
U.S. Department of Health and Human Services
One-to-One: Vermont's Nursing Home Transition Program
Steve Eiken, Marjorie Hatzmann and Anthony J. Asciutto
MEDSTAT
December 19, 2003
PDF Version: http://aspe.hhs.gov/daltcp/reports/2003/VTtrans.pdf (19 PDF pages)
This report was prepared under contract #HHS-100-97-0019 between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and The MEDSTAT Group. Additional funding was provided by the Center for Medicare and Medicaid Services. For additional information about the study, you may visit the DALTCP home page at http://aspe.hhs.gov/daltcp/home.htm or contact the ASPE Project Officer, Gavin Kennedy, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, SW, Washington, DC 20201. His e-mail address is: Gavin.Kennedy@hhs.gov.
This publication is based on research performed under Contract Number 100-97-0019, entitled "Case Studies of Nursing Home Transition Programs" sponsored by the Office of the Assistant Secretary for Planning and Evaluation (ASPE) and the Centers for Medicare and Medicaid Services (CMS) in the Department of Health and Human Services. The opinions expressed in this report are those of the authors and do not necessarily reflect the views of ASPE, CMS, or Medstat. The authors gratefully acknowledge the many people in Vermont who generously gave us their time and insights for the preparation of this report.
TABLE OF CONTENTS
Transition Coordination
Payment of Up-Front Costs
Identifying Program Participants
Coordinating with Nursing Homes
Obtaining Housing
Obtaining Home and Community-Based Services
EXHIBITS
CHART 1. One-to-One Grant Expenditures
CHART 2. One-to-One Grant Expenditures by Long Term Care Coalition
TABLE 1. One-to-One Program's Original Long Term Care Community Coalitions
TABLE 2. One-to-One Transitioned Consumers
INTRODUCTION
The Centers for Medicare & Medicaid Services (CMS), in association with Office of the Assistant Secretary for Planning and Evaluation (ASPE), sponsored the Nursing Home Transition Demonstration Program to assist states in providing transition options to nursing home residents who wish to move back to the community. CMS and ASPE awarded grants to 12 states between 1998 and 2000.1
The Demonstration permitted states to use grant funds for virtually any direct service or administrative item that held promise for assisting nursing home residents' return to the community. The grants provided targeted administrative or service resources to achieve the following objectives:
- To enhance opportunities for nursing home residents to move into the community by identifying nursing home residents who wish to return to the community and educating them and their families about available alternatives;
- To overcome the resistance and the barriers that may be in the way of their exercising this choice; and
- To develop the necessary infrastructure and supports in the community to permit former nursing home residents to live safely and with dignity in their own homes and communities.
This report, which describes an initiative called One-to-One: Vermonters in Transition (One-to-One), is one of a series of nine case studies presenting results from the Demonstration. The case studies, along with a final report summarizing results from all these states2, provide useful information as states consider nursing home transition efforts or implement nursing home transition programs. Lessons the demonstration states learned during this program are particularly important because CMS awarded a number of Nursing Home Transition grants in 2001 and 2002 under the Systems Change Grants initiative.3
During a February 2002 site visit, Medstat interviewed staff from the Vermont Agency of Human Services' Department of Aging and Disabilities (DA&D), the department responsible for the grant's administration. Medstat also interviewed representatives from three of the ten Long Term Care Coalitions responsible for implementing One-to-One and seven consumers who left nursing homes with the project's assistance. The State of Vermont provided additional information for this report through documents available on DA&D's Web site and documents provided by DA&D staff.4
This case study report focuses on three common components of nursing home transition programs:
- transition coordination or case management to help consumers access housing and services in the community;
- a fund to pay for the up-front costs consumers may incur as they leave a nursing home, such as a security deposit for an apartment; and
- a method to identify nursing home residents interested in transition.
The report also describes how three challenges common among the demonstration programs--coordinating with nursing homes, obtaining community housing, and obtaining home and community-based services--affected One-to-One, and how state and local program staff addressed these challenges. Finally, the report presents data on the results of the program and describes Vermont's subsequent efforts to support nursing facility residents interested in transition.
PROGRAM DESCRIPTION
Vermont received a $500,000 grant in September 1999 to fund the One-to-One program. In its proposal, DA&D set a goal to transition 190 nursing home residents. The One-to-One program started serving people in February 2000, after the state developed and provided initial training about the program for both nursing home employees and home and community-based services (HCBS) providers.
Transition Coordination
Vermont used its network of local Long Term Care Community Coalitions to coordinate transitions. The coalitions include most providers of long-term supports--Area Agencies on Aging, home health agencies, adult day care centers, nursing facilities, hospitals, and residential care homes--as well as consumers and advocates. The coalitions work on ways to improve the long-term care infrastructure and service coordination.
The coalitions had already coordinated nursing home transitions as part of implementation of a 1996 state law called Act 160. Act 160 set goals for reducing the state's nursing home utilization and increasing funding for HCBS. For example, 113 Vermonters left nursing homes and started using Medicaid home and community-based services waivers in state fiscal year 1998.
Vermont initially distributed grant funds to three of the ten coalitions. The state selected these coalitions in part because they served areas with large nursing home populations and had previous success supporting nursing home transitions. A year after the grant began serving consumers, Vermont expanded the One-to-One program to the other seven coalitions because the original coalitions had not been able to transition as many people as expected. The three original coalitions nonetheless accounted for most of the people transitioned under One-to-One.
| TABLE 1. One-to-One Program's Original Long Term Care Community Coalitions | |
| Long Term Care Coalition | Largest Town |
| Champlain Long Term Care Coalition | Burlington |
| Washington County Long Term Care Coalition | Barre |
| Rutland Area Initiative | Rutland |
Vermont established no standard process for coordinating transitions across the coalitions, but instead allowed coalitions the flexibility to continue their current transition efforts or to try something different. Each coalition interviewed for this case study considered One-to-One a continuation and expansion of its nursing home transition responsibilities and activities and did not change its process significantly. Each coalition assigned nursing home residents who wanted to transition to a team consisting of a registered nurse and a case manager. This team coordinated transitions on a part-time basis while also assisting people in the community.
The coalitions were well suited to connect transitioning nursing home residents to long-term supports in the community. The local Area Agency on Aging (AAA) and at least one home health agency were active in each of the coalitions. The state required each coalition to designate one of these organizations to administer Vermont's Medicaid HCBS waivers for older people and people with physical disabilities. Also, the AAA could connect former residents to services available under the federal Older Americans Act and a home health agency could connect people to home health care funded by Medicare or the Medicaid state plan. Staff from these organizations often formed the transition teams. Sometimes one or both of the transition coordinators was also a case manager for a waiver, enabling the resident to keep working with the same person after discharge.
Vermont encouraged the coalitions to contact residents as a first step after receiving a referral, to learn the residents' preferences. However, two interviewed coalitions approached residents only after talking to nursing home staff, reviewing the residents' charts, and talking to their family. Staff from these areas expressed concern about raising residents' expectations if these expectations cannot be met and said approaching residents first can cause negative outcomes for people who cannot move to the community.
Payment of Up-Front Costs
Vermont paid grants to each coalition for all expenses related to the One-to-One program, including transition coordination and transition expenses. Transition expenses did not require state approval, and the local coalitions could pay for necessary expenses right away. Each of the coalitions managed grant funds locally and reported their expenditures quarterly to DA&D.
Coalition members said the flexible funds were an important component of the One-to-One program. Coalitions used the grant to pay for home modifications, assistive technology, waste disposal, and items necessary to set up a household such as furniture and linens. Some coalitions also used grant funds to pay for personal care during trial days in the community, in which the person returned home for a few days to test whether he or she would feel comfortable in the community. Coalition members said they broadened their belief in who could be discharged from a nursing home because of the additional funds available for transition expenses. The coalitions already received some flexible funds from the state that could be used for transition expenses, but the amount was small ($10,000 per coalition) and was also used to provide flexible supports for people already in the community.
Identifying Program Participants
Vermont identified candidates for nursing home transition through two methods. First, coalitions identified transition candidates through the Medicaid assessment process for nursing home residents. Vermont requires an independent assessment to ensure Medicaid-funded nursing home services are necessary. Second, the state used the data nursing homes are required to collect for the federal Minimum Data Set (MDS).
A few months prior to starting the One-to-One program, DA&D started a pilot project to shift the responsibility for nursing home assessments from DA&D to local home health agencies. The home health agencies were able to provide a face-to-face review and, if the assessor believed the resident did not need a long-term stay, the home health agency could quickly work with the nursing home, HCBS providers, and the person to develop a discharge plan. The home health agencies were also able assess residents more quickly, which provided a benefit to nursing homes that could then bill Medicaid more quickly.
Vermont used the federal grant monies under One-to-One to pay for home health agencies' initial expenses--such as training--when conducting nursing home assessments. The three coalitions that originally started One-to-One were also the first coalitions where home health agencies conducted nursing home assessments. DA&D gradually extended these duties to home health agencies in the rest of the state. The home health agencies used the same registered nurses who determine functional eligibility for the Medicaid HCBS waivers that are alternatives to nursing homes. The nursing home assessments gave home health agency staff an opportunity to enter nursing homes and identify people who may move to the community.
Using MDS data, Vermont identified nursing home residents with characteristics that the state's earlier nursing home transition experience indicated would make transition easier. These characteristics were:
- an expressed a desire to live in the community;
- the Resource Utilization Group (RUG) Special Rehabilitation or Clinically Complex;
- bowel and bladder continence; and
- a Cognitive Performance Score indicating the person was cognitively intact or borderline intact.
Vermont then sent each of the original coalitions a list of residents in its area with these characteristics. The DA&D and the coalitions quickly found, however, that this list was not useful for One-to-One. A few months had elapsed between the time Vermont obtained the MDS data and the time the coalitions received their lists of residents. During that time, the majority of candidates on the lists had already left nursing homes. Coalition members said the people who remained in facilities were not appropriate for community services. Some coalitions noted that the criteria used to develop this list did not include some non-clinical factors that influence a person's ability to live in the community, such as the level of available informal support.
According to coalition members, early involvement of the nursing home in transition activities was the most effective means to identify transition candidates early in their admission. In addition to the state's efforts to involve nursing homes, described below, coalition members built on relationships they developed with nursing home staff during the nursing home transition efforts before the grant. A collaborative relationship with nursing home discharge planners in particular was considered critical to a successful program.
Coordinating with Nursing Homes
Vermont involved nursing homes early in the program. Vermont invited all twelve nursing homes in the three original coalitions to an introductory meeting for the One-to-One program. The meeting introduced nursing home staff to the program and enabled DA&D to address nursing homes' concerns and provide assurances that the transition coordinators and the home health agencies providing nursing home assessments were not also functioning as licensing surveyors.
Following the meeting, DA&D's Division of Licensure and Protection conducted nursing home assessment training in each nursing home in two of the coalition areas. During the training sessions, the nursing home administrator and discharge planner, the coalition's transition team, and the home health agency's assessment nurse met to develop and document the best process for assessments and for identifying transition candidates.
State staff said this activity was particularly useful in developing a streamlined and mutually agreed-upon process for identifying transition candidates. In the third coalition area, however, no nursing homes attended the initial meeting and DA&D did not conduct separate training sessions in each facility. Staff from the state and from that coalition reported more resistance to the program from nursing homes in that area. DA&D used the introductory meeting and training sessions format when it expanded the grant to other coalitions. DA&D expanded the grant gradually to ensure that training could be completed.
According to coalition members and consumers, nursing homes' involvement in One-to-One varied from supportive of residents' transitions to moderately involved to completely uninvolved. Some coalitions reported that nursing homes' initial reluctance to work with the transition coordinators lessened after DA&D contacted the nursing facility. DA&D noted that at least one rural coalition with a high number of nursing homes continued to experience facility resistance and was one of four coalitions that did not transition residents during the grant.
Obtaining Housing
State staff and coalition members said a lack of affordable, accessible housing was a significant barrier to transition. For some people, affordable housing was available but the housing was not accessible. Few affordable assisted-living or residential care options were available in most parts of the states, especially in rural areas. Each coalition noted that the availability of flexible funds to cover home accessibility modifications was a great benefit of One-to-One because it allowed participants to avoid the wait lists of other programs.
Obtaining Home and Community-Based Services
People leaving nursing homes had greater access to HCBS after the 1996 passage of Act 160. In addition to creating the Long Term Care Coalitions, Act 160 created a mechanism for increasing the state's budget for HCBS if nursing facility expenditures increased at a slower rate. As mentioned earlier, the law set goals for nursing home utilization. DA&D implemented several initiatives to meet these goals, including:
- Adding the capacity to serve 315 more people to Vermont's largest Medicaid HCBS waiver for older people and people with physical disabilities;
- Starting a Medicaid HCBS waiver that offers 24-hour care in a residential setting for over 100 older people and people with physical disabilities;
- Expanding the types of services provided in adult day care to include nursing, nutrition, and other social services; and
- Starting programs in which people can hire in-home attendants.
Another initiative to implement Act 160 improved nursing home residents' access to Medicaid HCBS waiver services. Like many states, DA&D has a waiting list for its largest Medicaid HCBS waiver serving older people and people with physical disabilities. In 1996, DA&D implemented a waiver prioritization policy that gives priority access to Medicaid HCBS waiver services to people who meet one of four criteria. One of those criteria is being a nursing home resident who wants to move to a home or a community-based setting but cannot do so without waiver services. According to state staff, priority waiver applicants, including transitioning nursing home residents, typically receive services within 60 days.
PROGRAM RESULTS
The One-to-One program served people from February 2000 until September 2001. It lasted one year longer than its initial September 2000 expiration date due to a no-cost extension granted by CMS and ASPE. Over twenty months, coalition members interviewed 231 people about the possibility of leaving a nursing home. Sixty-seven of these people said they were not interested in transition. Of the remaining 164 residents, the coalitions considered 101 people (62 percent) to be appropriate candidates for transition.
Seventy-three of the 101 candidates actually transitioned to community settings under One-to-One. The coalitions transitioned additional people without using the program's transition teams and transition services. This number was well short of Vermont's initial goal of 190 people transitioned. State staff and local coalition members said fewer nursing home residents than expected could easily move to the community because the coalitions had transitioned many people before the One-to-One program.
As Table 2 shows, 61 of the 73 transitioned residents (84 percent) were within the original three coalition areas. Table 2 also lists the number of persons transitioned in each coalition by age and gender. Women were 74 percent of transitioned residents, and people age 65 or older were 93 percent. These demographics reflected national nursing home resident demographics.5
| TABLE 2. One-to-One Transitioned Consumers | ||||
| Female | Male | |||
| Age 65 and Older | Under Age 65 | Age 65 and Older | Under Age 65 | |
| Bennington Community Based Coalition | 3 | 2 | 4 | 0 |
| Champlain Long Term Care Coalition* | 10 | 0 | 6 | 0 |
| Franklin-Grand Isle Counties Advocates for Long Term Care | 0 | 2 | 0 | 0 |
| Lamoille Valley Long Term Care Team | 1 | 0 | 0 | 0 |
| Rutland Area Initiative* | 4 | 0 | 2 | 0 |
| Washington County Long Term Care Coalition* | 32 | 0 | 6 | 1 |
| Total | 50 | 4 | 18 | 1 |
| * Original coalitions participating in One-to-One | ||||
The average length of stay for consumers transitioned under One-to-One was 64 days, which indicates some of these people may have left nursing homes without assistance. According to the 1999 National Nursing Home Survey, two-third of nursing home discharges occurred in the first three months of an admission.
| CHART 1. One-to-One Grant Expenditures |
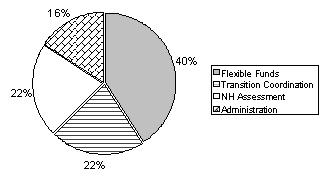 |
Vermont only spent $305,997 of the $500,000 grant. The largest portion of grant funds was spent on flexible funds for transition expenses (see Chart 1). The grant also paid for transition coordination, start-up expenses for home health agencies to conduct nursing home assessments, and the coalitions' grant-related administrative expenses.
| CHART 2. One-to-One Grant Expenditures by Long Term Care Coalition |
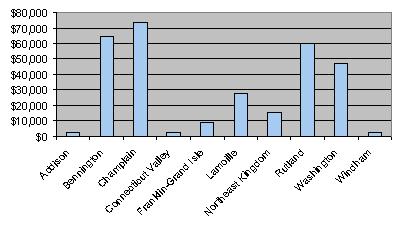 |
Chart 2 displays grant expenses for each of the ten coalitions. Even the four coalitions that did not transition nursing home residents reported expenditures, because all coalitions used grant funds to start their role conducting nursing home assessments. Some coalitions also spent money for transitioning residents that did not move until after the grant period.
NEXT STEPS
The coalitions identified two significant changes under the One-to-One program that increased their capacity to help people move from nursing homes back into the community. One of these changes, the availability of flexible funds specifically for the short-term supports people need when leaving nursing homes, did not continue when the grant concluded in September 2001. The other change, the movement of nursing home assessments from the state to local home health agencies, continued after the grant ended and is still in effect.
The DA&D started a new initiative in 2002 to prevent long-term nursing home admissions by giving people information to make long-term care decisions. Under this initiative, Options Counseling, the Long Term Care Community Coalitions provided information about home and community-based services to all people who were applying for a nursing home admission from the community or entering a nursing home from a hospital with an expected stay of more than 20 days. DA&D staff reported that the program provided information too late in people's decision-making process. The state is considering ways to reach people earlier with information about HCBS options.
BIBLIOGRAPHY
Murray, Joseph. Nursing Homes to Medicaid Waiver in Vermont: An Analysis of Nursing Home Residents who Made the Transition from Institutional Care to Medicaid Supported Community-Based Care In State Fiscal Year 1998
Vermont Department of Aging and Disabilities. 1999.
Vermont Department of Aging and Disabilities. Home-Based Medicaid Waiver Policies and Procedures Manual March, 2001.
Vermont Department of Aging and Disabilities. One to One: Vermonters in Transition. July 20, 1999.
INTERVIEWS
Vermont Department of Aging and Disabilities Camille George Karen Hammer-Williamson Joan Haslett Bard Hill Nancy Marinelli Joan Senecal Megan Tierney-Ward
Washington County Long Term Care Coalition Marilyn Aldrich, Central Vermont Home Health and Hospice Nancy Butryman, Central Vermont Home Health and Hospice Tina Donahue, Central Vermont Home Health and Hospice (with Central Vermont Area Agency on Aging during the grant) Luanne Powers, Rowan Court Health and Rehab Center Sheryl Walsh, Rowan Court Health and Rehab Center
Rutland Area Initiative Katrina Corbett, Southwestern Vermont Council on Aging Wendy Doley, Rutland Area Visiting Nurse Association & Hospice Marlee Mason, Rutland Community Programs Brenad Shortle, Interage Adult Date Care
Champlain Long Term Care Coalition Ann Dilley, Champlain Valley Area Agency on Aging Kathy Hart, Champlain Valley Area Agency on Aging Beverly Boget, Visiting Nurses Association of Chittenden and Grand Isle Counties Peter Lovett, Visiting Nurses Association of Chittenden and Grand Isle Counties Lynn Tracy, Visiting Nurses Association of Chittenden and Grand Isle Counties Sue Watson, Visiting Nurses Association of Chittenden and Grand Isle Counties
Seven consumers and informal caregivers for five consumers
NOTES
-
In 1998, Colorado, Michigan, Rhode Island, and Texas received grants between $160,000 and $175,000 each. In 1999, New Hampshire, New Jersey, Vermont, and Wisconsin received grants of $500,000 each. In 2000, Arkansas, Florida, Pennsylvania, and Nebraska received grants of $500,000 each.
-
Eiken, Steve and Burwell, Brian. Final Report of the Nursing Home Transition Demonstration Grants Case Study. Medstat: publication pending.
-
Twenty-three states and ten centers for independent living received nursing home transition grants in 2001 and 2002. More information is available at the following Web site: http://www.cms.hhs.gov/systemschange/default.asp.
-
References for these reports can be found in the bibliography.
-
Jones, A. "The National Nursing Home Survey: 1999 Summary." National Center for Health Statistics. Vital Health Statistics 13 (152), 2002.
COMPLETE LIST OF SITE VISIT REPORTS
Community Choice: New Jersey's Nursing Home Transition Program
HTML http://aspe.hhs.gov/daltcp/reports/2003/NJtrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2003/NJtrans.pdf
Fast Track and Other Nursing Home Diversion Initiatives: Colorado's Nursing Home Transition Grant
HTML http://aspe.hhs.gov/daltcp/reports/2003/COtrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2003/COtrans.pdf
Michigan's Transitioning Persons from Nursing Homes to Community Living Program
HTML http://aspe.hhs.gov/daltcp/reports/2002/MItrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2002/MItrans.pdf
One-to-One: Vermont's Nursing Home Transition Program
HTML http://aspe.hhs.gov/daltcp/reports/2003/VTtrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2003/VTtrans.pdf
Partnerships for Community Living: Florida's Nursing Home Transition Program
HTML http://aspe.hhs.gov/daltcp/reports/2003/FLtrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2003/FLtrans.pdf
Passages: Arkansas's Nursing Home Transition Program
HTML http://aspe.hhs.gov/daltcp/reports/2003/ARtrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2003/ARtrans.pdf
Pennsylvania Transition to Home (PATH): Pennsylvania's Nursing Home Transition Program
HTML http://aspe.hhs.gov/daltcp/reports/2003/PAtrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2003/PAtrans.pdf
Project CHOICE (Consumers Have Options for Independence in Community Environments): Texas' Nursing Home Transition Program
HTML http://aspe.hhs.gov/daltcp/reports/2003/TXtrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2003/TXtrans.pdf
The Homecoming Project: Wisconsin's Nursing Home Transition Demonstration
HTML http://aspe.hhs.gov/daltcp/reports/2002/WItrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2002/WItrans.pdf
To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human ServicesOffice of Disability, Aging and Long-Term Care PolicyRoom 424E, H.H. Humphrey Building200 Independence Avenue, S.W.Washington, D.C. 20201FAX: 202-401-7733Email: webmaster.DALTCP@hhs.gov
RETURN TO:
Office of Disability, Aging and Long-Term Care Policy (DALTCP) Home [http://aspe.hhs.gov/_/office_specific/daltcp.cfm]Assistant Secretary for Planning and Evaluation (ASPE) Home [http://aspe.hhs.gov]U.S. Department of Health and Human Services Home [http://www.hhs.gov]