestReleased&Rendition=Primary&allowInterrupt=1&noSaveAs=1&dDocName=dhs16_195660.
-
Centers for Medicare and Medicaid Services. (2013). Chronic condition SNP. Retrieved from http://www.cms.gov/Medicare/Health-Plans/SpecialNeedsPlans/ChronicConditionSNP.html.
-
Centers for Medicare and Medicaid Services. (2013). Institutional SNP. Retrieved from http://www.cms.gov/Medicare/Health-Plans/SpecialNeedsPlans/InstitutionalSNP.html.
-
Kaiser Family Foundation. (2012). Medicare Advantage: Special needs plan (SNP) enrollment, by SNP type. Retrieved from http://kff.org/medicare/state-indicator/snp-enrollment-by-snp-type/.
-
Kaiser Family Foundation. (2015). Number of dual eligible beneficiaries. Retrieved from http://kff.org/medicare/state-indicator/dual-eligible-beneficiaries/.
-
Not all states are pursuing these models at this time, and Minnesota has implemented an Alternate Model demonstration focused on administrative alignment of their current D-SNP and Medicaid managed care model, MSHO.
-
Centers for Medicare and Medicaid Services. (2012). State demonstrations to integrate care for dual eligible individuals. Retrieved from http://www.cms.gov/Medicare-Medicaid-Coordination/Medicare-and-Medicaid….
-
Centers for Medicare and Medicaid Services. (2012). Massachusetts memorandum of understanding. Retrieved from http://www.cms.gov/Medicare-Medicaid-Coordination/Medicare-and-Medicaid-Coordination/Medicare-Medicaid-Coordination-Office/FinancialAlignmentInitiative/Downloads/MassMOU.pdf.
-
Centers for Medicare and Medicaid Services. (2013). Washington managed fee for service (FFS) model final demonstration agreement. Retrieved from http://www.cms.gov/Medicare-Medicaid-Coordination/Medicare-and-Medicaid-Coordination/Medicare-Medicaid-Coordination-Office/FinancialAlignmentInitiative/Downloads/WAMFFSFDA.pdf.
-
National PACE Association. (2015). Who, what, and where is PACE. Retrieved from http://www.npaonline.org/website/article.asp?id=12&title=Who,_What_and_Where_is_PACE.
-
National PACE Association. (2015). PACE in the states. Retrieved from http://www.npaonline.org/website/download.asp?id=1741&title=PACE_in_the….
-
CenterLight Healthcare. (2014). About CenterLight Healthcare. Retrieved from http://www.centerlighthealthcare.org/.
-
InnovAge. (2014). How we work. Retrieved from http://www.myinnovage.org/.
-
AltaMed. (2014). Overview. Retrieved from http://www.altamed.org/.
-
On Lok Lifeways. (2014). Who we serve. Retrieved from http://www.onlok.org/.
-
Providence ElderPlace. (2014). Providence ElderPlace Irvington Village. Retrieved from http://oregon.providence.org/patients/facilities/providence-elderplace-irvington-village/Pages/default.aspx.
-
New York State Department of Health. (2013). About managed long term care. Retrieved from http://www.health.ny.gov/health_care/managed_care/mltc/aboutmltc.htm.
-
Medicaid.gov. (2013). Medicaid managed long term services and supports. Retrieved from http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Delivery-Systems/Medicaid-Managed-Long-Term-Services-and-Supports-MLTSS.html.
-
Medicaid.gov. (2012). Population groups enrolled in managed long term services and supports. Retrieved from http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Delivery-Systems/Downloads/MLTSS-Populations.pdf.
-
Medicaid.gov. (2012). The growth of managed long term services and supports programs: A 2012 update. Retrieved from http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Delivery-Systems/Downloads/MLTSSP_White_paper_combined.pdf.
-
Minnesota Department of Human Services. (2013). Minnesota Senior Care/Senior Care Plus. Retrieved from http://hcopub.dhs.state.mn.us/28_10_10_15.htm.
-
Wisconsin Department of Health Services. (2013). What is family care. Retrieved from http://www.dhs.wisconsin.gov/ltcare/generalinfo/whatisfc.htm.
-
Virginia Health Care Association. (2012). VHCA legal quarterly, spring 2012. Retrieved from http://lawmh.com/uploads/Nursing_Facilities_and_ACOs_-_A_Basic_Primer.pdf.
-
Butcher, L. (2013). Hospitals strengthen bonds with post-acute providers. Hospitals and health networks. Retrieved from http://www.hhnmag.com/display/HHN-news-article.dhtml?dcrPath=/templatedata/HF_Common/NewsArticle/data/HHN/Magazine/2013/Jan/0113HHN_Feature_strategy.
-
Centers for Medicare and Medicaid Services. (2013). Medicare shared savings program ACO fast facts. Retrieved from http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/sharedsavi….
-
Centers for Medicare and Medicaid Services. (2014). Shared savings program. Retrieved from https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/sharedsavingsprogram/index.html?redirect=/sharedsavingsprogram/.
-
Centers for Medicare and Medicaid Services. (2013). Advance payment accountable care organization (ACO) model. Retrieved from http://innovation.cms.gov/Files/fact-sheet/Advanced-Payment-ACO-Model-Fact-Sheet.pdf.
-
Centers for Medicare and Medicaid Services. (2014). Pioneer ACO model. Retrieved from http://innovation.cms.gov/initiatives/Pioneer-ACO-Model/.
-
Gamble, M., Punke, H. (2013). 100 accountable care organizations to know. Becker's Hospital Review. Retrieved from http://www.beckershospitalreview.com/lists/100-accountable-care-organizations-to-know.html.
-
Billings Clinic. (2014). Billings Clinic--An accountable care organization. Retrieved from http://www.billingsclinic.com/ACO.
-
Cathedral Square Corporation. (2013). SASH in the news. Retrieved from https://cathedralsquare.org/future-sash.php.
-
Cathedral Square Corporation. (2013). SASH Support and Services at Home. Retrieved from http://cathedralsquare.org/files/Nancy%20Eldridge%20-%20Funding%20and%2….
-
Cathedral Square Corporation. (2011). SASH peer-to-peer exchange. Retrieved from http://cathedralsquare.org/files/Molly%20Dugan%20-%20SASH%20Overview-Op….
-
Health IT.gov. (2014). Beacon community programs. Retrieved from http://www.healthit.gov/policy-researchers-implementers/beacon-community-program.
-
Health IT.gov. (2013). Beacon policy brief. Retrieved from http://www.healthit.gov/sites/default/files/private/beacon_quality_measurement_brief_final_14aug13.pdf.
-
McCarthy, D., Mueller, K., Wrenn, J. (2009). Geisinger Health System: Achieving the potential of system integration through innovation, leadership, measurement, and incentives.Commonwealth Fund. Retrieved from http://www.commonwealthfund.org/~/media/Files/Publications/Case%20Study/2009/Jun/McCarthy_Geisinger_case_study_624_update.pdf.
-
Keystone Health Information Exchange. (2014). About us. Retrieved from http://www.keyhie.org/about_us/about_us.html.
-
Bangor Beacon Community. (2014). Beacon grant details. Retrieved from http://www.bangorbeaconcommunity.org/.
-
Medicaid.gov. (2013). Health homes. Retrieved from http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Long-Term-Services-and-Support/Integrating-Care/Health-Homes/Health-Homes.html.
-
Medicaid.gov. (2013). State health home CMS proposal status. Retrieved from http://www.medicaid.gov/State-Resource-Center/Medicaid-State-Technical-Assistance/Health-Homes-Technical-Assistance/Downloads/HHMAP_v27.pdf.
-
Kaiser Family Foundation. (2011). Medicaid's new health home option. Retrieved from http://kaiserfamilyfoundation.files.wordpress.com/2013/01/8136.pdf.
-
Washington State Health Care Authority. (2013). Washington's health home SPA. Retrieved from http://www.hca.wa.gov/Documents/health_homes/HH_SPA.pdf.
-
Iowa Medicaid Enterprise. (2014). Health homes for providers. Retrieved from http://www.ime.state.ia.us/Providers/healthhome.html.
-
Centers for Medicare and Medicaid Services. (2015). Health Care Innovation Awards. Retrieved from http://innovation.cms.gov/initiatives/Health-Care-Innovation-Awards/ and http://innovation.cms.gov/initiatives/Health-Care-Innovation-Awards/Round-2.html.
-
Centers for Medicare and Medicaid Services. (2012). Health Care Innovation Award project profiles. Retrieved from http://innovation.cms.gov/initiatives/Health-Care-Innovation-Awards/.
-
Auerbach, D.I., Weeks, W.B., Brantley, I. (2013). Health care spending and efficiency in the U.S. Department of Veterans Affairs. Rand Corporation. Retrieved from http://www.rand.org/pubs/research_reports/RR285.html.
-
U.S. Department of Veterans Affairs. (2014). Guide to long term care: Home based primary care. Retrieved from http://www.va.gov/geriatrics/guide/longtermcare/home_based_primary_care.asp.
-
Beales, J.L. Edes, T. (2009). Veterans Affairs home based primary care. Clin Geriatr Med, Feb, 25(1), 149-54, viii-ix. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/19217499.
| TABLE A-1. Integrated Care Models | |||
|---|---|---|---|
| Integrated Care Model Type |
Definition | HIE Relevance | Examples |
| Medicare-Managed Care Special Needs Plans (SNPs) | A type of Medicare Advantage plan that provides coverage for a specific group of Medicare beneficiaries who share common traits, such as being dually eligible for Medicare and Medicaid (i.e., D-SNP). With the exception of FIDE-SNPs, Medicare Advantage plans are not responsible for LTSS, but they are responsible for coordinating the care of their enrollees. | Since Medicare Advantage plans coordinate care across acute and post-acute care providers, there is a degree of information exchange within all Medicare Advantage plans. FIDE-SNPs also coordinate care across acute care and LTSS providers. | FIDE-SNPs:
C-SNPs and I-SNPs:
|
| Financial Alignment Demonstrations | Provided by CMS for states to design new approaches to coordinate care for dual eligible individuals through either a capitated model (Medicare-Medicaid Plans) or managed fee-for-service model providing care coordination. | Successful coordination of all services across Medicare and Medicaid for dually eligible persons, requires significant information exchange across provider types and likely includes a range of approaches. | To date, 11 states implemented demonstrations:
|
| Program of All-inclusive Care for the Elderly (PACE) | Provides coordinated acute and LTSS for frail, older adults (age 55 and older) who receive Medicaid and/or Medicare and who are eligible for nursing facility care based on the level of care criteria in each state. | As the most fully, clinically integrated model of acute care and LTSS, PACE organizations rely on timely exchange of health information between the providers of services/health care and the PACE program care coordinators. In addition, PACE plans contract with inpatient, post-acute care, and residential care providers, with whom cross-setting information exchange must also occur. |
|
| Support and Services At Home (SASH) | Provides coordinated LTSS and housing to facilitate care for Vermonters who are aging in place. Hallmarks of the model include care coordination across providers and between primary care and HCBS. | SASH utilizes HIT to facilitate records management and provider communication. Vermont's Blueprint for Health clinical registry, DocSite, is used to capture information on SASH participants such as demographics, health status and wellness goals. DocSite supports SASH staff monitoring of participant progress towards healthy living plans and state tracking of SASH community trends (RTI & Leading Age, 2014). |
|
| Beacon Community Programs (2010-2014) | Designed to use HIT to advance the HHS aims of better health and better health care at a lower cost. Seventeen communities were awarded 3-year Beacon grants in 2010 through the ONC within HHS. | Beacon Community program activities included information exchange as a primary component. Programs that targeted inclusion of older adults and/or persons with disabilities provided details about how different models addressed information exchange to coordinate care for populations with high needs. |
|
| Health Homes | Provide care management for primary care, behavioral health, and HCBS for eligible individuals with chronic health conditions. | This process of housing an individual's health management under one care manager's purview creates a virtual home for health care and health information (i.e., "health home"). The use of HIT to link services, if applicable, is 1 of the 6 specific health home services defined by CMS. |
|
| Veterans Health Administration (VHA) | VHA hires its own physicians and maintains its own facilities, including acute care and LTSS, and electronic medical records used throughout the system. | The VHA electronic medical record system is deployed across their widely dispersed geographic locations and across their various provider settings. This provides a uniform platform for accessing a veteran's health information. |
|
| Medicaid Managed Long-Term Services and Supports (MLTSS) | Represent a type of Medicaid managed care plan that addresses specific LTSS needs, including delivery of HCBS and nursing home care. Some MLTSS models may be coordinated with a Medicare plan (e.g., as a FIDE-SNP or as part of Medicare-Medicaid plan under the Financial Alignment Initiative). | As MLTSS presents an opportunity for potential coordination between LTSS and acute care providers who serve Medicaid recipients, the type and volume of information exchange may vary between state programs. |
|
| Medicare Accountable Care Organizations (ACOs) | Consist of hospitals, physicians, and other types of providers who work together voluntarily to ensure coordination of care for Medicare recipients. The three primary components of ACOs are strong provider communication with a focus on primary care; payment systems that reflect the links between providers; and performance measures to ensure quality of care and assess potential cost savings. | ACOs may be promoting information exchange across acute and post-acute care settings, including skilled nursing facilities and home health agencies. Theoretically, they would also be coordinating care with LTSS providers. |
|
| Health Care Innovation Awards (HCIAs) | Designed to improve health care and reduce costs for individuals on Medicare, Medicaid, or the state Children's Health Insurance Program. Some models target workforce development; others focus on enhancing infrastructure, and still others propose new modes of health services delivery. A few models focus on care coordination and use of HIT, including efforts to reduce hospital emergency department use and hospital readmission and efforts to reach patients in rural settings. | While HCIAs vary significantly in their goals and target populations, some programs (such as those focused on care coordination) include possible information exchange between acute and LTSS providers. |
|
APPENDIX B. INTEGRATED CARE MODELS OVERVIEW--GEISINGER HEALTH SYSTEM
B.1. Overview of Geisinger
The Geisinger health system is an integrated provider of care that includes a 1,100 member multi-specialty group practice, eight hospital campuses, and two research centers. Geisinger also includes several health plans that provide coverage to 467,000 private, Medicare and Medicaid beneficiaries of central Pennsylvania. The Geisinger health system participates in the Keystone ACO, a Medicare Shared Savings Program ACO. As part of the Keystone ACO, Geisinger contracts with several hospitals and health systems, including Wayne Memorial Health System and Evangelical Community Hospital. The Geisinger health system received federal funding through the Beacon Community Grant (2010-2013) to organize physicians, hospitals, nursing homes, and LTSS (home health care organizations) in partnership with the KeyHIE for HIE. After 2013, the system has continued to exchange information under the Keystone ACO, Patient Centered Medical Home, and the Geisinger health plan.
Other key programs and tools that Geisinger has developed to help support information exchange include the development of a standard clinical summary document derived from Nursing Home MDS and Home Health OASIS data that meets Meaningful Use requirements to share across provider types. Geisinger uses specialized security (Transport Layer Security) to ensure HIPAA compliance, confidentiality, and patient safety when exchanging information across providers, which presents an opportunity to learn more about the types of precautions that must be in place for HIE. The Geisinger health system has also developed the Proven Wellness Neighborhood program that is developed from Geisinger's Patient Centered Medical Home program "ProvenHealth Navigator". The Proven Wellness Neighborhood program targets individuals in the community who have high medical and support service needs and uses licensed social workers and community health assistants to connect individuals with needed community support services.
B.2. Site Visit Participants
Program leadership and management:
- Director of Case Management of Geisinger Health Plan
- Director of Operations of Keystone ACO
- Associate Vice President, Population Health of Geisinger Health Plan
Program staff and providers (e.g., care coordinators or care managers, PCPs):
- Field Coordinators of ProvenWellness Neighborhood
- Community Health Assistant at ProvenWellness Neighborhood
- Case Managers at Keystone ACO
- Staff Physicians at Geisinger Community Practice Service Line
- Administrator of Mountain View Center (Nursing Home)
HIT program staff:
- Operations Director of KeyHIE
- Information Technology Director at Geisinger Health System and Director of KeyHIE
External providers:
- Quality Director of Wayne Memorial Community Health Centers
- Behavioral Health Medical Director of Wayne Memorial Community Health Centers
- Director of Lackawanna County AAA
- Administrator of Wayne County AAA
B.3. Information Exchange Overview
-
Figure B-1 is a diagram of how information flows among the various providers of Geisinger Health System and Geisinger Health Plan, its external partners, and its members.
-
The green arrows indicate an electronic exchange of information where both participating parties can send and receive information through the electronic system.
-
The Geisinger Health System acute care providers can send and receive information from the Geisinger EPIC EHR system.
-
The Keystone ACO providers, which Geisigner is a participant, can send and receive information from the Geisinger EPIC EHR system to communicate with Geisinger providers.
-
The EPIC Care Everywhere web-based portal can send and receive information from the Geisinger EPIC EHR system.
-
The KeyHIE system can send and receive information to all providers and staff who are participating in this HIE, including Geisigner acute care providers, Geisigner care managers, Keystone ACO providers, and other external acute care providers participating in KeyHIE.
-
Geisinger care managers can send and receive information from their case management system (Human Services Information Systems).
-
-
The blue arrows indicate an electronic exchange of information where just one participating party can send information and the other party can only receive or access the information through that electronic system.
-
The Geisinger care managers can only access information from the Geisigner EPIC EHR system but the care managers can not send information to the EHR.
-
External providers and patients can access electronic information from EPIC Care Everwhere.
-
-
The orange arrows indicate an information exchange process that requires manual methods of exchange, such as through phone, fax, or exchange of hardcopy documents.
-
Geisinger care managers exchange information (both send and receive) through these manual methods with patients, external acute care and LTSS providers, Geisinger's Proven Wellness Neighborhood, Keystone ACO providers, and Geisigner acute care providers.
-
The patient also exchanges information through these manual methods with all providers.
-
-
-
Geisinger's information exchange primarily relies on its case managers. Geisinger case managers are employees of Geisinger Health Plan but they work at all levels and providers within the Geisinger Health System and those providers external to the Geisinger Health System. The following is a list of all the different types of Geisinger case managers:
-
Case managers embedded at Geisinger outpatient clinics.
-
Case managers embedded at non-Geisinger sites. These sites are generally big providers in the area who have a long relationship with Geisinger.
-
Case managers who are telephonic-based. These case managers are for Geisinger patients who primarily using non-Geisinger providers but who are contracted with Geisinger.
-
Case managers who are part of the Keystone ACO.
-
-
Geisinger's information exchange relies on using the EPIC EHR system as a key tool to communication among Geisinger providers and staff. Most Geisinger providers have access to EPIC or EPIC messaging through the EPIC Care Everywhere system. However, the information exchange among non-Geisinger or external providers is primarily through phone and fax.
-
KeyHIE was founded by Geisinger and currently has 20 hospitals, 185 physician practices, 61 long-term care facilities, and 28 home health agencies participating. KeyHIE relies on GE Healthcare's eHealth Solutions to conduct the information exchange.
-
The system includes information exchange that focuses on medical information: emergency department summaries, discharge summaries, medical history and physicals, lab results, imaging reports, encounters, and CCDs. KeyHIE does not collect plan of care data.
-
Some key organizations, such as AAA, do not have access to KeyHIE at this point, because these organizations do not actually provide treatment and are not a "covered entity" under HIPAA.
-
-
While each set of informants stressed slightly different key pieces of information that they would like to have included in the exchange of information, all stressed having knowledge of a patient's basic demographics, medications, and current health conditions as important. Very few informants mentioned plans of care or patient preferences as being a key part of the information exchange process.
| FIGURE B-1. Geisinger Information Flow |
|---|
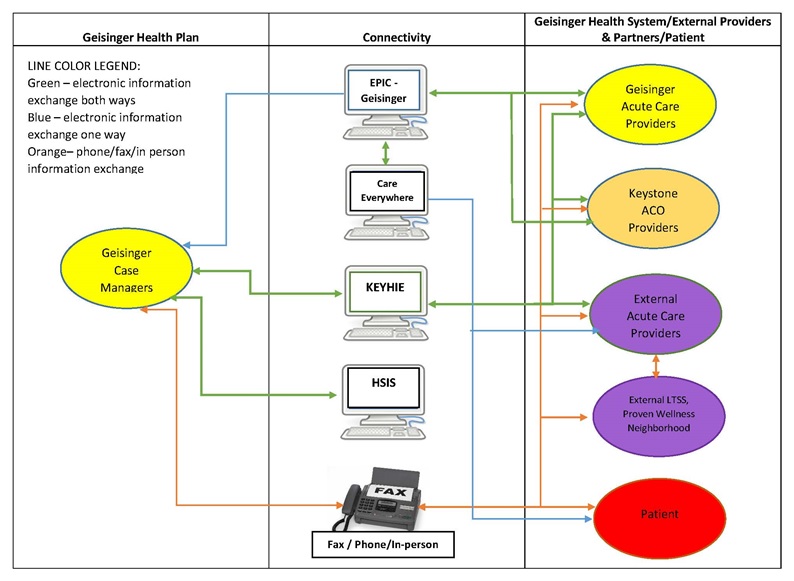 |
Short Diagram Description: Figure B-1 demonstrates how information flows among the various providers of Geisinger Health System and Geisinger Health Plan, its external partners, and its members. Different providers participating in or with the Geisinger Health System use different connectivity methods to share information about a patient.
|
APPENDIX C. MINNESOTA CASE STUDY (MSHO, Bluestone, and HealthPartners)
C.1. Overview of Minnesota MSHO and SNBC Programs
MSHO is a FIDE-SNP that combines Medicare and Medicaid benefits health programs and support systems into one health care package. It is for people aged 65 and older who are eligible for Medicaid and enrolled in Medicare Parts A and B. People can choose to join MSHO or stay in their current Medicare Advantage program. MSHO enrollees are assigned a care coordinator who will help them get their health care and related support services. MSHO is administered by the Minnesota Department of Human Services (DHS) and eight managed care organizations: Blue Plus, HealthPartners, Itasca Medical Care, Medica, Metropolitan Health Plan, PrimeWest Health, South Country Health Alliance and UCare.
The Minnesota SNBC program is a voluntary managed care program for people with disabilities aged 18-64 who have Medicaid. SNBC enrollees may have a care coordinator or navigator to help them access health care and support services. Some SNBC health plans coordinate with other payers including Medicare Parts A, B and D for enrollees who also have that coverage. SNBC is administered by the Minnesota DHS and five managed care organizations: Medica, Metropolitan Health Plan, PrimeWest Health, South Country Health Alliance, and UCare.
We chose to meet with both the state MSHO and SNBC staff as well as the Bluestone Physician Services and HealthPartners staff during our site visit.
C.2. Overview of Bluestone Physician Services
Bluestone Physician Services is a physician-led model that has provided on-site primary care in residential settings since 2006. Bluestone originally began providing on-site care in brain injury and psychiatric group home settings and has since expanded to assisted living and memory care settings. Bluestone provides primary care to nearly 4,000 patients through on-site medical teams. In addition to primary care, Bluestone provides care coordination for seniors and people with disabilities throughout Minnesota, serving nearly 2,000 people with disabilities in the community. Bluestone also serves the eastern Wisconsin region and in June 2015 started services in the Tampa and Orlando Florida areas. Bluestone Physician Services employs over 150 staff and serves approximately 200 assisted living facilities. Bluestone developed the Bluestone Bridge, which is an online communication and reporting portal that facilitates communication across the care team, and to families and community provider staff (e.g., assisted living facility).
C.3. Overview of HealthPartners
HealthPartners is a non-profit integrated health care system based in Minnesota and has been consumer governed since 1957. HealthPartners is a provider of care. The system is comprised of 50 primary care clinics with 750 primary care physicians, multi-specialty group practices of more than 1,700 physicians, 22 urgent care locations and six hospitals. Geriatric care teams are present at 70 facilities. HealthPartners is also a managed care plan with 1.5 million members, including 47,000 Medicare members, 103,000 Medicaid members, and 3,000 MSHO members. HealthPartners is the only health plan/health provider participating in MSHO. HealthPartners coverage for MSHO is offered in 12 counties around the St. Paul/Minneapolis area. Each member in their MSHO program is assigned their own care coordinator. Care coordinators are registered nurses, advanced practice nurse practitioners, or licensed social workers. Their MSHO program also has interdisciplinary care teams for each beneficiary. These care teams include the beneficiary, the care coordinator, the PCP, specialists, LTSS providers, and other providers involved with the member's care plan.
C.4. Site Visit Participants
The first day of the site visit we met with staff at the Minnesota DHS, including the following informants:
- Director of MSHO Program, Minnesota DHS
- Director of SNBC Program, Minnesota DHS
- Manager at Minnesota DHS
- Home Care Policy Lead, Disability Services Division at Minnesota DHS
We also met with representatives from Bluestone Physician Services, including:
- President
- Director of Operations
On the second day of the site visit, we met staff at HealthPartners, including:
-
Program leadership and management:
- Director of Disease and Case Management
- MSHO/MSC+ Program Manager
- Coordinator of State Public Programs
- Manager of State Public Programs
-
Program staff and providers (e.g., care coordinators or care managers, PCPs):
- Case Managers
- HealthPartners Medical Group
- Senior Manager of HealthPartners Geriatrics
- Clinical Pharmacy Program Manager
- Medical Director
- Manager of Behavioral Health Case Management
- Nurse Practitioner with HealthPartners Medical and Dental Group
- Homecare Manager at HealthPartners
-
HIT program staff:
- Senior Information Technology Project Manager
-
External providers:
- Housing Administrator at Presbyterian Homes and Services
C.5. Minnesota Information Exchange Overview
-
The state has made progress on developing the online system MnCHOICES, which is a single, comprehensive assessment and support planning web-based application for all LTSS. Providers and case managers will be able to use MnCHOICES and see functional assessment results for all individuals accessing Medicaid LTSS. It takes the place of the following assessment tools:
- Developmental Disability Screening
- Long-Term Care Consultation
- Personal Care Assistance Assessment
- In the future MnCHOICES will also replace the Home Care Nursing (formerly Private Duty Nursing) Assessment
MnCHOICES first was implemented in counties conducting functional assessments and providing care coordination services for individuals in HCBS waivers. The state expects the managed care plans to begin using MnCHOICES soon.
-
The state requirements for MSHO care coordination processes evolved organically. The state worked with providers and plans to set requirements around care coordination and then the state allowed plans to determine their own specific care coordination processes. Therefore, a variety of care coordination models exist as part of the MSHO program, including the following systems:
- County-based system (tends to be more LTSS focused)
- Care system (tends to be more medically focused)
- Health plans (create their own systems of care coordinators or sometimes contract with counties)
-
The care coordination processes in the SNBC program, are substantially dictated by the state. The state worked specifically with disability advocates to include more language in contracts with SNBC participating plans. The more explicit requirements are a result of lessons learned from previous managed care programs that have failed. One previous program, the Minnesota Disability Health Options (MnDHO), was a voluntary managed care program for Medicare enrollees with physical disabilities who were between the ages of 18 and 64. Evaluations of MnDHO note that the lack of information exchange among providers, particularly between care coordinators and other community-based providers, played a large role in the downfall of the program (Eoyang & Grossman, 2013).
C.6. Bluestone Information Exchange Overview
-
Bluestone's primary communication tool is the Bridge, a web-based messaging system that Bluestone providers use with other providers, including support service providers, to discuss treatment and care of beneficiaries. The Bridge messaging system is not part of any EHR, and therefore notes from the Bridge have to be entered into the Bluestone's EHR separately.
C.7. HealthPartners Information Exchange Overview
-
Figure C-1 is a diagram of how information flows among the various providers of HealthPartners Health System and HealthPartners Health Plan, its external partners, and its members:
-
The green arrows indicate an electronic exchange of information where both participating parties can send and receive information through the electronic system.
-
The HealthPartners Health System acute care providers can send and receive information from the HealthPartners EPIC EHR system.
-
The HealthPartners MSHO case managers can send and receive information from the HealthPartners EPIC EHR system.
-
The EPIC Care Everywhere web-based portal can send and receive information from the HealthPartners EPIC EHR system.
-
HealthPartners MSHO case managers can send and receive information from their case management system Care Partner.
-
-
The blue arrows indicate an electronic exchange of information where just one participating party can send information and the other party can only receive or access the information through that electronic system.
-
External acute care providers and patients can access electronic information from EPIC Care Everwhere.
-
-
The orange arrows indicate an information exchange process that requires manual methods of exchange, such as through phone, fax, or exchange of hardcopy documents.
-
HealthPartners MSHO case managers exchange information (both send and receive) through these manual methods with patients, external acute care and LTSS providers, and HealthPartners acute care providers.
-
The patient also exchanges information through these manual methods with all providers.
-
External acute care providers exchange information through manual methods with external LTSS providers.
-
-
-
HealthPartners' information exchange in their MSHO FIDE-SNP primarily relies on its case managers. HealthPartners case managers are employees of HealthPartners Health Plan and are housed within the Disease and Case Managers Division of HealthPartners. The case managers are disease management oriented and are trained in encouraging beneficiary self-management.
-
Like Geisinger, HealthPartners' information exchange relies on using EPIC EHR as a key communication tool used by HealthPartners providers and staff. Almost all hospitals in St. Paul and Minneapolis area are using EPIC and most HealthPartners providers have access to EPIC or the EPIC Care Everywhere portal to communicate with external providers. For those providers not using EPIC, information exchange is conducted primarily through phone and fax.
-
HealthPartners case managers use a separate electronic system from EPIC. Case managers rely on the Care Partner system for case management and care coordination activities. The EPIC system does not include standard templates that are applicable to the information the HealthPartners case managers would like to exchange. After collecting medical, LTSS and behavioral health information about members, case managers will upload certain data elements to the EPIC system, including whether or not the member is receiving HCBS; if receiving HCBS, what specific services the individual is receiving; any clinical goals of the individuals; and the case manager's name and contact information.
| FIGURE C-1. HealthPartners Information Flow |
|---|
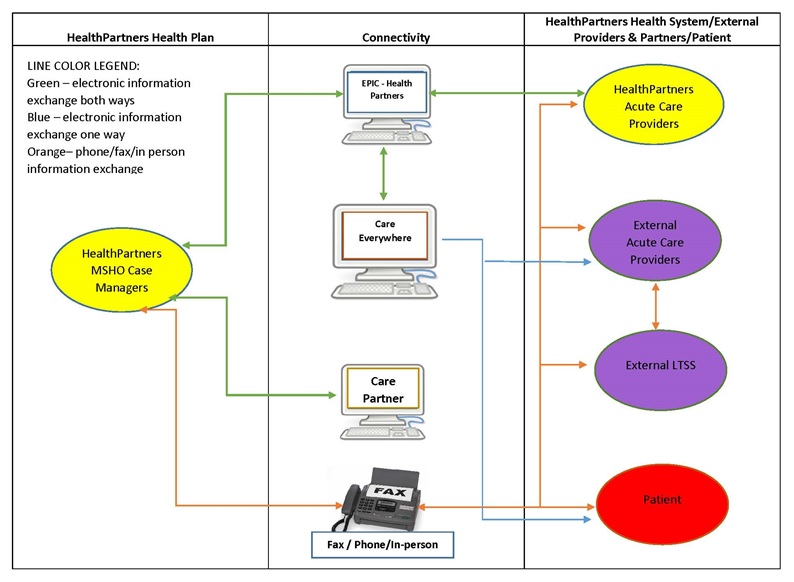 |
Short Diagram Description: Figure C-1 demonstrates how information flows among the various providers of HealthPartners Health System and HealthPartners Health Plan, its external partners, and its members. Different providers participating in or with the HealthPartners Health System use different connectivity methods to share information about a patient.
|
APPENDIX D. COMMUNITY CARE
D.1. Overview of Community Care
Wisconsin CCI includes a PACE program, the Partnership program (FIDE-SNP) for Medicare-eligible and Medicaid-eligible older adults and adults with disabilities, as well as the Family Care program (Medicaid MLTSS) and has been operating as a care coordination organization since 1977. All of CCI programs target low-income and minority populations, including older adults, who may need additional support to manage health needs. CCI's PACE and Partnership programs use interdisciplinary teams, including acute and LTSS providers (e.g., home care), to provide individualized care. CCI demonstrates how information exchange practices have evolved over time in a mature program, meeting a variety of service needs.
D.2. Site Visit Participants
-
Program leadership and management:
- Chief Executive Officer
- Director of Business Development
- Chief Medical Officer
- Chief Program Officer
- Director of Quality and Risk Management
- Program Officer
- Clinical Services Officer
- Regional Director
- Provider Quality Manager
- Director of Technical Assistance
-
Program staff and providers (e.g., care coordinators or care managers, PCPs):
- Director of Behavioral Health
- Palliative Care/Ethics Manager
- Director of Pharmacy
- Director of Clinical Services
- Transportation Manager
-
HIT program staff:
- Chief Information Officer
D.3. Community Care Information Exchange Overview
-
Figure D-1 is a diagram of how information flows among the various CCI, providers and staff, its external partners, and its members.
-
The green arrows indicate an electronic exchange of information where both participating parties can send and receive information through the electronic system.
-
The CCI Health System acute care and LTSS providers can send and receive information from the CCI Intergy EHR system.
-
The CCI care team can send and receive information from the CCI Intergy EHR system.
-
CCI care teams can send and receive information through various electronic systems, in addition to the Intergy EHR system, including SharePoint, which is a web application platform from Microsoft Office that provides snapshots of information on each member; the Provider Enterprise System (PES), which maintains information about all providers that CCI contracts with; and CCI's authorization portal, which external partners must use to notify CCI's care team when authorization is required for certain services.
-
-
The blue arrows indicate an electronic exchange of information where just one participating party can send information and the other party can only receive or access the information through that electronic system.
-
External acute care and LTSS providers can access electronic information from CCI's authorization portal.
-
-
The orange arrows indicate an information exchange process that requires manual methods of exchange, such as through phone, fax, or exchange of hardcopy documents.
-
CCI care teams exchange information (both send and receive) through these manual methods with patients, external acute care and LTSS providers, and CCI acute care and LTSS providers.
-
The patient also exchanges information through these manual methods with all providers and care teams.
-
CCI acute and LTSS providers exchange information through manual methods in addition to communicating through the CCI Intergy EHR system.
-
-
-
Care managers act as the information hub connecting providers exchanging information about CCI members. The care managers collect and extract data from other sources and then send on the information to other care team members or other providers, often as progress notes. All CCI programs include care teams who focus on care coordination, but the number of care team members differs by program. PACE includes at least 11 care team members (per statute requirements); the Partnership program care team includes a nurse practitioner, social worker and registered nurse; and the Family Care team includes a registered nurse and a care manager.
-
CCI has an EHR system for their internal providers. All CCI providers can access the EHR, but the basis of coordination really happens in the face-to-face interaction among the providers and care managers in care team meetings. Information shared between care coordinators and other providers of the care team is generally shared verbally, by fax, or by using an encrypted e-mail system. Several providers noted that the key to the coordination is around these care teams. Many also mentioned that building relationships with external providers is also critical to the information exchange process.
-
The primary method for receiving information from external providers is through the authorization process. CCI is in the process of developing a portal in which CCI providers will get an alert that they have authorization requests. When the CCI care team sends the authorization to the external provider, they will also plan to include the part of the care plan that this service applies and the provider will have to sign off on the receipt of that part of the care plan (per state requirement that all providers must acknowledge care plan). Communication around member goals with external providers may occur during discussions with care team and provider, but these goals will not be included in the electronic authorization portal.
-
The care teams also rely on several other electronic systems as part of their information exchange processes. SharePoint, which is a web application platform from Microsoft Office, is generally used during team meetings. SharePoint provides snapshots of information that the team needs to track for each member. The information in SharePoint is directly pulled from CCI's EHR. The PES is another electronic tool used by the care team. PES maintains information about all providers that CCI contracts with who provide services to their members. The tool includes specification about the providers so that the care team can search the providers by type and geographic location. The PES also includes information on the provider rates, any Office of Inspector General notices or other quality concerns. CCI maintains internal tracking of its provider network based on incidence reports or routine site visits conducted by CCI staff.
| FIGURE D-1. Community Care Information Flow |
|---|
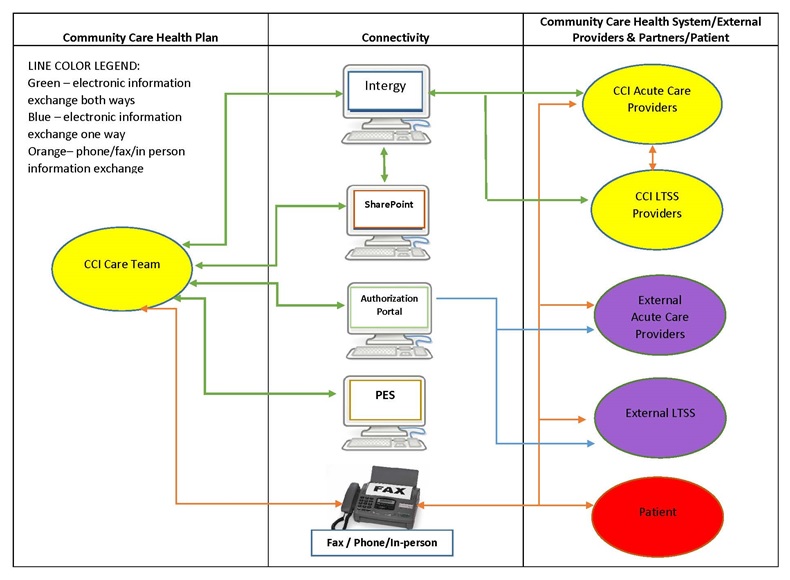 |
Short Diagram Description: Figure D-1 demonstrates how information flows among the various providers of Community Care, Inc. (CCI) providers and staff, its external partners, and its members. Different providers participating in or with the CCI system use different connectivity methods to share information about a patient.
|
This report was prepared under contract #HHSP23320100021WI between HHS's ASPE/DALTCP and RTI International. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/office-disability-aging-and-long-term-care-policy-daltcp or contact the ASPE Project Officer, Jhamirah Howard, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. Her e-mail address is: Jhamirah.Howard@hhs.gov.