
U.S. Department of Health and Human Services
Gauging the Use of HCBS Supports Waivers for People with Intellectual and Developmental Disabilities: Final Project Report
Gary Smith, John Agosta, Jon FortuneHuman Services Research Institute
Janet O'KeeffeRTI International
April 2007
PDF Version (47 PDF pages; 231 PDF pages total report)
This report was prepared under contract #HHS-100-03-0025 between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and the Research Triangle Institute. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the office at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. The email address is: webmaster.DALTCP@hhs.gov. The project officer was Linda Bergofsky.
The opinions expressed in this report do not necessarily reflect the views of the U.S. Department of Health and Human Services or RTI International.
TABLE OF CONTENTS
I. INTRODUCTION
Study Scope
Report Overview
II. METHODS
State Profiles
Case Studies
III. HCBS FOR PEOPLE WITH I&DD
Persons with I&DD
HCBS Waivers for People with I&DD
Effect of Increasing Service Demand on States
Federal Policy Factors
IV. OVERVIEW OF SUPPORTS WAIVERS
Defining Characteristics of Supports Waivers
Number of States Operating Supports Waivers
Age Groups Served
Funding Limits
Utilization: Supports Waiver Expenditure v. Funding Limit
Supports Waiver Service Coverage
Consumer/Self-Direction
Number of Individuals Participating in Supports Waiver
Trends in Total HCBS Waiver Expenditures
Expenditures Per Waiver Participant
Variance Across States in Per Person Spending
State Waiting Lists
Policy Goals
Waiver Operations
Waiver Impacts on State Systems
Key Issues in the Operation of Supports Waivers
VI. SUPPORTS WAIVERS: IMPACT AND CONTINUING CHALLENGES
Observations About the Impact of Supports Waivers
Challenges in the Operation of Supports Waivers
Concluding Observations
APPENDIX A. STATE-BY-STATE SUPPORTS WAIVER PROFILES (separate file)
Content of State Supports Waiver Profiles
APPENDIX B. STATE-BY-STATE CASE STUDY RESULTS (separate file)
APPENDIX C. CASE STUDY DISCUSSION GUIDES (separate file)*
Support Waivers for People with Intellectual and Developmental Disabilities: Core Elements Protocol
Support Waivers for People with Intellectual and Developmental Disabilities: Case Study Discussion Protocol
*This appendix is current available only as a PDF document at http://aspe.hhs.gov/daltcp/reports/2007/gaugingfr-appendC.pdf. [You will need a copy of the Acrobat Reader in order to view this document.]
LIST OF CHARTS
CHART 1: Supports and Comprehensive Waiver Enrollment 2000-2006
CHART 2: Comprehensive and Supports Waiver Expenditures Trends 2000-2006
CHART 3: Average Annual Expenditures Per Participant 2000-2006
LIST OF TABLES
TABLE 1: States Operating Supports Waivers
TABLE 2: Supports Waiver Expenditures and Funding Limits
TABLE 3: Supports Waiver Service Coverage
TABLE 4: State-by-State Average Comprehensive and Supports Waiver Expenditures per Participant
TABLE A-1: Support Waiver Service Categories and Services/Activities
I. INTRODUCTION
The per person cost of furnishing Medicaid home and community-based services (HCBS) to people with intellectual and other developmental disabilities (I&DD)1 is significantly higher than the cost of serving other target populations (e.g., older persons, younger persons with physical disabilities) and state I&DD systems are experiencing substantial annual increases in service demand. As a result, in recent years, a growing number of states have launched what have commonly come to be termed supports waivers for persons with I&DD.
These Medicaid waivers operate under the authority of §1915(c) of the Social Security Act that authorizes a state to furnish HCBS to persons who otherwise require the level of care that is furnished in a Medicaid-reimbursable institution. Seventeen states now operate supports waivers side-by-side with the traditional comprehensive waivers that provide more extensive services, including licensed residential services furnished outside the family home. The per waiver participant cost in comprehensive waivers is substantially greater than in supports waivers.
- A relatively low dollar cap on the total amount of HCBS waiver services that may be authorized on behalf of a beneficiary.
- Flexibility in the selection of services within the dollar cap.
- The expectation that unpaid family caregivers will provide significant support to waiver participants.
Supports waivers are designed to complement the unpaid supports that are provided to individuals with I&DD by family caregivers. Compared to the waivers that have traditionally provided services to this population, supports waivers impose relatively low dollar limitations on the total amount of HCBS that may be authorized for waiver participants. These dollar limitations are significantly lower than the costs of institutional services. Within the dollar limitation, individuals and families usually have flexibility in the selection of services and supports.
The use of two distinct HCBS waivers with markedly different cost caps is a new approach to employing the §1915(c) waiver authority to furnish long-term services and supports to people with I&DD. States have expressed various rationales for changing over to a dual or tiered waiver configuration. These include:
-
Reducing the high per person costs of HCBS by avoiding the high costs of furnishing 24/7 residential services and focusing on delivering services and supports in the family home.
-
Leveraging and complementing the supports that are furnished by family caregivers to people with I&DD.
-
Obtaining additional federal Medicaid dollars by leveraging state dollars that underwrite non-residential services in the community, which many states had not formerly covered under Medicaid.
-
Complying with the requirements set forth by the Centers for Medicare & Medicaid Services (CMS) State Medicaid Director Letter #01-006 (a.k.a., Olmstead Letter #4, discussed in more detail later).
-
Expanding services to more economically serve people with I&DD who have been wait-listed for services, sometimes in response to a lawsuit.
In some instances, supports waivers have also served as a vehicle for states to introduce consumer-direction of services into the delivery of Medicaid HCBS for persons with I&DD.
Study Scope
To gain an understanding of how and why states are reconfiguring their HCBS waivers for people with I&DD, the Office of the Assistant Secretary for Planning & Evaluation, U. S. Department of Health & Human Services, sponsored this study in order to compile systematic information about the supports waivers that states operate. This study was conducted by the Human Services Research Institute (HSRI) under subcontract to Research Triangle Institute (RTI).
The aims of this project included:
-
Determining how and why supports waivers have emerged as a means to address the needs of people with I&DD.
-
Compiling systematic descriptive information about the comprehensive and supports waivers for people with I&DD that operate side-by-side in 17 states.
-
Obtaining a better understanding of the range of participant characteristics and experiences that distinguish supports waivers from other HCBS waivers for people with I&DD.
-
More fully understanding how states view supports waivers as a strategic tool to address the need for HCBS.
Report Overview
This report contains the following major sections:
-
Methods. This section briefly describes how the information contained in this report was obtained and compiled.
-
HCBS for People with I&DD. This section provides background information concerning the role that Medicaid HCBS waivers play in supporting people with I&DD, critical factors affecting state I&DD service systems that have spurred the implementation of supports waivers, and federal Medicaid policies that affect how states use Medicaid HCBS waivers.
-
Overview of Supports Waivers. This section provides descriptive information about the supports waivers that are presently operating.
-
Summary of Case Studies. This section synthesizes information gleaned from case studies of six states that operate supports waivers.
-
Impact of Supports Waivers. This section presents observations about the impact that supports waivers appear to be having on the delivery of Medicaid waiver services to people with I&DD and identifies some of the issues that have emerged around the use of these waivers.
-
Appendix A: State Supports Waiver Profiles. These profiles present detailed information about the supports waivers operated by the 17 states.
-
Appendix B: Case Studies. This Appendix contains state-by-state results of the six case studies conducted by HSRI. The discussion protocols used to conduct these case studies are contained in Appendix C.
II. METHODS
This study entailed two major data collection activities. The first was to compile systematic profiles of the supports waivers that are operating in 17 states. The second was to conduct follow-up inquiries to complete more in-depth case studies of six states that operate supports waivers.
State Profiles
At the outset of the study, we identified 17 states operating supports waivers:
| AlabamaColoradoConnecticut FloridaIndiana | LouisianaMissouriMontanaNebraska | OhioOklahomaOregonPennsylvania | South Dakota TennesseeTexasWashington |
HSRI designed a computer-based template and a database to compile and sort a standard set of information about the HCBS waivers operating in each of these 17 states. This template and database were designed to capture consistent and comparable information about each state and to document a variety of defining characteristics of each states supports waiver (e.g., services offered, descriptive features, number of participants and associated costs by year, extent of consumer-direction, and text notes related to particular topics). This information was also used to aggregate information across the 17 states.
From January through December 2006, information was compiled on each state and its HCBS waivers for people with I&DD. Our actions included:
-
Contacting state staff to acquire CMS approved or submitted waiver documents, CMS 372 annual waiver statistical reports, relevant state documents, and other applicable reports.
-
Acquiring electronic information available at state websites.
-
Reviewing the national I&DD data sets compiled by the Research and Training Center on Community Living, Institute on Community Integration/ University Centers for Excellence in Developmental Disabilities at the College of Education & Human Development at the University of Minnesota.
-
Reviewing an earlier report on the supports waivers compiled by the National Association of State Directors of Developmental Disability Services.
Every effort was made to acquire the most up-to-date and accurate information about supports waivers. Where information from one source did not match with that from another or information was outdated, state officials were contacted to reconcile the differences in the data sets or acquire more current information. An initial set of state profiles was prepared. HSRI continually updated the database as the project progressed. The 17 state profiles are located in Appendix A of this report.
Case Studies
The project case studies were completed in three steps. First, six states were selected to explore more thoroughly--Florida, Missouri, Oklahoma, Oregon, Pennsylvania, and Tennessee. In selecting these states, the following factors were taken into account:
- length of time the supports waiver(s) had been in operation;
- services offered;
- self-direction features;
- the number of people enrolled in state comprehensive and supports waivers;
- the level of waiver spending; and
- trends in both enrollment and spending.
Second, two discussion guides were prepared. These guides are in Appendix C. The Core Elements Protocol was designed to gather from state officials supplementary detailed information concerning how the states HCBS waivers for people with I&DD are structured and operate. The Case Study Discussion Protocol guided discussions with selected key state informants about the waivers. These protocols addressed topics such as:
-
The policy goals that underpin the waiver(s) (e.g., reducing wait-lists, containing spending, redirecting service budgets, promoting consumer-directed approaches, and others).
-
Descriptive information on waiver utilization and waiting lists.
-
Operational elements related to program eligibility and access, individual budget allocations, service planning, service use, and quality assurance.
-
Opinions about how the waivers are functioning, their impact, and how they might be improved.
HSRI then identified key informants in each of the six states. HSRI sought to identify individuals who were familiar with the operation of the supports waiver. Consultations with state HCBS waiver operating agency personnel were essential to collect more in-depth information about various aspects of waiver operations. Such individuals included the state director of developmental disability services and the individual(s) responsible for HCBS waiver operations.
In addition to these informants, HSRI also identified individuals with varying perspectives who would be knowledgeable about the waivers and their impact. Depending on the state, HSRI talked with representatives from the Administration on Developmental Disabilities network (i.e., developmental disabilities planning councils, protection and advocacy agencies, university-based centers of excellence), the advocacy community (e.g., state ARC representatives, family advocacy groups), and the service delivery network (e.g., representatives of provider associations, case managers, planning agents or brokers).
On average, HSRI had discussions with 11 informants in each state. Discussions were conducted by telephone with four states--Missouri, Oklahoma, Pennsylvania, and Tennessee--and in-person during site visits to Oregon and Florida. HSRI completed the discussions and site visits between August and October 2006. The state-by-state results of these case study discussions are in Appendix B.
HSRI and RTI express their appreciation to the state officials and other key informants who generously provided both information and insight into the operation of supports waivers for people with I&DD.
III. HCBS FOR PEOPLE WITH I&DD
This section provides background information concerning the role that Medicaid HCBS waivers play in supporting people with I&DD. First, information is presented about the characteristics and prevalence of I&DD. This is followed by a summary explanation of how HCBS waivers are employed to provide services to people with I&DD. Finally, factors are identified that are prompting states to design and implement supports waivers.
- Autism
- Behavior disorders
- Brain injury
- Cerebral palsy
- Down syndrome
- Fetal alcohol syndrome
- Spina Bifida
Persons with I&DD
There are nearly five million children and adults with I&DD in the United States or 1.58 percent of the general population.2 The term intellectual disability has replaced mental retardation to describe individuals who have a significant mental or intellectual impairment that begins at birth. The term developmental disabilities refers to other conditions that are manifested after birth but before age 22 and are attributable to a mental or physical impairment or a combination of both types of impairments. I&DD are life-long. People with I&DD have one or more major functional limitations and often require assistance in one or more Activities of Daily Living and/or Instrumental Activities of Daily Living. Individuals with substantial mental and/or physical impairments may require daily or around-the-clock assistance, including supervision to assure safety.
The prevalence of I&DD is increasing. More infants with severe disabilities are surviving at birth and people with I&DD are living longer. Due to better health care, the longevity of people with I&DD has trended upward along with that of the general population. Most people with I&DD (including adults) live with family members who provide unpaid care and support.3 The increasing longevity of people with I&DD has resulted in a growing cohort of individuals who live with aging caregivers who are over age 60; about one-quarter of persons with I&DD have an aging primary caregiver.4 In 2005, state I&DD service delivery systems provided residential services outside the family home to approximately 411,000 individuals; another 30,000 individuals resided in nursing facilities.5 About 500,000 people who live with their families received services through state I&DD service systems. Public systems support approximately 21 percent of people with I&DD.
Once dominated by the provision of services in large state-operated institutions, state I&DD service systems are now primarily community-based. These systems predominantly serve adults with I&DD by furnishing a mix of residential, out-of-home day supports, supported employment, and home-based services.
HCBS Waivers for People with I&DD
Section 1915(c) of the Social Security Act permits a state to obtain federal financial participation in the cost of furnishing HCBS to Medicaid-eligible individuals who require the level of care furnished in a Medicaid-reimbursable institutional setting (i.e., a hospital, nursing facility, or an intermediate care facility for the mentally retarded (ICF/MR)). A state must obtain approval from CMS to operate an HCBS waiver and periodically request CMS approval to continue the operation of a waiver. HCBS waivers serve state-specified target populations. A state must ensure that its waiver is cost-neutral: that is, the average per person cost of furnishing HCBS to waiver participants will be no greater than the average cost of serving such persons in the institutional setting to which the waiver serves as an alternative.
States have flexibility in selecting the types of HCBS that they offer through a waiver. A state may offer services that it could not otherwise provide under its Medicaid state plan or has elected not to cover under its state plan. Waiver participants also have access to the full range of services available through a states basic Medicaid program. States have the authority to limit the number of persons who may participate in a waiver. Once a waivers enrollment limit is reached, a state may place individuals on a waiting list for future enrollment.
With respect to individuals with I&DD, waiver HCBS may be furnished to persons who require the level of care in an ICF/MR. ICFs/MR include state-operated institutions, large private facilities, and smaller group home settings. ICF/MR services may be furnished to individuals with an intellectual disability who have substantial limitations and persons with related conditions.
The term related condition is defined in 42 CFR 435.1009. Related conditions include cerebral palsy, epilepsy, and any other condition (except mental illness) that results in the impairment of intellectual function or adaptive behavior similar to the impairments that stem from intellectual disability (mental retardation). The related condition must have been present prior to age 22 and result in substantial functional limitations. Common related conditions include autism and traumatic brain injury.6
In order to qualify for waiver enrollment, individuals must also meet basic Medicaid eligibility tests, including financial eligibility and a determination that the person has a qualifying disability (e.g., the person meets the disability tests under Titles II and XVI of the Social Security Act). The combination of financial and disability-related eligibility criteria reduces the number of people with I&DD (especially children) who can qualify for Medicaid.
Since the 1981 enactment of the federal Medicaid HCBS waiver authority, states have employed HCBS waivers extensively to underwrite the costs of community services and supports for people with I&DD. The use of the HCBS waiver authority as a financing tool for community services for people with I&DD accelerated during the 1990s and has continued to grow over the past several years. In 2005, federal-state expenditures for waiver HCBS provided to persons with I&DD totaled $17.0 billion.7 Nationwide, states furnished waiver services to 443,608 persons with I&DD at an annual cost of $39,627 per waiver participant.8 Between 2000 and 2005, the number of individuals with I&DD participating in HCBS waivers increased by approximately 50 percent.
HCBS waivers for people with I&DD typically include the provision of case management/service coordination, residential services, day supports (facility-based habilitation programs), employment supports, personal care/personal assistance, respite, transportation, and clinical services. In 2005, about 45 percent of HCBS waiver participants with I&DD resided in the family home. Typically, however, the majority of state HCBS waiver expenditures underwrite the costs of furnishing residential services outside the family home.
States rely heavily on HCBS waivers to finance community services for people with I&DD. HCBS waivers have aided states to avoid the high cost of ICF/MR services,9 permitted them to leverage federal Medicaid dollars to underwrite the costs of community services that states commonly provide to people with I&DD, and take advantage of the underlying flexibility of the waiver authority to support individuals in a variety of community settings.
State use of the HCBS waiver authority has resulted in a decline in the utilization of institutional ICF/MR services. Between 1990 and 2005, the average daily population in large state-operated I&DD facilities was reduced by half nationally and in most states. In 2005, only 101,821 persons with I&DD were served in ICFs/MR in contrast to 146,657 in 1991.10 In 2005, about 77 percent of all persons with I&DD who received Medicaid-financed long-term services were supported through the Medicaid HCBS waiver authority.
HCBS waivers for people with I&DD account for a disproportionate share of total nationwide waiver expenditures for all populations. For example, in 2003, people with I&DD made up 40.4 percent of all HCBS waiver participants nationwide but accounted for 74.8 percent of all waiver expenditures.11 In 2005, HCBS waiver expenditures for people with I&DD accounted for 75 percent of all HCBS waiver expenditures for all populations. Expenditures per waiver participant with I&DD are substantially higher than per person expenditures for waivers that serve other target populations (e.g., older persons and working age adults with non-developmental disabilities).12
The relatively high costs of furnishing HCBS to people with I&DD is attributable to several factors, primarily the nature of their disabilities, which often require the provision of continuous personal assistance and supervision in licensed community residences. Individuals with I&DD also typically receive day habilitation services.
Effect of Increasing Service Demand on States
One of the most notable factors affecting states is the rising expressed demand for I&DD services. While the number of people with I&DD receiving Medicaid waiver HCBS has increased substantially since 2000, many states have seen their waiting lists for HCBS continue to grow rapidly. For example, starting in 1999, Florida doubled the number of people served through its HCBS waiver for people with I&DD from 12,000 to 25,000, in order to reduce its waiting list. However, more and more people are seeking services and the states waiting list for services has climbed to about 12,000 individuals. In Texas, the states interest list for I&DD services has reached 46,000 persons and continues to grow each month.
While there are no reliable comprehensive nationwide data regarding the total number of people with I&DD who are wait-listed for HCBS, the clear trend among the states has been for service demand to grow at a faster pace than the rate at which states have been able to expand service system capacity. Service demand also appears to be growing at a rate greater than underlying general population growth. In many states, the amount of time that people are spending on waiting lists exceeds three or more years. In several states, people who are wait-listed include individuals who are characterized as having emergency or critical needs.
In many states, the expansion of HCBS waivers for people with I&DD involved shifting the financing of services from programs supported only with state funds to Medicaid funding. Thus, in some states, the expansion of HCBS waivers did not result in a net increase in the number of individuals served. State budget problems earlier in this decade spurred this refinancing while also limiting the extent to which many states could respond to rising demand. The growing number of people with I&DD on waiting lists is also the byproduct of longer-term underlying trends, including increased longevity (which results in lower turnover among people receiving services), and the growing cohort of individuals who live with aging caregivers who over time are less able to provide care.
Twenty-five states have been sued in federal court by persons with I&DD who have been wait-listed for services. Many of these lawsuits have resulted in settlement agreements wherein the state agreed to expand services. More broadly, states are confronted by high and continually rising service demand that will be very costly to meet at the current per person HCBS waiver costs. States also face other cost pressures, including attracting an adequate workforce to provide HCBS.
Supports waivers that operate under relatively low cost maximums represent an effort by several states to address these pressures, that is: (1) reduce waiting lists by providing lower-cost service packages that presume the continued provision of unpaid family caregiver support; and (2) divert demand away from more costly residential services. As discussed in more detail in the next section, supports waivers are designed to complement the supports that family caregivers provide to people with I&DD, including adults.
The premise of supports waivers is that furnishing services to individuals who live with their families will reduce or at least postpone the demand for the costly residential services that have been the mainstay of HCBS waivers for people with I&DD. In their design, supports waivers share some of the same characteristics as waivers for older persons and people with other types of disabilities that rely on caregiver relatives to provide support to the waiver participant. They are not, however, modeled significantly on state family support programs that have traditionally served children living at home.
Federal Policy Factors
The emergence of supports waivers for people with I&DD has also been influenced by the evolution of federal policy concerning the operation of HCBS waivers. In particular, the January 2001 issuance of State Medicaid Director Letter #01-006 (a.k.a., Olmstead Letter #4) barred states from operating waivers that restricted some waiver participants to a limited benefit package. CMS policies concerning states authority to impose dollar limits on the amount of waiver services that a person may receive have also evolved.
Olmstead Letter #4.13 Historically, most states operated a single HCBS waiver for people with I&DD. Such waivers provided a comprehensive range of services, ranging from the provision of services and supports in licensed residential settings to services furnished in the family home. In practice, many of these waivers imposed internal capacity controls (i.e., limits on the total number of individuals who may receive specific services) that limited access to the full range of services covered in the waiver. Some states restricted individuals to receiving a smaller package of in-home support services and/or day services but did not allow access to residential and other types of services. Indeed, in some waivers, participants who lived with their families were wait-listed for residential services covered in the waiver.
In January 2001, the Health Care Financing Administration (now CMS) issued State Medicaid Director Letter #01-006 (hereinafter referred to as Olmstead Letter #4). This letter addressed the question of whether a state could operate a single waiver but within the waiver restrict some waiver participants to the receipt of a limited package of waiver services. The letter stated:
A state is obliged to provide all people enrolled in the waiver with the opportunity for access to all needed services covered by the waiver and the Medicaid state plan. Thus, the state cannot develop separate and distinct service packages for waiver population subgroups within a single waiver. The opportunity for access pertains to all services available under the waiver that an enrollee is determined to need on the basis of an assessment and a written plan of care/support.
The effect of Olmstead Letter #4 was to prevent a state from operating what is termed a waiver within a waiver--that is, a waiver that was internally partitioned to control the number of persons who could access certain types of waiver services. In essence, the letter made it clear that, once a person is enrolled in a waiver, the person must be able to obtain any service that is available through the waiver if needed. Olmstead Letter #4 established that a state must provide the full range of waiver services that such individuals might require without respect to budget limitations.
Olmstead Letter #4 has affected how states employ HCBS waivers to support people with I&DD and has spurred the emergence of distinct supports waivers. States interested in furnishing a limited package of waiver services to individuals could no longer operate a carve out limited benefit package within a single waiver. Instead, states would have to design a distinct waiver to cover the limited package. The outcome has been the creation of supports waivers that operate side-by-side with comprehensive waivers, with the latter covering more costly residential services. States can enroll individuals in the less costly supports waiver with less budgetary risk to the state. Capacity limits on both the comprehensive and supports waivers can be used to manage overall HCBS waiver spending.
Individual Cost Limits. A defining characteristic of supports waivers is their imposition of an overall dollar limitation on the amount of services that may be authorized for waiver participants. Changes in federal policy have made it clear that a state may set this dollar limit at a level that is below the average cost of institutional services, providing a basis for states to design and implement supports waivers.
Federal HCBS waiver regulations (42 CFR 441.301(a)(3)) permit a state to restrict enrollment in a waiver to individuals for whom the cost of waiver services is not expected to exceed the cost of serving the person in the Medicaid institutional setting for which the waiver stands as an alternative. That is, a state may elect to refuse the enrollment of a person in a waiver if the expected costs of supporting the person would exceed the average cost of the institutional services for which the person would be eligible.
With respect to HCBS waivers for people with I&DD, states have varied in whether they have imposed an individual cost limit as a condition of waiver enrollment. As a general matter, most states have not imposed such a limit so that they can accommodate individuals who have intensive support needs, including persons transitioning to the community from state public institutions. States that do not impose an individual cost limit manage waiver spending to an aggregate average through the imposition of utilization and cost controls on the services covered by the HCBS waiver. These states are sometimes portrayed as managing to an aggregate limit.
Prior to 2002, CMS permitted states to impose an individual cost limit that was significantly lower than the cost of institutional services. Setting a limit well below the costs of institutional services made it possible for states to exercise great financial control over the costs of waiver services. For example, the Colorado Supported Living Services (SLS) waiver imposed an individual cost limit of $35,000, well below the costs of ICF/MR services.
In 2002, CMS issued the Independence Plus waiver template, which was designed to facilitate the implementation of self-direction of waiver services. However, the template explicitly barred states from imposing an individual cost limit that was less than the cost of institutional services. At the time, CMS determined that such restrictive cost limits were not permitted under federal law.
In order to accommodate states that wished to limit their financial exposure in operating a waiver, CMS offered the alternative of allowing states to impose limitations on the dollar amount of clusters of waiver services that could be authorized. Between 2002 and 2005, CMS approved at least four supports waivers--in Ohio, Tennessee, Texas, and Washington--for people with I&DD that capped the dollar amount of groupings of services and, de facto, permitted a state to cap the total amount of services that would be provided to waiver participants.
In 2005, when revising the HCBS waiver application, CMS decided that the waiver statute in fact permitted setting an individual cost limit less than the cost of institutional services.14 Appendix B-2 of the revised waiver application permits a state to specify an individual cost limit that is less than the cost of institutional services.
Thus, current federal policy gives states the authority to design and implement supports waivers for people with I&DD that cap the dollar amount of services furnished. The ability to target waiver services to specific groups of waiver beneficiaries allows states to design waivers for people who have family caregivers who can furnish support to them and, further, exclude costly residential services from the array of services offered under a waiver.
IV. OVERVIEW OF SUPPORTS WAIVERS
This overview provides summary information about the supports waivers operating in 17 states. Individual state profiles that provide greater detail for each state are found in Appendix A.
Defining Characteristics of Supports Waivers
Supports waivers for people with I&DD generally have the following defining characteristics:
-
Target Population. The target population of these waivers is persons with I&DD who require the level of care furnished in an ICF/MR but who live with their families and do not require licensed residential services. In other words, the target population consists of persons who have access to unpaid supports that can meet a substantial portion of their overall support needs.
-
Dollar Limit. Supports waivers operate under a dollar limit on the total amount of HCBS that may be authorized for a participant. In general, these dollar limits are set at levels substantially below the average cost of serving a person in the states comprehensive waiver or in an ICF/MR.
-
Services. In general, supports waivers include the provision of personal assistance, day services outside the home and supported employment services (for adults) along with other ancillary services (e.g., therapeutic services). Supports waivers exclude the provision of services in licensed residential settings.
-
Service Planning/Authorization. As is the case in any HCBS waiver, the services that participants receive are authorized through a service planning process that determines which services a person may receive.
-
Quality Assurance. Supports waivers are subject to the same federal requirements as all waivers with respect to quality assurance, including periodic monitoring, the identification of issues that may negatively affect the health and welfare of participants, and remediation of such issues.
In some instances, states have incorporated consumer-direction/self-direction features into supports waivers. In the context of Medicaid HCBS waivers, self-direction means that the waiver participant (or a representative) may serve as the common-law employer of direct support workers and/or has the authority to manage an individual budget. The authority to manage an individual budget may include the allocation and reallocation of funds among goods and services and/or directing the provision of services.
Number of States Operating Supports Waivers
Table 1 shows the trend in the number of states operating supports waivers since 2000. In 2000, four states operated five supports waivers; 13 additional states launched supports waivers between 2001 and 2006. At the end of 2006, 17 states operated one or more supports waivers in tandem with a comprehensive HCBS waiver for people with I&DD. As can be seen, there has been steady annual growth in the number of states operating supports waivers since 2000. Colorado was the first state to operate a supports waiver, launching its SLS Waiver in 1995. Georgia has a request pending CMS approval to reconfigure its waivers for people with I&DD into a comprehensive/ supports waiver configuration that will be implemented in 2007. Additional states are developing supports waivers.
| TABLE 1. States Operating Supports Waiver | |||||||
|---|---|---|---|---|---|---|---|
| Through2000 | Implemented after 2000... | ||||||
| 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | ||
| Cumulative Number of States Operating Supports Waivers | 4 | 7 | 8 | 12 | 14 | 17 | 17 |
| States | COOK (2)*PASD | LA (1)MTOR | IN | ALMOOHNE (1) | TXWA (2)* | CTFLTN | NE (2)*LA (2)* |
| Cumulative Number of Supports Waivers in Operation | 5 | 8 | 9 | 13 | 16 | 19 | 21 |
| NOTE: Four states (Lousiana, Oklahoma, Nebraska, Washington) operated two or more supports waivers. Two (Louisiana and Nebraska) began with one and added another later. Two states (Oklahoma and Washington) implemented two supports waivers in the same year. | |||||||
Age Groups Served
Of the 21 supports waivers in operation, three (Louisiana, Oklahoma, and South Dakota) target only children with I&DD. Another seven (in Colorado, Louisiana, Montana, Nebraska, Oklahoma, and Oregon) serve only adults with I&DD. The remaining 11 target both children and adults with I&DD.
Funding Limits
Supports waivers funding limits (i.e., the maximum amount of waiver services that may be authorized on behalf of a waiver participant) range from a low of $5,000 per year (South Dakota) to a high of $52,000 per year (Connecticut). Each states limit is displayed in Table 2. In nine of the 17 states, the funding limit falls in a range between $13,000 and $22,000 per year. The funding limits that apply to supports waivers for children with I&DD tend to be lower than the limits for programs that support adults. These lower limits are due to the availability of the full range of Early and Periodic Screening, Diagnosis, and Treatment Medicaid state plan benefits as well as services funded through education agencies for school-aged children.
In a few states, the funding limit is variable. For example, the Tennessee supports waiver limit is $30,000 but up to an additional $6,000 may be authorized to address short-term emergency needs, a practice that Washington State also uses. In the Oregon supports waiver, the funding limit varies based on difficulty of care factors and family caregiver circumstances. In most states, the funding limit functions as an upper limit on the amount of waiver services that may be authorized. The actual amount of services authorized is based on the individuals waiver support plan and the assessed need for a service.
Some states also impose additional dollar/unit limitations on the amount of particular covered services that may be authorized. For example, in Colorado the total amount of environmental engineering services that may be authorized (which include home modifications, special equipment and supplies, and certain other types of supports) is limited to $10,000 per year.
| TABLE 2. Supports Waiver Expenditures and Funding Limits* | |||
|---|---|---|---|
| State | 2006 Expenditures Per Participant | Funding Limit | Percent of Limit Utilized |
| AL | $8,950 | $18,000 | 49.7% |
| CO | $15,983 | $35,000 | 45.7% |
| CT | $24,443 | $52,000 | 47.0% |
| FL | $8,700 | $14,700 | 59.2% |
| IN | $8,520 | $13,500 | 63.1% |
| LA | $9,225 | $15,000 | 61.5% |
| MO | $4,222 | $22,000 | 19.2% |
| MT | $6,252 | $7,800 | 80.2% |
| NE | $9,158 | $20,000 | 45.8% |
| OK | $9,661 | $18,899 | 51.1% |
| OR | $8,505 | $20,000 | 42.5% |
| PA | $12,738 | $21,200 | 60.1% |
| SD | $4,015 | $5,000 | 80.3% |
| TN | $18,051 | $36,000 | 50.1% |
| TX | $8,669 | $10,000 | 86.7% |
| WA | $13,581 | $19,000 | 71.5% |
| Average | 48.4% | ||
| * Ohio is not included because it does not have a fixed funding limit. | |||
Utilization: Supports Waiver Expenditure v. Funding Limit
Table 2 also shows the average expenditure for waiver services per supports waiver participant versus the annual funding cap for the supports waiver. As can be seen, in all states actual waiver expenditures per participant are below the applicable supports waiver funding limit. The percentage of the funding limit utilized ranged from a low of 19.2 percent in Missouri to a high of 86.9 percent in Texas. On average, actual supports waiver expenditures per participant are slightly less than one-half of the applicable funding limit.
The difference between the maximum amount of funding that may be authorized and actual expenditures per waiver participant likely stems from several factors. In some cases, the amount that is authorized on behalf of a specific waiver participant may be lower than the funding limit based on the persons assessed need for specific services and individual/family choices and preferences. In addition, some states impose additional limits on the amount that may be authorized for specific services. Other factors include staff scheduling problems and consumer absences. A relatively common complaint voiced by individuals and families is that they frequently experience difficulty in locating providers to furnish the services that have been authorized in their waiver service plans.
It is not unusual for actual expenditures to be less than the amount authorized in waiver service plans. However, the relatively large gap between the amount that may be authorized and actual expenditures is striking, especially because supports waiver funding limits themselves typically are 20-50 percent below the average costs of the comprehensive waivers with which they are paired.
Supports Waiver Service Coverage
Table 3 shows the types of services that are covered in supports waivers. The table employs a waiver service classification scheme that HSRI developed to facilitate the comparison of service coverages across supports waivers. This classification scheme is further described in the introduction to Appendix A.
As can be seen from Table 3, most supports waivers cover a common set of basic services and supports (e.g., respite, in-home supports [typically personal assistance], transportation, and home modifications). Supports waivers that serve adults with I&DD usually cover one or more types of day supports that are provided outside the family home such as supported employment, group or individual community participation activities, adult day habilitation training, and pre-vocational services.
As a general matter, the service coverages provided through supports waivers often mirror the services that states furnish through their comprehensive waivers except for the coverage of residential services. To the extent that the coverages are the same between both types of waivers, waiver participants are able to select from the states existing pool of established service providers. Some of the variation among states in the coverage of services is due to differences in the scope of services offered under the Medicaid state plan in each state.
| TABLE 3. Supports Waiver Service Coverage | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Service Category | AL | CO | CT | FL | IN | LA | MO | MT | NE | OH | OK | OR | PA | SD | TN | TX | WA | Total All Waivers |
| Case Management/ Service Coordination | * | * | * | X | X | X | * | * | * | * | * | X | * | * | * | * | 4 | |
| Supports for Participation Direction (Support Broker) | X | X | X | 3 | ||||||||||||||
| In-Home Services | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | 16 | |
| Respite | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | 16 | |
| Day Supports | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | 16 | |
| Health Related | X | X | X | X | X | X | X | X | X | X | X | X | X | 13 | ||||
| Supported Employment | X | X | X | X | X | X | X | X | X | X | X | X | X | 13 | ||||
| Transportation | X | X | X | X | X | X | X | X | X | X | X | X | X | X | 14 | |||
| Person Directed Goods and Services | X | X | 2 | |||||||||||||||
| Equipment/ Supplies | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | 17 |
| Vehicle Repair/ Modification | X | X | X | X | X | X | X | X | 8 | |||||||||
| Clinical Service | X | X | X | X | X | X | X | X | X | X | X | X | X | 13 | ||||
| Environmental Accessibility Adaptations | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | 15 | ||
| Financial Management Services | ** | X | ** | X | 2 | |||||||||||||
| Family and Caregiver Training | X | X | X | X | X | X | 6 | |||||||||||
| Other | X | X | X | X | X | X | X | X | X | 9 | ||||||||
| Total by State | 10 | 10 | 12 | 10 | 11 | 10 | 9 | 9 | 7 | 8 | 11 | 14 | 8 | 7 | 13 | 9 | 11 | |
| * Service coordination furnished as Targeted Case Management coverage or via Medicaid administrative claiming rather than as a waiver service. ** Financial management services furnished administratively rather than as a waiver service and are furnished to support individuals who hire their own workers and/or manage an individual budget. | ||||||||||||||||||
In most cases, case management (service coordination) is not covered as a waiver service but instead is furnished under the Medicaid state plan via the Targeted Case Management coverage under §1915(g) of the Social Security Act or as a Medicaid administrative expense. This means that the costs of performing case management on behalf of supports waiver participants does not result in a claim against the funding limit that applies to the waiver.
Consumer/Self-Direction
An important development in the delivery of HCBS is the incorporation of self-direction of services into waivers. A growing number of states are offering waiver participants the opportunity to directly manage their waiver services. However, so far, most states that operate supports waivers have not covered the infrastructure associated with the self-direction of waiver services. This can be detected from the absence of waiver services such as supports for participant direction (support brokers) or financial management services. Financial management services assist individuals and their families in directly hiring their own workers and/or managing an individual budget. Only five of the 17 states (Connecticut, Missouri, Nebraska, Oregon, and Tennessee) have structured their supports waivers to incorporate consumer/self-direction features. In other states, individuals and families are permitted to select services and service providers within their budget allocation but the full range of self-direction opportunities is not available to waiver participants.
About Self-Direction
Self-direction refers to service practices that grant individuals significant authority to manage their benefits. Key characteristics generally include:
- An individual budget allocation for services;
- Development of a person-centered plan of services that is driven by individual needs and preferences;
- Individual/family hiring and direct supervision of service providers;
- Specialized methods to process payments to service providers and track expenditures.
Number of Individuals Participating in Supports Waivers
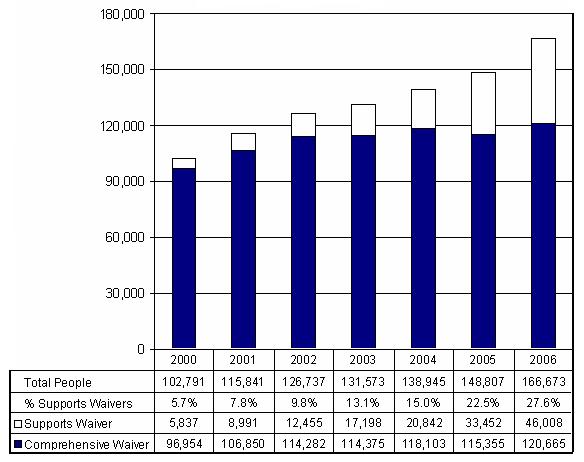
Chart 1 shows the trend in waiver enrollment from 2000 to 2006 for the 17 states that presently operate supports waivers. The chart shows total waiver enrollment and breaks down enrollment between the supports and comprehensive waivers operated in these states.15
In 2000, these 17 states accounted for 35.3 percent of all waiver participants with I&DD nationwide. During the period 2000-2006, total waiver enrollment in these states increased by roughly 64,000 individuals or 62.7 percent. Comprehensive waiver enrollment increased by 24 percent. Enrollment in supports waivers accounted for 62.9 percent of total enrollment growth. By 2006, 27.6 percent of all waiver participants in these states were enrolled in supports waivers.
The high rate of growth in number of supports waiver participants during this period, of course, is mainly due to the fact that many of these states were just launching their supports waivers. Still, it is evident that these states expanded overall waiver enrollment at a rapid pace and that the implementation of supports waivers accounted for a substantial share of enrollment growth. At the same time, these states also expanded the availability of comprehensive waiver services, albeit at a lower rate. As a general matter, it is evident that as the number of supports waivers in operation scaled up, the expansion of comprehensive waivers decelerated, especially after 2003.
| CHART 1. Supports and Comprehensive Waiver Enrollment 2000-2006 (17 States) |
 |
| CHART 2. Comprehensive and Supports Waiver Expenditures Trends 2000-2006 (17 States) ($ Billions) |
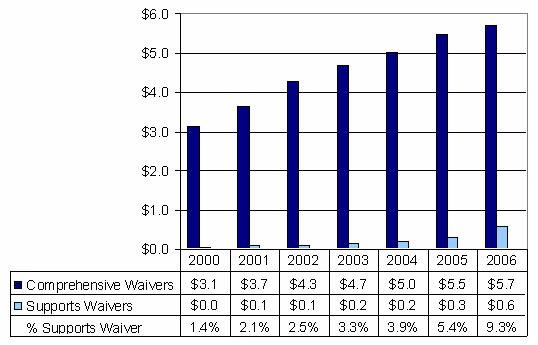 |
Trends in Total HCBS Waiver Expenditures
Chart 2 shows HCBS comprehensive and supports waiver expenditures during the period 2000-2006. As can be seen from the chart, supports waiver expenditure growth parallels the growth in the number of supports waiver participants. Among the 17 states, supports waiver expenditures made up 9.3 percent of the total $6.3 billion in I&DD waiver expenditures in 2006 while supports waivers participants accounted for 27.6 percent of the total waiver participants.
Expenditures Per Waiver Participant
Chart 3 shows average per participant expenditures for the comprehensive and supports waivers operated by the 17 states along with: (a) the weighted average per participant expenditure for both types of waivers in combination (weighted by the number of participants in each type of waiver); and (b) supports waiver per participant expenditures as a percentage of comprehensive waiver per participant expenditures.
| CHART 3. Average Annual Expenditures Per Participant 2000-2006 (17 States) |
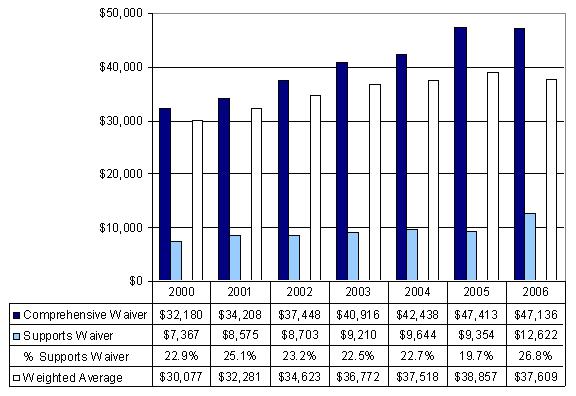 |
In 2006 the average expenditure per supports waiver participant was 26.8 percent of the average expenditure per comprehensive waiver participant. During the 2000-2006 period, the relationship between supports and comprehensive per participant costs ranged between 19.7 and 26.8 percent. Year-by-year variation in the relationship of per participant expenditures between the two types of waivers principally stems from the phase-in of additional supports waivers across the period.
Of potentially greater interest are the effects of the implementation of supports waivers on the weighted average cost of furnishing waiver services in these states. As can be seen from the chart, the effect of the introduction of supports waivers has been to stabilize average waiver participant costs in these states, especially after 2003. Across the 17 states, the weighted average cost per waiver participant for both types of waivers in combination remained essentially unchanged from 2004 to 2006. The increasing proportion of waiver participants served through supports waivers in these states has slowed the rate of increase in per participant expenditures.
Variance Across States in Per Person Spending
Table 4 shows the variance across states in average per person spending for both comprehensive and supports waivers. As shown, for supports waivers, average spending per participant in 2006 was $12,662, although spending ranged from a low of $4,222 in Missouri to a high of $24,443 in Connecticut. This variance is due in part to the different funding limits that states have adopted for their supports waivers.
The figures in the last column show per participant expenditures in supports waivers as a percentage of per participant expenditures in comprehensive waivers. States vary considerably with respect to this measure, ranging from a low of 11.3 percent of comprehensive waiver expenditures in Missouri to a high of 46.9 percent in Ohio. To date, no clear relationship has emerged between supports and comprehensive waiver per participant costs.
| TABLE 4. State-by-State Average Comprehensive and Supports Waiver Expenditures per Participant | |||
|---|---|---|---|
| State | Comprehensive Waiver Expenditures per Participant | Supports Waiver Expenditures per Participant | Supports Waiver Expenditures as a Percentage ofComprehensive WaiverExpenditures per Participant |
| AL | $41,433 | $8,950 | 21.6% |
| CO | $54,999 | $15,983 | 29.1% |
| CT | $72,205 | $24,443 | 33.9% |
| FL | $26,303 | $8,700 | 33.1% |
| IN | $65,569 | $8,520 | 13.0% |
| LA | $49,756 | $9,255 | 18.6% |
| MO | $37,208 | $4,222 | 11.3% |
| MT | $29,893 | $6,252 | 20.9% |
| NE | $50,526 | $9,158 | 18.1% |
| OH | $48,435 | $22,733 | 46.9% |
| OK | $63,577 | $9,661 | 15.2% |
| OR | $55,000 | $8,505 | 15.5% |
| PA | $67,574 | $12,738 | 18.9% |
| SD | $33,581 | $4,015 | 12.0% |
| TN | $60,385 | $18,051 | 29.9% |
| TX | $37,480 | $8,669 | 23.1% |
| WA | $56,771 | $13,581 | 23.9% |
| Average | $47,136 | $12,622 | 26.8% |
State Waiting Lists
One of the policy aims expressed by states for launching supports waivers is to reduce or at least slow the growth of the number of people waiting for services. The implementation of supports waivers has enabled these states to expand the availability of HCBS to a great extent. Except for South Dakota, each of the 17 states had a waiting list for services. Collectively, these waiting lists totaled 142,100 individuals. Wide variations in the relative number of people waiting for services existed across the 17 states, ranging from approximately 10 percent of the number of people served to, in some cases, upwards of twice the number of people served. In some states (e.g., Colorado, Louisiana, Oklahoma), supports waiver participants are wait-listed for comprehensive waiver services but are unable to receive them due to funding limitations. In other states (e.g., Florida and Texas), individuals who enroll in a supports waiver may continue to be wait-listed for comprehensive waiver services.
Except for Connecticut, none of the 16 states with waiting lists reported a decline in the overall number of people on waiting lists post-implementation of their supports waivers. The effect of the implementation of supports waivers on waiting lists is difficult to pinpoint. These states are continuing to experience surging service demand. While supports waivers have permitted these states to absorb some of this demand, not enough demand has been addressed to prevent waiting lists from continuing to grow.
V. SUMMARY OF CASE STUDIES
Six states were selected to examine in depth the status of supports waivers and the role they play in meeting the needs of people with I&DD. The states selected were: Florida, Missouri, Oklahoma, Oregon, Pennsylvania, and Tennessee. The case studies were compiled by conducting structured discussions with key informants in these states and the results of these state-by-state discussions are recapped in Appendix B. Unless otherwise cited, the information in this section is based on these discussions.
Each states supports waiver emerged as a result of circumstances unique to the state and operates under its own distinct policies and protocols. Nevertheless, the six states share much in common. The following summary highlights the findings in several key areas.
Policy Goals
Respondents described two primary policy goals that underpin their states interest in operating supports waivers: cost containment and wait-list reduction. Another goal that was often cited was to promote self-direction of HCBS.
Cost Containment. Respondents all agreed that supports waivers provide an economical alternative to comprehensive waivers. Reasons cited to illustrate how supports waivers reduce spending per participant are as follows:
-
They do not offer 24-hour care and supervision in a persons home or in a community residential facility.
-
They allow states to both specify the number of waiver participants and limit the amount spent per participant.
While states can hold down per participant spending within comprehensive waivers, the supports waiver caps are better defined and more readily enforced, enabling states to more accurately predict costs and control spending.
Wait-List Reduction. Most respondents expressed concern about wait-lists. The average number of persons on wait-lists across the six states was 4,988--ranging from 2,000 in Oregon to 12,011 in Florida.
-
All of the states have databases that enable them to track people as they move on and off the wait-list. In most states, individuals wait for services for more than two years. Oregon has set a goal to reduce the wait period to 90 days or less when its Staley lawsuit settlement agreement is completed. The longest wait time, reported by a Florida respondent, was five years.
-
Informants unanimously viewed the supports waiver as an important, practical tool for addressing the wait-list. Though most could not cite empirical evidence to this effect, they reasoned that the lower-costs associated with supports waivers allowed more people to receive services than would have been possible if the state had only a comprehensive waiver.
Self-direction. Some respondents indicated that incorporating self-direction into state policy and practice is an important policy goal of supports waivers. This includes granting individuals significant authority to manage their benefits by: (a) exercising authority over service planning within a specific benefits allocation; (b) selecting service providers; and (c) managing these providers. Some states also allow individuals to choose and manage support workers outside the traditional provider network, such as friends, neighbors, relatives, or others.
Respondents in Oregon said that its supports waiver was designed with the clear intent of promoting self-direction. Tennessee, Missouri, and Pennsylvania also permit some degree of self-direction. Overall, however, although many respondents expressed interest in self-direction as a policy goal, the majority of respondents admit that implementing self-direction is secondary to the goals of cost containment and wait-list reduction.
Waiver Operations
While particular waiver operations vary among states, they have much in common.
Information Available about Participants. Respondents from all states indicated that the ability to track individuals in a supports waiver by key characteristics, service use, and expenditures enabled the state agency to manage its resources more efficiently.
-
Most states use a variety of means to gather and analyze basic descriptive information on supports waiver participants (e.g., age, primary disability, living arrangement, functional status, and caregiver characteristics). However, most respondents noted the need to upgrade their information management systems (particularly in Missouri and Tennessee) to gain more in-depth information on beneficiaries and families and to more easily link to other state-managed databases. On the other hand, Oregon compiles especially robust information about its supports waiver participants.
-
As systems become increasingly decentralized and self-directed, states reported the need to be able to track in real-time the status of services and individual spending. Presently, states information systems lack this capacity, although some states, such as Oregon and Florida, are working toward it.
Access and Admission. States differ in how easily people can enroll in the supports waiver.
-
States vary in how--and how energetically--they inform potential users about the supports waiver. All states describe the program on their websites and make print materials available.
In all states, case mangers are often the ones who first bring the supports waiver to the attention of individuals and their families; but this practice appears to be uneven across a given state. Family advisors to states reported that individuals were not always informed of the option by case managers, but heard about it by word of mouth and at family-focused conferences or other meetings.
-
Enrollment depends on the availability of funds and urgency of need. Determining the urgency of need can be a complex process; some needs may not be as urgent as others, but may have greater implications if they are not met. For instance, some individuals may be in crisis, others have urgent needs but are not in crisis, and so on.
-
Some states use a systematic assessment process to sort applicants by urgency of need and give priority to emergency or crisis applications. In Missouri, for instance, a utilization review team considers applications to determine individual need status. Oregon uses an order of enrollment procedure that is detailed in two pages and includes a method for sorting waiver applicants by urgency of need. Likewise, Pennsylvania uses the Prioritization of Urgency of Need for Services system to obtain information about urgency of need.
Allocations per Participant. All states limit per participant budgets based on a pre-set allocation, which is set using systematic means such as an assessment instrument (e.g., the Supports Intensity Scale). These measures can be used in tandem with other descriptive information to quantify an individuals level of need and match it to a specific allocation.
Many respondents reported that the process used to set personal allocations is an on-going source of tension. Some argued that formal measures do not always satisfactorily capture individual circumstances and needs and questioned the amounts allocated. They sometimes cited examples where they believed that individuals received too low an allocation. Some also noted that the allocations inappropriately limited the type or amount of services a person could receive.
For example, budget limits can pose dilemmas for individuals and families that affect the selection of services. For example, using the budget to purchase more costly supported employment services can translate into fewer hours of services outside the family home than the selection of lower-cost facility-based day services. From the familys perspective, facility-based services may be preferred because more covered hours per day can be purchased and ensure that their family member has services at a set time and place each day. While integrated employment might be preferred by the individual, fewer hours can be purchased and the service schedule might be irregular.
In response, others argued that though the procedures may miscalculate by some degree a persons allocation, systematically applied processes offer a fair way to allocate resources. Further, some noted that by pre-setting budgets based on individual scores, state staff could more easily manage an overall budget.
Service Planning and Risk Assessment. States use case managers or support brokers within a person-centered planning protocol to generate service plans, assess risk, and accommodate requests to switch providers.
-
In most states, case managers or brokers are responsible, on average, for 50 people, ranging from a low of 29 in Oklahoma to a high of 70 in Missouri.
-
Individuals and families generally are informed of their allocation before they begin planning.
-
Many respondents indicated that individuals and their families have significant decision-making ability within their budget allocation, though they are not always fully aware of this authority.
-
Individual plans are limited in scope and flexibility depending on the waiver service array.
-
Family advisors to states expressed frustration about having a budget allocation for their family members that they hoped would be flexible enough to meet their needs, only to discover that the services permitted under the waiver did not satisfactorily match their needs. Several respondents advocated for expanding the waiver service array. They argued that, if funding is capped, it should not matter what particular services are covered because the cost to the state would be the same.
-
Service planning typically does not include a distinct process to identify and address risks related to health and well-being. Risks, however, are typically identified and well documented in the service planning process along with steps to address identified risks in the individualized waiver service plans.
-
Some respondents indicated that supports waivers entail the strong involvement of participants family, with whom they often live, which often reduces concerns about the individuals health and safety. Others fairly noted, however, that some families may not be able to provide the level or quality of support required.
-
All states have processes to help participants change their service plan or service providers, starting with contacting a case manger or service planner. The process that follows can take some time to complete, but respondents reported that it is generally managed easily within an acceptable period of time.
Services and Supports. Supports waivers, especially those emphasizing self-direction, encourage use of a diverse and flexible provider network that can offer individualized and sometimes unique services. We found that states vary in how well-developed local services and supports are. In addition, states must also be ready to respond to needs that exceed what can be offered through a supports waiver.
-
Individuals often seek alternative sources of support outside the traditional provider network. As a result, respondents explained that local providers are challenged to reshape the services they offer or to diversify their operations to accommodate new service demand. Some service agencies are open to change and seek to provide more flexible service arrays, while others resist change or complain that they cannot deliver services at the reimbursement rates at which they are offered.
-
Most respondents reported that provider networks--traditional or alternative--vary in their capacity to meet the emerging service demand generated by supports waivers. Participants sometimes have difficulty finding direct support workers due to workforce shortages--particularly in rural areas--caused in part by insufficient resources to offer wages and benefits that will attract workers.
-
Respondents in every state expressed concern about the competencies of workers that individuals and families are hiring, especially friends or neighbors who are not affiliated with service agencies. Respondents often described circumstances where individuals and their families had no assistance to train these workers. Respondents were concerned about the quality of support that these workers are providing.
Many respondents indicated that on one hand, individuals welcome the freedom to hire the workers of their choice, but workers often cannot be found, and a shortage of workers requires individuals to hire workers that they would rather not. Respondents in all states reported that more must be done to recruit, train, and support workers and that this responsibility cannot be left solely to individuals and their families.
All states have developed mechanisms to address the needs of individuals who require more support than the waiver can offer. Sometimes, the funding limit can be adjusted upward so that additional support can be purchased or funding is temporarily augmented from other state funds.
Ultimately, when participants needs exceed what the supports waiver can offer, the individual must be referred to the states comprehensive waiver.
If this waiver is at its limit, the individual is put on the wait-list but continues to receive services through the supports waiver. Respondents, however, reported that relatively few people need to transfer from supports to comprehensive waivers.
Quality Assurance. Supports waivers present state agencies with unique challenges related to quality monitoring and assurance activities. Respondents indicated that most states apply to the supports waiver the same basic quality assurance and quality management practices they use in their comprehensive waivers. However, they recognized that states need to modify their approach to quality assurance because supports waivers differ from comprehensive waivers in two important ways. First, the individuals place of residence is often not a licensed residential facility, but the family home. Second, the staff hired to provide supports are often not employed by traditional service providers but are recruited from among family, friends, or others in the community.
Because participants family homes are often their place of residence and the staff hired can be other family members or friends, the quality oversight mechanisms for the comprehensive waiver are not always a good match. Respondents wondered how on-site visits should be handled and how incident reports should be handled when difficulties arise in the family home. Further they wondered how the actions of a decentralized, alternative workforce can be properly overseen.
Issues like these are not so easily resolved, and respondents in all states indicate that they are working to determine how to modify quality assurance systems to match the unique service delivery circumstances of supports waivers. All states have methods for resolving complaints or grievances filed by participants. Typically they involve a systematic Fair Hearing process for complaints or a protocol designed to air and resolve grievances. States reported a low volume of grievances and complaints.
Waiver Impacts on State Systems
It is too early to report data on system impacts because the states selected for the case studies have relatively new supports waivers and are still focused on implementation--setting governing rules and regulations and working out various procedural difficulties. Oregon officials characterized the states supports waiver as an evolving program, which they continually review and revise to make improvements and address technical problems.
States are still developing the infrastructure to support these waivers, including: (a) information systems to track service delivery, spending, and impacts per participant; (b) training for service planners; (c) improvements in the capacity of local provider networks; and (d) revisions to quality assurance mechanisms.
While focused on implementation, respondents did report on the waivers operations and their perceptions of outcomes to date.
-
States are generally satisfied with the waivers ability to contain costs and reduce the waiting time for services, allowing them to serve many more people than would have been possible through the comprehensive waiver alone.
-
While self-direction was not typically a driving policy goal of these waivers, all states are interested in administering the waiver to incorporate self-direction. In this regard, Oregon is noteworthy in having a well-developed statewide service brokerage model.
-
Based on anecdotal reports, participants and their families are satisfied with supports waiver services in large part simply because they are off the waiting list and receiving some measure of support. In this regard, family members also value the supports waiver because they say it helps keep the family together and enables them to engage in other activities, including employment outside the home.
Key Issues in the Operation of Supports Waivers
We asked respondents to tell us about issues their states are dealing with as they implement their new supports waivers and to offer suggestions for improving them. Their comments are summarized below.
-
Wait-Lists and Resources. While the supports waivers have decreased the time spent on wait-lists for many, thousands of people remain on lists, due to lack of funding, an issue that is unlikely to change due to larger state budget issues. To address this problem, several respondents said that states need to redesign their systems to ensure that individuals receive only the supports they need. They felt that some people receiving comprehensive waivers services may be over-served and may be more efficiently served in the supports waiver.
-
Limits in Participant Allocations. Respondents differed in their views on funding limits. Some felt increases were needed to provide participants the support they need while others countered that raising the limit would undercut the cost-saving benefit associated with supports waivers, and that individuals with higher needs may be better served by the comprehensive waiver.
-
Staffing. Respondents in all states described difficulties recruiting and retaining staff. Some observed that supports waivers open opportunities to recruit additional workers who may be willing to work part-time or on an as-needed basis but it is still difficult to find workers, especially in rural areas. The inability to find staff can lead to families settling for workers they would not ordinarily hire. In addition to disrupting service delivery, high staff turnover increases training costs.
Respondents in all states recognized that the ability to recruit successfully from appropriate labor pools depends on the wages and benefits offered, including workers compensation coverage and health insurance and that allocations under the supports waivers are not sufficient to provide this coverage. As a result, as respondents observed, the prevailing hiring conditions reduces the labor pool that can be drawn from to secure staff.
-
Liability. Some respondents expressed concerns about liability for on-the-job injuries when workers do not have either private health insurance or workers compensation coverage. It was not clear to them who would or could be held legally liable for the costs associated with injuries but some felt it could ultimately be the state. Others, however, argued that if families and individuals acted independently to recruit, hire, train, and manage their own staff, then they alone may be liable for the costs of injuries.
Several respondents felt that workers should be covered by workers compensation insurance, but this may not be easily achieved given its cost. Covering workers could be particularly difficult for individuals or families who employ several workers, all of whom work part time.
In Florida, some families have purchased riders to their homeowners insurance to cover potential liabilities associated with workers being injured on-the-job in the familys home. Overall, many respondents agreed that states should implement policies to reduce family liability for job-related injuries.
-
Role of Representatives. In supports waivers that incorporate self-direction, services are often planned and directed by a representative--typically family members. Some respondents expressed concerns that care needed to be exercised to ensure that families were not taking over decision-making from the participant. Given that individuals often have an intellectual disability, respondents acknowledged the lack of a simple solution. Most agreed, however, that there is a growing awareness of the problem among people with developmental disabilities, family members, and policy makers, and attempts are being made by these parties to find workable solutions.
Oregon has developed a conflict of interest policy that addresses the potential for a conflict of interest when a representative such as a family member is directly involved in decision-making for an individual, but may derive personal financial benefit from a particular decision. In such instances, local supports brokers are required to: (a) identify and describe potential conflicts of interest; (b) determine if the decision does not accord with the participants preferences or interests; and (c) seek further action to resolve any apparent conflicts of interest.
-
Systems Infrastructure. Respondents mentioned several infrastructure shortcomings, including:
-
Management and information systems. All states operate management information systems to track use of their HCBS waivers. These systems, however, do not presently collect the full range of information on individual beneficiaries and their families that is needed to refine supports waiver policies and practices. In addition, these systems generally are not yet linked to other state-managed databases, such as those with information specific to quality enhancement or assurance. For example, although Florida initiated its supports waiver in 2005, the state has not yet modified its information systems to the degree needed to integrate information across databases.
Quality assurance. States need to develop specific quality monitoring and assurance systems for supports waivers because the systems developed for comprehensive waivers are not always a good match. For instance, states need to develop strategies to better assess the competencies of workers who are not affiliated with provider agencies.
Additionally, states need to develop a more outcome-oriented approach to supports waivers. Quality indicators would help participants and staff members identify areas where improvement is needed.
-
-
Training. Respondents acknowledged that states need to address workers training needs and provide participants and their families with training or other resources to acquire the skills they need to recruit, train, and retain satisfactory staff.
-
Program Design. Respondents mentioned several program design or procedural issues that states were working to resolve.
-
How to set reasonable individual allocations. Respondents disagreed about the best way to set individual service allocations as well as the amount of the allocation.
The comprehensiveness of the service array. Many respondents believe that supports waivers should at least cover the same services as comprehensive waivers (with the exception of residential care). Given that states set spending limits for each participant, covering a wide range of services can increase an individuals and familys ability to match services to needs without increasing costs.
-
VI. SUPPORTS WAIVERS: IMPACT AND CONTINUING CHALLENGES
Observations About the Impact of Supports Waivers
It is important to recognize that supports waivers are a relatively recent phenomenon, although they draw upon the long history in many states of furnishing more limited state-funded family support services to people with I&DD. At this juncture, while it is difficult to draw firm conclusions about their effect on state I&DD service delivery systems, based on the information obtained during this study, the following observations are offered:
-
Supports waivers improve access to HCBS. Supports waivers have enabled a greater number of people with I&DD to obtain essential services and supports. The availability of federal Medicaid financial participation for supports waivers has permitted states to leverage their dollars to serve more persons. In general, participants and their families--many of whom have spent extended periods on a wait-list--appreciate that they are now receiving some services. Nonetheless, all the states that operate supports waivers continue to struggle with growing waiting lists. While supports waivers have given states a tool to expand access to HCBS more economically, service demand continues to surge.
-
Supports waivers have slowed the growth of more costly comprehensive waivers. The implementation of supports waivers in the 17 states appears to have at least slowed the growth of comprehensive waiver services and stabilized the overall per participant costs of furnishing waiver services in these states. Service demand is being channeled away from higher cost services--specifically, residential services.
-
Supports waiver participants appear to have access to comprehensive waiver services when necessary. A major concern among families and disability advocates is that people who are enrolled in supports waivers will be cut off from access to comprehensive waiver services when needed. There is no systematic evidence that states are not transitioning individuals to comprehensive waiver services as necessary. In each of the six case study states, individuals have transitioned from one waiver to another based on urgency of need. In addition, states generally provide supplemental services/funding to supports waiver participants when necessary. Still, the lack of guaranteed access to comprehensive waiver services when necessary remains a source of concern for many individuals and families.
-
Supports waivers appear to be meeting the needs of most participants and their families. In the six case study states, there has been relatively little movement from the supports to the comprehensive waiver. This provides some measure of evidence that supports waivers are adequately meeting the needs of participants and families. In practical terms, the supports waivers appear to be meeting the objective of avoiding costly out-of-home placements through the provision of in-home and community-based day services. At the same time, in many states, there are significant numbers of supports waiver participants who are wait-listed for comprehensive waiver services. This indicates that supports waiver enrollment postpones but does not eliminate the need for comprehensive waiver services. Moreover, in many states that operate supports waivers, there are serious questions about whether supports waivers are fully responsive to the needs of individuals.
The experience to date with supports waivers leaves at least two major questions related to their impact unanswered:
-
What is the appropriate balance between supports and comprehensive waivers? Among the 17 states, different proportions of waiver participants are being served in their supports and comprehensive waivers. Similarly, there are wide differences in the amount of dollars allocated to each type of waiver.
-
What is the appropriate funding limit to apply to a supports waiver to ensure that individuals can be successfully supported in their homes and communities? As previously discussed, there is wide variation in the funding limits that states apply to supports waivers. The amount of the funding limit under which a supports waiver operates has implications for the extent to which the needs of individuals can be met without resorting to costly residential services.
Challenges in the Operation of Supports Waivers
Looking forward, states must grapple with three key challenges in the operation of supports waivers: (a) finding resources to build infrastructure to support service delivery; (b) resolving various design and procedural issues related to their operation; and (c) fitting supports waivers into existing service systems to efficiently and effectively complement comprehensive waivers.
Finding Resources to Build Infrastructure. Supports waivers have some unique infrastructure requirements that are still being identified and addressed. Too often, insufficient resources are available to build the needed infrastructure. For example:
-
When resources are limited and spending efficiencies valued, state officials need information systems that allow quick, real-time tracking of individual and aggregate spending. With such data, states can allocate funds more efficiently and serve additional people. Available information systems are not presently up to the task. In at least one state, the lack of these data led to the lapsing of funds that could have been used to support additional individuals.
-
In some respects, case managers are more important to the success of supports waivers than they are for comprehensive waivers where residential provider agencies manage services. Yet, respondents noted insufficient numbers of case managers, too high caseloads, insufficient training, and high turnover.
-
Supports waivers also challenge states to fashion new methods to monitor and ensure service quality, as well as participants health and well-being, within systems that are increasingly decentralized. Some services are delivered by traditional providers where time-tested practices still apply. Participants also receive services in their home, provided by relatives, neighbors, or friends. In this context, traditional quality assurance practices are not always appropriate.
With limited resources and pressure to serve additional people, states must determine what portion of available resources to dedicate to infrastructure development as opposed to increased enrollment.
Resolving Operational Challenges. To date, the implementation of supports waivers in most states has not been accompanied by expanded opportunities for individuals and families to direct the full range of their services and supports. A few states (Oregon and Connecticut) provide for the full range of opportunities for individuals to self-direct their supports waivers, by providing person-centered planning, individual budgets, choice of services and providers, and specialized means for processing payments to providers. Most states, however, do not provide such opportunities at all or only to a limited extent.
Implementation of full-featured self-direction appears to pose significant operational challenges for most states that operate supports waivers. Many of these challenges are relatively new to the state systems that serve individuals with I&DD, where services traditionally have been managed by/through a single provider agency. Some of the challenges include setting individual funding allocations, defining a satisfactorily broad service array, ensuring sufficient flexibility in service choice and delivery, ensuring that individuals lead the service planning process, finding ample numbers of support workers, offering these workers wages and benefits that will increase recruitment and retention, and others.
Another operational challenge is the development of methods to allocate individual funding limits. The application of single one-size-fits-all funding limits to supports waivers may be problematic, particularly when a crisis brings participants up against the waiver funding cap. Some supports waivers are already addressing this issue by allowing additional temporary funding increases to the waiver cap (e.g., Ohio, Tennessee, and Washington).
As states gain more experience operating supports waivers, they will likely need to develop more sophisticated approaches to setting budget allocations. Some states are already using assessment data and other information to establish individual or tiered funding limits within a supports waiver in order to graduate the amount of funding that is available to individuals. Different approaches to establishing funding limits/budget allocations may enable states to serve individuals in supports waivers that have a wider range of service needs while maintaining appropriate financial controls.
A potentially satisfactory alternative approach is to adopt graduated funding limits that scale upward from a base funding limit. Oregon uses such an approach in its supports waiver for people with developmental disabilities. All waiver entrants are subject to a standard funding limit ($9,600 per year). Oregon has created a tool that steps up the maximum amount of services that can be authorized based on participant difficulty of care factors and/or limitations on the ability of family caregivers to provide support. This tool is scored and funding can be increased to $14,400 and then $20,000, based on the score.
Fitting Supports Waivers into the Overall System Structure. A major challenge for states is determining how to incorporate supports waivers in the larger service system so they will complement comprehensive waivers and other state-funded options to create a seamless, cost effective approach to supporting people with I&DD in the community. Currently, states are using supports waivers as one service option among several to primarily address cost containment and wait-list goals.
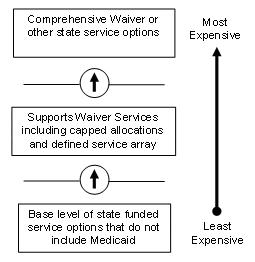
Several state leaders, however, view supports waivers as an option within a range of supports that includes the comprehensive waiver and other state-funded options, configured from least to most costly. Ideally, these options would fit together to provide a seamless, cost effective approach whereby individuals would be matched to the option that most effectively meets their needs. Individuals might start by accessing modest amounts of state-funded services that may suffice without any use of waiver services. If more supports are needed, individuals could be enrolled in a supports waiver. Finally, if still more supports were needed, the individual could be enrolled in the more costly comprehensive waiver.
Current systems are not nearly as efficient. Individuals, for example, may be enrolled in a more expensive comprehensive waiver when they could be ably served in a supports waiver. Alternately, some may be getting by in a supports waiver but might be better served in a comprehensive waiver. But supports waivers are still relatively new and modestly funded and individuals are not so easily assigned or reassigned to various service options. Individuals enrolled in the comprehensive waiver, for example, cannot be transferred to a supports waiver without their agreement.
If supports waivers and comprehensive waivers grow apart in policy and procedure over time, the resulting community services and supports system may be neither seamless nor coordinated. To prevent this from happening, states may need to revise the boundaries between supports and comprehensive waivers. For example, Colorado does not permit the delivery of comprehensive waiver services in the family home but is now considering changing that policy so that people who need especially intensive services can continue to reside with their families. In contrast, Oregon already provides for the continuation of services in the family home when people need to transition from the supports to the comprehensive waiver.
Concluding Observations
States face major challenges in addressing the needs of people with I&DD. Nearly every state is grappling with a large waiting list for services and the prospect that demand for services will continue to climb due to a wide range of demographic factors, including the aging of family caregivers with whom most people with I&DD reside. The high per person costs of furnishing comprehensive waiver services has led states to search for lower-cost alternatives to address rising service demand.
Clearly, operating supports waivers offers a means for a state to channel demand away from costly residential services and, thereby, address service demand more economically. Supports waivers have provided states with a vehicle in which to deliver community services and supports for people with I&DD more economically by leveraging family caregiving and employing tighter financial controls on the amount of services that are authorized. The rapid growth in the number of states operating these waivers--especially since 2003--is noteworthy.
States are using these waivers as a means to respond to rising service demand. There seems little doubt that the number of states operating these types of waivers will continue to grow. Additionally, because supports waivers offer a lower-cost alternative to comprehensive waivers, state policy makers may be more amenable to periodic increases in funding for services for people with I&DD.
Still much work remains. To make most effective use of supports waivers, states will need to ensure that proper resources are in place to support them, operational difficulties are resolved, and an appropriate role for these waivers is found within the larger state system. Within this context these waivers show great promise for establishing a next generation of person-centered home and community services for individuals with I&DD.
ACRONYMS
| A | |
|---|---|
| APD | Florida Agency for Persons with Disabilities |
| B | |
| BSCI | Basic Supplement Criteria Inventory (Oregon) |
| C | |
| CAP | Community Alternatives Program (Washington) |
| CCB | Community Centered Board (Colorado) |
| CDDP | Community Developmental Disability Programs (Oregon) |
| CLASS Waiver | Community Living Assistance and Support Services Waiver (Texas) |
| CMS | U.S. Centers for Medicare & Medicaid Services |
| CSLA | community supported living arrangements (Colorado) |
| CSP | Community Supports Program (Nebraska) |
| CSW | Community Supports Waiver (Missouri, Montana) |
| D | |
| DADS | Texas Department of Aging & Developmental Services |
| DD Waiver | Developmental Disabilities Waiver (Indiana) |
| DDSD | Oklahoma Developmental Disability Services Division |
| DDSPD | Oregon Office of Developmental Disability Services Seniors & Persons with Disabilities |
| DMRS | Tennessee Division of Mental Retardation Services |
| DPW | Pennsylvania Department of Public Welfare |
| F | |
| FICS | family and individual consultation and support (Connecticut) |
| FSL Waiver | Family and Supported Living Waiver (Florida) |
| FSW | Family Support Waiver (South Dakota) |
| FY | fiscal year |
| H | |
| HCB-DD Waiver | Home and Community-Based Services for the Developmentally Disabled Waiver (Colorado) |
| HCBS | home and community-based services |
| HCFA | U.S. Health Care Financing Administration |
| HCS | Home and Community-Based Services Program (Texas) |
| HSRI | Human Services Research Institute |
| I | |
| I&DD | intellectual and other developmental disabilities |
| ICF/MR | intermediate care facility for the mentally retarded |
| IFS Waiver | Individual and Family Support Waiver (Connecticut) |
| IO Waiver | Individual Options Waiver (Ohio) |
| ISO | intermediary service organization (Pennsylvania) |
| ISP | individual support plan |
| L | |
| LAH Waiver | Living at Home Wavier (Alabama) |
| M | |
| MOCDD Waiver | Missouri Children with Developmental Disabilities Waiver |
| MR/DD | mental retardation and other developmental disabilities |
| MRLA | Mental Retardation Local Authorities (Texas) |
| MSO | managed services organization |
| N | |
| NOW | New Opportunities Waiver (Louisiana) |
| O | |
| OBRA | Omnibus Budget Reconciliation Act |
| OCA | Oklahoma Office of Client Advocacy |
| OMR | Pennsylvania Office of Mental Retardation |
| P | |
| PERS | personal emergency response system |
| PFDS Waiver | Person and Family Direct Support Waiver (Pennsylvania) |
| PSR | Physical Status Review (Oklahoma) |
| PUNS | Prioritization of Urgency and Need for Services (Pennsylvania) |
| R | |
| RFW | Residential Facility Waiver (Ohio) |
| RTI | Research Triangle Institute |
| S | |
| SDWP | Self-Determination Waiver Program (Tennessee) |
| SLS Waiver | Supported Living Services Waiver (Colorado) |
| SSAW | Supports Services for Adults Waiver (Oregon) |
| SSI | supplemental security income |
| T | |
| TCM | Targeted Case Management (Nebraska) |
| TxHL | Texas Home Living Waiver |
| U | |
| UR | Utilization Review (Missouri) |
NOTES
-
Note that term "intellectual and developmental disabilities" (I&DD) is used throughout this report in place of the more traditionally known term "mental retardation and developmental disability" (MR/DD).
-
Larson et al. (2000). MR/DD Data Brief: Prevalence of Mental Retardation and/or Developmental Disabilities: Analysis of the 1994/1995 NHIS-D. Minneapolis, MN: University of Minnesota, Institute on Community Integration, Research and Training Center on Community Living.
-
Some 73.6% of adults with I&DD live with their families. Larson et al. (2001). MR/DD Data Brief: Demographic Characteristics of Persons with MR/DD Living in Their Own Homes or With Family Members: NHIS-D Analysis. Minneapolis, MN: University of Minnesota, Institute on Community Integration, Research and Training Center on Community Living.
-
HSRI (2000). Aging Family Care Givers: Needs and Policy Concerns. Portland, OR.
-
Robert Prouty, Gary Smith, and K. Charlie Lakin (2006). Residential Services for Persons with Developmental Disabilities: Status and Trends Through 2005. Minneapolis, MN: University of Minnesota, Research and Training Center on Community Living.
-
The definition of "related condition" is similar to but somewhat narrower than "developmental disability," which is defined in the federal Developmental Disabilities Assistance and Bill of Rights Act of 2000.
-
Steve Eiken, Brian Burwell, and Becky Selig (2006). Medicaid HCBS Waiver Expenditures, FY 2000 through FY 2005. Cambridge, MA: Medstat.
-
Robert Prouty et al., op. cit.
-
The average cost of ICF/MR services was $117,600 in 2005.
-
Martin Kitchener, Terence Ng, Charlene Harrington, and Molly O'Malley (2006). Medicaid 1915(c) Home and Community-Based Service Programs: Data Update. Washington, DC: Kaiser Commission on Medicaid and the Uninsured.
-
Ibid. In 2003, per participant expenditures through I&DD waivers were $35,888 versus $8,177 for waivers that served all other waiver target populations (e.g., seniors, people with other types of disabilities).
-
Located at: http://www.cms.hhs.gov/smdl/downloads/smd011001a.pdf.
-
The revised HCBS waiver application and accompanying instructions are located at: http://www.cms.hhs.gov/HCBS/02_QualityToolkit.asp.
-
Indiana, Montana, and Washington were unable to provide 2006 enrollment and expenditure figures. In this and the subsequent charts, 2005 enrollments and expenditures for these states have been carried forward.
APPENDIX A. STATE-BY-STATE SUPPORTS WAIVER PROFILES
PDF Version (100 PDF pages)
TABLE OF CONTENTS
CONTENT OF STATE SUPPORTS WAIVER PROFILES
CONTENT OF STATE SUPPORTS WAIVER PROFILES
The following profiles compile extensive information concerning supports waivers that are operated in 17 states. The profiles have been structured to capture uniform information across all the supports waivers in operation in 2006. In particular:
-
Waivers in Operation. A listing of the approved waivers for people with intellectual and other developmental disabilities (I&DD) operated by the state: The waivers are listed by name along with the following information: type (i.e., comprehensive or support), Centers for Medicare & Medicaid Services (CMS) waiver number, the number of participants in 2005, start date and status (e.g., on-going, initial, pending CMS approval). The list includes the comprehensive waiver to which the supports waiver is linked. In a few cases, states operate other waivers for people with I&DD that are not listed, but these waivers are not linked directly to comprehensive waivers.
-
Supports Waiver Features. This section contains basic descriptive information about each supports waiver, including:
- The target population (who the waiver serves);
Funding limits (the maximum dollar amount of waiver services that may be authorized for a waiver participant);
Funding parameters or relevant rules that govern how funds are allocated under the funding limit;
Exceptions (if any) to funding limit including how such exceptions are managed;
Provisions regarding transition to the comprehensive waiver to illustrate how an individual may move from the supports to the comprehensive waiver;
Whether the waiver includes features to promote self-direction. Waivers and state materials were reviewed for indicators to show that the waiver provides for individual budgets, permits participants to direct how these funds are spent, and/or supports participants in employing support workers.
- The target population (who the waiver serves);
-
Supports Waiver Services. This section provides information on the services that the supports waiver offers. To facilitate cross-state/cross-waiver comparisons of the scope of waiver services, Human Services Research Institute (HSRI) defined 16 broad service categories to classify the services offered through the supports waivers. State waiver service definitions were reviewed and services were sorted into these predefined categories. These service categories are further described in the table on the following page. In each profile, it is shown whether or not the waiver offers each service type. If so, the particular service label applied by the state is also shown.
-
Background Information on the Supports Waiver. This section offers background information on how and why the supports waiver was developed. This discussion identifies the unique state dynamics that may be in play that served as impetus for implementing a supports waiver. Common driving factors include: (a) holding down costs or make systems more cost efficient; (b) addressing increasing service demand (waiting list reduction); (c) developing service options to promote consumer-direction; and, (d) coming into compliance with CMS State Medicaid Director Letter #4.
-
Current/Major Issues or Changes Underway. This section discusses factors that may have an impact on a state’s waiver strategy. This could include: (a) the impact of active court cases regarding wait-lists; (b) anticipated outcomes resulting from consultations with CMS staff regarding waiver administrative structure or operations; (c) changes to waivers that states are planning to make; and (d) changes in state budgets that have the potential of altering how a waiver is structured or run.
-
Statistical Profile. This section provides information on comprehensive and support waivers regarding the number of participants served by waiver and associated costs. In most instances, the data depicts waiver utilization and expenditures during the period 2000-2006. In some instances, data were only available through 2005; in a few cases, states provided year out projections. Complementing graphics are also presented to illustrate changes over the period.
-
Web-Accessible Resources/Documents Inventory. This section offers information about waivers that is available on the Internet or that was collected in print copy.
-
State Contact Information. Information is offered to show the name of a key contact person and their address, phone number and email address.
| TABLE A-1. Support Waiver Service Categories and Services/Activities | |
|---|---|
| Service Category | Services/Activities Associated with Category |
| Case Management/Service Coordination | Home and Community-Based Services (HCBS) waiver intake, assessment, service planning, and on-going monitoring. |
| Supports of Participant Direction (Support Broker) | Assistance to individuals/families who self-direct services. Such assistance may include the development of the person-centered plan, managing individual budgets, recruiting workers and accessing generic services and supports. |
| In-Home Services | Personal care/assistance, chore services, companion services, homemaker services. |
| Person Directed Goods and Services | A service that a state may make available to individuals who self-direct. Coverage permits waiver participants to purchase goods and services that are not specifically covered in a waiver but contribute to meeting the person’s needs for assistance. |
| Equipment/Supplies | Adaptive equipment, augmentative communication devices, personal emergency response systems (PERS). |
| Vehicle Repair/Modification | Modification of a vehicle to accommodate a person with a physical disability. |
| Respite | Relief to a person’s primary caregiver. |
| Clinical Services | Physical therapy, occupational therapy, behavioral interventions, speech and language services, and similar services performed by credentialed professionals. |
| Day Supports | Services furnished outside the person’s residence in facility-based settings such as day habilitation centers or in the community to promote community inclusion (e.g., community participation). |
| Environmental Accessibility Adaptations | Home modifications to accommodate physical disabilities (e.g., ramps, bathroom modifications, etc.). |
| Health Related | Typically skilled nursing services. |
| Financial Management Services | Services furnished to support individuals who directly hire their own workers and/or manage an individual budget. |
| Supported Employment | Services to assist individuals to secure regular community jobs and support their on-going employment. |
| Family and Caregiver Training | Services that teach family members/caregivers to perform activities that address one or more dimensions of a person’s disability. |
| Transportation | Transportation to community activities and/or other waiver services. |
| Other | Services that do not fall into the foregoing categories (e.g., supported living coaching in Florida). |
ALABAMA
| WAIVERS | |||||
|---|---|---|---|---|---|
| Waiver Title | Type | CMS Waiver # | Participants (2005) | Start Date | Status |
| Living at Home (LAH) Waiver | Supports | 0391 | 125 | 04/2003 | Initial |
| Home and Community-Based Services for Persons with Mental Retardation | Comprehensive | 0190 | 4,854 | 08/1981 | On-going |
| BASIC SUPPORT WAIVER FEATURES | |
|---|---|
| Supports Waiver Target Population | Children age 3 and older and adults with mental retardation on the waiting list for community services. |
| Funding Limit | $18,000/year. |
| Funding Parameters | Amount authorized based on individual plan. |
| Exceptions to Funding Limit | Crisis intervention services may be furnished over and above the funding limit. |
| Transition to Comprehensive Waiver | Individuals whose needs cannot be safely met under the supports waiver program and who are in crisis may be admitted to the comprehensive waiver program. |
| Self-Direction | Limited. Community Specialist services provide assistance to families and individuals in the development of person-centered plans and on-going assistance, if desired. |
| SUPPORTS WAIVER SERVICES | ||
|---|---|---|
| Support/Service Category | Y/N | Alabama Waiver Services |
| Case Management/Service Coordination | N | [Case management provided through Targeted Case Management coverage] |
| Supports of Participant Direction (Support Broker) | N | |
| In-Home Services | Y | Residential Habilitation, Personal Care |
| Respite | Y | Respite In-Home, Respite Out-of-Home |
| Day Supports | Y | Day Habilitation, Pre-vocational Services |
| Health Related | Y | Skilled Nursing |
| Supported Employment | Y | Supported Employment |
| Transportation | Y | Personal Care Transportation |
| Person Directed Goods and Services | N | |
| Equipment/Supplies | Y | Specialized Medical Equipment and Supplies |
| Vehicle Repair/Modification | N | |
| Clinical Services | Y | Physical, Occupational, Speech and Behavior Therapy |
| Environmental Accessibility Adaptations | Y | Environmental Accessibility Adaptations |
| Financial Management Services | N | |
| Family and Caregiver Training | N | |
| Other | Y | Community Specialist, Crisis Intervention |
Background Information: Supports Waiver
The Living at Home (LAH) Waiver was first approved by CMS in 2002 but not implemented until 2003. The waiver was designed to provide low cost services and supports to individuals with mental retardation who live with their families or on their own and as a tool to reduce the state’s waiting list for services. The waiver provides both in-home and day supports as well as other ancillary services. The waiver stresses the use of person-centered planning methods in support of family/participant direction of services. Participants may select a community specialist to assist in the development and implementation of the person-centered plan. When community specialist furnishes on-going support, the frequency of case manager monitoring is reduced. State officials also report that the waiver is playing a role in its systems change initiative to eliminate the practice of “paying for the program” in Alabama (i.e., paying for slots in a particular program run by a private provider, rather than paying for the particular array of services and individual is determined to need). Community specialist services also have been added to the comprehensive waiver. The supports waiver uses a pre-authorized payment system to create a model that funds people, not programs. The state is implementing a new billing and data management system that will make the LAH Waiver much more usable by simplifying service authorization and billing.
The waiver has been slow to ramp up due to the lack of state funding. Recently, however, additional funds have been released to permit the program to be expanded. Alabama has been sued in federal court concerning the wait-listing of individuals for community services. Recently, a tentative settlement agreement was developed by the parties to eliminate the 1,400 person waiting list through a 3-year expansion of the LAH Waiver. However, this agreement was nixed by the Attorney General and the lawsuit continues to be litigated. Since openings are available in the comprehensive waiver, the state is able to shift individuals between the waivers as necessary. The state uses a criticality scale to determine placement on the waiting list, so that those with the most critical needs are the first to fill slots in the comprehensive waiver.
Alabama’s longer-standing comprehensive waiver provides a full-range of community services and supports. In recent years, the program has underwritten the costs of community placements from the state’s institutions as part of the settlement of the 33-year Wyatt v. Stickney lawsuit. At present, Alabama operates only one large public facility.
The next year, 2007, is a critical year in the waiver for developments that will help it become larger and viable. The developmental plan includes:
-
Implementing a revised billing and payment system that will put both the comprehensive and supports waiver on the same operational platform, that of funding people rather than programs. In this manner, applicants can be taken from the waiting list into whichever waiver meets their needs. Plans of care will be able to be changed on-line to meet a person’s needs, and plans will be monitored for timeliness, adequacy and full utilization through connection with paid claims history.
-
Implementing a comprehensive data management system that will connect all providers and all case managers to the Department of Mental Health and to the Medicaid Agency. All officials and staff whose function involves developing information about a person will be connected to the automated system. All information will be able to be aggregated and trended for analysis, outcomes and quality improvement. Applications and enrollments will be simplified and made faster, and enrolling providers and tracking their certification status will be automated.
-
Using the Supports Waiver to reach deep into the waiting list. This next year, funding has been requested to reach the next 600 people on the list.
Statistical Profile
| WAIVER PARTICIPANTS BY YEAR | ||||||||
|---|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006* | 2007* |
| Comprehensive | 4,037 | 4,395 | 4,764 | 4,437 | 4,868 | 4,854 | 5,100 | 5,200 |
| Supports | 0 | 0 | 0 | 7 | 84 | 125 | 300 | 584 |
| Total Participants | 4,037 | 4,395 | 4,764 | 4,444 | 4,952 | 4,979 | 5,400 | 5,784 |
| Supports Waiver % of Total Participants | 0% | 0% | 0% | 0.2% | 1.7% | 2.5% | 5.6% | 10.1% |
| * Approved cap. | ||||||||
Between 2000 and 2005, Alabama’s waiver enrollment increased by 23.3 percent, principally to support the community placement of individuals from the state’s large public facilities.
| ALABAMA WAIVER ENROLLMENT |
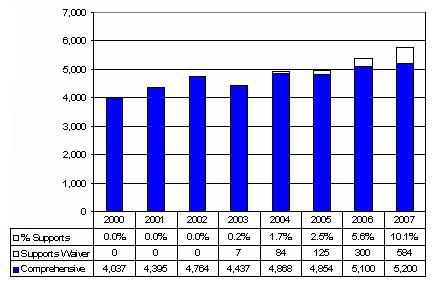 |
| EXPENDITURES BY YEAR | ||||||||
|---|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 |
| Comprehensive ($M) | $96.4 | $98.0 | $120.4 | $148.7 | $188.6 | $218.7 | $211.3 | $221.5 |
| Per Participant | $23,885 | $22,299 | $25,272 | $33,521 | $38,732 | $45,051 | $41,433 | $41,433 |
| Supports ($M) | $0 | $0 | $0 | $0.03 | $0.4 | $1.0 | $2.7 | $4.4 |
| Per Participant | $0 | $0 | $0 | $4,153 | $4,292 | $7,608 | $8,950 | $7,450 |
| Total Expenditures ($M) | $96.4 | $98.0 | $120.4 | $148.8 | $189.0 | $219.7 | $214.0 | $225.9 |
| Supports Waiver % of Total Expenditures | 0% | 0% | 0% | 0.1% | 0.2% | 0.4% | 1.3% | 1.9% |
| Cost Per Participant: % Supports to Comprehensive | 0% | 0% | 0% | 35.4% | 11.1% | 16.9% | 21.6% | 18.0% |
| Blended Cost Per Participant | $23,879 | $22,298 | $25,273 | $33,480 | $38,480 | $44,115 | $39,630 | $39,056 |
| ALABAMA WAIVER EXPENDITURES ($M) |
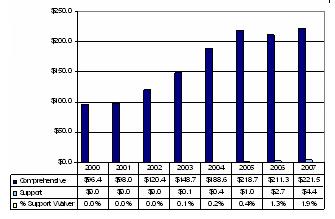 |
Between 2000 and 2005, total waiver expenditures more than doubled due principally to the expansion of the comprehensive services waiver.
| ALABAMA EXPENDITURES PER PARTICIPANT |
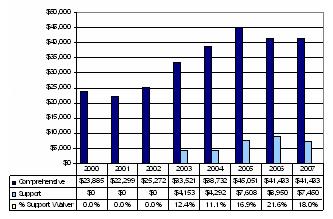 |
| WEB-ACCESSIBLE RESOURCES/ADDITIONAL INFORMATION | |
|---|---|
| Resource | Description/Web-Address |
| Alabama Department of Mental Health and Mental Retardation, Mental Retardation Services | Web page describing Alabama Mental Retardation Services http://mh.state.al.us/services/mr/index.htm |
| Alabama Medicaid Agency | LAH Waiver Fact Sheet http://medicaid.alabama.gov/documents/3D-1c-3-Fact-Sheet-Living_at_Home… Original LAH Waiver Application Mental Retardation Waiver Fact Sheet |
Document Inventory
- 2002 LAH Waiver Initial Waiver Application
- 2005 LAH Waiver 5 Year Renewal Application
- HCFA 372s: LAH 03-04, 372 LAH 04-05 and Comprehensive 00-01& 02-03 & 03-04
| STATE CONTACT INFORMATION | |
|---|---|
| Name | Fordyce Mitchel Director, MR Community Service Program |
| Agency | Department of Mental Health and Mental Retardation Mental Retardation Services |
| Address | 100 N. Union Street P.O. Box 301410 Montgomery, AL 36130-1410 |
| Telephone | 334-242-3719 |
| Fordyce.mitchel@mh.alabama.gov | |
COLORADO
| WAIVERS | |||||
|---|---|---|---|---|---|
| Waiver Title | Type | CMS Waiver # | Participants (2005) | Start Date | Status |
| Supported Living Services (SLS) Waiver | Supports | 0293 | 3,568 | 07/1995 | On-going |
| Home and Community-Based Services for the Developmentally Disabled (HCB-DD) Waiver | Comprehensive | 0007 | 3,996 | 10/1983 | On-going |
| BASIC SUPPORT WAIVER FEATURES | |
|---|---|
| Supports Waiver Target Population | Adults age 18 and older with developmental disabilities who do not require comprehensive 24/7 services. Each person must be in control of his or her own living arrangements, which is defined as: (1) a living arrangement which the individual has control over (house, apartment or condo) because he or she owns it or which the individual rents or leases in his or her own name; or (2) the individual lives with his or her family or legal guardian. The individual does not have to be in an eligible SLS setting to begin the process, however, once SLS services begin, the person must live in an eligible setting. No more than three persons with developmental disabilities may reside in one residential setting, unless they are all members of the same family. The state employs the 300 percent of Supplemental Security Income (SSI) special income eligibility standard. |
| Funding Limit | $35,000/year. |
| Funding Parameters | Individual funding amount previously was determined by each Community Centered Board (CCB). Board policies varied with respect to the amounts authorized. As a result of a CMS waiver review, the state has switched to determining the individual funding amount based on the approved services in each person’s plan. |
| Exceptions to Funding Limit | Colorado does not provide for exceptions to the overall funding limit. |
| Transition to Comprehensive Waiver | Entrance to 24-Hour Comprehensive Supports Waiver is limited to available openings. Entrance is prioritized to individuals experiencing crisis and persons aging out of children’s services. |
| Self-Direction | Limited Self-Direction. Some CCBs offer an “agency with choice” option that permits individuals to recruit workers who are then employed by CCB. Participants also receive “supporting living consultation” services that include assistance with decision-making, planning daily activities, and direct assistance to access community resources and/or service providers. |
| SUPPORTS WAIVER SERVICES | ||
|---|---|---|
| Support/Service Category | Y/N | Colorado Waiver Services |
| Case Management/Service Coordination | N | [Case management is furnished through targeted case management coverage] |
| Supports of Participant Direction (Support Broker) | N | |
| In-Home Services | Y | Personal Care, Specialized Habilitation, Household Activities |
| Respite | N | |
| Day Supports | Y | Community Access, Pre-vocational Services |
| Health Related | Y | Vision/Hearing/Dental Services; Personal Care Services Requiring Medical Professionals |
| Supported Employment | Y | Supported Employment |
| Transportation | Y | Transportation |
| Person Directed Goods and Services | N | |
| Equipment/Supplies | Y | Environmental Engineering* |
| Vehicle Repair/Modification | Y | Environmental Engineering* |
| Clinical Services | Y | Professional Services [behavioral services, therapeutic services, communication services] |
| Environmental Accessibility Adaptations | Y | Environmental Engineering* |
| Financial Management Services | N | |
| Family and Caregiver Training | N | |
| Other | Y | Supported Living Consultation; Mentorship activities |
| * Environmental engineering spans home and vehicles modifications as well as the acquisition of assistive technology and adaptive equipment. | ||
Background Information: Supported Living Services Waiver
Colorado was the first state to design and implement a “supports waiver.” In 1991, Colorado was one of eight states selected by the federal Health Care Financing Administration (HCFA, now CMS) to offer Community Supported Living Arrangements (CSLA) services. When the CSLA authority expired in 1995, Colorado decided to continue furnishing these services through a separate HCBS waiver (Supported Living Services (SLS) Waiver) that would operate side-by-side with the longer standing HCB-DD Waiver.
In the late 1990s, Colorado engaged in the Systems Change Project. An outcome of this project was to revamp both waivers to divide state payments for waiver services between comprehensive and supports services. The project also envisioned the state’s focusing on the expansion of the SLS Waiver as a means of reducing or containing the waiting list for community services. Systems Change featured positioning the state’s network of CCBs as “managed services organizations” and altering the flow of funding from a “fee for service” model to a quasi-capitated model. CCBs are nonprofit organizations that function as the single point of entry to community services for specified service areas. CCBs perform intake and case management as well as contract with service providers. CCBs also furnish various types of waiver services. Under Systems Change, SLS Waiver payments were restructured to a “per member per month” model and CCBs were expected to achieve performance minimums for participant enrollment within the overall state funding allocation. CCBs were given latitude in authorizing individual funding levels.1
The SLS Waiver was designed to furnish a comparably modest amount of supports to individuals who do not require 24/7 services and live with their families or in other living arrangements. Based on experience with the predecessor CSLA program, state officials believed that furnishing less than comprehensive supports would reduce pressures for costly out-of-home residential services. During the late 1990s, Colorado restricted growth in Comprehensive Waiver services and directed new funding to the SLS Waiver. The SLS Waiver also grew by virtue of the refinancing of state-funded services. Post 2000, the overall growth in Colorado community developmental disabilities services was affected by the downturn in the state’s economy and the state’s constitutional tax and spend limitation. Growth in Comprehensive Waiver services was held largely to accommodating youth aging out of state-funded residential services. This constrained state funding environment was offset somewhat by counties adopting mill levies earmarked for developmental disabilities services.
The operation of the SLS Waiver has varied by CCB. While all CCBs receive the same per participant payment ($16,445/participant/year in 2006), CCBs vary in their practices concerning the amount of services authorized for each participant. Some CCBs authorize a uniform amount while others vary the amount authorized based on individual needs. The program’s $35,000 funding limit is rarely authorized. CCBs also vary with respect to the types of services and supports that are authorized and the degree of participant/family flexibility in service selection. Issues have arisen concerning whether the program’s funding limit creates conflicts between the individual and family with respect to daytime activities, such as community participation and community employment.
State officials report that the SLS Waiver framework has created an atmosphere in which families are more prepared to think in terms of what services and supports they can provide for the individual and what they need the state to provide rather than focusing on what the state alone can provide. SLS also allows Colorado to offer some services to individuals who are on the waiting list for out-of-home placements but not in enough of a crisis situation to be immediately placed in the comprehensive waiver. The overall impact of the SLS Waiver is that more individuals now receive services and more individuals are able to access these services without out-of-home placements. This has also had the effect of reducing per participant costs of services system-wide. Informants also describe the waiver program as a precursor to self-directed services because it allows individuals and families more flexibility in arranging services and choosing providers. While there have been discussions within Colorado concerning implementing full-featured self-direction, the discussions have not resulted in modifications to the SLS Waiver.
In January 2006, there were 1,118 people waiting for Comprehensive waiver services and 2,171 people waiting for SLS Waiver services. Colorado has had a persistent waiting list for community services for many years. Some individuals wait-listed for HCB-DD Waiver services are persons who participate in the SLS Waiver program.
Major Issue(s):
CMS has recently challenged Colorado’s practices in operating its HCBS waiver programs for people with developmental disabilities. In particular, CMS has raised serious questions whether the latitude afforded CCBs in administering waiver services results in inconsistent treatment of program participants CCB-to-CCB. CMS has instructed Colorado to revamp its payments for waiver services. The state is implementing new policies to ensure uniformity in the authorization of services across the state.
In addition, in 2001, Colorado was sued in federal court concerning the waiting list. The aim of this lawsuit was to force the state to expand community residential services by expanding the use of small ICFs/MR. This lawsuit was dismissed by the federal district court in late 2005. The 10th Circuit Court of Appeals upheld the dismissal in 2006.
Statistical Profile
| WAIVER PARTICIPANTS BY YEAR | ||||||||
|---|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 |
| Comprehensive | 3,466 | 3,648 | 3,785 | 3,963 | 3,996 | 3,996 | 4,151 | 4,232 |
| Supports | 2,959 | 2,975 | 2,978 | 2,978 | 3,116 | 3,568 | 3,652 | 3,661 |
| Total Participants | 6,425 | 6,623 | 6,763 | 6,941 | 7,112 | 7,564 | 7,803 | 7,893 |
| Supports Waiver % of Total Participants | 46.1% | 44.9% | 44.0% | 42.9% | 43.8% | 47.2% | 46.8% | 46.4% |
Between 2000 and 2007, total Colorado waiver enrollment will have increased by 22.8 percent. Enrollment in each waiver increased at about the same pace. Since 2000, the proportion of SLS Waiver participants to total Colorado waiver participants has remained roughly the same.
| COLORADO WAIVER ENROLLMENT |
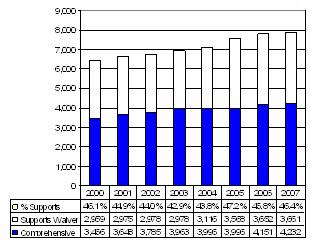 |
| EXPENDITURES BY YEAR | ||||||||
|---|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 |
| Comprehensive ($M) | $158.8 | $172.7 | $185.0 | $191.1 | $188.7 | $184.6 | $228.3 | $251.9 |
| Per Participant | $45,804 | $47,333 | $48,870 | $48,224 | $47,228 | $46,206 | $54,999 | $59,534 |
| Supports ($M) | $32.0 | $34.4 | $34.5 | $41.2 | $42.8 | $50.0 | $58.4 | $60.0 |
| Per Participant | $10,800 | $11,559 | $11,574 | $13,851 | $13,736 | $14,013 | $15,983 | $16,383 |
| Total Expenditures ($M) | $190.8 | $207.1 | $219.5 | $232.6 | $231.5 | $241.8 | $286.7 | $311.9 |
| Supports Waiver % of Total Expenditures | 16.8% | 16.6% | 15.7% | 17.7% | 18.5% | 20.7% | 20.4% | 19.2% |
| Cost Per Participant: % Supports to Comprehensive | 23.6% | 24.4% | 23.7% | 28.7% | 29.1% | 30.1% | 29.1% | 27.5% |
| Blended Cost Per Participant | $29,696 | $31,270 | $32,456 | $32,531 | $32,551 | $31,967 | $36,742 | $39,516 |
| COLORADO WAIVER EXPENDITURES ($M) |
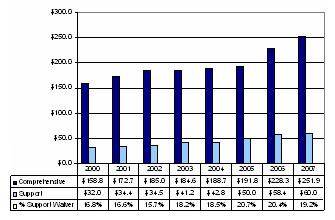 |
Between 2000 and 2007, total Colorado waiver expenditures will have increased by 63.5 percent. Expenditures leveled off between 2002 and 2005 due to state budget shortfalls. Additional funds were appropriated for 2006 and 2007. The proportion of dollars allocated to SLS Waiver services has ranged between 16-21 percent. Since 2003, the relationship between SLS and Comprehensive Services waiver per participant costs has remained relatively steady at 28-29 percent.
| COLORADO EXPENDITURES PER PARTICIPANT |
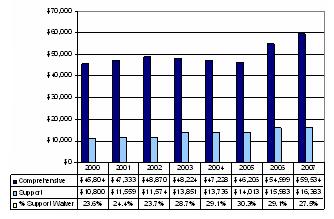 |
| WEB-ACCESSIBLE RESOURCES/ADDITIONAL INFORMATION | |
|---|---|
| Resource | Description/Web-Address |
| Start Here: A Resource Guide, Colorado Division for Developmental Disabilities, 2003 | Provides an overview of Colorado community services http://cdhs.state.co.us/ohr/StartHere-AResourceGuide.pdf |
| Home and Community-Based Services Medicaid Waivers | Six page description of waivers for Colorado citizens http://chcpf.state.co.us/HCPF/MedicaidEligibility/mefcc.asp |
Document Inventory
- Individual Choice Statement Both Waivers, Colorado HCPF Home and Community-Based Services Medicaid Waivers
- Services for People With Disabilities 2006 Legislative Briefing, 372 Lag and Initial for Comprehensive and Support Waivers 2002-2004
- Comprehensive and Support Waiver 2004-2009 renewal applications, and amended 2004-2009 renewal applications
| STATE CONTACT INFORMATION | |
|---|---|
| Name | Jay Kauffman |
| Agency | Division for Developmental Disabilities Colorado Department of Human Services |
| Address | 3824 W. Princeton Circle Denver, CO 80236 |
| Telephone | 303-866-7455 |
| Jay.Kauffman@state.co.us | |
CONNECTICUT
| WAIVERS | |||||
|---|---|---|---|---|---|
| Waiver Title | Type | CMS Waiver # | Participants (2006) | Start Date | Status |
| Individual and Family Support (IFS) Waiver | Supports | 0426 | 3,115 | 02/2005 | Initial |
| Comprehensive Support Waiver | Comprehensive | 0437 | 4,908 | 10/2005 | On-going |
| BASIC SUPPORT WAIVER FEATURES | |
|---|---|
| Supports Waiver Target Population | Children age three and older and adults with mental retardation and other developmental disabilities (MR/DD) who do not require paid 24-hour care or supervision as a result of the natural or informal supports in place, or as a result of the individual’s level of supervision needs. |
| Funding Limit | $52,000/year. |
| Funding Parameters | There are limits on three groups of waiver services:
Exceptions to these limits may be approved. Home and vehicle modifications and Family and Individual Consultation and Support (FICS) are subject to limits specified in the waiver. |
| Exceptions to Funding Limit | None. Persons who require additional services and supports are transitioned to Comprehensive Support Waiver. |
| Transition to Comprehensive Waiver | Persons who require more intensive services may be transitioned to Comprehensive Support Waiver. |
| Self-Direction | Full-Featured. Waiver earned CMS Independence Plus designation. Individuals may opt to exercise both budget and employer authority. Employer authority also includes an agency with choice option. Waiver provides for both support broker (FICS) and financial management services. |
| SUPPORTS WAIVER SERVICES | ||
|---|---|---|
| Support/Service Category | Y/N | Connecticut Waiver Services |
| Case Management/Service Coordination | N | [Targeted case management services are furnished by Department of Mental Retardation case managers] |
| Supports of Participant Direction (Support Broker) | Y | FICS |
| In-Home Services | Y | Personal Support; Individual Support Habilitation; Adult Companion; Supported Living |
| Respite | Y | Respite |
| Day Supports | Y | Group Day Service; Individual Day Support |
| Health Related | N | |
| Supported Employment | Y | Supported Employment |
| Transportation | Y | Transportation |
| Person Directed Goods and Services | N | |
| Equipment/Supplies | Y | Adaptive Aids; PERS; Specialized Medical Equipment and Supplies |
| Vehicle Repair/Modification | Y | Vehicle Modifications |
| Clinical Services | Y | Consultative Service |
| Environmental Accessibility Adaptations | Y | Environmental Adaptations |
| Financial Management Services | N | [Funded administratively] |
| Family and Caregiver Training | Y | Family Training |
| Other | Y | Interpreter Services |
Background Information: Supported Living Services Waiver
In 2005, Connecticut reconfigured its HCBS waiver for individuals with mental retardation. This reconfiguration involved splitting the waiver into two new waivers: the Comprehensive Support Waiver and the Individual and Family Support (IFS) Waiver. In addition, the state also incorporated self-direction features into both waivers.
In part, the reconfiguration also was driven by the settlement agreement that was arrived at in the Arc of Connecticut v. O’Meara waiting list lawsuit. In the settlement agreement, the state agreed to expand the availability of comprehensive services over a 5-year period and take other steps to revamp how waiver services are operated, including assuring that all necessary services are furnished to waiver participants in accordance with CMS State Medicaid Director Letter #4. Dividing the existing waiver into comprehensive and supports waivers was designed to ensure compliance with State Medicaid Director Letter #4.
Once both waivers were approved by CMS, Connecticut assigned waiver participants to one of the two new waivers based on living arrangement and service plan costs. Persons served in licensed community residences or who had service plans in excess of $52,000 were assigned to the Comprehensive Support Waiver. Other individuals were assigned to the IFS Waiver. In addition, Connecticut is stepping up waiver enrollments to include individuals who receive state-funded services but can qualify for Medicaid. Waiting list reduction entails offering waiver services to persons in the emergency and Priority 1 waiting list category (services required within one year). Individuals are offered services in the waiver that will meet their needs.
Both waivers include self-direction features. Connecticut had offered self-direction options under the previous waiver. The new waivers provide for more robust self-direction opportunities. About 800 individuals and families are currently taking advantage of these opportunities under both waivers.
Going forward, Connecticut is revamping how it determines provider waiver rates to improve funding portability by standardizing rates. This will facilitate participants exercising free choice of providers. Previously, Connecticut employed master contracts with providers that made it difficult for individuals to select a different provider. In the past, rates were determined through negotiation with provider agencies and varied considerably. In addition, Connecticut has developed a new individual budgeting tool that, when implemented, will replace the more current method of capping groups of services within each waiver.
Major Issue(s):
In April 2006, Connecticut’s waiver waiting list stood at 782 individuals. Under the terms of the settlement agreement, the state has made progress in reducing the waiting list. The waiting list is kept by urgency or need so individuals selected for the waiver are assigned to one of the two waivers. Statistical Profile
Statistical Profile
| WAIVER PARTICIPANTS BY YEAR | |||||||
|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006* |
| Comprehensive | 5,076 | 5,508 | 5,972 | 5,825 | 6,356 | 6,583 | 4,289 |
| Supports | 0 | 0 | 0 | 0 | 0 | 0 | 3,115 |
| Total Participants | 5,076 | 5,508 | 5,972 | 6,825 | 6,356 | 6,583 | 8,023 |
| Supports Waiver % of Total Participants | 0% | 0% | 0% | 0% | 0% | 0% | 41.6% |
| * Approved application. | |||||||
Between 2000 and 2006 waiver enrollment increased by 44.7 percent. The decline in comprehensive waiver enrollment in 2006 reflects the transfer of individuals to the IFS Waiver.
| CONNECTICUT WAIVER ENROLLMENT |
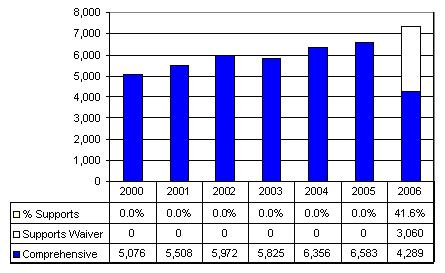 |
| EXPENDITURES BY YEAR | |||||||
|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 |
| Comprehensive ($M) | $345.0 | $350.1 | $386.5 | $393.8 | $410.7 | $421.3 | $309.7 |
| Per Participant | $67,965 | $63,563 | $64,726 | $67,607 | $64,614 | $64,000 | $72,205 |
| Supports ($M) | N/A | N/A | N/A | N/A | N/A | N/A | $74.8 |
| Per Participant | N/A | N/A | N/A | N/A | N/A | N/A | $24,443 |
| Total Expenditures ($M) | $345.0 | $350.1 | $386.5 | $393.8 | $410.7 | $421.3 | $384.5 |
| Supports Waiver % of Total Expenditures | N/A | N/A | N/A | N/A | N/A | N/A | 19.5% |
| Cost Per Participant: % Supports to Comprehensive | N/A | N/A | N/A | N/A | N/A | N/A | 33.9% |
| Blended Cost Per Participant | $67,965 | $63,563 | $64,726 | $67,605 | $64,614 | $64,000 | $52,320 |
| CONNECTICUT WAIVER EXPENDITURES ($M) |
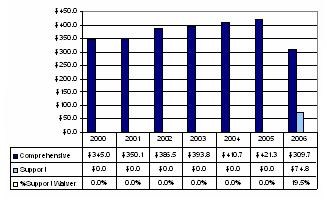 |
Between 2000 and 2006, total Connecticut waiver expenditures increased by 44.7 percent. In 2006, Comprehensive Waiver spending is dropping due to the transfer of participants to the IFS Waiver. The net effect of the implementation of the IFS Waiver is reducing overall per participant waiver expenditures.
| CONNECTICUT EXPENDITURES PER PARTICIPANT |
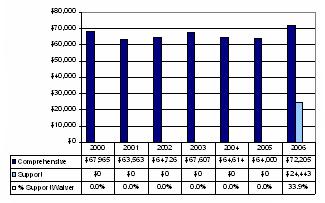 |
| WEB-ACCESSIBLE RESOURCES/ADDITIONAL INFORMATION | |
|---|---|
| Resource | Description/Web-Address |
| Connecticut Department of Mental Health (DMH) HCBS Waivers | Home for Connecticut mental retardation waivers http://www.dmr.state.ct.us/HCBS/index.htm |
| Individual and Family Fact Sheet About Connecticut HCBS Waivers | Web page contains two page IFS Waiver fact sheet http://www.dmr.state.ct.us/publications/centralofc/fact_sheets/ifs_hcbs… |
| Guidebook for Connecticut Consumers and Their Families | Web page provides a 56 page guidebook for individuals and families concerning Connecticut’s waivers http://www.dmr.state.ct.us/HCBS/HCBS_Guidebook.pdf |
| Consolidated Waiver Operations Manual for Both Connecticut Waivers | Web page offering of 95 page waiver operations manual for the support and comprehensive waivers http://www.dmr.state.ct.us/HCBS/Consolidated_HCBS_Manual_10_05_a.pdf |
| Frequently Asked Questions for Waiver Providers | Web page providing 14 pages of frequently asked questions concerning waiver services http://www.dmr.state.ct.us/HCBS/HCBS_Provider_FAQs.pdf |
Document Inventory
- Individual and Family Support Waiver Applications
- HCFA 372 reports: 2001-2004
| STATE CONTACT INFORMATION | |
|---|---|
| Name | Laura Nuss Director, Strategic Leadership |
| Agency | Department of Mental Retardation |
| Address | 460 Capitol Avenue Hartford, CT 06106 |
| Telephone | 860-418-6001 |
| laura.nuss@po.state.ct.us | |
FLORIDA
| WAIVERS | |||||
|---|---|---|---|---|---|
| Waiver Title | Type | CMS Waiver # | Participants (2006) | Start Date | Status |
| Family and Supported Living (FSL) Waiver | Supports | 294 | 5,721 | 10/2005 | Initial |
| Developmental Services HCBS Waiver | Comprehensive | 010b | 25,980 | 07/1995 | On-going |
| BASIC SUPPORT WAIVER FEATURES | |
|---|---|
| Supports Waiver Target Population | Children and adults with developmental disabilities who are on the waiver waiting list. Adults must be legally competent or have a legal guardian that helps them with their living situation. Adults also must be able to direct their own supports (or have family members who are willing to assist) in all but limited areas. |
| Funding Limit | $14,792 per year. |
| Funding Parameters | In the past, each waiver service had a dollar cap. The state has since discarded these service-by-service caps. |
| Exceptions to Funding Limit | None. |
| Transition to Comprehensive Waiver | Supports waiver participants maintain their position on the comprehensive waiver wait-list for potential future opportunities. |
| Self-Direction | No. Waiver, however, has participant/family-driven features. |
| SUPPORTS WAIVER SERVICES | ||
|---|---|---|
| Support/Service Category | Y/N | Florida Waiver Services |
| Case Management/Service Coordination | Y | Support Coordination |
| Supports of Participant Direction (Support Broker) | N | |
| In-Home Services | Y | In-Home Support |
| Respite | Y | Respite |
| Day Supports | Y | Adult Day Training |
| Health Related | N | |
| Supported Employment | Y | Supported Employment |
| Transportation | Y | Transportation |
| Person Directed Goods and Services | N | |
| Equipment/Supplies | Y | Consumable Medical Supplies; PERS |
| Vehicle Repair/Modification | N | |
| Clinical Services | Y | Behavioral Services |
| Environmental Accessibility Adaptations | Y | Environmental Adaptations |
| Financial Management Services | N | |
| Family and Caregiver Training | N | |
| Other | Y | Supported Living Coaching |
Background Information: FSL Waiver
The Family and Supported Living (FSL) Waiver was developed as part of Florida’s multi-year strategy to reduce the waiting list for home and community services. Florida’s efforts along these lines began in 1999 when the state settled the Prado-Steiman litigation and committed to serve all eligible individuals who were on the waiting list as of June 1999. As a result, the number of individuals receiving HCBS grew from 13,800 in 1999 to over 24,000 in 2004. Florida Governor Jeb Bush was instrumental in securing additional developmental disabilities funding during this period and continues to support year-over funding increases for developmental services. Despite tripling funding for developmental services and substantial expansion of the HCBS waiver, a “post-Prado” waiting list emerged that, at one point, reached about 15,000 individuals. The FSL Waiver was added in large part as a tool to support individuals and families who are on the comprehensive waiver waiting list by offering them a more limited package of in-home and other supports.
The FSL Waiver operates under a fixed dollar limit and offers basic services designed to support individuals who live with their families or who can live independently in the community with modest assistance. In July 2005, the program was expanded to include children as well as adults and the coverage of behavioral services was added. Florida triages waiver enrollment to direct individuals/families who do not require 24/7 services to the FSL Waiver.
The FSL Waiver has two relatively unique features. FSL Waiver participants receive support coordination services through independent support coordination agencies. After the first six months of enrollment, an individual/family may elect to reduce the intensity of support coordination in order to maximize the dollars available to purchase other services and supports. However, in practice, this option has almost never been selected. Second, the waiver includes the coverage of “supported living coaching,” a service designed to provide adults with a personal agent who assists them in meeting the challenges of everyday life. Supported living coaching has been covered in Florida’s comprehensive waiver for more than a decade and has been integral in supporting individuals in regular community living arrangements.
Major Issue(s):
Florida continues to aggressively expand services and supports for people with developmental disabilities. In November 2006, the waiting list stood at 12,011 people. FY 2005-2006 funding is enabling services to be further expanded to reach at least another 7,000 individuals. Statistical Profile
Statistical Profile
| WAIVER PARTICIPANTS BY YEAR | |||||||
|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 |
| Comprehensive | 21,126 | 24,910 | 25,921 | 24,301 | 24,079 | 23,353 | 25,980 |
| Supports | 0 | 0 | 0 | 0 | 0 | 2,650 | 5,721 |
| Total Participants | 21,126 | 24,910 | 25,921 | 24,301 | 24,079 | 26,003 | 31,629 |
| Supports Waiver % of Total Participants | 0% | 0% | 0% | 0% | 0% | 10.2% | 18.0% |
The year-over-year growth in waiver participants between 2005 and 2006 reflects a substantial increase in funding approved by the Florida legislature.
| FLORIDA WAIVER ENROLLMENT |
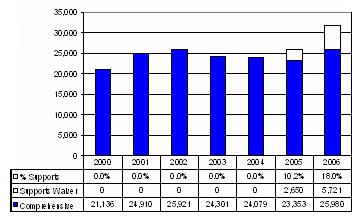 |
| EXPENDITURES BY YEAR | |||||||
|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 |
| Comprehensive ($M) | $251.8 | $419.1 | $487.5 | $554.4 | $598.5 | $664.0 | $681.5 |
| Per Participant | $11,921 | $16,183 | $18,805 | $22,677 | $26,377 | $28,433 | $26,303 |
| Supports ($M) | $0 | $0 | $0 | $0 | $0 | $5.6 | $49.8 |
| Per Participant | $0 | $0 | $0 | $0 | $0 | $2,105 | $8,700 |
| Total Expenditures ($M) | $251.8 | $419.1 | $487.5 | $554.5 | $598.5 | $669.6 | $731.2 |
| Supports Waiver % of Total Expenditures | 0% | 0% | 0% | 0% | 0% | 0.8% | 6.8% |
| Cost Per Participant: % Supports to Comprehensive | 0% | 0% | 0% | 0% | 0% | 10.2% | 33.1% |
| Blended Cost Per Participant | $11,921 | $16,183 | $18,805 | $22,677 | $26,377 | $25,751 | $23,069 |
| FLORIDA WAIVER EXPENDITURES ($M) |
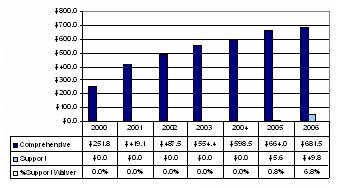 |
Florida experienced a 165.9 percent rise in overall waiver expenditures between 2000 and 2005. In 2006, the supports waiver and to a lesser degree the comprehensive waiver, grew another 9.2 percent while the people enrolled grew 27.0 percent in 2006.
| FLORIDA EXPENDITURES PER PARTICIPANT |
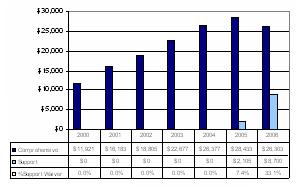 |
| WEB-ACCESSIBLE RESOURCES/ADDITIONAL INFORMATION | |
|---|---|
| Resource | Description/Web-Address |
| Agency for Persons with Disabilities (APD) | Web page provides an overview of Florida’s waivers for developmental disabilities http://apd.myflorida.com/2005-sc-handout-programs.htm#famlily-waiver |
| Consumer Guide for Family and Supported Living Waiver 2004 | Website with Consumer Guide for Family and Supported Living a 7 page document http://apd.myflorida.com/clients/docs/fsl_waiver.pdf |
Document Inventory
- 2003 HCBS Waiver Document
- 2004 Family and Supported Living Waiver Document
- November 2005 SPD presentation to Florida Legislature
- Family and Supported Living Waiver Services Directory
- Florida Medicaid 2005 and 2006 Developmental Disabilities Waiver Services Coverage and Limitations Handbooks
- Consumer Guide for the Family and Supported Living Waiver
- Individual Cost Guidelines for Children and Adults
- Have A Job Report, APD Waiting List Should Be Improved for Agency’s Planning and Budgeting Purposes (Report # 06-54 Office of Program Analysis & Governmental Accountability, Florida Legislature)
- HSRI Florida Visit Delmarva QA/QI Overview
- Interagency Quality Council June 2005 Minutes
- Developmental Disabilities Program Office E-Bulletin July 2002 and March 2004
- APD Crisis Review Committee
| STATE CONTACT INFORMATION | |
|---|---|
| Name | Linda Mabile Senior Management Analyst |
| Agency | Agency for Persons with Disabilities Community Development |
| Address | 4030 Esplanade Way, Suite 380 Tallahassee, FL 32399-0950 |
| Telephone | 850-414-9132 |
| Linda_Mabile@dcf.state.fl.us | |
INDIANA
| WAIVERS | |||||
|---|---|---|---|---|---|
| Waiver Title | Type | CMS Waiver # | Participants (2005) | Start Date | Status |
| Support Services Waiver | Supports | 387 | 3,548 | 04/2002 | On-going |
| Developmental Disabilities (DD) Waiver | Comprehensive | 378 | 5,400 | 09/1992 | On-going |
| BASIC SUPPORT WAIVER FEATURES | |
|---|---|
| Supports Waiver Target Population | Children and adults with developmental disabilities. |
| Funding Limit | $13,500 per year. |
| Funding Parameters | Case Management, Person-Centered Planning Facilitation and Transportation are funded outside the funding cap. There is an annual limit of $2,000 on respite care. |
| Exceptions to Funding Limit | Limited. |
| Transition to Comprehensive Waiver | As openings/funding available. |
| Self-Direction | No. |
| SUPPORTS WAIVER SERVICES | ||
|---|---|---|
| Support/Service Category | Y/N | Indiana Waiver Services |
| Case Management/Service Coordination | Y | Case Management and Initial and Outgoing Person-Centered Planning |
| Supports of Participant Direction (Support Broker) | N | |
| In-Home Services | N | |
| Respite | Y | Respite Care |
| Day Supports | Y | Community Habilitation Participation; Day Habilitation Service; Pre-vocational Service; Adult Day Services |
| Health Related | Y | Health Care Coordination; Enhanced Dental Service |
| Supported Employment | Y | Supported Employment Follow-along |
| Transportation | Y | Transportation |
| Person Directed Goods and Services | N | |
| Equipment/Supplies | Y | PERS; Specialized Medical Equipment/Supplies |
| Vehicle Repair/Modification | Y | Vehicle Modifications |
| Clinical Services | Y | Occupational Therapy; Physical Therapy; Speech/Language Therapy; Recreational Therapy; Music Therapy; Nutritional Therapy; Psychological Therapy; Behavioral Management |
| Environmental Accessibility Adaptations | N | |
| Financial Management Services | N | |
| Family and Caregiver Training | Y | Family and Caregiver Training |
| Other | Y | Interpretive Service; Crisis Intervention |
Background Information: Support Services Waiver
The Indiana Support Services Waiver was launched in 2002. Its purpose is to provide Medicaid-funded services and supports for children and adults with developmental disabilities who reside in the family home or who do not require 24/7 services. The creation of this waiver was an outgrowth of the state’s 317 Plan that aimed to expand and reform community services for people with developmental disabilities. The 317 Plan was developed by a task force made up of consumers, advocates and state officials and received gubernatorial support. The 317 Plan included several steps to refinance day and other services in order to leverage additional federal Medicaid dollars to reduce the state’s spiraling waiting list for community services. System reforms included adopting person-centered planning methods and placing greater stress on supporting individuals in integrated community settings and reducing the state’s over reliance on congregate care facilities.
The Support Services Waiver was designed to principally underwrite the costs of day time services, although the waiver offers some additional services supports. The Supports Services Waiver differs from a more typical supports waiver principally by not offering in-home and family support services. Indiana does not offer personal care services through its Medicaid state plan. Since 2002, the Support Services Waiver has grown to serve about 3,500 individuals. Per capita costs are running at approximately one-half the funding limit (taking into account services funded outside the limit). Going forward, the program may be expanded again to refinance other state-funded services and supports.
The longer-standing comprehensive Developmental Disabilities (DD) Waiver principally (but not exclusively) underwrites services and supports for individuals who require community residential services. In addition to residential services, the DD Waiver offers a more robust array of services than the supports waiver. Between 2001 and 2004, the number of individuals participating in the DD Waiver almost doubled, in part to capture additional federal Medicaid funds but also to underwrite the community placement of individuals from the state’s developmental centers. Indiana closed Muscatatuck Developmental Center and has targeted closure of Fort Wayne Developmental Center (its last state institution) in June 2007. Indiana also has a relatively large private intermediate care facility for the mentally retarded (ICF/MR) sector that currently serves about 3,800 individuals, most of whom reside in smaller group homes.
Major Issue(s):
Despite the implementation of the Support Services Waiver and the rapid expansion of DD Waiver, Indiana continues to experience a major upsurge in demand for community developmental disabilities services and supports. In April 2006, about 14,800 unduplicated persons were waiting for waiver services. In order to meet this demand, the state would have to more than double the number of individuals who receive waiver services. There is especially high demand for comprehensive waiver services, including by individuals who participate in the Support Services Waiver but are seeking residential and other supports. This high unmet demand in the face of the rapid increase in the number of waiver participants over the past several years is explained in part by the fact that waiver growth has been the result of substantial refinancing of services for individuals who were already receiving services in order to overcome shortfalls in state funding rather than expanding the number of people receiving services.
Indiana also has experienced rapid escalation in DD Waiver per participant costs. As a consequence, the state is implementing new cost controls. If these cost containment measures are successful, funds may be freed up to address the waiting list. Statistical Profile
Statistical Profile
| WAIVER PARTICIPANTS BY YEAR | |||||||
|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002* | 2003* | 2004* | 2005* | 2006** |
| Comprehensive | 2,081 | 2,646 | 3,567 | 4,665 | 5,303 | 5,400 | 5,304 |
| Supports | 0 | 0 | 449 | 2,997 | 3,658 | 3,548 | 4,591 |
| Total Participants | 2,081 | 2,646 | 4,016 | 7,662 | 8,961 | 8,948 | 8,818 |
| Supports Waiver % of Total Participants | 0% | 0% | 11.2% | 39.1% | 40.8% | 39.7% | 39.9% |
| * Based on Indiana Family and Social Services Administration periodic reports. ** Estimate based on year to date experience. | |||||||
Between 2000 and 2006, Indiana waiver enrollment has more than quadrupled. The addition of the Supports Services Waiver accounts for about 64 percent of the growth between 2002 and 2006.
| INDIANA WAIVER ENROLLMENT |
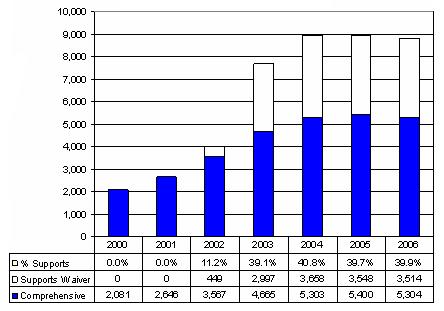 |
| EXPENDITURES BY YEAR | |||||||
|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002* | 2003* | 2004* | 2005* | 2006** |
| Comprehensive ($M) | $73.0 | $107.4 | $198.6 | $246.4 | $329.4 | $338.9 | $347.8 |
| Per Participant | $35,101 | $40,601 | $55,685 | $52,825 | $62,112 | $62,763 | $65,569 |
| Supports ($M) | $0 | $0 | $0.4 | $10.9 | $26.3 | $27.9 | $39.1 |
| Per Participant | $0 | $0 | $900 | $3,623 | $7,203 | $7,866 | $8,520 |
| Total Expenditures ($M) | $73.0 | $107.4 | $199.0 | $257.3 | $355.7 | $366.8 | $386.9 |
| Supports Waiver % of Total Expenditures | 0% | 0% | 0.2% | 4.2% | 7.4% | 7.6% | 10.1% |
| Cost Per Participant: % Supports to Comprehensive | 0% | 0% | 1.6% | 6.9% | 11.6% | 12.5% | 13.0% |
| Blended Cost Per Participant | $35,101 | $40,601 | $49,552 | $33,581 | $39,694 | $40,992 | $43,876 |
| * Based on Indiana Family and Social Services Administration periodic reports. ** Estimate based on year to date experience. | |||||||
| INDIANA WAIVER EXPENDITURES ($M) |
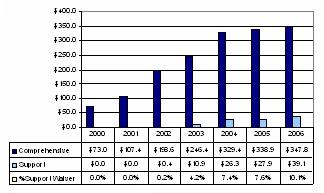 |
Between 2000 and 2006, the total Indiana waiver expenditures nearly quintupled, in part due to participant growth and in part due to rapidly escalating DD Waiver per capita costs. A relatively small share of the increase in spending is attributable to the implementation of the Supports Services Waiver. In 2006, per participant supports waiver costs were running at 13 percent of comprehensive waiver costs.
| INDIANA EXPENDITURES PER PARTICIPANT |
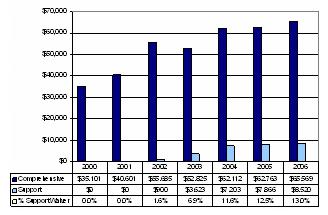 |
| WEB-ACCESSIBLE RESOURCES/ADDITIONAL INFORMATION | |
|---|---|
| Resource | Description/Web-Address |
| Indiana Family and Social Services Administration, People With Disabilities Division of Disability, Aging and Rehabilitative Services | Web page provides links to People With Disability information, including developmental disabilities services http://www.state.in.us/fssa/servicedisabl/ |
| Indiana’s Community-based Medicaid Waivers | Web page provides side-by-side comparisons of Indiana’s HCBS waivers http://in.gov/fssa/statistics/pdf/fssamedwaiverhart 20050930.pdf |
| Arc of Indiana | Useful guide to Medicaid and Medicaid Waivers in Indiana http://arcind.org/guide_to_medicaid_and_medicaid_w.htm Background information on the 317 Plan |
Document Inventory
- 2005 Support Service Waiver Renewal Application
- Developmental Disabilities Provider and Case Management Standards
| STATE CONTACT INFORMATION | |
|---|---|
| Name | Lynn Jump |
| Agency | Indiana Family and Social Services Administration People With Disabilities Division of Disability, Aging, and Rehabilitation Services Bureau of Developmental Disabilities Services |
| Address | P.O. Box 7083 Indianapolis, IN 46207-7083 |
| Telephone | 317-234-2764 |
| Lynn.Jump@fssa.in.gov | |
LOUISIANA
| WAIVERS | |||||
|---|---|---|---|---|---|
| Waiver Title | Type | CMS Waiver # | Participants (2005) | Start Date | Status |
| New Opportunities Waiver (NOW) | Comprehensive | 401 | 4,620 | 07/1992 | On-going |
| Children’s Choice | Supports | 381 | 785 | 02/2001 | On-going |
| Supports Waiver | Supports | N/A | 1 | 07/2006 | Initial |
| BASIC SUPPORT WAIVER FEATURES | |
|---|---|
| Supports Waiver Target Population | Children’s Choice: Children with developmental disabilities, birth through age 18 who live with their families. Supports Waiver: Adults with developmental disabilities, age 18 and older. |
| Funding Limit | Children’s Choice: $15,000 per year. Supports Waiver: No set limit; however, internal limits on the amount of specific services that may be authorized effectively cap this waiver at approximately $20,000. |
| Funding Parameters | Both Waivers: Amount authorized based on individual plan. Supports Waiver has dollar limits on specific services. |
| Exceptions to Funding Limit | Children’s Choice: Exceptions to funding limit may be authorized in crisis situations on a time limited basis. Supports Waiver: Exceptions to service funding limits may be authorized in order to assure participant health and welfare. |
| Transition to Comprehensive Waiver | Children’s Choice: Children who “age out” (reach their 19th birthday) will transfer with their slot to an appropriate MR/DD waiver as long as they remain eligible for waiver services. Supports Waiver: Transfer to NOW as slots are available. |
| Self-Direction | Children’s Choice: Limited. Families have flexibility in selection of services within the funding limitation. Agency with choice option available. Supports Waiver: No formal mechanisms. |
| CHILDREN'S CHOICE WAIVER SERVICES | ||
|---|---|---|
| Support/Service Category | Y/N | Louisiana Waiver Services |
| Case Management/Service Coordination | Y | Case Management |
| Supports of Participant Direction (Support Broker) | N | |
| In-Home Services | Y | Family Support |
| Respite | Y | Center-Based Respite |
| Day Supports | N | |
| Health Related | N | |
| Supported Employment | N | |
| Transportation | N | |
| Person Directed Goods and Services | N | |
| Equipment/Supplies | Y | Diapers |
| Vehicle Repair/Modification | Y | Environmental Accessibility Adaptations |
| Clinical Services | N | |
| Environmental Accessibility Adaptations | Y | Environmental Accessibility Adaptations |
| Financial Management Services | N | |
| Family and Caregiver Training | Y | Family Training |
| Other | N | |
| SUPPORTS WAIVER SERVICES | ||
|---|---|---|
| Support/Service Category | Y/N | Louisiana Waiver Services |
| Case Management/Service Coordination | N | [Case Management through Targeted Case Management] |
| Supports of Participant Direction (Support Broker) | N | |
| In-Home Services | Y | Personal Care Attendant |
| Respite | Y | Respite |
| Day Supports | Y | Group Employment; Day Habilitation and Training; Facility-Based Work |
| Health Related | Y | Individual Goods and Services (dental and vision) |
| Supported Employment | Y | Supported Employment |
| Transportation | N | |
| Person Directed Goods and Services | N | |
| Equipment/Supplies | Y | PERS |
| Vehicle Repair/Modification | N | |
| Clinical Services | N | |
| Environmental Accessibility Adaptations | N | |
| Financial Management Services | N | |
| Family and Caregiver Training | N | |
| Other | N | |
Background Information: Supports Waiver and Children’s Choice Waivers
Children’s Choice
The Children’s Choice Waiver was developed in lieu of Louisiana’s implementing the Katie Beckett (TEFR 134) Medicaid eligibility option due to cost concerns. The Children’s Choice waiver is designed to provide a limited array of services and supports to children who meet ICF/MR level of care and live with their families and afford access to Medicaid state plan benefits for a capped number of children. As initially implemented, the program operated under a $7,400/child annual funding limit. The limit was subsequently increased to $15,000 as a result of the efforts of advocacy groups. On average, Children’s Choice waiver participants receive about $12,500/year in Medicaid state plan services in addition to waiver services. As a consequence, the average amount expended on a Children’s Choice participant in 2005 was $21,710. The provision of family support services accounted for about 76 percent of waiver expenditures in 2005.
The New Opportunities Waiver (NOW) also serves children. However, there are 7-8 year wait times for entrance to NOW. A family may elect to accept Children’s Choice enrollment or continue to wait for a NOW opening. When a family that has been wait-listed for NOW accepts enrollment in the Children’s Choice waiver, the child is placed on inactive status on the NOW waiting list. While demand for NOW enrollment remains high, families have expressed satisfaction with the services and supports offered through Children’s Choice.
Supports Waiver
The Supports Waiver was originally intended to enable Louisiana to leverage additional federal Medicaid dollars and apply those dollars to reducing the state’s 13,000 person waiting list. In particular, the waiver design provided for refinancing state-funded adult vocational services and capturing the additional federal funds for application toward waiting list reduction. The Supports Waiver also was intended to create a viable alternative to NOW, which has experienced rapidly escalating costs since it was restructured in 2003.
In the aftermath of Hurricane Katrina, the state was forced to reduce the scope of the Supports Waiver to solely refinancing services for the current 1,800 recipients of state-funded vocational services and cannot deploy the additional federal dollars toward waiting list reduction. Despite this set back, shifting individuals to the Supports Waiver is expected to have positive outcomes in the form of giving individuals greater choices about their type of day support activity, including expanded community employment options. In addition, many of these individuals will now be able to access Medicaid State plan services. CMS approved the Supports Waiver for implementation on July 1, 2006.
Major Issue(s):
Louisiana continues to struggle with an especially large 13,000 person waiting list. In addition, Hurricane Katrina has negatively affected the state budget and, consequently, the capacity to expand services.
Statistical Profile
| WAIVER PARTICIPANTS BY YEAR | ||||||||
|---|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006* | 2007* |
| Comprehensive | 3,629 | 4,008 | 4,007 | 4,222 | 4,437 | 4,620 | 4,742 | 4,800 |
| Children's Choice | 0 | 0 | 225 | 587 | 762 | 785 | 800 | 800 |
| Supports | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2,088 |
| Total Participants | 3,629 | 4,008 | 4,232 | 4,809 | 5,199 | 5,405 | 5,542 | 7,688 |
| Supports Waiver % of Total Participants | 0% | 0% | 5.3% | 12.2% | 14.7% | 14.5% | 14.4% | 37.6% |
| * Estimates. | ||||||||
As can be seen, the number of Louisiana waiver participants has more than doubled since 2000. Nearly all of this growth is attributable to the implementation of the Children’s Choice waiver in 2002 and the addition of the Supports Waiver in 2007.
| LOUISIANA WAIVER ENROLLMENT |
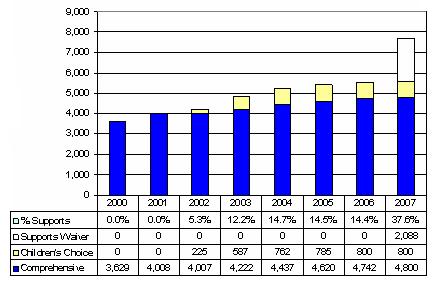 |
| EXPENDITURES BY YEAR | ||||||||
|---|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006* | 2007* |
| Comprehensive ($M) | $95.4 | $121.1 | $142.9 | $153.6 | $204.8 | $229.9 | $235.9 | $238.8 |
| Per Participant | $26,281 | $30,226 | $35,674 | $36,389 | $46,170 | $49,756 | $49,756 | $49,756 |
| Children's Choice ($M) | $0 | $0 | $0.9 | $3.8 | $5.2 | $7.3 | $7.4 | $7.4 |
| Per Participant | $0 | $0 | $4,000 | $6,500 | $6,841 | $9,255 | $9,255 | $9,225 |
| Supports ($M) | $0 | $0 | $0 | $0 | $0 | $0 | $0 | $36.0 |
| Per Participant | $0 | $0 | $0 | $0 | $0 | $0 | $0 | $17,243 |
| Total Expenditures ($M) | $95.4 | $121.1 | $143.8 | $157.4 | $210.1 | $237.2 | $243.3 | $282.2 |
| Supports Waiver % of Total Expenditures | 0% | 0% | 0.6% | 2.4% | 2.5% | 3.1% | 3.0% | 15.4% |
| Cost Per Participant: % Supports to Comprehensive | 0% | 0% | 11.2% | 17.9% | 14.8% | 18.6% | 18.6% | 30.2% |
| Blended Cost Per Participant | $26,281 | $30,226 | $33,979 | $32,730 | $40,392 | $43,885 | $43,901 | $36,707 |
| * Estimate. 2007 Support Waiver expenditures based on waiver application. | ||||||||
| LOUISIANA WAIVER EXPENDITURES ($M) |
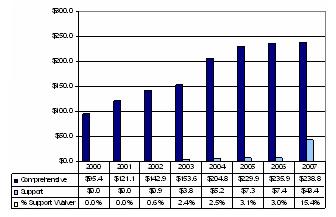 |
Between 2000 and 2007, total Louisiana waiver expenditures will have nearly tripled. Post-2004, the NOW comprehensive waiver experienced a substantial increase in per participant costs. The 2007 addition of the Supports Waiver will have a material effect in reducing overall per person costs.
| LOUISIANA EXPENDITURES PER PARTICIPANT |
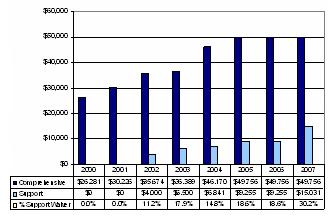 |
| WEB-ACCESSIBLE RESOURCES/ADDITIONAL INFORMATION | |
|---|---|
| Resource | Description/Web-Address |
| Office for Citizens with Developmental Disabilities (OCDD) main web portal | Web page provides People With Disability Information http://www.dhh.state.la.us/offices/?ID=77 |
| NOW Comprehensive Waiver | Web page on NOW comprehensive waiver http://dhh.louisiana.gov/offices/page.asp?ID=92&From Search=1&Detail=4042 |
| Children’s Choice Waiver | Web page for Children’s Choice waiver http://dhh.louisiana.gov/offices/page.asp?ID=92&Detail=4122 |
Document Inventory
- Fact Sheet on Louisiana’s HCBS Waiver -- NOW
- Louisiana Children’s Choice Waiver Fact Sheet
- 2006 Application for the Support Waiver
- CMS 372 Reports
| STATE CONTACT INFORMATION | |
|---|---|
| Name | Bonnie Callahan Executive Director |
| Agency | Office for Citizens with Developmental Disabilities Louisiana Department of Health and Hospitals |
| Address | 1201 Capital Access Road Baton Rouge, LA 70821 |
| Telephone | 225-219-0200 |
| bacallaha@dhh.la.gov | |
MISSOURI
| WAIVERS | |||||
|---|---|---|---|---|---|
| Waiver Title | Type | CMS Waiver # | Participants (2005) | Start Date | Status |
| MR/DD Community Supports Waiver (CSW) | Supports | 0404 | 808 | 07/2003 | On-going |
| MR/DD Comprehensive Waiver | Comprehensive | 0178 | 7,553 | 07/1988 | On-going |
| BASIC SUPPORT WAIVER FEATURES | |
|---|---|
| Supports Waiver Target Population | Children and adults with developmental disabilities. The supports waiver does not include residential services while the comprehensive waiver does. |
| Funding Limit | $22,000 per year. |
| Funding Parameters | Specific services are subject to cost limits. |
| Exceptions to Funding Limit | None. |
| Transition to Comprehensive Waiver | Individuals may transition to the MR/DD comprehensive waiver based on need and slot availability. |
| Self-Direction | Limited. Participants/families may elect to serve as the employer of record for personal assistance works. The same option is available in the comprehensive waiver. A fiscal intermediary is used to process payroll for participant-employed workers. Pending waiver renewal application provides for the addition of limited budget authority. |
| SUPPORTS WAIVER SERVICES | ||
|---|---|---|
| Support/Service Category | Y/N | Missouri Waiver Services |
| Case Management/Service Coordination | N | [Targeted case management. State employees serve as service coordinators.] |
| Supports of Participant Direction (Support Broker) | N | |
| In-Home Services | Y | Personal Assistant Individual; Personal Assistant Agency; Personal Assistant Medical/Behavioral; Personal Assistant Group |
| Respite | Y | In-Home Respite Day; In-Home Respite Hour; In-Home Respite Group; Out-of-Home Respite |
| Day Supports | Y | On-Site Day Habilitation Group; On-Site Day Habilitation Individual; Off-Site Day Habilitation Group; Off-Site Day Habilitation Individual; Community Specialist |
| Health Related | N | |
| Supported Employment | Y | Supported Employment -- Individual and Group |
| Transportation | Y | Transportation |
| Person Directed Goods and Services | N | |
| Equipment/Supplies | Y | Specialized Medical Equipment and Supplies |
| Vehicle Repair/Modification | Y | Environmental Accessibility Adaptations |
| Clinical Services | Y | Behavioral Therapy; Physical Therapy; Occupational Therapy; Speech Therapy; Crisis Intervention Prof; Crisis Intervention Tech; Communications Skills Instructor; Counseling |
| Environmental Accessibility Adaptations | Y | Environmental Accessibility Adaptations |
| Financial Management Services | N | [Funded administratively as noted in service category table] |
| Family and Caregiver Training | N | |
| Other | N | |
Background Information: Community Supports Waiver
Missouri operates three 1915(c) Home and Community Based Medicaid Waiver programs for individuals with mental retardation or other developmental disabilities: the Comprehensive Waiver; Missouri Children with Developmental Disabilities (MOCDD) Waiver (or the Sarah Jian Lopez Waiver); and Community Supports Waiver (CSW). The MOCDD Waiver is a model waiver enables children with developmental disabilities who are not otherwise eligible for Medicaid to access Medicaid State plan services.
The Comprehensive Waiver supports children and adults with developmental disabilities in the family home and community living arrangements (principally Individualized Supported Living settings for up to three individuals). There is limited utilization of ICF/MR services in Missouri apart from the state-operated Habilitation Centers (Missouri’s large public institutions). In Missouri, counties may establish “SB 40 Boards,” funded by local mill levies. Some SB 40 Boards provide matching funds for waiver services.
The CSW began in July 2003 and was renewed in 2006. The renewal provides for the expansion of CSW to 1,089 people by 2008. CSW was launched to serve as a lower-cost alternative to the comprehensive waiver and as a vehicle to reduce the waiting list. CSW also built on Missouri’s experience in operating state-funded family-centered services. The CSW services match comprehensive waiver services except that CSW does not offer residential services. In addition, CSW is subject to a $22,000/year cost limit that was increased while the MR/DD Comprehensive Waiver was also being renewed this year.
Missouri was one of the first states to install the “employer authority” in its HCBS waivers. Individuals and families are supported in serving as the common-law employers of personal assistance workers. The state employs the Organized Health Care Delivery System mechanism to facilitate consumer-direction of workers, including engaging a fiscal intermediary to perform payroll functions. Missouri is piloting a more robust approach to participant direction through an Independence Plus Pilot Program facilitated by a CMS Real Choice Systems Change grant.
Major Issues/Current Situation:
In December 2005, there were 441 persons waiting for Comprehensive Waiver residential services and another 3,246 persons waiting for CSW. For FY 2005-2006, the Missouri Legislature provided funding to reduce the waiting list by 370 persons, split evenly between both waivers. Progress has been made in reducing the residential services waiting list but the CSW waiting list grew by 16 percent (450 individuals) between December 2004 and December 2005.
A major current focus in Missouri is reducing the number of individuals served at the state’s Habilitation Centers by approximately 25 percent. Statistical Profile
Statistical Profile
| WAIVER PARTICIPANTS BY YEAR | |||||||
|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 |
| Comprehensive | 7,827 | 8,122 | 7,999 | 7,568 | 7,444 | 7,553 | 7,782 |
| Supports | 0 | 0 | 0 | 0 | 487 | 808 | 897 |
| Total Participants | 7,827 | 8,122 | 7,999 | 7,568 | 7,922 | 8,361 | 8,679 |
| Supports Waiver % of Total Participants | 0% | 0% | 0% | 0% | 6.0% | 9.7% | 10.3% |
During the period 2000-2006, total waiver enrollment in Missouri increased by 10.9 percent. In recent years, CSW has been the principal source of increased waiver enrollment.
| MISSOURI WAIVER ENROLLMENT |
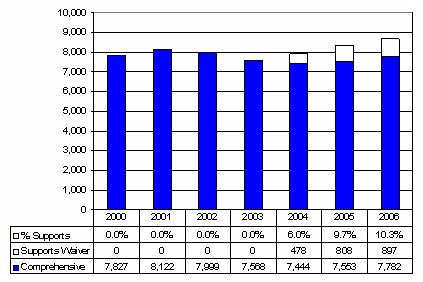 |
| EXPENDITURES BY YEAR | |||||||
|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 |
| Comprehensive ($M) | $199.9 | $217.4 | $238.1 | $268.5 | $272.3 | $275.4 | $289.6 |
| Per Participant | $25,544 | $26,762 | $29,770 | $35,475 | $36,585 | $36,466 | $37,208 |
| Supports ($M) | $0 | $0 | $0 | $0 | $1.6 | $4.3 | $3.8 |
| Per Participant | $0 | $0 | $0 | $0 | $3,299 | $5,360 | $4,222 |
| Total Expenditures ($M) | $199.9 | $217.4 | $238.1 | $268.5 | $273.9 | $279.8 | $293.3 |
| Supports Waiver % of Total Expenditures | 0% | 0% | 0% | 0% | 0.6% | 1.5% | 11.3% |
| Cost Per Participant: % Supports to Comprehensive | 0% | 0% | 0% | 0% | 31.5% | 50.8% | 33.7% |
| Blended Cost Per Participant | $25,544 | $26,762 | $29,770 | $35,475 | $34,575 | $33,453 | $33,806 |
| MISSOURI WAIVER EXPENDITURES ($M) |
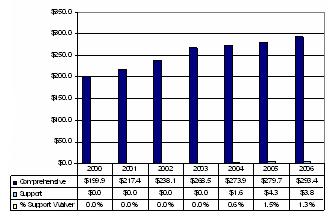 |
Between 2000-2006, Missouri’s total HCBS waiver expenditures grew by 48.7 percent. Expenditure growth slowed appreciably in 2003-2004 due to state budget shortfalls.
| MISSOURI EXPENDITURES PER PARTICIPANT |
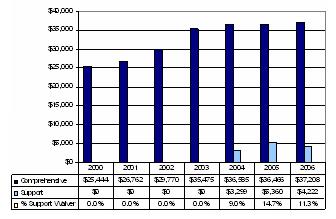 |
| WEB-ACCESSIBLE RESOURCES/ADDITIONAL INFORMATION | |
|---|---|
| Resource | Description/Web-Address |
| Missouri Department of Health, Division of Mental Retardation and Developmental Disabilities | Web page describes waiver services in Missouri http://dmh.mo.gov/mrdd/progs/waiver/factsheet.htm |
| Fact Sheet About Missouri’s Three Waivers | Web page provides information about Missouri’s three HCBS waivers http://www.dmh.mo.gov/mrdd/progs/waiver/factsheet.htm |
| Independence Plus Pilot | Website that contains information about Missouri’s Independence Plus Pilot http://www.ihd.umkc.edu/independenceplus/index.htm |
Document Inventory
- 2003 CSW application
- Comp & Support Waiver HCFA 372s for 2003, 2004 & 2005
- 2005 Amendment to Support Waiver
- DMR/DD updated expenditure and waiver participant count 2000-2008
- Missouri’s Medicaid Waiver for Persons with Mental Retardation and Developmental Disabilities Fact Sheet
- MR/DD Systems Transformation Initiative
| STATE CONTACT INFORMATION | |
|---|---|
| Name | Kay Green |
| Agency | Division of Mental Retardation and Developmental Disabilities Department of Mental Health |
| Address | P.O. Box 687 Jefferson City, MO 65101 |
| Telephone | 573-751-8213 |
| kay.green@dmh.mo.gov | |
MONTANA
| WAIVERS | |||||
|---|---|---|---|---|---|
| Waiver Title | Type | CMS Waiver # | Participants (2005) | Start Date | Status |
| Community Supports Waiver (CSW) | Supports | 0371 | 262 | 09/2001 | On-going |
| HCBS Waiver for Individuals with Developmental Disabilities | Comprehensive | 0208 | 1,882 | 12/1981 | On-going |
| BASIC SUPPORT WAIVER FEATURES | |
|---|---|
| Supports Waiver Target Population | Individuals 18 years or older who meet the Montana State definition of developmental disability according to MCA 53-20-202(3). |
| Funding Limit | $7,800/year. |
| Funding Parameters | All participants are eligible for base funding of $7,800/year. |
| Exceptions to Funding Limit | Cap can be exceeded under three conditions: (1) Short-term crisis (less than one year) (usually means hiring additional staffing); (2) Private duty nursing needs; and (3) Exceptional transportation needs (in practice, Montana has never exceeded the cost cap for exceptional transportation needs). |
| Transition to Comprehensive Waiver | Individuals may transition to comprehensive waiver based on need and slot availability. |
| Self-Direction | Limited. Waiver participants have state or contracted case managers who employ a person-centered planning process to help participant and/or family identify support needs. Participants have flexibility in choosing providers and negotiating service costs. |
| SUPPORTS WAIVER SERVICES | ||
|---|---|---|
| Support/Service Category | Y/N | Montana Waiver Services |
| Case Management/Service Coordination | N | [Case Management is furnished through targeted case management coverage.] |
| Supports of Participant Direction (Support Broker) | N | |
| In-Home Services | Y | Homemaker; Personal Care; Adult Companion; Residential Habilitation |
| Respite | Y | Respite |
| Day Supports | Y | Pre-vocational and Day Habilitation |
| Health Related | Y | Private Duty Nursing and Health/Safety/Maintenance |
| Supported Employment | Y | Supported Employment |
| Transportation | Y | Transportation (rides) and Transportation (client driving related expenses) |
| Person Directed Goods and Services | N | |
| Equipment/Supplies | Y | Specialized Medical Equipment and Supplies |
| Vehicle Repair/Modification | N | |
| Clinical Services | N | |
| Environmental Accessibility Adaptations | Y | Environmental Modifications |
| Financial Management Services | N | |
| Family and Caregiver Training | N | |
| Other | Y | Education (course work) and Social, Leisure, Recreation |
Background Information: Community Supports Waiver
The Community Supports Waiver (CSW) began in 1999 as a distinct waiver service “package” that was nested within Montana’s comprehensive waiver. The package was added as a response to the growing waiting list for services. Many wait-listed individuals lived with their natural families or wanted to live on their own but needed help. Financial resources were limited, so the waiver community supports package was designed to meet the “essential needs of persons in the effort to achieve and maintain successful placements in a variety of settings” and rely heavily on natural supports. The dollar-capped package emphasized maximum flexibility and efficiency in meeting participant needs. Services were designed to be portable -- funds would follow an individual if the person selected a different service provider or moved to a new community. Case managers were asked to support individuals and families in identifying needed services and supports.
The addition of the community supports “package” to the comprehensive waiver was approved in October 1999 based on an understanding between the state and HCFA (now CMS). After the issuance of State Medicaid Director Letter #4, Montana was informed that, in order to continue to offer the package, the state would have to shift community supports to a new waiver. Montana then submitted and CMS approved the CSW in 2001. The original 1999 funding limit of $7,800 per participant was carried forward to the new waiver and remains in effect.
Montana’s Comprehensive Waiver includes a children’s services component that blends in-home and out-of-home services for children with developmental disabilities. It also covers adult residential and daytime services and supported living services for adults.
Major Issue(s):
In 2005, there were 1,372 Montanans waiting for services with an average wait time of 36 months. There were 292 people waiting for the CSW and 1,080 waiting for the comprehensive waiver. Statistical Profile
Statistical Profile
| WAIVER PARTICIPANTS BY YEAR | ||||||
|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 |
| Comprehensive | 1,206 | 1,348 | 1,490 | 1,533 | 1,758 | 1,882 |
| Supports | 0 | 0 | 251 | 244 | 267 | 262 |
| Total Participants | 1,206 | 1,343 | 1,741 | 1,777 | 2,025 | 2,144 |
| Supports Waiver % of Total Participants | 0% | 0% | 14.4% | 13.7% | 13.2% | 12.2% |
In 2000 and 2001, community support services were provided through the Comprehensive waiver. Between 2000 and 2005, the number of waiver participants increased by 77.8 percent. Since 2002 there has been little change in the number of supports waiver participants.
| MONTANA WAIVER ENROLLMENT |
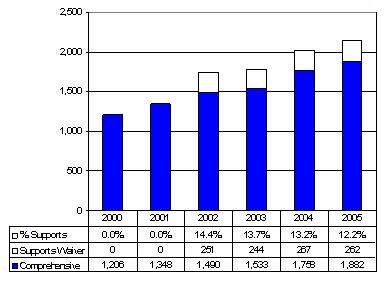 |
| EXPENDITURES BY YEAR | ||||||
|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 |
| Comprehensive ($M) | $33.6 | $36.9 | $41.9 | $58.5 | $53.9 | $56.3 |
| Per Participant | $27,829 | $27,466 | $28,105 | $38,138 | $30,632 | $29,893 |
| Supports ($M) | $0 | $0 | $0.1 | $1.4 | $1.3 | $1.6 |
| Per Participant | $0 | $0 | $515 | $5,676 | $4,712 | $6,252 |
| Total Expenditures ($M) | $33.6 | $36.9 | $42.0 | $59.9 | $55.1 | $57.9 |
| Supports Waiver % of Total Expenditures | 0% | 0% | 0.3% | 2.3% | 2.3% | 2.8% |
| Cost Per Participant: % Supports to Comprehensive | 0% | 0% | 1.8% | 14.9% | 15.4% | 20.9% |
| Blended Cost Per Participant | $27,829 | $27,466 | $24,124 | $33,708 | $27,259 | $27,006 |
| * Community Support included in Comprehensive Waiver Expenditures. | ||||||
| MONTANA WAIVER EXPENDITURES ($M) |
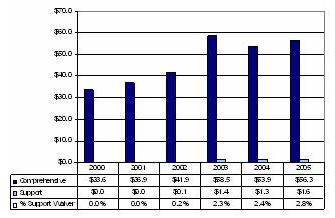 |
Between 2000 and 2005, Montana waiver expenditures increased by 72.3 percent. Only a small share of waiver funding is earmarked for the CSW. In 2005, expenditures per support waiver participant were 20.9 percent of comprehensive waiver expenditures. Comprehensive waivers per participant costs are significantly below levels observed in other comprehensive waivers, in part due to the low-cost child component.
| MONTANA EXPENDITURES PER PARTICIPANT |
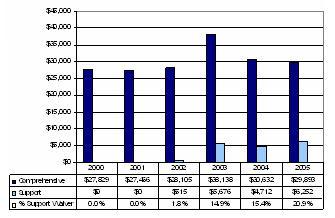 |
| WEB-ACCESSIBLE RESOURCES/ADDITIONAL INFORMATION | |
|---|---|
| Resource | Description/Web-Address |
| Montana Department of Public Health and Human Services, Disability Services Division, Developmental Disability Program | Who, What, How, Where? A list of web information related to Montana Developmental Disability Program http://www.dphhs.mt.gov/dsd/ddp/index.shtml |
| Home and Community-Based Waiver for Individuals with Developmental Disabilities (“The Big Waiver”) | MT 0208.90 Waiver http://www.dphhs.mt.gov/dsd/mt020890waiver/index.shtml |
Document Inventory
- HCFA 372 Reports
- 2005 Comp Waiver Renewal
- 2003 Support Waiver Renewal
- 2001 Support Waiver Application
| STATE CONTACT INFORMATION | |
|---|---|
| Name | Perry Jones |
| Agency | Montana Department of Public Health and Human Services Disability Services Division Developmental Disability Program |
| Address | P.O. Box 4210 Helena, MT 59604-4210 |
| Telephone | 406-444-2590 |
| pjones@mt.gov | |
NEBRASKA
| WAIVERS | |||||
|---|---|---|---|---|---|
| Waiver Title | Type | CMS Waiver # | Participants (2005) | Start Date | Status |
| HCB Day Services Waiver for Adults with Developmental Disabilities | Supports | 0394 | 664 | 03/2003* | On-going |
| Community Supports Program (CSP) HCBS Waiver for Adults with Developmental Disabilities | Supports | N/A | 0 | 07/2006 | On-going |
| HCBS Residential Waiver for Adults with Developmental Disabilities | Comprehensive | 0395 | 141 | 03/2003* | On-going |
| Comprehensive HCBS Waiver for Adults with Developmental Disabilities | Comprehensive | 0396 | 2,317 | 03/2003* | On-going |
| * Replaced single comprehensive waiver for adults that began in 1987. | |||||
| BASIC SUPPORT WAIVER FEATURES | |
|---|---|
| Supports Waiver Target Population | HCB Day Services Waiver for Adults: Targets adults with developmental disabilities age 21 and older. CSP Waiver: Also targets adults. |
| Funding Limit | HCB Day Services Waiver for Adults: No specific limit. CSP Waiver: $20,000/year. |
| Funding Parameters | HCB Day Services Waiver for Adults: Funding level based on objective assessment. CSP Waiver: The annual cap per person is $20,000 or his/her objectively assessed funding amount, whichever is less, except for individuals who need assistive technology, home modifications, or vehicle modifications. An additional $5,000 is available annually for the combined services. |
| Exceptions to Funding Limit | No. |
| Transition to Comprehensive Waiver | Based on slot availability. |
| Self-Direction | HCB Day Services Waiver for Adults: No. CSP Waiver: Employer but not budget authority. |
| SUPPORTS WAIVER SERVICES | ||
|---|---|---|
| Support/Service Category | Y/N | Nebraska Waiver Services |
| Case Management/Service Coordination | N | [Targeted case management coverage] |
| Supports of Participant Direction (Support Broker) | N | |
| In-Home Services | Y | Community Living |
| Respite | Y | Respite Care; Respite In-Home |
| Day Supports | Y | Day Supports |
| Health Related | N | |
| Supported Employment | N | |
| Transportation | N | |
| Person Directed Goods and Services | N | |
| Equipment/Supplies | Y | Assistive Technology; PERS |
| Vehicle Repair/Modification | Y | Vehicles Modification |
| Clinical Services | N | |
| Environmental Accessibility Adaptations | Y | Home Modification |
| Financial Management Services | N | |
| Family and Caregiver Training | N | |
| Other | N | |
| [Day Service Waiver for Adult DD Only] | ||
| Respite | Y | Respite |
| Day Supports | Y | Day Habilitation |
| Clinical Services | Y | Team Behavioral Consultation |
Background Information: Supports Waiver
Nebraska has three waivers for adults with developmental disabilities. There is also a relatively small HCBS waiver for children with developmental disabilities. In 2003, Nebraska replaced its single comprehensive waiver with three waivers. Two of the replacement waivers include the coverage of 24/7 residential services. The third waiver does not include residential services. The third waiver was designed to accommodate Nebraska’s long-standing policy of offering at least daytime services to youth with developmental disabilities after they leave the special education system. Previously, these individuals were enrolled in the single comprehensive waiver but not afforded access to residential services. The redesign of the previous comprehensive waiver brought Nebraska into compliance with the provisions of CMS State Medicaid Director Letter #4.
In April 2006, Nebraska developed and submitted a new Community Supports Program (CSP) HCBS Waiver to CMS with a July 1, 2006 effective date. The new waiver will serve 100 people in 2007 and scale up to 250 people by 2009. The CSP Waiver is designed to offer alternatives to the traditional model of services currently available through the Health and Human Services Developmental Disabilities System. The traditional model provides for services consisting of day and residential habilitation and respite, provided only by agencies certified as specialized providers of developmental disabilities services. The CSP Waiver would provide for a broader array of services and permit purchasing services from other community (independent or agency) providers. The aim is to give individuals and families more control over the type of services that they receive and the selection of the providers of those services, as well as allowing individuals to purchase services other than habilitative training. The CSP Waiver incorporates self-direction features.
The underlying philosophy of the CSP Waiver is to build upon the individual and family strengths and to strengthen and support informal and formal services already in place. The CSP utilizes a self-directed philosophy, designed to provide choice when determining the services and supports that are needed to maximize the independence of the person with a developmental disability. The individual has the right and responsibility to participate to the greatest extent possible in the development and implementation of his or her plan. The CSP is a funding stream that may be utilized either alone or in conjunction with other non-developmental disabilities funded services and supports, as appropriate for the individual. Individual funding is prior authorized by state staff at the local service area level and is based on the application of an objective assessment process.
Major Issue(s):
Like other states, Nebraska is wrestling with a persistent statewide waiting list. Currently there are 1,178 people waiting for services. There is a waiting list lawsuit that continues to be litigated. The lawsuit challenged both Nebraska’s practice of wait-listing individuals and its methods of authorizing community funding. In addition, the state is striving to strengthen HCBS waiver quality management in response to CMS review of the operation of its waivers. Statistical Profile
Statistical Profile
| WAIVER PARTICIPANTS BY YEAR | |||||||
|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 |
| Comprehensive | 2,372 | 2,504 | 2,490 | 2,558 | 2,550 | 2,458 | 2,386 |
| Supports | 0 | 0 | 0 | 192 | 595 | 664 | 937 |
| Total Participants | 2,372 | 2,504 | 2,490 | 2,750 | 3,145 | 3,122 | 3,323 |
| Supports Waiver % of Total Participants | 0% | 0% | 0% | 7.0% | 18.9% | 21.3% | 28.2% |
Between 2000 and 2006, total Nebraska waiver enrollment will have increased by increased by 40.1 percent. In general, waiver expansion since 2003 has been via the day services waiver. Enrollment in the comprehensive waivers has declined slightly.
| NEBRASKA WAIVER ENROLLMENT |
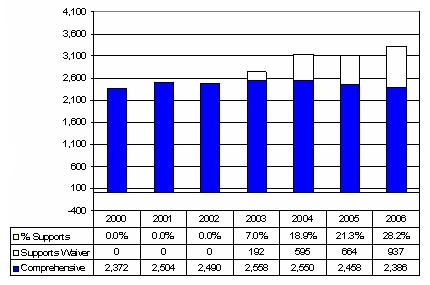 |
| EXPENDITURES BY YEAR | |||||||
|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 |
| Comprehensive ($M)* | $74.6 | $83.7 | $90.8 | $98.9 | $105.1 | $110.8 | $120.6 |
| Per Participant | $31,449 | $33,446 | $36,483 | $38,668 | $41,229 | $45,082 | $50,526 |
| Supports ($M)** | $0 | $0 | $0 | $0.4 | $5.9 | $7.8 | $8.6 |
| Per Participant | $0 | $0 | $0 | $2,069 | $9,865 | $11,745 | $9,158 |
| Total Expenditures ($M) | $74.6 | $83.9 | $90.8 | $99.3 | $111.0 | $118.6 | $129.1 |
| Supports Waiver % of Total Expenditures | 0% | 0% | 0% | 0.4% | 5.3% | 6.6% | 6.7% |
| Cost Per Participant: % Supports to Comprehensive | 0% | 0% | 0% | 5.4% | 23.9% | 26.1% | 18.1% |
| Blended Cost Per Participant | $31,449 | $33,446 | $36,483 | $36,109 | $35,294 | $37,988 | $38,881 |
| * The HCBS Comprehensive and Residential waivers. ** The HCBS Day Services waiver. | |||||||
| NEBRASKA WAIVER EXPENDITURES ($M) |
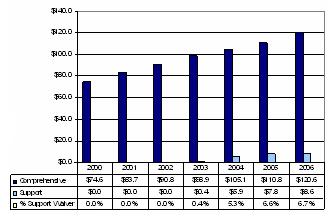 |
Total waiver expenditures will have increased by 73.2 percent between 2000 and 2006. While comprehensive waiver per participant costs have increased significantly year-over-year, the blended per participant cost has remained relatively stable since waiver expansion has been concentrated on the day services waiver.
| NEBRASKA EXPENDITURES PER PARTICIPANT |
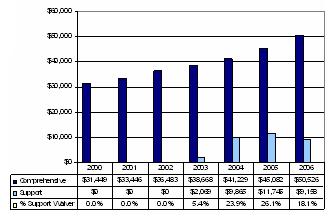 |
| WEB-ACCESSIBLE RESOURCES/ADDITIONAL INFORMATION | |
|---|---|
| Resource | Description/Web-Address |
| Nebraska Health and Human Services Developmental Disabilities System | Main website for developmental disabilities http://www.hhs.state.ne.us/dip/ded/dedindex.htm |
Document Inventory
- Approved waiver applications for residential and day services waivers
- Nebraska Health and Human Services Manual for HCBS and Targeted Case Management (TCM), and the child model waiver
- 2006 Community Supports Program Waiver Application
| STATE CONTACT INFORMATION | |
|---|---|
| Name | Pam Hovis Disability Services Coordinator |
| Agency | Nebraska Health and Human Services Developmental Disabilities System Aging and Disabilities Services |
| Address | P.O. Box 98925 Lincoln, NE 68509-8925 |
| Telephone | 402-479-5247 |
| pam.hovis@hhss.ne.gov | |
OHIO
| WAIVERS | |||||
|---|---|---|---|---|---|
| Waiver Title | Type | CMS Waiver # | Participants (2006) | Start Date | Status |
| Level One Waiver | Supports | 0380 | 3,344 | 03/2003 | Renewed |
| Individual Options (IO) Waiver Residential Facility Waiver (RFW) | Comprehensive | 0231 0291 | 11,634 | 02/1996 | On-going |
| BASIC SUPPORT WAIVER FEATURES | |
|---|---|
| Supports Waiver Target Population | Children and adults with MR/DD who have natural or informal supports in place. Individuals with aging caregivers are identified as a priority population. |
| Funding Limit | No fixed limit. |
| Funding Parameters | While the waiver does not have a fixed limit, groups of services are subject to dollar limits. In particular, homemaker/personal care, respite and transportation are subject to a $5,000/annual benefit limit. |
| Exceptions to Funding Limit | Supplemental funding up to $8,000 over a three year period is available to respond to emergencies. Such funding may take the form of additional personal care services. |
| Transition to Comprehensive Waiver | Based on the availability of IO Waiver slots. |
| Self-Direction | No. |
| SUPPORTS WAIVER SERVICES | ||
|---|---|---|
| Support/Service Category | Y/N | Ohio Waiver Services |
| Case Management/Service Coordination | N | [Targeted case management services are furnished through County Boards of MR/DD] |
| Supports of Participant Direction (Support Broker) | N | |
| In-Home Services | Y | Homemaker/Personal Care |
| Respite | Y | Respite Care |
| Day Supports | Y | Day Habilitation |
| Health Related | Y | Nutrition; Home-Delivered Meals |
| Supported Employment | N | |
| Transportation | Y | Transportation |
| Person Directed Goods and Services | N | |
| Equipment/Supplies | Y | Specialized Medical Adaptive Assistive Equipment and Supplies; PERS |
| Vehicle Repair/Modification | N | |
| Clinical Services | N | |
| Environmental Accessibility Adaptations | Y | Environmental Accessibility Adaptations |
| Financial Management Services | N | |
| Family and Caregiver Training | N | |
| Other | Y | Emergency Assistance |
Background Information: Supports Waiver
Ohio launched the Level One waiver in 2003 in order to provide a basic package of community services and supports to children and adults with developmental disabilities who live with their families or otherwise have other supports available to them. The waiver also was designed to leverage county property tax mill levy dollars to obtain additional federal Medicaid dollars to expand services in Ohio. The waiver was one element of Ohio’s Medicaid Reform strategy that has an overall goal of expanding access to community services. Historically, Ohio has relied more extensively on public/private ICF/MR services than is typical nationwide and underutilized the HCBS waiver program to meet the needs of people with developmental disabilities. Medicaid reform envisioned a major expansion of waiver services to meet service demand.
The Level One waiver provides a dollar-limited amount of personal care/homemaker/respite services in addition to day habilitation services and the coverage of home modifications and other equipment/supplies. The waiver also provides for supplemental emergency assistance funding to address situations when a person’s primary caregiver is unable or unavailable to meet the needs of the individual.
The Level One waiver operates side-by-side with the Individual Options (IO) Waiver that offers a full range of community services to participants, including supported living. Ohio is in the last stages of phasing out its Residential Facilities Waiver (RFW). RFW underwrites the costs of services in community residences. RFW services and participants are being shifted to the IO Waiver. In addition, in 2005 Ohio terminated its Medicaid state plan coverage of day habilitation and certain other therapeutic services to address compliance issues raised by CMS. The coverage of day habilitation was added to both the IO and Level One Waivers.
Ohio also is making major changes in the operation of its waivers in response to CMS concerns about inter-county variability in the authorization and delivery of waiver services. All waiver services are delivered through Ohio’s county boards of MR/DD. Counties had employed different policies and procedures in authorizing and paying for waiver services. CMS was concerned that these practices resulted in disparate treatment of waiver participants county-to-county. One element in this effort is instituting a new rate/reimbursement system that is designed to ensure greater uniformity in waiver payments. Ohio has not yet implemented participant-directed features in its waivers.
Major Issue(s):
The extent to which Ohio is satisfying the demand for waiver services is unclear. Waiting lists by waiver are maintained by counties but are not compiled statewide. There is longstanding but still unresolved litigation (Martin v. Taft) concerning access to Medicaid funded services and enabling people served in ICFs/MR to access alternative services in the community. The Martin v. Taft lawsuit was originally filed in federal court in 1989. By September 2006 the comprehensive waiver was serving 11,715 individuals and the support waiver served 3,984. Statistical Profile
Statistical Profile
| WAIVER PARTICIPANTS BY YEAR | |||||||
|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006** |
| Comprehensive* | 5,666 | 6,050 | 9,188 | 10,278 | 11,342 | 11,705 | 11,634 |
| Supports | 0 | 0 | 0 | 100 | 470 | 1,791 | 3,344 |
| Total Participants | 5,666 | 6,050 | 9,188 | 10,378 | 11,812 | 13,498 | 14,978 |
| Supports Waiver % of Total Participants | 0% | 0% | 0% | 1.0% | 4.0% | 13.3% | 22.3% |
| * Includes the IO Waiver and the RFW. ** Ohio Department of Mental Retardation and Developmental Disabilities projection. | |||||||
Between 2000 and 2005, total Ohio waiver enrollment increased by 138.2 percent. By 2008 this rose an additional 76.0 percent with the successful waiver renewals in January 2007 and careful examination of eligibility and waiver membership. As can be seen expansion of the Supports Services Waiver accounts for most of the enrollment growth from 2004 on.
| OHIO WAIVER ENROLLMENT |
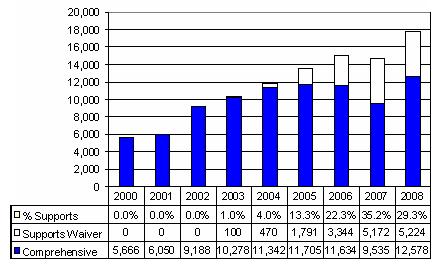 |
| EXPENDITURES BY YEAR | |||||||
|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006* |
| Comprehensive ($M) | $188.0 | $212.1 | $340.0 | $412.9 | $466.7 | $563.5 | $563.5 |
| Per Participant | $33,189 | $35,055 | $36,985 | $40,172 | $41,147 | $48,141 | $48,435 |
| Supports ($M) | $0 | $0 | $0 | $0.07 | $1.0 | $10.3 | $76.0 |
| Per Participant | $0 | $0 | $0 | $729 | $2,127 | $5,733 | $22,733 |
| Total Expenditures ($M) | $188.0 | $212.1 | $340.0 | $413.0 | $467.7 | $573.8 | $632.7 |
| Supports Waiver % of Total Expenditures | 0% | 0% | 0% | 0% | 0.2% | 1.8% | 11.9% |
| Cost Per Participant: % Supports to Comprehensive | 0% | 0% | 0% | 1.8% | 5.2% | 11.9% | 46.9% |
| Blended Cost Per Participant | $33,189 | $35,055 | $33,985 | $34,590 | $32,017 | $42,516 | $42,696 |
| * Projection of Ohio staff for comp waiver document for support waiver. | |||||||
| OHIO WAIVER EXPENDITURES ($M) |
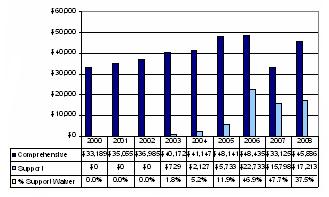 |
Ohio waiver expenditures increased by 205.2 percent between 2000 and 2005. In 2005, Level One waiver expenditures accounted for 1.8 percent of total expenditures even though 13.3 percent of all waiver participants were served in the Level One waiver. Level One waiver per participant expenditures were 11.9 percent of IO Waiver per participant spending. The increased implementation of the Level One waiver resulted in notable reduction in overall spending per waiver participant. These same trends are projected to continue with 95.9 percent additional total waiver expenditure expansion by 2008. The Level One waiver will then account for 13.5 percent of total expenditures and 29.3 percent of all waiver participants were served in the Support Services Waiver.
| OHIO EXPENDITURES PER PARTICIPANT |
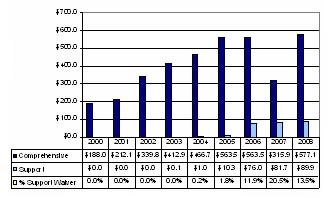 |
| WEB-ACCESSIBLE RESOURCES/ADDITIONAL INFORMATION | |
|---|---|
| Resource | Description/Web-Address |
| Ohio Department of MR/DD | Main web portal for Ohio MR/DD http://odmrdd.state.oh.us |
| Level One Waiver (support waiver) | Ohio’s support waiver for individuals with developmental disabilities http://odmrdd.state.oh.us/Includes/Waivers/LevelOne/ Level1Waivers.htm |
| Ohio’s Waivers for Developmental Disabilities | Ohio’s waiver information for developmental disabilities waivers http://odmrdd.state.oh.us/Includes/Waivers/Waivers.htm |
| Ohio’s New Waiver Reimbursement System: The Basics You Need to Know | Ohio’s Reimbursement System http://odmrdd.state.oh.us/Includes/Press_Releases/WaiverReimbursementDe… |
Document Inventory
- Individual Options (Comprehensive) Waiver 2004
- 2002 and 2003 Level One (Support) Waiver
- Residential Facility Waiver (RFW) (comp waiver) 2000
- Community Access Model Initial Waiver 2004
- April 4, 2006 Teleconference Big Picture Perspective
- 2006 Level One Waiver Renewal
| STATE CONTACT INFORMATION | |
|---|---|
| Name | Linda Lewis-Day |
| Agency | Ohio Department of Mental Retardation and Developmental Disabilities Division of Medicaid Development and Administration |
| Address | 1810 Sullivant Avenue Columbus, OH 43223-1239 |
| Telephone | 614-728-2736 |
| Linda.lewis-day@dmr.state.oh.us | |
OKLAHOMA
| WAIVERS | |||||
|---|---|---|---|---|---|
| Waiver Title | Type | CMS Waiver # | Participants (2006) | Start Date | Status |
| In-Home Child Support Waiver | Supports | 0351 | 522 | 07/1999 | On-going |
| In-Home Adult Support Waiver | Supports | 0343 | 1,279 | 07/1999 | On-going |
| Community Waiver + Homeward Bound | Comprehensive | 0179 399 | 3,388 | 07/1986 | On-going |
| BASIC SUPPORT WAIVER FEATURES | |
|---|---|
| Supports Waiver Target Population | Child Support Waiver: Children with developmental disabilities ages 3-17 who reside in the family home and who have critical support needs that can be met through a combination of non-waiver and Medicaid state plan resources available to the individual within the waiver funding allowance. Adult Support Waiver: Adults with developmental disabilities age 18 and older who reside in the family home or own home who have critical support needs that can be met through a combination of non-waiver and Medicaid state plan resources available to the individual within the waiver funding allowance. |
| Funding Limit | Child Support Waiver: $12,828/year. Adult Support Waiver: $19,225/year. |
| Funding Parameters | Amount authorized based on individual plan. |
| Exceptions to Funding Limit | Additional funding may be approved due to participant changes or circumstances. |
| Transition to Comprehensive Waiver | If the person’s needs cannot be adequately met through the supports waiver program, services may be offered through the Community Waiver when openings are available. |
| Self-Direction | No. Oklahoma may add self-direction to the In-Home Support Waivers during the renewal process in 2006. Individuals and families, however, exercise choice in the selection of waiver services and supports under the funding limits. |
| SUPPORTS WAIVER SERVICES | ||
|---|---|---|
| Support/Service Category | Y/N | Oklahoma Waiver Services |
| Following services offered in both In-Home Support Waivers | ||
| Case Management/Service Coordination | N | [Furnished by state Developmental Disabilities Service Division employees] |
| Supports of Participant Direction (Support Broker) | N | |
| In-Home Services | Y | Homemaker Services; Habilitation Training Specialist |
| Respite | Y | Respite Care |
| Day Supports | Y | Pre-vocational Habilitation; Community-Based Skill Development Habilitation |
| Health Related | N | |
| Supported Employment | Y | Supported Employment |
| Transportation | Y | Transportation Service |
| Person Directed Goods and Services | N | |
| Equipment/Supplies | Y | Assistive Technology, Specialized Medical Equipment |
| Vehicle Repair/Modification | N | |
| Clinical Services | Y | Therapy Services including Audiology, Physical Therapy, Occupational Therapy, Speech Therapy |
| Environmental Accessibility Adaptations | Y | Environmental Accessibility; Architectural Modifications |
| Financial Management Services | N | |
| Family and Caregiver Training | Y | Family Training |
| Other | N | |
| Following services offered only in the Adult In-Home Support Waiver | ||
| Health Related | Y | Prescribed Drugs; Dental Services; Nutritional Services; Home Health Care Services; Physician Services (Psychiatric) |
| Person-Directed Goods and Services | Y | Self-Directed Supports |
| Equipment and Services | Y | Specialized Medical Equipment; Adaptive Equipment Service |
| Clinical Services | Y | Psychology Services; Audiology Services |
Background Information: Supports Waiver
Oklahoma launched its two In-Home Support Waivers in 1999. The implementation of these waivers was based on a 1997 study of Oklahoma’s waiting list conducted by Oklahoma State University. The study surveyed the entire waiting list to identify the services people most needed. The findings showed that 82 percent of the individuals on the waiting list lived in their own or family homes and that the most needed services were help with daily living activities, respite care, and vocational services. The purpose of the waivers was to reduce the waiting list by offering limited supports to adults and children who lived with their families. The rationale for and design of both In-Home Support Waivers was influenced by Colorado’s SLS Waiver.
Oklahoma also operates two comprehensive waivers: the Community Waiver and the Homeward Bound Waiver. The latter waiver serves persons placed from state institutions into the community as a result of the Homeward Bound et al. v. The Hissom Memorial Center lawsuit. Approximately 950 individuals are served in this waiver. Both comprehensive waivers provide a full array of services, including out-of-home around-the-clock residential supports.
Both supports waivers operate under funding limits. The adult waiver limit is approximately $6,000 greater than the child waiver limit. The difference in the two limits stems from: (a) the fact that special education services are furnished to children but adults require waiver-funded day supports; and (b) children have access to more robust Medicaid state plan benefits through the Early and Periodic Screening, Diagnosis, and Treatment program. In 2004, average annual participant outlays were approximately $3,300 below the adult waiver funding cap but roughly at the cap for the child waiver.
The In-Home Supports Waiver programs operate differently from the comprehensive waivers. Individuals and families have flexibility in selecting services and supports, based on the person-centered plan. Participants may train their own providers and have the authority to sign a “Certificate of Competency” for the provider in lieu of the provider completing state mandated training, if the family chooses to exercise this option. Case management required contacts in the In-Home Support Waiver program are less intensive than the comprehensive waivers. This reduced oversight role allows a higher caseload ratios for case managers of individuals in the In-Home Support Waiver programs. State officials observe that the supports waivers have helped lower the average cost per participant for services while affording more flexibility in tailoring services to consumers and families. The supports waivers have proven beneficial in shifting their system to a supports model that assists individuals to remain in their own or family home. The Community Waiver has come to be the waiver used in emergency situations and when a person has complex and/or residential needs.
Oklahoma also operates the Family Support Assistance Payment Program, which provides a cash payment to families who are raising children with developmental disabilities under the age of 18. In June 2005, this program was furnishing assistance to 1,735 children. In addition, in 2005, Oklahoma implemented the “Katie Beckett” Medicaid eligibility option to extend Medicaid benefits to children with disabilities by waiving the deeming of parental income. As a result of this program, there are 950 children living at home with their families.
Once an individual is enrolled in the In-Home Support Waiver, additional supports can be provided on a temporary basis to deal with emergencies. While the state does not place a time limit on these additional funds, the intent of the additional funding is to maintain the person’s current situation. If, over time, the In-Home Support Waiver programs can no longer meet the needs of the individual, the person may potentially move to the Community Waiver. Decisions about movement from one waiver to another are made on an individual basis. Oklahoma reserves Community Waiver capacity to serve high-priority individuals identified as needing emergency placement.
Oklahoma also operates the Family Support Assistance Payment Program, which provides a cash payment to families who are raising children with developmental disabilities under the age of 18. In June 2005, this program was furnishing assistance to 1,735 children. In addition, in 2005, Oklahoma implemented the “Katie Beckett” Medicaid eligibility option to extend Medicaid benefits to children with disabilities by waiving the deeming of parental income. As a result of this program, there are 950 children living at home with their families.
Major Issue(s):
In November 2006, there were 4,200 people on the waiting list. In its 2005 session, the Oklahoma Legislature appropriated additional funds to move 2,148 people off the waiting list in FY 2005-2006, principally by expanding the In-Home Supports Waivers. As of December 2006, the number of people on the waiting list had been reduced to 3,074. Statistical Profile
Statistical Profile
| WAIVER PARTICIPANTS BY YEAR | |||||||
|---|---|---|---|---|---|---|---|
| Waiver | 2000* | 2001* | 2002 | 2003 | 2004 | 2005 | 2006 |
| Comprehensive* | 2,780 | 3,010 | 3,065 | 3,012 | 3,020 | 3,041 | 3,388 |
| In-Home Child Supports | 47 | 174 | 269 | 287 | 263 | 237 | 522 |
| In-Home Adult Supports | 137 | 516 | 691 | 719 | 735 | 740 | 1,279 |
| Total Participants | 2,964 | 3,700 | 4,025 | 4,018 | 4,018 | 4,018 | 5,189 |
| Supports Waiver % of Total Participants | 6.2% | 18.6% | 23.9% | 25.0% | 24.8% | 24.3% | 27.4% |
| * Includes Community and Homeward Bound Waivers. All participant counts based on Oklahoma Department of Human Services Annual Reports. | |||||||
As can be seen, waiver enrollment in Oklahoma was flat between 2002 and 2005. In 2006, enrollment grew by 2,148 persons (about 70.6 percent) as a result of additional funds appropriated to reduce the waiting list.
| OKLAHOMA WAIVER ENROLLMENT |
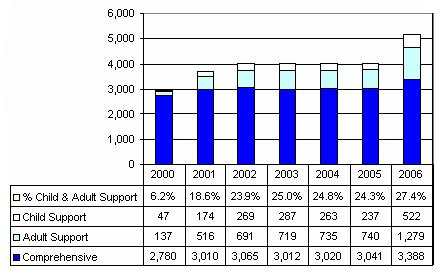 |
| EXPENDITURES BY YEAR* | |||||||
|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 |
| Comprehensive ($M)** | $157.5 | $188.5 | $214.5 | $200.3 | $205.0 | $199.4 | $215.4 |
| Per Participant | $56,645 | $62,639 | $69,968 | $66,515 | $67,866 | $65,580 | $63,577 |
| Supports ($M) | $1.3 | $6.5 | $10.6 | $11.8 | $13.1 | $12.9 | $17.4 |
| Per Participant | $7,063 | $9,437 | $11,094 | $11,747 | $13,124 | $13,167 | $9,661 |
| Total Expenditures ($M) | $158.8 | $195.0 | $225.1 | $212.2 | $218.1 | $212.2 | $232.8 |
| Supports Waiver % of Total Expenditures | 0.8% | 3.3% | 4.7% | 5.6% | 6.0% | 6.1% | 7.5% |
| Cost Per Participant: % Supports to Comprehensive | 12.5% | 15.1% | 15.9% | 17.7% | 19.3% | 20.1% | 15.2% |
| Blended Cost Per Participant | $53,568 | $52,714 | $55,926 | $52,803 | $54,269 | $44,864 | |
| * Expenditures by waiver from: Steve Eiken, Brian Burwell and Eileen Walker (May 2005). Medicaid HCBS Waiver Expenditures, FY 1999 through FY 2004. Cambridge, MA: MEDSTAT. 2005 expenditures from Department of Human Services Annual Report. ** Includes Community and Homeward Bound Waivers. | |||||||
| OKLAHOMA WAIVER EXPENDITURES ($M) |
 |
Between 2002 and 2005, total Oklahoma waiver funding was largely unchanged. Comprehensive waiver per participant costs reflect the relatively high costs associated with operating the Homeward Bound waiver. Both waivers total spending increased as a result of the waiting list reduction initiative but the In-Home Support Waiver covered most of the new people.
| OKLAHOMA EXPENDITURES PER PARTICIPANT |
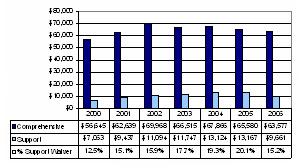 |
| WEB-ACCESSIBLE RESOURCES/ADDITIONAL INFORMATION | |
|---|---|
| Resource | Description/Web-Address |
| Oklahoma Developmental Disability Services Division | Website for the waiver operating agency http://www.okdhs.org/ddsd |
| What is the Medicaid Waiver? | Web page that describes the four Oklahoma waivers http://www.okdhs.org/ddsd/Division/Resources/what_is_a_medicaid_waiver.htm |
Document Inventory
- 2006 Community and Homeward Bound Waiver renewal applications
- HCFA 372 annual reports
- 2005 amendment In-Home Support Waiver for Children
- Two Brochures Building Bridges of Support One Person At A Time (General) and In-Home Supports Waiver 2006
- SSI Disabled Children’s Program Family Support Division Brochure
- TEFRA Helping Oklahoma Children with Disabilities 2006 Brochure
- Oklahoma Developmental Disabilities Council 5 Year Plan 2006
- Rules Chapter 40 Developmental Disabilities General Provisions 2006
- 2006 Quality Management Strategy
- Principles of Individual Planning
- Building Bridges of Support One Person At A Time Annual Report 2005
- OKDHS Hearings Brochure
- Consumer Service Evaluation Brochure
- Rules 2006 for: Part 7 Assistance Program, Quality Assurance
- Contract Performance Surveys and Administrative Inquiries
- Volunteer Guardianship Program
- Pre-Employment Screening for Community Service Workers
- Procedure for Reporting Suspected Abuse, Neglect, Verbal Abuse, Caretaker Misconduct, and Exploitation, Office of Client Advocacy Investigation Protocols
- Human Rights Committee, Community Staff Training, Staff Providing Supports Through the In-home Support Waiver, Training for Case Managers, Program Coordinator Training, Medication Administration Training, Medication, and Health Related Services
- Developmental Disabilities Services Division Heath Alert 2nd Quarter 2006
| STATE CONTACT INFORMATION | |
|---|---|
| Name | Kristi Blackburn |
| Agency | Oklahoma Department of Human Service Developmental Disability Services Division |
| Address | Sequoyah Memorial Office Building P.O. Box 25352 Oklahoma City, OK 73125 |
| Telephone | 405-521-6257 |
| Kristi.Blackburn@okdhs.org | |
OREGON
| WAIVERS | |||||
|---|---|---|---|---|---|
| Waiver Title | Type | CMS Waiver # | Participants (2005) | Start Date | Status |
| Supports Services for Adults Waiver (SSAW) | Supports | 0375 | 3,266 | 07/2001 | On-going |
| 24 Hour Comprehensive Supports | Comprehensive | 0117 | 5,597 | 12/1981 | On-going |
| BASIC SUPPORT WAIVER FEATURES | |
|---|---|
| Supports Waiver Target Population | Adults age 18 and older with developmental disabilities who do not reside in a community-based home/residential licensed or certified by the State of Oregon. The state employs the 300 percent of SSI special income eligibility standard. |
| Funding Limit | $20,000/year. |
| Funding Parameters | All participants are eligible for base funding of $9,600/year. Funding may be increased to $14,400 or $19,999 based on Basic Supplement Criteria Inventory (BSCI) score. The BSCI assesses long-term health needs, physical needs, need for behavioral supports, and caregiver circumstances. As of July 2005, participants who have personal care needs may receive a supplement of up to $2,467 (previously, waiver participants were eligible to receive 20 hours of personal care through the Medicaid state plan). |
| Exceptions to Funding Limit | Emergent services may be furnished to individuals who are in jeopardy of losing their living situation due to inability or unavailability of the primary caregiver and no alternative resources are available. Services are short-term, for up to 270 consecutive days in 12 consecutive months to prevent a permanent out-of-home placement. Services necessary to maintain the individual in the community and stabilize the situation include short-term residential placement or additional support services. The amount of the emergent services in combination with other services may exceed the $20,000 per plan year limit. |
| Transition to Comprehensive Waiver | Entrance to 24-Hour Comprehensive Supports Waiver is limited to individuals experiencing crisis. Oregon provides for modest year-over-year increases in Comprehensive Supports Waiver capacity to accommodate individuals who are not experiencing crisis. |
| Self-Direction | Full-Featured Self-Direction. Waiver participants engage personal agents through Support Services Brokerages. Personal agents employ a person-centered planning process to help participant add/or family identify support needs. Individuals/families exercise choice and control over services/supports included in the plan. Support brokerages furnish financial management services. Brokerages are Internal Revenue Service Fiscal/Employer Agents for participant-hired workers. Brokerages function as “fiscal agents” by assisting participants to manage funding, keeping track of funds used, and paying workers or agencies that provide services. |
| SUPPORTS WAIVER SERVICES | ||
|---|---|---|
| Support/Service Category | Y/N | Oregon Waiver Services |
| Case Management/Service Coordination | Y | Support Service Brokerage [County developmental disabilities program performs intake, eligibility determination and approves Individual Support Plan (ISP)] |
| Supports of Participant Direction (Support Broker) | Y | Support Service Brokerage |
| In-Home Services | Y | Community Living Supports; Homemaker; Chore Services |
| Respite | Y | Respite |
| Day Supports | Y | Community Inclusion Supports |
| Health Related | Y | Special Diets |
| Supported Employment | Y | Supported Employment |
| Transportation | Y | Non-Medical Transportation |
| Person Directed Goods and Services | N | |
| Equipment/Supplies | Y | Specialized Medical Equipment and Supplies; PERS |
| Vehicle Repair/Modification | N | |
| Clinical Services | Y | Specialized Supports; Physical Therapy; Occupational Therapy; Speech/Hearing/Language Services |
| Environmental Accessibility Adaptations | Y | Environmental Accessibility Adaptations |
| Financial Management Services | Y | Support Service Brokerage |
| Family and Caregiver Training | Y | Family Training |
| Other | Y | Emergent Services |
Background Information: Supports Waiver
Oregon’s Supports Services for Adults Waiver was a direct outgrowth of the Staley et al. v. Kitzhaber lawsuit that was filed in January 2000. The lawsuit alleged that Oregon’s failure to provide Medicaid services with reasonable promptness to eligible individuals violated federal Medicaid law and the Americans with Disabilities Act. The lawsuit stemmed from the large waiting list for services. In December 2000, the federal court approved a settlement agreement that was based on the Universal Access Plan which, in turn, had been previously proposed as a means of ensuring that all eligible adults with developmental disabilities receive at least a basic level of supports. The settlement agreement committed Oregon to design and implement the supports waiver and eliminate its waiting list for services over a multi-year period.2 The original settlement provided for eliminating the waiting list by the 2007-2009 biennium by extending services to an additional 4,600 individuals. Due to budgetary shortfalls, the agreement was modified in 2004 to stretch out the period for eliminating the waiting list to the 2009-2011 biennium.
Oregon was influenced by Colorado’s waiver design of operating separate supports and comprehensive waivers. The Supports Services Waiver design also was significantly influenced by self-determination principles. System stakeholders played a critical role in shaping the waiver. The state and stakeholders saw the new waiver as an opportunity to make improvements in service delivery and stakeholders continue to be actively involved through the Staley Implementation Group. Consumers were already seeking more flexible alternatives to the traditional services system including options to self-direct services. The Supports Services Waiver offers flexible in-home supports to consumers and families that are intended to prevent out-of-home placement and thus reduce comprehensive waiver enrollment pressures. Consumers and families enter into contracts directly with providers, affording a high degree of choice and control over the nature of the services. The new waiver also adopted a different approach to management through the development of Support Service Brokerages to assist the person in the development of a plan, including an individualized budget, and identifying service providers. The Supports Brokerage Personal Agent facilitates person-centered planning, assists participants in selecting and purchasing services, performs day to day oversight and monitoring of the services, and furnishes additional assistance to help participants access other services. Oregon counties (which provide full range case management in the Comprehensive Waiver) perform play a more limited role in the Supports Services Waiver. Counties perform eligibility reviews, approve the individual plan for Medicaid compliance, provide protective services, and assist in crisis management. These services are billed under Medicaid administration.
The waiver operates under a $20,000 per participant funding cap. Waiver participants are eligible for a base funding allotment of $9,600. Individuals with more intensive support needs may receive additional funding. The need for additional funding is determined by administering the BCSI.3 In August 2005, 34 percent of participants had plans that were funded in excess of $9,600. In addition, Oregon provides that “emergent services” in excess of the $20,000 cap may be authorized for individuals in crisis. In August 2005, 4 percent of service plans exceeded $20,000. Also in August 2005, plan authorizations averaged $767/participant/month ($9,204 per year) while average monthly expenditures per participant $613/month ($7,356 per year).
Some 95 percent of waiver participants have intellectual disabilities and frequently have multiple disabilities (e.g., behavior dysfunction and other health impairments). About 79 percent of participants live with their families; 9 percent live on their own. Two-thirds of waiver participants are between the ages of 21 and 40.
Order of selection criteria regulate the selection of individuals for entrance to the waiver. Currently, the order of selection is: (a) individuals experiencing crisis; (b) persons with aging (over 75) caregivers; (c) persons aging out of Oregon’s two model waivers for children; (d) persons transitioning from school; and, (e) persons on the general waiting list. Since inception and through October 2005, 1,553 individuals have entered the waiver from the adult waiting list. Other enrollees included persons who entered the waiver from other programs (e.g., child family support, high school transition) where funding would have stopped due to aging out or other reasons. Absent the waiver, 56 percent of enrollees would have remained on the waiting list or been wait-listed. About 44 percent of participants are persons who had been receiving services that qualified for waiver funding.
Waiver expenditures are concentrated in two waiver services: community living supports (a form of in-home supports) (39 percent) and community inclusion supports (a form of day supports) (39 percent). Respite care accounts for 8 percent of expenditures, supported employment for 7 percent and non-medical transportation for 6 percent. All other covered services account for only 1 percent of expenditures.
The Oregon Comprehensive Supports Waiver furnishes services primarily to individuals who reside in various types of community residential settings, including group homes and supported living arrangements. A small number of waiver participants are served in the family home. The Comprehensive Supports Waiver does not include self-direction features. Oregon operates only one small public institution that serves approximately 40 individuals. There are no privately-operated ICFs/MR in Oregon. Under the terms of the Staley settlement, persons who experience crisis must be offered Comprehensive Supports Waiver services. Since inception, 221 Supports Waiver participants have transitioned to the Comprehensive Supports Waiver. Oregon also operates two small model waivers for children: one supports children who have intensive behavioral challenges while the other serves children with extraordinary medical needs.
In 2004, there were 2,270 people waiting for Oregon’s Supports Services Adult Waiver. In 2006, the number waiting was somewhat lower -- about 2,000 individuals. The number of persons waiting for the Comprehensive Supports waiver was 1,500.
Major Issue(s):
System-wide, Oregon is experiencing a significant increase in the number of individuals experiencing crisis. This is causing funding stress within both waivers. Statistical Profile
Statistical Profile
| WAIVER PARTICIPANTS BY YEAR | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007* | 2008* |
| Comprehensive | 5,688 | 5,821 | 6,343 | 6,125 | 5,437 | 5,597 | 5,808 | 5,886 | 5,935 |
| Supports | 0 | 0 | 999 | 1.661 | 2.646 | 3.266 | 4.122 | 5.122 | 6.697 |
| Total Participants | 5,688 | 5,821 | 7,342 | 7,786 | 8,083 | 8,863 | 9,930 | 11,008 | 11,632 |
| Supports Waiver % of Total Participants | 0% | 0% | 13.6% | 21.3% | 32.7% | 36.8% | 41.5% | 46.5% | 53.0% |
| * Oregon Department of Human Services projections. | |||||||||
Between 2000 and 2005, total Oregon waiver enrollment increased by 55.8 percent. The next three years through 2008 adds another 66.3 percent. As can be seen expansion of the Supports Services Waiver accounts for all net enrollment growth since 2002.
| OREGON WAIVER ENROLLMENT |
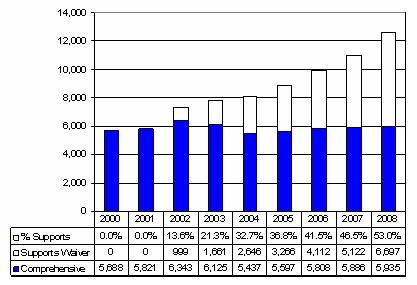 |
| EXPENDITURES BY YEAR | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 |
| Comprehensive ($M) | $227.0 | $257.2 | $282.3 | $292.2 | $293.7 | $305.1 | $319.5 | $326.6 | $332.4 |
| Per Participant | $39,907 | $44,186 | $44,497 | $47,704 | $54,015 | $54,516 | $55,000 | $55,000 | $55,000 |
| Supports ($M) | $0 | $0 | $4.4 | $15.5 | $22.5 | $27.2 | $35.1 | $44.4 | $50.4 |
| Per Participant | $0 | $0 | $4,405 | $9,313 | $8,508 | $8,338 | $8,505 | $8,675 | $7,527 |
| Total Expenditures ($M) | $227.0 | $257.2 | $286.7 | $307.7 | $316.2 | $332.3 | $354.6 | $371.0 | $382.8 |
| Supports Waiver % of Total Expenditures | 0% | 0% | 1.5% | 5.0% | 7.1% | 8.2% | 9.9% | 12.0% | 13.2% |
| Cost Per Participant: % Supports to Comprehensive | 0% | 0% | 9.9% | 19.5% | 15.8% | 15.3% | 15.5% | 15.8% | 13.7% |
| Blended Cost Per Participant | $39,907 | $44,186 | $39,049 | $39,520 | $39,119 | $37,493 | $35,746 | $33,703 | $30,304 |
| OREGON WAIVER EXPENDITURES ($M) |
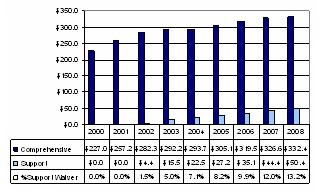 |
In Oregon, total waiver expenditures increased by 46.4 percent between 2000 and 2005. Expenditure growth slowed in 2003, due to effects of the downturn in the Oregon economy. In 2005, Support Services Waiver expenditures accounted for 8.2 percent of total expenditures even though more than one-third of all waiver participants were served in the Support Services Waiver. Supports Services Waiver per participant expenditures were 15.3 percent of Comprehensive Waiver per participant spending. The implementation of the Support Services Waiver resulted in stabilizing overall spending per waiver participant. These same trends are projected to continue with 22.2 percent additional total waiver expenditure growth by 2008. The Support Services Waiver will then account for 13.2 percent of total expenditures even though 53.0 percent of all waiver participants were served in the Support Services Waiver.
| OREGON EXPENDITURES PER PARTICIPANT |
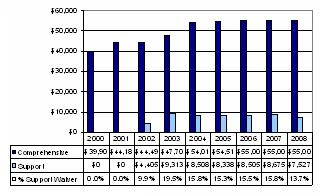 |
| WEB-ACCESSIBLE RESOURCES/ADDITIONAL INFORMATION | |
|---|---|
| Resource | Description/Web-Address |
| A Road Map to Support Services, Oregon Advocacy Center, Oregon Council on Developmental Disabilities, Oregon Department of Human Services, December 2005 | Consumer-focused publication that provides a complete description of support services http://ocdd.org/support_services.htm |
| Descriptive Information Concerning Support Services for Adults Waiver, Oregon Department of Human Services | Web page describes the waiver and contains links to additional, more detailed information http://oregon.gov/DHS/dd/adults/supports.shtml |
| Support Services Administrative Rules | Oregon Administrative Rules governing the operation of the Support Services Waiver http://www.dhs.state.or.us/policy/spd/rules/411_340.pdf |
| Supports Services for Adults Waiver Renewal Application | CMS-approved waiver application http://egov.oregon.gov/DHS/spd/qa/ssa_waiver_icfmr.pdf |
| Staley Settlement Agreement and Associated Materials | A description of the Staley settlement agreement http://oregon.gov/DHS/spd/pubs/dd/staley/staley.shtml The most recent (2005) status report concerning the implementation of the agreement. The status report provides robust information concerning enrollments in the waiver |
Document Inventory
- Oregon's Personal Outcome Statements and Indicators of Brokerage Services
- 2003 Adult Comprehensive Waiver Renewal application
- The ARC of Oregon description of the Self-Directed Support Services
- 372 Reports for Comprehensive and Support waivers from 2000 to 2005
- 2004 Report on Statewide HCBSS Waiver Quality Review
- 2004 Fragile Child model waiver, 2004 five year Support Services Waiver renewal, and 2003 Oregon's Response to HCFA Regional Office Protocol
- Staley Lawsuit Settlement Agreement Progress Report #4 -- Issued 01/25/06
- Roadmap to Support Services 2nd Edition
- Overview of A Roadmap to Support Services Training Program
- Training Materials to Accompany the Roadmap 2nd Edition
- Self-Directed Support Services, Welcome to The Integrated Services Network Support Service Brokerage
- Service Wait-Lists for Persons with Developmental Disabilities Rules 2002
- Oregon Support Waiver Statistics Enrollment and Termination
- VR-DD Supported Employment Partnership 2004
- Working Together To Reach Employment Goals for Persons with Developmental Disabilities, Guide #2
- Supported Employment Guidelines and Toolkit for Support Service Brokerage and Office of Vocational Rehabilitation Services Staff 2005
- Planning and Writing Support Goals
- Staley Settlement Agreement, Modification of Staley Settlement Agreement, Support Services Brokerage Expense and Reporting Reference July 2002
- Basic Supplement Criteria Inventory
- Support Service Expenditure Guideline
- Individual Support Plan Authorization Checklist
- Contract for the Services of a Support Services Brokerage
- Rules for the Operation of a Community Developmental Disability Program 2004
- ISN Support Services Brokerage Customer Satisfaction Report
- Summary of Support Services Customer Satisfaction Surveys
- Customer Satisfaction Survey
- Customer Survey for Support Services
- Report on Field Review Findings, July-October 2004
- September 2004 Revision #2 Updated Rate Policy and Ranges for Support Services
- 2006 Support Services Rate Ranges
- DSI Brokerage Quality Assurance Plan 2005-2006
- Creative Supports, Inc. Quality Assurance Plan FY 2005-2006
- Inclusion, Inc., QA Committee/Board adopted Plan 2003-2004
- Resource Connections of Oregon Link Letter April 2006
- Eastern Oregon Support Services Brokerage News July 2006
- Support Services Brokerage Estimated Revenue for Operations by Capacity Level
- Support Brokerage Director’s Strategic Planning Document for 2005
- Oregon’s Personal Outcome Statement and Indicators for Brokerage Services 2003
- Support Services for Adults with Developmental Disabilities Oregon Department of Human Services Chapter 411, Division 340 Administrative Rules 2005
- Brokerage Order of Enrollment Categories -- “Wait-List” Priorities
- Developmental Disabilities Service System
- Staley Implementation Group Retreat July 2005
- Summary of Brokerage Enrollments 2005
- Resource Connections of Oregon Brochure
- Handling Emergencies: A Guide to Personal Safety & Emergency Management 2006
- Rate-Setting and the Purchase of Self-Directed Support Services from State Licensed or Certified Provider Organizations 2005
| STATE CONTACT INFORMATION | |
|---|---|
| Name | Deanna J. Hartwig |
| Agency | Office of Developmental Disabilities Services Seniors and People with Disabilities Oregon Department of Human Services |
| Address | 500 Summer Street, NE, #E02 Salem, OR 97301-1073 |
| Telephone | 503-947-1180 |
| deanna.j.hartwig@state.or.us | |
PENNSYLVANIA
| WAIVERS | |||||
|---|---|---|---|---|---|
| Waiver Title | Type | CMS Waiver # | Participants (2005) | Start Date | Status |
| Person and Family Direct Support (PFDS) Waiver | Supports | 0354 | 7,445 | 07/1999 | On-going |
| Consolidated Waiver | Comprehensive | 0102 | 13,821 | 07/2000 | On-going |
| BASIC SUPPORT WAIVER FEATURES | |
|---|---|
| Supports Waiver Target Population | The Person and Family Direct Support (PFDS) Waiver program targets persons with mental retardation age three or over who do not need licensed community residential services. As such, the program is aimed at furnishing services and supports to individuals who live with their families and/or have other available supports that -- in combination with HCBS -- enable their needs to be met short of placement in community residence. Most individuals expected to participate in this program are persons who presently receive some services but need additional support or who receive no supports at all. |
| Funding Limit | $21,225/year. |
| Funding Parameters | Amount authorized is based on individual plan. |
| Exceptions to Funding Limit | Yes. [State funds are used to supplement as necessary. Waiver does not provide for exception to limit.] |
| Transition to Comprehensive Waiver | Individuals are transferred to Consolidated Waiver as slots are available. |
| Self-Direction | Employer Authority. Personal care workers can be chosen by participants and their families. Waiver participants and their families may exercise employer authority through the use of two different models of Intermediary Service Organizations (ISOs) -- Agency with Choice and Vendor/Fiscal. Availability of an ISO varies by county. In January 2007, the state will contract with one or more vendor/fiscal administrative ISOs to ensure statewide availability. |
| SUPPORTS WAIVER SERVICES | ||
|---|---|---|
| Support/Service Category | Y/N | Pennsylvania Waiver Services |
| Case Management/Service Coordination | N | [Case management is furnished through targeted case management coverage] |
| Supports of Participant Direction (Support Broker) | N | |
| In-Home Services | Y | Residential Habilitation; Homemaker/Chore; Personal Support |
| Respite | Y | Respite |
| Day Supports | Y | Day Habilitation |
| Health Related | Y | Visiting Nurse |
| Supported Employment | N | |
| Transportation | Y | Transportation |
| Person Directed Goods and Services | N | |
| Equipment/Supplies | Y | Adaptive Appliances/Equipment |
| Vehicle Repair/Modification | N | |
| Clinical Services | Y | Physical Therapy; Occupational Therapy; Speech/ Language Therapy; Behavioral Therapy; Visual/Mobility Therapy |
| Environmental Accessibility Adaptations | Y | Environmental Accessibility Adaptations |
| Financial Management Services | N | [Employer authority supported via state-contracted ISOs] |
| Family and Caregiver Training | N | |
| Other | N | |
Background Information: Supports Waiver
The PFDS Waiver was developed as part of Pennsylvania’s multi-year strategic plan to rebalance the state’s mental retardation service delivery system. Rebalancing included downsizing/closure of state facilities and expansion of HCBS. A key goal was to reduce the waiting list and position the system to meet future demand. Stakeholders in collaboration with the Office of Mental Retardation (OMR) and Department of Public Welfare (DPW) leadership developed a five-year plan to reduce the waiting list that was endorsed by then Governor Ridge and the Pennsylvania legislature. The design and implementation of the PFDS Waiver was an important waiting list reduction initiative element. The waiver’s design also was intended to introduce self-determination principles into the delivery services and supports.
The PFDS Waiver was approved by CMS in 1999. By 2005, this waiver was supporting 7,361 participants at an average yearly expenditure of $14,592 per participant. When initially implemented, the program was designed to support about 3,300 individuals. In addition to this waiver, the Pennsylvania operates two other HCBS waiver programs for people with mental retardation.4 The “Consolidated Waiver” served 15,149 in 2005 at an average annual cost of $67,574 per participant. Most Consolidated Waiver participants reside in licensed community residential living arrangement. Pennsylvania also operates a “zero-to-three” HCBS waiver program for infants, toddlers, and their families.
The PFDS Waiver was designed to offer a limited array of services and supports to complement family caregiving and reduce demand for community residential services. DPW/OMR leadership recognized that it would be impossible to achieve significant waiting list reduction and address future service demand by relying solely on the expansion of the much more costly Consolidated Waiver where per participant costs were in excess of $50,000.
The PFDS Waiver embraced person-centered planning methods to assure that “each person is able to live where and with whom they want, with the home and community-based support they need.” The introduction of person-centered planning through the PFDS Waiver paved the way for its extension to the Consolidated Waiver. The PFDS Waiver contains several features intended to strengthen the role of the individual or family in selecting and managing services.
PFDS is defined as an “array of habilitation and related services and supports that is directed by persons receiving this assistance, in conjunction with their family and others that is directed by persons receiving this assistance, in conjunction with their family and others whom the person chooses.” The waiver support plan takes into account both HCBS and other generic or informal supports available to the person and details the health and safety responsibilities of family, friends, and providers.
Pennsylvania reports several positive impacts from the waiver. Many families who were seeking for out-of-home placement have found that their needs of their relative could be met in the family home through the PFDS Waiver. Furthermore, families have expressed appreciation for the greater flexibility and control they have in selecting and procuring services. Some families, especially in rural areas where the cost of transportation is higher, have encountered difficulty in balancing the many needs of the individual and the family. Overall, Pennsylvania reports that the PFDS Waiver is popular with families; the state would like to raise the participant cap but lacks the funds to do so.
Current Issues/Changes Underway
Pennsylvania continues to face persistent waiting lists for community services. Pennsylvania classifies people waiting for services as: (a) emergency “needing services now;” (b) critical (needing services within the year); and, (c) planning (needing services somewhere between one and five years out). In November 2006, there were a total of 3,274 people termed emergency, 9,999 termed critical, and 11,634 termed planning for a total of 24,927 people waiting. The waiting list is not broken down by type of waiver. The state is budgeting for 7,930 people on the support waiver and 15,340 on the comprehensive waiver by FY 2007.
Pennsylvania presently is implementing major changes in the operation of its waivers. CMS has required that the state standardize Consolidated Waiver operations across counties. Some of these changes include a new operating agreement with counties (local administrative agents), development and implementation of a standardized rate-setting methodology, implementation of a process to address changes in need, use of a standardized needs assessment (Supports Intensity Scale “Plus”) implementation of a new provider dispute resolution process, development of a statewide administrative vendor/fiscal ISO, and development of a new statewide provider qualifications process. Many of these same issues also will need to be addressed in the PFDS Waiver. ISO costs are being shifted from the waiver to administration. This will free up dollars in waiver participant budgets.
Statistical Profile
| WAIVER PARTICIPANTS BY YEAR | |||||||
|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 |
| Comprehensive | 11,588 | 12,946 | 13,417 | 13,703 | 13,922 | 13,821 | 15,149 |
| Supports | 2,400 | 5,009 | 6,247 | 7,036 | 7,337 | 7,445 | 7,478 |
| Total Participants | 13,988 | 17,955 | 19,664 | 20,739 | 21,329 | 21,266 | 22,627 |
| Supports Waiver % of Total Participants | 17.2% | 27.9% | 31.8% | 33.9% | 34.4% | 35.0% | 33.0% |
Between 2000 and 2006, total enrollment in Pennsylvania’s waivers for persons with mental retardation increased by 61.7 percent between 2000 and 2006. Expansion of the PFDS Waiver accounted for 58.8 percent of the overall increase in waiver enrollment. In 2006, about one-third of all waiver participants were enrolled in the PFDS Waiver.
| PENNSYLVANIA WAIVER ENROLLMENT |
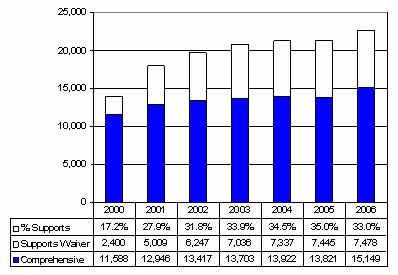 |
| EXPENDITURES BY YEAR | |||||||
|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 |
| Comprehensive ($M) | $614.0 | $705.8 | $809.7 | $874.1 | $875.4 | $964.0 | $1,023.7 |
| Per Participant | $52,882 | $54,517 | $60,347 | $63,789 | $62,565 | $69,751 | $67,574 |
| Supports ($M) | $9.2 | $35.6 | $57.0 | $72.5 | $80.0 | $76.8 | $95.2 |
| Per Participant | $3,832 | $7,105 | $9,127 | $10,299 | $10,904 | $10,321 | $12,738 |
| Total Expenditures ($M) | $623.2 | $741.4 | $866.7 | $946.6 | $955.4 | $1,040.8 | $1,118.9 |
| Supports Waiver % of Total Expenditures | 1.5% | 4.8% | 6.6% | 7.7% | 8.4% | 7.4% | 8.5% |
| Cost Per Participant: % Supports to Comprehensive | 7.2% | 13.0% | 15.1% | 16.1% | 17.4% | 14.8% | 18.9% |
| Blended Cost Per Participant | $4,.552 | $41,292 | $44,075 | $45,643 | $44,941 | $48,942 | $49,450 |
| PENNSYLVANIA WAIVER EXPENDITURES ($M) |
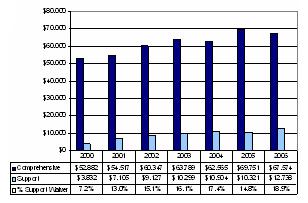 |
Between 2000 and 2006, total Pennsylvania HCBS waiver expenditures grew by approximately 80 percent. In 2006, PFDS Waiver expenditures are 8.5 percent of total expenditures even though PFDS participants account for one-third of all participants. In 2006, PFDS participant costs were 18.9 percent of the costs of supporting a person in the Consolidated Waiver and significantly below the PFDS funding limit of $21,225. When the two waivers are blended, the average cost participant in Pennsylvania increased across the period but remain below the Consolidated Waiver cost per participant in 2000.
| PENNSYLVANIA EXPENDITURES PER PARTICIPANT |
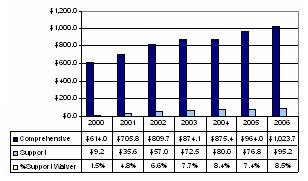 |
| WEB-ACCESSIBLE RESOURCES/ADDITIONAL INFORMATION | |
|---|---|
| Resource | Description/Web-Address |
| Person/Family Directed Support Waiver | Web page describes the PFDS Waiver http://www.dpw.state.pa.us/Disable/HomeCommServices/003671641.htm |
| Consolidated Waiver for Individuals with Mental Retardation | Web page describes the Consolidated waiver http://www.dpw.state.pa.us/Disable/HomeCommServices/003671640.htm |
| Community Living Advisory Committee | Web page describes the Community Living Advisory Committee http://www.dpw.state.pa.us/Disable/HomeCommServices/Clac |
| HCBS Stakeholder Planning Team | Web page describes the HCBS Stakeholder Planning Team and has other links of interest http://www.dpw.state.pa.us/Disable/HomeCommServices/HCBSTeam |
| Mental Retardation Services | Web page describes services for individuals with mental retardation http://www.dpw.state.pa.us/Disable/MentalRetardationServices |
Document Inventory
- 2001 Approved Consolidated Waiver
- Provider Qualifications Pilot Program, Provider Agreement 2005 following CMS Guidance
- Fact Sheet Provider Qualifications Pilot Program
- 2002 Renewal of Person/Family Directed Support Waiver
- 372 reports
- Interim Rate-Setting Procedures for Counties 2006
- Waiting List and Employment Data 2003 to 2006
- Administrative Agreement Operating Agreement, Clarifying Procedures for Individual and Provider Appeals
- Individual Support Planning
- Pennsylvania’s Guide to Medicaid-Funded Home and Community Based Services: Support Services to Help Persons with Disabilities
- Office of Mental Retardation’s Monitoring of Counties
- Understanding the Mental Retardation System in Pennsylvania: Waivers, Service Preference in Medicaid Waivers for Individuals with Mental Retardation
- What are Waivers and How Do They Help Me FAQ No. 2, 2002
| STATE CONTACT INFORMATION | |
|---|---|
| Name | Kelly Svalbonas Statewide Waiver Coordinator |
| Agency | Pennsylvania Department of Public Welfare Office of Mental Retardation Services |
| Address | Health & Welfare Building, Room 512 P.O. Box 2675 Harrisburg, PA 17105-2675 |
| Telephone | 717-783-1003 |
| ksvalbonas@state.pa.us | |
SOUTH DAKOTA
| WAIVERS | |||||
|---|---|---|---|---|---|
| Waiver Title | Type | CMS Waiver # | Participants (2005) | Start Date | Status |
| Family Support Waiver (FSW) | Supports | 0403 | 409 | 03/2000 | On-going |
| Home and Community-Based Services Program | Comprehensive | 0044 | 2,009 | 05/1982 | On-going |
| BASIC SUPPORT WAIVER FEATURES | |
|---|---|
| Supports Waiver Target Population | Children and youth with developmental disabilities under age 22 who live full-time in the family home. Parental income and resources are not deemed. |
| Funding Limit | No fixed limit; general target is $5,000 annual cost or less each year. |
| Funding Parameters | Based on individual plan. |
| Exceptions to Funding Limit | The state may make exceptions in individual situations because of circumstances or changes. |
| Transition to Comprehensive Waiver | Individuals may select the comprehensive waiver with state approval. |
| Self-Direction | No. However, the waiver operates under family support principles and stresses family direction of services. |
| SUPPORTS WAIVER SERVICES | ||
|---|---|---|
| Support/Service Category | Y/N | South Dakota Waiver Services |
| Case Management/Service Coordination | N | [Case management is furnished by providers] |
| Supports of Participant Direction (Support Broker) | N | |
| In-Home Services | Y | Personal Care, Companion Care |
| Respite | Y | Respite Care |
| Day Supports | N | |
| Health Related | Y | Nutritional Supplements |
| Supported Employment | N | |
| Transportation | N | |
| Person Directed Goods and Services | N | |
| Equipment/Supplies | Y | Adaptive Equipment; Diapers |
| Vehicle Repair/Modification | Y | Environmental Accessibility Adaptations |
| Clinical Services | N | |
| Environmental Accessibility Adaptations | Y | Environmental Accessibility Adaptations |
| Financial Management Services | N | |
| Family and Caregiver Training | N | |
| Other | N | |
Background Information: Supports Waiver
The Family Support Waiver (FSW) was launched in 2000 in order to expand the availability family support for children with developmental disabilities in South Dakota. The FSW operates side-by-side with South Dakota’s longer-standing comprehensive waiver for individuals with developmental disabilities age six and above that has a principal (but not exclusive) focus on supporting adults with developmental disabilities and the provision of services outside the family home. The FSW was designed around supporting families who have children with developmental disabilities. The FSW operates within the general framework of the state’s broader family support program.
Family support coordinators assist families to identify and access a broad range of natural and formalized services to meet their family’s identified needs. One of the "hats" frequently worn by the family support coordinator is that of advocate on behalf of the family. The role of advocacy is best accomplished by someone independent of any agency or entity that might also be providing services for a family. Otherwise a family support coordinator might be placed in the precarious position of advocating for the desires of a family that are in direct conflict with the desires of one’s employer.
Another very essential tenet of a family support program is a pool of flexible funds that can be utilized to purchase services or supports not otherwise available and to assist families with extraordinary expenses. For example, rather than establishing a formal program to provide for home modifications, the flexible funds can be utilized to purchase the needed modifications from private contractors. Another example would be assistance with extraordinary expenses such as the purchase of diapers or nutritional supplements.
Major Issue(s)/Current Situation:
South Dakota is noteworthy as a state that has avoided wait-listing individuals for services. South Dakota furnished Medicaid HCBS to individuals with developmental disabilities at a rate relative to population that is more twice the nationwide average. >Statistical Profile
Statistical Profile
| WAIVER PARTICIPANTS BY YEAR | |||||||
|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006* |
| Comprehensive | 1,697 | 1,851 | 1,949 | 1,969 | 2,009 | 2,058 | 2,255 |
| Supports | 294 | 317 | 346 | 390 | 404 | 409 | 667 |
| Total Participants | 1,991 | 2,168 | 2,295 | 2,359 | 2,413 | 2,467 | 2,922 |
| Supports Waiver % of Total Participants | 14.8% | 14.6% | 15.1% | 16.5% | 16.7% | 16.6% | 22.8% |
| * Approved Cap. | |||||||
Between 2000 and 2005, total waiver enrollment increased by 23.9 percent. Since 2002, overall enrollment growth has been modest.
| SOUTH DAKOTA WAIVER ENROLLMENT |
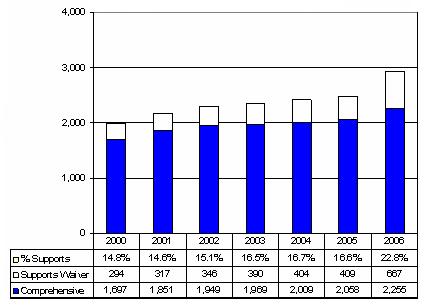 |
| EXPENDITURES BY YEAR | |||||||
|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 |
| Comprehensive ($M) | $49.5 | $53.3 | $58.4 | $61.9 | $65.9 | $72.2 | $75.7 |
| Per Participant | $29,161 | $28,785 | $29,986 | $31,445 | $32,818 | $35,077 | $33,581 |
| Supports ($M) | $0.5 | $0.6 | $0.5 | $0.8 | $0.9 | $0.9 | $2.7 |
| Per Participant | $1,615 | $1,840 | $1,422 | $2,126 | $2,298 | $2,193 | $4,015 |
| Total Expenditures ($M) | $50.0 | $53.9 | $58.9 | $62.8 | $66.9 | $73.1 | $78.4 |
| Supports Waiver % of Total Expenditures | 1.0% | 1.1% | 0.8% | 1.3% | 1.3% | 1.2% | 3.4% |
| Cost Per Participant: % Supports to Comprehensive | 5.5% | 6.4% | 4.7% | 6.8% | 7.0% | 6.3% | 12.0% |
| Blended Cost Per Participant | $25,113 | $24,862 | $25,664 | $26,579 | $27,683 | $29,631 | $26,831 |
| SOUTH DAKOTA WAIVER EXPENDITURES ($M) |
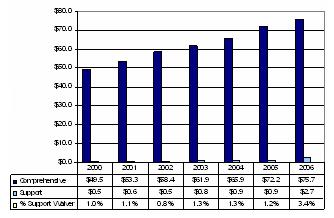 |
From 2000 to 2005, waiver expenditures increased by 46.2 percent. Both comprehensive and support waiver expenditures per participant have been relatively stable. In 2005, Medicaid state plan expenditures for FSW participants were $5,681/participant or more than twice HCBS waiver expenditures.
| SOUTH DAKOTA EXPENDITURES PER PARTICIPANT |
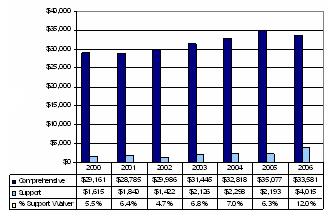 |
| WEB-ACCESSIBLE RESOURCES/ADDITIONAL INFORMATION | |
|---|---|
| Resource | Description/Web-Address |
| South Dakota’s Family Support | Web page describing South Dakota family support principles and system http://www.state.sd.us/dhs/dd/family/index.htm |
| Family Support Waiver (FSW) | Web page provides an overview of the FSW http://www.state.sd.us/social/MedElig/Families/FamSupport.htm |
| Comprehensive Waiver | Web page provides an overview of the Comprehensive waiver http://www.state.sd.us/social/MedElig/LTC/Disabled.htm |
Document Inventory
- HCFA 372 reports for both waivers: 2000-2005
- 2003 comprehensive waiver renewal
- 2005 amendment to FS Waiver
| STATE CONTACT INFORMATION | |
|---|---|
| Name | Carol Ruen |
| Agency | Department of Human Service Division of Developmental Disabilities |
| Address | Hillsview Plaza, East Highway 34 c/o 500 East Capitol Pierre, SD 57501-5070 |
| Telephone | 605-773-3438 |
| carol.ruen@state.sd.us | |
TENNESSEE
| WAIVERS | |||||
|---|---|---|---|---|---|
| Waiver Title | Type | CMS Waiver # | Participants (2005) | Start Date | Status |
| Self-Determination Waiver Program (SWDP) | Supports | 0427 | 63 | 01/2005 | Initial |
| Statewide Mental Retardation Waiver Program | Comprehensive | 0128 | 4,806 | 01/2005* | Initial |
| * Replaced previous waiver that first went into effect in 1987. | |||||
| BASIC SUPPORT WAIVER FEATURES | |
|---|---|
| Supports Waiver Target Population | The target population for the Self-Determination Waiver Program (SDWP) consists of children and adults with mental retardation who meet ICF/MR level of care criteria and who are on the Division of Mental Retardation Services (DMRS) waiting list for community services. Enrollment in the program is prioritized and offered first to persons in the crisis wait-list category, then to individuals in the urgent category, and then to persons in the active category up to the number of persons authorized to be served in the program each year. The SDWP serves persons who have an established non-institutional place of residence where they live with their families, a non-related caregiver or in their own home and whose needs can be met effectively by the combination of services available through this waiver program and the natural and other supports available to them. The SDWP does not include licensed residential services or supported living services. |
| Funding Limit | Funding limits apply to categories of specified services. The total budget for all waiver services, including emergency assistance services, may not exceed $36,000 per year per participant. The amount of the participant’s initial individual budget may be increased to address newly identified needs or changes in the participant’s life circumstances, provided that the combination of service components does not exceed $30,000. Supports for Community Living Category. Funding is limited to $23,000 per year per participant unless an exception to the service limit is approved. This category of services includes Behavioral Respite Services, Respite, Personal Assistance, Day Services, Individual Transportation Services, Supports Brokerage, Financial Administration, Participant Designated Goods and Services. Professional and Technical Supports Service Category. A participant’s use of any service or combination of services in the Professional and Technical Supports Service Category is limited to $7,000 per year per participant unless an exception to the service limit has been approved. This category includes Occupational Therapy, Physical Therapy, Speech, Language, and Hearing, Nursing, Specialized Medical Equipment and Supplies and Assistive Technology, Behavioral Services, Vehicle Accessibility Modifications, Environmental Accessibility Modifications, PERS, Orientation and Mobility Training, Nutrition Services, and Adult Dental Services. Exceptions to the limits on each group of services may be approved so long as the total amount of services initially authorized does not exceed $30,000. |
| Funding Parameters | See above. |
| Exceptions to Funding Limit | The waiver provides for temporary emergency assistance of up to $6,000 as an override to the overall $30,000 dollar limit. Emergency assistance is a temporary increase in the level of any waiver service for the purpose of preventing permanent out-of-home placement and provide an extra measure of protection when the person experiences a crisis or emergency situation that threatens his/her health and well-being. |
| Transition to Comprehensive Waiver | Individuals may transition to the HCBS Waiver for Persons with Mental Retardation based on need and slot availability. |
| Self-Direction | Yes. Individuals/families may elect to self-direct specified waiver services (personal assistance, respite, day services and certain others). For persons who self-direct, supports brokerage and financial administration (financial management) services are available. |
| SUPPORTS WAIVER SERVICES | ||
|---|---|---|
| Support/Service Category | Y/N | Tennessee Waiver Services |
| Case Management/Service Coordination | N | [Case management furnished by state employees] |
| Supports of Participant Direction (Support Broker) | Y | Support Brokerage |
| In-Home Services | Y | Personal Assistance |
| Respite | Y | Respite, Behavioral Respite Care |
| Day Supports | Y | Day Services |
| Health Related | Y | Nutrition Services; Nursing Services; Adult Dental Services |
| Supported Employment | Y | Supported Employment |
| Transportation | Y | Individual Transportation Services |
| Person Directed Goods and Services | Y | |
| Equipment/Supplies | Y | Specialized Medical Equipment, Supplies and Assistive Technology; PERS |
| Vehicle Repair/Modification | Y | Environmental Accessibility Adaptations |
| Clinical Services | Y | Behavior Services; Physical Therapy; Occupational Therapy; Speech, Language and Hearing Services; Orientation and Mobility |
| Environmental Accessibility Adaptations | Y | Environmental Accessibility Adaptations; Environmental Access |
| Financial Management Services | Y | Financial Administration |
| Family and Caregiver Training | N | |
| Other | N | |
Background Information: Supports Waiver
The development and implementation of the Tennessee Self-Determination Waiver Program (SDWP) was a direct outgrowth of the 2004 Brown vs. Tennessee Department of Finance and Administration waiting list lawsuit settlement agreement. The settlement provided that Tennessee would create a new waiver that specifically targeted children and adults with developmental disabilities who were wait-listed for services and could be supported in the family home or other non-licensed living arrangements. The settlement recognized that Tennessee could not reduce its waiting list if it relied solely on the expansion of its existing HCBS waiver, which had relatively high per participant costs. The settlement also required the state to design SDWP to incorporate “self-determination” principles. The settlement provided for phasing in the SDWP and furnishing “interim services” to persons on the waiting list until they are enrolled in SDWP or the existing waiver. As approved by CMS, SDWP waiver enrollment is expected to reach 1,500 persons in its third year.
The implementation of the SDWP waiver was affected by the state’s need to resolve a variety of long-standing CMS-identified problems in the operation of its comprehensive HCBS waiver (Statewide Mental Retardation Waiver Program). CMS limited new waiver enrollment to individuals in crisis until those problems were resolved. Finally, in January 2005, CMS approved a replacement waiver for the comprehensive waiver and the SDWP. In March 2005, CMS approved a resumption of waiver enrollments. As consequence, enrollment in SDWP did not begin until June 2005.
SDWP serves Tennessee citizens with mental retardation who have moderate service needs that can be satisfactorily met with a cost effective array of home and community services that complement other supports available to them in their home and the community, including personal assistance and day supports. SDWP affords participants the opportunity -- based on individual preference and the willingness to assume the responsibilities that accompany self-determination -- to lead the person-centered planning process and directly manage services, including the recruitment and management of service providers. Participants and families (as appropriate) who elect self-determination are empowered and have the responsibility for managing a self-determination budget that affords flexibility in service design and delivery. During the development of the ISP, individuals and families receive an orientation to self-determination, including information concerning the added responsibilities and benefits of self-determination. When self-determination is selected, the ISP details the services that are participant-managed and the participant’s responsibilities. Participants and families who prefer may elect to receive some or all of their services through the standard service delivery method through which an enrolled service provider chosen by the individual hires and manages the staff, delivers the services in accordance with the ISP and is paid directly by the state.
SDWP funding is limited to $30,000. The waiver provides for funding limits on two groups of services. However, the group limits may be exceeded so long as the overall funding limit is not exceeded. The grouping of services was patterned after similar groupings in the Texas Home Living supports waiver. In addition, Tennessee provides that the $30,000 limit may be exceeded up to $6,000 in the event of crisis or emergency. Emergency funding may be used to purchase additional services covered in the waiver.
Major Issue(s):
Tennessee continues to face high demand for waiver services due to large part to the states historically low level of effort in funding services. Between June 2005 and January 2006, about 200 additional persons per month sought services. Despite enrolling approximately 1,500 individuals to its HCBS waivers, the state saw its waiting list grow from 3,762 persons to 4,761 persons in November 2006, although the total number of individuals on the waiting list appears to have stabilized. However, absent the SDWP, the state would be facing an even larger waiting list. Statistical Profile
Statistical Profile
| WAIVER PARTICIPANTS BY YEAR | |||||||
|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 |
| Comprehensive | 4,311 | 4,537 | 4,311 | 4,263 | 4,390 | 4,806 | 6,123 |
| Supports | 0 | 0 | 0 | 0 | 0 | 63 | 834 |
| Total Participants | 4,311 | 4,537 | 4,311 | 4,263 | 4,390 | 4,869 | 6,957 |
| Supports Waiver % of Total Participants | 0% | 0% | 0% | 0% | 0% | 1.3% | 12.0% |
During the period 2000-2004, Tennessee waiver enrollment was affected by a CMS moratorium on new enrollments. Enrollment resumed in March 2005. Enrollment in SDWP started in June 2005.
| TENNESSEE WAIVER ENROLLMENT |
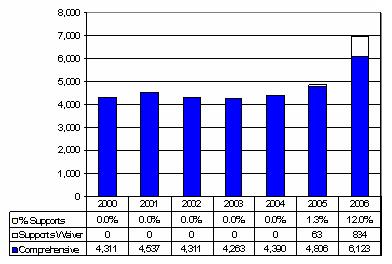 |
| EXPENDITURES BY YEAR | |||||||
|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 |
| Comprehensive ($M) | $159.9 | $201.3 | $182.7 | $187.1 | $245.1 | $279.0 | $369.7 |
| Per Participant | $37,100 | $44,357 | $42,373 | $43,885 | $55,829 | $58,062 | $60,385 |
| Supports ($M) | $0 | $0 | $0 | $0 | $0 | $0.2 | $15.1 |
| Per Participant | $0 | $0 | $0 | $0 | $0 | $2,563 | $18,051 |
| Total Expenditures ($M) | $159.9 | $201.3 | $182.7 | $187.1 | $245.1 | $279.2 | $384.8 |
| Supports Waiver % of Total Expenditures | 0% | 0% | 0% | 0% | 0% | 1.3% | 3.9% |
| Cost Per Participant: % Supports to Comprehensive | 0% | 0% | 0% | 0% | 0% | 4.4% | 29.9% |
| Blended Cost Per Participant | $37,100 | $44,357 | $42,373 | $43,885 | $55,829 | $57,342 | $55,311 |
| TENNESSEE WAIVER EXPENDITURES ($M) |
 |
The resumption of enrollments in the comprehensive waiver and the initiation of SDWP enrollment will result in a significant increase in waiver expenditures during 2006. Support waiver costs per participant in 2006 reflect phased-in enrolled. At full build out, per participant costs are estimated at $31,000/year.
| TENNESSEE EXPENDITURES PER PARTICIPANT |
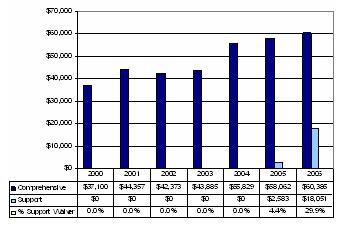 |
| WEB-ACCESSIBLE RESOURCES/ADDITIONAL INFORMATION | |
|---|---|
| Resource | Description/Web-Address |
| Family Handbook: A Road Map to State Services for Adults and Children Who have Mental Retardation | Handbook provides an overview of services, including the SDWP http://state.tn.us/dmrs/consumer_services/FamilyHandbook.pdf |
| Annual Report: DMRS | Report describes changes in services during FY 2005, including implementation of SDWP and changes in waiting list http://state.tn.us/dmrs/newsroom/AnnualReportfinal103105.pdf |
| Brown v. Tennessee Settlement Agreement | Full text of settlement agreement which directed Tennessee to establish SDWP http://state.tn.us/dmrs/compliance/brown_settle_agree.pdf |
| Self-Determination Waiver Program Application and Related Materials | Website contains application and related materials http://state.tn.us/tenncare/ltcare/ltcdd_waiver1.htm |
Document Inventory
- Comprehensive Waiver 372 reports for 2002, 2003 and 2004
- Self-Determination Waiver Program application
- Three Year Plan 2007-2009, Tennessee Department of Mental Health and Developmental Disabilities
| STATE CONTACT INFORMATION | |
|---|---|
| Name | Paula McHenry and Denine Hunt |
| Agency | Division of Mental Retardation Services Department of Finance and Administration |
| Address | Andrew Jackson Building, 15th Floor 500 Deadrick Street Nashville, TN 37243 |
| Telephone | 615-532-6540 |
| Paula.McHenry@state.tn.us | |
TEXAS
| WAIVERS | |||||
|---|---|---|---|---|---|
| Waiver Title | Type | CMS Waiver # | Participants (2006) | Start Date | Status |
| Texas Home Living (TxHL) Waiver | Supports | 403 | 1,933 | 03/2004 | Initial |
| Home and Community-Based Services (HCS) Program | Comprehensive | 110 | 10,104 | 09/1985 | On-going |
| BASIC SUPPORT WAIVER FEATURES | |
|---|---|
| Supports Waiver Target Population | Children and adults with mental retardation who meet Level 1 ICF/MR level of care criteria, live on their own or with their families, and do not require intensive supervision. The Texas Home Living (TxHL) Waiver does not use the 300 percent of SSI standard. It is limited to people who qualify under “community” Medicaid rules, which means that from a financial eligibility standpoint, it is more restrictive than the HCBS waiver. |
| Funding Limit | $10,000 per year. |
| Funding Parameters | Service costs are controlled by the overall $10,000 funding limit. Under this limit, costs are further subject to limits on two groups of waiver services: a $2,000 cap on Professional and Technical Support Services (e.g., therapies) and an $8,000 limit on the Community Living Services (e.g., day services). So long as the overall $10,000 limit is not exceeded, services may be authorized above the group service limits. |
| Exceptions to Funding Limit | None. |
| Transition to Comprehensive Waiver | Participants may transition to comprehensive waiver based on need, availability of waiver slots and position on the waiting list. |
| Self-Direction | Not at present. State plans to amend the waiver to add self-direction, including the employer and budget authorities. |
| SUPPORTS WAIVER SERVICES | ||
|---|---|---|
| Support/Service Category | Y/N | Texas Waiver Services |
| Case Management/Service Coordination | N | [Service coordination is furnished under targeted case management coverage] |
| Supports of Participant Direction (Support Broker) | N | |
| In-Home Services | Y | Community Support |
| Respite | Y | Respite |
| Day Supports | Y | Day Habilitation; Employment Assistance |
| Health Related | Y | Dental; Nursing; Dietary |
| Supported Employment | Y | Supported Employment |
| Transportation | N | |
| Person Directed Goods and Services | N | |
| Equipment/Supplies | Y | Adaptive Aids |
| Vehicle Repair/Modification | N | |
| Clinical Services | Y | Behavioral Support; Physical Therapy; Occupational Therapy; Speech and Language Pathology; Audiology |
| Environmental Accessibility Adaptations | N | Minor Home Modifications |
| Financial Management Services | N | |
| Family and Caregiver Training | N | |
| Other | N | |
Background Information: Texas Home Living Waiver
The Texas Home Living (TxHL) Waiver was implemented in 2004 in order to provide a limited array of services and supports to individuals who are on the general waiting list for waiver services. The program was designed to be self-financing. That is, the enrollment of individuals already receiving waiver-like services would permit releasing state funds that would serve as match to expand waiver services to roughly the same number of individuals on the waiting list. The TxHL Waiver operates side-by-side with the longer standing Home and Community-Based Services (HCS) Waiver for persons with mental retardation. HCS offers a full range of community services, including residential services.
The TxHL Waiver targets persons with mental retardation who meet Level 1 ICF/MR level of care criteria. Such individuals have less intensive needs than other persons who require a higher level of ICF/MR care criteria. The waiver offers day and other supports that complement natural and other community supports. Access to the waiver is through the state’s network of Mental Retardation Local Authorities (MRLAs). MRLAs conduct intake and furnish service coordination, including assisting individuals and families in developing service plans. MRLAs also manage provider enrollment, including the enrollment of consumer-identified providers, and conduct waiver quality management functions. Individuals who accept TxHL Waiver services retain their position on the HCS waiting list. That is, individuals receive TxHL Waiver services may transfer to the HCS Waiver when their names rise to the top of the HCS list and slots are available.
The waiver has funding limits on two “clusters” of waiver services. The application of funding limits to clusters of waiver services reflected the CMS policy that was in effect when the waiver was submitted that a state could not impose an overall limit on the total amount of waiver services but could apply dollar limits to groups of services. This CMS policy has since been replaced with explicit authority for states to apply an overall limit on the total amount of waiver services.
Individuals with other developmental disabilities (related conditions) are served through a separate waiver (Community Living Assistance and Support Services (CLASS) waiver). There is no equivalent supports waiver for persons with related conditions. Texas has an especially large ICF/MR service sector. In 2004, 12,300 individuals received ICF/MR services, including nearly 5,000 persons in state institutions. About 4,800 individuals receive ICF/MR services in smaller six-bed group home facilities. Texas accounted for 11.8 percent of nationwide ICF/MR utilization in 2004.
Major Issue(s):
Texas has a very large waiting list for community services. In February 2006, there were nearly 29,000 individuals waiting for waiver services or almost three times the number of people with mental retardation who were receiving waiver services. In Texas, people who seek waiver services are placed on an “interest list.” Movement off the interest list is on a “first come, first served” basis. When a person’s name rises to the top of the interest list, an eligibility determination is made. Approximately 90 percent of the individuals who are on the interest list are found to be eligible when offered waiver services. The number of people on the interest list has been growing year-over-year.
For the 2006-2007 biennium, the Texas legislature earmarked additional funds to reduce waiting lists across all waiver programs. With respect to waivers for persons with mental retardation, funding was earmarked to offer services to approximately 2,900 more individuals on the HCS waiting list by June 2007. In September 2002, a lawsuit (McCarthy v. Hawkins) was filed in federal district court challenging the wait-listing of individuals for home and community services. This litigation has not yet been resolved. The plaintiffs demanded that Texas commit to a multi-year plan to eliminate the waiting list for both HCS and CLASS waiver services. The lawsuit has been settled. The state agreed to make budget requests sufficient to prevent the waiting list from growing larger. Statistical Profile
Statistical Profile
| WAIVER PARTICIPANTS BY YEAR | |||||||
|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006** |
| Comprehensive* | 5,420 | 6,133 | 6,951 | 7,268 | 8,932 | 9,040 | 10,104 |
| Supports | 0 | 0 | 0 | 0 | 0 | 1,482 | 1,933 |
| Total Participants | 5,420 | 6,133 | 6,951 | 7,268 | 8,932 | 10,552 | 12,037 |
| Supports Waiver % of Total Participants | 0% | 0% | 0% | 0% | 0% | 14.1% | 16.1% |
| * Includes MRLA and HCS and HCS-Omnibus Budget Reconciliation Act (OBRA) Waiver participants through 2003. OBRA Waivers are a very specialized subset of very small 1015(c) waivers and are known as OBRA Waivers because they originate from changes to the Social Security Act of 1987 made as a result of the OBRA. These waivers were terminated and the participants shifted to HCS Waivers. ** Texas Department of Aging and Developmental Services (DADS) projection. | |||||||
As can be seen, waiver enrollment increased modestly between 2000 and 2003. Since 2003, waiver enrollment has stepped up due to the combined impact of the implementation of the TxHL Waiver and the appropriation of additional funds to reduce the waiting list.
| TEXAS WAIVER ENROLLMENT |
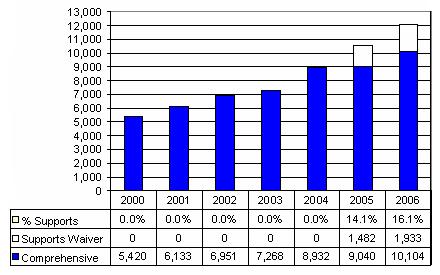 |
| EXPENDITURES BY YEAR | |||||||
|---|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003* | 2004 | 2005 | 2006** |
| Comprehensive ($M)* | $200.5 | $227.4 | $262.5 | $290.2 | $317.5 | $325.7 | $378.7 |
| Per Participant | $37,000 | $37,072 | $36,771 | $39,938 | $35,548 | $36,038 | $37,480 |
| Supports ($M) | $0 | $0 | $0 | $0 | $0 | $2.9 | $16.8 |
| Per Participant | $0 | $0 | $0 | $0 | $0 | $1,928 | $8,669 |
| Total Expenditures ($M) | $200.5 | $227.4 | $262.5 | $290.2 | $317.5 | $328.6 | $395.5 |
| Supports Waiver % of Total Expenditures | 0% | 0% | 0% | 0% | 0% | 0.9% | 4.2% |
| Cost Per Participant: % Supports to Comprehensive | 0% | 0% | 0% | 0% | 0% | 5.3% | 23.1% |
| Blended Cost Per Participant | $37,000 | $37,072 | $37,771 | $39,938 | $35,548 | $31,239 | $32,857 |
| * Includes the HCS Waiver with MRLA and HCS-OBRA Waiver expenditures through 2003. ** Estimate. | |||||||
| TEXAS WAIVER EXPENDITURES ($M) |
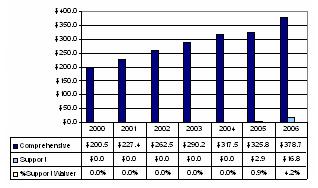 |
Between 2000 and 2006, the total Texas waiver expenditures will have nearly doubled. There will be a substantial increase in spending between 2005 and 2006 as a result of the additional funds appropriated to reduce the interest list. HCS expenditures per participant are relatively low for a comprehensive waiver. This is due in part to Texas limiting HCS enrollment to persons whose service needs can be met at less than the cost of ICF/MR services. In 2006, TxHL Waiver per participant costs are running at 87 percent of the $10,000 funding limit.
| TEXAS EXPENDITURES PER PARTICIPANT |
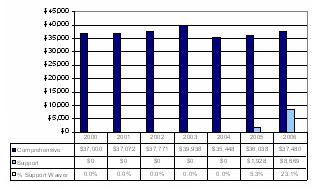 |
| WEB-ACCESSIBLE RESOURCES/ADDITIONAL INFORMATION | |
|---|---|
| Resource | Description/Web-Address |
| Texas Home Living Waiver | Web page has the original approved Home Living Waiver application http://www.dads.state.tx.us/business/mental_retardation/txhml/TexasHome… |
| Texas Department of Aging and Disability Services (DADS) | Main web page to Texas DADS http://www.dads.state.tx.us |
| Home and Community-Based Services (HCS) Program | Website contains information about the HCS Waiver http://www.dads.state.tx.us/services/dads_help/mental_retardation/HCSpr… |
Document Inventory
- Description of Home and Community-Based Services (HCS) Program
- History of Numbers of People Served Community System FY 1990 through FY 2003 in Texas, and Utilization and Expenditure Summary from Texas
| STATE CONTACT INFORMATION | |
|---|---|
| Name | Beverly Sawyer Program Specialist |
| Agency | Texas Department of Aging and Disability Services |
| Address | 701 W. 51st Street Austin, TX 78751 |
| Telephone | 512-438-3530 |
| beverly.sawyer@dads.state.tx.us | |
WASHINGTON
| WAIVERS | |||||
|---|---|---|---|---|---|
| Waiver Title | Type | CMS Waiver # | Participants (2005) | Start Date* | Status |
| Basic Waiver | Supports | 0408 | 3,407 | 04/2004 | Initial |
| Basic Plus Waiver | Supports | 0409 | 2,202 | 04/2004 | Initial |
| Core Waiver | Comprehensive | 0410 | 4,185 | 04/2004 | Initial |
| Consumer Protection | Comprehensive | 0411 | 403 | 04/2004 | Initial |
| * Waivers replaced Community Alternatives Program (CAP) Waiver which started in 1984. | |||||
| BASIC SUPPORT WAIVER FEATURES | ||
|---|---|---|
| Supports Waiver Target Population | Basic Waiver. Targets children and adults with developmental disabilities living with family or in their own homes who have strong natural supports systems but may be at risk of more restrictive placement due to needs for physical, mental health or behavioral services or need for support t a caregiver. Basic Plus Waiver. Targets children and adults with developmental disabilities living at home with family or in another setting with assistance. These individuals are at high risk of out-of-home placement or loss of their current living situation due to issues such as abuse and neglect, serious medical problems requiring close monitoring, challenging behavior, and/or mental health or substance abuse concerns. The individuals served through the Basic Plus Waiver program also generally have substantial functional limitations resulting in need for frequent assistance to remain at home or participate in community activities and/or the individual has need for protective supervision due to impaired judgment. The Basic Plus Waiver also covers services in generic living arrangements such as adult foster care settings. | |
| Funding Limit | Each support waiver is subject to different funding limits. In both waivers, there are funding limits that apply to groups of certain services: | |
| Service Group: Respite care, environmental accessibility adaptations, transportation, specialized medical equipment and supplies, physical therapy, occupational therapy, speech, hearing and language services, behavior management and consultation, staff/ family consultation and training, specialized psychiatric services, and community guide. | Basic Waiver Limit: $1,425/year. Basic Plus Waiver Limit: $6,070 [N.B., Basic Plus also includes skilled nursing in this group] | |
| Service Group: Person-to-person, supported employment, community access, pre-vocational services. | Basic Waiver Limit: $6,500/year. Basic Plus Waiver Limit: $9,500 but may be increased to $19,000 based on assessed need. | |
| In addition, participants in both waivers are eligible for Medicaid state plan personal care services and waiver-funded supplements to personal care. The amount of such services is determined through the application of the state’s Comprehensive Assessment Reporting Evaluation functional assessment tool. The amount of respite care is authorized through a separate assessment. | ||
| Funding Parameters | See above. | |
| Exceptions to Funding Limit | Both waivers provide for temporary emergency assistance of up to $6,000 as an override to the dollar limits that apply to the service groups above. Emergency assistance is a temporary increase in the level of any waiver service for the purpose of preventing permanent out-of-home placement. Emergency assistance is provided in one of the following emergency situations: involuntary loss of present residence for any reason either temporary or permanent; loss of present caregiver for any reason, including death of a caregiver or changes in the caregiver’s mental or physical status resulting in the caregiver’s inability to perform effectively for the individual; significant changes in the emotional or physical condition of the individual that necessitate substantial expanded accommodations. | |
| Transition to Comprehensive Waiver | Individuals may transition to the Core Waiver (not an acronym but the central comprehensive waiver offering residential services) or Consumer Protection waiver based on need and slot availability. | |
| Self-Direction | Limited. Community guide and person-to-person services are similar to “support broker” services. Participants or families may hire, fire, and supervise personal care workers. | |
| SUPPORTS WAIVER SERVICES | ||
|---|---|---|
| Support/Service Category | Y/N | Washington Waiver Services |
| Case Management/Service Coordination | N | [State-operated case management is furnished as a Medicaid administrative activity] |
| Supports of Participant Direction (Support Broker) | N | |
| In-Home Services | Y | Personal Care (supplement to Medicaid state plan personal care services) |
| Respite | Y | Respite Care |
| Day Supports | Y | Person-to-Person; Community Access; Pre-vocational Services |
| Health Related | N | |
| Supported Employment | Y | Supported Employment |
| Transportation | Y | Transportation |
| Person Directed Goods and Services | N | |
| Equipment/Supplies | Y | Specialized Medical Equipment and Supplies |
| Vehicle Repair/Modification | N | |
| Clinical Services | Y | Specialized Psychiatric Services and Behavior Management; Physical Therapy, Speech, Hearing, and Language Services, Occupational Therapy are furnished as supplements to Medicaid state plan services |
| Environmental Accessibility Adaptations | Y | Environmental Accessibility Adaptations |
| Financial Management Services | N | |
| Family and Caregiver Training | Y | Staff/Family Counseling and Training |
| Other | Y | Emergency Assistance; Community Guide |
| The following services are only available in the Basic Plus Waiver | ||
| Health | Y | Skilled Nursing |
| Other | Y | Adult Foster Care and Adult Residential Care |
Background Information: Supports Waiver
In January 2004, Washington replaced its single Community Alternatives Program (CAP) HCBS waiver for persons with developmental disabilities with four new waiver programs. The four replacement waivers are: Basic Waiver, Basic Plus Waiver, Core Waiver, and Community Protection Waiver. The Basic and Basic Plus waivers are supports-type waivers; the Core waiver is a comprehensive waiver offering a full array of services, including residential services; and, the Community Protection waiver targets individuals who have been charged with and/or convicted of certain type of crimes, including violent crimes or sex offenses.
Washington used a step-up approach in designing these waivers. Funding scales upward based on the service need intensity/profile of the individuals that each waiver serves as illustrated by the following 2005 per participant costs for each waiver:
| Waiver | Estimated Per Capita Cost (Year 1) |
|---|---|
| Basic | $11,890 |
| Basic Plus | $15,913 |
| Core | $53,111 |
| Community Protection | $94,781 |
The Basic Waiver provides participants with day supports funding plus a modest amount of additional funds to purchase other services. Basic Plus provides steps up funding for both day support and other services. Except for the addition of skilled nursing and payment for generic community residential services in the Basic Plus waiver, both waivers have the same service package. The Core Waiver includes comprehensive specialized residential services in addition to the Basic Plus waiver service package. The Core Waiver does not include funding limits on groups of services.
The decision to split the predecessor CAP waiver into four distinct waivers was an outgrowth of CMS State Medicaid Director Letter #4 which provided in part that all services offered under a waiver must be available without limit to all participants in a waiver. State officials determined that continuing to operate a single waiver that spanned individuals who have differing need/situational characteristics would be problematic in light of State Medicaid Director Letter #4. Dividing the CAP waiver into four separate waivers subject to differential funding limits emerged as a means for the state to ensure compliance with State Medicaid Director Letter #4 and ensure that waivers could be managed within available funds. Washington officials decided that they needed to better tools to “sort out” what are the appropriate services for an individual and manage access to the full range of services for those most in need. The reconfiguration of the waivers led the state to clarify under what conditions individuals are eligible for a specific array of supports and services. The multiple waiver strategy and entrance criteria make it clear to consumers and families that not everyone will receive full around-the-clock supports, but supports and services are tailored to individual situations and need.
The Basic and Basic Plus imposition of funding limits on groups of services rather than the total amount of waiver services reflected CMS policy at the time that Washington reconfigured the CAP waiver. In order to establish funding limits, CMS required that a state impose dollar limits on the amount of services that could be authorized rather than impose an overall limit.5 Washington is in the process of establishing waiting list criteria for entrance into the reconfigured waivers. Statistical Profile
Statistical Profile
| WAIVER PARTICIPANTS BY YEAR | ||||||
|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 |
| Comprehensive | 8,984 | 9,413 | 9,063 | 8,685 | 8,260 | 4,588 |
| Basic Supports | 0 | 0 | 0 | 0 | 0 | 3,407 |
| Basic Plus Supports | 0 | 0 | 0 | 0 | 0 | 2,202 |
| Total Participants | 8,984 | 9,413 | 9,063 | 8,685 | 8,260 | 10,197 |
| Supports Waiver % of Total Participants | 0% | 0% | 0% | 0% | 0% | 55.0% |
During the period 2000-2005, waiver enrollment in Washington increased by 12.8 percent. The drop in comprehensive waiver enrollment in 2005 is an outgrowth of the redistribution of CAP waiver participants to the new waivers.
| WASHINGTON WAIVER ENROLLMENT |
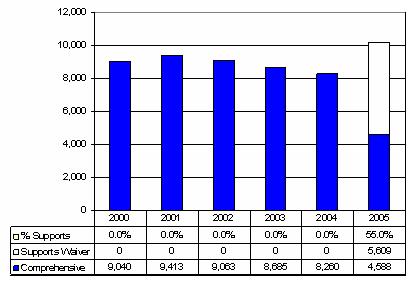 |
| EXPENDITURES BY YEAR | ||||||
|---|---|---|---|---|---|---|
| Waiver | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 |
| Comprehensive ($M)* | $195.1 | $203.1 | $237.9 | $247.8 | $190.6 | $260.5 |
| Per Participant | $21,723 | $21,573 | $26,255 | $28,533 | $23,081 | $56,771 |
| Supports ($M) | $0 | $0 | $0 | $0 | $0 | $76.2 |
| Per Participant | $0 | $0 | $0 | $0 | $0 | $13,581 |
| Total Expenditures ($M) | $195.1 | $203.1 | $237.9 | $247.8 | $190.6 | $336.7 |
| Supports Waiver % of Total Expenditures | 0% | 0% | 0% | 0% | 0% | 22.6% |
| Cost Per Participant: % Supports to Comprehensive | 0% | 0% | 0% | 0% | 0% | 23.9% |
| Blended Cost Per Participant | $21,723 | $21,573 | $26,255 | $28,533 | $23,081 | $33,020 |
| * The comprehensive waiver of 2005 is not comparable to the prior five years due to the reconfiguration fo the predecessor CAP waiver. | ||||||
| WASHINGTON WAIVER EXPENDITURES ($M) |
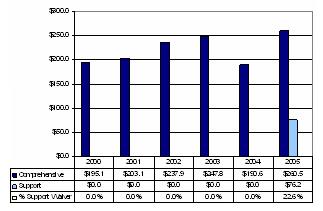 |
During the period 2000-2005, Washington’s total HCBS waiver expenditures increased by 83 percent. The comprehensive waiver per participant cost in 2005 is not comparable to the prior five years due to the reconfiguration of the predecessor CAP waiver.
| WASHINGTON EXPENDITURES PER PARTICIPANT |
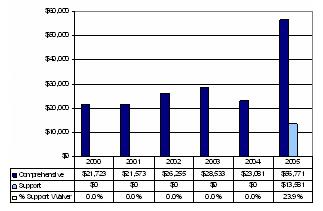 |
| WEB-ACCESSIBLE RESOURCES/ADDITIONAL INFORMATION | |
|---|---|
| Resource | Description/Web-Address |
| Washington’s Home and Community-Based Waiver Program | Web page describing Washington’s HCBS waivers http://www1.dshs.wa.gov/ddd/waivers.shtml |
| Chapter 388-845 WAC -- HCBS waiver rules | Web page with links to waiver rules http://apps.leg.wa.gov/WAC/default.aspx?cite=388-845 |
| Basic Waiver Document | http://www1.dshs.wa.gov/pdf/adsa/ddd/BasicWaiver.pdf |
| Basic Plus Waiver Document | http://www1.dshs.wa.gov/pdf/adsa/ddd/BasicPlusWaiver.pdf |
| Core Waiver Document | http://www1.dshs.wa.gov/pdf/adsa/ddd/CoreWaiver.pdf |
| Fact Sheet Washington Developmental Disabilities Waiver Plan, revised May 2005 | Fact sheet that summarizes Washington’s four developmental disabilities waivers http://www1.dshs.wa.gov/word/adsa/ddd/waiverFacts.doc |
| Washington’s Waivers for Developmental Disabilities | Two page brochure describing Washington’s HCBS waivers http://www1.dshs.wa.gov/pdf/Publications/22-605.pdf |
Document Inventory
- 2004 Core, Basic, Basic Plus, and Community Protection Waiver Documents (as initially approved by CMS)
- Power Point on Support Waivers
- 2005 Description of Individual Living Options
- 372 reports for four waivers for 2005
- Basic Plus Amendment #4 2006
- CMS 372 initial reports for 2005, 2006 Basic Waiver Amendment #3 Final
| STATE CONTACT INFORMATION | |
|---|---|
| Name | Shannon Manion |
| Agency | Washington State Department of Social and Health Services Division of Developmental Disabilities Aging and Disability Services Administration |
| Address | P.O. Box 45310 Olympia, WA 98504-5310 |
| Telephone | 360-725-3445 |
| maniosk@dshs.wa.gov | |
NOTES
-
For background information concerning the Systems Change Project, see Gary Smith, John Agosta, and Reena Wagle (2002). An Evaluation of the Colorado Systems Change Project. Tualatin, Oregon: Human Services Research Institute. Available at: http://www.cdhs.state.co.us/ohr/dds/HSRI%20-%20Systems%20Change%20Evalu….
-
See Gary Smith (2006). Status Report: Litigation Concerning Home and Community Services for People with Disabilities. Portland, OR: Human Services Research Institute.
-
Located at http://egov.oregon.gov/DHS/dd/adults/benefitlevels.shtml.
-
In Pennsylvania, services for persons with related conditions are furnished through separate programs.
-
The Texas Home Living, Ohio Level One, and Tennessee supports waivers are similarly structured.
APPENDIX B. STATE-BY-STATE CASE STUDY RESULTS
PDF Version (66 PDF pages)
TABLE OF CONTENTS
FLORIDA
Introduction
Florida’s Family and Supported Living (FSL) Waiver was initiated in October 2005 with enrollment quickly growing to 2,650 recipients. The focus of these supports is to provide services to children and adults with disabilities living at home. Today there are 5,921 people enrolled in the supports waiver and 26,079 others served through the state’s comprehensive waiver.
Method
In September and October 2006, the Human Services Research Institute (HSRI) staff visited Florida to conduct face-to-face consultations with key informants and also conducted discussions by telephone with additional informants. The individuals included in these conversations were: (a) state Agency for Persons with Disabilities (APD) staff including the state director, waiver manager and others along with personnel with the Florida Medicaid, Bureau of Medicaid Services, Developmental Disabilities Services Division; (b) representatives from interests outside the state agencies including the chair for community living and family committee from the Developmental Disabilities Planning Council and several families representing regional Family Care Councils; (c) service providers associated with the Florida Association of Rehabilitation Facilities; (d) independent support coordinators who perform service planning and monitor service delivery; and (e) staff of the Delmarva Foundation which manages Florida’s statewide waiver quality assurance/improvement program.
Results
What follows are results of the conversations. First, information is presented to describe the policy goals of the waivers, information on waiting lists, and the fundamental waiver operations. Second, views offered by the informants are presented related to: (a) access to the waiver; (b) waiver operations such as budget allocations, service planning, service delivery, and safeguards; (c) outcomes; and (d) key issues in play.
Florida Policy Goals
Question: What are the major policy goals of the supports waivers and how successful have the waivers been in meeting them?
- Cost containment and budget related goals were a primary focus of the FLS waiver. The FSL Waiver employs a funding cap in order to serve more people with fewer dollars than would ordinarily possible.
- Goals related to addressing the waiting list are also a primary focus. When the state settled the Prado-Steiman litigation, it committed to serving all eligible individuals who were on the waiting list as of June 1999. This goal was met, and the number of people receiving waiver services grew from 13,800 in 1999 to over 24,000 in 2004. Florida Governor Jeb Bush was instrumental in securing additional funding during this period and continues to support funding increases for developmental disability services.
- However, despite tripling funding for developmental disabilities during the period and substantial and necessary expansion of the comprehensive waiver, the waiting list climbed to 15,000 people. The FSL Waiver emerged as a means to support individuals and families who are on the comprehensive waiver waiting list by offering them a more limited package of in-home and other supports. In February 2007 the Florida legislature has continued its debate on the waiting list and additional potential future funding.
- Consumer-direction and person-centered planning goals are not primary goals of the FSL Waiver. The state is interested in flexible budget usage and improving its ability to assess individual support needs. Florida operates a pilot Centers for Disease Control and Prevention waiver that serves about 1,000 people and incorporates self-direction.
- Rebalancing the long-term care system and refinancing community services have not been primary policy goals.
- The state also is pressing for increased use of supported employment and supported living services.
Wait-lists
Question: How many people are on the consolidated (i.e., all wait-lists for developmental disabilities services) wait-list?
- In 2005, after a strong enrollment effort, 5,600 people were admitted to the waiver, reducing the wait-list to 6,200. To promote the waiver, 11,000-12,000 letters were sent to potential enrollees. But the wait-list has climbed back to about 12,000 due to: (a) continuing increases in the numbers each year who come forward seeking services; and (b) delayed impacts of population disruption and population migration due to hurricane impacts.
- State officials expect that there will be 9,000-10,000 people on the waiting list at year’s end.
- In July 2006, the Florida Office of Program Policy Analysis and Government Accountability called for APD to improve its management of the waiting list with more regular review, updating, and identifying service needs. APD was encouraged to develop a multi-year plan for addressing the waiting list for waiver services that considers the length of time individuals have been on the waiting list, how soon the individual is expected to need waiver services, the expected level of services to be provided, and whether the individual is receiving services from other waivers or programs. In February 2007, the Florida legislature was weighing additional funding to help people move from the wait-list.
- People enrolled in the FSL Waiver may maintain their position waiting for the comprehensive Developmental Services Home and Community-Based Services (HCBS) Waiver (the comprehensive waiver).
Question: How are wait-lists maintained?
- Waiting lists are maintained for each waiver. State area offices process enrollment requests and maintain a consolidated wait-list that is also shared with the APD central office. Individuals apply for APD services and are later identified as potential waiver enrollees. A preliminary needs assessment is used by the state to select individuals who are on the waiting list for the FSL Waiver. When a waiver opening becomes available, the person is assigned a support coordinator. The central APD office keeps a running tally of the waiting list counts as information flows in from the area offices.
Question: How long generally is the wait?
- The average time on the waiting or interest list before an individual is enrolled is now five years or less, down from eight years in 2003. Some 81 percent of the individuals waiting are age 30 and under. Most of these potential enrollees have an intellectual disability. In January 2007, Florida’s APD was anticipating a $230 million deficit through the next year and a half. The Florida Legislature in February 2007 continued to examine the wait-list. Since then, Florida’s new Governor Charlie Crist released his budget recommendations for FY 2007-2008 that includes $119 million to cover the growing demand for waiver services through increased utilization from existing customers, and to provide waiver services to customers transitioning from the developmental services institutions.
- Governor Crist also earmarked funds to take care of citizens with developmental disabilities that find themselves in extreme need due to a caretaker or housing crisis. Over $7 million will be used to care for 500 new crisis customers in the upcoming year and another $6.7 million will pay for the crisis customers that will enter the program this year.
- In addition, the proposed budget provides $6.6 million to allow the agency to serve more people in its Mentally Retarded Defendant Program and may take steps to reduce it.
Basic Operations
Question: How are people selected for enrollment?
- The enrollment process for the FSL Waiver is a step by step process that is coordinated by the central office and area office to track and guide applicants through the enrollment process. Interest letters are used by the area office with screening questions to check for HCBS eligibility criteria. A preliminary needs assessment is used to select individuals for the support waiver. Foster children with individual and other developmental disabilities (I&DD) and referrals with I&DD from the corrections system are covered by the comprehensive waiver but entry to the comprehensive waiver is now restricted due to funding limitations. In the current FY support waiver enrollment is also severely limited due to funding limitations. When the support waiver began, the enrollment process was controlled by the central office but this process has been moved to the area offices throughout Florida.
Question: Is there descriptive information available on the people served in the supports waiver (e.g., age, primary disability, living arrangement, functional status, caregivers)? Is systematic information available regarding waiver impacts?
- The APD annual report and brochures broadly defines profiles of those served in the supports waiver.
- More descriptive information is available to describe individual characteristics such as age, primary and secondary disability, and living arrangement.
- Systematic information about the impact of the supports waiver on is produced by the statewide quality assurance program.
Question: How is quality assurance and quality management managed?
- The same quality management architecture is employed for both waivers.
- Family Care Councils have been organized by region. The councils have many families of individuals who are relatively new to waiver services. The councils provide information to families and serve as a conduit of information and experience about the waiver among families. (See the booklet Planning Ahead which is available on-line at http://www.fddc.org or the brochure titled Protecting Legal Rights: It’s in Your hands! available at http://apd.myflorida.com.
Question: How are individual service plans developed?
- Independent service coordinators meet with the person and their family or representative/legal guardian to complete needs assessments; identify supports needed and develop a plan to address stated needs.
- As a practical matter, the service coordinators often feel that if an individual wants a particular service or support, it can be submitted in the plan even though it may not be approved.
Question: How are individual allocations set?
- In September 2006, the waiver funding cap was increased to $14,792, up from $14,282. Previously, varying “soft caps” per person were applied but have been eliminated in favor of an overall total dollar cap per person. Exceptions are not made to the overall total support waiver cap.
- Individual assessments are conducted using a tool called the Individual Cost Guidelines. It determines the recipient’s specific resource allocation for waiver funds for recipients receiving supports.
- The individual has knows the funding allocation before planning starts. However, some informants expressed the concern that sometimes the amount of the funding allocation is not made known to families and individuals before a plan is created.
Question: What decision-making authority do individuals/families have over the budget?
- They can plan within capitated dollar limit and determine services and supports needed. Among people with two full years of plan development the average plan cost was approximately $9,000 but the actual expenditures averaged about $4,000. Understanding this pattern and the reasons driving it may take several years, in part because of the rapid growth and relative newness of the support waiver.
Question: Who has primary responsibility for developing the service plan?
- Individual support coordinators have primary responsibility.
- Among the service planners, the average caseload is 36 individuals per service planner, ranging from 18 to 42 individuals per planner.
- In Florida, people do not have paid outside assistance available to them during the planning process to help design the service plan.
Question: Does the service planning include a distinct risk assessment process to identify and address identified risk?
- Service planning does not include a distinct risk assessment process to identify and address identified risks and negotiated risk agreements are not used.
Question: Is the process the same or different from that used in the comprehensive waiver?
- Yes, it is the same process. The FSL Waiver has fewer services and supports and the resulting plans are often simpler but similar to the plans written in the comprehensive waiver.
Question: What happens to individuals when they need more support than the waiver can offer, either by way of particular services and/or overall cost?
- Individuals can apply for crisis enrollment on the comprehensive waiver. A specialized state committee examines individual requests and assessed needs. Sometimes Medicaid state plan services can help with portions of the problems presented.
Question: What parameters govern transition from the supports waiver to the comprehensive waiver?
- FSL Waiver participants retain their position on the comprehensive wait-list for potential future opportunities. Due to funding limits, at present enrollment in the comprehensive waiver is tightly controlled.
Question: How might a person be disenrolled from the supports waiver?
- An individual may be disenrolled from the supports waiver when the individual: (a) request such action; (b) is incarcerated; (c) no longer has a disability; (d) is no longer financial eligible; (e) moves out of state; (f) no longer meets level of care; (g) is admitted to nursing facility or intermediate care facility for the mentally retarded (ICF/MR); (h) is no longer eligible for Medicaid; (i) refuses services; or (g) fails to cooperate.
Question: What if the individual wants to change their service plan, or wants to change providers?
- The individual notifies his or her service coordinator that they wish to change, select a new provider, and set a date for new provider to begin providing services. The service coordinator works through the required notifications and new authorizations.
Question: How is quality assurance and quality management managed?
- The Quality Assurance System has produced a wealth of information with a uniform state system that measures the results of both the comprehensive and supports waivers. The system is contracted out to the Delmarva Foundation.
- The overall quality assurance approach has changed from an outcome perspective to quality assurance with “we are here to help you” theme. The entire and extensive body of work is available on the Internet at http://www.dfmc-florida.org.
- Monitored elements have been reduced from 175 elements to 11 elements. These include five related to service process (e.g., background screenings, documentation for billings) and six tied to outcomes (e.g., health status, skills building).
- The implementation of policies by providers, not just having them, has been a key Florida discovery. The providers meet the extensive FSL Waiver handbook at 85-90 percent level but the quality assurance efforts stress a focus on the person and their outcomes.
- The Quality Assurance/Quality Management System for the FSL Waiver is the same as the comprehensive waiver. It is also the same provider network with 95-98 percent of the service providers the same. Next year the quality assurance system will differentiate between the FLS Waiver and the comprehensive waiver.
Question: How are complaints resolved?
- Individuals can file a complaint through a “Fair Hearing” process that is used to appeal a decision made by the state, or through a grievance available through the recipient’s chosen support and service providers.
- Where a grievance procedure is used, the grievant identified their grievance and proposed resolution. The provider responds to the grievance, this response can be appealed to the governing body. Grievance logs are examined by the state and must be maintained by providers.
Question: What is the process that is used to monitor the health and well-being of individuals participating in the supports waiver?
- The process used includes service coordination consultation, on site consultation, desk reviews, and follow consultations.
- On-site monitoring is performed a minimum of every six months.
- A primary difference between the approach to supports waiver monitoring and comprehensive waiver monitoring is that the comprehensive waiver requires monthly face-to-face visits.
- Service coordination follows up to resolve problems revealed by monitoring. Area offices track incidents and share them with quality assurance.
Opinions on Waiver Operations and Effects
Access to the Waiver
Explanation: Access refers to how easily people can apply for and gain admission to the supports waiver.
- Potential enrollees learn about this supports waiver program from current consumers, conferences, family care councils, printed matter and the website. Funding also shapes how people learn about the FSL Waiver. Many people are referred to the APD website for information. In the current year when new dollars for enrollment are very limited, some complain that people have been discouraged from applying for the consolidated waiting list.
- The supports waiver is not aggressively publicized. Word of mouth is probably the most common way families and individuals learn about this opportunity.
- It is “Very Easy” to apply. The demand for this FSL Waiver among people is increasing steadily. Personal documentation for some, however, may be difficult to provide. Cultural diversity issues in some locations in Florida make it harder to get and use services.
Service Planning
Explanation: Service planning refers to the process to develop individual support plans for waiver recipients.
- Some informants indicate individuals “somewhat” leads the planning process
- However, the state officials indicate that the FLS Waiver “very much” permits recipients to define their own service needs, and choose the agencies or support givers to offer the needed support.
- Informants note that the recipients “somewhat” exercise choice and control over service plans but this is shaped by the community they live in, provider issues that may limit it, sometimes parental control, and depends on the support coordinator. Others suggest that the supports waiver is inherently limited in choice because it does not offer as many services or dollars as the comprehensive waiver. Many indicated that they would like to see more services, no caps, and more flexibility for families and individuals.
- State staff feels that service planners get to know the individuals they are planning for “Very Well” while others would not go so far.
- Most agree that there are some very good support coordinators who know the individual and families well. Yet, there is a high turnover and some may be new and developing the necessary skill set. The state has tightened up qualifications and is examining competency-based certification and instruction for support coordinators.
Question: What if the individual wants to change their service plan, or wants to change providers?
- It is very easy is it for individuals to change service providers and this generally can be accomplished within days.
- Waiver participants cannot generally hire and manage their own support workers. While the workers are employed by an agency, participants often identify and refer potential workers to the agency and manage them on a day to day basis.
- Where “in-home” supports are offered to adults living home with family, the services are seen by the state as most often person directed; some feel that it depends on the individual and family.
- The services available through these waivers are generally broad enough to meet participant needs for individuals who do not have high needs or need to live in a group home.
- Informants indicate that it is “Somewhat Easy” for individuals to change their service plans. Regional offices can deal with emergency situations.
Service Delivery and Safeguards
Explanation: Service delivery and safeguards refers to the services that individuals received and their operations, and the safeguards in place to assure health and well-being.
- Once services are authorized, informants indicate that it is neither “Easy” nor “Hard” for individuals to get these services.
Satisfaction with Outcomes
- Generally, informants indicate that recipients are not living on their own or with friends, but are participating in community events.
- Informants indicate that there is “Some” emphasis on services to promote community integration versus services that are more traditional (sheltered work, enclaves, segregated activities…). Many individuals, however, use segregated services.
- Employment outcomes have been increasing from a 2,428 person baseline in 2004 to 4,441 people maintaining employment in 2006 with the five-year target of 5,842 people maintaining employment by 2009.
- To assure the health and well-being of participants, the safeguards in place are generally thought to be working well.
Key Issues in Play
Question: What are the waiver’s greatest strengths?
- A major strength of the FLS Waiver is the ability to serve a large number of services recipients at a predictable cost.
- Generally, many people report being satisfied with services and report being very happy.
- Governor Jeb Bush has invested significant sums in making waiver options available.
- The privately contracted quality assurance project is effective in documenting system change through statewide efforts.
- Many Florida applicants have come off the waiting list and are now receiving services.
Question: What are the barriers to achieving the waiver’s goals?
- Workforce issues. Workers cannot be found easily and there is concern over what they are paid and the associated benefits.
- Some see shortcomings as difficulties in accessing professional therapies in some communities and the time it takes to get service authorizations approved.
- Many people, families and individuals, report a desire for increased self-determination with more choices and control over their chosen services, units, and activities.
- People are being taken off the waiting list but the list continues.
- Restrictions require the individual to leave the family home if they need a lot of care. Sometimes this seems neither less costly nor better for the individual.
Question: Are there topics where there is disagreement or concern?
- There is pressure to both add services and dollars to existing plans and also to take people off of the waiting list.
- The state has worked hard to get the supports waiver up and running and continues to seek refinements in practice as it gains experience.
- Like most states the individual (independent) Medicaid certified providers who are direct support workers look at the person served and their families as the employer of record. This creates problems in liability, workmen’s compensation, routine paying of Federal Insurance and Compensation Act and other taxes that can create trouble for the employer in some situations.
Question: What are the TOP THREE things that could be done to improve the waiver?
- Increase flexibility. Allow people to use more of the funds for needs during the year (parallel funding for horizontal needs).
- Add a self-directed service option. In some cases people do not know how to use the services and supports.
- Remove cap limits on spending when a person needs more services to stay in their family home. Currently if they need nursing, therapies, or extensive care they have to leave their family home and join the comprehensive waiver. Some say that this is not always optimal for care or cost. Others feel like the cap should be flexible in some situations and that expenditures should be more in some individual situations.
- Add funds to adjust current plans and eliminate the waiting list.
- Many felt that the FSL Waiver should be expanded to include all or most of the services on the comprehensive waiver although it would need to have the same annual cap. Others suggest adding speech therapy, durable medical equipment, therapy for adults, and/or all the services in the comprehensive waiver.
- Find a way to enable environmental one time costs that hit once in a person’s plan but wipes out most of their dollars for the entire year.
Question: What other points should be raised?
- Many parents, appreciative of the supports waiver, continue to desire additional service choices and sometimes more services overall.
- The need to eliminate any soft caps for services within the FSL Waiver and add supports for children, including needed behavioral supports.
Overall Impressions
All informants agree that the supports waiver is generally a positive development though early in its development. It has been effective at helping to reduce the wait-list and contain costs within a predictable budget. Still, many suggest that:
- The comprehensive waiver needs to continue to be available for those that “cap out” of the “supports waiver.”
- More service options might be added to this waiver to better tailor services and supports to needs.
- Many want more flexibility in the services and an increase in the range of choices that individuals and families could use.
Florida provides an excellent example of what can be done, in a relative short time, with what is already the second largest support waiver in the United States.
MISSOURI
Introduction
The Missouri Community Supports Waiver (CSW) for people with developmental disabilities was launched in 2003. Missouri built on its experience in furnishing state-funded, family-centered services in designing this waiver to underwrite alternatives to residential services. The waiver’s major aim is to reduce the waiting list through the delivery of lower-cost services.
Method
In August and September 2006, HSRI talked with key Missouri informants to obtain more in-depth information concerning CSW. Informants included: (a) Division of Mental Retardation and Developmental Disabilities staff, including the Division director and senior program managers; (b) the director of the Missouri Planning Council for Developmental Disabilities; and, (c) personnel at the Institute for Human Development at the University of Missouri-Kansas City, the Missouri University Centers for Excellence in Developmental Disabilities. The Institute works extensively with individuals and families throughout the state.
Results
What follows are results from the key informant consultations. First, information is presented to describe the policy goals of the waiver, information on any service wait-lists, and the fundamental operations of the waiver. Second, opinions offered by the discussion participants are offered related to: (a) access to the waiver; (b) waiver operations, service planning, service delivery and safeguards; (c) outcomes; and (d) key issues in play.
Missouri Policy Goals
Question: What are the major policy goals of the supports waivers and how successful have the waivers been in meeting them?
- CSW was designed to serve as a low-cost alternative to the comprehensive waiver and as a vehicle to reduce the waiting list. CSW was not launched in response to a lawsuit.
- The CSW has been successful in relieving pressure on the mental retardation and other developmental disabilities (MR/DD) Comprehensive Waiver. Still, the overall number of people waiting for services continues to grow.
- Implementing self-direction direction and person-centered planning are seen as secondary goals. Presently, there is limited use of waiver self-direction opportunities.
- Rebalancing the long-term care system was not a policy goal. CSW permitted Missouri to refinance some state-funded community services in order to finance system expansion.
Wait-lists
Question: How many people are on the consolidated (i.e., all wait-lists for developmental disabilities services) wait-list?
| CSW | Comprehensive Waiver | |
|---|---|---|
| 2005 | 3,246 | 441 |
| 2004 | 446 | 1,540 |
| 2003 | 256 | 1,180 |
Question: How are wait-lists maintained?
- Missouri maintains a statewide waiting list. State service coordinators maintain the waiting list and track the status of individuals on the waiting lists. (Missouri maintains two statewide waiting lists, one for residential services and one for in-home services). However, some of the people on these lists are not Medicaid-eligible and others are eligible for Missouri Division of MR/DD Services but do not qualify for ICF/MR level of care. That is, eligibility for a waiver has not been determined for all individuals on these lists. Further, individuals may be added to the residential waiting list for “planning purposes.”
- Missouri uses a scored instrument to assess the urgency of need of people on the waiting list.
Question: How long generally is the wait?
- The average wait time is more than two years.
Basic Operations
Question: How are people selected for enrollment?
- People are selected for services by a utilization review (UR) committee based on waiting list score. Available funds are prioritized to support people who are experiencing an emergency or crisis.
Question: Is there descriptive information available on the people served in the supports waiver (e.g., age, primary disability, living arrangement, functional status, caregivers)? Is systematic information available regarding waiver impacts?
- There is no systematic information about the impact of the CSW on participants. By report, many people informally report that they are very happy with services and this result has been so common that more formal measures have not been used.
- Centers for Medicare & Medicaid Services (CMS) waiver reviews serve as the formal evaluations of the supports waiver.
- Missouri officials indicate that they know whether the waiver is effective by reviewing its impact on the waiting lists and by examining costs and reported satisfaction.
Question: How are individual service plans developed?
- State service coordinators meet with the person and their family or representative/legal guardian to complete a person-centered plan. Person-centered planning guidelines are posted on the state website.
- When the service plan is developed, a draft budget is also created that then goes to the UR committee. The committee considers the individual needs in the plan, any alternative means of meeting the needs, and the amount of service other individuals with similar needs receive in approving budgets.
Question: How are individual allocations set?
- The planning process identifies needs. A budget is drafted to meet the needs. The budget and plan are reviewed by the UR committee when it is the individual’s first plan/budget and when there is a request to increase supports. The individual does have general knowledge of the allocation before planning if the person had a plan the previous year.
- Missouri does not have a budget allocation tool. Individuals receive a copy of their approved budget annually.
Question: What decision-making authority do individuals/families have over the budget?
- Individuals and families have input in the planning process where needs are identified and how the needs can best be met are proposed. The budget is developed. All new budgets or requests for increases in a budget must go through UR.
Question: Who has primary responsibility for developing the service plan?
- State employee service coordinators located at Regional Centers have primary responsibility; some SB-40 County Boards also employ service coordinators. Missouri uses targeted case management to finance service coordination. Service coordinators facilitate the planning process with the consumer and legal representative and others they request to participate.
- Each service coordinators supports 50 individuals on average. Service coordinators support a range of 40-70 individuals. Case loads have been growing due to budget limits.
Question: Does the service planning include a distinct risk assessment process to identify and address identified risk?
- Negotiated risk agreements are not used.
- The new service planning process in the renewal for both the support and comprehensive waivers provides for risk assessment for people who self-direct their services. The state also is using the Health Inventory Screening tool. Nurses ensure that health needs are addressed in the plan. There is a registered nurse in each region and this has worked well.
Question: Is the process the same or different from that used in the comprehensive waiver?
- The planning process is the same as that used in the comprehensive waiver.
- Individuals usually do not utilize paid outside assistance to help design the service plan. Community Specialists (waiver service) can assist in facilitating the development of the plan when an independent facilitator is requested.
Question: What happens to individuals when they need more support than the waiver can offer, either by way of particular services and/or overall cost?
- Service coordinators may authorize additional services. Regional directors are empowered to respond to emergencies in individual circumstances. Exceptions may be granted based on need. If the increased need is long-term, the person may be transferred to the Comprehensive waiver. In the renewal, the CSW cap was increased to $22,000.
Question: What parameters govern transition from the supports waiver to the comprehensive waiver?
- In the last year, only 14 people moved from the CSW to the Comprehensive Waiver. People transition to the comprehensive waiver due emergencies and crises.
Question: What if the individual wants to change their service plan, or wants to change providers?
- The process that an individual must follow to change service providers includes notifying the service coordinator and over the course of 2-6 weeks the service plan is changed.
- The time it takes to change providers varies from days to months or more.
Question: How is quality assurance and quality management managed?
- The principle features of the waiver’s Quality Assurance/Quality Management System include case management, statewide UR committee, and quality management committee. The Quality Assurance/Quality Management System for the supports waiver is the same as the comprehensive waiver. A score card system has been developed. This area is seen by some as not as open and transparent or designed for sharing as it could be.
Question: How are complaints resolved?
- The process that an individual must follow to file a complaint includes a Department telephone hot line (800-364-9687). Also, the state has consolidated its complaint processes and pulled investigations and consumer complaints into one unit. Investigators who live in local areas around the state have been consolidated into a pool. The system is able to investigate abuse and neglect but additional investigators are needed.
- It is generally thought that the community safety and health record is good but the state has shared only limited information about abuse and neglect. Most provider types are licensed or certified by the state or nationally accredited. Training has helped regional centers better monitor fiscal matters. Service coordinators and local quality assurance staff throughout the state often play a key role in resolving complaints that are not considered abuse and neglect.
- The Task Force also has called for a toll-free phone number for reporting suspected abuse and for the public to have access to completed investigative reports as long as patients’ protected health information is not revealed.
Question: What is the process that is used to monitor the health and well-being of individuals participating in the supports waiver?
- The process includes service coordination and the quality assurance team. Monitoring is performed at least quarterly in CSW. In the Comprehensive waiver, service coordinators conduct monthly face-to-face monitoring for persons who receive residential (placement) services.
- One recent development is the emergence of self advocates and families excellence volunteer visits to homes. The state is recruiting volunteers.
- If there is a problem, service coordinators take immediate action. These situations are also reported to service coordinator supervisors and the Regional Center quality assurance team.
Opinions on Waiver Operations and Effects
Access to the Waiver
Explanation: Access refers to how easily people can apply for and gain admission to the supports waiver.
- The potential enrollees/families learn about this supports waiver program from service coordinators and other Regional Center or SB-40 County Board staff, with brochures and the new Network of Care website. Regional Center service coordinators perform intake and also explain services that are available.
- The supports waiver is somewhat publicized and individuals apply for services, qualify for the supports waiver waiting list, and are then enrolled by regional center service coordinators when openings become available through attrition or new funding.
- It is somewhat easy to apply for services but the demand for this waiver is growing quickly. Enrollment is dependent on identifying needs during the planning process and the scoring of the need through the UR process. The score determines the priority of the individual’s need in comparison with others who have needs.
Service Planning
Explanation: Service planning refers to the process to develop individual support plans for waiver recipients.
- Overall, respondents indicated that the planning process “somewhat” encourages individuals to exercise leadership, define their own service needs, and choose the agencies or support givers to offer the needed support.
- Overall, respondents indicated that recipients exercise some choice and control over service plans but this varies somewhat by region and participants may not have funds to secure the supports that they want.
- Overall, respondents indicated that service planners “somewhat” know the individuals they plan for. Problems arise due of staff turnover and case load variations that is caused, in part, by rotating service coordinators.
- The waiver renewal provides for a supports broker to assist individuals who self-direct services. It is now possible to hire independent facilitator.
- A Missouri company currently operates fiscal intermediary services and is able to respond quickly to timesheets and payroll responsibilities.
- The services available through CSW are generally broad enough to meet participant needs. The waiver is written adequately but implementation of the waiver is a challenge. Personal assistance varies a lot in the plans and there are frequent modifications.
- Overall, respondents indicated that it is “somewhat” easy for clients to change their service plans with variations among the different state regional centers.
- The strengths of the approach to individual planning are its ability to allow people to choose services and leave the waiting list.
- Some see shortcomings as difficulties in finding a more uniform experience in all of the regional centers for support waiver recipients.
Service Delivery and Safeguards
Explanation: Service delivery and safeguards refers to the services that individuals received and their operations, and the safeguards in place to assure health and well-being.
- Once services are authorized, respondents generally indicated that it is “somewhat” easy for individuals to secure services. Some rural areas present more difficulty but generally support waiver services are reasonably available.
Satisfaction with Outcomes
- Generally people do not seek/acquire/hold integrated employment but are quick to use segregated day habilitation. This is an aspect that the state is trying to change.
- Generally people do not live on their own or with friends and sometimes participate in community events.
- There is some emphasis in the waiver to stress services that promote community integration over services that more traditionally offer segregated options (e.g., sheltered work, enclaves, and other segregated activities). However, many participants are quick to use the segregated services.
- Waiver participants can hire and manage their own support workers. The addition of support brokers in the CSW renewal will help recipients manage workers on a day to day basis. About 200 individuals are managing their workers.
- Liability issues pertaining to these workers persist, as they do elsewhere. For instance, workers are not offered workers’ compensation.
- Fiscal intermediary support is adequate. This activity has been expanded in the newly renewed CSW.
- Where “in-home” supports are offered to adults living at home with family, the services are seen as most often as family directed rather than person directed. Family members probably manage the activities and workers 70 percent of the time.
- To assure the health and well-being of participants, the safeguards in place are generally thought to work well and families are helping to ensure the health and welfare of the waiver recipients.
- The more people in their lives who care for them the safer individuals are. Service coordination can often work well. But smaller service coordination case loads and more caring people in participant’s lives would be an improvement.
Key Issues in Play
Question: What are the waiver’s greatest strengths?
- A major strength of the CSW is its ability to serve more people at a lower-cost and take the pressure off the Comprehensive Waiver.
- The waiver renewal has added support broker and has additional waiver opportunities to help more people in the next couple years.
- The legislature has been more willing to listen to people and political direction may be changing.
- People have more hope of getting off the waiting list and receiving services.
Question: What are the barriers to achieving the waiver’s goals?
- More flexibility is needed to better customize services and supports. Self-direction needs to be enhanced so that participants are not stuck with provider-managed model of supports.
- State leadership has turned over with three directors in three years.
- Achieving greater uniformity in recipient experiences at the 11 regional centers.
- Continued high growth in people seeking services.
Question: Are there topics where there is disagreement or concern?
- There should be more residential choices and more done to promote community employment.
- More funding is needed to meet the demand for support waiver services.
- The current prior authorization method sometimes interferes with structuring services to meet participant needs.
- Community providers are at capacity in some areas of the state. There is a need for more behavioral support with increased funding to meet the needs of some individuals adequately.
Question: What are the TOP THREE things that could be done to improve the waiver?
- Expand use of the newly added support broker service. This new service offers the potential of creating a renaissance in support efforts in Missouri.
- Supported employment rates need to be increased.
- Add funds to reduce the CSW waiting list.
Question: What other points should be raised?
- Increased self-direction currently translates into more work for regional center staff. This may explain why relatively small numbers of families and individuals have used this feature.
- The natural support networks are as critical as anything.
Overall Impressions
All informants agree that the implementing the supports waiver has been a positive development in Missouri. The CSW has helped people stay at home and secure respite or other needed supports within the overall waiver cap.
A key change was shifting to an annual individual cap versus applying caps to each service. In addition, the state has means for managing extraordinary requests or “exceptions.” State staff feel that such flexibility is essential to the successful implementation of support waivers.
Many feel too that additional improvements are possible because as a result of changes that were made in the CSW renewal. The changes concerned quality management, increased consumer choice, possibilities for self-direction, and the new support broker services.
Informants, however, pointed out that there is still much to do. The state lacks sufficient infrastructure, including technology for managing information, to make the supports waiver work as well as it might.
OKLAHOMA
Introduction
Oklahoma presently operates two In-Home Supports Waivers, one for adults and one for children. These two support waivers are currently being used by over 1,800 children and adults (who use 76 percent of the support waiver capacity) in Oklahoma.
Method
In August, September and October 2006, HSRI talked with people within and outside the Oklahoma system. These included: (a) state staff associated with the Developmental Disabilities Services Division, including the state director and others; and (b) representatives from interests outside the state agency including the state association of providers, the Developmental Disabilities Council, and the Center for Leadership and Learning at the University of Oklahoma.
Results
The results of the key informant conversations follow. First, information is presented to describe the policy goals of the waivers, information on any service wait-lists, and the fundamental operations of the waivers. Second, opinions offered by the consultation participants are offered related to: (a) access to the waiver; (b) waiver operations such as budget allocations, service planning, service delivery, and safeguards; (c) outcomes; and (d) key issues in play.
Oklahoma Policy Goals
Question: What are the major policy goals of the supports waivers and how successful have the waivers been in meeting them?
- Cost containment and related budget goals were a major policy goal of both In-Home Supports waivers in Oklahoma. Since 1999, both waivers have applied caps in spending per person to contain costs make waiver services available to more people than the comprehensive waiver could accomplish alone.
- Reducing the wait-list was also a major policy goal. At one time the wait for enrollment in the state’s comprehensive services waiver had reached ten years, and the supports waiver presented significant opportunity to address this issue. The In-Home Supports Adult and Children Waivers help keep the number of people waiting and the length of time waiting much smaller than in the past. Presently, the current waiting for services is no longer than three years.
- Consumer-direction and person-centered planning goals are seen as less primary goals of the supports waiver. State officials note, however, that they will apply with CMS to change the supports waiver within the next 12 months during the renewal process with CMS to include self-direction opportunities to the waivers.
- Rebalancing the long-term care system and refinancing community services are not policy goals.
Wait-lists
Question: How many people are on the consolidated (i.e., all wait-lists for developmental disabilities services) wait-list?
- In recent years as much as 75 percent of new dollars for the In-Home Supports Waivers were used by existing service users for their plans.
- Wait-list figures are illustrated in the accompanying table:
| 2006 | 3,074 |
|---|---|
| 2005 | 3,853 |
| 2004 | 4,081 |
| 2003 | 3,494 |
Question: How are wait-lists maintained?
- Oklahoma maintains a statewide wait-list. Intake case managers maintain waiting lists and track the status of people who apply for waiver services but for whom slots are not available.
- The state observes a “woodwork effect” whereby when new funding dollars became available many new people who were not previously known seek waiver services. Referrals to other service systems to meet needs are often made.
Question: How long generally is the wait?
- Presently, the average time on the waiting or interest list before an individual is enrolled is more than two years but no one has been waiting for more than three years.
Basic Operations
Question: How are people selected for enrollment?
- People are selected for enrollment based on the order of requests for services, though emergency cases have priority. These emergency circumstances include people: (a) who no longer are able to care for themselves; or (b) individuals with caregivers who themselves are hospitalized, placed in nursing homes, permanently incapacitated or have died. Some individuals periodically utilize Family Support Subsidy state funds.
Question: Is there descriptive information available on the people served in the supports waiver (e.g., age, primary disability, living arrangement, functional status, caregivers)? Is systematic information available regarding waiver impacts?
- There is descriptive information concerning the supports waivers participants. Additionally, an annual report and related brochures broadly describe profiles of participants.
- Oklahoma conducts satisfaction analysis annually of the support waivers.
- There is systematic information available about the impact of the supports waiver on participant costs with some limitations.
- The state has the capability to sort results by waiver but it is currently difficult. The state is making needed changes to improve its capacity to sort information by waiver.
- The CMS reviews and Quality Assurance surveys are the current formal evaluations of the supports waiver.
Question: How are individual service plans developed?
- State case managers meet with the person and their family or representative/legal guardian to complete need assessments; identify supports needed and include others as-needed to develop plan individual service plans.
Question: How are individual allocations set?
- The full annual cap of $12,828 dollars a year for children and $19,225 for adults is available to the recipient as long as they stay at or under the cap. These caps are increased based on service rate increases. Increases in the cap are possible if circumstances warrant and justification is provided and accepted.
- The individual does have knowledge of the allocation before planning.
Question: What decision-making authority do individuals/families have over the budget?
- Individuals with disabilities and their families plan within a capitated dollar limit and determine services and supports needed.
Question: Who has primary responsibility for developing the service plan?
- State case managers.
- Among the service planners the average caseload is 29 individuals per service planner in a year.
- The case load range the average service planner during this period is from 14 to 55 individuals per planner.
- In Oklahoma people do not have paid outside assistance available to them during the planning process to help design the service plan?
Question: Does the service planning include a distinct risk assessment process to identify and address identified risk?
- Negotiated risk agreements are not used.
Question: Is the process the same or different from that used in the comprehensive waiver?
- The comprehensive waiver uses a more detailed Individual Planning process. In the supports waiver, family members are often relied on to lead the process and address various risk factors. As a result, the planning is generally not as detailed or intrusive as that required when traditional community services are used.
Question: What happens to individuals when they need more support than the waiver can offer, either by way of particular services and/or overall cost?
- Case managers identify other alternatives when available. If none are available or identified, exceptions to increasing the cap can be approved and entry to the comprehensive waiver can be offered when slots are available. So far Oklahoma has been able to accommodate individuals as-needed in its comprehensive waiver.
Question: What parameters govern transition from the supports waiver to the comprehensive waiver?
- People may move to the comprehensive waiver when their critical support needs no longer can be met with the supports waiver, non-waiver services, or other resources as determined by the Developmental Disability Services Division (DDSD) Director or designee and funding is available.
Question: What if the individual wants to change their service plan, or wants to change providers?
- The individual notifies his or her case manager that they wish to change, select a new provider, and set date for new provider to begin providing services. The case manager works through the required notifications and new authorizations.
Question: How is quality assurance and quality management managed?
- The Quality Assurance/Quality Management System for the supports waiver is the same as the comprehensive waiver.
- The principle features of the waiver’s quality assurance and quality management system include: (a) case management; (b) various surveys and reviews (i.e., consumer satisfaction surveys, provider performance surveys, critical incident reviews, medication event review, retrospective audit reviews); and (c) uses of oversight committees (i.e., statewide behavioral review committee, human rights committee, quality management committee).
- The state’s Office of Client Advocacy (OCA) approves community provider grievance policies and procedures.
Question: How are complaints resolved?
- Individuals may file complaints by pursuing:
- A Fair Hearing process to appeal a decision made by the Department. Complainants (and/or their representatives and witnesses) and Department representatives present their case. A Hearing Officer issues a written decision that can be appealed to the Director of Human Services, the Director’s written decision can be appealed in District Court.
- A grievance process through the OCA whereby local offices and providers retain “grievance coordinators” who assist recipients with the process. Complainants (and/or their representatives and witnesses) identifies their grievance and a proposed resolution. A local official responds to the grievance, this response can be appealed to the governing body, if not resolved there, the grievance moves to an independent administrative committee.
- An administrative inquiry that can be initiated by calling, writing, or emailing the state Quality Assurance office with a complaint related to provider performance. After receiving a complaint, this office completes an investigation and issues findings which may include provider citations.
Question: What is the process that is used to monitor the health and well-being of individuals participating in the supports waiver?
- The process includes a mix of preventative activities (i.e., provider training, provider background and abuse registry checks, pre-employment screenings), on-going monitoring (i.e., case management, provider monitoring, critical incident reporting), and look-behind review through consumer satisfaction surveys.
- Systematic monitoring of individual well-being is performed a minimum of every six months.
- When issues are uncovered, case managers are charged with following up and seeking resolution.
- A key difference the supports and comprehensive waiver is that the comprehensive waiver requires monthly face-to-face visits by case managers. For those in residential services, it also includes completion of the Physical Status Review (PSR) by the case manager and monitoring by DDSD registered nurses in accordance with the Health Care Level identified on the PSR.
Opinions on Waiver Operations and Effects
Access to the Waiver
Explanation: Access refers to how easily people can apply for and gain admission to the supports waiver.
- Some indicated that applicants and families must work hard to find out about services and that the new website is still difficult to navigate.
- Informants noted that the supports waiver is only “somewhat” publicized. Families learn about this supports waiver through brochures and word of mouth. In addition, applicants can learn about and apply for the program by contacting area office intake staff via telephone, mail, or through the Internet. Referrals may also come from staff of other service agencies, including from the statewide referral services, Outcome and Assessment Information Set.
- Informants indicated that it is neither “easy” nor “hard” to apply, and that individual experiences vary.
- Informants noted the demand for this waiver among people is increasing somewhat.
Service Planning
Explanation: Service planning refers to the process to develop individual support plans for waiver recipients.
- Overall, the planning process encourages individual to somewhat lead the planning process and somewhat define their own service needs. Families in some cases just need to be better informed and some say the state errs on the conservative side, so that participants do not always see the flexibility they seek in the program. Others note that the system is evolving and that in ten years that participants and families will be leading the planning process more.
- Overall, the planning process “Very Much” encourages individuals to choose the agencies or support givers to offer the needed support.
- Recipients do exercise choice and control over service plans, but may not have funds for all of the choices they make.
- Service planners “Somewhat” know the individuals they are planning for because of turnover in staff and case load variations.
- There is no supports broker or personal agent to assist individuals to put together the plan and/or negotiate services for the individual.
- It is very easy is it for clients to change their service plans. Informants note that it is a common occurrence.
- The strengths of the approach to individual planning are its ability to allow people to choose services and leave the waiting list.
Service Delivery and Safeguards
Explanation: Service delivery and safeguards refers to the services that individuals received and their operations, and the safeguards in place to assure health and well-being.
- Once services are authorized, it is neither “Easy” nor “Hard” for individuals to get these services. It can vary by location, given geographic differences, but generally the system responds well. For instance, some note that it can be difficult to get professional therapies in some communities.
- The services available through these waivers are generally broad enough to meet participant needs.
- Some informants feel that the release of “service authorization numbers” can be managed more promptly to reduce the time between authorization and actual service delivery.
- Informants note that it is “Very Easy” for individuals to change service providers. This generally takes a few days, up to 30 days.
- Waiver recipients cannot generally hire and manage their own support workers. Workers are typically employed by an agency. Recipients, however, often identify and refer potential workers to an agency and subsequently manage them day to day.
- There is “Some” emphasis on promoting community integration versus services that are more traditional (sheltered work, enclaves, segregated activities…). Many recipients, however, use segregated services.
- There is a pilot for a small group of 17 IHSW service recipients whereby they utilize a fiscal agent. Except for this pilot group, there is not a fiscal intermediary or payroll service available to help the individual control or manage the amount allocated for his or her services.
- To assure the health and well-being of participants, the safeguards in place are generally thought to be working well. Family members help assure the health and welfare of the waiver recipients.
- Where “in-home” supports are offered to adults living home with family, services are seen by the state as most often person directed. Others feel, however, that it depends on the individual and family and that it is instead often “family directed.”
Satisfaction with Outcomes
- Generally, many people report being satisfied with services and report being very happy.
- These waivers make services available that effectively support individuals to.
- Generally seek/acquire/hold integrated employment.
- Generally live with family, on their own or with friends.
- Generally participate in community events.
- It is thought that recipients are basically safe and there is a good fit of supports.
Key Issues in Play
Question: What are the waiver’s greatest strengths?
- To serve a large number of services recipients at a predictable cost.
- State leadership has been sustained and many believe that the state staff members are effective advocates. These circumstances have been an on-going strength of the system for the ten years.
- People have hope of getting off the waiting list and receiving services.
Question: What are the barriers to achieving the waiver’s goals?
- Workforce issues. Only one company was found who was willing to offer worker’s compensation to direct support workers involved with the supports waiver.
- Increased self-determination. Oklahomans believes in the power of local personal relationships, so many note that the supports waiver, which depends on such relationships, is a good fit for the state.
- People are being taken off the waiting list but the list continues.
Question: Are there topics where there is disagreement or concern?
- Some suggest that to save dollars support waiver recipients are being encouraged to room with other waiver recipients. Others argue that such practice is not state policy.
- One significant issue pertains to the amount of money service providers make and what amount they may retain as “profit.”
- Another issue pertains to the use of paid family members. To the extent they are paid, the pattern may limit other service choices the recipient would have had otherwise.
Question: What are the TOP THREE things that could be done to improve the waiver?
- Add a self-directed service option.
- Add funds to adjust allow greater flexibility within current service plans and to eliminate the waiting list.
- Some feel that the waiver is inadequate to provide even the most basic services and is sorely under funded. In short, they feel that it amounts to a “band aid on a very large wound” and argue that more resources are needed to add new recipients and expand the service array.
- Some feel that being tied to Medicaid providers and products that can be purchased through Medicaid adds to costs. They noted that sometimes particular products can be purchase elsewhere (i.e., “off the shelf”) from discount stores, for instance, at a lower price. They argue that such skill and independence should be promoted. For example, a young man in a rural part of the state should be allowed to use the affordable local gym and exercise plan and not be forced to take the limited services of a physical therapist who must travel hundreds of miles to serve him.
Question: What other points should be raised?
- Many participants want increased self-direction within the waiver. While a relatively new concept, Oklahoma has some experience with the concept through its family support system.
- There is a need for an effective advocacy group in Oklahoma. Such groups tend to form on an issue and then disappear. The Tulsa Arc has been long standing but some offered that there is really no enduring and effective statewide advocacy organization.
- Transit options are available in two larger cities, but a significant issue elsewhere.
- Adults who are out in the community have “come off the radar” and are difficult to anticipate and count.
- The state has every kind of employment setting and some feel that vocational rehabilitation is not an active enough player in promoting systems change and community employment.
Overall Impressions
Although the supports waiver is early in its development (with a successful CMS recent renewal), all agree that it generally has had a positive impact. The waiver has proven to be financially predictable and as an effective tool for addressing the wait-list. There is some disagreement, however, over the need for dollars to fund existing plans versus the need for dollars to reduce the wait-list further. The health and welfare of recipients has not been a problem due to strong family ties and family supports, and other mechanisms that the state has put into place. Most people agree though that more can be done to promote self-direction. In response, the State plans on adding “self-direction” options in July 2007.
One major expansion for 2008 or later from the principle target group (i.e., people with mental retardation) involves the addition of people with autism. The planned expansion would include family mentoring and behavior analysis, use of TEACH techniques, and other methods.
OREGON
Introduction
Oregon’s Supports Services for Adults Waiver (SSAW) was a direct outgrowth of the Staley et al. v. Kitzhaber lawsuit that was filed in January 2000. The Staley litigation was filed on behalf of over 5,000 people waiting for community services. The resulting settlement required that the state systematically address its waiting list. In doing so, the state proceeded in ways to promote self-direction, but also needed to work within a very difficult state budget climate. The SSAW was launched in July 2001.
Method
In August, September and October 2006, HSRI staff conducted face-to-face discussions with key informants on-site and follow-up conversations by telephone with additional informants. The individuals we spoke with included: (a) state staff associated with the Office of Developmental Disability Services Seniors and Persons with Disabilities (DDSPD), Oregon Department of Human Services including the state DDSPD director and others; and (b) representatives from interests outside the state agency including the Oregon Developmental Disabilities Council, the state provider association, experienced county program managers and managers of the support brokerages, and the Oregon Advocacy Center.
Results
The results of the discussions with key informants follow. First, information is presented to describe the policy goals of the waiver, information on any service wait-lists, and the fundamental operations of the waiver. Second, opinions offered by the consultation participants are related to: (a) access to the waiver; (b) waiver operations such as budget allocations, service planning, service delivery, and safeguards; (c) outcomes; and (d) key issues in play.
Oregon Policy Goals
Question: What are the major policy goals of the supports waivers and how successful have the waivers been in meeting them?
- Given the Staley court settlement, cost containment and budget goals were a major policy goal. This waiver survived the Oregon state budget crisis, though the settlement was modified. In particular, start-up actions were scheduled to end in 2007 but were put off to 2011 with a measured entry of 1,000 people per biennium.
- As part of the Staley litigation, the wait-list became a major focus of the supports waiver. Original goals, however, had to be modified due to the state budget crisis of the time, though the state is making steady progress on the wait-list.
- Consumer-direction and person-centered planning goals are cornerstones of the Oregon support waiver approach.
- Rebalancing the long-term care system and refinancing community services are not the primary policy goals associated with support services.
- The Staley settlement agreement in 2000 set the stage for the successful emergence of this supports waiver, and the success of the waiver appears to be ending the litigation.
Wait-lists
Question: How many people are on the consolidated (i.e., all wait-lists for developmental disabilities services) wait-list?
- The following table shows the number of people waiting for services from 2003-2006.
| Adult Services Year | Comprehensive Waiver | Support Waiver | Total |
|---|---|---|---|
| 2006 | 2,000 | 1,500 | 3,500 |
| 2005 | 2,000 | 1,500 | 3,500 |
| 2004 | 1,000 | 2,270 | 3,270 |
| 2003 | 1,300 | 1,000 | 2,300 |
Question: How are wait-lists maintained?
- The wait-list along with a great deal of other support waiver information is tracked by either the Community Developmental Disability Programs (CDDP), the support brokerages and state as part of the Staley settlement with careful periodic counts and Internet summary report postings. The wait-list has been monitored for years and is thought by most people that it will be eliminated as the roll-out of the settlement agreement is completed over the next several years.
Question: How long generally is the wait?
- Once the phase-in is completed in 2009, an eligible person requesting Support Services must be enrolled within 90 days. There will still be a wait-list for comprehensive services. Previously, there was a 20-year wait.
Basic Operations
Question: How are people selected for enrollment?
- Individuals apply for services through county offices.
- During the phase-in period of the waiver, Oregon uses a well-defined order of enrollment. First priority are those in “crisis”, with crisis defined as being at risk of civil commitment or at imminent risk of losing their homes. Next are a range of others including those with, aging caregivers, children transitioning from with existing support plans in programs such as family support, individuals “aging out” of educational system, and other wait-listed individuals. Enrollment is carefully analyzed to provide trend information as to the categories of individuals enrolling into support services. Waiting list rules are extensive and readily available.
Question: Is there descriptive information available on the people served in the supports waiver (e.g., age, primary disability, living arrangement, functional status, caregivers)? Is systematic information available regarding waiver impacts?
- Oregon conducts consumer satisfaction evaluations annually with all participants, includes questions regarding improvement in quality of life and identifies those improvements.
- The CMS reviews, consumer satisfaction surveys, and quality assurance surveys are the current formal evaluations of the supports waiver. The state relies on the involvement of parents and families.
- The state is also conducting reviews of the service brokerages in a manner that follows the CMS Quality Framework. Some brokerage directors, however, comment that some of the most innovative and imaginative support plans are not captured by the routine application of the framework.
- Oregon staff members indicate that they understand whether the waiver is effective especially in areas such as costs and reported satisfaction with services.
Question: How are individual service plans developed?
- County case management has a limited role. Counties perform eligibility reviews, approve the individual plan for Medicaid compliance, provide protective services, assist in crisis management, and bill under Medicaid administration.
- Oregon has established a network of independent “support service brokerages” throughout the state. Brokerages were selected by a competitive request for proposal process. Parents cannot be brokers to their own children.
- Support brokers called Personal Agents meet with individuals and their family or representative/legal guardian to develop a plan based on needs. The Personal Agent works with the individual to complete a customer goal survey. This survey guides the collection of information related to the individual’s available and needed supports as well as health and safety concerns in a variety of areas. Based on the customer goal survey a plan of support is developed.
Question: How are individual allocations set?
- Allocations per person are capped according to several benefit levels. The basic funding available to a Medicaid Waiver recipient is $9,600 per year. If the individual’s needs are significant, as measured by a standardized tool (Basic Supplement Criteria Inventory or BSCI), that amount my increase. A score of 60-80 on the BSCI allows access to $14,400 per year while a score of 81 or greater allows access to funding up to $19,999 annually for Medicaid waiver recipients. Non-Medicaid Waiver recipients receive a base benefit rate of $3,840 or $5,760 or $8,000 per year depending on the needs as assessed using the BSCI.
- Individuals, along with Personal Agents and members of the individual’s chosen circle of support identify supports needed and goals. They then develop an individual support plan (ISP) to address needs.
- Oregon has a 76 page handbook entitled Rate Setting and Purchase of Self Directed Support Services from State Licensed or Certified Providers Organizations that explains what can and cannot be purchased with support waiver funds. This guides the provider to reasonable and customary charges. This and the extensive, over 94 pages of rules that the state developed, have helped Oregon manage the Support Services for Adults.
- The State of Oregon has developed and made available a set of Expenditure Guidelines that explains to Personal Agents what can and cannot be purchased with support waiver funds. Additionally, a Rate Guidelines exists that sets reasonable and customary rates for services.
- Emergency crisis services are available and have in the current year been used more than anticipated.
- The individual has knowledge of the allocation BEFORE planning. The planning process is not geared towards spending the allocation, but rather identifies support needs first, then looks for ways to address those needs. Only when other options, particularly natural supports, cannot be found are support funds utilized.
- Individuals budget for an average of approximately $800 a month but have actually expended an average $630 a month. Consistently about 70-80 percent of the budgeted plan dollars are spent. For a number of years this has resulted in some dollars being returned to the state budget. Subsequently the state has changed its budgeting methodology to more closely align with the anticipated actual per person expenditure of plan costs.
Question: What decision-making authority do individuals/families have over the budget?
- Individuals can plan within the benefit level for which they are eligible and determine services and supports needed. Effort is made to change the commonly held perception that they “have a grant” and use the expenditure guidelines and training to assist individuals and families in making a problem solving ISP.
Question: Who has primary responsibility for developing the service plan?
- Personal agents have the primary responsibility for developing the service plan of care. This is a service as defined in the supports waiver. Currently there are 100 Personal Agents in Oregon employed by nine support brokerages.
- Personal Agents help set up the plan. CDDP case managers authorize the plan from a Medicaid perspective, but do not otherwise judge the ISP.
- Among the Personal Agents the average caseload is 40 individuals. It started at ten when the support waiver began and with current budget plans will end up at 45 individuals.
- The average case load range for a Personal Agent during this period is from 38-42 with a maximum average of 45 individuals per agent.
Question: Does the service planning include a distinct risk assessment process to identify and address identified risk?
- While there is not a formal risk assessment, the service planning includes elements of a distinct risk assessment process to identify and address identified risks.
- Negotiated risk agreements are not used.
Question: What happens to individuals when they need more support than the waiver can offer, either by way of particular services and/or overall cost?
- Brokers can look past “paid Medicaid” services and look out and connect people with other public or community resources.
- If the individual is in “crisis,” the brokerage and CDDP staff members work jointly to develop a plan.
- In Oregon people do not have paid outside assistance available to them during the planning process to help design the service plan.
Question: What parameters govern transition from the supports waiver to the comprehensive waiver?
- An individual may be disenrolled from the supports waiver if the individual: (a) is incarcerated for a defined period of time; (b) no longer has a disability; (c) is no longer financial eligible; (d) moves out of state; (e) no longer meets level of care; (f) is admitted to nursing facility or ICF/MR; (g) is no longer eligible for Medicaid; (h) refuses services; or (i) fails to cooperate with plan development. One emerging issue is recipients who engage in risky behavior or do not want to perform required planning activities. The technical bias of the support waiver is not to disenroll. However, not being eligible for the supports waiver does not exclude an individual from being eligible for supports services. The difference is the level of benefit the individual will be entitled to.
- Approximately 700 people have left the support service brokerages after initial enrollment. The following table suggests common reasons for termination including the top two reasons moving to the comprehensive waiver or moving out of state. As shown, 38 percent of individuals who leave the supports waiver are moved to the comprehensive waiver if no other intervention is sufficient. The percentage of individuals refusing services has decreased significantly from the first year of the services to the current year. Individuals are now given more information prior to enrolling in services.
| Termination Reasons | Percent |
|---|---|
| Refused services | 22% |
| No longer eligible | 4% |
| Moved from area | 22% |
| Moved to Comprehensive Waiver | 38% |
| Deceased | 10% |
| Legal Rep withdrew | 1% |
| Health/other issues | 0% |
| Other/unknown | 3% |
Question: What if the individual wants to change their service plan, or wants to change providers?
- The individual must contact their Personal Agent. Individuals can terminate arrangements at will. It is very easy for individuals to change service providers. The time it takes to do this varies.
Question: How is quality assurance and quality management managed?
- Personal Agents work with individuals and families to develop a plan of support where non-traditional workers may be hired. In such instances, brokerages follow the Internal Revenue Service rules and process to become the “employer agent”. Direct service workers are generally determined to be domestic workers, but also may be bona fide independent contractors or supplied by a licensed agency individuals and families can acquire information on this matter by visiting the following website: http://www.sdri-pdx.org/customers/index.html.
- Fiscal intermediary or payroll services are available to help individuals control or manage the amount allocated for his or her services.
- State officials argue that quality assurance is not just for individuals, but that it is important to build in safeguards to maintain cohesion in thought and action among various system players, offer supports to the brokerages, maintain vigilant oversight to assure that policies are appropriate and decisions are acceptable. Staff members find that operational policies tend to be narrow and that increased flexibility is needed over time.
- State staff conducts field reviews and file reviews to oversee individual circumstances.
- The state uses the components of the CMS quality framework as a reference to assess its various waivers.
- The Quality Assurance and Quality Management System for the supports waiver differs from the comprehensive waiver. In part due to the settlement agreement the SSAW routinely collects extensive information about recipient outcomes and group characteristics.
- The Staley Implementation Group has created a series of benchmarks to monitor services. Likewise, the state uses a series of personal indicators and support indicators covering 13 pages to see what is or is not working. The results have not been published yet as a statewide quality measure.
Question: How are complaints resolved?
- Individuals may file either an administrative complaint or a Medicaid Fair Hearing request.
- A Fair Hearings request is processed according to the rules of the Department of Human Services. There has been one hearing to date.
- An administrative complaint may also be filed locally with the relevant brokerage. Here, the grievant identifies their grievance and a proposed resolution. The matter is managed locally through a stated protocol within the brokerages. If not resolved at the brokerage level, the complaint may be forwarded to the CDDP level, and eventually the state level for resolution. Any corrections are carefully spelled out with detailed written specifications.
Question: What is the process that is used to monitor the health and well-being of individuals participating in the supports waiver?
- Personal Agents are active in pursuing health and welfare concerns and completing any necessary follow-up activities. Personal Agents may use a “well being assessment” to help understand the circumstances of the individual.
- Personal Agents contacts with individuals vary in frequency, based on the needs and desires of the individual. They review the support plan from a financial perspective quarterly to see if it is working however, these actions do not require a face to face contact.
- There is an adequate provider pool and over five years only three providers in Oregon have not continued support waiver services and two are not taking new support waiver recipients. However, concerns are being raised about the continuing adequacy of the provider pool, particularly as it relates to the current rate structure used within support services.
- Customer monitoring of quality can vary among brokerages and may involve personal agents’ use of periodic check-ins, satisfaction surveys or post cards, and use of “Quality Committees.” A Quality Committee is a group of recipients who meet to give feedback to the brokerage about how their supports are working and to suggest ways that their supports or the help they receive from their supports could be improved.
- A key difference between the supports waiver and comprehensive waiver is that the comprehensive waiver requires more intense monitoring by case managers.
Opinions on Waiver Operations and Effects
Access to the Waiver
Explanation: Access refers to how easily people can apply for and gain admission to the supports waiver.
- The potential enrollees and their families learn about the supports waiver with through the CDDP, printed matter, such as brochures, and related websites.
- In addition a 20 page publication, A Roadmap To Support Services, is available. This product, developed in cooperation by the Oregon Advocacy Center, the Oregon Council on Developmental Disabilities, and Oregon Department of Human Services, offers an understandable guide to the waiver. It is available in hard copy or by Internet http://www.ocdd.org/pdfs/Roadmap_2nd_edition.pdf.
- Respondents indicate that it is “Somewhat Easy” to apply and the demand for this waiver among people is increasing. People are referred to the support brokerage when they reach the top of the wait-list, based on their particular enrollment category.
Service Planning
Explanation: Service planning refers to the process to develop individual support plans for waiver recipients.
- Overall, respondents indicated that recipients “Very Much” lead the planning process and define their own service needs and, choose the agencies or support givers to offer the needed support
- Recipients do exercise a lot of choice and control over service plans, but may not have funds for all of the choices they make.
- Overall, respondents indicate that service planners generally “Know Well” the individuals they are planning for, though there are a few exceptions. Recipients may not always want to be known well. Assuring that planners know the people they are planning for is more of a challenge as case loads have grown.
- Overall, respondents indicate that the services available through this waiver are generally broad enough to meet participant needs.
- Respondents indicate that it is “Very Easy” for individuals to change their service plans. About 10 percent of costs change during the life of the ISP.
Service Delivery and Safeguards
Explanation: Service delivery and safeguards refers to the services that individuals received and their operations, and the safeguards in place to assure health and well-being.
- Once services are authorized, respondents indicate that it is “Somewhat Easy” for individuals to receive designated services.
- A protective service statute and mandatory reporting is part of the training for personal agents and it is working well.
Satisfaction with Outcomes
- Generally, respondents indicate that individuals do not seek, acquire or hold integrated employment but this is a currently a point of emphasis and promotion by the state.
- About 80 percent of support waiver recipients live with their families.
- Generally, respondents indicate that individuals do participate in community events.
- Respondents indicate that there is “Some” promotion in the waiver to promote community integration versus services that are more traditional (sheltered work, enclaves, segregated activities…) segregated services.
- Waiver recipients can generally hire and manage their own support workers. About half do.
- When “in-home” services are offered to adults living at home with family, the services are “Sometimes” family directed and “Sometimes” person-directed or both. This can be a point of friction.
Key Issues in Play
Question: What are the waiver’s greatest strengths?
- The waiver allows people to live at home with their families and to self-direct their services. Many supporters of the waiver characterize it as a “remarkable adventure.” Some feel that within Oregon the support waiver is will be seen in the future as an “entitlement.”
- Most agree that the self determination aspect of the support waiver is the “king of the world.”
- There is a feeling of shared success and ability to work through things with the state, support brokerages, advocacy community, and various stakeholder groups like the Staley Implementation Group. In general these parties speak well of each other and credit each other for the level of success Oregon has enjoyed. The support waiver roll-out survived the 2003 enrollment freeze.
- Most (71 percent) waiver recipients report they were “Happy” with the supports and services they receive. There is also an ease within families because someone else is involved in life event planning and in a supportive relationship with the recipient and family. Some report more frustration and dissatisfaction as they learn and become more informed overtime.
- The Oregon support waiver has numerous written products that are useful. For example, the 25 page Handling Emergencies: A Guide to Personal Safety & Emergency Management that came out in September 2006 is concise, understandable, and cogent. This is typical of 20 other written documents that have emerged within the Oregon support waiver.
Question: What are the barriers to achieving the waiver’s goals?
- Some see support waiver shortcomings as need for continued refinement in helping people throughout the state understand how they can better use the support waiver to make meaningful changes in their lives.
- There is a need to find “financial balance” between the comprehensive and supports waivers. The supports waiver has had the same fee structure since its beginning and it is not currently on the table for discussion. This threatens in several ways. For instance:
- The $37, five hour a day cap on day activities may limit future providers involvement. One provider, a college, has stopped enrolling waiver recipients and one community provider is talking with recipients to find ones that it is can afford to serve with that allotment.
- The ability of the system to maintain a skilled and dedicated set of personal agents and other service workers without cost of living and other adjustments through the years may result in an unavoidable loss of quality services. Due to lack of funds, Personal Agents are forced to balance between health and welfare and self determination.
Overall, the state is struggling with the cost of growing numbers of crisis cases and the culmination of the roll-out of the Staley settlement with only the planned appropriations.
- Some say that the state has insufficient resources for overseeing the entire waiver system. They argue that the supports waiver has gotten a lot of focus, but challenges also exist regarding operations of the comprehensive waiver as well.
- Due to diminishing resources and the lack of cost-of-living adjustments over the past several years, the providers are struggling to maintain quality staff and facilities. Employee turnover runs at above 60 percent and providers complain about a lack of qualified applicants. Providers suggest that Oregon must significantly increase support of community providers or many will collapse. If the community system fails, in part or completely, the state will be forced to find alternatives that are either substantially more expensive, or poorer quality, or both. The Oregon Developmental Disabilities Coalition supports the DHS Policy Option Package that would increase funding to the system by $63 million.
- Issues have been raised pertaining to direct support workers that individuals hire outside the traditional provider network. Issues pertaining to “employer liability” regarding these workers linger. These workers typically are not offered worker’s compensation or other benefits. Oregon has had litigation where the support brokerage was determined not to be the actual employer. One practical part of this challenge is in rural areas where over half of the support workers are family and 80 percent are direct service workers not employed by an agency. Oregon is unusual because direct support workers serving seniors and people with physical disabilities became unionized and acquired worker’s compensation and other benefits as a result. There is now a Home Care Commission, but the workers are not state employees, but as a result of a recent state initiative passed by the voters were allowed to unionized and bargain. This resulted in a large increase in worker’s compensation claims. Most feel that this employer liability is an Achilles’ heel of this type of waiver that could bankrupt support brokerages or result in successful litigation against the state.
- Some observe that operations involved with the supports waiver are much more involved, difficult, and risky than was commonly believed at the beginning. The need for a fiscal intermediary, for example, created a common understanding about certain forms of “risk” and the need to manage it.
- Most feel that the personal agent relationship is a pivotal piece of the support waiver and their skill, ability, reimbursement, and training will be critical to the continued success of the support waiver.
Question: Are there topics where there is disagreement or concern?
- One issue of tension involves the capacity of providers to request payment, even when circumstances result in a service not being delivered. This issue arises when an individual agrees to receive services but for whatever reason fails to show. The provider, as a result, may be left with expenses but having failed to deliver the service, cannot seek reimbursement. The state took a strong stand to refuse payment in circumstances like these. Providers objected, arguing that they could not bear the loss of such revenue. State officials, while pressing providers to factor in such occasional losses within their overall business plans are relying on intelligent and cooperative problem solving to resolve the issue. The system, however, is already stretched fiscally and the solution may simply require more money.
- Personal Agents wrestle with growing caseloads and extensive paperwork. One recent survey suggests that half of personal agent’s time is now engaged in necessary paperwork.
- The real challenge of changing service plans often rests with the need for CDDP reauthorization. Not all CDDP’s are county based; some are independent of the local county. Personal Agents are skillful at making needed changes without triggering a cumbersome reauthorization process.
- Reconciling the time sheets of direct support workers can pose a significant difficulty for fiscal intermediaries. Some report that the fiscal agent duties are costing them more than they are paid. Some report the duties are a helpful part of the overall support waiver economics.
- Individuals who are waiver recipients sometimes live “risky” lifestyles. Brokers are taught not to ignore these but assuring the health and well-being of such individuals is sometimes much more difficult.
Question: What are the TOP THREE things that could be done to improve the waiver?
- More funding is needed to improve training, raise service rates of pay, and provide additional needed services.
- Increase the flexibility in the services that can be purchased. The supports waiver sometimes lacks flexibility and injecting more flex would not always cost more. Some feel that state monies are necessary to pay for services that Medicaid cannot fund but would make a lot of sense in individual cases.
- More training for people and families to advocate for themselves.
- More structure, training, benefits for workers on supports waiver with more agency backup.
- Better training for personal agents about services in general and the many pieces they work with including services in general, food stamps, social security, mental health care, and alcohol and drug treatment.
- Some voices feel that the initial roll-out could have been more ambitious. More could have been done to identify millions of dollars were not used in support plans and returned to the state general funds. The state has not allowed any back fill for the vacancies that have developed. Others believe that the state has made “frugality” a cherished alter goal for the support waiver at the cost of forward movement.
- Many respondents felt that the Oregon state staff worked hard with others in the state to fashion a supports waiver that is well thought out and has many superior features. Respondents also indicated that they had learned much about its operations over the past few years and have made adjustments along the way. Participants expressed willingness to describe their system to others elsewhere and share their experiences.
Question: What other points should be raised?
- All informants argued that there is a great need to promote supported employment. The state launched a website promoting supported employment to illustrate successful employees (See http://www.dhs.state.or.us/dd/supp_emp/). Some note that Vocational Rehabilitation staff should move more quickly to identify when it can do no more, and allow the individual to move into the supports waiver instead of offering services at a “a glacial rate.”
- Oregon has diverse geographic areas. For example, one support brokerage covers 13 counties in Eastern Oregon and serves a geographic area greater than the rest of the brokerages combined. In rural parts of the state travel time can provide an economic challenge. Towns vary enormously on how much transportation is possible and available. Almost always recipients move to larger towns to get the supports and help they need, especially if they have mobility impairments.
- Some say that participants are not getting sufficient training, support and education so they can “play” a true self-directed role in their services.
- One dilemma for direct service staff members who are employed as “domestic workers” is that they are not paid for training time and can only be paid for direct face to face recipient services.
- One development worth noting is the emergence of “affiliated apartments” where parents may assist their son or daughter to move in with others who are receiving supports waiver services. Three of these apartments existed three years ago, and at least five more are in planning. These sites can be, unintended, almost facility like because of the high concentration of waiver recipients in one area.
- Overall there are nine brokerages. There are seven support waiver brokerages that are stand-alone and non profits. While most are strong, one has struggled with providing progress reports in a timely way. Brokerage capacity can be expanded through a request for proposal process.
- Five years of policy work by the state continues to be revisited and sometimes old decisions are changed. Generally the state receives high marks for its forethought. Some decisions, usually revolving around funding limitations, are seen by some as being too directed.
Overall Impressions
The Oregon SSAW has increased in enrollment to ten times what it was when it began five years ago. It has served as an effective means for addressing the wait-list and to do so cost effectively. More than that, however, it has provided systematic means for the state to advance policy goals tied to self-direction.
The waiver was built on a commitment to self-direction and has steadily evolved to improve its associated policies, procedures, and operations. The state has identified and kept to seven core functions of self-direction, including: (a) assisting customers to determine their needs and plan supports; (b) assisting customers to find and arrange resources and supports; (c) providing education and technical assistance for customers; (d) providing fiscal intermediary services; (e) providing customer employment administrative support; (f) facilitating community building; and (g) assuring customer monitoring of quality.
With time, systems have been put into place to translate these functions into actual policy and practice. All agree, however, that in the doing that new, often unexpected, difficulties have emerged that press the system to redefine itself continually and reshape itself. State leaders and others often must challenge themselves to revisit and change standing policies. Other difficulties remain in play and defy easy solution. Issues pertaining to the workforce, for instance are not easily resolved. Likewise, assuring quality within a system that promotes diversification and self-direction is a challenging task.
Still, the Support Services for Adults Waiver has proven itself with most stakeholders and leaders in Oregon. It faces all of the challenges faced by the other support waivers around the nation and is threatened most by the future availability of necessary funding.
PENNSYLVANIA
Introduction
The Pennsylvania Person and Family Direct Support (PFDS) Waiver was launched in July 1999 to provide services that enable people with I&DD to continue living in their own homes or with their families. This waiver was developed in great part as a response to the state’s waiting list. By the end of the current state FY, overall, the children and adults on the PFDS Waiver total of 7,930 are expected to be enrolled in the PFDS Waiver and another 15,340 in the comprehensive Consolidated Waiver.
Method
In August and September 2006, HSRI talked with key Pennsylvania informants to obtain more in-depth information concerning the PFDS Waiver. Informants included: (a) state staff in the Office of Mental Retardation (OMR), including the Deputy Secretary for Mental Retardation and others; and (b) representatives from interests outside the state agency including the Developmental Disability Planning Council, Temple University, the Training Partnership that works extensively with individuals receiving waiver services and their families in a statewide coalition, and Pennsylvania Protection and Advocacy.
Results
The results of the key informant conversations follow. First, information is presented to describe the policy goals of the waiver, information on any service wait-lists, and the fundamental operations of the waiver. Second, informant view are summarized concerning: (a) access to the waiver; (b) waiver operations such as budget allocations, service planning, service delivery, and safeguards; (c) outcomes; and (d) key issues in play.
Pennsylvania Policy Goals
Question: What are the major policy goals of the supports waivers and how successful have the waivers been in meeting them?
- While important, cost containment and budget goals are currently not the most emphasized goals. Since 1999, individual allocations within the PFDS Waiver have been capped, allowing the state to work towards its budget goals. Note that the cap was raised from $22,083 for FY 2005/2006 to $22,525 for FY 2006/2007.
- In 2006 the statewide mental retardation waiting list reached 24,927 people. People observe that use of a cap within the PFDS Waiver has helped the state to serve more people than could have been served with only the Consolidated Waiver.
- State officials would like to accommodate all “emergency cases” identified within the wait-list but realize that such action will require additional funds. There is widespread agreement that the waiting list remains a major concern.
- State officials are striving to promote “consumer-direction” through both waivers. The intent is to work out various operational issues pertaining to self-direction involving how to set individual budgets, service planning, budget authority, and quality assurance.
- Rebalancing the long-term care system and refinancing community services are not primary policy goals. Overall 80 percent of services are financed through the waiver with the remainder paid for by county or state dollars.
- The state has two other goals which are both aimed at the use of more integrated settings. For example, state officials want to increase community employment, moving from sheltered work experiences to supported employment opportunities.
Wait-lists
Question: How many people are on the consolidated (i.e., all wait-lists for developmental disabilities services) wait-list?
- OMR uses the Prioritization of Urgency of Need for Services (PUNS) system to track wait-lists. In 2003, OMR began to collect PUNS information electronically; therefore the 2003 data may not accurately depict a full year of waiting list information. In addition, the PUNS form was revised in early 2006, which may have also affected the data. For these reasons, it is difficult to compare waiting list data across years. These limitations aside, this information tracking system allows the state to detect increased demand for its community waiver services over time.
| Year | Emergency | Critical | Planning | Total |
|---|---|---|---|---|
| 2006 | 3,274 | 9,999 | 11,654 | 24,927 |
| 2005 | 2,231 | 8,365 | 10,626 | 21,222 |
| 2004 | 1,920 | 7,463 | 10,181 | 19,564 |
| 2003 | 1,537 | 5,826 | 5,240 | 12,603 |
Question: How are wait-lists maintained?
- Local supports coordinators complete the PUNS with the individual and family and counties use the PUNS data for budgeting and planning. The state uses the PUNS system to maintain a comprehensive waiting list using its three categories of need.
- The emergency category indicates a need within the next six months.
- The critical category indicates a need in more than six months, but less than two years.
- The planning category indicates a need in more than two but less than five years.
Question: How long generally is the wait?
- The average length of time for those in the emergency category alone is a year (369 days).
- The average time on the planning list before an individual is enrolled is 643 days. This includes people who seeking services at a future date, such as upon transition out of the special education system.
- People are selected for enrollment based on the categories of need, generally with emergency cases being chosen first.
Basic Operations
Note that OMR expects to apply to CMS to alter certain features of the PFDS Waiver within the next 12 months during the waiver renewal process. Currently Pennsylvania is moving away from program funding to fee-for-service payments. OMR is establishing new requirements on county administrative entities to increase waiver recipient control, choice, and to create more consistent waiver experiences for recipients across the state.
Question: Is there descriptive information available on the people served in the supports waiver (e.g., age, primary disability, living arrangement, functional status, caregivers)? Is systematic information available regarding waiver impacts?
- Individuals are generally described as younger and living on their own or at home with their families.
- More descriptive information is available in the state’s Home and Community Services Information System to describe individual characteristics such as age, primary and secondary disability and living arrangement, though state officials plan to improve the available information.
- Systematic information about the impact of the supports waiver on participant costs is available with some limitations. Additionally, Pennsylvania conducts consumer satisfaction Interviews through an independent monitoring process. The process involves interviews with a sample of individual receiving services and their family and friends.
- The CMS reviews, quality assurance surveys, and the evaluation and monitoring of counties by the OMR provide formal evaluations of the PFDS Waiver.
Question: How are individual service plans developed?
- Local supports coordinators meet with the person and their family or representative/legal guardian to complete a needs assessment. Subsequently, an ISP is developed to address the identified needs.
Question: How are individual allocations set?
- Needs assessment is conducted every year as part of the planning process. Currently, there is not a consistent statewide needs assessment; however, OMR will begin implementing the Supports Intensity Scale as the standardized needs assessment tool starting in September 2007. The needs assessment results in the identification of support needs that are used by the planning team to develop an ISP. The ISP includes services and supports (including service units) to address the assessed needs. The individual budget is established after the planning process, based on the needed waiver services included in the plan.
Question: What decision-making authority do individuals/families have over the budget?
- OMR has instructed County Programs to provide participants with their individual budget upon request. Yet, informants note that some counties do not consistently follow this policy. State officials plan to develop and implement a more systematic protocol for setting individual budgets.
Question: Who has primary responsibility for developing the service plan?
- Local supports coordinators develop ISPs through a person-centered planning process.
- Among the supports coordinators, the average caseload is 50 individuals.
- The support coordinator caseloads presently range from 14 to 55 individuals.
- Participants may access personal support services to assist in developing the service plan.
Question: Does the service planning include a distinct risk assessment process to identify and address identified risk?
- ISPs are developed using a standardized format, which includes components related to risk, which are discussed during the planning process. However, the planning process does not include a distinct risk assessment protocol. Negotiated risk agreements are not used. OMR is in the early stages of developing a distinct risk assessment tool for use in planning.
- OMR utilizes additional mechanisms to identify and remediate risk. First, the statewide incident reporting system and policies generate standardized incident reports, which are reviewed by counties and OMR Regional Offices. The individual and systemic review of incident reports can result in the identification of risk issues, as well as opportunities for improvement. In addition, OMR relies on inspections of licensed providers to reveal potential risk issues. Any identified issues are relayed to the provider, and are addressed through provider plans of correction. OMR reviews incident, licensing and other information as part of its Regional Risk Management teams, and reports findings to the appropriate provider and county.
- OMR expects providers and counties to conduct analysis of their risk management and review procedures. Generally, OMR believes that risk management is working well.
Question: Is the process the same or different from that used in the comprehensive waiver?
- The process is the same as that used in the Consolidated Waiver.
Question: What happens to individuals when they need more support than the waiver can offer, either by way of particular services and/or overall cost?
- Supports coordinators review other options that can be used, such as the community’s natural supports or additional assistance using state dollars. State officials incorporate the potential for such cases within its budgeting process and transfer individuals into the Consolidated Waiver as necessary.
Question: How might a person be disenrolled from the supports waiver?
- An individual may be disenrolled from the PFDS Waiver when the individual: (a) requests such action; (b) is incarcerated; (c) no longer has a disability; (d) is no longer financial eligible; (e) moves out of state; (f) no longer meets level of care; (g) is admitted to nursing facility or ICF/MR; (h) is no longer eligible for Medicaid; (i) refuses services; or (j) fails to cooperate with waiver requirements.
Question: What if the individual wants to change their service plan, or wants to change providers?
- The individual notifies his or her supports coordinator when they need to change their plan or wish to change providers. The individual then selects a new provider and a date is established for the new provider to begin providing services. The supports coordinator works through the required notifications and new authorizations.
Question: How is quality assurance and quality management managed?
- The system used is the same as the Consolidated Waiver.
- Principle features include standardized monitoring forms used by support coordinators, independent monitoring teams, and on-going evaluation by OMR of local administrative entities that, with one exception, are counties.
- A strong feature of both waivers is the use of health care quality units and the use of certified investigators to investigate certain types of incidents at the state, county, and provider levels.
- The state participates in the National Core Indicators project that tracks approximately 100 consumer, family, systemic, cost, and health and safety outcomes -- outcomes that are important to understanding the overall health of public mental retardation agencies.
- The state will be stepping up oversight of ISPs and its oversight of administrative entities.
- One challenge for the implementation of standardized supports coordination monitoring is increasingly large caseloads that sometimes make the monitoring role difficult for the supports coordinators to fulfill.
Question: How are complaints resolved?
- Informal complaints can be made to OMR at its toll-free customer service number, or to the OMR Regional Offices. Informal complaints are also made directly to supports coordinators, supports coordination entities, counties, and providers.
- Many complaints come from people on the wait-list who want to acquire waiver services sooner.
- The formal complaint process (fair hearing and appeal) takes time and the state asks people to submit their request within ten days. Participants, however, have 30 days to appeal a decision. There are specified time lines and checks in the process that begin at the county level and move to the state level. It is felt by some that complaint handling has improved.
- OMR conducts a Service Review of certain waiver appeals for the purpose of evaluating county compliance with applicable policies and requirements. The Service Review results in state findings, which are distributed to the individual/family, the county, and the Department of Public Welfare’s (DPW’s) Bureau of Hearing and Appeals. Upon receipt of the Service Review findings, the individual/family can choose to continue on to fair hearing or withdraw their appeal.
- Some feel that the Fair Hearing process option is not always accessible for individuals and tends to be highly technical with hearing officers who are not versed in the rights and protections intended in the waivers. OMR is planning training for hearing officers in an effort to alleviate some of these issues.
Question: What is the process that is used to monitor the health and well-being of individuals participating in the supports waiver?
- The process includes mix of preventative activities (i.e., provider training, provider background and abuse registry checks, pre-employment screenings), on-going monitoring (i.e., supports coordination, local provider monitoring, and consumer satisfaction interviews).
- A key difference between the PFDS and Consolidated waivers is that the Consolidated Waiver requires more frequent face-to-face visiting.
- The Consolidated Waiver requires three face-to-face visits each quarter with one at the waiver participant’s residence, one at the waiver participant’s day service, and one at any place agreeable to the waiver participant.
- The PFDS Waiver requires face-to-face monitoring at least every six months with contact every three months for people living with a family member. The minimum frequency is increased for people living in their own homes, Personal Care Homes, or Domiciliary Care Homes to face-to-face monitoring at least every three months and contact at least once a month.
- Supports coordinators, and their supervisors, follow-up on issues to resolve them when monitoring reveals problems.
Opinions on Waiver Operations and Effects
Access to the Waiver
Explanation: Access refers to how easily people can apply for and gain admission to the supports waiver.
- Potential enrollees can learn about the PFDS Waiver in a wide variety of ways including: searching the blue pages in the phone book, local county assistance offices, informational fliers, and extensive statewide family training. Information is also presented by way of a 24 page guide to waiver services and through the DPW website. Local intake staff members also describe the services available and other sources, including educators in the school system, often make referrals.
- Informants note that the PFDS Waiver is “Somewhat” publicized and is well known within the system. Individuals apply for the program through contacting the local county assistance office, using the telephone, using the mail, or through the Internet.
- Informants note that it is “Somewhat Easy” to apply and that demand for this waiver among people is increasing “Somewhat.”
Service Planning
Explanation: Service planning refers to the process to develop individual support plans for waiver recipients.
- Overall, respondents indicated that recipients “Very Much” lead the planning process, but “Somewhat” define their own service needs. OMR is firmly committed to the person-centered approach and uses a standardized format to develop the plan, which is entered into the state information system.
- Overall, respondents indicated that recipients “Somewhat” choose agencies or support givers to offer the needed support.
- Overall, respondents indicated that individuals exercise “Some” choice and control over support plans, but it depends a lot on the people involved. People can hire their own staff and act as “employer of record” (through Vendor Fiscal Intermediary Service Organizations (ISOs)) or hire an agency to manage this function (through Agency with Choice ISOs).
- Overall, respondents indicated that supports coordinators “Somewhat” know the individuals they are planning for because of high turnover and high caseloads. The state is increasingly professionalizing the role of supports coordinators and is in the process of developing a supports coordinator curriculum and increased credentialing.
- Individuals may access personal support services to assist them in putting together their plan and/or negotiating services.
- Informants indicate that the services available through these waivers are generally broad enough to meet participant needs.
- Overall, respondents indicated that it is neither “Easy” nor “Hard” for recipients to change their support plans because they can begin the process to change with a simple telephone call to their supports coordinator. However, the approval process can be cumbersome and it can take 30-60 days to make changes. There is currently an OMR-led work group that is currently working on improving this process.
- Statewide consistency regarding application of the PFDS Waiver has been an issue. Protocols pertaining to wait-list management, training, and plan formation have been or are being, standardized. Efforts are being made to increase the expectations of county performance and measure quality around the state in systematic ways.
Service Delivery and Safeguards
Explanation: Service delivery and safeguards refers to the services that individuals received and their operations, and the safeguards in place to assure health and well-being.
- Informants indicate that once services are authorized, it is “Very Easy” for individuals to receive services with only a few exceptions. Once the approval process has been completed the only problem that emerges are the few times that agencies have been unable to hire or maintain staff.
- Informants indicate that services to promote community integration are emphasized over services that are more traditional (e.g., sheltered work, enclaves, segregated activities).
- Informants indicate that it is “Somewhat Easy” for individuals to change service providers and this generally takes weeks to months.
- Waiver recipients can hire and manage their own qualified support workers through vendor fiscal ISOs or with an agency with choice ISO serving as the “the employer of record.” Sometimes recipients choose an agency to hire and manage support workers. These options are being utilized a small percentage of the time but OMR expects the use of this option to grow.
- “In-home” supports utilized by adults living at home with family are most often family directed but sometimes are person-directed or both.
- Workforce issues related to liability have not been a concern to date.
- Informants generally indicate that the safeguards in place are working well. The active participation of families in the PFDS Waiver is helpful.
Satisfaction with Outcomes
- Generally, informants indicate that the PFDS Waiver encourages people to seek, acquire and hold integrated employment. There are two relevant services, job support and job finding, and OMR encourages people to utilize these services more. Across all of its mental retardation county services in January 2006 there were 2,366 people competitively employed, 2,768 employed through supported employment, and 7,565 in vocational programs. Others feel, however, that there is little opportunity for employment.
- OMR indicates that generally people live on their own or with friends. Some feel, however, that people do not live on their own or with friends often enough. There is shared agreement that people in the PFDS Waiver participate in community events.
Key Issues in Play
Question: What are the waiver’s greatest strengths?
- A major strength of the PFDS Waiver is its demonstrated ability to serve a large number of services recipients at a lower-cost.
- There is widespread agreement that the PFDS Waiver has been effective at addressing the wait-list.
- There is common agreement that the statewide training efforts are first rate with support from the highest levels. There are at least three highlights to this statewide training.
- The “Partnership” is a coalition of five self-advocacy and family groups and Temple University’s Institute on Disabilities that has provided 250 training sessions in the last three years to over 5,000 people in each of the 67 counties throughout the state. This million dollar effort has led to a survey of topics that people have felt were needed and the formation of a series of two hour power points that are used by a train the trainer model to share with families and individuals across Pennsylvania. The curriculum currently includes eight topics for self advocates and seven topics for families and is also available to professionals.
- The College of Direct Support, available by Internet has attracted over 17,000 learners in the past four years. One new learning group that has appeared recently is comprised of direct support workers who provide PFDS Waiver services.
- The “OMR Academy for Administrative Entities” is managed by OMR and reaches County Programs/administrative entities to share information and standardize processes.
- There is agreement that the PFDS Waiver should increasingly emphasize integrated employment.
- The incident reporting system and self-advocacy efforts are commonly viewed by many as strong and a positive parts of the service system.
- The increasing emphasis of the PFDS Waiver on individuals directing their own services is considered by many as a strength.
Question: What are the barriers to achieving the waiver’s goals?
- The absence of sufficient funding inhibits efforts to increase access to the PFDS Waiver.
- There is a lack of consistency with PFDS Waiver policy and its application across the state that needs to be overcome.
- Some note that there are some unreported cases of abuse of waiver recipients who are minors. The reliance within the PFDS Waiver on families may leave individuals vulnerable to such abuse.
Question: Are there topics where there is disagreement or concern?
- One issue is how much control families and individuals have and how much is retained by counties and providers.
- There is no adult protective service system currently in the Commonwealth of Pennsylvania for people age 18-59. There is proposed legislation to add this protection and all agree that is creates undesirable risks for many individuals in the state as well as, unfortunately, some PFDS Waiver participants.
- One challenge that is frequently mentioned is keeping the PFDS Waiver “theory real in practice” across the state.
- Some feel that, to this day, the counties control the supports coordinators who in turn control the support planning and this leaves the waiver recipient faced with a county that essentially needs to balance its budget.
Question: What are the TOP THREE things that could be done to improve the waiver?
- OMR should move decisively to assure consistency in the application of waiver policies throughout the state.
- Pennsylvania is also eager to clarify policies and its expectations pertaining to self-direction, including issues associated with setting individual budgets and potential tensions over whether services are actually individual or family directed.
- There is a statewide push to standardize quality management across the state. In revamping quality management, OMR is stressing communicating better with stakeholders while it designs the final structure and identifies priorities.
Question: What other points should be raised?
- In Pennsylvania there is a constant tension between the need to address a large standing waiting list and improving service delivery.
- There is a need to improve information management systems to keep pace with changes in service design and delivery.
Overall Impressions
All informants agreed that the PFDS Waiver has helped people gain access to supports and move off the waiting list. There is also widespread agreement that the statewide training efforts that support individuals and families involved in the supports waiver are top notch. Meanwhile, OMR is working to achieve more consistency in the application of its waiver policies across the state. Overall, the PFDS Waiver is one of the tools that Pennsylvania uses to address its waiting list and contain costs. Added to that it seeks to explore and establish consistent practices that, from the onset of enrollment on, promote self-direction and community integration.
TENNESSEE
Introduction
The Tennessee Self-Determination Waiver Program (SDWP) is designed for children and adults with I&DD and was launched in 2005. Its major aim is to address the wait-list, but gives priority according to urgency of need. First priority for enrollment is afforded persons in the “crisis,” then with an “urgent” need, and finally to those categorized as “active.” Potential enrollees must have a non-institutional place of residence where they live with their families, non-related caregiver or in their own home, and have needs that can be met effectively by the combination of waiver services and other available supports. Presently, the SDWP waiver serves 800 participants, while the state’s comprehensive waiver serves 6,000 individuals.
Method
In August and September 2006, HSRI talked with key informants in Tennessee to obtain more in-depth information concerning the SDWP. Informants included: (a) state staff with the Division of Mental Retardation Services (DMRS), including the state director, manager, and others; and (b) representatives from interests outside the state agency, including representatives of the state Protection and Advocacy Agency and families.
Results
The results of the key informant consultations follow. First, information is presented to describe the policy goals of the waiver, information on service wait-lists, and the fundamental waiver operations. Second, the views expressed by the informants are summarized with respect to: (a) access to the waiver; (b) waiver operations, service planning, service delivery and safeguards; (c) outcomes; and (d) key issues in play.
Tennessee Policy Goals
Question: What are the major policy goals of the supports waivers and how successful have the waivers been in meeting them?
- There is strong agreement that cost containment was a major policy goal in launching SDWP. CMS had identified several major shortcomings with the state’s comprehensive waiver (i.e., Statewide Mental Retardation Waiver Program). CMS limited new waiver enrollment to individuals in crisis until those problems were resolved. In January 2005, CMS approved a replacement comprehensive waiver and the SDWP and subsequently approved the resumption of waiver enrollments in March 2005. Since then, the SDWP has offered means for children and adults to receive waiver services in a more cost efficient way than through use of the comprehensive waiver alone.
- The SDWP waiver is viewed by all as cost effective and people generally report being satisfied with their waiver services.
- Tennessee also views the SDWP as a useful means for addressing its waiting list. Presently, 4,761 people are waiting services and state officials expect the demand for services to continue to scale up.
- While the SDWP waiver provides for consumer-direction, there has been limited implementation thus far.
- Rebalancing the long-term care system and refinancing community services were not major policy goals in launching SDWP.
- The SDWP was a direct outgrowth of the 2004 Brown vs. Tennessee Department of Finance and Administration waiting list lawsuit settlement agreement. The settlement provided for Tennessee to create a new waiver that specifically targeted children and adults with I&DD who were wait-listed for services and could be supported in the family home or other non-licensed living arrangements. SDWP waiver enrollment is expected to reach 1,500 persons in its third year.
Wait-lists
Question: How many people are on the consolidated (i.e., all wait-lists for developmental disabilities services) wait-list?
- The accompanying table shows the number of children and adults on the consolidated wait-list. Overall, about 1,000 individuals on the waiting list are inactive. The remainder includes 818 applicants in the “crisis” category and 422 who have “urgent” needs.
| 2006 | 4,761 |
|---|---|
| 2005 | 4,046 |
| 2004 | 3,660 |
| 2003 | 3,663 |
- The waiting list has grown by 1,300 people since the settlement but 1,900 people have been enrolled in the state waiver programs. People First of Tennessee has made the waiting list reduction its primary goal.
- Many, 43 percent now and 46 percent six years ago, of new waiver recipients come from school referrals. However, there are potentially 2,000 new children each year that are possible support waiver referrals and their presence is understated on the current waiting list.
Question: How are wait-lists maintained?
- State case managers maintain waiting lists and track the status of people who are seeking enrollment but for whom slots are not available by using a priority system that accommodates emergency cases first. There is a process enrollment committee that selects the absolutely most critical cases from the state’s regions.
Question: How long generally is the wait?
- People in the “crisis category” can wait over one year and the wait for some can last up to 13 years.
- In the last several months there have been 10-15 people enrolled into the waiver a month, but given the resources available and the expected demand, the waiting list may reach 12,000-15,000.
Basic Operations
Question: How are people selected for enrollment?
- Applicants are selected by the eight person process enrollment committee.
Question: Is there descriptive information available on the people served in the supports waiver (e.g., age, primary disability, living arrangement, functional status, caregivers)? Is systematic information available regarding waiver impacts?
- The state does not have a systemized electronic data retrieval system for this purpose. The annual report and brochures broadly defines profiles of those served in the supports waiver. Some descriptive information to profile SDWP participants is available, however, resulting from various quality management activities. Such information is compiled on spread sheets, but is not easily available.
- Some information on the impact of the supports waiver on participant costs is available with limitations. The state has the capability to sort information by waiver, but these processes are new. The state is making needed changes to build better databases but there is still more work to be done. Informally, there are growing numbers of success stories from support waiver recipients.
- The CMS reviews and state administered quality assurance surveys are the current formal evaluations of the supports waiver.
Question: How are individual service plans developed?
- State case managers meet with individual recipients and their family or representative/legal guardian to complete individual service plans.
Question: How are individual allocations set?
- The full cap of $30,000 for service components is available to the recipient as long as they stay at or under the cap. Increases in the cap are possible if circumstances warrant and justification is provided and accepted. The total budget for all waiver services, including emergency assistance services, may not exceed $36,000 per year per participant.
- Individuals have knowledge of the allocation before planning.
Question: What decision-making authority do individuals/families have over the budget?
- They can plan within the funding limit and determine services and supports needed. The general allocation process has category limits but these can be worked around when necessary.
- There is a fiscal intermediary or payroll service available to help the individual control or manage the amount allocated for his or her services.
Question: Who has primary responsibility for developing the service plan?
- State case managers have primary responsibility for developing the service plan.
- Among service planners the average annual caseload is 50 individuals per planner.
- The case load range for service planners is from 35 to 50 individuals per planner.
- In Tennessee people usually do not have paid outside assistance available to them during the service planning process. Support brokers are available later to help recipients with the waiver processes and managing direct support staff.
Question: Does the service planning include a distinct risk assessment process to identify and address identified risk?
- The service planning includes a distinct risk assessment process to identify and address identified risks. Negotiated risk agreements are not used.
Question: Is the process the same or different from that used in the comprehensive waiver?
- The planning process parallels the process used in the comprehensive waiver.
Question: What happens to individuals when they need more support than the waiver can offer, either by way of particular services and/or overall cost?
- Other alternatives are identified by the case manager when available to meet their needs. If none are available or identified, exceptions to increasing the cap can be approved up to a point. Transfer to the comprehensive waiver is possible when slots are available. If slots were not available, the individuals would be placed on the waiting list.
Question: What parameters govern transition from the supports waiver to the comprehensive waiver?
- Only in the most extreme cases of need are individuals able to move from the supports waiver to the comprehensive waiver. So far, all such individuals have been accommodated.
- An individual may be dis-enrolled from the supports waiver if the health and safety of the individual or others cannot be assured or if the individual: (a) no longer manages his or her own service (support waiver); (b) is incarcerated; (c) no longer has a disability; (d) is no longer financial eligible; (e) moves out of state; (f) no longer meets level of care; (g) is admitted to nursing facility or ICF/MR; (h) is no longer eligible for Medicaid; (i) refuses services; or (j) fails to cooperate. Two individuals have been disenrolled in the past two years.
Question: What if the individual wants to change their service plan, or wants to change providers?
- The individual must contact his or her case manager and declare their want to change providers.
Question: How is quality assurance and quality management managed?
- The principle features of the waiver’s Quality Assurance and Quality Management System includes: (a) use of a dedicated Quality Management Committee; (b) oversight by case manages; (c) consumer satisfaction surveys; and (d) use annually, and even monthly, of an extensive, standardized quality assurance tool.
- This system is the same as is used for the comprehensive waiver.
- Where problems are discovered, the state may fine providers or apply other sanctions, provide technical assistance or training.
Question: How are complaints resolved?
- There are units within the regional or central offices to manage complaints. To file a complaint, individuals make a formal complain through one of these offices. Staff pursue investigations, act to reach resolution and offer mediation though there have been very few mediations over time. Last year there were 52 complaints statewide.
- Individuals may seek a fair hearing through this complaint procedure or they may file a local grievance.
- In Fair Hearings, a hearing is held before a Hearing Officer where the complainant requesting the appeal (and/or their representatives and witnesses) presents their case with the state presenting theirs as well. The Hearing Officer issues a written decision that can be appealed to the Director. The Director’s written decision can be appealed in District Court.
- In the grievance procedure, the grievant identifies their grievance and a proposed resolution. A local official responds to the grievance. This response can be appealed to a local governing body. If not resolved there, the grievance moves to an independent administrative committee. If not resolved at this level, the grievance may remain unresolved. In administrative inquiries, quality assurance completes an investigation and issues findings which may include provider citations.
Question: What is the process that is used to monitor the health and well-being of individuals participating in the supports waiver?
- The process includes case management, provider training, consumer satisfaction surveys, provider monitoring, provider background and abuse registry checks, pre-employment screenings, and critical incident reporting. The standardized monitoring tool that Tennessee uses to sort categories of need for the waiting list also has a subset for monitoring health and well-being.
- In-person monitoring is performed a minimum of every six months.
- The differences between the approach to SDWP monitoring and comprehensive waiver monitoring is that the comprehensive waiver requires more frequent face to face visits by case managers. Quality management personnel accumulate individual studies for future action and looks over time for problem people and patterns.
- Case management is responsible for resolving problems identified through monitoring.
- The state expects to change the supports waiver within the next 12 month by increasing internal monitoring of state case management and increased technical assistance to support brokers. There is a request for proposal to establish a permanent fiscal intermediary combined with support brokerage.
Opinions on Waiver Operations and Effects
Access to the Waiver
Explanation: Access refers to how easily people can apply for and gain admission to the supports waiver.
- The potential enrollees and their families learn about this waiver through generally through contact with printed matter such as a “family handbook” or brochures, and through the website. Special educators also frequently make referrals.
- Informants indicate that the supports waiver is “somewhat” publicized and individuals apply for the program through regional state case managers.
- It is very easy to apply and the demand for this waiver among people is growing.
Service Planning
Explanation: Service planning refers to the process to develop individual support plans for waiver recipients.
- Overall, state staff indicate that individuals “Very Much” lead the planning process, define their own service needs, and choose the agencies or support givers to offer the needed support.
- In contrast, advocates believe that individuals are not in the driver’s seat during the service plan development process.
- Overall, respondents indicate that recipients can exercise choice and control over service plans and make decisions about trade offs. Financial administration has been good.
- Overall, respondents indicate that service planners know the person they are planning for “Well” or “Somewhat.” However, there is turnover in staff and case load variations. It is a mixed bag. After the lawsuit, the state progressed rapidly to institute the SDWP and case managers were put into place and trained on-the-job. This led to quality problems related to case management
- The services available through this waiver are generally broad enough to meet participant needs. There are few requests for upward migration to the comprehensive waiver.
- It is “Very Easy” for individuals to change their service plans.
- The strengths of the individual planning approach are its ability to allow people to choose services, hire staff, and decide on trade offs.
- Some see shortcomings as a lack of training and preparation for the support waiver case managers.
Service Delivery and Safeguards
Explanation: Service delivery and safeguards refers to the services that individuals received and their operations, and the safeguards in place to assure health and well-being.
- Once services are authorized, it is very easy for individuals to get the supports they need.
Satisfaction with Outcomes
Employment outcomes:
- Generally people do not seek/acquire/hold integrated employment though it is a support waiver option that is being encouraged. A broad coalition of support for Employment First! has led to an on-going commitment across the state to expand integrated employment. As a component of the Employment First! initiative, benchmark goals were developed to track state progress in increasing integrated employment placements. Providers are asked to report specific data on the number of people in integrated employment, number of hours worked, wages earned per hour, and job title.
- The Employment First! Initiative boosted the number of individuals with I&DD employed in competitive jobs by nearly 40 percent in its three years of implementation. In 2002, when the Tennessee DMRS first launched the Employment First! Initiative, there were about 1,100 individuals employed in competitive jobs. That number grew to 1,542 by the end of December 2005.
Other outcomes:
- Generally, informants indicate that people can live on their own or with friends. However, families are very protective.
- Generally, informants indicate that people in the supports waiver participate in community events.
- There is some promotion in the waiver to promote community integration versus services that are more traditional (e.g., sheltered work, enclaves, and other segregated activities). However, many recipients continue to use the segregated services. Overall integration happens the most often with the family in regular community activities.
- There are currently 120 waiver recipients who hire and manage their own support workers. While the workers are employed by an agency, they often identify and refer potential workers to the agency and manage them on a day to day basis. Support brokers can help and assist them in evaluating workers and in filing the necessary forms.
- Where “in-home” supports are offered to adults living home with family, the services are seen by the state as most often family directed. This is true in the comprehensive waiver as well.
- To date, there have been no participants who have experienced major health, abuse, or neglect issues.
Key Issues in Play
Question: What are the waiver’s greatest strengths?
- Its ability to serve a large number of services recipients “in-home” while being cost effective with rapid deployment of the supports. Most people see the SDWP as early in its development with greater potentials for expanding self-determination.
- Generally, most individuals and families report being satisfied and very happy with services. There is flexibility of selection and potentially creative plans with enough services and components. People can stay home and the waiver reduces parental burnout.
- The state hosts eight town meetings each year and is working on better connections with school districts to help transitioning students become accomplished waiver recipients with more planning and fewer surprises for all parties.
- People have hope of getting off the waiting list and receiving services. The caps make people careful about what they select and careful what they buy.
- It allows for more flexibility and control for people with disabilities and family members in service delivery.
Question: What are the barriers to achieving the waiver’s goals?
- Tennessee has a large waiting list.
- Self-determination is often seen by many as an all or nothing proposition. This can cause people not to want to pursue it.
- Improvements are needed in case management and support brokering. The support waiver needed to begin quickly which meant the case managers did not have as much time to be trained and oriented to the new waiver. Case management case loads have grown too large. Their comprehensive waiver counterparts have been organized and operating for some time. More training, mentoring, and monitoring is needed by the support waiver case managers and support brokers. They need more information about the possibilities the supports waivers offer and what people can do. The support broker role is new and offers an opportunity for recipients and their families to have much more help in individualizing and customizing their own supports and plan.
- Services offered by licensed clinicians and therapists might be delivered more cost effectively by professionally guided direct service workers.
- People need more information about how to utilize other sources of supports. The series of lawsuits and newness of the support waiver have left many stakeholders afraid, uncertain and not trusting communications and regular state information.
Question: Are there topics where there is disagreement or concern?
- People on the waiting list remain unserved and so are accorded no safeguards or support.
- Tennessee direct support professionals and Tennesseans with disabilities earn low wages, often have limited career paths, and have trouble finding affordable (accessible, and safe) homes to buy.
- Community providers have difficulty maintaining a stable workforce. Low ages in the community are a problem.
- There are difficulties concerning differences in service provision requirements for various therapies provided under the waiver as opposed to the state Medicaid plan. State officials are working to make these differences more apparent to reduce unintended errors.
- There is a need to continue to train and monitor state case managers.
- It is presently very difficult to monitor costs; millions of dollars can be spent before it is realized. Better information management systems are needed.
- More should be done to increase information sharing about the supports waiver, the opportunities it brings for self-direction and emerging best practices.
Question: What are the TOP THREE things that could be done to improve the waiver?
- Add funds to eliminate the waiting list or increase the existing cap on the support waiver, for example to $50,000, to enroll people that would otherwise be in the more expensive and uncapped comprehensive waiver.
- More should be done to promote additional legislative and political support for the SDWP.
- Overall, there is a crying need for sharing information to help people obtain the supports they need.
Question: What other points should be raised?
- The SDWP is relatively new, and innovation should be encouraged.
- About five million new dollars is needed to bolster the existing comprehensive waiver. This is difficult choice because of the waiting list but is probably unavoidable.
Overall Impressions
All informants agree that the SDWP is making important contributions to supporting people with I&DD in the community, although it is still early in its development. CMS has influenced much of the decision-making to this point because of the shortcomings that it found in the operation of the comprehensive waiver. Now, however, it is time for state officials to step back and determine how the supports waiver can be best applied and shaped to improve the overall system of services. Clearly, the SDWP is a strong tool for containing costs and addressing the wait-list. Yet, much underlying infrastructure must still be developed, such as developing improved information management systems, assuring the presence of well-trained case managers and an agile provider community, and working out operational procedures to promote self-direction. Still, most agree that the SDWP has had a good start.