
TRENDS IN THE USE OF RESIDENTIAL SETTINGS AMONG OLDER ADULTS ISSUE BRIEF
Matthew Toth, PhD; Lauren A. Martin Palmer, PhD; Lawren E. Bercaw, PhD; Helena Voltmer, BA; and Sarita Karon, PhD
RTI International
October 2020
Printer Friendly Version in PDF Format (10 PDF pages)
ABSTRACT
This brief presents data on the estimated change in the size of residential care population and characteristics of older adults within different settings. This brief builds upon work previously conducted under the direction of John Drabek of ASPE.
This brief was prepared under contract #HHSP233201600021I between HHS's ASPE/BHDAP and RTI International. For additional information about this subject, you can visit the BHDAP home page at https://aspe.hhs.gov/bhdap or contact the ASPE Project Officers at HHS/ASPE/BHDAP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201; William.Haltermann@hhs.gov, William.Marton@hhs.gov, Helen.Lamont@hhs.gov.
DISCLAIMER: The opinions and views expressed in this brief are those of the authors. They do not reflect the views of the Department of Health and Human Services, the contractor or any other funding organization. This brief was completed and submitted on September 2019.
Background
Long-term services and supports (LTSS) include a variety of personal care, mobility, and social services to assist individuals with functional limitations due to disability or other physical or cognitive conditions (Tach & Weiner, 2018). LTSS can be provided in a variety of residential settings, from traditional housing and assisted living (non-institutional) to nursing homes (institutional). As the United States population ages, the prevalence of disability and functional limitations, as well as the demand for LTSS, is anticipated to increase (Freedman et al., 2013; Tach & Weiner, 2018). Yet we lack consistent and reliable estimates of older adults' use of each setting type.
Most research has identified a trend toward an increasing use of non-institutional residential care, such as assisted living facilities (Silver et al., 2018), and a decline in the use of institutional care, such as nursing homes (Spillman & Black, 2006; Grabowski, Stevenson, & Cornell, 2012; Degenholtz et al., 2016). However, survey and regulatory differences in the definitions of non-institutional LTSS can vary across surveys and states, hindering researchers' and policy makers' understanding of LTSS offered in these settings, and the LTSS needs of older adults residing in those settings.
Researchers and policy makers need to rely on multiple data sources to fully understand changes in the demographic and health characteristics of the residential care population, the range of services available in these settings, and how they are used (Spillman & Black, 2006; Stevenson & Grabowski, 2010; Caffrey et al., 2012; Zimmerman, Sloan, & Reed, 2014). Understanding changes in the use of residential settings and in the characteristics of older adults residing in these settings is crucial for policy makers to address the LTSS needs of the aging population. Using multiple data sources can provide a more reliable understanding of the number of older adults living in different residential settings, and their characteristics.
This brief presents data on the estimated change in the size of residential care population and characteristics of older adults within different residential settings. Through a longitudinal analysis of multiple data sources, we address the following questions:
-
How many older adults live in traditional housing, community-based residential care facilities, or nursing homes, and how have these numbers changed in recent years?
-
What do we know about the demographic, health, and functional characteristics of older adults living in different settings, and how they have changed in recent years?
Methods
We used multiple data sources to estimate the older adult (age 65+) population in the United States, their places of residence, and their demographic, health, and functional characteristics. These data sources include the Medicare Current Beneficiary Survey (MCBS) 2008 and 2013 Cost and Use Files; the 2008 and 2014 Health and Retirement Study (HRS); and the 2011 and 2015 National Health and Aging Trends Study (NHATS). We incorporated MCBS and HRS 2002 estimates from prior analyses (Spillman & Black, 2006) as a baseline year for our analyses.
Using survey data from these sources, we identified whether respondents resided in traditional housing, community-based residential care, or a nursing home. We categorized individuals into these settings based on their responses to whether they resided in a private home or apartment with or without access to some types of LTSS (traditional housing), or an alternative type of facility (e.g., assisted living facility) that offers support for activities of daily living (ADLs) such as meal preparation, housework or laundry support, and medication management (community-based residential care), or whether the survey identifies the residence type as a nursing facility. Survey data from these sources also were used to capture demographic information and health status characteristics, such as functional limitations and comorbidities.
We used survey-specific cross-sectional weights to produce nationally representative estimates of older adults residing in each setting for each survey year. We also estimated the age-standardized prevalence of all demographic and health characteristics for older adults residing in each setting to improve comparability across years. Age-standardization was based on the age distribution of the baseline year for each survey (2002 for HRS and MCBS, and 2011 for NHATS). F-tests were conducted between the baseline and later years of the survey within settings.
Findings
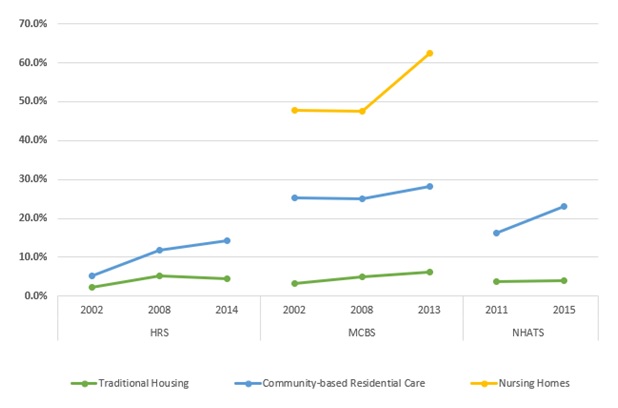
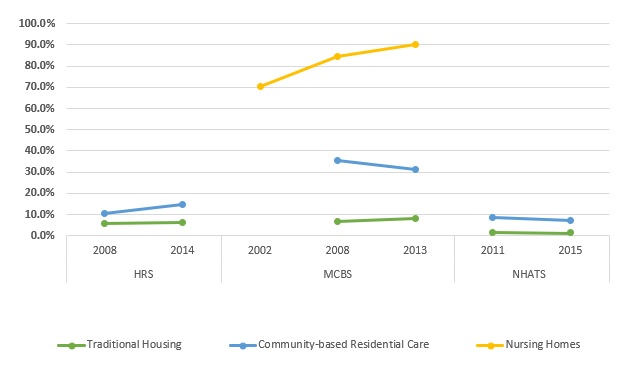
The number of older adults in the United States grew from approximately 34 million in 2002 to 42 million in 2015 (Table 1). Data from the HRS show a somewhat larger population than do the other surveys. All surveys indicate that the vast majority of older adults (over 90%) reside in traditional housing, and that there was a statistically significant increase in proportion of older adults in traditional housing over time (Exhibit 1). Each survey also shows that the number of people living in community-based residential care has increased over time. Despite an increase in absolute terms, the proportion of people residing in community-based residential care has been consistent (Exhibit 2). The number of people in nursing homes has declined or slightly increased, depending on the survey. However, proportionately fewer older adults have been residing in nursing homes over time (Exhibit 3).
| TABLE 1. Age-Standardized Residential Population Estimates and Percentages of Older Adults 65 Years and Older, by Housing Setting, Data Source, and Year | ||||||||
|---|---|---|---|---|---|---|---|---|
| Data Source | Year | Total | Housing Setting | |||||
| Traditional Housing | Community-Based Residential Care | Nursing Home | ||||||
| # | % | # | % | # | % | |||
| MCBS1 | 2002 | 34,347,619 | 32,120,018 | 93.5 | 781,982 | 2.3 | 1,445,619 | 4.2 |
| 2008 | 36,726,354 | 34,915,661 | 95.1** | 756,993 | 2.1 | 1,053,700 | 2.9** | |
| 2013 | 42,184,842 | 40,349,942 | 95.7** | 979,481 | 2.3 | 855,419 | 2.0** | |
| HRS2 | 2002 | 35,841,266 | 33,524,186 | 93.5 | 674,984 | 1.9 | --- | --- |
| 2008 | 38,812,253 | 36,934,841 | 95.2* | 475,710 | 1.2* | --- | --- | |
| 2014 | 46,214,893 | 44,171,963 | 95.6 | 835,060 | 1.8 | --- | --- | |
| NHATS3 | 2011 | 36,385,946 | 33,355,114 | 91.7 | 1,950,517 | 5.4 | 1,080,315 | 3.0 |
| 2015 | 41,789,316 | 38,696,907 | 92.6* | 2,005,887 | 4.8 | 1,086,522 | 2.6 | |
--- = not applicable. *p0.05, **p0.01.
| ||||||||
In all settings, there was increase in the age-standardized prevalence of dementia[1] (Exhibit 4). Relative to the baseline year, there was a statistically significant increase in dementia each year among those residing in traditional housing (HRS and MCBS, p0.01), among those in community-based residential care in 2014 (HRS, p0.05), and among those in nursing facilities in 2013 (MCBS, p0.01). Not surprisingly, the age-standardized prevalence of dementia was lowest among older adults living in traditional housing, and was much higher among those living in the other two settings, with the highest rates among those living in nursing homes.
We found mixed results in our estimates of age-standardized prevalence of having three or more limitations in ADLs across settings and time.[2] Among older adults in traditional housing, HRS data indicated that the percentage of those with three or more limitations in ADLs remained stable, MCBS data indicated an observable and statistically significant increase (p0.01), and NHATS data indicated a small decline that was not statistically significant (Exhibit 5). Both the MCBS and NHATS showed declines in the proportion of individuals with three or more functional limitations living in community-based residential care, but the declines were not statistically significant, while the HRS showed a non-statistically significant increase in the proportion of residents with three or more ADL limitations. Among older adults in nursing homes, the MCBS data showed a statistically significant increase in the proportion of residents with three or more ADL limitations over time (p0.05). The differences in the size and trend of the estimates across surveys are likely due to differences in how each data source defines functional limitations and setting location. The NHATS includes a broader definition of community-based residential care than the HRS and MCBS, likely covering individuals with fewer functional limitations than reported in other surveys.
| EXHIBIT 1. Change in the Proportion of the Older Adult Population Residing in Traditional Housing, by Year and Data Source |
|---|
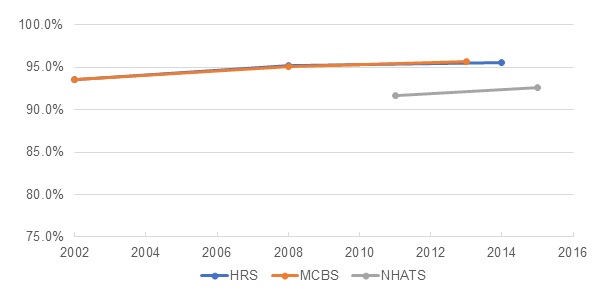 |
| EXHIBIT 2. Change in the Proportion of the Older Adult Population Residing in Community-Based Residential Care, by Year and Data Source |
|---|
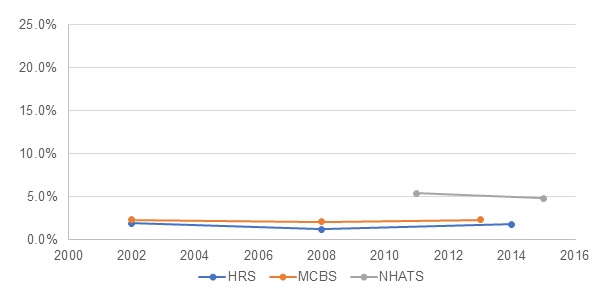 |
| EXHIBIT 3. Change in the Proportion of the Older Adult Population Residing in Nursing Homes, by Year and Data Source |
|---|
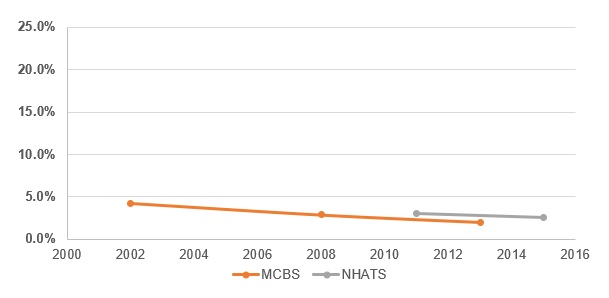 |
| EXHIBIT 4. Prevalence of Alzheimer's Disease or Other Dementia Over Time among Individuals Living in Different Residential Settings |
|---|
 |
| EXHIBIT 5. Prevalence of Older Adults with 3+ Limitations in ADLs in Each Setting |
|---|
 |
Discussion
The proportion of older adults residing in nursing homes is declining, and there is a corresponding increase in the proportion living in traditional housing. The size of the United States older adult population (age 65+) grew from 34 million in 2002 to roughly 42-46 million in 2014. However, this study found a statistically significant decline in the proportion of older adults residing in nursing homes, with a corresponding statistically significant increase in the proportion of older adults residing in traditional housing in at least one survey. The proportion of people residing in community-based residential care has remained stable.
Although these trends demonstrate less use of institutional LTSS over time, it is likely not because the population is getting healthier or has fewer LTSS needs. Coinciding with the shift from residence in nursing homes to residence in traditional housing is an increase in the prevalence of dementia, and some evidence of increasing functional limitations among those living in traditional housing.
There are several possible explanations for these findings.
-
Residential settings outside of formal community-based residential care may be becoming more accommodating to those with LTSS needs. One possibility is that private homes and other residential settings may be becoming more accommodating to adults who want to age in place, remaining in their own homes and communities with supportive LTSS provided by informal caregivers, paid services, and/or supplemented by assistive devices and technology. For example, access to occupational therapy, nursing assistance, and home modifications can help promote aging in place (Szanton et al., 2016). Moreover, assistive technology to help older adults age in place has become more available and effective in helping reduce functional limitations and informal caregiver burden (Anderson & Wiener, 2013; Spillman, 2012; Schulz et al., 2015; Lin & Wu, 2014). Our findings may supplement previous studies by indicating that despite evidence of increasing LTSS needs, older adults may be finding ways to meet their changing needs while aging in place.
-
Changes to federal and state policy to emphasize access to home and community-based LTSS. Federal programs such as Money Follows the Person (Robison et al., 2015), the Balancing Incentives Program, and the Financial Alignment Initiative are indicative of efforts to better meet LTSS needs outside of institutional settings. Medicaid spending on HCBS services for older adults increased by 148% from 2003 to 2013, compared to only a 19% increase on institutional services (Eiken et al., 2018), indicative of a shift toward home and community-based spending at the state level (Tach & Wiener, 2018). The number of nursing homes in the United States has declined from 2005 to 2014 (CMS, 2015), further evidence of the shift toward home and community-based LTSS. Our findings showing a decline in the proportion of older adults residing in nursing homes correspond with trends identified in previous work (Degenholtz et al., 2016; Silver et al., 2018).
Conclusion
Increases in cognitive and functional limitations among older adults, coupled with a decline in the use of nursing homes and more older adults using community-based residential care, highlights the importance of meeting the LTSS needs of older adults in the community. Further research is needed to better understand whether older adults can access all needed services at home or in community-based residential care, as well as institutional care when needed.
References
Anderson, W.L., & Wiener, J.M. (2013). The impact of assistive technologies on formal and informal home care. Gerontologist, 55(3), 422-433.
Arno, P.S., Levine, C., & Memmott, M.M. (1999). The economic value of informal caregiving: President Clinton's proposal to provide relief to family caregivers opens a long-overdue discussion of this "invisible" health care sector. Health Affairs, 18(2), 182-188.
Caffrey, C., Sengupta, M., Park-Lee, E., Moss, A., Rosenoff, E., & Harris-Kojetin, L. (2012). Residents Living in Residential Care Facilities: United States, 2010. NCHS Data Brief No. 91. Hyattsville, MD: National Center for Health Statistics. Retrieved from https://www.cdc.gov/nchs/data/databriefs/db91.pdf.
Centers for Medicare & Medicaid Services (CMS). (2015). Nursing Home Data Compendium 2015 Edition. Available at https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/CertificationandComplianc/Downloads/nursinghomedatacompendium_508-2015.pdf. Accessed 30 June 2019.
Degenholtz, H.B., Park, M., Kang, Y., & Nadash, P. (2016). Variations among Medicare beneficiaries living in different settings: Demographics, health status, and service use. Research on Aging, 38(5), 602-616.
Eiken, S., Sredl, K., Burwell, B., & Amos, A. (2018). Medicaid Expenditures for Long-Term Services and Supports in FY 2016. IBM Watson Health. Available at https://www.medicaid.gov/medicaid/ltss/downloads/reports-and-evaluation…. Accessed 1 August 2019.
Freedman, V.A., Spillman, B.C., Andreski, P.M., Cornman, J.C., Crimmins, E.M., Kramarow, E., Lubitz, J., Martin, L.G., Merkin, S.S., Schoeni, R.F., Seeman, T.E., & Waidmann, T.A. (2013). Trends in late-life activity limitations in the United States: An update from five national surveys. Demography, 50(2), 661-671.
Grabowski, D.C., Stevenson, D.G., & Cornell, P.Y. (2012). Assisted living expansion and the market for nursing home care. Health Services Research, 47(6), 2296.
Harris-Kojetin, L., Sengupta, M., Park-Lee, E., & Valverde, R. (2013). Long-term care services in the United States: 2013 overview. National Center for Health Statistics. Vital Health Stat, 3(37).
Harris-Kojetin, L., Sengupta, M., Park-Lee, E., Valverde, R., Caffrey, C., Rome, V., & Lendon, J. (2016). Long-term care providers and services users in the United States: Data from the National Study of Long-Term Care Providers, 2013-2014. National Center for Health Statistics. Vital Health Stat, 3(38).
Lin, I.F., & Wu, H.S. (2014). Activity limitations, use of assistive devices or personal help, and well-being: Variation by education. Journals of Gerontology Series B: Psychological Sciences & Social Sciences, 69(S1), S16-S25.
Medicare Payment Advisory Commission (MedPAC). (2018). A Data Book: Health Care Spending and the Medicare Program. Available at http://www.medpac.gov/docs/default-source/data-book/jun18_databookentirereport_sec.pdf.
National Alliance for Caregiving & AARP. (2004). Caregiving in the United States. Available at http://www.caregiving.org/data/04finalreport.pdf.
Osterman, P. (2017). Who Will Care for Us?: Long-Term Care and the Long-Term Workforce. Russell Sage Foundation.
Robison, J., Porter, M., Shugrue, N., Kleppinger, A., & Lambert, D. (2015). Connecticut's "money follows the person" yields positive results for transitioning people out of institutions. Health Affairs (Millwood), 34(10), 1628-1636. doi: 10.1377/hlthaff.2015.0244.
Schulz, R., Wahl, H.W., Matthews, J.T., De Vito Dabbs, A., Beach, S.R., & Czaja, S.J. (2015). Advancing the aging and technology agenda in gerontology. Gerontologist, 55, 724-734. doi: 10.1093/geront/gnu071
Silver, B.C., Grabowski, D.C., Gozalo, P.L., Dosa, D., & Thomas, K.S. (2018). Increasing prevalence of assisted living as a substitute for private-pay long-term nursing care. Health Services Research, 53(6), 4906-4920.
Spillman, B.C. (2012). Subtask 3: Memorandum on Available Long-Term Care Projections. Prepared for the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. Washington, DC: Urban Institute.
Spillman, B.C., & Black, K.J. (2006). The size and characteristics of the residential care population: Evidence from three national surveys. Prepared for the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. Washington, DC: Urban Institute. Available at https://aspe.hhs.gov/basic-report/size-and-characteristics-residential-care-population-evidence-three-national-surveys.
Stevenson, D.G., & Grabowski, D.C. (2010). Sizing up the market for assisted living. Health Affairs, 29(1), 35-43.
Szanton, S.L., Leff, B., Wolff, J.L., Roberts, L., & Gitlin, L.N. (2016). Home-based care program reduces disability and promotes aging in place. Health Affairs, 35(9), 1558-1563.
Thach, N., & Wiener, J. (2018). An Overview of Long-Term Services and Supports and Medicaid: Final Report. Prepared for the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. Research Triangle, NC: RTI International. Available at https://aspe.hhs.gov/basic-report/overview-long-term-services-and-supports-and-medicaid-final-report. Accessed on 1 August 2019.
Zimmerman, S., Sloane, P.D., & Reed, D. (2014). Dementia prevalence and care in assisted living. Health Affairs (Millwood), 33, 658-666. doi:10.1377/hlthaff.2013.1255.
Endnotes
-
Defined in all surveys as whether the respondent has ever been told they had Alzheimer's/dementia, with exception to MCBS survey of people residing in nursing facilities and in some cases community-based residential care. For individuals classified in these settings, the MCBS uses assessment or administrative data to determine whether the respondent has been diagnosed with Alzheimer's or dementia.
-
We do not show the 2002 values for traditional housing and community-based residential care because they are not comparable to the later year values. The 2002 values define functional limitations as having "help with" the ADL/IADL activities, whereas the MCBS/HRS 2008 and most recent year define limitations as having "any difficulty with" the ADL/IADL activity.
Analyses of Disability, Aging and Long Term Care Policy and Data
Reports were prepared under contract #HHSP233201600021I between HHS's ASPE/BHDAP and RTI International. For additional information about this subject, you can visit the BHDAP home page at https://aspe.hhs.gov/bhdap or contact the ASPE Project Officers at HHS/ASPE/BHDAP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201; William.Haltermann@hhs.gov, William.Marton@hhs.gov, Helen.Lamont@hhs.gov.
Reports Available
Trends in the Use of Residential Settings among Older Adults Issue Brief
- HTML version: https://aspe.hhs.gov/basic-report/trends-use-residential-settings-among-older-adults-issue-brief
- PDF version: https://aspe.hhs.gov/pdf-report/trends-use-residential-settings-among-older-adults-issue-brief
Understanding the Characteristics of Older Adults in Different Residential Settings: Data Sources and Trends