
U.S. Department of Health and Human Services
Pennsylvania Transition to Home (PATH): Pennsylvania's Nursing Home Transition Program
Steve Eiken and Alexandra Heestand
MEDSTAT
December 22, 2003
PDF Version: http://aspe.hhs.gov/daltcp/reports/2003/PAtrans.pdf (20 PDF pages)
This report was prepared under contract #HHS-100-97-0019 between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and the MEDSTAT Group. Additional funding was provided by the Center for Medicare and Medicaid Services. For additional information about the study, you may visit the DALTCP home page at http://aspe.hhs.gov/daltcp/home.htm or contact the ASPE Project Officer, Gavin Kennedy, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, SW, Washington, DC 20201. His e-mail address is: Gavin.Kennedy@hhs.gov.
This publication is based on research performed under Contract Number 100-97-0019, entitled "Case Studies of Nursing Home Transition Program" sponsored by the Office of the Assistant Secretary of Planning and Evaluation (ASPE) and the Centers for Medicare and Medicaid Services (CMS) in the Department of Health and Human Services. The opinions expressed in this report are those of the authors and do not necessarily reflect the views of ASPE, CMS, or Medstat. The authors gratefully acknowledge the many people in Pennsylvania who generously gave us their time and insights for the preparation of this report.
TABLE OF CONTENTS
Transition Coordination
Identifying Program Participants
Payment of Up-Front Costs
Coordinating with Nursing Facilities
Obtaining Housing
Obtaining Home and Community-Based Services
COMPLETE LIST OF SITE VISIT REPORTS
EXHIBITS
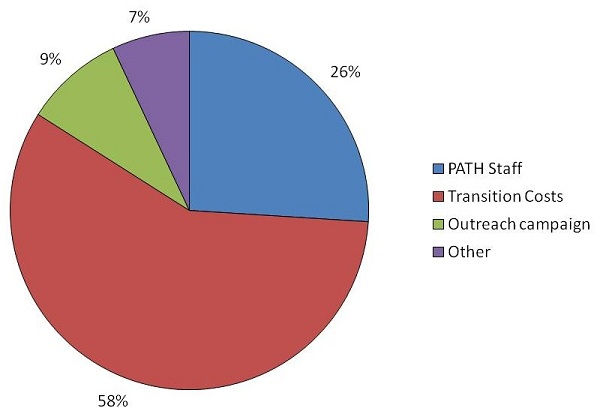
CHART 1. Planned Distribution of PATH Project Expenses
CHART 2. Type of Disability for PATH Transitioned Consumers
INTRODUCTION
The Centers for Medicare & Medicaid Services (CMS), in association with Office of the Assistant Secretary for Planning and Evaluation (ASPE), sponsored the Nursing Home Transition Demonstration Program to assist states in providing transition options to nursing home residents who wish to move back to the community. CMS and ASPE awarded grants to 12 states between 1998 and 2000.1
The Demonstration permitted states to use grant funds for virtually any direct service or administrative item that held promise for assisting nursing home residents' return to the community. The grants provided targeted administrative or service resources to achieve the following objectives:
- To enhance opportunities for nursing home residents to move into the community by identifying nursing home residents who wish to return to the community and educating them and their families about available alternatives;
- To overcome the resistance and the barriers that may be in the way of their exercising this choice; and
- To develop the necessary infrastructure and supports in the community to permit former nursing home residents to live safely and with dignity in their own homes and communities.
This report, which describes an initiative called Pennsylvania Transition to Home (PATH), is one of a series of nine case studies presenting results from the Demonstration. The case studies, along with a final report summarizing results from all these states2, provide useful information as states consider nursing home transition efforts or implement nursing home transition programs. Lessons the demonstration states learned during this program are particularly important because CMS awarded a number of Nursing Home Transition grants in 2001 and 2002 under the Systems Change Grants initiative.3
During a September 2002 site visit, Medstat interviewed PATH staff, who are independent contractors for Pennsylvania, as well as Pennsylvania Department on Aging (PDA) staff involved in implementing the project. Medstat also interviewed four consumers who left nursing homes with the help of PATH and staff from three nursing homes that have provided referrals to PATH. After the site visit, Medstat interviewed staff from other organizations involved in PATH: Pennsylvania's Medicaid agency (the Department of Public Welfare), Pennsylvania Protection and Advocacy, and one of the Area Agencies on Aging that provided home and community-based services to PATH consumers. The Commonwealth of Pennsylvania provided additional information for this report through a progress report on the grant available on PDA's Web site.4
This case study report focuses on three common components of nursing home transition programs:
- transition coordination or case management to help consumers access housing and services in the community;
- a fund to pay for the up-front costs consumers may incur as they leave a nursing home, such as a security deposit for an apartment; and
- a method to identify nursing home residents interested in transition.
The report also describes how three challenges common among the demonstration programs--coordinating with nursing homes, obtaining community housing, and obtaining home and community-based services--affected PATH, and how program staff addressed these challenges. Finally, the report presents data on the program's results and describes Pennsylvania's subsequent efforts to support nursing facility residents interested in transition.
PROGRAM DESCRIPTION
Pennsylvania received a $500,000 grant award in September 2000 to fund the PATH program. Pennsylvania received two one-year, no-cost extensions for the grant, which expired in September 2003. The state's Intra-Governmental Council on Long Term Care (IGCLTC) oversees the grant and several organizations that participate on the Council serve on the program's advisory group. The IGCLTC comprises three members of the governor's cabinet, four members of the state legislature, and governor-appointed representatives that include consumers, advocates, and providers from different long-term care service sectors. The IGCLTC includes the stakeholders who most affect Pennsylvania's long-term care system. The Secretary of Aging chairs the IGCLTC, and the IGCLTC's Executive Director works for the Pennsylvania Department on Aging (PDA).
In its proposal to CMS, the IGCLTC set a goal to transition 95 people, including at least 80 people age 60 or older. Since it planned to target older nursing home residents, the IGCLTC selected four contiguous pilot counties from central and eastern Pennsylvania with a relatively high number of nursing home residents age 60 or older. These counties include two mid-size cities, Harrisburg in Dauphin County and Allentown in Lehigh County. The other two counties (Cumberland and Schuylkill Counties) are rural. In early 2003, the state added three rural pilot counties from the southwest corner of the state (Fayette, Greene, and Washington).
The state hired four independent contractors--a program manager and three transition coordinators--to operate the grant. Two transition coordinators serve the original four pilot counties: one serves Dauphin and Cumberland Counties and the other serves Lehigh and Schuylkill Counties. The third transition coordinator serves the southwest Pennsylvania pilot counties.
As indicated in Chart 1, Pennsylvania planned to spend almost three-fifths of the grant on transition expenditures: items and services people need to establish a home in the community. An additional 26 percent of the grant was earmarked for staff, and the remaining portion was set aside for state-level administrative and outreach expenses.
| CHART 1. Planned Distribution of PATH Project Expenses |
 |
Pennsylvania had to delay PATH implementation for several months because it had difficulty transferring federal funds from the agency that officially received the grant--the Medicaid agency, the Department of Public Welfare (DPW)--to a subcontractor that would serve as the grant's fiscal entity. A fiscal entity was necessary because the IGCLTC did not have legislative authority to spend $500,000 in federal funds. Before the subcontracting process was complete, the Pennsylvania Department of Aging started the program in May 2001 by hiring the project manager, using $6,000 in discretionary funds from its budget. In July 2001, DPW contracted with United Disability Services (UDS) to be the PATH fiscal agent. UDS was already the fiscal intermediary for a home and community-based services program for people with disabilities, so it had a record of working with DPW. The project started serving consumers in the original four counties in November 2001.
Transition Coordination
Pennsylvania hired independent contractors to assist residents who want to transition, believing the traditional civil service hiring processes would be time-consuming and impractical given the short-term nature of the project. The transition coordinators' orientation included meeting with members of the PATH Advisory Committee, which included IGCLTC members and people involved in the pilot areas' long-term care system. These meetings gave the coordinators knowledge about the long-term care system in their service areas and the stakeholders involved in the program. Before serving consumers, the coordinators also met separately with all nursing homes, public housing authorities, and home and community-based services (HCBS) providers in their service area.
After learning about a resident who may be interested in transition, a coordinator contacted the consumer's facility to verify the person's name and to learn the person's Medicaid eligibility status. The coordinator met separately with the potential candidate and the nursing facility discharge planner to assess the person's willingness to transition. If the potential candidate indicated that he or she was not interested in PATH, the transition coordinator left a business card and brochure and told the person that he or she may request PATH assistance at any time. During future visits to that facility, the coordinator briefly visited the resident so the person could express interest in transition if the person changed his or her mind.
The coordinators assisted all residents interested in transition, regardless of the person's financial status. If the person was not eligible for Medicaid, the coordinator and nursing facility discharge planner worked with the resident to develop a plan to support the person in the community. For Medicaid-eligible participants, the coordinator contacted the local agency that assessed eligibility for the appropriate Medicaid home and community-based services (HCBS) waiver. The transition coordinators generally waited until the HCBS agency completed its assessment and developed a community service plan before following up with the resident. Interviewees estimated this wait could be as short as one week or as long as two months. One interviewee recommended more frequent contact from coordinators during this time to address the residents' uncertainty regarding their eligibility for HCBS. Once a plan for community supports was in place, the transition coordinators then worked with the nursing home discharge planner and the resident to access community housing.
In addition, the transition coordinators often connected consumers to peer counselors through the local Area Agency on Aging or Center for Independent Living. Transition coordinators said consumers were often reluctant to transition, even if they are interested in community living, because they feared they would not be safe in the community. Peer counselors provided a consumer perspective on both the benefits and risks of community living.
Pennsylvania developed a database for PATH to help transition coordinators manage their work. The database contained demographic and transition planning information for each PATH consumer. Each consumer's record included an "action needed" reminder to ensure the coordinator knew what tasks to do for that consumer. The database also included contact information from all nursing facilities in the pilot area, and enabled transition coordinators to store additional information about each facility, such as what outreach efforts had been successful. Both the program manager and the coordinators had access to the database, so both could see the same information when the coordinator asked the program manager's advice, even when they were miles from each other. Pennsylvania spent $7,000 developing the database, and the state is willing to share information about it with other nursing home transition programs.
The PATH database, along with laptops funded by the grant, enables the original two coordinators to telecommute. When expanding PATH to the third area, the state required the coordinator to work out of local Area Agency on Aging (AAA) offices in each of the three pilot counties to increase the coordinators' interaction with the AAA staff, who provide Medicaid HCBS waiver case management for older people as well as supports traditionally provided by the Aging Network. Program staff said this arrangement has allowed the coordinator to work more closely with AAA staff.
Identifying Program Participants
The only restriction was that the resident's onset of disability must have occurred on or after age 22. Pennsylvania set this requirement to avoid duplicating an existing program that transitions people whose disability manifest before age 22 and served 35 people in 2001. However, PATH's outreach efforts emphasized that the program was primarily for nursing home residents not likely to transition without assistance.
To promote the program and address stakeholders' questions, PATH staff held meetings in each county to introduce the program before the transition coordinators were hired. The meetings included the local Center for Independent Living (CIL), the local AAA, other home and community based services providers, and nursing facility administrators.
The transition coordinators conducted additional outreach as their first order of business. Each coordinator met staff from every nursing home and home and community-based service provider in his or her territory to encourage referrals to PATH and to learn more about the local long-term care system. In the first year of the program's operation (November 2001-October 2002), about 70 percent of PATH referrals were from nursing facility discharge planners. CILs, AAAs, residents, family members, friends, nursing home ombudsman, public housing authorities, and Pennsylvania Protection and Advocacy also referred people to the program.
To identify additional nursing home residents who could transition, PATH staff collaborated with DPW and PDA staff to use data from the federally required Minimum Data Set (MDS) assessment, which nursing facilities must complete for all residents. PATH, DPW, and PDA staff selected characteristics to identify people with high discharge potential, such as:
- The number occupational therapy days,
- The person's short-term memory ability,
- The person's desire to return to the community, and
- The availability of informal support after discharge.
Pennsylvania then generated a list of consumers who met these characteristics and their facilities. Transition coordinators then asked these facilities' discharge planners about the residents' current status. The MDS data was from calendar year 2000, so the most recent resident data were more than a year old when the transition coordinators contacted nursing homes in 2002. Many of the consumers had died, left the facility, or experienced a significant change in condition during that time, so the use of MDS identified few people who could transition.
In late 2002, PATH hired a public relations firm to develop and implement an outreach campaign to encourage more referrals. The campaign targeted nursing home staff, nursing home resident councils, other resident groups, family members, medical personnel, home health agencies, and older people and people with disabilities in the community. PATH used $45,000 of grant funds for this campaign, which is managed by the state's Centers for Independent Living and the governor-appointed Pennsylvania Statewide Independent Living Council.
Payment of Up-Front Costs
Pennsylvania set aside most of the grant to pay for transition expenses. The transition coordinators requested transition expenses, and PATH's program manager had final approval of these expenses. The grant paid for a variety of transition expenses, including security deposits, home modifications, assistive technology, an initial supply of groceries, moving expenses, common household goods, and medical equipment not available through Medicaid. The grant also paid rent for a few participants' community residences when the housing was available before the person could receive services, due to delays in Medicaid HCBS waiver eligibility determination.
PATH and UDS, the program's fiscal intermediary, set up a process to quickly pay for small expenses. Initially, UDS paid all transition expenses directly. State staff reported UDS generally sent a check within 30 days of the program manager's approval. Often, however, providers could not wait 30 days for payment. For example, landlords usually wanted housing deposits on the same day they agreed to a lease. As a result, UDS agreed to deposit some grant funds into a checking account from which the PATH program manager could write checks to providers who need quick payment. The checking account could not be used for expenses over $500.
PATH staff were encouraged to open accounts with local vendors (such as durable medical equipment vendors) so the vendors could directly bill UDS. Using vendor accounts, transition coordinators obtained equipment without waiting for UDS to send a check, even if the cost was more than $500.
Coordinating with Nursing Facilities
Among transition coordinators' first tasks was to meet staff at all nursing homes in their counties. The transition coordinators made subsequent outreach visits to nursing facility discharge planners because PATH program staff learned that some nursing home staff forgot about PATH if they were not in regular contact with the program. PATH staff indicated that the in-person visits enabled the coordinators to work collaboratively with the discharge planners.
Transition coordinators reported working regularly with only one-third of the facilities in the original pilot area. PATH data in October 2002 indicated lack of facility support was a common barrier to transition, and transition coordinators reported several nursing homes have not supported residents who want to transition. Relationships with nursing facilities grew more amicable as the coordinators developed a good reputation among nursing home discharge planners.
Obtaining Housing
Lack of available housing was the most significant barrier to transitioning, according to the PATH program managers, transition coordinators, advocates, and nursing facility staff. People who needed public housing faced waiting lists of several months and difficulty finding an accessible apartment or house. Transition coordinators have had more success finding affordable, accessible housing in rural areas.
In December 2001, the U.S. Department of Housing and Urban Development awarded 50 Section 8 vouchers to four Public Housing Authorities (PHAs) in the original four pilot counties as part of Project Access, which awarded 400 vouchers nationwide that were specifically targeted to former nursing home residents. The vouchers provided PATH consumers an opportunity to obtain housing without joining a waiting list. Staff from the lead PHA, Dauphin County PHA, initially decided to use the vouchers only for PATH consumers. However, the vouchers were available only for people under age 62, while PATH selected this pilot area because it had a high proportion of older nursing facility residents. As of the September 2002, PATH consumers had received seven vouchers, and three of these participants had moved into voucher-funded housing.
Some PATH participants needed home modifications to make housing accessible, and faced two main barriers when pursuing modifications. First, indoor home modifications were more difficult to arrange during the summer, because many area contractors preferred to schedule indoor construction during the colder months when outdoor construction is not feasible. Second, while some of Pennsylvania's Medicaid HCBS waivers paid for home modifications, the waivers required the person live in the home before the modification was complete--which was not feasible for a transitioning consumer. Pennsylvania used PATH funds for a few, limited home modifications so the person could enter and exit the home (e.g., a ramp to the entrance). Then the person could access HCBS waiver funds for other home modifications to enable the person to live more independently.
Obtaining Home and Community-Based Services
As of October 2002, 40 percent of the PATH participants who transitioned--and a majority of Medicaid-eligible consumers--used Medicaid HCBS waivers in the community. The transition coordinators emphasized the importance of starting the waiver application process as soon as possible because the time to determine waiver eligibility could be as long as two months.
Pennsylvania had eleven Medicaid HCBS waivers, but most PATH consumers used one of three waivers. Consumers age 60 or older used the Aging Waiver, administered by AAAs at the local level and the Pennsylvania Department on Aging at the state level. PATH's start coincided with a funding increase for the Aging Waiver, financed by part of the state's tobacco settlement. The new funding allowed Pennsylvania to serve 2,500 additional waiver participants, and the state continued to avoid a waiting list for this waiver.
Consumers under age 60 generally used either the Independence Waiver, which offers a broad array of services (including service coordination, assistance with daily living, respite, home modifications, and specialized equipment and supplies), or the Attendant Care waiver, which offers consumer-directed attendant services. Both waivers serve people with physical disabilities and are administered at the state level by the Department of Public Welfare's Office of Social Programs (OSP). OSP contracts with agencies that administer the waivers at the local level. Most of these agencies are Centers for Independent Living, local chapters of United Cerebral Palsy, or United Disability Services.
Interviewees reported some PATH participants have had difficulty obtaining HCBS waiver eligibility. Each of Pennsylvania's waivers targets people with particular diagnoses, and some consumers with complex needs or multiple diagnoses (e.g., both a physical disability and a mental illness) had difficulty accessing the waivers since they did not meet the criteria for any particular waiver. Coordinators worked with local waiver agencies and other providers, like mental health providers, to provide comprehensive support for consumers. In addition, local waiver agencies have at times denied assistance because they believe they cannot serve a person safely in the community. Transition coordinators assisted some consumers in appealing a local waiver agency's ruling that the person was not eligible for a waiver.
PROGRAM RESULTS
PATH began serving people in November 2001 and ended in September 2003, after two one-year extensions of the one-year federal grant. As of the second week of August, 2003, 39 people had left nursing facilities with support from PATH.
The most recent information available about participants' characteristics was published in the PATH program's first annual report. These data only include the first eleven months of PATH's operation, November 2001 through October 2002. This data only includes the original four pilot counties, since PATH was not operating the in southwest Pennsylvania until 2003.
During this time period, PATH received 90 referrals and transitioned 25 people. Despite PATH's original goal to serve primarily older people, a little more than half (52 percent) of the program's referrals, and of the transitioned consumers, were under age 60. Transitioned consumers were also almost evenly divided between male and female consumers (52 percent female) and between consumers with informal support in the community (56 percent) and those without such support.
As Chart 2 indicates, most consumers transitioned by PATH had physical disabilities that limited their mobility (76 percent). Three of the 25 consumers had no disability (12 percent); they had entered a nursing home for a planned short-term stay paid by Medicare, but were still in the facility. Medicaid paid for their continued nursing home stay after Medicare coverage stopped. PATH program staff are exploring ways to generate a list of people with similar circumstances, because program staff consider these residents good candidates for transition.
| CHART 2. Type of Disability for PATH Transitioned Consumers |
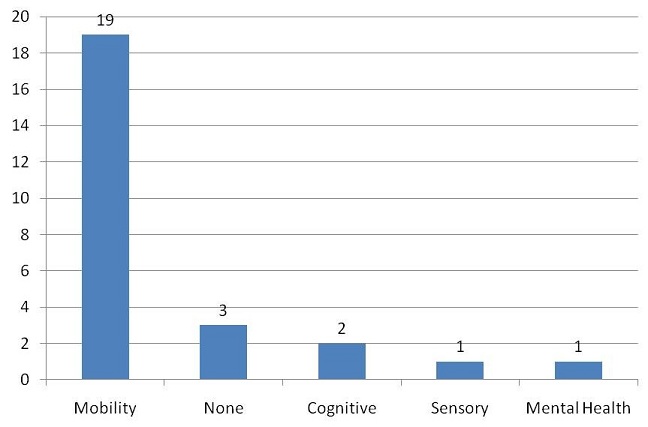 |
| The sum of people in each category is greater than the total number of transitioned consumers because one consumer had more than one type of disability. |
Most PATH consumers (21, or 84 percent) lived in nursing homes between three months and three years. This information is consistent with the program's emphasis on people who would not discharge without assistance, since most nursing home discharges occur within the first three months of admission.5
NEXT STEPS
After the grant ended in September 2003, Pennsylvania provided state funding to continue the pilot program for nine months. It is not certain how Pennsylvania will facilitate nursing home transitions after this nine-month period, which ends in June 2004, other than the long-running program for nursing home residents whose disability manifest before age 22.
INTERVIEWS
Pennsylvania Department on Aging (including independent contractors) Dale Laninga Jennifer Burnett Lynne Miles Amy Townson
Self-Determination Housing Project Diana Myers
Dauphin County Housing Authority Chuck Gassert Mike Weisberg Betsy Rios
Manor Care Harrisburg Simone Sewell
Seton Manor Jennifer Howanitz
Tremont Health and Rehabilitation Center Daniel Daub Linda Uzipis
Four consumers
After the site visit
Pennsylvania Department of Public Welfare Chuck Tyrrell
Pennsylvania Protection and Advocacy Deborah Delgado
Schuylkill County Area Agency on Aging Marie Beauchamp
NOTES
-
In 1998, Colorado, Michigan, Rhode Island, and Texas received grants between $160,000 and $175,000 each. In 1999, New Hampshire, New Jersey, Vermont, and Wisconsin received grants of $500,000 each. In 2000, Arkansas, Florida, Pennsylvania, and Nebraska received grants of $500,000 each.
-
Eiken, Steve and Burwell, Brian. Final Report of the Nursing Home Transition Demonstration Grants Case Study. Medstat: publication pending.
-
Twenty-three states and ten centers for independent living received nursing home transition grants in 2001 and 2002. More information is available at the following Web site: http://www.cms.hhs.gov/systemschange/default.asp.
-
Pennsylvania Intra-Governmental Council on Long Term Care. Pennsylvania Transition to Home: Year One Progress Report. October 2002.
-
Jones, A. "The National Nursing Home Survey: 1999 Summary." National Center for Health Statistics. Vital Health Statistics 13 (152), 2002.
COMPLETE LIST OF SITE VISIT REPORTS
Community Choice: New Jersey's Nursing Home Transition Program
HTML http://aspe.hhs.gov/daltcp/reports/2003/NJtrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2003/NJtrans.pdf
Fast Track and Other Nursing Home Diversion Initiatives: Colorado's Nursing Home Transition Grant
HTML http://aspe.hhs.gov/daltcp/reports/2003/COtrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2003/COtrans.pdf
Michigan's Transitioning Persons from Nursing Homes to Community Living Program
HTML http://aspe.hhs.gov/daltcp/reports/2002/MItrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2002/MItrans.pdf
One-to-One: Vermont's Nursing Home Transition Program
HTML http://aspe.hhs.gov/daltcp/reports/2003/VTtrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2003/VTtrans.pdf
Partnerships for Community Living: Florida's Nursing Home Transition Program
HTML http://aspe.hhs.gov/daltcp/reports/2003/FLtrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2003/FLtrans.pdf
Passages: Arkansas's Nursing Home Transition Program
HTML http://aspe.hhs.gov/daltcp/reports/2003/ARtrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2003/ARtrans.pdf
Pennsylvania Transition to Home (PATH): Pennsylvania's Nursing Home Transition Program
HTML http://aspe.hhs.gov/daltcp/reports/2003/PAtrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2003/PAtrans.pdf
Project CHOICE (Consumers Have Options for Independence in Community Environments): Texas' Nursing Home Transition Program
HTML http://aspe.hhs.gov/daltcp/reports/2003/TXtrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2003/TXtrans.pdf
The Homecoming Project: Wisconsin's Nursing Home Transition Demonstration
HTML http://aspe.hhs.gov/daltcp/reports/2002/WItrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2002/WItrans.pdf
To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human ServicesOffice of Disability, Aging and Long-Term Care PolicyRoom 424E, H.H. Humphrey Building200 Independence Avenue, S.W.Washington, D.C. 20201FAX: 202-401-7733Email: webmaster.DALTCP@hhs.gov
RETURN TO:
Office of Disability, Aging and Long-Term Care Policy (DALTCP) Home [http://aspe.hhs.gov/_/office_specific/daltcp.cfm]Assistant Secretary for Planning and Evaluation (ASPE) Home [http://aspe.hhs.gov]U.S. Department of Health and Human Services Home [http://www.hhs.gov]