

We would like to acknowledge the contributions of Michael Millman our Contract Officer’s Representative (COR) from the Assistant Secretary for Planning and Evaluation (ASPE) who has provided detailed edits and contributed key writing on different sections of this draft and participated in all of our discussions and case studies.
We would also like to recognize the members of our Technical Expert Panel (TEP) who provided guidance and valuable assistance at various stages of the project. Several members of the TEP took the time to offer detailed edits and input that contributed to the strength of this report. The National Association of County and City Health Officials (NACCHO) and the Association of State and Territorial Health Officials (ASTHO) were part of the team that developed this report and provided guidance and access to key stakeholders and offered invaluable contributions.
Finally, we are indebted to the many federal, state and local public health department stakeholders who took the time to hold engaging and detailed discussions with us for this project. We list individuals who contributed to this project as TEP members and key discussants in the Appendices to this report.
Contents
Public Health Practice and Health IT. 4
Relevant Program and Policy Initiatives. 7
Chapter 2: Project Approach.. 21
Chapter 3: Public Health Practice and Health IT.. 25
Tracking, Monitoring and Taking Public Health Action. 25
Funding for Public Health IT. 34
Chapter 4: HITECH, ACA and Public Health Systems. 37
The Affordable Care Act and Public Health. 40
National Public Health Informatics Initiatives. 44
Potential for a Public Health Information Systems Architecture. 47
Potential Future Directions for Public Health Informatics. 48
Chapter 6: Findings from Case Studies. 50
Findings from Northern Florida. 50
Findings from Central Michigan. 54
Findings from Western Oregon. 60
Chapter 7: Emerging Themes. 65
Understanding the Public Health Process. 65
Structural Factors and Public Health Informatics. 70
Appendix 1: Technical Expert Panel Members . 75
Appendix 2: Stakeholders Participating in Key Informant Discussions. 73
This project conducted for the Assistant Secretary for Planning and Evaluation (ASPE) at the United States Department of Health and Human Services assesses trends in the use of information technology (IT) by state and local governmental public health departments. Although public health departments routinely capture and manage data electronically and use the Internet and system-to-system interfaces to transfer information, they struggle to establish integrated approaches to capturing, managing, analyzing and sharing information across programs and jurisdictions.
We found public health departments making important advances in use of IT, but we did not find a single “best practice” approach. Public health officials face common challenges, including variation and ongoing evolution of public health activities, lack of training on informatics and process re-design, shrinking funding and constraints that limit strategic investment and encourage data silos. Most agree that, in the future, public health practice will require an integrated approach to managing information and collaboration with health-care providers and other partners.
The Patient Protection and Affordable Care Act (ACA), the Health Information Technology for Economic and Clinical Health (HITECH) Act, and the field of public health informatics bring opportunities while revealing important gaps and posing new challenges. HITECH motivates electronic reporting but does not emphasize the IT needs of public health practice. The ACA emphasizes population health goals but does not define a role for public health departments. Informatics projects break new ground, but have not yet benefited most public health departments. Many stakeholders await more direction before acting on opportunities from ACA and HITECH.
Discussions with dozens of public health leaders suggest that public health departments need access to predictable, sustained and flexible resources supporting capital investments, workforce training, business process analysis and, importantly, use of standards and interoperable systems. Public health departments can benefit from planning IT investments around underlying work processes and their current and future information needs.
By articulating a strategic framework for using IT, some public health departments are pursuing a path that reduces unnecessary redundancy and improves the quality and scope of information available for public health practitioners. For example, by capturing demographic data one time to support multiple services; aligning data from multiple administrative and programmatic sources to help address service needs or using health-care provider generated data, public health departments can increase efficiency and innovation.
Developing an effective strategic framework requires knowledgeable leadership to identify relevant data sources, document public health practice, understand legacy systems, work with vendors and visualize how to improve functions through better information flow. A framework helps agencies address known priorities as funds become available rather than simply react to funding opportunities. Stakeholders uniformly believe that the federal government, national organizations and funders of all kinds can facilitate progress towards improved use of public health IT by endorsing and fostering integration, interoperability, common standards and business processes and increased collaboration between health-care providers and agencies with public health responsibility at all levels.
NORC at the University of Chicago is pleased to submit this final report for Assessing the Status and Prospects of State and Local Health Department Information Technology Infrastructure, a project of the Assistant Secretary for Planning and Evaluation (ASPE) at the United States Department of Health and Human Services. NORC and ASPE worked in close partnership with the National Association of County and City Health Officials (NACCHO) and the Association of State and Territorial Health Officials (ASTHO).
This report describes how state health agencies (SHAs) and local health departments (LHDs) use information technology systems to capture, manage, analyze, and report information. We assess trends in use of information technology (IT) among SHAs and LHDs following the Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009, the Patient Protection and Affordable Care Act (ACA) of 2010, recent work in public health informatics, and other factors. This project assumes that IT tools and resources should play a role in governmental public health practice. However, we also assume that rigorous assessments of public health goals should motivate IT projects and that stakeholders should design and implement IT in direct service of those goals.
This report reflects synthesis information gathered from public health stakeholders as well as existing literature and reports. We describe key elements of our approach below.
■ Technical expert panel (TEP). Appendix 1 to this report lists the TEP members selected for their experience and expertise in public health practice, public health information science or public health program management. We conducted one TEP meeting in February of 2012. This meeting helped inform case study locations selected as well as the topics. We met with the TEP again in October of 2012 to discuss findings from case studies and receive comments on an interim version of this report. In many cases, we also conducted one-on-one discussions with TEP members and TEP members offered detailed edits and contributions to this report.
■ Telephone discussions with key stakeholders. In Appendix 2, we list a number of leaders from public health informatics and state, local and federal public health. We met with these stakeholders by telephone to discuss specific public health applications or topics. In some cases, we present key elements of these conversations as “mini-case studies” referenced as examples throughout this report.
■ Review of existing literature and reports. We conducted a thorough review of existing peer reviewed literature, gray literature and online information related to use of IT by public health practitioners.
■ In-depth case studies in three locations. Finally, we conducted in-person site visits in three different locations: Northern Florida, Central Michigan and Western Oregon. As part of these site visits we held discussions with leadership, epidemiologists and clinical staff from SHAs and LHDs. We chose locations, in part, based on their innovation in specific areas. However, we also sought a comprehensive understanding of each agency’s mission, activities and the role of IT in their work.
Public health officials need timely access to valid and reliable data necessary to monitor health status and health-related factors. They rely on data to develop and implement programs that protect health and ensure safety. Like their counterparts in other domains, public health professionals increasingly turn to advances in IT to support their need to capture, exchange, manage and analyze data. This project does not cover all public health activities, but we look at several public health functions and common uses of IT to support these functions.
While public health officials rely on surveys and other population-wide data collection strategies for some purposes, much of the information relevant to public health originates with the health-care delivery system or other social service sectors. These data include diagnosis and treatment information for infectious and chronic diseases, patterns in patient complaints or symptoms that may suggest an outbreak, vaccination records, birth and death records, results from screening of newborns for life-threatening conditions, and data related to other priority areas.
Public health departments have adopted different information systems to help capture data from health-care providers and other sources. For example, SHAs manage disease surveillance systems, designed to capture data on the diagnosis and treatment of a series of “notifiable” diseases specified in state law.
LHDs and SHAs also manage registries for specific purposes, such as vaccine registries, where pediatricians and other providers supply data on vaccinations, or cancer registries, where providers submit information on cancer diagnoses. SHAs and LHDs capture records of the births and deaths taking place in their jurisdiction and results from beginning of life screening for life-threatening conditions, early hearing detection and birth defects. Finally, SHAs and LHDs often collect, manage and report data related to federal programs such as maternal and child health authorized under Title V of the Social Security Act, and the Department of Agriculture’s Supplemental Feeding Program for Women, Infants and Children (WIC).
LHDs may provide clinical services or other personal health services. Direct services include full primary medical care services for uninsured and low-income individuals through Federally Qualified Health Centers (FQHCs), oral health, behavioral health, clinics for HIV/AIDS funded under the Ryan White Care Act, sexually transmitted disease (STDs) clinics, WIC services, vaccine clinics and maternal and child health programs funded under Title V. Like their private and non-profit sector clinical counterparts, LHDs use applications such as practice management systems and electronic health records (EHRs) to capture demographics, assess eligibility for public programs, record encounters and report to state systems.
Like other providers of clinical services, LHDs provide data to SHA systems such as immunization registries. As agents of the state or federal government implementing programs under Title V and the Ryan White Comprehensive AIDS Resources Emergency (CARE) Act, LHDs also submit data to state and federal agencies for program reporting.
LHD epidemiologists and case investigators use data from local and state disease surveillance systems to assess local trends and follow-up with affected clients, their providers and contacts. In this way, LHDs both report data to state systems and use data from state systems to do their work. LHDs also maintain environmental health databases used to manage information on inspection and licensing of businesses and facilities that pose environmental health risks (e.g., restaurants, septic tanks, water treatment facilities).
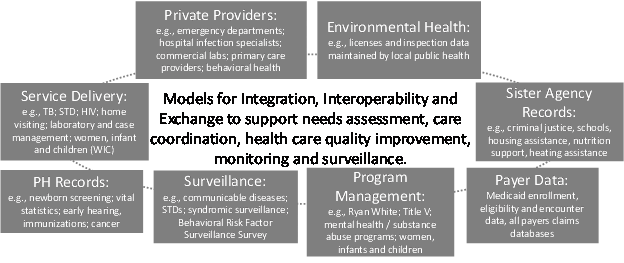
The data necessary to support public health action comes from sources far beyond those captured and managed by public health applications. Exhibit ES-1 below shows different types of relevant data including those generated by the health-care delivery system and other governmental agencies that can inform population health assessments and case management. Many public health stakeholders seek efficient ways to routinely integrate data across these sources to support public health action.
Exhibit ES-1: Sources of Data Relevant to Public Health Practice and Questions for Stakeholders
Funding opportunities and the general availability of funds can drive IT adoption among local and state governmental public health stakeholders as they have done for individual and organizational providers. The majority of funding for LHDs comes from local revenues, state revenue and federal program funding passed through the states. Remaining funds come from direct federal grants, third party reimbursement and fees. SHAs receive the plurality (45 percent) of their funding from federal sources, slightly less from state revenue (39 percent) and the remainder from smaller sources including fees.[1] At both the state and local level, these percentages vary considerably as do overall public health expenditures. For example, per capita spending among LHDs varies between over $50 and less than $20 dollars per resident depending on the jurisdiction.[2]
Regardless of the source of funding, stakeholders note serious challenges with maintaining steady funding to SHAs and LHDs. Public health currently accounts for less than 0.1 percent of GDP and less than three percent of federal health-related expenditures.[3] [4] In 2011, 58 percent of LHDs reported core funding cuts, and 55 percent reduced funding to at least one program. Furthermore, LHDs faced budget reductions of 52 percent in the next year.[5] Because of budget shortfalls at the federal, state, and local levels SHAs and LHDs have lost 15 percent of the state and local workforce from 2008 to 2011. Forty-four percent of SHAs and LHDs reported that they lost staff in 2011.[6]
Unfortunately, relatively little systematic information is available on LHD and SHA spending for IT and related expenditures. In some jurisdictions, processes used to fund IT across all departments also govern public health systems investments. LHDs sit within a larger governmental structure such as a city or county. Department practitioners do not always direct or control how the larger local or state governmental IT staff makes decisions regarding new investments in IT systems and capacity.
Overcoming Silos in New York State
In New York State, the Department of Health’s Division of Family Services (DFS) has used funding from the HRSA-administered Maternal and Child Health Services Title V Block Grants and the State Systems Development Initiative to undertake a program called Child Health Information Integration (CHI2), which aims to integrate newborn screening, newborn hearing screening, immunization, lead, early intervention, WIC, Medicaid, vital statistics and other data sources into one interface and create bi-directional sharing of DFS’s maternal and child health data with its external partners.
We found that public health practitioners base IT decisions on pragmatic factors including cost and ease of compliance with reporting requirements. For example, an agency that begins receiving funding under a different federal or foundation grants may use these requirements to justify the acquisition or development of a new system to capture, manage and report data in the format required by that funder. This results in a series of data silos set up for individual programs where data are not easily integrated.
We found some examples of specific initiatives designed to overcome the silos created by programs funded under categorical grants (see example in text box at left). Many stakeholders have urged funders to allow greater flexibility in allowing use of some funds to support an underlying infrastructure that serves multiple programs.
Recently, a series of initiatives have led to changes in the way stakeholder use IT to capture data relevant to public health. While many initiatives focus primarily on health care providers, they do affect LHDs and SHAs as well. We explore key initiatives below.
HITECH Programs and Public Health Information Systems
The HITECH Act encourages health-care provider adoption and use of EHRs to electronically exchange data. HITECH affects whether local and state governmental health departments can connect with health-care provider and organization information systems and participate in health information exchange (HIE) in a number of ways.
First, HITECH created the Medicare and Medicaid EHR Incentive Program which provides financial incentives for individual health-care providers and hospitals. Providers are eligible for incentives if they have a significant share of Medicare or Medicaid patients, adopt EHRs certified through a process established under the law, and can demonstrate “Meaningful Use” of their EHRs. Some of the criteria associated with Meaningful Use require use of EHRs to submit data electronically to SHA systems such as notifiable disease reporting systems, syndromic surveillance systems and immunization registries.
This, in turn, requires that the state or local governmental public health department systems are able to accept and use provider data submitted electronically using messaging and content standards specified under Meaningful Use. Some states plan to use federal 90 percent matching funds under Medicaid to support investments in their public health systems to help providers meet the public health reporting criteria associated with Meaningful Use.
These opportunities are available under State Medicaid Director Letters 10-016 (Federal funding for Medicaid HIT activities)[7] and 11-004 (Federal funding for HIE development).[8] Eight states have been approved for funding to support different types of HIE under this letter. For example, Massachusetts is developing a single public health gateway to obtain data on reportable laboratory results, immunizations and syndromic surveillance from eligible providers and eligible hospitals.[9]
Partnership for Diabetes and Asthma in SE Minnesota
The Southeast Minnesota Beacon Community, public health-care managers are helping to facilitate transitions between ambulatory care and hospital settings through electronic exchange of EHR data using a CCD format. One participating county notes a reduction in hospital re-admissions for diabetes and childhood asthma through this initiative.[10]
However, stakeholders note than in many cases public health departments cannot fund the 10 percent required to take advantage of these funds or do not have close ties to their Medicaid agency to facilitate this use of matching funds.
In some cases clinical staff at LHDs may also be eligible for the Medicare and Medicaid EHR Incentive Program payments. However, bachelor’s level public health nurses that administer much of the care in public health clinics are not eligible for Meaningful Use payments. Furthermore, many public health clinics predominantly care for uninsured individuals rather than those covered by Medicare or Medicaid. Finally, because of an increased emphasis on case management and care for individuals with specific infectious conditions, many public health clinicians are not able to find certified EHRs that meet their needs and do not have the resources to develop customized applications that meet certification criteria.
Other HITECH programs also relate, in part, to public health. The State HIE Cooperative Agreement Program supports state-based efforts to ensure that providers have options for effective standards-based electronic exchange of clinical information with other providers and local and state governmental public health departments. In a recent review of 27 state programs, 74 percent indicated that their SHA is heavily involved in state HIE activities. Still, it appears that public health reporting was not an initial priority for many state HIE programs as slightly less than half of 27 programs indicated that they support public health use cases for HIE such as exchange with immunization registries or notifiable disease reporting.[11] Some states, including Florida have moved forward with public health use cases including working towards “public health nodes” to allow local public health clinics a mechanism to access information on care received in other settings and to facilitate reporting from health-care providers to SHAs.
HITECH’s Beacon Community Cooperative Agreement Program provides another link to population health objectives. Under Beacon, ONC provided selected communities resources to build and strengthen their health IT and quality reporting infrastructure and support improvements in quality of care and efficiency. Public health involvement in some of the funded Beacon communities highlights the intersection between health reform objectives, population health objectives and health IT. For example, the Louisiana Public Health Institute and the Louisiana Department of Health and Hospitals contribute to the Crescent City Beacon Community based in New Orleans. This program uses EHR data to help clinicians track and manage health outcomes for diabetics in New Orleans. Similarly, in Southeast Minnesota, a Beacon Community collaborates with the LHD to facilitate effective communication and care coordination following hospital discharge to reduce re-admissions for ambulatory care sensitive conditions.
Also related to HITECH, ONC’s Office of Interoperability and Standards manages the Standards and Interoperability Framework (S&I framework). This is a process where public and private sector stakeholders collaborate to identify priorities for HIE standards, create and harmonize standards and test standards through pilots. The S&I framework includes a Public Health Reporting Initiative supported in-part by the Centers for Disease Control and Prevention (CDC) focusing on standards for electronic reporting for health-care providers to public health departments.
The Public Health Data Standards Consortium (PHDSC) working through the S&I framework and related initiatives has helped establish and test standards for public health functions. They have helped develop standards to support programs for early hearing detection and intervention (EHDI) services, public health laboratory reporting and standards for reporting to state-level cancer registries.
The Affordable Care Act and Public Health
Collaboration on Chronic Disease in Denver
Denver Health (a local public health agency), collaborates with local ambulatory care providers to establish a cardiovascular disease (CVD) registry, maintained by public health officials, populated by EHRs from providers in the community that receive data and analysis from the registry to support their quality reporting.
Stakeholders note that programs to track population health and target public health resources and interventions can work effectively to promote improvement in health care delivery and lead to improved health outcomes. While the ACA does focus on achieving population health objectives, it does not map out a specific mechanism for public health departments to engage with health care providers to achieve these goals.
The ACA creates demonstration and pilot programs emphasizing care transitions, referral management and care coordination. Some ACA initiatives focus on use of “community pathway hubs” where community health workers coordinate services including social support, behavioral health and housing assistance for high-need individuals. The ACA also specifically promotes population health by requiring insurance coverage for preventive services, supporting Title V maternal and child health home visiting programs and requiring hospitals to conduct community-based health needs assessments. While stakeholders are not required to work with public health departments to achieve these objectives, they do represent potential opportunities for collaboration.
We identified pockets of innovation, including in Oregon and Vermont, where state and LHDs provide data, analytic resources and public health interventions supporting goals outlined in the ACA. Stakeholders suggest that demand for community-level data on health-care quality and outcomes will increase because of ACA and cost-containment efforts. With the improved access to data and new models for analyzing and tracking trends, public health may be in a good position to be a neutral arbiter in this area providing objective information on health status and outcomes using provider-generated data.
Some officials noted optimism that public health could contribute to ACA by helping manage the health of populations in tandem with health-care providers and payers, but acknowledged uncertainty regarding the best path for bringing this idea to fruition. In addition, some stakeholders note that new ACA rules requiring health insurers to offer more comprehensive coverage of preventive services recommended by entities such as the United States Preventive Services Task Force (USPSTF) may benefit public health departments that are able to effectively bill for these services. However, they also note that these provisions may have the unintended consequence of reducing the need for categorical funding to public health for preventive services. These funds represent important financial support for public health departments.
In this section we highlight findings from our three case studies. We visited Northern Florida, Central Michigan and Western Oregon and, in each location, spoke in-depth with public health practitioners from two LHDs and leadership within each state’s health department. The case studies offered an opportunity to observe dynamics across programs and state and local boundaries and assess the role of IT in states with different models governing state and local public health. In this Executive Summary, we briefly summarize the context and main findings from each of these case studies.
Northern Florida
In Florida, we visited the Duval County Health Department in Jacksonville, the Alachua County Health Department based in Gainesville, and the State Department of Health in Tallahassee. Florida has a state-operated or consolidated model where LHDs adapt to the needs of their communities but rely on the state to support staffing, oversight, information systems and technical support.
We investigated the state’s development of a practice management and clinical solution called the Health Management System (HMS). The state developed HMS using a database platform provided by the InterSystems Corporation. The state’s informatics lead works very closely with software developers and staff at LHDs to create and customize specific clinical modules within HMS that meet the personal care delivery and reporting needs of local public health practitioners in Florida. As of November 2012, the public health department has gained accreditation for the HMS system as a certified EHR, which will allow some public health practitioners to qualify for Meaningful Use incentive payments.
States typically manage multiple public health systems. In Florida, these systems include a newborn screening records system, an immunization registry (FL SHOTS), a notifiable disease surveillance system (Merlin), a syndromic surveillance system (ESSENCE), an STD surveillance and contact management system (PRISM) and systems for reporting to the federal government under Title V and Ryan White (CAREWare). These are typical of the silos referenced above.
Many of public health clinical service providers use a hybrid approach, capturing some data in HMS, some on paper and some using disease specific systems such as PRISM and CAREWare. Furthermore, although most of the state systems for reporting (e.g., newborn screening, immunizations, surveillance) have effectively adopted electronic laboratory reporting (ELR) practitioners in hospitals and LHDs continue to enter data twice, once for their own use and a second time for reporting to the state.
Even with a state-run consolidated model, Florida illustrates how multiple systems and data silos emerge given the diverse clinical, case management and reporting requirements facing public health departments. This case study shows the challenges to consolidating data from different systems and building interfaces to support local and state governmental public health department action.
Findings from Florida also highlight characteristics of sound leadership in public health information systems planning. Leadership within the state had a good understanding of the history and constraints that led to current practice and were able to put the state on a strategic path.
Central Michigan
Michigan has a decentralized system of local governmental public health departments. In Michigan, we investigated public health use of IT at the Michigan Department of Community Health (MDCH), a superagency that covers Medicaid, mental and behavioral health and public health (but not many environmental health and licensing functions); the Ingham County Health Department (ICHD), and the Mid-Michigan District Health Department (MMDHD). Michigan illustrates some important models for data integration and exchange of data between public health and providers.
The state’s immunization registry, the Michigan Care Improvement Registry (MCIR) pulls data from the newborn screening database as well as the state’s Medicaid data warehouse. This gives providers easy access to information on newborn screening testing results, early hearing detection and intervention (EHDI) assessments, blood lead screening results and information on early and periodic diagnosis and treatment (EPSDT) requirements for children on Medicaid.
The Medicaid data warehouse itself serves as an example of strategic planning to integrate data relevant to public health from different systems. MCDH’s Office of Medicaid Health Information Technology plans to build on an existing warehouse of Medicaid encounter data by allowing users to combine these data with the state’s notifiable disease surveillance system, vital records, syndromic surveillance, state public health laboratories, a cancer registry, and a future chronic disease registry. The data warehouse uses a master patient index (MPI) to match data to clients across disparate systems. Michigan envisions including provider-generated data from EHRs into the warehouse through links with a state-wide HIE hub.
Like Florida, stakeholders at the state-level in Michigan have a solid vision for organizing and managing data related to public health. However, they may be less able to leverage this vision to break down silos at the local level. Because LHDs in Michigan are independent and governed by county leaders, there is not a single state-wide clinic management application to support patient-facing services at public health clinics in Michigan. Nor does the vision include integration with other local and state non-clinical operations and data which can provide useful information about the patient, resident and their environment.
Mid-Michigan Health Department uses Netsmart’s Insight application as a public health practice management and EHR application. Meanwhile in Ingham County, the local health department has just adopted the NextGen EHR for their FQHC sites and is working on customizing NextGen to work in their other clinical programs such as communicable disease clinics, maternal and child health clinics and home visiting programs.
We found some stand-alone systems that were outside of the strategic plan led by the Office of Medicaid Health IT. Specifically, the state’s Maternal and Infant Health Program that manages all the Title V funding in the state still uses some paper-based reporting systems. The systems used to manage data related to these programs do not easily share data with any other state or local health department systems.
Despite the sophisticated Medicaid systems and innovative registry projects like MCIR, the Michigan case illustrates the challenge of bringing data together across disparate and uncoordinated systems for public health action. As in other states, LHDs in Michigan procure their own IT systems. Like many state governmental public health departments, these LHDs sometimes lack the expertise, time and resources to adequately plan for implementation.
Western Oregon
In Oregon, we met with Washington County Department of Public Health, Multnomah County Department of Public Health and the Oregon Health Authority (OHA). As in Michigan, Oregon’s LHDs are legally independent of the state’s public health agency. LHDs receive very little state funding, technical assistance, and oversight. As a result, LHDs have developed homegrown and stand-alone data systems. Additionally, Oregon has a number of small rural and frontier counties with extremely limited resources- these jurisdictions may not have any full-time IT staff and make very limited use of computers and information technology to support their mission.
We visited Oregon, in part, because of innovative efforts to include public health in health-care reform. In August of 2012, the state began implementing Coordinated Care Organizations (CCOs). CCOs are local health umbrella organizations that will deliver health-care coverage for people who are eligible for Medicaid managed care in Oregon and will have performance based payment incentives that will reward quality improvement and cost control.
Staff from OHA and LHDs take part in CCO planning and implementation. The initial focus for these efforts is around reducing “high cost” hospital care. In some parts of Oregon, such as Washington County, public health departments have developed collaborative efforts with local providers to support community-wide quality of care measurement.
Currently, Oregon has multiple state systems with limited interoperability or capacity to share data to support core public health functions including epidemiology, surveillance, monitoring and assurance. ORPHEUS, the state’s main communicable disease surveillance system, does not interface with providers’ EHRs, but does receive data automatically from clinical laboratories through electronic lab reporting (ELR). Oregon’s immunization registry program, called ALERT IIS currently interfaces with multiple EHR products including the Insight public health EHR used in Washington County. The immunization registry also accepts batched data in formats such as flat-files, Excel and HL7 from different provider organizations.
As in other places, Oregon’s LHDs adopt and customize information systems on their own. Although the FQHC in Multnomah County has long used the Epic EHR, the public health clinics have not been able to find resources to use Epic for their work. One barrier cited is the lack of case management functionality built into Epic, a core public health activity.
As a result, Multnomah County has developed dozens of individual systems to support different programs and services. Multnomah County recently established an informatics committee to document these homegrown applications. This committee also educates staff about the process used within their county government for proposing IT capital improvement projects.
We began by noting that public health department IT investments should be driven by an objective assessment of public health goals and activities and the information needs necessary to support those efforts. Findings from this project illustrate support for this concept among public health stakeholders, but highlight a series of organizational and funding-related challenges as well as challenges stemming from shifting emphasis in public health activities.
LHDs need resources to plan, design, and implement coordinated IT systems for their own use and to integrate with the rapidly developing clinical sector. While clinical services are a small and diminishing part of public health department activities, public health departments conducting case investigation, care coordination or case management will continue to capture data from individuals. This project illustrates the importance of establishing tools for the capture, management and use of data needed to support personal services in public health clinics and those delivered by public health visiting nurses and case managers. Ideally these tools would allow easy exchange or integration of these data with data on the same populations from other sources.
Health departments need a better understanding and documentation of the business rules and processes underlying public health function. A clear theme in our work is that effective investments in the design and implementation of public health information resources must begin with a detailed and well documented understanding of public health practice, both broadly and as practiced in specific jurisdictions. Many public health departments understand this imperative, but lack the necessary staff expertise, time and resources to prioritize this activity.
Currently, public health relies on non-integrated IT systems. Overcoming data silos will be a clear objective for future public health systems initiatives. Stakeholders identify two paths for moving past silos. The first involves adoption of a common meta-data model or scheme for how data elements used in public health relate to one another. This scheme would be common to all applications used by an agency or would govern a data repository underlying each of these applications. This would enable multiple applications within an agency to draw on commonly structured data and avoid duplication. The second involves assuring interoperability across systems used by different public health departments and health-care providers through use of common messaging standards, content standards and interfaces.
Vendors can play an important role as landscape evolves. While a relatively new and immature market, IT vendors targeting public health departments are increasingly aware of the importance of integration and the benefits of standardized business processes and information standards for public health. Currently, limited resources and a lack of a common venue for engaging with public health department customers may preclude beneficial engagement between potential public health department customers and vendors. While there are a limited number of vendors committed to the public health market, we spoke with some vendors familiar with public health processes and eager to engage with knowledgeable and sophisticated partners at LHDs.
Having a vision and model for capturing, maintaining and using data may be more realistic and useful than adoption of a comprehensive infrastructure for public health information systems in the near future. Given variations in the priorities and capacities of public health departments, the path for achieving single common data architecture for public health remains unclear. Use of a standard architecture to support public health programs across departments will require significant time and resources. As a first step, programs, policy and funding opportunities may encourage consistent use of data content and messaging standards and establish a common understanding of the relationship between different data elements relevant to public health programs.
HITECH raises awareness, but also highlights gaps in IT capacity at public health departments. HITECH has raised awareness of the exchange of data between public health and health care and highlights gaps in defining best practices for public health IT. Examples of public health participation in initiatives to improve care through the Beacon Cooperative Agreement program show the potential benefits of public health engagement on quality improvement initiatives leveraging data from health IT systems. While these efforts are limited to a few locations in the country, they will offer some useful case examples for consideration in other jurisdictions.
Public health’s ability to assess and improve quality of care and chronic disease management post-ACA remains unclear. Many stakeholders agree that public health departments can play an important role in advancing the objectives of the ACA by providing objective community-level health assessments bringing together multiple sources of data and supporting care coordination across providers. SHAs in OR, MI and likely elsewhere are involved in state-wide Medicaid health-care delivery reform efforts and federal demonstration projects.
However, even in these cases, stakeholders have not comprehensively defined how public health departments will participate and the capacity-building necessary for public health departments to take on this role. Clarifying a role for public health will require a better understanding of the business processes and data flow necessary to support public health surveillance and programs related to chronic diseases as well as a commitment from public health departments, the care delivery community and public and private payers to work together on these issues.
Models for incorporating provider-generated data to support population health management need additional attention. Most public health departments have not yet developed models to access and use provider-generated data, to monitor processes of care or outcomes or assess the status of vulnerable populations. This will require development of new models to capture, transmit and analyze data and, importantly, cooperation on the part of the medical care community. New York City, Vermont and Denver offer early examples of public health working collaboratively with health-care providers in this area. A 2010 NACCHO report shows that local health department staff prioritized “using clinical data to improve quality of care” as a subject for workforce training over other informatics topics.[12]
Public health operational, governance and financing models vary. Several factors drive variation across public health departments including the extent to which federal funds administered at the state-level make use of LHDs as care providers; the extent to which SHAs control or manage LHDs; the priority state and local government leaders place on public health and the historic role of public health in a given jurisdiction. This is one reason why a single architecture or model for public health infrastructure may not be feasible.
Strategic investments may require a different approach to financing IT. Our findings suggest that public health departments fund innovation largely by making creative use of operational funds from programmatic grants or special projects. This approach can limit the strategic impact of these innovations, limit the extent to which they facilitate useful integration of data across programs and affect their sustainability. Using time-limited operational funds may constrain the timing of investments and not allow for strategic planning or the use of best practices from informatics.
Importance of leadership. Leadership is a critical element to the success of an endeavor to improve the use of data and information systems to achieve public health objectives. Public officials making strides in public health informatics come with a very detailed understanding of workflows and data flows associated with public health and the extent to which public health officials struggle with manipulating data in different ways to answer key questions. They bring a willingness to engage in a detailed way with vendors and IT professionals on mapping out requirements, re-thinking workflows and processes and then building enthusiasm among public health staff for continuous quality improvement and informatics. They also bring knowledge of national initiatives and how they relate to the specific objectives and challenges facing their state or local jurisdiction. And they place importance on these activities, ensuring they occur.
Implications for technical assistance programs. We found limited take-up of resources from past and current technical assistance programs, but an appetite for more technical assistance related to data, informatics and IT challenges. Specifically, stakeholders adopting new systems would benefit from support with workflow optimization and data standards. Agencies could use assistance selecting vendors, describing requirements and configuring new applications. In some cases, stakeholders noted the potential benefit of sharing learning and best practices among a community of agencies that are using a common vendor platform to achieve similar public health objectives.
We found public health departments making important advances in use of IT, but we did not find a single “best practice” approach. Public health officials face common challenges, including variation and ongoing evolution of specific public health activities, lack of training on informatics and process re-design, shrinking funding for public health programs and constraints that limit strategic investment and encourage data silos.
Most agree that, in the future, effective public health practice will require a more integrated approach to managing information and increased collaboration with health-care providers and other social service departments. Public health departments themselves may benefit from openness to engaging with non-traditional partners, including health-care payers and providers.
Public health departments can benefit from planning IT investments around underlying work processes and their current and future information needs. Importantly, investments should promote use of standards and interoperability and avoid creating incentives for additional silos. Some findings suggest that state-level planning on public health IT investments may yield the most benefits. We found that by articulating a strategic framework for using IT, some public health departments have taken their IT infrastructure down a path that reduces unnecessary redundancy and improves the quality and scope of information available for public health practitioners. For example, by capturing demographic data one time to support multiple services, aligning data from multiple administrative and programmatic sources to help address service needs, or integrating data generated by health care providers, public health departments can more efficiently tackle current activities and take on innovation.
Developing an effective strategic framework requires agency leadership with the knowledge to identify a wide-range of relevant data, document current public health practice, understand legacy systems, work closely with IT vendors and visualize how to improve public health functions through better information flow. This gives agencies the opportunity to identify and address IT priorities as funds become available rather than letting funding opportunities alone drive investment decisions. The federal government, organizations representing public health, medical associations and funders of all types can contribute to progress in the use of IT by public health departments by endorsing the ideas of integration and improved use of systems as priorities and fostering increased collaboration among agencies with public health responsibility at all levels.
NORC at the University of Chicago is pleased to submit this final report for Assessing the Status and Prospects of State and Local Health Department Information Technology Infrastructure, a project funded by the Assistant Secretary for Planning and Evaluation (ASPE) at the United States Department of Health and Human Services. NORC and ASPE worked in close partnership with the National Association of County and City Health Officials (NACCHO) and the Association of State and Territorial Health Officials (ASTHO).
This report describes how state and local governmental public health agencies (hereinafter referred to as local health departments “LHDs” and state health agencies “SHAs”) use health IT to capture, manage, analyze, share and disseminate data and information in service of their mission. We focus particularly on how new programs and other contextual factors affect the use of information systems to support public health functions.
We assess progress in the use of information technology (IT) in the public health arena in the context of the Health IT for Economic and Clinical Health (HITECH) Act of 2009, the Patient Protection and Affordable Care Act (ACA) of 2010, ongoing public health informatics initiatives and recent limits on funding available to public health agencies. This project begins with the premise that stakeholders must use objective and rigorous assessments of public health goals to motivate IT projects and implement systems in direct service of those goals.
This report addresses an important gap. Given the variety and complexity of public health activities, literature on public health information systems can be either too general or too technical to inform public policy. Public health informatics is limited to a small group of specialists, and a broader understanding of technical problems and potential solutions may help set program priorities.
We ground our findings in the experience of public health professionals who use IT on a daily basis, document local innovation and relate this information to national initiatives. We uncover innovative thinking about difficult issues such as public sector IT governance, integration of different public health data sources, development and customization of software for use delivering services in public health settings and strategies for pursuing and using grant funding.
Key Acronyms
CDC: Centers for Disease Control and Prevention
HRSA: Health Resources and Services Administration
ASPE: Assistant Secretary for Planning and Evaluation
NACCHO: National Association of County and City Health Officials
ASTHO: Association of State and Territorial Health Officials
PHDSC: Public Health Data Standards Consortium
PHII: Public Health Informatics Institute
JPHIT: Joint Public Health Information Task Force
PHAB: Public Health Accreditation Board
ACA: Patient Protection and Affordable Care Act
HITECH: Health Information Technology for Clinical and Economic Health Act
SHA: State Health Agencies
LHD: Local Health Departments
FQHC: Federally Qualified Health Centers
CARE: Ryan White Comprehensive AIDS Resources Emergency Act
EHDI: Early Hearing Detection and Intervention
STD: Sexually Transmitted Diseases
S&I Framework: Standards and Interoperability Framework
EHR: Electronic Health Records
HIE: Health Information Exchange
ELR: Electronic Laboratory Reporting
MPI: Master Patient Index
RLS: Record Locator Service
CDA: Clinical Data Architecture, document standard
SOA: Service-Oriented Architecture
At a time when the federal government oversees major investments promoting health IT and reforming health-care delivery in the United States, the public health community grapples with their role in a changing health-care delivery environment. This report offers a view into the current activities of LHDs/SHAs, the effect of process improvement and IT on these activities and their role in capturing, managing and sharing information to promote population health.
We organize this report in chapters building towards a set of cross-cutting themes and conclusions. After describing our project approach, we summarize selected public health activities and the role of IT. We also highlight data sources relevant to the public health mission, funding for public health and the current and potential future impact of HITECH and ACA.
In these sections, we summarize available literature as well as discussions with public health thought leaders and practitioners. We use “real-world” examples to illustrate key points.
We then present findings from our three in-depth case studies illustrating how public health professionals use information systems activities across programs and jurisdictions. We end the report with recurring themes from the project relevant to future program and policy initiatives.
This report reflects our synthesis of information gathered from public health practitioners, policy leaders and academic experts as well as existing literature, reports and documentation on relevant topics. Below, we describe the four components of our approach.
Technical expert panel (TEP). Appendix 1 to this report lists the TEP members selected for their experience and expertise in public health practice, public health information science, public health program management and other relevant disciplines. We conducted one TEP meeting in February of 2012 to identify key themes and topics for our discussions with public health practitioners. This meeting helped inform the cases selected as well as the topics covered during the detailed case study phase of the project. We met with the TEP again in October of 2012 to discuss findings from the case study and review comments on an interim version of this report. In many cases, we also conducted one-on-one discussions with TEP members.
Telephone discussions with key stakeholders. In Appendix 2, we list a number of public health informatics leaders and state, local and federal public health officials we met with by telephone. These discussions focused mainly around specific topics in the discussants’ area of expertise. In some cases, we present key elements of these conversations as “mini-case studies” referenced as examples throughout this report. In order to cast a wide net, we spoke SHAs and LHDs at various levels of advancement. Exhibit 1 below provides examples of the topics covered as part of the mini-case studies.
Review of existing literature and reports. Early in the project, and at various subsequent stages, we conducted a thorough review of existing peer reviewed literature, gray literature and online information related to use of health IT by public health practitioners.
Exhibit 1: Examples of Mini-Case Study Participants and Topics
| Agency | Participants | Topic Overview |
| HIV/AIDS, Hepatitis, STD, TB Administration Washington, DC | Dr. Greg Pappas Tiffany West | Adoption of a common platform to facilitate care delivery, surveillance, program monitoring and care coordination for HIV/AIDS and communicable diseases in DC. |
| South Carolina Budget and Control Board Office of Research and Statistics, State HIT Coordinator, State Public Health Agency | Dr. David Patterson (Control Board) Michael Patterson (Public Health) | Integration of program data across the state with geographic analysis. Linking data from multiple sectors with health-care and public health data to support program management and public health action. |
| Utah Department of Health | Dr. Wu Xu | Use of statewide health information exchange network (UHIN) provider directory to send public health alerts to health-care providers and receive data relevant to public health from health-care providers. |
| North Carolina Department of Health and the Carolina Center for Health Informatics | Amy Ising | Use of the North Carolina Disease Event Tracking and Epidemiologic Collection Tool (NC DETECT) for syndromic surveillance (data capture and sharing) working with data from emergency departments, Carolina Poison Center and emergency medical services (EMS). |
| New York City Department of Health and Mental Hygiene | Thomas Cannell | Use of data from primary care providers with EMRs supported through the Primary Care Improvement Project (PCIP) for analysis of chronic disease outcomes and continuous quality improvement at the practice level. |
| Denver Health | Dr. Arthur Davidson | Public health effort to leverage data on cardio-vascular disease patients from provider EMRs, create a CVD registry and provide data back to provider community using a Community Transformation Grant from the Centers for Disease Control and Prevention (CDC). |
| Olmsted County (MN) Public Health Services | Dan Jensen | Public Health Documentation system (PH-Doc) effort to capture clinical care document (CCD) on patients from participating providers to track care delivered to population’s with chronic conditions, facilitate exchange of data across providers and support quality improvement. Funded through the Beacon Cooperative Agreement Program. |
In-depth case studies in three locations. Finally, we conducted in-person site visits to three different locations: Northern Florida, Central Michigan and Western Oregon. As part of each of these site visits we held in-depth discussions with leadership, epidemiologists and clinical staff from LHDs and SHAs.
Meetings conducted for in-depth case studies produced a broad understanding of systems used by SHAs and LHDs in a single geographic area. We discussed systems supporting all functions and identified and investigated specific barriers impeding progress on public health informatics.
We selected locations with a recent history of innovation. We also selected cases to be geographically diverse and to represent different models for governing and managing public health functions. For example, we selected Florida, where all LHDs are part of the state infrastructure and two others, Michigan and Oregon that have a decentralized model. In Michigan, we explored the opportunities afforded by the presence of a “superagency” supporting both public health and Medicaid. In all three cases we met with relevant officials from the SHA as well as staff and leadership from two LHDs. Exhibit 2 below lists the specific departments and discussant categories that we covered in each of these cases.
Exhibit 2: Summary of In-Depth Cases
| Case Study Region | Agencies Covered | Discussants | Key Topics of Interest |
| Northern Florida | Florida Department of Health Duval County Health Department Alachua County Health Department State Health IT Coordinator | Leadership from state and local agencies (IT and overall): Meade Grigg, Tom Herring, Bob Harmon State and local epidemiologists: Janet Hamilton, Karen Elliott Clinic staff for TB, HIV/AIDS, STDs and primary care: Victor Ferreira State-wide surveillance leaders: Jo Ann Steele State registry leadership (immunization, newborn screening, vital records): Susan Lincicome, Lois Taylor Environmental health leadership Health Information Exchange Stakeholders: Heidi Fox | ■ Home grown public health clinical management system ■ Home grown STD tracking system: PRISM ■ Syndromic surveillance using the ESSENCE system ■ Epidemiologic case reporting using Merlin ■ Large state with consolidated model (locals report to the state) |
| Central Michigan | Michigan Department of Community Health Mid-Michigan District Health Department Ingham County Health Department | Leadership from state and local agencies (IT and overall): Cynthia Green-Edwards, Marcus Cheatham, Debbie Edokpolo, Corinne Miller, Jim Collins, Carol Callaghan, Alethia Carr State and local epidemiologists: Patti McKane, Mary Kleyn, Norm Keon, Cassandre Larrieux Clinic staff for TB, HIV/AIDS, STDs and primary care State-wide surveillance leaders State registry leadership (immunization, newborn screening, vital records) MCIR Region 3 Support: Hazel Hall Environmental health leadership: Bob Gouin Health Information Exchange Stakeholders | ■ Implementation of EHRs and HIE efforts at LHDs ■ Advanced use and expansion of the state immunization registry ■ Establishment of a Medicaid data warehouse with plans to integrate data from public health agencies ■ CMS awards for using community-hubs and care coordination ■ Home grown disease surveillance system ■ Partnership and integration between Medicaid and Public Health |
| Western Oregon | State of Oregon Health Authority Multnomah County Health Department Washington County Health and Human Services | Leadership from state and local agencies (IT and overall): Dina Dickerson, Shawn Messick, Kathryn Broderick, Robert Johnson State and local epidemiologists: Sean Schafer Clinic staff for TB, HIV/AIDS, STDs and primary care: Michelle Karaffa State-wide surveillance leaders: Kenneth Rosenberg State registry leadership (immunization, newborn screening, vital records): Mary Beth Kurilo, Jennifer Woodward Environmental health leadership Health Information Exchange Stakeholders | ■ Utilization of OCHIN practice management system and EHR by LHDs ■ Use of public health focused EHRs by some LHDs ■ Development and/or adoption of electronic case management systems in local agencies ■ Role of LHDs in community health assessment ■ State vision for streamlining capture of public health data ■ Impact of coordinated care organizations on HIT |

We worked closely with the TEP at the early stages of the project to define criteria for case study selection and discussion topics. Overall our questions related to the following areas:
■ The use of IT in current public health practice
■ Funding for IT investments in public health
■ Unmet needs and challenges related to using IT to further public health objectives
■ Potential role of HITECH, ACA and other federal initiatives
■ Opportunities and challenges related to integrating disparate data systems related to public health or enabling effective exchange of data across systems
■ The role of recent and ongoing public health informatics initiatives
■ Cultural, organizational and leadership factors affecting effective use of information systems to support public health function
■ Potential paths forward in terms of federal funding, strategy and planning on the part of SHAs and LHDs
In the section that follows, we provide some background on the core public health functions and how public health practitioners use IT.
In this chapter we describe some aspects of public health mission and operations focusing on the ways in which public health officials use information systems. Importantly, we distinguish between the concepts of “informatics” and “IT” throughout the report. A premise of our report is that informatics or the science of how to organize the capture, management and exchange of information to support specific functions should drive decisions related to the use of IT in public health.
Public health officials monitor health status and factors influencing health and improve access to resources supporting population health. Public health officials also develop and carry out policies that protect health and ensure safety.[13] To achieve this mission, public health officials need timely access to accurate data from a variety of sources. Increasingly, technology allows us to capture, exchange, manage and analyze these data electronically. [14] However, best use of this technology requires financial and human resources. Most core public health systems work with population-wide data obtained from clinicians and hospitals, clinical laboratories, social service providers, and clinicians and inspectors. However, LHDs also work with data on the specific population they serve as direct providers of care (often uninsured and vulnerable groups).
In monitoring the factors affecting population health, LHDs and SHAs address areas prioritized by policy makers. These include areas where categorical funding by the Centers for Disease Control and Prevention (CDC), Health Resources and Services Administration (HRSA) and other federal agencies support specific activities as well as priority areas for state and local officials.
LHDs and SHAs track and monitor data on health and health-related factors in a number of ways. Public health officials capture these data both to meet government reporting requirements and to target specific services to individuals and communities. Data on conditions designated as notifiable diseases under the laws of a given state are captured from health-care providers as are data to support population-based public health records for immunizations, newborn screenings, vital records (birth and death records) and other diagnoses (e.g., cancer, birth defects) as required by the state.
The usefulness of these systems depend to some degree on whether data can be brought together to produce a comprehensive picture of the health of individuals in a community. In the paragraphs below, we discuss how information systems generally support different core public health activities such as disease reporting, registries, surveillance, and case management.
Reportable disease surveillance and case investigation. Under the United States Constitution, states retain the police powers associated with public health assurance. Therefore, state laws govern requirements regarding reporting of diseases of public health significance. SHAs collect information on approximately 60 defined notifiable diseases (exact numbers vary by state). Providers are legally required to report information on new diagnoses (cases) to the state. Although requirements for case reporting vary modestly from state to state, public health officials are moving towards increased harmonization of these requirements through working with the Council of State and Territorial Epidemiologists (CSTE) and the CDC.
National Notifiable Disease Surveillance System (NNDS)
The NNDS is the system used by the CDC to monitor the occurrence and spread of nationally notifiable diseases reported voluntarily by states to the CDC. The National Electronic Disease Surveillance System (NEDSS) provides standards and support to states in establishing systems to capture notifiable diseases. This includes support for electronic lab reporting (ELR) into state surveillance systems when hospital or free-standing laboratories find positive test results for notifiable conditions. As of October 2011, approximately 15 states used the NEDSS Base System (NBS) for notifiable disease surveillance. NBS is a tool developed by CDC that states can use to capture information on the occurrence of notifiable conditions in their state, provide aggregate reports to the CDC and support the case investigation efforts of local public health agencies.
Although all health-care providers are required to report notifiable diseases, the vast majority of reports come from clinical laboratories and infection control professionals in the hospital setting. For most notifiable diseases, data provided to state and local authorities includes names, but state officials de-identify these data for voluntary reporting to the CDC (see text box below on the National Notifiable Disease Surveillance System). Public health officials manage data about affected individuals using disease surveillance systems and epidemiologic case management systems so LHDs and SHAs can engage with affected individuals, health-care providers, their associates and others.
These case reports required by state law serve two purposes. First, they allow follow-up with individuals to prevent the spread of communicable disease and limit adverse effects. Second, they allow public health officials to study the relationships and trends in the incidence of diseases that affect population health, identify potential unmet needs and plan interventions.
In many ways, SHAs and LHDs have been moving towards electronic reporting of notifiable conditions. Many states have worked with national clinical laboratories and hospital based laboratories to establish electronic laboratory reporting (ELR) from a laboratory information system (LIS) to the state’s disease surveillance system, automating laboratory results for notifiable diagnoses. Many states also now have online portals where providers such as hospital-based preventionists or public health clinicians can enter data on notifiable diseases. In some cases, notifiable diseases are diagnosed and treated presumptively without diagnostic testing, and these cases are underreported due to limited clinician (i.e., not laboratory) reporting.
For capturing, maintaining and analyzing surveillance data, some states take advantage of the National Electronic Disease Surveillance System (NEDSS) Base System,[15] developed by the CDC, while others rely on similar systems developed by in-house developers or by vendors. Automated and seamless exchange of structured data represent an important challenge for public health reporting. Notably, states have largely automated the process of reporting de-identified data on notifiable conditions to the CDC. In this regard, the 2011 ASTHO Profile of State Public Health indicates that 90 percent of states report communicable disease electronically to the federal government.[16]
In many states, regardless of whether reports are filed by hospitals and physicians, data on notifiable conditions diagnosed using clinical laboratory tests are reported to public health agencies automatically through ELR applications that identify notifiable conditions within a set of results active in a laboratory system and transmit standardized messages with relevant information to populate a case directly to the SHA system. Hospitals can use ELR reporting to address Meaningful Use criteria under HITECH’s EHR incentive program.[17]
Maintaining population-based public health record systems. SHAs also collect, maintain, and report population-based clinical information associated with preventive services, screenings, or diagnoses of specific public health relevant conditions. Registries or stand-alone record systems often track information services of importance to younger populations such as immunizations, newborn screenings, and hearing exams. These systems can also provide a means for tracking chronic conditions such as diabetes, as well as for identifying trends in the diagnosis of diseases susceptible to environmental factors, such as cancer.
In all of these cases, federal, state and local stakeholders have developed specifications to use common messaging standards to obtain these data from health-care providers electronically. Stakeholders have recently developed specifications for electronic exchange of data between hospitals and SHAs for newborn screening.[18] In most states, immunization registries give providers access to information on the immunizations their patients may have received with other providers and facilitate required reporting from the providers to the state electronically through interfaces with provider systems or portals where provider staff enter data online. Electronic reporting to cancer and immunization registries are criteria for Meaningful Use of EHRs under HITECH.
Syndromic surveillance. In addition to reportable disease surveillance, state and local public health agencies are responsible for monitoring the trends of significant medical symptoms. Syndromic surveillance provides rapid awareness of surging illness rates even before definitive diagnosis. It tracks emerging health conditions for which case-based reporting has not been established or may be impractical due to volume (e.g., influenza).
In recent years, the CDC has adopted syndromic surveillance as a key strategy for early detection of conditions and infections including those caused by bioterrorism and pandemic influenza. Typically, syndromic surveillance uses trends in the occurrence of patient complaints to detect statistical anomalies in syndromes (rash, acute respiratory illness) that may signal outbreaks. Syndromic surveillance also helps officials assess trends over time, in different geographic areas and among specific populations.
The CDC’s BioSense 2.0 project supports standardized capture, storage and analysis of syndromic surveillance data and collaboration for public health at the local, state, and federal levels.[19] Some states have adopted BioSense as a mechanism to facilitate syndromic surveillance at all levels of government. CDC plans to examine stakeholder requirements and needs assessments to determine how to best meet the needs of SHAs and LHDs.
They aim to have 80 percent of the population covered by BioSense by 2015. The CDC has also indicated that they may find a need to expand the BioSense platform to incorporate other applications commonly used by states for syndromic surveillance. For example, many states have adopted the ESSENCE application originally developed by the Department of Defense to support their own syndromic surveillance work. Electronic reporting of syndromic surveillance data is among the criteria that health-care providers may use to establish Meaningful Use of EHRs under HITECH Medicare and Medicaid incentive programs. The International Society of Disease Surveillance (ISDS) developed guidelines for electronic exchange of syndromic surveillance data.[20]
Environmental health. LHDs also license and inspect restaurants, water treatment facilities, swimming pools, septic tanks and other facilities and equipment. They maintain information on these facilities to assess and track environmental health risks. LHDs often maintain separate systems to capture this information to support public safety.
Characterizing and supporting community health. SHAs and LHDs also aggregate data from surveys, public health reporting systems and other data sources to help service providers and leaders in a community assess health status and needs. In particular, many SHAs and LHDs develop state and community profiles that capture information on health risks, incidence of significant disease, demographic trends and other factors affecting health. These profiles then help support effective allocation of public health and health-care resources.
As in the case of the Beacon Community Cooperative Agreement program described below, new programs may leverage this public health function to improve outreach to at-risk populations and support better care and outcomes. Community profiles developed using data from EHRs can help providers and public health professionals target health education and locate resources in areas of greatest need.
As a part of the assurance function, public health departments often provide services directly to individuals. The nature of these services varies considerably across different states and local jurisdictions. Clinical services provided by public health include primary care, family planning, some maternal and child health services, oral health, HIV screening and treatment, and tuberculosis (TB) and sexually transmitted disease (STD) care. In many cases, public health nurses with bachelor’s degrees provide these services under protocol orders set by a physician or advanced practice nurse. This is significant, in part, because these individuals (Bachelor’s degree level public health nurses) do not qualify for Meaningful Use payments under HITECH (discussed below).
In addition to clinical services, personal health services provided by public health agencies include case management, care delivered as part of home visitation and care coordination for selected populations. In providing these services, public health staff capture and maintain data used in the course of delivering care. The personal health services offered by LHDs vary by jurisdiction. This is due to differences in state priorities and a given state’s approach to implementing federal programs under Title V and other federal programs.
In a limited number of jurisdictions, LHDs house Federally Qualified Health Centers (FQHCs) or other primary medical care services for groups who otherwise lack access to care. In this capacity, public health clinicians often work to detect and address risk factors associated with the onset of chronic conditions, such as diabetes and heart disease. They also provide immunizations, screenings, routine physical examinations and health education services designed to maintain and improve health among vulnerable groups. Finally, primary care providers in a public health context work with patients to manage and control chronic conditions after diagnosis to help patients avoid costly complications and maintain a viable quality of life. In the area of communicable diseases, public health providers are often the only source (or only free source) of treatment, preventive services and counseling for STDs, HIV/AIDS and TB.
Public health-based clinicians both use and contribute to data housed in public health information systems, such as statewide record systems for immunizations and newborn screenings, vital statistics, syndromic surveillance, epidemiology, environmental health, and other relevant data streams. Also, as medical providers, public health providers can use and contribute to data exchanged electronically with clinical laboratories, pharmacies, inpatient providers, long term care facilities, medical specialists, and others. This may occur through one-to-one exchange or via centralized health information organizations (HIOs) including those supported by HITECH’s State HIE cooperative agreement program.[21],[22]
Like other health-care providers, some public health clinicians use practice management systems (PMS) to store admission, discharge and transfer (ADT) data such as demographics. In some cases, they also use EHRs configured or customized to meet their needs. A limited number of public health clinicians can qualify for HITECH sponsored Medicare or (more likely) Medicaid Meaningful Use payments as eligible providers. The 2010 Profile of Local Health Departments published by NACCHO shows that approximately 15 percent of LHDs use some form of PMS and another 19 percent use some form of EHR.[23]
Notably, some public health clinical settings face a disadvantage with respect to achieving Meaningful Use, both because stakeholders note the dearth of certified EHR products geared to meet the needs of public health and because public health nurses with bachelor’s degrees do not qualify as “eligible providers” under HITECH.
Public health officials have broad responsibilities to monitor and assure population health and track factors related to health in their states and communities. Data relevant to this mission comes from multiple governmental and non-governmental sources. As noted above, LHDs capture and maintain data on a small portion of the population in the context of delivering personal services including clinical and case management services. LHDs also maintain data related to other services such as their environmental health protection responsibilities.
Local public health officials are required to submit some of these data to SHAs to meet reporting requirements of federal programs administered at the state level (e.g., Title V, Maternal and Child Health grants) and standard public health reporting (e.g., communicable disease and immunizations) required of all health-care providers in the state.
Addressing the Needs of Patients with Sickle Cell Disease (SCD)
The Registry and Surveillance System for Hemoglobinopathies (RuSH) pilot program sponsored by CDC and NIH demonstrates the value of bringing different existing sources of data together to support public health action.[24] In this example, public health leaders seek a resource to answer basic questions related to the incidence of SCD in their state, trends in how the condition is treated, develop an understanding of the needs of these patients and ultimately improve the quality of care provided to reduce the burden of illness. To do this, states participating in the pilot worked to pull together relevant data from a number of the data sources identified in Exhibit 3, including vital records and newborn screening for incidence and creation of cases (this works for recent cases and for cases where the patient was born in the United States), and then immunization records and claims data from public payers to assess the progression of the illness and methods of treatment. Pilot states found the linking of records to create these registries was possible, but required extensive work to identify the legal basis for accessing different data sets for this purpose and the technical task associated with linking data across disparate sources to a common patient. Importantly, in many states there is no established way to create new repositories of this kind populated from multiple data sources on an ongoing basis.
As we have seen, private health-care providers and clinical laboratories report data on specific communicable diseases, immunizations, results of newborn screenings and vital records to the state. Health-care stakeholders maintain other data relevant to public health (but not currently reported to SHAs), including patient data in EHRs and health-care administrative data from public and private payers.
Finally, some data relevant to public health fall outside of traditional health-care and public health sphere entirely. These include data relevant to the social determinants of health and services designed to help address broader social priorities such as housing, nutrition, criminal justice, education and heating assistance.
In current practice, most stakeholders managing these data use the information in limited ways and share data only under legal reporting requirements. Many stakeholders envision a future where data across disparate systems can be brought together efficiently to provide richer information to support a range of decisions affecting personal and population health. Improved ability to query and analyze these data could help public health administrators, managers, clinicians and case managers provide appropriate services to individuals, support improvement in health-care quality and outcomes on a population level, facilitate emergency response and preparedness and help plan needs-based allocation resources. Exhibit 3 below outlines some of the major sources of data of public health relevance.
Exhibit 3: Sources of Data Relevant to Public Health Practice and Questions for Stakeholders
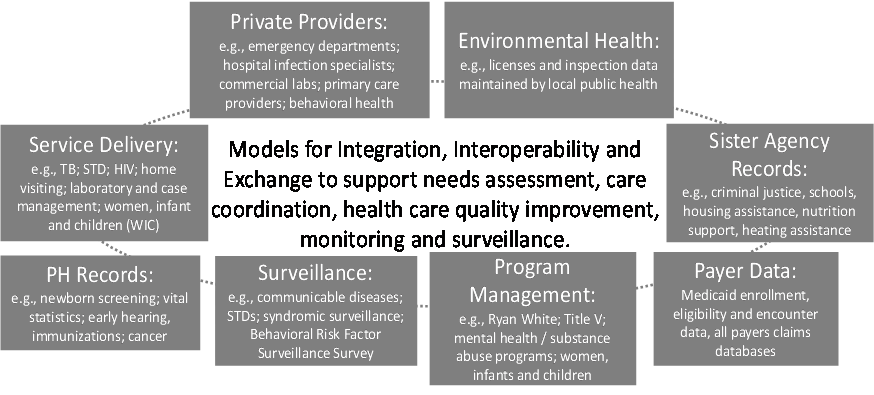
As noted in Exhibit 3, agencies outside of public health often manage data relevant to the social determinants of health. A significant challenge to linking public health to other sources of health data is privacy. Public health is dependent on the health-care sector for clinic and patient level data.[25] Federal policies such as the expansion of the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule under the Recovery Act (disclosure of personal health information needed for patient care and other important purposes) to business associates and more stringent disclosure requirements may create new processes for data access.
Linking Data in South Carolina
In South Carolina, the state’s Budget Control Board Office of Research and Statistics has developed a linking algorithm that allows public health officials and other authorized state employees to query dozens of state agency databases for data on client services and demographics. Datasets included in this initiative encompass claims from Medicaid, public health records, environmental health, social service data and other state data sources. This query capacity combined with mapping technologies allows South Carolina officials identify high-need areas and target resources and support a number of population-health use cases. In addition to technical challenges associated with matching cases across different datasets, officials in South Carolina spent decades working on technical architecture and data-sharing policies to facilitate this effort. They have developed a framework and culture of cooperation that they were able to leverage resulting in quick progress on new funding initiatives. When the State Health Information Exchange Cooperative Agreement program was initiated, the state was able to use this source of funds to address well understood gaps in the ability to capture and exchange clinical data in the state.
Furthermore, federal privacy laws in other sectors similar to and including the Family Educational Rights and Privacy Act (FERPA) complicate data exchange among community partners.[26] State policies can also complicate efforts to share data. Taken together federal laws and state policy form a patchwork of privacy laws that extend beyond HIPAA. This poses a challenge to inter-jurisdictional and cross-program information exchange. Additionally, when behavioral and mental health service data are exchanged, compliance with federal rules under Title 42 Part 2 of the Code of Federal Regulations (CFR) entitled “Confidentiality of Alcohol and Drug Abuse Patient Records” applies. Finally, organization-level privacy and data-sharing policies complicate matters even further.
Still, states that are adopting models to overcome data sharing barriers can achieve important benefits from consolidating data from public health, health-care delivery and social service programs. The state of South Carolina (highlighted in the text box) and Montgomery County Maryland offer examples of jurisdictions that have made progress in breaking down barriers to accessing data from multiple government sources that are relevant to public health. In Montgomery County, the Department of Health and Human Services provides services to over 120,000 residents. Most of these residents receive services from more than one clinic or program so the county developed a global data sharing and confidentiality policy with clearly understood rules on sharing data.
Like other jurisdictions, Montgomery County is working on developing a technical infrastructure that would support access to these data for public health purposes. In some cases, they see opportunities to leverage state-supported technical solutions to support health information exchange (HIE). Potential benefits include a “front door” or “no wrong door” approach to determining eligibility and enrolling individuals and families in benefits programs. Cross-sector data integration also can provide increased access to data on social service needs and benefits for public health and health-care case managers and care coordinators.
Public health stakeholders cite funding limitations as a barrier to more effective use of information systems. Recent analysis, including some recently concluded by the Institutes of Medicine (IOM) suggests that public health is underfunded generally and that the funds that are available do not offer public health stakeholders the flexibility required to make strategic investments in infrastructure.[27]
Variation in the functions and priorities of public health agencies in different jurisdictions relate to differences in available funds and spending. For example, some smaller county health departments spend less than a few hundred thousand dollars per year, while major city health departments can spend upwards of several hundred million dollars. Per capita spending among LHDs varies as well between over $50 and less than $20 dollars per resident depending on the jurisdiction.[28]
Key sources of funding. The majority of financial support for most LHDs comes from a handful of categorical sources of funding. In 2010, NACCHO reported that 26 percent of funding for LHDs came from general revenues from local governments, 21 percent from state funds, 14 percent from federal funding passed through the state such as Title V and Ryan White program initiatives and another 6 percent came directly from the federal government. LHDs receive smaller amounts from third party reimbursement for clinical services (13 percent from Medicaid) and fees for delivering services (7 percent). Importantly, these averages do not illustrate the wide variation in the level of funding from different sources for public health across jurisdictions and between states.[29]
2011 data from ASTHO shows that the plurality (45 percent) of funding for state public health agencies comes from federal sources, 39 percent from state funds and the remainder from a variety of smaller sources including fees and fines. The same report shows that the plurality of expenditures by SHAs in 2009 went towards infectious disease programs (13 percent) while 1 percent each went to health data and vital statistics and 5 percent went to administration.[30] Stakeholders note that there is limited integration and strategic planning among funders and within and across federal, state and local government.
Trends in public health funding. Regardless of the source of funding, stakeholders note serious challenges with maintaining steady funding to SHAs and LHDs. Public health currently accounts for less than 0.1 percent of GDP and only 3 percent of federal health-related expenditures.[31] In recent years, stakeholders note reductions in funding for public health with negative consequences for making strategic investments in information systems.
In 2011, 58 percent of LHDs reported core funding cuts, and 55 percent reduced funding to at least one program. Furthermore, LHDs faced budget reductions of 52 percent in the next year.[32] Because of budget shortfalls at the federal, state, and local levels, public health has lost 15 percent of the state and local workforce from 2008 to 2011. Forty four percent of LHDs and SHAs reported that they lost staff in 2011.[33]
An Institute of Medicine report released in April of 2012 looks at public health investments and how federal initiatives can assure allocation of appropriate resources to population health. The report advocates for the development of a common “minimum set” of public health activities and ongoing federal investments to enable public health officials to uniformly conduct these activities.[34]
Factors driving IT and systems investments in health departments. Relatively little systematic information is available on funding for public health informatics or information systems. However, many stakeholders report the need for more investment and more effective use of existing investments in public health systems infrastructure. We found that bureaucratic and program related factors affect systems investments. For example, because LHDs and SHAs typically sit within a larger governmental structure, department practitioners do not always direct or control how governmental IT staff makes decisions regarding new investments in IT systems and capacity.
Stakeholders note that current methods for funding public health systems establish incentives to create data silos. An agency that begins receiving funding under a specific grant may use these requirements to justify the acquisition or development of a new system to capture, manage and report information for that specific grant. Sometimes assets procured under a grant are restricted from use for other purposes. Over time, this results in a series of program-specific data silos, not allowing officials to easily integrate data across systems. Most state and local officials we spoke with acknowledged that relatively few programs actually require the development of a new system. However, in the absence of clear incentives to build upon existing systems to meet new requirements, those responsible for administering a grant often find it easiest to establish a new mechanism meeting an immediate need.
We did however find some examples of specific initiatives designed to overcome the potential silos created by programs funded under categorical grants. In New York State, the Department of Health’s Division of Family Services (DFS) has used funding from the HRSA-administered Maternal and Child Health Services Title V Block Grants and the State Systems Development Initiative to undertake a program called Child Health Information Integration (CHI2), which aims to integrate newborn screening, newborn hearing screening, immunization, lead, early intervention, WIC, Medicaid, vital statistics and other data sources into one interface and create bi-directional sharing of DFS’s maternal and child health data with its external partners. To address this issue broadly, many stakeholders call for the federal programs to provide a clear signal to encourage integration and allow agencies the flexibility to use program funding to support a common data infrastructure.[35]
In this chapter we focus on the specific opportunities to advance the use of health IT to support public health objectives occasioned through HITECH and the ACA. In the paragraphs below we highlight specific initiatives and how they affect public health based on discussions with stakeholders as part of our case studies.
The Medicare and Medicaid Electronic Health Record Incentive program creates financial incentives for eligible health care providers (individual clinicians and hospitals) to adopt EHRs and to meet criteria defining “Meaningful Use.” Meaningful Use criteria are being developed and rolled out in stages. Under Stage 1 Meaningful Use, CMS identified three “menu set” criteria related to public health reporting. Two of these criteria, sending data electronically from EHRs to immunization registries and sending information relevant to syndromic surveillance electronically from EHRs to state public health agencies, apply both to eligible hospitals and eligible providers. The third Stage 1 public health “menu set” criterion, sending electronic laboratory results to the state’s public health system, applies only to eligible hospitals with in-house laboratories.[36]
As part of Stage 2 Meaningful Use for eligible providers, transmission of continuous immunization data to the state registry is a “core” or required criterion. Eligible providers under Stage 2 are also required to meet three of six “menu set” criteria which include three public health criteria: successful ongoing transmission of syndromic surveillance data; successful ongoing transmission of cancer case information; and successful ongoing transmission of data to a specialized registry. For eligible hospitals, Stage 2 Medicaid Meaningful Use includes three “core” (or required) objectives related to public health including ongoing transmission of syndromic surveillance data, immunization data and electronic laboratory results.[37]
Implications for local public health agencies. As noted above, providers practicing at LHDs may also be eligible providers under the program definition for Medicaid Meaningful Use. Providers meet eligibility criteria if they have appropriate credentials (physicians or nurse practitioners); provide services that are reimbursable under Medicaid; and maintain at least a 30 percent Medicaid case load. To receive Medicaid Meaningful Use incentive payments (up to more than $63,750 over six years), eligible providers at LHDs, like any traditional health-care provider, have to demonstrate they have adopted a certified EHR in the first stage and in subsequent stages demonstrate that they are using the EHR to support functions included in the criteria for Meaningful Use.
We spoke with some LHDs with extensive safety net primary care programs including FQHCs that have already adopted certified EHR systems and are moving rapidly towards demonstrating Meaningful Use and receiving Medicaid Meaningful Use payments. Public health agencies whose direct patient care services focus on specialized areas such as HIV/AIDS, STDs, TB and family planning are less likely to have already adopted a certified EHR. They also express interest in achieving Meaningful Use over time, but face challenges in terms of finding and adopting certified EHR products that meet their need for extensive case management.
As noted above, public health nurses with BSN degrees provide much of the care in LHDs. These individuals are not eligible providers under Meaningful Use. Additionally, because public health clinics (not FQHCs) offer a constrained set of services, they may not meet Medicare or Medicaid thresholds. Finally, Meaningful Use criteria specify certain standards for electronic messaging, (e.g., use of vocabulary standards such as HL7) which are not commonly used among many public health agencies accustomed to more rudimentary methods for electronic transfer (e.g., flat file imports).
State public health agencies and Meaningful Use. In the case of each public health Meaningful Use criterion, state public health agencies are recipients of data and must be able to cooperate with providers to allow for electronic reporting and confirm effective exchange of data for testing. Despite noting limited funding, SHAs we met with had moved relatively quickly to allow providers to take advantage of the criteria for reporting of electronic reporting of immunizations and ELR for notifiable diseases.
HITECH invested resources to support eligible professionals and eligible hospitals in meeting these requirements through the Health IT Research Center (HITRC), an initiative providing a community of practice and online resources to support Meaningful Use. Recently, the HITRC developed guidance supporting exchange with immunization registries and a tool to develop an inventory of EHR vendor capacity in this area. In addition, the CDC has sponsored a new initiative supporting ELR for disease surveillance as part of the Laboratory Interoperability Cooperative.[38]
Opportunities to enhance public health systems to support Meaningful Use. Some states are using federal 90 percent matching funds to support investments in public health systems for Meaningful Use. These opportunities are available under State Medicaid Director Letters 10-016 (Federal funding for Medicaid HIT activities)[39] and 11-004 (Federal funding for HIE development).[40] Eight states have received funding to support different initiatives. For example, Massachusetts is developing a single public health gateway to obtain data on reportable laboratory results, immunizations and syndromic surveillance from eligible providers and eligible hospitals.
Other states that have received authorization for systems improvements to facilitate public health reporting under Meaningful Use include North Carolina, Iowa and Arizona.[41] However, stakeholders note that in many cases public health departments cannot fund the 10 percent required to take advantage of these funds or do not have close ties to their Medicaid agency to facilitate this use of matching funds.
State HIE Cooperative Agreement Program. HITECH also created a cooperative agreement program providing resources to states to facilitate and enable HIE among providers. State officials can address the issue of supporting HIE in different ways under this program. In some cases, states have focused on creating state-wide resources to enable exchange that would allow providers to query or search for and retrieve data on individual patients from other providers. In other cases, states count on the ability to support and link across regional HIE initiatives within their state. Elsewhere, states provide opportunities for providers treating the same patients to send and receive clinical information to each other.
In conducting activities under the program, many states report that they are actively engaging public health. In a recent review of 27 states’ activities under the program, 74 percent indicated that their SHA is heavily involved in state HIE activities and slightly less than half of these states indicated that they support public health use cases for HIE such as exchange with immunization registries or notifiable disease reporting.[42]
In the case of state health officials participating in our telephone and in-person discussions, some noted the presence of a “public health node” being developed as part of their cooperative agreement work. In some cases, such as Illinois, this refers to a single reporting interface that would accept different types of public health messages (e.g., immunizations, cancer case reports, syndromic surveillance information, and lab results) from provider systems. In other cases, such as Florida, the “public health node” allows health departments to query data on their patients from other providers.
Beacon Cooperative Agreement Program. Under the Beacon Cooperative Agreement Program, managed by the Office of the National Coordinator for Health IT, 17 Communities (represented by providers, public health agencies and other organizations) across the country receive resources to build and strengthen their health IT and HIE infrastructure and to implement improvements in health-care delivery that take advantage of health IT. Each community developed interventions tailored to their needs and chose specific and measurable improvement goals relating to quality, efficiency, and population health.
These interventions include the use of care managers, more deliberate and structured care transitions and use of clinical decision support tools to meet specific objectives. Some Beacon interventions represent variations on emerging practices such as the use of patient-centered medical homes (PCMH), physician profiling through regular quality reporting, use of health IT (including text messages) to improve patient education and outreach, telemedicine and structured referral management.
Some Beacon projects actively involve SHAs and LHDs. For example, in the Southeast Minnesota Beacon Community, public health-care managers are helping to ease transitions between public health and hospital settings by helping to eliminate duplication of effort through more timely, electronic exchange of information at discharge from hospitals. One county that is taking part in the Southeast Minnesota Beacon, Olmsted County, notes early success in reducing hospital re-admissions for diabetes and childhood asthma by facilitating communication across providers using data captured from their EHRs in a CCD format.[43] The cost savings associated with this outcome has the potential to generate new revenue for the LHD and providers who support care coordination.
Additionally, in Utah, the Beacon Community is working to build on the state’s pre-existing HIE plan by connecting hospitals, practice sites, laboratories and other support providers and public health agencies to the UHIN’s statewide clinical health information exchange. The Southern Piedmont Beacon Community in North Carolina is developing a public health portal, which is an interactive web-based, geo-mapping tool that allows stakeholders, including representatives from LHDs, to combine, analyze and display health information. Finally, the Crescent City Beacon Community in New Orleans is using EHR data to monitor and improve care for diabetic patients.
The Affordable Care Act changes the landscape for public health. It addresses preventive services by issuing new coverage requirements and investments in a Public Health and Prevention Fund.[44] The ACA strengthens Title V programs through the funding of Maternal, Infant, and Early Childhood Home Visiting Program.[45] The ACA also establishes demonstration projects encouraging care coordination and community-based strategies for improving health outcomes for individuals and groups. It helps streamline enrollment in Medicaid and human service programs by offering considerable federal support to state efforts to streamline eligibility determination systems.[46] Finally, ACA creates a new requirement for non-profit hospitals to conduct community health needs assessments and developing strategic action plans to govern their community benefit investments.[47]
Opportunities for Public Health Agencies under ACA
In many ways, the ACA promotes principles that align with the population health objectives and operational strengths of public health agencies. The law creates a series of demonstration and pilot programs under Medicare and Medicaid that emphasize the importance of managing referrals, care transitions and providing other care coordination services.
LHDs provide care coordination, case management and referral management as part of their everyday practice. Many staff at LHDs communicate and coordinate across different service providers (e.g., behavioral health, primary care, substance abuse services, human service providers and others) and may serve as useful contributors to these demonstration programs.
Some ACA programs leverage the “pathways community hub” model where community health workers coordinate across social services, behavioral medical care, public health, housing and other sectors.[48] These hubs serve to track service delivery and assure the accountability and quality of the services provided to a population of high risk individuals. Many public health agencies can provide this service if they have the appropriate relationships and contracting mechanisms in place. However, the ACA does not create a specific role in these demonstration projects or other initiatives for LHDs and SHAs. Some stakeholders expressed concern that absent investments in public health infrastructure to support these new coordination efforts, other entities will provide them making LHDs less relevant and, perhaps, limiting the benefits associated with the programs.
Promising Models for Public Health Engagement with Health-care Providers
Many of the opportunities facing public health agencies under ACA require active engagement with health-care delivery and financing organizations. SHAs and LHDs conducting data-based health needs assessments might drive improvement in the health-care delivery and patient engagement. For example, LHDs may be in the best position to complete the ACA-mandated community health needs assessments (CHNAs) and implementation planning efforts on the part of non-profit hospitals.
We identified pockets of innovation where LHDs and SHAs help address goals of the ACA by providing analytic resources. For example, Denver Health collaborates with local ambulatory care providers to establish a cardiovascular disease (CVD) registry, populated by EHRs from providers in the community. Denver Health provides reports and analysis from the registry to guide quality improvement. This effort was supported through Community Transformation Grants (CTG) supported through CDC.
In New York City, the Department of Health and Mental Hygiene (DOHMH) initiated and operates the Primary Care Improvement Project (PCIP). This project helped support EHR adoption among safety-net clinics and small provider offices in New York City. Currently, PCIP uses EHR data to track key primary care metrics related to the city’s public health priorities. DOHMH aggregates EHR data and produces city-wide reports on public health priorities. They use practice level reports to help clinicians with quality improvement, PCMH accreditation or other quality and prevention goals.
In another example, the Blueprint for Health program-based in Vermont is a state public health initiative that encourages patient centered medical home and coordinated care for populations covered by multiple payers in the state. The program includes active engagement between community health teams consisting of care coordinators embedded in primary care practices and group of community based organizations and public health clinics that serve as “extenders” to assure access to services such as behavioral health, counseling, prevention and other services. Exchange of information on patients facilitated through use of EHRs, robust HIE and the use of registries to track needs of specific populations.[49]
Stakeholders believe demand for analysis on community-level health-care quality will increase because of ACA and cost-containment efforts. As EHRs increase available data for tracking cost and quality of care, public health officials need models for using these data. A recent article in the New Yorker by Atul Gwande illustrates how provider-generated data identifying frequent users of health-care services can facilitate targeted interventions.[50] The article describes how robust data can improve provider performance assessment through geographic surveillance of trends.
Public health may be in a good position to play a neutral arbiter role by using provider-generated data to profile care in a community. These data may help target preventive services to areas of greatest need and guide provider-initiated quality improvement work. However, it is likely that improvements in infrastructure, new analytic models and additional workforce training will be necessary. A 2010 NACCHO report shows that local health department staff prioritized “using clinical data to improve quality of care” as a subject for training over other informatics topics.[51]
New Roles for Public Health
Taking advantage of the opportunities described above requires some public health agencies to re-position within their environment. Engagement with health-care providers and payers means setting up new relationships and administrative mechanisms to support contracting. More coverage for preventive services may lead to increased emphasis on billing and collecting from third-party payers. However, these provisions may have the unintended consequence of reducing the need for categorical funding to public health for preventive services.
New ACA rules requiring health insurers to offer more comprehensive coverage of preventive services may have the unintended consequence of reducing the need for categorical funding to public health for preventive services. Some stakeholders note that public health agencies will need to position themselves as “preferred providers” of screening and prevention services newly covered by private insurers for specific populations, or focus more specifically on outreach to populations who will remain uncovered even following full implementation of the ACA.
A March 2012 IOM report emphasizes the need to move towards integrating the activities of population health monitoring and primary care through engaged leadership, collaboration between health-care providers and public health. To come to fruition, public health officials’ interest in use of clinical data requires cooperation and interest on the part of the medical community. The report notes that integration and coordination between public health and health care requires greater collaboration within and across federal agencies such as the CDC and HRSA.[52]
As noted earlier, this report approaches systems and IT as the “means to the end” of better public health practice. Information systems can help public health officials to capture, analyze and share information more efficiently. Ultimately, these systems must support case investigation and follow-up, response to outbreaks, resource planning and other public health action.
The field of informatics helps design work processes and systems that prioritize information needs for parties working towards a common goal. Informatics experts define standard practices for capturing, managing and exchanging data. The goal is to provide stakeholders access to timely, relevant and valid information while avoiding unnecessary steps and redundancy. Informatics projects often focus on achieving interoperability by specifying methods for coding and sharing data that allow seamless transfer of data from one organization to another while meeting each organization’s practice needs.
Informatics projects begin with the assumption that information systems design, adoption and use should serve a well-understood mission. These projects require documenting the business processes and requirements, interactions and data hand-offs for each of the specific activities related to that mission. Before leading to specifications for systems, these efforts lead stakeholders to assess and streamline their day-to-day work.
Several ongoing initiatives highlight the potential for bringing an informatics lens to key public health functions. Notably, the Public Health Data Standards Consortium (PHDSC) is a national non-profit membership-based consortium that creates standards that serve the specific functions and mission of SHAs and LHDs. The PHDSC identifies priorities, designs and tests standards, represents public health within standards development organizations and educates public health practitioners.
To support the goal of interoperability, PHDSC specifies an approach for using the clinical document architecture (CDA) for transferring health-care information for public health. The CDA defines a comprehensive format for organizing and sharing all public health relevant content for a single patient. Some use cases may require exchange of a limited data set for specific purposes (e.g., immunizations or screenings) rather than the full CDA. Regardless of the scope of content being exchanged, messaging standards such as HL7 2.5.1 define data elements for exchange and specify the coding schemes used to represent those elements in a message.
Recently, PHDSC working with the Public Health Reporting Initiative of the S&I framework has developed a constrained specification of the CDA for communicable disease reporting. The specifications would govern how to organize information exchanged for communicable diseases into discrete elements and the taxonomy or codes used to represent each element. PHDSC working with the CDC and the North American Association of Central Cancer Registries also recently piloted electronic reporting standards from ambulatory care EHRs to central (e.g., state) cancer registries using the CDA as the content messaging standard. Reporting to cancer registries is among the “menu” set of Meaningful Use criteria for Stage 2 Meaningful Use.
Most stakeholders agree that the work to develop and test CDA-specifications to support the exchange of data necessary for public health action will ultimately improve access to data among public health officials. However, at this time, experts also agree that establishing and popularizing public health specific CDA-specifications or more systematic use of HL7 2.5.1 for messaging, will not, on their own, address all issues with access to data and interoperability. Public health specifications of the CDA will support interoperability if a large portion of public health agencies prioritize standards and are in a position to require systems developers and vendors to adopt these specifications.
The PHDSC is currently working to establish a more comprehensive public health functional profile (PHFP). This will be a modular framework with a core set of broad interoperability specifications and more specific requirements for different public health functions. Functions would include disease reporting, case investigation, treatment for infectious diseases and delivering family planning services and others.
Once the PHFP is developed, PHDSC will work with EHR standards experts to incorporate these requirements into HL7’s overall functional model for EHR systems. If incorporation of these public health focused requirements becomes part of EHR certification standards, public health officials could benefit. However, realizing this benefit will require improvements in systems used by LHDs and SHAs to receive and use these messages.
Joint Public Health Informatics Taskforce (JPHIT), A consortium focusing on standards and interoperability
JPHIT harmonizes the work of the associations to help public health speak clearly and effectively about public health data and information policy. Organizations collaborating include:
ISDS. International Society for Disease Surveillance. Collaborative agreement with CDC to develop standards for transmission of syndromic surveillance data from EHRs.
CSTE. Council of State and Territorial Epidemiologists. Leads the Electronic Lab Reporting Task Force and published the implementation guide for HL7 2.5.2.
AIRA. American Immunization Registry Association. Collaborative agreement with CDC to develop standards and protocols for exchange of data with immunization registries.
APHL. Association of Public Health Laboratories. Supported by CDC to lead the Public Health Laboratory Interoperability Project.
NAHDO. National Association of Health Data Organizations. Disseminates guidance on integrating state and hospital health data systems and the use of data for quality and health outcome improvement.
NAPHSIS. National Association of Public Health Statistical Information Systems. Leads the development of the nation’s vital events reporting systems.
PHDSC. Public Health Data Standards Consortium. Promotes the development of and use of standards across the public health enterprise.
NACCHO. National Association of County and City Health Officials. Promotes the development of interoperable systems among LHDs and Co-chairs JPHIT.
ASTHO. Association of State and Territorial Health Officials. Works to enhance the capacity of states and territories to address public health needs and Co-chairs JPHIT.
Several additional organizations and groups have also been working to help promote informatics as a central construct for driving decisions related to public health informatics. For example, the Public Health Informatics Institute (PHII) works with public health professionals and their stakeholders on projects centered around requirements development, workflow assessment and informatics training.
In the recent past, PHII has served as the key implementation organization for projects providing grants to public health agencies sponsored by the Robert Wood Johnson Foundation to support public health involvement in HIE through the InformationLinks initiative and helping public health agencies develop new systems requirements beginning with a rigorous analysis of business practices as part of the Common Ground project.
Currently, PHII is engaged with the de Beaumont Foundation to apply their “requirements lab” approach to defining all of the major functions and sub-functions of public health and documenting detailed business processes for public health work. This documentation, though it is likely to apply differently to specific agencies, is intended to lead to consistent and detailed understanding of information needs that will in turn drive the work of standards developers and inform systems and technology decision making at SHDs and LHAs. PHII also runs training and educational programs designed to help public health practitioners apply concepts from informatics and business process re-design to their work.
Associations representing public health practitioners have adopted public health informatics as a priority. Many of these associations work with each other under the Joint Public Health Informatics Task Force (JPHIT). JPHIT members, listed in the text box above, recently developed a consensus framework with a commitment to working towards advancing the application of informatics principles to public health work and assuring public health involvement in HIE efforts.[53]
Finally, the relatively newly established Public Health Accreditation Board (PHAB) is a nonprofit organization focused on developing and implementing accreditation programs that will advance the quality and performance of Tribal, state, local and territorial public health departments. PHAB’s current accreditation standards require that public health agencies develop and maintain an operational infrastructure to support the performance of public health functions. As part of required documentation for this standard, health departments need to demonstrate the use of technology to support public health functions, produce a complete inventory of hardware and describe their capacity for data analysis, word processing and Internet connectivity.
Many of the initiatives described above help create data management and exchange protocols associated with isolated public health activities. Some have suggested a broader approach to defining a comprehensive systems architecture for public health modeled after service-oriented architectures (SOAs) developed for other sectors such as the Medicaid Information Technology Architecture (MITA).
Architectures such as these provide principles or a framework for documenting “practice” needs (or needs related to fulfilling a mission); the information architecture needed to support that mission and the necessary technology components. Implementation in the context of an SOA allows for the development of common services and applications used at different times and as part of different functions. Examples of services that are common to multiple activities within the Medicaid enterprise might include capturing patient demographics and processes for making eligibility determinations and managing provider payments for different covered benefits.
Establishing a single standard data architecture for public health practice offers the benefits of providing detailed guidance and support for public health professionals struggling with the question of how to optimize their use of information systems resources. In some of our case studies, we noted public health leaders’ work on data modeling activities or conceptual diagrams that mimicked some of the characteristics of an architecture. For example, informatics leaders at the Oregon Health Authority developed a public health shared services model with 36 defined public health services organized by 10 IOM-defined functions and domains defined by PHAB.[54] This model has helped underpin the work of other organizations such as PHII.
Some of the vendors we spoke with including Consilience, which offers a product called Maven, are moving towards a modular, SOA-based approach incorporating patient-facing applications such as those used by LHDs as well as reporting and surveillance applications used by SHAs to collect information.
A formal architecture might provide a common basis for SHAs and LHDs to frame their information needs and then make cogent decisions that allow them to meet local needs and maintain a basic level of consistency and interoperability with peer systems. Sometimes the same experts considering development of a public health data architecture note the challenges associated with applying this type of structure to public health systems.
These challenges stem from the idiosyncratic nature of public health functions, governance and operational models at the state and local level and the evolving and dynamic nature of the work of LHDs in particular. Given the importance of state government as the main recipient of public health data, some have argued for state-specific data models or architectures that give guidance to providers and LHDs within a given state.
Another alternative is the use of a platform as a service (PaaS) approach where multiple public health agencies could leverage externally-hosted core services such as database services, MPI services and query tools as well as software products developed in collaboration with CDC, vendors and across public health agencies.[55] While this “cloud-based” model offers a potential low cost way to distribute IT capacity across agencies, mechanisms for implementing the platform, cultivating users and developing a comprehensive set of software applications remains unclear.
Like other public health stakeholders, public health informatics experts work in a dynamic environment with evolving priorities and boundaries. Given the trends described in this report, informatics work may help facilitate the relationship between public health and health-care delivery. For example, public health practitioners may need data specifications and analytic models necessary for validating data from health-care providers (e.g., EHR data), combining them with traditional sources of data (surveys, surveillance systems) and using them for public health action.
A range of public health activities might benefit from use of provider-generated data. Relevant functions might include identifying “high-risk” individuals for targeted case management or seamless and comprehensive syndromic surveillance. Although informatics is distinct from IT, to be effective, recent and ongoing work in the area of informatics will need to guide the design, implementation and use of IT hardware and applications.
For a number of reasons, decision-makers at most LHDs and SHAs do not currently have the benefit of applying the latest thinking on public health informatics to their decisions. First, public health informatics is still growing as a field and many commercial off-the-shelf applications do not incorporate the latest work in public health informatics.
Many public health agencies lack the expertise and resources to take on the challenging project of finding a path that marries the latest advances in public health informatics with what is available from vendors and their own needs. Additionally, some state and local jurisdictions are undergoing fiscal challenges and use poorly understood and out-of-date methods for governing capital investments in IT.
Some note that incorporating informatics principles into the day to day work of LHDs may require more leadership from state and federal officials. Many states currently have public health informatics experts working at the SHAs. Stakeholders are pursuing efforts to formalize these job descriptions and make a case for a broader role for state public health informatics experts. Discussions with vendors focusing on the public health agency market, including Netsmart and Consilience, reveal their interest in working with savvy customers in position to adopt specifications coming from the informatics community.
In this section we highlight key findings from our in-depth case study work in three regions. As noted earlier, each case study involved in-person visits with two LHDs and an SHA. As part of these visits and a series of phone conversations before and after the visit, we asked public health leaders and staff about the functions their agency performs, the information and data needs necessary to perform those functions and the applications used to capture, manage, exchange, and analyze these data.
In each discussion we touched on one or more of the key challenges identified early in the project, including defining workflow and business processes, capacity and skills within the public health workforce, and governance and financing issues affecting public health systems. We also focused on the potential impact of policy and program initiatives including those established under HITECH and ACA. Exhibit 2 above lists the case study locations and participants.
In Florida, we visited the Duval County Health Department in Jacksonville, the Alachua County Health Department based in Gainesville, and the State Department of Health in Tallahassee. Florida has a state operated model where LHDs adapt to the needs of their communities but rely on the state for staffing, information systems and technical support. Under this model, the state provides centralized oversight of LHD operations and leadership. LHDs in Florida focus largely on specialized clinical and case management functions, while providing some local epidemiological and monitoring functions. Meanwhile the SHA enforces reporting requirements and maintains population-health records systems.
The backdrop of our visit was a decision on the part of state’s public health leadership to pursue the in-house customization of their Health Management System (HMS), a clinical application developed by Florida using a relational database platform offered by Intersystems Corporation. The state’s informatics lead works very closely with software developers and staff at LHDs to create and customize specific clinical modules that meet the personal care delivery and reporting needs of public health practitioners in Florida. As of November 2012, the SHA obtained accreditation for the HMS system as a certified EHR, which will allow some public health practitioners in Florida to qualify for Meaningful Use incentive payments.
Despite the consolidated model and the efforts to move to a single clinical application, we found that silos persist. The state manages multiple systems, and LHDs and health-care providers submit data into each of these systems. There are no straightforward and automated mechanisms for sharing data across systems. Exhibit 4 below outlines some of the public health systems that we discussed in Florida. In addition to HMS, state HIV/AIDS providers use several systems used to document and report care provided under the Ryan White Care Act, and in STD clinics, staff use a system called PRISM to report and track and document contacts to STD cases. Providers and LHDs report incidence of notifiable conditions to the state’s communicable disease surveillance system, Merlin, and to several separate state registry and population-based health records systems including those tracking birth and death records, newborn screening results and immunizations.
Exhibit 4: Examples of Data Systems Used by Public Health Agencies in Florida
| System | Data Sources, Uses, & Management | Interfaces and Data Capture |
| The Health Management System (HMS) | HMS is a practice management system with EHR modules used in public health clinics. 11,000 registered users on 50 interfaces to manage encounter and services data entered by providers at LHDs. Includes registration, eligibility, scheduling, and care coordination. Additional modules include unified service reporting, billing, TB, HIV, Healthy Start, clinical encounter data, and dental. Most EHR modules are "homegrown," with a few that are off-the-shelf products (e.g.,) e-Prescribing. | Interfaces with 4 other state systems and 14 external systems. |
| ADAP database for tracking HIV care | Real-time enrollment information for HIV/AIDS clients inputted by eligibility staff at LHDs. Client-level data used in reporting to tie cost to each client, thus meeting reporting requirements. Displays medications prescribed by clinicians and indicates when the prescriptions are picked-up. | Beginning to develop an ADAP module on CAREWare to integrate the two systems. |
| CAREWare | CAREWare is open-source software that allows Ryan White Care Act recipients to document and report on care delivered to HIV/AIDS clients and produce the Ryan White HIV/AIDS Services Report to HRSA. Staff at LHDs and private providers treating the HIV/AIDS population covered under Ryan White enter client-level data. | Health departments that provide HIV care must upload their data from CAREWare into HMS manually. Private providers enter data into CAREWare directly. |
| Enhanced HIV/AIDS Reporting System (eHARS) | HIV/AIDS reporting system that states use to voluntarily report cases for surveillance to the CDC. Includes reports of positive HIV cases not only from public health clinicians but from patients served by all providers. | Data reported directly from clinical laboratories using ELR. |
| Merlin | The state’s disease surveillance system. The system also tracks foodborne illness outbreaks. Public health clinics and laboratories report confirmed cases into Merlin. Data are maintained by the Bureau of Epidemiology in Tallahassee. System produces automated notification for LHDs about individual cases. Real-time aggregate data is available to the public online. | Merlin is populated primarily through direct data input by LHDs or the ELR from clinical laboratories. Currently the system is not interoperable with HMS. |
| Patient Reporting, Investigation and Surveillance Manager (PRISM) | Surveillance system used by state STD epidemiologists and STD clinic staff at LHDs. Positive lab reported automatically via ELR. STD clinics enter patient demographics, patient contact information, travel history and sexual contacts by name. STD surveillance functions include monitoring reporting timeframes for labs and providers, tracking volume of testing by lab and provider, tracking disease prevalence by area, county, disease, and selected dates, assigning field records to disease investigators, targeting providers to improve reporting. Produces disease reports on prevalence, common risk behaviors, shared demographics and geographic concentrations. Also generates automated text messages of test results for clients (opt-in). PRISM is a web-based system developed and maintained at FL DOH and currently used by multiple states. | Fully integrated with the ELR from public health and clinical labs. Not currently integrated with HMS. |
| The Electronic Surveillance System for the Early Notification of Community-based Epidemics (ESSENCE) | The syndromic surveillance system used to identify outbreaks. It collects emergency department chief complaint data from hospitals and urgent care centers, call data from poison control, reportable disease data from Merlin and mortality data from the Florida Office of Vital Statistics. Used for outbreak detection, situational awareness monitoring and post-hurricane disaster surveillance. Produces graphics and summary statistic tables that LHDs use in their reports. State epidemiologists meet weekly to review trends discovered by ESSENCE. | Receives data from the Merlin database and vital statistics records. Otherwise data are entered by hospital and urgent care facility staff. |
| Florida SHOTS | FL SHOTS is the state’s immunization registry. Vendors include Bay systems, Vtech, Henry Elliot & Company, Advanced Systems Design. LHDs manually enter data into FL SHOTS. SHOTS experiences a very high number of electronic transactions. The registry is also a decision support system, providing information for managing immunization clinics and ensuring appropriate immunization levels. Providers can run reports and are able to generate reminder calls to bring children for scheduled vaccinations. Almost all LHDs use this function extensively. | Public health staff downloads SHOTS data into the HMS system through a manual process. |
| SpecimenGate | A PerkinElmer runs newborn screening system. Laboratory results reported via ELR. Physicians have ability to add information via e-reports add-on. FL DOH developed web-based system for physicians to access newborn screening results online-can produce a PDF copy of lab report to the physician. | Working on consolidating newborn screening and vital records systems |
| Community Health Assessment Resource Tool Set (CHARTS) | A data dissemination tool built in a web-based platform called DUNDAS. The program provides data visualizations incorporating data from multiple public health systems including vital statistics, Merlin, Medicaid, Department of Education, Department of Juvenile Justice, and the Behavioral Risk Factor Surveillance System (BRFSS). A web-based interface is available to the public. Generates reports and charts on various topics including such health statistics as births, deaths, disease morbidity, population and behavioral risk factors. | Users can export data to MS Excel for analysis. |
| Environmental Health Database (EHD) | Tracks inspection results, date of inspection, demographics, septic system or food facility owners, location, soils, sanitary nuisances at the local level. | No active interfaces with other systems. |
Like many states, during the time of our visit Florida was going through substantial budget cuts requiring LHDs to manage and expand functions with fewer staff. The SHA was also experiencing a re-organization to achieve efficiencies through integration of offices with related functions.
Implementing a vision and data model. Leadership in Florida has a vision for how to organize public health data resources to address functional requirements and mission. They have a strategy around using HMS as the main platform for capturing patient-level information in LHDs. Implementation of this vision is ongoing. For example, many of public health clinical service providers use a hybrid approach, capturing some data in HMS, some on paper and some using disease specific systems such as PRISM and CAREWare. Furthermore, although most of the state systems for reporting have effectively adopted ELR, practitioners in hospitals and LHDs continue to enter data manually at least twice, once for their own use and a second time for reporting to the state.
Over time, public health leaders in Florida plan to expand the use of interfaces with HMS and use HMS to report directly to state databases. To address the challenge associated with bringing together data on a single client who may have records in multiple systems, stakeholders point to the potential for using master patient indices (MPIs) and record locator services (RLSs) that would be developed and managed by HIE organizations. These services would allow LHDs to query different state public health systems and bring together data relevant to a single case facilitating case investigation and follow-up.
In the future, the state hopes to improve interoperability across systems. For example, they plan to create protocols where receipt of a positive lab result from ELR into a state surveillance system automatically triggers a query of the relevant clinical data from an HIE organization. Furthermore, they are looking to develop interfaces between their syndromic surveillance system and emergency management systems (EMS), e-Prescribing and STD surveillance.
Connecting to state HIE efforts. Stakeholders in Florida noted strong collaboration between public health leadership and officials responsible for the state’s HIE efforts. Florida is supporting a federated model for state-wide HIE with regional health information organizations, larger provider groups and other “nodes” providing data to the statewide exchange. Under this model, participating providers would be able to send “queries” to their local or state HIE infrastructure seeking records on particular patients they are treating. The same providers would offer up their own patient-level data for other providers to query.
The main function of the statewide HIE will be to support a statewide MPI that will help providers access data from other providers across nodes. LHD clinics will represent their own node, and the state planned to make these clinics among the first groups to participate in the state-wide exchange. Public health officials noted that their participation in the exchange would allow them to query clinical data for limited case investigation purposes.
Key takeaways from Florida. It is likely that the systems landscape in Florida is less complicated than in other states where LHDs have more autonomy. However, even with a centralized model, Florida illustrates the diversity of systems and data silos that emerge in public health.
Despite these challenges, Florida’s progress on developing a strategy and path forward rests on some characteristics of effective leadership. Leaders within the state understand the history and constraints that led to current information systems and practices and articulated a more strategic path for the future. This required an understanding of informatics principles used in other industries to drive IT decision-making as well as the history and operations of public health agencies in the state.
In Michigan, we investigated use of systems at the Michigan Department of Community Health (MDCH), a superagency that covers both Medicaid and public health; the Ingham County Health Department (ICHD); and the Mid-Michigan District Health Department (MMDHD). The state does not directly oversee the LHDs in Michigan.
LHDs in Michigan are primarily responsible for direct patient services in the context of communicable disease clinics, maternal and child health programs, including home visiting and HIV/AIDS care. In the case of Ingham County, the LHD also manages an FQHC with several local sites. LHDs also license and inspect homes and businesses that pose potential public health concerns (e.g., restaurants, swimming pools, septic systems) and conduct epidemiologic and case investigation to follow-up on potential outbreaks or incidence of reportable conditions. State public health officials work on the assurance, monitoring and surveillance functions and maintain related data systems, manage federal programs and conduct epidemiologic studies.
The relationship between the SHA and LHDs bears important implications for the approach to public health systems in Michigan. The state operates a robust immunization registry and strong statewide communicable disease reporting systems used locally for both information gathering and reporting purposes. However, a lack of centralized systems for other public health program areas contributes to use of stand-alone systems at the state and local level.
In Michigan, Medicaid and public health are part of the same agency (MDCH). While the state spreads responsibility for Medicaid and public health programs across different divisions within MDCH, we did see some evidence that the “superagency” structure may contribute to better integration of public health and Medicaid data.
Although the state runs all of the required population-level public health records systems including vital statistics, syndromic surveillance, a cancer registry and newborn screening, stakeholders emphasized the importance of two state-based systems in particular: the Michigan Disease Surveillance System (MDSS) and the Michigan Care Improvement Registry (MCIR). We describe these systems and others we encountered in the case study in Exhibit 5 below.
The Michigan Disease Surveillance System. MDSS is a web-based communicable disease reporting system to support the core public health functions of epidemiology, surveillance, and monitoring. Providers are required to submit notifiable disease reports to the MDSS. Reports come into MDSS through a combination of ELR, manual entry by providers and LHDs, and manual entry of faxed reports from laboratories. The system geocodes incoming communicable disease data based on the patient’s address and assigns new cases to the work queue of the appropriate local jurisdiction for case investigation and follow-up.
Exhibit 5: Examples of Data Systems Used by Public Health Agencies in Michigan
| System | Data Sources, Uses, & Management | Interfaces and Data Capture |
| Michigan Care Improvement Registry (MCIR) | A single, secure electronic database run by MDCH where providers and public health officials submit immunization data as well as other types of health data (e.g., BMI) through either a web-portal, batch transfer from EHRs, or paper scans. Providers also get special information on for Medicaid-enrolled children (such as need for EPSDT services based on administrative data) through MICR. | MCIR is linked with other state systems such as Vital Records, Medicaid, WIC, Department of Education, and Lead Screening. MDCH is in the process of linking MCIR with Newborn Hearing and Newborn Metabolic Screening and building an interface between MCIR and the Great Lakes HIE (GLHIE) |
| Michigan Disease Surveillance System (MDSS) | A web-based communicable disease reporting system, built by MDCH based on national data standards. MDSS captures communicable disease data through a combination of ELR, manual entry, and faxed reports. Incoming data is geocoded for jurisdiction and assigned to the work queue of the local agency for case investigation and follow-up. | Efforts are ongoing to build an interface between MDSS and GLHIE. MDSS will also be linked to Medicaid administrative data through a larger data linking effort undertaken by MDCH’s Office of Medicaid and Health IT. |
| SpecimenGate | Michigan uses SpecimenGate, a Perkin-Elmer system to capture and manage data related to newborn screening results. | PH laboratory submits results to the Perkin-Elmer system. Michigan worked with Perkin-Elmer on developing a follow-up module as part of the system. |
| Michigan Syndromic Surveillance System (MSSS) | MSSS is a web-based syndromic surveillance system monitoring chief complaints from emergent care settings. The system collects over 9000 registrations daily from 70 healthcare facilities across Michigan’s eight emergency preparedness regions. | Currently, data are entered by emergency departments (EDs) and other providers. State supports direct exchange into MSSS from hospital systems to support Meaningful Use, but hospitals do not currently use this service. |
| NextGen Electronic Health Record | Ingham County health department is in the process of adopting the NextGen EHR. They recently implemented NextGen in their FQHC and are working on defining workflow and requirements necessary to customize NextGen for use in maternal and child health clinics, home visiting programs and infectious disease clinics. | County is working on building an interface to state databases for maternal and infant health program monitoring. However, interface efforts to date are limited due to plans for using GLHIE as a “hub” for populating public health databases. |
| Netsmart’s Insight | Some LHDs in Michigan use Netsmart’s Insight software as a practice management and EHR software solution. To support public health programs, the Insight practice management system consists of modules geared towards patient registration, scheduling, encounter processing, and accounts; the EHR contains the patient’s medical records, tracks laboratory results, keeps an inventory of immunizations, and tracks follow-up needs. | Some Insight modules allow for direct interfaces with clinical laboratories and immunization registries. |
| Vital Records Registry | State’s system for monitoring births and deaths. | Vital Records data is linked to a variety of other state data sources, including newborn screening, Medicaid, PRAMS, and BRFSS. Michigan recently implemented electronic reporting of birth and death data to this registry. |
| Community Health Automated Medicaid Processing System (CHAMPS) | Michigan’s Medicaid Management Information Systems that feeds data into a Medicaid data warehouse. | Data from CHAMPS gets used as part of the data warehouse for public health purposes, including informing Medicaid providers when EPSDT services are indicated. |
| Cancer Registry | Registry system with direct reporting of cancer cases from health-care providers. | Data feeds into the Medicaid data warehouse. |
| Chronic Disease Registry | Under development; will ultimately feed into the Medicaid data warehouse. | Ultimately, will link to other state resources including Vital Records, Birth Defects, newborn screening and MDSS. |
| Environmental Health Databases | In-house databases maintained at local departments to track inspections and services related to food safety, sewage disposal, and water supply and to fulfill reporting requirements to the state. | Does not automatically connect to MDSS to assist with epidemiology/outbreak tracking. |
Unlike Florida, the state does not maintain separate systems for surveillance for specific types of diseases such as STDs outside of MDSS. MDSS serves as a central resource for the LHDs. Local public health officials report both successes and challenges in using the system for their analytic purposes. MDSS has a variety of built-in reports to facilitate analysis but they do not always provide the flexibility desired by local epidemiologists. Additionally, LHDs only have access to their county’s data on MDSS. To view patient data from another jurisdiction, local agencies must call or fax one another, wasting valuable time in the event of an outbreak. Finally, there is no ability for electronic transfer of cases of notifiable diseases from LHD clinical systems to MDSS.
Expanding the features of an immunization registry. The state built MCIR as an electronic statewide immunization registry and it still serves this purpose for all providers in the state. Immunization data comes into MCIR through data entry by providers (both public health and private providers) into a web-portal or with paper scans from health providers and schools that are then manually-entered. Recently, the state also instituted a program that allows providers to upload data on multiple immunizations simultaneously from a provider EHR to MCIR (batch-uploads). Use of MCIR in the context of immunizations fulfills local departments’ reporting requirements, facilitates case management and supports preparedness for pandemic flu and other public health emergencies.
MCIR now also provides additional data on care for children covered by Medicaid. For example, MCIR includes information on whether or not children on Medicaid are due for tests or screenings included in the Early Period Screening, Diagnosis and Treatment program (EPSDT). These data come from the states’ Medicaid data warehouse. MCIR also provides results of blood lead, newborn screening and hearing screenings from other state-managed systems.
The state is continuing to build upon MCIR with additional tabs for other types of health data (e.g., BMI entered directly by providers). By adding in data from payer records and encouraging providers to enter their own data, the state hopes to use MCIR as broad-based children’s health registry.
Relationship between public health and Medicaid. At the MDCH “superagency,” the Office of Medicaid Health Information Technology leads data integration efforts through their development of a data warehouse. They are building infrastructure to pull together a variety of state data sources (representing both public health and social services) which would ultimately connect with the statewide HIE. Data sources include MCIR, MDSS, Vital Records Registry, Michigan Syndromic Surveillance System (MSSS), Community Health Automated Medicaid Processing System (CHAMPS), state public health laboratories, a cancer registry, and a chronic disease registry (under development). The data warehouse uses an MPI to match data to clients across disparate systems, avoiding duplication of records and providing for a fuller picture of health and health care for individuals, groups and populations.
The use of a data warehouse that integrates Medicaid administrative data and public health data represents an innovation only possible when there is solid collaboration between Medicaid and public health in a state. In the future, Michigan’s Office of Medicaid Health Information Technology plans to connect this warehouse project with the larger state-wide HIE infrastructure in the state (described below) which would allow a single query on a patient to identify clinical records as well as any record from the Medicaid administrative data or public health surveillance data.
Presence of stand-alone systems. Although, like Florida, stakeholders at the state-level in Michigan have a solid vision for organizing and managing data related to public health, they may be less able to leverage this vision to break down silos at the local level. Because LHDs in Michigan are independent and governed by municipal leaders, there is not a single state-wide clinic management application to support patient-facing services at public health clinics in Michigan.
The Mid-Michigan Health Department uses Netsmart’s Insight application as a public health practice management or EHR application. Meanwhile in Ingham County, the local health department has just adopted NextGen for their FQHC sites and is working on customizing NextGen to their other clinical programs such as communicable disease clinics, maternal and child health clinics and home visiting.
We also found evidence of stand-alone systems that were outside of the strategic plan led by the Office of Medicaid Health IT. The state’s Maternal and Infant Health Program that manages all the Title V funding in the state still uses some paper-based reporting and the systems used to manage data related to these programs do not interface or easily share data with other SHA or LHD systems. In describing the challenges associated with managing their own systems and getting them to report appropriately to the state, some local public health officials noted that they would welcome more leadership and guidance from the state on software applications and approaches to reporting.
History of collaboration between public health and HIE. Overall, Michigan has a long history of health IT investments and stakeholder support and engagement around HIE. The Michigan Health Information Network (MiHIN) is the central exchange for connecting sub-state HIEs to each other and the State of Michigan internal HIE. LHDs have been heavily involved in establishing sub-state HIEs. For example, Ingham County’s health department was critical to getting the Great Lakes Health Information Exchange (GLHIE) off the ground.
Workflow and staffing. The two LHDs we visited engage in ongoing efforts to document and analyze their workflow with the goal of promoting the efficiency and utility of using EHRs. Through these efforts, LHDs hope they will be better able to systematically allocate resources to support systems across program areas. While local public health leaders acknowledged the importance of these activities, they also noted the difficulty with finding staff with the right informatics and business process training, knowledge of public health systems and time to devote to the task.
ACA and provider engagement strategies. The state of Michigan has actively and successfully pursued CMS innovation awards to improve care to Medicaid and dually-eligible populations in the state. State public health leaders in the chronic disease epidemiology division have partnered with Medicaid to lead these applications and manage the grants. While acknowledging that it is largely uncharted territory, public health officials and epidemiologists in Michigan are optimistic that ACA-based efforts to establish an all-payer claims database will help support an array of public health assessment and planning activities.
CMS recently awarded the state and the Michigan Public Health Institute a “Pathways Community Hub” award. This project uses community health workers to help vulnerable groups access non-health-care services such as housing, nutrition and heating assistance that are relevant to health status and outcomes. State public health officials are involved in the oversight of these efforts, but at the time of our visit they had not developed plans for how or whether to involve LHDs.
Challenges and opportunities. Even in a sophisticated environment like Michigan, we find some disparate and uncoordinated silos for capturing and managing data. For example, the data warehousing work to date, does not include systems that support Title V reporting. Also, LHDs in Michigan work on their own to procure and customize systems to support their needs and report to the state. Local public health leaders have limited resources and expertise to apply an informatics-based approach to using systems.
Challenges aside, Michigan demonstrates how sophisticated use of Medicaid data can serve important public health purposes. They show innovation in the use of an immunization registry to deliver information derived from encounter data to support EPSDT. Their emerging model for data integration uses a robust Medicaid data warehouse to link encounter data, clinical data and public health reporting data, and this may be a path for other states to consider.
In Oregon, we met with Washington County Department of Public Health, Multnomah County Department of Public Health and the Oregon Health Authority (OHA). In each location we asked about major systems supporting public health functionality and how they see their use of systems and data changing in light of HITECH, ACA and other recent developments.
LHDs in Oregon are legally independent of the SHA. They receive very little state funding, technical assistance or oversight. As a result, some LHDs have developed multiple homegrown and stand-alone data systems. Oregon has a number of small rural and frontier counties with extremely limited resources. These jurisdictions may not have any full-time IT staff and may make limited use of information technology.
Like many states, Oregon is going through budget cuts. At the local level, LHDs depend almost exclusively on categorical federal grant and cooperative agreement funding to support their efforts. Stakeholders in Oregon noted that categorical funding opportunities create incentives for states and LHDs to manage their data in silos to meet specific reporting requirements.
With some exceptions, LHDs in Oregon focus largely on targeted clinical areas such as infectious disease, immunization and home visiting. They also assist the state in surveillance and monitoring activities specific to their jurisdiction and provide environmental health services involving licensing and inspections of potential public health hazards. Exhibit 6 below outlines examples of systems we encountered in Oregon.
Exhibit 6: Examples of Data Systems Used by Public Health Agencies in Oregon
| System | Data Sources, Uses, & Management | Interfaces and Data Capture |
| Epic Electronic Health Record | Primary care clinics that are part of the FQHC run by Multnomah County Health Department have used Epic software for practice management and electronic health records (EHRs) for several years. Multnomah County also uses Epic for some home visiting program encounters. However, Multnomah County has not been able to employ Epic in public health clinics. | Epic used in FQHC setting has interfaces to Oregon’s immunization registry and clinical laboratories. Some LHD clinics (e.g., STD clinic) have “read only” access to Epic records for their patients. |
| MS Access Databases | Multnomah County noted that they have over 30 Access databases used to manage data and client interactions related to different programs. One of these systems known as “TOURS” is used to document care delivered by HIV/AIDS providers under Ryan White Care Act Programs. | These are mostly stand-alone systems that provide reports formatted to meet funder requirements, but are not interoperable with other applications. |
| Netsmart Insight | Public health clinics in Washington County are moving to the Insight public health EHR and practice management system. Originally, Washington County used Insight only for practice management functions such as scheduling and billing. Recently, they have rolled out modules to support client encounters in TB, STD, immunization and family planning clinics. | Currently Washington County is able to upload immunization records from Insight into the state’s immunization registry. They have not purchased modules necessary for “real-time” interfacing with labs or state systems. |
| ALERT IIS (Immunization Information System) | ALERT IIS is Oregon’s Immunization Information System that captures immunization information from all health-care providers performing immunizations in the state. ALERT IIS also gives those providers access to information on immunization status of patients, tools to track their immunization inventory and other functionality. | The state supports different ways to interface with ALERT IIS for some EHRs (including Epic) interfaces support direct transmission of immunization data from within the EHR system. They also accept flat-files for batch uploads. |
| Oregon Child Health Information Data System (ORCHIDS) | State system used by LHDs and providers to report information on home visit encounters and other maternal and child health programs. | Stand-alone system that requires manual data entry. Separate from systems used by LHDs to manage client and encounter information to support care delivery. |
| TWIST | State system used by LHDs to report information on benefits provided through the women, infant and children’s (WIC) program. | Stand-alone system used by LHDs for reporting to state. |
| Oregon Public Health Epidemiologists’ User System (ORPHEUS) | State-run communicable disease surveillance system. Used for submitted state-required reports on notifiable diseases and for tracking and case investigation involving those cases. One system integrates all reportable conditions including STDs, HIV/AIDS, TB and other infectious diseases. | System is ELR enabled. Otherwise, LHDs and hospital providers enter data into the system and are able to access information on cases in their area. |
| Vital Events Registration System | A web-based Netsmart application used by the state to capture and manage vital events data including births, deaths, abortions, marriages and divorces. | Have developed electronic reporting systems that allow providers (hospitals) to submit data on births and deaths. All births and many deaths are now reported electronically. Also, links to state’s birth defects registry and cancer registry. |
Health-care reform in Oregon. Health-care reform plays a large role in defining Oregon’s evolving health IT strategy and the role of public health. In August of 2012, the state began implementing Coordinated Care Organizations (CCOs). CCOs are local health umbrella organizations that will deliver health care and coverage for individuals eligible for Medicaid managed care in Oregon and will have performance based payment incentives to reward quality improvement and cost control.
CCOs are designed to encourage coordination and exchange of information across providers. Because of new reporting requirements, CCOs will provide data that were previously unavailable, such as data on emergency department utilization. Staff from the SHA and LHDs take part in CCO planning and implementation. However, the initial focus for these efforts is around reducing “high cost” hospital care rather than traditional public health concerns.
Even though typical public health concerns are not among the early objectives of the CCO initiative, in some parts of Oregon, such as Washington County, LHDs have developed new collaboration with local providers. As part of this effort, Washington County will use data from providers to profile health outcomes in their community and generate reports for use in assessing the success of the CCO program in their area.
Streamlining data from programs affecting high-risk infants and children. The governor of Oregon has implemented an Early Learning Council to integrate and streamline existing state programs for at-risk youth, including health-related programs. Public health officials in the state hope to leverage this focus on early childhood to develop a coherent, informatics-driven strategy for capturing relevant data from public health programs.
During the time of our visit, OHA staff was developing and application for a one-year planning project to the federal Administration for Children and Families (ACF) for the OMB-funded State Systems Interoperability and Integration Projects. Oregon was not awarded the grant, but stakeholder relationships established in the course of pulling together the grant will be valuable for future collaborations around data sharing. The proposal focused initially on maternal and child health home visiting programs and the requirements of a system to effectively deliver care, manage referrals and track outcomes as part of this program.
Distributed public health systems. Oregon has multiple state systems with limited interoperability or capacity to share data to support core public health functions including epidemiology, surveillance, monitoring and assurance. ORPHEUS, the state’s main communicable disease surveillance system, does not interface with providers’ EHRs, but does receive data automatically from clinical laboratories through ELR. ALERT IIS system, Oregon’s immunization registry program has worked closely with a variety of providers and EHRs vendors and currently accepts messages via interfaces from multiple EHRs products including the Insight public health EHR used in Washington County. The immunization registry also accepts data in flat-files, Excel and HL7 batch format from different provider organizations.
As in other places, LHDs largely “go it alone” in terms of developing, adopting and customizing systems to capture and manage data to support their functions and produce necessary reports. Although the FQHC in Multnomah County has long used the Epic EHR, the core public health clinics have not been able to find resources to use Epic for their work. One barrier cited is the lack of case management functionality built into Epic, but the larger barrier might be the cost of additional Epic licenses and the cost of customizing the Epic interface to meet the needs of clinics focused on infectious disease, immunizations or other targeted public health clinical services.
Therefore, Multnomah County developed and maintained dozens of stand-alone systems and data resources including Excel spreadsheets and MS Access to support the needs of managing different programs and reporting to funders. The health department recently hired staff and took on the effort of trying to gather documentation and develop workflows associated with the use of these applications.
Recent efforts of the informatics committee. At the time of our visit to Multnomah County, they had recently established an informatics committee tasked with developing a strategic approach to aligning information system investments with the mission, public health functions and information needs of key stakeholders. As a part of this process the county is developing an informatics roadmap and assembling data dictionaries and workflow descriptions from each of their programs. When the roadmap is completed, they will use these materials to identify problem areas and opportunities to improve workflow and make systems improvements.
In addition to the documentation and inventory projects described above, the informatics committee saw a critical need to educate staff at the public health department about the process used within their county government for proposing and evaluating IT capital improvement projects including software and hardware acquisition. They found that many staff felt that operational grants were the only option for addressing new software needs and that staff did not clearly understand the county’s own financing mechanisms.
A vision for increased consolidation and integration of systems. OHA is planning leveraging early childhood home visiting and “Race to the Top” funding, to design a modular information architecture to support multiple functions across the SHA and LHDs and to integrate data from education and social service agencies. Staff expressed interest developing a state-maintained modularized application to support work among LHDs and facilitate reporting. State employees are working on an initial design for this application for a home visiting program that requires some extensive referral management functionality, but have a vision that an integrated application may support a range of point of care and surveillance needs. The modularized approach would provide a single resource for entering data common to all programs (such as demographic information) and then add modules linked to this common resource to support the needs of different programs.
In this chapter we review themes emerging across case studies, telephone discussions and our initial environmental scan. We organize these themes around specific opportunities and challenges articulated by public health stakeholders through various parts of the project.
Health departments need a better understanding and documentation of the business rules and processes underlying public health function. Effective investments in the design and implementation of IT resources must begin with a detailed and well-documented understanding of public health practice, both broadly and as practiced in specific jurisdictions. Efforts such as RWJ’s Common Ground implemented by PHII, ongoing work by PHII funded by de Beaumont foundation and work by the PHDSC provide useful resources to support workflow documentation and process improvements. But, future work will need to address the evolving roles of public health in the new health-care delivery environment.
Resource constraints and workforce training needs. LHDs struggle to find the time and resources to adequately assess vendors, develop requirements, lay out an approach to using standards, customize applications to meet their needs, optimize between their own practice needs and state and federal reporting requirements and conduct other basic activities that may be essential to effective use of IT.
An ongoing barrier is the lack of expertise in business process analysis among the staff at LHDs and limited IT resources to help understand and define business processes and then translate those processes into systems requirements. In addition to tools, resources and technical assistance, direct training of staff under programs such as those led by PHII are needed. Also, resources for LHDs to hire informatics professionals with knowledge of public health functions may be necessary. Often, LHD leadership will re-assign an experienced member of the care delivery team to lead the organization’s efforts to document existing processes and work on systems implementation.
Managing data for public health services. This project illustrates the importance of establishing tools for capturing, managing and using data to support services delivered by public health clinicians and case managers. These tools, sometimes referred to as public health EHRs, help capture patient-level data for reporting, third party billing, care management and delivery of direct services.
Even as LHDs deliver less clinical care, their role in case management and care coordination suggests the need for a patient-level health record for public health use will persist. Also, LHDs will continue to face challenges with using EHRs designed for the medical environment because these applications typically lack robust case management functionality.
An evolving applications landscape. Currently, most LHDs work independently to secure resources to support their practice management and billing systems and many do not have the benefit of EHRs. Some that we spoke with in Michigan and Oregon are using commercially available EHR software such as Netsmart geared specifically towards public health. Others, such as Ingham County, MI are adopting primary care EHR systems to support public health services and, yet others, such as the State of Florida are pursuing efforts to build and configure their own version of a public health EHR.
The HIV/AIDS, Hepatitis, STD and TB Agency (HAHSTA) in Washington, DC is working with a vendor, Consilience, to establish a modular approach to public health data management using their Maven software product. Systems like Maven provide an interesting model for integrating data captured in public health clinics with population-wide public health reporting databases. This system is consistent with the use of a common data model for supporting various public health interventions including direct services, programmatic reporting and surveillance.
Vendors can play an important role as landscape evolves. While a relatively new and immature market, IT vendors targeting public health departments are increasingly aware of the importance of integration and the benefits of standardized business processes and information standards for public health. Currently, limited resources and a lack of a common venue for engaging with public health department customers may preclude beneficial engagement between potential public health department customers and vendors. While there are a limited number of vendors committed to the public health market, we spoke with some vendors familiar with public health processes and eager to engage with knowledgeable and sophisticated partners at LHDs.
Public health agencies and stakeholders commonly cite data silos as a barrier to effective targeting of services and integration of data to understand trends within a population. We found that data silos emerge for different reasons. Some data resources such as vital records registries and immunization registries operate under legislatively mandated parameters and administrators of these resources are not free in all states to broadly share these resources.
Many programs implemented by LHDs are subject to specific eligibility, service delivery and reporting requirements based on state and federal rules. While programs funded categorically do not often require use of a specific information system, many stakeholders note that developing a new system is often the least complicated way to get a program running in the short-term.
Stakeholders identify two paths for moving past silos. The first involves use of single module-based systems with an integrated data architecture to support multiple public health functions and required reporting. The second involves assuring interoperability based on standards systems used by different public health agencies and health care providers. Many stakeholders agree that both can and should play an important role.
Potential for integrating public health systems. In some states, SHA officials are interested in establishing a single-modularized public health information system that would be available to LHDs to capture patient-level information, coordinate referrals to care in other public service providers and health-care providers and report relevant information to the state. The emphasis would be on populating and updating information relevant to multiple programs (e.g., demographic data) once and then linking this “core” system to modules with workflow and requirements specific to particular programs or services.
Even if public health officials do not achieve the opportunity to substantially integrate public health data applications using a common modular infrastructure, more assiduous use of messaging and document standards may offer greater interoperability across systems. This type of interoperability would allow stakeholders who are primary users of one application to benefit from use of data that are originally captured outside their home application. Furthermore, public health officials in some states note that they look forward to leveraging MPIs and RLSs set up by state or regional HIE organizations that could allow public health officials to query outside systems that may have captured information relevant to a particular case or patient.
Some basic conditions must be present to facilitate adoption of common messaging and document standards to improve interoperability. With respect to interoperability, many stakeholders agree that the use of a CDA-based standard would represent an opportunity to have a flexible and extensible document based standard that allows the sharing of multiple types of health-care data for public health purposes. In some cases, stakeholders note that use of the HL7 2.5.1 messaging standard may be a very effective tool even if content is limited to less than a full CDA.
However, public health providers and agencies have not yet broadly adopted standards for exchanging data. Many LHDs may not be asking vendors about their ability to comply with these emerging public health data exchange standards. Direction from state or federal authorities that lays out basic requirements for systems used to capture, exchange and manage person-level data by LHDs and SHAs may support greater adoption of standards in systems used by public health staff.
Public health informaticists have worked extensively on standards for messaging, content and transport to support interoperability and information exchange. At the ground-level, public health practitioners need additional instruction on how these standards should influence the types of systems they elect to adopt and how they use those systems.
Vision and model for capturing, maintaining and using data versus detailed architecture. Some stakeholders argue that a service oriented architecture (SOA) model that allows public health agencies in a particular jurisdiction to use common software solutions to address the needs associated with common functions is necessary. However, given variations in the priorities and capacities of SHAs and LHDs, the path for achieving such an architecture remains unclear.
Building a common platform that supports full interoperability and allows for both population health assessment and direct service delivery to individuals is a complex and expensive undertaking. SHAs and LHDs face both technical and financial challenges in achieving this goal. A starting point for many jurisdictions may be to articulate a more general “data model” and strategic vision that drives all data captured, maintained, and used by LHDs and SHAs, along with some requirements around the ideal format and nature of these data even if the requirements are not realized immediately. Data models would ideally include features that would allow for consistent use of standards over time and establish consensus about how to organize and link public health data that would drive interoperability.
We found important potential lessons from public health agencies’ role in HITECH programs where public health is not the focus of the program, but remains an important player. Public health’s role with respect to health-care reform and broader change in health-care delivery and financing remains unclear.
HITECH raises awareness, but also highlights gaps in IT capacity at public health departments. HITECH has raised awareness of the exchange of data between public health and health care and highlights gaps in defining best practices for public health IT. Examples of public health participation in initiatives to improve care through the Beacon Cooperative Agreement program show the potential benefits of public health engagement on quality improvement initiatives leveraging data from IT systems. While these efforts are limited to a few locations in the country, they will offer some useful case examples for consideration in other jurisdictions.
Some experts note that many public health agencies face the challenge of having to receive more electronic messages as a result of HITECH without additional resources. The small number of states taking advantage of 90-10 matching for enhancements to public health systems to support Meaningful Use may be attributable to lack of state funds even to fund the 10 percent match.[56]Finally, Meaningful Use does not address appropriate use of IT by LHDs. Some experts indicate that public health service providers (e.g., STD clinicians, visiting nurses, public health case managers) would benefit from their own set of Meaningful Use criteria and accreditation standards.
Potential role for public health in health reform. Many stakeholders agree that LHDs and SHAs can play an important role in advancing the objectives of the ACA. For example, public health can provide objective community-level health assessments bringing together multiple sources of data and supporting care coordination across providers. SHAs in OR, MI and likely elsewhere are involved in state-wide Medicaid health-care delivery reform efforts and federal demonstration projects. However, even in these cases, the new role of LHDs in light of the changing landscape is still unclear.
Although efforts are proceeding slowly, many do see a role for public health monitoring data to support decision-making, particularly with respect to the Medicaid population. In states like North Carolina and Indiana, LHDs collect health-care quality data and share these data with Medicaid. In this context, Medicaid may look to LHDs as the source for objective analysis on the performance of the health-care delivery system.Overall, stakeholders seem to suggest that public health can play an important role in health-care reform efforts. However, most LHDs and SHAs have yet to engage actively with health-care providers on delivery reform.
Incorporating provider-generated data and data from other service providers to support population health management. Beyond the limited examples described in this report, most LHDs and SHAs have not adopted analytic or operational models to routinely access and use data generated by health-care providers or other service providers. This will require development of new models to capture, transmit and analyze data and, importantly, cooperation on the part of the medical care community. Effective use of these data could help monitor the quality of care or outcomes for chronic conditions or systematically assess the status of vulnerable populations.
Public health officials with early experience conducting this work emphasize the importance of extensive engagement between public health and health-care providers on data entry, reporting and quality improvement. LHDs and SHAs also have not widely adopted effective models for incorporating data relevant to social determinants of health from other sectors (education, social services) into their case management systems, a key step for meeting population health objectives.
LHDs and SHAs vary across jurisdictions in terms of their priorities and organizational governance. Several factors drive this variation including the extent to which federal funds administered at the state-level such as Title V maternal and child health clinics or home visiting programs make use of LHDs as care providers, the extent to which SHAs control or manage LHDs, the priority state and local government leaders place on public health, the historic role of public health in a given jurisdiction and other factors. This is one reason why a single architecture or model for public health infrastructure may not be feasible at this time. It also illustrates the importance of the participation of state and local public health leadership and staff in national public health informatics standards development initiatives.
Potential role of accreditation. Accreditation through PHAB supported through funding from the Robert Wood Johnson Foundation and the CDC serves as a potential incentive for encouraging more strategic planning and purposeful investments in IT and processes among LHDs. In the future, PHAB may align accreditation with the use of standards to facilitate interoperability or require public health departments demonstrate how business functions drive workflow and use of systems in their agency.
Potential role for technical assistance. We found an appetite among LHDs and SHAs for technical assistance related to data, informatics and IT challenges. Specifically, agencies adopting new systems seemed poised to benefit from tools for workflow optimization and data standards. They seek assistance with vendor decisions, defining requirements and configuring new applications. In some cases, stakeholders noted the potential benefit of sharing best practices among a community of agencies that are using a common vendor’s platform.
Despite the perceived need, we found limited uptake of resources from past and current technical assistance programs in informatics. In some cases, local stakeholders were not aware of existing resources or could not find the time to apply them to their work. Many times, resources developed for national initiatives do not relate specifically to the needs of specific SHAs or LHDs with particular reporting requirements and focus, and the national experts developing those resources cannot afford to focus in on the particular needs of an individual jurisdiction. In these cases, public health professionals may benefit most from training on the goals of informatics and direct support with applying those goals to their situation. This might help LHDs and SHAs approach IT projects as opportunities to assess and improve workflow and movement of data rather than automating existing processes “as is” or simply adopting the vendors “out of the box” solution.
Collaboration and integration across federal, state and local agencies. LHDs may benefit from more collaboration across departments on informatics and more direction from the state. SHAs manage the majority of public health data and generally have more resources to maintain expertise. In some states, such as Florida, state leadership has maintained local flexibility while providing a common public health EHR to LHDs. Collaboration may also give agencies greater leverage in negotiating price, functionality and technical support with vendors.
Funding and governance of IT resources. Our findings suggest that public health funds some IT projects largely by making creative use of operational funds from one or more programmatic grants or special projects. Some stakeholders point out that this approach limits the strategic impact of these investments and can limit innovation. Funding new systems and IT investments using operational funds may constrain the timing of investments and leave limited time for appropriate planning and incorporation of informatics best practices into decision-making.
Use of programmatic funds specifically, may preclude agencies from making design investments that allow for integration and exchange across programs within public health and between public health and related sectors. We found that many SHAs and LHDs find it difficult to work within existing governance structures to make strategic capital investments in IT and systems. In order to fully adopt strategic approaches to using information systems, public health officials may need better tools for comparing alternatives and making best use of available resources. [57]
Characteristics of leadership. Successful planning and implementation of public health systems projects requires committed and knowledgeable leadership. Typically, these individuals come with a very detailed and practical understanding of the practice of public health as well as information needs facing public health officials on a regular basis.
Successful leaders engage with vendors and IT professionals on re-thinking workflows and processes and specifying requirements. They build enthusiasm for continuous process improvement and systems projects among public health staff. In some cases, leaders come with extensive experience and understanding of IT outside of the public health arena, very often in health-care delivery. Finally, successful leaders also understand and engage with national public health informatics initiatives and bring the resources and tools from those initiatives to bear in their work.
We found public health departments making important advances in use of IT, but we did not find a single “best practice” approach. Public health officials face common challenges, including variation and ongoing evolution of specific public health activities, lack of training on informatics and process re-design, shrinking funding for public health programs and constraints that limit strategic investment and encourage data silos.
Most agree that, in the future, effective public health practice will require a more integrated approach to managing information and increased collaboration with health-care providers and other social service departments. Public health departments themselves may benefit from openness to engaging with non-traditional partners, including health-care payers and providers.
Public health departments can benefit from planning IT investments around underlying work processes and their current and future information needs. Importantly, investments should promote use of standards and interoperability and avoid creating incentives for additional silos. Some findings suggest that state-level planning on public health IT investments may yield the most benefits. We found that by articulating a strategic framework for using IT, some public health departments have taken their IT infrastructure down a path that reduces unnecessary redundancy and improves the quality and scope of information available for public health practitioners. For example, by capturing demographic data one time to support multiple services, aligning data from multiple administrative and programmatic sources to help address service needs or integrating data generated by health care providers, public health departments can more efficiently tackle current activities and take on innovation.
Developing an effective strategic framework requires agency leadership with the knowledge to identify a wide range of relevant data, document current public health practice, understand legacy systems, work closely with IT vendors and visualize how to improve public health functions through better information flow. This gives agencies the opportunity to identify and address IT priorities as funds become available rather than letting funding opportunities alone drive investment decisions. The federal government, organizations representing public health, medical associations and funders of all types can contribute to progress in the use of IT by public health departments by endorsing the ideas of integration, interoperability and improved use of systems as priorities and fostering increased collaboration among agencies with public health responsibility at all levels.
| Name | Affiliation |
| Dr. Seth Foldy | Formerly with Public Health Surveillance and Informatics Program Office, CDC |
| Dr. Roland Gamache | Indiana Center of Excellence in Public Health Informatics, Regenstrief Institute |
| Dr. Dave Ross | Public Health Informatics Institute |
| Dr. Robert Harmon | Formerly with Duval County Health Department (Florida) Chair, NACCHO Public Health Informatics Workgroup |
| Dr. Anna Orlova | Public Health Data Standards Consortium |
| Dr. Martin LaVenture | Director, Center for Health Informatics & e-Health, Minnesota Department of Health |
| Dr. Bryant Karras | Chief Informatics Officer, Washington Department of Health |
| Ms. Uma Ahluwalia | Director, Montgomery County Department of Health and Human Services (Maryland) |
| Ms. Jessica Kahn | Center for Medicaid and CHIP, CMS |
| Mr. Robert Pestronk | National Association of County and City Health Officials (NACCHO) |
| Mr. Michael Coletta | National Association of County and City Health Officials (NACCHO) |
| Mr. David Dyjack | National Association of County and City Health Officials (NACCHO) |
| Ms. Valerie Rogers | National Association of County and City Health Officials (NACCHO) |
| Mr. Jim Kirkwood | Association of State and Territorial Health Officials (ASTHO) |
| Mr. James Daniel | Office of the National Coordinator for Health Information Technology |
| Ms. Jennifer Fritz | Minnesota Department of Health |
| Dr. Theresa Cullen | Department of Veterans Affairs |
| Dr. Arthur Davidson | Denver Public Health |
| Mr. Charles Lehman | Centers for Medicare & Medicaid Services |
| Ms. Kathleen Nolan | National Association of Medicaid Directors |
| Name | Affiliation |
| Dr. Seth Foldy | Formerly with Public Health Surveillance and Informatics Program Office, CDC |
| Dr. Roland Gamache | Indiana Center of Excellence in Public Health Informatics, Regenstrief Institute |
| Dr. Dave Ross | Public Health Informatics Institute |
| Dr. Robert Harmon | Formerly with Duval County Health Department (Florida) Chair, NACCHO Public Health Informatics Workgroup |
| Dr. Anna Orlova | Johns Hopkins University Public Health Data Standards Consortium |
| Ms. Kathy Cook | Lincoln-Lancaster County Health Department (Nebraska) National Association for Public Health Information Technology |
| Dr. Thomas Safranek | State Epidemiologist, Nebraska Department of Health Council of State and Territorial Epidemiologists |
| Dr. Robert Rolfs | Deputy Director, Utah Department of Health |
| Dr. Theresa Cullen | Director, Health Domain Information Technology, Office of the Secretary |
| Dr. Arthur Davidson | Director, Public Health Preparedness and Informatics, Denver Public Health |
| Dr. Althea Grant | Chief, Epidemiology and Surveillance Branch, National Center for Birth Defects and Developmental Disabilities |
| Dr. Sara Copeland | Acting Chief, Genetics Services Branch, Division of Services for Children with Special Health Needs |
| Dr. David Patterson | Chief, Health and Demographics, SC Budget and Control Board Office of Research and Statistics, State HIT Coordinator |
| Mr. Dan Jensen | Associate Director of Olmsted County Department of Public Health (Minnesota) |
| Ms. Amy Ising | Program Director, North Carolina Disease Event Tracking and Epidemiologic Collection Tool (NC DETECT) |
| Ms. Uma Ahluwalia | Director, Montgomery County Department of Health and Human Services (Maryland) |
| Dr. Marcus Cheatham | Health Officer, Mid-Michigan District Health Department (Michigan) |
| Dr. Taha Kass-Hout | Deputy Division Director for Information Science at CDC |
| Ms. Vicki Hohner | Senior Consultant on Health Information Technology (HIT), Fox Systems |
| Dr. Wu Xu | Director for Office of Public Health Informatics at Utah Department of Health |
| Ms. Jessica Kahn | Center for Medicaid and CHIP, CMS |
| Mr. Thomas Cannell | Director of Community Technology at Primary Care Information Project, NYC DOHMH |
| Ms. Kathleen Nolan | Director of State Policy & Programs, National Association of Medicaid Directors |
| Ms. Debi Sarkar | Maternal and Child Health Bureau, Genetic Services Branch, HRSA |
| Ms. Rebecca Goodwin and Dr. Alan Zuckerman | National Library of Medicine (NLM), NIH |
| Dr. Ray Nicola | Medical Officer, CDC |
| Dr. Joshua Jones | Medical Director, Public Health Informatics, Chicago Department of Public Health |
| Ms. Lakshmi Phatak, Mr. Zach Zettler, & Mr. Jack McKitrick | Netsmart Technologies |
| Dr. Guang Zhao | Director, Office of Public Health Statistics and Information Services, South Carolina Department of Health and Environmental Control |
| Mr. Jeff Sellers | Abbott Labs |
| Mr. Eric Jones | Chicago Department of Public Health |
| Dr. Abel Kho | Northwestern Memorial Hospital/CHITREC |
| Ms. Laura Zaremba & Ms. Mary McGinnis | Illinois Office of Health Information Technology |
| Dr. Bala Hota | Cook County Health and Hospitals System |
| Ms. Mary Driscoll, Ms. Judy Kauerauf, Mr. Matthew Roberts, Dr. Craig Conover & Dr. Mike Jadala | Illinois Department of Public Health |
| Dr. Patrick Lenihan | University of Illinois at Chicago |
| Dr. Robert Pestronk | Executive Director, NACCHO |
| Dr. Gregory Pappas & Ms. Tiffany West | HIV/AIDS, Hepatitis, STD, TB Administration Washington, DC |
| Mr. Richard Ehni | President, Consilience Software |
[1] Association of State and Territorial Health Officials (ASTHO). (2011). Profile of State Public Health. Volume II. Retrieved from: http://www.astho.org/uploadedFiles/_Publications/Files/Survey_Research/ASTHO_State_Profiles_Single%5B1%5D%20lo%20res.pdf on January 28, 2013.
[2] National Association of County and City Health Officials (NACCHO). (2010). National Profile of Local Health Departments. Retrieved from: http://www.naccho.org/topics/infrastructure/profile/resources/2010report/upload/2010_Profile_main_report-web.pdf on January 28, 2013.
[3] Kinner, K., & Pellegrini, C. (2009). Expenditures for public health: Assessing historical and prospective trends. American Journal of Public Health 99(10):1780-91.
[4] Institute of Medicine (IOM). (2010). For the Public’s Health: The Role of Measurement in Action and Accountability. Report Brief. Retrieved from: http://www.iom.edu/~/media/Files/Report%20Files/2010/For-the-Publics-Health-The-Role-of-Measurement-in-Action-and-Accountability/For%20the%20Publics%20Health%202010%20Report%20Brief.pdf on January 28, 2013.
[5] National Association of County and City Health Officials (NACCHO). (2011). Local Health Department Job Losses and Program Cuts: State-Level Tables from July/August 2011 Survey. Retrieved from http://www.naccho.org/topics/infrastructure/lhdbudget/loader.cfm?csModule=security/getfile&PageID=218960 on January 28, 2013.
[6] Robert Wood Johnson Foundation (RWJF). (2011). Investing in America's Health: A State-by-State Look at Public Health Funding and Key Health Facts. Retrieved from: http://healthyamericans.org/assets/files/Investing%20in%20America's%20Health.pdf on January 28, 2013.
[7] Centers for Medicare and Medicaid Services (CMS). (2010). Federal Funding for Medicaid Health IT Activities. State Medicaid Director Letter 10-106. Retrieved from: http://downloads.cms.gov/cmsgov/archived-downloads/SMDL/downloads/SMD10016.pdf on January 28, 2013.
[8] Centers for Medicare and Medicaid Services (CMS). (2011). Use of Administrative Funds to Support Health Information Exchange as part of the Medicaid EHR Incentive Program. State Medicaid Director Letter 11-004. Retrieved from: http://downloads.cms.gov/cmsgov/archived-downloads/SMDL/downloads/SMD11004.pdf on January 28, 2013.
[9] Centers for Medicare and Medicaid Services (CMS). (2012). Medicaid EHR Incentive Program: Public Health & Meaningful Use. Presentation by John Allison from CMS.
[10] Office of the National Coordinator for Health Information Technology (ONC). (2012). Southeast Minnesota Beacon Community (Rochester, MN). Retrieved from: http://www.healthit.gov/sites/default/files/private/beacon-factsheet-semn.pdf on January 28, 2013.
[11] Office of the National Coordinator for Health Information Technology (ONC). (2012). Evaluation of the State Health Information Exchange Cooperative Agreement Program: Early Findings from a Review of Twenty-Seven States. Retrieved from: http://www.healthit.gov/sites/default/files/private/pdf/state-health-info-exchange-coop-program-evaluation.pdf on January 28, 2013.
[12] National Association of City and County Health Officials (NACCHO). (2010). The Status of Local Health Department Informatics: Results from the 2010 NACCHO Informatics Needs Assessment. Retrieved from: http://www.naccho.org/ on January 28, 2013.
[13] Centers for Disease Control and Prevention (CDC). (2010). 10 Essential Public Health Services. Retrieved from: http://www.cdc.gov/nphpsp/essentialservices.html on January 28, 2013.
[14] Nangle, B., Xu, W., & Sundwall, D. N. (2009). Mission-driven priorities: Public health in health information exchange. AMIA Annual Symposium Proceedings Archive: 468-472.
[15] Magruder, C., Burke, M., Hann, N.E., & Ludovic, J.A. (2005). Using information technology to improve the public health system. Journal of Public Health Management and Practice 11(2):123-30.
[16] Association of State and Territorial Health Officials (ASTHO). (2011). Profile of State Public Health. Volume II. Retrieved from: http://www.astho.org/uploadedFiles/_Publications/Files/Survey_Research/ASTHO_State_Profiles_Single%5B1%5D%20lo%20res.pdf on January 28, 2013.
[17] Centers for Medicare and Medicaid Services (CMS). (2012). Medicaid EHR Incentive Program: Public Health & Meaningful Use. Presentation by John Allison from CMS.
[18] Abyankar, S., Lloyd-Puryear, M. A., Goodwin, R., Copeland, S., Eichwald, J., et al. (2010). Standardizing newborn screening results for health information exchange. AMIA Annual Symposium Proceedings: 1-5.
[19] Centers for Disease Control and Prevention (CDC). (2012). BioSense. Retrieved from: http://www.cdc.gov/Biosense/ on January 28, 2013.
[20] International Society for Disease Surveillance (ISDS). (2012). Draft Guidelines for Syndromic Surveillance Using Inpatient and Ambulatory Clinical Care EHR Data. A Report from the International Society for Disease Surveillance. Retrieved from: http://www.syndromic.org/uploads/files/MU_DraftGuideline_FINAL_pdf(1).pdf on January 28, 2013.
[21] Centers for Disease Control and Prevention (CDC). (2010). 10 Essential Public Health Services. Retrieved from: http://www.cdc.gov/nphpsp/essentialservices.html on January 28, 2013.
[22] Magruder, C., Burke, M., Hann, N.E., & Ludovic, J.A. (2005). Using information technology to improve the public health system. Journal of Public Health Management and Practice 11(2):123-30.
[23] National Association of County and City Health Officials (NACCHO). (2010). National Profile of Local Health Departments. Retrieved from: http://www.naccho.org/topics/infrastructure/profile/resources/2010report/upload/2010_Profile_main_report-web.pdf on January 28, 2013.
[24] National Institutes for Health (NIH). (2010). NHLBI, CDC Launch Surveillance and Research Program for Inherited Blood Diseases. Six States to Study Sickle Cell Disease and Thalassemias in National Pilot Project. Retrieved from: http://www.nih.gov/news/health/feb2010/nhlbi-18.htm on January 28, 2013.
[25] US Department of Health and Human Services (HHS). Health Information Privacy. Retrieved from: http://www.hhs.gov/ocr/privacy/ on January 28, 2013.
[26] US Department of Health and Human Services (HHS). (2003). Health Information Privacy: Public Health. Retrieved from: http://www.hhs.gov/ocr/privacy/hipaa/understanding/special/publichealth/index.html on January 28, 2013.
[27] Institute of Medicine (IOM). (2010). For the Public’s Health: The Role of Measurement in Action and Accountability. Report Brief. Retrieved from: http://www.iom.edu/~/media/Files/Report%20Files/2010/For-the-Publics-Health-The-Role-of-Measurement-in-Action-and-Accountability/For%20the%20Publics%20Health%202010%20Report%20Brief.pdf on January 28, 2013.
[28] National Association of County and City Health Officials (NACCHO). (2010). National Profile of Local Health Departments. Retrieved from: http://www.naccho.org/topics/infrastructure/profile/resources/2010report/upload/2010_Profile_main_report-web.pdf on January 28, 2013.
[29] Ibid.
[30] Association of State and Territorial Health Officials (ASTHO). (2011). Profile of State Public Health. Volume II. Retrieved from: http://www.astho.org/uploadedFiles/_Publications/Files/Survey_Research/ASTHO_State_Profiles_Single%5B1%5D%20lo%20res.pdf on January 28, 2013.
[31] Institute of Medicine (IOM). (2010). For the Public’s Health: The Role of Measurement in Action and Accountability. Report Brief. Retrieved from: http://www.iom.edu/~/media/Files/Report%20Files/2010/For-the-Publics-Health-The-Role-of-Measurement-in-Action-and-Accountability/For%20the%20Publics%20Health%202010%20Report%20Brief.pdf on January 28, 2013.
[32] National Association of County and City Health Officials (NACCHO). (2011). Local Health Department Job Losses and Program Cuts: State-Level Tables from July/August 2011 Survey. Retrieved from http://www.naccho.org/topics/infrastructure/lhdbudget/loader.cfm?csModule=security/getfile&PageID=218960 on January 28, 2013.
[33] Robert Wood Johnson Foundation (RWJF). (2011). Investing in America's Health: A State-by-State Look at Public Health Funding and Key Health Facts. Retrieved from: http://healthyamericans.org/assets/files/Investing%20in%20America's%20Health.pdf on January 28, 2013.
[34] Institute of Medicine (IOM). (2010). For the Public’s Health: The Role of Measurement in Action and Accountability. Report Brief. Retrieved from: http://www.iom.edu/~/media/Files/Report%20Files/2010/For-the-Publics-Health-The-Role-of-Measurement-in-Action-and-Accountability/For%20the%20Publics%20Health%202010%20Report%20Brief.pdf on January 28, 2013.
[35] First Focus, Nemours Foundation, The California Endowment and Voices for America’s Children. (2011). Improving Children’s Health and Well-being by Integrating Children’s Programs. Retrieved from: http://www.firstfocus.net/sites/default/files/private/Improving%20Children's%20Health%20and%20Well-being%20by%20Integrating%20Children's%20Programs_Final%20Report.pdf on January 28, 2013.
[36] Centers for Medicare and Medicaid Services (CMS). (2012). Medicaid EHR Incentive Program: Public Health & Meaningful Use. Presentation by John Allison from CMS.
[37] Centers for Medicare and Medicaid Services (CMS). (2012). Medicaid EHR Incentive Program: Public Health & Meaningful Use. Presentation by John Allison from CMS.
[38] Lab Interoperability Cooperative (LIC). (2012). LIC Services for Public Health. Retrieved from: http://labinteroperabilitycoop.org/public_health_services.htm on January 28, 2013.
[39] Centers for Medicare and Medicaid Services (CMS). (2010). Federal Funding for Medicaid Health IT Activities. State Medicaid Director Letter 10-106. Retrieved from: http://downloads.cms.gov/cmsgov/archived-downloads/SMDL/downloads/SMD10016.pdf on January 28, 2013.
[40] Centers for Medicare and Medicaid Services (CMS). (2011). Use of Administrative Funds to Support Health Information Exchange as part of the Medicaid EHR Incentive Program. State Medicaid Director Letter 11-004. Retrieved from: http://downloads.cms.gov/cmsgov/archived-downloads/SMDL/downloads/SMD11004.pdf on January 28, 2013.
[41] Centers for Medicare and Medicaid Services (CMS). (2012). Medicaid EHR Incentive Program: Public Health & Meaningful Use. Presentation by John Allison from CMS.
[42] Office of the National Coordinator for Health Information Technology (ONC). (2012). Evaluation of the State Health Information Exchange Cooperative Agreement Program: Early Findings from a Review of Twenty-Seven States. Retrieved from: http://www.healthit.gov/sites/default/files/private/pdf/state-health-info-exchange-coop-program-evaluation.pdf on January 28, 2013.
[43] Office of the National Coordinator for Health Information Technology (ONC). (2012). Southeast Minnesota Beacon Community (Rochester, MN). Retrieved from: http://www.healthit.gov/sites/default/files/private/beacon-factsheet-semn.pdf on January 28, 2013.
[44] The Urban Institute Health Policy Center. (2011). What Directions for Public Health under the Affordable Care Act? Retrieved from http://www.urban.org/UploadedPDF/412441-Directions-for-Public-Health-Under-the-Affordable-Care-Act.pdf on January 28, 2013.
[45] General Services Administration (GSA) Catalog of Federal Domestic Assistance. Affordable Care Act (ACA) Maternal, Infant, and Early Childhood Home Visiting Program. Retrieved from https://www.cfda.gov/?s=program&mode=form&tab=step1&id=63733ca5e5902beb890e19c5fbb36be8 on January 28, 2013.
[46] U.S. Department of Health and Human Services. January 23rd 2012 letter to state exchange grantees, Medicaid and CHIP directors, and Health and Human Services directors. Retrieved from http://www.fns.usda.gov/snap/rules/Memo/2012/SMD-1-23-12.pdf on January 30, 2013.
[47] Congressional Research Service. (2012). 501(c)(3) Hospitals: Proposed IRS Rules under § 9007 of the Affordable Care Act. Retrieved from http://www.naccho.org/topics/infrastructure/mapp/loader.cfm?csModule=security/getfile&pageID=237458 on January 28, 2013.
[48] Agency for Healthcare Research and Quality (AHRQ). Addressing the Problem through a Pathways Community HUB. Retrieved from: http://www.innovations.ahrq.gov/guide/HUBManual/addressing-problem.aspx on January 28, 2013.
[49] Department of Vermont Health Access. Blueprint for health. Retrieved from http://hcr.vermont.gov/blueprint on January 28, 2013.
[50] Gawande, A. (2011). The hot spotters: Can we lower medical costs by giving the neediest patients better care? The New Yorker. Retrieved from http://www.newyorker.com/reporting/2011/01/24/110124fa_fact_gawande on January 28, 2013.
[51] National Association of City and County Health Officials (NACCHO). (2010). The Status of Local Health Department Informatics: Results from the 2010 NACCHO Informatics Needs Assessment. Retrieved from: http://www.naccho.org/ on January 28, 2013.
[52] Institute of Medicine (IOM). (2012). Primary Care and Public Health: Exploring Integration to Improve Population Health. Report Brief. Retrieved from http://www.iom.edu/Reports/2012/Primary-Care-and-Public-Health.aspx on January 28, 2013.
[53] Joint Public Health Informatics Task Force (JPHIT). (2011). Consensus Framework for Advancing Public Health Informatics. Retrieved from: http://jphit.org/wp-content/uploads/2011/12/jphit_consensus-framework-approved-april202011.pdf on January 28, 2013.
[54] Dickerson D. (2012). Public health shared services model: applying public health standards to health department services and functions. Retrieved from https://apha.confex.com/apha/140am/webprogram/Paper258737.html on January 30, 2013.
[55] Lenert, L., & Sundwall, D. N. (2012). Public health surveillance and meaningful use regulations: A crisis of opportunity. American Journal of Public Health 102(3):e1–e7.
[56] Centers for Medicare & Medicaid Services (CMS). (2011). HITECH, Meaningful Use, and Public Health: Funding Opportunities for State Immunization Registries. Retrieved from: http://www.medicaidhitechta.org/Portals/0/Users/011/11/11/ImmunRegWhitePaper.pdf on January 28, 2013.
[57] Jacobson, P. D., & Neumann, P. J. (2009). A framework to measure the value of public health services. Health Services Research 44(5):1880-1896.