
Friday, October 19, 2018
Printer Friendly Version in PDF Format (24 PDF pages)
Panel 2: Managing Behavioral Symptoms of AD/ADRD
Michelle Dionne-Vahalik
Laura Gitlin
Panel Discussion
- Helen Kales, MD, University of Michigan, Ann Arbor
- Ellen McCreedy, PhD, Brown University
- Moderator: Laura Gitlin
Moving evidence-informed assessment and management of behavioral symptoms out of the ivory tower and into the real world: The DICE Approach and the WeCareAdvisor
Helen C. Kales MD
Professor of Psychiatry
Director, Program for Positive Aging
University of Michigan
 |
What made the difference?
- ABILITY TO ACCESS RELEVANT RESOURCES PRECISELY WHEN NEEDED=Technology ("Sat Nav"; AirBnB; Google for walking maps and hours of operation)
- PERSONALIZATION=Trip included something for everyone (shopping, kitschy hats, Guinness factory)
- TRAINING=Knew what to expect (roundabouts; driving on left side of road; guest house ladies don't like check-ins after tea time)
- Currently, the 5 million people with dementia and their 15 million family caregivers find themselves navigating without resources, personalization or training
- Spheres that people with dementia and their families must navigate
- Medical
- Legal
- Functional
- Social
- Financial
Dementia behaviors (BPSD) and their consequences
|
|
Dementia Care for BPSD: Big problem #1
- Big problem #1=Inability to access relevant resources precisely when needed
- Few specialists, concentrated in academic centers
- Primary care physicians with too little training
- Dementia is more than a "medical" illness, there are multiple other spheres it impacts (legal, financial, functional, social)
- Resources are available but can be hard for caregivers to find and access
Lack of resources impacts on family caregivers and people with dementia
- Caregiver themselves:
- Stress
- Burden
- Depression
- Burnout
- Lost income
- To the person with dementia:
- Unoptimized health and function
- Limited social engagement
- Lack of tailored activities
- Within the dyad:
- Lack of understanding about dementia ("he's doing this on purpose")
- Poor communication (yelling, negative communications)
- Expecting too much for the person's dementia stage
Dementia Care for BPSD: Big problem #2
- Personalized medicine=treatment focusing on patients based upon their individual clinical characterization
- Precision medicine=focus on identifying which treatment approaches will be effective for which patients
- Big problem #2=Current dementia care is neither personalized nor precise
- Given the lack of a cure for dementia, the current focus is on day to day management
- Much of that management is focused on the ubiquitous and extremely challenging behaviors that accompany dementia
- Current real-world care (community or NH) for behaviors is largely centered on medicating/sedating people with dementia
Current "Assessment"/Treatment of Physical vs. Behavioral Symptoms
- Family caregiver dealing with a behavior:
- "Joe is agitated"
- "I need something to calm Joe down"
- "Can we get an order for Risperdal 0.5 BID?"
- PCP
- "I'll write for the Risperdal now"
Dementia Care: Big problem #3
- Medications not very effective (1950's treatment for 21st century patients)
- In most cases, medications do not treat the underlying problem, but cover it over (e.g. sedate)
- Medications are associated with significant side effects including mortality
- Efforts by national policy bodies to limit use of one medication (e.g. antipsychotics) drive up use of others (e.g. anticonvulsants)
- Behavioral and environmental treatment strategies if selected appropriately (precision medicine) are more effective
 |
| Table 3. Adjusted Mortality Risk Differences in Death Rates During the 180-Day Observation Period Between Medication Users and Antidepressant Usersa | ||
|---|---|---|
| Medication | Risk Difference, % (95% CI) |
NNH (95% CI) |
| Antidepressant | [Reference] | NA |
| Hiloperidol | 12.3 (8.6-16.0)b | 8 (6-12) |
| Olanzapine | 7.0 (4.2-9.8)b | 14 (10-24) |
| Quetiapine | 3.2 (1.6-4.9)b | 31 (21-62) |
| Risperidone | 6.1 (4.1-8.2)b | 16 (12-25) |
| Valproic acid | 5.1 (1.8-8.4)b | 20 (12-56) |
Antipsychotic use HAS declined--but does that mean that fewer people with dementia are being medicated with psychiatric drugs?
- Programs such as CMS' National Partnership have driven down nursing home AP use
- Unintended consequences?: Shift to other psychotropics with less evidence of benefit and similar risks?
| Figure 1. Percentage of Long-Stay Nursing Home Residents Prescribed an Antipsychotic or Other Psychotropic Medication |
|---|
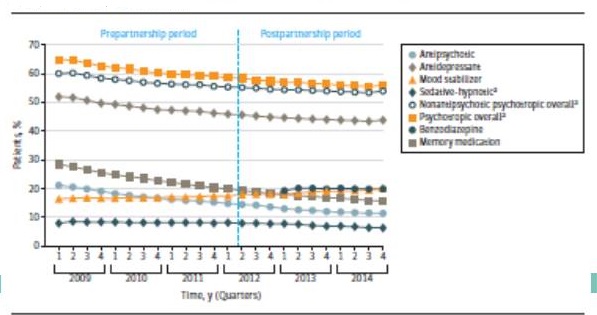 |
| Maust, Kales et al, JAMA Internal Med, 2018 |
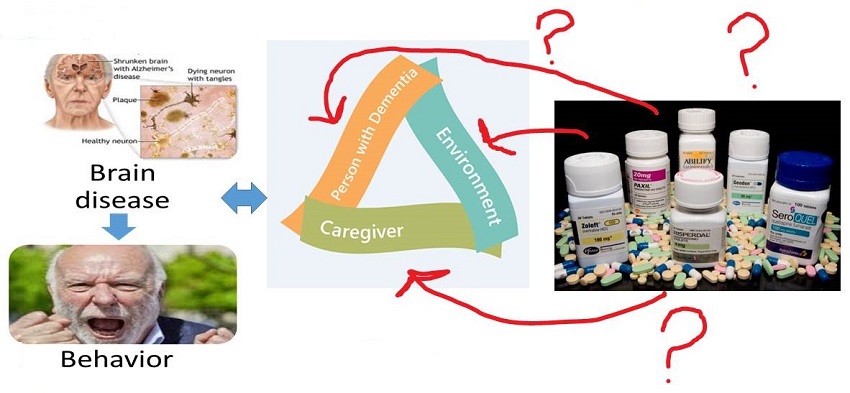
BMJ Conceptual Model
- Consequence of neurodegeneration associated with dementia
- Creates an increased vulnerability to stressors
- Stressors include patient, caregiver and environmental factors
- No one-size-fits all solution
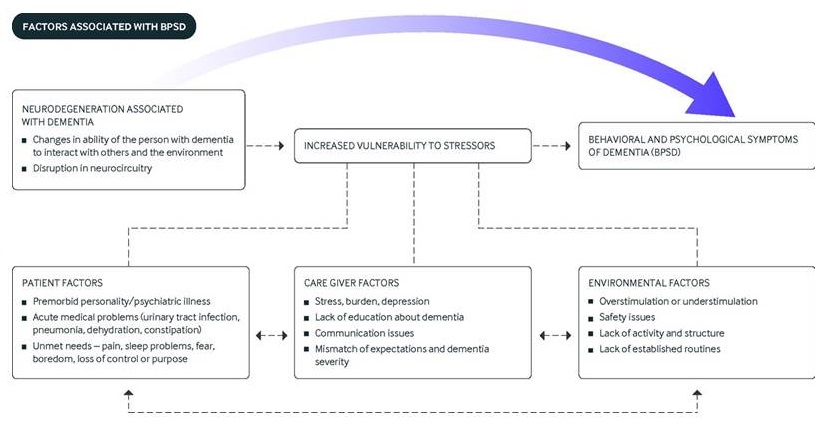 |
| Kales, Gitlin, Lyketsos BMJ 2015 |
Does how we treat behaviors currently make sense?
 |
Non-pharmacologic treatment
- Numerous expert bodies recommend as first-line
- May be better stated as "ecobiopsychosocial" interventions
- Largely NOT been translated to real-world care and clinical settings
- Lack of scalable training programs for caregivers and providers
- Time required
- Lack of guidelines-what strategy to use and when?
- So many interventions (e.g. acupuncture, music therapy, reminiscence)--what works?
- Big problem #3: Lack of training among caregivers (or providers) on how to use proven non-pharmacological strategies to manage behavioral symptoms
Molinari et al, 2010; Cohen-Mansfield et al, 2013
How can we solve Big Problems #1, 2 and 3?
With innovation, "packaging" and technology
The DICE Approach
- Program for Positive Aging organized and funded a 2011 meeting of national experts across disciplines
- Consider possible etiologies
- Include caregiver in process
- Integrate pharmacologic and non-pharmacologic
- Build in flexibility to use in various care settings
- Goal to avoid knee-jerk prescribing without assessment of underlying causes
- *We need to better PACKAGE non-pharmacologic approaches
Kales, Gitlin, Lyketsos JAGS 2014
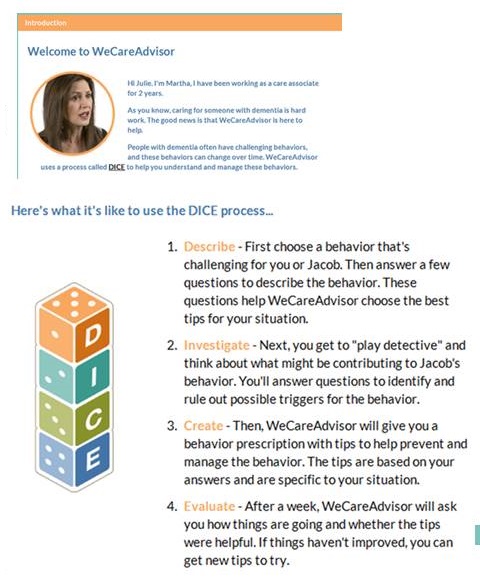
Describe, Investigate, Create, Evaluate
- Describe a behavior that challenges; who, what, where, when, and how the behavior occurs
- Investigate thinking like a detective and explore the person with dementia, the caregivers, and environment for possible clues to triggers underlying possible causes of behavior
- Create a prescription in collaboration with your team to help prevent and manage behaviors
- Evaluate and review prescription effectiveness, and modify or restart the process as needed
- Describe: Consider psychiatric medication use only if there is concern for harm/risk including significant person with dementia distress
- Investigate: Consider psychiatric medication use if behavior is not allowing a full investigation to occur (e.g. fear of aggression preventing blood draw or urine sample)
- Create: Consider psychiatric drug use as a first-line if there is serious depression, psychosis or aggression with risk
- Evaluate: If medications were used, how well did they work? Evaluate for adverse effects, whether there is still risk and whether medications could be tapered and discontinued
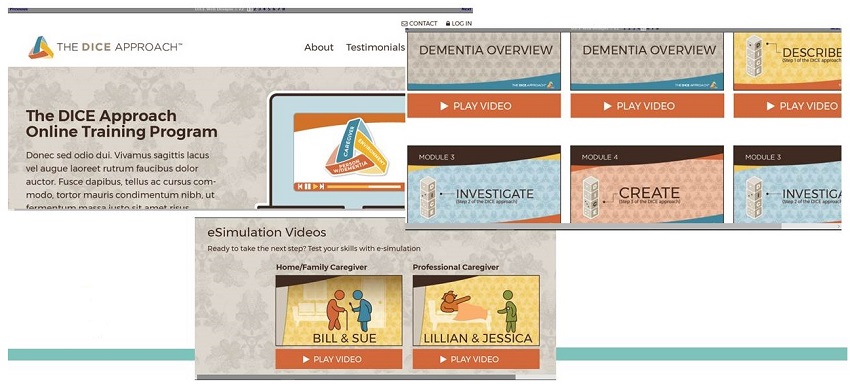
We've "Packaged" the Approaches Via DICE, How do we Deliver Them?
- Pilot of DICE Training: 1 day; 8 modules with 1.5 hour brainstorming session
- Wisconsin-1 statewide training n=125, results pending
- Michigan-3 trainings (Grand Rapids, Ann Arbor, East Lansing)
- Mix of family and professional (RN, LPN, CNA, PT, RT, SW) caregivers
- N=182
- Both groups with significant improvement from pre to post
- Most helpful aspects:
- Use of workshop materials (case studies, role playing, time to talk to other providers)
- Combining paid professionals and home/family care givers for interaction and learning
- Use of simple framework (DICE) that is understandable to all
- Covering medication issues (effect on older adult, family, paid caregivers)
- Handouts to take home
DICE Website--Coming Soon (Dec 1, 2018)
 |
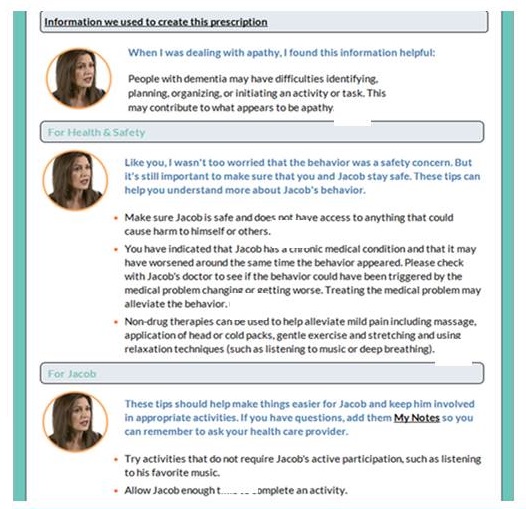
The WeCareAdvisor
- Big Problem #1=Inability to access relevant resources precisely when needed
- The WeCareAdvisor contains a comprehensive "Caregiver Survival Guide" that includes vetted medical, legal, financial, functional and social information. It also includes linkage to additional outside resources
- Daily supportive/motivational messaging for caregivers
 |
- Big Problem #2=Current dementia care is neither personalized nor precise
- Personalized peer navigator to lead caregivers through the tool
- Use of the DICE Approach within the tool to figure out the individual reasons for behavioral and functional changes (personalized care)
 |
- Big Problem #3=Lack of training for caregivers on how to use non-pharmacologic strategies to manage dementia behaviors
- After using the DICE approach within the WeCareAdvisor (to figure out the underlying causes of behaviors), an individualized "prescription" is created for the caregiver and person with dementia (precision medicine)
- Using a proprietary algorithm, (based on caregiver input during DICE) treatment strategies are selected from over 1000 contained in the tool
 |
Nice. But does it work?
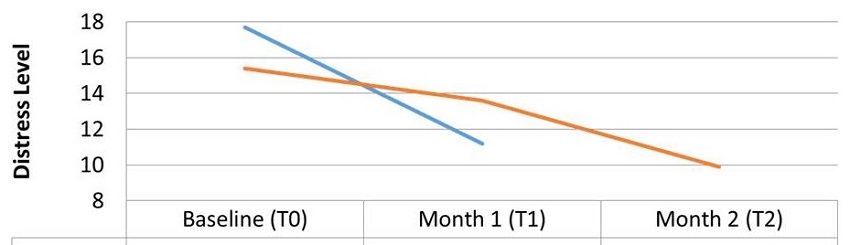
- Randomized controlled trial of the WeCareAdvisor in comparison to wait-list control (BMC Geriatrics, 2017)
- During brief (one-month) use of the tool:
- Family caregivers had significant reductions on the primary outcome of DISTRESS
- Distress is associated with most of the negative outcomes of dementia caregiving (hospitalizations, NH placement)
- Trends to decreased dementia behaviors
| Caregiver Distress |
|---|
 |
Caregiver Feedback
- "Wonderful new tool in my caregiving arsenal"
- "DICE structures my thinking"
- "Survival guide is comprehensive"
- "I shared the tool with my support group and everyone was impressed by the content and ease of use"
- "Love the feeling of support"
- "Ease of use if very nice"
- "Daily tips are awesome"
- "I wish I would have had this a long time ago"
- "I learned a great deal more about dementia and the skills to use in dealing with related behaviors"
- "This week my spouse had a UTI and the WeCareAdvisor helped to trigger in my mind that something was wrong and he should see the doctor"
- "We can go to the doctor, go to support groups, but I see the value of having this daily. This is advice every day"
Summary
- The number of people with dementia and their family caregivers is large and growing every day with the aging of the population
- Living well with dementia is the goal
- Current care systems are inadequate and lead to multiple poor outcomes
- Innovative solutions like the DICE Approach with delivery methods including a manual, training and website as well as the WeCareAdvisor can put the key components of good dementia care at the fingertips of the people who need it most
Acknowledgements
- NIMH: R01MH081070 (Antipsychotic Pharmacoepidemiology)
- H. Myra Kim PhD
- Donovan Maust MD MS
- Lon S. Schneider MD
- Frederic C. Blow PhD
- NINR: R01NR014200 , DOD W81XWH-16-1-0551, Michigan Health Endowment Fund, MDHHS (WeCareAdvisor and DICE Approach)
- Laura Gitlin PhD
- Kostas Lyketsos MD
- Katherine Marx PhD
- Barbara Stanislawski MSW MPH
- VA Merit IIR 15-330 and Donahue Foundation (Unintended Consequences of AP reduction efforts)
- Ilse Wiechers MD
- Donovan Maust MD MS
- Kara Zivin PhD
- Orna Intrator PhD
Music & Memory: A Pragmatic Trial for Nursing Home Residents with Alzheimer's Disease (METRIcAL)
Study Principal Investigator: Vince Mor, PhD
Study Director (Presenter): Ellen McCreedy, PhD
Center for Long-Term Care Quality & Innovation
Brown University, School of Public Health
Acknowledgements & Disclaimers
- METRIcAL: Music & MEmory: A Pragmatic TRIal for Nursing Home Residents with ALzheimer's Disease
- NIA R21AG057451 (PI: Vincent Mor, PhD)
- NIA R33AG057451 (PI: Vincent Mor, PhD)
- The views and opinions expressed in this presentation are those of the presenter and do not necessarily reflect the official policy or position of the funder.
- Pilot results do not imply causality. Brown will be conducting a pragmatic, cluster-randomized controlled trial (P-RCT) of the Music & Memory program in 81 nursing homes. This trial is set to begin in January, 2019.
What is Music & Memory?
- Music & Memory is a personalized music program
- Description: Staff identify music a nursing home resident with dementia preferred when s/he was a young adult and load music on a personal music device (MP3 player)
- Popularity: Thousands of nursing homes in the US have become certified in the program, several state initiatives, subject of a powerful documentary "Alive Inside"
- Potential benefits: non-pharmaceutical alternative to managing agitated behaviors; improve sleep / alertness; decrease resistance to staff assistance with dressing or bathing; appetite stimulation; improve quality of life
- Limitation: Rigorous evaluation is necessary to establish efficacy and to characterize factors associated with effective implementation
How does Music & Memory work?
- The mechanism for action is not totally understood
- Groundbreaking neuroscience suggests musical memories are encoded in regions of the brain that are "relatively spared in Alzheimer's disease." (Jacobsen, et al., Brain, 2015)*
- Based on Cohen-Mansfield's unmet needs model for behaviors in dementia, we hypothesize that personalized music (or familiar musical memories) may reduce agitated behaviors by addressing boredom, sensory deprivation, and/or loneliness. (Cohen-Mansfield et al., Psychiatry Research, 2015)*
*Full references available upon request: ellen_mccreedy@brown.edu
Preliminary Evidence
- Using available administrative data, identified 98 nursing homes who became certified in the Music & Memory program during 2013 (Thomas et al., American Journal of Geriatric Psychiatry, 2017)*
- Matched to nursing homes which "looked like" the Music & Memory certified nursing homes in 2012 (pre-intervention)
- Found greater increases in antipsychotic discontinuation among residents with dementia living in nursing homes with Music & Memory certification
- 2.6% increase in discontinuation in Music & Memory homes versus a .7% decrease in discontinuation in matched homes that did not become certified
- Found residents with dementia in nursing homes which became certified in Music & Memory were more likely to have reductions in agitated behaviors
- 5.6% increase in behavior reductions in Music & Memory homes versus a .1% increase in behavior reductions in matched homes that did not become certified**
*Full references available upon request: ellen_mccreedy@brown.edu
**Among residents with behaviors at baseline
Preliminary Evidence (Limitations)
- Music & Memory certification (4 hour online training) used as indicator of program implementation
- large variation in intervention protocol and implementation intensity
- unclear what is in the syringe
- Music & Memory certification subject to selection
- Nursing homes becoming certified in Music & Memory are likely high performing, interested in quality improvement, and/or participating in other programs to reduce antipsychotic use
- We are unable to observe these factors in the available administrative data
- Effect on behaviors was statistically significant but relatively small
- Potential underreporting of behaviors in standardized residents assessments
- Need better measures to capture change in agitated behaviors in response to Music & Memory
Pragmatic Trial of Music & Memory
- Music & Memory: A Pragmatic Trial for Nursing Home Residents with Alzheimer's Disease (METRIcAL)
- 6-month pilot in 4 nursing homes to standardize protocol and test measurement strategy (R21) followed by a four year pragmatic, cluster-randomized trial in 81 nursing homes (R33)
- Addresses limitations of previous research by:
- standardizing protocol and measuring variation in implementation,
- randomizing nursing homes to timing of intervention (includes lower quality homes), and
- supplementing administrative measures of agitated and aggressive behaviors with direct observation of residents when they are using and not using the music and staff reporting of resident behaviors
| Characteristics of Participating Corporations | ||||
|---|---|---|---|---|
| Corporations | ||||
| A | B | C | D | |
| Eligible Nursing Homes (#) | 69 | 12 | 25 | 76 |
| Geographic Region | Mid-West | Mid-West | Mid-Atlantic | South |
| African American Residents (%) | 1% | <1% | 53% | 42% |
| CMS Overall Quality Star Rating (Mean) | 3.4 | 4.5 | 2.0 | 3.1 |
| Ownership Type | Non-Profit | Non-Profit | For-Profit | For-Profit |
| Any Antipsychotic Use in Last 7 days (% of residents*) | 23% | 18% | 25% | 26% |
| Any Agitated Behaviors in Last 7 days (% of residents*) | 27% | 14% | 15% | 17% |
| *Long-stay nursing home residents with moderate to severe dementia | ||||
| Measuring Agitated and Aggressive Behaviors (Tradeoffs) |
|---|
 |
| Study Data Sources | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Study Data Sources | Agitation / Aggression |
Antipsychotics | Anxiolytics | Antidepressants | Sedatives | Depression | Quality of Life |
Intervention Characteristics |
Implementation Adherence |
| Evaluating Study Outcomes | |||||||||
| Standardized Assessments (MDS) * | X | X | X | X | X | ||||
| Resident Observation ** | X | X | X | ||||||
| Staff Interview ** | X | X | X | ||||||
| Medication Order Records * | X | X | X | X | |||||
| Evaluating Implementation | |||||||||
| User Defined Assessment (EHR) * | X | X | |||||||
| iPod Metadata ** | X | X | |||||||
| Key Informant Interviews | X | ||||||||
| Environmental Scan | X | ||||||||
| * = secondary data ** = primary data MDS = Minimum Data Set EHR = Electronic Health Record |
|||||||||
Music & Memory Pilot (R21)
- 4 nursing homes, 1 per partnering corporation
- 47 residents with moderate or severe dementia received the Music & Memory program during the 6-month pilot (January, 2018 - June, 2018)
- 34 of the 47 residents had data available pre-music and post-music
- Measured agitated behaviors by:
- Directly observing residents when using and not using music (Agitated Behaviors Mapping Instrument),
- Interviewing staff members about resident behaviors (Cohen-Mansfield Agitation Inventory), and
- Using available administrative data (MDS 3.0, Section E)
- The staff interview tool was the Cohen-Mansfield Agitation Inventory (CMAI)
- 29-item scale to assess agitated behaviors in nursing home residents with dementia
- For each behavior, staff indicate average frequency during last two weeks
- Seven response choices for each item, ranging from never (1) to several times per hour (7)
- Validated overall score and sub-scores (domains): physically aggressive behaviors, physically nonaggressive behaviors, verbally agitated behaviors, and hiding and hording behaviors
| Unpublished Pilot Data (do not distribute without permission): Within-Person Changes in Agitated Behaviors Before and After Using Music & Memory, Based on Staff Interviews using the Cohen-Mansfield Agitation Inventory* | ||||
|---|---|---|---|---|
| Before Music & Memory |
After Music & Memory |
Within Person Change |
Wilcoxon signed rank test |
|
| Mean (SD) | Mean (SD) | Mean (SD) | p-value | |
| Total Score | 61.24(16.32) | 51.24(16.05) | -10.00(18.94) | 0.002 |
| Physically aggressive behaviors | 18.03(7.16) | 15.03(5.78) | -3.00(5.98) | 0.013 |
| Physically nonaggressive behaviors | 15.85(6.51) | 13.38(6.84) | -2.47(5.07) | 0.002 |
| Verbally agitated behaviors | 13.74(6.20) | 11.03(6.02) | -2.71(7.47) | 0.033 |
| Hiding and hording behaviors | 2.65(1.23) | 2.44(1.69) | -0.21(1.93) | 0.303 |
| *Includes 34 of the 47 residents with moderate to severe dementia who received Music & Memory during the pilot and had staff interviews before and after receiving the Music & Memory program. Higher scores = more frequent behaviors | ||||
- The direct observation tools were the Agitation Behavior Mapping Instrument (ABMI) and the Lawton's Modified Behavior Stream (LMBS)
- The Agitation Behavior Mapping Instrument (ABMI) records count of the number of times 13 specific verbally and physically agitated behaviors occurred during short, 3-minute observation windows
- After 3-minute observation, Lawton's Modified Behavior Stream (LMBS) used to record perceived affect / mood states
- Duration was of perceived mood states was recorded as: Never (1), Less than 16 seconds (2), Less than half (3), More than half (4), All or nearly all (5)
| Unpublished Pilot Data (do not distribute without permission): Within-Person Changes in Agitated Behaviors and Mood while Using and not Using Music & Memory, Based on Direct Observation using the Agitation Behavior Mapping Instrument and Lawton's Modified Behavior Stream* | ||||
|---|---|---|---|---|
| Not During Music & Memory |
During Music & Memory |
Within Person Change |
Wilcoxon signed rank test |
|
| Mean (SD) | Mean (SD) | Mean (SD) | p-value | |
| Total Agitated Behaviors | 4.40(2.26) | 1.56(1.49) | -2.83(2.25) | <0.001 |
| Pleasure | 1.41(0.46) | 2.47(1.02) | 1.06(1.07) | <0.001 |
| Sadness | 1.37(0.71) | 1.06(0.28) | -0.30(0.80) | 0.050 |
| Interest | 1.77(0.80) | 3.11(0.83) | 1.34(1.23) | <0.001 |
| Anxiety | 2.53(0.88) | 1.79(0.90) | -0.74(1.20) | 0.003 |
| *Includes 31 of the 47 residents with moderate to severe dementia who received Music & Memory during the pilot and had observations when using and not using the music. Higher scores = more frequent behaviors or more time spent in mood state | ||||
| Unpublished Pilot Data (do not distribute without permission): Percent of residents perceived as experiencing pleasure, interest, and sadness for more than half of a 3-minute observation, while using and not Music & Memory, Using the Lawton's Modified Behavior Stream* |
|---|
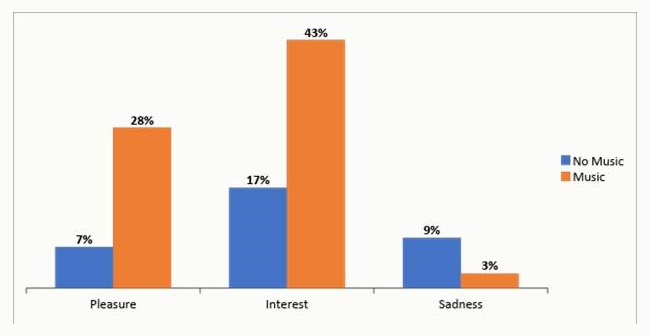 |
| *Includes 31 of the 47 residents with moderate to severe dementia who received Music & Memory during the pilot and had observations when using and not using the music. |
- "[Resident] fell in love with it and didn't want to take it off. She sat and hummed, an emotional peace for her, so she doesn't have flashbacks and calling out for people. [The music] keeps her happy."
- "[Resident] has anxiety and tearful...loves his music, says "you got good music here." Wife visits, use splitter and listen together...sat a long while, holding hands."
- "[Resident] was hard to wake up, slept through meals. When they put on music 15 minutes before meals, he listened. After about 10 minutes, he'd wake up, take off head phones, eat whole meal."
- "[Resident] constantly moving at meals, shoveling food and grabbing others' food...now she sits at table. When done eating, she took her plate and put it aside and sat down calmly for 20 minutes."
- "[Resident] likes gospel...She is agitated when washing up. [We] put [music] on her and calmed her down. Now do it any time there is a sign she is refusing care. She didn't want to take it off."
- "Put it on [Resident] when she was upset and crying, three minutes of listening and then she calmed down and went to sleep."
Pilot results show a 16% decrease in nursing staff reported agitated behaviors among long-stay nursing home residents with moderate to severe dementia after exposure to Music & Memory program (No causality implied -- stay tuned for RCT results)
Several barriers identified which likely apply to other pragmatic trials of non-pharmaceutical interventions:
- Measurement challenges around capturing effects of non-pharmaceutical alternatives with varying "half lives"
- Providing opportunities for nursing staff to "own" and witness the value of non-pharmaceutical interventions for managing agitated and aggressive behaviors. This is a necessary step, if these interventions are to be used as alternatives to PRN medications.
- Technology! Lower quality nursing homes without consistent high-speed Wi-Fi will have difficulty downloading preferred music. All interventions must have low-tech adaptations or the most vulnerable will be left out.
Contact
Ellen McCreedy, PhD
Assistant Professor
Center for Gerontology and Healthcare Research
Brown University, School of Public Health
121 South Main Street, Suite 6
Providence, RI 02903
ellen_mccreedy@brown.edu
(401) 863-7345
More info:
brown.edu/go/innovation
@LTC_Innovation
Pragmatic Trial of Music & Memory
- Population: Long-stay nursing home residents with moderate to severe dementia
- Intervention: Resident preferred music delivered by individual music players
- Comparator: Usual care (no personalized music)
- Primary Outcome: Staff reported frequency of resident agitated and/or aggressive behaviors
- Secondary Outcomes: Directly observed frequency of resident agitated and/or aggressive behaviors, frequency of resident agitated and/or aggressive behaviors from administrative data, antipsychotic use, anxiolytic use, antidepressant use, hypnotic use, quality of life, depression
- Follow-up: 8-months
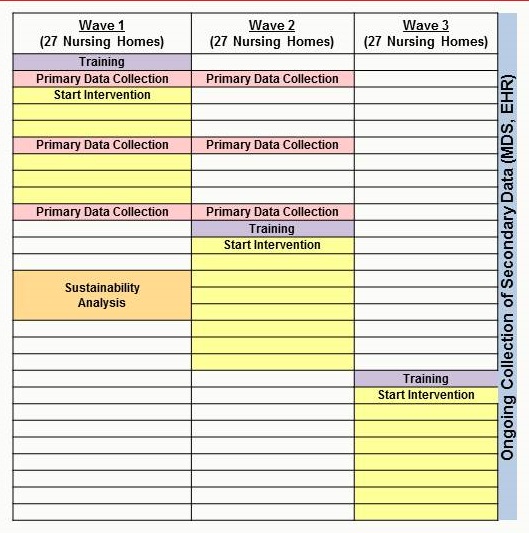
- Trial Design
- Primary outcome assessed using parallel design (Waves 1 and 2)
- Secondary outcomes assessed using stepped wedge design (All Waves)
- By combining primary and secondary measures of agitated behaviors, we are able to capture the "true effect" of the music and look for signal in widely available administrative data
 |