
U.S. Department of Health and Human Services
Community Choice: New Jersey's Nursing Home Transition Program
Steve Eiken
MEDSTAT
December 22, 2003
http://aspe.hhs.gov/daltcp/reports/2003/NJtrans.pdf (26 PDF pages)
This report was prepared under contract #HHS-100-97-0019 between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and The MEDSTAT Group. Additional funding was provided by the HHS Centers for Medicare and Medicaid Services. For additional information about the study, you may visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, Gavin Kennedy, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, SW, Washington, DC 20201. His e-mail address is: Gavin.Kennedy@hhs.gov.
The opinions expressed in this report are those of the authors and do not necessarily reflect the views of ASPE, CMS or Medstat. The authors gratefully acknowledge the many people in New Jersey who generously gave us their time and insights for the preparation of this report.
TABLE OF CONTENTS
Transition Coordination
Payment of Up-Front Costs
Identifying Program Participants
Coordinating with Nursing Homes
Obtaining Housing
Obtaining Home and Community-Based Services
Project Specialists
Assistive Technology Fund
Other Grant Expenditures
COMMUNITY CHOICE PROGRAM RESULTS
LIST OF CHARTS
CHART 1. Distribution of 2000 Nursing Home Transition Grant Expenses
CHART 2. Community Choice Consumers Approximate Average Nursing Home Length of Stay
LIST OF TABLES
TABLE 1. Community Choice Marketing Materials
INTRODUCTION
The Centers for Medicare & Medicaid Services (CMS), in association with Office of the Assistant Secretary for Planning and Evaluation (ASPE), sponsored the Nursing Home Transition Demonstration Program to assist states in providing transition options to nursing home residents who wish to move back to the community. CMS and ASPE awarded grants to 12 states between 1998 and 2000.1
The Demonstration permitted states to use grant funds for virtually any direct service or administrative item that held promise for assisting nursing home residents' return to the community. The grants provided targeted administrative or service resources to achieve the following objectives:
- To enhance opportunities for nursing home residents to move into the community by identifying nursing home residents who wish to return to the community and educating them and their families about available alternatives;
- To overcome the resistance and the barriers that may be in the way of their exercising this choice; and
- To develop the necessary infrastructure and supports in the community to permit former nursing home residents to live safely and with dignity in their own homes and communities.
This report is one of a series of nine case studies presenting results from the Demonstration. The case studies, along with a final report summarizing results from all these states,2 provide useful information as states consider nursing home transition efforts or implement nursing home transition programs. Lessons the demonstration states learned during this program are particularly important because CMS awarded a number of Nursing Home Transition grants in 2001 and 2002 under the Systems Change Grants initiative.3
The report describes New Jersey's nursing home transition program, called Community Choice. Community Choice is one of the first permanent, publicly funded nursing home transition programs in the United States. In addition to describing Community Choice as a whole, this case study describes how New Jersey improved Community Choice using a federal Nursing Home Transitions Demonstration grant.
During a December 2001 site visit, Medstat interviewed current and former program staff, including state administrators and staff at two of the eight local offices that administer the program. Medstat staff also interviewed three consumers who left nursing homes with the help of Community Choice and one consumer who left a nursing home one month after the site visit. The Community Choice Web site, several unpublished reports from the state, and three reports about Community Choice by Rutgers University's Center for State Health Policy also informed this case study.4
This case study report focuses on three common components of nursing home transition programs:
- transition coordination or case management to help consumers access housing and services in the community;
- a fund to pay for the up-front costs consumers may incur as they leave a nursing home, such as a security deposit for an apartment; and
- a method to identify nursing home residents interested in transition.
The report also describes how three challenges common among nursing home transition programs--coordinating with nursing homes, obtaining community housing, and obtaining home and community-based services--affected Community Choice, and how state and local program staff addressed these challenges. After a brief description of efforts to improve Community Choice using the federal grant, the report presents data on the program's results and discusses New Jersey's efforts since the grant period to support nursing facility residents interested in transition.
PROGRAM DESCRIPTION
Community Choice, which began serving people in March 1998, is a statewide program that provides nursing home residents with (1) information about home and community-based service and housing alternatives and (2) assistance to those who want to move out of a nursing home. New Jersey's Department of Health and Senior Services (DHSS) employs registered nurses and social workers, called Community Choice counselors, to provide information and assistance to nursing home residents. The counselors are based at New Jersey's eight Long Term Care Field Offices throughout the state, but are supervised by a program manager in the DHSS Central Office.
Before Community Choice, nursing home transition was one of the functions of the state's pre-admission screening (PAS). New Jersey requires PAS for Medicaid consumers and people who would be eligible for Medicaid if they lived in a nursing home for 180 days. Interviewees said resources for nursing home transition services were limited, few community alternatives were available, and PAS staff did not always know all the options available in the community. As a result, many people approved for short-term stays remained in nursing facilities for months or years.
Transition Coordination
The Community Choice counselors are based in New Jersey's eight Long Term Care Field Offices; the same offices where PAS staff are located. PAS staff still assess people before a nursing home admission, but now a team of counselors dedicated to nursing home transition works with residents who want to live in the community. Both program administrators and counselors said that creating this team was important for the program's success. New Jersey initially hired a team of ten counselors, and each was assigned two nursing homes. At the time, counselors were not available outside the 20 assigned nursing homes. In 1999, New Jersey made Community Choice available statewide and hired additional counselors. Since then, the program has employed between 30 and 40 counselors.
Community Choice counselors receive many referrals from PAS staff and also receive referrals from nursing home staff, residents, family members, and others (see Identifying Program Participants). Upon receiving a referral, a counselor's first step is to determine financial eligibility for Community Choice and to assess the resident's long-term support needs. During the assessment, the counselor reviews the resident's chart and pre-admission screening report, interviews nursing home staff--especially the discharge planner and therapists--and then interviews the resident. If the resident is eligible for Community Choice and interested in transition, the counselor will give the resident a business card, and, if the resident permits, interview the person's family.
Counselors said they see their role as assisting the nursing home discharge planners who develop a resident's discharge plan, which includes identifying available housing and services. Sometimes the discharge planner does most of the work; sometimes the counselor has a greater role. If the discharge planner does not believe the person will be safe in the community, the counselor first attempts to persuade the discharge planner that community living is a viable alternative. If the nursing home discharge planner is not persuaded, the counselor can, and does, still work with the consumer toward transition. Program staff stressed that the decision on whether or not to leave a nursing home belongs to the resident and not to the facility.
After a resident's discharge to the community, counselors must make at least two follow-up contacts to ensure the person has the support he or she needs. Community Choice policy requires counselors to call the former resident 24 to 48 hours after discharge, and to call again between 14 and 30 days after discharge. Only a phone call is required, although some counselors said they visited the person's new home because they could learn more about a person's needs during an in-person visit.
Community Choice counselors are not responsible for follow-up more than one month after transition. After the second contact, the person is encouraged to call New Jersey Easy Access, Single Entry (NJ EASE), a statewide 1-800 information and referral system operated by Area Agencies on Aging, or to contact his or her waiver case manager if he or she is receiving services from a Medicaid HCBS waiver. A few counselors said they believed additional follow-up case management by the counselors would help some consumers with complex needs because these consumers needed intensive case management and the waiver and NJ EASE case managers usually had much higher caseloads than the counselors.
To prepare counselors, DHSS provided extensive staff training during the first six months of Community Choice. Every two weeks, all the counselors attended full-day staff meetings that focused on training. The training informed counselors about Medicaid services, state-funded HCBS, Older Americans Act services, and public and private housing options. Since counselors use the assessment tool used in pre-admission screenings, counselors also observed the pre-admission screening process. DHSS provides ongoing counselor training as well, including training sessions based on issues raised by individual counselors, such as working with nursing home staff.
Payment of Up-Front Costs
To support a person's transition, New Jersey offers up to $600 per person for transition expenses. New Jersey uses state funds to pay for housing deposits, furniture, appliances, other household items, and other expenses necessary to support the consumer in the community. Counselors recommend expenditures to Community Choice staff at the DHSS Central Office, who then must approve the expenditures. A person may receive more than the $600 per-person limit under special circumstances if approved by the Central Office. Most Community Choice participants do not use this funding for transition services, but counselors reported the funds are very important for the people who need them. People who have been in nursing homes more than a few months are reportedly more likely to need help with transition expenses.
Program staff reported people often need assistive technology (AT) when leaving a nursing home, and that this technology often costs more than the $500 per item limit on what New Jersey can purchase without competitive bidding. In the fall of 2001, New Jersey used part of its Nursing Home Transition Demonstration Grant to establish a fund for prompt payment of AT costing more than $500. The state gave $172,000 in grant funds to the Assistive Technology Advocacy Center (ATAC), the National Institute on Disability and Rehabilitation Research's State Technology Assistance Program for New Jersey, to pay for evaluation and purchase of AT not covered by Medicaid. ATAC is part of a private non-profit organization and does not have to follow the competitive bidding process required of state agencies. As of the end of 2002, one consumer had used the fund, which is a fund of last resort.
Identifying Program Participants
Community Choice is available to Medicaid beneficiaries and people who would be eligible for Medicaid within 180 days if they remain in a nursing home, the same people for whom the state requires pre-admission screening. New Jersey does not restrict eligibility for Community Choice based on the severity of a person's disability, but counselors reported that a person who needs assistance or supervision at all times cannot transition unless an informal caregiver is available.
The state established a process for counselors to learn about nursing facility residents soon after their admission. When a person meeting the Community Choice eligibility requirement enters a nursing facility, state regulations require the nursing facility to notify the local Long Term Care Field Office. At the field office, the person is assigned to the counselor serving that nursing facility's residents. The program also receives referrals from Area Agencies on Aging (AAAs), nursing facility staff, the nursing facility ombudsman, residents, and residents' families.
The program initially focused on people recently admitted to a nursing facility. One reported benefit of concentrating on these admissions was to build the counselors' confidence by allowing them to work with residents who needed less assistance. Program staff and consumers reported that it is more difficult to transition people who have spent several months or years in a nursing home. New nursing facility residents are more likely to have a home in the community, and many of these residents already plan to leave the facility after a few weeks of rehabilitation or convalescence. By initially working with more people with short-term stays, counselors gained experience in working with nursing facility discharge planners and connecting consumers to HCBS, housing, and other resources. Although Community Choice still works with many residents soon after their admission, counselors serve residents referred to them regardless of length of stay.
Coordinating with Nursing Homes
Senior state staff reported that they worked with nursing homes during program implementation to encourage cooperation, and emphasized to the nursing homes that the purpose of Community Choice was to give people options, not to empty facilities. Nursing homes reportedly did not strongly oppose the program because it was hard to visibly oppose a voluntary program. In fact, nursing homes referred several people to Community Choice.
Program staff, and some consumers, said nursing homes were often valuable allies in helping someone transition. Counselors reported that some discharge planners use them as a resource to make their jobs easier and that some nursing home staff--including physical therapists, discharge planners, certified nursing assistants, and nurses--were motivated to provide referrals and work with counselors after seeing one or two successful transitions. Some consumers said facilities assisted their transition by encouraging them to perform their activities of daily living more independently. For example, staff would stand by while a resident transferred himself from his bed to his wheelchair and assist if necessary, rather than transfer the resident.
Program staff and consumers also reported that some nursing homes opposed transitions. For example, early on in the program several nursing homes reportedly delayed notifying the Long Term Care Field Office of new admissions for as long as two months. This delay made transition for more difficult. Counselors reported resistance from nursing homes has decreased as the program has continued, in part due to presentations about the program made to nursing home staff under the federal grant.
To provide nursing homes a reason to cooperate with counselors, New Jersey gave Community Choice counselors some of the Pre-Admissions Screening (PAS) duties. If a person becomes eligible for PAS after entering a nursing home (e.g., spends enough resources to be Medicaid-eligible within six months), Community Choice counselors now perform the screening. In a focus group of counselors held by Rutgers University's Center for State Health Policy, counselors indicated their role in PAS is one factor that improved their working relationships with nursing homes. At the same time, counselors in that group said that PAS screening decreased the time spent with residents preparing for transition.
Obtaining Housing
One of the most difficult challenges for Community Choice participants is finding affordable, accessible housing. Most subsidized senior housing units have waiting lists, and people often wait as long as two years to obtain housing. Program staff and one consumer indicated people under age 65 have more difficultly locating housing because there are fewer subsidized apartment buildings for younger people with disabilities. Interviewees also said people under age 65 are less likely to choose assisted living, preferring their own apartments.
Community Choice took several steps to increase housing access, including improving communication and coordination with housing providers at both the state and local level. At the state level, the state housing agency (a division of the Department of Community Affairs) notifies Community Choice staff if it learns about particular properties with openings. At the local level, counselors have convinced some individual apartment managers to notify them when apartments become available. Also, new counselors visit local subsidized apartment buildings for older people and assisted living facilities as part of their training. These visits allow counselors to introduce themselves and increase awareness of Community Choice, while at the same time increasing counselors' knowledge of local housing options.
To further inform counselors about housing, the state used federal grant funds to pay for training by the Supportive Housing Association of New Jersey, a provider association that advocates supportive housing. The training was already standard training for supportive housing providers, and counselors attended to network with these providers as well as to learn more about affordable, accessible housing options. Two or three counselors from each of the eight Long Term Care Field Offices attended the training, and these counselors shared their knowledge with their colleagues.
Obtaining Home and Community-Based Services
Community Choice consumers vary widely in the level of assistance they need after discharge. Many consumers use in-home and residential services available through Medicaid home and community-based services (HCBS) waivers and a state-funded in-home services program. Another option is services from Area Agencies on Aging (AAAs), including case management, paid by the federal Older Americans Act. Some former residents--including one consumer interviewed for this report--do not need paid long-term support after discharge. New counselors meet local waiver and AAA case managers during their training to increase awareness of Community Choice and to begin building good working relationships with case managers.
In the late 1990s, when Community Choice started and later expanded, New Jersey launched several other initiatives to increase home and community-based services options for older people and improve service coordination. These new initiatives included:
- The Enhanced Community Options waiver (ECO), a new Medicaid HCBS waiver for older people and people with physical disabilities that for the first time covered community residential options in the state and made self-directed services available for older people;
- Jersey Assistance for Community Caregiving (JACC), a state-funded in-home services program; and
- New Jersey Easy Access Single Entry (NJ EASE), a statewide toll-free phone number that provides older people a single contact point for a variety of health services, social services, financial information, and other resources.
The new HCBS options served an average of 1,000 people in State Fiscal Year 2001 and significantly reduced the waiting list for the Community Care Program for the Elderly and Disabled (CCPED), New Jersey's first waiver for older people and people with physical disabilities. Program staff reported that the increase in HCBS options contributed to Community Choice's ability to serve a large number of people.
Even with the increase in available options and the ability to serve more people in the community, many consumers experienced difficulty obtaining HCBS. Like many states, New Jersey has a shortage of direct support workers. Counselors reported that it was particularly hard to find workers and home-delivered meal services in rural areas.
Counselors also reported difficulty coordinating services with HCBS case managers, although they said this coordination usually worked well. For example, sometimes counselors recommended a consumer receive case management from an AAA, while the AAA believed case management was unnecessary. Counselors also said many Medicaid HCBS waiver case managers initially were unwilling to conduct a waiver functional eligibility assessment until the person left a nursing home, although waiver case managers are now working with them before a resident's discharge. Waiver case managers were initially unable to bill Medicaid for case management before the person left a nursing home. This changed in 2000 when the state took advantage of new federal flexibility to fund Medicaid HCBS waiver case management during the last six months of a nursing home stay if the person enrolls in the waiver upon discharge.
DEMONSTRATION GRANT
New Jersey received a $500,000 federal Nursing Home Transition Demonstration Grant in September 1999, one-and-a-half years after Community Choice began. The grant ended in March 2001, after New Jersey received a six-month no-cost extension. The state used the grant to improve the program's infrastructure by hiring three project specialists to improve three aspects of the program: marketing, quality of services after discharge, and addressing barriers to transition. The state also created the assistive technology fund specifically for people leaving nursing homes, hired a consultant to support project management later in the grant period, and used a small portion of the grant to pay for staff training on housing options.
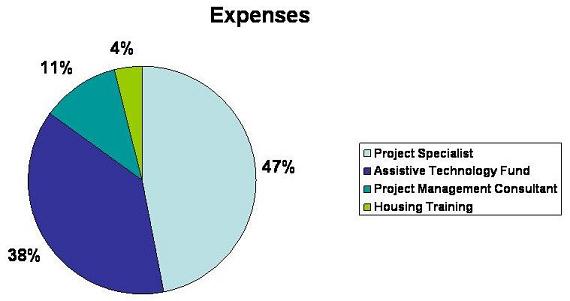
Chart 1 shows the distribution of grant funds. Overall, New Jersey spent a little over 90 percent of the grant ($454,509 of $500,000). The state spent nearly half the money, or $214,432, on project specialists' salaries and on expenses related to their work. This included $29,301 for printing marketing materials and manuals and $24,153 in audiovisual equipment to videotape training presentations so they are available for new staff at the field offices. New Jersey used over one-third of the grant, or $172,077, to start the assistive technology fund. The grant also paid $50,000 for the project management consultant, and $18,000 for Community Choice counselors to attend the housing training provided by the Supportive Housing Association of New Jersey.
| CHART 1. Distribution of 2000 Nursing Home Transition Grant |
 |
Project Specialists
Each specialist was responsible for improving a particular aspect of Community Choice. DHSS created permanent positions for two of the three specialists to continue improving the program. These positions are now vacant because the specialists accepted jobs elsewhere in DHSS and the state currently has a hiring freeze.
Identifying and Addressing Barriers
The project specialist charged with identifying and addressing barriers to transition first prepared a report that identified barriers to transition and recommended remedies. The specialist worked with an advisory committee of counselors to create this report, and also met with staff at the Long Term Care Field Offices and reviewed state policies that affect transition. A summary of the report was sent to the DHSS senior management with oversight over Community Choice.
Most barriers required legislative changes and were outside DHSS' control, so Community Choice staff focused on doing what was under their control. In particular, they focused on two barriers: resistance from nursing facility staff and incomplete awareness of alternatives to nursing facilities among many health care professionals. To address these barriers, the project specialist developed a PowerPoint presentation for nursing home staff that explained Community Choice and New Jersey's home and community-based service options.
The presentation addressed specific concerns that nursing home staff had expressed. For example, the presentation explained that counselors were there to assist nursing facility discharge planners, not to replace them. The presentation also assured nursing facility staff that the counselors were not making reports on the facility for licensing penalties, nor were they forcing residents to leave.
Counselors made presentations in every facility, and invited as many nursing facility staff as possible to attend. DHSS gave counselors the flexibility to add to the presentation. Depending on the counselor and the audience, the presentations were between 30 minutes and 2 hours long. Counselors reported the presentations improved working relationships between nursing facilities and Community Choice staff. Counselors noted that the explanation of the counselor's and the nursing facility discharge planner's roles in the transition process was particularly useful. Counselors also said discharge planners and administrators were particularly interested in learning about the states' Medicaid waivers.
The project specialist subsequently adapted the presentation for other audiences in order to increase awareness of Community Choice, to encourage referrals, and/or to encourage cooperation with counselors. These other audiences included:
- Hospital discharge planners;
- County Boards of Social Service staff who determine financial eligibility for Medicaid;
- Physicians; and
- Social workers.
Quality Assurance
The project specialist charged with improving quality found confusion among counselors regarding standard procedures and how to complete paperwork. For example, Medicaid waiver case managers said they often did not receive all the information they needed when a counselor referred someone to the waiver. As a result, the project specialist focused on standardizing procedures.
The project specialist worked closely with a small work group of counselors and Long Term Care Field Office managers to develop a policy and procedure manual for Community Choice. The work group included Long Term Care Field Office managers because the manual needed to clarify the interactions between counselors and PAS staff, which these managers supervise. A larger policy advisory group of counselors and Field Office Managers now meets quarterly to discuss possible changes to policies and procedures.
Interviewees reported the establishment and dissemination of standard processes reduced confusion among counselors. As a result, staff meetings became more focused on how to meet consumers' needs than how to correctly complete paperwork. Community Choice also developed a standard measure of counselors' caseloads and activities, so program managers can better distribute the program's workload. Counselors expressed satisfaction with the manual, according to a summary of counselors' comments on the manual.
After the manual was complete, the project specialist performed three audits at the Long Term Care Field Offices to ensure that counselors were following the standard procedures. To provide feedback, the project specialist sent each counselor the audit's results for the records he or she completed in addition to reporting statewide and Field Office results. The project specialist found staff became more consistent with standard procedures as the program continued.
The project specialist also developed a policy and procedure manual for administrative staff at the Long Term Care Field Offices. The manual sets standards for what data needs to be collected during intake for Community Choice and Pre-Admission Screening. The manual also includes human resources policies, and instructions on computer system usage and file maintenance.
Marketing
The third project specialist was responsible for increasing awareness of Community Choice in the general community and for developing program materials for consumers, families, providers, and the general public. The project specialist developed a variety of paper materials and a Community Choice Web site (http://www.state.nj.us/health/consumer/choice/index.shtml). She also prepared information about Community Choice and other HCBS initiatives that the Governor mentioned in a weekly radio address.
Table 1 describes the written material created to increase awareness about Community Choice. Most of the materials are available on the Community Choice Web site at http://www.state.nj.us/health/consumer/choice/publications.shtml.
| TABLE 1. Community Choice Marketing Materials | ||
| Product | Audience | Content |
| Fact Sheet | General Public | Describes Community Choice in one page. |
| Brochure | Consumers and Families | Describes Community Choice. Counselors show to consumers and families to explain program. |
| Large Print Brochure | Consumers | Describes Community Choice. Counselors show to consumers with vision impairments to explain program. Brochure also uses simpler language. |
| Booklet | Consumers and Families | Counselors use with a brochure to provide information about HCBS options. |
| Tri-fold booklet | DHSS LTC Field Offices, Nursing Facilities, Area Agencies on Aging | More in-depth information about HCBS options. |
The project specialist worked closely with an advisory committee of counselors when developing these products. The advisory committee counselors circulated a first draft of each product to colleagues, nursing facility staff, assisted living providers, and a focus group of families in order to get feedback. To record the feedback, counselors used a small survey (five to six questions) the project specialist developed. The project specialist also led consumer focus groups in adult day centers for additional feedback and suggestions. Other than the fact sheet, all the written materials required final approval from the DHSS Office of Communications.
The process for developing the Web site was similar to the development process for printed materials. The site describes how Community Choice works and how Community Choice and other state programs can assist nursing home residents who want to move into the community and community residents who want to stay in their own homes. The Web site also contains a provider information page, online versions of marketing materials, and an e-mail address where people can send questions. In 2001, the Web site averaged 1000 hits per month and program staff received e-mails from families across the U.S. who had relatives in New Jersey and who used the Web site.
Assistive Technology Fund
New Jersey used the federal grant to establish a fund that allows for prompt payment of assistive technology that costs more than $500. This fund is described above. (See Payment of Up-front Costs.)
Other Grant Expenditures
New Jersey used the remaining grant funds for consultant services and staff training. It paid $50,000 in grant funds for consultant services to support overall management of Community Choice, which allowed the original project director to support the program on a part-time basis after her retirement from DHSS. The state also used $18,000 to pay for previously mentioned training by the Supportive Housing Association of New Jersey (See Obtaining Housing).
COMMUNITY CHOICE PROGRAM RESULTS
More than 3,400 people left nursing homes with the help of Community Choice counseling between State Fiscal Years (SFY) 1998 and 2001. During SFY 2000 and 2001, Community Choice assisted an average of 1,500 former nursing home residents each year. Community Choice and other initiatives to serve older people in the community contributed to reduced Medicaid nursing home utilization between 1998 and 2001. The number of Medicaid nursing home residents decreased by 1,600: from 29,610 in SFY 1998 to 28,028 in SFY 2001.
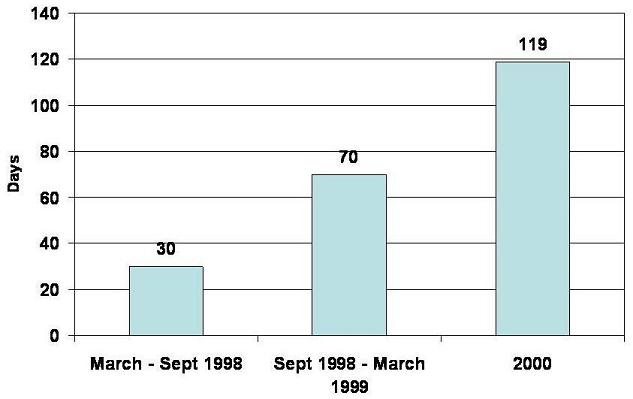
Available data on Community Choice consumers' nursing home lengths of stay reflect the program's initial emphasis on short-term admissions. As Chart 2 illustrates, Community Choice consumers' average nursing home length of stay has increased as the program has continued. Program staff reported the average length of stay was approximately 30 days in the program's first six months. Six months later, the average length of stay had increased to approximately 70 days. The average length of stay further increased to 119 days for people discharged during calendar year 2000.
| CHART 2. Community Choice Consumers Approximate Average Nursing Home Length of Stay |
 |
Unlike other nursing home transition demonstration programs, most Community Choice consumers are over 60 years old. Between July 2000 and February 2001, eighty-two percent of Community Choice consumers were age 61 or older. Nearly two-fifths (39 percent) of consumers were age 81 or older, including two people over 100. Program staff reported serving an increasing number of people under age 60, including people with mental illness and developmental disabilities. However, information about Community Choice consumers' diagnoses is not available.
New Jersey contracted with the Rutgers University Center for State Health Policy (CSHP) to evaluate Community Choice. CSHP surveyed former Community Choice consumers discharged throughout 2000 approximately six to eight weeks after discharge. CSHP attempted to interview all 1,975 consumers who left nursing homes, but was only able to interview 859 people. 211 (11 percent) of these consumers had deceased. CSHP was not able to locate an additional 560 people, and other people either refused to participate or were not able to participate and had no proxy available. A little over half of the respondents were proxies: friends or family members responding on former residents' behalf.
For most of the respondents, the consumer still lived at home and was satisfied with his or her living arrangement. Most consumers (77 percent) lived in an apartment, their own home, or someone else's home. Four percent of consumers lived in nursing homes, and another 17 percent lived in assisted living, boarding homes, or other community residential settings. Almost half (47 percent) of home-based consumers lived with a spouse or child, and another 14 percent lived with other people such as friends, other relatives, and paid caregivers. Regardless of their current living arrangement, six out of seven respondents (86 percent) reported satisfaction with the person's living situation, while 7 percent said they were somewhat satisfied and 7 percent reported they were dissatisfied.
While respondents in all settings expressed satisfaction with the consumer's living arrangement, former residents in facilities and their proxies reported a higher quality of life. More than two-thirds (68 percent) of respondents in houses and apartments said the consumer enjoyed life, compared to 81 percent of people in facilities. Facility-based consumers also were more likely to report visiting with friends or family. Poor health was the most commonly reported reason for not enjoying life.
Some respondents reported few functional limitations. More than half of the consumers were able to perform all five Activities of Daily Living (ADLs) measured in the survey. On average, consumers could perform four ADLs and four of the nine Instrumental Activities of Daily Living (IADLs) measured in the survey. One-third of respondents reported an unmet need, in terms of assistance with an ADL or IADL, assistance to avoid injury, or help to continue living where they were. Former residents in houses or apartments were more likely to have unmet needs than former residents in facilities.
In an earlier report on surveys of residents who transitioned between January and April, 2000, CSHP reported the frequency of adverse events that may happen after discharge, such as falls, hospitalizations, and nursing home readmissions. About one-quarter of consumers had fallen in the first two or three months after discharge. Twenty-two percent of consumers had been hospitalized in that time, and one-fourth of these people were hospitalized two or three times. About one-eighth (12.3 percent) of consumers were readmitted to a nursing home, but less than one-third of these people were still in a nursing home at the time of the survey. CSHP noted that there is no appropriate comparison population to suggest whether these frequencies are high or low, since this population is not comparable to all nursing home residents or to all community-dwelling older people.
NEXT STEPS
New Jersey is developing several initiatives to focus on transitioning people under age 65 from nursing homes. State staff estimated that there are 3,000 people under age 65 in nursing homes, out of a total Medicaid nursing home population of approximately 28,000. The state legislature authorized $4 million in State Fiscal Year 2002 for Medicaid HCBS waiver services specifically for former nursing home residents under age 65. New Jersey's Division of Disability Services, part of the Department of Human Services, changed its Medicaid HCBS waiver for people with physical disabilities to serve more people and to make environmental modifications and personal emergency response systems available. Also, New Jersey received 40 Project Access Section 8 vouchers from the U.S. Department of Housing and Urban Development (HUD) available only for former nursing home residents under age 62.
CMS awarded two Nursing Home Transition grants in September 2002 to New Jersey: one to the DHSS Division of Consumer Support, which includes Community Choice, and the other to Resources for Independent Living, Inc., a Center for Independent Living (CIL), in partnership with other CILs. Both these grants have goals to improve supports for people under age 65 leaving nursing homes. The grant to DHSS includes training Community Choice counselors on the challenges people under age 65 face when attempting to transition. The CILs plan to use their grant to develop this training for Community Choice counselors, to develop assessment and service planning tools for the counselors to use with nursing home residents under age 65, and to create peer support and mentoring programs for nursing home residents.
BIBLIOGRAPHY
Cell, Paula. Evaluation: Manual of Operating Policies and Procedures, Community Choice Counselors. New Jersey Department of Health and Senior Services. August 29, 2000.
Ginsberg, Dorothy. Barriers to Implementing the Community Choice Initiative.
New Jersey Department of Health and Senior Services. March 2000.
Howell-White, Sandra. Current Living Situation and Service Needs of Former Nursing Home Residents: An Evaluation of New Jersey's Nursing Home Transition Program. Rutgers University Center for State Health Policy, June 2003.
Howell-White, Sandra; Palmer, Suzanne; and Bjerklie, J.R. Transitions to the Community: A Survey of Former Nursing Home Residents Discharged After Community Choice Counseling. Rutgers University Center for State Health Policy, October 24, 2001.
New Jersey Department of Health and Senior Services. Community Choice Counselor Manual of Policies and Operating Procedures. Spring 2000.
New Jersey Department of Health and Senior Services. Long Term Care Field Offices Administrative Manual.
Spring 2001.
New Jersey Department of Health and Senior Services. FY01 Discharges by Age. March 22, 2001.
Palmer, Suzanne and Howell-White, Sandra. Perspectives of the Community Choice Counselors: Report on a Focus Group. Rutgers University Center for State Health Policy, October 24, 2001.
Perriello, Tracy. Cost and Caseload Report. New Jersey Department of Health and Senior Services. November 28, 2001.
INTERVIEWS
New Jersey Department of Health and Senior Services (DHSS), Division of Consumer Support Central Office (Princeton, NJ) Leslie Hendricksen Sharon Briggs Rosemary Kidder Rebecca McMillen Amy Ancharski Paula Cell Dorothy Ginsberg Barbara Parkoff, consultant for DHSS through SP Consultants, L.L.C.
DHSS Middlesex Long Term Care Field Office (Edison, NJ) Cynthia Barnes Terri Kiczek Jennifer McKnight Ann Lorfing Betty Ann Zrinko
DHSS Burlington Field Office (Mount Laurel, NJ) Mary Malec Dolores Kuenzel Lisa Melnyk Veronica Novak Cindy Segura
Four Consumers
Phone Interviews after Site Visit
New Jersey Protection and Advocacy, Inc.: Assistive Technology Advocacy CenterEllen Lence
Rutgers University Center for State Health PolicySandra Howell-White
NOTES
-
In 1998, Colorado, Michigan, Rhode Island, and Texas received grants between $160,000 and $175,000 each. In 1999, New Hampshire, New Jersey, Vermont, and Wisconsin received grants of $500,000 each. In 2000, Arkansas, Florida, Pennsylvania, and Nebraska received grants of $500,000 each.
-
Eiken, Steve and Burwell, Brian. Final Report of the Nursing Home Transition Demonstration Grants Case Study. Medstat: publication pending.
-
Twenty-three states and ten centers for independent living received nursing home transition grants in 2001 and 2002. More information is available at the following Web site: http://www.cms.hhs.gov/systemschange/default.asp.
-
References for these reports can be found in the bibliography.
COMPLETE LIST OF SITE VISIT REPORTS
Community Choice: New Jersey's Nursing Home Transition Program
HTML http://aspe.hhs.gov/daltcp/reports/2003/NJtrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2003/NJtrans.pdf
Fast Track and Other Nursing Home Diversion Initiatives: Colorado's Nursing Home Transition Grant
HTML http://aspe.hhs.gov/daltcp/reports/2003/COtrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2003/COtrans.pdf
Michigan's Transitioning Persons from Nursing Homes to Community Living Program
HTML http://aspe.hhs.gov/daltcp/reports/2002/MItrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2002/MItrans.pdf
One-to-One: Vermont's Nursing Home Transition Program
HTML http://aspe.hhs.gov/daltcp/reports/2003/VTtrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2003/VTtrans.pdf
Partnerships for Community Living: Florida's Nursing Home Transition Program
HTML http://aspe.hhs.gov/daltcp/reports/2003/FLtrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2003/FLtrans.pdf
Passages: Arkansas's Nursing Home Transition Program
HTML http://aspe.hhs.gov/daltcp/reports/2003/ARtrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2003/ARtrans.pdf
Pennsylvania Transition to Home (PATH): Pennsylvania's Nursing Home Transition Program
HTML http://aspe.hhs.gov/daltcp/reports/2003/PAtrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2003/PAtrans.pdf
Project CHOICE (Consumers Have Options for Independence in Community Environments): Texas' Nursing Home Transition Program
HTML http://aspe.hhs.gov/daltcp/reports/2003/TXtrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2003/TXtrans.pdf
The Homecoming Project: Wisconsin's Nursing Home Transition Demonstration
HTML http://aspe.hhs.gov/daltcp/reports/2002/WItrans.htm
PDF http://aspe.hhs.gov/daltcp/reports/2002/WItrans.pdf
To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human ServicesOffice of Disability, Aging and Long-Term Care PolicyRoom 424E, H.H. Humphrey Building200 Independence Avenue, S.W.Washington, D.C. 20201FAX: 202-401-7733Email: webmaster.DALTCP@hhs.gov
RETURN TO:
Office of Disability, Aging and Long-Term Care Policy (DALTCP) Home [http://aspe.hhs.gov/_/office_specific/daltcp.cfm]Assistant Secretary for Planning and Evaluation (ASPE) Home [http://aspe.hhs.gov]U.S. Department of Health and Human Services Home [http://www.hhs.gov]