
U.S. Department of Health and Human Services
The Effect of Nursing Home Use on Medicaid Eligibility
Korbin Liu, SC.D.Urban Institute
Kenneth G. Manton, Ph.D.Duke University
1989
PDF Version: http://aspe.hhs.gov/daltcp/reports/1989/nhumedes.pdf (22 PDF pages)
This report was prepared under grant #87ASPE185A between the U.S. Department of Health and Human Services (HHS), Office of Social Services Policy (now known as the Office of Disability, Aging and Long-Term Care Policy (DALTCP)) and Duke University. This was published in The Gerontologist, Vol.19, No.1, 1989, pp.59-66. For additional information about the study, you may visit the DALTCP home page at http://aspe.hhs.gov/daltcp/home.shtml or contact the office at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, SW, Washington, DC 20201. The e-mail address is: webmaster.DALTCP@hhs.gov. The DALTCP Project Officer was Robert Clark.
Research for this paper was supported by grants from the Travelers Companies Foundation and the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation (No. 87ASPE185A), Health Care Financing Administration (18-C-98641), and National Institute on Aging (AGO7198). We are indebted to Drs. Joshua Wiener and Pamela Doty for their comments on an earlier draft of this article.
Presented are results of a descriptive analysis of the effects of nursing home use on Medicaid eligibility status. Data from the 1982 and 1984 National Long-Term Care Surveys were used to track a cohort of disabled elderly persons residing in the community in 1982 over the 2 years that followed. Although 12% spent some time in nursing homes between 1982 and 1984, about 40% was for short stays. In contrast to persons who did not use nursing homes, persons who entered nursing homes had a 4- to 5-fold risk of spending down to Medicaid eligibility. KEY WORDS: Catastrophic costs, Long-term care.
TABLE OF CONTENTS
- LIST OF FIGURES AND TABLES
- FIGURE 1. Nursing Home and Medicaid Status Transitions: Non-Medicaid, Community Residents in 1982
- TABLE 1. Proportion of the Community Disabled Elderly in 1982 Who Were in Nursing Homes in 1984
- TABLE 2. Proportions of the Community Disabled Elderly in 1982 Ever in a Nursing Home Between 1982 and 1984
- TABLE 3. Community Duration Prior to Nursing Home Admission
- TABLE 4. Nursing Home Payment Sources at Admission and at Survey Date
Private expenses for long-term care can reach catastrophic proportions for some older Americans with chronic physical or mental disabilities. Because of the high costs of nursing home care, which is about $25,000 per year, many individuals who enter nursing homes as private-pay patients can expect to spenddown their assets and become dependent on Medicaid as the source of payment for the remainder of their nursing home stay. Similarly, private expenses for the long-term care services required by disabled persons residing in the community can exceed income and lead to an erosion of assets.
Recognition that the potentially catastrophic costs of long-term care are generally borne out-of-pocket by individuals and their families has heightened consideration of alternative means for financing long-term care. A wide range of options is being considered, with considerable recent attention focused on different types of private long-term care insurance (Meiners, 1983). In addition, there has been discussion recently of the possibility of expanding Medicare benefits to cover long-term care (Blumenthal et al., 1986). Some analysts believe that, given the magnitude of the likely costs and recent fiscal and socio-demographic trends, options which combine private and public cost sharing are the most likely to be adopted (Wiener et al., 1987).
Despite increasing concern about private expenses for long-term care, the development of policy is currently hampered by the paucity of information on the conditions under which catastrophic expenses are incurred, especially how private expenses that are initially manageable eventually escalate into catastrophic financial burdens. Although the potential financial consequences of long-term care are widely recognized (Rice & Gabel, 1987), studies of the spenddown phenomenon and its implications have been scarce.
Presented are results from a descriptive analysis of data from the 1982 and 1984 National Long-Term Care Surveys (NLTCS). The analysis was designed to measure the use of nursing homes over time by disabled persons and the effects of nursing home use on Medicaid eligibility. The results are focused not only on the relationship between nursing home use and Medicaid eligibility, but also on how Medicaid eligibility is related to long and short nursing home stays as well as long-term care without nursing home use. The research is presented in four sections. First, information from the 1982 and 1984 NLTCS used in this analysis is described. Second, the use of nursing homes between 1982 and 1984 is presented. Third, results on the relationship between Medicaid status and nursing home use between 1982 and 1984 are discussed. Finally, the implications of the findings for future long-term care research and policy are discussed.
1982 AND 1984 NATIONAL LONG-TERM CARE SURVEYS (NLTCS)
The 1982 NLTC Survey
The 1982 NLTCS was a nationally representative survey of the noninstitutional Medicare population over age 65 needing assistance with one or more Activities of Daily Living (ADL) or Instrumental Activities of Daily Living (IADL). It was sponsored by the Department of Health and Human Services and conducted by the Census Bureau. A sample of 36,000 Medicare enrollees was drawn from Health Care Financing Administration (HFCA) administrative files and interviewed by telephone to identify those with assistance needs. Approximately 6,000 persons who were identified as requiring assistance with ADLs or IADLs for a period of 3 months or longer and residing in the community were included in the survey.
For all 36,000 sampled individuals, the screener document contained data on age, race, sex, and birth date. For each of 9 ADL and 7 IADL items, the person was asked if he or she had problems performing that activity and the duration of the difficulty. If the individual responded that the actual or expected duration had been (or was expected to be) more than 3 months, the respondent was given the detailed interview.
The detailed portion of the survey was administered to all noninstitutionalized persons with chronic (90 days or more) difficulty performing one or more ADL or IADL functions as indicated by the screener. Questions were asked about the presence of 17 chronic medical conditions, and whether in the last 12 months any of 12 medical events had occurred (e.g., heart attack, stroke, broken hip). A series of detailed questions were asked regarding each function included in the ADL scale: eating, transferring, walking, dressing, bathing, and toileting. Questions on health insurance involved coverage by Medicaid, CHAMPUS, other public assistance programs, or private health insurance.
Respondents were also asked a series of questions about prior stays in a nursing home, including admission dates and durations. Income questions addressed receipt of payments by each household member in the past month from various sources (e.g., Social Security or Railroad Retirement benefits, Supplementary Security Income, wages, salaries).
The 1984 NLTC Survey
The 1984 survey was designed to provide both longitudinal information on persons in the 1982 survey and a nationally representative cross-section of disabled persons in 1984. The longitudinal component was intended to provide insights into factors contributing to or inhibiting change in functional and health status and institutionalization.
Because of the focus of this paper on transitions in nursing home use and Medicaid status, the longitudinal data on the cohort of cases for whom detailed information was available in both the 1982 and 1984 surveys were employed. In 1982, these persons were functionally disabled and residing in the community. In 1984, they were still in the community, residing in nursing homes, or had died between 1982 and 1984. For these three different situations that were possible in 1984, three different survey instruments were used in the 1984 NLTCS.
The community questionnaire, which was similar to the 1982 survey instrument, was used for all functionally limited persons living in the community in 1984. Few modifications were introduced, but one was the addition of information on liquid assets such as equities and savings accounts.
The questionnaire on deceased persons, which was administered to next of kin, had two sections: health care and personal information. The health care section elicited data on nursing home, convalescent home and hospital stays if that was where the patient died. Questions included the sources of payment for those stays. For patients who did not die in such institutions, the questionnaire was used to ask about stays just prior to death. There were also questions about earlier periods of institutionalization. Finally, there were questions about others who provided care to the decedent, both paid and unpaid. Personal information surveyed included marital status, race, ethnic origin, and income.
The questionnaire for institutionalized persons included three major sections: cognitive functions, ADL impairments, and payment sources at admission and at the time of survey. As with the other questionnaires, there was an indicator for whether the sample person or a proxy answered the questions. Questions were asked about admission to nursing homes and periods of institutionalization prior to the current nursing home stay. There was also a question about hospital stays in the last 12 months. Finally, it was determined who paid for care, both at admission and on the date of the survey.
The analysis is focused on transitions between 1982 and 1984 of the sample of noninstitutionalized disabled persons who received the detail community questionnaire in 1982. Although the 1982 survey was representative of the disabled persons in the community, detailed information on disabled persons in nursing homes in 1982 was not collected. Hence, the transitions analyzed reflected the experience of only noninstitutionalized persons when the sample was drawn. If detailed information were available on the institutionalized persons, it would have been included in the analysis of transition. Overall rates of future nursing home and Medicaid status transitions might be different with their inclusion, but a different data source would be required to answer this question.
For most of the comparisons, status at the time of the surveys in 1982 and 1984 was employed. For example, persons who had died in the 2 intervening years were regarded as being dead as of 1984. One major intra-interval measure that was constructed was any use of nursing homes between 1982 and 1984. Hence, this measure included persons who had entered nursing homes and were discharged dead or alive to the community, as well as persons who were residents of nursing homes in 1984. To measure Medicaid status, the information that was available from the community, institutional, and deceased questionnaires was used. For the community surveys, Medicaid eligibility for both 1982 and 1984 were employed, whereas for the institutional and deceased questionnaires, Medicaid status referred to actual use of Medicaid as a payment source for nursing homes or hospitals. Although a uniform definition would have been preferable, this option was not possible in light of the data available.
Findings track the cohort between 1982 and 1984. Described in three sequential sections are nursing home use, changes in Medicaid status associated with nursing home use, and payment source changes in nursing homes.
FINDINGS
Nursing Home Use
Nursing homes are use d for different purposes ranging from short-term rehabilitative care to long-term care for persons with chronic disabilities that preclude their residency in the community. The fact that short- and long-stay patients both occupy nursing homes suggested that different types of patients need to be differentiated in estimating the risks of nursing home entry and the costs of nursing home care over time. To date, the identification and measurement of long- versus short-stay nursing home episodes have been based primarily on surveys of persons already in nursing homes. In several studies of the 1977 National Nursing Home Survey (NNHS), admission characteristics and utilization patterns of nursing home patients after they were in institutions were described (Keeler et al., 1981; Liu & Manton, 1983; Liu and Manton, 1984). The distinction between long- and short-stays is important to the consideration of Medicaid spenddown issues because many short-stay patients may not have to expend personal assets for their nursing home stays. Results presented below illustrate the effects of this distinction.
Because the 1984 NLTCS elicited detailed information on nursing home use in the 2 years since the 1982 NLTCS, it was possible to estimate the total incidence of nursing home admissions in this period, as well as to distinguish admissions that were long- versus short-stay. In this initial analysis, persons who entered nursing homes during the interval and who were still residents in nursing homes in 1984 were viewed as long-stay patients. The assumption underlying this distinction is the observation that institutionalized persons captured in a cross-sectional sample (e.g., persons in nursing homes at the time of the 1984 survey) tended to have much longer lengths of stay on average than persons in an admission or discharge sample (Manton et al., 1984). For example, the median length of completed stays in the 1977 NNHS discharge sample was 75 days whereas the average length of stay in the 1977 NNHS current resident sample was 597 days (National Center for Health Statistics, 1979).
Table 1 presents the proportion of disabled community residents in 1982 who were in nursing homes as of the survey in 1984. Hence, this table is used to describe the long-stay patients. Subgroup rates of nursing home use are also presented by 1982 Medicaid eligibility status and other personal characteristics. Overall, 7% of the disabled community residents in 1982 were in nursing homes in 1984. As expected, the risk of being a nursing home resident increased with age, rising from 4% for those 65 to 74 to 12% for persons over age 85. Higher rates of nursing home use were found for females and whites, results consistent with other research (NCHS, 1979). Nursing home use risks were also strongly related to disability status, with a monotonic increase of nursing home use rates by disability status up to ADL 5 to 6. Persons with the greatest ADL dependency in 1982 might be expected to have the highest rates of nursing home use; the slightly lower rate was due to the high mortality risks of this subgroup (Manton, 1987). Although not shown in Table 1, 21% of the 1982 community disabled persons had died whereas the remainder who were not in nursing homes were residing in the community. About 36% of persons with 5 to 6 ADLs in 1982 had died by 1984, in contrast to 15% to 23% for other ADL categories.
Of particular importance is the relationship between income and nursing home use. As shown in Table 1, nursing home use rates declined with increasing income for the total sample. This finding suggests that availability of financial resources to pay for community care may reduce a persons's need to enter nursing homes, all other factors being equal.
| TABLE 1. Proportion of the Community Disabled Elderly in 1982 Who Were in Nursing Homes in 1984 | |||
| Medicaid in 1982 (N = 1385) | Not Medicaid in 1982 (N = 4281) | Totala (N = 5795) | |
| Nursing homes in 1984 | Nursing homes in 1984 | Nursing homes in 1984 | |
| All cases | 7.3% | 7.0% | 7.1% |
| 65-74 | 4.6 | 3.9 | 4.1 |
| 75-84 | 7.8 | 8.2 | 8.1 |
| 85+ | 11.6 | 11.4 | 11.5 |
| Male | 5.2 | 5.1 | 3.6 |
| Female | 8.1 | 8.1 | 7.7 |
| White | 9.0 | 7.3 | 7.7 |
| Non-White | 2.8 | 3.8 | 3.6 |
| Not disabled | 2.4 | 1.0 | 1.3 |
| IADL | 5.8 | 5.4 | 5.5 |
| ADL 1-2 | 6.9 | 7.7 | 7.5 |
| ADL 3-4 | 11.9 | 8.9 | 9.5 |
| ADL 5-6 | 7.9 | 10.4 | 9.8 |
| Married | 4.5 | 4.2 | 4.4 |
| Not married | 8.4 | 9.6 | 9.3 |
| $4,000 | 7.2 | 10.7 | 8.8 |
| $4,000-7,000 | 7.2 | 8.3 | 7.9 |
| $7000-10,000 | 9.5 | 5.6 | 6.2 |
| $10,000-20,000 | --- | 4.0 | 3.9 |
| $20,000+ | --- | 3.2 | 3.0 |
| |||
Medicaid status did not differentiate nursing home use by demographic characteristics. The patterns of nursing home use by income categories, however, were different between the Medicaid and non-Medicaid groups. Nursing home use rates were similar across the income categories for Medicaid, whereas nursing home use rates declined monotonically with income for non-Medicaid persons. A comparison of lower income groups (i.e., less than $10,000) suggests that differences in nursing home use rates were small between Medicaid and non-Medicaid persons at these income levels. Higher income non-Medicaid persons had notably lower rates of nursing home use, suggesting that income is a more important determinant of nursing home use than Medicaid status.
Shown in Table 1 is the proportion of community residents who were found in nursing homes after 2 years, but it does not fully represent the nursing home use experience of the sample because some persons used nursing homes and returned to the community or died. In Table 2 are presented the proportions of the persons who had any use of nursing homes in the 1982-1984 period. Also shown in Table 2 is that a much higher proportion of the 1982 community residents spent some time in a nursing home (about 12%) than was recorded in the cross-sectional results in Table 1. As with the Table 1 results, the proportions of persons who used nursing homes any time between 1982 and 1984 were associated with specific personal characteristics in 1982. The risk of nursing home use, regardless of reasons for nursing home use, tended to be associated with those characteristics in expected directions.
| TABLE 2. Proportions of the Community Disabled Elderly in 1982 Ever in a Nursing Home Between 1982 and 1984 | |||
| Medicaid in 1982 (N = 1385) | Not Medicaid in 1982 (N = 4281) | Totala (N = 5795) | |
| Any use | Any use | Any use | |
| All cases | 11.7% | 11.8% | 11.8% |
| 65-74 | 7.1 | 5.8 | 6.1 |
| 75-84 | 12.8 | 14.6 | 14.2 |
| 85+ | 18.3 | 19.3 | 19.1 |
| Male | 10.0 | 9.2 | 9.4 |
| Female | 12.4 | 13.5 | 13.2 |
| White | 14.0 | 12.3 | 12.7 |
| Non-White | 5.9 | 5.8 | 5.8 |
| Not disabled | 4.7 | 2.5 | 3.0 |
| IADL | 8.0 | 8.4 | 8.3 |
| ADL 1-2 | 11.9 | 12.9 | 12.7 |
| ADL 3-4 | 18.7 | 16.4 | 17.0 |
| ADL 5-6 | 13.2 | 17.7 | 16.6 |
| Married | 8.7 | 7.9 | 8.3 |
| Not married | 12.9 | 15.4 | 14.7 |
| $4,000 | 11.4 | 14.0 | 12.5 |
| $4,000-7,000 | 10.3 | 13.8 | 12.5 |
| $7000-10,000 | 14.2 | 9.9 | 10.7 |
| $10,000-20,000 | --- | 8.9 | 9.4 |
| $20,000+ | --- | 3.7 | 3.4 |
| |||
Also presented in Table 2 is nursing home use by Medicaid status in 1982. Similar to the findings in Table 1, Medicaid status did not differentiate the overall patterns that were found between demographic characteristics and nursing home use. Also similar was the finding that Medicaid and non-Medicaid persons in the lower income categories had approximately the same use rates, whereas non-Medicaid persons with incomes of $20,000 or more had notably lower rates.
Of the 12% of respondents who spent any time in nursing homes in the 2-year interval, 24% died by 1984,15% returned to the community with 60% still in nursing homes in 1984. Hence, 40% of nursing home admissions were for relatively short periods of stay. Among the persons who entered nursing homes but returned to the community by 1984, approximately half were in nursing homes for less than 30 days and 80% had lengths of stay of less than 90 days. Those residents used nursing homes for convalescent or rehabilitative care and were distinct from others who were institutionalized for very long stays. Further analyses indicated no notable difference in length of stay for those who were Medicaid eligible and not Medicaid eligible in 1982.
After examining the risk of nursing home use, the amount of time it took for individuals with specific characteristics to enter nursing homes since the 1982 survey was investigated. As shown in Table 3 for both Medicaid and non-Medicaid persons who entered nursing homes, the mean time before admission was about 470 days. Approximately 15% entered a nursing home after less than 6 months in the community. Although not presented here, in additional analyses no notable differences were found in duration prior to nursing home admissions between subsets of the Medicaid and non-Medicaid samples in terms of their demographic and functional characteristics.
Although these findings are contradictory to widely held notions that Medicaid patients have greater problems than private pay patients in gaining access to nursing homes, a possible explanation is that many disabled elderly persons who were not Medicaid eligible were only marginally better off than their Medicaid eligible counterparts and were subject to similar access barriers to nursing homes.
Nursing Home and Medicaid Status Changes
Described in the prior section was the use of nursing homes of the 1982 NLTCS sample. Examined in this section is how their use of nursing homes resulted in spenddown to Medicaid. Although individuals can be on and off Medicaid eligibility over time, an important issue is whether nursing home use, particularly long stays in nursing homes, resulted in indefinite Medicaid eligibility. Because most policy concerns have been on how individuals who are not Medicaid eligible become impoverished through use of long-term care and remain Medicaid recipients over time, focus was on the transitions experienced by persons who were non-Medicaid in 1982.
To investigate the relationship between nursing home use and change from non-Medicaid to Medicaid status, the likelihood of Medicaid spenddown given that the person had been in a nursing home and the likelihood of Medicaid spenddown in the absence of a nursing home admission were compared. These results are presented in Figure 1, and reflect the joint events of nursing home use and qualification for Medicaid eligibility. Depicted in Figure 1 is the partitioning of the 1982 sample of disabled non-Medicaid persons in 1982 by whether nursing homes were used between 1982 and 1984, whether location status in 1984 was nursing home residency, community residency or deceased, and whether persons were Medicaid eligible in 1984.
| TABLE 3. Community Duration Prior to Nursing Home Admission | ||||
| Medicaid 1982 (N = 149) | Non Medicaid 1982 (N = 479) | |||
| MeanSD | 478 days228 days | 472 days217 days | ||
| LOS Category | Percent | Cumulative Percent | Percent | Cumulative Percent |
| 0-89 | 6.0 | 6.0 | 5.4 | 5.4 |
| 90-179 | 10.1 | 16.1 | 7.5 | 12.9 |
| 180-359 | 15.4 | 31.5 | 20.1 | 33.0 |
| 360-539 | 22.2 | 53.7 | 21.7 | 54.7 |
| 540-719 | 29.5 | 83.2 | 33.2 | 87.9 |
| 720+ | 16.8 | 100.0 | 12.1 | 100.0 |
Shown in Figure 1 is that 12% of non-Medicaid eligible community disabled persons in 1982 spent some time in a nursing home between 1982 and 1984. The remaining 88% remained in the community for the entire 2-year period or died between 1982 and 1984. Next, the nursing home use and non-nursing home use groups are each separated by their 1984 status, i.e., they were still in the community, in a nursing home, or died between 1982 and 1984. Among the persons who had spent any time in nursing homes, 17% had returned to the community, 24% had deceased but 60% were still in nursing homes in 1984. Over 90% of the persons who entered nursing homes, but returned to the community, were not Medicaid eligible in 1984. Although the number of cases at this point was small, the apparently high proportion of nursing home patients who did not spend down because they did not spend much time in nursing homes is consistent with expectation. In contrast, persons who were still in nursing homes in 1984, the expected long-stay patients, had a much higher proportion (41%) who had become Medicaid patients. For the deceased, 21% had become Medicaid eligible by the time they died.
Among the persons who had not used nursing homes at any time between 1982 and 1984, 80% were still in the community in 1984 whereas 20% had died. Regardless of their vital status in 1984, only 6% to 7% were Medicaid eligible as of 1984. In contrast to the persons who had used nursing homes at any time between 1982-84, this rate of Medicaid eligibility was quite low.
Results in Figure 1 indicated several important relationships between nursing home use and Medicaid status. First, there is a strong relationship between nursing home use and Medicaid spenddown. In comparing persons who were Medicaid eligible in 1984 who spent time in nursing homes in the prior 2 years with those who had not, it was found that the likelihood of being Medicaid eligible was 31% if they spent any time in a nursing home compared to 7% if nursing homes were not used. From Figure 1, summing the cases that used nursing homes and were Medicaid eligible as of 1984 (n = 155) and dividing by the number of cases experiencing any nursing home use between 1982 and 1984 (n = 506) yielded the proportion (31%) of nursing home users who were Medicaid eligible. A similar calculation can be made with the non-nursing home users which yielded a 7% Medicaid eligibility rate. Hence, a disabled elderly person has 4 to 5 times greater risk of being Medicaid eligible in 2 years if he or she were admitted anytime in the 2-year period.
| FIGURE 1. Nursing Home and Medicaid Status Transitions: Non-Medicaid, Community Residents in 1982 |
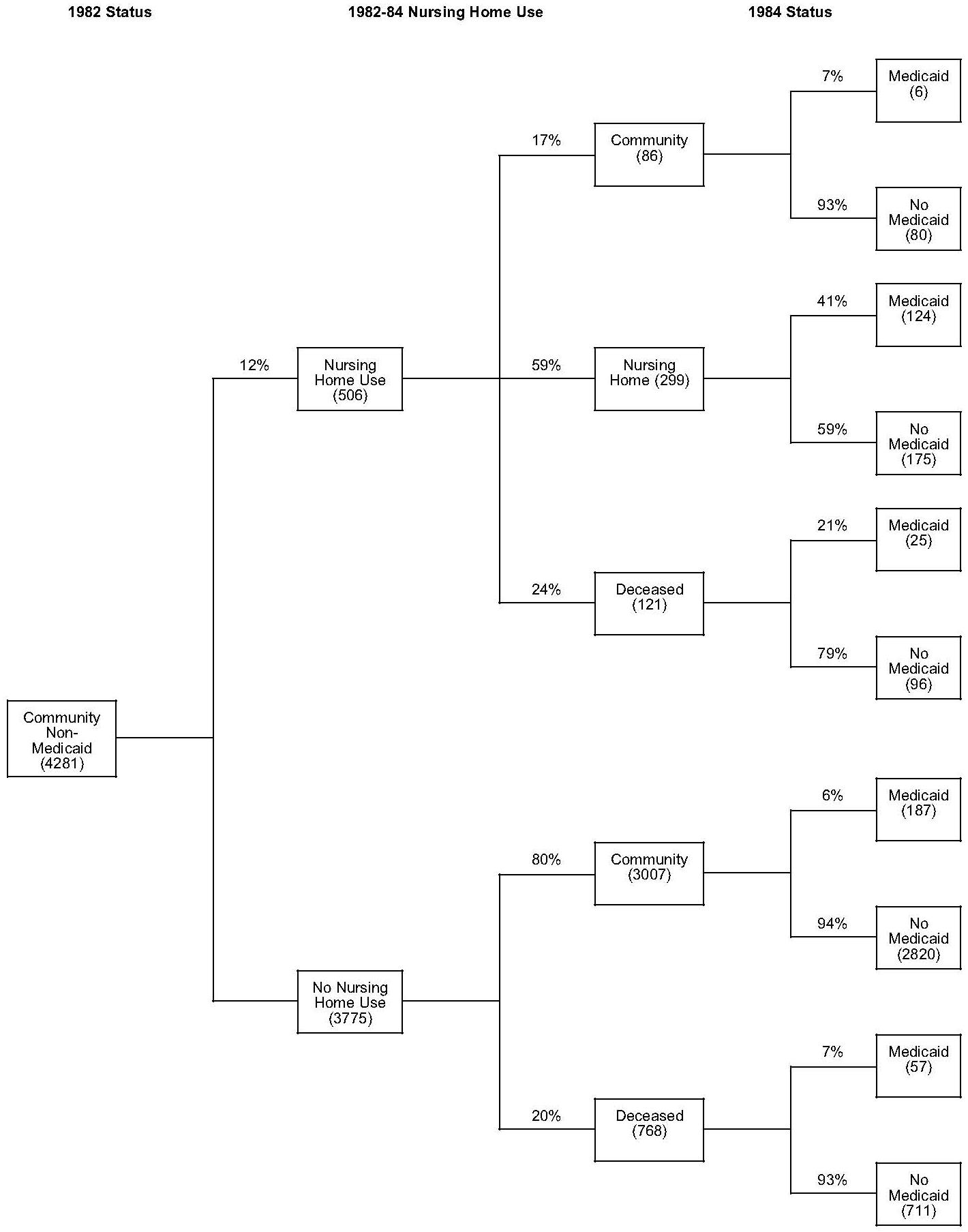 |
| NOTE: Number in parentheses is the number of cases. |
Second, temporary or short stays in nursing homes do not increase one's risk of spending down to Medicaid. Only 7% of persons who entered nursing homes and returned to the community were Medicaid eligible in 1984; this rate of Medicaid eligibility is similar to the 6% to 7% of community residents in 1984 who became Medicaid eligible and did not spend time in a nursing home. In contrast, 41 % of the persons still in nursing homes in 1984, the long stayers, were Medicaid eligible. Hence long-term residents had a 7-fold increase in risk of Medicaid spenddown.
Third, Figure 1 also indicated that spenddown to Medicaid can occur without nursing home use. About 6% to 7% of the disabled elderly people who were not Medicaid eligible are expected to become eligible within 2 years without high costs of nursing home care.
The analysis presented in Figure 1 is an initial assessment of the important relationship between nursing home use and Medicaid eligibility. It is limited in several ways. For example, the description of the process by which noninstitutionalized, non-Medicaid persons in 1982 used nursing homes and became Medicaid eligible by 1984 offered in Figure 1 is limited to a comparison of differences in status at two fixed points in time. Between 1982 and 1984, multiple nursing home admissions could have been experienced by persons in the sample, with Medicaid spenddown occurring at any point in the interval. In addition, the results reflected the average national experience of a sample of disabled older persons. The patterns of transitions may differ considerably between states because of the variability of Medicaid eligibility policies and the variation of socio-economic characteristics of disabled elderly populations across states. Finally, the analysis was focused on changes in Medicaid eligibility. Not described is the rate at which Medicaid costs were being incurred for services. Hence, although the results of this analysis were intended to provide insights for the development of cost assessment strategies, the data available from the NLTCS were not designed to make specific analyses of Medicaid costs.
Payment Sources Changes of Nursing Home Admissions
Described earlier was the relationship between nursing home use between 1982 and 1984 and the conversion of non-Medicaid disabled persons to Medicaid status as of 1984. Examined in this section in greater detail are payment sources of persons who were nursing home patients in 1984.
Data in the NLTCS on payment source changes for nursing home care were available only for persons who were residents of nursing homes in 1984. Approximately 400 persons from the 1982 community sample fell into this category. Because persons in the 1982 cohort were known to reside in the community, at the lime of the 1982 survey they could only have been institutionalized for 2 years or less by 1984. In addition, since the survey was conducted in 1984, the length of stay in nursing homes of this group was also truncated. Thus, in assessing payment source changes, only partial information was available be cause some sample members had not been in nursing homes long enough for all changes in payment source to occur.
Presented in Table 4 are the sources of payment reported at admission and at the time of the 1984 survey. For both time points, asked in the 1984 NLTCS were sources that contributed to payment for care. Hence, Table 4 results reflected multiple responses to the payment source questions. A major source of payment for most persons is Social Security which in the NLTCS was included under the response category self. The most significant comparison in this table is the percentage of persons who were Medicaid eligible at admission and at the time of the 1984 survey. It is important to recall, however, that most Medicaid eligible nursing home patients are expending other sources of funds (e.g., Social Security) toward the payment of their nursing home care, and Medicaid does not normally pay for 100% of per them nursing home costs.
Shown in Table 4 is that Medicaid was reported to be a source of payment at admission in 40% of the cases and a payment source at the time of the survey in 50% of the cases. The increases in the proportion of cases with Medicaid as a payment source from admission to current residence reflects the process of spenddown. This estimate (i.e., 10%) may be high, however, because persons who reported Medicare as a payment source might have been Medicaid eligible while Medicare was paying for the days of nursing home care.
Approximately half the sample reported self as a source of payment both at admission and at the time of the 1984 survey. Children contributed to the payment of nursing home care for 8% of both samples. Private insurance was a source of payment in 5% of the cases at admission. This proportion declined to 3% by the time of the survey. Similarly, Medicare, which was a source of payment in 21% of the cases at admission, declined to 12% by the time of the survey.
| TABLE 4. Nursing Home Payment Sources at Admission and at Survey Date | ||
| Payment Source | Admission(N = 412) | Current(N = 389) |
| Self | 50% | 53% |
| Spouse | 6 | 6 |
| Children | 9 | 8 |
| Insurance | 5 | 3 |
| Medicare | 21 | 12 |
| Medicaid | 40 | 50 |
| Data refer to persons who were disabled and residing in the community in 1982 NLTCS and were residents in nursing homes at the time of the 1984 NLTCS. Multiple responses result in percentages exceeding 100%. | ||
The decline in the proportion of residents using private insurance and Medicare payments from admission to the survey date reflected the relatively short period to time these payment mechanisms cover nursing home costs. Medicare, for example, has a maximum duration of coverage of 100 days. The change in private insurance suggested that durations of coverage by this source could also have been short, possibly as a benefit of Medigap policies.
Another important question with policy implications is the duration in which people spenddown. Because sample persons had not completed their nursing home stays, it was not possible to describe this phenomenon completely. Additionally, many private payers had not been in facilities long enough for spenddown to occur. For those who did spenddown, however, by the time the 1984 survey was conducted, it was possible to measure the duration between non-Medicaid and Medicaid status. Specifically, information on spenddown over time was available from the 1982-84 NLTCS on only 22 cases for the 1982 cohort. Because of the selection for short stayers in the 1982 cohort (i.e., the constraint that they were in the community 2 years earlier), the mean spenddown period for this group was only 159 days whereas 73% converted in 6 months. This duration is short relative to prior estimates by the U.S. Government General Accounting Office (1979) and the U.S. House of Representatives Aging Committee (1985). The GAO, for example, found that approximately half of the private patients took about 6 months to convert to Medicaid.
DISCUSSION
Initial findings were presented on the transition of nursing home use and Medicaid status of functionally impaired persons originally residing in the community. Simple measures were employed to provide insights on the relationship between use of nursing homes, by type of stay, and catastrophic costs from the 1982-84 NLTCS. For example, short- versus long-stay nursing home patients were identified by their institutional status in 1984. This provided only a crude approximation of long- and short-stays. Improved estimates could be derived by employing other characteristics of patients entering nursing homes such as clinical conditions (e.g., hip fracture versus Alzheimer's disease). Similarly, transition from non-Medicaid to Medicaid status was used as a measure of catastrophic long-term care costs. Although other constructs (e.g., costs relative to ability to pay) (Wyszewianski, 1986) could produce different results, there is general consensus that the spenddown of personal wealth to Medicaid eligibility reflects the effects of catastrophic health care costs.
Initial findings from the 1982-84 NLTCS added new information for the consideration of long-term care research and policies. First, the analysis indicated that short-stays in nursing homes had virtually no impact on the risks of becoming Medicaid eligible, whereas long-stays greatly increased the risk of Medicaid spenddown. Because 40% of the nursing home admissions between 1982-84 were short-stays, adjustments for the heterogeneity of nursing home use would be important in actuarial and policy analysis of long-term care requirements. Although prior research on determinants of nursing home use tended to view nursing home entry as a homogeneous event, it is likely that functions predicting different types of nursing home use could be quite different types of nursing home use could be quite different.
Second, the results indicated a strong association between nursing home use and Medicaid spenddown. Whereas disabled older persons who were not Medicaid eligible and residing in the community had a 7% risk of becoming Medicaid eligible in 2 years, those who used nursing homes at any time had 4 to 5 times the risk of spending down to Medicaid eligibility. Although nursing home use heightens the risks of spenddown, the results also indicated that disabled older Americans incur catastrophic long-term care costs without entering nursing homes.
Third, the results indicated that overall duration prior to nursing home admission were similar for Medicaid and non-Medicaid eligible persons. Moreover, nursing home use rates of disabled older persons were similar for Medicaid eligible persons and non-Medicaid persons in lower income categories. On the other hand, nursing home use rates were notably lower for non-Medicaid individuals with higher incomes. These results suggest that income rather than Medicaid status is the important determinant of nursing home use. Future research involving multivariate analyses of health and functional status, income and informal support would be required, however, to determine the extent to which differences by Medicaid eligibility status or income were due to need for nursing home care or ability to pay for community based care.
Fourth, although the payment source information presented provided further information on the nursing home spenddown process, the paucity of data on how long patients use one payment source before hanging to another continues to be a limitation in the consideration of many public and private policies on nursing home care. Other sources of information would be needed to provide actuarial estimates of the costs of nursing home care to individuals and to Medicaid. Ideally, a data source that permits the derivation of the full nursing home use experience of an admission cohort by proportion of total costs would be needed for this purpose. Moreover, this information for specific states would be desirable because of the variability of the state Medicaid policies noted earlier.
Although further research would clarify the different ways in which financially catastrophic long-term care costs are incurred, the findings presented earlier highlighted the fact that both community based care and nursing home care costs need to be addressed in the consideration of new policies to reduce the financial risks of older Americans. Further research is required to translate these preliminary findings into empirical models to estimate Medicaid program costs, private costs, and the potential effects of programs, such as long-term care insurance, that might alter the period of private payment for nursing home care.
CONCLUSIONS
Congressional deliberations about catastrophic health care costs have resulted in the recommendation of new Medicare policies to reduce the risks of catastrophic costs from acute care. Although policy makers also recognized that costs of long-term care can be catastrophic, there has been less movement toward safeguarding individuals and their families from the financial hazards of long-term care costs. The absence of action to address the financially catastrophic long-term care risk of elderly people stems from many reasons including the anticipation that coverage of long-term care could have high public costs. The high potential costs of long-term care have also induced private insurers to proceed cautiously in the development and marketing of private long-term care policies.
The collective findings from the preliminary analysis begin to describe a highly vulnerable subgroup of the elderly population in terms of its use of and financial ability to pay for long-term care. An overall 9% Medicaid spenddown rate indicated that many non-Medicaid disabled persons had marginal incomes and assets above Medicaid eligibility and were at high risk of impoverishment. Their high rates of nursing home use, in contrast to higher income persons, suggest a possible combination of more severe disabilities and inability to pay for formal community based care.
As policy makers continue to deliberate long-term care policies to mitigate the risks associated with chronic disabilities, a key consideration should be the availability of private financial resources to pay for long-term care. It is apparent that both financial status and health status predispose subgroups of the disabled elderly population toward becoming Medicaid beneficiaries. Although elderly persons of all income categories are at risk of requiring long-term care, those with limited financial resources are particularly subject to catastrophic costs and possible limitations in access to care. As various new public and private options for financing long-term care are considered, a clear priority concern for public policies should be the financially vulnerable among the disabled elderly population.
REFERENCES
Blumenthal, D., Schlesinger, M., & Drumheller, P.B. (1986). The future of Medicare. New England Journal of Medicine, 314, 722-723.
Keeler, E.B., Kane, R.L., & Soloman, D.H. (1981). Short- and long-term residents of nursing homes. Medical Care, 19, 363-369.
Liu, K., & Manton, K.G. (1983). The characteristics and utilization pattern of an admission cohort of nursing home patients. The Gerontologist, 23, 92-98.
Liu, K., & Manton, K.G. (1984). The characteristics and utilization pattern of an admission cohort of nursing home patients (II). The Gerontologist, 24, 71-76.
Manton, K.G. (1987 September). Gender differences in the linkages between functioning, disability, and mortality. Presented at the NIA Conference on Gender and Longevity, Bethesda, MD.
Manton, K.G., Woodbury, M.A., & Liu, K. (1984). Life table methods for assessing the dynamics of U.S. nursing home utilization: 1976-1977. Journal of Gerontology, 39, 79-87.
Meiners, M.R. (1983). The case for long-term care insurance. Health Affairs. Summer. 55-79.
National Center for Health Statistics. (1979). The national nursing home survey: 1977 summary for the United States. Vital and Health Statistics, Series 13, Number 43.
U.S. General Accounting Office. (1979). Entering a nursing home: Costly implications for Medicaid and the elderly. Report to the Congress, November 26. U.S. Government Printing Office.
U.S. House of Representatives, Select Committee on Aging. (1985). Americas elderly at risk. Committee Print (July).
Wiener, J.M., Hanley, R.J., Spence, D.A., Murrary, S., Kennell, D., & Shells, J. (1987). Estimating the demand for the impact of private sector financing options for long-term care. Final Report, Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services, Grant #86ASPE105A. [http://aspe.hhs.gov/daltcp/reports/estdemnd.htm]
Wyszewianski, L. (1986). Financially catastrophic and high-cost cases: Definitions, distinctions, and their implications for policy information. Inquiry, 23, 382-394.
CHARACTERISTICS OF THE ELDERLY LONG-TERM CARE POPULATION AND ITS SERVICE USE REPORTS AVAILABLE
- Epidemiological, Demographic and Social Correlates of Disability among the Elderly
- HTML http://aspe.hhs.gov/daltcp/reports/1988/epdemes.htm
- PDF http://aspe.hhs.gov/daltcp/reports/1988/epdemes.pdf
- Recent Changes in Service Use Patterns of Disabled Medicare Beneficiaries
- HTML http://aspe.hhs.gov/daltcp/reports/1990/recentes.htm
- PDF http://aspe.hhs.gov/daltcp/reports/1990/recentes.pdf
- Risks of Entering Nursing Homes for Long and Short Stays
- HTML http://aspe.hhs.gov/daltcp/reports/1988/nhlsstes.htm
- PDF http://aspe.hhs.gov/daltcp/reports/1988/nhlsstes.pdf
- The Effect of Nursing Home Use on Medicaid Eligibility
- HTML http://aspe.hhs.gov/daltcp/reports/1989/nhumedes.htm
- PDF http://aspe.hhs.gov/daltcp/reports/1989/nhumedes.pdf
To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human ServicesOffice of Disability, Aging and Long-Term Care PolicyRoom 424E, H.H. Humphrey Building200 Independence Avenue, S.W.Washington, D.C. 20201FAX: 202-401-7733Email: webmaster.DALTCP@hhs.gov
RETURN TO:
Office of Disability, Aging and Long-Term Care Policy (DALTCP) Home [http://aspe.hhs.gov/_/office_specific/daltcp.cfm]Assistant Secretary for Planning and Evaluation (ASPE) Home [http://aspe.hhs.gov]U.S. Department of Health and Human Services Home [http://www.hhs.gov]