
U.S. Department of Health and Human Services
Michigan's Transitioning Persons from Nursing Homes to Community Living Program
Steve Eiken, Brian Burwell and Anthony Asciutto
The MEDSTAT Group
July 31, 2002
PDF Version: http://aspe.hhs.gov/daltcp/reports/2002/MItrans.pdf (26 PDF pages)
This report was prepared under contract #HHS-100-97-0019 between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and The MEDSTAT Group. Additional funding was provided by the Center for Medicare and Medicaid Services. For additional information about the study, you may visit the DALTCP home page at http://aspe.hhs.gov/daltcp/home.htm or contact the ASPE Project Officer, Gavin Kennedy, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, SW, Washington, DC 20201. His e-mail address is: Gavin.Kennedy@hhs.gov.
The opinions expressed in this report are those of the authors and do not necessarily reflect the views of ASPE, CMS or Medstat. The authors gratefully acknowledge the many people in Michigan who generously gave us their time and insights for the preparation of this report.
TABLE OF CONTENTS
- PROGRAM DESCRIPTION
- 1998 Federal Grant
- State Grants
- DEMONSTRATION RESULTS
- 1998 Federal Grant
- State Grants
- BARRIERS TO COMMUNITY TRANSITION AND HOW ADDRESSED
- Housing
- Home and Community-Based Services
- Equipment Access
- DISCUSSION
- Transition Team Manual
- Coordination with Other Organizations
- LIST OF CHARTS
- CHART 1. Community Housing for 2000 Nursing Home Transition Program Consumers
- CHART 2. Source of Long Term Services for 2000 Nursing Home Transition Program Consumers
- CHART 3. Reason CIL Consumers Were Still in a Nursing Home -- Third Quarter 2000
- LIST OF TABLES
- TABLE 1. Centers for Independent Living Funded by Michigan Nursing Home Transition Grant
- TABLE 2. Michigan's Home Help and MI CHOICE Program Characteristics
INTRODUCTION
Across the broad spectrum of public policy, American society is increasing opportunities for persons with all types of disabilities, including people with the physical disabilities and frail older persons, to live lives of their own choosing, in places of their own choosing. Recent policy initiatives in civil rights, health and long term care, income assistance, employment, and housing have a common objective--to create systems of supports and services that allow persons with disabilities, even the most severe impairments, to live independently in accordance with their own choices and decisions. President Bush's New Freedom Initiative provides additional impetus for the continued expansion of community-based supports and services and continued reduction of the nation's reliance on institutional models of care for persons of all ages with disabilities.
Nursing Home Transitions Demonstration
The Centers for Medicare & Medicaid Services (CMS), in association with the Assistant Secretary of Planning and Evaluation (ASPE), sponsored the Nursing Home Transitions Demonstration Program. Under the Demonstration program, CMS and ASPE awarded grants to 12 states between 1998 and 2000 to help nursing home residents move to the community.1 CMS and ASPE selected The MEDSTAT Group to evaluate the Demonstration Program. The evaluation methodology employed is a case study approach, based upon site visits to nine Demonstration states. The case studies will provide useful information to other states as they begin or continue nursing home transition programs, particularly the states that received 2001 and 2002 Systems Change Grants for Community Living from CMS to affect Nursing Facility Transitions.2
Michigan Nursing Home Transition Demonstration
This case study describes the Michigan Nursing Home Transition Demonstration program. It is based on a two-day site visit conducted in January 2001, follow-up interviews in January 2002, and written reports from the State of Michigan and the Michigan Association of Centers for Independent Living (MACIL). The report describes the program under the CMS grant, the program's transition to a state-funded grant, and the program's results. The report then discusses how program staff responded to barriers to successful transition, and how nursing home transition funding continued in Michigan. Observations that may be helpful to other states interested in implementing nursing home transition programs conclude this report.
PROGRAM DESCRIPTION
1998 Federal Grant
The State of Michigan received a $170,000 one-year Nursing Home Transition grant from CMS in September 1998. The grant supported a partnership between the Michigan Department of Community Health (MDCH) and the Michigan Association of Centers for Independent Living (MACIL) to identify and transition people in nursing homes who would be better served in the community. Michigan's goals for the Demonstration were: (1) to help ten people leave nursing homes; (2) to develop tools that could successfully identify transition candidates and facilitate nursing home transitions; and (3) to identify the costs of nursing home transitions in order to inform future transition efforts.
To meet the first goal, MACIL subcontracted with four centers for independent living (CILs) to identify and transition nursing home residents in their service area. MACIL selected CILs with experience in nursing home transition and/or a history of collaboration with local agencies that administer the Medicaid personal care benefit. MACIL used the latter criterion because they expected people to use personal care, as well as other services, after leaving a nursing home. MACIL also selected CILs that reflected a mix of urban, suburban, and rural communities. Table 1 lists the four CILs that received subcontracts under the grant and the cities in which they are located.
Each CIL received $22,500 to pay for staff time devoted to nursing home transitions ($90,000 total). MDCH and MACIL allocated an additional $10,000 (for a total of $100,000) to pay for transition expenses necessary to help a person live in the community for which no other funding source was available--such as apartment deposits, housekeeping supplies, phones, and home modifications.
| TABLE 1. Centers for Independent Living Funded by Michigan Nursing Home Transition Grant | |
| CIL | Location |
| Ann Arbor Center for Independent Living | Ann Arbor |
| Disability Resource Center | Kalamazoo |
| Grand Rapids Center for Independent Living | Grand Rapids |
| Oakland and Macomb Center for Independent Living | Sterling Heights (north of Detroit) |
MACIL employed a Project Manager to develop tools for future transition efforts, gather data on transition costs and benefits, and analyze policy and program barriers to transition. The Project Manager worked with two standing committees: the Project Work Group and the Oversight Committee. The Project Work Group included people directly involved in facilitating transitions from the four CILs funded under the grant, as well as representatives from MDCH, MACIL, and seven other CILs. The Project Work Group developed tools for people that facilitate transitions and provided a forum to share transition strategies. The Oversight Committee included Project Work Group members and representatives from several state agencies and advocacy groups. It analyzed the barriers people face when leaving nursing homes and recommended policy changes and other initiatives to address these barriers. It also recommended future funding for nursing homes transitions.
Identifying Candidates for Nursing Home Transition
In determining whether an individual was a candidate for transition, the Michigan Nursing Home Transition Program used no criteria other than the resident's stated preference. The CILs were philosophically opposed to using any other criteria to determine whether a person should receive help to leave a nursing home, and the state was supportive of that philosophy. One of the tools the Work Group developed was a brief interview to learn whether a resident was interested in transition.
The CILs performed little outreach to find people who wanted to leave nursing homes. CILs expected sufficient referrals to meet the program's goal to transition ten people, since they believed many residents wanted to leave nursing homes. Instead of outreach, CILs focused their efforts on working with the people who came to their attention. Although some CIL representatives reported that the demand for transition assistance exceeded their capacity to provide it, CILs provided at least a limited amount of assistance to all referrals and did not establish a waiting list. Residents' family members were the most common source of referrals. CILs also received referrals from nursing home social workers, nursing home rehabilitation staff, and other sources. Some nursing home residents asked for a CIL representative's assistance after noticing that person working with another resident.
Person-Centered Planning Approach
CILs used a person-centered planning process. CIL representatives worked with each resident to develop a plan based on his or her preferences, strengths, and needs. The process began with an introductory interview to discern each resident's interest in leaving the nursing home. CIL representatives said no person participating in an introductory interview expressed a preference for remaining in the nursing home, although a few residents changed their minds after the introductory interview. To reduce risk of a lawsuit in case a person had a crisis after leaving the nursing home, MACIL recommended CILs ask residents to sign a statement indicating the decision to transition was their own. MACIL was not certain whether all CILs required residents to sign this statement.
If the person was interested in transition, CIL staff conducted a second interview to learn the resident's expectations for community living and to understand the supports the resident would need to ensure safety. CIL staff then scheduled one or more planning meetings with the resident. The meetings often included family members or friends of the resident, according to the resident's preference. During the meetings, the resident and other attendees developed a person-centered plan to prepare for moving to the community.
Transition Assistance
After the planning meeting, CIL staff and the resident implemented the person-centered plan. Transition facilitators often asked residents to perform some activities necessary for transition. For example, some residents called housing agencies and visited apartment buildings to learn about housing options. The facilitators often provided independent living skills training to help the resident adapt to the increased responsibilities of living in the community. This training covered a wide range of skills, including budgeting, using public transportation, and working with personal assistants.
CILs used a variety of government and non-profit sources to obtain housing, equipment, and other supports necessary for the person to live in the community. The CILs worked with the local agencies responsible for Medicaid personal care services and Medicaid home and community-based waiver services to obtain services for the person. CILs also used demonstration funds set aside for transition expenses for housing deposits, furniture, equipment, and other expenses for which no other funding source was available.
While facilitators focused on training residents and obtaining the housing and services necessary for the person to live independently, CIL staff said the ability to consult someone with medical knowledge was also important. Facilitators without a medical background consulted with nurses and occupational therapists connected with the CIL (either as staff or serving on the CIL's board or an advisory council) to learn about the person's medical condition, possible adverse reactions to medications, and ways to overcome barriers to transition related to the person's medical condition.
When a resident left a nursing home, CILs provided continued support. One CIL committed to providing follow-up services for a six-month period after a transition had been made. Other CILs had no formal policies regarding follow-up services, and kept in touch with former residents for shorter or longer periods of time. CIL staff often called and visited transitioned residents during the follow-up period, asked about his or her personal assistants, and checked to see whether the person was participating in social activities to become more integrated in the community. MACIL recommended CILs ask residents to sign a statement acknowledging that the CIL is providing temporary transition assistance and not providing case management for an unlimited period of time. MACIL was not certain that all CILs followed this recommendation.
CILs' Relationships with Nursing Homes
CIL staff reported that the level of cooperation and coordination with nursing homes varied considerably by facility. Cooperation from nursing home staff made transitions easier to facilitate, even though CIL staff did succeed in nursing homes that did not cooperate. CIL staff identified three factors that, in their opinion, indicated nursing homes were more cooperative:
- the nursing home administrator's support for nursing home transition in general,
- a high occupancy rate, and
- a resident who had displayed challenging behavior.
One CIL representative reported that she had established good relationships with about half of the nursing homes in her area. When the program first started, she sent letters explaining the program to both nursing home social workers and Medicaid home and community-based services waiver care managers. In her letter to nursing home social workers, she tried to frame her task in terms of making their jobs easier. This CIL representative found that nursing homes became the source of most of her referrals.
CILs' Relationships with Home and Community-Based Services Programs
One of the keys to the successful transition of a nursing home resident to community living is securing the supports and services necessary for that person to live safely in a community setting.
In Michigan, the two largest publicly funded home and community-based services programs used by people at risk of nursing home admission are: (1) the Michigan Home Help Program, funded under the Medicaid personal care benefit; and (2) MI CHOICE, Michigan's Medicaid home and community-based services waiver for people with disabilities, including older persons.
The Michigan Home Help Program is the larger of the two community-based services program. It served approximately 37,000 people each month in state fiscal year 2000. County Family Independence Agencies (FIAs) set payment rates and approve services for Home Help participants. The Home Help Program uses a consumer-directed, independent provider model; consumers are responsible for hiring, training, and supervising their own provider.
MI CHOICE served over 14,000 people in state fiscal year 2000. It began in 1992 as a pilot program, and has operated statewide since 1998. The local MI CHOICE administrative agencies are called waiver agents. A majority of waiver agents are Area Agencies on Aging, but several for-profit and non-profit organizations are also waiver agents. Unlike Home Help, the waiver does not offer consumer-directed services. Waiver agents have a contract with MDCH to provide waiver services in a region. The waiver agents then contract with provider agencies for direct services, and consumers choose from contracted providers. Table 2 summarizes key characteristics of MI CHOICE and Home Help.
MDCH and CIL staff interviewed for this report considered MI CHOICE more attractive for most people leaving nursing homes. These people stated that people leaving nursing homes are usually more impaired than the average Home Help and MI CHOICE consumer, and can benefit from the additional services and more intensive case management available in MI CHOICE. MI CHOICE offers 13 services while Home Help provides only personal care. FIAs employ Home Help case managers who assess the person's needs and develop a care plan for the person, but these case managers generally have higher caseloads than MI CHOICE case managers do.
| TABLE 2. Michigan's Home Help and MI CHOICE Program Characteristics | ||
| Characteristic | Home Help | MI CHOICE |
| Medicaid payment authority | State plan personal care option | 1915(c) waiver |
| Services |
|
|
| Consumer direction | Required | Not available |
| Local administration | County Family Independence Agency (FIA) | Waiver agent contracted with state. Often an Area Agency on Aging (AAA). |
| Estimated number of consumers in state fiscal year 2000 | 37,000 | 14,000 |
The CILs reported significant variation in their coordination with county FIAs and waiver agents. Some FIAs and waiver agents worked cooperatively with the CILs to help residents return to the community; others were less cooperative. For example, CIL staff reported access to MI CHOICE for people with severe disabilities was limited because waiver agents provided inconsistent information regarding MI CHOICE's cost limits. Local waiver agents were reimbursed for each individual's actual service costs, but were limited to an overall group average of $32 per day. If someone needs 24-hour assistance, the state can approve additional expenses beyond the group average limit. Some waiver agents acted as if the average payment limit was the maximum amount available per person, while others were willing to serve people whose service costs exceeded the average payment limit.
Most of the efforts to increase cooperation with local home and community-based service agencies focused on waiver agents. According to the Project Manager during the federal grant period, this focus was due to: (1) the belief that the waiver was a better option then Home Help for most former residents; and (2) MDCH's contractual relationship with waiver agents, which increased MDCH's ability to influence them. To encourage waiver agents to work with the CILs, MACIL presented the Nursing Home Transition Program at a statewide meeting of waiver agent representatives. In addition, the Project Manager routinely worked with MDCH's waiver contract managers to resolve issues between CILs and waiver agents.
Development of Transition Tools
Based on the CILs' experience, the Work Group developed several tools to help transition facilitators. Because the CILs used person-centered planning, all of the tools emphasize resident control over and responsibility for the transition process. Further, CIL staff emphasized that the resident could skip some recommended activities or add additional activities, depending on the resident's preferences and circumstances.
The CILs used these tools for two years after the federal grant ended, when two state-funded grants paid for transition assistance. The Work Group revised the tools and added to them based on the CILs' additional experience. The tools developed during the federal grant include:
- an interview tool for residents interested in transition to assess preferences;, service support needs, and available resources;
- an interview tool for residents not interested in transition to ensure the residents are making an informed choice (this tool was not used because no residents said they were not interested in transition);
- an overview and explanation of person-centered planning;
- a guide for person-centered planning meeting preparation;
- an outline for the person-centered planning meeting;
- a timeline recommending activities to consider before leaving a nursing home and during the first month after leaving a nursing home; and
- a tool to identify sensitive issues that affect access to community housing or services, like substance abuse history and credit history.
State Grants
MDCH and MACIL decided to continue the program after the federal grant ended in December 1999. MDCH gave MACIL a grant of $236,410 in state general revenue funds to facilitate transitions from January 1, 2000, and December 31, 2000 (Chaney, DeLisle, and O'Hara, 2002). A few months after the first state grant ended, MDCH awarded a $361,892 grant to fund transitions between July 1, 2001, and February 28, 2002. The second grant was one of 48 grants MDCH awarded as part as of an initiative of the state's Long Term Care Work Group, a task force of four state legislators and four MDCH administrators. The initiative used $7.4 million in tobacco settlement funds for one-time funding of projects related to the Work Group's recommendations to improve long-term care services in Michigan.
The state grants continued the program and expanded it to more areas of the state. The CILs also gave presentations to small groups of nursing home residents to increase awareness of community options. For both grants, MACIL allocated funds among 12 of Michigan's 15 CILs, awarding more funds to CILs with a greater capacity to facilitate transitions. For example, during the first state grant, six CILs received less funding because they had to build capacity (e.g., hiring and training transition facilitators) that other CILs had developed. The three newest CILs, which were founded in 1999 and 2000, did not receive transition funding. As in the federal grant, MACIL set aside funds for transition services like housing down payments, housing deposits, and medical equipment. MACIL also continued to support the Project Manager position.
During the state grants, the Work Group refined the transition tools based on the CILs' additional experience with transitions. The Work Group also added a list of issues to consider when facilitating transitions and several planning worksheets to identify issues facilitators may need to address before the resident moves to the community. The Work Group organized worksheets around major life areas like housing, financial matters, and health.
DEMONSTRATION RESULTS
1998 Federal Grant
According to final report of the grant submitted by MDCH (Medical Services Administration, 2000) CILs started the person-centered planning process for 43 nursing home residents during the fifteen-month federal grant period, October 1998 through December 1999. Twelve of the 43 people moved to the community, exceeding the program's goal of 10 people. This number includes people who began the transition process before the grant period, notably in the Ann Arbor area, where the CIL had been facilitating transitions for years with local funding. All the former residents were still living in the community several months later when MDCH's final report for the federal grant was submitted.
Nine of the 12 former residents used Medicaid home and community-based services after transition. Five former residents used the MI CHOICE waiver, three former residents used the Home Help program, and one person used Michigan's waiver for people with developmental disabilities. Of the three people that did not use Medicaid home and community-based services, one person used vocational rehabilitation services; one person required only a scooter, transportation, and informal support from a family member; and one person relied on informal support from people at her church.
DCH and MACIL tracked the staff costs and other direct costs of transitioning individuals to the community. The estimated cost in CIL staff time and other resources for people who left the nursing home, including follow-up, averaged $2,052. Most of this cost was staff time. The CILs only spent one-third of the $10,000 budgeted for transition services; an average of less than $300 per person.
State Grants
As of January 2002, when this report was written, one hundred and fifty-five people had left nursing homes with the help of CIL staff during the two state-funded grants. During both grants, MACIL collected data from the CILs regarding the number of people interviewed for possible transition, consumer demographics, expenditures for each consumer, consumers' status in the transition process (e.g., waiting for housing, transitioned), and the equipment and services consumers used after leaving a nursing home.
At the time this report was written. MACIL had not yet analyzed data about former residents discharged during the second grant. Data analysis is available for the first grant period, the calendar year 2000 (Chaney, DeLisle, and O'Hara, 2002). CIL staff gave 159 presentations to 674 nursing homes residents and their family members. Of these 674 people, CIL staff interviewed 174 residents who expressed interest in transition. Fifty-eight people, one-third of those interviewed, left nursing homes. CIL staff reported one of the 58 people--who had a terminal prognosis--died in the community. CIL staff reported one person returned to a nursing home by choice, citing loneliness, and two people returned to nursing homes due to injury or illness. Both of these persons reportedly planned to move back to the community again.
The age and gender demographics of people who left nursing homes with the CILs' assistance reflect the CILs' traditional focus on younger people with disabilities. While only one of the 12 CILs specifically targeted younger people with disabilities, CIL staff said that most people referred to them were under age 65. Almost three-fourths of the people who left nursing homes were under age 60, while only 8% of all Michigan nursing home residents were under age 65 in 1998, the most recent year in which data is available (Long Term Care Data System, 2000). A majority (59%) of the people who left nursing homes in 2000 were men. This proportion is a little higher than the proportion of men among younger nursing home residents (49%).
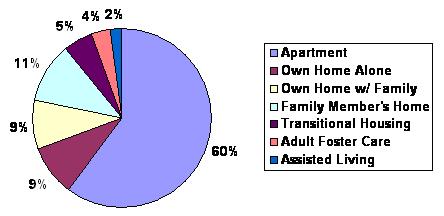
MACIL collected data regarding former residents' housing and home and community-based services for 55 of the 58 former residents who left nursing homes in 2000. As Chart 1 shows, thirty-three former residents (60%) rented apartments, thirty of which were subsidized apartments. Ten people (18%) returned to homes they owned: five of these people lived with family members and five lived alone. Six people (11%) moved into homes owned by family members. The other six people lived in transitional housing, an adult foster care home, or an assisted living facility.
| CHART 1. Community Housing for 2000 Nursing Home Transition Program Consumers |
 |
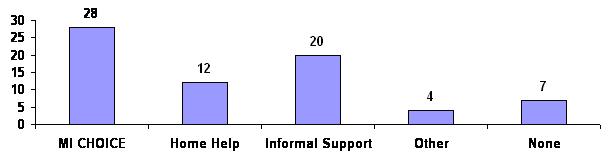
Forty of the 55 (73%) former residents for whom data is available used either the Medicaid waiver for elderly people and people with disabilities (MI CHOICE) or Michigan's personal care benefit (Home Help). More than half (28) of the former residents received services from the MI CHOICE waiver, while 12 received services from the Home Help program (see Chart 2 below). Twenty of the 55 individuals (36%) received help from family and/or friends, sometimes combined with formal services. Seven people (13%) received no assistance from any source after their move.
| CHART 2. Source for Long Term Services for 2000 Nursing Home Transition Program Consumers |
 |
Most former residents used assistive technology in the community, funded by a variety of sources. Medicare, the regular Medicaid state plan, and the MI CHOICE waiver paid for many items, particularly durable medical equipment. Four other frequently used funding sources were the consumers' family and friends, the CILs' loan closets, the U.S. Veterans Administration, and a state-funded assistive technology program called Physical Disability Services.
In the final report for 2000, MACIL combined the reporting of cost data for facilitating nursing home transitions and for CILs' work in preventing nursing home admissions. As a result, MACIL did not calculate the average cost of facilitating nursing home transitions. MACIL did, however, report the amount CILs spend on transition services. During the first state grant, CILs used only half of the $50,000 fund set aside for equipment, household items, housing deposits, and other items for which no other funding source was available. On average, CILs spent $424 per person on these services.
BARRIERS TO COMMUNITY TRANSITION AND HOW ADDRESSED
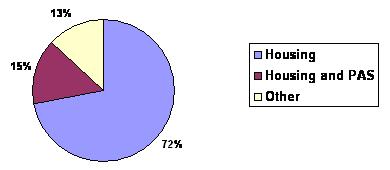
MACIL identified the lack of accessible, affordable housing and a shortage of personal attendant services as the two biggest barriers to moving individuals out of nursing homes and back to community life. After the third quarter of 2000, 32 people were still in the transition process. As shown in Chart 2, 28 of those people (87%) needed only housing and/or personal attendant services to move to the community (Weaver, 2000).
| CHART 3. Reason CIL Consumers |
 |
Housing
CILs reported that people often completed other preparations for living in the community but remained in a nursing home due to a lack of accessible, affordable, safe housing. Many communities had a long waiting list for public housing. The availability of publicly subsidized senior housing complexes made this less of a barrier for people age 60 or older than for younger people with disabilities. Although people could use HUD Section 8 vouchers, the vouchers were difficult to acquire and often not sufficient to pay market rents. Some nursing home residents the CILs served had bad credit histories (sometimes due to unpaid medical bills before the person was eligible for Medicaid), a history of substance abuse, or a criminal history that increased the difficulty in finding private housing.
How addressed: CIL staff identified few means to improve access to housing. Their primary strategy was to help the consumer apply for public housing or a Section 8 voucher as soon as possible. While the consumer was on a waiting list for housing, CIL staff provided other transition assistance to prepare the person for the move. For people with a home that needed a modification to be accessible, Habitat for Humanity and other organizations provided assistance. To increase the supply of affordable, accessible housing, CILs advocated that communities count nursing home residents as homeless people when developing the local housing assessment plans that are required for several federal and state housing funding sources. This advocacy has succeeded in a few communities.
Home and Community-Based Services
Most former nursing home residents required Medicaid long-term care services after transition, usually either personal care (Home Help) or a Medicaid waiver (MI CHOICE). CIL representatives reported a shortage of direct support professionals (e.g., personal care assistants and home health aides) often delayed transition because the former resident had no service provider. The initial difficultly CILs faced in working with some of the local agencies that administer Home Help and MI CHOICE exacerbated the challenge of obtaining services.
Home Help presented a special challenge for people leaving a nursing home because the consumer needed to find his or her own provider. Many consumers used family or friends as Home Help providers. CIL staff report people leaving a nursing home are less likely than people with disabilities in the community to have willing and able family and friends to fill this role. CILs help former residents use Home Help by identifying potential providers and training the person so he or she can act as an employer.
Occasionally, CILs worked with Community Mental Health (CMH) agencies, local agencies responsible for providing publicly funded services for people with mental illness, substance abuse, and developmental disabilities. Five of the 58 people who left nursing homes in 2000 under the Nursing Home Transition Program had developmental disabilities. CIL staff reported some CMH agencies were not willing to provide services to the residents planning a move to the community. For example, twice CMH agencies refused services to someone with cerebral palsy because they did not consider it a developmental disability. One of these denials of service was overturned on appeal after the consumer died. As a result, at least two of people with developmental disabilities used the MI CHOICE waiver, not the waiver for people with developmental disabilities (Chaney, DeLisle, and O'Hara, 2002).
How addressed: Again, MDCH and the CILs identified few means of working around this barrier. One tool MDCH has used is reserving waiver slots for people leaving nursing homes. In recent years, MDCH has had to close the MI CHOICE waiver to new enrollees for a few months near the end of each waiver contract year as the program reached the limit for the number of consumers approved by the legislature. MDCH closed the waiver to new people living in the community first, and reserved the last waiver slots for people leaving nursing homes. MDCH did not close the MI CHOICE waiver to new enrollees from nursing homes until 2001. In that year, MDCH first closed to the waiver to people living in the community, and then had to close the waiver to all new enrollees.
The CILs identified mutual interests in order to improve their relationship with local waiver agents, who administer the MI CHOICE waiver. At the state level, MACIL and the state association of Area Agencies on Aging (the majority of waiver agents are AAAs) often worked together when advocating for changes at the state legislature or at MDCH. The directors of these two organizations shared information about innovative practices or new policies to each other, and then passed this information to local CILs and AAAs. MACIL staff indicated this statewide working relationship contributed to improved local relationships between CILs and AAAs. Also, as the program continued CIL and waiver agent staff better understood each others' challenges, capabilities, and constraints.
For individual consumers with limited access to services, some CILs paid for one or two months of services between a person's move from a nursing home and the time Home Help or MI CHOICE services began. In a few instances, a CIL transition facilitator temporarily provided a former residents' personal care herself.
Equipment Access
Most transitioned residents used some kind of assistive technology in the community, some of which they did not use in the nursing home. CIL staff described the process for securing approval from the Medicaid for durable medical equipment purchases as cumbersome. For example, CIL staff reported waiting several months for a lifeline or for a power wheelchair. They also reported that Medicaid denied payment for some equipment, like a tub bench, that some people in the program needed for successful independent living.
How addressed: In may cases, the program used grant funds to purchase durable medical equipment, rather than seek Medicaid authorization, given the difficulties encountered in getting Medicaid approval. Many of the CILs also maintained their own "equipment closets" which contained various used equipment donated by consumers and staff over the years. Michigan also has a state-funded program to pay for equipment (called Physical Disability Services), but people are not eligible for this program until they leave a nursing home. County FIAs administer this program, but state staff indicated counties vary in the degree they use it. Some counties use it frequently while others use it in limited circumstances or not at all.
NEXT STEPS FOR THE NURSING HOME TRANSITION PROGRAM
In September 2001, CMS awarded MDCH a $770,000 Nursing Facility Transition Grant. A large portion of the grant will address housing, the greatest barrier to transition in Michigan's Nursing Home Transition Program. Under the grant, MDCH will develop programs in four to ten demonstration communities that connect people who want to leave nursing homes--or avoid nursing home admission--to available affordable, accessible housing.
To identify people who need housing, MDCH will use four sources of referrals (1) the CILs; (2) Michigan's Pre-Admission Screening and Annual Resident Review (PASARR) screens of people entering nursing homes, which identifies people with a mental illness or developmental disability; (3) Turner Geriatric Clinic at the University of Michigan, which will receive funds from the federal grant to identify people in hospitals and in the community who are at risk of nursing home admission; and (4) a case management model to be developed by the Michigan State Housing Development Authority (MSHDA) that is also funded by the federal grant. MDCH also plans to hire a contractor to identify people who want to leave nursing homes.
To increase housing options, MDCH awarded a $300,000 grant to the non-profit Corporation for Supportive Housing to establish several community partnerships, in which local home and community-based services agencies, local housing agencies, advocates, and other stakeholders develop comprehensive plans to improve affordable, accessible housing options. This grant expands an initiative between MDCH, MSHDA, and the Corporation for Supportive Housing that established four community partnerships in the late 1990s. A U.S. Department of Housing and Urban Development award of 40 Section 8 vouchers targeted to people leaving nursing homes will further increase housing opportunities for people leaving nursing homes.
One goal of the Michigan demonstration, as with most demonstrations, was to find a mechanism for sustaining the activities of the demonstration after the initial grant period was over. Michigan has not yet identified a permanent source of funding for nursing homes transitions. The second state grant to MACIL ended on February 28, 2002. At the time this report was written, MDCH had not decided whether to provide another grant to fund MACIL's transition efforts.
DCH is considering a more permanent financing mechanism for nursing home transitions. In June 2000, Michigan's Long Term Care Work Group--a task force of four state legislators and four MDCH administrators--recommended significant changes to Michigan's long-term care system. The recommendations include establishing managed long-term care organizations financially responsible for nursing home and home and community-based services. The work group recommended four different managed care models, which MDCH intends to develop and implement. When established, the organizations will have a financial incentive to provide nursing home transition services, since they are responsible for the cost of nursing home services and home and community-based services.
Another option under consideration is to support transition planning under the Medicaid state plan as targeted case management. An important issue concerns what kind of reimbursement methodology to use in supporting these services--either a "cost-based" approach that would pay providers for the amount of time devoted to transitional planning, or a "capitated" approach that would pay providers a fixed amount for each person transitioned, or for each person who was at least identified as a candidate for transition.
Another consideration in developing a permanent program is identifying who would provide the services. While CILs have provided transition assistance under three grants, some CIL representatives expressed concern about the implications of becoming permanent Medicaid providers. These people believed the CILs' fundamental mission is to serve as consumer advocates, and that this mission might be compromised by the requirements of Medicaid participation. On the other hand, some CIL staff believe CILs should accept Medicaid funding for transition assistance. MDCH is considering developing the service in a way that allows other agencies to provide this assistance, including MI CHOICE waiver agents.
DISCUSSION
In summary, over a three-year period, the Michigan Nursing Home Transition Program helped 167 people leave nursing homes and return to community living. Michigan relied on the existing infrastructure of centers for independent living to lead the transition effort. CILs identified potential candidates for transition, and conducted all the planning activities necessary to affect a successful transition of a nursing home resident back to community life.
Two elements of Michigan's experience in the Nursing Home Transition Demonstration Program may be particularly helpful for other states: the transition team manual and the impact of coordination between the CILs and nursing homes and between the CILs and the local agencies that administer publicly funded community-based long-term care services.
Transition Team Manual
Participants in the Michigan demonstration program made a dedicated effort to develop program tools that would lead to a more systematic approach to transition activities. CIL staff then used these tools for almost two years. They continuously updated and revised the tools as they gained more experience with nursing home transitions over the course of the demonstration. These tools may prove to be useful to staff in other states that are implementing transition program. The tools are available on the Internet at http://www.copower.org/pas/nursinghometransition.php.
Coordination with Other Organizations
CIL representatives reported inconsistent relationships with nursing homes and with the local agencies that approve MI CHOICE and Home Help services. One CIL had better relationships with nursing homes, ostensibly because this CIL notified the nursing homes before starting the program and framed the program in terms of nursing home social workers' interests. CILs steadily improved their relationship with waiver agents by finding common interests in other areas of long-term care. Organizations involved in future transition programs may want to develop relationships with nursing homes and home and community-based services agencies before they start facilitating transitions, in order to increase their programs' initial success.
BIBLIOGRAPHY
Burwell, Brian "Medicaid Long Term Care Expenditures in FY 2000". May 2001.
Chaney, Roanne; DeLisle, Norm; and O'Hara, Liz. "Accessing Community-Based Long Term Care: Sustaining the Initiative". Final Report submitted to the Michigan Department of Community Health. January, 2002.
Long-term Care Data System, Division for Vital Records and Health Statistics, Michigan Department of Community Health. "Patient Census at End of Reporting Period Michigan Nursing Care Facilities, 1996-1998". Available on the Internet at http://www.mdmh.state.mi.us/pha/osr/ltc/census.asp. Last updated August 1, 2000.
Medical Services Administration, Michigan Department of Community Health. "Transitioning Persons from Nursing Homes to Community Living: Lessons from a Pilot Project". Final Report submitted to the U.S. Health Care Financing Administration, 2000.
Weaver, Ellen. "Transitioning Individuals from Nursing Homes to Community: Sustaining the Initiative". Quarterly Report for July 1-September 30, 2000 submitted to Michigan Medical Services Administration, November 2000.
MEETING ATTENDEES
MEDSTAT Tony Asciutto Brian Burwell Steve Eiken
Michigan Association of Centers for Independent Living (MACIL) and Partners RoAnne Chaney, Michigan Disability Rights Coalition Mona Kalid, The Disability Resource Center Marsha Moers, Capitol Area Center for Independent Living Elizabeth O'Hara, MACIL Kim Sherwood, Ann Arbor Center for Independent Living Ellen Weaver, MACIL
Michigan Department of Community Health Michael Daeschlein, Long-Term Care Initiative Brenda Fink, Long-Term Care Initiative Mary Gear, Long-Term Care Initiative
NOTES
-
In 1998, Colorado, Michigan, Rhode Island and Texas were awarded grants of between $160,000 and $175,000 each. In 1999, New Hampshire, New Jersey, Vermont, and Wisconsin received grants of $500,000 each. In 2000, Arkansas, Florida, Pennsylvania and Nebraska received grants of $500,000 each.
-
For more information on the Systems Change Grants for Community Living, see the following website: http://www.hcfa.gov/medicaid/systemschange.htm.
COMPLETE LIST OF SITE VISIT REPORTS
- Community Choice: New Jersey's Nursing Home Transition Program
- HTML http://aspe.hhs.gov/daltcp/reports/2003/NJtrans.htm
- PDF http://aspe.hhs.gov/daltcp/reports/2003/NJtrans.pdf
- Fast Track and Other Nursing Home Diversion Initiatives: Colorado's Nursing Home Transition Grant
- HTML http://aspe.hhs.gov/daltcp/reports/2003/COtrans.htm
- PDF http://aspe.hhs.gov/daltcp/reports/2003/COtrans.pdf
- Michigan's Transitioning Persons from Nursing Homes to Community Living Program
- HTML http://aspe.hhs.gov/daltcp/reports/2002/MItrans.htm
- PDF http://aspe.hhs.gov/daltcp/reports/2002/MItrans.pdf
- One-to-One: Vermont's Nursing Home Transition Program
- HTML http://aspe.hhs.gov/daltcp/reports/2003/VTtrans.htm
- PDF http://aspe.hhs.gov/daltcp/reports/2003/VTtrans.pdf
- Partnerships for Community Living: Florida's Nursing Home Transition Program
- HTML http://aspe.hhs.gov/daltcp/reports/2003/FLtrans.htm
- PDF http://aspe.hhs.gov/daltcp/reports/2003/FLtrans.pdf
- Passages: Arkansas's Nursing Home Transition Program
- HTML http://aspe.hhs.gov/daltcp/reports/2003/ARtrans.htm
- PDF http://aspe.hhs.gov/daltcp/reports/2003/ARtrans.pdf
- Pennsylvania Transition to Home (PATH): Pennsylvania's Nursing Home Transition Program
- HTML http://aspe.hhs.gov/daltcp/reports/2003/PAtrans.htm
- PDF http://aspe.hhs.gov/daltcp/reports/2003/PAtrans.pdf
- Project CHOICE (Consumers Have Options for Independence in Community Environments): Texas' Nursing Home Transition Program
- HTML http://aspe.hhs.gov/daltcp/reports/2003/TXtrans.htm
- PDF http://aspe.hhs.gov/daltcp/reports/2003/TXtrans.pdf
- The Homecoming Project: Wisconsin's Nursing Home Transition Demonstration
- HTML http://aspe.hhs.gov/daltcp/reports/2002/WItrans.htm
- PDF http://aspe.hhs.gov/daltcp/reports/2002/WItrans.pdf
To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human ServicesOffice of Disability, Aging and Long-Term Care PolicyRoom 424E, H.H. Humphrey Building200 Independence Avenue, S.W.Washington, D.C. 20201FAX: 202-401-7733Email: webmaster.DALTCP@hhs.gov
RETURN TO:
Office of Disability, Aging and Long-Term Care Policy (DALTCP) Home [http://aspe.hhs.gov/_/office_specific/daltcp.cfm]Assistant Secretary for Planning and Evaluation (ASPE) Home [http://aspe.hhs.gov]U.S. Department of Health and Human Services Home [http://www.hhs.gov]