
This paper summarizes opportunities for states to utilize time-limited federal cost-sharing to modernize human services program eligibility systems and to use data from health programs to streamline eligibility determination for human services.
"Executive Summary
The Patient Protection and Affordable Care Act (Affordable Care Act or ACA) creates opportunities for human services programs to modernize their eligibility systems and to use data from health programs to streamline eligibility determination for human services.
Modernizing eligibility systems
For information technology (IT) improvements that are in place by no later than December 31, 2015, and that are required for Medicaid eligibility purposes, the federal Medicaid program will pay 90 percent of investment costs. Even if human services programs also benefit, a time-limited exception to normal cost-allocation rules eliminates the need for them to share in those investment expenditures, so long as the investment involves either—
- the development or procurement of a business service that serves both Medicaid and human services programs; or
- the construction of an interface between Medicaid and a human services program that helps the Medicaid program (1) verify eligibility or (2) “fast track” Medicaid enrollment of uninsured individuals, based on information in their human services case files. This step can also include development of functionality needed for the interface to obtain necessary information from human services records, functionality that can help the human services program in other ways as well.
This opportunity is available in all states. Whether or not a state expands Medicaid eligibility, the ACA requires it to use data matches with reliable sources, whenever possible, to determine eligibility. That shift to data-driven eligibility has required, in turn, a significant investment of federal IT funds needed to modernize Medicaid’s previously outdated eligibility systems. Human services programs can participate in such modernization efforts, but they may increase their likelihood of successfully tapping into these resources by taking an approach that minimizes time demands on Medicaid staff, given the competing demands of ACA implementation. As one possible strategy, the human services agency could volunteer to carry out most of the work needed to develop or procure a new service or interface that promises to serve both health and human services programs.
Streamlining human services programs’ eligibility determinations by accessing data from health programs
Once the ACA’s insurance affordability programs are fully phased in, Medicaid will be the country’s most widely-used need-based program—particularly in states that expand eligibility. If all states did so, the number of people eligible for help would be up to 60 percent higher for Medicaid than for the Supplemental Nutrition Assistance Program (SNAP), the need-based program with the second-largest number of people who qualify for help. Even among individuals with incomes below 138 percent FPL, expanded Medicaid eligibility would reach more than a third (36 percent) more people than SNAP.
Under nationwide Medicaid expansion, Medicaid and CHIP eligibility would reach 97 percent of SNAP recipients, 85 percent of families participating in the Special Supplemental Nutrition Program for Women, Infants and Children (WIC), 99 percent of recipients of Temporary Assistance to Needy Families (TANF), and 87 percent of participants in the Low Income Home Energy Assistance Program under age 65.1
Especially in states that expand Medicaid, health programs are likely, several years hence, to have considerable information about the vast majority of low-income households who apply for or receive human services benefits. Much of the data will be stored by marketplaces or subject to marketplace legal requirements. Under federal regulations revised in March 2014, human services programs can access most of this information (except for tax records) by taking several steps:
- obtaining consent from the affected individuals;
- showing that the health insurance marketplace would benefit; and
- ensuring that the information will remain protected by confidentiality and data security safeguards no less stringent than those that apply within the marketplace.
TANF, SNAP, and certain other human services program can also access Medicaid information directly, outside the marketplace, under Social Security Act §1137.
Household definitions and other detailed eligibility rules differ between human services programs and Medicaid, which for most beneficiaries now follows Modified Adjusted Gross Income (MAGI) principles derived from federal income tax law. Nevertheless, eligibility information from Medicaid records could prove useful to human services programs, in several ways:
- Medicaid records could confirm that particular individuals meet non-financial eligibility requirements for human services benefits, such as citizenship or status as a qualified alien.
- The human services program could “deem” someone eligible based on Medicaid’s finding of financial eligibility, notwithstanding technical differences between program eligibility rules.
- The human services program could change its eligibility rules so that, for some or all households, Medicaid and the human services program define income in the same way. A Medicaid income determination could then establish eligibility and benefit levels for the human services program.
- Medicaid’s records could be used to pre-populate an application form for human services benefits—e.g., with an address or social security number—or provide the human services program with verification obtained by the health program, either confirming eligibility for human services or raising a “red flag” suggesting a need for further investigation.
Which (if any) of these strategies proves most useful will depend on the circumstances facing the human services program in the applicable state.
Introduction
The Patient Protection and Affordable Care Act (Affordable Care Act or ACA) was one of the most significant pieces of domestic legislation enacted since the 1960s. It has many repercussions, including for human services programs. This paper focuses on two potential gains that such programs can realize from this legislation:
- Modernizing the information technology (IT) systems human services programs use for eligibility purposes by accessing more generous federal funding than has been available in the past—and that will only be available through the end of calendar year 2015; and
- Lowering the cost and expanding the reach of human services programs’ own eligibility determination and verification procedures by leveraging the data that health programs will obtain about numerous applicants for and beneficiaries of insurance affordability programs.
In each of these two areas, we briefly inventory the potential benefits that human services programs could obtain and outline possible options for moving forward.
Generous federal funding to modernize eligibility systems
Opportunities presented by the ACA
Eligibility systems for many human services programs are highly outdated. This can render operations cumbersome, raise administrative costs, create obstacles to effective data use, make changes costly and slow, present burdens for consumers, and create other inefficiencies in eligibility determination. Although state agencies recognize these constraints, the federal funding environment has historically not provided generous support for major system overhauls.
Federal officials are implementing ACA in a way that permits states, for a limited time only, to address this longstanding problem. For goods and services that are furnished by the end of calendar year 2015:
- the federal government will pay 90 percent of Medicaid programs’ IT development costs for eligibility systems; and
- an exception to normal cost-allocation rules relieves human services programs, under some circumstances, of the need to share in the cost of IT development that benefits both Medicaid and human services programs.2
Federal funding levels for eligibility system modernization are now available that have not been experienced in the history of health and human services programs, and it is not clear when or if this opportunity will recur. States could pursue targeted upgrades to strategically selected functions within their eligibility systems. Alternatively, states could implement more sweeping changes, integrating health and human services programs’ eligibility systems across the board, using more generous federal funding to accelerate such development and lower the state share of costs.
A state is not required to expand Medicaid eligibility in order to qualify for these funds. All Medicaid programs, whether or not they expand eligibility, must now use data-driven eligibility procedures, and enhanced federal funding is available in every state to support the investments needed to make such procedures possible.
The opportunity is clear. But to take advantage of it, state officials need to understand the background and basic ground rules of the cost-allocation exception, which are described in the next sections of the paper.
Background of enhanced federal funding and the cost-allocation exception
When the ACA was signed into law in 2010, outdated eligibility systems for Medicaid and the Children’s Health Insurance Program (CHIP) presented a serious obstacle to effective implementation. Not only were those systems expected to handle an influx of significant numbers of new applicants, the ACA substantially changed the rules for eligibility determination. For example:
- Whenever possible, verification will now be based on data from reliable, electronic sources;
- Consumer-provided documentation will be a last resort, requested only when data are unavailable or insufficient to demonstrate eligibility;
- Regardless of the agency at which a consumer applies for coverage, data must be exchanged seamlessly “behind the scenes” to determine the program for which the consumer qualifies; and
- When eligibility is being renewed, if information in the beneficiary’s case record combined with data from reliable external sources show continuing qualification for Medicaid, eligibility is renewed administratively, without requesting documentation from beneficiaries.3
This new approach seeks to lower ongoing administrative costs, increase participation levels among eligible consumers by streamlining enrollment and retention, and reduce the proportion of erroneous eligibility determinations.
However, satisfying the ACA’s call for integrated and data-driven eligibility determination presented a daunting challenge for states operating outdated, “legacy” IT systems. Unlike the optional Medicaid eligibility expansion, the transformation of Medicaid eligibility from paper-driven to data-driven methods remains in effect nationwide. Such a major transition has required massive overhauls or complete replacement of Medicaid programs’ archaic eligibility systems. To make this possible, the federal government has been providing substantial funding to states for modernizing eligibility systems. Specifically, states can access 100 percent federal grant funding through December 31, 2014, for IT activities related to building a state-based marketplace. Under special federal financing rules for Medicaid Management Information Systems (MMIS),4 states can also receive 90 percent federal matching funds for developing Medicaid eligibility IT through December 31, 2015. Seventy-five percent matching funds will be available for operating such automated systems, including for eligibility workers interacting with the eligibility system, for the indefinite future.
By themselves, these steps were not sufficient to fund the necessary modernization of Medicaid eligibility systems, however. Cost allocation rules, under Office of Management and Budget (OMB) Circular A-87,5 generally require that all programs benefiting from an investment must share in its cost.6 If that principle had applied in this case, the eligibility systems that serve Medicaid programs would have received considerably less than the 90 percent federal funding that CMS sought to provide. All but five states use their Medicaid eligibility systems for human services programs as well—most commonly the Supplemental Nutrition Assistance Program (SNAP) and Temporary Assistance to Needy Families (TANF).7 Altogether, 39 states and the District of Columbia have systems that are fully integrated between Medicaid and SNAP, and an additional seven states integrate the two programs for certain populations or geographic areas.8 Normal cost-allocation rules would thus have required the cost of IT upgrades to be shared between Medicaid, for which the federal government pays a 90 percent match; SNAP, for which the federal government pays a 50 percent match; and TANF, which funds IT from the state’s block grant, presumably by reducing other expenses covered by the grant.
Operating under normal cost-allocation rules, Medicaid programs typically paid 40 to 60 percent of eligibility system costs.9 The 90 percent matching percentage would have applied only to that Medicaid share of eligibility system upgrades, so states would have been asked to pay significantly more than 10 percent of IT modernization costs. States may not have modernized Medicaid eligibility systems, endangering accomplishment of the ACA’s core goals.
To avoid this result, OMB created an exception to the normal application of cost-allocation rules, for a limited period of time. The exception is described in a letter from the U.S. Departments of Health and Human Services (HHS) and Agriculture (USDA), dated August 2011, explaining that federally funded human services programs, such as SNAP, TANF, the Child Care and Development Fund (CCDF), the Low Income Home Energy Assistance Program (LIHEAP), and the Special Supplemental Nutrition Program for Women, Infants and Children (WIC), can benefit from investments made to modernize eligibility systems for Medicaid, CHIP and state-based marketplaces, without allocating the system development costs across all benefiting programs. That letter, along with other relevant policy documents establishing the terms of the cost-allocation exception, are discussed in the next section.
Some basic ground rules of the cost-allocation exception
The cost-allocation exception has raised the proportion of eligibility system investment costs paid by Medicaid to approximately 88 percent,10 greatly increasing the feasibility of modernizing eligibility IT. The August 2011 letter from HHS and USDA contained language broadly supportive of integration efforts, explaining that the exception “allows States the opportunity to thoughtfully consider the benefits of integrating the eligibility determination functions across health and human services programs... Integrated systems can realize efficiencies for States and better customer service for families.”11 This language reflected OMB’s support for efficiency gains that can result from such integration across the boundaries of multiple programs.
The letter also explained that the cost allocation exception “allows human services programs … to utilize systems designed specifically for determining a person’s eligibility for certain health coverage programs (Medicaid, CHIP, and premium tax credits and cost sharing benefits through the Exchange) without sharing in the common system development costs, so long as those costs would have been incurred anyway to develop systems for the Exchanges, Medicaid, and CHIP.” (Emphasis added.) Even if an expenditure incidentally benefits a health coverage program, it cannot qualify for the cost-allocation exception unless it “would have been incurred anyway” for purposes of the health coverage program.
The letter further noted the “short timeframe” available “to accomplish the eligibility system changes needed to implement Affordable Care Act health insurance changes...” A follow-up, 2012 letter from HHS and USDA emphasized that favorable federal funding is limited to goods and services that are furnished by December 31, 2015. If a state contracts with and pays an IT vendor before that date but some goods and services have not yet been provided, the goods and services that remain to be furnished cannot benefit from either 90 percent federal funding or the cost allocation exception. The letter explained:
“States would need to incur costs for goods and services furnished no later than December 31, 2015 to make use of this exception. This would mean that if an amount has been obligated by December 31, 2015, but the good or service has not yet been furnished by that date, then such expenditure must be cost allocated as currently required under OMB Circular A-87.”12
The letter went on to explain that if a state will be requesting funding for only Medicaid and CHIP IT, it should go through the Advance Planning Document (APD) process with CMS. The APD process involves a state submitting its plan for IT modernization and obtaining federal approval. If funds are also being sought from other federal programs, the state’s APD should be sent to the corresponding federal program offices. In addition, the state could send its proposal “if necessary, to [the Administration of Children and Families’] Office on Administration,” which “acts as the clearinghouse for all HHS-related APDs that include two or more HHS entitlement programs and coordinates review with [the USDA’s Food and Nutrition Service, or FNS].” Further, as a prudential matter, a state would likely be well-advised to keep all affected federal offices informed of IT development efforts that may affect non-Medicaid programs, even if Medicaid is the sole provider of federal funds under the cost-allocation exception.
Given the many other issues facing state Medicaid agencies, it may be important for human services officials to carefully track the APD and work behind the scenes to ensure that it moves forward expeditiously. Nevertheless, CMS will require the state Medicaid agency to take the lead in submitting a Medicaid-specific APD, responding to CMS questions, and serving as the state entity formally responsible for the APD.
According to other CMS materials, a Medicaid/CHIP APD that seeks a cost allocation exception should add the following information to the standard contents of a Medicaid APD:
- A narrative detailing the human services programs that will eventually be included;
- A narrative explaining how the state will “identify, capture, and implement the foundational needs” of the applicable human services programs; and
- The identity of human services agencies and staff working on the project’s design and implementation.13
CMS guidance further explains that “any expansion of these services or increase in capacity beyond that required for health programs must be cost allocated to the benefitting program, consistent with current practice under OMB Circular A-87;” and that the exception applies only to the development of automated eligibility systems, not to their operation and maintenance, which remain subject to standard cost allocation rules. To qualify for the exception, IT investments must satisfy all conditions and standards for enhanced funding under Medicaid rules, which require a consumer-friendly interface supported by a 21st-century IT infrastructure.14
Options for taking advantage of this opportunity
Jointly buying or building service capacities that will serve both programs
The most straightforward way for human services programs to benefit from this time-limited opportunity is to join with Medicaid programs in the joint procurement or development of software or hardware that will serve both programs. The 2012 letter from HHS and FNS includes the following, non-exhaustive list of business services that could fit within this approach:15
✓ Client Portals
✓ User Interfaces
✓ Master Client Index
✓ Business Rules Engine and Operating Systems
✓ Interfaces to: Federal and State verification sources; Community Assisters/ Outreach Organizations; Exchange Infrastructure
✓ Enterprise Service Bus
✓ Data Warehouse
✓ Privacy and Security Controls
✓ Workflow Management Tools
✓ Business Intelligence
✓ Notices
✓ Customer Services Technical Support
✓ Automated Account Creation and Case Notes
✓ Identity Management
✓ Document Imaging and Digitization of Case Records
✓ Analytic Tools, including Decision Support and Program Integrity
✓ Telecommunications
✓ Information Security and Privacy Controls
✓ Infrastructure and Data Center Hosting
The American Public Human Services Association (APHSA) has developed a “toolkit” that provides state officials with a practical and thorough guide towards pursuing this general strategy.16 There is no need to revisit that ground here.
We do note the wide spectrum of possibilities facing states in this general area. A state can use the cost-allocation exception to develop specific, joint functionalities that achieve incremental gains; or it can take advantage of enhanced federal funding, for as long as it lasts, to pursue a broad vision of integrated eligibility determination for health and human services programs.
Developing an efficient interface between health and human services programs
In addition to jointly procuring or developing business functions that can serve both health and human services programs, a second approach can potentially qualify for the cost-allocation exception. A state can develop an interface between health and human services programs that serves two important functions for Medicaid:17
- Verification. The interface can provide Medicaid with automated access to information about applicants for and current or former recipients of human services benefits. This can be used to verify Medicaid eligibility efficiently, without the manual intervention of caseworkers from either health or human services agencies. Such automated eligibility determination reduces administrative costs for Medicaid agencies while strengthening program integrity by providing an additional check on the accuracy of Medicaid’s eligibility decisions.
In addition, automating verification can increase health coverage for Medicaid-eligible consumers. If less work is required for consumers to document initial or continuing eligibility for Medicaid, fewer eligible consumers will be denied or lose health coverage because they fail to gather, organize, and furnish the necessary documentation. Developing an effective interface between health and human services programs is thus integral to realizing the ACA’s vision of maximizing health coverage for those who qualify by streamlining eligibility determination.
- Fast-tracking Medicaid enrollment. An interface between health and human services programs could identify recipients of human services benefits who do not yet participate in Medicaid but who are likely to qualify for Medicaid as newly eligible adults and can therefore become the subject of “fast track” enrollment into health coverage. In May 2013, CMS released a letter to state health officials describing the opportunity to automatically enroll some or all of a state’s current SNAP recipients into Medicaid, based on their receipt of SNAP. The process included a waiver under Social Security Act §1902(e)(14)(A) that allowed states to avoid making individual income calculations, instead relying on SNAP eligibility findings to qualify consumers for Medicaid.18 This process was especially convenient for the SNAP and Medicaid programs, in part because of the common eligibility systems that Medicaid and SNAP programs shared before the ACA in most states, as explained earlier. With the kind of interface discussed here, other human services programs could also partner with Medicaid using the same strategy to automatically enroll groups of Medicaid-eligible consumers based on their receipt of human services benefits.
Particularly important to human services programs is that investments needed for the interface to gather necessary information from human services program records can qualify for the cost-allocation exception, so long as they would not have been made but for the Medicaid program’s need for the interface. In some cases, the capabilities that result from such investments could prove helpful to human services programs in other contexts.
For example, the interface with Medicaid may require the human services program to improve its ability to respond to queries from Medicaid. In turn, this may involve strengthening the capacity to search its records efficiently (which may require some initial indexing capacity) and then reporting requested information about specific individuals within households receiving benefits—capacities that could ultimately prove useful in other contexts as well.
The cost-allocation exception would cover the cost of developing the searching and reporting functions needed for the interface with Medicaid to function properly. If the human services program sought to use those functions for other purposes—to develop data analytic functions, for example, that analyze human services program performance or that facilitate linkages to other third-party data sources with information potentially relevant to eligibility for human services benefits—those subsequent efforts would be funded entirely by the human services program, without any role played by Medicaid or the cost-allocation exception. Nonetheless, the Medicaid-focused investment covered by the cost-allocation exception could significantly lower the later, incremental cost of developing capacities specifically focused on meeting the human services program’s needs.
Reducing the amount of work required from state Medicaid officials
As a practical matter, human services agencies may benefit from developing strategies that minimize the demands their proposals place on Medicaid agencies’ time and effort. The Great Recession left in its wake understaffed agencies in most states, and the demands of ACA implementation on Medicaid administrators remain considerable, even after passage of the ACA’s initial sign-up deadlines.
One approach to address this challenge would, as suggested above, use an interface with the human services program to enhance the Medicaid program’s ability to verify eligibility through data matches. This would contribute to more efficient Medicaid operations by potentially reducing the need for caseworker verification. Put differently, the development of a Medicaid-human services interface could be one of several methods through which both Medicaid and human services benefit from the cost-allocation exception, thereby encouraging the Medicaid agency to devote at least some time to this effort.
Another possible approach would have the human services agency volunteer to invest much of the effort needed to build or procure the shared service or interface, thus limiting demands placed on the Medicaid agency. As noted earlier, the Medicaid agency would need to lead the process of gaining APD approval from CMS, but much if not most of the other work might be done by the human services agency. Operationally, Medicaid and human services would both benefit from the investment; state general fund dollars would be used to “draw down” federal Medicaid dollars to finance the investment; but given the competing demands on both agencies’ time, human services staff would do much of the work outside the direct interaction with CMS.
Using data from health programs to expedite eligibility determination and verification for human services programs
Opportunities presented by the ACA
If all states implemented the ACA’s Medicaid expansion, more people would qualify for Medicaid and CHIP than for SNAP, the need-based program with the second-highest number of eligible people. Assessing SNAP’s reach as of 2010, when the program’s eligibility for childless adults was at historically high levels, Medicaid- and CHIP-eligible nonelderly individuals under the ACA’s Medicaid expansion would exceed those who qualify for SNAP by—
- 36 percent among such individuals with incomes at or below 138 percent FPL, mainly because Medicaid will cover more childless adults than did SNAP;
- 47 percent if one also takes into account individuals (mainly children) above 138 percent FPL but does not include CHIP children enrolled in employer-sponsored coverage; and
- 60 percent, if one also includes CHIP-eligible children in employer-sponsored coverage among those who could potentially qualify for Medicaid or CHIP, in which case the total number of Medicaid/CHIP eligibles would reach an estimated 91.9 million. 19
In addition to Medicaid, another 17.8 million individuals would qualify for subsidies in health insurance marketplaces.
Particularly in states with expanded Medicaid eligibility, health coverage programs will thus become a repository of information about a very large number of low-income households. If health programs have already evaluated the circumstances of someone applying for human services, the human services agency may be able to rely on the health program’s work, lowering the cost of eligibility determination and verification.
Those efficiencies could apply to a considerable fraction of human services agency caseloads. If all states implement the Affordable Care Act’s Medicaid expansion, Medicaid and CHIP eligibility will reach 97 percent of SNAP recipients, 85 percent of families participating in WIC, 99 percent of TANF recipients, and 87 percent of LIHEAP participants under age 65 (Figure 1). This suggests that, once the ACA’s expansions are fully implemented, human services programs may be able to expedite eligibility determination for numerous applicants and participants based on data from health programs.
Figure 1. Among recipients of various human services benefits under age 65, the percentage who will qualify for health programs under the Affordable Care Act
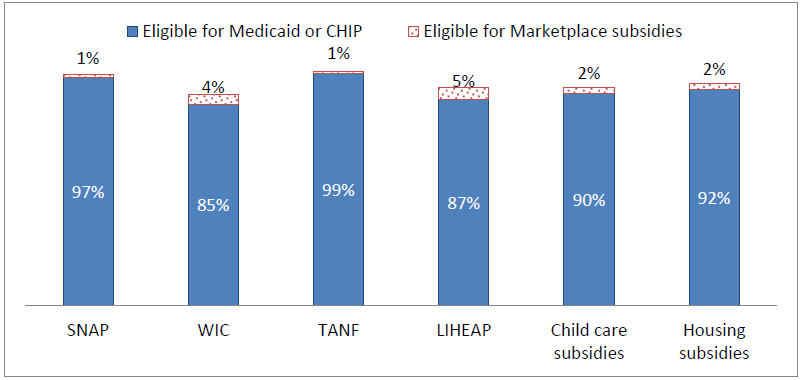
Source: Dorn, Isaacs, et al., 2013. Notes: Based on the application of 2014 ACA health coverage rules to estimated average monthly participants in human services programs during calendar year 2010. Assumes that all states expand Medicaid eligibility for adults to 138 percent FPL. Children’s eligibility for Medicaid and CHIP includes pre-ACA categories above 138 percent FPL and does not exclude recipients of employer-sponsored insurance. Estimates for children and adults include people with disabilities who receive Medicare. WIC and child care counts include spouses and dependents under age 19 who do not directly receive subsidies. Housing subsidies include public housing and rent vouchers.
Several limitations are important to acknowledge. First, this information shows the potential reach of health programs. That is, we show the number of human services participants who will qualify for Medicaid, CHIP, and marketplace subsidies if states expand Medicaid eligibility. Human services programs will not fully benefit from health programs until the latter have had time to ramp up enrollment among new eligibles.
Second, the information available from health programs may not be recent. Eligibility for health programs will typically be redetermined only once every 12 months, under the ACA’s new procedures. The human services program may thus need to consider the date on which the health program determined eligibility before deciding whether to rely on that determination.
Third, Medicaid programs that have expanded eligibility will often not make precise income determinations. The only fact relevant to financial eligibility is whether a consumer’s income is at or below 138 percent of the federal poverty level (FPL).20
For example, suppose that an applicant attests to income at 115 percent FPL and data matches with prior-year income tax records and recent quarterly wage records show income between 125 and 130 percent FPL. In that case, the Centers for Medicare and Medicaid Services (CMS) have made clear that available data are “reasonably compatible” with the applicant’s attestations and thus verify financial eligibility. The applicant is known to have income below 138 percent FPL and should not be asked for any financial documentation.21
A human services program will need more precise information to decide eligibility if its upper income limit is below 138 percent FPL. Moreover, many human services programs need precise income information to set benefit levels. Such programs may gain little from learning that a particular consumer qualified as financially eligible for Medicaid in a state that expanded eligibility.
It is important to note that neither of these timeliness and imprecision issues affect SNAP, which typically updates eligibility information every six months and attempts to ascertain income levels with great exactitude to determine benefits. It is true that SNAP does not offer Medicaid’s advantages in terms of the largest possible number of consumers potentially reached after full ACA implementation and the near-term benefits of accessing 90 percent federal funding to modernize eligibility systems. Nevertheless, SNAP is the country’s second-largest need-based program and a valuable information resource for other human services programs considering integration strategies for streamlining eligibility determination and verification. In addition, child support agencies are an important source of information that can help determine and verify eligibility for both health and human services programs. The latter agencies are likely to serve as useful partners given their experience in data matching, knowledge of confidentiality and data security issues, their regular practice of mandatory data exchange with numerous health and human services programs, and their access to a broad range of information sources potentially relevant to eligibility.
Options for taking advantage of this opportunity
In this section of the paper, we address strategies for overcoming two potential challenges:
- gaining legal access to eligibility data from health programs; and
- using data from health programs to establish and verify eligibility for human services programs, notwithstanding differences between the household definitions and other program rules used by health and human services programs.
Gaining legal access to health programs’ eligibility records
Marketplace records. Regulations governing marketplaces limit their ability to disclose “personally identifiable information” (PII) they either create or collect “for the purposes of determining eligibility for enrollment in a qualified health plan; determining eligibility for other insurance affordability programs…; or determining eligibility for exemptions from the individual responsibility” requirement.”22
In their 2012 version,23 these regulations forbade such disclosures except to accomplish marketplaces’ specifically assigned functions, which did not include helping human services programs determine eligibility. Had they remained in that form, human services programs would likely have been barred from receiving much if not all of the information used to determine Medicaid eligibility, which under the ACA will increasingly be under marketplaces’ control or obtained through eligibility services subject to marketplaces’ constraints. Much of that information includes data from the Federal Data Sharing Hub, which provides a single portal through which health programs can access information from multiple federal agencies as well as other entities with which the federal government contracts.
However, revised regulations published in March 2014 permitted marketplaces to disclose PII for other purposes, so long as applicable requirements are met. The most important of these requirements, for purposes of this paper, are the following:
- The individual who is the subject of the information consents to disclosure;
- HHS determines that the information will be used only for the purposes of and to the extent necessary to ensuring the efficient operation of the marketplace;
- Tax return information the IRS provided the marketplace may be used only to determine eligibility for insurance affordability programs (and thus not for other purposes, including the determination of eligibility for human services programs);24 and
- Privacy and security standards applicable to the recipient of the information are no less stringent than those that apply to the marketplace itself.
The relevant text from the applicable regulation—45 CFR 155.260—is included in Appendix A, along with the key provisions from a cross-referenced statute.
Applying this regulation to the current context, a human services program wishing to use information from a health coverage program to establish or verify eligibility should obtain consent from the person who is seeking to qualify for human services. Such consent might be obtained as part of the standard “boilerplate” contained in human services forms for application and renewal. However, the human services program may have a stronger case supporting its request for information from the exchange if it could demonstrate that it will obtain consumer consent that goes beyond the “pro forma” level.
Human services programs will also need to explain why providing them with access to PII will help marketplaces function more efficiently. At least two arguments seem reasonable on this count:
- If a marketplace does not provide the human services program with direct access to PII relevant to an applicant’s eligibility for human services, the human services program could ask the applicant for a written record, from the marketplace, showing the same information. In that case, the marketplace would be legally required to provide such a written record, upon the applicant’s request.25 That would be more costly to the marketplace than providing the human services program with direct access to PII via data matching.
- If the marketplace provides the human services program with direct access to PII that helps the program verify eligibility, the human services program could agree, in return, to provide the marketplace with access to the program’s own eligibility records to help the marketplace verify eligibility for insurance affordability programs. That exchange of information would help the marketplace carry out its core eligibility determination functions more effectively and efficiently.
Finally, human services programs will need to enter into agreements with marketplaces specifying the circumstances of data exchange, storage, and use, assuring that all relevant legal requirements will be satisfied. Federal officials could consider providing technical assistance to facilitate this process, perhaps including the development of model contractual terms. That assistance could also shape the disclosure to take into account any limitations that may be imposed by agreements between CMS and the source agencies that provide information to the Federal Data Sharing Hub.
Going beyond the legal documents, however, it may prove challenging for human services programs that operate outdated, legacy systems to meet 21st-century requirements for data security and confidentiality. Each program will need to carefully assess the roles it is able to assume and the steps it will need to take to safeguard the data it receives under these agreements.
Medicaid records. Human services programs could seek to obtain information from Medicaid programs directly, including final determinations of FPL and eligibility. In this context, several federal statutes could be helpful. First, Social Security Act §1137(a)(4)(A) provides that the state agencies administering Medicaid, TANF, SNAP, unemployment insurance, and various other programs listed in §1137(b), “will exchange with each other information in their possession which may be of use in establishing or verifying eligibility or benefit amounts under any other such program.” This appears to authorize a Medicaid program to provide information from a consumer’s Medicaid records, including information about the Medicaid eligibility determination and final conclusion about an individual’s FPL, to a state agency administering another program listed in Section 1137 if the latter agency believes the information may be of use in establishing or verifying the person’s eligibility or benefit amounts for such other program.
Section 1137(a)(4)(B) also requires Medicaid and the other listed programs to make information available to child support enforcement agencies. Other provisions of §1137 require safeguards to prevent unauthorized disclosure and to ensure that consumers receive notice of possible disclosure at the time of application and periodically thereafter.26
The second relevant statute is Social Security Act §1902(a)(7)(A), which requires Medicaid programs to “provide safeguards which restrict the use or disclosure of information concerning applicants and recipients to purposes directly connected with the administration of the plan.” Arguments like those discussed above in connection with the efficient operation of the marketplace might apply here. Namely, if a Medicaid program provides a human services program with direct access, via data exchange, to Medicaid eligibility information, that could allow more efficient operation of the Medicaid program, since it would eliminate the need for Medicaid to provide written print-outs of that same information to consumers upon their request, for the consumers to take to the human services program in documenting eligibility. And by offering data to help human services programs determine eligibility, Medicaid could obtain similar information from human services programs to help Medicaid determine eligibility.
These arguments may be considerably strengthened if the Medicaid program provides access to this information with the consent of the affected individual. In that case, disclosure serves the privacy interests of the individual by allowing the individual to determine what happens to his or her personal information.
The Health Insurance Portability and Accountability Act of 1996 (HIPAA) does not prevent health programs from sharing relevant eligibility-related information with human services programs. HIPAA regulations specify that protected health information, normally subjected to privacy controls under HIPAA, may be disclosed in the following circumstances:
“A covered entity that is a government agency administering a government program providing public benefits may disclose protected health information relating to the program to another covered entity that is a government agency administering a government program providing public benefits if the programs serve the same or similar populations and the disclosure of protected health information is necessary to coordinate the covered functions of such programs or to improve administration and management relating to the covered functions of such programs.”27
Accordingly, HIPAA should not bar a Medicaid program from disclosing information from a person’s Medicaid eligibility files, including information about a person’s Medicaid eligibility determination, to an agency administering a different program if (a) Medicaid and that other program serve overlapping populations; (b) the information demonstrates that the individual probably falls within the overlapping population; and (c) disclosure of the information would improve the coordination, administration, and management of one or both programs.
Addressing differences between program rules for health and human services programs
Health and human services programs may use different rules for determining eligibility, including:
- Different definitions of the household members whose needs and resources are considered in determining eligibility;
-
Different methods for valuing or counting income or assets; and
-
Different deductions or disregards that are subtracted from “gross” income to determine the “net” income levels used to decide final eligibility or benefit levels.
- Medicaid records could establish, verify, or confirm non-financial eligibility. When Medicaid uses definitions and verification procedures that are at least as stringent as those employed by the human services program, a finding of Medicaid eligibility should suffice to establish that the household meets the applicable requirement for purposes of the human services program. Examples of such non-financial factors include—
- Citizenship or qualified alien status;
- State residence; and
- Non-incarceration.
- The human services program could “deem” someone eligible based on their receipt of Medicaid, notwithstanding differences in the technical details of the two program’s eligibility rules. WIC already does this by granting so-called “adjunctive eligibility” whenever an applicant has already been found eligible for Medicaid. As another example, the National School Lunch Program is conducting pilot projects under which children automatically qualify for free school lunches, without any need to conduct separate income determinations, if Medicaid has already found that they have family income at or below 133 percent FPL.29 (Federal law is more likely to permit rule changes along these lines in a human services program that operates pursuant to a federal block grant than with uncapped funds, since block grant programs typically provide states with considerable flexibility in defining eligibility criteria.)
- As one variant of the “deeming” approach, a human services program could deem eligibility only for limited purposes where the program finds it particularly warranted. For example, LIHEAP might grant automatic financial eligibility for crisis assistance, but not for other forms of aid, when households have been found eligible for Medicaid based on income at or below 138 percent FPL.
- A human services program could change its rules to more closely resemble those applied by Medicaid under MAGI principles. Such a program could automatically grant eligibility and at least interim benefit levels based on Medicaid’s eligibility determinations.
- A human services program may value, for policy reasons, income disregards that are not included in the MAGI income determination. Such a program could inform households that they may be able to obtain more generous benefits or a more favorable eligibility determination by providing information showing they qualify for such income disregards. As a result, if behavioral factors prevent a household from providing this information, at least the household will receive human services benefits based on the Medicaid eligibility determination. But a household that is willing and able to demonstrate qualification for an applicable income disregard can do so and obtain additional assistance.
- A human services program could likewise prefer to retain its traditional household definitions, rather than move to those used for federal tax purposes. Among other reasons, that may avoid exposure to increased benefit costs, depending on the state and the benefit program. In such cases, officials could simply decide that they will incorporate MAGI income counting and income deduction rules. For households that are defined in the same way both by MAGI rules and by the human services program—which will often mean that they consist of parents, step-parents, adoptive or foster parents, and/or their minor children living together—the Medicaid eligibility determination will suffice to establish eligibility and benefit levels for the human services program. With other household types, additional work will be required to build on Medicaid’s findings and reach a determination of human services eligibility.
- Medicaid’s records could provide specific information that is used to automatically pre-populate an application form for human services benefits. Examples of such information include address and social security number. Other information, such as that contained in payroll records, quarterly wage records, or state tax records already obtained by the Medicaid agency, could help verify eligibility for the human services program, sparing the latter program the need to seek out that same information.
- Information in an applicant’s Medicaid records could either confirm attestations in a human services application or raise “red flags” suggesting a need for further verification—in either case, safeguarding program integrity for the human services program.
Which (if any) of these strategies is most useful will depend on the specific circumstances facing the human services program, including the state in which it operates.
Conclusion
Human services programs could gain significant rewards from integrating and coordinating their eligibility systems with those operated by health programs. In the near term, generous federal funding is available for systems modernization needed by health programs, without any obligation for human services programs to share in those costs, even if they benefit from the investment. In the medium term, health programs are likely to serve more low-income households than any other need-based program, particularly in states that expand Medicaid. They will thus garner information about the vast majority of applicants for and recipients of human services benefits, creating opportunities to leverage that information for human services programs to streamline enrollment procedures, save administrative costs, strengthen program integrity, and improve benefits access by trimming clients’ paperwork burdens.About the authors and acknowledgments
Stan Dorn and Rebecca Peters are a senior fellow and research associate, respectively, at the Urban Institute Health Policy Center. The authors appreciate the financial support of the Office of the Assistant Secretary for Planning and Evaluation and well as the substantive guidance of our project officer, Alana Landey. The authors are also grateful for the feedback provided by Brigette Courtot of the Urban Institute; Jessica Kahn of CMS; Rick Friedman, formerly of CMS and currently an independent consultant and adviser to American Public Human Services Association; and the Technical Working Group for this project, the members of which are listed in Appendix B. Neither those individuals, ASPE, nor the Urban Institute are responsible for the opinions expressed in this report, which are the authors’.Appendix A: Excerpts from final text of 45 CFR §155.260 and ACA §1411
45 CFR §155.260 Privacy and security of personally identifiable information.
(a) Creation, collection, use and disclosure.
(1) Where the Exchange creates or collects personally identifiable information for the purposes of determining eligibility for enrollment in a qualified health plan; determining eligibility for other insurance affordability programs, as defined in §155.20; or determining eligibility for exemptions from the individual responsibility provisions in section 5000A of the Code, the Exchange may only use or disclose such personally identifiable information to the extent such information is necessary:
(i) For the Exchange to carry out the functions described in §155.200;
(ii) For the Exchange to carry out other functions not described in paragraph (a)(1)(i) of this section, which the Secretary determines to be in compliance with section 1411(g)(2)(A) of the Affordable Care Act and for which an individual provides consent for his or her information to be used or disclosed; or
(iii) For the Exchange to carry out other functions not described in paragraphs (a)(1)(i) and (ii) of this section, for which an individual provides consent for his or her information to be used or disclosed, and which the Secretary determines are in compliance with section 1411(g)(2)(A) of the Affordable Care Act under the following substantive and procedural requirements:
(A) Substantive requirements. The Secretary may approve other uses and disclosures of personally identifiable information created or collected as described in paragraph (a)(1) of this section that are not described in paragraphs (a)(1)(i) or (ii) of this section, provided that HHS determines that the information will be used only for the purposes of and to the extent necessary in ensuring the efficient operation of the Exchange consistent with section 1411(g)(2)(A) of the Affordable Care Act, and that the uses and disclosures are also permissible under relevant law and policy.
(B) Procedural requirements for approval of a use or disclosure of personally identifiable information. To seek approval for a use or disclosure of personally identifiable information created or collected as described in paragraph (a)(1) of this section that is not described in paragraphs (a)(1)(i) or (ii) of this section, the Exchange must submit the following information to HHS:
(i) Individual access. Individuals should be provided with a simple and timely means to access and obtain their personally identifiable information in a readable form and format;
(ii) Correction. Individuals should be provided with a timely means to dispute the accuracy or integrity of their personally identifiable information and to have erroneous information corrected or to have a dispute documented if their requests are denied;
(iii) Openness and transparency. There should be openness and transparency about policies, procedures, and technologies that directly affect individuals and/or their personally identifiable information;
(iv) Individual choice. Individuals should be provided a reasonable opportunity and capability to make informed decisions about the collection, use, and disclosure of their personally identifiable information;
(v) Collection, use, and disclosure limitations. Personally identifiable information should be created, collected, used, and/or disclosed only to the extent necessary to accomplish a specified purpose(s) and never to discriminate inappropriately;
(vi) Data quality and integrity. Persons and entities should take reasonable steps to ensure that personally identifiable information is complete, accurate, and up-to-date to the extent necessary for the person's or entity's intended purposes and has not been altered or destroyed in an unauthorized manner;
(vii) Safeguards. Personally identifiable information should be protected with reasonable operational, administrative, technical, and physical safeguards to ensure its confidentiality, integrity, and availability and to prevent unauthorized or inappropriate access, use, or disclosure; and,
(viii) Accountability. These principles should be implemented, and adherence assured, through appropriate monitoring and other means and methods should be in place to report and mitigate non-adherence and breaches.
(4) For the purposes of implementing the principle described in paragraph (a)(3)(vii) of this section, the Exchange must establish and implement operational, technical, administrative and physical safeguards that are consistent with any applicable laws (including this section) to ensure—
(i) The confidentiality, integrity, and availability of personally identifiable information created, collected, used, and/or disclosed by the Exchange;
(ii) Personally identifiable information is only used by or disclosed to those authorized to receive or view it;
(iii) Return information, as such term is defined by section 6103(b)(2) of the Code, is kept confidential under section 6103 of the Code;
(iv) Personally identifiable information is protected against any reasonably anticipated threats or hazards to the confidentiality, integrity, and availability of such information;
(v) Personally identifiable information is protected against any reasonably anticipated uses or disclosures of such information that are not permitted or required by law; and
(vi) Personally identifiable information is securely destroyed or disposed of in an appropriate and reasonable manner and in accordance with retention schedules;
(5) The Exchange must monitor, periodically assess, and update the security controls and related system risks to ensure the continued effectiveness of those controls.
(6) The Exchange must develop and utilize secure electronic interfaces when sharing personally identifiable information electronically.
(b) Application to non-Exchange entities.
(1) Non-Exchange entities. A non-Exchange entity is any individual or entity that:
(i) Gains access to personally identifiable information submitted to an Exchange; or
(ii) Collects, uses, or discloses personally identifiable information gathered directly from applicants, qualified individuals, or enrollees while that individual or entity is performing functions agreed to with the Exchange.
(2) Prior to any person or entity becoming a non-Exchange entity, Exchanges must execute with the person or entity a contract or agreement that includes:
(i) A description of the functions to be performed by the non-Exchange entity;
(ii) A provision(s) binding the non-Exchange entity to comply with the privacy and security standards and obligations adopted in accordance with paragraph (b)(3) of this section, and specifically listing or incorporating those privacy and security standards and obligations;
(iii) A provision requiring the non-Exchange entity to monitor, periodically assess, and update its security controls and related system risks to ensure the continued effectiveness of those controls in accordance with paragraph (a)(5) of this section;
(iv) A provision requiring the non-Exchange entity to inform the Exchange of any change in its administrative, technical, or operational environments defined as material within the contract; and
(v) A provision that requires the non-Exchange entity to bind any downstream entities to the same privacy and security standards and obligations to which the non-Exchange entity has agreed in its contract or agreement with the Exchange.
(3) When collection, use or disclosure is not otherwise required by law, the privacy and security standards to which an Exchange binds non-Exchange entities must:
(i) Be consistent with the principles and requirements listed in paragraphs (a)(1) through (6) of this section, including being at least as protective as the standards the Exchange has established and implemented for itself in compliance with paragraph (a)(3) of this section;
(ii) Comply with the requirements of paragraphs (c), (d), (f), and (g) of this section; and
(iii) Take into specific consideration:
(A) The environment in which the non-Exchange entity is operating;
(B) Whether the standards are relevant and applicable to the non-Exchange entity's duties and activities in connection with the Exchange; and
(C) Any existing legal requirements to which the non-Exchange entity is bound in relation to its administrative, technical, and operational controls and practices, including but not limited to, its existing data handling and information technology processes and protocols.
(f) Compliance with the Code. Return information, as defined in section 6103(b)(2) of the Code, must be kept confidential and disclosed, used, and maintained only in accordance with section 6103 of the Code.
(g) Improper use and disclosure of information. Any person who knowingly and willfully uses or discloses information in violation of section 1411(g) of the Affordable Care Act will be subject to a civil penalty of not more than $25,000 per person or entity, per use or disclosure, in addition to other penalties that may be prescribed by law.
ACA Section 1411. Procedures for determining eligibility for Exchange participation, premium tax credits and Reduced cost-sharing, and individual responsibility exemptions.
(g) CONFIDENTIALITY OF APPLICANT INFORMATION.—
(1) IN GENERAL.—An applicant for insurance coverage or for a premium tax credit or cost-sharing reduction shall be required to provide only the information strictly necessary to authenticate identity, determine eligibility, and determine the amount of the credit or reduction.
(2) RECEIPT OF INFORMATION.—Any person who receives information provided by an applicant under subsection (b) (whether directly or by another person at the request of the applicant), or receives information from a Federal agency under subsection (c), (d), or (e), shall—
(A) use the information only for the purposes of, and to the extent necessary in, ensuring the efficient operation of the Exchange, including verifying the eligibility of an individual to enroll through an Exchange or to claim a premium tax credit or cost-sharing reduction or the amount of the credit or reduction; and
(B) not disclose the information to any other person except as provided in this section.
Appendix B. Members of the Technical Working Group
Federal Officials
- HHS
- Susan Golonka, ACF/OFA
- Vicki Turetsky (along with Jennifer Burnszynski), ACF/OCSE
- Mark Fucello, ACF/OPRE
- Rochelle Rollins, advisor to the Chief Medical Officer, ACF
- Jeannie Chaffin, ACF/OCS
- Suma Nair, HRSA/Bureau of Primary Care Ben O’Dell and
- Lisa Carr, Center for Partnerships
- Gregorio Hunt, OIEA
- Elizabeth Hadley and Christie Peters, ASPE/Office of Health Policy
- Donna Cohen Ross, CMS/CMCS
- USDA/FNS
- Kathryn Law, Office of Policy Support
- SSA
- Craig Streett, Office of Income Security Programs
Craig Streett, Office of Income Security Programs
Louisiana
- Ruth Kennedy, Medicaid director
Nongovernmental Members
Notes
1 Stan Dorn, Julia Isaacs, Sarah Minton, Erika Huber, Paul Johnson, Matthew Buettgens, and Laura Wheaton. “Overlapping Eligibility and Enrollment: Human Services and Health Programs Under the Affordable Care Act.” Washington, DC: Prepared by the Urban Institute for the Assistant Secretary for Planning and Evaluation, DHHS, December 2013.
2 Letter from Cindy Mann, CMCS/CMS/HHS, Kevin Concannon, FNS/USDA, George Sheldon, ACF/HHS, and Steve Larsen, CCIIO/CMS/HHS, to State Exchange Grantees, Medicaid and CHIP Directors, and Health and Human Services Directors, August 10, 2011, http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Data....
3 Section 1413(c)(3)(A) of the ACA requires that “to the maximum extent practicable” Medicaid and other health programs must “establish, verify, and update eligibility” based on data matches. See also Centers for Medicaid and CHIP Services (CMCS). April 19, 2012. Medicaid and CHIP in 2014: A Seamless Path to Affordable Coverage: Application, Verification and Renewals. http://www.medicaid.gov/State-Resource-Center/Downloads/4-19-12-Applicat... (Medicaid and CHIP in 2014). Legislation signed by the President following the ACA’s enactment required that: (a) before tax credits and cost-sharing reductions for marketplace coverage were made available, the HHS Secretary was obliged to certify to Congress that eligibility for such subsidies was being verified; (b) by January 1, 2014, the Secretary was required to submit a report to Congress that detailed how eligibility for those subsidies was being verified; and (c) by July 1, 2014, the HHS Office of Inspector 21 General must submit a report to Congress describing the effectiveness of “procedures and safeguards… for preventing the submission of inaccurate or fraudulent information by applicants” for marketplace coverage. Section 1001 of the Continuing Appropriations Act of 2014, H.R. 2775, First Session, 113th Congress, http://www.gpo.gov/fdsys/pkg/BILLS-113hr2775enr/pdf/BILLS-113hr2775enr.pdf.