
Susan G. Pfefferle, Samantha S. Karon, and Brandy Wyant
Abt Associates
Printer Friendly Version in PDF Format (44 PDF pages)
ABSTRACT
The purpose of the Opioid Use Disorder, Housing Instability and Housing Options for Recovery project was to help ASPE and HUD describe the housing models available for individuals with Opioid Use Disorder (OUD) who experience housing instability or homelessness. This issue brief presents project findings from the literature and discussions with experts and community housing providers about housing models that can best serve people with OUD who also experience homelessness or housing instability. While people experiencing homelessness have no housing at all, those experiencing housing instability experience challenges such as having trouble paying rent, living in an overcrowded space, moving frequently, staying with relatives, or spending the bulk of the household income on housing. This brief aims to bridge these two provider worlds to foster development of programs that support both housing and OUD related needs.
This report was prepared under contract #HHSP233201600010I between HHS's ASPE/DALTCP and Abt Associates. For additional information about this subject, you can visit the DALTCP home page at https://aspe.hhs.gov/office-disability-aging-and-long-term-care-policy-daltcp or contact the ASPE Project Officer, Emily Rosenoff, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201; Emily.Rosenoff@hhs.gov.
DISCLAIMER: The opinions and views expressed in this report are those of the authors. They do not reflect the views of the Department of Health and Human Services, the contractor or any other funding organization. This report was completed and submitted on September 17, 2018.
TABLE OF CONTENTS
1. INTRODUCTION
2. METHODS
2.1. Environmental Scan
2.2. Discussions with Experts
2.3. Discussions with Providers in Four Communities
3. HOUSING MODELS FOR PEOPLE WITH OPIOID USE DISORDER
3.1. Populations at Risk
3.2. Housing Models and Opioid Use Disorder Treatment Outcomes
3.3. Medication-Assisted Treatment
4. INTEGRATION OF MEDICATION-ASSISTED TREATMENT, CASE MANAGEMENT, AND HEALTH SERVICES
4.1. Brief Community Provider Profiles
APPENDICES
- APPENDIX A: Housing Typology
- APPENDIX B: Glossary of Terms
- APPENDIX C: Expert Discussants and Community Providers
LIST OF EXHIBITS
- EXHIBIT 1: Housing and Support Options to Provide OUD Recovery
ACRONYMS
The following acronyms are mentioned in this report and/or appendices.
| ADA | Americans with Disabilities Act |
|---|---|
| ASPE | HHS Office of the Assistant Secretary for Planning and Evaluation |
| CEO | Chief Executive Officer |
| COR | Contracting Office Representative |
| CSH | Corporation for Supportive Housing |
| DCPP | New Jersey Division of Child Protection and Permanency |
| DESC | Downtown Emergency Service Center |
| EBP | Evidence-Based Practice |
| FDA | HHS Food and Drug Administration |
| FQHC | Federally Qualified Health Center |
| HHS | U.S. Department of Health and Human Services |
| HUD | U.S. Department of Housing and Urban Development |
| KFT | Keeping Families Together |
| LPC | Licensed Professional Counselor |
| MAT | Medication-Assisted Treatment |
| MS | Master of Science |
| NARR | National Alliance for Recovery Residences |
| OBOT | Office-Based Opioid Treatment |
| OTP | Opioid Treatment Program |
| OUD | Opioid Use Disorder |
| PSH | Permanent Supportive Housing |
| SAMHSA | HHS Substance Abuse and Mental Health Services Administration |
| SMI | Serious Mental Illness |
| STEP | Stepped Treatment Engagement Program |
| SUD | Substance Use Disorder |
EXECUTIVE SUMMARY
Introduction. The purpose of the Opioid Use Disorder, Housing Instability and Housing Options for Recovery project was to help the U.S. Department of Health and Human Services (HHS) Office of the Assistant Secretary for Planning and Evaluation and U.S. Department of Housing and Urban Development (HUD) describe the housing models available for individuals with opioid use disorder (OUD) who experience housing instability or homelessness. The association between OUD and homelessness has been examined and established.[1, 2] Veterans -- who have higher rates of both homelessness and OUD than are observed in the general population -- and youth are particularly at risk.[3, 4] To better understand housing models that may support those with OUD, the study team conducted an environmental scan and held discussions with experts and providers in four communities. Medication-assisted treatment (MAT), using the HHS Food and Drug Administration-approved medications methadone, buprenorphine, and naltrexone, along with counseling and behavioral therapies, is well documented as an evidence-based treatment for OUD.[5] All community housing providers chosen for discussions allowed people receiving MAT to be housed in their programs. Some housing programs the study team examined partnered with treatment providers who used naltrexone. Others used buprenorphine and/or coordinated with opioid treatment programs to treat individuals in need of methadone. Most closely collaborated with MAT providers. Two of the housing programs served families with children, and two served single adults.
| Elements of the Housing First Model
|
Findings. People without stable housing are less able to engage in MAT.[6] Further, although MAT has been well documented as an evidence-based practice (EBP) to treat OUD,[5] individuals without housing who are receiving MAT still experience barriers to supportive housing because of misconceptions about medications used for MAT.[7]
Despite the strong relationship between OUD and housing instability,[1, 2] we found few programs that specifically targeted individuals with OUD who also had housing instability. The most relevant models we identified include: the Housing First Model, other permanent supportive housing that follow housing first approaches, and recovery housing.
The Housing First model emphasizes immediate access to housing with intensive supports and case management without the preconditions of sobriety or participation in supportive services.[8] If Housing First services are integrated or coordinated with provision of MAT and substance use disorder (SUD) treatment, the model shows promise for assisting individuals with OUD and other SUDs to remain housed and attain recovery. The HHS Substance Abuse and Mental Health Services Administration and HUD recognize the Housing First Model as a best practice for reducing chronic homelessness.[5, 9] The U.S. Interagency Council on Homelessness supports the Housing First approach and a system-wide Housing First orientation.[10] Importantly, individuals served through the Housing First Model are more likely than individuals served through other programs to continue taking MAT medications as prescribed for at least three years.[11] Individuals served through the Housing First Model are also less likely to misuse substances compared to clients who are involved in programs that require SUD treatment as a condition of housing.[12]
Recovery housing programs are intended to support individuals with SUD in their recovery, often as a step-down from inpatient or residential SUD treatment. The recovery housing approach is based on the belief that individuals with a history of SUD are better off in a home environment of peer support that emphasizes abstinence. Those who treat and provide support for individuals with OUD understand that some individuals find the sober environment and peer support provided through recovery housing to be beneficial to their recovery. Some recovery housing programs serve people receiving MAT, and others do not.[13] Unlike Housing First providers,[14] the recovery housing community differs in opinion as to the appropriate role for MAT for those with OUD living in recovery housing.[15]
Also unlike Housing First,[13]recovery housing has no commonly established implementation model, and some recovery housing models consider MAT a violation of abstinence. State regulations for recovery housing programs still vary widely, and no federal regulations or standards address recovery housing.[13] Evaluations of recovery housing programs have been promising but would benefit from more-rigorous designs.
Experts interviewed as part of this study agreed that peer support, specifically support from an individual who has experienced both OUD and homelessness, is extremely important in outreach and treatment. Experts also mentioned that while co-location of services such as MAT and health care is ideal, housing programs with closely coordinated off-site services can also work well. Finally, the expert respondents in this study stressed that self-determination and individual choice of model and treatment are central to recovery and choice of housing model and treatment can vary over the course of recovery.
Staff from the programs we examined emphasized that persistence is key: staff need to continuously reach out to the population they seek to serve, to build trust. They also address other barriers such as the need for security deposits, credit histories, criminal records for drug-related offenses, and the lack of trust many individuals who experience chronic homelessness have in service providers. The programs we highlight in this issue brief work to build trust with individuals served, provide peer support services, coordinate closely with local pharmacies, engage the community, collaborate closely with health and behavioral health providers, and use funds braided from multiple sources to pay for housing, treatment, and supportive services.
Future Considerations. While some research is available, there are still major gaps in the research literature. Research is lacking that compares the Housing First EBP to other housing models for individuals and families with OUD. Additionally, we did not find programs that were specifically developed to meet the special needs of youth who were experiencing homelessness and OUD. Such research could assist individuals and providers to better understand which housing models are most effective for different populations of individuals and families with OUD before choosing a particular program. Finally, it should be understood that OUD is a chronic condition and should be treated as such. Housing and SUD treatment providers, and communities at large, could benefit from education about the nature of OUD, medications for its treatment, and the process of recovery.[16]
1. INTRODUCTION
The purpose of the Opioid Use Disorder, Housing Instability and Housing Options for Recovery project was to help the U.S. Department of Health and Human Services (HHS) Office of the Assistant Secretary for Planning and Evaluation (ASPE) and U.S. Department of Housing and Urban Development (HUD) describe the housing models available for individuals with opioid use disorder (OUD) who experience housing instability or homelessness. This issue brief presents project findings from the literature and discussions with experts and community housing providers about housing models that can best serve people with OUD who also experience homelessness or housing instability. While people experiencing homelessness have no housing at all, those experiencing housing instability experience challenges such as having trouble paying rent, living in an overcrowded space, moving frequently, staying with relatives, or spending the bulk of the household income on housing.[17]
Housing providers and substance use disorder (SUD) providers may make different assumptions, based on their own experience, about the needs of people who have both OUD and experience of housing instability or homelessness. Each type of provider may use different language to describe their services.
This brief aims to bridge these two provider worlds to foster development of programs that support both housing and OUD related needs.
2. METHODS
This section describes the research questions and methodology the project used.
2.1. Environmental Scan
As part of a scan of the published literature, the study team identified 42 articles from over 56,000 returned results that addressed the research questions. Websites of government agencies and nongovernmental organizations were also searched to scan for relevant unpublished literature, white papers, and research briefs. Organizations with known expertise in OUD and/or housing were also contacted to identify other sources; these organizations included HHS Substance Abuse and Mental Health Services Administration (SAMHSA), the National Association of County Behavioral Health and Developmental Disability Directors, the American Association for the Treatment of Opioid Dependence, Brandeis University, the Alcohol Research Group, the National Development and Research Institutes, and Washington University in St. Louis.
| Research Questions
|
2.2. Discussions with Experts
The study team conducted telephone interviews with nine experts, identified and prioritized through discussion with the ASPE COR. All experts considered for discussions had expertise at the intersection of OUD or SUD and homelessness. Experts were identified based on specific research domains to ensure that discussions addressed project priorities. Areas of expertise included high-risk populations (veterans, seniors, youth, individuals with co-occurring conditions, and people in rural areas); medication-assisted treatment (MAT); housing models; and lived experience (see Appendix C).
2.3. Discussions with Providers in Four Communities
The study team conducted telephone interviews with housing providers and collaborating partners in the communities such as MAT providers, housing developers, and a pharmacist. Communities were identified through the environmental scan, discussions with experts, and additional web searches, and the final communities were selected in consultation with the ASPE COR. All community housing providers chosen for discussions allowed people receiving MAT to be housed in their programs. Additionally, most closely collaborated with MAT providers. Two of the housing programs served families with children and two served single adults.
3. HOUSING MODELS FOR PEOPLE WITH OPIOID USE DISORDER
3.1. Populations at Risk
3.1.1. Prevalence of Housing Instability among Individuals with OUD and Other SUDs
SUD increases a person's risk of homelessness,[1, 18] and research shows SUD to be a leading cause of homelessness in the United States.[2] Individuals with SUD are more likely to be homeless for a longer time[19, 20, 21] and to have become homeless at an earlier age[22] compared to individuals without an SUD. Further, individuals with a history of illicit drug use are more likely than the general population to be unemployed and to have a criminal record, which can lead to additional barriers to accessing housing.[19]
| Many people with SUDs have poor credit histories and criminal records that make it difficult, if not impossible, to find housing and employment. |
3.1.2. OUD Prevalence among Individuals Experiencing Homelessness
Adults with a history of homelessness and SUD are very likely to report that they have misused opioids. About 72% of 296 adults who were currently experiencing homelessness when surveyed in San Francisco reported opioid misuse. About 37% of individuals surveyed reported illicit opioid use and prescription opioid misuse within the past 90 days.[23, 24]
| The extent of OUD and homelessness was hidden in one Midwest community. It was not until one person had jury duty that she learned of the extent of OUD in their community. |
Research has demonstrated,[25] and the experts we spoke with noted, that youth are particularly vulnerable to and at risk of OUD and homelessness, noting that OUD is both a cause of homelessness and a risk for youth already experiencing homelessness. Rates of prescription drug misuse are high among youth who experience homelessness, and a multi-city survey found that nearly one-quarter of youth reported misusing prescription drugs in their lifetime.[26] Opioid overdose is also more common in young adults who experience homelessness than in young adults who inject drugs but are not homeless.[27] In a Los Angeles study, 50% of 451 youth who were experiencing homelessness reported a lifetime history of prescription drug misuse, with 24.5% of youth respondents reporting prescription opioid misuse and 14.9% reporting misuse of some combination of prescription opioids and other drugs.[28]
Individuals who experience homelessness are also more likely to continue using drugs after overdose than individuals who inject drugs but are not homeless.[19] Injection drug use is more common in ZIP codes with a higher rate of homelessness.[19] Adults who experience homelessness are nine times more likely to die from an opioid overdose than adults with stable housing.[29] Many individuals with SUD who experience homelessness have co-occurring illnesses.[18, 30] The combined effect of physical illness, mental illness, and lack of housing results in higher mortality rates for individuals experiencing homelessness.[20]
| Most expert discussants identified the role of trauma in homelessness/SUD, and acknowledged that there is a strong association between trauma, SUD, and homelessness. |
Rates of illicit opioid use and prescription opioid misuse are particularly high among veterans who experience homelessness. Veterans are more likely than civilians to experience homelessness,[4] and veterans seeking treatment for OUD are ten times more likely to be homeless than veterans without OUD who seek services through the U.S. Department of Veterans Affairs.[3] Drug overdose is a major cause of death among adults who experience homelessness.[31]
3.2. Housing Models and Opioid Use Disorder Treatment Outcomes
Many program models exist to address homelessness. Regardless of model, three key features emerged from the environmental scan when considering housing projects for individuals experiencing homelessness and SUD: social support, a trauma-informed approach, and personal choice.
In a study of veterans who were experiencing homelessness in Los Angeles, many with SUD, social support was identified as critical in maintaining housing. Those in stable, independent housing relied on family, friends, and other peers such as 12-step sponsors both for practical support in finding and maintaining housing and for emotional support. Those in supportive housing predominantly used formal support such as case management to find and maintain housing. In contrast, veterans with unstable housing received only superficial support from others to find housing, described getting very little emotional support, and had informal supporters who encouraged risky behaviors.[32] Any of the housing models discussed in this brief can incorporate program elements that foster social support.
The majority of experts we spoke with stated that it was important for individuals to choose their own recovery environment, not have one prescribed to them. Furthermore, because trauma is so prevalent among people with OUD who are without housing, establishing a relationship and trust-building were identified as a key first step in engaging these individuals in housing and medication-assisted treatment (MAT).
3.2.1. Housing First Model
The most commonly endorsed housing model among experts contacted through this project was Housing First, particularly Housing First with on-site treatment and supportive services. Experts favor the Housing First Model because it does not require sobriety, which improves retention rates and subsequently the housing model's ability to provide services to individuals with SUD.[8, 12] Relapse is common among those with SUD, and the Housing First Model recognizes this reality.[11] Several research studies conducted in different cities have consistently found a housing retention rate of 85% after five years in Housing First programs.[14] Client satisfaction is similar in both Housing First programs and programs that require treatment for either mental disorder or SUD before housing.[33]
Prior to the development of Housing First, most housing providers had preconditions, such as sobriety, before a person could enter housing. Further, individuals generally had to advance through the steps of emergency shelter and transitional housing before they were considered ready for permanent housing. Housing First offers a low-barrier approach to housing, with relationships and trust built over time, to encourage engagement and retention in treatment.
In New York City, many organizations addressing homelessness have adopted the Housing First Model, notably Pathways to Housing, Inc. Implementation of Housing First has shown several positive outcomes, including higher retention rates in housing one year after program entry.[34] For example, clients in programs that implement the Housing First Model with fidelity are more likely to remain in the program one year later compared to clients in programs that identify as Housing First but actually lack some of the components of the Housing First Model.[35] Although one study found that veterans in New York City who participated in Housing First were less likely to remain in housing one year later compared to participants in other program models, this study was small, with low enrollment, so further research is needed.[36]
Housing First clients are more likely than clients in other programs to continue using MAT as prescribed for at least three years.[11] Housing First clients are also less likely to misuse substances compared to clients who are involved in programs that require SUD treatment as a condition of receiving housing.[12]
SAMHSA and HUD recognize the Housing First Model as a best practice for reducing chronic homelessness. Housing First has also been shown to reduce the use of emergency shelters, detoxification centers, jails, hospitalizations, and emergency room visits among individuals with SUD.[37] The model can be used to support integration of people without housing into the community by placing individuals transitioning out of homelessness into scattered-site apartments within the community. For example, Pathways to Housing does not rent more than 20% of the units in any one building.[14] These findings indicate that Housing First offers low-barriers to stable housing for individuals with SUD.
3.2.2. Permanent Supportive Housing
While the Housing First evidence-based practice (EBP) includes use of permanent supportive housing (PSH), not all PSH uses the Housing First or low-barrier model. PSH is targeted to households that have at least one member with a chronic disabling condition that requires ongoing support in order for the household to live independently. PSH projects provide permanent housing (either in a permanent housing property or through tenant-based rental subsidies) and supportive services to support residents' needs. Some PSH programs use the Housing First philosophy while some PSH models require SUD treatment and abstinence.[38] Several studies have been conducted concerning the success of PSH. Veterans with SUD appear to do just as well at maintaining their housing in PSH as veterans who do not have SUD.[38] However, veterans with SUD require additional services, for example SUD and mental health treatment: PSH alone has not been shown to reduce rates of substance use.[38] For the general (nonveteran) population, PSH is associated with a decline in total health costs as well as decreased substance use among individuals with an SUD.[39]
3.2.3. Recovery Housing
Recovery housing programs are intended to support individuals with SUD in their recovery, often as a step-down from inpatient or residential SUD treatment. The recovery housing approach considers that individuals with a history of SUD are better off in a home environment that emphasizes abstinence. A research review article reported that when other clients in the housing program are actively using, individuals seeking recovery from an SUD may be triggered to relapse.[15] Program policies on the use of medications such as buprenorphine while in recovery housing vary. Recovery housing programs vary according to what they consider being "drug free". Some programs consider MAT medications as drugs, which may limit access to recovery housing for persons receiving MAT for their OUD.[40] The National Association of Recovery Residences developed quality standards for recovery residences.[41] All recovery residences must:
Have a clear mission and vision, with forthright legal and ethical codes. This includes requirements to be financially honest with prospective residents.
-
Be recovery-oriented and prohibit the use of alcohol or illicit drugs.
-
Have a role for peers to staff and govern the housing.
-
Uphold residents' rights.
SAMHSA recently held a meeting, "Recovery Housing: Establishing Best Practices That Support the Inclusion of People Receiving Medication-Assisted Treatment" to assist SAMHSA to develop a guidance document on best practices and recommendations for supporting people living with OUD, both with and without medications, in recovery housing.
Policies related to recovery housing vary state by state.[13] To obtain certification from the National Alliance for Recovery Residences (NARR), a recovery residence must provide a place for residents to store their prescriptions securely, as well as the ability to take medications as prescribed.[42] Recovery housing programs may refuse to admit individuals participating in MAT when the residence is not adequately staffed to accommodate medication supervision. In such cases, NARR recommends that clients be referred to alternative programs.[42, 43]
There is limited research on the effectiveness of recovery housing in assisting residents to maintain housing and decrease substance use. Recovery housing has been shown to improve clients' functioning, including better employment and treatment outcomes and reduced criminal activity;[15] but these studies have had a number of limitations, including inconsistent definitions of "recovery housing," small sample sizes, and outcomes from a single-site without a comparison group.
3.2.4. Housing Choice
Housing Choice, developed by Central City Concern in Portland, Oregon, is a combined approach that incorporates elements of both recovery housing and Housing First to allow individuals to select housing based on their personal needs. Individuals can choose from a range of housing options, including transitional housing, PSH, family housing, Housing First, and recovery housing.[44] Individuals who choose the recovery housing option may enter the program through self-initiated detox or residential detox, and then are placed in a recovery community setting and provided with short-term rental assistance.[44] Integrated health care with specialty addiction and mental health services, including MAT, as well as supported employment, are offered on-site and nearby.[6, 44] Housing Choice's recovery housing includes a range of treatment options, including primary care, outpatient treatment, and MAT.[44] Recovery housing is offered as both a transitional and a permanent option, but individuals actively using are still accepted into the program and offered professional and peer support. On average, short-term recovery housing through Housing Choice costs $9,894 for six months, compared to $27,480 for a four-month placement in residential treatment.[44] The Housing Choice model is currently being evaluated, so outcome data are not available.
3.3. Medication-Assisted Treatment
MAT, which includes pharmacotherapy and counseling, is the EBP for OUD.[5] MAT has been shown to improve outcomes for people living with OUD compared to counseling alone,[45] but patients who receive MAT face considerable stigma.[46, 47] Numerous court cases have found that individuals in recovery from an OUD and engaged in MAT are protected under the ADA and Fair Housing Act, but many patients as well as SUD treatment and housing professionals are unaware of these legal protections.[47, 48] Individuals receiving MAT to support their recovery are protected by the ADA if the housing residence receives state or local government funding, and by the Rehabilitation Act if the residence receives federal financial assistance.[48] People receiving MAT to support their recovery cannot be excluded from a residence due to their health condition, nor can the residence prohibit them from participating in MAT.
| People with SUDs are not recognized as disabled by many federal programs, so it is often not known when policies do apply to this population. |
Currently in the United States, three medications are approved for MAT: methadone, buprenorphine, and naltrexone. These HHS Food and Drug Administration (FDA)-approved medications come in several formulations. Methadone is available only through a certified opioid treatment program (OTP). Buprenorphine may also be prescribed outside an OTP in office-based settings by a physician, physician assistant, or nurse practitioner who meets the statutory requirement for a DATA2000 waiver. Unlike methadone and buprenorphine, naltrexone is not a federally controlled substance and may be prescribed by any health care provider with prescribing authority.
| MAT was endorsed as the evidence-based treatment for individuals with OUD by experts from different subject matter backgrounds (i.e., research, implemented response, lived experience). |
The following MAT models have been implemented with populations experiencing homelessness. Office-based opioid treatment (OBOT) has been demonstrated to work among individuals without housing.[49] However, clinical guidelines, such as a requirement to attend the clinic at a particular time, pose a barrier to access to OBOT for individuals without stable housing.[50, 51]
| Avalon participates in the local opioid workgroup, which engages in systems-level advocacy. Staff are well educated to recognize when MAT might be an appropriate treatment pathway for a client and to work with providers accordingly. Peer specialists accompany clients on methadone to the OTP and work with the providers who prescribe different medications. |
A number of innovative delivery approaches of MAT have shown positive outcomes for those less likely to participate in MAT because they are unstably housed. Depending on their region of the country, unstably housed individuals may not have connections with physicians able to prescribe MAT.[6] The Stepped Treatment Engagement Program (STEP) was developed in order to provide MAT for hard-to-reach populations. Research indicates that providing buprenorphine treatment in nontraditional treatment settings, such as shelters, community-based recovery centers, and needle exchange programs improves access to treatment and recovery among underserved populations.[52] STEP combines buprenorphine and syringe services in a nontraditional treatment setting to engage individuals without housing.[52] In a STEP pilot program with needle exchange clients that included medical intake, buprenorphine detoxification, peer support, drug testing, and SUD counseling, 78% of participants completed the program and 33% entered long-term MAT.[52]
| SUDs are not linear, so housing models and recovery services should be flexible to the different stages of recovery. |
Community-based recovery centers provide another location in which to provide MAT in nontraditional settings. Research has shown high rates of abstinence and treatment adherence, and locating such programs close to underserved communities and existing supportive services can improve access.[53] A study of clients served in a buprenorphine treatment program at a community-based recovery center in Baltimore found that clients were highly likely to resist opioid use and remain in compliance with their buprenorphine prescription. At the end of the program, about half of clients successfully transitioned into buprenorphine treatment in primary care settings.[53]
The Boston Health Care for the Homeless Program has developed and now uses an intervention to treat OUD at a family shelter.[54] Physicians provide buprenorphine on site at the shelter, to address transportation and childcare barriers that prevent patients from coming to the physician's office. The program also includes intensive case management and psychotherapy for co-occurring mental health conditions. After three months in the program, participants had fewer positive urine screens for opioids and fewer positive results for unexpected urine drug tests. The number of employed participants increased, and the overdose rate decreased.[54]
| Shop and Carry Pharmacy The pharmacist communicates with Pathways PA physicians on client cases and uses the Prescription Drug Monitoring Program to check the client's prescription history and instances of multiple prescribing that could indicate "doctor shopping" for prescriptions. |
The Downtown Emergency Service Center (DESC) in Seattle aims to bring MAT to clients in locations where they are comfortable, through health care providers located within emergency shelters, in outpatient behavioral health clinics, and at DESC's supportive housing locations.[6] Pathways to Housing PA partners with a local pharmacy to deliver MAT prescriptions to supportive housing sites.[55] Avalon Housing also works closely with a local pharmacy for blister-packing medications. These strong collaborations with local pharmacies may be a promising strategy to address many of the challenges of ensuring access to medication for individuals receiving MAT.
4. INTEGRATION OF MEDICATION-ASSISTED TREATMENT, HOUSING, CASE MANAGEMENT, AND HEALTH SERVICES
Experts we spoke with agreed that MAT alone is insufficient, and for long-term stability MAT should be combined with a range of supportive services. For example, employment services can assist people to be self-sufficient and provide hope for recovery. The programs we explored in depth combine supportive housing, primarily using the Housing First Model, with numerous support services, and on-site or linkages to health services and MAT. Some experts also noted the need to braid funding for rental assistance and services through community and foundation grants and other sources.
Discussions with housing providers revealed that they integrated or coordinated a wide variety of services, including MAT, SUD services, health care, and supportive services. Exhibit 1 shows the choices that housing providers can make when deciding on housing models, MAT, supportive services, and housing settings to meet the needs of those with OUD who experience homelessness or housing instability.
The housing typology (Appendix A) outlines the different housing models by populations, along with options for siting of housing, coordination or integration of MAT, health, and behavioral health services, and supportive services.
| EXHIBIT 1. Housing and Support Options to Promote OUD Recovery |
|---|
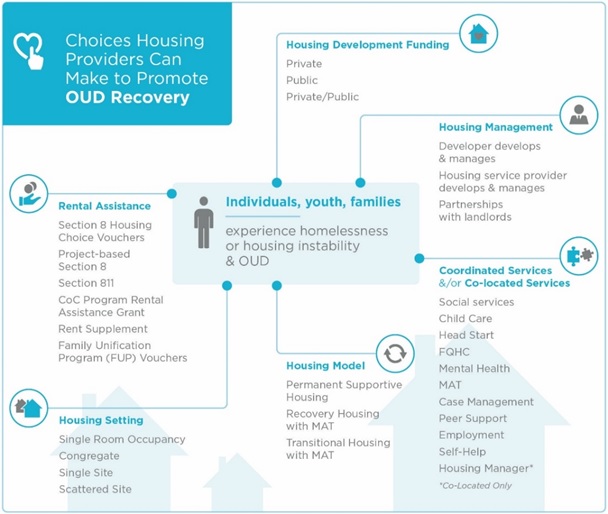 |
| NOTE: Housing First is a model of PSH. |
4.1. Brief Community Provider Profiles
This section includes overviews and brief profiles from discussions with housing and MAT providers in four communities. The profiles provide examples of the array of housing programs that can serve individuals and families with OUD and a variety of funding streams used to support rental assistance. As shown in the work of the profiled providers, housing providers may consider strengthening partnerships with local medical providers to ensure success of MAT in their clients who receive it.[55] Leaders of housing and employment programs may consider bringing MAT providers into the discussion when new program elements are being designed, to ensure that the homeless population with OUD are guaranteed access to MAT.[56]
4.1.1. HousingNow: A Housing First Model using Harm-Reduction Strategies
Pathways to Housing Pennsylvania (PA) has operated a high-fidelity Housing First program with intensive supports for individuals with serious mental illness (SMI) and SUD since 2008. In 2017, with support from the City of Philadelphia, in 2017 they created HousingNow to serve individuals with OUD who were experiencing homelessness.
The treatment model follows three main pillars:
-
Recognizing that complex prior trauma lies at the root of clients' addiction, and that clients need to be able to define recovery on their own terms in order to avoid re-traumatizing them in the housing system.
-
Making MAT easier to get than heroin and other illegal opioids.
-
Not penalizing people for showing symptoms of a disease for which they are seeking help.
A central characteristic of Pathways' treatment model is that there is no prolonged intake. MAT services are available at the co-located Pathways Federally Qualified Health Center (FQHC) office satellite site at Pathways and at the main FQHC partner site. Pathways staff also conduct home visits and will even go out onto the streets to provide treatment to clients.
A key part of the program is the strong relationship with a local pharmacy to assist with medication compliance and accessibility of MAT. Case managers and nurses monitor MAT and other medications. Pathways will provide MAT to individuals who still have benzodiazepines in their drug screens, while working closely with them to stop use of nonprescription benzodiazepines and work with them to transfer to a higher-level of care if needed. In Philadelphia, people experiencing homelessness who use heroin are also often using benzodiazepines, which can pose a significant barrier to treatment access. Some clients benefit from starting on methadone prior to transitioning to buprenorphine, because the daily administration of methadone provides structured contact with the service provider. Conversely, some individuals start with buprenorphine, but realize they would benefit from the structure of methadone maintenance, and Pathways works with them to transfer to a methadone maintenance program. OTPs are the main outside provider for MAT, as well as detox providers and 30 day inpatient treatment.
HousingNow has been operating for only 17 months; therefore, long-term retention outcomes are not yet available. However, the program has seen 100% retention for the past 17 months.
4.1.2. Avalon Housing, Housing First Model Focused on Coordinating Care for High-Needs Individuals
Avalon Housing is a supportive housing provider, real estate developer, and service provider for individuals transitioning out of homelessness. Avalon has been in operation for 25 years and has always used a Housing First approach. For past three years, Avalon has been involved in the community's coordinated entry system, which is used to identify and prioritize housing for the hardest-to-house population.
Five years ago, Avalon was one of four agencies involved in a demonstration of the Frequent Users System Engagement (FUSE) model.[57] Through the FUSE demonstration, Avalon participated in a large randomized controlled trial that examined the cost impact of supportive housing for frequent users of crisis services.[58] As part of the FUSE initiative, Avalon recognized the population of individuals struggling with chronic homelessness who were also impacted by OUD, and began to consider ways to better support this population. Avalon's partners, including FQHCs, Washtenaw County Community Mental Health, and SUD treatment organizations, provide traditional clinical supports. Avalon provides harm reduction services, including syringe services and case management. Avalon also conducts community-building initiatives such as innovative youth programming. Staff are well educated to recognize when MAT might be an appropriate treatment pathway for a client and to work with providers accordingly. All staff are also trained in the use of naloxone. Peer specialists accompany clients on methadone to the OTP and work with the providers who prescribe different medications. They also work closely with a local pharmacy that provides blister-packaging of medications.
4.1.3. HomeSafe, A Keeping Families Together Model
HomeSafe is a program funded through the State of New Jersey using the Keeping Families Together (KFT) model developed by the Corporation for Supportive Housing and first piloted from 2007 through 2010 in New York.[59] The KFT targets families who have had multiple contacts with the child welfare system, families with members with SUD, including OUD, and families experiencing housing instability. The program provides housing and supportive services for the whole family. The New Jersey Department of Children and Families awarded FamilyConnections the funds for the New Jersey KFT pilot program, HomeSafe, in 2014. Since then KFT has moved out of the pilot phase, with KFT programs in five counties as of 2017.
Under KFT's Housing First approach, services are not mandatory but are strongly encouraged. The clinical team consists of a manager and three clinicians, and the case management team includes three housing case managers, an employment specialist, and a parent advocate. Each staff person has a case assignment of about 15 families. SUD services are co-located with MAT delivered by outside providers. Employment services include a fiscal fitness program, job training, and assistance connecting participants to local employers. HomeSafe staff work with local employers to build relationships and facilitate employment of participants. For families receiving Division of Mental Health and Addiction Services subsidized vouchers, HomeSafe will continue to pay rent for a family's apartment for up to six months if the parent is in treatment, so that the parent will have housing after treatment to support the case for reuniting the parent with the children. Case conferences are essential to the coordination of services between FamilyConnections HomeSafe and the Division of Child Protection and Permanency (DCPP). During case conferences, FamilyConnections can coordinate with DCPP to ensure that all providers are on the same page about how to support families in the program with SUD, including OUD. The overarching goal for both HomeSafe and DCPP is for the family to be stabilized and reunified, and their child welfare case to be closed.
4.1.4. Pearl House, a Supportive Housing Program for Families
Pearl House has 21 two-bedroom apartments that provide PSH for families impacted by SUDs, including OUD. The apartment building also offers a children's room, a common room with computers, a living room, and a large kitchen. Head Start has been co-located on site for about 1.5 years, a first for the state. The Pearl House initiative began approximately 3.5 years ago to meet the need for a residential program specific to families with OUD who were experiencing chronic homelessness. Fairfield Homes, a for-profit housing developer, partnered with the Recovery Center, an outpatient mental health and substance abuse treatment facility, the Metropolitan Housing Authority, and the Lancaster-Fairfield Community Action Agency to develop PSH for low income families with OUD. Fairfield Homes is the landlord and property manager, Fairfield Metropolitan Housing Authority provides the housing vouchers, and the Lancaster-Fairfield Community Action Agency helped develop the building, provides resources, and runs the local on-site Head Start Program.
Pearl House focused on families because there were already housing programs for individual adults in the community. Most people who move in are at very early stages of recovery. To live at Pearl House, individuals are required to have children in their custody, though a few have shared parental custody or are in the process of being reunified with their children. A number of families have been reunited once parents have obtained housing. The goal is to help parents reunify with their children. Clients usually are involved with the Recovery Center for 14-18 months at various stages of treatment and recovery services. Staff report that families have completed the program and are doing well, but they do not collect data on successes.
| Avalon Housing Ann Arbor, Michigan |
|---|
| Housing Model: Housing First Population Served: Individuals and families who experience chronic homelessness. OUD Service Integration/Coordination of MAT:
Social and Health Services:
Partners:
Staffing: Case managers, recovery coach-certified peer specialists, housing staff; every resident has an assigned case manager and peer specialist. Data on Outcomes: No data on services for people with OUD, but Avalon was part of the 5-year FUSE demonstration evaluation, which used a randomized controlled trial design.[1] Property Management: Avalon develops and manages its own properties and works with local landlords to secure housing. Financing:
|
| Avalon provides case management 24/7, 365 days/year, and every client has a case manager. Avalon also has peer specialists who are certified recovery coaches. Avalon provides medication management but does not administer medication. |
|
| HousingNow (Pathways to Housing, PA) Philadelphia, Pennsylvania |
|---|
| Housing Model: Housing First Population Served: Individuals with OUD who experience homelessness. OUD Service Integration/Coordination of MAT:
Social and Health Services:
Partners:
Staffing:
Data on Outcomes:
Property Management: Does not manage property but works closely with local landlords and pays for any damages. Financing:
|
| Pathways to House, PA partnered with Project HOME's FQHC to become a FQHC satellite site. Because most of their population has experienced difficulty getting into OUD treatment, Pathways applied to the state to become a Center for Excellence in OUD so they can provide buprenorphine/naloxone and naltrexone in their clinic. MAT services are available at the Pathways office satellite site and the main FQHC partner site, and Pathways staff do home visits, and will even go out onto the streets to provide treatment to clients. |
|
| HomeSafe (FamilyConnections, NJ) Essex, Passaic and Hudson Counties, New Jersey |
|---|
| Housing Model: PSH using CSH's Keeping Families Together (KFT) program model.[1] Housing is provided in both project-based and scattered-site settings. Population Served: Families involved in the child welfare system who are affected by SUD, SMI, and housing instability. OUD Service Integration/Coordination of MAT: Parents with OUD are receiving MAT when referred to the program by the Department of Children and Families, DCPP. Socials Services:
Partners:
Staffing:
Data on Outcomes: None available other than CSH evaluation of KFT. Property Management: Work closely with area landlords. Financing:
|
| HomeSafe works with local employers to build relationships and facilitate employment of participants. |
|
| Pearl House Lancaster, Ohio |
|---|
| Housing Model: Single-site PSH. Population Served: Families affected by OUD and housing instability. OUD Service Integration/Coordination of MAT:
Socials Services:
Partners:
Staffing:
Data on Outcomes: Not available. Fairfield Homes is replicating an adapted model in another location. Property Management: The building, with 21 2-bedroom apartments, was developed by Fairfield Home, which owns and manages it. Services are provided. Financing:
|
| Pearl House has 21 2-bedroom apartments that project PSH for families impacted by SUDs, including OUD. The apartment building also offers a children's room, a common room with computers, a living room, and a large kitchen. Head Start has been co-located on-site for about 1.5 years, a first for the state. Community members come to the facility to offer outreach to residents about budgeting, riding a city bus, etc. |
5. GAPS IN THE EVIDENCE BASE
While this project identified research and promising models relating to serving individuals with OUD who are experiencing homelessness, there were significant gaps in the evidence base. We did not identify research related to understanding which models and which types of housing arrangement (scattered-site or single-site) might work best for individuals and families with OUD. No literature was found related to rapid re-housing and individuals with OUD, nor was literature found relating to the success of transitional housing in the population of individuals with OUD, despite extensive funding for transitional housing programs. We did not identify any studies with side-by-side comparisons of various housing models to serve people with OUD.
Many studies have described the association between OUD and homelessness. However, much less evidence exists to describe the pathway by which OUD may lead to homelessness. If we understand this pathway better, we may be able to develop efforts to prevent homelessness in individuals with OUD.
Youth and young adults with OUD and experiencing homelessness are typically designated "special populations" in the fields of SUD and housing. This study did not find examples of housing models developed to serve these special populations, despite existing literature on the prevalence of opioid misuse among youth who are homeless. In addition, age restrictions included in shelter policies and state-level MAT policies prevent youth and young adults from getting housing services developed for the general adult population.[60]
6. FUTURE CONSIDERATIONS
Although MAT has been well documented[51] to assist in recovery from OUD, individuals experiencing homelessness can have more difficulty adhering to MAT that individuals in stable housing.[55] Still more concerning is that opioid overdose is more common in individuals who experience homelessness than in individuals who inject drugs but are not homeless.[27]
The discussions with experts and program staff emphasized that it is crucial to support individuals and families in choosing the housing and services that work best for them at each stage of recovery and individuals may want to move between models at different points in time. The models of Housing First, PSH, and recovery housing all show promise when the individuals experiencing OUD have chosen that type of housing.
Given the current opioid epidemic in the United States, and the association between OUD and homelessness, more-rigorous research is urgently needed to identify whether there are housing models that most efficiently and effectively assist individuals to access treatment and achieve both recovery and housing stability, particularly for subpopulations that may have special needs.
The Housing First Model is particularly promising; at least one study has shown that individuals served through Housing First are more likely than those served by other models to remain adherent to MAT,[11] and they are less likely to misuse substances than individuals who are required to engage in SUD treatment as a condition of receiving housing.[32] While the outcomes of the Housing First Model are promising, comparative effectiveness studies could assist policymakers and providers to prioritize scarce resources to address the needs of people with OUD who experience homelessness or housing instability.
According to expert and provider discussants, use of multiple funding streams and strong local partnerships are key to successful housing programs. Partnerships that increase access to housing subsidies for individuals with OUD similar to those for individuals with mental illness could significantly strengthen housing stability for this group. In many locations, affordable housing is scarce or nonexistent, which limits options for individuals and providers seeking safe affordable housing.[61] Housing developers can also play a role in making more affordable housing solutions available, through creative partnerships and by developing affordable housing specifically targeted for this group.
The literature review and discussions with subject matter experts and providers revealed that stigma is still a major barrier to both housing and OUD treatment, and that clarity is lacking about civil rights protections for individuals beginning their recovery through MAT. Federal law prohibits housing discrimination against individuals receiving MAT to support their recovery.[48] However, individuals receiving MAT may experience challenges when living in recovery residences that use an abstinence-only approach to SUDs. MAT patients have faced considerable stigma, not only from the general population, housing programs, and landlords, but also from fellow individuals in recovery who are not using MAT; this is referred to as "double stigma."[7]
Experts agreed that peer support, specifically support from an individual who has experienced both OUD and homelessness, is important in outreach and treatment. Co-location of medical treatment and MAT is ideal, but housing programs with closely coordinated off-site services can also work well.[18, 62] Integrating employment training and opportunities into housing programs for people with OUD can increase hope for recovery and lead to self-sufficiency.[18] Such opportunities for integration warrant further study.
Housing approaches for youth and young adults who experience homelessness and OUD are particularly needed. Youth and young adults who experience homelessness have fewer available housing options, often have histories of trauma, and are at high risk for OUD.[18] Research on programs for this population is needed.
Approaches to supportive housing that emphasize choice for individuals with OUD offer both the supports and opportunities for individuals to enter into and maintain recovery.[6] Opportunities should be explored to both support the adoption of housing models that assist people with OUD in their recovery and to empirically study the impacts of these models. This study made clear that there is a need for provider and community education about the fact that OUD is a chronic disorder and that individual paths to recovery vary. While research is needed to identify which housing models might benefit which populations, individual choice of housing and services is essential to support individuals over the course of their recovery.
APPENDIX A. HOUSING TYPOLOGY
| Housing Model | Populations | Timeframe | Housing Setting | MAT | Health Care/Behavioral Health | Support Services Include/May Include |
|---|---|---|---|---|---|---|
| Housing First Model[1] | Single adults or families who experience chronic homelessness, including people with OUD | Unlimited | Scattered-site Single-site | Coordinated Co-located | Coordinated Co-located | Intensive case management Medication management (in most cases) Pharmacy services Peer support Linkage to other services Landlord support Rental assistance |
| Other Permanent Supportive Housing | Prioritized for people experiencing chronic homelessness and disability, families where parent SMI, traumatic brain injury, etc.[2] | Unlimited | Scattered-site Single-site | May or may not accept a person receiving MAT | Coordinated Co-located | Case management (long-term or short-term) Peer support Linkage to other services Landlords Rental assistance |
| Keeping Families Together[3] | Families involved in the child welfare system who are affected by SUD, SMI, and housing instability | Unlimited | Scattered-site Single-site | Serve people with SUDs including OUD | Coordinated Co-located | Case management Family preservation Coordination with child welfare Parenting skills Job training Life skills training Domestic violence services Peer support Crisis support Landlord support |
| Recovery housing | People in recovery from OUD and other SUDs, most often post-treatment | Usually time-limited | Congregate Single-site | May or may not accept person receiving MAT | Varies | Peer recovery support Counseling Referrals to other support services |
| Transitional housing | Individuals who need time-limited supports to address gaps in housing because of domestic violence, discharge from mental or SUD inpatient, or as transition from shelter | Time-limited | Congregate Scattered-site | No data | Coordinated | Case management with initially intensive supports that decrease over time individuals may transition between levels in the program Peer support Referrals to other services |
| Rapid re-housing | Individuals who need short-term rental assistance and engagement to obtain housing stability[4] | Time-limited | Scattered-site | No data | Client directed | Brief case management Lease assistance Linkage to supportive services Crisis resolution Short-term rental assistance |
| Housing Choice[5]: Individual choice of transitional housing, rapid re-housing; housing first; or recovery housing | People experiencing chronic homelessness--people have a choice of housing model | Varies | Scattered-site Single-Site | Coordinated Co-located | Coordinated Co-located | Case management Peer support Supported employment Rental assistance Crisis services Linkage to supportive services |
NOTES:
| ||||||
APPENDIX B. GLOSSARY OF TERMS
| Term | Definition | ||
|---|---|---|---|
| Behavioral health services | Services for people with a mental and/or substance use disorder diagnosis. Includes clinical and supportive services. | ||
| Opioid use disorder (OUD) | A problematic pattern of opioid use leading to clinically significant impairment or distress. | ||
| Medication-assisted treatment (MAT) | Combination of medication and behavioral therapies used to treat OUD. Three FDA-approved medications are used in MAT: methadone, buprenorphine, and naltrexone for treatment of an OUD. | ||
| Medication-assisted recovery[1] | An approach to treating individuals with SUD using counseling, social and peer supports and services, and medication therapy to help individuals achieve and maintain recovery over the long term. | ||
| Opioid treatment program[2] | A specialized program where MAT is provided. | ||
| Buprenorphine waiver[3] | Physicians, physician assistants, and nurse practitioners may complete additional training to obtain a waiver to prescribe buprenorphine in office-based settings. Also known as Data2000 practices. Providers are limited to 30 patients in the first year and may apply to increase treatment to 100 patients. Physicians who have prescribed buprenorphine to 100 patients for at least 1 year may apply to increase treatment to 275 patients. | ||
| Housing instability[4] | A situation where an individual family has a place to stay but housing is not stable. Examples include being doubled up living with family or friends, being at risk of eviction, and not having enough money for food, basic needs, and housing. | ||
| Chronic homelessness[5] | A situation in which a person has lived in a place not meant for human habitation, a safe haven, or an emergency shelter, either continuously for at least 12 months or on at least 4 separate occasions totaling at least 12 months within the last 3 years. A person must have a disability to meet the federal definition of chronic homelessness. A high proportion of individuals experiencing chronic homelessness have severe mental illness and/or an SUD. | ||
| Housing First | A low-barrier approach to connecting individuals and families who have experienced homelessness to permanent housing without preconditions and barriers to entry, such as sobriety, treatment, or service participation requirements. | ||
| Rapid re-housing | Time-limited rental assistance for individuals or families who have lost housing or are experiencing housing instability. The aim is to move people rapidly into housing to reduce the harmful effects of homelessness on families and individuals. | ||
| Permanent supportive housing (PSH) | Subsidized housing combined with case management and linkages to intensive services to support individuals with behavioral health and other conditions or disabilities. Neither housing assistance nor services are time-limited. | ||
| Transitional housing | Time-limited housing to help adults, youths, and/or families who experience homelessness to gain work and permanent housing. Frequently used with individuals newly in recovery, transitioning from other settings. Case management, behavioral health treatment, and supportive services are provided. | ||
| Residential re-entry center/halfway house | Time-limited congregate housing that offers treatment on site to help individuals with severe behavioral disabilities and/or criminal records to reintegrate back into the community. Participation in treatment is tied to housing. | ||
| Recovery housing | Short-term or longer-term substance-free housing with recovery supports. Some recovery housing providers serve people who are receiving MAT, while others do not. | ||
| Continua of Care[6] | A term used by HUD to describe community-wide coordinated approaches aimed at preventing and ending homelessness. A goal of the Continuum of Care is to implement central access to help individuals/families at risk of homelessness or those who are homeless to find housing and supports. | ||
| Case management | Case management includes needs assessments, service planning, and monitoring, as well as coordination and linkages to services and supports, with the aim of improving an individual's wellbeing. Case management services can be time-limited or ongoing. They can be focused solely on housing and employment, health, behavioral health, or all aspects of a person's life. | ||
| Harm reduction | Approaches and policies meant to mitigate the negative effects of human behavior. Such approaches also aim to help individuals avoid behaviors that put them at risk, and reduce the negative effects of some dangerous behaviors. | ||
| Fair Housing Act (Title VIII of the Civil Rights Act) | The Fair Housing Act forbids discrimination in the sale or rental of housing based on a person's race, color, religion, sex, familial status (e.g., children or marital status), national origin, or handicap/disability. | ||
| Service integration | Well-coordinated behavioral health, housing, social, and/or health services, sometimes co-located in 1 site and provided by 1 team. The aim is to make sure that all providers work together to coordinate their services to treat/support the whole person. | ||
| Holistic model of care | A model that takes the whole person into account: physical, emotional, spiritual, social, intellectual, and financial wellbeing. Holistic models are premised on the fact that stable housing is essential to good health and wellbeing. | ||
| Wraparound | Services that are "wrapped" around the individuals to make sure that the person's needs for stable housing and recovery are met. May include employment services, budgeting, child care or family interventions, transportation, peer supports, and other services. | ||
| Patient-centered[7] | Process by which individuals are provided with information they need in a format they can understand, so that they can make decisions about their own services/treatment, in partnership with providers. Services are voluntary and flexibly provided to meet needs of the individual or family, in a way that is acceptable, and when services are needed. | ||
| Health Homes[8] | A Medicaid program option where FQHCs, community mental health centers, or primary care practices and partners offer coordinated, integrated services and supports for people with 2 or more chronic conditions, including people with OUD. States must include Health Home services in their state Medicaid plans for services to be reimbursed by Medicaid for eligible individuals. | ||
| Patient-centered medical home[9] | Aims to provide comprehensive care that is patient-centered, coordinated, accessible, and of high quality. Treatment teams can consist of doctors, nurses, nurse practitioners, case managers, behavioral health clinicians, health educators, pharmacists, and nutritionists. | ||
| Patient navigation | Behavioral health care, health care, and other service systems can be difficult to navigate. Systems and providers can use terms differently and have different rules. Patient navigators help individuals get through the system to needed services and to understand treatment/service options. Navigators can act as advocates, can provide transportation, and participate in appointments. Navigators can work in housing programs, health clinics, and other settings. They may be peers or other staff. | ||
| Patient, client, resident, individual, program participant | Different systems use different terms when referring to individuals they serve. For example, opioid treatment providers refer to the individuals they treat as "patients" because they are providing a medical intervention. Individuals served through mental health systems are often referred to as "clients" or individuals who are "receiving treatment." Housing providers refer to individuals they serve as "residents," while other service providers may use the term "program participant." Each of these terms is used in this report, depending on the literature cited. | ||
NOTES:
| |||
APPENDIX C. EXPERT DISCUSSANTS AND COMMUNITY PROVIDERS
Expert Discussants
-
Suzanne Borys, EdD, Assistant Division Director of the New Jersey Department of Health Division of Mental Health and Addiction Services
-
Lori Criss, MSW, LSW, Vice President of the National Alliance of Recovery Residences and the Associate Director of the Ohio Council of Behavioral Health and Family Services Providers
-
Leon Evans, former President and CEO of the Center for Health Care Services in San Antonio, TX
-
Terrye Sukari Finley, member Los Angeles Health Center Board of Directors and the National Healthcare for the Homeless Council Consumer Advisory Board Steering Committee
-
Jessie Gaeta, MD, Chief Medical Officer at Boston Health Care for the Homeless Program
-
Stefan Kertesz, MD, Professor in the Division of Preventive Medicine at the University of Alabama School of Medicine
-
Rachel Post, LCSW, Senior Consultant at Health Management Associates
-
Brian and Neli Rowland, Co-Founders of A Safe Haven, Inc., with Martin Wah, MD
-
Paul Toro, PhD, Professor of Psychology and the Director of the Research Group on Homelessness and Psychology at Wayne State University
Community Provider Contacts
| Provider Agency | Point of Contact |
|---|---|
| Avalon Housing | Audrey Patiño Executive Director |
| HomeSafe (Keeping Families Together, NJ) | Alexandria Riley, LPC Director of Programs |
| Pathways to Housing PA | Christine Simiriglia, MS President & CEO |
| Pearl House | Trisha Farrar, CEO |
REFERENCES
-
National Alliance to End Homelessness. (2016). Opioid Abuse and Homelessness. Retrieved from https://endhomelessness.org/resource/opioid-abuse-and-homelessness/. Accessed on December 4, 2017.
-
U.S. Conference of Mayors. (2008). Hunger and Homeless Survey: A status report on hunger and homelessness in America's cities. Washington, DC: U.S. Conference of Mayors.
-
Bachhuber, M.A., Roberts, C.B., Metraux, S., & Montgomery, A.E. (2015). Screening for homelessness among individuals initiating medication-assisted treatment for opioid use disorder in the Veterans Health Administration. Journal of Opioid Management, 11(6), 459-462.
-
National Alliance to End Homelessness. (2015b). Veteran Homelessness. Retrieved from https://endhomelessness.org/resource/veteran-homelessness/. Accessed on December 4, 2017.
-
Substance Abuse and Mental Health Services Administration. (2015). Federal Guidelines for Opioid Treatment Programs. Rockville, MD: SAMHSA.
-
U.S. Interagency Council on Homelessness. (2017). Successfully Connecting People Affected by Opioid Use to Housing: Central City Concern in Portland, Oregon. Retrieved from https://www.usich.gov/resources/uploads/asset_library/case-study-central-city-concern-march-2017.pdf.
-
Shinholser, J. (2016). Medication-Assisted Treatment Housing [PowerPoint slides]. Presented at the National Alliance for Recovery Residences Conference 2016, Boston, MA.
-
Tsemberis S. (2010). Housing First: The Pathways Model to End Homelessness for People with Mental Illness and Addiction. Center City, MN: Hazelden Press.
-
U.S. Department of Housing and Urban Development. (2016). Notice on Prioritizing Persons Experiencing Chronic Homelessness and Other Vulnerable Homeless Persons in Permanent Supportive Housing. Retrieved from https://www.hudexchange.info/resources/documents/notice-cpd-16-11-prioritizing-persons-experiencing-chronic-homelessness-and-other-vulnerable-homeless-persons-in-psh.pdf.
-
U.S. Interagency Council on Homelessness. (2018). Deploy Housing First Systemwide. Retrieved from https://www.usich.gov/solutions/housing/housing-first/.
-
Appel, P.W., Tsemberis, S., Joseph, H., Stefancic, A., and Lambert-Wacey, D. (2012). Housing First for severely mentally ill homeless methadone patients. Journal of Addictive Diseases, 31(3), 270-277.
-
Padgett, D.K., Stanhope, V., Henwood, B.F., and Stefancic, A. (2011). Substance use outcomes among homeless clients with serious mental illness: Comparing Housing First with Treatment First programs. Community Mental Health Journal, 47(2), 227-232.
-
National Council for Behavioral Health. (2018). Building Recovery: State Policy Guide for Supporting Recovery Housing. Washington, DC: National Council for Behavioral Health.
-
Tsembris, S., & Henwood, B. (2013). Housing First: Homelessness, recovery and community integration. In V. Vandiver (Ed.), Best Practices in Community Mental Health: A Pocket Guide. Chicago, IL: Lyceum Books, Inc.
-
Reif, S., George, P., Braude, L., Dougherty, R.H., Daniels, A.S., Ghose, S.S., & Delphin Rittmon, M.E. (2014). Recovery housing: Assessing the evidence. Psychiatric Services, 65(3), 295-300.
-
HHS Office of the Surgeon General. (2016). Facing Addiction in America: The Surgeon General's Report on Alcohol, Drugs, and Health. Washington, DC: HHS.
-
HealthyPeople.gov. (n.d.) Housing Instability. Retreived from https://www.healthypeople.gov/2020/topics-objectives/topic/social-determinants-health/interventions-resources/housing-instability.
-
Saxon, A., & Malte, C.A. (2017). Intensive Addiction/Housing Case Management (AHCM) for Homeless Veterans in Substance Use Treatment [Webinar]. Retrieved from https://va-eerc-ees.adobeconnect.com/_a1089657440/p47ededfwcvg/.
-
Linton, S.L., Celentano, D.D., Kirk, G.D., & Mehta, S.H. (2013). The longitudinal association between homelessness, injection drug use, and injection-related risk behavior among persons with a history of injection drug use in Baltimore, MD. Drug and Alcohol Dependence, 132(3), 457-465.
-
National Health Care for the Homeless Council. (2016). Medication-Assisted Treatment: Buprenorphine in the HCH Community. Nashville, TN: National Health Care for the Homeless Council.
-
Spinner, G.F., & Leaf, P.J. (1992). Homelessness and drug abuse in New Haven. Hospital and Community Psychiatry, 43(2), 166-168.
-
Cambioli, L., Maremmani, A., Bacciardi, S., Nikoo, N., Addorisio, S., Gehring, N., Krausz, M. (2016). Are substance use and mental illness associated to an earlier onset of homelessness? Mental Health in Family Medicine, 12, 205-212.
-
Hansen, L., Penko, J., Guzman, D., Bangsberg, D., Miaskowski, C., & Kushel, M.B. (2011). Aberrant behaviors with prescription opioids and problem drug use history in a community-based cohort of HIV-infected individuals. Journal of Pain and Symptom Management, 42(6), 893-902.
-
Vijayaraghavan, M., Penko, J., Bangsberg, D.R., Miaskowski, C., & Kushel, M.B. (2013). Opioid analgesic misuse in a community-based cohort of HIV-infected indigent adults. JAMA Internal Medicine, 173(3), 235-237.
-
Corporation for Supportive Housing (CSH). (2016) Youth Systems Estimated Supportive Housing Need. Retrieved from: https://d155kunxf1aozz.cloudfront.net/wp-content/uploads/2018/07/Youth-10-7-16.pdf. Accessed online January 3, 2018.
-
Administration for Children and Families. (2016). Administration for Children and Families and Youth Services Bureau Street Outreach Program: Data Collection Study Final Report. Washington, DC: Administration for Children and Families.
-
Sherman, S.G., Cheng, Y., & Kral, A.H. (2007). Prevalence and correlates of opiate overdose among young injection drug users in a large U.S. city. Drug and Alcohol Dependence, 88(2), 182-187.
-
Rhoades, H., Winetrobe, H., & Rice, E. (2014). Prescription drug misuse among homeless youth. Drug and Alcohol Dependence, 138, 229-233.
-
Baggett, T.P., Hwang, S.W., O'Connell, J.J., Porneala, B.C., Stringfellow, E.J., Orav, E.J., Rigotti, N.A. (2013). Mortality among homeless adults in Boston: Shifts in causes of death over a 15-year period. JAMA Internal Medicine, 173(3), 189-195.
-
National Health Care for the Homeless Council. (2017). Addressing the Opioid Epidemic: How the Opioid Crisis affects Homeless Populations. Nashville, TN: National Health Care for the Homeless Council.
-
Bauer, L.K., Brody, J.K., Leon, C., & Baggett, T.P. (2016). Characteristics of homeless adults who died of drug overdose: A retrospective record review. Journal of Health Care for the Poor and Underserved, 27(2), 846-859.
-
Gabrielian, S., Young, A.S., Greenberg, J.M., & Bromley, E. (2016). Social support and housing transitions among homeless adults with serious mental illness and substance use disorders. Psychiatric Rehabilitation Journal. Advance online publication.
-
Robbins, P.C., Callahan, L., and Monahan, J. (2009). Perceived coercion to treatment and housing satisfaction in housing-first and supportive housing programs. Psychiatric Services, 60(9), 1251-1253.
-
National Center on Addiction and Substance Abuse at Columbia University, & Corporation for Supportive Housing. (2012). Unlocking the Door: An Implementation Evaluation of Supportive Housing for Active Substance Users in New York City. New York, NY: National Center on Addiction and Substance Abuse at Columbia University.
-
Davidson, C., Neighbors, C., Hall, G., Hogue, A., Cho, R., Kutner, B., & Morgenstern, J. (2014). Association of Housing First implementation and key outcomes among homeless persons with problematic substance use. Psychiatric Services, 65(11), 1318-1324.
-
Westermeyer, J., & Lee, K. (2013). Residential placement for veterans with addiction: American Society of Addiction Medicine criteria vs. a veterans homeless program. Journal of Nervous and Mental Disease, 201(7), 567-571.
-
Corporation for Supportive Housing (CSH). (2017). Supportive Housing's Vital Role in Addressing the Opioid Epidemic in New Jersey. New York, NY: CCH.
-
Tsai, J., Kasprow, W.J., & Rosenheck, R.A. (2014). Alcohol and drug use disorders among homeless veterans: Prevalence and association with supported housing outcomes. Addictive Behaviors, 39(2), 455-460.
-
Edens, E.L., Mares, A.S., Tsai, J., & Rosenheck, R.A. (2011). Does active substance use at housing entry impair outcomes in supported housing for chronically homeless persons? Psychiatric Services, 62(2), 171-178.
-
National Alliance for Recovery Residences. (2012). A Primer on Recovery Residences: Frequently Asked Questions. Atlanta, GA: National Alliance for Recovery Residences.
-
National Alliance for Recovery Residences. (2015). Recovery Residence Quality Standards. St. Paul, MN: National Alliance for Recovery Residences.
-
National Alliance for Recovery Residences. (2016). NARR Position Statement on Medication-Assisted Treatment. Atlanta, GA: National Alliance for Recovery Residences.
-
Paquette, K., Greene, N., Sepahi, L., Thom, K., & Winn, L. (2013). Recovery Housing in the State of Ohio: Findings and Recommendations from an Environmental Scan. Columbus, OH: Ohio Council of Behavioral Health and Family Service Providers and Center for Social Innovation.
-
Post, R. (2017). Recovery Housing Principles and Practices [PowerPoint slides]. Presented at the 2017 National Conference on Ending Homelessness, Washington, DC.
-
Solotaroff, R. (2016). Expanding Access to and Capacity for Medication Assisted Treatment for Opioid Use Disorder [PowerPoint slides]. Presented at the 2016 North Coast Opioid Summit, Seaside, OR.
-
Gregg, J. (2016). Follow-up to nonfatal opioid overdoses: More of the same or an opportunity for change? Annals of Internal Medicine, 164(1), 62-63.
-
Woods, J.S., & Joseph, H. (2015). Stigma from the viewpoint of the patient. Journal of Addictive Diseases, 34(2-3), 238-247.
-
Legal Action Center. (2009). Know Your Rights: Rights for Individuals on Medication-Assisted Treatment. (HHS Publication No. (SMA) 09-4449). Rockville, MD: SAMHSA.
-
Alford, D., LaBelle, C., Richardson, J., O'Connell, J., Hohl, C., Cheng, D., & Samet, J. (2007). Treating homeless opioid dependent patients with buprenorphine in an office based setting. Journal of General Internal Medicine, 22(2), 171-176.
-
Substance Abuse and Mental Health Services Administration. (2004). Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction. Treatment Improvement Protocol (TIP) Series, No. 40. (HHS Publication No. (SMA) 04-3939.) Rockville, MD: SAMHSA.
-
Substance Abuse and Mental Health Services Administration. (2005). Medication-Assisted Treatment for Opioid Addiction in Opioid Treatment Programs. Treatment Improvement Protocol (TIP) Series, No. 43. (HHS Publication No. (SMA) 12-4214.) Rockville, MD: SAMHSA.
-
Tringale, R., Subica, A.M., Danielian, A., & Kaplan, C. (2015). The stepped treatment engagement protocol for homeless, needle exchange heroin-dependent patients. Journal of Addiction Medicine, 9(2), 163-164.
-
Daniels, A., Salisbury-Afshar, E., Hoffberg, A., Agus, D., & Fingerhood, M.I. (2014). A novel community-based buprenorphine program: Client description and initial outcomes. Journal of Addiction Medicine, 8(1), 4-46.
-
Chatterjee, A., Obando, A., Strickland, E., Nestler, A., Harrington-Levey, R., Williams, T., & LaCoursiere-Zucchero, T. (2017). Shelter-based opioid treatment: Increasing access to addiction treatment in a family shelter. American Journal of Public Health, 107(7), 1092-1094.
-
U.S. Interagency Council on Homelessness. (2017). Strategies to Address the Intersection of the Opioid Crisis and Homelessness. Washington, DC: U.S. Interagency Council on Homelessness.
-
Raymond, D. (2016). Syringe Exchange Exposed! Amazing Secrets from the Frontlines of Harm Reduction[PowerPoint slides]. Presented at the 2016 National Conference on Ending Homelessness, Washington, DC.
-
Corporation for Supportive Housing (CSH). (n.d.). FUSE. Retrieved from: https://www.csh.org/fuse.
-
CSH Social Innovation Fund Initiative. (2018). Evaluating Supportive Housing as a Solution for People with Complex Health Care Needs. Retrieved from: https://www.csh.org/wp-content/uploads/2018/01/CSH-SIF-Evaluation-Summary-02-02-18Final.pdf.
-
Robert Wood Johnson Foundation (RWJF) & Corporation for Supportive Housing (CSH). (2012). Keeping Families Together Matters: An Introduction to Creating Supportive Housing for Child Welfare-Involved Families. Retrieved from: https://d155kunxf1aozz.cloudfront.net/wp-content/uploads/2012/07/KFT-Guidebook-120711.pdf.
-
U.S. Department of Housing and Urban Development (HUD). (2014). SNAPS in Focus: Youth Homelessness. Retrieved from https://www.hudexchange.info/news/snaps-in-focus-youth-homelessness/.
-
Glynn, C., & Casey, A. (2018). Homelessness Rises Faster Where Rent Exceeds a Third of Income. Zillow Research. Retrieved from https://www.zillow.com/research/homelessness-rent-affordability-22247/. Accessed January 3, 2018.
-
Corporation for Supportive Housing. (2018) Supportive Housing and Healthcare Utilization Outcomes, State of the Literature. Retrieved from https://d155kunxf1aozz.cloudfront.net/wp-content/uploads/2018/07/CSH-supportive-housing-outcomes-healthcare_Final.pdf.
OPIOID USE DISORDER, HOUSING INSTABILITY AND HOUSING OPTIONS FOR RECOVERY
This report was prepared under contract #HHSP233201600010I between HHS's ASPE/DALTCP and Abt Associates. For additional information about this subject, you can visit the DALTCP home page at https://aspe.hhs.gov/office-disability-aging-and-long-term-care-policy-daltcp or contact the ASPE Project Officer, Emily Rosenoff, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201; Emily.Rosenoff@hhs.gov.
Reports Available
Choice Matters: Housing Models that Promote Recovery for Individuals and Families Facing Opioid Use Disorder
- HTML https://aspe.hhs.gov/basic-report/choice-matters-housing-models-may-promote-recovery-individuals-and-families-facing-opioid-use-disorder
- PDF https://aspe.hhs.gov/pdf-report/choice-matters-housing-models-may-promote-recovery-individuals-and-families-facing-opioid-use-disorder
Choices Matter: Housing Models that May Promote Recovery for Individuals and Families Facing Opioid Use Disorder Report Highlights
- HTML https://aspe.hhs.gov/basic-report/choices-matter-housing-models-may-promote-recovery-individuals-and-families-facing-opioid-use-disorder
- PDF https://aspe.hhs.gov/pdf-report/choices-matter-housing-models-may-promote-recovery-individuals-and-families-facing-opioid-use-disorder
Housing Options for Recovery for Individuals with Opioid Use Disorder: An Environmental Scan