
Advance Care Planning Among Medicare Fee-For-Service Beneficiaries and Practitioners: Research Brief
Fang He, PhD; Angela Gasdaska, BS; Hannah Friedman, BA; Brendan Wedehase, BS; Alexis Kirk, PhD; Ila Broyles, PhD; Sarita L. Karon, PhD
RTI International
September 2020
Printer Friendly Version in PDF Format (5 PDF pages)
ABSTRACT
Advance care planning (ACP) is planning that aligns the care an individual wants to receive if they become unable to speak for themselves with their values and goals. Prior research show that end-of-life wishes were more likely to be known and respected for people who received ACP. We used quantitative methods to examine the use of the ACP codes in Medicare fee-for-service and qualitative methods to supplement the results from this quantitative data analysis. We found low but increasing use of the ACP codes, with variation by practitioner type, beneficiary mortality, and place of service. Although barriers to ACP remain, we identified a wide variety of other interventions encouraging ACP.
This brief was prepared under contract #HHSP233201600021I between HHS's ASPE/BHDAP and RTI International. For additional information about this subject, you can visit the DALTCP home page at https://aspe.hhs.gov/bhdap or contact the ASPE Project Officers, William Haltermann and Iara Oliveira, at HHS/ASPE/BHDAP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C., 20201; William.Haltermann@hhs.gov, Iara.Oliveira@hhs.gov.
DISCLAIMER: The opinions and views expressed in this brief are those of the authors. They do not reflect the views of the Department of Health and Human Services, the contractor or any other funding organization. This brief was completed and submitted on September 2019.
Background
Advance care planning (ACP) is a voluntary face-to-face service between a physician (or other qualified health care professional) and a patient to discuss the patient's health care wishes if they become unable to make decisions about their care. As part of this discussion, the practitioner may talk about advance directives (ADs) with or without completing relevant legal forms (CMS, 2019).[1] This process can help health care practitioners, families, and caregivers meet an individual's needs and align their care with their values and goals. Findings from a randomized controlled trial show that end-of-life wishes were more likely to be known and respected for people who received ACP (Detering et al., 2010). Yet many adults in the United States have not participated in ACP.
In 2015, the American Medical Association (AMA) introduced Current Procedural Terminology (CPT) codes 99497/99498 to describe ACP services. The Centers for Medicare & Medicaid Services (CMS) adopted these codes in 2016. The AMA defines these codes as follows:
-
Codes 99497/99498 are used to report the face-to-face service between a physician or other qualified health professional and a patient, family member, or surrogate in counseling and discussing ADs, with or without completing relevant legal forms. 99497 is for the first 30 minutes and 99498 is for each additional 30 minutes (AMA, 2018).[2]
In addition, in 2017, CMS introduced a temporary billing code G0505 to pay practitioners for providing cognitive assessment and care planning services to individuals with cognitive impairment. The AMA introduced CPT code 99483 in 2018, which CMS adopted to replace the temporary code G0505. The AMA defines this code as follows:
-
Assessment of and care planning for a patient with cognitive impairment, requiring an independent historian, in the office or other outpatient, home or domiciliary or rest home, with one of the required elements being the development, updating or revision, or review of an advance care plan (AMA, 2018).[2]
Study Methods
We used quantitative methods to examine the use of the ACP codes in Medicare fee-for-service (FFS) and qualitative methods to supplement the results from this quantitative data analysis. To conduct our data analysis, we used the 5% sample of Medicare's Limited Data Set files. These data include beneficiary enrollment and Part B service claim data from 2015-2018 Quarter 3 for a random 5% sample of Medicare FFS beneficiaries. We compared the characteristics of beneficiaries and practitioners with billed ACP claims to those without.
Our qualitative analysis included a literature review and interviews with subject matter experts (SMEs). For our literature review, we identified prior studies examining the use of the ACP codes. We also reviewed studies that identified barriers that may inhibit, and interventions that may facilitate, the use of the ACP codes and ACP in general. For our SME interviews, we conducted semi-structured, key informant interviews with CMS and nine SMEs knowledgeable about ACP and the ACP codes 99497, 99498, and 99483/G0505.
Findings
-
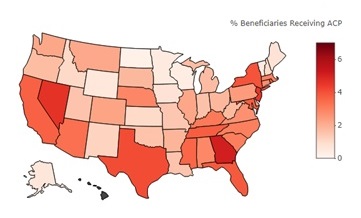
Use of the billing codes for ACP and for care planning for cognitively impaired individuals has been low but increasing. However, use varies by state.
| Percentage of Medicare FFS Beneficiaries with a Billed ACP Claim in 2017, by State | ||
|---|---|---|
 | Highest Percentage States | |
| State | Percentage of FFS Beneficiaries with Billed ACP Claim | |
| Hawaii | 7.77 | |
| Georgia | 5.10 | |
| Nevada | 4.65 | |
| New Jersey | 4.54 | |
| Texas | 4.10 | |
| Lowest Percentage States | ||
| State | Percentage of FFS Beneficiaries with Billed ACP Claim | |
| North Dakota | 0.22 | |
| Wisconsin | 0.39 | |
| Vermont | 0.44 | |
| Minnesota | 0.47 | |
| Wyoming | 0.59 | |
-
Practitioners. Internists and family practice physicians were the two specialties that billed ACP most often. However, nurse practitioners were most likely to provide ACP that lasts beyond 30 minutes. Neurologists and internists topped the specialties who billed for care planning for cognitively impaired individuals.
-
Beneficiaries. Compared with beneficiaries without a billed ACP claim, those with a billed ACP claim were older (75 on average versus 71), more likely to die within the year, and more likely to live in a county with higher socioeconomic status. In 2017, 48% of those with a billed add-on code (99498), for an additional 30 minutes, died that year. Although beneficiaries with a billed claim for care planning for individuals with cognitive impairment were older than those without a billed ACP claim, a similar percentage (4% in 2017) died within the year.
-
Claims. In 2017, 63% of billed ACP services were conducted in an office and 13% in an inpatient hospital. In contrast, only 15% of billed ACP services for an additional 30 minutes were conducted in an office and 48% in an inpatient hospital. 46% of billed ACP services occurred during an annual wellness visit (Medicare waives patient cost-sharing in these cases). The vast majority (75%) of claims for care planning for individuals with cognitive impairment were for services conducted in an office.
The low use of these ACP codes may be reflective of certain barriers, such as patient cost-sharing outside the annual wellness visit, practitioners' lack of awareness of the codes, patients' lack of awareness of ACP, and exclusion of certain clinical staff from billing these ACP codes. Although the literature and SMEs stressed the importance of paying practitioners for ACP separately as a method to facilitate ACP, barriers to ACP still exist. These include lack of time for practitioners to provide ACP, practitioner and patient discomfort with conversations covering end-of-life and other sensitive topics, and lack of training and education. However, we also identified a variety of interventions aimed at addressing these barriers. The most common are training and education programs for patients and practitioners.
Conclusion
We found low but increasing use of the ACP codes, with variation by practitioner type, beneficiary mortality, and place of service. Although barriers to ACP remain, we identified a wide variety of other interventions facilitating ACP. For example, more education and training may help increase use.
References
American Medical Association (AMA). (2018). CPT 2019: Professional Edition.
Centers for Medicare & Medicaid Services (CMS). (2019). Advance Care Planning MLN Fact Sheet. Retrieved from: https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/Downloads/AdvanceCarePlanning.pdf.
Detering, K., Hancock, A., Reade, M., & Silvester, W. (2010). The impact of advanced care planning on end of life care in elderly patients: Randomised controlled trial. BMJ 340: c1345.
He, F., Gasdaska, A., Friedman, H., Wedehase, B., Kirk, A., Broyles, I., & Karon, S. (2019). Advance Care Planning Among Medicare Fee-For-Service Beneficiaries and Practitioners: Final Report. Prepared for the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation.
Endnotes
-
There is no consensus definitions of ACP. Please see our discussion on the differences in ACP definitions in He et al. (2019).
-
For the complete definition, please see He et al. (2019).
ANALYSIS OF DISABILITY, AGING AND LONG-TERM CARE POLICY AND DATA
This report was prepared under contract #HHSP233201600021I between HHS's ASPE/BHDAP and RTI International. For additional information about this subject, you can visit the BHDAP home page at https://aspe.hhs.gov/bhdap or contact the ASPE Project Officers, at HHS/ASPE/BHDAP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C., 20201; William.Haltermann@hhs.gov, Iara.Oliveira@hhs.gov.
Reports Available
Advance Care Planning Among Medicare Fee-For-Service Beneficiaries and Practitioners: Final Report
- HTML version: https://aspe.hhs.gov/basic-report/advance-care-planning-among-medicare-fee-service-beneficiaries-and-practitioners-final-report
- PDF version: https://aspe.hhs.gov/pdf-report/advance-care-planning-among-medicare-fee-service-beneficiaries-and-practitioners-final-report
Advance Care Planning Among Medicare Fee-For-Service Beneficiaries and Practitioners: Research Brief