
Robert Mollica and Heather Johnson-Lamarche
National Academy for State Health Policy
Janet O'Keeffe
RTI International
PDF Version: http://aspe.hhs.gov/daltcp/reports/2005/04alcom.pdf (510 PDF pages)
This report was prepared under contract #HHS-100-01-0025 between the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Disability, Aging and Long-Term Care Policy and Research Triangle Institute. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, Gavin Kennedy, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. His e-mail address is: Gavin.Kennedy@hhs.gov.
"Acknowledgments
We would like to acknowledge the following for their contributions to this project: the Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services for its financial support; Christine O'Keeffe for her extensive research assistance; and the many people in state agencies through the country who answered questions and provided copies of the statutes, regulations, and reports needed to update this compendium. We greatly appreciate the willingness of these dedicated professionals to share their knowledge and expertise.
Section 1: Overview of Residential Care and Assisted Living Policy
Introduction
This compendium describes regulatory provisions and Medicaid policy for residential care settings in all 50 states and the District of Columbia. It updates an earlier report completed in 2002. Information was collected between February and June 2004 by reviewing state web sites and regulations and calling key state contacts to verify information. Section 1 provides an overview of residential care and assisted living policy. Section 2 presents six tables, which compare states' policy in selected areas. Section 3 provides summaries of each state's regulations and policy for residential care settings, including assisted living facilities.
This edition of the compendium differs from earlier editions in that it uses "residential care setting" or "residential care facility" as the generic terms for all types of group residential care settings, rather than the term assisted living. Although many states use the term assisted living generically to cover virtually every type of group residential care on the continuum between home care and nursing homes, for many stakeholders the term assisted living still represents a unique model of residential care that differs significantly from traditional types of residential care such as board and care. When discussing state statutes and regulation, the compendium uses the terms that each state uses.
Although adult foster care/adult family care is a type of residential care, it is not included in this report. However, some states now license adult foster/family care under their assisted living regulations. For example, North Carolina's statute defines adult family homes as serving two to six residents and adult care homes serve seven or more residents, but licenses both settings as assisted living residences.
Thirteen states (Alabama, Connecticut, Georgia, Kentucky, Louisiana, New Hampshire, New Mexico, North Carolina, Oklahoma, Rhode Island, South Carolina, South Dakota, and Utah) define at least one licensing category to include all residential care settings that serve one or more residents. Three states (Florida, Minnesota, and Tennessee) have a threshold of two or more, and eight states (Alaska, Arkansas, Colorado, Idaho, Illinois, Massachusetts, Missouri, and Vermont) have a threshold of three or more. A few states have different thresholds within a licensing category.
Consequently, in some states, the number of people served is no longer a major factor distinguishing the licensing category of adult foster/family care from that of assisted living. However, these states may still designate the number of people who may be served to distinguish between types of settings for other regulatory purposes, e.g., staffing requirements. Information about thresholds is generally noted in the state summary tables in Part III of this compendium.
Residential care is an important long-term care service option, particularly for individuals who cannot live alone but do not require the skilled level of care that nursing homes provide. The purpose of this compendium is to inform residential care policy by providing detailed information about each state's approach to regulating residential care, as well as its funding for services in these settings.
Overview of Policy Developments Since 2002
In 2004, states reported 36,451 licensed residential care facilities with 937,601 units/beds compared to 36,283 facilities with 909,196 units/beds in 2002; these numbers do not include facilities licensed as adult foster/family care or facilities licensed by Departments of Mental Retardation/Developmental Disabilities (MR/DD) or Mental Health.1 Compared to the previous four years, the growth rate in the supply of licensed facilities was basically flat between 2002 and 2004, and the number of number of units or beds rose only 3 percent. See Figure 1-1 for a comparison of growth rates in these years.
FIGURE 1-1. Supply Changes
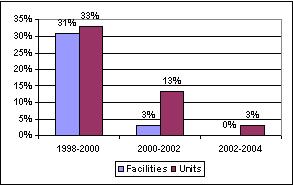
While growth was considerably higher between 1998 and 2000--30 percent nationwide--much of that increase resulted from high growth rates in a few states (214 percent in Delaware; 144 percent in Iowa, 139 percent in New Jersey, and 119 percent in Wisconsin); and ten states with growth rates between 40 percent and 100 percent (Alaska, Arizona, Kansas, Indiana, Massachusetts, Minnesota, Nebraska, New York, South Dakota, and Texas). Between 2000 and 2002, only two states, Arizona and Kansas, reported growth above 40 percent, and three--Nebraska, Nevada, and New Jersey--above 36 percent.
While the growth rate in units/beds nationwide was only 3 percent between 2002 and 2004, growth in ten states exceeded 20 percent (Alabama, Delaware, Hawaii, Kansas, Louisiana, Michigan, New Jersey, Oregon, Utah, and Wisconsin) as smaller facilities closed and larger, new facilities were licensed. Seven states reported a decline in the number of facilities but modest growth in the number of units (Colorado, Florida, North Carolina, Oklahoma, Pennsylvania, South Carolina, and Tennessee). Oregon extended a moratorium on new assisted living and residential care facilities. In 2004, three states--California, Florida and Pennsylvania--account for 33 percent of all units/beds, down slightly from 34 percent in 2002 and 36 percent in 2000.
The 2004 review of state policy and activity found that regulation of residential care settings continues to evolve. Regulatory changes tend to address the challenges posed by serving frailer and sicker residents and concerns among state licensing staff about inappropriate retention, adequacy of care, and the shortage of trained staff. Provisions revised include those related to staffing requirements, direct care and administrative training requirements, criminal background checks, admission and retention criteria, disclosure requirements, and resident agreements.
Twenty-eight states revised their regulations in 2003 and 2004, and 22 states reported current activity to revise regulations. States continue to address the need for specialized care for residents with Alzheimer's disease and other dementias; 44 states now have requirements for residential care facilities serving people with dementia. These requirements address disclosure, services available, admission/discharge criteria, staffing, training, activities, environment, and security. Twenty-six states have specific disclosure requirements for facilities that market themselves as special care facilities for persons with dementia.
| State | 2000 | 2002 | 2004 |
|---|---|---|---|
| Arizona | 1,240 | 2,300 | 3,067 |
| Colorado | 2,654 | 3,773 | 3,804 |
| Florida1 | 1,458 | 2,681 | 4,167 |
| Georgia | 2,262 | 2,759 | 2,851 |
| Minnesota2 | 397 | 2,895 | 4,144 |
| New Jersey | 699 | 1,500 | 2,195 |
| Oregon1 | 2,573 | 3,600 | 3,731 |
| Washington1 | 2,919 | 3,762 | 7,404 |
|
|||
States also continue to revise their residential care regulations to add a service philosophy. Finally, the number of states using the term assisted living for residential care settings continues to increase. Since 2002 the term was adopted in Rhode Island, Vermont, and in statute in New Hampshire (regulations were still being drafted in 2004). Forty-one states and the District of Columbia now have a licensing category or statute that uses the term assisted living.
Another continuing trend is the increase in Medicaid coverage of services in residential care settings. In 2004, 41 states reported serving about 121,000 residents in residential care settings--including assisted living but excluding adult foster/family care--up from 102,000 in 2002.2 Since 2002, Medicaid coverage has been implemented in Arkansas, extended to a new licensing category of residential care in Vermont, and approved in Alabama and the District of Columbia. California is developing a 1915(c) waiver application for a demonstration project. CMS approved a Medicaid HCBS waiver for West Virginia to conduct a pilot program in public housing sites in four counties. The number of people served under Medicaid grew more slowly between 2002 and 2004 compared to earlier years. Table 1-1 presents the number served under Medicaid waivers in six states over a 4-year period.
| State | Activities | Public Financing |
|---|---|---|
| Alabama | The state revised rules governing building requirements for assisted living facilities and special care assisted living facilities in July 2003; and revised provisions for incident investigations provisions in 2004. A waiver to serve persons with dementia in assisted living facilities has been approved but not implemented due to budget constraints. | Medicaid Waiver approved |
| Alaska | The state is consolidating state licensing statutes, which are expected to be completed in 2004 and effective by the end of 2005. The state transferred the Assisted Living Licensing Unit from the Division of Senior and Disability Services to the Division of Public Health. | Medicaid Waiver |
| Arizona | The state is forming a small workgroup to make recommendations for revisions to the assisted living rules which were expected to be final by the end of 2004. | Medicaid Waiver |
| Arkansas | The state approved rules for a new category of assisted living. A Medicaid waiver was approved to cover services in ALFs. Personal care services in RCFs are covered under the Medicaid state plan. | Medicaid State Plan Waiver Planned |
| California | State agencies are studying broad changes to the regulations. A task force has been formed to develop Medicaid coverage for two models: licensed residential care facilities and supportive housing and services. | Medicaid Waiver Planned |
| Connecticut | The state is reviewing provisions related to the level of care provided by managed residential communities. The state revised medication administration rules in 2002. The state's Housing Finance Agency and Medicaid are implementing a pilot affordable assisted living program. | Medicaid Waiver State funds |
| Colorado | The state approved rules changing the licensing category to assisted living and adding intermediate sanctions in March 2004. | Medicaid Waiver State funds |
| Delaware | Changes in the definition of "incident" and "reportable" have been proposed by the state's licensing agency in 2004. | Medicaid Waiver State funds |
| District of Columbia | An RFP has been issued to develop rules for an assisted living category approved by the District Council. The Medicaid waiver will be implemented once the rules are adopted. | Medicaid Waiver approved |
| Florida | The state is considering technical changes to the assisted living regulations. The Department of Elder Affairs transferred responsibility for training administrators and direct care workers to private organizations. | Medicaid Waiver State Plan |
| Georgia | The state issued rules for a new residential care category called community living arrangements in 2002. | Medicaid Waiver |
| Hawaii | The licensing agency is planning to establish licensing fees that would be used for training and other activities related to licensing. The state is considering changes to the structural requirements for facilities. | Medicaid Waiver |
| Idaho | The state is reviewing residential care statutes and rules and is developing draft revisions for comment in 2004. | Medicaid Waiver |
| Illinois | The state modified life safety code requirements for shelter care facilities rules in 2003. In 2004, the licensing agency proposed rules allowing designation of licensed units in assisted living and shared housing establishments. | Medicaid Waiver |
| Indiana | The state revised regulations in 2003. | Medicaid Waiver |
| Iowa | Revised regulations became effective in May 2004. The state has transferred oversight authority from the Department on Aging to the Department of Inspection and Appeals. | Medicaid Waiver |
| Kansas | The state transferred responsibility for regulating assisted living facilities to the Department of Aging in 2004. | Medicaid Waiver |
| Kentucky | No reported changes since 2001. | None |
| Louisiana | The state will consider revisions to the regulations dealing with dementia care, negotiated risk agreements, and other issues during 2004 and 2005. | Medicaid Waiver for demonstration planned |
| Maine | New regulations consolidating several categories of assisted living (congregate housing, residential care facilities, and adult family homes) became effective in September 2003. | Medicaid Waiver State Plan State funds |
| Maryland | The state formed a work group in 2003 to conduct a thorough review of the regulations and recommend changes to the legislature at the end of 2004. | Medicaid Waiver State funds |
| Massachusetts | The state revised regulations in December 2002 and continues to review statutes and regulations to determine if further changes are needed. | Medicaid State Plan |
| Michigan | In 2004, the licensing agency submitted revisions to the Homes for the Aged rules to the legislature for review before being promulgated. * Michigan's Medicaid waiver serves residents in elderly housing buildings that are called assisted living but are not required to be licensed. |
Medicaid Waiver* State Plan |
| Minnesota | The state adopted new training requirements for facilities that serve people with dementia in 2003. The state amended its waiver to cover residents with incomes up to 300 percent of the federal SSI benefit in 2003. | Medicaid Waiver |
| Mississippi | The state adopted rule revisions in 2002 and 2003. The most significant change expanded requirements for criminal background checks. | Medicaid Waiver |
| Missouri | The Department of Health and Senior Services submitted revisions addressing fire safety and evacuation and administrator requirements to the Board of Health. The changes are expected to be finalized in the fall of 2004. | Medicaid State Plan |
| Montana | In 2003, the state enacted legislation changing the licensing category from personal care facilities to assisted living and modifying the requirements for assisted living facilities. The state is working on regulations, which are expected to be effective in May 2004. The state developed separate requirements for facilities serving people with dementia. | Medicaid Waiver |
| Nebraska | The state revised its regulations for assisted living facilities in 2003. Facilities may not use the assisted living term unless they are licensed. | Medicaid Waiver |
| Nevada | In 2004, the state amended its Medicaid waiver to cover a broader array of services in assisted living and clarified various definitions in the licensing rules. The state also enacted a new law limiting sharing of units to two residents by consent and requires toilet facilities in each unit. | Medicaid Waiver |
| New Hampshire | The state is still revising rules for its assisted living category and will operate under expired rules until the new rules are issued. | Medicaid Waiver |
| New Jersey | The regulations expire in 2004 and the state is drafting revisions, which will be published in the fall of 2004. In the same year, the state enacted legislation establishing training requirements for staff serving people with dementia. | Medicaid Waiver |
| New Mexico | The state is revising rules for adult residential care facilities. A Committee formed by the Department of Health is working on revisions to education and training requirements for direct care workers and administrators, which are expected to be finalized in 2004. | Medicaid Waiver |
| New York | In 2004, the state enacted an assisted living reform law creating a new level of service for assisted living facilities. Facilities may obtain a certificate allowing them to offer enhanced assisted living services to support aging in place. | Medicaid State Plan |
| North Carolina | The state gave its Division of Facility Services temporary rule making authority to enable it to respond quickly to priority issues such as discharge requirements, compliance, and training. | Medicaid State Plan |
| North Dakota | In 2003, the state replaced its registration process for assisted living programs (housing with services) with new licensing requirements. | Medicaid Waiver State funds |
| Ohio | The state is revising its residential care facility rules. | None |
| Oklahoma | In 2004, the Department of Health proposed rules to change physical plant standards. | None |
| Oregon | The state extended a moratorium on new assisted living facilities until June 2005. The state adopted substantial changes to the regulations for residential care facilities in 2004, and revised requirements for criminal background checks. | Medicaid Waiver |
| Pennsylvania | The state expects to finalize revisions to its personal care home rules in September 2004. Legislation is pending that would create an assisted living services licensing program and expand Medicaid coverage of assisted living services. | Medicaid Waiver pilot |
| Rhode Island | The state implemented rule revisions in 2004, which address dementia training requirements, quality improvement, staff training, functional assessments, and care philosophy. The state also implemented a pilot residential care project for low-income persons, designed by the state Department of Elderly Affairs and the RI Housing Finance Agency. | Medicaid Waiver |
| South Carolina | The state issued guidelines for conducting criminal background check in October 2002 and enacted legislation allowing trained aides to administer selected prescribed medications. Coverage under the Medicaid state plan was implemented. | Medicaid State Plan |
| South Dakota | The state made minor rule changes in December 2002 and is working on revisions to the life safety code. The state is planning to amend its Medicaid waiver to broaden coverage of services available in assisted living centers. | Medicaid Waiver State funds |
| Tennessee | The state revised assisted care living facility rules in 2003, which addressed reporting of unusual events, policies and procedures for health care decision-making for incompetent residents, and the retention of residents. | None |
| Texas | The state revised regulations in 2002 and 2003 and is considering further revisions that would authorize electronic monitoring, set an administrative penalty schedule, and require central air conditioning in new facilities. | Medicaid Waiver |
| Utah | The state revised rules in 2002 and has formed a work group to review provisions regarding medication administration. In 2004, the state expanded its Medicaid state plan managed care program that covers assisted living. | Expanded Medicaid State Plan |
| Vermont | New regulations for a category of assisted living were made effective in March 2003. Medicaid waiver coverage was extended to assisted living residences, and the state has implemented a program to reimburse for "assistive care services" under the Medicaid state plan. | Medicaid Waiver State Plan |
| Virginia | The state is reviewing regulations. Some revisions were made effective in March 2003. * Virginia uses state funds to support a limited number of residents formerly served under a discontinued waiver. |
None* |
| Washington | The state has completed a two year process for revising its regulations. Revisions will be effective in September 2004. The state also revised its Medicaid reimbursement methodology and implemented a case mix reimbursement system in 2003. | Medicaid Waiver State Plan |
| West Virginia | In 2004, the state received CMS approval for a pilot Medicaid waiver to serve elders in converted public housing buildings in four counties. In 2003, the state combined personal care homes and residential board and care homes into one category of assisted living residences. The state finalized rules for assisted living residences in February 2004. | Medicaid Waiver pilot |
| Wisconsin | The state is working with providers and stakeholders to develop strategies to improve quality and to identify needed changes in the rules for Community Based Residential Facilities. | Medicaid Waiver State Plan |
| Wyoming | No reported changes since 2001. | Medicaid Waiver |
Defining Assisted Living
The widespread use of the term assisted living and the considerable state variability in its definition continues to fuel debate about what assisted living is and should be, how it should be regulated, particularly as the number of residents with higher levels of need increases, and whether facilities that do not support key assisted living principles should use the term.
States historically have licensed two general types of residential care: (1) adult foster care or family care, which typically serves five or fewer residents in a provider's home; and (2) group residential care that typically serves six or more residents in a range of settings (from large residential homes to settings that look like commercial apartment buildings or nursing homes). States have used many names for these larger group residential care settings, including: board and care homes, rest homes, adult care home, domiciliary care homes, personal care homes, community-based residential facilities, and assisted living. Until recently, the most frequently used term was board and care, though today all types of group residential care are generally referred to as assisted living.
The physical character of a substantial portion of older group residential care facilities is quite institutional, with two to four persons sharing a bedroom, and as many as eight to ten residents sharing a bathroom. Concerned about the institutional character of these settings, policymakers in Oregon--and gradually in other states--developed a new licensing category called assisted living. What was new and desirable about assisted living was that it offered residents what traditional board and care facilities did not--a philosophy of care that emphasized privacy and the ability to have greater control over daily activities such as sleeping, eating, and bathing.
Consumer preference for the new assisted living model of residential care led providers to market all types of residential care facilities as "assisted living"--whether or not they provided private units or operated with a service philosophy that assures resident autonomy. Forty-one states and the District of Columbia now use the term assisted living in their residential care regulations. In some states, assisted living is a specific model with a consumer-centered service philosophy, private apartments or units, and a broad array of services which support aging-in-place. In others states, residential care licensing categories have been consolidated under a new general set of "assisted living" rules that might cover the new model of assisted living, as well as board and care, multi-unit elderly housing, congregate housing and sometimes even adult family or foster care (e.g., Maine, Maryland, and North Carolina).
Assisted living may be a licensed setting in which services are delivered or a licensed agency that delivers services in a range of settings. Four states (Connecticut, Maine, Minnesota, and New Jersey) describe assisted living services that may be provided in two or more settings. Connecticut and Minnesota see assisted living as a service, and license the service provider (which may be a separate entity from the organization that owns or operates the building). Other states see assisted living as a building in which supportive and health related services are provided. The operator of the building is licensed, and services may be provided by the operator's staff or contracted to an outside agency. See ">Box 1-1 for a more detailed description of state's licensing and regulatory approaches.
BOX 1-1. State Licensing and Regulatory Approaches
Institutional Model. This model has minimum building and unit requirements; typically, multiple occupancy bedrooms without attached baths, and shared toilets, lavatories, and tub/shower areas. Generally, states permit these facilities to serve people who need assistance with activities of daily living (ADLs). But they either do not allow nursing home eligible residents to be admitted or do not allow facilities to provide nursing services. Historically, this model did not allow residents who met the criteria for placement in a nursing home to be served. However, as residents have aged in place, some states have made their rules more flexible to allow a higher level of service. For example, some states allow skilled nursing services to be provided for limited periods by a certified home health agency. North Carolina is one of the states that using this approach.
Housing and Services Model. This model licenses or certifies facilities to provide a broad range of long-term care services in apartment settings to persons with varying service needs, some of whom may be nursing home eligible. The state allows providers to offer relatively high levels of care, although licensed facilities may set their own admission/retention polices within state parameters and may choose to limit the acuity of its residents. Depending on the state, some or all of the needs met in a nursing home may also be met in residential care settings. By creating a separate licensing category for this model and retaining other categories, states distinguish these facilities from board and care facilities. Oregon is one of the states using this approach.
Service Model. This model licenses the service provider, whether it is the residence itself or an outside agency, and allows existing building codes and requirements--rather than new licensing standards--to address the housing structure. This model simplifies the regulatory environment by focusing on the services delivered rather than the architecture. Approaches for regulating services may also specify the type of buildings, apartment or living space that can qualify as assisted living. Minnesota is one of the states using this approach.
Umbrella Model. This model uses one set of regulations to cover two or more types of housing and services arrangements: residential care facilities, congregate housing, multi-unit or conventional elderly housing, adult family care, and assisted living. Maine is one of the states using this approach.
Multiple Levels of Licensing for a Single Category. Some states set different licensing requirements for facilities in a single category, based on the extent of the assistance the facility provides or arranges and on the type of residents served. For example, Maryland licenses facilities based on the characteristics of residents they serve. The state categorizes low-, moderate-, and high-need residents based on criteria for health and wellness, functional status, medication and treatment, behavior, psychological health, and social/recreational needs. The state may grant a limited number of waivers to facilities allowing them to serve residents who develop needs that exceed the facility's licensing level.
Some of these approaches are not mutually exclusive and may be combined.
Generic use of the term assisted living obscures the differences between types of residential care settings, and makes it difficult for consumers to determine which setting will best meet their current and future needs. A recent study of six states' use of Medicaid to fund services in residential care settings, stakeholders in every state except Oregon cited public confusion about residential care options as a major problem.3
In 2000, the U.S. Senate Aging Committee held a hearing and challenged the industry to address concerns raised in a General Accountability Office (GAO) report, one of which was the lack of a common definition of assisted living and resulting consumer confusion about this long-term care option. This and subsequent hearings led to the formation of the Assisted Living Workgroup (ALW) designed to bring together assisted living stakeholders to make recommendations to ensure high-quality care for all assisted living residents and to develop a common definition. The workgroup included over 50 organizations with a variety of interests including industry associations, professional organizations, consumer and advocacy groups, and regulators. See ">Box 1-2 for examples of various definitions of assisted living, including the one proposed by the ALW.
As states allow residential care settings to provide more health-related and nursing services, many observers believe that the key challenge in defining assisted living is to distinguish it from nursing homes while recognizing that both settings may serve some similar residents.
Federal law defines a nursing facility as an institution (or a distinct part of an institution) that is primarily engaged in providing skilled nursing care and related services for residents who require medical or nursing care, rehabilitation services for injured, disabled, or sick persons (a skilled level of care), or on a regular basis, health-related care and services to individuals who because of their mental or physical condition require care and services (above the level of room and board) which can be made available to them only through institutional facilities (the minimum level of care).4
Many individuals who qualify for Medicaid coverage of nursing home care--particularly those who do not require a skilled level of care--receive care at home from family members, home health agencies and publicly funded programs such as the Medicaid home and community-based services (HCBS) waiver program. Because HCBS programs may only serve Medicaid beneficiaries who meet each state's nursing home criteria, their emergence challenged the assumption that persons who needed nursing home care could only be served in a nursing home. It is now recognized that many nursing home eligible persons can be appropriately served in multiple settings, including residential care settings.
BOX 1-2. Examples of Definitions of Assisted Living
Assisted Living Workgroup*
Assisted living is a state regulated and monitored residential long term care option. Assisted living provides or coordinates oversight and services to meet the residents' individualized scheduled needs, based on the residents' assessments and service plans and their unscheduled needs as they arise. Services that are required by state law and regulation to be provided or coordinated must include but are not limited to:
- 24-hour awake staff to provide oversight and meet scheduled and unscheduled needs
- Provision and oversight of personal care and supportive services
- Health related services (e.g., medication management services)
- Meals, housekeeping, and laundry
- Recreational activities
- Transportation and social services
These services are disclosed and agreed to in the contract between the provider and resident. Assisted living does not generally provide ongoing, 24-hour skilled nursing. It is distinguished from other residential long-term care options by the types of services that it is licensed to perform in accordance with a philosophy of service delivery that is designed to maximize individual choice, dignity, autonomy, independence, and quality of life.
Joint Commission on Accreditation of Healthcare Organizations
An assisted living residence is "a congregate residential setting that provides or coordinates personal services, 24-hour supervision and assistance (scheduled and unscheduled), activities, and health-related services. It is designed to minimize the need to move; accommodate individual residents' changing needs and preferences; maximize residents' dignity, autonomy, privacy, independence, choice and safety; and encourage family and community involvement."**
Oregon
Assisted living means a building, complex or distinct part thereof, consisting of fully self-contained individual living units where six or more seniors and persons with disabilities may reside. The facility offers and coordinates a range of supportive personal services available on a 24-hour basis to meet the ADL, health services, and social needs of the residents described in these rules. A program approach is used to promote resident self-direction and participation in decisions that emphasize choice, dignity, privacy, individuality, independence and homelike surroundings." No facility in Oregon may use the term assisted living unless they are licensed.
* The ALW final report and recommendations may be found at http://www.aahsa.org/alw.htm.
** Joint Commission on Accreditation of Healthcare Organizations. 2003-2005 Accreditation Manual for Assisted Living.
Because HCBS waiver programs serve some nursing home eligible persons in home and residential care settings, it is not really possible to develop mutually exclusive definitions for nursing homes and residential care, except for the provision of a skilled level of care. Doing so would severely limit states' ability to offer these residential care settings as a service alternative for nursing home eligible persons. States want to be able to serve at least some nursing home eligible individuals in more homelike residential care settings without imposing the nursing homes' regulatory structure.
Some observers believe there is perhaps too much emphasis on developing a common definition of assisted living given that all 50 states have the authority to define it how they want. Some believe that a better approach would describe assisted living in a way that recognizes the overlap of needs that can be met and the services that can be offered by both nursing homes and assisted living, yet highlights differences between them. One state regulator has suggested the following definition--"Assisted living is a facility which provides housing, meals and long-term care services in a group residential setting that is not a nursing home"--adding that specific requirements for different types of assisted living should then be spelled out in regulation. At the same time, providers need to understand what their liability is in taking a medically fragile individual and their requirements to meet a resident's needs.5
To help prospective residents understand the differences between nursing homes and different types of residential care, some states might require--as Oregon does--that facilities use standardized disclosure forms to describe their scope of service, rate structure, caregiver and nursing staff levels. Many believe that this approach will be much more helpful for consumers than a uniform definition of assisted living.
In short, individuals with health needs and impaired abilities can be served in a range of settings by a variety of service providers: home health agencies, home care agencies, adult day care, different types of residential care (adult foster care, board and care, assisted living), and nursing homes. Residential care is an important service option for people who cannot live alone and do not have informal care.
States have the responsibility for regulating residential care settings and their definitions and approaches reflect each state's unique policy environment and preferences. Consequently, development of a standard definition of assisted living is unlikely. The approach to defining and categorizing residential care for research purposes depends on the research question. One national survey grouped facilities according to the level of services and the amount of privacy they offered (high and low).6 A study comparing resident outcomes in residential care and nursing homes would need to categorize facilities according to characteristics relevant to outcomes, such as staffing levels and the provision of nursing services and oversight.
Assisted Living Philosophy
Twenty-nine states and the District of Columbia reported that they include provisions regarding assisted living concepts such as privacy, autonomy and decision making in their residential care regulations or Medicaid standards. (See ">Table 1-3.) Some states regulations are more detailed in these matters, others are less so. For example, regulations may state the importance of privacy, but only 11 states with a statement of the philosophy of assisted living require private apartment units;7 five have mixed requirements, allowing bedrooms in some settings and individuality apartments in new construction; and 14 allow sharing (apartments or bedrooms) only by resident choice. (See section on Occupancy Requirements and Privacy for additional information.) Examples of state provisions that reference assisted living principles follow.
| TABLE 1-3. States with Regulations that Include Assisted Living Philosophy | |||
|---|---|---|---|
| Alaska Arizona Arkansas District of Columbia Florida Hawaii Idaho Illinois |
Iowa Kansas Louisiana Maine Maryland Massachusetts Montana Nebraska |
Nevada New Jersey New Mexico New York North Dakota Oklahoma Oregon |
Rhode Island South Carolina Texas Vermont Washington Wisconsin Wyoming |
-
Florida's statute describes the purpose of assisted living as "to promote availability of appropriate services for elderly and disabled persons in the least restrictive and most homelike environment, to encourage the development of facilities which promote the dignity, privacy and decision-making ability" of residents. The Florida law also states that facilities should be operated and regulated as residential environments and not as medical or nursing facilities. Regulations require that facilities develop policies to maximize independence, dignity, choice, and decision-making.
-
Illinois' statute defines assisted living, in part, as a model that (1) assumes that residents are able to direct their services and will designate a representative to direct them if they are unable to do so; and (2) supports the principle that there is an acceptable balance between consumer protection and resident willingness to accept risk and that most consumers are competent to make their own judgments about the services they are obtaining. The statute states that regulation of assisted living establishments and shared housing establishments "shall be operated in a manner that provides the least restrictive and most homelike environment and that promotes independence, autonomy, individuality, privacy, dignity, and the right to negotiated risk in residential surroundings."
-
New Jersey requires facilities to coordinate services "in a manner which promotes and encourages assisted living values. These values are concerned with the organization, development, and implementation of services and other facility or program features so as to promote and encourage each resident's choice, dignity, independence, individuality, and privacy in a homelike environment," as well as "aging in place and shared responsibility."
-
Texas' authorizing statute specifies that rules must be developed to promote policies that maximize the dignity, autonomy, privacy, and independence of each resident; and that service delivery should be driven by a philosophy that emphasizes personal dignity, autonomy, independence, and privacy and should enhance a person's ability to age in place.
-
Oregon, the first state to adopt a specific philosophy for assisted living, states that: "Assisted living … is a program that promotes resident self-direction and participation in decisions that emphasize choice, dignity, privacy, individuality, independence and homelike surroundings."
-
Washington requires that the basic training curriculum for staff in residential care settings includes instruction on how to perform tasks while incorporating resident preferences; how to maintain residents' privacy and dignity; and how to create opportunities that encourage resident independence.
Unless states operationalize assisted living concepts as specific regulatory requirements--for example, assuring privacy by requiring private rooms or apartments--the choices that facilities make in their physical and organizational structures and their service and training policies will generally determine whether the state's intent is realized. In the absence of specific regulatory requirements, it may be difficult to determine whether a facility is carrying out the regulations' philosophy.
Consumer advocates have questioned whether staff that inspect or survey nursing facilities should also inspect residential care facilities operating under an assisted living philosophy and related rules, without having specific training about this philosophy. Some states provide this training (e.g., Texas requires training for state inspectors on how assisted living differs from nursing homes). The National Academy of State Health Policy (NASHP) 2002 survey of state licensing agencies found that 24 states use different staff to survey residential care facilities than they use for nursing facilities; survey staff in the remaining states inspect both.
Negotiated Risk Agreements
As illustrated in the examples above, assuring resident autonomy is a central concept in the assisted living philosophy. Fifteen states and District of Columbia have regulations referencing a process or approach for negotiating disagreements about residents' autonomy and risk taking and providers' concerns about risk (Alaska, Arkansas, Delaware, Florida, Hawaii, Illinois, Iowa, Kansas, New Jersey, Ohio, Oklahoma, Oregon, Vermont, Washington, and Wisconsin.) States use different terms to describe the process--negotiated risk, managed risk, shared responsibility, compliance agreement, and negotiated plan of care.
Despite differences in the term, most of the regulations share common features, such as requiring that the agreement be written and signed by the resident and the appropriate facility administrator. State regulations typically require that the agreement describe the possible consequences of the resident's actions, the specific concerns of the facility, options that will both minimize the risk and respect resident's choices. They also generally require documentation of the negotiation process, and agreement or lack thereof, and the decision reached by the resident after consideration of the facility's concerns. Several states allow surrogates or sponsors to negotiate risk agreements.
Examples of state's specific provisions follow.
-
The District of Columbia defines a shared responsibility agreement is a "tool to recognize a resident's right to autonomy by respecting his or her right to make individual decisions regarding lifestyle, personal behavior, safety and individual service plans.
-
New Jersey defines managed risk as the process of balancing residents' choice and independence with the health and safety needs of the resident and other persons in the facility or program. If a resident's preference or decision places the resident or others at risk or is likely to lead to adverse consequences, the facility may discuss such risks or consequences with the resident (and their representative if the resident wants). The facility can then negotiate with the resident a formal plan to avoid or reduce negative or adverse outcomes.
-
Oregon's rules do not allow managed risk plans "with or on behalf of a resident who is unable to recognize the consequences of his/her behavior or choices."
-
Vermont's rules require that the facility notify the resident that the state Long Term Care Ombudsman is available to assist in the negotiated risk process.
-
Wisconsin's rules state that risk agreements do not mitigate or waiver any tenant's rights.
State licensing officials indicated that the negotiated risk process is not widely used.
Occupancy Requirements and Privacy
Historically, the physical character of a substantial portion of residential care was quite institutional--as permitted by state regulation--with two to four persons sharing a bedroom, and as many as eight to ten residents sharing toilet and bathing facilities. The new assisted living model of residential care became popular with older people in large part because it offers what traditional board and care facilities generally do not: privacy and the concomitant opportunity to have greater control over daily activities such as eating and sleeping. Another reason for its popularity is that assisted living facilities built in the 1990s have more desirable physical environments than do board and care facilities, many of which were built in the 1960s and 1970s.
Consequently, single occupancy apartments or rooms dominate the assisted living private-pay market. A survey of non-profit facilities conducted in 1999 by the Association of Homes and Services for the Aging found that 76 percent of the units in free-standing facilities and 89 percent of units in multi-level facilities were private (studio, one-, or two-bedroom units).8 A similar survey by the Assisted Living Federation of America found that 87.4 percent of units in its member facilities were studio, one-, or two-bedroom units and 12.6 percent were semi-private.9 In a national survey of assisted living facilities in the late 1990s, Hawes, et al. found that 73 percent of the units were private, 25 percent of the units were semi-private (shared by two unrelated persons), and 2 percent were "ward-type" rooms that housed three or more unrelated persons.10
A 1998 survey of assisted living facilities by the National Investment Conference (NIC) found that 17 percent of the residents shared a unit. Of these, 52 percent said that they shared their unit for economic reasons, 30.4 percent for companionship, and 14.9 percent because a private unit was not available. Just under 65 percent of those who shared a unit were satisfied with the arrangement and 35.7 percent preferred a single unit.11
Nationally, consumer demand, the availability of subsidized units, and the extent of competition are more likely than regulatory policy to determine whether studio or apartment-style living units are available for private pay residents. However, for Medicaid eligible residents, state regulatory policy and Medicaid policy determine the types of units available. For example, Medicaid contracting requirements in Washington require participating facilities to provide private apartments shared only by choice.
Due to the popularity of assisted living, many providers of all types of residential care settings market themselves as assisted living, whether or not they give all private rooms to all residents. Some board and care homes that want to be licensed as assisted living may have an interest in opposing rules requiring apartment-style units and single occupancy. On the other hand, advocates of assisted living as a unique model of care oppose the use of the term assisted living by facilities that do offer private rooms or units to all residents. Consequently, occupancy requirements have become a contentious issue. States have taken a number of approaches to setting occupancy requirements.
Some states have simply amended their statutes to rename board and care homes as assisted living and continue to permit dual occupancy. Others have allowed dual occupancy standards in grandfathered buildings but require new buildings to offer single occupancy units. Some states maintain separate licensing categories, allowing dual occupancy in some settings and requiring single occupancy in others. Several states have multiple licensing categories, and the two-person limit may apply to only one of the categories.
Thirty-five states have rules that allow two people to share a unit or bedroom. Several of these states have multiple licensing categories, and the two-person limit may apply to only one of the categories. Ten states have licensing categories that allow four people to share a room; three states allow three people to share units. A few states to do not specify how many people may share a bedroom.
States that have developed a multiple-setting assisted living model vary the requirements by the setting. For example, New York allows sharing for board and care facilities participating in the Medicaid program but requires apartments in the "enriched housing category," which includes purpose-built residences and subsidized housing. Additional examples of states' requirements follow.
-
Florida licenses two types of assisted living, one which allows up to four people to share a bedroom, and extended congregate care, which requires private apartments or private rooms shared only by a resident's choice.
-
New Mexico's Medicaid assisted living waiver provides services in two types of facilities offering "home-like" environments, which offer either units with 220 square feet of living and kitchen space (plus bathroom), or single or semi-private rooms in adult residential care facilities; rooms may be shared only by choice.
-
Texas covers assisted living services through Medicaid to residents in three settings: assisted living apartments (single occupancy); residential care apartments (double occupancy allowed); and residential care non-apartments (double occupancy rooms).
Four people may share a room under what might be considered board and care licensing rules in Delaware, Georgia, Indiana, Iowa, Michigan, Mississippi, Missouri, Nebraska, Pennsylvania, Rhode Island, South Carolina, and Virginia. Shared toilet facilities and bathing facilities are the rule among states with board and care regulations. State rules that allow bedrooms to be shared by two to four residents require bathrooms and lavatories for every six to ten residents.
While a state's policy sets the parameters for what may be offered and provided, the actual practice may be narrower. Shared units may be allowed, but the market may produce very few or no projects that offer shared units. Further, facilities constructed prior to the development of the assisted living model may offer shared units while most, if not all, newly constructed buildings have predominantly or solely private units.
Disclosure Requirements and Residency Agreements
A GAO study of assisted living facilities in four states concluded that while most facilities provide information about the services available, they do not routinely provide information about discharge criteria, staff training and qualifications, services not available from the facility, grievance procedures, and medication policies. The GAO report concluded that the need to provide adequate information to prospective and current residents is a major issue that requires additional oversight.12
With few exceptions, states that license residential care require facilities to include specific information in residency agreements. Two states do not require residency agreements and Connecticut and Minnesota do not use residency agreements because they license the service provider and the housing provider executes a lease agreement with tenants. Table 1-4 lists the type of information that states may provide in resident agreements and the number of states that require the provision of this information.
| Topics Covered | States Requiring |
Topics Covered | States Requiring |
|---|---|---|---|
| Services included in basic rate | 49 | Grievance procedures | 21 |
| Cost of service package | 44 | Termination (including admission and discharge) | 20 |
| Admission/discharge | 29 | Terms of occupancy | 18 |
| Refund policy | 29 | Temporary absences | 14 |
| Cost of additional services | 27 | Accommodations | 12 |
| Service beyond basic rate | 26 | Advance payments | 7 |
| Rate changes | 25 | Period covered | 11 |
| Payment/billing | 23 | Services not available | 9 |
| Residents rights | 22 | Other | 20 |
As can be seen, the majority of states provide information about services, but only about half or less provide information about most of the other topics. Few states require information about medication policy and staffing.
Examples of "other" requirements follow:
-
Colorado requires facilities to disclose whether it has an automatic sprinkler system.
-
Kansas requires facilities to give prospective residents citations of relevant statutes, information on advance medical directives, resident rights, and the facility's grievance procedure, before an agreement is signed.
-
Maine does not allow the resident agreement to contain any provision for discharge which is inconsistent with state rules or law or which implies a lesser standard of care than is required by rule or law. Agreements in Maine must also include information on grievance procedures, tenant obligations, resident rights, and the facility's admissions policy.
-
Maryland requires disclosure in the agreement of the level of care that the facility is licensed to provide and the level of care needed by the resident at the time of admission. The state also requires facilities to disclose policies concerning shared occupancy and procedures that will be followed when a resident's accommodations are changed due to relocation, change in roommate assignment, or an adjustment in the number of residents sharing a unit.
-
New Hampshire issued regulations in 2003 requiring disclosure of information to allow residents to compare assisted living residences, independent retirement communities and elder housing, in order to make an informed choice about where to live. The state requires facilities to disclose whether they are licensed; the basic rate; the personal care and other services included in the rate; meals provided; transportation services; recreation and leisure activities; amenities in the living unit; policies regarding deposits/advance payment requirements and refundability; services not included in the basic rate and their cost. Facilities must also provide information about their staffing, including whether staff are available 24-hours a day, and the availability of licensed nurses, personal care attendants, nursing assistants, and maintenance staff.
-
Wisconsin requires that the qualifications of staff that will provide services be included in the agreement as well as whether services are provided directly or by contract.
Some states require facilities to provide some of the information listed in Table 1-4 in a residents' rights statement rather than a residency agreement, particularly information about grievance procedures.
The GAO study cited unmet consumer expectations for aging-in-place and forced moves as a major resident complaint. Only 20 states require agreements to include information about the facility's criteria for admission, discharge, or transfer.
Finally, several states have rules regarding the format of resident agreements. Kansas requires that agreements be written in clear and unambiguous language in 12-point type. Maryland requires agreements to use accurate, precise, easily understood, legible, readable, "plain" English. Wisconsin requires that agreement formats make it easy to readily identify the type, amount, frequency, and cost of services. Some states require information about provisions that allow staff to inspect living quarters, with the resident's permission.
Most state rules do not have rules for revising or updating resident agreements. However, Alabama, Illinois, Mississippi, and Oregon require that agreements include the period covered by the agreement. Wisconsin required that the agreement be reviewed and updated when there is a change in the resident's condition or at the request of the facility or the resident. Updates are otherwise made as mutually agreed to by the resident and the provider.
Admission and Retention Criteria
States regulations pertaining to admission and retention typically consider applicants' or residents' general condition, health-related need including the need for nursing care, physical and cognitive function, and behavioral problems.
Only a few states (e.g., North Carolina and Illinois) do not allow individuals who meet their minimum nursing home level of care criteria to be served in residential care settings. However, virtually all states do not allow persons who need a skilled level of nursing home care to be served in residential care settings (e.g., individuals who require 24 hour-a-day skilled nursing oversight or daily skilled nursing services).
State approaches for setting admission and retention policies can be grouped into three categories:
- Full Continuum--states allow facilities to serve people with a wide range of needs;
- Discharge Triggers--states develop a list of medical needs or treatments that cannot be provided in a facility and that will result in a resident's discharge from a facility; and
- Levels of Licensure--states license facilities based on the needs of residents or the services that may be provided in a specific kind of facility.
These approaches are not mutually exclusive. States may use more than one approach and may also grant waivers for facilities to serve residents whose needs exceed those allowed. Since 2002, Arkansas, Delaware, South Carolina, South Dakota, Vermont, and Washington have modified their admission criteria.
Full Continuum
States using a full continuum approach have broad criteria that allow facilities to serve residents with a wide range of needs, permitting residents to age in place. However, providers are not required to serve everyone who meet these criteria and can establish their own admission and discharge standards within state parameters. They are required to inform prospective residents about these standards and the type of conditions that would trigger discharge. For example, Massachusetts allows providers to meet personal care needs and at a minimum must provide assistance with bathing, dressing, and ambulation. However, they are not required to offer assistance with other ADLs such as toileting and eating. Most other states allow, but do not require, residences to serve people with ADL needs.
States using the full continuum approach include Hawaii, Kansas, Maine, Minnesota, Nebraska, New Jersey, and Oregon, and those with the most flexible rules include Arizona, Hawaii, Kansas, Maine, Maryland, Minnesota, New Jersey, Oklahoma, and Oregon. Examples of this approach follow.
-
Oregon generally does not limit whom facilities may serve. The rules contain "move out" criteria that allow residents to choose to remain in their living environment despite functional decline as long as the facility can meet the resident's needs. However, facilities are not required to serve all residents whose needs increase. Providers may ask residents to move if: (1) their needs exceed the level of ADL services available; (2) the resident exhibits behaviors or actions that repeatedly interfere with the rights or well being of others; (3) the resident, due to cognitive decline, is not able to respond to verbal instructions, recognize danger, make basic care decisions, express need, or summon assistance; (4) the resident has a complex, unstable, or unpredictable medical condition; or (5) the resident has failed to make payment for charges.
-
Hawaii's rules do not specify who may be admitted and retained. Rather, each facility may use its professional judgment and the capacity and expertise of the staff to determine who it will serve. Facilities are required to develop their own admission and discharge policies and procedures. Discharge with 14 days notice is allowed based on behavior, needs that exceed the facility's ability to meet them, or a resident's established pattern of non-compliance.
-
Washington may accept and retain residents if: (1) they can meet the individual's needs, and provide required specialized training to resident-care staff; (2) the individual's health condition is stable and predictable, as determined jointly by the boarding home and the resident or the resident's representative if appropriate; and (3) the individual is ambulatory, unless the boarding home is approved by the Washington state director of fire protection to care for semi-ambulatory or non-ambulatory residents. Individuals must also meet all of the boarding home's established acceptance criteria.
-
Maine's rules are flexible to allow residents to age in place. The rules allow facilities to determine whom they will admit and the type of services they will provide. They may discharge residents who pose a direct threat to the health and safety of others, damage property, or whose continued occupancy would require modification of the essential nature of the program. Rules regarding the provision of nursing care vary by setting. Residential care facilities may provide nursing services with their own staff only to residents who do not meet the state's nursing home level of care criteria. Residents who meet the level of care criteria can be served, but nursing services must be provided by a licensed home health agency. Congregate housing programs may receive a license to provide nursing and medication administration services by registered nurses (RNs) employed by the program.
-
New Jersey's rules state that assisted living is not appropriate for people who are incapable of responding to their environment, expressing volition, interacting, or demonstrating independent activity. The rules allow facilities to provide a very high level of care, but they are not required to do so. The rules specifically state that facilities may choose to serve residents who:
- Require 24-hour, seven-day a week nursing supervision,
- Are bedridden longer than 14 days,
- Are consistently and totally dependent in four or more ADLs,
- Have cognitive decline that interferes with simple decisions,
- Require treatment of Stage III or IV pressure sores or multiple Stage II sores,
- Are a danger to self or others, or
- Have a medically unstable condition and/or special health problems.
The state also has a provision that can be characterized as a discharge trigger: facilities may not serve residents who require a respirator or mechanical ventilator or people with severe behavior management problems, such as combative, aggressive, or disruptive behaviors.
-
Vermont has two levels of licensure. One level--for assisted living--allows for a full continuum of care to be provided to residents who meet the nursing home level of care to be served if the facility can meet their needs except for the following conditions:
- A serious acute illness requiring medical, surgical, or nursing care provided by a general or special hospital;
- Ventilators;
- Respirators;
- Care of Stage III or IV ulcers;
- Suctioning; or
- Two person assistance with transfer or ambulation.
Vermont's other level of licensure--for residential care facilities--allows the provision of personal care and nursing services. Facilities may retain current residents who develop a serious, acute illness as long as the care needs are met by appropriate licensed personnel. However, if the resident wanders, the facility must document appropriate interventions to manage this behavior. Residents may be discharged if they pose a serious threat to self or other residents and are not capable of entering into a negotiated risk agreement; are ordered by a court to move; or fail to pay rent, service, or care charges.
Discharge Triggers
Discharge triggers are used by states to regulate the specific medical needs or treatments that can and cannot be provided by certain kinds of facilities and to determine when a resident can no longer reside in a facility. Most prohibited treatments require performance by skilled nursing personnel. States that use these triggers include: California, Delaware, Florida, Idaho, Illinois, Maryland, Mississippi, Nevada, New Mexico, South Carolina, Tennessee, Virginia, and West Virginia. State rules may overlap as Idaho, Maryland, and Mississippi also license by level of care, and New Jersey, which allows a full continuum of care. Examples of this approach follows.
-
Tennessee allows facilities to retain for up to 21 days (but not admit) individuals who require intravenous or daily intramuscular injections; gastronomy feedings; insertion, sterile irrigation, and replacement of catheters; sterile wound care; or treatment of extensive Stage III or IV decubitus ulcers or exfoliative dermatitis; or who, after 21 days, require four or more skilled nursing visits per week for any other condition.
-
Virginia does not allow residential care facilities to serve people who are ventilator dependent; have Stage III or IV dermal ulcers (unless a Stage III ulcer is healing); need intravenous therapy or injections directly into the vein except for intermittent care under specified conditions; have an airborne infectious disease in a communicable state; need psycho-tropic medications without an appropriate diagnosis and treatment plan; or have nasogastric tubes and gastric tubes (except when individuals are capable of independently feeding themselves and caring for the tube or by exception.)
Levels of Licensure
Several states--Arizona, Arkansas, Idaho, Maine, Maryland, Mississippi, Missouri, and Vermont--have two or more levels of licensure based on the needs of residents or the services that may be provided. Examples of this approach follow.
-
Arizona licenses three levels of care: supervisory care, personal care, and directed care. Residential care facilities providing supervisory care may serve residents who need health or health-related services if these services are provided by a licensed home health or hospice agency. Those with a personal care service license may not accept or retain any resident who is unable to direct self-care; requires continuous nursing services unless the nursing services are provided by a licensed hospice agency or a private duty nurse; has a Stage III or IV pressure sore; or is bed bound due to a short illness unless the primary care physician approves, the resident signs a statement and the resident is under the care of a nurse, a licensed home health agency, or a licensed hospice agency. Facilities licensed to provide directed care may serve residents who are bed bound, need continuous nursing services, or have a Stage III or IV pressure sore.
-
Arkansas licenses two levels of facilities. Level I facilities cannot serve nursing home eligible residents or residents who need 24-hour nursing services; are bedridden; have transfer assistance needs that the facility cannot meet; present a danger to self or others; and require medication administration performed by the facility.
Level II assisted living facilities can serve nursing home eligible residents and participate in a Medicaid HCBS waiver, but cannot serve residents who need 24-hour nursing services; are bedridden; have a temporary (no more than 14 consecutive days) or terminal condition unless a physician or advance practice nurse certifies the resident's needs may be safely met; have transfer assistance needs, including but not limited to assistance to evacuate the facility in case of emergency, that the facility cannot meet with current staffing; present a danger to self or others; or engage in criminal activities. Facilities may be licensed for both levels of care in distinct parts or separate wings but separate licenses are required for the beds providing each level.
-
Florida licenses four types of facilities: basic assisted living facilities, limited nursing services, limited mental health services, and extended congregate care (ECC) which is the highest level of care. ECC facilities serve residents with higher needs and provide more services than the other levels including total help with bathing; nursing assessment more frequently than monthly; measurement and recording of basic vital functions; dietary management; supervision of residents with dementia; health education and counseling; assistance with self-administration and administration of medications; provide or arrange rehabilitative services and escort services to health appointments.
-
Utah licenses two levels of facilities. Type I facilities serve residents who are ambulatory, have stable health conditions, require limited assistance with ADLs and need regular or intermittent care or treatment from facility staff. Type II facilities serve residents who need substantial assistance with ADLs, offer separate living units, and enable residents to age in place as much as possible. Level II residents may be independent or semi-independent but not dependent (needing in-patient or 24-hour continual nursing care for more than 15 days, or needing a two-person assist to evacuate the building). Both types of facilities may assist with or administer medications under supervision of a licensed nurse.
Nursing Home Level of Care Issues
States typically have two or more levels of nursing home care and not all persons served in nursing homes may be served in residential care. States distinguish among levels of care primarily for payment purposes. As noted in the discussion of admission and retention policies, above, states typically do not allow facilities to serve persons who require a skilled level of nursing care (as opposed to discrete skilled services, which many states allow in residential care on a limited basis). Only a few states do not allow facilities to serve persons who do not meet the minimum or threshold nursing home level of care criteria.
Generally, it is individuals who meet a state's minimum level of care criteria who can be and are served in residential care settings and states' minimum nursing home criteria vary markedly. Individuals who meet the nursing home criteria in one state may not meet the criteria in another state. Thus, the statement that most states permit residential care settings to serve individuals who are "nursing home eligible" obscures sometimes significant differences in the type and level of care provided in these facilities in different states.
States fall on a continuum from low to high thresholds for nursing home admission. Some states require a person to need assistance with only two ADLs, while others may require that a person be totally dependent in three or more ADLs. Some states require individuals to have a combination of medical conditions/needs and functional limitations; others require only certain medical needs. Of the 45 states whose criteria were reviewed for this study, two used medical criteria only; 13 used medical and functional needs; eight used an assessment score based on a combination of medical and functional needs; and 22 used ADL thresholds. 3 provides information about each state's nursing home level-of-care criteria.13 A few examples of states' criteria follow.
-
Medical. Alabama requires an individual to need daily nursing or medical services that as a practical matter can only be provided in a nursing facility on an in-patient basis.
-
Medical and/or functional. Maine requires individuals to need skilled care on a daily basis (nursing or rehabilitation therapies); or extensive assistance with three of the following ADLs (bed mobility, transfer, locomotion, eating, and toileting); or one of several specified combinations of nursing and functional needs.
-
ADL Threshold. New Hampshire requires individuals to either need assistance with two or more ADLs, or to need 24-hour care for at least one of the following: medical monitoring and nursing care; restorative nursing or rehabilitative care; or medication administration.
-
Combination of Factors. Illinois requires individuals to have a specific score on a standardized assessment. The score is derived using a score on the Mini-Mental State Examination (MMSE), and impairments in six ADLs and nine instrumental activities of daily living (IADLs) (including ability to perform routine health and special health tasks, and ability to recognize and respond to danger when left alone).
Because Centers for Medicare and Medicaid Services (CMS) gives states considerable flexibility in setting minimum nursing home level of care criteria, states may choose to make this criteria more stringent in response to budget deficits, as Oregon has recently done. In states that cover Medicaid waiver services in residential care settings, increasing the threshold level of care criteria for nursing homes will also increase the threshold for residential care. For example if a state raises its threshold criteria from 2 out of 5 ADL impairments to 3 out of 5 ADL impairments, a person in the former category will no longer be eligible for Medicaid coverage in both nursing homes and residential care settings.
If a state markedly increases the stringency of its minimum nursing home level of care criteria to control nursing home admissions, it would need to ensure that admission and retention criteria for residential care settings allow these settings to continue serving Medicaid waiver clients with the higher level of need required for Medicaid nursing home admission.
Services
One of the attractive philosophical tenets of assisted living is that it allows aging-in-place--meaning that as individuals age and become more disabled, additional services can be provided so that they will not have to move to another residential care setting or to a nursing home.
States seeking to facilitate aging-in-place and to offer consumers a full range of long-term care options allow more extensive services to be provided in residential care facilities, just as they can be provided in an individual's home through home health agencies and in-home service programs.
However, facilities vary in the extent to which aging-in-place is possible, because states generally specify the range of allowable services and a minimum that must be provided, but do not require facilities to provide the full range of allowable services. Facilities are usually authorized to determine which services they will provide within state parameters. Facilities may offer very limited, moderate, or extensive services. Thus, both state regulations and facility policy govern the type, amount, frequency and duration of services provided, and, hence, the ability to age in place.
Thus, although state regulations frequently state their support for aging-in-place, they may also allow facilities to discharge individuals with higher levels of need. A key determinant of the ability to age in place is the extent to which states permit residential care facilities to address residents' nursing and health related needs.
Some experts contend that residential care settings cannot and should not be expected to meet the needs of persons with a high level of disability and/or medically complex conditions. Others agree, arguing that residential care should be a social care model and having nurses on staff is not only unnecessary but undesirable. However, other regulators, particularly in states that allow nurses to delegate specified nursing tasks, believe that residential care settings, like a person's own home or apartment, are appropriate settings for people with severe disabilities and/or health needs. But some observers have expressed concern about direct care staff's ability to recognize and address health problems in medically fragile residents when they are not trained nursing assistants. Many states do allow residential care facilities to provide skilled nursing care, as indicated in the following examples.
-
Illinois allows health services such as medication administration, dressing changes, catheter care, and therapies, if provided on an intermittent basis.
-
Florida allows the provision of nursing services under two types of licensure: limited nursing services and extended congregate care. A license for limited nursing services allows facilities to provide nursing services including medication administration and supervision of self-administration, heat and ice cap application, passive range of motion exercises, urine tests, routine dressing changes that do not require packing or irrigation, and intermittent nursing services (e.g., change of colostomy bag and related care, catheter care, administration of oxygen, routine care of an amputation or fracture, prophylactic, and palliative skin care). A license for extended congregate care permits a facility to provide nursing services in addition to those provided under the limited nursing services license.
However, the state specifies nursing services that may not be provided under either type of license, including oral or nasopharyngeal suctioning, assistance with tube feeding, monitoring of blood gasses, intensive rehabilitation services for a stroke or fracture or treatment of surgical incisions that are not clean and infection-free, and any treatment requiring 24-hour nursing supervision.
-
Washington's regulations specify which skilled services may and may not be delivered by licensed nurses and unlicensed staff in residential care settings. RNs or licensed practical nurses (LPNs) may insert catheters, provide nursing assessments, and glucometer readings. Unlicensed staff under the supervision of a licensed nurse may provide Stage I skin care, routine ostomy care, enemas, catheter care, and wound care. Statutory changes in the nurse practice act that would allow greater delegation are pending in the legislature.
-
New Jersey allows levels of skilled nursing care that are specifically barred in many states; for example, care of Stage III or IV pressure sores, ostomy care, and 24-hour nursing supervision.
-
Missouri's rules governing residential care facilities allow advanced personal care services to be provided. They include providing services to residents with a catheter or ostomy, those who require bowel or bladder routines, range of motion exercises, assistance applying prescriptions or ointments and other tasks requiring a highly trained aide.
-
Maine allows residential care facilities and congregate housing programs to provide skilled nursing services.
Several states limit the provision of skilled nursing services in residential care settings by restricting their frequency and duration. Others prohibit facilities from providing these services directly, but allows them--and/or residents--to arrange for their provision through a home health agency. Some states use a combination of approaches, all of which are illustrated in the following examples.
-
Massachusetts like many states, does not allow residential care facilities to serve residents who need 24-hour nursing services. Skilled services may only be provided by a certified home health agency on a part-time or intermittent basis to persons whose medical conditions require services on a periodic, scheduled basis. In addition, the state allows residents "engage or contract with any licensed health care professional and providers to obtain necessary health care services … to the same extent available to persons residing in private homes.
Because the Massachusetts statute allows skilled nursing services to be provided only by a certified home health agency, RNs hired by an assisted living facility are not allowed to deliver skilled care. An initial draft of new state regulations did not allow the provision of skilled services for more than 90 days in a 1-year period. When the state attorney general's office determined that such limits may conflict with fair housing rules, the state removed the 90-day limit.
-
Ohio limits the provision of skilled services in residential care facilities to 120 days in a 12 month period with exceptions for special diets, dressing changes, and medication administration.
-
Iowa allows facilities to provide health related care (i.e., services provided by a RN, a LPN, or home care aide; and services provided by other licensed professionals as defined in regulations). Health-related and personal care services can be provided on an intermittent and part-time basis, which is defined as up to 35 hours a week of personal care and health-related services on a less than daily basis, or up to eight hours personal care and health related services provided seven days a week for temporary periods not exceeding 21 days.
-
Kentucky allows residents to arrange for additional services under direct contract or arrangement with an outside agent, professional, provider, or other individual designated by the client if permitted by facility policy.
Quality Assurance and Monitoring
In 2003 and 2004, hearings held by the U.S. Senate Special Committee on Aging, reports by the GAO, and newspaper articles all raised concerns about the quality of care in residential care settings, and the challenges providers and state oversight agencies face in assuring quality. In April 2004, the GAO issued a report on quality assurance initiatives in Florida, Georgia, Massachusetts, Texas, and Washington.14
The report stated that assisted living facilities are more likely to meet and maintain licensing standards if they can obtain help in interpreting those standards and in determining what concrete changes they need to make to satisfy them. It described an initiative in Washington, which established a staff of quality consultants to provide such training and advice to assisted living providers on a voluntary basis. Evaluations at 6 months and 2 years after implementation documented improvements in provider compliance as well as resident health and safety. However, a statewide budget crisis required the state to end funding for the program in order to maintain traditional licensing enforcement functions.
Wisconsin and Kansas have recently initiated activities to better assure quality. The Wisconsin Bureau of Quality Assurance created an Assisted Living Forum for stakeholders to discuss current issues, interpretation of regulations, best practices, quality improvement, staffing issues, national and state trends, and other public policy issues.
Wisconsin has also revised its survey process for residential care apartment complexes, its apartment model of assisted living, which is not licensed but has to be either registered, or certified to serve Medicaid clients. The new process includes a technical assistance component to interpret requirements, provide guidance to staff on consumer quality of life and care; review provider systems, processes and policies; and explain new or innovative programs. The revised survey strategy includes seven types of surveys: initial, standard, abbreviated, complaint, verification, monitoring and self-report. The state determines which type of survey to conduct for each facility based on a range of factors, including its citation history. Abbreviated surveys are performed for facilities without any enforcement actions over the past 3 years and no substantial complaints or deficiency citations.
Kansas has adopted a collaborative oversight approach. Facility staff accompany the surveyor during the review. Observations are discussed during the process and, when necessary, problem areas are reviewed in the context of the regulatory requirements. Deficiency statements focus on consumer outcomes. The licensing director also conducts a full day training course several times a year on the role of licensed nursing in assisted living facilities for nurses, operators and owners. The training covers use of the assessment, developing a services plan, managing medications and the nurse practice act. The state believes that the combination of regular visits, consistent application of the regulations, and a more collaborative oversight process and training have resulted in better compliance with the regulations and fewer complaints.
Several states reported organizing periodic trainings for facility staff or including articles in a newsletter about specific problems that surveyors find are occurring in a number of facilities. Others cited a conflict between oversight and consultation functions. One state indicated that facilities are responsible for resolving quality problems and the state provides consultants to assist them to do so. Other states clarify rules or statutes with facility staff during the survey or during exit interviews after the survey is completed. If the facility is able to correct the problem during the survey, no deficiency is issued. Utah allows new administrators to request assistance, and has procedures for the licensing agency to review survey forms with administrators, as well as previous reports and deficiencies. Pennsylvania provides guidance by disseminating information about best practices.
A few states indicated that they could not provide consultation and technical assistance due to staff shortages and the need to complete surveys.
In 2002, NASHP conducted a survey of licensing officials in all the states and asked them to rank ten areas by the frequency of deficiencies and complaints. Thirty-four states ranked the areas in the following order:
- Medications (48 percent indicated that problems occurred frequently or very often)
- Problems with staff quality and qualifications (41 percent indicated that problems occurred frequently or very often)
- Sufficient staff (36 percent)
- Records (32 percent)
- Care plans (24 percent)
- Inadequate care (21 percent)
- Admission/discharge (15 percent)
- Access to medical care (3 percent)
- Abuse (3 percent)
- Billing/charges (3 percent)
Fifty-eight percent of the states indicated that their penalty trends remained about the same in 2001 compared to 1999-2000; 34 percent reported that the number of penalties increased and 8 percent reported that they had declined. Eighty percent of the states felt their monitoring and enforcement systems were effective or very effective. The survey asked states to describe aspects of their process that were working well. A number of states identified the process of making follow-up visits when survey findings/complaints indicated areas of concern. Several states noted that having a range of remedies available to act on survey findings was effective as well as making unannounced visits. Progressive enforcement based on the facility's history and response was also cited as an effective strategy.
One state indicated that counties are involved in monitoring Medicaid waiver participants and that service negotiations helped clarify service contracts. Another said that using state nurse consultants and specialty staff, such as pharmacists and dieticians, to monitor facilities with serious or numerous problems was effective.
Other quality assurance strategies cited include providing technical assistance and follow-up; acting within 10 days on complaints; having clear lines of communication for and definition of duties for survey staff; developing clear enforcement procedures that are well understood by staff; meeting with providers to discuss issues; providing training; conducting follow-up visits; and maintaining a consumer perspective that focuses on improving care not just punishing past failures. States described a number of quality initiatives underway including:
- Furnishing provider training;
- Implementing new training requirements for medication aides;
- Revising the survey process;
- Developing a more formalized consultation program;
- Providing more technical assistance;
- Conducting forums for providers to discuss quality issues; and
- Implementing quality assurance and quality improvement regulations.
Other strategies focused on revising standards for assessment, training, and level of care, including:
- Working with providers to develop minimal standards for assessments, service plans, negotiated risk agreements, and disclosure requirements;
- Adding disclosure requirements for dementia care providers;
- Increasing the licensing authority for staffing, training, disclosure, and Alzheimer's care;
- Working to increase staff training requirements;
- Working to establish specific staffing requirements for special care units;
- Conducting regulatory reviews to bring provisions up to national standards; and
- Increasing requirements for a comprehensive resident assessment.
Over half the states reported that the number of staff available for survey and monitoring was not keeping pace with the growth in the supply of facilities.
Medication Administration
As facilities are allowed to serve residents with greater needs, regulators have cited medication administration and assistance with self-medication as a major concern. A study cited in a literature review on medication use in assisted living found that residents were prescribed an average of 4.6 medications per month; 37 percent took four to seven medications a month; and 11 percent took eight or more.15 Comparing prescriptions to the "Beers List," the study found that 25 percent of the residents had inappropriate medication orders.16 Another study found that 11 percent of residents were taking two or more psychotropic medications and 70 percent were taking psychotropic agents without receiving mental health services. The literature review found that there was substantial use of medications considered inappropriate for use by elders; widespread use of psychotropic medications; under-treatment of depression; and use of medications with undocumented diagnosis or reason for use.
States were asked to indicate how often problems with medications were reported or identified during survey activity. Eighty-two percent of the responding states said the incidence of medication problems has remained the same since 2002, 12 percent reported a decline in medication problems, and 6 percent report an increase in problems with medications. However, while most states reported that the incidence of medication problems remained the same as in 2002, the number of states reporting that problems occurred frequently or very often rose significantly. For example, 61 percent of the 46 states and the District of Columbia reported that problems with medications occurred frequently or very often (up from 51 percent in 2002). Twenty-three percent responded that this was a problem sometimes, and 18 percent responded rarely or occasionally.17 Other reported problem areas included pharmacy and physician medication errors.
Several states noted that its licensing agency is paying more attention to medication issues as the acuity level increases and more residents are taking increasing numbers of medications. States that did not previously track the prevalence of medication issues are now doing so.
The 2002 study asked whether states allowed trained aides to administer medications or to assist with self-administration of medications. Of the responding states, 98 percent allow trained aides to assist with self-administration, and 63 percent allow aides who have completed and passed a training program to administer medications. Thirteen percent of responding states require facilities to have a consulting pharmacist. Several states require record reviews of medications by a RN.
States are addressing problems with medication administration by offering additional training, enacting changes to nurse delegation provisions, and tracking medication issues on survey reports. A few states indicated that problems with medication administration are consistently among the top eight or ten deficiencies and a few reported it was the most frequently cited deficiency. On the other hand, states reported that deficiencies and problems dropped after the licensing agency offered more training on medication administration to administrators, supervisory and direct care staff.
Training Requirements
Staff training requirements are a key component of quality assurance. A national study found that the types of required staff training and orientation varied across facilities, but for the most part, relatively little training was required.18 Three-quarters of unlicensed personnel were required to attend some type of pre-service training or orientation, most commonly lasting between 1 and 16 hours. Only 11 percent of the staff who received required training completed it prior to the start of work; the remainder received on-the-job training or a combination of pre-service and on-the-job training. In contrast, nursing homes aides are required to have a minimum of 75 hours of training (10 days) and to pass an exam before they can work on a unit providing direct resident care.
Staff reported receiving training on--or an orientation to the philosophy of assisted living and how that philosophy differs from traditional nursing home care and other residential care settings. However, the study found the staff were not well informed about normal aging and care for persons with dementia.
States regulations specify initial and ongoing training requirements for staff and administrators but the level of specificity in the training requirements varies considerably. Some states specify only general requirements, while others specify topics to be covered, the number of training hours required, the completion of approved courses, or some combination thereof.
National Activities
At the national level, stakeholders involved in the ALW implemented its recommendation to establish a Center for Excellence in Assisted Living (CEAL).19 The CEAL's mission is to "foster access to high quality assisted living by creating resources and acting as an objective resource center to facilitate quality improvement in assisted living; increasing the availability of research on quality in assisted living; providing a national clearinghouse for information on assisted living; building upon the work of the Assisted Living Workgroup; promoting availability of and innovation for high quality affordable assisted living; and providing information, tools, and technical expertise to facilitate the development and operations of high quality affordable assisted living programs to serve low and moderate-income individuals."
The CEAL will provide reports on quality using objective measures and data, disseminate information, promote research, identify and describe effective practices and provide technical assistance to states on policy, programs, effective practices, the integration of outcome measures, and the ALW recommendations into state policies and programs.
Lack of Information About Residential Care Facilities for Consumers
The 2004 GAO report cited earlier found that consumers faced with choosing an assisted living facility often do not have key information they need in order to identify the one most likely to meet their individual needs. Such information includes staffing levels and qualifications, costs and potential cost increases, and the circumstances that could lead to involuntary discharge from the facility.
The report described initiatives in Florida and Texas that have made critical data to aid consumer selection more readily available. Florida created a Web site that provides information about facilities by geographic area and identifies those providing the services the consumers are seeking at a specified price range. Texas has mandated a standardized disclosure statement for assisted living facilities, giving consumers concise and consistent data that facilitates comparisons across providers regarding services, charges, and policies.
Many states help consumers compare assisted living facilities by publishing brochures, consumer guides, and by providing information on Web sites. The following list offer examples of Web sites that have been developed by states, provider associations, and consumer groups. Many other states have Web sites, which the reader can find by conducting standard searches.
-
State Web sites
- Colorado--http://www.cdphe.state.co.us/hf/broch/assist.htm. The state's Web site for its licensing agency--www.cdphe.state.co.us/hf/static/pcbhpp.htm--lists each facility with links to survey findings and complaints. The site has other consumer information such as a brochure for solving problems and a checklist for selecting facilities.
- Florida--http://www.floridaaffordableassistedliving.org/
- New Jersey--http://www.state.nj.us/health/ltc/alinnj
- Oregon--http://www.dhs.state.or.us/seniors/publications/oregon_consumer_guide.p…
- Washington--http://www.aasa.dshs.wa.gov/Library/publications/htmlversions/CARE%20IN…
- Wisconsin--http://dhfs.wisconsin.gov/guide/find/asstliving.htm
-
National and State Association Web sites
- Assisted Living Federation of America--http://www.alfa.org/public/articles/index.cfm?cat=6
- American Association of Homes and Services for the Aging--http://www2.aahsa.org/
- National Center for Assisted Living--http://www.ncal.org/consumer/consumer.htm
- MassALFA--http://www.massalfa.org/docs/assist.htm
- NorALFA--http://www.noralfa.org/tips.cfm
-
National Consumer Groups Web sites
- Consumer Consortium for Assisted Living--http://www.ccal.org/
- AARP--http://www.aarp.org/life/housingchoices/Articles/a2004-02-27-assistedli…
- National Cooperative Bank Development Corporation--http://www.ncbdc.org
Provisions for Residents with Alzheimer's Disease and Dementia
Forty-four states have specific regulatory provisions for facilities serving people with Alzheimer's disease and other dementias, an increase from 36 in 2002 and 28 in 2000. Examples of state activities regarding dementia care and the regulations for facilities serving residents with dementia follow.
-
Rhode Island requires a license for dementia care when one or more resident's dementia symptoms affect their ability to function as demonstrated by behaviors that adversely impact the rights of others; elopement; or an inability to self-preserve. Facilities that advertise or represent special dementia services or that segregates residents with dementia also need a license for dementia care. In addition to basic license requirements dementia care licenses require staff training specific to dementia care; a RN on staff and available for consultation at all times; and a secure environment appropriate for the resident population.
-
Pennsylvania has drafted rules that contain provisions for securing units and providing adequate indoor and outdoor wandering space. They also specify competency-based training requirements for administrators and staff covering mandated topics such as the definition and diagnosis of dementia, differences between dementia, delirium, and depression, managing behavioral symptoms, and working with family members.
-
Montana created a new licensure category for facilities that serve residents who are not capable of expressing their needs or making basic decisions. Requirements include staffing provisions; general staff education, training, and experience requirements; dementia specific annual continuing education requirement, including the teaching of skills necessary to care for, intervene and direct residents who are unable to perform ADLs; and techniques for minimizing challenging behavior. Other requirements apply to locked units or distinct parts of facilities.
-
Washington revised its regulations to require staff with experience and training in dementia care to coordinate outside services, offer monthly educational and family support meetings, and advocate for residents. Staff training requirements include a minimum of 30 hours on care for residents with dementia; nature, stages, and treatment of the disease; therapeutic interventions; communication techniques; medication management; therapeutic environmental modifications; assessment and care planning; the role of family and their need for support; staff burn-out prevention; and abuse prevention. Eight hours of continuing training is required annually.
Staff must be able to provide 2.25 hours of direct care per resident per day. At least two staff must be present for units serving more than five residents. An RN must be available if residents require nursing procedures. The rules describe special requirements for the physical environment with security measures, including secured outdoor spaces.
Licensed facilities that do not market themselves special care units but serve residents with early symptoms of dementia must provide staff training on dementia care, including strategies to help residents manage their behaviors.
Disclosure
Twenty-four states have disclosure requirements for facilities that advertise themselves as operating special care facilities or units, or that care for people with Alzheimer's disease or other dementias. These facilities are required to describe in writing how they are different from other facilities. The regulations may require a description of the philosophy of care, admission/discharge criteria, the process for arranging a discharge, services covered and the cost of care, special activities that are available, and differences in the environment. See Table 1-5 for an overview of disclosure requirements. Specific examples of regulations regarding disclosure requirements follow.
-
California has a voluntary disclosure process for facilities offering special services for people with dementia. The state developed a consumer's guide that alerts family members to key questions that should be asked when seeking residential care for people with dementia. They include how the program meets the needs of people with Alzheimer's; the facility's pre-admission assessment process; the transition from the individual's current living arrangement to residential care; the care and activities that will be provided; staffing patterns and the special training received by staff.
-
Illinois' standard disclosure form, which all providers must use, addresses the form of care or treatment; philosophy; admission and retention policies; assessment care planning and implementation guidelines; staffing ratios; physical environment; activities; family members' roles; and the cost of care.
-
Minnesota adopted disclosure requirements in 2001, which require facilities to provide information about the form of care or treatment; the treatment philosophy; unique features for screening, admission and discharge; assessment and care planning; staffing patterns; the physical environment; security features; type and frequency of activities; opportunities for family involvement; and the costs of care.
-
Texas requires a disclosure statement that describes the nature of the care or treatment provided the pre-admission and admission processes, discharge and transfer policies, the planning and implementation of care, policies related changes in residents' condition, staff training on dementia care, the physical environment, and staffing.
Staffing and Training
Thirty-six states have requirements for dementia specific training and staffing for facilities serving people with Alzheimer's disease and other dementias. Examples follow.
-
In Alabama, staff in specialty care facilities must complete a training program developed by the Department of Mental Health and Mental Retardation and receive six hours of ongoing training a year on topics specified in the regulations.
-
Arizona requires staffing ratios of one staff per six residents during the morning and evening, and one per twelve residents at night.
-
Indiana requires six hours of training for direct service workers within 6 months of employment and three hours annually.
-
Rhode Island requires new direct service workers to receive at least twelve hours of orientation and training about dementia, communicating effectively with dementia residents, and managing problem behaviors. The state also requires that a RN be available to residents on site as needed, and available for consultation at all times.
-
Massachusetts, Nevada, and Oklahoma require 24-hour coverage by awake staff.
| TABLE 1-5. Comparison of Disclosure Requirements | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Topics Required | AR | CA | CO | DE | FL | GA | ID | IL | KY | MD | ME | MI | MN | MO |
| Philosophy | X | X | X | X | X | X | X | X | X | X | ||||
| Services | X | X | X | X | X | X | ||||||||
| Cost | X | X | X | X | X | |||||||||
| Population served | X | X | X | X | ||||||||||
| Admission and discharge process | X | X | X | X | X | X | X | X | X | X | ||||
| Assessment and care planning process | X | X | X | X | X | X | X | X | ||||||
| Staffing | X | X | X | X | X | X | X | X | X | X | X | |||
| Training | X | X | X | X | X | X | X | X | X | X | ||||
| Physical environment | X | X | X | X | X | X | X | X | X | |||||
| Resident activities | X | X | X | X | X | X | X | |||||||
| Family role | X | X | X | X | X | X | X | |||||||
| Psychosocial services | X | |||||||||||||
| Nutrition | X | |||||||||||||
| Form of care | X | X | ||||||||||||
| Security features | X | X | ||||||||||||
| Other | X | X | ||||||||||||
| Topics Required | MT | NH | NJ | NC | OH | OK | OR | PA | RI | SC | TX | VT | WA | WV |
| Philosophy | X | X | X | X | X | X | X | X | ||||||
| Services | X | X | X | X | ||||||||||
| Cost | X | X | X | X | X | X | X | X | X | |||||
| Population served | X | |||||||||||||
| Admission and discharge process | X | X | X | X | X | X | X | X | X | |||||
| Assessment and care planning process | X | X | X | X | X | X | X | X | X | |||||
| Staffing | X | X | X | X | X | X | X | X | X | |||||
| Training | X | X | X | X | X | X | X | X | ||||||
| Physical environment | X | X | X | X | X | X | X | |||||||
| Resident activities | X | X | X | X | X | X | ||||||||
| Family role | X | X | X | X | X | |||||||||
| Psychosocial services | X | |||||||||||||
| Nutrition | ||||||||||||||
| Form of care | X | X | X | X | X | |||||||||
| Security features | ||||||||||||||
| Other | X | X | X | X | X | |||||||||
Public Financing
Medicaid Financing for Services in Residential Care Settings
Medicaid is a significant payer of long-term care services, comprising about 64 percent of all nursing home care expenditures and 33 percent of Medicaid spending overall (see Table 1-6). States are steadily shifting the balance of long-term care spending from institutional to home and community settings. Although Medicaid spending for institutional care in nursing homes and intermediate care facilities for persons with mental retardation (ICFs-MR) rose from $35.4 billion in 1993 to $56.1 billion. In 2003, spending for home and community services (state plan personal care, home health, and HCBS waivers) grew from $6.7 billion to $27.8 billion during the same time period.20 Consequently, Medicaid spending for institutional care dropped from 86 percent of all Medicaid long-term care spending in 1991 to 67 percent in 2003.
| Service | 1993 | 2003 |
|---|---|---|
| Home Health | $1.4 | $2.9 |
| Personal Care State Plan | $2.5 | $6.3 |
| HCBS Waiver | $2.8 | $18.6 |
| ICF-MR | $9.3 | $11.3 |
| Nursing Home | $26.1 | $44.8 |
| Total Long-Term Care | $42.1 | $83.8 |
| Total Medicaid | $126.4 | $259.6 |
Much of the growth in HCBS spending has been for services for persons with mental retardation and other developmental disabilities, which account for 75 percent of all spending.21
The expansion of home care programs, home health services, and residential care options has afforded persons with long-term care needs a number of alternatives to nursing homes. People with fewer ADL impairments are less likely to enter a nursing home.22 Thus, while the absolute number of nursing home beds increased from 1.8 million in 1985 to 1.9 million in 1999, the rate per thousand persons over age 75 declined from 141 beds to 117 beds, and nursing home occupancy rates dropped from 92.3 percent in 1987 to 87.0 percent in 1996,23 and further declined to 85.6 percent in December 2003.24 See Table 1-7 for occupancy rates in each state.
Declining nursing home occupancy rates create some concerns for states. First, as higher income elders choose assisted living, the proportion of nursing home residents who are Medicaid beneficiaries increases. Increased reliance on Medicaid creates pressure to raise payment rates to replace revenue formerly received from private pay residents. Second, excess capacity creates a greater likelihood that Medicaid nursing home expenditures will rise if Medicaid beneficiaries do not have access to sufficient home and community services, and must rely to nursing homes at greater expense to the states.
| State | NF Supply/ 1000 65+ |
Occupancy Rate |
Residential Care Supply/ 1000 65+ |
State | NF Supply/ 1000 65+ |
Occupancy Rate |
Residential Care Supply/ 1000 65+ |
|---|---|---|---|---|---|---|---|
| US | 50.0 | 85.6 | US | 50.0 | 85.6 | ||
| AL | 44.8 | 90.0 | 16.8 | MT | 60.9 | 77.0 | 30.4 |
| AK | 20.6 | 83.9 | 12.3 | NE | 70.5 | 86.7 | 39.4 |
| AZ | 23.4 | 82.7 | 34.9 | NV | 21.6 | 83.6 | 16.7 |
| AR | 78.6 | 73.3 | 21.3 | NH | 51.0 | 92.4 | 26.3 |
| CA | 35.8 | 85.5 | 41.7 | NJ | 45.1 | 87.8 | 14.3 |
| CO | 46.3 | 81.9 | 31.7 | NM | 33.6 | 85.4 | n.a. |
| CT | 66.1 | 93.4 | 7.9 | NY | 49.6 | 92.7 | 17.6 |
| DC | 45.4 | 91.8 | 2.7 | NC | 43.1 | 89.0 | 17.6 |
| DE | 44.4 | 91.0 | 16.5 | ND | 69.4 | 93.5 | 30.3 |
| FL | 28.9 | 88.0 | 26.2 | OH | 79.3 | 86.0 | 27.7 |
| GA | 49.1 | 90.9 | 31.3 | OK | 71.1 | 67.3 | 21.0 |
| HI | 22.4 | 95.0 | 23.3 | OR | 28.8 | 67.8 | 47.5 |
| IA | 93.2 | 83.2 | 12.1 | PA | 47.6 | 89.9 | 40.0 |
| ID | 41.4 | 76.0 | 40.8 | TN | 52.8 | 92.0 | 19.3 |
| IL | 71.0 | 80.1 | 9.7 | SC | 36.4 | 91.8 | 33.1 |
| IN | 72.9 | 83.2 | 15.5 | SD | 68.0 | 92.4 | 31.0 |
| KS | 76.2 | 85.7 | 22.4 | TN | 52.8 | 89.3 | 19.3 |
| KY | 50.3 | 91.1 | 14.5 | TX | 56.4 | 77.5 | 19.6 |
| LA | 73.1 | 77.2 | 9.6 | UT | 37.4 | 72.7 | 22.5 |
| MA | 60.2 | 91.2 | 12.3 | VA | 38.5 | 89.9 | 42.3 |
| MD | 47.7 | 86.1 | 27.8 | VT | 44.5 | 92.4 | 30.4 |
| ME | 40.8 | 93.0 | 48.4 | WA | 35.0 | 85.7 | 36.2 |
| MI | 39.9 | 87.2 | 38.6 | WI | 60.2 | 86.6 | 38.9 |
| MN | 65.2 | 92.5 | n.a. | WV | 40.7 | 89.9 | 11.9 |
| MO | 71.9 | 75.7 | 28.8 | WY | 51.7 | 80.8 | 21.7 |
| MS | 52.4 | 88.6 | 14.2 | ||||
| SOURCES: Population Division, U.S. Census Bureau. Annual Estimates of the Resident Population by Selected Age Groups for the United States and States: July 1, 2003. American Health Care Association: December 2003. The supply of residential care settings was calculated by NASHP using Census data and data reported by state licensing agencies. (n.a.--not available) | |||||||
State officials thus have an interest in ensuring that the supply of nursing facilities declines as the supply of home and community services expand. The 1999 U.S. Supreme Court Olmstead decision gives further impetus for shifting spending from institutions to home and community settings. That decision, and guidance to states from CMS, requires that states have plans for serving people with disabilities in the most integrated setting. Additionally, the ruling states that if states have a waiting list for services, the list must move at a "reasonable pace."
While some areas of the country, particularly rural areas, have an inadequate supply of residential care facilities, in other areas, developers have over-built facilities. As nursing homes compete with assisted living facilities for market share, these facilities are competing among themselves for residents. Low occupancy rates in assisted living facilities may lead to greater interest in serving low-income beneficiaries, thereby increasing the availability of this service option for Medicaid beneficiaries.
Medicaid Coverage Options
States have several options for using Medicaid to fund services in residential care settings (see Table 1-8): the Medicaid state plan, HCBS waivers (also called 1915(c) waivers), Section 1115 demonstration programs, and 1915(b) managed care initiatives. States most often use the HCBS waiver. See Table 1-9 for the sources of funding each state uses to pay for services in residential care settings.
- 36 states have CMS approval to cover services under a 1915(c) waiver;
- 14 states use the Medicaid state plan;
- 10 states use solely state-funded long-term care programs;
- 8 states use both Medicaid waivers and the state plan;
- 3 states use all three sources;
- Arizona uses a managed care program authority under an 1115 waiver; and
- Utah uses a 1915(a) state plan amendment managed care authority.
| Waiver (29) | Personal Care (6) | Waiver & Personal Care (8) | |
|---|---|---|---|
| Alabama* Alaska Arizona Colorado Connecticut Delaware District of Columbia* Georgia Hawaii Illinois Indiana Iowa Kansas Maryland Mississippi |
Montana Nebraska Nevada New Hampshire New Jersey New Mexico Oregon Pennsylvania Rhode Island South Dakota Texas Washington West Virginia Wyoming |
Massachusetts Missouri New York North Carolina South Carolina Utah |
Arkansas Florida Idaho Maine Michigan Minnesota Vermont Wisconsin |
| * Alabama and the District of Columbia have not yet implemented approved 1915(c) waivers. | |||
Congress authorized HCBS waivers in 1981 under Section 1915(c) of the Social Security Act. Under this provision, states may apply to the U.S. Department of Health and Human Services for a waiver of certain federal requirements to allow states to provide home and community services to individuals who would otherwise require services in an institution.
Under the HCBS waiver authority, states can provide services that are not covered by a state's Medicaid program, such as personal care not covered by the state plan, home delivered meals, adult day care, personal emergency response systems, respite care, environmental accessibility adaptations, and other services that are required to keep a person from being institutionalized. The waiver authority also allows states to provide waiver participants a greater amount, duration, and scope of services than are provided under the state plan.
| State | Source of Funding | State | Source of Funding | ||||
|---|---|---|---|---|---|---|---|
| Medicaid Waiver |
Medicaid State Plan |
State Funds |
Medicaid Waiver |
Medicaid State Plan |
State Funds |
||
| Alabama | 1915 (c) | Missouri | X | ||||
| Alaska | 1915 (c) | Montana | 1915 (c) | ||||
| Arizona | 1115 | Nebraska | 1915 (c) | ||||
| Arkansas | 1915 (c) | X | Nevada | 1915 (c) | |||
| California | Planned | New Hampshire | 1915 (c) | ||||
| Colorado | 1915 (c) | X | New Jersey | 1915 (c) | |||
| Connecticut | 1915 (c) | X | New Mexico | 1915 (c) | |||
| Delaware | 1915 (c) | New York | X | ||||
| District of Columbia | 1915 (c) | North Carolina | X | ||||
| Florida | 1915 (c) | X | North Dakota | 1915 (c) | |||
| Georgia | 1915 (c) | Oregon | 1915 (c) | ||||
| Hawaii | 1915 (c) | X | Pennsylvania | 1915 (c) | |||
| Idaho | 1915 (c) | X | X | Rhode Island | 1915 (c) | ||
| Illinois | 1915 (c) | South Carolina | X | ||||
| Indiana | 1915 (c) | X | South Dakota | 1915 (c) | X | ||
| Iowa | 1915 (c) | Texas | 1915 (c) | ||||
| Kansas | 1915 (c) | Utah | X | ||||
| Maine | 1915 (c) | X | X | Vermont | 1915 (c) | ||
| Maryland | 1915 (c) | X | Virginia | X | |||
| Massachusetts | X | Washington | 1915 (c) | ||||
| Michigan | 1915 (c) | X | West Virginia | 1915 (c) | |||
| Minnesota | 1915 (c) | X | X | Wisconsin | 1915 (c) | X | X |
| Mississippi | 1915 (c) | Wyoming | 1915 (c) | ||||
| Total | 39 | 14 | 10 | ||||
The waiver authority also allows states to limit services to specific counties or regions of a state and to target services to certain groups--strategies that are not normally allowed under Medicaid. State Medicaid agencies must ensure that waiver programs have provisions to assure the health and welfare of participants. In addition, states must establish in advance how many people they will serve during the course of a year. Thus, in contrast to the regular Medicaid program, states may establish waiting lists for waiver programs.
Finally, average expenditures for waiver beneficiaries must be the same or less than they would have been without the waiver (no more than average Medicaid nursing home costs).25 Importantly, while services may be covered in residential care facilities, room and board may not. Medicaid can cover room and board only in institutions, such as nursing homes, ICFs-MR, and hospitals.
From the inception of the waiver program, states have used waivers to pay for services in residential care settings as an alternative to ICFs-MR. In 1981, Oregon became the first state to use the waiver program to fund services in residential care settings for elderly persons, but few states followed suit until the 1990s.
CMS has streamlined the waiver process, allowing applicants to fill in a pre-printed application form by checking off essential aspects of its proposal. On the waiver application form, CMS defines assisted living as:
"Personal care and services, homemaker, chore, attendant care, companion services, medication oversight (to the extent permitted under State law), therapeutic social and recreational programming, provided in a home-like environment in a licensed (where applicable) community care facility, in conjunction with residing in the facility. This service includes 24 hour on-site response staff to meet scheduled or unpredictable needs in a way that promotes maximum dignity and independence, and to provide supervision, safety and security. Other individuals or agencies may also furnish care directly, or under arrangement with the community care facility, but the care provided by these other entities supplements that provided by the community care facility and does not supplant it.
"Personalized care is furnished to individuals who reside in their own living units (which may include dually occupied units when both occupants consent to the arrangement) which may or may not include kitchenette and/or living rooms and which contain bedrooms and toilet facilities. The consumer has a right to privacy. Living units may be locked at the discretion of the consumer, except when a physician or mental health professional has certified in writing that the consumer is sufficiently cognitively impaired as to be a danger to self or others if given the opportunity to lock the door. (This requirement does not apply where it conflicts with fire code.) Each living unit is separate and distinct from each other. The facility must have a central dining room, living room or parlor, and common activity center(s) (which may also serve as living rooms or dining rooms). The consumer retains the right to assume risk, tempered only by the individual's ability to assume responsibility for that risk. Care must be furnished in a way which fosters the independence of each consumer to facilitate aging in place. Routines of care provision and service delivery must be consumer-driven to the maximum extent possible, and treat each person with dignity and respect.
| Assisted living services may also include | |
|---|---|
| Medication administration Intermittent skilled nursing services Transportation Periodic nursing evaluations |
Home health care Physical therapy Occupational therapy Speech therapy |
"However, nursing and skilled therapy services (except periodic nursing evaluations if specified above) are incidental, rather than integral to the provision of assisted living services. Payment will not be made for 24-hour skilled care or supervision. Federal financial participation is not available for the cost of room and board furnished in conjunction with residing in an assisted living facility."
States that want to provide waiver services in residential care settings do not have to conform their programs to the CMS definition, but may submit different definitions of assisted living in their application, which are subject to CMS approval. States may also choose to provide waiver services in congregate housing even if the waiver does not specifically cover a service category called "assisted living."
Differences Between State Plan and Waiver Services
HCBS waivers and state plan services differ in several important ways. First, waiver services are available only to beneficiaries who meet the state's nursing home level of care criteria; that is, they would be eligible for Medicaid payments in a nursing home if they applied. Nursing home eligibility is not required for beneficiaries using state plan services.
Second, states may set limits on the number of beneficiaries that can be served through waiver programs. The limits are defined as expenditure caps that are part of the cost neutrality formula required for CMS approval. Waivers are only approved if the state demonstrates that Medicaid long-term care expenditures under the waiver will not exceed expenditures that would have been made in the absence of the waiver. States do not receive federal reimbursements for any waiver expenditures that exceed the amount stated in the cost neutrality calculation. In contrast, state plan services are an entitlement, meaning that all beneficiaries who meet the eligibility criteria must be served. Federal funding matches state expenditures without any cap.
Perhaps the most significant difference between the two options is the ability under HCBS waivers to use a more generous eligibility standard. HCBS programs allow states to use the special income level, an optional eligibility category that allows states to set eligibility at up to 300 percent of the federal Supplemental Security Income (SSI) benefit ($1,692 in 2004). To cover beneficiaries through this option under the waiver, it must also be available to individuals in a nursing home. The higher eligibility standard in the waiver programs is designed to "level the playing field" between institutional and non-institutional services.
In contrast, to be eligible for personal care under the state plan, individuals must meet usual community-based eligibility standards, which (depending on the state) are: (1) the SSI level of income ($564 in 2004) up to 100 percent of the federal poverty level, or (2) the state's medically needy income standard.26 Table 1-10 summarizes the major differences between waiver services and state plan services.
Although the majority of states use Medicaid to cover services in residential care settings, the number of Medicaid beneficiaries who receive such services is considerably lower than might be expected because many states limit the number of people served under waivers. States using personal care under the state plan to cover services have higher participation rates than states using the waiver because state plan services cannot be capped.
Roughly 20 percent of all Medicaid beneficiaries living in residential care settings are in North Carolina, and another 25 percent are in Missouri and New York. These states cover services under the state plan. Waiver participation, while lower, has risen in many states over the past 2 years. Participation rose in New Jersey from 119 in 1998 to 1,500 in 2002 and 2,195 in 2004. Oregon reported that the number served rose from about 1,500 in 1998 to 3,600 in 2002 and 3,731 in 2004. Other states with relatively high waiver participation rates include Arizona (3,067), Colorado (3,804), both Georgia and Texas served 2,851 each, Florida serves 4,167 in its waiver program and 14,000 through the state plan.
| Issue | State Plan Service | 1915(c) Waiver Services |
|---|---|---|
| Entitlement | States must provide services to all beneficiaries who qualify for Medicaid | States may limit spending for waiver services |
| Scope | Must be available in the same amount, scope, and duration to all beneficiaries across the state | May be limited to specific geographic areas or groups of beneficiaries |
| Duplication | Provided in accordance with state plan | May not duplicate services available in the plan; may have different limits, definitions, or providers than state plan |
| Service Criteria | Must meet requirements of the state plan program to receive the service | Must meet the state's nursing home level of care criteria |
| Income | Must be SSI eligible or meet the state's community eligibility standard for Medicaid | State may set eligibility up to 300 percent ($1,692) of the monthly federal SSI payment standard ($564) |
| Approval Period | Continuous unless amended by the appropriate state agency | Initial waivers approved for 3 years; 5 years for renewals |
States do not report this information by age or type of disability. The vast majority served are age 65 and older but some may be under age 65. Some may have serious mental illness, acquired brain injuries, mental retardation, or other developmental disabilities. Whatever their age or diagnosis, to be eligible for Medicaid coverage all must meet either the state's nursing home level of care criteria for waiver services, or the state's service criteria for Medicaid state plan personal care services.
Participation figures are under-reported since a few states do not track and report the number of Medicaid beneficiaries by home or community settings. A few states reported the annual unduplicated number of Medicaid beneficiaries served in residential care settings, but most reported the number of people for a given month. Based on available data, participation is estimated to have grown from 58,544 beneficiaries in 2000, to about 102,000 beneficiaries in 2002, and 121,282 in 2004.
Limitations of Using Waiver Programs to Cover Services in Residential Care and How States Have Addressed Them
A major challenge facing policymakers who support a comprehensive range of home and community services is finding the resources to expand their availability. Waiver services are not an entitlement and most waiver programs operate with a specific appropriation based on a number of budgeted "slots." Although states may cover services in residential care settings through a waiver program, limited slots may lead to a waiting list for services. On the other hand, nursing home care is an entitlement, and its budget is likely to rise each year through rate increases. In the event of a budget deficit, non-entitlement services are the most vulnerable to budget cuts. States are addressing this issue in several ways.
-
Colorado, Oregon and Washington have shifted resources from institutions to home and community services by creating a single appropriation for long-term care services, sometimes called "pooled funding" or "unified funding."
-
Arizona, Florida, Massachusetts, Minnesota, New York, Texas, Utah, Wisconsin and states with PACE programs have capitated funding for long-term care services, which gives contracting organizations the flexibility to approve the most appropriate service for beneficiaries.
-
Kansas, Maryland, and Texas have adopted a "Money Follows The Person" policy, which allows funding appropriated for nursing homes to be spent on home and community services for individuals who relocate from a nursing home. Texas has a one year waiting list for waiver services. Since they adopted this policy in 2001, the state has relocated 3,400 people from nursing homes to community settings. Twenty-six percent moved to their own home; 37 percent moved in with family members; and 32 percent moved to a residential care setting.
-
Illinois uses funds from its nursing home appropriation in a demonstration waiver program that provides services for residents of Supportive Living Facilities (SLFs). The program was built on the premise that about 10 percent of nursing home residents could be served in residential care settings with access to supportive services 24 hours a day. Because the program is funded from the nursing home budget rather than the waiver budget, the state is able fund all approved SLF slots and there is no waiting list. Although the waiver was approved to serve 5,000 participants, in November 2001, the state placed a moratorium on new SLFs due to budget difficulties, which is still in effect.
-
Vermont enacted a law in 1996 allowing the Department of Aging and Disabilities to shift funding for 234 nursing home beds over 4 years to fund home and community services. It has allowed the Department to increase HCBS waiver slots for in-home and residential care settings, with priority for people at immediate risk of nursing home placement. Funds redirected but not spent remain available for home and community services in subsequent years. During the first 3 years of the program, 200 nursing home beds were taken off-line. Since enactment, spending on home and community services rose from 11.6 percent of total long-term care spending to 31 percent in 2002.
All of these financing strategies give states a mechanism to assure that people who can be served in the community are not required to stay in nursing homes because of a waiting list for waiver services.
Enabling Medicaid Beneficiaries to Pay for Room and Board
Medicaid beneficiaries with limited income may not be able to pay residential care facilities' room and board rates. As noted earlier, Medicaid pays for room and board only in institutions, except in limited circumstances such as respite care and meals that are served as part of a day care program (§441.360(b)). For Medicaid purposes, room and board comprises real estate costs (debt service, maintenance, utilities, and taxes) and raw food. The costs of preparing, serving and cleaning up after meals can be covered as a waiver service.
Although Medicaid beneficiaries are responsible for room and board costs, states have a range of options to make them affordable.
- Limit the amount facilities can charge Medicaid clients for room and board to the federal SSI benefit, which in 2004 is $564 minus a small personal needs allowance;
- Provide a state supplement to the SSI payment for persons living in residential care settings, and limit the amount that can be charged to the combined SSI plus state supplement payment;
- Use the 300 Percent of SSI Income Standard for waiver eligibility and set the maintenance allowance at a level that allows residents to retain sufficient income to pay for room and board;
- Provide housing subsidies for low-income persons;
- Allow family supplementation to increase the funds available for room and board, particularly to pay the difference in cost between a shared and a private room; and
- Use the federal Food Stamp Program, when possible, to reduce board costs.
Each of these options is discussed below.
Limiting the Amount Facilities Can Charge for Room and Board
States can limit the amount that can be charged for room and board by setting a combined rate for Medicaid beneficiaries that includes service costs and room and board costs, essentially capping the room and board rate that Medicaid beneficiaries pay. See Table 1-11 for a list of states that do so. Medicaid programs that specify how much facilities may charge Medicaid beneficiaries for room and board usually limit the charges to the state's SSI payment for a single elderly beneficiary living in the community, plus a state supplement, if any. This approach guarantees that Medicaid beneficiaries can afford room and board costs.
| TABLE 1-11. States That Limit Charges for Room and Board | ||
|---|---|---|
| Arizona Colorado Delaware District of Columbia Georgia Hawaii Idaho* Illinois Indiana |
Maryland Minnesota Mississippi Montana Nebraska New Jersey New Mexico North Carolina North Dakota |
Oregon Pennsylvania South Carolina South Dakota Texas Vermont Washington Wisconsin |
| * The limit is "suggested." | ||
If providers feel that the room and board rate is too low to cover costs, they may decide not to admit Medicaid beneficiaries. Only New Jersey has passed a law requiring that facilities licensed after September 2001 set aside 10 percent of their units to serve Medicaid residents within 3 years of licensing.
Persons in residential care settings who qualify for SSI receive a basic federal SSI payment ($564 in 2004). In settings that do not have housing subsidies, they retain a personal needs allowance (PNA), typically $30 or higher as determined by the state, and the remaining income is paid to the facility for room and board. If the resident lives in a Department of Housing and Urban Development (HUD) 202 subsidized unit in which the tenant's share of the costs for rent and utilities is limited to 30 percent of the resident's income, the resident may have additional income that could be used to pay for services. If a person is SSI eligible and received $564 a month, they will pay 30 percent of this amount for rent ($169.20), and have $394.80 left over.
HUD's housing subsidy rules do not allow residential care settings to impose an additional charge for rent and utilities, but they can charge the resident for board (i.e., meal costs) or for services that are not covered by the Medicaid state plan in a residential care setting. The amount of the permitted meal charge depends on the scope of the Medicaid service payment (i.e., whether it includes the cost of meal preparation). In all cases, Medicaid may not pay for raw food.27
Under HCBS waivers, the cost of preparing and serving food may be covered under the service payment. If preparing and serving meals is covered, the meal cost charged to tenants would be lower. If not, charges for a meal program would include raw food, preparation, and serving. States covering personal care in residential care settings under the state plan may also allow payment for the preparation and serving of meals but may not include the cost of food.
Medicaid beneficiaries with incomes over the SSI level must contribute income above the amount of room and board (minus a small personal needs allowance) to pay for services. Medicaid then pays the difference between the resident's payment and the maximum service rate. Because beneficiaries in this category have more income than SSI beneficiaries, when they live in subsidized units, they will pay a higher rent, because the rent is calculated as a percentage of income. They also may have more income available after the rental payment is made.
Providing State Supplements to the SSI Payment
To increase access for SSI beneficiaries in areas with high development costs, states can create a special SSI state supplement for persons in residential care facilities and limit what providers may charge to the amount of the federal payment plus the state supplement.28 Many states have such State Supplemental Payment (SSP) programs to supplement the federal SSI payment, which in 2004 is $564 a month; the payment is adjusted each January based on the cost of living. Individual states may use a specific term to refer to their supplement and some use the term SSI to refer to both the federal payment and any state supplement.
State supplements are totally state-determined and vary widely.29 Of the 28 states that have a supplement, 21 provide less than $100 a month.30 States may pay different supplements based on a person's living arrangement. A few states have developed a supplemental payment rate specifically for beneficiaries in residential care settings to provide them with sufficient income to afford room and board.
Some policymakers might question the efficiency of providing 100 percent state funding to enable residents to pay for room and board. However, it is important to consider the net state cost of services in a residential setting compared to a nursing home. If the program diverts people from entering a nursing home or allows individuals to move from a nursing home to the community, states may fund a fairly substantial supplement to the federal SSI payment and still reduce their net state cost. For example, the net state cost for a state with an average nursing home payment of $3,000 a month and a 50 percent federal match is $1,500. A state could use a portion of the state match that would normally pay for nursing home care to raise the payment standard for residential care settings. Policymakers would have to determine how many people would be covered if the supplement were increased in order to calculate whether the change is "budget neutral" (or better) relative to the amount of the supplement.
Providing Housing Subsidies for Low-Income Persons
Many states are exploring ways to combine Medicaid funding and subsidized housing to develop residential care options for low-income persons. Housing subsidies can reduce housing costs for Medicaid beneficiaries and other low-income persons, and are available through a number of programs:
- Low Income Housing Tax Credits;
- HUD Section 202 Assisted Living Conversion Program;
- Section 8 Rental Assistance Vouchers;
- HUD Fair Housing Act Section 232 Mortgage Insurance Program;
- Federal Home Loan Bank Affordable Housing Program;
- Low Interest Bonds;
- U.S. Department of Agriculture (USDA) Housing Services Programs;
- Community Reinvestment Act; and
- State, City, and other Local Programs.31
Some federal housing programs either provide direct grants to public housing agencies and to developers or they reduce the debt incurred by the owner and, therefore, the revenue that needs to be raised through tenant rental fees. Others provide rental assistance directly to low-income tenants who would otherwise be unable to afford even reduced rents.
The HUD Section 8 Housing Choice program contains some provisions that states can use to subsidize housing costs for waiver clients in residential care settings. Housing Choice offers two broad voucher programs: Fair Share and Special Purpose.
Fair share vouchers are allocated to serve people on waiting lists for Section 8 assistance. They are awarded through a competitive process and an additional 15 points are given to proposals that set aside 15 percent of the vouchers for people with disabilities. In addition, proposals qualify for 5 points if they demonstrate collaboration with Medicaid waiver programs and set aside 3 percent of the vouchers for waiver participants. Special purpose programs offer mainstream vouchers to help people with disabilities find affordable private housing, which can include residential care settings.
Typically, multiple public programs are needed to provide an adequate housing subsidy. For example, one affordable assisted living development in Vermont was financed by a combination of funds from HUD's Section 202 Assisted Living Conversion Program, the Vermont Housing and Conservation Board, the Community Development Block Grant and City Trust, HUD Special Purpose Funding, and tax exempt bond financing through the Vermont Housing Agency. However, because housing subsidy programs and Medicaid operate under different requirements, including those related to eligibility, extensive planning and collaboration is needed to enable multiple programs to work together.
Using the 300 Percent of SSI Income Standard and Providing an Adequate Personal Maintenance Allowance
States have the option to cover persons in an HCBS waiver program using the special income standard, which sets eligibility at up to 300 percent of the federal SSI payment (i.e., a person's income must be at or below 300 percent of the maximum SSI benefit--in 2004, $1692 per month). This option is attractive for waiver programs that cover services in residential care settings, because it expands the program to include beneficiaries who are better able to afford room and board costs. To make this option effective, however, states must allow eligible persons to retain enough of their income to cover "maintenance needs" including the room and board charges in residential care settings. Setting a higher maintenance allowance may allow more beneficiaries to be served in residential care settings; however, it will increase Medicaid's service payment since it reduces the "excess income" that is applied to the cost of services.
Under Medicaid's post-eligibility treatment of income rules for HCBS waivers, states are allowed to use "reasonable standards" to establish the maintenance allowance, and may vary the allowance based on the beneficiary's circumstances. For example, states can permit Medicaid beneficiaries to keep sufficient income to pay for the needs of a dependent, health care costs not covered by Medicaid, and other necessary expenses.
Beneficiaries living in residential care settings may have different income needs depending on the type of facility: private market-rate facility or subsidized housing facility. The "rent" component of the monthly fee charged by facilities built with low-income housing tax credits will be lower than the rent charged by privately financed facilities. Through tax credits, rents in assisted living can be reduced to around $400 a month. Setting the allowance based on the area's average monthly charge for room and board may be overly generous when applied to residents in subsidized units. On the other hand, setting the maintenance allowance based on the amount paid by residents in subsidized units may be too low for private market facilities and create access barriers. If a state wants to improve access to both private and subsidized assisted living facilities, it can set a separate maintenance allowance for each setting.
Interaction with housing subsidies. Under HCBS waivers using the 300 percent eligibility option, treatment of the additional income retained by residents because of rent subsidies depends upon the threshold set by the state for the maintenance allowance. If the state sets the maintenance allowance at the SSI level, all income above that amount is applied to the cost of Medicaid services. If the person has income between SSI and the maximum ($1,692 in 2004), residents receiving housing subsidies may have additional income that is protected. For example, a person with $1,000 a month in social security and other income would have a maintenance allowance of $564 and apply the excess income ($436) to the cost of services. However, instead of paying $564 (less the PNA) for rent and utilities, if the resident is living in HUD Section 202 subsidized housing, the resident pays 30 percent of his or her income ($300) and keeps $264 for other expenses.
If the maintenance allowance is higher, the resident can retain the additional income and use it to pay for other costs. For example, if the resident is allowed to keep the entire $1,000 a month, the resident's portion of the rent and utility charge would be $300 a month and the resident keeps $700. States typically set one maintenance amount for all waiver participants. However, there can be differences among beneficiaries. Those who do not receive a rent subsidy have a greater need for income to pay for room and board than those with subsidies. Yet, they have the same maintenance allowance and pay different amounts for room and board.
Separate maintenance allowance. Medicaid rules allow states to set different maintenance allowances, for example, for beneficiaries whose rent is subsidized. The Medicaid manual (3590.9 (A)(1)) states: "You may establish a different amount for each individual, or for groups of individuals, if you believe that different amounts are justified by the needs of the individuals or groups." A lower maintenance amount for individuals with rent subsidies means more income is available to share the cost of services.
States face many challenges in their efforts to expand the supply of affordable assisted living by combining available housing programs and Medicaid funding. Housing subsidies may not be available in a particular area or, as is often true with waiver services, waiting lists may exist for rent vouchers. To be effective, a rent subsidy voucher must be available when a waiver participant applies and at the same time that a facility is available that will accept the voucher as well as Medicaid payment. From application to implementation, close collaboration is needed between public housing agencies, waiver programs, and service providers. These challenges require knowledgeable housing operators and local housing authorities and state policymakers who are able to identify and address the barriers.
Family Supplementation
Family members may be able and willing to help with room and board costs when the beneficiary is unable to pay them. As presented in Table 1-12, 21 states reported that they allow family supplementation, and nine states have not set a policy on this issue. Twelve states do not allow supplementation compared to fourteen in 2002 and eight in 2000. The remaining states either do not cover services in residential care settings or did not report whether they have a policy on supplementation.
| Allow Supplementation | No Policy | Prohibit Supplementation | ||
|---|---|---|---|---|
| Arizona Colorado Florida Georgia Kansas Idaho Illinois Iowa Maine Michigan Minnesota |
Missouri Montana Nevada New Jersey New Mexico New York North Carolina North Dakota Texas Utah Wisconsin |
Alaska District of Columbia Hawaii Indiana Massachusetts Mississippi New Hampshire Wyoming |
Connecticut Delaware Indiana Maryland Nebraska Oregon |
Pennsylvania Rhode Island South Carolina South Dakota Vermont Washington |
States set their own rules governing family supplementation. Since Medicaid does not pay for room and board in residential care settings, rules regarding supplementation in nursing facilities do not apply (e.g., families of nursing home residents may not supplement Medicaid payments, which cover room and board and services). Several states indicated that supplementation is permitted to allow beneficiaries to upgrade to a private unit.
While supplementation is not prohibited, it is considered in determining eligibility for SSI. Federal SSI regulations contain provisions for treating unearned income during the eligibility determination process. A family contribution paid directly to an SSI beneficiary is counted as unearned income. Consequently, supplementation can lead to a reduction in the SSI payment or the loss of SSI altogether, and with it, potentially Medicaid as well.
If, however, the family contribution is paid directly to a residential care facility on the beneficiary's behalf, it is treated differently, as an "in-kind" payment, and reduces the monthly SSI benefit by one-third or, if documented, the actual amount of support provided if it is lower than one-third of the federal benefit. The maximum reduction is one-third even if the payment exceeds one-third of the SSI payment.
For example, a facility may have a room and board rate of $800, and because the SSI payment is not high enough to cover the charge, family members agree to help pay the cost. If the payment is made to the resident, it is considered unearned income and the federal SSI payment is reduced $1 for every $1 in unearned income, after a $20 per month exclusion. If the payment is made directly to the facility, the amount of the payment is considered "in-kind," and the one-third reduction rule applies (i.e., the federal benefit is reduced by one-third, or less if documented).
If the room and board rate is $800, the difference between that rate and the SSI benefit of $564 is $236. If the family pays $236 directly to the facility, then the individual's SSI benefit is reduced by one-third ($188) to $376. The family would then have to pay to the facility an additional $188. The consequence of the one-third reduction, then, is that the family must increase its supplementation from $236 to $424.
Because the rule states that the SSI payment will be reduced by up to one-third, there is no federal limit on the amount of money that can be paid to a facility on behalf of the SSI beneficiary. If a family chooses, they can subsidize services other than room and board, as well as pay for room and board costs in more expensive facilities, without jeopardizing an individual's eligibility for SSI.
However, states that provide SSI supplements may choose to set a limit on in-kind payments. Florida, for example, limits the amount families may contribute to twice the amount of the combined SSI payment and state supplement, which is $643. Thus, families or other third parties can provide up to $1,284 directly to the facility, and the beneficiary will still receive a federal payment of $376 plus a $79 state supplement, and remain eligible for Medicaid. However, the state reduces the state supplement dollar for dollar for any payment above $1,284.
Family supplementation also has implications for Medicaid eligibility. Since Medicaid income and resource rules follow SSI rules, payment to a residential care setting would be considered in-kind income to the beneficiary. If the individual still receives SSI, and therefore remains a Medicaid beneficiary, there is no impact.32 Beneficiaries who are eligible through spend-down or the 300 percent special income level might be affected if the supplementation raises their income above the medically needy income standard or the 300 percent level.
To prevent beneficiaries from losing Medicaid eligibility, states could explore submitting a state plan amendment to exempt in-kind income that supports a person's accommodations or services not covered by the Medicaid payment in residential care settings. Section 1902(r)(2) of the Social Security Act allows states to use such less restrictive income and resource methodologies in determining eligibility for most Medicaid eligibility groups than are used by the cash assistance programs, such as SSI. States can elect to disregard different kinds or greater amounts of income and/or resources than the cash assistance programs, giving states more flexibility to design and operate their Medicaid programs.33
Food Stamps
The use of food stamps to pay for meals subsidizes the board component of the room and board cost, making it more affordable for Medicaid beneficiaries and others with low incomes. USDA regulations allow meals provided in certain group living arrangements to elderly, blind, or disabled residents to be supported by food stamps (7 CFR §271.2). Group living arrangements are defined as a public or non-profit residential setting that serves no more than 16 residents. Facilities that can participate as food stamp vendors receive stamps from beneficiaries, which are used as payment toward meal costs.
Wisconsin officials are working with USDA to allow Residential Care Apartment Complexes to become approved food stamp vendors for eligible residents. SLFs in Illinois and Community-Based Residential Care Facilities in Wisconsin have been approved as food stamp vendors. Massachusetts continues to explore this option with USDA. SLFs in Illinois that participate in the program receive about $97 a month for eligible beneficiaries.
One final approach states can use to make room and board costs more affordable is to examine the facility's monthly room and board charges to identify any coverable services--such as laundry assistance, light housekeeping, or food preparation--that Medicaid can reimburse for beneficiaries who require assistance with these IADLs. Including all coverable services in the state's assisted living service payment reduces the beneficiary's monthly payment solely to room and board and any other charges that Medicaid does not cover.
Effect of Medically Needy Rules on the Ability to Pay for Room and Board (34)
States have the option of covering medically needy beneficiaries under their Medicaid programs. The medically needy are persons who, except for income, would qualify in one of the other Medicaid eligibility categories (such as being over age 65 or meeting SSI disability criteria). Medicaid payments can begin for this group once they have "spent down"--that is, incurred expenses for medical care in an amount at least equal to the amount by which their income exceeds the medically needy income level. Any family supplementation is considered part of the excess income that must be spent down.
The medically needy eligibility option can allow people who have income greater than 300 percent of SSI to become eligible for Medicaid services. But federal law imposes two significant constraints on the use of this option:
-
The state must cover medically needy children and pregnant women before it can elect to cover any other medically needy group. Additionally, the state may not place limits on who is eligible for Medicaid by using such characteristics as diagnosis or place of residence. Thus, it cannot use medically needy policies to extend Medicaid services only to HCBS waiver beneficiaries in residential care settings.
-
The maximum income eligibility limit that a state medically needy program may use is based upon its welfare program for families--levels that are typically lower than SSI. The income level must be the same for all medically needy groups in the state (i.e., states are not permitted to establish higher income eligibility levels for selected subsets of the medically needy, such as beneficiaries in residential care settings).
These rules have several implications that states need to consider when trying to make the medically needy eligibility option work for higher income individuals in residential care settings. First, these individuals may find it more difficult to incur sufficient medical expenses to meet the spend-down requirements while living in the community than they would in a nursing home. The higher their "excess" income, the higher the amount of their spend-down--which means only beneficiaries with extremely high medical expenses may qualify. Second, community providers are less willing to deliver services during the spend-down period, since payment cannot be guaranteed and collection may be difficult. Third, spend-down rules combined with low medically needy income-eligibility levels mean that individuals may not have enough total income to pay both the bills they incur under the spend-down provision and room and board.
In sum, room and board costs may present a barrier to residential care living for Medicaid beneficiaries unless states take specific steps to make them affordable. Several observers have suggested that the Medicaid program be allowed to pay for room and board in residential care settings as it does in nursing homes, a policy change that would require Congressional approval. However, such a change would likely lead the SSI program to classify residential care as an institution, regardless of how states license it, and SSI pays only a personal needs allowance of $30 to individuals who reside in institutions. Because such a change would shift costs from the federal SSI program to state Medicaid programs, it is highly unlikely.
Medicaid Policy Issues for Housing Investors, Developers, and Operators
The growth of assisted living has sparked interest in developing or expanding assisted living for elderly persons with low-incomes. However, facilities may be reluctant to participate in the Medicaid program if they are unsure they will have a reliable source of potential residents and payments. Housing providers and lenders need to project revenues to determine the feasibility of each project. The rent-up period and a stable occupancy rate help them determine cash flow. Public agencies that provide subsidies to developers to build affordable assisted living need assurances that there will be a stable source of funding for residents' service needs. Consequently, in addition to being knowledgeable about the Medicaid program generally, assisted living investors, developers, owners, and operators need to be aware of several Medicaid policy and program issues.
Reliability of Medicaid Funding Options
State plan services are an entitlement and all beneficiaries who meet the service requirements must be served. Personal care is the most common service covered in residential care settings under the state plan, but New York combines payments for personal care, home health services, including skilled therapies. States that do not already cover personal care through their state plan have been reluctant to add it because it is an entitlement and services must be provided statewide. However, CMS has allowed states to limit the provision of personal care provided under the state plan to specific providers, which may address state concerns about adding an open-ended entitlement to personal care under its state plan. South Carolina, for example, allows only licensed community residential care facilities to provide personal care under the state plan.
On the other hand, services provided under Medicaid waivers are not entitlements and states may limit their provision to particular geographic areas, target groups, and care settings. Additionally, states may limit the number of waiver participants and further reduce this number during state budget cutbacks. States can also use solely state-funded long-term care programs to pay for services in assisted living. However, because they also are not entitlements, these programs are also vulnerable during state budget cutbacks.
Types of Waivers
As discussed earlier, states can cover services in residential care settings through a waiver program that provides services in the full range of home and community settings, or through a waiver that covers services only in residential care settings. The type of waiver can affect the pattern of referrals. States that include assisted living as one of a menu of home and community services must always offer beneficiaries a choice of services and cannot guarantee that applicants will choose assisted living. Single service waivers are better able to assure referrals as long as the number of providers contracting with Medicaid does not exceed the capacity of the waiver.
Waiting Lists
Some states have long waiting lists for waiver services, which can present a significant obstacle to serving Medicaid beneficiaries in assisted living. If waiver slots are not available, Medicaid-eligible persons who cannot be served at home will need to enter a nursing home (if they meet the state's nursing home level of care criteria) and the assisted living facility will have to look elsewhere for new residents. Recognizing this as a potential problem, lenders may require that facilities establish a reserve to cover low occupancy in the event that Medicaid funds are not as available as projected.
States that fund waiver services and nursing homes from a pooled appropriation (Oregon and Washington) or who allow funding to "follow the person" who transfers from a nursing home to community settings (Indiana, Maryland, Texas, and Vermont) have more flexibility.35 States that permit money to follow the person, essentially allow a person transitioning from nursing homes to bypass the waiting list. States that make a concerted effort to help nursing home residents re-locate to community settings have staff that will generate referrals to assisted living facilities.
State Policy Regarding Room and Board Payments
About half of the states limit the amount that facilities can charge Medicaid beneficiaries for room and board--usually to an amount equal to the federal SSI payment plus a state supplement (if offered). Others do not restrict the amount that can be charged, but providers need to understand their states' income eligibility rules and cost sharing requirements to determine how much Medicaid beneficiaries can afford. Persons eligible for Medicaid because they are receiving SSI have no income other than the federal payment and a state supplement (if any). State supplements vary considerably among states. Of the 28 states that have a supplement, 21 provide less than $100 a month.36 Even in states that use the 300 percent of SSI income eligibility standard for its HCBS waiver program ($1,692 a month in 2004), beneficiary cost sharing requirements can reduce the amount of income available to pay for room and board.
Time Frame for Determining Medicaid Eligibility
Some states may not determine eligibility for services until financial eligibility has been determined, a process that can take up to 45 days. An extended time frame for determining Medicaid eligibility can be a major deterrent to participation in the Medicaid program, because providers will generally not want to admit someone if they are unsure about payment. If Medicaid eligibility cannot be determined quickly, beneficiaries in the midst of a transition, especially those being discharged from a hospital, may be more likely to enter a nursing home. To address this problem, 11 states report having a process for expediting eligibility determination: Colorado, Connecticut, Florida, Georgia, Idaho, Maryland, New Mexico, North Carolina, Oregon, Washington, and Wisconsin.
Some states expedite the determination of Medicaid eligible or allow case managers or eligibility workers to "presume eligibility" based on preliminary information. However, if the eligibility is later found incorrect, states do not receive federal reimbursement for expenditures made while the determination was pending and must pay providers solely with state funds. Nebraska, Ohio, and Washington have provisions for allowing presumptive eligibility, and Michigan allows its Area Agencies on Aging, which administer HCBS programs, to have such provisions as well. Georgia and Pennsylvania have developed initiatives to expedite the application process.
State Approaches to Reimbursing Services
The extent to which low-income older people have access to residential care settings as an alternative to nursing homes depends in large part on the extent to which states use Medicaid to cover services in these settings and providers' views on the adequacy of Medicaid's service reimbursement rates. In addition to the amount of the payment, the reimbursement approach can also serve as incentives or disincentives for providers.
Data suggest that states have increased their payments over the past 4 years, although they are still quite low relative to private-pay rates, and may not cover residents' needs. However, key informants suggest that providers' willingness to accept Medicaid rates is increasingly driven by an over-supply of facilities and difficulty finding private-pay residents.
States face a number of major challenges in developing Medicaid payment methodologies for residential care services, including: (1) defining and distinguishing types of services, (2) collecting data on which to base payments while avoiding complex and burdensome new data collection requirements, (3) developing rates that support quality care and aging-in-place, and (4) providing reimbursement that is sufficient to assure provider participation within state budget constraints.
States use five primary approaches to set rates for Medicaid services provided in residential care settings:
- Flat rates;
- Flat rates that vary by type of setting;
- Tiered rates;
- Case-mix rate; and
- Cost-based reimbursement and fee-for-service rates.
Table 1-13 lists the states that use Medicaid to cover services in residential care settings according to their rate-setting approach. Descriptions of each states' reimbursement approach and rates can be found in Section 3 under the heading public financing.
Flat Rates
Under a flat rate system, providers receive the same monthly payment regardless of the amount of services and staff assistance a resident requires. As in the health care system, flat rates for residential care create incentives for facilities to admit residents with lighter care needs, not those with multiple impairments in ADLs, cognitive impairments or health needs. Twelve states use flat rate reimbursements, examples of which are described below.
| Flat Rates | Tiered Rates | Case-Mix | Modified Case-Mix |
Cost-Based and Fee-for-Service |
|---|---|---|---|---|
| Colorado Florida Georgia Illinoisa Massachusetts Mississippi Nebraska New Hampshire New Jerseyb New Mexico Rhode Island South Dakota |
Alaska Arizona Arkansasc Delaware Maryland Nevada Oregon Texasc Vermont |
Minnesotad New York |
Maine North Carolinae Washingtona |
Arkansasf Idaho Iowa Kansas Mainee Michigan Missouri Montana North Dakota Wisconsin |
|
||||
-
Florida pays facilities $28 a day for services provided through the waiver program and $9.28 a day for personal care services provide through the Medicaid state plan. Facilities may not charge Medicaid beneficiaries more than $588.40 for room and board, whether they are receiving waiver services or state plan services.
-
Massachusetts uses Group Adult Foster Care (GAFC)--a Medicaid state plan service--to cover services in residential care settings. Using the state plan to cover services allows Medicaid to serve people who are frail but are not eligible to enter a nursing home following a tightening of the level of care criteria. Massachusetts pays a flat daily service rate of $37.75 for Medicaid beneficiaries.
-
Colorado's Medicaid monthly rate for services is $1094.30 a month ($36.50 a day). The rate covers oversight, personal care, homemaker, chore, and laundry services. The state limits room and board charges for Medicaid beneficiaries to $518 a month.
-
Georgia pays a flat rate of $31.04 a day for waiver services provided to residents of group homes serving seven to 24 people. The state limits room and board charges for Medicaid beneficiaries to $475, for a combined monthly rate of $1,419.
-
Illinois has different daily service rates for each of its seven regions, ranging from $47.54 to $61.94. Rates are set at 60 percent of the weighted average nursing facility rate for the region and are adjusted annually to reflect changes in the rates paid to nursing homes.
Flat Rates that Vary by Setting
States may vary its flat rates for different types of residential care settings. Texas pays a higher rate for apartment and other private occupancy settings, reflecting the states' preference for these settings. Varying rates by setting may reflect differences in the average level of resident service needs in each setting. For example, a state may reimburse for services in both traditional elderly housing buildings and purpose-built assisted living facilities. Generally, tenants in elderly housing sites are less impaired than those in purpose-built assisted living facilities. Unlike purpose-built assisted living facilities, elderly housing sites typically do not have 24-hour staffing and the capacity to meet the unscheduled needs of tenants. Consequently, elderly housing facilities receive a lower rate than purpose-built assisted living facilities with 24-hour staffing.
New Jersey licenses assisted living services, which are provided in a range of settings. The state developed rates for each of three settings regardless of the level of services needed (see Table 1-14). Newly constructed assisted living residences receive $1,800 a month to cover waiver services, and comprehensive personal care homes receive $1,500 a month. Assisted living programs (services provided in subsidized housing) receive $1,200. The state limits room and board charges in both settings to $630.55. Residents in subsidized housing pay a percentage of their income for rent; the housing subsidy pays the difference between this amount and the actual rent.
| Assisted Living Residences |
Personal Care Homes |
Assisted Living Programs |
|
|---|---|---|---|
| Room and Board | $630.55 | $630.55 | n.a. |
| Medicaid waiver services | $1,800.00 | $1,500.00 | $1,200.00 |
| Total | $2,434.55 | $2,134.55 |
Tiered Rates
Tiered rates have been developed to more accurately and fairly reimburse providers for services provided to frailer residents. Tiered systems usually include three to five tiers based on the type, number, and severity of ADL limitations and/or cognitive or behavioral impairments, and create incentives for providers to serve residents with higher service needs. Eight states use tiered rates, examples of which are described below.
-
Arizona's Long Term Care System has three rate levels based on resident needs. The rate levels vary by type of setting; assisted living homes serve 10 or fewer residents and assisted living centers serve 11 or more residents. The service payments are negotiated and vary by program contractor (county). Daily rates for Level 1 range from $42.59 to $59.26; for Level 2 from $49.10 to $69.00; and for Level 3 from $49.10 to $87.27.
-
Delaware has three levels of waiver service monthly payments, which were developed based on an analysis of spending for HCBS waiver clients living in their own homes and in adult foster care. Level I is $940; Level II is $1,180; and Level III is $1460. Facilities receive an additional 10 percent for residents with cognitive impairments. The state limits the room and board payment for SSI beneficiaries to $598 in 2004, so maximum payments rates for each level range from $1,538 to $2,058. Residents whose incomes exceed $704 may be charged a higher amount for room and board.
-
Oregon has five payment levels based on the type and degree of residents' impairments. ADLs assessed include eating/nutrition, dressing/grooming, bathing/personal hygiene, mobility, bowel and bladder control, and behavior Table 1-15 lists the impairments needed for each level, and the payments per level. The state limits the room and board payment for Medicaid beneficiaries to $455.70. The distribution of residents by level is: Level 1--2 percent; Level 2--1 percent; Level 3--6 percent; Level 4--59 percent; and Level 5--32 percent, resulting in an average monthly service cost of $1,643 a month.
-
Texas uses a tiered payment system for HCBS waiver services derived from their nursing home case-mix system. Payments vary by level and by setting, which are listed in Table 1-16. The state limits the room and board payment for Medicaid beneficiaries to $479 a month.
Rates Based on Case-Mix Systems
Several states have adopted payment systems based on their nursing home case-mix methodology. Like tiered rate approaches, the case-mix approach creates incentives to serve more impaired residents by linking reimbursement to the level of care needed. Case-mix approaches typically have more categories that tiered rates. The case-mix approach requires extensive functional and health data for residents.
| Impairment Level |
Service Priority | Service | R&B | Total Rate |
|---|---|---|---|---|
| Level 5 | Dependent in 3 to 6 ADLs OR dependent in behavior and 1 to 2 other ADLs | $1,944.02 | $455.70 | $2,399.72 |
| Level 4 | Dependent in 1 to 2 ADLs OR assistance in 4 to 6 ADLs plus assistance in behavior | $1,574.64 | $455.70 | $2,030.34 |
| Level 3 | Assistance in 4 to 6 ADLs OR assistance in toileting, eating, and behavior | $1,204.07 | $455.70 | $1,659.77 |
| Level 2 | Assistance in toileting, eating and behavior or behavior AND eating or toileting | $910.23 | $455.70 | $1,365.93 |
| Level 1 | Assistance in 2 critical ADLs or assistance in any 3 ADLs or assistance in 1 critical ADL and 1 other ADL | $688.36 | $455.70 | $1,144.06 |
| Assisted Living Apartment |
Double Occupancy Apartment |
Residential Care Non-Apartment |
|
|---|---|---|---|
| AL 1 | $59.88 | $53.29 | $37.35 |
| AL 2 | $55.78 | $49.19 | $33.25 |
| AL 3 | $50.18 | $43.59 | $27.66 |
| AL 4 | $52.38 | $45.80 | $29.85 |
| AL 5 | $47.16 | $40.58 | $24.64 |
| AL 6 | $45.74 | $39.15 | $23.21 |
Both tiered rates and case-mix rates are subject to "category creep" or "gaming," a tendency for facilities to interpret assessment data to support payment of the next higher rate, or to request an adjustment because the resident has become more impaired and requires more staff support than upon admission. To address "gaming," states may use an assessment by an independent case management agency to determine the original payment level. Subsequent requests to adjust the payment level can be reviewed by either a case management agency or the state agency before being approved. Five states use tiered rates, examples of which are described below.
-
Washington uses a 12-payment level rate structure for waiver services provided in homes and residential care settings. A case manager conducts a comprehensive assessment to measure level of need and the appropriate rate tier. Three sections of the assessment are used to set the payment level based on a score: health status, psychological/social/cognitive status, and functional abilities and supports. Individuals must be substantially or totally impaired in an ADL to receive a score. Points are also assigned for impairments in speech, sight, and hearing, the number of medications, disorientation, memory impairment, impaired judgment, wandering, and disruptive behavior. The total score determines the payment level. A computer program reviews the assessment and determines the residents "level" and payment amount.
-
New York modeled its reimbursement rates on its case-mix system for paying nursing homes. The service reimbursement is set at 50 percent of the Resource Utilization Group (RUG) rate for nursing home residents. The state has created RUG rates for 16 geographic areas of the state. The reimbursement category is determined through a joint assessment by the Assisted Living Program and the designated home health agency or long-term home health care program. The Department of Social Services' district office reviews the assessment and the RUG category. In 2004, the combined SSI and state supplement rate was $999 in New York City, Nassau, Suffolk, and Westchester counties and $969 in the rest of the state. Beneficiaries retain a personal needs allowance of $127 and the balance is paid to the facility for room and board.
-
North Carolina covers personal care in adult care homes as a Medicaid state plan service and uses a modified casemix payment system. The payment includes a flat rate for basic personal care with add-ons for residents with specific ADL impairments. Residents with extensive or total impairments in eating, toileting, or both eating and toileting qualify for a higher rate. In 2004, the basic payment is $16.74 for facilities with 30 or fewer beds and $18.34 for facilities with more than 30 beds. The additional daily rate for residents with extensive or total impairments in eating is $10.33, toileting $3.69, and impairments in both eating and toileting are reimbursed at $14.02. An additional payment for residents needing assistance with ambulation/locomotion is $2.64 a day. These payment levels are in addition to the basic rate. Eligibility for the additional payment is based on an assessment by the adult care home, which is verified by a county case manager. The state SSI and state supplement payment standard is $1,112 monthly room. The resident keeps $36 a month for personal needs and pays the remaining $1,066 to the facilities for room and board.
Cost-Based Reimbursement and Fee-for-Service Rates
Cost-based reimbursement pays the facility for aggregate costs incurred for Medicaid eligible residents for allowable services.
Fee-for-service rates are determined by the number of hours of service identified in a care plan or a point system based on an assessment. For example, Kansas treats assisted living facilities as providers of home care services, and reimburses for the services delivered. This approach may be cumbersome for some facilities to implement because they are used to receive a regular monthly payment and providing resident services as needed pursuant to a plan of care. If services are reimbursed on a fee-for-service basis, facilities must track service delivery and prepare and submit bills to the payment agency. Depending on the pricing structure, assisted living facilities may not be set up to prepare and submit itemized bills for each increment of service delivered to each resident.
Service delivery in assisted living facilities also differs significantly from in-home service programs. Participants in home care programs typically receive services in block authorizations (e.g., 2 hours of care, 5 days a week). Assisted living residents typically receive services in 15-minute increments at various times 7 days a week including nights. Home care programs typically do not cover services at night, and, of course, cannot meet unscheduled needs.
Tracking, aggregating, and billing can become cumbersome and time consuming, especially for facilities used to charging a single all-inclusive service fee. However, the pricing structure of many facilities includes a basic package of services with additional charges based on the increments of service used by residents. Facilities with this policy for private-pay residents may be better able to participate in Medicaid programs that reimburse using a fee-for-service approach.
Eleven states use fee-for-service rates, examples of which are described below.
-
Arkansas allows personal care services to be provided through the state plan in a person's home "or other setting" such as a residential care facility (RCF). RCFs can be reimbursed for up to 64 hours of personal care per month.
-
In Missouri, personal care and advanced personal care services are reimbursed as a Medicaid state plan service in RCFs. Facilities are reimbursed at an hourly rate for the number of hours authorized in the care plan. The hourly payment rate is $13.16 for personal care aides, $15.20 for advanced personal care aide services, and $28.07 for nursing visits. The maximum payment is $2,368 a month, which is equal to the state's Medicaid cost for nursing home care. No more than one nursing visit a week can be authorized. Very few residents receive advanced personal care and nursing visits.
The state limits the room and board rate for Medicaid beneficiaries to the federal SSI payment plus the state supplement, also called a "cash grant," which varies depending on the type of facility. Type I facilities provide room and board, supervision, and protective oversight and receive a monthly payment of $695, comprising the SSI payment and a state supplement of $131. Type II facilities provide personal care, dietary supervision, and health care in addition to Type I services, and receive a combined monthly payment of $826, comprising the SSI payment and a state supplement of $262.
-
Montana uses a payment system that have elements of a tiered system but lack the structure and limited number of payment levels of tiered approaches. The payment amount varies widely based on the number and type of impairments, a structure more like a fee-for-service reimbursement approach. Montana's payment is based on a point system. Agency field staff determine the number of points based on an assessment of impairments, and the provider receives $33 a month per point. Residents with severe impairments, totally dependent in more than three ADLs, can receive $44 a month for each point.
Monthly waiver reimbursement rates for personal care facilities vary between $520 (the basic service rate) and $1,800, depending on the residents' level of care needs. Additional payments are calculated based on ADL and other impairments. The points determine the actual payment within the range. The state limits monthly room and board payments for Medicaid beneficiaries to $564. The total monthly amount facilities receive (for services, room and board) ranges from $1,084 to $2,363, although very few participants have been approved at the highest service rate.
Adequacy of Rates
At first glance, it appears that states are paying markedly different rates for services, suggesting that some states may not be paying rates that are adequate to meet residents' service needs. However, it is not possible to compare service rates across states due to significant differences in their admission and retention criteria for residential care settings. Most notably, rates for providers who do not serve nursing home eligible residents are not comparable to rates for providers who do serve this population. Additionally, because nursing home level of care criteria themselves vary markedly across states, a person who is nursing home eligible in one state, may not be in another state.
States have no models on which to build reimbursement methodologies for residential care settings. Nursing home payment methods include both room and board and service costs, and must address the needs of higher acuity residents than are generally served in residential care settings, even those that serve individuals who meet a nursing home level of care. Historically, board and care homes have provided room, board and very limited services, and payment rates typically have been set at SSI plus state supplement levels. The trend is for residential care settings to provide a level of care somewhere between traditional board and care and nursing homes.
A potential source of comparable cost data for developing reimbursement rates is in-home services provided under HCBS waiver programs. However, significant differences exist between services provided in-home and in residential care settings. First, in-home service utilization may be constrained by the times during which it is available, state funding limits, or the lack of in-home workers. Second, in-home utilization may overstate the amount of services an individual needs because services are reimbursed in blocks of time such as 2-hour increments. In contrast, because residential care staff are on-site at all times, this setting is able to offer more intermittent services in smaller time increments. On the other hand, in-home utilization may understate services received because it does not include the sometimes considerable amount of unpaid care provided by family and friends, particularly during the evening, at night, and on weekends, when in-home services are generally not available.
These differences in utilization patterns may or may not offset one another in the aggregate. Consequently, states may need to collect data on service provision in residential care settings in order to develop adequate service rates. Washington and Maine have both conducted time studies to determine the amount of time direct care staff spend with residents.
Expanding the Supply of Assisted Living for Low-Income Individuals
Both federal and state governments recognize that, in order to reduce costly institutionalization, a range of supportive housing and service options is needed. An increasing number of persons 65 and older who can no longer live independently view assisted living as a preferred alternative to nursing home care, or as a means to forestall admission to a nursing home. But market rate assisted living that provides private rooms and a high level of services is generally far beyond the means of most low-income elderly persons.
There are several sources of funding available to finance the development or renovation of housing to create affordable assisted living. The Federal Government's main vehicle for creating affordable housing is the low-income housing tax credit program. Other sources of funding are programs in HUD and USDA, and state programs. These departments provide funds to both finance new housing units and provide rental assistance in existing housing. However, not all programs that create and/or support affordable housing can be used for affordable assisted living.
Developing affordable assisted living is a complex undertaking. Different statutory authorities and administrative structures, and a lack of communication among those who manage housing and service programs, present major difficulties. A major issue for some housing subsidy programs is that the lenders and investors they depend on require evidence of a stable revenue source over the life of their commitment to protect their investment--typically 15 to 30 years. But state service programs may be unable to provide a table revenue source because they are subject to annual appropriations that depend on the state's budget.
Additionally, despite targeting the same or similar populations, housing and service programs often have different and often conflicting income, age, and functional eligibility rules that make it difficult to create the supportive housing plus services arrangements that frail elderly persons need. Medicaid program requirements can also pose barriers to the receipt of services in residential care settings. Medicaid's rules regarding financial eligibility and post-eligibility treatment of income may limit an individual's ability to pay for room and board.
Housing programs also have conflicting requirements. Yet, successful projects often need to combine funding from multiple housing finance programs (e.g., low-income housing tax credits, HUD's HOME program, the Federal Home Loan Bank's Affordable Housing Program, conventional debt, and Housing Choice Vouchers), with two or more service subsidy programs (e.g., Medicaid state plan or waiver programs, state supplements to the SSI program, state funded service programs).37
At the state level, some agencies that manage Medicaid waiver programs have begun working with state and local housing agencies, and non-profit housing organizations to explore ways to combine housing subsidies with Medicaid services. At the federal level, HUD and the U.S. Department of Health and Human Services are currently looking at ways in which the agencies can work together to expand housing and service choices for people with disabilities.
Notes
-
The data were reported by state licensing agencies. Partial information was reported for some categories in Delaware, Kentucky, Minnesota, New Jersey, New York, New Mexico and West Virginia. (See Table 2-1 in Section 2 for each state's information.) While these numbers do not include facilities licensed by state Mental Retardation/Developmental Disabilities (MR/DD) agencies, some individuals with MR/DD may be living in facilities licensed as residential care/assisted living.
-
The number of residents receiving Medicaid in residential care settings is slightly underreported because it does not include data from Kansas. Kansas' reporting system does not differentiate between waiver clients served in their own homes and those served in residential care settings. Additionally, Alabama and the District of Columbia have not yet implemented approved 1915(c) waivers.
-
The six states were Florida, Minnesota, Oregon, North Carolina, Texas, and Wisconsin. Oregon is the only state of the six that requires assisted living providers to offer private apartments. (See Janet O'Keeffe, Christine O'Keeffe, and Shula Bernard. Using Medicaid to Cover Services for Elderly Persons in Residential Care Settings: State Policy Maker and Stakeholder Views in Six States. Report prepared for the U.S. Department of Health and Human Services, Office of Disability, Aging, and Long-Term Care Policy. [http://aspe.hhs.gov/daltcp/reports/med4rcs.htm])
-
42 U.S.C. 1396r.
-
Wendy Fearnside, Program and Planning Analyst, Bureau of Aging and Long Term Care Resources, Wisconsin Department of Health and Family Services.
-
Catherine Hawes, Ph.D. and Charles D. Phillips, Ph.D., M.P.H. A National Study of Assisted Living for the Frail Elderly: Final Summary Report. Texas A&M University System Health Science Center. US DHHS, Office of the Assistant Secretary for Planning and Evaluation, contract number HHS-100-94-0024 and HHS-100-98-0013. November 2000. [http://aspe.hhs.gov/daltcp/reports/finales.htm]
-
Oregon defines a "unit" as an individual living space constructed as a completely private apartment, including living and sleeping space, kitchen area, bathroom and adequate storage areas.
-
Ruth Gulyas. The Not-for-Profit Assisted Living Industry: 1997 Profile. American Association of Homes and Services for the Aging. Washington DC. 1997. Also, 2000 Overview of the Assisted Living Industry. The Assisted Living Federation of America and Coopers and Lybrand. Washington, DC. 2000.
-
Ronald K. Tinsely, Robert G. Kramer, et al. Overview of the Assisted Living Industry. Assisted Living Federation of America. Fairfax, VA. 2000.
-
Hawes et al., op. cit.
-
National Survey of Assisted Living Residents: Who Is The Customer? National Investment Conference and the Assisted Living Federation of America. Washington, DC. 1998.
-
"Assisted Living: Quality of Care and Consumer Protection Issues." GAO. T HEHS-99-111. April 26, 1999.
-
Some state summaries do not include this information because it was not readily available.
-
_____. Assisted Living: Examples of State Efforts to Implement Consumer Protections. U.S. General Accounting Office. GAO-04-684. Washington, DC. April 2004.
-
Thomas Clark, Director of Professional Affairs for the American Society of Consulting Pharmacists Medication Use and Pharmacist Impact in Assisted Living Facilities, located at http://www.ascp.com/public/pr/assisted/2003/rximpact.pdf.
-
The Beer's List identifies medications to avoid or use within specified dose and duration ranges for elderly persons, and medications to avoid in elderly persons with specific diseases.
-
Due to rounding, the percentages add to 102.
-
Catherine Hawes, Ph.D., et al. op.cit.
-
The Board of Directors comprises representatives from four consumer or advocacy groups (AARP, Paralyzed Veterans of America, Alzheimer's Association, Consumer Consortium on Assisted Living); four provider associations (American Association of Homes and Services for the Aging, Assisted Living Federation of America, American Seniors Housing Association and National Center for Assisted Living); and three representatives from professional organizations or associations (National Cooperative Bank Development Corporation, the Pioneer Network, America Assisted Living Nurses Association).
-
Medicaid spending for services delivered in residential care settings is not reported separately.
-
Data provided by Brian Burwell, The MEDSTAT Group. Memorandum, 2004.
-
Jones, A. "The National Nursing Home Survey: 1999." National Center for Health Statistics. Vital Statistics 13(15) 2002.
-
Rhoades, Jeffrey A. and Krauss, Nancy A. Nursing Home Trends, 1987-1996. Rockville, MD: Agency for Health Care Policy and Research; 1999. MEPS Chartbook No. 3. AHCPR Pub. No. 99-0032.
-
American Health Care Association. Based on CMS-OSCAR form 671:F41-F43. 2003.
-
States can use either a fixed per capita amount for each beneficiary or they can average expenditures across waiver beneficiaries. The latter method provides more flexibility because it allows some beneficiaries to exceed the nursing facility cost as long as costs for others in the program are lower and the average waiver cost does not exceed the average nursing facility cost. States have the option of setting a cap on waiver services at a percentage of nursing home costs (e.g., 80 percent).
-
Except in 209(b) states which have a Medicaid income eligibility threshold that is lower than the federal SSI payment.
-
Capitated programs have more flexibility to pay for room and board costs than is allowed under standard Medicaid rules).
-
Many states have a state supplement for residential care settings that may be too low to cover more intense services needs and higher capital costs in some residential care settings.
-
Stone. J.L. (2002). Medicaid: Eligibility for the Aged and Disabled. Congressional Research Service. Report prepared for Members and Committees of Congress.
-
For further information, see: "A Technical Assistance Guide for Housing Resources and Strategies," prepared by the Technical Assistance Collaborative Inc. for the Rutgers Center for State Health Policy Community Living Exchange Collaborative, funded by CMS to assist Real Choice Systems Change Grantees. http://www.nashp.org/Files/Final_Regional_Forum_guide.pdf. Also, Ruth A. Gulyas. How States Have Created Affordable Assisted Living: What Advocates and Policymakers Need to Know. AARP. Washington, DC.
-
Payments in 209(b) states might affect Medicaid eligibility since it is not linked to SSI eligibility.
-
Medicaid Eligibility Groups and Less Restrictive Methods of Determining Countable Income and Resources. CMS memorandum. 5/11/2001.
-
Some of the information in this section is taken directly from Smith, O'Keeffe, et al., Medicaid Home and Community Services: A Primer. [http://aspe.hhs.gov/daltcp/reports/primer.htm]
-
Wisconsin has a special waiver to assure community placement for individuals who want to transfer when their nursing home closes.
-
Stone. J.L. (2002). Medicaid: Eligibility for the Aged and Disabled. Congressional Research Services. Report prepared for Members and Committees of Congress.
-
Robert Jenkens, Deputy Director, Coming Home Program, Vice President, NCB Development Corporation. Personal communication, June 2004.
Section 2. Comparison of State Policies
TABLE 2-1. Comparison of State Residential and Assisted Living Regulations: Supply
| State | Category | 2004 | 2002 | 2000 | CoN | |||
|---|---|---|---|---|---|---|---|---|
| Facilities | Units/Beds | Facilities | Units/Beds | Facilities | Units/Beds | |||
| AL | Assisted living facilities | 335 | 9,876 | 327 | 9,738 | 304 | 8,000 | N |
| AK | Assisted living homes | 162 | 1,650 | 143 | 1,497 | 123 | 1,346 | N |
| AR | Residential long-term care facilities | 111 | 4,369 | 122 | 4,647 | 152 | 5,438 | Y |
| Assisted living facilities | 6 | 275 | NA | NA | NA | NA | Y | |
| AZ | Assisted living facilities | 1,509 | 24,500 | 1,524 | 24,002 | 1,242 | 22,848 | N |
| CA | Residential care facilities for elderly | 6,543 | 154,830 | 6,207 | 147,580 | 6,152 | 136,719 | N |
| CO | Assisted living residences | 525 | 13,799 | 538 | 14,291 | 551 | 13,868 | N |
| CT | Assisted living service agencies | 65 | NA | 63 | NA | 48 | NA | N |
| Residential care homes | 101 | 2,753 | 109 | 2,949 | 113 | 3,015 | Y | |
| DC | Community residence facilities | 200 | 1,866 | NR | NR | NR | NR | N |
| DE | Rest residential homes | 3 | NR | 6 | 160 | 4 | 99 | N |
| Assisted living | 29 | 1,738 | 27 | 1,300 | 18 | 927 | N | |
| FL | Assisted living facilities standard | 2,250 | 74,762 | 2,328 | 78,348 | 2,361 | 77,292 | N |
| Limited nursing services | ||||||||
| Assisted living extended congregate | ||||||||
| GA | Personal care homes | 1,687 | 25,434 | 1,648 | 25,563 | 1,606 | 24,437 | Y/M |
| HI | Assisted living facilities | 7 | 1,008 | 3 | 354 | 0 | 0 | N |
| Adult residential care home | 542 | 2,882 | 545 | 2,882 | 552 | 2,866 | ||
| Expanded care adult residential care home | 77 | 157 | ||||||
| ID | Residential and assisted living facilities | 266 | 6,160 | 253 | 5,815 | 226 | 5,185 | N |
| IL | Assisted living facilities | 120 | 5,830 | 24 | 1,667 | NA | NA | N |
| Shelter care facilities | 149 | 8,484 | 156 | 8,240 | 156 | 8,302 | N | |
| Shared housing | 13 | 92 | NR | NR | NR | NR | N | |
| IN | Residential care facilities | 147 | 11,767 | 140 | 11,555 | 127 | 10,098 | N |
| IA | Assisted living programs | 184 | 5,220 | 154 | 4,180 | 78 | 3,409 | N |
| KS | Assisted living | 191 | 7,971 | 129 | 5,658 | 80 | 4,521 | N |
| Residential health care facility | 98 | 2,918 | 43 | 2,355 | N | |||
| KY | Assisted living communities | 83 | NA | 73 | NA | 6 | NA | N |
| Personal care homes | 204 | 7,389 | 204 | 7,792 | 201 | NR | N | |
| LA | Personal care homes | 44 | 286 | 29 | 176 | 33 | 216 | N |
| Assisted living | 67 | 4,157 | 66 | 3,906 | 66 | 3,119 | N | |
| ME | Assisted living programs | 30 | 1,429 | 24 | 1,133 | 14 | 799 | N |
| Residential care facilities - 1 (I-IV 2004) Residential care facilities - II-IV |
711 | 7,593 | 473 192 |
1,711 5,220 |
509 189 |
1,799 4,094 |
N N |
|
| MD | Assisted living programs | 1,248 | 17,148 | 2,000 | 14,273 | 2,500 | NR | N |
| MA | Assisted living residences | 171 | 10,585 | 139 | 9,796 | 139 | 8,200 | Y |
| MI | Homes for the aged | 190 | 14,588 | 188 | 14,500 | NR | NR | N |
| Adult foster care: small group homes Adult foster care: large group homes Adult foster care: congregate homes |
4,265 | 32,915 | 4,353 | 33,317 | 3,735 | 26,015 | N N N |
|
| MN | Housing with services establishments | 931 | NA | 600 | NA | 592 | NA | N |
| MO | Residential care facilities I | 280 | 6,363 | 285 | 6,533 | 313 | 7,030 | Y |
| Residential care facilities II | 363 | 15,434 | 363 | 15,106 | 364 | 15,405 | Y | |
| MS | Personal care homes | 194 | 4,197 | 207 | 5,137 | 197 | 4,568 | Y |
| MT | Personal care facilities | 177 | 3,730 | 149 | 3,276 | 127 | 2,600 | N |
| NE | Assisted living facilities | 259 | 9,187 | 227 | 8,369 | 167 | 7,077 | N |
| NV | Residential care facilities for groups | 300 | 4,021 | 374 | NR | 326 | 4,581 | N |
| NH | Supported residential care facilities | 137 | 4,013 | 148 | 3,936 | 75 | 2,797 | N |
| Residential care home facilities | 67 | 769 | N | |||||
| NJ | Assisted living residences | 152 | 13,696 | 129 | 11,645 | 91 | 8,672 | Y |
| Assisted living programs | 13 | NA | 17 | NA | 16 | NA | Y | |
| Comprehensive personal care homes | 43 | 2,388 | 41 | 2,642 | 29 | 1,752 | Y | |
| NM | Adult residential care | 346 | NR | 305 | NR | 255 | NR | N |
| NY | Adult care homes | 431 | 32,859 | 449 | 34,805 | 453 | 33,589 | N |
| Enriched housing programs | 90 | 7,227 | 83 | 5,308 | 44 | 3,147 | N | |
| Residences for adults | 6 | 200 | 8 | 345 | 8 | 464 | N | |
| Assisted living programs | 57 | 3,315 | 53 | 3,034 | 45 | 2,522 | N | |
| NC | Adult care homes | 629 | 35,247 | 631 | 34,776 | 610 | 32,995 | Y |
| Family care homes | 648 | 3,642 | 682 | 3,816 | 743 | 4,134 | N | |
| Multi-unit housing with services | 23 | 1,053 | 20 | 1,538 | NR | NR | N | |
| ND | Basic care facilities | 46 | 1,490 | 47 | 1,490 | 43 | 1,436 | N |
| Assisted living facilities | 42 | 1,361 | NA | NA | NA | NA | N | |
| OH | Adult care facilities (3-16) | 712 | 5,666 | 805 | 5,783 | 860 | 6,017 | N |
| Residential care facilities (17+) | 510 | 36,255 | 462 | 31,937 | 439 | 28,139 | N | |
| OK | Residential care home | 103 | 3,358 | 210 | 8,620 | 147 | 8,478 | N |
| Assisted living centers | 115 | 6,308 | 8 | 1,253 | 87 | NR | N | |
| OR | Assisted living facilities | 190 | 12,566 | 180 | 11,998 | 138 | 8,661 | M |
| Residential care facilities | 236 | 8,504 | 220 | 8,227 | 187 | 6,805 | M | |
| PA | Personal care homes | 1,718 | 76,385 | 1,786 | 79,929 | 1,803 | 73,075 | N |
| RI | Assisted living facilities | 73 | 3,676 | 68 | 3,270 | 68 | 3,196 | N |
| SC | Community residential care facilities | 504 | 16,641 | 545 | 17,761 | 553 | 16,119 | N |
| SD | Assisted living centers | 162 | 3,360 | 153 | 3,084 | 127 | NR | N |
| TN | Assisted care facilities | 184 | 10,699 | 178 | 10,495 | 160 | 8,691 | N |
| Homes for the aged | 155 | 3,230 | 166 | 3,307 | 198 | 3,994 | N | |
| TX | Assisted living facilities | 1,378 | 42,245 | 1,324 | 41,424 | 1,304 | 39,596 | N |
| UT | Assisted living facilities type I | 92 | 1,678 | 108 | 1,886 | 116 | 1,954 | Y |
| Assisted living facilities type II | 49 | 2,800 | 43 | 2,460 | 26 | 1,221 | Y | |
| VA | Assisted living facilities | 636 | 34,598 | 659 | 34,200 | 663 | 32,768 | N |
| VT | Residential care facilities | 110 | 2,302 | 109 | 2,213 | 114 | 2,351 | N |
| Assisted living residences | 3 | 108 | NA | NA | NA | NA | N | |
| WA | Boarding homes | 538 | 24,498 | 525 | 23,830 | 498 | 22,140 | Y/M |
| WV | Personal care homes | NA | NA | 50 | 2,310 | 52 | 2,342 | N |
| Residential board and care homes | NA | NA | 82 | 1,498 | 80 | 1,197 | N | |
| Residential care communities | 3 | 88 | 3 | 88 | 3 | 88 | N | |
| Assisted living residences | 113 | 3,197 | NA | NA | NA | NA | N | |
| WI | Residential care apartment complexes | 151 | 6,001 | 122 | 4,452 | 94 | 3,211 | N |
| Community-based residential facilities | 1,359 | 21,374 | 1,350 | 21,242 | 1,340 | 21,064 | N | |
| WY | Assisted living facilities | 15 | 970 | 14 | 1,005 | 13 | 960 | N |
| Boarding homes | 17 | 315 | NR | NR | 26 | 419 | ||
| Total | 36,451 | 937,601 | 36,283 | 909,196 | 35,066 | 801,148 | ||
| NOTES: M: Moratorium NR: Not reported NA: Not aplicable AZ: Figures represent combined supply for three categories GA: CoN applies to facilities serving more than 24 residents |
||||||||
TABLE 2-2. Comparison of State Residential and Assisted Living Regulations: Characteristics
| State | Category | Size Definition1 |
Apt Required |
Sharing by Choice?2 |
Max # Occupants |
Size- Single |
Size 2+3 |
#/ Toilet |
#/ Bath |
|---|---|---|---|---|---|---|---|---|---|
| AL | Assisted living facilities | 2 | N | N | 2 | 80* | 130* | 6 | 8 |
| AK | Assisted living homes | 3 | N | Y | 2 | 80 | 140 | NS | NS |
| AR | Residential long-term care facilities | 3 | N | Y | 2 | 100 | 160 | 6 | 10 |
| Assisted living facilities | 3 | Y* | Y | 2 | 150 | 230 | 2 | 2 | |
| AZ | Assisted living facilities | <10, >10 | N | Y | 2 | 80/220* | 120/320 | 8 | 8 |
| CA | Residential care facilities for elderly | NS | N | Y* | 2 | ** | ** | 6 | 10 |
| CO | Assisted living residences | 3 | N | N | 2 | 100 | 120 | 6 | 6 |
| CT | Assisted living service agencies | NS* | Y | Y | * | * | * | * | * |
| Residential care homes | 2 | N | Y | 2 | 150 | 250 | 4 | 8 | |
| DE | Rest residential homes | NS | N | N | 4 | 100 | 80 | 4 | 4 |
| Assisted living | NS | N | Y | 2 | ** | ** | NA | NA | |
| FL | Assisted living facilities (standard) | 1 | N | N | 2* | 80 | 60* | 6 | 8 |
| Limited nursing services | N | 2* | 6 | 8 | |||||
| Assisted living extended congregate care | Y | 2 | 4 | 4 | |||||
| GA | Personal care homes | 2 | N | N | 4 | 80 | 60 | 4 | 8 |
| Community living arrangements | 2 | N | N | 2 | NS | NS | 4 | 4 | |
| HI | Assisted living facilities | NS | Y | Y | NS | 220 | NA | 1 | 1 |
| Adult residential care home | <6, >6 | N | N | 4 | 90 | 70 | 8 | 14 | |
| ID | Residential and assisted living facilities | 3 | N | N | 2 | 100 | 80 | 6 | 8 |
| IL | Assisted living facilities | 3 | N* | Y | NS | NS | NS | 1 | NS |
| Shelter care facilities | NS | NS | NS | 4 | 70 | 60 | 10 | 15 | |
| Shared housing | < 12 | N | NS | NS | NS | NS | 4 | 6 | |
| IN | Residential care facilities | NS | N | N | 4 | 100 | 80 | 8 | 8 |
| IA | Assisted living programs | 6 | N | Y | 2 | 240/70* | 340/70 | 1 | 1 |
| KS | Assisted living | 6 | Y | Y | NS | 200 | NS | 1 | 1 |
| KY | Assisted living communities | 5 | N | Y | 2 | 200 | 200 | NA | |
| Personal care homes | NS | N | N | 4 | NS | NS | 8 | 12 | |
| LA | Personal care homes | 2-8 | N | N | 2 | 100 | 70 | NS | NS |
| Assisted living | 2 | Y | Y | 2 | 250 | 250* | 1 | 1 | |
| ME | Assisted living programs | NS | Y | Y | NA | NA | NA | NA | NA |
| Assisted living residential care I-IV | NS | N | N | 2 | 100 | 160 | 6 | 10 | |
| MD | Assisted living programs | NS | N | N | 2 | 80 | 120 | 4 | 8 |
| MA | Assisted living residences | 3 | ** | NS | 2 | NS | NS | ** | ** |
| MI | Homes for the aged | > 20 | N | N | 4 | 100 | 80 | 8 | 15 |
| Adult foster care: small group homes | < 12 | N | N | 2 | 80 | 170 | 8 | 8 | |
| Adult foster care: large group homes | 13-20 | ||||||||
| MN | Housing with services establishments | 1 | ** | ** | ** | ** | ** | 10 | 20 |
| MO | Residential care facilities I & II | 3 | N | N | 4 | 70 | 70 | 6 | 20 |
| MS | Personal care homes | NS | N | N | 4 | 80 | 80 | 6 | 12 |
| MT | Personal care facilities | NS | N | N | 4 | 100 | 80 | 4 | 12 |
| NE | Assisted living facilities | 4 | N | N | 2 | 100 | 80 | 1* | 8* |
| NV | Residential care facilities for groups | 3 | N | N | 3 | 80 | 60 | 4 | 6 |
| NH | Supported residential care facilities | 2 | N | N | 2 | 80 | 140 | 6 | 6 |
| Residential care home facilities | 2 | N | N | 2 | 80 | 140 | 6 | 6 | |
| NJ | Assisted living residences | 4 | Y | Y | 2 | 150 | 230 | 1 | 1 |
| Assisted living programs | NS* | NA | Y | NA | NA | NA | NA | NA | |
| Comprehensive personal care | 4 | N | Y | 2 | 80 | 130 | NS | NS | |
| NM | Adult residential care | 2 | N | N | 2 | 100 | 80 | 8 | 8 |
| NY | Adult care homes | 5 | N | N | 2 | 100 | 160 | 6 | 10 |
| Enriched housing programs | 5 | Y | Y | NS | NS | NS | 3 | 3 | |
| Residence for adults | NS | N | N | 2 | 100 | 160 | 6 | 10 | |
| Assisted living programs | 5 | Y/N | Y/N | ** | ** | ** | ** | ** | |
| NC | Adult care homes | 7 | N | N | 4 | 100 | 80 | 5 | 10 |
| ND | Basic care facility | 5 | N | N | NS | 100 | 80* | 4 | 15 |
| Assisted living facilities | 5 | ** | ** | ** | ** | ** | ** | ** | |
| Adult care facilities | 3-16 | N | N | 4 | 80 | 60 | 8 | 8 | |
| OH | Adult care facilities | 3-16 | N | N | 4 | 80 | 60 | 8 | 8 |
| Residential care facilities | 17+ | N | N | 3 | 100 | 80 | 8 | 8 | |
| OK | Residential care home | NS | N | N | NS | 80 | 60 | 6 | 10 |
| Assisted living centers | 2 | N | N | 2 | ** | ** | 4 | 4 | |
| OR | Assisted living facilities | 6 | Y | Y | 1 | 220 | NA | 1 | 1 |
| Residential care facilities | 6 | N | N | 2 | 70 | 120 | 6 | 10 | |
| PA | Personal care homes | 4 | N | N | 4 | 80 | 60 | 6 | 15 |
| RI | Assisted living facilities | 2 | N | N | 2 | 100 | 80 | 8 | 10 |
| SC | Community residential care facilities | 2 | N | N | 4 | 80 | 60 | 8 | 10 |
| SD | Assisted living centers | 2 | N | N | 2 | 120 | 220 | 1 | 1 |
| TN | Assisted living facilities | NS | N | N | 2 | 80 | 160 | 6 | 6 |
| Homes for the aged | 1 | N | N | 2 | 80 | 80 | 6 | 6 | |
| TX | Assisted living facilities | 4 | N | Y | 4 | 100* | 80* | 6 | 6 |
| UT | Assisted living facilities type I | 2 | N | N | 2 | 100 | 160 | 6 | 10 |
| Assisted living facilities type II | 2 | N | Y | 2 | 120 | 200 | 4 | 10 | |
| VA | Assisted living facilities | 4 | N | N | 4 | 100 | 80 | 7 | 10 |
| VT | Residential care facilities | 3 | N | N | 2 | 100 | 80 | 8 | 8 |
| Assisted living facilities | NS | Y | Y | 2 | 225 | NA | 1 | 1 | |
| WA | Boarding homes | 7 | N | N | 2 | 80 | 70 | 8 | 12 |
| Assisted living facilities (Medicaid) | 7 | Y | NA | 1 | 220 | NA | 1 | 1 | |
| WV | Assisted living residences | 4 | -- | -- | 2 | 100 | 180 | 6 | 10 |
| Residential care communities | 17 | Y | Y | 2 | 300 | * | NS | NS | |
| WI | Residential care apartment complexes | NS | Y | Y* | 2 | 250 | NA | NS | NS |
| Community-based residential facilities | 5 | N | N | 2 | 100 | 80 | 8 | 8 | |
| WY | Assisted living facilities | NS | N | N | 2 | 120 | 80 | 2 | 10 |
| Boarding homes | |||||||||
| NOTES: M: Moratorium. NR: Not reported. NA: Not applicable. NS: Not specified. */** See state notes below.
AL: Private room with sitting areas, 160 square feet. Double room with sitting area, 200 square feet. AR: Rules for assisted living require apartments. AZ: Unit size figures are for rooms/apartment units. Apartments are required in centers that contract with the ALTCS (Medicaid) Program. CA: Choice whenever possible. No requirements for size of bedrooms. CT: Rules only address requirements for assisted living service agencies. Unit requirements are specified by the housing funding source. DE: Space requirements are not specified. FL: Facilities licensed after October 1999. Four persons may share a room in standard facilities licensed prior to 1999. IA: Additional habitable rooms in any unit must be at least 70 square feet. IL: Nursing homes converting a portion of a facility to supportive living must offer apartments with 160 square feet for single occupancy and 320 square feet for units shared by two persons. LA: Rules require 250 square feet of living space. Units with two bedrooms must have 190 square feet of living/dining/kitchen space and 120 square feet for each bedroom. MA: New construction requires private bathroom and kitchenette or access to cooking capacity. Existing construction requires private half bathroom. Full bathrooms may be shared by up to three residents. Bedrooms may be shared. MN: Licensing rules apply to service providers. Local codes apply to the building based on its use. NE: New construction facilities must have a toilet and sink adjoining each bedroom. Existing or new facilities may have shared toilet rooms provided the following: one toilet for every six beds in existing facilities; one toilet per four beds in new facilities. Facilities must provide a bathing facility consisting of a tub and/or shower adjacent to each room or provide a central bathing room. In existing facilities, rooms must have 80 square feet and in multiple occupancy rooms 60 square feet per bed with no more than four persons occupying a room. In new construction, apartments must have 150 square feet for one resident and 110 square feet for each additional resident. In existing facilities, apartments must have 120 square feet for one resident and 100 square feet for each additional resident. NJ: ALPs operate in conventional publicly subsidized senior housing complexes. NY: Assisted living programs comply with the relevant requirements under which the contracting facility is licensed (i.e., adult home or enriched housing program). ND: Rooms for three or more, 70 square feet per bed. There are no unit requirements for assisted living facilities. New rules define a living unit as a portion of an assisted living facility occupied as the living quarters of an individual who has entered into a lease agreement with an assisted living facility. OK: Regulations do not specify requirements for the size of bedrooms. TX: Type A facilities require 80 square feet for single occupancy and 60 square feet per resident in multiple occupancy rooms. UT: A single occupant unit without additional living space shall be a minimum of 120 square feet. A double occupant unit without additional living space shall be a minimum of 200 square feet. A single occupant bedroom in a unit with additional living space shall be a minimum of 100 square feet. A double occupant bedroom in a unit with additional living space shall be a minimum of 160 square feet.. WV: Multi-occupancy apartments must have at least 80 square feet of bedroom space per resident and no more than two residents may occupy an apartment. WI: Allows sharing with a spouse or a roommate chosen by the tenant. |
|||||||||
TABLE 2-3. Requirement for Facilities Serving Residents with Dementia
| TABLE 2-3. Requirement for Facilities Serving Residents with Dementia | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AL | AK | AZ | AR | CA | CT | CO | DE* | FL | GA | HI | ID | IL* | IN | IA | KS | KY* | |
| Training | X | X | X | X | X | X | X | X | X | X | |||||||
| Staffing | X | X | X | X | X | ||||||||||||
| Activities | X | X | X | X | X | X | |||||||||||
| Environment | X | X | X | X | X | X | X | X | X | ||||||||
| Disclosure | X | X | X | X | X | X | X | X | |||||||||
| Other | X | X | X | X | |||||||||||||
| LA | ME | MD | MA | MI | MN | MS | MO | MT* | NE* | NV* | NH | NJ | NM | NY* | NC | ND | |
| Training | X | X | X | X | X | X | X | X | X | X | X | X | X | ||||
| Staffing | X | X | X | X | X | X | X | X | X | ||||||||
| Activities | X | X | X | X | X | X | |||||||||||
| Environment | X | X | X | X | X | X | X | X | X | ||||||||
| Disclosure | X | X | X | X | X | X | X | X | |||||||||
| Other | X | X | X | X | X | X | X | X | |||||||||
| OH | OK | OR | PA | RI* | SC | SD* | TN* | TX | UT | VA | VT | WA | WV | WI | WY* | ||
| Training | X | X | X | X | X | X | X | X | X | X | X | X | X | X | |||
| Staffing | X | X | X | X | X | X | X | X | |||||||||
| Activities | X | X | X | X | X | X | X | X | X | ||||||||
| Environment | X | X | X | X | X | X | X | X | |||||||||
| Disclosure | X | X | X | X | X | X | X | X | X | ||||||||
| Other | X | X | X | X | X | ||||||||||||
| *STATE NOTES: DE: Facilities must develop policies to prevent wandering and safe storage of medications. IL: An Alzheimer's facility has been selected for one pilot program, and it must meet all applicable state, federal, and local requirements. KY: Lease agreements contain a description of special programming, staffing or training for serving clients with special needs. MT: Requirements for administrators. NE: Admission and discharge criteria. NV: Administrators have three years experience serving people with Alzheimer's disease or equivalent education and training. NY: See state summary. May not operate dementia units without written authorization from the Department of Health. RI: Philosophy and criteria for placement. SD: Also have fire safety/evacuation provisions. TN: An interdisciplinary team must review residents with early stage Alzheimer's disease to examine appropriateness of placement on a quarterly basis. WY: Facilities must provide cuing with guidance for ADLs for people who are intermittently confused and/or agitated and require occasional reminders to time, place, and person. |
|||||||||||||||||
TABLE 2-4. Requirements for Resident Agreements
| TABLE 2-4. Requirements for Resident Agreements | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AL | AK | AZ | AR | CA | CT | CO | DE | FL | GA | HI | ID | IL | IN | IA | KS | KY | |
| Services included in the basic rate | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X |
| Cost of the basic service package | X | X | X | X | X | X | X | X | X | X | X | X | X | X | |||
| Accommodations included | X | X | |||||||||||||||
| Terms of occupancy | X | X | X | X | X | X | X | ||||||||||
| Period covered | X | X | X | X | |||||||||||||
| Services beyond basic rate | X | X | X | X | X | X | X | X | X | X | X | X | |||||
| Cost of additional services | X | X | X | X | X | X | X | X | X | ||||||||
| Services not available/not covered | X | X | X | ||||||||||||||
| Temporary absence policy | X | X | X | X | X | ||||||||||||
| Payment/billing provisions | X | X | X | X | X | X | |||||||||||
| Statement of resident's rights | X | X | X | X | X | X | X | ||||||||||
| Admission/discharge criteria | X | X | X | X | X | X | X | ||||||||||
| Refund policy | X | X | X | X | X | X | X | X | X | X | |||||||
| Provisions for changing rates | X | X | X | X | X | X | X | X | X | ||||||||
| Termination provisions | X | X | X | X | X | X | X | X | |||||||||
| Purpose of deposits/advance payments | X | X | X | ||||||||||||||
| Grievance process | X | X | X | X | X | X | X | X | |||||||||
| Other | X | X | X | X | X | X | X | X | X | X | X | X | X | ||||
| LA | ME | MD | MA | MI | MN | MS | MO | MT | NE | NV | NH | NJ | NM | NY | NC | ND | |
| Services included in the basic rate | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | |
| Cost of the basic service package | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X |
| Accommodations included | X | X | X | X | X | X | X | ||||||||||
| Terms of occupancy | X | X | X | X | X | ||||||||||||
| Period covered | X | X | X | ||||||||||||||
| Services beyond basic rate | X | X | X | X | X | X | X | X | |||||||||
| Cost of additional services | X | X | X | X | X | X | X | X | X | ||||||||
| Services not available/not covered | X | X | X | X | |||||||||||||
| Temporary absence policy | X | X | X | X | |||||||||||||
| Payment/billing provisions | X | X | X | X | X | X | X | X | X | X | X | ||||||
| Statement of resident's rights | X | X | X | X | X | X | X | ||||||||||
| Admission/discharge criteria | X | X | X | X | X | X | X | X | X | X | X | X | |||||
| Refund policy | X | X | X | X | X | X | X | X | X | X | |||||||
| Provisions for changing rates | X | X | X | X | X | X | X | X | X | ||||||||
| Termination provisions | X | X | X | X | X | ||||||||||||
| Purpose of deposits/advance payments | X | X | X | ||||||||||||||
| Grievance process | X | X | X | X | X | X | X | ||||||||||
| Other | X | X | X | X | X | X | X | X | X | X | X | ||||||
| OH | OK | OR | PA | RI | SC | SD | TN | TX | UT | VA | VT | WA | WV | WI | WY | ||
| Services included in the basic rate | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X | ||
| Cost of the basic service package | X | X | X | X | X | X | X | X | X | X | X | X | X | ||||
| Accommodations included | X | X | X | ||||||||||||||
| Terms of occupancy | X | X | X | X | X | X | |||||||||||
| Period covered | X | X | X | X | |||||||||||||
| Services beyond basic rate | X | X | X | X | X | X | |||||||||||
| Cost of additional services | X | X | X | X | X | X | X | X | X | ||||||||
| Services not available/not covered | X | X | |||||||||||||||
| Temporary absence policy | X | X | X | X | X | X | |||||||||||
| Payment/billing provisions | X | X | X | X | X | X | |||||||||||
| Statement of resident's rights | X | X | X | X | X | X | X | X | |||||||||
| Admission/discharge criteria | X | X | X | X | X | X | X | X | X | X | X | ||||||
| Refund policy | X | X | X | X | X | X | X | X | X | ||||||||
| Provisions for changing rates | X | X | X | X | X | X | X | ||||||||||
| Termination provisions | X | X | X | X | X | X | X | X | |||||||||
| Purpose of deposits/advance payments | X | X | |||||||||||||||
| Grievance process | X | X | X | X | X | X | |||||||||||
| Other | X | X | X | X | X | X | X | X | X | X | |||||||
| STATE NOTES: AL: A statement that the facility is not staffed to provide skilled nursing or care for residents with severe cognitive impairments. AK: Duties and obligations of the resident. AR: Health care services available through home health agencies; parameters for pets; policy on acceptance of responsibility for personal funds and valuables; responsibility for medication; a copy of facility rules; and provisions for emergency transfers. CA: A monthly statement of services and charges; a statement acknowledging the acceptance or refusal to purchase the additional services shall be signed and dated by the resident or the resident's representative and attached to the admission agreement; an explanation of the use of third-party services within the facility that are related to the resident's service plan, including, but not limited to, ancillary, health, and medical services, how they may be arranged, accessed, and monitored, any restrictions on third-party services, and who is financially responsible for the third-party services; the facility's policy concerning family visits and other communication with residents; refund policy; conditions under which the agreement may be terminated; and an explanation of the resident's right to notice prior to an involuntary transfer, discharge, or eviction, the process by which the resident may appeal the decision and a description of the relocation assistance offered by the facility. CO: Transportation services; therapeutic diets; and whether the facility will be responsible for providing bed and linens, furnishing and supplies. There must also be written evidence that the facility has disclosed the policies and procedures (admissions; discharges; emergency plan and fire escape procedures; illness, injury or death; smoking; management of residents' funds; investigation of abuse and neglect allegations; and restrictive egress devices); method of determining staffing levels and the extent to which certified or licensed health professionals are available on-site; whether the facility has an automatic sprinkler systems; if the facility uses restrictive egress alert devices and the types of individual behaviors exhibited by persons needing such devices. DE: Transfer procedures, security, staff's right to enter a resident's room, resident rights and obligations, temporary absence policy, interim service arrangement during an emergency, obligations of the facility, and a listing of the resident's personal belongings. The financial areas include the party responsible for handling finances, obtaining equipment and supplies, arranging services not covered by the contract, disposing of belongings. FL: Statement of any religious affiliation; notice of transfer if the facility is not able to serve the resident. GA: Copy of house rules; provisions for ongoing resident assessments; provisions for transportation services; authorization to release medical records. ID: Whether or not the resident is responsible for his or her own medications; statement regarding managing personal funds; conditions for emergency transfers; permission to transfer information. IL: Statement of the annual licensing on-site review process; statement that Medicaid is not available for payment of services; description of the process for terminating or modifying the contract; the admission, risk management, and termination procedures; and policy concerning notification of relatives of changes in the resident's condition. IA: Statement regarding the impact of the fee structure on third-party payments and whether they are accepted; emergency response policy; staffing policy and whether staff are available 24 hours a day; whether nurse delegation will be used and staffing will be adapted to meet changing needs. KS: Negotiated service agreement; provider of services; agreement supports individual dignity, choice, privacy, etc.; addresses services refused by resident and resident's acceptance of risk. KY: Assisted living residences: 30-day notice of move-out for non-payment, assistance finding appropriate housing, other community rights, practices and procedures, policy concerning the ability to contract directly with outside agents, professionals, providers, or other individuals. LA: Authority of the licensing agency to review records; responsibilities for overseeing medical care; purchasing supplies and equipment. Must allow review by an attorney. MD: Includes a clear and complete reflection of commitments and actual practices; level of care for which the facility is licensed; obligations of all parties for arranging for medical care and other provisions (see summary). MA: Sponsor's covenant to comply with applicable laws; reasonable rules for staff, management, and resident behavior, and limits on what the residence will as well as policy on self-administration of medication. MI: AFC: Assurance of provision of care, supervision, and protection; agreement to provide necessary intake information and current health appraisal; statement of how funds and valuables are handled; statement that the home is licensed to provide care. MO: Right to make treatment decisions; provisions in a medical emergency; state laws relating to advance directives. MT: Availability of skilled nursing and other professional services from third-party payers; specific assistance available with ADLs. NE: Included in the terms of occupancy requirement. NH: Notification required for involuntary and emergency transfer. NJ: Some information is provided during admission interviews. NY: Includes a list of services, material, equipment required by law; guarantee that supplemental services are made at the resident's option; offer to manage funds received from public sources; statement that the resident will provide a signed medical statement and inform operator of changes in health conditions, status, or medications. NC: Policy on smoking, alcohol consumption, and visitation. OH: A statement is included about discharge of residents when skilled nursing needs exceed their capacity. OK: Conformity with state law. PA: Amount of personal needs allowance; method of payment for long distance calls; financial management arrangements; explanation of annual screening and medical evaluation requirements. RI: Also includes shared space and facilities, special care provisions, resident responsibilities and house rules, and evaluation and service plan. A general provision called financial terms would cover cost of services, additional charges, and refunds. SD: Policies for protection of personal funds; list of names, addresses, and numbers of client advocates; how to contact the resident's physician; how to apply for Medicare/Medicaid. TN: Information on the cost of services is provided to residents but it is not part of the agreement. The agreement includes the procedure for handling transfers and discharges. TX: See summary. Some provisions are part of the disclosure requirement or part of the written policies of the facility. UT: Notice that the state has the authority to examine resident records. VT: See state summary. VA: Stipulation about the transfer of ownership of any property, real estate, or money to the facility; description of the type of staff, services available and the hours of service. WA: Rules of operation. WV: 1. Personal care homes: house rules; how emergencies are addressed; arrangement for transportation; procurement and payment for medications; storage and administration of medications. 2. Residential board and care homes: how health care will be provided; provide copies of all inspection reports; how to access activities and assurances that the home offers services to meet identified needs. 3. Residential care communities: procurement and payment for medications; storage and administration of medications; assurance that the resident is not liable for undisclosed costs; assurance that the individual's needs will be met. WI: 1. CBRFs: bed hold fee. 2. RCAC: Some of the requirements are posted and others are included in a service agreement. Activity and social connections the resident will be assisted in maintaining. WY: Managers are required to establish policies in the specified areas that are available to residents and staff on items that are normally specified in resident agreements. |
|||||||||||||||||
TABLE 2-5. Staff Training Requirements (see note)
| State | Initial | Annual | State | Initial | Annual | State | Initial | Anaual |
|---|---|---|---|---|---|---|---|---|
| AL | Topics | Topics | KY | Topics | Not specified | ND | Topics | Not specified |
| AK | Topics | 12 hours | LA | Topics | Annual plan | OH | Training course | Not specified |
| AZ | Topics/hours* | 12 hours | ME | Complete course | 8 hours/2 years | OK* | 8 hours | 8 hours |
| AR | Topics | 6 hours | MD | Topics* | Topics | OR | Topics | Not specified |
| CA | Topics | Plan | MA | 7 hours | 10 hours | PA | Topics | Not specified |
| CO | Topics | Topics | MI | Topics | Not specified | RI* | Topics | Not specified |
| CT | 10 hours/topics* | 6 hours | MN | Competency test | Not specified | SC | Topics | General |
| DE | Topics | 12 hours | MS | Topics | Quarterly | SD | Topics | Not specified |
| DC | 40 hours | 12 hours | MO* | 1 hour | Not specified | TN | Not specified | Not specified |
| FL | 26 hours* | Not specified | MT | Topics/16 hours* | Not specified | TX | 16 hours | 6 hours |
| GA | Topics | 16 hours | NE | Topics | 12 hours | UT | Topics | Not specified |
| HI | Topics | 6 hours | NV | General | 8 hours | VT* | Topics | 20 hours |
| ID | 8 hours | 8 hours | NH | Topics | Topics | VA | Topics | 12 hours |
| IL | 20 hours | 12 hours | NJ | Complete course | 20 hours/2 years* | WA* | Topics/competency test | Not specified |
| IN | Topics | Topics/hours* | NM | Complete course | Topics | WV | Topics | Topics |
| IA | Plan on file | Not specified | NY | Complete course | Not specified | WI | Topics | Not specified |
| KS | Topics | Topics | NC | Complete course | Not specified | WY | Topics | Not specified |
| NOTE: Rules specifying a number of hours also include topics that are covered. Rules listing topics only do not specify how many hours of training are needed. *STATE NOTES: AZ: Hours/topics vary by level of licensing. CT: Aides must pass a competency exam. FL: Core training for staff is 26 hours. Additional hours are required for specific tasks or settings e.g., medication assistance (4) and extended congregate care (2). IN: Nursing staff, 8 hours per year; non-nursing staff, 4 hours per year. MD: For Medicaid waiver programs, 8 hours on medication administration is also required. MO: Complete course for medication administration. MT: Topics are listed for category A and 16 hours of training in services provided by category B facilities. NJ: 20 hours every 2 years; medication aides, 10 hours every 2 years. OK: For residential care homes. RI: Medicaid waiver: one hour orientation; 12 hours annual. VT: For residential care homes. WA: Additional requirements for Medicaid providers. |
||||||||
TABLE 2-6. Comparison of State Reimbursement Policy
| State | Coverage | Payment Method |
Rates | Rates Include R&B |
R&B Limits |
Family Supplement |
Personal Needs Allowance |
SSI Payment Standard1 |
|
|---|---|---|---|---|---|---|---|---|---|
| Date | Method | ||||||||
| AL | NA | Waiver submitted | TBD | $30.00 | $564.00 | ||||
| AK | 1993 | Waiver | Tiered | $70.54-$93.70 | N | No | No policy | $100.00 | $907.00 |
| AZ | 1989 | Waiver | Tiered | $34.67-$87.10* | Y | $497.10 | Y | $66.90 | $564.00 |
| AR | 1993 2003 |
State plan Waiver |
Care plan Tiered |
$790.40 cap $39.51-$49.91 |
N | No | No policy | $30.00 | $564.00 |
| CA | Planning | Planned | TBD | $111.00 | $853.00 | ||||
| CO | 1984 1987 |
Waiver State funds |
Flat | $36.03/day | N | $518 | Y | $46.00 | $564.00 |
| CT | 2003 NR |
Waiver State funds |
Tiered | $65/day cap | N | % of income* | N | $164.00 | $1692 cap* |
| DE | 1999 | Waiver | Tiered | $940-$1460 | N | $598 | N | $106.00 | $704.00 |
| DC | Approved | Waiver | TBD | No policy | $70.00 | $564.00 | |||
| FL | 1997 2001 |
Waiver State funds |
Flat Flat |
$28/day $9.28/day |
N | No | Y | $54.00 | $642.40 |
| GA | 1981 | Waiver | Flat | $31.04/day | N | $475 | Y | $89.00 | $564.00 |
| HI | 2000 | Waiver | Flat | $58.46/day* | N | $418 | No policy | $150.90 | $568.90 |
| ID | 1999 2000 |
Waiver State plan State funds |
Care plan Care plan |
Capped/NF cost $921.92* |
N N |
$497* $497* |
Y | $67.00 | $564.00 |
| IL | 1999 | Waiver | Regional variations | $45.54-$61.94 | N | $474* | N | $90.00 | $564.00 |
| IN | 2001 | Waiver | Tiered | $45.86-$61.68 | N | $512 | No policy | $52.00 | $564.00 |
| IA | 1990 | Waiver | Care plan | Cap of $1,025 | N | No | Y | $30.00 | $564.00 |
| KS | 1997 | Waiver | Care plan | Varies | N | No | Y | $30.00 | $564.00 |
| KY | NA | NS | $906.00 | ||||||
| LA | NA | Planned | NS | $564.00 | |||||
| ME | 1970s 1990 |
State funds State plan Waiver |
Care plan Cost based/ case-mix |
Varies | & | % of income | Y | $50.00 | $574.00 |
| MD | 1993 1986 |
Waiver State funds |
Tiered | $1611-$2031* | Y | $420 | N | $60.00 | $564.00 |
| MA | 1992 | State plan | Flat | $37.75 per day | N | N | No policy | NS | $1018.00 |
| MI | 1983 | State plan | Flat | $174.38 | N | N | Y | $44.00 | $724.30* $721.50 |
| MN | 1988 1991 |
Waiver State funds |
Case-mix | $1029-$2392* | N | $674 | Y | $72.00 | $752.00 |
| MS | 2001 | Waiver | Flat | $33.18/day | N | $520 | No policy | $44.00 | $564.00 |
| MO | 1993 1973 |
State plan State funds |
Care plan | Varies/capped at NF cost | N | N | Y | $25.00 | $720.00 $856.00 |
| MT | 1994 | Waiver | Care plan | $520-$1800* | N | $525 | $100.00 | $625.00 | |
| NE | 1998 | Waiver | Flat (rural/urban variations) | $1520-2150* | Y | $504 | N | $60.00 | $564.00 |
| NV | 1993 | Waiver | Flat | $20, $45, $60/day | N | N | No policy | $88.00 | $914.00 |
| NH | 1999 | Waiver | Flat | $50/day $1250/month* |
N Y |
N Y |
Y | $50.00 | $758.00 |
| NJ | 1997 | Waiver | Setting* | $2130.55-$2430.55 | Y | $631.50 | Y | $80.50 | $714.05 |
| NM | 1996 | Waiver | Flat | $50.50/day | N | $1024 | No policy | $30.00 | $664.00 |
| NY | State plan | Case-mix | Varies by county and case-mix | N | N | Y | $70.00* $115.00 |
$969.00- $999.00* |
|
| NC | 1995 | State plan | Case-mix | Varies/$49.62 max* | N | $1066 | Y | $46.00 | $1132.00 |
| ND | Waiver State funds |
Care plan Care plan |
$80/day cap $40/day cap |
N N |
$375 NR |
Y Y |
$60 NS |
$564.00 | |
| OH | NA | $50.00 | $850.00 | ||||||
| OK | NA | $50.00 | $564.00 | ||||||
| OR | 1990 | Waiver | Tiered | $1144-$2399 | Y | $455.70 | N | $110.00 | $565.70 |
| PA | 2000 | Waiver demo | Care plan | Cap 80% of NF | N | $898.30 | N | $60.00 | $958.30 |
| RI | 1999 |
Waiver | Flat Flat |
$37/day* $1400 |
N Y |
N N |
N | $100.00 | $1159.00 |
| SC | 2002 | State plan | Flat | $12.80/day | N | $865.00 | N | $47.00 | $912.00 |
| SD | 1988 | State funds Waiver |
Flat Flat |
$1094 $43.92/day |
Y | $534.00 | N | $30.00 | $1094.00 $564.00 |
| TN | NA | NS | $564.00 | ||||||
| TX | 1994 1985 |
Waiver State funds |
Tiered | $23.21- $59.88/day |
N | $479 | N | $85.00 | $564.00 |
| UT | 2000 | 1915 (a) | Negotiated | Negotiated | Y | NA | Y | $45.00 | $560.00 |
| VA* | NA | $62.00 | $833.00- $958.00 |
||||||
| VT | 1996 1999 |
Waiver State plan |
Tiered Flat |
$42-$55 $30.25* |
N | $564 | N | $47.76 | $592.66 III $735.94 IV |
| WA | 1991 | Waiver | Tiered | See summary | Y | $453.16 | N | $58.84 | $564.00 |
| WV | 2004 | Waiver approved | $69.00 | $627.00 | |||||
| WI | 1997 | Waiver State funds |
Care plan Care plan |
Cap $77.81* No cap |
N | $626.77 | Y | $65.00- $240.00 |
$647.78* |
| WY | 2001 | Waiver | Tiered | $32-$40/day | N | N | No policy | NS | $564.00 |
| GENERAL NOTES: TBD: To be determined NR: Not reported NA: Not applicable NS: Not specified
CT: Pilot program with the Housing Finance Agency to create affordable assisted living. The SSI rate in residential care homes is based on the rate for the facility but cannot exceed $1,692 less a personal needs allowance of $90.70. The payment is lower in the assisted living pilot. The PNA is $164 and there is a meal allowance of $300 and up to a $400 allowance for rent. HI: This rate is for facilities of six or more beds; the rate for five or less is $1066.90. ID: The room and board amount is a suggested cap. State plan service cap is based on a rate of $13.40 an hour, maximum 16 hours per week. IL: In addition to the Medicaid payment, participating facilities receive an average of $97 a month in food stamp benefits. MD: Additional amounts are allowed for assistive equipment and environmental modifications which may be more likely to be applied to in-home settings. MI: Payment rate for Homes for Aged is $724.30; Adult Family Care, $721.50. PNA is the same for both categories. MN: Statewide average costs with caps that vary by county. MT: Actual rate depends on a scoring of functional needs. NE: Rates vary by urban/rural and single/double occupancy. NH: Elderly housing with services sites receive $50 a day; licensed facilities receive $1,250 a month. NY: Payment standards and the PNA varies by groupings of counties. NC: Rate varies using a base rate and additional components determined by the combination of ADL needs. RI: A regular waiver and a pilot program are operating. The room and board charge for both programs is set by the facility. The regular waiver pays the difference between $1,400 and the room and board charge. Room and board is not related to the Medicaid payment under the pilot waiver. SSI beneficiaries participating in the two waivers retain a PNA of $100. SSI beneficiaries not in the waiver retain a PNA of $55. Facilities receive one month prospective payment and would hold the unit for the remainder of the month. VA: The state continues to support residents with state funds who were formerly covered by a Medicaid waiver that was not renewed. The SSI benefit varies by grouping of the counties. VT: $30.25 for residents receiving Assistive Community Care Services (ACCS); the higher tiers include ACCS and Medicaid waiver services. Room and board of $564 is allowed in facilities participating in the ACCS program. The SSI rates for Level III and IV are in facilities that do not participate in ACCS. WI: Actual rates negotiated by counties. Cap is based on 85 percent of the cost of nursing facility care. Family supplementation allowed by the state agency; counties set their own policy. PNA amounts are also set by counties. Residents in certified RCACs may qualify for an additional state supplement of $95.99 if they have exceptional needs. WV: A pilot program in public housing in four counties was approved in August 2004. |
|||||||||
Section 3. State Summaries
Notes on State Summaries
Each state summary includes the regulatory or statutory citation and category name and includes information on the following, when available:
- a description of the state’s approach to assisted living or board and care,
- the term(s) used to define facilities,
- unit requirements,
- tenant admission and retention policies,
- services that may be provided and negotiated risk agreements,
- dietary provisions and policies,
- tenant agreements,
- provisions for people with dementia,
- medication assistance,
- financing, including the availability of Medicaid reimbursement for low-income residents,
- nursing facility level of care,
- staffing requirements,
- training requirements for staff,
- background checks,
- monitoring of facilities, and
- licensing fees.
The information for each state is based on statutes, regulations, and draft regulations. Information based on draft material is presented to indicate the potential direction of state policy. Final rules may vary from the source material. The Medicaid nursing home level-of-care criteria are included for all states to allow comparison with admission/retention criteria and highlight the functional eligibility requirements for home and community based services waivers (several states use the Medicaid state plan to pay for services in residential settings, which has different financial and functional eligibility criteria than waivers).
Alabama
Citation
Assisted Living: Chapter 420-5-4,
Specialty Care Assisted Living Facilities: Chapter 420-5-20
General Approach and Recent Developments
Sections of the regulations governing building requirements for assisted living facilities and specialty-care facilities were revised in July 2003. Revisions to incident investigations were effective in 2004. The regulations license three categories of facilities:
- Congregate assisted living facilities serve seventeen or more adults;
- Group assisted living facilities serve four to 16 adults; and
- Family assisted living facilities serve two to three adults.
Specialty-care facilities must receive a separate certification from the Board of Health.
The Department of Health is evaluating whether the regulations adequately address safety related issues, e.g., if residents have recurring problems with falls, should the rules limit admission/retention or should the staffing and training requirements be changed. The Department, Board of Nursing and Legislature are considering proposals to allow unlicensed staff to administer medications either through nurse delegation or creation of medication technician category.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted living facilities | 241 | 7,260 | 302 | 9,140 | 304 | 8,000 |
| Specialty-care facilities | 94 | 2,616 | 25 | 598 | NA | NA |
Definition
Assisted living facility “means an individual, individuals, corporation, partnership, limited partnership, or any other entity that provides or offers to provide residence and personal care to individuals who are in need of assistance with activities of daily living. A facility shall not be deemed to meet the definition of assisted living facility unless a residence and personal care services are provided to two or more individuals not related to the owner or administrator. To be deemed related to the owner or administrator for the purposes of this definition, an individual residing at the facility and receiving personal care must be the parent, sibling, grandparent, great-grandparent, child, grandchild, niece, nephew, aunt, uncle, first cousin, or spouse of the owner or administrator, or must stand in such relationship to the owner’s or administrator’s spouse.
Building requirements vary for congregate assisted living facilities, group assisted living facilities and family assisted living facilities.
“Specialty Care Assisted Living Facility” means a facility that meets the definition of Assisted Living Facility but which is specially licensed and staffed to permit it to care for residents with a degree of cognitive impairment that would ordinarily make them ineligible for admission or continued stay in an assisted living facility.
Unit Requirements
The regulations do not require separate living and sleeping quarters. Private bedrooms without sitting areas must provide 80 square feet, and double rooms 130 square feet. If sitting areas are included, private rooms must be 160 square feet and double rooms 200 square feet. Bathtubs or showers must be available for every eight beds; lavatories and toilets for every six beds. Lockable doors are permitted. No more than two people may share a room.
Admission/Retention Policy
Facilities may not admit nor retain a resident who requires medical care, skilled nursing care, is severely cognitively impaired, or requires any care beyond assistance with activities of daily living unless the resident is capable of performing and does perform all tasks related to his or her own care; or is incapable of performing some or all tasks related to his or her own care due to limitations of mobility or dexterity but has sufficient cognitive ability to direct his or her own care and is able to direct others and does direct others to provide the physical assistance needed to complete such tasks, and the facility staff is capable of providing such assistance and does provide such assistance.
The statute allows residents to be served who need medical care, medication administration, or skilled nursing care due to an injury as long as the need does not exceed 90 days and arrangements are made for care from “properly licensed individuals.”
Facilities may not serve individuals with acute infectious pulmonary disease, such as influenza or active tuberculosis, or other communicable diseases, and individuals with infected draining wounds until the wound is sufficiently healed.
Nursing Home Admission Policy
A physician must certify the need for continuing stay. Nursing care is required on a daily basis that as a practical matter can only be provided in a nursing facility on an in-patient basis. Residents must need two of the following services on a regular basis:
-
Administration of a potent and dangerous injectable medication and intravenous medications and solutions on a daily basis or administration of routine oral medications, eye drops, or ointment.
-
Restorative nursing procedures (such as gait training and bowel and bladder training) in the case of residents who are determined to have restorative potential and can benefit from the training on a daily basis.
-
Nasopharyngeal aspiration required for the maintenance of a clear airway.
-
Maintenance of tracheostomy, gastrostomy, colostomy, ileostomy, and other tubes indwelling in body cavities as an adjunct to active treatment for rehabilitation of disease for which the stoma was created.
-
Administration of tube feedings by naso-gastric tube.
-
Care of extensive decubitus ulcers or other widespread skin disorders.
-
Observation of unstable medical conditions required on a regular and continuing basis that can only be provided by or under the direction of a registered nurse.
-
Use of oxygen on a regular or continuing basis.
-
Application of dressing involving prescription medications and aseptic techniques and/or changing of dressing in noninfected, post-operative, or chronic conditions.
-
Comatose patient receiving routine medical treatment.
Services
Assisted living facilities must provide personal care for bathing, oral hygiene, hair and nail care, shaving, laundry services, personal safety and assistance making and keeping appointments. Facilities may provide for general observation and health supervision and may arrange for or assist residents in obtaining medical attention or nursing services when needed. Home health may be provided by a certified agency as long as residents do not require hospital or nursing home care. A written plan of care is required at the time of admission based on the medical examination, diagnoses, and recommendations of the resident’s treating physician. It shall document the personal care and services required from the facility. Plans of care are kept current and reviewed and updated at least annually by the attending physician.
Dietary
Menus must be planned and posted one week in advance. Alternate food selections must be available for residents on medically prescribed diets, including hypertension, diabetes, hyperlipdemia, and modified consistency diets. A dietician is available for residents who need special diets. Congregate assisted living facilities must be under the direction and supervision of a full- or part-time professionally qualified dietician or a consulting dietician.
Agreements
Agreements must be signed prior to or at the time of admission and include: basic charges (room, board, laundry, personal care, and services); period covered; services for which there are special charges; refund policy and termination provisions; bed hold policy and process; documentation that the resident and sponsor understand that the facility is not staffed and not authorized to perform skilled nursing services nor to care for residents with severe cognitive impairment and that the resident and sponsor agree that if the resident should need skilled nursing services or care for a severe cognitive impairment as a result of a condition that is expected to last for more than ninety days, that the resident will be discharged by the facility after prior written notice; and a reminder to the resident or sponsor that the local ombudsman may be able to provide assistance if the facility and the resident or family member are unable to resolve a dispute about payment of fees or monies owed.
Provisions for Serving People with Dementia
No facility may serve anyone with Alzheimer’s disease or dementia unless they have a specialty-care facility license. Facilities are allowed to serve residents who do not have dementia if they have readily available egress from the facility. Specialty-care facilities must have a medical director, at least one registered nurse who is responsible for staff training, resident assessment, and plans of care and medication. Minimum ratios of awake staff are specified: two staff for less than 16 residents; one staff for every eight residents for facilities with 16 or more residents from 7 a.m. to 9 p.m.; three staff from 9 p.m. to 7 a.m. for facilities with 17-24 residents; and three staff plus one for every 16 residents for facilities serving 25 or more residents. Activity programs are required. Residents must have a Physical Self Maintenance Scale score of 23 or less and may not have unmanageable behavior problems.
Continuing Education. All staff members of a specialty care assisted living facility shall have at least six hours of continuing education annually. All direct care staff, including the administrator, shall have initial training and refresher training as necessary. An RN shall identify staff refresher training needs and shall provide or arrange for needed training. Prior to providing any resident care, all staff shall complete the DETA (Dementia Education and Training Act) Brain Series Training developed by the Alabama Department of Mental Health and Mental Retardation or equivalent training approved by the State Health Officer. In addition to the training areas for staff in assisted living facilities, special care staff members must receive training on: resident fire and environmental safety; specialty care assisted living facilities Chapter 420-5-20; understanding the aging mind; basic brain function; common neuro-psychiatric disorders in the elderly; basic evaluation of the dementia patient; cognitive symptoms of dementia; psychiatric symptoms of dementia; behavioral problems associated with dementia; end of life issues in dementia; dementia other than Alzheimer’s; research and dementia; nutrition and hydration needs of the resident with dementia to include feeding techniques; safety needs of residents with dementia.
Medication Administration
Assistance is limited to reminders, reading container labels to the resident, checking the dosage, and opening containers. Licensed nurses are allowed to administer medications for residents who are not aware of their medications.
Residents who are aware of their medications may self-administer medications. A licensed nurse may administer medication to a resident who is capable of self-administration. Facility staff may assist with the self-administration of medication. Assistance includes reminding, physically assisting by opening or helping to open a container holding oral medications, offering liquids, physically bringing a container of oral medications. Assistance does not include giving injections, administering eye drops, eardrops, nose drops (unless the resident is aware but has dexterity limitations), inhalers, suppositories, or enemas, telling or reminding a resident that it is time to take a PRN, or as needed medication, crushing or splitting medications, placing medications in a feeding tube, or mixing medications with food or liquids.
Public Financing
A Medicaid waiver to cover people with dementia in assisted living was approved in 2003 by CMS but has not been implemented due to budget limitations. The legislature is considering funding in 2004. The program would service SSI recipients and people who qualify under the 300 percent option. The personal needs allowance would be between $65 to $72 per month and room and board would be capped at about $500 a month. The program planned to pay providers $66 per day or $2,046 per month--total monthly reimbursement $2546. If implemented, the waiver would serve 500 people in Year 1, 650 in Year 2, and 700 in Year 3. Families would be allowed to supplement the room and board charges.
Staffing
An assisted living facility shall employ sufficient staff and ensure sufficient staff are on duty to meet the care needs of all residents 24 hours a day, seven days a week. This means that an assisted living facility must not only have a sufficiently large number of staff members to meet the care needs of all residents, it must also manage and direct the activities of staff members in a manner that results in adequate care being provided. An assisted living facility shall likewise employ sufficient staff, ensure sufficient staff are on duty, and manage and direct staff activities in a manner that results in maintenance of a neat, clean, orderly, and safe environment at all times.
Training
Administrators. Legislation passed in 2001 creates a Board of Examiners for Assisted Living Administrators. Within 18 months of passage, all administrators must be licensed which includes passing an examination and meeting education and training requirements. Existing rules require that administrators have 6 hours of continuing education annually.
Staff. Administrators and direct care staff receive initial and refresher training on state law and rules on assisted living facilities; identifying and reporting abuse, neglect and exploitation; special needs of the elderly, mentally ill, and mentally retarded; basic first aid; advance directives; protecting resident confidentiality; safety and nutritional needs of the elderly; resident fire and environmental safety; and identifying signs and symptoms of dementia.
Background Check
Not specified. Facilities are required to check the nurse abuse registry before hiring staff.
Monitoring
Facilities are monitored through licensing review and periodic inspections by the Board of Health depending on funding for inspectors. Incidents are reported through a hotline. Written reports may be requested to determine the cause of an incident or if the facility acted appropriately. Facilities are currently inspected every 2 to 3 years. The oversight agency is seeking additional staff to permit annual inspections.
Fees
Licensure fees for assisted living facilities and specialty-care assisted living facilities rising to the level of intermediate care are $200, plus $15 per bed.
Alaska
Citation
Assisted living homes: Alaska Statute §47.33.005 et seq.; 7 Alaska Administrative Code §75.010 et seq.; 7ACC 43:1050 (g)
Medicaid waivers: Amounts of reimbursement for HCB services General Approach and Recent Developments
General Approach and Recent Developments
During 2003-2004, Alaska has been developing plans to consolidate state statutes for licensing. The changes are expected to be completed in 2004 and effective by the end of 2005. The Assisted Living Licensing Unit is being transferred from the Division of Senior and Disability Services to the Division of Public Health and should be completed by July 2004.
The State continues to support the expansion of assisted living homes into rural areas. Assistance with planning and technical support is provided wherever possible. One area of concern in some of the assisted homes is the language differences between administrators, staff and residents. Plans to evaluate the scope of this concern and to develop a plan of action are under way. Key informants noted there has been an increase in assisted living homes that have specialized in providing care to specific populations, such as residents with dementia, residents with physical disabilities, behavioral health residents and men-only or women-only homes.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted living homes | 162 | 1,650 | 143 | 1,497 | 123 | 1,346 |
Definition
The law creates “Chapter 33. Assisted Living Homes” to emphasize that assisted living serves as the resident’s home. The statute applies to residential facilities serving three or more adults who are not related to the owner of the residence by blood or marriage; that provide housing and food service; and that provide, obtain, or offer to provide or obtain assistance with activities of daily living, personal assistance (help with IADLs, obtaining supportive services [recreational, leisure, transportation, social, legal, etc.], awareness of the resident’s whereabouts when traveling in the community, and monitoring activities), or a combination of ADL assistance and personal assistance.
The term “adult foster care” is the prior name used for what is now known, and licensed as, assisted living homes. Nothing in the regulations prohibit an assisted living home that is licensed and that serves five or fewer residents from using the term “adult foster home” or “assisted living foster home” in connection with that facility.
Unit Requirements
Single occupancy units must provide 80 square feet and double occupancy units, 140 square feet. No more than two residents may share a room. A facility must meet life safety code requirements applicable for buildings of its size. Homes for six or more people must meet applicable state and municipal standards for sanitation and environmental protection. Because of the size of the State and the geographic variation within it, the licensing standards are based on community and neighborhood standards rather than a statewide standard. This allows homes to be licensed that are consistent with prevailing local housing standards.
Admission/Retention Policy
Residents who have exceeded the 45 consecutive day limit for receiving 24-hour skilled nursing (see below) may continue to live at the home if the home and the resident or resident’s representative have consulted with the resident’s physician and discussed the consequences and risks. In addition, a revised plan without 24-hour nursing must have been reviewed by a registered nurse. Terminally ill residents may continue to reside in the residence if a physician certifies that the person’s needs are being met.
Evacuation requirements are included in life safety code standards and facility procedures for emergency evacuation drills.
Since the regulations governing admission/retention are broad, waivers of the requirements are not needed. The rules do allow variances of any provision of the chapter that will promote aging in place and meet the goals of the rules.
Nursing Home Admission Policy
Alaska implemented a new assessment tool, Consumer Assessment Tool (CAT), in May 2004 for the Medicaid waiver program. Individuals meet the level of care criteria if they:
- Receive a listed nursing service daily;
- Receive a nursing service less than daily and require limited, extensive, or total assistance with two ADLs (bed mobility, transfer, locomotion, eating, toilet use, personal hygiene, walking, bathing);
- Have impaired cognition and require limited, extensive or total assistance with two ADLs; or
- Have behaviors (wandering, verbal or physical abuse, socially inappropriate) and require limited, extensive, or total assistance with two ADLs.
Services
Each resident must have an assisted living plan (developed within 30 days of move-in and approved by the resident or their representative) that identifies strengths and weaknesses performing ADLs, physical disabilities and impairments, preferences for roommates, living environment, food, recreation, religious affiliation and other factors. The plan also identifies the ADLs with which the resident needs help, how help will be provided by the home or other agencies, and health-related services and how they will be addressed. Health-related services include assistance with self-administration of medication, intermittent nursing services, 24-hour skilled nursing for 45 days, and hospice services.
The plan must promote the resident’s participation in the community and increased independence through training and support, in order to provide the resident with an environment suited to the resident’s needs and best interests.
Negotiated risk is addressed during the care planning process. The plan must recognize the responsibility and right of the resident or the resident’s representative to evaluate and choose, after discussion with all relevant parties, including the home, the risks associated with each option when making decisions pertaining to the resident’s abilities, preferences, and service needs; and recognize the right of the home to evaluate and to either consent or refuse to accept the resident’s choice of risks.
The plan must also identify the resident’s reasonable wants and how those will be addressed. If health related services are provided or arranged, the evaluation must be done quarterly. If no health related services are provided, an annual evaluation is required. Assisted living homes may provide intermittent nursing services to residents who do not require 24-hour care and supervision. Intermittent nursing tasks may be delegated to unlicensed staff for tasks designated by the board of nursing. Twenty-four hour skilled care may be provided for not more than 45 consecutive days.
Hospice services may be provided. Homes are required to have copies of living wills or advance directives for residents who have them.
Dietary
An assisted living home shall offer three balanced, nutritious meals and at least one snack daily at consistent times. A home shall ensure that the meals and snacks offered include the recommended number of servings of each food type set out in the U.S. Department of Agriculture publication, The Food Guide Pyramid, as revised October 1996 and adopted by reference. The home shall offer a wide variety of food that includes fresh fruits and vegetables as often as possible. Additionally, the home shall consider each resident’s health-related or religious restrictions, cultural or ethnic preferences in food preparation, and preference for smaller portions, as reflected in the resident’s residential services contract.
Agreements
A residential services contract must be signed prior to move-in that describes the services and accommodations; rates charged; rights; duties and obligations of the resident; policies and procedures for termination of the contract; amount and purpose of advance payments; and refund policy.
A person may not begin residency in an assisted living home unless a representative of the home and either the person or the person’s representative sign a residential services contract that complies with the provisions of this section. Upon signing of the contract, the home shall give the resident and the resident’s representative, if any, a copy of the contract and place a copy of the contract in the resident’s file.
Provisions for Serving People with Dementia
The rules do not include specific provisions.
Medications
Aides (home staff persons) may provide medication reminders, read labels, open containers, observe a resident while taking medication, check self-administered dosage against the label, reassure the resident that the dosage is correct, and direct/guide the hand of a resident at the resident’s request. The authority for registered nurses to delegate tasks is contained in the nurse delegation statute and rules.
Public Financing
A broad HCBS waiver covers services in assisted living homes for elders and adults with disabilities. The room-and-board payment is negotiated between the home and the resident. In a limited number of cases, room and board and some services are covered by the State’s “general relief” program. The payment standard for SSI recipients is $907 and the personal needs allowance is $100 a month. Family supplementation is allowed for room and board. A new payment standard is being created for assisted living homes ($654, including a $100 personal needs allowance). Funds previously used to support a higher payment standard will be used to increase the basic Medicaid rate $8 a day.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participation | Facilities | Participation | Facilities | Participation |
| 174 | 632 | 126 | 492 | 108 | 363 |
Services for Medicaid waiver certified individuals in assisted living homes are funded under the State’s Choice Program, a Medicaid HCBS waiver. Rates vary by area of the State. A multiplier that ranges from 1.0 to 1.38 is applied to the rates, resulting in higher payments in rural and frontier areas (i.e., $100 service in one region may be reimbursed at $138 in another region). Providers receive a basic service rate that varies for adult foster care, adult residential I, and adult residential II. An “augmented service rate cost factor” is available for clients whose needs warrant the hiring or designating of additional staff. The “augment care” payment recognizes the added staffing needed by homes caring for residents needing incontinent care, skin care, added supervision, and help with medication. Some residents also attend adult day care (ADC). The basic service rate is lower for residents attending day care at least 3 days a week.
Contracted homes have the option of receiving payment according the tiers or cost based reimbursement. About half the contracted homes have applied for cost based reimbursement. The average cost based rate is $130 a day but is as high as $234.
| Anchorage Area | ADC Basic Rate |
Basic Service Rate |
Augmented Factor |
Basic and Augmented |
|---|---|---|---|---|
| Adult foster care | $32.93 | $44.52 | $17.37 | $70.54 |
| Adult residential I | $44.52 | $56.10 | $17.37 | $82.13 |
| Adult residential II | $56.10 | $67.68 | $17.37 | $93.70 |
Staffing
Administrators must be 21 years of age or older and have sufficient experience, training, or education to fulfill the responsibilities of an administrator. Administrators in homes with 10 or fewer units must fulfill at least one of the following requirements: complete an approved management or administrator training course and 1 year of documented experience relevant to population to be served, or complete a certified nurse aide training program and have at least 1 year of documented experience relevant to the population to be served, or 2 years of documented care experience relevant to the population to be served.
Staff. Homes must have the type and number of staff needed to operate the home and must develop a staffing plan that is appropriate to provide services required by resident care plans. Staff must pass a criminal background check.
Training
Regulations require that administrators receive 18 hours of training annually, direct care staff, 12 hours annually. Staff providing direct care without supervision must have sufficient language skills to meet the needs of residents. Staff must receive orientation that covers emergency procedures, fire safety, resident rights, universal precautions, resident interaction, house rules, medication management and security, physical plant layout, and reporting responsibilities.
Background Check
No person may be employed who has been convicted of crimes listed in the regulations. Administrators and staff must provide a sworn statement regarding conviction of listed crimes, the results of a name check criminal background check initially and every 2 years, and a national criminal history check based on fingerprints and conducted by the Alaska Department of Public Safety initially and every 6 years.
Monitoring
Both the Department of Health and Social Services and the Division of Senior and Disabilities Services are responsible for screening applicants, issuing licenses, and investigating complaints. The departments may delegate responsibility for investigating and making recommendations for licensing to a state, municipal, or private agency. Homes must submit an annual self-monitoring report on forms provided by the Department of Health and Social Services. Case managers monitor Choice waiver participants monthly.
Regulations require an annual monitoring visit or self-monitoring report filed by the facility. The licensing agency may impose a range of sanctions: revoking or suspending the license, denying renewal, issuing a probationary license, restricting the type of care provided, banning or imposing conditions on admissions, or imposing a civil fine.
The State describes its oversight and monitoring process as consultative. The State acts as a licensing body first, but also sees itself as educators and teachers. If violations are found through the inspection and monitoring process, the State will hand out notices of violation, but will provide education regarding how to improve care, or address the violation.
Currently, the State has limited staff resources to provide as much education and training, as they would like. When a pattern of violations is identified, a more industry-wide, versus a one-on-one, training approach is implemented. The State still holds planned orientations for new or potentially new assisted living homes every 3 months, but training can be extended out to 6 months if there is not staff available to conduct formal orientation training.
Licensing staff currently monitor homes as well as provide consultation through education and teaching. After the consolidation of Assisted Living Licensing with Public Health this process may change at some point in the future. They envision possibly rearranging, or reassigning existing staff to perform separate functions.
Fees
Voluntary license: $25 per resident. License for 3-5 residents--$75, 6 or more residents--$150, plus $25 per resident over three residents.
Arizona
Citation
Assisted living facilities. Comprehensive administrative rules and regulations §R9-10-701 et seq.
General Approach and Recent Developments
The licensing rules, established in 1998, set requirements based on the size of the facility along with supplemental requirements depending on the level of service provided. The core requirements address facilities serving 10 or fewer residents, 11 or more residents, and adult foster homes which serve one to four residents. Facilities are licensed to provide one of three levels of care (supervisory care services, personal care services, and directed care services) and must meet supplemental requirements.
The directed care level serves people with Alzheimer’s disease or dementia who cannot self-direct their care, e.g., cannot recognize danger, summon assistance, express need, or make basic decisions. Requirements for specialized training, activities, physical plant, and services will be established.
The regulations will be revised in 2004. A small task force including state agencies and stakeholders will be convened to discuss changes. The areas likely to be discussed include oversight of the approval of training programs; address the skills and background of staff who complete the assessment; oversight and documentation of medications; content of the resident’s record; designation of representatives for people receiving directed care services. Legislation expanding the Department of Health Services’ enforcement authority for overseeing training programs is pending. HB 2024 would allow the Department to grant, deny, suspend or revoke the approval of training programs and to impose civil penalties for violations of the training requirements.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted living home: < 10 | 1,509 | 24,500 | 1,077 | 8,616 | 1,241 | 22,848 |
| Assisted living centers: 11+ | 196 | 14,384 | ||||
| Adult foster care: 1-4 | 251 | 1,041 | ||||
The Arizona Health Care Cost Containment System (AHCCCS), which administers the State’s Medicaid managed care program, contains higher standards (e.g., private living units) for larger facilities serving Medicaid beneficiaries. The agency is undertaking a study of policy and practice related to serving people with dementia.
Definition
Assisted living facility means a residential care institution, including adult foster care, that provides or contracts to provide supervisory care services, personal care services, or directed care services on a continuing basis.
Supervisory care services mean general supervision, including daily awareness of resident functioning and continuing needs, the ability to intervene in a crisis, and assistance in the self-administration of prescribed medications.
Personal care services mean assistance with activities of daily living that can be performed by persons without professional skills or professional training and include the coordination or provision of intermittent nursing services and the administration of medication and treatments by a nurse who is licensed pursuant to Title 32, Chapter 15, or as otherwise provided by law.
Directed care services mean programs and services, including personal care services, provided to persons who are incapable of recognizing danger, summoning assistance, expressing need, or making basic care decisions.
Assisted living homes serve 10 or fewer residents and assisted living centers serve 11 or more residents. The Arizona Long Term Care Systems (ALTCS) Program contracts with adult foster care (four or fewer in which the provider lives in the home), assisted living homes (10 or fewer, owner is not a resident), and assisted living centers, but only centers that offer residential units (apartments).
Unit Requirements
Assisted living centers (11+ residents) may provide residential units or bedrooms. Residential units must have at least 220 square feet of floor space (excluding bathroom and closet) for one person, with an additional 100 square feet for a second person. Units must have a keyed entry, bathroom, resident controlled thermostat, and a kitchen area with sink, refrigerator, cooking appliance that may be removed or disconnected, and space for food preparation.
Assisted living centers and homes providing bedrooms must have 80 square feet in single rooms and 60 square feet per resident in double rooms. No more than two residents may share a room. Rooms occupied by residents receiving personal care services or directed care services must have a bell, intercom, or other mechanical means to contact staff. At least one toilet, sink, and shower is required for every eight residents.
Admission/Retention Policy
Assisted living facilities (ALFs) providing supervisory care services may serve residents who need health or health related services if these services are provided by a licensed home health or hospice agency.
ALFs with a personal care service license may not accept or retain any resident who is unable to direct self-care; requires continuous nursing services unless the nursing services are provided by a licensed hospice agency or a private duty nurse; residents with a Stage III or IV pressure sore, or someone who is bed bound due to a short illness unless the primary care physician approves, the resident signs a statement, and the resident is under the care of a nurse, a licensed home health agency, or a licensed hospice agency.
ALFs licensed to provide directed care services may admit residents who are bedbound, need continuous nursing services, or have a Stage III or IV pressure sore if the requirements for facilities providing personal care services are met.
A copy of the resident agreement, resident rights, and consumer resources must be provided to residents upon move-in.
Since each facility is licensed to provide a specific level of care, waivers for admission/retention requirements are available.
Nursing Home Admission Policy
Assessment information in three categories is scored: functional, emotional and cognitive, and medical. Functional areas include ADLs (bathing, dressing, grooming, eating, mobility, transferring, and toileting), communication and sensory skills, and continence. Emotional and cognitive information is obtained on orientation and behavior (wandering, self-injurious behavior, aggression, suicidal behavior, and disruptive behavior). Medical information is collected on conditions and their impact on ADLs, conditions requiring medical or nursing services and treatment, medication, special services and treatments needed, and physical measurements, history, and ventilator dependency.
Each score is weighted and totaled. The weighted functional score (ADLs and cognition) can range from 0-15 on each item, and the maximum total is 141. Applicants are grouped into two medical groups based on their conditions. Applicants in either medical group with a total score of 60 or over and those in groups 1 and 2, whose total scores are less than 60 but exceed a specified numerical threshold in each component, are eligible.
Services
Residents must receive an assessment and a service plan within 14 days of acceptance. Plans must be reviewed every 12 months for residents receiving supervisory care services, every six months for residents receiving personal care services, and every three months for residents receiving directed care services. Services must meet scheduled and unscheduled needs. Facilities must provide general supervision; promote resident independence; autonomy; dignity; choice; self-determination; and the resident’s highest physical, cognitive, and functional capacity; help utilize community resources; encourage residents to preserve outside supports; and offer individual attention and social interaction and activities.
Facilities providing personal care services also provide skin maintenance, sufficient fluids to maintain hydration, incontinence care, and an assessment by a primary care provider for residents needing medication administration or nursing services.
Facilities providing directed care must provide cognitive stimulation and activities to maximize functioning; encouragement to eat meals and snacks; and an assessment by a primary care provider.
Hospice care may be provided by a licensed hospice agency.
Arizona Long Term Care Systems (ALTCS)
An interdisciplinary team (manager, staff, RN [if nursing services are provided], resident and/or representative, and case manager, if applicable) conducts an assessment within 12 days of enrollment and every 90 days, or as needed, thereafter. A plan of care is developed with the resident or their representative that identifies the services needed, the person responsible for providing the service, the method and frequency of services, the measurable resident goals, and the person responsible for assisting the resident in an emergency.
Dietary
Facilities must provide three meals a day and one snack to meet nutritional needs based on resident health and age. Menus must be based on the Food Guide Pyramid, USDA Center for Nutrition Policy and Promotion, Home and Garden Bulletin Number 252. If therapeutic diets are offered, a manual must be available for use by employees. Diets must be consistent with physicians’ orders or as prescribed by law. Provisions for the storing and preparation of food are included. Nutrition, hydration, food preparation, service, and storage are part of the orientation and training requirements.
Agreements
Resident agreements that include the following must be signed upon move-in: terms of occupancy; services to be provided; amount and purpose of fees, charges, and deposit (including fees/charges for days the resident is absent); services available for additional charges; refund policy; responsibility to provide 30 days notice of any fee changes; policy and procedures for termination of residency; and the grievance procedure.
Provisions for Serving People with Dementia
The rules contain specific provisions for facilities serving people with dementia. A minimum of four hours of training in dementia care must be provided to staff each year. Direct supervision must be available and facilities must provide cognitive stimulation and activities to maximize functioning. Facilities must have egress controls and access to secure outside areas for residents who wander. Staff ratios must be not more than six residents per staff during morning and evening hours and 12:1 at night.
Medication Administration
Facilities must have policies and procedures governing the procurement, administration, storing, and disposal of medications. Untrained aides may supervise self-administration by opening bottle caps, reading labels, checking the dosage, and observing the resident taking the medication. Medications which cannot be self-administered must be administered by an RN or “as otherwise permitted.” The phrase as otherwise permitted was included to accommodate any future statutory changes in the state’s nurse practice act. Medication organizers can be prepared a month in advance by an RN or family member. Rules governing assistance with medications are contained in the licensing rules.
Public Financing
Services in assisted living facilities are covered through the Arizona Long Term Care Systems program which operates under a §1115 waiver. The program serves 32,076 elders, people with disabilities, MR/DD, and mentally ill beneficiaries. Program administrators originally used rates set for adult foster care, nursing facilities, the Oregon assisted living program, and the Arizona HCBS program as guidelines in setting the rates. Three classes of rates are negotiated based on the level of care: low, intermediate, and high skilled. The rates include room and board which is paid by the resident. The monthly room-and-board amount is the resident’s “alternative share of cost” (spend down) or 85 percent of the current SSI payment, whichever is greater. For residents who receive SSI, the payment rate is $564.00 a month of which $497.10 is paid to the residence to cover room-and-board charges and $66.90 is retained by the resident as a personal needs allowance. Rates are presented in the table below. The weighted average reflects participation among the program contractors by level.
Family members may supplement the resident’s income in order to allow the resident to have a one-bedroom rather than an efficiency unit.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participation | Facilities | Participation | Facilities | Participation |
| NA | 3,076 | NA | 2,300 | 670 | 1,249 |
| Level I | Level II | Level III | |||||||
|---|---|---|---|---|---|---|---|---|---|
| AFC | AL Homes |
AL Centers |
AFC | AL Homes |
AL Centers |
AFC | AL Homes |
AL Centers |
|
| Program A | $49.45 | $43.09 | $55.44 | $49.45 | $50.13 | $70.83 | $49.45 | $58.36 | $84.85 |
| Program B | $41.65 | $47.60 | $57.00 | $42.75 | $49.10 | $62.95 | $51.95 | $49.10 | $80.61 |
| Program C | $42.99 | $42.59 | $54.05 | $49.30 | $49.30 | $69.00 | $57.95 | NA | $84.00 |
| Program D | $51.63 | $53.51 | $59.26 | $59.11 | $60.82 | $65.18 | $80.40 | $82.72 | $87.10 |
| Program E | $41.72 | $49.14 | $58.12 | $48.86 | $62.32 | $66.29 | NA | $76.03 | $83.18 |
| Program F | $34.67 | $43.27 | $48.46 | $41.86 | $49.75 | $55.90 | $48.21 | $54.52 | $67.62 |
| Program G | $44.00 | $56.53 | $56.20 | NA | $60.47 | $67.81 | NA | $87.27 | $83.99 |
Staffing
Facilities are required to ensure that sufficient staff are available to provide: services consistent with the level of care for which the facility is licensed; services established in a care plan; services to meet resident needs for scheduled and unscheduled needs; general supervision and intervention in a crisis 24-hours a day; food services; environmental services; safe evacuations; and ongoing social and recreational services.
Training
Managers must be 21 years old, certified, and have a minimum of 12 months of health-related experience.
Staff must complete an orientation that includes the characteristics and needs of residents; the facility’s philosophy and goals; promotion of resident dignity, independence, self-determination, privacy, choice and resident rights; the significance and location of service plans and how to read and implement a service plan; facility rules, policies, and procedures; confidentiality of resident records; infection control; food preparation, service, and storage if applicable; abuse, neglect, and exploitation; accident, incident, and injury reporting; and fire, safety, and emergency procedures.
Managers and staff must complete twelve hours of ongoing training annually covering the promotion of resident dignity; independence; self-determination; privacy; choice; resident rights; fire, safety, and emergency procedures; infection control; and abuse, neglect, and exploitation. Staff in facilities licensed to provide directed care services must also receive a minimum of four hours of training in providing services to residents.
In addition to the above topics, training may include providing services to residents; nutrition, hydration, and sanitation; behavioral health or gerontology; social, recreational, or rehabilitative services; personnel management, if applicable; common medical conditions, medication procedures, medical terminology, and personal hygiene; service plan development, implementation, or review; and other needs identified by the facility.
Staff must also maintain current CPR certification and complete 6 hours of continuing education annually pursuant to §36-448.11(D). Nurses aides in good standing are deemed to meet the initial training requirements.
Certificate of training. Staff must obtain a certificate of training. Facilities may develop their own training and certificate program with approval from the department. Department approved training programs have requirements for instructors and the method of instruction. The competency-based approach sets standards for supervisory care services, personal care services, directed care services, and manager training.
Supervisory care services: 20 hours or the amount of time needed to verify a person demonstrates skills and knowledge in assisted living principles; communication; managing personal stress; preventing abuse, neglect, and exploitation; controlling the spread of disease and infection; documentation and record keeping; implementing service plans; nutrition, hydration, and food services; assisting with self-administration of medications; providing social, recreational, and rehabilitative activities; and fire, safety, and emergency procedures.
Personal care services: 30 hours (50 total) or the amount of time needed to verify a person demonstrates skills and knowledge in additional skills areas such as the aging process, common medical conditions associated with aging or physical disabilities, and medications; assisting with ADLs; and taking vital signs.
Directed care services: 12 hours (62 total) or the amount of time needed to verify a person demonstrates skills and knowledge of Alzheimer’s disease and related dementia; communicating with residents who are unable to direct care; providing services including problem solving, maximizing functioning, and life skills training for those unable to direct care; managing difficult behaviors; and developing and providing social, recreational, and rehabilitative activities for such persons. Four hours per year of ongoing training is required.
Background Check
Managers and staff must comply with fingerprint requirements under A.R.S. 36-411.
Monitoring
The licensing agency conducts annual renewal inspections. Licenses may be renewed for 2 years for facilities that are free of deficiencies. Penalties for violations include civil money penalties, provisional licensing, and restricted admissions. Fines against unlicensed facilities have been increased.
Facilities are monitored by ALTCS program contractors and the Department of Health Services. Sites are recertified annually by the Department of Health Services. During the pilot phase of the waiver, program contractors monitored resident care on a quarterly basis, provided technical assistance, and conducted meetings of providers to obtain feedback on the program. With statewide expansion, participants are visited at least quarterly by their ALTCS case manager. Annual operating and financial reviews of ALTCS contractors (HMOs) are conducted annually by AHCCCS. The reviews also include case management and provider records and claims data. AHCCCS also reviews a random sample of residents, including assisted living residents, to evaluate the appropriateness and quality of care. The review found no unmet needs or quality of care problems.
Fees
There is a $50 application fee. Facilities with 1-59 beds pay an additional fee of $100 plus $10 per bed; 60-99 beds: $200 plus $10 per bed; 100-149: $300 plus $10 per bed; 150+: $500 plus $10 per bed.
Arkansas
Assisted living facilities; Arkansas Annotated Code §§20-10-1701
Residential long-term care facilities; Arkansas Annotated Code §§20-76-201 (b)(3), 20-10-203, and 20-10-224
General Approach and Recent Developments
Regulations establishing two levels of assisted living facilities were finalized in 2002 and updated in 2003 and requires that any newly-constructed Level II facility shall have to be in accordance with the requirements for I-2 Groups as specified in the International Building Code (IBC) 2000, with exceptions as listed. This regulation formally required “I-1 Groups” compliance.
Assisted living facilities in both levels provide services in a homelike setting for elderly and disabled persons. The philosophical tenets of individuality, privacy, dignity and independence, the promotion of resident self-direction and personal decision-making while protecting resident health and safety are emphasized.
While there have been no facilities who have requested special care units, the State is exploring the possibility of adopting the nursing home special care unit requirements for all assisted living facilities, particularly as it relates to staffing. Currently, the assisted living facility regulations require separate staff for special care units. In nursing facilities, special care units require sufficient staff across the entire facility to meet resident needs. The State Assisted Living Association is pushing to eliminate the residential care home regulations, and create one set of rules for assisted living facilities. There is no identified time frame for accomplishing this.
Additionally, residential care facilities would like to see changes in the assisted living regulations in the areas of programming and staffing. The State is exploring this request. There has been no timetable set to address this.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted living level 1 | 1 | 54 | NA | NA | NA | NA |
| Assisted living level 2 | 5 | 221 | NA | NA | NA | NA |
| Residential care | 111 | 4,369 | 122 | 4,647 | 152 | 5,438 |
The Living Choices Assisted Living 1915 (c) Waiver Program was implemented in January 2003. Legislation revising Alzheimer’s special care standards passed (HB 1407) in 2001. Personal care services are covered under the state plan for Medicaid beneficiaries.
Definition
Residential long-term care facility (RCF) means a building or structure which is used or maintained to provide, for pay on a 24-hour basis, a place of residence and board for three or more individuals whose functional capabilities may have been impaired, but who do not require hospital or nursing home care on a daily basis but could require other assistance with activities of daily living.
An assisted living facility (ALF) is any building or buildings, section, or distinct part of a building, boarding home, home for the aged, or other residential facility whether operated for profit or not that undertakes through its ownership or management to provide assisted living services for a period exceeding 24 hours to more than three adult residents of the facility who are not relatives of the owner or administrator. ALF means facilities in which assisted living services are provided either directly or through contractual arrangements or in which contracting in the name of residents is facilitated. An ALF provides, at a minimum, services to assist residents in performing all activities of daily living on a 24-hour basis.
An Alzheimer’s special care unit (ASCU) is a separate and distinct unit within an assisted living or other long term care facility that segregates and provides a special program for residents with a diagnosis of probable Alzheimer’s disease or related dementia, and that advertises, markets, or otherwise promotes the facility as providing specialized Alzheimer’s or related dementia care services.
Unit Requirements
Residential long term care facility. A minimum of 100 square feet is required for single rooms and 80 square feet per resident in shared rooms. Rooms may be shared by two residents. A minimum of one toilet/lavatory is required for every six residents and one tub/shower for every 10 residents.
Assisted living facility. All units must be apartments of adequate size and configuration to permit residents to carry out, with or without assistance, all the functions necessary for independent living, including sleeping; sitting; dressing; personal hygiene; storing, preparing, serving, and eating food; storing clothing and other personal possessions; doing personal correspondence and paperwork; and entertaining visitors. Each apartment or unit shall be accessible to and useable by residents who use a wheelchair or other mobility aid consistent with the accessibility standards. Each apartment must have a lockable door. Separate bathroom and kitchen areas are required. Single occupancy apartments must be at least 150 square feet excluding entryway, bathroom and closets, and 230 square feet for two persons. Apartments may not be occupied by more than two persons. Each unit must provide for a small refrigerator as well as a microwave oven, except as may be otherwise provided in the regulations, and a call system monitored 24-hours a day by staff.
Admission/Retention Policy
Residential long term care facility. Tenants must be 18 or older; independently mobile (physically and mentally capable of vacating the facility within 3 minutes); able to self-administer medications; be capable of understanding and responding to reminders and guidance from staff; do not have a feeding or intravenous tube; are not totally incontinent of bowel and bladder; do not have a communicable disease that poses a threat to the health or safety of others; do not need nursing services which exceed those that can be provided by a certified home health agency on a temporary or infrequent basis; do not have a level of mental illness, retardation, or dementia or addiction to drugs or alcohol that requires a higher level of medical, nursing, or psychiatric care or active treatment than can safely be provided in the facility; does not require religious, cultural, or dietary regimens that cannot be met without undue burden; and do not require physical restraints or have current violent behavior.
Waivers of the admission/retention policy are not available. Residents who require frequent skilled nursing services from a home health agency must be assessed by the Office of Long Term Care to determine if a nursing home placement is needed.
Level 1 assisted living facilities cannot serve nursing home eligible residents or residents who need 24-hour nursing services except as certified by a licensed home health agency for a period of 60 days with one 30-day extension; are bedridden; have transfer assistance needs that the facility cannot meet, including assistance to evacuate the building in case of an emergency; present a danger to self or others; and require medication administration performed by the facility.
Level II facilities are allowed to serve nursing home eligible residents but cannot serve residents who need 24-hour nursing services; are bedridden; have a temporary (more than 14 consecutive days) or terminal condition unless a physician or advance practice nurse certifies the resident’s needs may be safely met by a service agreement developed by the assisted living facility, the attending physician or advance practice nurse, a registered nurse, the resident or his or her responsible party if the resident is incapable of making decisions, and other appropriate health care professionals as determined by the resident’s needs; have transfer assistance needs, including but not limited to assistance to evacuate the facility in case of emergency, that the facility cannot meet with current staffing; present a danger to self or others or engage in criminal activities.
Nursing Home Admission Policy
To be determined a functionally disabled individual, the individual must meet at least one of the following three criteria as determined by a licensed medical professional:
- The individual is unable to perform either of the following:
- At least one of the three ADLs of transferring/locomotion, eating, or toileting without extensive assistance from or total dependence upon another person; or
- At least two of the three ADLs of transferring/locomotion, eating, or toileting without limited assistance from another person; or,
- The individual has a primary or secondary diagnosis of Alzheimer’s disease or related dementia and is cognitively impaired so as to require substantial supervision from another individual because he or she engages in inappropriate behaviors which pose serious health or safety hazards to himself or others; or,
-
The individual has a diagnosed medical condition which requires monitoring or assistance at least once a day by a licensed medical professional and the condition, if untreated, would be life threatening.
Services
Residential long-term care facility. Facilities may provide personal care; supportive services (occasional or intermittent guidance, direction, or monitoring for ADLs); activities and socialization; assistance securing professional services; meals; housekeeping; and laundry. Residents have a choice of providers for receiving personal care services, and they may use an agency that is not the facility. RCFs may not provide medical or nursing services. Home health services may be provided by a certified home health agency when ordered by a physician.
Assisted living facilities. Level 1 facilities provide 24-hour staff supervision by awake staff; assistance in obtaining emergency care 24 hours a day (this provision may be met with an agreement with an ambulance service or hospital or emergency services through 911); assistance with social, recreational, and other activities; assistance with transportation (this does not include the provision of transportation); linen service; three meals a day; and medication assistance. Other services include attendant care, homemaker, and medication oversight. Level 1 facilities may provide occasional guidance, direction or monitoring, or assistance with ADLs and social activities and transportation.
Level II facilities offer services that directly help a resident with certain routines and activities of daily living such as assistance with mobility and transfers; hands-on assistance to resident with feeding, grooming, shaving, trimming or shaping fingernails and toenails, bathing, dressing, personal hygiene, bladder and bowel requirements, including incontinence; and assistance with medication only to the extent permitted by the state Nurse Practice Act. The assessment for residents with health needs must be completed by an RN.
Health services are available that assist in achieving and maintaining well-being (e.g., psychological, social, physical, and spiritual) and functional status. This may include nursing assessments and the monitoring and delegation of nursing tasks by registered nurses pursuant to the Nurse Practice Act, care management, records management, and the coordination of basic health care and social services in such settings.
The regulations provide for negotiation of a compliance agreement to deal with risk of an adverse outcome. In the agreement, the facility identifies the specific concern(s); provide clear, understandable information about the possible consequences of his or her choice or action; negotiates a compliance agreement with the resident or his or her responsible party that will minimize the possible risk and adverse consequences while still respecting the resident’s preferences.
The compliance agreement must address any situation or condition that is or should be known to the facility that involves risk; the probable consequences; the resident or his or her responsible party’s preference concerning how the situation will be handled and the possible consequences of action on that preference; what the facility will and will not do to meet the resident’s needs and comply with the resident’s preference to the identified course of action; alternatives offered to deal with the risk; and the agreed-upon course of action.
Dietary
Residential long-term care facility. Facilities must provide three balanced meals a day and make snacks available, served at about the same time each day, not more than 5 hours apart between breakfast and lunch and between lunch and the evening meal, and no more than 14 hours between breakfast and the evening meal. Facilities must notify the physician if a resident does not eat meals for more than 2 consecutive days. State, county, and local health departments may have rules that deal with sanitation, safety, and health. Recommended daily allowances are established in the regulations. In large facilities (> 17), staff involved in food and dietary services cannot perform other duties on the same shift.
Assisted living facilities. Three balanced meals, snacks, and fluids are required.
Agreements
Residential long-term care facility. Residents must receive a copy of the resident agreement at or prior to moving in that covers: services, materials and equipment, and food to be included in the basic charge; additional services and charges to be provided; residency rules; conditions and rules for termination; provisions for changing the charges; and refund policy.
Assisted living facilities. Covers core services (24-hour staff supervision by awake staff; assistance obtaining emergency care; assistance with social, recreational, and other activities; assistance with transportation; linen service; three meals a day; medication assistance); additional services; health care services available through home health agencies; parameters for pets; current statement of all fees and daily, weekly, or monthly charges; 30-day notice of changes in charges; identification of the party responsible for payment; refund policy; procedures for nonpayment; policy on acceptance of responsibility for personal funds and valuables; responsibility for medication; a copy of facility rules; provisions for emergency transfers; and conditions of termination of the occupancy agreement.
Provisions for Serving People with Dementia
Residential long term care facility. The admission and retention rules limit a facility’s ability to serve anyone with dementia.
Assisted living facilities. Facilities must provide a disclosure statement that includes: the philosophy of how care and services are provided to the residents; the pre-admission screening process; the admission, discharge and transfer criteria and procedures; training topics, amount of training time spent on each topic, and the name and qualification of the individuals used to train the direct care staff; the minimum number of direct care staff assigned to the ASCU each shift; and a copy of the Residents’ Rights.
The licensing rules include program requirements that provide 24-hour care; promote social, physical, and mental well-being and protect resident rights. Nursing, direct care, and personal care staff cannot perform the duties of cooks, housekeepers, or laundry staff during their direct care shifts. An individual support plan must be prepared. Standards for the physical design of the unit are described. Policies are required for egress control and standards for locking devices are specified. Staff must have 30 hours of training on policies (1 hour); etiology, philosophy, and treatment of dementia (3 hours); stages of Alzheimer’s disease (2 hours); behavior management (4 hours); use of physical restraints, wandering, and egress control (2 hours); medication management (2 hours); communication skills (4 hours); prevention of staff burn out (2 hours); activities (4 hours); ADLs and individual centered care (3 hours); and assessment and Individual Service Plans (3 hours). Staff must receive 2 hours of ongoing training each quarter. A disclosure statement must be provided that includes the treatment philosophy; pre-admission screening process; admission, discharge, and transfer policies; assessment, care planning, and implementation; training topics and time required; minimum number of direct care staff; residents rights; assessment; individual support plan and implementation; activities; and the stages for which care is provided.
Medication Administration
Residential long-term care facility. Residents must be familiar with their medications and the instructions for taking them. Aides may remind residents to take medications, read label instructions, and remove the cap or packaging, but the resident must remove the medication from the package or container. The State does not have provisions for nurse delegation.
Assisted living facilities. Staff of Level I facilities may assist with self-administration of, but cannot administer, medications. Staff of Level II facilities may administer medications. A pharmacy consultant is required.
Public Financing
The State implemented the Living Choices Assisted Living HCBS Waiver Program in January 2003. A Living Choices Assisted Living Waiver “assisted living services” provider must be licensed as a Level II Assisted Living Facility or a licensed Class A Home Health Agency who has a contract with a licensed Level II Assisted Living Facility to provide waiver “assisted living services” and provide pharmacy consultant services.
The assisted living waiver program serves clients who are age 65 and over, or who are 21 years of age or over and blind or disabled. A Division of Medical Services, Office of Long Term Care registered nurse determines level of care eligibility. A Division of Aging & Adult Services assisted living waiver registered nurse completes the comprehensive assessment and establishes the tier of need, and completes the service plan upon admission to the program, and annually or at times of significant change.
Services provided under the waiver include attendant care (assistance with ADLs); therapeutic social and recreational activities; medication oversight to the extent permitted by law; medication administration; periodic nursing evaluations; limited nursing services; and non-medical transportation as specified in the plan of care.
Personal care services are reimbursed as a state plan service under Medicaid based on a plan of care. Residential Care facilities are reimbursed on a fee-for-service basis. A maximum of 64 hours of care per month at $12.35 an hour (maximum payment of $790.40) may be covered without prior authorization. Services may exceed the cap if approved. Approximately 1,155 residents living in residential long-term care facilities receive personal care services under the Medicaid state plan. The State uses a presumptive eligibility process to expedite determinations.
| Source | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Participation | Facilities | Participation | Facilities | Participation | |
| State plan | NA | 1,155** | NA | 1,178** | NA | 1,143** |
| Waiver | 5 | 50 | NA | NA | NA | NA |
| ** Unduplicated number of residents in residential long-term care facilities. | ||||||
Medicaid reimbursement under the Living Choices waiver is determined through the comprehensive assessment and a four-tier method of need (see table below). The daily rate pays for all direct services in the participant’s plan of care. Pharmacy consultant services are a daily rate. The waiver will pay for 3 prescription drugs beyond the Medicaid State Plan Prescription Drug Program’s monthly benefit limit. Persons receiving assisted living waiver services may not receive Medicaid State Plan Personal Care. Reimbursement is for services only and may not pay for room and board.
Based on the level of assistance, scores are assigned for ADLs (eating [2], toileting [2], ambulation [2], bathing [2], transfer [1], and body care [1]); medication assistance; sensory ability; and psycho-social/cognitive ability. Points are awarded for ADLs for people who need substantial supervision, physical assistance, or total assistance. Points for medication assistance vary with the type of assistance multiplied by the number of medications (see table).
Staffing
Residential long-term care facility. Ratios for the number of direct care staff varies by the time of day (daytime, evening, and night) and the number of residents. Staffing must be sufficient to meet the needs of residents.
Assisted living facilities. Administrators must be certified as an ALF, RCF, or Nursing Home administrator. Staffing sufficient to meet the needs of residents is required according to staff ratios that vary by facility size and shift.
Level 2 facilities must designate a full-time (40 hour per week) administrator who must be on the premises during normal business hours. Sharing of administrators between assisted living facilities and other types of long-term care facilities is permitted. The facility may employ an individual to act both as administrator and as the facility’s registered nurse. At no time may the duties of administrator take precedence over, interfere with, or diminish the responsibilities and duties associated with the registered nurse position. Level 2 facilities must employ or contract with at least one RN. The assisted living Level 2 RN is responsible for the preparation, coordination, and implementation of the direct care services plan portion of the resident’s occupancy admission agreement. The Living Choices waiver plan of care developed by the Division of Aging & Adult Services assisted living waiver RN is to be filed in the resident’s occupancy admission agreement with the assisted living facility’s direct services plan of care. The assisted living facility RN, in conjunction with the physician, shall be responsible for the preparation, coordination, and implementation of the health care services plan portion of the resident’s occupancy admission agreement and shall review and oversee all LPN, CNA, and PCA staff. Level II facilities must employ a consulting pharmacist. The assisted living facility RN need not be physically present at the facility, but must be available to the facility by phone or pager.
Training
Residential long-term care facility administrators must have a current certification as a residential care facility administrator or complete a course of instruction and training prescribed by the department.
Residential long-term care facility staff. An orientation covering, at a minimum, job duties, resident rights, abuse/neglect reporting requirements, and fire and tornado drills is required. For direct care staff, four hours of in-service training or continuing education must be provided on a quarterly basis covering residents’ rights, evacuation of a building, safe operation of fire extinguishers, incident reporting, and medication supervision.
Assisted living facilities. Staff must receive orientation on the following topics: philosophy of independent living in an assisted living residence; residents’ rights; abuse, neglect, and exploitation; safety and emergency procedures; communicable diseases; communication skills; review of the aging process; dementia/cognitive impairment; resident health and related problems; job requirements; medication supervision/management, and incident reporting. A minimum of 6 hours of ongoing training a year is required.
Monitoring
Written policies and procedures for monitoring quality of care are required. Remedies for violations include Civil Money Penalties, denial of admissions, directed in-service training, directed plan of correction, state monitoring, temporary administrator, temporary license, and transfer of residents.
Assisted Living Facilities: The State provides more education than consultation in their oversight and monitoring processes. This process has been very successful. With newly licensed facilities, the State will conduct mock surveys to educate the facility about the process and expectations. This has become more of a teaching/learning model regarding the interpretation of the regulations.
Education is provided on an industry-wide level versus facility-based consultation. The education is typically provided through the assisted living association. Survey nurses do not provide consultation and training. There are separate staff to perform each individual function.
Background Check
Residential long-term care and assisted living administrators may not have any prior conviction pursuant to Arkansas Code Annotated §20-10-401 or relating to the operation of a long term care facility nor any conviction for abusing, neglecting, or mistreating individuals. Administrators must also successfully complete a criminal background check pursuant to Arkansas Code Ann. §20-33-201, et seq.
Criminal background checks are required for all employees. Checks include the Adult Abuse Registry.
Fees
- Residential long term care facility: $5 per bed.
- Assisted living: The application fee is $250 plus $10 per bed.
| Assisted Living Waiver Program Tiers and Daily Rates | ||
|---|---|---|
| Tier 1 | 0-5 total ADL points and 0-39 total other points | $39.51/day |
| Tier 2 | 0-5 total ADL points and 4-60 total other points or 6-10 total ADL points and 0-39 total other points | $42.83/day |
| Tier 3 | 0-5 total ADL points and 61 or more total other points or 6-10 total ADL points and 40-69 total other points | $47.47/day |
| Tier 4 | 6-10 total ADL points and 70 or more total other points | $49.97/day |
| NOTE: The Living Choices Waiver has a built-in annual rate increase of 2.9% for Year 2 based on the FY 04 market basket forecast and 3.0% for Year 3 based on the FY 05 market basket forecast. The rates shown in the above chart are the rates for Year 2. | ||
| Task | Points |
|---|---|
| Eating | 2 points |
| Toileting | 2 points |
| Ambulation | 2 points |
| Bathing | 2 points |
| Transfer | 1 point |
| Body care | 1 point |
| Medication reminding/monitoring | 0.5 times number of medications |
| Needs RX assistance | 0.75 times number of medications |
| Dosage prep | 1 times number of medications |
| Needs administration | 2 times number of medications |
| Speech not understandable, unable to speak, unable to communicate | 10 points |
| Sight: Legally blind with corrective lenses/blind | 10 points |
| Hearing: Must be loud even with aides; unable to hear | 10 points |
| Disorientation | 12 points |
| Memory impairment | 16 points |
| Impaired judgment | 17 points |
| Wandering | 15 points |
| Disruptive behavior | 20 points |
California
Citation
Residential care facilities for the elderly (RCFEs) Title 22, Division 6, Chapter 87100-87730
General Approach and Recent Developments
A series of changes are being implemented following passage of several bills by the legislature. The changes replace the exceptions requirements for facilities serving people with health conditions with requirements for documentation, staff training and oversight, add requirements for special care facilities, and admissions agreements. Due to budget reductions, the licensing agency is unable to continue its technical support program that provided consultation to facilities. Staffing shortages have also changed the schedule for inspection visits. Instead of inspecting each facility annually, a sample of facilities will be visited each year.
The Department of Health Services (DHS) was directed by the legislature to develop a pilot program to test two models for covering assisted living services under a Medicaid HCBS waiver. One model will cover services in licensed residential care facilities for the elderly and the second will deliver services in elderly housing settings.
The Community Care Licensing Division plans to revise and post technical guides on their Web site. The Web site includes a manual that interprets regulations and gives guidance to facilities about how to apply the rules.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Residential care facilities for the elderly | 6,543 | 154,830 | 6,207 | 147,580 | 6,152 | 136,719 |
Definition
A residential care facility for the elderly is defined as a housing arrangement chosen voluntarily by the resident--or the resident’s guardian, conservator, or other responsible person--where 75 percent of the residents are 60 years of age or older, or, if younger, have needs compatible with other residents, and where varying levels of care and supervision are provided, as agreed to at time of admission or as determined necessary at subsequent times of reappraisal.
Unit Requirements
Occupancy is limited to two residents per bedroom, which must be large enough to accommodate easy passage between beds, required furniture, and assistant devices such as wheelchairs or walkers. One toilet and sink is required for every six residents and a bathtub or shower for every 10 residents.
Admission/Retention Policy
Facilities may admit or retain residents who are capable of administering their own medications; receive medical care and treatment outside the facility or from a visiting nurse; residents who need to be reminded to take medications; and people with mild dementia or mild temporary emotional disturbance resulting from personal loss or change in living arrangement. Facilities may not admit or retain anyone with a communicable disease; anyone who requires 24-hour skilled nursing or intermediate care. The regulations allow residents with health conditions requiring incidental medical services which are specified in the rules (e.g., administration of oxygen, catheter care, colostomy/ileostomy care, contractures, diabetes, enemas, suppositories, and/or fecal impaction removal, incontinence of bowel and/or bladder, injections, intermittent positive pressure breathing machine, and Stage 1 and 2 dermal ulcers) to be admitted and retained if the resident can perform the care or a licensed professional provides care. Facilities may not serve people who require care for Stage 3 and 4 dermal ulcers, gastrostomy care, naso-gastric tubes, tracheostomies, staph infection or other serious infection, and/or who depend on others to perform all activities of daily living.
Residents who will be bedridden more than 14 days may be retained if the facility notifies the Department of Social Services that the condition is temporary.
Nursing Home Admission Policy
Beneficiaries must have a medical condition that requires an out-of-home protective living arrangement with 24-hour supervision and skilled nursing care or observation on an ongoing intermittent basis to abate health deterioration.
Services
Services are divided into (1) basic services and (2) care and supervision. Basic services include safe and healthful living accommodations; personal assistance and care; observation and supervision; planned activities; food service; and arrangements for obtaining incidental medical and dental care. Care and supervision covers assistance with activities of daily living and assumption of varying degrees of responsibility for the safety and well being of residents. Tasks include assistance with dressing, grooming, bathing, and other personal hygiene; assistance with self-administered medications; and central storing and distribution of medications.
Legislation enacted a few years ago requires that RCFEs inform residents that they have the right to have an advance directive. A brochure explaining advance directives was developed for care providers to give residents.
Legislation enacted in 1994 allows hospice care provided the resident contracts individually with a hospice agency. Facilities must request a waiver to allow hospice care and be able to meet the resident’s needs when the hospice agency is not present. If the resident shares a room, the other party needs to agree to allow hospice care in the shared living space.
Dietary
The total daily diet must meet the recommended dietary allowances of the Food and Nutrition Board of the National Research Council. At least three meals and snacks must be provided in facilities that have responsibility for all food arrangements. Meals must include an appropriate variety of foods, planned in consideration of cultural and religious backgrounds and resident preferences. Modified diets prescribed by physicians are provided. Facilities with 16 to 49 residents must designate one person with appropriate training to be responsible for food planning, service, and preparation. Staff must have training or related experience on the assigned job tasks.
Agreements
Admission agreements must be signed within 7 days of admission and include provisions for: the basic services available; optional services; payment provisions (basic rate, optional service rate, payer, due date, funding source); process for changing the requirements and a 60-day notice; and refunds.
Legislation passed in 2003 (SB 211, Chapter 211, Statutes of 2003), adds Health and Safety (H&S) Code Sections 1569.880 through 1569.888 to ensure that RCFE admission agreements do not violate residents’ rights and to provide residents with the information necessary to make informed choices. Many requirements overlap existing statutes or regulations in Title 22 California Code of Regulations (CCR) chapter 6. The applicability of some requirements will depend on the type of services provided by the facility. The law specifies that the admission agreement includes the following: a comprehensive description of any items and services provided under a single fee; a comprehensive description of, and the fee schedule for, all items and services not included in a single fee; the resident shall receive a monthly statement itemizing all separate charges incurred by the resident and authorized by the admission agreement; a statement acknowledging the acceptance or refusal to purchase the additional services shall be signed and dated by the resident or the resident’s representative and attached to the admission agreement; an explanation of the use of third-party services within the facility that are related to the resident’s service plan, including, but not limited to, ancillary, health, and medical services, how they may be arranged, accessed, and monitored, any restrictions on third-party services, and who is financially responsible for the third-party services; a comprehensive description of billing and payment policies and procedures; the conditions under which rates may be increased; the facility’s policy concerning family visits and other communication with residents; refund policy; conditions under which the agreement may be terminated; and an explanation of the resident’s right to notice prior to an involuntary transfer, discharge, or eviction, the process by which the resident may appeal the decision and a description of the relocation assistance offered by the facility.
Provisions for Serving People with Dementia
During 1995, legislation (Chapter 550 of the Acts of 1995) was passed that allows RCFEs that serve people with dementia to develop secure perimeters. Based on the results of a pilot project, the law allows facilities that meet specific additional requirements to secure exterior doors or perimeter fences, or to install delayed egress devices on exterior doors and perimeter fence gates. Resident supervision devices--wrist bracelets that activate a visual or auditory alarm when a resident leaves the facility--may also be used. Facilities must provide interior and exterior space for residents to wander freely, must receive approval from the local fire marshal, and must conduct quarterly fire drills. Facilities with delayed egress devices must be sprinklered and contain smoke detectors, and the delayed egress devices must deactivate when the sprinkler system or smoke detectors activate. The devices must also be able to be deactivated from a central location and deactivate when a force of 15 pounds is applied for more than two seconds to the panic bar. In addition, facilities shall permit residents to leave, who continue to indicate such a desire, and staff must ensure continued safety. Reports must be submitted when residents wander away from the facility without staff. Delayed egress devices may not substitute for staff.
Facilities may admit and retain people with dementia who are not able to respond to verbal instructions to leave a building without assistance provided they have:
- A plan of operation which specifically addresses the needs of residents with dementia;
- A training plan which ensures that facility staff can meet the needs of residents;
- An activity program and resident assessment and re-assessment procedures;
- Procedures to notify physicians when behavior changes;
- A written plan to minimize the use of psycho-tropic medications; and
- A disaster and mass casualty plan.
Medication Administration
Facility staff may assist with self-administration of medications and, if authorized by law, administer injections. Medications may also be administered by licensed home health agency personnel.
Public Financing
The California legislature (HB 499, 2000) directed the Department of Health Services to develop an Assisted Living Waiver Pilot Project (ALWPP) in three counties: Sacramento, San Joaquin and Los Angeles, and will serve 1,000 people over 3 years in two different settings--licensed RCFEs and conventional elderly housing sites. About 100 sites are expected to participate in the pilot. An HCBS waiver will be submitted to CMS to implement the pilot. The pilot defines assisted living based on the work of the Assisted Living Work group:
“Assisted living is a state regulated and monitored residential long-term care option. Assisted living provides or coordinates oversight and services to meet the residents’ individualized scheduled needs, based on the residents’ assessments and service plans and their unscheduled needs as they arise.”
The pilot will require private occupancy, with shared occupancy only by residents’ choice. Units will have a kitchen area equipped with a refrigerator, a cooking appliance (microwave is acceptable), and storage space for utensils and supplies.
The project developed a four-tiered payment methodology based on the tiers used in Arkansas. The bundled rate will include payment for the following services: 24-hour awake staff to provide oversight and meet the scheduled and unscheduled needs; provision and oversight personnel and supportive services (assistance with activities of daily living and instrumental activities of daily living); health related services (e.g., medication management services); social services; recreational activities; meals; housekeeping and laundry; and transportation
As of January 1, 2004 the SSI/State Supplement in licensed facilities is $853 a month with a personal needs allowance of $111. The remainder of $742 pays for Room and Board.
Staffing
Administrators of facilities with 16 to 49 beds must have 15 college credits and in facilities with 50 or more units, 2 years of college or 3 years of experience or equivalent education and experience. Administrators who do not have a license must complete a certification program and 12 hours of classroom training.
Sufficient staff must be employed to deliver services required by residents. On-the-job training or experience is required in the principles of nutrition, food storage and preparation, housekeeping, and sanitation standards; skill and knowledge to provide necessary care and supervision; assistance with medications; knowledge to recognize early signs of illness; and knowledge of community resources.
Requirements for awake staff vary by the size of the facility. For 16 or fewer, staff must be available in the facility; 16 to 100, at least one awake staff; 101 to 200, one on call and one awake, with an additional awake staff for each additional 100 residents.
Training
Administrators. Individuals shall complete an approved certification program prior to being employed as an administrator. The program must include 40 hours of classroom training which covers laws, rights, regulations, and policies (12 hours); business operations (3 hours); management and supervision (3 hours); psycho-social needs of the elderly (5 hours); physical needs of the elderly (5 hours); community and support services (2 hours); use, misuse, and interaction of drugs (5 hours); and admission, retention, and assessment procedures (5 hours). All administrators shall be required to complete at least 20 clock hours of continuing education per year in areas related to aging and/or administration.
Staff. Personnel must be given on-the-job training or have related experience in: the principles of good nutrition, good food preparation and storage and menu planning; housekeeping and sanitation procedures; skill and knowledge required to provide necessary resident care and supervision including the ability to communicate with residents; knowledge required to safely assist with prescribed medications which are self-administered; knowledge necessary in order to recognize early signs of illness and the need for professional help; and knowledge of community services and resources.
Facilities licensed for 16 or more must have a planned on-the-job training program in the above areas including orientation, skill training, and continuing education.
Background Check
The licensing agency conducts a criminal background check of officers of the organization, staff responsible for administration and direct supervision, persons providing direct care, and employees having frequent contact with residents and others and may approve or deny a license or employment based on its findings. A fingerprint clearance shall be received by the licensing agency on all persons subject to criminal record review prior to issuing a license. All facility staff must be fingerprint cleared prior to their physical presence in the facility.
Monitoring
Facilities are inspected on a rotating basis. Facilities are inspected on a random sample basis, but at least once every 5 years. Facilities that require “targeted visits” will be visited on an annual basis. These consist of facilities that need closer attention because of their compliance histories. Three levels of penalties are allowed for violations with an (A) immediate, (B) potential, and (C) technical impact. Fifty dollars per day civil penalties are allowed for A and B violations increasing to $100 per day if the same violation is repeated three times in a 12-month period. Consultation is provided for Type C violations. The licensing agency is mandated to conduct an investigation within 10 days on any complaint received against a facility.
Fees
Licensing fees required at initial licensure and annually thereafter are adjusted by facility size: 1 to 6--$375, 7 to 15--$563, 16 to 49--$750, and 50+--$938 (effective August 4, 2003). A proposal to increase the licensing fees due to declines in state revenues is pending.
Colorado
Citation
Assisted living residences; Chapter VII, §1.1 et seq.
General Approach and Recent Developments
Revisions to rules based on legislation that passed in 2002 were approved by the Board of Public Health in March 2004. HB 02-1323 changed the licensing category to assisted living residences and added intermediate sanctions. Supply has remained fairly stable with new construction replacing smaller independently-owned homes. The Department anticipates that once the regulations are approved, work might begin on some issues that are not addressed in the pending regulations such as administrator requirements and staffing.
The Department of Public Health web site has links to interpretive guidelines, the survey protocol, and a consumer comparison checklist that covers provider agreements, license/certification, Medicaid participation, space, safety, care plans, personal services, staff, meals, socialization, communication, and facility tour/observations. It also posts the 10 most commonly cited deficiencies for each quarter.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted living residences | 525 | 13,779 | 538 | 14,291 | 551 | 13,868 |
Definition
The new law defines “assisted living residence” or “residence” as a residential facility that makes available to three or more adults not related to the owner of such facility, either directly or indirectly through a resident agreement with the resident, room and board and at least the following services: personal services; protective oversight; social care due to impaired capacity to live independently; and regular supervision that shall be available on a 24-hour basis, but not to the extent that regular 24-hour medical or nursing care is required. The term “assisted living residence” does not include any facility licensed in this State as a residential care facility for individuals with developmental disabilities, or any individual residential support services that are excluded from licensure requirements pursuant to rules adopted by the department.
Unit Requirements
The rules allow no more than two people to share a room for facilities built after July 1, 1986. Single occupancy rooms must have at least 100 square feet and double occupancy rooms at least 60 square feet per person. One full bathroom is required for every six residents. Cooking is not allowed in bedrooms, and facilities provide access to a food preparation area for heating or reheating food or making hot beverages subject to “house rules.” Cooking may be allowed in facilities that provide apartments rather than bedrooms. Facilities that are Medicaid certified are prohibited from cooking. However, microwaves can be used if the facility has assessed the resident for his or her ability to safely use the appliance.
Admission/Retention Policy
Assisted living residences may not admit or retain residents who are:
- Consistently, uncontrollably incontinent unless the resident or staff is able to prevent it from becoming a health hazard;
- Totally bedridden with limited potential for improvement;
- In need of 24-hour nursing or medical service;
- In need of restraints; or
- Have a communicable disease.
A facility may keep a resident who becomes bedridden if a physician describes the services needed to meet the health needs of the residents, there is an ongoing assessment and monitoring by a licensed home health agency or hospice service that ensures that the resident’s physical, mental and psychological needs are met, and there is adequate staff trained in the needs of bedridden residents.
Additional criteria are applied to facilities contracting with Medicaid as alternative care facilities (ACFs). ACFs may not admit or retain anyone needing more than intermittent skilled services; who has an acute illness that cannot be managed through medications or therapy; is unable or unwilling to meet his or her own personal hygiene needs under supervision; has ambulation limitations, unless compensated by assistive devices or staff; is consistently disoriented to the extent that he or she poses a danger to themselves or others; requires tray food service on a continuous basis; or is consistently unwilling to take prescribed medication.
Each facility develops admission criteria based on the capacity of the facility. A review of Medicaid pre-admission screening assessment forms showed that Medicaid waiver participants in ACFs had fewer skilled needs than nursing home residents.
Residents may be allowed to receive hospice care if they are long-term residents (i.e., the facility has been their home), the facility can continue to meet the needs of the other residents, and staff are trained and are not doing things outside their scope of practice. Residents requiring hospice care upon admission would not be accepted.
Nursing Home Admission Policy
Medical eligibility is determined by local Utilization Review Contractors according to guidelines based on a functional needs assessment of the following areas: confusion or contact with reality; behavior; communication; mobility; bathing; dressing; eating/feeding; bowel continence; bladder continence; skin care; vision; hearing; need for supervision and observation; and living skills (i.e., cooking, shopping, laundry, etc.). Residents must need skilled or maintenance services at least 5 days a week. Skilled and maintenance services are performed in the following areas: skin care; medication; nutrition; activities of daily living; therapies; elimination; and observation and monitoring. (Note: The determinations were formerly made by the statewide Peer Review Organization.)
The scores in each of the functional areas are based on a set of criteria and weights developed by the PRO and approved by the State which measures the degree of impairment in each of the functional areas. When the combined score in each of the functional areas exceeds 19 points, the nurse reviewer may certify that the person being reviewed is eligible for placement in a nursing facility. If the score is less than 20 points, the PRO physician advisor may use professional judgment to determine the individual’s need for the level of services provided in a nursing facility.
Services
Facilities must provide a physically safe and sanitary environment, room and board, personal services (transportation, assistance with activities of daily living and instrumental activities of daily living, individualized social supervision), social and recreational services, protective oversight, and social care. Written care plans, which must be reviewed at least annually, are required for each resident and include a comprehensive assessment of physical, health, behavioral and social needs and capacity for self-care, a list of current prescribed medications (dosage, time and route of administration, whether self-administered or assisted), dietary restrictions, allergies, and any physical or mental limitations or activity restrictions. Nursing and therapies may be received if provided by a home health agency.
Dietary
Three nutritionally balanced meals using a variety of foods from the basic food groups and snacks of nourishing quality are required. Therapeutic diets prescribed by a physician are provided, and the recipes are available for review. Meals cannot be routinely provided in resident rooms unless indicated on the care plan. Staff must receive on-the-job training or have experience in the tasks assigned to them.
Agreements
A copy of the resident agreement must be provided upon move-in. The agreement must include: charges, refunds and deposit policies; services included in the rates and charges, including optional services for which there will be an additional, specified charge; types of services provided by the facility, those services which are not provided, and those which the facility will assist the resident in obtaining; bed hold fees; transportation services; therapeutic diets; and whether the facility will be responsible for providing bed and linens, furnishing and supplies. There must also be written evidence that the facility has disclosed the policies and procedures (admissions; discharges; emergency plan and fire escape procedures; illness, injury or death; resident rights; smoking; management of residents’ funds; internal grievance process; investigation of abuse and neglect allegations; and restrictive egress devices); method of determining staffing levels and the extent to which certified or licensed health professionals are available on-site; whether the facility has an automatic sprinkler system; if the facility uses restrictive egress alert devices and the types of behavior exhibited by persons needing such devices.
Provisions for Serving People with Dementia
Facilities must disclose that they operate a secure environment, information about the type of diagnosis or behaviors served and for which staff are trained. Facilities serving people whose right to move outside the environment is limited must have a secured environment. For a facility to serve a resident in a secured environment, legal authority must be established by guardianship, court order, health care proxy, or durable power of attorney. Assessments that evaluate (by a qualified professional) the need for a secured environment must be completed. Reassessments must be completed within ten days of a significant change to determine whether placement is appropriate. Staff and the owner/operator must have appropriate training. Facilities with secured environments must establish a forum that meets at least quarterly for family members to make suggestions, and express concerns and grievances. Families meet with the administrator and a staff representative. Suggestions must be responded to in writing.
In addition to the interior common areas required by this regulation, the facility shall provide a safe and secure outdoor area for the use of residents year round. Fencing or other encloses may be installed around secure areas. Residents must be able to access the secure areas in facilities establishing a secured environment after June 1, 2004.
Medication Administration
Most larger facilities have hired LPNs to administer or manage medications and ensure that physicians’ orders have been received and recorded. Staff who have completed a medication training course given by a licensed nurse, physician, physician’s assistant, or pharmacist and who have passed a competency test may assist with and administer medications (except injections).
Public Financing
Services in alternative care facilities have been covered since 1984 under a 1915(c) waiver for elders, people with disabilities, MR/DD, and people with mental illness. Medicaid rules limit room-and-board charges for Medicaid recipients to $518 a month. The Medicaid rate for services is $36.03 a day. The rate covers oversight, personal care, homemaker, chore, and laundry services. A pilot program tested the impact of an enhanced rate to create incentives to retain people as their needs increased and to accept residents with greater needs from nursing homes and hospitals. An additional $400 per month was available for residents who have enhanced needs in three of four areas: personal care, mobility, incontinence, and behavior/confusion. There is continuing interest in developing a tiered rate methodology.
The SSI payment is $564 and the PNA is $46 a month.
| Monthly Rates 2004 | |
|---|---|
| Room and board | $518.00 |
| Service | $1,094.31 |
| Total | $1,612.31 |
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participation | Facilities | Participation | Facilities | Participation |
| 273 | 3,804 | 266 | 3,773 | 243 | 2,654 |
Family members are allowed to supplement resident income for items that are not covered in the Medicaid rate. Most supplementation allows residents to move from a semiprivate to private unit. Medicaid allows residents up to 42 days “leave” per year for nonmedical purposes. Facilities receive the Medicaid payment during this period.
Staffing
Facilities must employ sufficient staff to ensure provision of services necessary to meet resident needs including services provided under the care plan and services provided under the resident agreement. Facilities contracting with Medicaid must maintain a 1:10 staff ratio during the day and a 1:15 ratio from 7 p.m. to 6 a.m., unless a lower ratio that does not jeopardize the health and safety of residents can be documented. Facilities that are Medicaid certified and provide a secure environment must have a 1:6 ratio and awake staff at all times.
Training
Administrators must meet the minimum education, training, and experience requirements by successfully completing a program approved by the department. Acceptable programs may be conducted by an accredited college; university or vocational school; or a program, seminar, or in-service training program sponsored by an organization, association, corporation, group, or agency with specific expertise in that area. The curriculum includes at least 30 actual clock hours of which at least 15 consist of a discussion of each of the following topics: resident rights; environment and fire safety, including emergency procedures and first aid; assessment skills; identifying and dealing with difficult behaviors; and nutrition.
The remaining 15 hours shall provide emphasis on meeting the personal, social, and emotional care needs of the resident population served.
Administrators of facilities contracting with Medicaid must complete training on rules and regulations for ACFs.
Staff. All staff, including volunteers, must be given on-the-job training or have related experience in the job assigned to them and shall be supervised until they have completed on-the-job training appropriate to their duties and responsibilities or have had previous related experience evaluated. Training and orientation in emergency procedures shall be provided to each new staff member, including volunteers, within three days of employment.
Staff members not serving as an operator of the facility who have direct responsibility for the provision of personal care, i.e. hygiene, of residents or for the supervision or training of residents in the residents’ own personal care, shall provide documentation of either successful completion of course work in the provision of personal care or previous and related job experience in providing personal care to residents.
Before providing direct care, staff must receive training specific to the needs of the population served, resident rights, environment and fire safety, first aid and injury response, the care and services of current residents, and the facility’s medication administration program.
The facility shall provide adequate training and supervision for staff comprising a discussion of each of the following topics: resident rights, environment and fire safety, including emergency procedures and first aid; assessment skills; and identifying and dealing with difficult situations and behaviors.
ACF staff must be trained in the needs of the population served.
Background Check
The owner or licensee may have access to and shall obtain any criminal history record information from a criminal agency for all persons responsible for the care and welfare of residents. Owners and administrators must undergo a finger print check. Owners are responsible for obtaining a criminal background check of administrators to determine whether they have been convicted of a felony and misdemeanor that could pose a risk to the health, safety and welfare of residents.
Monitoring
The regulations require that facilities provide the ombudsman program with access to the facility and residents at reasonable times. New remedies were incorporated in HB 02-1323 and include requiring written plans to correct violations found as a result of inspections; retaining a consultant to address corrective measures; monitoring by the department for a specific period; providing additional training to employees, owners, or operators of the residence; complying with a directed written plan to correct the violation; or paying a civil fine not to exceed $2,000 in a calendar year.
Civil fines are used for expenses related to continuing monitoring; education to avoid restrictions or conditions or to facilitate the application process or the change of ownership process; education for residents and their families about resolving problems with a residence, rights of residents, and responsibilities of residences; providing technical assistance to any residence for the purpose of complying with changes in rules or state or federal law; relocating residents to other facilities or residences; maintaining the operation of a residence pending correction of violations; closing a residence; or reimbursing residents for personal funds lost.
Fees
HB 02-1323 sets fee of $150, plus $23 per bed. Fees for facilities with a high percentage of Medicaid beneficiaries pay $15 per bed. Fees for new construction are $5,000. Facilities pay a fee of $2,500 to reissue a license due to a change in ownership. Facilities with secure environments are assessed a fee of $1,500.
The new rules establish fees for reviewing construction plans: new construction or remodeling of 2,000 square feet or less, $500; and $.25 per additional square foot over 2,000. Remodeling limited to installation or renovation of fire suppression systems: 3-16 beds, $500; 17-40 beds, $750; 41-60 beds, $1,000; and 61 or more beds, $1,250. Fees cannot exceed $2,000.
Connecticut
Citation
Assisted living services agency; Connecticut General Statutes §19a-490
Connecticut Department of Public Health, Public Health Code §19-13-D105
Residential care homes (homes for the aged, rest homes) §19-13-D-6
General Approach and Recent Developments
Assisted living regulations issued by the Health Department were last revised in June 2001. The regulations take a unique approach by allowing “managed residential communities” (MRCs) to offer assisted living services through assisted living services agencies (ALSAs). MRCs may obtain a license to also serve as an ALSA. Rules governing medication administration in residential care homes were revised in March 2002. Medicaid waiver and state funds are being used to cover services provided by Assisted Living Service Agencies.
The State is currently focusing on level of care concerns in managed residential communities providing assisted living services. Since the regulations went into effect, residents have aged in place, and the State wants to ensure that residents are receiving the right amount of services. The State encourages aging in place, but as the regulatory body, needs to ensure that services are available to meet resident needs.
| Category | 2004 | 2002 | 2000 | 1998 | ||||
|---|---|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted living services agencies | 65 | NA | 63 | NA | 48 | NA | 22 | NA |
| Managed residential communities | 104 | NA | NR | NR | NR | NR | NR | NR |
| Residential care homes | 101 | 2,753 | 109 | 2,949 | 113 | NR | 113 | NR |
The ALSA regulations focus on the licensing of agencies to provide services rather than the licensing of building and services as an entity. MRCs have to notify the health department of their intention to provide assisted living services and present specified information and assurances to the department. The ALSA, either the MRC or another agency, must be licensed by the Department of Public Health to provide services. The MRC is not licensed by the Department of Public Health. MRCs must show evidence of compliance with local zoning ordinances and building codes.
A pilot program to build 300 units to serve low-income residents has been implemented jointly by the Department of Social Services, Department of Economic Development, Department of Public Health, Office of Policy and Management and the Connecticut Housing Finance Authority.
Definition
An assisted living services agency means an institution that provides, among other things, nursing services and assistance with activities of daily living to a population whose conditions are chronic and stable.
Assisted living services means nursing services and assistance with ADLs provided to clients living within a managed group-living environment having supportive services that encourage clients primarily age 55 or older to maintain a maximum level of independence. Routine household services may be provided as assisted living services or by the managed residential community. These services provide an option for elderly persons who require some help or aid with ADLs and/or nursing services.
A managed residential community means a facility consisting of private residential units that provides a managed group living environment, including housing and services primarily for persons age 55 or older.
Residential care home means an institution having facilities and all necessary personnel to furnish food, shelter and laundry for two or more persons unrelated to the proprietor and in addition, providing services of a personal nature which do not require the training or skills of a licensed nurse. Additional services of a personal nature may include assistance with bathing, help with dressing, preparation of special diets and supervision over medications which are self-administered.
Unit Requirements
Managed residential communities. To qualify as a managed residential community and a setting in which assisted living services may be provided, units are defined as a living environment belonging to a tenant(s) that includes a full bathroom within the unit including water closet, lavatory, tub or shower bathing unit, and access to facilities and equipment for the preparation and storage of food. Managed residential communities may not require tenants to share units. Sharing of a unit shall be permitted solely upon the request and mutual consent of tenants.
Residential care homes. Single rooms must have a minimum of 150 square feet, excluding closets, toilet rooms, lockers or wardrobes and vestibule. Multiple bed rooms must have a minimum of 125 square feet per bed. A resident unit shall be 25 beds. No resident room shall be designed to permit more than two (2) beds. Baths must have one separate shower or bathtub for every eight residents. There must be one separate shower and one separate bathtub per resident unit. One toilet may serve two resident rooms, but no more than four residents.
Admission/Retention Policy
Assisted Living Service Agencies. Each ALSA agency will develop its own admission and discharge criteria but the regulations do not allow the ALSAs to impose unreasonable restrictions and screen out people whose needs may be met by the ALSA. Assisted living services may be provided to residents with chronic and stable health, mental health, and cognitive conditions as determined by a physician or health care practitioner.
Discharge policies must include categories for the discharge of clients, which include but are not limited to change in resident’s condition; routine discharge; emergency discharge; financial discharge; and premature discharge.
Nursing Home Admission Policy
The State requires that residents have uncontrolled and/or unstable and/or chronic conditions requiring continuous skilled nursing services and/or nursing supervision or have chronic conditions requiring substantial assistance with personal care on a daily basis.
Services
Assisted Living Service Agencies. Core services provided by managed residential communities include three meals a day; laundry; scheduled transportation; housekeeping; maintenance services including chore services for routine domestic tasks that the tenant is unable to perform; and social and recreational services. In addition, 24-hour a day security and emergency call systems in each unit are required. Communities must have a service coordinator who assists tenants and acts as a liaison with the ALSA. Service coordinators ensure that all core services are provided to or are made available to residents, assist residents in making arrangements to meet their personal needs, establish collaborative relations with provider agencies, support services and community resources, establish a resident council, and ensure that a resident information system is in place.
The managed residential community, through its service coordinator or any other representative, may not provide health services, including but not limited to the provision of rehabilitative therapy, administration or supervision of the self-administration of medications, nursing care or medical treatment, unless it has been licensed as an assisted living services agency. It may contract with one or more assisted living services agencies, home health care agencies, or other appropriately licensed health care providers to make available health services for tenants provided by such licensed persons or entities.
Trained aides may provide assistance with ADLs; assistance with exercise, ambulation, transfer, and self-administration of medications; and routine household tasks.
Nursing services may only be provided by licensed ASLAs or other appropriately licensed agencies or individuals. Nursing services include client teaching, wellness counseling, health promotion and disease prevention, medication administration and delegation of supervision of self-administered medications, and provision of care and services to clients whose conditions are chronic and stable.
Registered nurses may also perform quarterly assessments, coordination, orientation, training, and supervision of aides.
Residential care homes. Services provided include recreational activities, laundry, housekeeping, and maintenance services.
Dietary
Assisted Living Service Agencies. Managed residential communities must offer three meals a day. Other aspects of food service are not specified in the Assisted Living Service Agency regulations.
Residential care homes. Menus shall be prepared, posted and filed and shall meet state department of health requirements for basic nutritional needs.
Agreements
Assisted Living Service Agencies. A “bill of rights” must be developed and signed for each resident upon move-in. The agreement includes: services available, charges and billing mechanisms; 15-day notice of changes; criteria for admission to service; rights to participate in service planning; client responsibilities; information about the complaint process; circumstances for discharge; description of Medicare-covered services and billing and payment for such services and other rights.
Residential care homes. Agreements are not required for residential care homes.
Provisions for Serving People with Dementia
Not specified.
Medication Administration
Assisted Living Service Agencies. The regulations allow for administration of medications by licensed staff. Assisted living aides may supervise the self-administration of medications which includes reminding, verifying, and opening the package. All medications must be stored in the resident’s unit.
Residential care homes. Residents of licensed residential care homes may self administer medications, and may request assistance from staff with opening containers or packages and replacing lids. Unlicensed personnel who administer medications must be certified.
Prior to the administration of any medication by program staff members, the program staff members who are responsible for administering the medications shall first be trained by a registered pharmacist, physician, physician assistant, advanced practice registered nurse or registered nurse in the methods of administration of medications and shall have successfully completed a written examination and practicum administered by the Connecticut League For Nursing or other department-approved certifying organization.
Public Financing
The State provides assisted living services through ALSAs to elders in sixteen state funded congregate housing projects and three HUD facilities that have been approved as MRCs. State general revenue and Medicaid waiver funds were made available January 1, 2003, for a pilot program that serves 75 people in private assisted living facilities. State funds are available to residents who do not meet Medicaid financial or functional criteria.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participation | Facilities | Participation | Facilities | Participation |
| 34 | 65 | NA | NA | NA | NA |
A nursing home transition grant is being implemented to assist residents to relocate to community settings. The grant includes funding for transitional expenses. The grant is going to be coming to a close in 2004. However, the Governor’s budget for FY 2005 includes a recommendation for the State to fund 100 percent of the grant for an additional 3 years.
An RFP was issued in 1999 by the Connecticut Housing Finance Authority “to test the extent to which subsidized assisted living communities are a viable and cost effective response for frail seniors facing inappropriate nursing facility admission.” Four projects have been approved for development. Two of the projects are under construction with the first to open this summer and the other in late 2004/early 2005. Two hundred nineteen subsidized units have been selected thus far. At least 40 percent of the units must be occupied by residents with less than 50 percent of the median income. Services for eligible low-income residents (less than $1,692 per month income or 300 percent of the federal SSI benefit) are covered by the State’s home care and Medicaid waiver programs. Tenants may retain a personal needs allowance of $164. Residents pay a share of the rent and $330 a month for meals. Any remaining income is applied to the cost of the Medicaid, or state-funded, services. Family supplementation is allowed.
Reimbursement for core services (housekeeping, laundry, maintenance/chore, recreation, medical and nonmedical transportation, emergency response, and service coordination) is $8 per day. Meals are billed to the client. Per diem payments for four levels of personal assisted living services are reimbursed as follows:
- Occasional personal services: 1 hour per week and up to 3.75 hours, including nursing supervision as needed
- Limited personal services: 4 hours per week and up to 8.75 hours per week of personal services plus nursing visits as needed
- Moderate personal services: 9 hours per week and up to 14.75 hours of personal services plus nursing visits as needed
- Extensive personal services: 15 hours per week and up to 25 hours of personal services plus nursing visits as needed.
Under the Demonstration project described above, each project sets its own rates for each level of care but cannot exceed a maximum amount for each level. For the other assisted living initiatives the State is sponsoring, the rate for each level of care is set by the State.
Staffing
ALSAs must have at least one RN in addition to an on-site supervisor. A supervisor must be available 20 hours a week for every 10 or fewer licensed nurses or assisted living aides and a full-time supervisor for every 20 licensed nurses or aides. A sufficient number of aides must be available to meet residents’ needs. All aides must be certified Nurses Aides or Home Health Aides and must complete 10 hours of orientation and one hour of in-service training every 2 months.
Twenty-four hour awake staff are not required since the needs vary among managed residential communities. However, 24-hour staffing could be required if indicated by resident plans of care. An RN must be available on-call, 24 hours a day.
Residential care homes. There must be at least one attendant on duty at all times for every 25 residents.
Training
Each ALSA must have a 10-hour orientation program for all employees which shall include but not necessarily be limited to the following:
- Organizational structure of the agency and philosophy of assisted living services;
- Agency client services policies and procedures;
- Agency personnel policies; and
- Applicable regulations governing the delivery of assisted living services.
Aides must pass a competency exam. Each agency shall have an in-service education policy that provides an annual average of at least 1 hour bimonthly for each assisted living aide.
The in-service training shall include but not be limited to current information regarding specific service procedures and techniques and information related to the population being served.
Residential care homes. New staff must receive an initial orientation prior to being allowed to work independently including, but not limited to, safety and emergency procedures for staff and residents, the policies and procedures of the residential care home, and resident rights.
Continuing education for program staff shall be required for 1 percent of the total annual hours worked (to a maximum of 12 hours) per year. Such education shall include, but is not limited to, resident rights, behavioral management, personal care, nutrition and food safety, and health and safety in general.
Background Check
Not described.
Monitoring
ALSAs are required to establish a quality assurance committee that consists of a physician, a registered nurse, and a social worker. The committee meets every four months and reviews the ALSA policies on program evaluations, assessment and referral criteria, service records, evaluation of client satisfaction, standards of care, and professional issues relating to the delivery of services. Program evaluations are also to be conducted by the quality assurance committee. The evaluation examines the extent to which the managed residential community’s policies and resources are adequate to meet the needs of residents. The committee is also responsible for reviewing a sample of resident records to determine whether agency policies were followed, whether services are provided only to residents whose level of care needs can be met by the ALSA, and whether care is coordinated and appropriate referrals are made when needed. The committee submits an annual report to the ALSA summarizing findings and recommendations. The report and actions taken to implement recommendations are made available to the State Department of Public Health.
Agencies are inspected biennially. Penalties include revocation, suspension, or censure; letter of reprimand; probation; a restriction on acquisition of other entities; a consent order compelling compliance; and civil monetary penalties.
Fees
Fees are not required for ALSAs.
Delaware
Citation
Assisted living facilities; Title 16 Health and Safety, Part II, Chapter II, §63.0 et seq.
Rest residential homes; Delaware code, Part II §59.0 et seq.
General Approach and Recent Developments
The State added an assisted living category in 1997. No additional rest residential homes will be licensed and most have converted to assisted living facilities. A Medicaid waiver was implemented in 1999.
Revised rules were adopted in October 2002. A new “purpose” section describes the goal of the regulations to “promote and ensure the health, safety and well-being of all residents of assisted living facilities…to ensure that service providers will be accountable to their residents and the Department and to differentiate assisted living from nursing facilities.” It replaces the purpose statement that directs that the “services are provided based on the social philosophy of care and must include oversight, food, shelter and the provision or coordination of a range of services that promote quality of life of the individual. The social philosophy of care promotes the consumer’s independence, privacy, dignity and is provided in a home-like environment.”
Further revisions were proposed in 2004. The definition of incident and reportable will be refined to include all reportable incidents and the additional occurrences or events listed in the regulations. The proposed changes will require emergency electrical generators in assisted living facilities and revise the prohibition against facilities serving an individual with a central line from an assisted living facility by creating an exception for subcutaneous venous ports.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted living facilities | 29 | 1,738 | 27 | 1,300 | 18 | 927 |
| Rest residential homes | 3 | NR | 6 | 160 | 4 | 99 |
Definition
Assisted living is a special combination of housing, supportive services, supervision, personalized assistance, and health care designed to respond to the individual needs of those who need help with activities of daily living and/or instrumental activities of daily living.
Rest residential home is an institution that provides resident beds and personal care services for persons who are normally able to manage activities of daily living. The home should provide friendly understanding to persons living there as well as appropriate care in order that the resident’s self-esteem, self-image, and role as a contributing member of the community may be reinforced.
Unit Requirements
Assisted living. The rules require 100 square feet for single bedrooms in new facilities and converted facilities of more than 10 units, and 80 square feet per resident for rooms with two residents. No more than two residents may share a room. Bathrooms are provided in the unit or, if shared, one for every four residents. Consumers must have access to a readily available central kitchen if one is not provided in the unit. Bathing facilities must be provided in the unit or in a readily accessible area.
Rest residential homes provide 100 square feet for single occupancy and 80 square feet per resident for multiple occupancy rooms. No more than four people may share a room. One bathtub or shower and one toilet and wash basin are required for every four residents.
Admission/Retention Policy
Assisted living. The rules do not allow agencies to admit people who require more than intermittent or short-term nursing care; require skilled monitoring, testing, and aggressive adjustment of medications and treatments; require monitoring of a chronic medical condition that is not essentially stabilized; are bedridden more than 14 days; have Stage III or IV pressure sores; require a ventilator; require treatment for a disease or condition which requires more than contact isolation; have an unstable tracheotomy or a stable tracheotomy of less than six months’ duration; have an unstable peg tube; require IV or central line; wander to the extent that facilities cannot provide adequate supervision or security arrangements; pose a threat to themselves or others; or are socially inappropriate. Waivers may be granted to allow facilities to temporarily care for people with excluded conditions for up to 90 days so long as services are provided by appropriate health professionals. Pending regulations would allow individuals needing an IV or central line to be served if the facility meets specified documentation and service requirements.
Rest residential homes. No specific requirements are stated other than in the definition of a resident.
Nursing Home Admission Policy
Eligibility for the waiver is based on professional judgment concerning ADLs, and medication and safety supervision. Individuals must have impairments in two ADLs to receive waiver services in the home, and services in assisted living facilities are targeted to people with three ADL impairments.
Services
Assisted living. A medical evaluation and an assessment by an RN must be completed 30 days prior to admission using the Department’s uniform assessment instrument and must be reviewed within 30 days after admission. Individual service agreements address all the physical, medical and psychosocial services to be provided: personal care, services by a licensed nurse, food, nutrition and hydration, environmental services (laundry, housekeeping, trash removal, and safety), psychosocial/emotional, banking, transportation, furnishings, assistive technology and durable medical equipment, rehabilitation services, and interpretive services.
Managed or negotiated risk agreements are used to describe mutually agreeable action that balances resident choice and independence with the health and safety of the resident and others. A managed/negotiated risk agreement is negotiated when the risks are tolerable to all parties participating in the development of the managed/negotiated risk agreement and a mutually agreeable action is negotiated to provide the greatest amount of resident autonomy with the least amount of risk. The resident must be capable of making choices and decisions and understanding consequences. The agreement clearly describes the problem, issue or service that is the subject of the managed/negotiated risk agreement; describes the choices available to the resident as well as the risks and benefits associated with each choice, the assisted living facility’s recommendations or desired outcome, and the resident’s desired preference; indicates the agreed-upon option; describes the agreed upon responsibilities of all parties and is a part of the service agreement.
Rest residential homes provide shelter, housekeeping, board, and personal surveillance or direction in activities of daily living.
Dietary
Food services are covered in the tenant service agreement.
Agreements
Prior to executing a contract, residents must receive a statement of all charges. The contract includes nonfinancial and financial components. The nonfinancial issues include a listing of basic and optional services; optional services that may be provided by third parties; a statement of resident’s rights and an explanation of the grievance procedure; occupancy provisions such as policies concerning modifications to the resident’s living area, procedures for changing the resident’s accommodations (relocation, roommate, number of occupants in the room), transfer procedures, security, staff’s right to enter a resident’s room, resident rights and obligations, temporary absence policy, interim service arrangement during an emergency, discharge policies and procedures, obligations of the facility, and a listing of the resident’s personal belongings. The financial areas include the party responsible for handling finances, obtaining equipment and supplies, arranging services not covered by the contract, disposing of belongings, and the rate structure and payment provisions.
Provisions for Serving People with Dementia
Facilities offering special care must disclose the philosophy of care; the population served; admission and discharge process and criteria; the assessment, care planning and implementation process; staffing plan and training policies; physical environment and design features; resident activities; family role; psychosocial services; nutrition and hydration services; policies on wandering, safe storage of medications and costs.
Medication Administration
Aides who have passed an examination are allowed to assist with self-administration of medications. Rules governing assistance with medications are covered by regulations issued by the Board of Nursing. An RN must review medications within 30 days of admission for people who self-administer to assess the resident’s cognitive and physical ability and need for assistance. Reviews are also conducted for residents who self-administer to ensure proper labeling and storage, that medications have been received, and to determine their effects and the presence of adverse side effects.
Public Financing
The State provides waiver services to elders and adults with disabilities in assisted living facilities with income below 250 percent of the federal SSI level. The SSI payment and state supplement is $704 a month. The room-and-board payment for SSI beneficiaries is $598 and residents retain a personal needs allowance of $106 a month. Residents with higher incomes may be charged a higher room-and-board amount.
Three levels of payment for services are available. Facilities receive a 10 percent additional payment for residents with cognitive impairments. The payment levels are based on spending for HCBS waiver clients living in their own homes and participants in the adult foster care program. Family members are allowed to supplement room and board payments.
The Medicaid waiver program coverage began late in 1999.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participation | Facilities | Participation | Facilities | Participation |
| 29 | 14 | 11 | NR | 7 | 20 |
| Level I | Level II | Level III | |
|---|---|---|---|
| Room and board | $598 | $598 | $598 |
| Services | $940 | $1,180 | $1,460 |
| Total | $1,538 | $1,778 | $2,058 |
Staffing
Assisted living facilities must employ a sufficient number of trained staff to meet the needs of residents. They must also have a director of nursing who is a registered nurse who is full time in facilities over 25 beds, 20 hours a week in facilities with 5 to 24 beds, and 8 hours a week in facilities under 5 beds.
Training
Assisted living--Administrators. Requirements for administrators vary with the size of the facility. Facilities over 25 units must have a full-time nursing home administrator; 5 to 24 beds, a half-time nursing home administrator. Facilities with four or fewer beds must have an administrator with a baccalaureate degree or associates degree with 2 years experience, an RN with 4 years experience or an LPN with 4 years experience or 5 years experience in a related health or social service field.
Staff. Resident assistant orientation covers fire and life safety and emergency disaster plans; infection control; basic food service; first aid and the Heimlich maneuver; job responsibilities; health and psychosocial needs of the residents served; the assessment process; use of service agreements; resident rights and reporting of abuse, neglect, and mistreatment; and hospice services. A minimum of 12 hours of annual training must be provided. Orientation is required for temporary staff.
Rest residential homes. Nurse aide/nurse assistant staff must complete a training course approved by the State Board of Nursing and the Board of Health. Aides/assistants must be certified prior to employment. Section 609 describes the curriculum and the competencies that must be measured in the following areas: nurse aide role and function; environmental needs; psychosocial needs; and physical needs. Section 59.610 describes the qualifications of instructors and the training instructors must receive.
Background Check
Facilities must obtain a report of each employee’s entire criminal history record from the State Bureau of Identification and a report from DHSS regarding its review of a report of the person’s entire federal criminal history. The State also has a mandatory drug testing law. Civil money penalties of $1,000 to $5,000 per occurrence for violations of the criminal background check and drug testing law may be imposed by the licensing agency.
Monitoring
Assisted living. Facilities must develop and implement an ongoing quality assurance program that includes internal monitoring of performance and resident satisfaction. Satisfaction surveys of all residents must be conducted twice a year. Pending regulations will require reporting of falls without injury and falls with injuries that do not require transfer to an acute care facility or do not require reassessment of the resident; errors or omissions in treatment or medication; injuries of unknown source and lost items, in accordance with facility policy.
Fees
Fees are set by statute. The fee for an initial application and background examination is $500. Annual fees are $400 for facilities under 100 beds and $550 for facilities over 100 beds.
District of Columbia
Citation
Community Residence Facilities; DC Law 5-48; DC Code §32-1301 et seq.; Chapter 34, §3400 et seq.
Assisted Living Residences; DC Law 13-127 §60847 of DC Register, p. 2647
General Approach and Recent Developments
An RFP was issued in March 2004 to hire a contractor to develop a program to license and monitor Assisted Living Residences (ALRs). The goals of the program are to assure the quality of care provided in ALRs according to the Act, develop a monitoring system that is client centered, and develop an evaluation system that will measure the quality of care being given to residents. The Assisted Living Residence Regulatory Act was passed in June 2000. The assisted living law includes a philosophy of care that emphasizes personal dignity, autonomy, independence, privacy, and freedom of choice. The services and physical environment should enhance a person’s ability to age in place in a home-like setting by increasing or decreasing services as needed.
The HCBS Medicaid waiver was amended in June 2003 to include a new category of service for assisted living. The service will be implemented after licensure regulations for assisted living are developed.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Community residence facility | 200 | 1,866 | NR | NR | NR | NR |
Definition
An assisted living residence means an entity, whether public or private, for profit or not for profit, that combines housing, health services, and personal assistance--in accordance with individually developed service plans--for the support of individuals who are unrelated to the owner or operator of the entity.
A community residence facility is one that provides safe, hygienic sheltered living arrangements for one or more individuals aged 18 years or older (except in the case of group homes for mentally retarded persons, no minimum age limitation shall apply), not related by blood or marriage to the residence director, who are ambulatory and able to perform the activities of daily living with minimal assistance. The definition includes facilities, including halfway houses and group homes for mentally retarded persons, which provide a sheltered living arrangement for persons who desire or require supervision or assistance within a protective environment because of physical, mental, familial, or social circumstances, or mental retardation. The definition does not include facilities providing sheltered living arrangements to persons who are in the custody of the Department of Corrections of the District of Columbia.
Unit Requirements
Assisted living residences. Newly constructed or renovated rooms must have 80 square feet per resident. No more than two persons may share a bedroom. Full bathrooms must be available for every six residents. ALRs serving more than 16 residents may offer living units that include kitchenette, living rooms, and bathrooms. Units that do not include bathrooms must limit sharing of bathrooms to four residents.
Community residence facilities. No more than four persons may share a bedroom. Minimum square footage and bathing and toilet facilities requirements are specified in the DC Housing Code (14 DCMR).
Admission/Retention Policy
Assisted living residences. ALRs may not accept those who are dangerous to themselves or others, exhibit behavior that negatively impacts the lives of others, are at risk for health or safety complications which cannot be addressed by the home, and requires more than 35 hours a week of skilled nursing and home health aide services, provided on less than a daily basis, and residents who require more than intermittent skilled nursing care, treatment of Stage III or IV skin ulcers, ventilator services, or treatment for an active, infectious, and reportable disease.
Residents have the right to remain in the facility despite a recommendation to transfer, if they obtain additional services that are acceptable to the ALR.
Community residence facilities. Prospective residents, the residence director and the resident’s physician must agree that the prospective resident does not need professional care and can be assisted safely and adequately within a community residence facility. Residents must be able to perform ADLs with minimal assistance, generally be oriented as to person and place, and capable of exercising proper judgment in taking action for self-preservation under emergency conditions. By special permission of the mayor, persons who are not generally oriented or who are substantially ambulatory but need minimal ADL assistance may be admitted if sufficient staff resources are available.
Services
Assisted living residences. ALRs must offer or coordinate for payment 24-hour supervision, assistance with scheduled and unscheduled ADLs and IADLs as needed, as well as provision or coordination of recreational and social activities and health services in a way that promotes optimum dignity and independence for residents. Services include 24-hour supervision and oversight, three nutritious meals and snacks modified to meet individual dietary needs, at a minimum some assistance with ADLs and IADLs to meet scheduled and unscheduled needs, and laundry/housekeeping services. ALRs facilitate access to appropriate health and social services and provide or coordinate transportation to community based services.
An assessment must be completed within 30 days of admission. An individual service plan is required that is signed by the resident and identifies services provided, when they are provided, and by whom. The plan is based on a medical, rehabilitation, and psychosocial assessment; functional assessment; and reasonable accommodation of resident and surrogate preferences. A shared responsibility agreement is also required. Whenever disagreements arise as to lifestyle, personal behavior, safety, and service plans the ALR staff, resident or surrogate, and other relevant service providers shall attempt to develop a shared responsibility agreement.
The ALR must explain to the resident, or surrogate, why the decision or action may pose risks and suggest alternatives to the resident; and discuss with the resident, or surrogate, how the ALR might mitigate potential risks. If the resident decides to take action that may involve increased risk of personal harm and conflict with the ALR’s usual responsibilities, the ALR describes to the resident the action or range of actions subject to negotiation; and negotiate a shared responsibility agreement, with the resident as a full partner, acceptable to the resident and the ALR that meets all reasonable requirements implicated. The shared responsibility agreement shall be signed by the resident or surrogate and the ALR.
Community residence facilities. Meals, housekeeping, laundry, and dietary services are provided. Short-term nursing care, 72 hours, may be provided or arranged by the facility.
Agreements
Assisted living residences. Written contracts cover the ALRs’ organizational affiliation, the nature of any special care offered, services included or excluded, residents’ rights and grievance process, unit assignment procedures, admission and discharge policies, responsibilities for coordinating health care, arrangements for notification in the event of the resident’s death, obligations for handling finances, renting of equipment, coordinating and contracting for services not provided by the ALR, purchase of medications and durable medical equipment, rate structure and payment provisions, 45-day notice for changes in rates, procedures to be followed in the event the resident can no longer pay for services, and terms governing refunds.
Provisions for Serving People with Dementia
Not described.
Medication Administration
Assisted living residences. Trained aides may administer medications. A medication aide training program approved by the board of nursing will be developed. ALRs must arrange for an on-site review by a registered nurse every 45 days that covers supervision of administration by trained medication aides, resident responses to medications, and resident ability to self-administer medications.
Community residence facilities. Facilities must provide each resident a means of storing medications. Assisting with self-administration is listed as an activity of daily living.
Public Financing
Assisted living residences. A Medicaid HCBS waiver amendment was approved by CMS in June 2003. The amendment added the 18 to 64 population with physical disabilities, and added two additional services: consumer-directed care and assisted living. Assisted living, while an approved service, will not be implemented until assisted living licensure regulations have been passed. The State has contracted with an independent consultant to develop a case-mix reimbursement system for nursing homes, and will also develop assisted living rates. This work cannot be completed until the assisted living licensure regulations are in effect.
Community residence facilities. The SSI payment standard is $564 a month and the PNA is $70.
Staffing
Administrators must have a high school diploma or GED and at least 1 year’s experience as a direct care provider/administrator and have satisfactory knowledge of the philosophy of assisted living, the health and psychosocial needs of residents, assessment process, development and use of ISPs, medication administration, provision of ADL/IADL assistance, residents’ rights, fire and life safety codes, infection control, food safety and sanitation, first aid and CPR, emergency disaster plans, human resource management, and financial management.
The ALR must have a staffing plan to assure the safety and proper care of residents based on the needs of residents, the size and layout of the facility, and the capabilities and training of staff.
Training
Forty hours of initial training is required on delivering care for bedbound residents, use of first aid kits, procedures for detecting and reporting abuse, managing difficult behaviors, advanced body mechanics, communicating with adults with communication deficits, recognizing the signs and symptoms of dementia, caring for people with cognitive impairments, techniques for assisting in overcoming trauma, awareness of changes in conditions, and basic competence in housekeeping.
Staff must complete 12 hours of in-service training annually on emergency procedures and disaster drills, and rights of residents. Staff must also complete 12 hours of annual training on managing residents with dementia conducted by a nationally recognized organization with experience in Alzheimer’s care.
Background Check
Assisted living residences. Background checks as required by federal and district laws are required.
Community residence facilities. The licensing agency may conduct background checks on the licensee which include contacts with the police to determine criminal convictions.
Monitoring
Assisted living residences. The proposed system, as outlined in the RFP, will measure the ability of the ALR to fulfill customers’ expectations and to provide for the health and safety of the residents. Surveyors will gather information from a variety of sources including: a survey questionnaire; interviews with the residents, family, staff and other customers; and, from a review of the medical records. It will also include a customary inspection of life safety support, fire safety systems, emergency and disaster planning, physical plant, environmental services, food services, sanitation, medical administration and other systems.
Fees
Not reported.
Florida
Citation
Assisted living facilities; Florida Statutes Chapter 400 Part 3; Florida Administrative Code Chapter 58A-5 et seq.
General Approach and Recent Developments
The State provides for several types of assisted living facility (ALF) licensing: standard, extended congregate care, limited nursing services, and limited mental health services. Following passage of legislation signed into law on May 15, 2001, requiring the filing of ALF adverse incident reports and liability claims, less than 5 percent of the facilities reported that liability claims have been filed. The regulations were revised in 2001. A number of technical changes are being considered. In July 2003, responsibility for training administrators and service staff were transferred from the Department of Elder Affairs to private organizations.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted living facilities | 2,250 | 74,762 | 2,328 | 78,348 | 2,361 | 77,292 |
Definition
Assisted living facility means any building or buildings, section or distinct part of a building, private home, boarding home, home for the aged, or other residential facility, whether operated for profit or not, which undertakes through its ownership or management to provide housing, meals, and one or more personal services for a period exceeding 24 hours to one or more adults who are not relatives of the owner or administrator.
Standard: A facility licensed to provide housing, meals, and one or more personal care services for a period exceeding 24 hours. Personal services include direct physical assistance with or supervision of a resident’s activities of daily living and the self-administration of medication and similar services. The facility may employ or contract with a person licensed under Chapter 464, F.S., to administer medication and perform other tasks as specified in §400.4255, F.S., such as take vital signs, manage individual weekly pill organizers for residents who self-administer medication, give prepackaged enemas ordered by the physician, observe residents, and document in the resident’s record.
Limited nursing services: A facility licensed to provide any of the services under a standard license and those services specified in §58A-5.031(1)(a)-(m). Those services include: conducting passive range of motion exercises; applying ice caps or collars; applying heat; cutting toenails of diabetic residents or residents with a documented circulatory problem if the written approval of the resident’s health care provider has been obtained; performing ear and eye irrigations; conducting a urine dipstick test; replacing established self-maintained in-dwelling catheter or performing intermittent urinary catheterizations; performing digital stool removal therapies; applying and changing routine dressings that do not require packing or irrigation, but are for abrasions, skin tears, and closed surgical wounds; caring for Stage II pressure sores; caring for casts, braces, and splints; conducting nursing assessments if conducted by, or under the direct supervision of, a registered nurse; and for hospice patients, providing any nursing service permitted within the scope of the nurse’s license, including 24-hour supervision.
Extended congregate care: A facility licensed to provide any of the services under a standard license and LNS license, including any nursing service permitted within the scope of the nurse’s license consistent with ALF residency requirements and the facility’s written policy and procedures. A facility with this type of license enables residents to age in place in a residential environment despite mental or physical limitations that might otherwise disqualify them from residency under a standard or LNS license. This definition creates a higher level of care in assisted living which requires an additional license. Facilities with an ECC license must develop policies which allow residents to age in place and which maximize independence, dignity, choice, and decision making; specify the personal and supportive services that will be provided; specify the nursing services to be provided; and describe the procedures to ensure that unscheduled service needs are met.
Limited mental health license: An ALF that is licensed to serve three or more mental health residents. A mental health resident is an individual who receives social security disability income or SSI income due to a mental disorder as defined by the Social Security Administration and receives optional state supplementation. The facility, mental health resident, and case manager must complete a community living support plan that includes the needs of the resident that must be met in order to enable the resident to live in an ALF and the community. The mental health provider and the facility must execute a cooperative agreement with each mental health resident which provides procedures and directions for accessing emergency and after-hours care.
Unit Requirements
Facilities licensed to provide extended congregate care must provide private rooms or apartments, or semi-private room or apartment shared with a roommate of choice, with a lockable entry door. Facilities that offer rooms rather than apartments must have bathrooms shared by no more than four residents. Private rooms must be 80 square feet and shared rooms 60 square feet per resident.
Facilities that do not have the ECC license and were licensed after October 1999 may offer shared rooms (maximum of two per room), a bathroom for every six residents, and bathing facilities for every eight residents. Facilities licensed prior to October 1999 may allow four people to share a room.
Admission/Retention Policy
Admission. The regulations for “admissions” to all assisted living facilities are specific (see matrix below).
Continued residency. Additional criteria affect continued residency. In standard assisted living facilities, people who are bedridden more than seven days or develop a need for 24-hour nursing supervision may not be retained. Residents with Stage II pressure sores may remain if the facility has a limited nursing license or the resident contracts with a home health agency or registered nurse.
In ECC facilities, residents may not be retained if they are bedridden for more than 14 days. Terminally ill residents may continue to reside in any assisted living facility if a licensed hospice agency coordinates services, an interdisciplinary care plan is developed, all parties agree to the continued residency, and all documentation requirements are maintained in the resident’s file.
To receive services under the Assisted Living for the Elderly (ALE) Medicaid waiver, which covers assisted living services, case management services, and incontinence supplies, tenants must be 60 years of age or older and meet the following requirements:
-
Medicaid eligible;
-
Determined disabled according to Social Security standards if under 65 years of age;
-
Deemed appropriate for ALF placement by the facility administrator;
-
Moving out of a nursing facility or other institutional program, be an ALF resident needing additional services in order to remain in the ALF, or be living at home and determined at risk of nursing facility placement and desiring to move into an ALF;
-
Have a case manager employed by a waiver enrolled case management agency; and
-
Meet one or more functional criteria listed below:
- Require assistance with four or more ADLs or three ADLs plus supervision or administration of medications;
- Require total help with one or more ADLs;
- Have a diagnosis of Alzheimer’s disease or another type of dementia and require assistance with two or more ADLs;
- Have a diagnosed degenerative or chronic medical condition requiring nursing services that cannot be provided in a standard ALF but are available in an ALF licensed for LNS or ECC;
- Be a Medicaid-eligible recipient who meets ALF criteria, awaiting discharge from a nursing home but cannot return to a private residence because of a need for supervision, personal care, periodic nursing services, or a combination of the three.
Only facilities with an ECC or LNS and semi-private rooms and bathrooms are allowed to participate in the ALE waiver program.
Nursing Home Admission Policy
Eligibility for the waiver is higher than the nursing home criteria. Waiver eligibility is limited to the following conditions as determined by using the Comprehensive Client Assessment:
- Requires assistance with four or more activities of daily living (ADLs) or three ADLs plus assistance with administration of medication; or
- Requires total help with one or more ADLs; or
- Has a diagnosis of Alzheimer’s disease or another type of dementia and requires assistance with two or more ADLs; or
- Has a diagnosed degenerative or chronic medical condition requiring nursing services that cannot be provided in a standard licensed ALF but are available for an ALF that is licensed to provide Limited Nursing Services (LNS) or Extended Congregate Care Services (ECC); or
- Is a Medicaid-eligible resident awaiting discharge from a nursing home who cannot return to a private residence because of the need for supervision, personal care services, periodic nursing services, or a combination of the three; and
- Is receiving case management and is in need of assisted living services as determined by the community case manager and meets eligibility criteria as determined by the State’s Comprehensive Assessment and Review for Long-Term Care Services (CARES) program.
Services
Four licensure types are available: standard, limited nursing service, limited mental health, and extended congregate care. Standard facilities provide personal care services, and may provide administration of medications if offered by the facility. Facilities with an ECC license may provide a higher level of service and must make available the following additional services if required by the resident’s service plan: total help with bathing, dressing, grooming and toileting; nursing assessments conducted more frequently than monthly; measurement and recording of basic vital functions and weight; dietary management including provision of special diets, monitoring nutrition, and observing the resident’s food and fluid intake and output; assistance with self-administered medications; or the administration of medications and treatments pursuant to a health care provider’s order. If the individual needs assistance with self-administration the facility must inform the resident of the qualifications of staff who will be providing this assistance, and if unlicensed staff will be providing such assistance, obtain the resident’s or the resident’s surrogate, guardian, or attorney-in-fact’s informed consent to provide such assistance; supervision of residents with dementia and cognitive impairments; health education and counseling and the implementation of health-promoting programs and preventive regimes; provision or arrangement for rehabilitation services; and provision of escort services to health-related appointments.
Other supportive services that may be provided include social service needs, counseling, emotional support, networking, assistance securing social and leisure services, shopping, escort, companionship, family support, information and referral, transportation, and assistance developing and implementing self-directed activities. In addition, facilities provide ongoing medical and social evaluation, dietary management, and medication administration.
ECC facilities may not provide oral or nasopharyngeal suctioning, assistance with nasogastric tube feeding, monitoring of blood gasses, intermittent positive pressure breathing therapy, skilled rehabilitative services; or treatment of surgical incisions, unless the surgical incision and the condition which caused it have been stabilized and a plan of care developed.
ECC facilities are allowed to use managed risk agreements which is defined as “the process by which the facility staff discuss the service plan and the needs of the resident with the resident and, if applicable, the resident’s representative or designee or the resident’s surrogate, guardian, or attorney in fact, in such a way that the consequences of a decision, including any inherent risk, are explained to all parties and reviewed periodically in conjunction with the service plan, taking into account changes in the resident’s status and the ability of the facility to respond accordingly.
“Shared responsibility” means exploring the options available to a resident within a facility and the risks involved with each option when making decisions pertaining to the resident’s abilities, preferences, and service needs, thereby enabling the resident and, if applicable, the resident’s representative or designee, or the resident’s surrogate, guardian, or attorney in fact, and the facility to develop a service plan which best meets the resident’s needs and seeks to improve the resident’s quality of life.
The Medicaid waiver includes the following services for recipients in ECC settings: personal care, homemaker, attendant and companion, medication administration and oversight, therapeutic social and recreational programming, physical, occupational and speech therapy, intermittent nursing services, specialized medical supplies, specialized approaches for behavior management for people with dementia, emergency call systems, and case management.
Dietary
The State’s tenth edition of the recommended dietary allowances is the standard used to evaluate meals. The rules specify the servings of protein, vegetables, fruits, bread and starches, milk, fats, and water that must be served. All special diets must be reviewed annually by a registered dietician, licensed dietician/nutritionist, or a dietetic technician supervised by a register dietician or nutritionist. Therapeutic diets must be prepared as ordered by a health professional. The person responsible for food service must obtain 2 hours of continuing education in nutrition and food service. Staff who prepare or serve food must receive a minimum of 1 hour in-service training in safe food handling practices within 30 days of employment.
Agreements
Information made available to potential residents through promotional brochures or resident contracts must contain residency criteria; daily, weekly, or monthly charges and the services, supplies, and accommodations included; personal care services provided and additional costs, if any; nursing services available and additional costs, if any; food service and the ability to accommodate special diets; availability of transportation and additional costs, if any; social and leisure activities; and any service that the facility does not provide but will arrange.
Facilities with an ECC license must describe the additional personal, supportive, and nursing services provided; the costs; and any limitations on where residents must reside.
Resident contracts must include a list of specific services, supplies and accommodations provided, including limited nursing services and extended congregate care services; the basic daily, weekly, or monthly rate; a list of any additional services available and their charges; a provision giving at least a 30-day notice of rate changes; rights, duties, and obligations of residents; purpose of advance payments or deposits and refund policy; bed hold policy; a statement of any religious affiliation; and a notice of transfer if the facility is not able to serve the resident.
Provisions for Serving People with Dementia
Facilities may admit and retain residents with dementia. Training requirements have been increased for facilities advertising themselves as providing special care for persons with Alzheimer’s disease or related dementia. Facilities must provide supervision for all residents.
In addition to assisted living core training, staff must receive 4 hours of initial training covering understanding Alzheimer’s disease; characteristics of the disease; communicating with resident; family issues; resident environment; and ethical issues. Direct caregivers must obtain an additional 4 hours of training within 9 months of employment covering: behavior management; assistance with ADLs; activities for residents; stress management for the caregiver; and medical information. Direct caregivers must receive annually 4 hours of training on topics specified by the Department of Elder Affairs.
State law requires that facilities that provide special care for persons who have Alzheimer’s disease or other related disorders must disclose in its advertisements or in a separate document those services that distinguish the care as being especially applicable to, or suitable for, such persons.
Medication Administration
Unlicensed staff who meet training requirements may assist with self-administration of medications. Assistance includes taking previously dispensed, properly labeled containers from where they are stored and bringing it to the resident; reading the label, opening the container, removing a prescribed amount of medication, and closing the container; placing an oral dosage in the resident’s hand or in another container and helping the resident lift the container to his or her mouth; applying topical medications; returning the medication container to proper storage; and keeping a record of when a resident receives assistance with self-administration. Licensed nursing staff may administer medications.
Public Financing
Services are reimbursed for low-income residents through SSI, SSDI, an optional state supplement to the federal SSI payment, and a Medicaid home and community-based services waiver, called Assisted Living for the Elderly (ALE), in qualified ALFs. In addition, coverage of assistive care services (ACS) under the state plan was implemented in September 2001 in all assisted living facilities. ACS include health support; assistance with activities of daily living; assistance with instrumental activities of daily living and assistance with self-administration of medication.
Beneficiaries of ACS must be ambulatory with or without assistance, may not exhibit chronic inappropriate behavior, are capable of taking their own medication, do not have Stage III or IV pressure sores, and do not require 24-hour supervision. Residents receive $642.40, retain $54 for personal needs, and pay the remaining $588.40 to the facility for room and board. Facilities can bill Medicaid at the rate of $9.28 per day for ACS services for eligible residents, for a total reimbursement of $866.80 for a 30-day month. To be eligible for the ACS services under the Medicaid state plan, ACS recipients must receive SSI or have income under 88 percent of the federal poverty level.
ALE waiver services are available in assisted living facilities licensed for extended congregate care and/or limited nursing services. The waiver reimburses providers up to $28 a day ($840 per 30-day month) for services. SSI beneficiaries in ALE facilities receive $642.40, retain $54 for personal needs and pay the remaining $588.40 to the facility for room and board. Recipients with incomes above this standard pay a share of cost. Payments are calculated to maintain a total provider reimbursement rate of $1,576 per month.
To be eligible for the waiver program, ALE recipients must be 60 years of age or older, require a nursing home level of care, receive SSI or have income under 300 percent of the federal SSI benefit, or have income under 88 percent of the federal poverty level.
Only facilities with an ECC or limited nursing services license may participate in the waiver program. The State allows and caps the amount of supplemental income that may be received. ALE waiver beneficiaries must be offered a private room or apartment or a unit that is shared with the approval of the beneficiary. Additionally, to be eligible for participation, a facility may not have had a Class I or Class II violation during the past 5 years, nor have had uncorrected Class III violations during the past 2 years.
Services reimbursed include: attendant call system; attendant care; behavior management; personal care services; chore and homemaker services; medication administration; intermittent nursing care services; occupational therapy; physical therapy; speech therapy; therapeutic social and recreational services; specialized medical equipment; and incontinence supplies.
Facilities may receive payment for both waiver services and assistive care services. Recipients eligible for both ACS and ALE waiver assistance must have a service plan in which services that are considered ACS are shown and identified separately from those provided under the waiver.
| 2004 | 2002 | 2000 | ||||
|---|---|---|---|---|---|---|
| Facilities | Participation | Facilities | Participation | Facilities | Participation | |
| ALE | 581 | 4,167 | 299 | 2,681 | 210 | 1,410 |
| ACS | 1,527 | 14,188 | 1,565 | 9,990 | NA | NA |
Florida’s Coming Home Program
In 2001, NCB Development Corporation awarded the Florida Department of Elder Affairs a Robert Wood Johnson Foundation Coming Home Program Grant designed to help bring affordability and accessibility to assisted living statewide. Through assisted living research, policy analysis, technical assistance, information dissemination, and the development of affordable assisted living models, Florida’s Coming Home Program has focused on the promotion of assisted living facilities and services for low-income, frail elders residing in rural and small towns, as well as in public housing. The Program and its partners have also worked diligently to develop effective collaborative relationships with vital long-term care and housing developers, providers, regulators, funding sources, and consumer service agencies with the goal of facilitating affordable assisted living through integrating and maximizing existing resources. Three affordable facilities are operating as a result of the Coming Home program and eight additional facilities are in the process of obtaining financing. The program created a searchable database that allows consumers to easily locate facilities based on cost, participation in Medicaid, services, and unit characteristics. The site may be found at <http://www.floridaaffordableassistedliving.org>.
Staffing
Every ALF must be under the supervision of an administrator who is responsible for the operation and maintenance of the facility including the management of all staff and the provision of adequate care to all residents.
LNS facilities must employ or contract with a nurse(s) who must be available to provide nursing services as needed by residents. The LNS facility shall maintain documentation of the qualifications of nurses providing limited nursing services in the facility’s personnel files.
ECC facilities must provide, as staff or by contract, the services of a nurse who must be available to provide nursing services as needed by ECC residents, participate in the development of resident service plans, and perform monthly nursing assessments. An ECC staff member must serve as the ECC supervisor if the administrator does not perform this function. The ECC supervisor is responsible for the general supervision of the day-to-day management of an ECC program and ECC resident service planning.
Rules require that facilities must employ sufficient staff in accordance with required ratios (staff hours/week) and based on the physical and mental condition of residents, size and layout of the facility, capabilities of trained staff, and compliance with all minimum standards (up to five residents, 168 staff hours per week; six to 15 residents, 212 hours; 16 to 25 residents, 253 hours). Staff must be employed that are able to assure the safety and proper care of individual residents and implement the evacuation and emergency management plan. At least one staff must be awake in facilities with 17 or more residents.
Training
Administrators must be at least 21 years old, have received a high school diploma or GED, or have been an administrator for one of the last 3 years of a licensed Florida ALF that met minimum standards. Effective July 1997, administrators must complete a competency exam following completion of ALF core training. Administrators must undergo Federal Bureau of Investigation (FBI) and Florida Department of Law Enforcement (FDLE) background screening.
Administrators and direct care staff must successfully complete a 26-hour ALF core training program and a competency test. The 26-hour core educational requirement must cover at least the following topics:
- State law and rules on assisted living facilities;
- Resident rights and identifying and reporting abuse, neglect, and exploitation;
- Special needs of elderly persons, persons with mental illness, and persons with developmental disabilities and how to meet those needs;
- Nutrition and food service, including acceptable sanitation practices for preparing, storing, and serving food;
- Medication management, recordkeeping, and proper techniques for assisting residents with self-administered medication;
- Fire safety requirements, including fire evacuation; and other emergency procedures; and
- Care for persons with Alzheimer’s disease and related disorders.
Nutrition and food service. The administrator or person responsible for the facility’s food service and day-to-day supervision of food services staff shall participate in continuing education a minimum of two hours annually.
Administrators must also receive 12 hours of continuing education every 2 years. The administrator of an ECC facility and the ECC supervisor must complete 6 hours of initial training on the physical, psychological, or social needs of frail elders or persons with Alzheimer’s disease and adults with disabilities, and 6 hours of continuing training every 2 years.
Staff. In addition to the core training, new staff must complete 1 hour of training in each of the following areas: infection control, including universal precautions and sanitation procedures. A minimum of 1 hour must cover reporting major incidents and emergency procedures. A minimum of 1 hour must also cover resident rights and recognizing/reporting abuse, neglect, or exploitation. Three hours is required on resident behavior and needs and providing assistance with ADLs. Staff who prepare or serve food must receive a minimum of 1 hour in-service training in safe food handling practices. HIV/AIDS training is required biennially. Staff that assist with self-administration of medications must receive 4 hours of training prior to assuming these responsibilities.
Two hours of in-service training that addresses ECC care, concepts, statutory and rule requirements and delivery of personal care and supportive services is required for ECC direct care staff.
Facilities which advertise that it provides special care for persons with Alzheimer’s disease or other related disorders or who maintain secured areas are required to ensure that staff who have regular contact with or provide direct care to residents with Alzheimer’s disease and related disorders receive 4 hours of initial training within 3 months of employment in understanding the disease, characteristics of Alzheimer’s disease, communication with residents with Alzheimer’s disease, family issues, resident environment, and ethical issues. An additional 4 hours is required for direct care staff within 9 months covering behavior management, assistance with ADLs, activities, stress management for caregivers, and medical information. Direct care staff must participate in 4 hours of continuing education each year.
Core training and Alzheimer’s disease training may be obtained from persons approved by the Department of Elder Affairs, or designee. The Department maintains a Web site listing approved trainers. Competency evaluations are conducted by the University of South Florida.
Background Check
Florida law requires assisted living facility (ALF) owners (if individuals), administrators, and financial officers to be screened by the FBI and FDLE. ALF owners or administrators must screen all employees who provide personal services to residents through FDLE. An FBI and FDLE screening must also be conducted on an officer or board member of a firm, corporation, partnership, or association, or any person owning 5 percent or more of the facility if the agency has probable cause to believe that such person has been convicted of any offense in Section 435.04, F.S., Employment Screening.
Monitoring
A registered nurse or appropriate designee representing the licensing agency must visit ECC facilities quarterly to monitor residents and to determine facility compliance. An RN representing the agency must also visit LNS facilities twice a year to monitor residents who are receiving limited nursing services and to determine facility compliance.
Rules adopted in 2001 allow facilities to voluntarily adopt an internal risk management and quality assurance program. Facilities are required to file preliminary and full adverse incident reports within 1 and 15 days respectively. The reports are confidential as provided by law and cannot be used in civil or administrative actions, except in disciplinary proceedings by the Florida Agency for Health Care Administration or appropriate regulatory board. Facilities must also report monthly liability claims filed. The quality assurance program is intended to assess care practices, incident reports, deficiencies, and resident grievances and develop plans of action in response to findings.
Fees
The base biennial fee for a standard ALF license is $308 per license plus $51 per bed. Facilities providing ECC services pay an additional fee of $430, plus $10 per bed. Facilities with a limited nursing license pay $254, plus $10 per bed. Facilities do not pay a per-bed fee for any resident that is receiving Optional State Supplementation benefits (a monthly state supplement to a qualifying resident’s monthly income).
| Basic Assisted Living, Limited Nursing Service, Limited Mental Health |
Extended Congregate Care |
|---|---|
|
|
Georgia
Citation
Personal Care Homes; Georgia Code Annotated §31-2-4 et seq.; §31-7-2.1 et seq.; Georgia Regulations §290-5-35.01 et seq.
Community Living Arrangements; Georgia Code Annotated §31-7-1 et seq.; §37-1-22, et seq., Chapter 290-9-37
General Approach and Recent Developments
Rules for a new category, community living arrangements, were issued in 2002. The new category serves people with mental health, developmental disabilities and addictive diseases. The supply of personal care homes has been stable over the past 2 years although smaller homes comprise about 62 percent of the total supply compared to 80 percent a few years ago. The Department of Community Health administers a certificate of need requirement for facilities with 25 or more residents. The Office of Regulatory Services is planning to expand their Web site to include a frequently asked questions (FAQ) section to provide information about the regulations. The current FAQ section addresses requirements for criminal background checks that were implemented in 2002.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Personal care homes | 1,687 | 25,434 | 1,648 | 25,563 | 1,606 | 24,407 |
| Community living arrangements | 163 | 543 | NA | NA | NA | NA |
Definition
Personal care home means any dwelling, whether operated for profit or not, which undertakes through its ownership or management to provide or arrange for the provision of housing, food services, and one or more personal services for two or more adults who are not related to the owner or administrator by blood or marriage.
Community living arrangement means any residence, whether operated for profit or not, that undertakes through its ownership or management to provide or arrange for the provision of daily personal services, supports, care, or treatment exclusively for two or more adults who are not related to the owner or administrator by blood or marriage and whose residential services are financially supported, in whole or in part, by funds designated through the Department of Human Resources, Division of Mental Health, Developmental Disabilities, and Addictive Diseases.
Unit Requirements
Personal care homes. Bedrooms must have at least 80 square feet of usable floor space per resident. There may be no more than four residents per bedroom. Spouses may be permitted, but not required to share a bedroom. Both the occupant and the administrator or on-site manager must be provided with keys for rooms with lockable doors.
Community living arrangement. Two people may share a room if there is sufficient space. One bathroom must be available for every four residents.
Admission/Retention Policy
Personal care homes serve people 18 and older who meet the personal care definition of ambulatory, “a resident who has the ability to move from place to place by walking, either unaided or aided by prosthesis, brace, cane, crutches, walker or hand rails, or by propelling a wheelchair; who can respond to an emergency condition...and escape with minimal human assistance....” Personal Care Homes cannot admit or retain persons who need physical or chemical restraints, isolation, or confinement for behavioral control. Residents may not be bed-bound or require continuous medical or nursing care and treatment.
If short-term medical, nursing, health or supportive services are necessary, the resident (or representative) is responsible for purchasing them from licensed providers that are managed independently of the home. The home may assist in the arrangement for such services, but not the provision of those services. Applicants requiring continuous medical or nursing services shall not be admitted or retained. Facilities may receive waivers of the admission/retention requirements.
Community living arrangement. Facilities may not admit or retain anyone they are not equipped to serve.
Nursing Home Admission Policy
Revisions to the criteria are being considered. Currently, to qualify for an intermediate level of care, the individual has a stable medical condition requiring intermittent skilled nursing services under the direction of a physician and a mental or functional impairment that would prevent self-executing of the required nursing care (see table).
| Medical Condition | Mental Status | Functional Status |
|---|---|---|
One of the following:
|
One of the following:
|
One of the following:
|
Services
Personal care homes. Room, meals, and personal services which include, but are not limited to, individual assistance with, or supervision of, self-administered medication, assistance with ambulation and transfer, and essential activities of daily living. Homes are responsible 24 hours a day for the well-being of residents.
Community living arrangement. Services include meals, and services that are commensurate with the needs of residents, and social, recreational and educational activities. Each resident must have a service plan or a course of action written by an appropriate health professional that includes areas of the resident’s life that require services, supports, or care; goals, outcomes, and expectations; objectives; and interventions to be carried out.
Dietary
At least three meals a day shall be provided that meet the general requirements for nutrition published by the department as found in the recommended daily diet allowances of the Food and Nutrition Board. One nutritious snack must be offered mid-afternoon and evening. At least one person qualified by training or experience shall be responsible for food preparation. Homes shall arrange for special diets as prescribed.
Agreements
Personal care homes. Resident agreements must be made available prior to and upon move-in that cover all fees and daily, weekly, or monthly charges; services available for an additional fee; 60-day notice of changes; authorization to release medical records; provisions for ongoing assessment of resident needs; provisions for transportation services; refund policy; and a copy of house rules.
Community living arrangement. The agreement includes all services to be delivered; fees and charges and a description of how they are assessed; refund policy; a statement of the facility’s responsibility for personal belongings; a copy of the expectations of the resident; and the procedures for handling discharges and transfers.
Provisions for Serving People with Dementia
Any program advertised as serving residents with Alzheimer’s disease must complete a disclosure form that describes the philosophy, services, the cost of services, admission and discharge criteria, staff ratios, training, the physical environment, frequency and type of activities, and family support programs.
Medication Administration
Personal care homes. Staff may assist with self-administration by reminding, reading labels, checking dosage, and pouring medications. Generally, medications may only be administered by a licensed registered nurse from an outside agency. Injectable medications may be administered by an appropriately licensed person. Physicians may designate a staff person to inject insulin under an established medical protocol.
Community living arrangement. A licensed nurse, physician assistant or other certified staff may administer medications. Other staff may administer certain medications if they have been trained by a licensed nurse or physician assistant, and the person’s training and ability are verified.
Public Financing
A Medicaid HCBS waiver reimburses two models of personal care homes--group homes serving seven to 24 people and the family model agencies serving two to six people in the Community Care Services program. Group homes are reimbursed at $31.04 per day for Medicaid services. SSI beneficiaries receive $564 a month, from which $475 is paid for room and board and the beneficiary retains a personal needs allowance of $89 a month. Room-and-board payments may be supplemented by family members or other parties. Residents who do not receive SSI may be charged a higher amount for room and board.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participation | Facilities | Participation | Facilities | Participation |
| 465 | 2,851 | 444 | 2,759 | 442 | 2,261 |
Staffing
Personal care homes. At least one administrator, on-site manager, or responsible staff person must be on the premises 24 hours a day. The minimum on-site, staff-to-resident ratio is one staff person per 15 residents during waking hours and one staff person per 25 residents during non-waking hours.
Community living arrangement. Facilities provide qualified and trained staff that is sufficient to meet the needs of residents.
Training
Personal care homes. All employees must receive work-related training acceptable to the Department within the first 60 days of employment. This training must include: current certification in emergency first aid, except where the staff person is a currently licensed health care professional; current certification in CPR; emergency evacuation procedures; medical and social needs and characteristics of the resident population; residents’ rights; and a copy of the Long Term Care Resident Abuse Reporting Act.
Direct care staff are required to complete 16 hours of continuing education a year in courses approved by the Department covering but not limited to: working with the elderly; working with residents with Alzheimer’s disease; working with the mentally retarded, mentally ill, and developmentally disabled; social and recreational activities; legal issues; physical maintenance and fire safety; housekeeping; or topics as needed or determined by the Department.
Community living arrangement. Staff must be trained in medical, physical, behavioral and social needs; ethics and cultural competence; techniques of de-escalation and to prevent behavioral crises; fire safety and emergency evacuation techniques; policies and procedures for use of restraints, quiet time and other protection devices; and medications of residents.
Background Check
Personal care homes. The Administrator and on-site manager must obtain a satisfactory fingerprint records check determination obtained from the local law enforcement agency.
The director or onsite manager and staff who provide personal services to a resident on behalf of the personal care home or to perform any duties at the personal care home which involve personal contact with any paying resident are required to have a criminal background check. The fee for a finger print check is $3 and $24 for a criminal records check.
Community living arrangement. Fingerprint and criminal background checks are required.
Monitoring
The Office of Regulatory Services (ORS) conducts initial, annual, and follow-up inspections and complaint investigations. Inspections are generally conducted on an unannounced basis. ORS has the authority to take the following actions against a licensee: impose fines, revoke a license, limit or restrict a license, prohibit persons in management or control, suspend any license for a definite period or for an indefinite period, or administer a public reprimand. ORS has the authority to take the following actions against applicants for a permit: refuse to grant a license, prohibit persons in management or control, or limit or restrict a license.
Fees
None.
Hawaii
Citation
Assisted living facilities; Hawaii Administrative Rules §11-90-1 et seq.
Adult residential care homes; Hawaii Administrative Rules §11-100-1 et seq.
Extended care adult residential care homes; Hawaii Administrative Rules §11-101-1 et seq.
General Approach and Recent Developments
The licensing agency is planning to develop changes to structural requirements for assisted living facilities. The agency responsible for enforcing building codes has intervened with facilities that meet the R-1 (residential apartment) code. As a result, these facilities must only serve residents who are ambulatory and can evacuate in an emergency. Providers contend enforcement limits their ability to implement other aspects of the regulations supporting aging in place. The agency also worked with providers to develop guidelines for implementing managed risk agreements, disclosure, resident agreements, and transfer/discharge procedures.
One condominium association developed a service plan for owners. Because all the residents participate, it meets the requirements for licensing. A court decision upheld the agency’s position requiring a license. A new state law allows individuals who own a condominium unit to receive an assessment and to develop a service plan using outside providers without requiring that the entire project be licensed.
The licensing agency expects to receive approval to establish fees for licensing facilities that would be deposited into a special fund that could be used for training and other activities related to licensing.
Revised rules for adult residential care home and extended care adult residential care homes are pending.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Adult residential care homes | 542 | 2,882 | 545 | 2,882 | 552 | 2,866 |
| Assisted living | 7 | 1,008 | 3 | 354 | 0 | 0 |
Definition
Assisted living facility means a facility as defined in §321-15.1, HRS. This facility shall consist of a building complex offering dwelling units to individuals and services to allow residents to maintain an independent assisted living lifestyle. The environment of assisted living shall include one in which meals are provided, staff are available on a 24-hour basis, and services are based on the individual needs of each resident. Each resident, family member, and significant other shall work together with the facility staff to assess what is needed to support the resident in his or her greatest capacity for living independently. The facility shall be designed to maximize the independence and self-esteem of limited-mobility persons who feel that they are no longer able to live on their own.
Assisted living means encouraging and supporting individuals to live independently and receive services and assistance to maintain independence. All individuals have a right to live independently with respect for their privacy and dignity and to live in a setting free from restraints.
Adult residential care home means any facility providing 24-hour living accommodations, for a fee, to adults unrelated to the family, who require at least minimal assistance in ADLs, but who do not need the services of an intermediate care facility. There are two types of homes--Type I homes serve five or fewer residents and Type II serve six or more residents. Adult residential care homes may obtain an extended care license to serve a limited number of residents who meet the nursing home level of care.
Unit Requirements
Assisted living. The rules require apartment units with a bathroom, refrigerator, and cooking capacity, including a sink and a minimum of 220 square feet, not including the bathroom (sink, shower, and toilet). The cooking capacity may be removed or disconnected depending on the needs of the resident. Other requirements include wiring for phone and television, a private accessible mail box, and a call system monitored 24 hours a day by staff.
Adult residential care homes. The current rules for Type II facilities allow four residents to share a room. Single rooms must have 90 square feet and multiple-occupancy rooms 70 square feet per occupant. One toilet is required for every eight residents, one shower for every 14 residents, and one lavatory for every 10 residents.
Admission/Retention Policy
Assisted living facility. Each facility must develop admission policies and procedures that support the principles of dignity and choice. Facilities must also develop discharge policies and procedures that allow a 14-day notice for behavior or needs that exceed the facility’s ability to meet, or based on the resident’s established pattern of non-compliance. The rules do not specify who may be admitted and retained. Rather, each facility may use its professional judgment and the capacity and expertise of the staff in determining who may be served.
Nursing Home Admission Policy
To qualify for an ICF level, beneficiaries must need intermittent skilled nursing, daily skilled nursing assessment and 24-hour supervision provided by RNs or LPNs. They may also require non-skilled nursing services such as administration of medications, eye drops and ointments, general maintenance care of colostomies or ileostomies, and other services and significant assistance with ADLs.
Services
Assisted living facilities shall provide awake, 24-hour, on-site staff; three dietician approved meals a day; laundry services; opportunities for individual and group socialization; services to assist with ADLs; nursing assessment, health monitoring and routine nursing tasks; housekeeping; medication administration; services for residents with behavior problems (staff support, intervention, and supervision); and recreational and social activities. Facilities must also arrange or provide transportation, ancillary services for medically related care (physician, pharmacist, therapy, podiatry), barber/beauty care, hospice, home health, and other services.
Managed risk agreements may be used by facilities. A separate form is used for the agreement and the provisions are included in the service plan.
Dietary
Facilities provide three meals a day, snacks, and modified diets that have been evaluated and approved by a dietitian on a semiannual basis and are appropriate to the residents’ needs and choices.
Agreements
Assisted living facilities. Residents’ agreements are required to be available prior to and upon move-in and describe the services provided, rates charged, and the conditions under which additional services or fees may be charged.
Adult residential care homes. Homes without an extended care license may not serve residents needing nursing home care. Type I extended care homes may serve no more than two residents qualifying for nursing home care and Type II homes may serve no more than 10 percent of its residents needing this level of care.
Provisions for Serving People with Dementia
Not specified.
Medication Administration
Assisted living facilities. The rules allow assistance with self-administration and administration of medication as allowed under the Nurse Practice Act. Residents may keep medications in their unit. Medications in units shared by two residents may be kept in a locked container in the unit. Medications administered by the facility must be reviewed at least every 90 days by a registered nurse or physician.
Public Financing
Assisted living was added as a Medicaid waiver service in 2000 for elders and people with disabilities. Assisted living facilities and extended adult residential care homes (E-ARCH) may participate; however, no assisted living facilities have contracted to participate in the program. Participation figures for E-ARCH were not available. The State offers a flat rate of $58.46 a day for services. Room-and-board charges are limited to $418 a month. The monthly SSI payment is $568.90.
Staffing
Assisted living facilities must have licensed nursing staff available 7 days a week to meet care management and monitoring needs of residents.
Adult residential care homes. Licensees must submit a plan showing how they will obtain a registered nurse and case manager. Sufficient staff must be on duty 24-hours a day to meet resident needs.
Training
Assisted living facilities. The administrator/director must have 2 years experience in the health and social services field and show evidence of having completed an assisted living facility administrator’s course acceptable to the Department.
All staff shall be trained in CPR and first aid. The facility shall have written policies and procedures that incorporate the assisted living principles of individuality, independence, dignity, privacy, choice, and home-like environment. In-service education consists of an orientation for all new employees to acquaint them with the philosophy, organization, practice and goals of assisted living; and ongoing in-service training on a regularly scheduled basis (minimum of 6 hours annually).
Adult residential care homes. A registered nurse must train and monitor primary caregivers.
Background Check
Assisted living facilities. Licensure may be denied for convictions in a court of law or substantiated findings of abuse, neglect, or misappropriation of resident funds or property.
Adult residential care homes. All staff, including the licensee, must have no history of confirmed abuse, neglect, or misappropriation of funds.
Monitoring
Assisted living facilities. Facilities are inspected biannually. The agency may suspend, revoke, or refuse to issue a license for violations of regulations. Other enforcement steps include increased monitoring frequency, restrictions, requiring additional training, and monetary fines. The licensing agency holds quarterly meetings with providers to discuss general survey findings and other regulatory issues.
Fees
None. A plan to establish fees is being developed.
Idaho
Citation
Residential or Assisted Living Facilities; Idaho Administrative Rules IDAPA 16, Title 03, Chapter 22
General Approach and Recent Developments
The title and scope of the regulations describes the philosophy that includes a humane, safe and home-like arrangement, a negotiated service agreement and the development of facilities that are tailored to meet the needs of individual populations that operate in integrated settings in communities where sufficient supportive services exist to give residents opportunities to participate in community activities and opportunities. Extensive changes made to the State’s regulations were effective in 2000. The State added coverage under the Medicaid state plan and the HCBS waiver during 2000.
Minor changes to the regulations were made in May 2003, including a changing of the name of the regulations from Residential and Assisted Living Facilities to Residential or Assisted Living Facilities, the addition of language concerning “authorized providers,” and a new definition for “substantial compliance.” The State is currently in the process of restructuring the assisted living program, reviewing the statute, rules, and the survey process. Draft rules are expected to be available in July 2004.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Residential care or assisted living | 266 | 6,193 | 253 | 5,815 | 226 | 5,185 |
Definition
Residential or assisted living facility means one or more buildings constituting a facility or residence, however named, operated on either a profit or nonprofit basis, for the purpose of providing 24-hour care for three or more adults who need personal care or assistance and supervision essential for sustaining activities of daily living or for the protection of the individual.
Specialized care units/facilities for Alzheimer’s and dementia residents “are specifically designed, dedicated, and operated to provide the elderly individual with chronic confusion, or dementing illness, or both, with the maximum potential to reside in an unrestrictive environment through the provision of a supervised life-style which is safe, secure, structured but flexible, stress-free and encourages physical activity through a well developed activity and recreational program. The program constantly strives to enable residents to maintain the highest practicable physical, mental, or psychosocial well-being.”
Unit Requirements
Facilities licensed after July 1, 1992, must not have more than two residents in each bedroom and provide 100 square feet of floor space per single-bed room and 80 square feet per resident in multi-bed rooms. There must be at least one toilet for every six persons, residents, or employees, and at least one tub or shower for every eight persons, residents, or employees. New construction must meet the requirements of the Americans with Disabilities Act Accessibility Guidelines. Existing facilities must remove as many barriers as possible without creating an undue burden on the facility.
Admission/Retention Policy
Facilities are licensed by the level of care provided: minimal assistance, moderate assistance, and maximum assistance (see table).
| Level I Minimum Assistance |
Level II Moderate Assistance |
Level III Maximum Assistance |
|---|---|---|
| Resident requires room, board, and supervision, and may require only minimal assistance with ADLs or non-medical personal assistance or minimal assistance with mobility (independently mobile), is capable of self-preservation, or does not require medication management or supervision or minimal behavior management. | Resident requires room, board, and supervision, and may require moderate assistance with ADLs or non-medical personal assistance or moderate assistance with mobility or self-preservation or medication management or behavior management. | Resident requires room, board, supervision, and 24-hour awake staff and may require extensive assistance with ADLs or personal assistance or mobility (may be non-mobile without assistance) or assistance in an emergency (may be incapable of evacuation without assistance) or medications or assistance with training or behavior management. |
Residents may not be admitted or retained if they require ongoing skilled nursing, intermediate care, or care that is not within the legally licensed authority of the facility unless there are specialized facility provisional agreements that allow for skilled nursing or intermediate care. Residents who require ongoing highly technical skilled nursing services may not be served. Residents who require 24-hour skilled nursing; have pressure ulcers or open wounds that are not healing; draining wounds; have needs beyond the fire safety rating of the facility or whose physical, emotional, or social needs are not compatible with the other residents may not be served. Residents may not be admitted without a written physician’s order, authorized provider, or Department, or if the resident places the facility over its licensed bed capacity.
Facilities may request a waiver to serve people if they show good cause for granting the waiver, describe the extenuating circumstances and any compensating factors such as additional floor space or staffing that have a bearing on the waiver.
Facilities are required to ask if the resident has an advance directive, and they may assist residents in developing advance directives.
Nursing Home Admission Policy
The assessment areas are divided into critical, high, and medium indicators. To qualify for nursing home admission, applicants must have one or more critical indicators; two or more high indicators; one high and two medium indicators; or four or more medium indicators. The indicators are presented below.
| Indicators | Level of Need |
|---|---|
| Critical (one or more) |
|
| High (two or more; or one high and two medium) |
|
| Medium (four or more) |
|
Services
Services include assistance with activities of daily living, arrangements for medical and dental services, provisions for trips to social functions, recreational activities, maintenance of self-help skills, special diets, arrangement for payments, and medication management. A licensed nurse must visit the facility at least once a month to conduct a nursing assessment of each resident’s response to medications and to assure that the medication orders are current. The nurse also assesses the health status of each resident and makes recommendations to the administrator regarding any needs.
A uniform assessment and a negotiated service agreement must be used with residents. The agreement covers the assessment, service needs, need for limited nursing, need for medication assistance, frequency of needed services, level of assistance, habilitation/training needs, behavioral management needs, physician signed and dated orders, admission records, community support systems, resident desires, transfer/discharge, and other items.
Dietary
Larger facilities (>16 beds) must have written policies covering job descriptions and personnel responsibilities. Menu must reflect current recommended dietary allowances; as well as include foods commonly served within the community; seasonal food selections and residents’ food habits, preferences, and physical abilities. Menus must be reviewed, signed, and dated by a dietician, nutritionist, or home economist to ensure that current RDAs are met. Physicians’ orders must be received for therapeutic or modified diets.
Agreements
Agreements must be signed prior to or on the date of admission. The agreements cover: services provided; whether or not the resident will be responsible for his or her own medication; whether the facility is responsible for personal funds; handling of a partial month’s refund; responsibility for valuables; 15- or 30-day written notice of transfer or discharge; conditions for emergency transfers; permission to transfer pertinent information; resident’s responsibilities; and other items. The agreement may be integrated with the negotiated service agreement provided all requirements for both are met.
An agreement may not be terminated except under the following conditions: a 15 day written notice; the resident’s physical or mental condition deteriorates to a level where the facility can no longer provide care; nonpayment; for the protection of the resident or other residents from harm; and other conditions.
Provisions for Serving People with Dementia
Services in specialized care units for Alzheimer’s disease include habilitation services, activity program, and behavior management according to the individualized negotiated service agreement. Residents of specialized care units for Alzheimer’s disease must be evaluated by their primary care physician for the appropriateness of placement in the unlocked specialized care unit/facility prior to admission. No resident shall be admitted to these units without a diagnosis of Alzheimer’s disease or related disorder. Residents must be at a stage in their disease such that only periodic professional observation and evaluation is required. Residents in these units must be re-evaluated quarterly. No resident shall be admitted who requires physical or chemical restraints. Staff must have an additional 6 hours of training in addition to orientation, and must have an additional 2 hours of continuing education annually beyond the required 8 hours dedicated to the provision of services to people with Alzheimer’s disease or other dementias.
Facilities have to describe the population served; the philosophy, objectives, and beliefs upon which decisions will be made; admission and discharge criteria; security systems; staffing pattern; plan for specialized training; and the program and social activities.
Medication Administration
Licensed nurses may fill medi-sets for residents. Aides who have passed required training may administer medications. The requirements are specified by the Board of Nursing.
Problems with medication administration occur frequently. Common problems include failure to follow doctors’ orders, failure to get medications from the pharmacy, and an unclear line between medication assistance and medication administration.
Public Financing
Personal care in assisted living was added as a state plan service in 2000. Services under a Medicaid HCBS waiver using the waiver application definition and including medication administration and assistance with personal finances was implemented in 1999. Elders, people with disabilities, and people with mental retardation, traumatic brain injuries, or developmental disabilities are eligible. Coverage was phased in across the State. The HCBS aged and disabled waiver program now serves 1,714 residents living in residential or assisted living facilities. Individuals are eligible for the waiver using the 300 percent SSI eligibility criteria. There are two programs covering services for individuals living in residential or assisting living facilities:
-
State plan services are available to individuals who require no more than 16 hours of personal care services per week. Individuals must meet state income limits for financial eligibility. The service payment is currently $13.40/hour. The amount of payment a facility receives is based upon the number of hours a resident’s plan of care requires. The resident is responsible for paying for room and board. The State’s suggested limit is $497 per month; however the facility may charge the resident more. Family supplementation is allowed. Any money remaining after paying for room and board is retained as a personal needs allowance.
-
HCBS waiver payments are capped at the average per capita nursing home cost and individual payments are based on a care plan. The facility can charge whatever it wants for room and board however the State’s suggested rate is $497 per month for rent, utilities, and food. The individual SSI payment rate for individuals residing in residential facilities is currently $564. Any monies remaining after payment of room is board is retained as the personal needs allowance.
State supplementation to the SSI program has been phased out. In 2002, the Legislature directed the transition of individuals who were receiving the supplemental grant to the Medicaid state plan. Supplementation for the room-and-board payment is allowed in all categories. A uniform assessment instrument is used to determine the unmet ADL needs for all applicants. The unmet needs are converted to a payment that is available to the beneficiary regardless of where he or she lives: in assisted living or their own home or apartment. The process was developed to eliminate differences in payment and service delivery depending on where a person lived.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participation | Facilities | Participation | Facilities | Participation |
| 265 | 1,870 | 35 | 720 | NR | NR |
Staffing
Facilities must have sufficient staff to serve residents in keeping with negotiated service plans. At least one staff member must be immediately available to residents at all times. Facilities admitting Level III residents or a combination of Level I, II, or III residents must have a minimum of one awake staff during sleeping hours. Waivers may be sought by small facilities. A full-time administrator must devote no less than 20 hours per week to the day-to-day administrative duties.
Training
Administrators must have a valid residential care administrator’s license. Personnel must be given an orientation to the facility and participate in a continuing training program developed by the facility.
Staff. Each facility shall develop and follow a structured written orientation program for a minimum of 8 hours. Continuing training: staff providing personal assistance must receive a minimum of 8 hours of training a year. Evidence of the completed training and topics are kept on file. Staff, including housekeeping personnel and contract personnel must be trained in Universal Precautions.
Staff in specialized care units for Alzheimer’s/dementia residents must have an additional 6 hours of orientation covering information on Alzheimer’s and dementia, symptoms and behaviors of memory impaired people, communication with memory impaired people, resident’s adjustment, inappropriate and problem behavior of residents and appropriate staff response, activities of daily living for special care unit residents, and stress reduction for special care unit staff and residents. Staff must have an additional 2 hours of continuing education, beyond the required 8 hours of continuing training, on the provision of services to persons with Alzheimer’s disease.
Background Check
Applicants for licensure must submit a criminal history clearance as described in IDHW rules Title 05, Chapter 06 which is repeated every 3 years. The rules include finger printing, FBI, National Criminal History Background Check System, state registries and Medicaid sanctions lists. Individuals pay $34 for the cost of the check which must be updated every 5 years.
Monitoring
With the exception of the initial surveys for licensure, all inspections and investigations shall be made unannounced and without prior notice. Inspections are conducted at least annually. Inspections entail reviews of the quality of care and service delivery, resident records, and other items relating to the running of the facility. If deficiencies are found, then plans of correction are made and follow-up surveys are conducted to determine if corrections have been made. Complaints against the facility are investigated by the licensing agency. A complainant’s name or identifying characteristics may not be made public unless “the complainant consents in writing to the disclosure; the investigation results in a judicial proceeding and disclosure is ordered by the court; or the disclosure is essential to the investigation. The complainant shall be given the opportunity to withdraw the complaint before disclosure.”
Inspections of specialized care units for Alzheimer’s disease are conducted by the licensing agency with participation from the Regional Department staff who have program knowledge of and experience with the type of residents to be served and the proposed program offered by the facility. Facilities that are specialized or have specialized care units must submit a synopsis of the program of care to be offered by the unit/facility.
Enforcement options include ban on admissions, ban on residents with certain diagnosis, civil monetary penalties, appointment of temporary management, suspension or revocation of the license, transfer of residents, issuing a provisional license and other remedies. Facilities operating without a license may be subject to six months in jail and fines up to $5,000.
Historically, the State has reported that the consultative process used during the monitoring process has positively impacted overall quality of care and compliance. Typically, surveyors would be able to provide input and suggestions to problems that were identified, and providers welcomed this feedback. In recent years, due to a shortage of staff, the State is working hard just to keep up with the surveys they are required to do. As a result, they do not have the time to provide feedback and suggestions to providers during the survey process. They also do not have the staff to go back and determine whether corrections have been made.
Fees
$500 for a building evaluation.
Illinois
Citation
Assisted Living and Shared Housing Act Title 210 ILCS 9
Assisted living and shared housing establishments; 77 ILL Admin. Code Part 295
Sheltered care facility; 77 ILL Admin. Code Part 330 et seq.
Supportive living facilities; Title 89, Chapter I, Subchapter d, Part 146
General Approach and Recent Developments
Rules governing assisted living establishments and shared housing establishments were effective January 2002. These establishments are exempt from the certificate of need law. The law does not allow Medicaid to cover services in assisted living establishments; however, a “supportive living facility” (SLF) program has been implemented in “certified” locations that offers similar services. Because of budget deficits, a moratorium has been placed on the number of SLFs that may be approved. The State is considering lifting the moratorium. The program serves elderly and disabled Medicaid beneficiaries who need assistance with activities of daily living. It targets lighter need nursing facility residents who are unable to remain in their homes. An SLF may be converted nursing home units or free standing buildings that integrate housing, health, personal care, and supportive services in home-like residential settings. A maximum of 2,750 Medicaid residents can be served under a 1915 (c) waiver that applies only to the demonstration.
The Assisted Living and Shared Housing Establishment regulations are being amended to implement P.A. 93-141 which added a provision for a floating license and clarified requirements concerning care for residents with Alzheimer’s disease and dementia, hospice care, and unlicensed establishments.
The floating license rules will allow an establishment in which 80 percent of the residents are at least 55 years of age or older, that is operated as housing for the elderly, and meets the construction and operating standards contained in Section 20 of the Act, to request a floating license for any number of individual living units within the establishment, up to, but not including, total capacity. Living units designated as licensed living units shall be referred to as such. The establishment must have adequate staff to meet the scheduled and unscheduled needs of the residents living in the licensed living units, and all staff must meet the requirements of the assisted living regulations. All mandatory and optional services must be available to residents of the licensed units. Designation as a licensed living unit may be temporary to accommodate a resident’s changing needs without requiring the resident to move.
The Sheltered Care Facility rules were updated in 2003. The revisions update the incorporation by reference of National Fire Protection Association (NFPA) standards (Life Safety Code) applicable to construction of new facilities from 1997 standards to 2000 standards.
Legislation consolidating different licensing categories was considered by the legislature in 2004. The State is currently working with its assisted living advisory committee to discuss dedicating permanent state staff to the assisted living program.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted living | 97 | 5,999 | 24 | 1,667 | NA | NA |
| Shared housing | 9 | 82 | NA | NA | NA | NA |
| Shelter care facilities | 149 | 8,484 | 156 | 8,740 | 156 | 8,302* |
| * NOTE: The number of units was revised from the 2000 report due to an error that may have reported occupied rather than licensed beds. | ||||||
Definition
Assisted living establishment means a home, building or residence, or any other place where sleeping accommodations are provided for at least three unrelated adults, at least 80 percent of whom are 55 years of age or older and where the following are provided consistent with the purpose of this act:
- Services consistent with a social model that is based on the premise that a resident’s unit in assisted living and shared housing is his or her own home;
- Community-based residential care for persons who need assistance with ADLs, including personal, supportive, and intermittent health-related services available 24 hours per day, if needed, to meet the scheduled and unscheduled needs of a resident;
- Mandatory services, whether provided directly by the establishment or by another entity arranged for by the establishment with the consent of the resident; and
- A physical environment that is a homelike setting that includes the following and such other elements as established by the Department in conjunction with the assisted living and shared housing advisory board: individual living units each of which shall accommodate small kitchen appliances and contain private bathing, washing, and toilet facilities, or private washing and toilet facilities with a common bathing room readily accessible to each resident. Units shall be maintained for single occupancy unless shared by consent.
Shared housing establishment means a publicly or privately operated free-standing residence for 12 or fewer persons, at least 80 percent of whom are 55 years of age or older and who are unrelated to the owners and one manager of the residence, where the following are provided:
- Services consistent with a social model that is based on the premise that the resident’s unit is his or her own home;
- Community-based residential care for persons who need assistance with ADLs, including housing and personal, supportive, and intermittent health-related services available 24 hours per day, if needed, to meet the scheduled and unscheduled needs of a resident, and
- Mandatory services, whether provided directly by the establishment or by another entity arranged for by the establishment with the consent of the resident.
Sheltered care facility means a facility licensed under the nursing home care act that provides maintenance and personal care but does not provide routine nursing care.
Supportive living facility (SLF) means a residential setting that provides personal care services, 24-hour supervision and assistance (scheduled and unscheduled), activities, and health related services with a service program and physical environment designed to minimize the need for residents to move within or from the setting to accommodate changing needs and preferences; has an organized mission, service programs, and a physical environment designed to maximize residents’ dignity, autonomy, privacy, and independence; and encourages family and community involvement.
Unit Requirements
Assisted living establishments require single occupancy units unless shared by choice. Units must accommodate small appliances, include a sink, toilet, and assistive devices if needed. Bathing facilities may be in the unit or in a common room.
Shared housing establishments may have shared bathrooms (1:4) and tub/shower facilities (1:6).
Sheltered care facilities allow no more than four persons to share a room. Single rooms must be 70 square feet and multiple occupancy rooms 60 square feet per person. One lavatory is required for every 10 residents and one shower/bath is required for every 15 residents. A lavatory and shower/bath is required on each floor.
Supportive living facility. To participate in the Department of Public Aid program, facilities must have not less than 10 and no more than 150 apartments. Freestanding sites must provide apartments with 300 square feet of living space, including closets and bathroom. Apartments for individuals wishing to share the unit must have 450 square feet of living space, including closets and bathroom. Units must have a full bathroom, lockable doors, emergency call system, heating and cooling controls, wiring for private telephone, access to cable television or satellite dish, a sink, microwave oven or stove, and refrigerator. Nursing homes converting a portion of a facility must offer apartments with 160 square feet for single occupancy and 320 square feet if two people want to share a unit.
Admission/Retention Policy
Assisted living establishments. Facilities may not accept residents who are a danger to themselves or others, are not able to communicate their needs and do not have a representative residing in the facility, require total assistance with two or more ADLs, require assistance of more than one paid caregiver with any ADL, require more than minimal assistance in moving to a safe area in an emergency. Persons with severe mental illness may not be admitted, which is characterized in the DSM-IV as substantially disabled for not less than one year in the areas of self-maintenance, social functioning, activities of community living and work skills. This does not include Alzheimer’s disease and other forms of dementia. They may also not accept residents who need the following health services unless self-administered or administered by a qualified, licensed health care professional who is not employed by the owner or operator of the establishment, its parent entity, or any other entity with ownership common to either the owner or operator or parent entity, including but not limited to an affiliate of the owner or operator:
- Intravenous therapy or feedings;
- Gastronomy feedings;
- Insertion, sterile irrigation, and replacement of a catheter, except for routine maintenance of urinary catheters;
- Sterile wound care;
- Sliding scale insulin;
- Routine insulin injections; and
- Stage III or IV decubitus ulcers.
In addition, residents may not be accepted who need five or more skilled nursing visits a week for 3 or more weeks unless the course of treatment is rehabilitative and the need is temporary.
If any of the above conditions are met, a resident’s occupancy agreement shall be terminated, except for individuals who are terminally ill who receive or would qualify for hospice and such care coordinated by a licensed hospice provider.
Proposed rules would require the establishment to advise the prospective resident to consult a physician to determine whether a pneumococcal pneumonia vaccine is recommended.
Sheltered care facility. No resident needing nursing care may be admitted or retained. Persons who have a communicable disease or are mentally ill, need treatment for mental illness, are likely to harm others, or are destructive of property or themselves may not be admitted or retained.
Supportive living facilities may serve elderly (age 65 or older) or disabled residents age 22 or over who have been screened and determined to meet the nursing facility level of care criteria. Residents may be discharged if they are a danger to self or others or have needs that cannot be met by the SLF. The SLF must develop a service plan and execute a written contract with each resident that includes services the resident will receive and other terms of the agreement.
Nursing Home Admission Policy
Waiver eligibility is based on a Determination of Need score. The score is derived from the Mini-Mental State Examination (MMSE), six ADLs, nine IADLs (including ability to perform routine health and special health tasks and ability to recognize and respond to danger when left alone). Each ADL, IADL and special factors are rated by level of impairment (0-3) and unmet need for care (0-3). Scores for each area are summed and applicants with a DON score of 29 or more are eligible. The MMSE component is weighted toward people with moderate or severe dementia. The process is designed to target services to people with high levels of impairment who may have informal supports and people with lower levels of impairment without informal supports.
Services
Assisted living establishments. No more than 180 days prior to admission, a comprehensive assessment that includes an evaluation of a prospective resident’s physical, cognitive, and psychosocial condition shall be completed by a physician. This assessment must be updated annually by a physician, or upon significant change in condition. Establishments may use their own evaluation/assessment tools, but this does not take the place of the physician assessment. Mandatory services include three meals a day, housekeeping, laundry, security, emergency response system, and assistance with ADLs. Optional services include medication reminders, supervision of self-administered medications and medication administration, and nonmedical services defined by rule.
Assisted living, which promotes resident choice, autonomy, and decision making, should be based on a contract model designed to result in a negotiated agreement between the resident or the resident’s representative and the provider, clearly identifying the services to be provided. This model assumes that residents are able to direct services provided for them and will designate a representative to direct these services if they themselves are unable to do so. This model supports the principle that there is an acceptable balance between consumer protection and resident willingness to accept risk and that most consumers are competent to make their own judgments about the services they are obtaining. Regulation of assisted living establishments and shared housing establishments must be sufficiently flexible to allow residents to age in place within the parameters of this Act. The administration of this Act and services provided must therefore ensure that the residents have the rights and responsibilities to direct the scope of services they receive and to make individual choices based on their needs and preferences. These establishments shall be operated in a manner that provides the least restrictive and most homelike environment and that promotes independence, autonomy, individuality, privacy, dignity, and the right to negotiated risk in residential surroundings.
“Negotiated risk” is the process by which a resident, or his or her representative, may formally negotiate with providers what risks each are willing and unwilling to assume in service provision and the resident’s living environment. The provider assures that the resident and the resident’s representative, if any, are informed of the risks of these decisions and of the potential consequences of assuming these risks. The rules allow assisted living and shared housing establishments to use a risk agreement that describes the problem, issue or service that is covered, the choices available to the resident and their risks or consequences, the resulting agreement, mutual responsibilities, and a review time frame. The agreement is limited to the individual’s care and personal environment and does not waive any requirements of the regulations.
Sheltered care facility may provide personal care, group and individual activities, assistance with self administration of medications or administration by a physician or licensed nurse.
Supportive living facilities must provide a combination of housing, personal, and health related services that promote autonomy, dignity, and quality of life and respond to the individual needs of residents. Room and board includes three meals per day. Services include nursing services, personal care, medication oversight and assistance in self-administration, housekeeping services, laundry service, social and recreational programs, 24-hour response/security staff, emergency call systems, health promotion and referral, exercise, transportation, and maintenance services. Nursing services include completion of a resident assessment and service plan, a quarterly health status evaluation, administration of medication when residents are temporarily unable to self-administer, medication set-up, health counseling, episodic and intermittent health promotion or disease prevention counseling, and teaching self-care in meeting routine and special health care needs that can be met by other staff under supervision of a registered nurse. Facilities are expected to involve family members in service planning. Residents must receive an initial assessment within 24 hours of admission and a comprehensive assessment within 14 days. Assessments are updated at least annually.
Dietary
Assisted living and shared housing facilities offering special diets must contract with or employ a dietician. Meals must be nutritionally balanced and accommodate resident preferences.
Shelter care facilities must provide three meals or two meals and a breakfast bar. Meals must meet the requirements for a general diet for an adult recommended by the Food and Nutrition Board, National Research Council. Therapeutic diets ordered by a physician must be provided.
SLFs must contract with a licensed dietitian who is on-site at least twice a quarter for at least 8 hours (cumulative) to provide consultation and training.
Agreements
Assisted living and shared housing. Contracts with residents include the duration of the contract; base rate and a description of services; additional services available and their fee; description of the process for terminating or modifying the contract; the complaint resolution process; resident obligations; billing and payment procedures; the admission, risk management, and termination procedures; resident rights; the department’s annual on-site review process; terms of occupancy; charges during absences; refund policy; notice for changes in fees; and policy concerning notification of relatives of changes in the resident’s condition. Contracts must also include statements that Medicaid is not available for payment of services and that there is a risk management procedure.
Supportive living facilities. Agreements cover services provided under Medicaid; arrangements for payment; grievance procedure; termination provisions; rules for staff, management, and resident conduct; and resident rights. The agreement includes services available for an additional fee and arrangements to share a unit.
Provisions for Serving People with Dementia
Assisted living and shared housing facilities that offer special care programs for people with dementia must file a disclosure statement if they serve people with dementia. The statement includes the form of care or treatment; philosophy; admission and retention policies; assessment care planning and implementation guidelines; staffing ratios; physical environment; activities; role of family members; and the cost of care.
Facilities are not allowed to serve people with dementia whose mental or physical condition is detrimental to the health, welfare, or safety of the resident or other residents as determined by the resident’s physician prior to admission and annually thereafter. The rules specify that residents must be assessed prior to admission with any one or a combination of assessment tools, based upon the resident’s condition and stage in the disease process. The rules list a number of tools that may be used, such as the Functional Activities Questionnaire, Clock Drawing Test, and Functional Assessment Staging, among others.
Shelter care facilities. The law does not allow facilities to serve anyone with dementia if they do not have the staff with the skills to meet the individual’s needs. The rules will provide for use of a validated dementia specific standard to assess residents. The assessment must be completed and approved by the resident’s physician prior to move-in and annually. Residents cannot be accepted if they pose a danger that cannot be eliminated through treatment. Facilities offering special care units must disclose information about their program, ensure that residents have a designated representative, and develop and implement policies and procedures for people who wander, need supervision and assistance when evacuating. In addition, they must provide cognitive stimulation, appropriate staffing patterns, and emergency procedures. Facilities must provide each resident 1.4 hours of service per day (ADLs, activities, and other services to meet unique needs).
Managers of special care facilities must have a college degree with course work in dementia and one year of experience and must complete 6 hours of training a year. Staff receive 4 hours of orientation in dementia care, 16 hours of on-the-job training, and 12 hours in-service training a year. The rules list the topics that are covered under each requirement.
Medication Administration
Assisted living and shared housing establishments may assist with self-administered medications, supervise, or administer medications. Policies related to administration must be approved by a physician, pharmacist, or registered nurse. Only a licensed health care professional employed by the establishment may administer medications including injections, oral medications, topical treatments, eye and ear drops, or nitroglycerin patches.
Sheltered care facilities. All medications taken by residents shall be self-administered, unless administered by licensed personnel. No person shall be admitted to a facility who is not capable of taking his or her own medications. Facility staff may remind residents when to take medications and watch to ensure that they follow the directions on the container. All medications must be stored in a locked area at all times. Although there is some conflict between the sections of the regulation governing medication administration, in practice, licensed staff are allowed to administer medications “to some residents for control purposes” when it is not safe for the resident to self-administer.
Public Financing
Assisted living and shared housing. The law does not permit the use of Medicaid funds in licensed facilities.
Supportive living facilities. The State has implemented a pilot program to serve elders and adults with disabilities who are Medicaid waiver beneficiaries in supportive living facilities (SLFs) (see http://www.slfillinois.com). SLFs are exempt from state licensing requirements. For Medicaid residents, participating facilities must be willing to accept the SSI rate, $564 a month in 2004 (less a $90 personal needs allowance) as payment for room and board. The service payment is based on 60 percent of the average nursing facility rate paid in the region. Because SLFs are not licensed, they may be certified as eligible food stamp vendors and receive these benefits for eligible residents. The average monthly service cost is $1,883 paid by Medicaid. Residents pay, on average, $455 for room and board and receive $96 in food stamp benefits. Income supplementation is allowed. Funding for services is included in the Medicaid nursing home budget and is not part of a separate appropriation.
A moratorium on new applications was instituted in November 2001 due to budget constraints. However, applicants that had submitted prior to the moratorium will be allowed to participate. The program has 41 operating SLFs with 2,983 units in fall 2004. Thirty more sites are approved. Eighty six percent of the SLF units are occupied and 63 percent (1,602 units) are occupied by Medicaid beneficiaries.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participation | Facilities | Participation | Facilities | Participation |
| 41 | 1,602 | 13 | 293 | NR | 35 |
The program targets “lighter” care nursing home eligible residents with a Determination of Need (DON) score (see below) between 29 and 47 on a 100-point scale. Residents with scores above 47 may be served if the facility has the capacity to do so.
| Region | Daily | R&B | Food Stamps | Medicaid | Total |
|---|---|---|---|---|---|
| Chicago | $61.94 | $474 | $97 | $1,883 | $2,454 |
| South suburb | $59.11 | $474 | $97 | $1,797 | $2,368 |
| Northwest | $53.90 | $474 | $97 | $1,639 | $2,210 |
| Central | $51.05 | $474 | $97 | $1,552 | $2,123 |
| West central | $47.54 | $474 | $97 | $1,552 | $2,016 |
| St. Louis | $50.75 | $474 | $97 | $1,445 | $2,114 |
| South | $45.54 | $474 | $97 | $1,384 | $1,955 |
Staffing
Assisted living and shared housing. Establishments must have sufficient numbers of trained staff to meet the 24 scheduled and unscheduled needs of residents. Assisted living establishments must have at least one awake staff on duty who has CPR training.
Sheltered care facility. Facilities must have staffing patterns that are sufficient to meet the needs of residents. At least one awake staff member is required.
Supportive living facilities must provide licensed and certified staff that are sufficient to meet the needs of residents in conjunction with contractual agreements. Personal care services and assistance with self-administration of medications must be provided by certified nurse assistants. SLFs must contract with a dietician.
Training
Assisted living and shared housing. Administrators must be 21 and have a high school diploma or equivalency, 1 year management experience or 2 years of experience in health care, housing, or hospitality.
Staff must complete an orientation that addresses philosophy and goals; promotion of dignity, independence, self-determination, privacy, choice, and resident rights; confidentiality; hygiene and infection control; abuse and neglect prevention and reporting; and disaster procedures. Additional orientation covers needs of residents; service plans; internal policies; job responsibilities and limitations; and ADLs. Eight hours of annual training is required for staff and managers on topics listed above.
Sheltered care facility. The administrator shall arrange for facility supervisory personnel to annually attend appropriate education programs on supervision, nutrition, and other pertinent subjects. Staff training shall include an in-service program embracing orientation to the facility and its policies, skill training, and ongoing education carried out to enable all personnel to perform their duties effectively. Written records of program content and personnel attending shall be kept.
Supportive living facilities. Administrators must have at least 5 years’ experience in providing health care services in assisted living settings, in-patient hospital, long-term care setting, adult day care, or in a related field. The manager also must have at least 2 years of progressive management experience. Staff shall receive documented training by qualified individuals in their area(s) of responsibility prior to employment and semiannual training thereafter. Nurses’ assistants must be certified or enrolled in and pursuing certification. A trained staff person must be responsible for planning and directing social and recreation activities. Nurses must be licensed. Twenty-four-hour response staff must be certified in emergency resuscitation.
Background Check
The State has introduced proposed rules titled “Health Care Worker Background Check Code” in 77 ILL Admin. Code 955. New qualifying crimes have been added, which become effective January 1, 2004. Two new provisions have been added that are not in any of the existing rules. Health care employers will be required to establish a policy concerning employment of individuals whose criminal history record checks indicate convictions for offenses that are not disqualifying. The employer will also be required to develop a policy concerning employment of individuals who have been granted waivers. Additionally, prior to hiring, proposed rules would require the establishment to check employee status with the Nurse Aide Registry.
Rules passed in November 2003 changed waivers of the health care worker criminal history background check requirements. The new rule specifies that waiver applicants must have met all court obligations (probation, adhering to a fine or restitution schedule) and satisfactorily completed a drug and/or alcohol recovery program, if applicable. Mitigating circumstances are expanded to reference drug/alcohol rehabilitation programs, anger management or domestic violence prevention programs, completion of court-ordered obligations, and nurse registry and criminal history status in other states.
Managers who provide direct care must complete a background check. The rules list specific offenses that preclude hiring of staff.
State legislation passed during the spring of 1995 prohibits sheltered care facilities from knowingly hiring, employing, or retaining any individual in a position with duties involving direct care for residents who have been convicted of committing or attempting to commit designated criminal offenses, unless a waiver has been granted by the Illinois Department of Public Health. Further, the legislation requires facilities to check the Certified Nurse Aid Registry in the State and ensure that appropriate background criminal history record checks are initiated or have been conducted. The legislation was expanded to include SLFs in 1999.
Monitoring
Assisted living and shared housing establishments are inspected annually. This is an annual unannounced visit. The annual visit focuses on compliance with rules, solving resident issues and concerns and the facility’s quality improvement (QI) process. Each facility must have a QI program that covers oversight and monitoring; resident satisfaction; and a QI process that has benchmarks, is data driven, and focuses on resident satisfaction. A system is needed to detect and resolve problems. The existence, results, and process of the QI system cannot be used as evidence in any civil or criminal proceeding.
Civil penalties may be applied up to $5,000 a day for violations and up to $3,000 a day for keeping residents who exceed the care needs in the law.
The monitoring process is collaborative in nature, with an emphasis on meeting the needs of the residents. During this process, the State provides information on best practices and shares concerns about the quality of care with suggestions for how to fix the problems or the names of individuals the facility may contact for assistance. Oversight is not enforcement-driven, but is based more on a social model promoting quality of care. The functions of surveying and providing education are the responsibility of the same staff. Currently, the surveyors are earning overtime in these positions. The surveyors are contractual employees of the State and many come from the nursing home model. The State is trying to hire its own staff to monitor assisted living. They are seeking individuals who come from a more social model background, with an understanding of the assisted living approach and philosophy.
Supportive living facilities. Participating facilities will be Medicaid certified and monitored, at least annually, by the Department of Public Aid. Monitoring includes contract requirements, resident autonomy, resident rights, adequacy of service provision, quality assurance process, safety of the environment, program policies and procedures, information provided to low-income residents, review of resident assessment and service plans, resident satisfaction surveys, check-in system, and food service.
Facilities must have a grievance process and a quality assurance process. Complaints may be heard informally. If not resolved or if the resident prefers, grievances may be submitted through the facility’s formal process. Residents may use the Medicaid appeals process for denial or delay of service.
Internal quality assurance procedures must encompass resident satisfaction, oversight and monitoring; peer review; utilization review; procedures for preventing, detecting and reporting resident neglect and abuse; and ongoing quality improvement. The committee must establish review schedules, objectives for improving service quality, including quality indicators and measures, and a mechanism for tracking improvements based on care outcomes. A system with outcome indicators must be developed that measures: quality of services; residents’ rating of services; cleanliness and furnishings in common areas; service availability and adequacy of service provision and coordination; provision of a safe environment; socialization activities; and resident autonomy.
Fees
Fees for sheltered care facilities are $200 per year. The fee for assisted living establishments is $300 per facility, plus $5 per unit. The fee for shared housing is $150.
Indiana
Citation
Assisted living: House Enrolled Act 1630 (1997)
Residential care facilities: 410 IAC 16.2-5 et seq.
General Approach and Recent Developments
Residential care facilities are licensed under the licensure category for health facilities. This licensure category also includes rules for comprehensive care facilities, commonly known as nursing homes. Disclosure documentation legislation for housing with services establishments was passed during the 1998 legislative session. This legislation is very broad, and includes many different types of licensed and unlicensed providers, including licensed residential care facilities. The purpose of the legislation was to require all licensed and unlicensed providers to complete a disclosure form on an annual basis and submit the form along with a copy of the resident contract to the Division of Disability, Aging and Rehabilitation Services. An establishment may not use the term “assisted living” if it has not filed a disclosure form. The form includes the following information: the name and address of the owner and managing agent, description of services provided and the base rate, additional services available and their fees, the resident’s designated representative, if any, referral procedures if the contract is terminated, the process for modifying and terminating the contract, description of the complaint resolution process, and criteria for determining who may continue to reside in the establishment. As of March 2004, approximately 300 housing with service establishments that may be called assisted living facilities have filed disclosure information.
Revised regulations for residential care facilities went into effect in March 2003. A separate Medicaid assisted living waiver was implemented in October 2001. The State recently received a 5-year waiver renewal. The number of slots requested was reduced from 2,250 to a maximum capacity of 400 in Year 5 due to provider capacity and budget projections.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Residential care facilities | 147 | 11,767 | 140 | 11,555 | 127 | 10,098 |
| Housing with services establishments | 300 | NR | NR | NR | NR | NR |
Definition
Residential care facilities. A health facility that provides residential nursing care and administers medications prescribed by a physician must be licensed as a residential care facility. A facility that provides services such as room, meals, laundry, activities, housekeeping, and limited assistance in activities of daily living, without providing administration of medications or residential nursing care is not required to be licensed.
A housing with service establishment is defined as an establishment providing sleeping accommodations to at least five residents and offering or providing for a fee at least one regularly scheduled health-related service or at least two regularly scheduled supportive services, whether offered or provided directly by the establishment or by another person arranged for by the establishment. Health-related services mean home health services, attendant and personal care services, professional nursing services, and central storage and distribution of medications. Supportive services mean help with personal laundry, handling or assisting with personal funds, arranging for medical services, health related services, or social services.
Unit Requirements
Residential care facilities. Rules require 100 square feet for single rooms and 80 square feet per bed for multiple occupancy rooms. For facilities licensed after 1984, no more than four people may share a room. One toilet and sink is required for every eight residents in facilities licensed after 1984.
Admission/Retention Policy
Residential care facilities may not admit or retain individuals who require 24-hour comprehensive nursing care. Facilities that retain appropriate professional staff may provide comprehensive nursing care to residents needing care for a self-limiting condition. Residents must be discharged if the resident is a danger to self or others, requires 24 hour a day comprehensive nursing care or comprehensive nursing oversight; requires less than 24 hour per day comprehensive nursing care, comprehensive nursing oversight, or rehabilitative therapies and has not entered into a contract with an appropriately licensed provider of the resident’s choice to provide those therapies, is not medically stable or meets two of the following three criteria unless the resident is medically-stable and the facility can meet the resident’s needs: (1) requires total assistance with eating; (2) requires total assistance with toileting; and (3) requires total assistance with transferring.
Housing with services establishments. The establishment must, in the disclosure form, indicate when a resident must be transferred because the establishment and the resident are unable to develop a means for assuring that the resident is able to respond to an emergency in a manner that is consistent with local fire and safety requirements and when the establishment is unable to assure that the resident’s physical, mental, and psychosocial needs can be met. Except as stated in the contract, residency in the housing with services establishment may not be terminated due to a change in a resident’s health or care needs. Except where the resident’s health or safety or the health or safety of others are endangered, an operator shall provide at least thirty (30) days notice to the resident or the resident’s designated representative before terminating the resident’s residency.
Nursing Home Admission Policy
Individuals are eligible if they have an unstable medical condition or three or more of 14 substantial medical conditions or ADL impairments. The list includes: supervision and direct assistance on a daily basis to ensure that prescribed medication is taken correctly; 24-hour supervision and/or direct assistance due to confusion; disorientation not related to a mental illness; inability to eat, transfer from bed or chair, change clothes, bathe, manage bladder and/or bowel functions or ambulate or use a wheelchair without direct assistance. The criteria allow a person with three ADLs or 2 ADLs and the need for medication assistance to receive waiver services.
Services
Residential care facilities. Services offered to a resident must be appropriate to the scope, frequency, need and preference of the resident. Services must be reviewed and revised as appropriate and discussed with the resident as his or her needs change. If administration of medications and/or the provision of residential nursing services are needed, a licensed nurse must be involved in the determination and documentation of needed services. The administration of medications and the provision of residential nursing services must be ordered by a physician and supervised by a licensed nurse on the premises or on call.
The facility must provide activities programs appropriate to the ability and interests of the residents. Scheduled transportation must be provided or coordinated to community-based activities.
Each facility must determine whether it will administer medications or provide residential nursing services. This must be clearly stated in the admission agreement.
Residential nursing care may include, but is not limited to: identifying human responses to actual or potential health conditions, deriving a nursing diagnosis, executing a minor regimen based upon a nursing diagnosis or as prescribed by a physician, physician’s assistant, chiropractor, dentist, optometrist, podiatrist, or nurse practitioner, or administering, supervising, delegating, and evaluating nursing activities.
A minor regimen may include, but is not limited to: assistance with self-maintained ex-dwelling or indwelling catheter care for a chronic condition; prophylactic and palliative skin care; routine dressing that does not require packaging or irrigation; general maintenance care of ostomy; restorative nursing assistance; toileting care; routine blood glucose testing; enema and digital stool removal therapies; general maintenance care in connection with braces, splints, and plaster casts; observation of self-maintained prosthetic devices; administration of subcutaneous and intramuscular injections; metered dose inhalers, nebulizer/aerosol treatments self-administered by a resident, and routine administration of medical gases after a therapy regimen has been established.
Housing with services establishments. Except as stated in the contract and identified in the disclosure document, an operator may not restrict the ability of a resident to use a home health agency, home health provider, or case management service of the resident’s choice or require a resident to use home health services.
Dietary
Residential care facilities. Facilities must make available three meals a day, seven days a week that provide a balanced distribution of the daily nutritional requirements. Facilities must meet daily dietary requirements and requests, with consideration of food allergies, reasonable religious, ethnic, and personal preferences, and temporary need for meals to be delivered to the resident’s room. All modified diets must be prescribed by a physician.
Housing with services establishments. Not specified
Agreements
Residential care facilities. Some of the provisions typically included in resident agreements are contained in the section on resident rights. They include the right to receive (at the time of admission) a written notice of the basic daily or monthly rate; all facility services (including those offered on a need basis); information on related charges; and admission, readmission, and discharge policies. A 30-day notice of changes in rates or services is required.
An evaluation of the individual needs of each resident must be initiated before admission and must be updated at least semiannually or upon a significant change in condition. Subsequent evaluations must be used to compare against the baseline evaluation to assure that the care a resident requires is within the range of personal care and supervision provided by the facility. At a minimum the evaluation must include information on the resident’s physical and mental status, independence in activities of daily living, weight, and ability to self-administer medications.
Housing with services establishments. The disclosure document must be provided to a prospective resident or his or her legal guardian and made readily available at any time.
Provisions for Serving People with Dementia
Residential care facilities. Staff caring for residents in dementia-specific units must have a minimum of 6 hours of dementia-specific training within 6 months and 3 hours annually thereafter.
Housing with services establishments. Not specified.
Medication Administration
Residential care facilities. Medications may be administered under physician’s order by licensed nursing personnel or qualified medication aides. Other treatments may be given by nurse aides upon delegation by licensed nursing personnel except for injectable medications which may be given only by licensed staff. The resident must be observed for effects of medications and documentation of undesirable effects is required, followed by notification of the resident’s physician.
Residents who self-medicate may keep and use prescription and non-prescription medications in their unit as long as they are kept secure.
Public Financing
Assisted living. Services are covered under an HCBS waiver. The waiver renewal was approved to serve 186 beneficiaries in the first year, 282 in Year 2, 330 in Year 3, 359 in Year 4, and 400 in Year 5. Currently, 14 facilities have been approved for the waiver program and 71 beneficiaries are being served. Provider and client participation has not expanded as quickly as the State initially projected due to start up delays, and difficulty recruiting providers. Licensed facilities must meet additional requirements for private bedrooms and baths, and a number of additional service requirements. Existing unlicensed assisted living facilities that have submitted a disclosure form and are considered housing with services establishments and meet the waiver program requirements have not expressed an interest in becoming waiver providers because they would need to become licensed, and would need to serve a much higher acuity population than desired.
Medicaid contracting requirements provide for private apartments, shared only by choice, square footage, meal preparation, temperature controls, and door locks that differ from the licensing rules. A three-tiered payment system has been developed based on points from the assessment process (see table below). The rates do not include room and board. The SSI payment maximum is currently $564 (less a $52 personal needs allowance). The State has not issued a policy on family supplementation. The waiver uses the definition and covered services included in the HCBS waiver preprinted format: case management, RN oversight, personal care, homemaker, chore, attendant care, companion, medication oversight, and therapeutic and recreational programming.
The Residential Care Assistance Program is a state-funded program that covers limited services for residents who are aged, blind, mentally ill or disabled, low income, and/or cannot live alone but do not qualify for nursing home care. Payments are based on a flat rate. County home (housing with services establishments) rates are $27 per day for room, board, laundry, housekeeping, and limited oversight. Private residential care facility rates are $39.35 per day. Nineteen county homes and 42 RCFs served 418 county home residents and 1,121 people in private residential care facilities respectively as of March 2004.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participation | Facilities | Participation | Facilities | Participation |
| 14 | 71 | 8 | 22 | NA | NA |
| Level | Daily Rate |
|---|---|
| Level 1: (<36 points) | $45.86 |
| Level 2: (36-60 points) | $53.78 |
| Level 3: (61-75 points) | $61.68 |
Staffing
Residential care facilities. Each facility must have one administrator who is responsible for the overall administration of the facility. Staff shall be sufficient in number, qualifications and training to meet the 24-hour scheduled and unscheduled needs of the residents and services provided. A minimum of one awake staff person, with CPR and first aid certificates, must be on duty at all times. If 50 or more residents require nursing services and/or administration of medication, at least one nursing staff person must be on staff at all times. For facilities with 100 or more residents requiring nursing services and/or administration of medication, at least one awake staff person must be on duty at all times, with an additional staff person required for every additional 50 residents.
A consultant pharmacist must be employed or under contract. The facility must designate an activities director who is a recreational therapist, an occupational therapist or a certified occupational therapist assistant, or someone who will complete, within 1 year, an activities director training course approved by the State.
Housing with services establishments. Not specified.
Training
Residential care facilities. Administrators must be licensed.
Staff (residential care facilities). Prior to working independently, each employee shall be given an orientation of the facility by the supervisor. Orientation of all employees shall include:
- Instructions on the needs of the specialized populations served in the facility;
- A review of the facility’s policy manual and applicable procedures including organizational chart, personnel policies, appearance and grooming, and resident rights;
- Instructions in first aid, emergency procedures, and fire and disaster preparedness, including evacuation procedures;
- A detailed review of the appropriate job description, including a demonstration of equipment and procedures required of the specific position to which the employee will be assigned;
- Review of ethical considerations and confidentiality in resident care and records;
- For direct care staff, personal introduction to and instruction in the particular needs of each resident to whom the employee will be providing care; and
- Documentation of orientation in the employee’s personnel record.
Ongoing training must include resident’s rights, prevention and control of infection, fire prevention, safety, and accident prevention, the needs of specialized populations served, medication administration, and nursing care. For nursing personnel, training must include at least 8 hours of in-service per calendar year and 4 hours of training for nonnursing personnel.
Any unlicensed employee providing more than limited assistance with activities of daily living must be either a certified nurse aide or home health aide.
Background Check
Not described.
Monitoring
Residential care facilities. Annual surveys are conducted by the Department of Health.
Housing with services establishments. The State may impose financial penalties for violations of the disclosure requirement. A housing with services establishment may request a review of the penalty. If the State determines that an establishment has had substantial and repeated violations, the State may prohibit an establishment from using the term “assisted living” to describe the establishment’s services and operations to the public. If the State determines that the establishment has made intentional violations of the disclosure requirement or has made fraudulent and material misrepresentatives to a resident, the State may request the attorney general to investigate and take appropriate action against the operator or administrator.
Fees
Licensure fees are collected annually: $200 for the first 50 beds and each additional bed is $10.
Iowa
Citation
Assisted living programs: Iowa Code 231C and 321 IAC Chapter 25, 26, and 27; IAC 661--5.626 Assisted Living Housing (Life Safety)
Residential care facilities: IAC Chapter 57 and Chapter 60
Related codes that affect but do not specifically reference assisted living: 655 IAC Chapter 6-Nurse Practice; 645 IAC Chapter 63-Salons; Iowa Code Chapter 155A-Pharmacy; 481 IAC Chapters 30 & 32-Food Service Establishments
General Approach and Recent Developments
Revisions to the regulations were effective May 14, 2004. During the past few years, the level of care provided has received attention. Assisted living programs are viewed as a point along a continuum of settings and not appropriate for people who are dependent in ADLs, have late-stage dementia or compromised health conditions.
Responsibility for oversight and monitoring was transferred from the Department on Aging to the Department of Inspection and Appeals. The Department on Aging retains responsibility for issuing regulations. The shift has changed the monitoring from responding to events triggered by complaints to examining program operations and practices in relation to the regulations. The State continues to emphasize consumer choice and autonomy. The nursing and social work staff responsible for oversight are located in a separate monitoring (rather than survey) unit which is separate from the institutional survey staff.
A task force will issue a report recommending creation of a Medicaid assisted living benefit and a payment that includes waiver and state plan services.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted living programs | 184 | 5,220* | 154 | 4,180* | 78 | 3,409 |
| * The total capacity is 8,246 in 2004 and 6,199 in 2002, including double occupancy units. | ||||||
Definition
“Assisted living means provision of housing with services which may include, but are not limited to, health related care, personal care and assistance with instrumental activities of daily living to six or more tenants in a physical structure which provides a home-like environment. Assisted living also includes encouragement of family involvement, tenant self-direction, and tenant participation in decisions that emphasize choice, dignity, privacy, individuality, shared risk, and independence. Assisted living includes the provision of housing and assistance with instrumental activities of daily living only if personal care or health related care is also included.” 96 Acts, Chapter 1192. SF 2193 modified the definition by including housing and IADLs only if personal care and health related services are included.
A dementia-specific assisted living program means an assisted living program that either serves five or more tenants with dementia or cognitive disorder at Stage 4 or above on the Global Deterioration Scale or holds itself out as providing special care for persons with cognitive disorder or dementia, such as Alzheimer’s disease, in a dedicated setting.
Unit Requirements
Assisted living programs may have private dwelling units with lockable doors and individual cooking facilities. In facilities built before July 2001, units must have at least one room with not less than 120 square feet of floor area. Other habitable rooms must have at least 70 square feet. Each single occupancy dwelling unit in buildings built after July 2001 must have at least 240 square feet of floor area, excluding bathrooms. Units used for double occupancy must have at least 340 square feet, excluding bathrooms. The space requirements are lower for dementia units.
Admission/Retention Policy
Programs may not admit or retain tenants who are bedbound, require two person assistance with standing, transfer or evacuation; pose a danger to self or others; are in an acute stage of alcoholism, drug addiction or uncontrolled mental illness; are under age 18; require more than part-time or intermittent health related care (21 days); on a routine basis have unmanageable incontinence; or meet the program’s transfer criteria. Part-time or intermittent nursing care includes licensed nursing care for unstable conditions, daily medication injections (except stable diabetes), daily assessment or treatment of conditions such as an open wound or pressure ulcer, total care for unmanageable incontinence, or routine two-person assistance with standing, transfer, or evacuation. Managed risk statements must be used. The facilities policy is stated in the application for certification.
Exceptions to the limit on part-time or intermittent health care may be requested for residents who need hospice care or temporarily need more than part-time or intermittent health care for more than 21 days. Approvals may be given for limited time periods if the resident makes an informed choice to remain, the program has the staff to meet the extended needs, and the health and welfare of other tenants is not jeopardized.
Nursing Home Admission Policy
Intermediate level of care can be approved if the individual requires daily supervision with dressing and personal hygiene in conjunction with one of the following: cognitive functions, mobility, skin, pulmonary status, continence, physical functioning--eating, medications, communication/hearing/vision patterns, or prior living circumstances--psychosocial.
Intermediate level of care can also be approved if the individual requires physical assistance by one or more persons to perform dressing and personal hygiene.
Services
The certification application includes the process for assessing tenants’ functional and cognitive ability and a copy of the assessment tool. Individualized service plans are required. Programs must provide some personal care or health related services and at least one meal a day. Health related services mean less than daily skilled nursing services and professional therapies for temporary but not indefinite periods of time of up to 21 days a month. Skilled services and therapies combined with personal care and nurse delegated activities may not total more than eight hours a day. Service plans must be developed for each tenant, and plans for tenants needing personal care or health related services must be developed with a multidisciplinary team (including a health professional and human services professional) and the tenant.
The rules allow a managed risk statement which includes the tenant’s or responsible person’s signed acknowledgment of the shared responsibility for identifying and meeting needs and the process for managing risk and upholding tenant autonomy when tenant decision making may result in poor outcomes for the tenant or others.
Dietary
Facilities must have the capacity to provide hot or other appropriate meals at least once a day or to coordinate with other community providers to make arrangements for the availability of meals. Therapeutic diets may be provided.
Agreements
Each tenant signs an occupancy agreement and managed risk statement prior to occupancy. The agreement includes a shared responsibility/managed risk policy, all fees, charges, and rates describing tenancy and basic services covered, any additional and optional services and their cost. It also includes a statement regarding the impact of the fee structure on third party payments and whether they will be accepted by the program; procedure for non-payment of fees; identification of the person responsible for making payment; guarantee of a 30-day written notice of any changes in the agreement unless the tenant’s health status or behavior creates a substantial threat to health and safety; occupancy and transfer criteria; grievance policies; emergency response policy; the staffing policy including whether or not staff are available 24-hours a day, whether delegation will be used and how staffing will be adapted to meet changing needs. Additional provisions are added for programs serving people with dementia; refund policy; statement regarding billing, telephone number to make a complaint; a copy of the tenant’s rights provisions; and a statement that tenant landlord law applies to assisted living programs.
Provisions for Serving People with Dementia
Units built in a neighborhood design offer 150 square feet of floor excluding bathroom for single occupancy and 250 square feet for double occupancy. The difference in square footage must be added to the common areas. Facilities must have an operating door alarm system. Visual or audible alarms may be disconnected if it is disruptive to a tenant. The tenant agreement must include a description of the services and programming.
Programs must have a system, program, or staff procedure that responds to emergency needs in lieu of a personal emergency response system. Training for all employees includes 6 hours on specified topics that include: explanation of the disease; philosophy and program; skills for communicating with residents and family; family issues; importance of planned and spontaneous activities; providing ADL assistance; service planning and social history; working with challenging tenants; simplifying cuing and redirecting; and staff support and stress reduction.
Medication Administration
Written medication plans are required. Medications may be administered in accordance with state rules governing administration. Nurse delegation rules allow administration and supervision of routine, oral medications by trained unlicensed personnel. Registered nurses may delegate injections to licensed nursing staff. Delegation rules are issued by the Board of Nursing. Registered nurses must monitor administration, ensure orders are current and are administered consistent with the orders. They must also document the resident’s health status and progress every 90 days.
Public Financing
Assisted living is covered through a Medicaid HCBS waiver, state service funds, and a state funded rent supplement program.
Medicaid: Certified or accredited assisted living programs may be providers of Medicaid home and community based waiver services including: assistive devices, chore, consumer directed attendant care, emergency response, home delivered meals, home health aide, homemaker, nursing, nutritional counseling, respite, senior companions, and transportation.
Services are reimbursed on a fee-for-services basis according to the care plan. There is a maximum cap of $1,025 per month on care plans.
One affordable facility has opened under the Coming Home Program. The Iowa Finance Authority will be tracking the state/federal dollar savings on a monthly basis. The State estimates that it saves $905.52 a month in state and federal Medicaid expenditures for each resident served.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participation | Facilities | Participation | Facilities | Participation |
| 73 | 126 | 54 | 129 | 12 | NR |
The SSI payment standard is $564 and the personal needs allowance is $30. The resident’s room-and-board payment is separate from the Medicaid service amount. The State uses the 300 percent Medicaid eligibility option. Residents may retain up to $1,692 a month of their income to cover room and board and other costs. Family supplementation of resident income for room and board costs is allowed up to the $1,692 limit.
State Supplementary Assistance: This state funded program provides up to $483 a month in payments for in-home health related services that are not covered under other programs or for HCBS assisted living residents who need more care than is available under the service cap. Services may include nursing and personal care tasks when certified by a physician that the services can be provided in a person’s home, including assisted living.
State rental assistance program: This program works like HUD’s Section 8 program and pays rental expenses for low income beneficiaries who do not have access to rent subsidies. Beneficiaries pay 30 percent of their income for rent. The program can pay the difference between the tenant’s payment and the fair market rent set by HUD. Participants must be eligible for waiver services. A special one-time grant of $500 is available to pay for household furnishings and supplies for people who are moving from an institution.
Staffing
Sufficient staffing must be available at all times to meet the needs of residents. Programs administering medications or providing health related services must provide for a registered nurse to monitor medications, ensure physician orders are current (30 days), and assess and monitor health status (90 days). Each program must provide access to a 24-hour emergency response system.
Training
Administrators. The owner or sponsor of the assisted living program is responsible for ensuring that both management and direct service employees receive training appropriate to the task.
Staff. The assisted living program shall have a training and staffing plan on file and shall maintain documentation of training received by staff. All personnel of the assisted living program shall be able to implement the assisted living program’s accident, fire safety, and emergency procedures.
Background Check
Not described.
Monitoring
Monitoring staff hold community meetings with tenants during their site reviews. The meetings often identify concerns about quality and practice for the monitors. A protocol based on the certification requirements is used to guide the review. Tenants, program staff, and family members are interviewed. During the review, rules may be clarified and explained. Monitoring staff often participate in training meetings organized by three associations representing assisted living programs.
Fees
The fee structure was changed in 2004. Distinctions between small and large programs were eliminated. The regulations require a $900 fee for reviewing blue prints. The 2-year initial certification fee is $750. The recertification fee for a nonaccredited program is $1,000 and $125 for an accredited program.
Kansas
Citation
Assisted living/Residential Health Care Facilities: KAR §28-39-144-148, KAR 28-39-240-256
General Approach and Recent Developments
Licensing rules were last amended in October 1999 and the recent focus has been on monitoring, training and improving outcomes. The law created an overall framework of adult care homes which includes nursing facilities, nursing facility for mental health, intermediate care facility for the mentally retarded, assisted living facility, residential health care facility, home plus, boarding care home, and adult day care facility. The regulations differentiate among the categories of adult care homes.
Responsibility for regulating assisted living facilities has been transferred from the Department of Health and Environment to the Department on Aging. A Money Follows the Person pilot program began in 2003 to support the service costs for people who move from a nursing home to a community setting.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted living facilities | 191 | 7,971 | 129 | 5,658 | 80 | 4,521 |
| Residential health care facilities | 98 | 2,918 | 43 | 2,355 | ||
| Home plus | NR | NR | 44 | 94 | 51 | 224 |
Definition
Assisted living facility means any place or facility caring for six or more individuals not related within the third degree of relationship to the administrator, operator, or owner by blood or marriage and who, by choice or due to functional impairments, may need personal care and may need supervised nursing care to compensate for activities of daily living limitations and in which the place or facility includes apartments for residents and provides or coordinates a range of services including personal care or supervised nursing care available 24-hours a day, seven days a week for the support of resident independence. The provision of skilled nursing procedures to a resident in an assisted living facility is not prohibited by this act. Generally, the skilled services provided in an assisted living facility shall be provided on an intermittent or limited term basis, or, if limited in scope, on a regular basis.
The rules provide that the administrator or operator of facilities ensure that written policies and procedures are developed and implemented which incorporate the principles of individuality, autonomy, dignity, choice, privacy, and a home-like environment.
Unit Requirements
Each facility must offer apartments which include areas for sleeping, living, storage, kitchen (with sink, refrigerator, stove or microwave, and space for storage of utensils and supplies), and bathroom. They must also offer at least 200 square feet of living space, excluding bathroom, closets, lockers, wardrobes, other built-in fixed items, alcoves, and vestibules. Facilities licensed prior to January 1, 1995, as an intermediate personal care facility, are not required to offer kitchens and private baths.
Residential health care facilities are required to have individual living units with at least 100 square feet of living space and a private toilet room with a bathing facility.
Admission/Retention Policy
Each facility develops admission, transfer, and discharge policies which protect the rights of residents. Facilities may not admit or retain people with the following conditions unless the negotiated service agreement includes hospice or family support services which are available 24 hours a day or similar resources:
- Incontinence where the resident cannot or will not participate in management of the problem;
- Immobility requiring total assistance in exiting the building;
- Any ongoing condition requiring two-person transfer;
- Any ongoing skilled nursing intervention needed 24 hours a day for an extended period of time; or
- Any behavioral symptom that exceeds manageability.
Nursing Home Admission Policy
A Standard Client Assessment Referral Evaluation (CARE) is used to assess impairments in ADLs and IADLs and risk. ADLs and IADLs are weighted. ADLs: dressing and mobility (3); bathing and eating (4); toileting and transfer (5). IADLs: meal preparation and medical management (5); money management (4); and shopping, transportation, telephone use, laundry, and housekeeping (3). The weightings are multiplied by a factor based on the need for no assistance (0); physical assistance or supervision (1), and unable to perform (3). Risk factors include: bladder incontinence (5), risk of abuse, neglect, or exploitation by others (5), falls (3), lack of support (4), and impaired cognition (4).
To be eligible, applicants must have a minimum of two ADLs with minimum combined weight of six; impairments in a minimum of three IADLs with a minimum combined weight of nine; and a total minimum score of 26, or a minimum score of 26 with at least 12 points in IADL impairments and the remaining 14 in any combination of IADL, ADL, and risk factor points.
Services
Services may include meals; health care services based on an assessment by a licensed nurse; housekeeping; medical, dental, and social transportation; and other services necessary to support the health and safety of the resident. Health care services include personal care, supervised nursing care, and wellness and health monitoring. The service agreement contains the skilled nursing services to be provided and the licensed person or agency providing services.
The Medicaid waiver includes assisted living facilities as a provider of respite and health care attendant services. The services covered by the waiver include respite care, sleep cycle support, health care attendant (Level I and Level II), adult day care, and wellness monitoring. Sleep cycle support means “non-nursing physical assistance and supervision during the consumer’s normal sleeping hours in the consumer’s place of residence, excluding nursing facilities” and includes “physical assistance or supervision with toileting, transferring and mobility, prompting and reminding of medication.”
Health care attendant “provides physical assistance with activities of daily living and instrumental activities of daily living for individuals who are unable to perform one or more activities independently.” IADLs, excluding medication management or medication administration, may be performed without nurse supervision. These services are limited to 12 hours a day.
Level I activities include assistance with ADLs and IADLs (bathing, grooming, toileting, transferring, feeding, mobility, accompanying to obtain necessary medical services, shopping, house cleaning, meal preparation, laundry, and life management).
Level II activities are health maintenance activities and include monitoring vital signs, supervision and/or training of nursing procedures, ostomy care, catheter care, enteral nutrition, medication administration/assistance, wound care, range of motion, and reporting changes in function or condition. These services must be authorized by a physician or a nurse.
Dietary
A dietetic services supervisor or licensed dietician must provide scheduled on-site supervision in facilities with 11 or more residents. Therapeutic diets are provided if included in the negotiated service agreement, based on instructions from a physician or licensed dietician. Menus must be planned based on the dietary guidelines for Americans, 4th edition, published by USDA and DHHS.
Agreements
Facilities must develop a negotiated service agreement with each resident in collaboration with the resident, the resident’s legal representative, family (if agreed to by the resident), or case manager. The agreement describes the services to be provided, the provider of service, and the parties responsible for payment when services are provided by an outside agency. The agreement supports the dignity, privacy, choice, individuality, and autonomy of the resident. The agreement is reviewed at least annually or when requested by any of the participating parties. The agreements also address services that are refused by the resident; the potential negative consequences; and the resident’s acceptance of the risks involved.
Provisions for Serving People with Dementia
People with special needs may be served if the facility has admission and discharge criteria that identify the diagnosis, behavior, or specific clinical needs of the residents to be served. A written physician’s order is required for admission. Prior to admission, the resident or their legal representative must be informed of the services and programs available. Staff must complete training on the needs of the residents to be served. Exits must be controlled in the least restrictive possible manner.
Medication Administration
A drug regimen review conducted by a pharmacist is required for residents who receive assistance with medication administration or whose medications are administered by facility staff. Medication aides may administer oral and topical medications and assist with medication administration. Medication reminding may be performed by a licensed nurse, medication aide, or nurse aide. Medication reminding includes asking if the medication has been taken, handing the medication to the resident, and opening the container. Medication reminding does not include taking the medication out of the container.
Public Financing
A “Money Follows the Person” pilot program began in 2003. Using available HCBS waiver slots for 75 nursing residents, the State uses funds from the nursing home appropriation to pay for services in the community, many of whom are moving to assisted living facilities.
Medicaid waiver services have been available since 1997 to elderly recipients who meet the nursing home level of care criteria and have income below 300 percent of the federal SSI payment. The room-and-board amount is negotiated between the facility and the resident but the amount of income that may be retained by the resident is limited to $716 a month, which is the maintenance allowance. SSI beneficiaries retain a $30 personal needs allowance.
The State uses a “care plan” method for paying for services. The care plan is developed by a case manager in the Area Agency on Aging. Services are billed fee for service. The maximum rate for health care attendant services is $3.18 per unit (15 minutes) for Level I tasks and $3.52 per unit for Level II tasks. Plans requiring a mix of both levels are reimbursed at the Level II rate. Family members may supplement resident income for room and board costs.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participation | Facilities | Participation | Facilities | Participation |
| 155* | 769* | 155 | 769 | NR | NR |
| * Estimate. | |||||
Staffing
Sufficient numbers of qualified personnel must be available to ensure that residents receive services in accordance with negotiated service agreements.
Training
Administrator. The licensee shall appoint an administrator or operator who holds a Kansas license as an adult care home administrator or has successfully completed an operator training program as designated by the secretary. The hours of training for operators was increased from 24 to 32 to spend more time on regulatory requirements and nursing issues.
Staff. Facilities shall provide orientation to new employees and regular in-service training for all employees to ensure that services provided assist residents to attain and maintain their individuality, autonomy, dignity, independence, and ability to make choices in a home-like environment.
In-service education must include: principles of assisted living; fire prevention and safety; disaster procedures; accident prevention; resident rights; infection control; and prevention of abuse, neglect, or exploitation of residents.
In-service education on treatment of behavioral symptoms shall be provided to all employees of facilities that admit residents with dementia.
Background Check
Not described.
Monitoring
Surveyors inspect every facility annually. Consistent enforcement of the regulations has been credited with improved compliance and fewer complaints. Deficiencies are written more concisely with a focus on the consumer and outcomes. Under a new survey process, facility staff accompany the surveyor during the review. Problem areas are identified and discussed with the staff. Educational efforts have been increased. The licensing agency conducts regular one-day training courses for nurses, owners and operators on the role of nursing in assisted living, how to conduct an assessment and develop a service plan, managing medications and the nurse practice act. During the training, scenarios are presented and participants prepare a care plan based on the information presented.
Fees
$50, plus $15 for each resident.
Kentucky
Citation
Assisted living community certification 910 KAR 1:240; relates to KRS 194A.700-729; 42 USC 3029
Statutory authority: KRS 194A.050(1), 194A.707(1)
Personal care homes 902 KAR 20:036
General Approach and Recent Developments
An assisted living community must be certified by the State in order to operate and market itself as an assisted living community. Assisted living communities are considered private business entities. There is no public funding. A bill (HB 174) was passed in 2001 that requires coverage of services in assisted living facilities by long-term care insurance policies. Regulations were promulgated in 2001.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Personal care homes | 204 | 7,389 | 204 | 7,792 | 201 | NR |
| Assisted living communities | 83 | NA | 73 | NA | 6 | NA |
Definition
Assisted living community (ALC) means a series of living units on the same site, operated as one business entity, and certified under KRS 194A.707 to provide services for five or more adult persons not related within the third degree of consanguinity to the owner or manager.
Personal care homes (PCHs) are establishments with permanent facilities including resident beds. Services provided include continuous supervision, basic health and health-related services, personal care services, residential care services, and social and recreational activities.
Unit Requirements
ALC. Each living unit in an assisted living community shall have at least 200 square feet for single occupancy, or for double occupancy if the room is shared with a spouse or another individual by mutual agreement; include at least one unfurnished room with a lockable door, private bathroom with a tub or shower, provisions for emergency response, window to the outdoors, and a telephone jack; and have an individual thermostat control if the assisted living community has more than 20 units. Units may be shared only by choice. Any assisted living community that was open or under construction on or before July 14, 2000, is exempt from the requirement for each living unit to have a bathtub or shower, or for each living unit having 200 square feet for single occupancy, or for double occupancy if the room is shared with a spouse or another individual by mutual agreement. Such communities must have a minimum of one bathtub or shower for every five residents.
PCH. No requirements are specified for room size. The maximum number of beds per room is four. At least 66 percent of the beds in the facility must be located in rooms designed for one or two beds. Facilities using central bathing areas must have bathrooms and showers/baths for each sex on each floor. One toilet is required for every eight residents, a lavatory for every 16 residents, and a shower/bath tub for every 12 residents.
Admission/Retention Policy
ALC. A client shall be ambulatory or mobile non-ambulatory, unless due to a temporary health condition for which health services are being provided in accordance with KRS 194A.705(2) and (3) not be a danger to self or others.
PCH. Personal care homes may admit persons who are 16 years or older and who are ambulatory or mobile nonambulatory and whose care needs do not exceed the capability of the home. Persons who are nonambulatory or nonmobile may not be admitted to a personal care home. Residents must be able to manage most of the activities of daily living. Residents must have a complete medical evaluation upon admission or within 14 days prior to admission. Residents whose care is not within the scope of services of a personal care home must be transferred to an appropriate facility.
Services
ALC. The assisted-living community shall provide each client with the following services according to the lease agreement: assistance with activities of daily living and instrumental activities of daily living; three meals and snacks made available each day; scheduled daily social activities that address the general preferences of clients; and assistance with self-administration of medication. Clients of an assisted-living community may arrange for additional services under direct contract or arrangement with an outside agent, professional, provider, or other individual designated by the client if permitted by the policies of the assisted-living community. Upon entering into a lease agreement, an assisted living community must inform the client in writing about policies relating to the contracting or arranging for additional services. Assisted living communities may not provide health care services.
PCH. All homes must provide basic health and health-related services including: continuous supervision and monitoring; supervision of self-administration of medications, storage, and control when necessary; and arrangements for obtaining therapeutic services ordered by the resident’s physician which are not available in the facility; activities; housekeeping and maintenance services; laundry; three meals a day; and personal care.
Dietary
ALC. No provisions specified.
PCH. Three meals and snacks are required. Therapeutic diets may be provided. If provided, consultation with a qualified dietician or nutritionist is required unless the person responsible for food service has those qualifications. Menus must meet the nutrition needs of residents as contained in the current recommended dietary allowances of the Food and Nutrition Board. All staff must be trained in accordance with their duties. Training for food staff must cover therapeutic diets.
Agreements
ALC. A lease agreement is required that includes: client data for the purposes of providing services which includes a functional needs assessment pertaining to a client’s ability to perform activities of daily living and instrumental activities of daily living; emergency contact name; name of responsible party or legal guardian; attending physician’s name; information regarding personal preferences and social factors; advance directives; optional information helpful to identify services that meet the client’s needs; general services and fee structure; information regarding specific services provided, unit, and associated fees; a minimum 30-day notice for a change in fee structure; a minimum 30-day notice for move-out notices for nonpayment; refund and cancellation policies; payment responsibilities and arrangements; the owner’s covenant to comply with appropriate laws and regulations; conditions for termination; terms of occupancy; reasonable rules of conduct for staff, management, and tenant; grievance policies; and a copy of the tenant’s rights. It may also include additional services that will be provided or arranged. Agreements must provide for single occupancy apartment unless shared by mutual agreement. An assisted-living community must assist a client in making alternative living arrangements in the event of a move-out notice.
PCH. Upon admission the resident and a responsible family member must be informed in writing of the home’s policies, fees, reimbursement, visitation rights during serious illness, visiting hours, types of diets offered, and services rendered.
Provisions for Serving People with Dementia
ALC. Resident lease agreements contain a description of special programming, staffing, or training for serving clients with special needs. Facilities serving people with special needs are required to provide consumers with information about the special programming, staffing, or training that is offered.
PCH. Not specified.
Medication Administration
ALC. Not specified.
PCH. Medications shall not be administered or provided to any resident except on the order of a licensed physician or other ordering personnel acting within the limits of their statutory scope of practice. Administration of all medications must be kept in the resident’s record. All medications must be kept in a locked place.
Public Financing
No Medicaid funds are available for either category.
Staffing
ALC. Staffing in assisted-living communities shall be sufficient in number and qualification to meet the 24-hour scheduled and unscheduled needs of its clients and services provided. One awake staff member must be on site at all times. A designated manager who is at least 21 years of age with a high school or GED diploma must be employed.
PCH. Based on the needs of residents. One attendant must be awake and on duty on each floor in the facility at all times. The home must identify a staff person responsible for the activities program.
Training
ALC. Assisted-living community staff and management shall receive orientation and in-service education on the following topics as applicable to the employee’s assigned duties: client rights; community policies; adult first aid; cardiopulmonary resuscitation; adult abuse and neglect; Alzheimer’s disease and other types of dementia; emergency procedures; aging process; assistance with ADLs and IADLs; particular needs or conditions if the assisted-living community markets itself as providing special programming, staffing, or training on behalf of clients with particular needs or conditions; and assistance with self-administration of medication.
PCH. All personal care home employees shall receive in-service training to correspond with the duties of their respective jobs. Documentation of in-service training shall be maintained in the employee’s record and shall include: who gave the training, date and period of time training was given, and a summary of what the training consisted of. In-service training shall include but not be limited to the following:
- Policies of the facility in regard to the performance of their duties;
- Services provided by the facility;
- Record-keeping procedures;
- Procedures for reporting adult and child abuse, neglect, or exploitation;
- Patient rights;
- Methods of assisting patients to achieve maximum abilities in activities of daily living;
- Procedures for the proper application of physical restraints;
- Procedures for maintaining a clean, healthful, and pleasant environment;
- The aging process;
- The emotional problems of illness;
- Use of medication; and
- Therapeutic diets.
Background Check
ALC applicants must assure that no officer, director, trustee, limited partner, or shareholder has ever been convicted of a felony, Class A misdemeanor or abuse of a person.
Monitoring
ALC. Unless there is a formal complaint lodged against a facility, the State does not conduct oversight and monitoring of the quality of care in assisted living communities. The State conducts a certification review upon application, and an annual recertification review. These reviews ensure compliance with the certification requirements. Any assisted-living community that provides services or markets itself as assisted living without filing a current application or receiving certification may be fined up to $500 per day.
Fees
ALC. $20 per unit, $300 minimum, and $1,600 maximum. A fee of $250 is charted for architectural review, lease agreement, and notification of conditional compliance to a lender.
Louisiana
Citation
SB 1560 (1997). Adult residential care facility: Louisiana Revised Statutes Annotated §2151 et seq.; LA administrative code title 48, §8901 et seq.
General Approach and Recent Developments
The regulations for adult residential care facilities, which include assisted living facilities, were initially approved in 1999, and created core requirements for adult residential care facilities plus three modules for assisted living facilities, personal care homes, and shelter care facilities. The modules contain separate requirements for administrators, staff training, and living units. The rules state that the purpose of the regulations is to promote the availability of appropriate services for elderly and disabled persons in a residential environment; to enhance the dignity, independence, privacy, choice, and decision-making ability of the residents; and to promote the concept of aging in place.
The regulations may be revised later in 2004 or 2005 to address issues related to caring for people with Alzheimer’s disease, negotiated risk agreements and other issues. A report to the legislature was filed in response to legislation that directed that Department of Health and Hospital nurses who conduct nursing home surveys accompany Department of Social Service surveyors on a sample of facilities.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted living facilities | 67 | 4,157 | 66 | 3,906 | 66 | 3,119 |
| Personal care homes | 44 | 286 | 29 | 176 | 33 | 216 |
| Shelter care homes | 17 | 543 | 26 | 841 | 26 | 670 |
Definition
Adult residential care home means a publicly or privately operated residence that provides personal assistance, lodging, and meals (for compensation) to two or more adults who are unrelated to the residence licensee, owner, or director.
Assisted living home/facility means an adult residential care facility that provides room, board, and personal services, for compensation, to two or more residents that reside in individual living units which contain, at a minimum, one room with a kitchenette and a private bathroom.
Personal care home means an adult residential care facility that provides room, board, and personal services, for compensation, to two but not more than eight residents in a congregate living setting and is in a home that is designed as any other private dwelling in the neighborhood.
Shelter care home means an adult residential care facility that provides room, board, and personal services, for compensation, to nine or more residents in a congregate living and dining setting.
Unit Requirements
Assisted living facilities must offer apartment style units with lockable doors to ensure privacy, dignity, and independence. Efficiency/studio units must provide 250 square feet excluding bathrooms and closets and may be shared by no more than two people by choice. Units with separate bedrooms shall have a living area of at least 190 square feet, excluding bathroom and closets. Each separate bedroom must have 120 square feet.
Personal care homes offer a home-like atmosphere with 100 square feet in single occupancy rooms and 70 square feet per resident for double occupancy rooms.
Shelter care facilities must have 100 square feet in single occupancy rooms and 160 square feet for double occupancy rooms. No more than two residents may share a room, and they must agree in writing to share a room. Facilities must have adequate toilet, bathing, and hand washing facilities in conformance with the state sanitary code.
Admission/Retention Policy
Residents may include those who need or wish to have available room, board, personal care, and supervision due to age, infirmity, physical disability, or social dependency. Residents with advanced or higher care needs may be accepted or retained if the resident can provide or arrange for care through appropriate private duty personnel, does not need continuous nursing care for more than 90 days, and the provider can meet the resident’s needs. Facilities may not enter into contracts with outside providers to deliver health related services. These services must be arranged by the resident, family members, or the resident’s representative. Residents must be discharged if a physician certifies that more than 90 days of continuous care is needed or the resident is a danger to himself or others.
Nursing Home Admission Policy
The State has criteria for skilled nursing care and two levels of intermediate care. The minimum criteria for admission to a nursing home include: requiring supervision or assistance with personal care needs, assistance in eating, administration of medications, injections less than daily, skin care, protection from hazards, mild confusion or withdrawal, medications for stable conditions or those requiring monitoring once a day, and stable blood pressure requiring daily monitoring. The determination is made by a physician based on his or her professional judgment of the above factors.
Services
Basic services provided include assistance with ADLs and IADLs, three meals a day, personal and other laundry, opportunities for individual and group socialization, housekeeping, services for residents who have behavior problems, recreation services, and assistance with self-administration of medications. Providers must plan or arrange for health assessments, health care monitoring, and assistance with health tasks as needed or requested. Facilities must have the capacity to provide transportation for medical services, personal services (barber/beauty), personal errands, and social/recreational activities.
Dietary
Menus must be reviewed and approved by a nutritionist or dietician to assure nutritional appropriateness. Facilities must make reasonable accommodations to meet dietary requirements and religious and ethnic preferences; to make snacks, fruit, and beverages available when requested; and to provide meals in a resident’s room (on a temporary basis). Medically prescribed special diets must be provided and planned or approved by a registered licensed dietician.
Agreements
Agreements must include: clear and specific occupancy criteria and procedures (admission, transfer, and discharge); basic services available; optional services available; payment provisions (covered and non-covered services; service packages; and á la carte, regular, and extra fees; payer; due date; funding source); modification provisions including at least a 30-day notice of rate changes; refund policy; authority of the licensing agency to examine records; general facility policies/house rules; responsibilities of the facility, resident, and family for overseeing medical care, purchasing supplies/equipment, and handling emergencies and finances; and the availability of a service plan. Facilities must allow review by an attorney.
Provisions for Serving People with Dementia
None specified. Regulations in this area may be developed later in 2004 or early 2005.
Medication Administration
Facilities may provide assistance with self-administration of medications, however, residents may be assisted with pouring or otherwise taking medications only if they are cognitive of what the medication is, what it is for, and the need for the medication. Residents may contract with an outside source for medication administration. Staff assisting with medications must have training on the policies and procedures for assistance.
Public Financing
A four-year pilot program approved by the legislature in 1997 to test the feasibility of covering assisted living under Medicaid has been deferred by budget problems. Legislation passed in 2000 extended authority for the project until 2005. Funds to implement the project have been requested in the 2005 budget, which was pending before the legislature. The project, intended to serve 60 people in two sites, will be implemented by the Department of Health and Hospitals. The project will include two assisted living facilities and serve elderly Medicaid beneficiaries who can no longer live at home because they need additional care with ADLs but do not require continuous nursing care and have no alternative under the traditional model except institutional care. The pilot “shall maximize the independence of the elderly while providing the assistance that the special needs of this population require.” The bill defines assisted living as “a residential congregate housing environment combined with the capacity by in-house staff or others to provide supportive personal services, 24-hour supervision and assistance, whether or not such assistance is scheduled, social and health related services to maximize residents’ dignity, autonomy, privacy, and independence and to encourage facility and community involvement.” Residents must be offered a chance to live in private quarters with a lockable door, bedroom, kitchenette, and bathroom.
The RFP will request that bidders propose a flat monthly rate to serve beneficiaries. Room and board will be limited to the SSI payment, less $100 for personal needs. The State plans to use the 300 percent eligibility option.
Staffing
Providers must demonstrate that sufficient staff are scheduled and available to meet the 24-hour scheduled and unscheduled needs of residents and show adequate coverage for each day and night. Assisted living facilities and shelter care facilities must have at least one awake staff on duty at night.
Training
Administrators must be 21 years of age. Assisted living administrators must have a bachelor’s degree plus two years of experience in the field of health, social, management administration, or in lieu of a degree, 6 years of experience and education or a master’s degree in geriatrics, health care administration, or a human service related field.
Shelter care home administrators must have 2 years of college and 2 years experience or 4 years experience in lieu of college or a bachelor’s degree. Personal care home administrators must have 2 years of college training plus 1 year experience or 3 years of experience in lieu of college or a bachelor’s degree.
Staff. An orientation program shall include but not be limited to thorough coverage of the following areas: facility policies and procedures, emergency and evacuation procedures, residents’ rights, procedures for and legal requirements concerning the reporting of abuse and critical incidents, and instruction in the specific responsibilities of each employee’s job. Direct care staff orientation must cover training in resident care services (personal care), infection control, and any specialized training to meet resident needs. All direct care staff must receive certification in first aid. An annual training plan must be developed that includes the topics covered by the orientation.
Background Check
Licenses may be denied based on a criminal conviction of any board member, owner, or staff if the act that caused the conviction would cause harm to a resident if repeated. Providers must include the results of a criminal history check in each employee’s personnel file.
Monitoring
The Department of Health shall make at least annual inspections. Complaints are to be reviewed and investigated by the appropriate state agency.
Fees
The annual licensing fee for ALFs is $175 for two to four beds; $200 for five to eight beds; and $250 for nine or more beds. The fee for personal care homes is $200.
Maine
Citation
Assisted Living Programs 10-144 Chapter 113
General Approach and Recent Developments
The State licenses five types of facilities providing assisted living services--assisted living programs and four levels of residential care facilities. The levels vary primarily by size. Residential care facilities may offer the same services assisted living programs do, but provide bedrooms rather than apartment units. The scope sections of the rules establish a philosophy of regulation to support services that are individualized to meet resident needs and encourage each resident’s right to independence, choice and decision-making, while providing a safe environment.
Regulations implementing the legislation passed (Chapter 1664) in 2002 were effective in September 2003.
| Category | 2004 | Category | 2002 | 2000 | |||
|---|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | ||
| Level I RCF | 95 | 161 | Level I residential care | 473 | 1,711 | 509 | 1,799 |
| Level II and III RCF | 415 | 1,785 | Level II residential care | 192 | 5,220 | 189 | 4,904 |
| Level IV RCF | 201 | 5,647 | |||||
| ALP | 30 | 1,429 | Congregate housing | 24 | 1,133 | 14 | 799 |
Definition
Assisted living services means the provision by an assisted living program, either directly by the provider or indirectly through contracts with persons, entities or agencies, of assisted living services which include personal supervision; protection from environmental hazards; assistance with activities of daily living and instrumental activities of daily living; diversional, motivational or recreational activities; dietary services; care management services; administration of medications; and nursing services.
Assisted living services may be provided in two types of settings--assisted living programs and residential care facilities. Residential care facilities are further divided into four subgroups.
Assisted living program means a program of assisted living services provided to consumers in private apartments in buildings that include a common dining area, either directly by the provider or indirectly through contracts with persons, entities or agencies. The types of assisted living programs governed by these regulations include:
-
Type I--an assisted living program that provides assisted housing services and medication administration directly or indirectly through contracts with persons, entities or agencies.
-
Type II--an assisted living program that provides assisted housing services, medication administration and nursing services directly or indirectly through contracts with persons, entities or agencies to provide services of a registered professional nurse; and/or registered professional nurse coordination and oversight of consumer services provided by unlicensed health care assistive personnel.
Residential care facility means a house or other place that, for consideration, is maintained wholly or partly for the purpose of providing residents with assisted living services. (Note: both assisted living programs and residential care facilities provide assisted living services. The definition of the living unit differs.)
Residential care facilities provide housing and services to residents in private or semi-private bedrooms in buildings with common living areas and dining areas. There are four types of residential care facilities:
-
Level I--licensed capacity of 1 to 2 residents (licensing is voluntary for this group).
-
Level II--licensed capacity of 3 to 6 residents.
-
Level III--licensed capacity of 3 to 6 residents and which employs three or more persons who are not owners and are not related to the owner.
-
Level IV--licensed capacity of more than 6 residents.
Alzheimer’s/dementia care unit means a unit, facility, or distinct part of a facility that provides care/services in a designated separate area for residents with Alzheimer’s disease or other dementia. The unit, facility, or distinct part provides specialized programs, services, and activities and is locked, segregated, or secured to provide or limit access by a resident outside the designated or separated area.
Unit Requirements
Assisted living programs are multi-unit residential buildings that provide apartments and must meet state and local building codes.
Level I-IV residential care facilities must offer 100 square feet for single room and 80 square feet for double rooms. Level IV facilities provide one toilet and sink for every six residents. Facilities licensed on or after May 30, 2002, must have one bathing facility for 10 users (one for 15 residents for facilities licensed prior to May 30, 2002). No more than two residents may share a room.
Admission/Retention Policy
The rules encourage aging in place and have very flexible policies to achieve that goal. In its application, all facilities must describe who may be admitted and the types of services, including the scope of nursing services, to be provided. Facilities may discharge tenants who pose a direct threat to the health and safety of others, damage property, or whose continued occupancy would require modification of the essential nature of the program. The rules also require facilities to permit reasonable modifications at the expense of the tenant or other willing payer to allow persons with disabilities to reside in licensed facilities. Providers may require the disabled individual to return the premises to its prior condition.
Nursing Home Admission Policy
In brief, individuals must meet medical, medical/functional or cognitive/behavior requirements. Individuals must have a need for daily skilled nursing or extensive assistance in three of the following ADLs: bed mobility, transfer, locomotion, eating and toileting; or a combination of three needs in the following areas: skilled nursing, cognition, behavior, and at least limited assist in 1 of the following ADLs: bed mobility, transfer, locomotion, eating and toileting. The list of nursing services includes any specified physician-ordered services provided on a frequent rather than daily basis; professional nursing assessment, observation and management for impaired memory, and impaired recall ability, and impaired cognitive ability; professional nursing assessment, observation, and management for problems including wandering, physical abuse, verbal abuse or socially inappropriate behavior; administration of treatments, procedures, or dressing changes that involve prescription medications and require nursing care and monitoring; and professional nursing for physician-ordered radiation therapy, chemotherapy, or dialysis. Skilled services also include physician-ordered occupational, physical, or speech/language therapy or some combination of the three, which must require the professional skills of a licensed or registered therapist.
The cognition and/or behavior requirements apply for individuals who do not require professional nursing intervention at least 3 days per week but are eligible if they have a qualifying score on the Cognitive Screen and/or Behavioral Screen, in combination with a need for at least “limited assistance” with an ADL, for a total of three service needs. The qualifying scores are cognitive score = 13 points and two ADL’s; or cognitive score = 13 points and behavioral score = 14 and one ADL; or behavioral score = 14 points and two ADL’s.
Services
All facility levels are required to describe the scope of services provided, including scope of nursing services consistent with applicable state and federal law as part of their licensing application.
Assisted living programs must offer service coordination, housekeeping services, assistance with ADLs and IADLs, at least one nutritious meal a day, chore services and other services identified in a service plan.
Level I, II, and III residents have the right to receive assistance from the provider to implement any reasonable plan of service developed with community or state agencies.
Level IV residents are able receive individualized services that help them age in place, function optimally in the facility and in the community, engage in constructive activity, and manage their health conditions and accommodate individual choices and preferences. The regulations require reasonable accommodation in regulations, policies, practices or services, including permitting reasonable supplementary services to be brought into the facility/program unless it imposes an undue financial burden or results in a fundamental change in the program.
Residents must be assessed within 30 calendar days of admission and reassessed annually or when there is a significant change in condition. A service plan must be developed and implemented within 30 calendar days of admission based upon the assessment. The plan addresses areas in which the resident needs encouragement, assistance or an intervention strategy. The plan describes strategies and approaches to meet the resident’s needs, names of who will arrange and/or deliver services, when and how often services will be provided and goals to improve or maintain the resident’s level of functioning. Residents are encouraged to be as independent as possible in their functioning, including ADLs and normal household tasks if they choose, unless contraindicated by the resident’s duly authorized licensed practitioner.
Dietary
Assisted living program. A registered dietician must approve menus and menu cycles annually. Menus must be planned in accordance with resident needs and preferences. Therapeutic diets must be ordered by any duly licensed practitioner in all levels. A least one nutritious meal a day must be delivered by the assisted living program.
Levels I-IV require a nourishing, well-balanced diet that meets the daily nutritional and special dietary needs of each resident and that meets the Recommended Dietary Allowances of the Food and Nutrition Board of the National Research Council, National Academy of Sciences. Level IV facilities must have a meal plan that provides three meals in a 24-hour period and a dietary coordinator who has experience and/or training in food service suitable to the size of the facility.
Agreements
The State requires adoption of a standard contract for all assisted living services. All resident contracts will contain standard provisions regarding services and accommodations to be provided and the rates and charges for such and any other related charges not covered by the facility/program’s basic rate. Each contract may not contain a provision for the discharge of a resident that is inconsistent with state law or rule; a provision that may require or imply a lesser standard of care or responsibility than is required by law or rule; provide for at least 30 calendar day’s notice prior to any changes in rates, responsibilities, services to be provided or any other items included in the contract; may not require a deposit or other prepayment, except one month’s rent in an assisted living program, which may be used as a security deposit provided there is a statement of the explicit return policy of the facility with regard to the security deposit; and may not contain a provision that provides for the payment of attorney fees or any other cost of collecting payments from the resident. Additional information is appended to the contract--grievance procedure, tenancy obligations, resident rights, and a copy of the admissions policy.
In addition, an information packet must also be provided that contains advance directives information; information regarding the type of facility and the licensing status; the Maine Long Term Care Ombudsman Program brochure; toll-free telephone numbers for the Office of Advocacy of the Department of Behavioral and Developmental Services (BDS) if the facility has residents who receive services from BDS; Adult Protective Services; Assisted Living Licensing Services and Division of Licensing and Certification; the process and criteria for placement in, or transfer or discharge from, the program; and the program’s staff qualifications.
Provisions for Serving People with Dementia
The provisions for serving people with dementia apply to all levels. Facilities must provide written information about their philosophy; the process used for resident assessment and establishment of a residential services plan and its implementation; the physical environment and design features that support the functioning of adults with cognitive impairments; the frequency and types of group and individual activities provided by the program; a description of family involvement and the availability of family support programs; a description of security measures provided by the facility; a description of in-service training provided for staff; and policies with criteria and procedures for admission and discharge of residents to and from the facility/unit.
The design must include secured outdoor space and walkways; high contrast between floors, walls, and doorways; nonreflective surfaces; and even lighting to minimize glare. Residents may not be locked inside or outside of their rooms. Residents are encouraged and assisted to decorate their unit with personal items and furnishings. Facilities try to individually identify each resident’s room to help with recognition. Facilities also have policies and procedures to deal with wandering. Electronic locking devices may be used on exterior doors if they release in an emergency.
These facilities must provide individual and/or group activities covering gross motor skills, self care, social interaction, crafts, sensory enhancement, as well as outdoor and spiritual activities.
For pre-service training, all facilities with Alzheimer’s/dementia care units must provide a minimum of 8 hours of classroom orientation and 8 hours of clinical orientation to all new employees assigned to the unit. The trainer(s) shall be qualified with experience and knowledge in the care of individuals with Alzheimer’s disease and other dementias. In addition to the usual facilities orientation, which should cover such topics as resident rights, confidentiality, emergency procedures, infection control, facility philosophy related to Alzheimer’s disease/dementia care, and wandering/egress control, the eight hours of classroom orientation should include the following topics: a general overview of Alzheimer’s disease and related dementias, communication basics, creating a therapeutic environment, activity focused care, dealing with difficult behaviors, and family issues.
Medication Administration
Unlicensed staff who have successfully completed a training program approved by the licensing agency may administer medications and/or treatments. All residents are assessed for their ability to self-administer medications or their need for assistance. A standard curriculum for training in medication administration was adopted for use statewide.
Public Financing
Maine uses two programs to cover services in residential care facilities: a Medicaid state plan option and state revenues. While assisted living is not listed as a covered waiver service, residents of residential care facilities could receive HCBS waiver services (personal support services, homemaker, chore, home health, transportation, personal emergency response) as long as there is no duplication between the services covered in the residential care facility payments and the waiver services. The state plan program provides reimbursement for personal care services through contracts with Private Non-Medical Institutions (PNMIs) licensed as Residential Care Facilities. Payment levels are based on the average acuity of residents in the facility. The same reimbursement restrictions on duplication of payment apply to HCBS waiver services for people living in assisted living programs.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participation | Facilities | Participation | Facilities | Participation |
| 150 | 3,762 | 151 | 3,096 | 141 | 3,190 |
The state SSI payment standard was changed July l, 2004, to $574 which includes personal needs allowance of $70/month ($50 if there is no earned income). State general fund are available to supplement the resident’s room and board payment when the allowable cost of room and board exceeds the resident cost of care.
A State-funded demonstration program serves 175 beneficiaries in seven affordable assisted living programs. Services are based on a plan of care. The resident pays standard HUD rents, and contributes 30 percent of his or her income toward services retaining at least $100 for their personal needs. On July 1, 2004, these services were covered as Medicaid state plan services. Payments are based on Medicaid beneficiary-specific rates according to their acuity.
Staffing
Administrators
Assisted living programs. The sponsor must assure that services will be provided to residents in accordance with individual service plans. Administrators must hold a professional license related to residential or health care or have a combination of 5 years of related education and experience.
Residential care facilities. Level IV administrators must demonstrate capacity to operate and manage the facility and allow access to records of professional licensing boards or registers, any criminal record, child protective record or adult protective record relating to the applicant/licensee and administrator, and other records.
Administrators must successfully complete a Department-approved training program for administrators unless they have a license from the Nursing Home Administrators Licensing Board as a Residential Care Administrator or Multi-Level Facility Administrator. They must obtain 12 hours a year of continuing education.
Staff
Levels I and II. Operators must have a person available to provide supervision in their absence. Staffing must be adequate to implement service plans. The department may require additional staff based on the needs of residents and the size and lay out of the facility.
Level III. Staffing must be adequate to implement service plans. Additional staffing may be required by the Department. The licensing agency has the authority to require that Level I-III facilities obtain services from a consulting nurse, pharmacist or dietician and a consulting dietician for Level IV facilities.
Level IV. RCFs serving over ten residents must have two awake staff on duty at night (one must be direct care staff. The rules require a ratio of one direct care staff to12 residents from 7 a.m. to 3 p.m.; one direct care staff to 18 residents from 3 p.m. to 11 p.m.; and one direct care staff to 30 residents from 11 p.m. to 7 a.m. The revised rules require a registered nurse on staff or contract to observe signs and symptoms; review records, medication records, medication administration practices and procedures, and therapeutic diets; and recommend staff training. The frequency of these activities varies with the size of the facility from weekly for larger facilities to quarterly for smaller facilities.
Level IV facilities with more than 10 beds must have a pharmacy consultant no less than quarterly to review written policies and procedures for pharmaceutical services; medication areas for labeling, storage, temperature, expired medications, locked compartment, access to keys and availability and completeness of a first aid kit; review to ensure that only approved drugs and biologicals are used in the facility; review medication records and initial and date the records when reviewed; review adherence to stop orders; and review staff performance in carrying out pharmaceutical policies and procedures.
Training
Administrators must successfully complete a department approved training program. Ongoing training of at least 12 classroom hours annually is required in areas related to care of the population served.
Staff. Level I, II, III. Residential care staff must attend and show evidence of successful completion of any training that the department determines to be necessary.
Level IV. All staff, other than certified nursing assistants (CNAs) and licensed professional staff, whose job responsibilities include direct service to residents for at least 20 hours per week, shall successfully complete a Personal Support Specialist certification course within 120 days of hiring. Additional training specific to a facility’s programs may be identified and required by the Department for any staff.
Any person working in the facility must demonstrate the following: conduct which demonstrates an understanding of, and compliance with, residents’ rights; the ability and willingness to comply with all applicable laws and regulations; the ability to provide safe and compassionate services; and a history of honest and lawful conduct.
Additional requirements for individuals who administer medications in Levels III and IV. Staff must complete a training program approved by the department and must have 8 hours of refresher training every 2 years. If the training program is substantially revised, they must be re-certified within 1 year of the change.
Background Check
During the licensure process, a criminal background check is conducted for the applicant and the administrator. Facilities must contact the CNA Registry and determine that the CNA or CNA-M is on the Registry and has not been annotated. Facilities may not employ a CNA or CNA-M who is not on the Registry, or who has been annotated for abuse, neglect or misappropriation of patient/client/resident funds in a health care setting. Further changes are pending that would expand the types of individuals for whom the registry must be checked and who may not be employed if there is a positive finding.
Monitoring
The department is authorized to make regular and unannounced inspections of all facilities. The regulations specify the grounds for imposition of intermediate sanctions and the method of calculating penalties. The State ombudsman program is authorized to visit facilities and receive and investigate complaints.
Fees
Chapter 1664 sets fees of $10 per bed for residential care facilities and $200 for assisted living programs.
Maryland
Citation
Assisted living programs Title 10.07.14
General Approach and Recent Developments
The opening section of the rules state that the purpose of the chapter is to set minimum, reasonable standards for licensure of assisted living programs that are intended to maximize independence and promote the principles of individuality, personal dignity, freedom of choice, and fairness for all individuals residing in assisted living programs.
Assisted living program rules were revised in 2002 to clarify medication administration requirements and to add disclosure provisions for facilities serving residents with Alzheimer’s disease. The HCBS waiver has been expanded to include all assisted living facilities.
Legislation passed in 2004 requiring an 80-hour training course for managers. The curriculum is being drafted by the licensing agency.
The uniform assessment tool was revised in 2003. The previous tool did not adequately assess and determine a level of care for people with behavior problems and dementia. As a result, more residents are likely to be assigned to level three.
A workgroup was formed in 2003 to initiate a thorough review of the regulations and current trends. A preliminary report was submitted to the legislature in 2003. The workgroup will continue to meet and submit recommendations to the legislature in the fall of 2004. A major focus of the workgroup is the definition of assisted living which currently requires that people caring for one person to be licensed. The group is considering setting a minimum number of people served and setting different requirements for small and larger programs. The group is likely to recommend requiring awake overnight staff and nursing oversight in homes serving more than 17 residents.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted living programs | 1,248 | 17,148 | 2,000 | 14,273 | 2,500 | NR |
| * 2000 and 2002 reports were based on estimates as the State converted from its previous regulatory structure to one that consolidated difference. | ||||||
Definition
An assisted living program is “a residential or facility-based program that provides housing and supportive services, supervision, personalized assistance, health related services, or a combination thereof to meet the needs of residents who are unable to perform, or who need assistance in performing, the activities of daily living or instrumental activities of daily living in a way that promotes optimum dignity and independence for the residents.” The term “assisted living program” may not be used in advertising unless the facility is licensed.
Unit Requirements
Programs licensed after the effective date of the regulations must provide a minimum of 80 square feet of functional space for single occupancy and 120 square feet for double occupancy rooms. No more than two residents may share a room. Facilities previously licensed as domiciliary care homes must provide a minimum of 70 and 120 square feet for single and double occupancy, respectively. Buildings with one to eight occupants must have one toilet for every four occupants and larger buildings must also have at least one toilet on each floor. Showers/baths must be available for every eight occupants.
Admission/Retention Policy
Facilities are licensed by the level of impairment of residents. Residents are assigned to a level based on an assessment score. The assessment includes 12 questions that cover medical illnesses/conditions and additional questions covering cognitive and psychiatric conditions, treatment requirements, medication management, ADL assistance, risk factor management, and management of problematic behaviors.
In general, programs may not serve anyone who, at the time of admission, requires more than intermittent nursing care; treatment of Stage III or IV skin ulcers; ventilator services; skilled monitoring, testing, and aggressive adjustment of medications and treatments where there is the presence of, or risk for, a fluctuating acute condition; monitoring of a chronic medical condition that is not controllable through readily available medications and treatments; treatment for an active reportable communicable disease; or treatment for a disease or condition which requires more than contact isolation. Residents may not be admitted if they are a danger to self or others and the danger cannot be eliminated through appropriate treatment modalities or if they are at risk for health or safety complications which cannot be adequately managed.
A program may request a waiver to care for residents with needs that exceed the licensure level. It must demonstrate that it can meet the resident’s needs and others will not be jeopardized.
Waivers for Level I and Level II programs may not be granted for more than 50 percent of the licensed bed capacity. Level III programs may not receive waivers for more than 20 percent of capacity or 20 beds, whichever is less.
Nursing Home Admission Policy
Nursing home care is covered when an individual requires health related services provided on a daily basis by or under the supervision of a nurse due to medical, cognitive or physical disability. The need for intermittent, part-time services does not qualify (for example home health nursing), nor does the need for unlicensed care (e.g., personal care) even if care is needed full time. There is some overlap in how the term intermittent nursing care is applied under the licensing and Medicaid level of care policies.
Services
Before move-in, the assisted living manager determines whether the resident may be admitted and whether the resident’s needs can be met by the program based on an assessment and an examination by a health care professional. A functional assessment is completed within 30 days of admission that includes: level of functioning in activities of daily living; level of support and intervention needed, including any special equipment and supplies required to compensate for the individual’s deficits in activities of daily living; current physical or psychological symptoms requiring monitoring, support, or other intervention by the assisted living program; capacity for making personal and health care-related decisions; presence of disruptive behaviors, or behaviors which present a risk to the health and safety of the resident or others; and specified social factors.
Services include three meals in a common dining area, special diets, personal care, laundry, housekeeping, social and spiritual activities, and medication management. The program must facilitate access to health care and social services (social work, rehabilitation, home health, skilled nursing, physician services, oral health, counseling, psychiatric care, and others).
Dietary
Three meals a day and snacks that are well-balanced, palatable, varied, properly prepared, and of sufficient quantity and quality to meet daily nutritional needs are required. As part of the licensing process, facilities submit a 4-week menu cycle with documentation by a licensed nutritionist or licensed dietician that the menus are nutritionally adequate. Special diets as ordered by a physician or needed by the resident must be provided.
Agreements
Agreements must include a clear and complete reflection of commitments and actual practices and a recommendation for review by an attorney. The agreement includes: the level of care for which the facility is licensed; the level of care needed by the resident; a statement that describes that a resident may be discharged if the level of care increases and a waiver is not approved; a list of services provided and not provided; complaint/grievance procedure; occupancy provisions (room assignment, relocation, change in roommate, transfer policy, availability of locks for storage); the staff’s right to enter a room (if any); resident rights; bed hold policy; admission and discharge policy; obligations of all parties for arranging for and overseeing medical care and monitoring health status.
The agreements must also include financial information that includes: obligations for payment; handling finances; purchase of rental equipment; arranging and contracting for services not provided by the facility; durable medical equipment; and disposition of resident property upon discharge or death. Also included are the rate structure for the service package, fee-for-service rates; notification of changes; third-party payments; person responsible for payment; procedures if the resident is no longer able to pay; and terms governing refunds. If the resident’s needs change significantly, the agreement must be amended.
Provisions for Serving People with Dementia
Programs with an Alzheimer’s special care unit or program must complete the department’s disclosure form that describes: a statement of philosophy or mission; staff training and staff job titles, including the number of hours of dementia-specific training provided annually for all staff by job classification and a summary of training content; admission procedures, including screening criteria; assessment and care planning protocol, including criteria to be used that would trigger a reassessment of the resident’s status before the customary 6-month review; staffing patterns, including the ratio of direct care staff to resident for a 24-hour cycle, and a description of how the staffing pattern differs from that of the rest of the program; a description of the physical environment and any unique design features appropriate to support the functioning of cognitively impaired individuals; a description of activities, including frequency and type, how the activities meet the needs of residents with dementia, and how the activities differ from activities for residents in other parts of the program; the program’s fee or fee structure for services provided by the Alzheimer’s special care unit or program as part of the disclosure form that is required in §E(1) of this regulation; discharge criteria and procedures; and any services, training, or other procedures that are over and above those that are provided in the existing assisted living program.
Medication Administration
Aides who have passed required training may administer medications. Untrained aides may assist with self-administration. Management must arrange for quarterly, on-site reviews of medications by a registered nurse, authorized prescriber, or licensed pharmacist for each resident who self-administers medications.
Public Financing
The State administers an HCBS waiver and a state funded program that serves beneficiaries age 50 and older in residential settings. A waiver amendment included assisted living services as part of a broad package of services available to people 50 years of age or older in their own or in residential settings. Amendments to the waiver raised eligibility to 300 percent of the federal SSI benefit. Room and board, paid by the resident, is capped at $420 a month. Medicaid pays the lesser of the provider’s usual and customary charge or $1,602.75 a month for Assisted Living Level II services and $2,021.75 for Level III services. The Level I licensing level of care does not qualify for the Medicaid waiver. Non-SSI beneficiaries are allowed a personal needs allowance of $60 and all additional income is applied to the cost of care. SSI beneficiaries retain SSI benefits above the amount paid for rent and do not pay toward the cost of services. The Medicaid waiver program served 1,473 beneficiaries in 763 facilities in 2004, up from 730 beneficiaries in 362 facilities in 2002.
| 2004 | 2002 | 2000 | ||||
|---|---|---|---|---|---|---|
| Facilities | Participation | Facilities | Participation | Facilities | Participation | |
| Medicaid | 763 | 1,473 | 362 | 730 | 132 | 135 |
| State | NR | 350 | 259 | 520 | NR | NR |
Additional payments are available for assistive equipment and environmental modifications. Medicaid will pay the actual costs and payment is capped at $1,000 per participant for 12 months. Medicaid will pay 67 percent of the costs of environmental modifications (the provider pays 33 percent), up to a maximum of $3,000 per participant. Exceptions to the maximum are allowed at the discretion of the Department on Aging.
The state-subsidized Senior Assisted Housing program served 350 participants in 2004. Participants with incomes no greater than 60 percent of the statewide median income and assets no greater than $11,000 apply their income (less a $60 needs allowance) toward the cost of care. State-funded subsidies may cover the difference between the participant’s contribution and the monthly fee, up to a maximum of $550 a month.
The law directs the Office of Aging to develop assisted living programs in conjunction with public or private, profit or nonprofit entities, maximizing the use of rent and other subsidies available from federal and state sources. These activities can include finding sponsors; assisting developers formulating design concepts and meeting program needs; providing subsidies for congregate meals, housekeeping and personal services; developing eligibility requirements in connection with the subsidies; adopting regulations governing eligibility; and reviewing compliance with relevant regulations.
| Level II | Level III | |
|---|---|---|
| Services | $1,610.66 | $2,030.86 |
| Room and board | $420 | $420 |
| Total | $2,031.66 | $2,451.86 |
| Assistive equipment add on | up to $1,000 | up to $1,000 |
| Environmental modification | up to $3,000 | up to $3,000 |
| NOTE: Rates reflect a .5% increase effective July 1, 2004. | ||
Staffing
Based on the number of residents to be served and their needs, the facility develops a staffing plan that identifies the type and number of staff needed to provide the services required. The staffing plan includes on-site staff sufficient in number and qualifications to meet the 24-hour scheduled and unscheduled needs of the residents. A staff member must be present when a resident is in the facility.
Programs must have staff capacity to deliver the care for which they are licensed (see table below). Facilities contracting with Medicaid must have one staff member for every eight residents during daytime hours.
Training
Administrators. Assisted living managers must have adequate knowledge of the health and psycho-social needs of the population served; resident assessment process; use of service plans; cuing, coaching and monitoring residents who self-administer medications with and without assistance; providing assistance with ambulation, personal hygiene, dressing, toileting, and feeding; residents’ rights; fire and life safety; infection control; basic food safety; basic first aid; basic CPR; emergency disaster plans; and individual job requirements of all staff.
Staff must participate in an orientation and ongoing training program to ensure that residents receive services that are consistent with their needs and generally accepted standards of care for the specific conditions of those residents to whom staff will provide services. Staff must receive initial and on-going training in: fire and life safety; infection control, including standard precautions; basic food safety; basic first aid; emergency disaster plans; and individual job requirements as appropriate to their job.
Staff must have knowledge in: health and psycho-social needs of the population served as appropriate to their job responsibilities; resident assessment process; use of service plans; and resident rights.
If job duties involve the provision of personal care services, staff must have knowledge in cuing, coaching, and providing assistance with ADLs.
Facilities participating in the Medicaid waiver: staff must complete an 8-hour training on medication administration and pass a performance test.
Background Check
Applicants must document any felony conviction of the applicant, assisted living manager, or household member (in small, owner-occupied facilities). Management must conduct either a criminal history records check or a criminal background check consistent with §19-1901 et seq. Annotated Code of Maryland.
Monitoring
Under the law, the Department of Health and Mental Hygiene may delegate monitoring and inspection of programs to the Office on Aging and the Department of Human Resources or to local health departments through an interagency agreement. Survey findings and plans of correction must be posted in the facility.
Fees
$25 a year for programs monitored by the Department of Human Resources or the Department on Aging; $100 a year for programs inspected and monitored by the Department of Health and Mental Hygiene. Programs with 16 beds or more pay $100 a year plus $6 for each bed over 15.
| Area | Level I-- Low (0-25) |
Level II-- Moderate (26-60) |
Level III-- High (61+) |
|---|---|---|---|
| Health and wellness | Ability to recognize the cause and risks associated with a resident’s health condition once these factors are identified by a health care professional. Provide occasional assistance in accessing and coordinating health services and interventions. | Ability to recognize and accurately describe and define a resident’s health condition and identify likely causes and risks associated with the resident’s condition. Provide or ensure access to necessary health services and interventions | Ability to recognize and accurately describe and define a resident’s health condition and identify likely causes and risks associated with the resident’s condition. Provide or ensure ongoing access to coordination of comprehensive health services and interventions |
| Functional | Provide occasional supervision, assistance, support, set up, or reminders with some but not all ADLs. | Provide or ensure substantial support with some, but not all, ADLs or minimal supports with any number of ADLs. | Provide or ensure comprehensive support as frequently as needed to compensate for any number of ADLs. |
| Medication and treatment | Ability to assist with self-administration of medications or coordinate access to necessary medications and treatments. | Provide or ensure assistance with self-administration of medications or administer necessary medications and treatments, including monitoring their effects. | Provide or ensure assistance with self-administration of medications or administer necessary medications and treatments, including monitoring or arranging for monitoring the effects of complex medication and treatment regimens. |
| Behavioral | Monitor and provide uncomplicated intervention to manage occasional behaviors that are likely to disrupt or harm the resident or others. | Monitor and provide or ensure intervention to manage frequent behaviors which are likely to disrupt or harm the resident or others. | Monitor and provide or ensure ongoing therapeutic intervention or intensive supervision to manage chronic behaviors which are likely to disrupt or harm the resident or others. |
| Psychological | Monitor and manage occasional psychological episodes or fluctuations that require uncomplicated intervention or support. | Monitor and manage frequent psychological episodes or fluctuations that may require limited skilled interpretation or prompt intervention or support. | Monitor and manage a variety of psychological episodes involving active symptoms, condition changes, or significant risks that may require some skilled interpretation or immediate interventions. |
| Social and recreational | Occasional assistance in accessing social and recreational services | Ability to provide or ensure ongoing assistance in accessing social and recreational services. | Provide or ensure ongoing access to comprehensive social and recreational services. |
Massachusetts
Citation
Assisted living: 651 CMR 12.00 et seq.
General Approach and Recent Developments
Chapter 354 (Acts of 1994) created a certification process for assisted living facilities by the Executive Office of Elder Affairs. The law provides that the regulations “shall be sufficiently flexible to allow assisted living residences to adopt policies and methods of operation which enable residents to age-in-place.” To be certified, residences must submit information such as the number of units and number of residents per unit, location of units, common spaces, and egress by floor; base fees to be charged; services to be offered and arrangement for delivering care; number of staff to be employed; and other information required by the Executive Office of Elder Affairs. The buildings are considered residential use for applying appropriate building codes.
Revisions to the regulations were final in December 2002. The State initiated a major review of the assisted living statute and regulations during summer 2004. The review will examine the experience in other states with particular attention to quality, the quality improvement process, and how quality can be woven into the regulations.
The Governor announced a new initiative, “Helping Our Massachusetts Elders” (HOME) that will provide alternatives to nursing home care. This new initiative creates an interagency task force of government agencies and establishes a $4 million trust fund as part of the state supplemental budget to support programs that allow elders to remain in home and community-based settings and supports a voluntary managed care program that emphasizes preventative care. Elder Affairs believes this new initiative will have a significant impact on assisted living and other residential alternatives in the State. The request for funding is pending.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted living residences | 171 | 10,585 | 139 | 9,796 | 139 | 8,200 |
Definition
Assisted living residence is any entity, however organized, whether conducted for profit or not for profit, which meets all of the following criteria:
Provides room and board; provides, directly by employees of the entity or through arrangements with another organization which the entity may or may not control or own, assistance with activities of daily living for three or more adult residents who are not related by consanguinity of affinity to their care provider; and collects payments or third-party reimbursements from or on behalf of residents to pay for the provision of assistance with the activities of daily living.
Unit Requirements
Units must be single or double occupancy with lockable doors. New construction must provide for private baths. Existing buildings may qualify if they provide private half baths and one bathing facility for every three persons. All facilities must provide, at a minimum, either a kitchenette or access to cooking capacity for all living units. Cooking capacity is defined as each resident having access to a refrigerator, sink, and heating element. Facilities must comply with all federal and state laws and regulations regarding sanitation, fire safety, and access by persons with disabilities. The Secretary of Elder Affairs is authorized to waive the requirements for bathrooms and bathing facilities when determined to meet public necessity and to prevent undue economic hardship as long as the residence provides a home-like environment and promotes privacy, dignity, choice, individuality, and independence.
Admission/Retention Policy
The statute does not allow people needing 24-hour skilled nursing supervision to be admitted or retained in an assisted living residence. Facilities may admit and retain residents in need of skilled nursing care only if the care will be provided by a certified provider of ancillary health services or by a licensed hospice, and the provider does not train the residence staff to provide skilled nursing care.
To qualify for reimbursement under the Medicaid Group Adult Foster Care program, tenants must require daily assistance with at least one ADL and assistance with managing medications as documented by a physician and a nursing assessment; be at risk of requiring nursing home placement; be chronically disabled; and require 24-hour supervision.
Nursing Home Admission Policy
Individuals must need one skilled service daily from a specified list or have a medical or mental condition requiring a combination of at least three services including at least one nursing service. The nursing services that must be performed at least 3 days a week include: specified physician ordered skilled services; positioning while in bed or chair; measurement of intake or output based on medical necessity; administration of oral or injectable medications that require a registered nurse to monitor the dosage, frequency, or adverse reactions; staff intervention requirements for selected types of behavior considered dependent or disruptive, unable to avoid simple dangers, wandering; physician ordered occupational, speech, or physical therapy; nursing observation and/or vital signs monitoring; or treatment involving prescription medication for uninfected post-operative or chronic conditions or routine dressing changes that require nursing care and monitoring. Two services may be required for assistance with bathing (direct care, attendance or constant supervision), dressing (direct care, attendance or constant supervision), toileting, bladder or bowel control for incontinence, scheduled assistance, or routine catheter/ostomy care, transfers, mobility/ambulation or eating.
Services
Chapter 354 requires that residences provide or arrange for opportunities for socialization and access to community resources; supervision or assistance with ADLs identified in a service plan (at a minimum residences must offer support for bathing, dressing, and ambulation); instrumental activities of daily living; self-administered medication management; timely assistance to urgent or emergency needs by 24-hour per day on-site staff, personal emergency response systems, or any additional response systems required by the Executive Office of Elder Affairs; up to three regularly scheduled meals per day (minimum of one meal per day). The administrator may arrange for the provision of ancillary health services in the residence but may not use residence staff for these services unless the staff is an employee of a certified provider of ancillary health services and/or an employee of a licensed hospice. Nursing services provided by a certified provider of ancillary health services such as injection of insulin or other drugs used routinely for maintenance therapy of a disease may be provided to residents.
Twenty-four hour nursing services are not allowed. Skilled services may only be provided by a certified home health agency on a part-time or intermittent basis. Medical conditions requiring services on a periodic, scheduled basis are also allowed. In addition, residents may “engage or contract with any licensed health care professional and providers to obtain necessary health care services…to the same extent available to persons residing in private homes.”
All residents must have an individual services plan that is developed prior to admission and reviewed/reassessed at least every 6 months or when health status or family circumstances change. The plan is based on information from the resident, family members and the physician, including diagnosis, medications, allergies and dietary needs. It includes the services needed based on physical, cognitive, and social needs and behavioral concerns as well how the residence will provide for 24-hour staffing. If provided by the residence, the plan describes the type of assistance with medication that will be provided.
Dietary
A minimum of one meal a day must be provided (facilities may provide three meals a day). Menus for assisted living residences should meet the current Dietary Reference Intake (DRI) established by the Food and Nutrition Board, Institute of Medicine, National Academy of Sciences (NAS), and the Dietary Guidelines for Americans (DG) published by the Secretaries of Health and Human Services and Agriculture. At a minimum, these dietary plans must allow a resident to adhere to sodium-restricted, sugar-restricted, and low-fat diets. The residence’s menus or meal plans shall be evaluated at least every 6 months by a qualified dietician. Residences must disclose to residents and prospective residents the types of special diets they can accommodate and any additional costs associated with providing this service as well as limitations on addressing food allergies. Dietary needs must be reviewed every 6 months and included in the resident service plan. The residence is not responsible for ensuring that the resident follows the diet plan but must provide enough food choices and information so that the resident can adhere to the diet if he or she chooses.
Staff managing dietary services must complete a food service sanitation certification course. Therapeutic diets must be reviewed by a qualified dietician and evaluated every 6 months unless otherwise specified by a physician.
Agreements
Resident agreements include: charges, expenses, and other assessments for resident services; personal care services; lodging and meals; resident’s agreement to make payment; arrangements for payment; grievance procedure and the right to contact the ombudsman; sponsor’s covenant to comply with applicable federal and state laws; provisions for terminating the agreement; reasonable rules for staff, management, and resident behavior; and a copy of the residents rights. Additionally, it must include the specific unit number in which the resident will reside; a signature of parties, term of agreement; liability (the residence may not require a resident to maintain liability insurance); a right to privacy; and a right to contract with outside providers.
A Disclosure of Rights and Services (disclosure statement) shall be delivered to a prospective resident at the time of or prior to the execution of the residency agreement, or at the time of or prior to the transfer of any money to a sponsor by or on behalf of a prospective resident. The disclosure statement is required to be issued only once, and is required to be delivered as an independent document. Included in this disclosure is the grievance procedure; an explanation of any limitations on services; a description of the role of the nurse; policy concerning self-administration and limited administration of medications; rules of conduct for staff, management and residents; provisions of the resident agreements; and nursing and personal care worker staffing levels by shift.
Provisions for Serving People with Dementia
The service plan includes how the specialized needs of resident with dementia shall be addressed, including the provision of 24-hour awake staff. The staff orientation program includes training in dementia and cognitive impairment. New rules require that 1 hour of ongoing training annually cover dementia/cognitive impairment topics.
Medication Administration
When assisting a resident to self-administer medication the individual performing self-administered medication management (SAMM) must:
- Remind resident to take medication;
- Check the package to ensure that the name on the package is that of the resident;
- Observe the resident while they take the medication; and
- Document in writing the observation of the resident’s actions regarding the medication.
The individual performing SAMM may open prepackaged medications and/or opened bottles, read the name of the medications and directions to the resident and respond to questions the resident may have concerning the directions on the label. The residence may assist a resident with SAMM from a medication container that has been removed from its original pharmacy-labeled packaging or container by another person, however if this service is performed, full written disclosure of the risks involved and consent by the resident or legal representative shall be provided. SAMM shall only be performed by an individual who has completed personal care service training. Central storage of resident medications (the storage of medication in an area outside of the resident’s unit) is prohibited in an assisted living residence.
Limited Medication Administration (LMA) is an optional service. Assisted living residences must disclose the availability of this service and the cost in the residency agreement and/or Disclosure of Rights and Services. Limited Medication Administration may only be provided in assisted living residences by a family member or by a practitioner or a nurse registered or licensed under state law. Nurses may administer non-injectible medications to residents. Limited medication administration requires detailed documentation including the resident’s service plan. All medication must be kept in the resident’s unit.
Public Financing
Services for eligible low-income tenants in residences that contract with Medicaid are subsidized through the Group Adult Foster Care (GAFC) program. GAFC is a service available under the “state plan” rather than a Medicaid waiver. The program serves adults over age 22 who have a physician’s authorization confirming they are at risk of entering an institution. Participants must have at least one ADL impairment. GAFC is available in assisted living residences and conventional elderly housing.
GAFC provides an average of $37.75 per day for services and administrative costs. Participants receive assistance with ADLs and IADL; a multidisciplinary care team; access to 24-hour scheduled and unscheduled care; and minimum professional staffing of 3.5 hours per week per resident. The rate assumes participants receive one hour of personal care a day. In addition to GAFC services, participants may also receive up to 2 days of adult day health services or 8 hours of home health aide services with prior approval.
To support low-income residents who do not have sufficient income to pay for room and board, the State has created a special SSI living arrangement for assisted living residences. The SSI payment standard is $1,018 a month for a single individual. In January 2003, the program contracted with 141 GAFC providers and served 3,110. Of this number, 101 providers were assisted living residences and they served 1,120 residents.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participation | Facilities | Participation | Facilities | Participation |
| 101 | 1,120 | 44 | 922 | 74 | 547 |
Staffing
No staffing specific guidelines are included concerning the type and number of staff. However, the residence must maintain an ability to provide timely assistance to residents and to respond to urgent or emergency needs through on-site staffing, personal emergency response, or other means.
Training
Administrators. The manager of an assisted living residence must be at least 21 years old and have demonstrated administrative experience. The manager must have a Bachelor’s degree or equivalent experience in human services management, housing management, and/or nursing home management. The service coordinator of a residence must have a minimum of 2 years of experience working with elders or disabled individuals and a Bachelor’s degree or equivalent experience.
Staff. Prior to active employment, all staff and contracted workers having direct contact with residents and all food service personnel must receive a 7-hour (up from six) orientation covering the following topics:
- Philosophy of independent living in an ALR;
- Resident bill of rights;
- Elder abuse, neglect, and financial exploitation;
- Communicable diseases;
- Communication skills;
- Review of the aging process;
- Dementia/cognitive impairment including a basic overview of the disease process, communication skills, and behavior management;
- Resident health and related problems;
- Job requirements;
- Self-administered medication management; and
- Sanitation and food safety.
The ongoing training requirement was raised from 5 to 10 hours per year for all employees.
All employees and providers shall receive ongoing in-service education and on-the-job training aimed at reinforcing the initial training. ALR staff and contracted providers of personal care services must complete an additional 54 hours of training prior to providing personal care services to a resident (34 hours general training and 20 hours of training specific to the provision of personal care). The 20 hours of personal care training must be conducted by a qualified registered nurse with a valid Massachusetts license. The 54 hours of training include, but are not limited to, the following topics:
- Personal hygiene;
- Self-administration of medications;
- Elimination;
- Nutrition;
- Human growth and development;
- Family dynamics;
- Grief, loss, death and dying;
- Mobility;
- Maintenance of a clean, safe, and healthy environment;
- Home safety; and
- Assistance with appliances.
Background Check
Applicants must assure that none of its officers, directors, trustees, limited partners, or shareholders has ever been found in violation of any local, state, or federal statute, regulation, ordinance, or other law by reasons of the individual’s relationship to an assisted living residence.
No person working in an assisted living residence may have been convicted of a felony.
Monitoring
The Executive Office of Elder Affairs conducts compliance reviews of assisted living residences every two years. The reviews include inspections of the common areas, living quarters (by consent of the resident), inspection of the service plans, and a review of the resident satisfaction survey. Compliance reviews may be initiated at any time with probable cause.
The State sees their oversight process as consultative. This is not applied uniformly, however. This process is more a result of assisted living residences contacting the State for assistance.
During a compliance review, state staff will address issues of concern during a debriefing meeting with the administrator. The State will write a letter with the findings from the review and a request for a corrective action plan. Most frequently this relates to rewriting a policy or retraining staff. Medication issues are also common. The assisted living residence must submit documentation that corrective actions have occurred. If the State determines that the compliance review requires more intensive action (severity of problem, number of residents affected, willingness of assisted living residence to address problem) they will do a follow-up visit. In many cases, the State is citing the same issues on repeat visits or compliance reviews.
The State ombudsman program may require other corrective action and become more involved at the resident level.
Fees
Fees are set by the Secretary of Administration and Finance based on the number of units. The current application fee is $200. Residences pay a certification of $125 per unit every 2 years.
Michigan
Citation
Homes for the aged: Michigan Comp. Law §333.20106(3); 333.21301 et seq.; Michigan administrative code R.325.1801 et seq.
Adult foster care: 400.701 et seq.
Adult foster care: Family homes (6 or less residents) R400.1401 et seq.
Adult foster care: Small group homes R400.14101
Adult foster care: Large group homes R400.15101 et seq.
General Approach and Recent Developments
The State licenses several types and levels of residential care and work continues on updating rules for homes for the aged. A public hearing was held in November 2003. Modifications were based on testimony received during public hearings. Recommended changes were submitted to a legislative committee for review and approval before they are promulgated. House Bill H4322, enacted in 2001, requires coverage of assisted living by long-term-care insurance policies. There has been a prohibition of new adult foster homes-congregate homes since the 1980s. There are only 13 adult foster care facilities remaining across the State that are licensed for 20+ residents. The trend in Michigan is away from large institutional-like settings.
Medicaid personal care coverage is available to beneficiaries in adult foster care and homes for the aged. Waiver services are available to beneficiaries living in housing that may be operated as an unlicensed facility, that is, a facility or building that does not provide personal care services and therefore not required to be licensed. Since these unlicensed settings are considered a person’s home, services can be received from providers of one’s choice.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Adult foster care--family homes | 1,247 | 5,825 | 4,353 | 33,317 | 1,361 | 6,271 |
| Adult foster care--small group homes | 2,527 | 17,610 | 1,904 | 10,760 | ||
| Adult foster care--large group homes | 485 | 9,001 | 454 | 8,380 | ||
| Adult foster care--congregate homes | 13 | 491 | NR | NR | NR | NR |
| Homes for the aged | 190 | 14,588 | 188 | 14,500 | NR | NR |
Definition
Homes for the aged means a supervised personal care facility, other than a hotel, adult foster care facility, hospital, nursing home, or county medical care facility, that provides room, board, and supervised personal care to 21 or more unrelated, nontransient individuals 60 years of age or older. Home for the aged includes a supervised personal care facility for 20 or fewer individuals 60 years of age or older if the facility is operated in conjunction with and as a distinct part of a licensed nursing home.
Adult foster homes. There are four levels of adult foster homes:
- Adult foster care family homes serve 6 or fewer residents and the licensee must reside in the home;
- Adult foster care small group homes serve between 1 and 12 residents;
- Adult foster care large group homes serve between 13 and 20 residents; and
- Adult foster care congregate care homes serve 21 or more residents.
An adult foster care facility is a governmental or non-governmental establishment that provides foster care to adults. Adult foster care facilities include small and large group homes, adult foster care family homes and congregate homes that serve residents who are aged, mentally ill, developmentally disabled, or physically handicapped and require supervision on an ongoing basis but who do not require continuous nursing care. Adult foster homes in good compliance may apply for a certification for specialized programs for the mentally ill, developmentally disabled, or both populations. This certification is required in order to contract with community mental health agencies.
Unit Requirements
Homes for the aged. Homes constructed, converted or expanded after 1981 must provide 100 square feet of usable space for single rooms and 80 square feet per resident in shared rooms. Rooms may not be shared by more than four people. Homes licensed prior to 1981 must offer at least 80 square feet of usable floor space for single rooms while shared rooms must provide 70 square feet per resident. The regulations do not limit the number of residents that may share a room if licensed prior to 1981. Toilet facilities are required for every eight residents per floor and bathing facilities for every 15 residents.
Adult foster homes. A single bedroom must have at least 80 square feet of usable floor space; a multi-bed room must have at least 65 square feet of usable floor space per bed. A maximum of two beds are allowed per bedroom unless the facility has been continuously licensed since the effective date of the rules and unless the resident (or the resident’s representative) has agreed to reside in the multi-occupancy room, the home is in compliance with all state fire safety and environmental standards, and the bedroom provides no less than 70 square feet (65 square feet for homes licensed on or before December 31, 1976) of usable floor space per bed.
Admission/Retention Policy
Homes for the aged. Residents requiring nursing care cannot be admitted. After admission, residents requiring 24-hour nursing care or intensive nursing care may not be retained. However, an amendment to the statute in 2002 allows for the retention of residents whose condition changes after moving into the home, with the approval of the resident, resident’s family, resident’s physician, and the facility’s governing board, as long as the facility assures the care the resident needs can be provided. Physicians must certify that new residents are free from communicable diseases. Residents with a mental condition disturbing to others may not be admitted or retained.
Adult foster homes may not accept, retain, or care for residents who require continuous nursing care. This does not preclude the accommodation of a resident who becomes temporarily ill while in the home but does not require continuous nursing care, or a resident who becomes a patient of a licensed hospice program. All residents must be assessed by the facility to determine the amount and type of services required by the resident are available at the facility. Facilities may not accept or retain residents who require isolation or restraint.
Nursing Home Admission Policy
The criteria were revised in 2004. The state has adopted a system that uses seven “doors” to eligibility (see table).
Services
Homes for the aged provide necessary assistance with personal care, including care of the skin, mouth and teeth, hands and feet, and the shampooing and grooming of hair. The rules require that residents wash their hands before meals and receive a bath or shower at least once a week.
Services in adult foster homes include supervision, protection, personal care, medication administration, social activities, and assistance with activities of daily living. Homes must arrange for transportation services.
For adult foster care homes, personal care means personal assistance provided by a licensee or an agent or employee of a licensee to a resident who requires assistance with dressing, personal hygiene, grooming, maintenance of medication schedule as directed and supervised by the resident’s physician, or the development of those personal and social skills required to live in the least restricted environment.
| Door | Areas Scored | Threshold |
|---|---|---|
| 1. ADLs | (A) Bed mobility, transfers, toilet use and (B) eating |
Score of 6: (A) independent or supervision, 1; limited assistance, 3; extensive or total, 4; did not occur, 8. (B) independent/supervision, 1; limited assistance, 2; extensive or total, 3; did not occur, 8 |
| 2. Cognitive performance | Short-term memory, cognitive skills for daily decision making, communication | Must have severely impaired decision making, memory problems and moderate or severely impaired decision making, or memory problem and sometimes or rarely understood |
| 3. Physician involvement | Under care for an unstable medical condition | Based on frequency of physician visits and orders |
| 4. Treatments and conditions | Stage 3-4 pressure sores; intravenous or parenteral feedings; intravenous medications; end-stage care; daily trach care, respiratory care, or suctioning; pneumonia; daily oxygen therapy; daily insulin with two order changes in past 14 days; peritoneal or hemodialysis | At least one of nine conditions |
| 5. Skilled rehabilitation therapies | Speech, occupational, or physical therapy | Requires at least 45 minutes of active therapy in last 7 days and continues to require therapy |
| 6. Behavior | Wandering, physical/verbal abuse, socially inappropriate/disruptive, resists care, delusions/hallucinations | Either has delusions/hallucinations or exhibits other behaviors at least 4 of last 7 days |
| 7. Service dependency | Currently receiving services in a NF or waiver program | Must be a participant for 1 year |
Dietary
Adult foster care. Administrators and/or licensees must have competency in nutrition. Homes serving seven or more residents must have a specific staff person who is experienced in food preparation by education or experience. Three nutritious meals must be provided according to the recommended daily allowances contained in the Basic Nutrition Facts: A Nutrition Reference published by the Michigan Department of Health. Special diets must be provided when prescribed by a physician.
Homes for the aged. Three meals a day and snacks that meet the recommended dietary allowances are required. Fluid, supplementary nourishments and special diets ordered by a physician must be provided.
Agreements
Adult foster care. The agreement includes: assurance of the provision of care, supervision, and protection; description of the services provided and the fee; costs in addition to the basic fee; description of the transportation services provided and the fee; agreement by the resident/family to provide necessary intake information; agreement to provide a current health care appraisal; agreement to follow house rules; to respect and safeguard resident’s rights and to provide a written copy; discharge policy and procedures; refund policy; statement of how funds and valuables are handled; and a statement that the home is licensed to provide care.
Homes for the aged. Not specified.
Provisions for Serving People with Dementia
Regulations cover admission-retention and staff training. Facilities serving people with dementia must disclose the services that are available.
Medication Administration
Trained aides may administer medications.
Public Financing
Medicaid personal care coverage has been available since 1983 through the state plan. Over time, the number of licensed adult foster home facilities serving Medicaid beneficiaries has dropped from 80 percent to 20 percent, due both to the rise in the number of private pay only facilities and the payment rate compared to private rates which may not be supplemented. Personal care services are provided to approximately 14,138 residents living in adult homes for the aged and adult foster care. Adult foster homes receive $174.38 a month in Medicaid personal care funds. Adult foster care residents receive $721.50 from SSI and the state supplementfrom which $44 a month personal needs allowance is paid to the facility. Homes for the aged residents receive $743.30 from SSI and the state supplement, from which $44 a month personal needs allowance is paid to the facility.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participation | Facilities | Participation | Facilities | Participation |
| NA | 14,138 | NA | 13,000 | NR | NR |
Eligible beneficiaries may receive Medicaid waiver services in unlicensed assisted living facilities and elderly housing buildings. Participation data is not tracked separately for persons in unlicensed facilities.
Staffing
Homes for the aged. The governing body shall appoint a competent administrator and shall delegate the responsibility for operating the home. An administrator and all other persons in supervisory positions shall be at least 21 years of age. An administrator designates a competent person at least 21 years old to carry out the responsibilities and duties of the administrator in his or her absence. A sufficient number of attendants are required for each shift to assist residents with personal care under direction from a supervisor.
Adult foster homes. The ratio of direct care staff in facilities housing between 13 and 20 residents must be no less than one staff to 15 residents during waking hours and one staff to 20 residents during normal sleeping hours. The ratio for facilities for 12 or fewer residents must be no less than one staff per 12 residents. In all facilities, there must be sufficient direct care staff on duty at all times for the supervision, personal care, and protection of residents and to provide the services specified in the resident’s care agreement and assessment plan. Direct care staff must be at least 18 years old.
Training
Homes for the aged. A licensee or administrator shall provide in-service training or make training available through other sources to direct care staff. Direct care staff shall be competent before performing assigned tasks.
In adult foster homes, administrators must have at least one year of experience working with persons who are mentally ill, developmentally disabled, physically handicapped, or aged. Both the licensee of the home and the administrator must complete either 16 hours of training approved by the Michigan Family Independence Agency or 6 credit hours at an accredited college or university in content areas that are relevant to the licensee’s admission policy and program statements as approved by the Family Independence Agency. The licensee or administrator must provide in-service training or make training available through other sources for direct care staff in the following areas: reporting requirements, first aid, CPR, personal care, supervision, protection, resident rights, safety and fire prevention, and prevention and containment of communicable disease.
Adult foster homes (large group homes). Before a license is issued, an applicant and an administrator shall be competent in all of the following areas: nutrition; first aid; CPR; foster care; safety and fire prevention; financial and administrative management; needs of the population to be served; resident rights; and prevention and containment of communicable diseases. Direct care staff shall be competent before performing assigned tasks which shall include being competent in all of the areas detailed above for adult foster homes. A licensee, administrator, or direct care staff must be trained in the proper handling and administration of medication before supervising the taking of medication by a resident.
Background Check
Homes for the aged. As of September 2002, shall not employ, independently contract with, or grant clinical privileges to an individual who regularly provides direct services to patients or residents in a facility who has been convicted of a felony, and a list of other crimes. Each facility must conduct a criminal background check before hiring any staff.
Adult foster care. Criminal background checks are completed on licensees, administrators, and non-employee adult members of the household. Currently, it is the licensee’s responsibility to determine the good moral character of his/her employees. A statute requiring criminal background checks on newly hired adult foster care employees was signed into law in April 2004 but will not be effective until August 2004. Large group homes must submit to the licensing agency the name of any employee or volunteer who is on a court-supervised probation or parole or who has been convicted of a felony.
Monitoring
Adult foster care homes are inspected by the Family Independence Agency, Department of Labor and Economic Growth for fire safety inspections, or a local health department at the request of the Family Independence Agency. Homes for the aged are inspected annually by the Family Independence Agency, and the Department of Labor and Economic Growth for fire safety. Licenses for homes for the aged are renewed annually and adult foster home licenses are renewed every 2 years.
Fees
| Type | Original | Renewal |
|---|---|---|
| AFC foster home (1-6) | $65 | $25 |
| AFC small group (1-6) | $105 | $25 |
| AFC small group (7-12) | $135 | $60 |
| AFC large group (13-20) | $170 | $100 |
| AFC congregate (21+) | $220 | $150 |
| Home for the aged (21+) | $3.13* | $6.27* |
| * Per bed per year. | ||
Minnesota
Citation
Housing with services establishments (registration): MS §144D.01 et seq.
Home care licensure: MS 144A.43 to 144A.48.
Minnesota rule, Chapter 4468 et seq. and Chapter 4669
General Approach and Recent Developments
The State registers housing with services establishments and licenses the service provider. Registered establishments may contract with a licensed agency or obtain its own license based on the level of care provided. Licensing categories include assisted living home care providers and Class E assisted living services, which covers standby assistance and no hands on care. Most service agencies are licensed as assisted living home care providers. Chapter 37 of the Acts of 2003 established new training requirements for assisted living home care providers and housing with services establishments that serve people with Alzheimer’s disease or related disorders. Interest in defining assisted living has emerged among stakeholder, consumers, counties and the attorney general’s office.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Housing with services establishments | 931 | NA | 600 | NA | 592 | NA |
Definition
A housing with services establishment means an establishment providing sleeping accommodations to one or more adult residents, at least 80 percent of which are 55 years of age or older, and offering or providing for a fee one or more regularly scheduled health-related services and two or more regularly scheduled supportive services, whether offered or provided directly by another entity arranged for by the establishment.
The statute defines assisted living home care provider as a home care provider who provides nursing services, delegated nursing services, other services performed by unlicensed personnel, or central storage of medications solely for residents of one or more housing with services establishments registered under Chapter 144D.
The State’s Medicaid waiver program defines Assisted living services as “up to 24-hour oversight and supervision, supportive services, home care aide tasks and individualized home management tasks…” provided in all settings that are registered as Housing with Services Establishments and provided by management or by providers under contract with the establishment.
Unit Requirements
Housing with services. No requirements stated. Must meet appropriate building and fire codes for the structure.
Admission/Retention Policy
Housing with services. The statute requires written contracts between facilities and tenants that describe the registration status; terms; a description of services to be provided directly or through other arrangements; fee schedules; a description of the process through which the contract may be modified, amended, or terminated; complaint procedures; retention policies; and other items.
Medicaid waiver and state program. Participants for the Alternative Care and Medicaid waiver programs must be screened by the county pre-admission screening team and must meet the nursing home level of care criteria. The Alternative Care (AC) program, funded solely with state revenues, was implemented in 1991 and supports certain home and community services for persons age 65 and over, who are at risk of nursing home placement, have low levels of income and assets, but do not meet Medicaid financial criteria.
Nursing Home Admission Policy
Professional judgment based on the assessment.
Services
Residential care settings may have specific service requirements and limitations based on their particular licensing category. Beyond those requirements, they may choose from an array of possible “supportive” and “health-related” services to develop their own service packages based on the needs of their community and their target market. Assisted living home care providers must deliver at least one of the following services: delegated nursing services, other services performed by unlicensed personnel, or central storage of medications.
Services furnished or arranged for by a provider may include supervision, supportive services, individualized home care aide tasks, individualized home health aide-like tasks, and individualized home management tasks. Individualized means services are chosen and designed specifically for each resident’s needs, rather than provided or offered to all residents regardless of their illnesses, disabilities, or physical conditions.
Home care licensing rules define health related services as professional nursing services or home health aide tasks such as administration of medication; routine delegated medical, nursing, or assigned therapy procedures; assistance with body positioning or transfers of people who are not ambulatory; the feeding of clients who are at risk of choking; assistance with bowel and bladder control, devices, and training programs; assistance with therapeutic or passive range of motion exercises; and provision of skin care and of services to maintain hygiene during episodes of illness.
Home care aide tasks are differentiated from home health aide and include assisting with dressing, oral hygiene, hair care, and grooming and bathing. If the client is ambulatory and has no serious illness or infectious disease, these tasks include preparing modified diets, medication reminders, and household chores in the presence of technically sophisticated medical equipment or during episodes of acute illness or infectious disease.
Home management tasks include housekeeping, laundry, preparation of regular snacks and meals, and shopping. Supportive services includes assisting clients in setting up medical and social services, assisting clients with funds, arranging for or providing transportation, and socialization (when socialization is part of the plan of care, has specific goals and outcomes established and is not diversional or recreational in nature.)
Assisted living plus is a group of services, one of which must be 24-hour supervision, delivered in three settings: one to five unrelated people in a residential unit; five or more unrelated people in a setting which is licensed as a board and lodge; or a residential center which is a building or complex of adjacent buildings with separate living units which clients rent or own. Providers must be registered as a housing with services establishment and licensed as a class A home care agency or an assisted living home care provider. Assisted living can be delivered in the same settings but does not include 24-hour supervision.
NOTE: In the last legislative session, the Housing with Services Act was modified to allow residential care settings that don’t have at least 80 percent elderly persons to voluntarily register as Housing with Services Establishments, thus enabling their residents to be served with the Assisted Living Plus package.
Under the Elderly Waiver program (and the Alternative Care program), residents may also receive home health and skilled nursing services, which are reimbursed separately from the payment for assisted living services. However, individuals receiving assisted living services may not receive homemaking and personal care services as well as assisted living services.
Dietary
Not specified.
Agreements
The registration statute requires contracts between the housing operator and tenants that include: name and address of the establishment and owners; a statement describing the registration and licensure status of the establishment; term of the contract; description of the services provided and the base rate; fee schedules for any additional services; process for modifying, amending, or terminating the contract; complaint process; billing and payment procedures; resident’s designated representative; criteria for determining who may reside in the establishment; statement regarding the ability of tenants to receive services from providers that do not have an arrangement with the establishment; and a statement regarding the availability of public funds.
Home care regulations cover the service agreement which includes a description of the service to be provided and the frequency of each service, the persons or category of persons who will provide the service, the schedule or frequency of sessions of supervision or monitoring, fees for each service, and a plan for contingency action if scheduled services cannot be provided.
Provisions for Serving People with Dementia
Housing with Services Establishments are required to disclose the form of care or treatment, the treatment philosophy, unique features for screening, admission and discharge, assessment, care planning and implementation, staffing patterns, the physical environment, security features, frequency and type of activities, opportunities for family involvement, and the costs of care. Direct care staff must receive 4 hours of training within the first month of employment and 4 hours a year. The statute specifies that training is required in the following areas: an explanation of Alzheimer’s disease and related disorders; assistance with activities of daily living; problem solving with challenging behaviors; and communication skills. The licensee shall provide to consumers in written or electronic form a description of the training program, the categories of employees trained, the frequency of training, and the basic topics covered.
Medication Administration
The assisted living home care provider rules allow medication administration. Staff administering medications must be instructed by a registered nurse, the instructions must be written, and the person must demonstrate competence in following the instructions.
Public Financing
Services for low-income residents have been covered through the state-funded Alternative Care Program (AC) since 1991 and the Medicaid Home and Community Based Services Waiver program since 1993. The AC Program serves nursing home eligible residents whose gross monthly income is greater than 120 percent of Federal Poverty Level or whose gross assets are greater than the asset limit for the Medical Assistance (MA) program, but whose combined adjusted monthly income and adjusted assets are no greater than the cost of 180 days of nursing facility care. The HCBS waiver covers aged and disabled Medicaid recipients who meet the nursing home criteria.
The HCBS waiver program served 2,895 beneficiaries in 281 facilities in FY 2001 and the AC program served 1,588 beneficiaries in 247 facilities. Rates for services are negotiated between the county and the provider with limits based on the client’s case-mix classification.
| 2004 (FY03) | 2002 (FY01) | 2000 | ||||
|---|---|---|---|---|---|---|
| Facilities | Participation | Facilities | Participation | Facilities | Participation | |
| HCBS | 396 | 4,114 | 281 | 2,895 | NR | 397 |
| AC* | 325 | 2,328 | 247 | 1,588 | NR | NR |
| * AC is a state-funded program. | ||||||
Alternative Care Program. Service rates under this state-funded program cannot exceed the State’s Medicaid share of the average monthly nursing home payment. The client pays for room and board (raw food costs only; meal preparation is covered as a service). The cost of services in addition to assisted living services may not exceed 75 percent of the average nursing home payment for the case-mix classification.
HCBS waiver. Rates for assisted living services in the waiver program are also capped at the state share of the average nursing home payment, and the total costs, including skilled nursing and home health aide in addition to assisted living services, cannot exceed 100 percent of the average cost for the client’s case-mix classification. The statewide maximum service rate for assisted living services beginning July 1, 2003, for elderly recipients ranged from $982 a month to $2,283 a month depending upon the case-mix classification. These rates are effective through June, 30, 2005. Rates in a particular county could be higher or lower than the averages. In addition to the assisted living rates, the waiver has caps for all waiver services including assisted living. The Alternative Care Program maximum paid for all services including assisted living ranged from $1,543 to $3,588 a month. Medicaid waiver maximum costs ranged from $2,057 to $4,784 a month depending upon the case-mix classification (see table below). Around 90 percent of the Elderly Waiver participants fall into Categories A through E.
The above rates do not include room and board. The Special Income Standard (SIS) or 300 percent eligibility option, for all Elderly Waiver recipients during state fiscal year 2004, is $1692. The maintenance allowance that residents retain for their expenses is $766, which includes a $74 personal needs allowance (equal to the PNA for nursing facility residents), and the remaining $692 pays for room and board costs. Any income above the $766 maintenance allowance is applied toward the cost of waiver services. Elderly Waiver participants who have a gross monthly income which exceeds 300 percent of Supplemental Security Income (SSI) may not use the SIS when determining their Medicaid budget but must pay a medical spend down (all monthly income greater than the State’s Medically Needy standard for aged, blind and disabled or $582) toward all incurred medical expenses.
| Case- Mix |
Average Assisted Living Payment a |
Total Rate Limits for All Servicesb |
Description | |
|---|---|---|---|---|
| AC Program |
Elderly Waiver |
|||
| A | $1,029 | $1,543 | $2,057 | Up to 3 ADL dependenciesc |
| B | $1,169 | $1,755 | $2,340 | 3 ADLs + behavior |
| C | $1,372 | $2,059 | $2,745 | 3 ADLs + special nursing care |
| D | $1,418 | $2,127 | $2,836 | 4-6 ADLs |
| E | $1,564 | $2,346 | $3,128 | 4-6 ADLs + behavior |
| F | $1,611 | $2,417 | $3,223 | 4-6 ADLs + special nursing care |
| G | $1,663 | $2,494 | $3,326 | 7-8 ADLs |
| H | $1,876 | $2,814 | $3,752 | 7-8 ADLs + behavior |
| I | $1,925 | $2,888 | $3,851 | 7-8 ADLs + needs total or partial help eating (observation for choking, tube, or IV feeding and inappropriate behavior) |
| J | #2,051 | $3,079 | $4,105 | 7-8 ADLs + total help eating (as above) or severe neuromuscular diagnosis or behavior problems |
| K | $2,392 | $3,588 | $4,784 | 7-8 ADLs + special nursing |
|
||||
Staffing
The Department of Health’s standards for home care services licenses do not apply to the building itself. Housing with services providers may not accept anyone for whom services cannot be provided and must provide adequate staff to meet the needs of clients/residents.
Training
Staff. Orientation and training are required based on the tasks performed by the worker.
Training requirements are specified for staff performing home care aide tasks, home management tasks, and delegated nursing tasks. Each person who applies for a license and/or provides direct care, supervision of direct care, or manages services for a licensee must receive an orientation to home care requirements covering: the general approach of the statute and regulations, handling of emergencies, reporting abuse/neglect, home care bill of rights, handling and reporting of complaints, and services of the ombudsman.
Training and a competency evaluation are required for unlicensed people who perform assisted living home care tasks. The curriculum includes: a general overview of the Minnesota statutes; recognition and handling of emergencies and use of emergency services; reporting the maltreatment of vulnerable adults; home care bill of rights; handling of complaints; services of the ombudsman; observation, reporting, and documentation of client status and of the care or services provided; basic infection control; maintenance of a clean, safe, and healthy environment; communication skills; basic elements of body functioning and changes in body function that must be reported to an appropriate health care professional; and the physical, emotional, and developmental needs of clients.
Staff who provide medication administration and active assistance with medications must complete the above training program, pass a competency test, and be instructed by a registered nurse in the procedures to administer the medications to each client/resident. The instruction is specific to each resident.
Staff providing home management tasks (housekeeping, meal preparation, and shopping) must receive training on the bill of rights and orientation on the aging process and the needs and concerns of elderly and disabled persons.
Background Check
A license may be denied or suspended for conviction of any of 15 types of crimes listed in the regulations. Each employee with direct contact with clients must sign a statement disclosing convictions of all crimes, except minor traffic violations. Employees may be required to sign a release statement authorizing local authorities to provide the commissioner a history of criminal convictions.
Monitoring
Not described.
Fees
Housing with services buildings must pay a registration fee of $35 per address. Assisted living home care agencies pay a graduated fee based on average census:
- $125 annually for those providers serving a monthly average of 15 or fewer clients, and for assisted living providers of all sizes during the first year of operation;
- $200 annually for those providers serving a monthly average of 16 to 30 clients;
- $375 annually for those providers serving a monthly average of 31 to 50 clients; and
- $625 annually for those providers serving a monthly average of 51 or more clients.
Mississippi
Citation
Personal care homes--assisted living: Mississippi regulations Part I §101.1 et seq.
Personal care homes--residential living: Mississippi regulations Part I §101.1 et seq.
Personal care homes--Alzheimer’s Disease/Dementia care unit: Part I §101.1 et seq.
General Approach and Recent Developments
Revisions to the rules were adopted in 2002 and 2003. The most significant change expanded requirements for criminal background checks. Regulations covering Alzheimer’s disease units were adopted July 2001. The rules create two types of personal care homes: assisted living and residential living. A Medicaid waiver has been implemented. H1478 was signed into law and allows residents needing skilled nursing to reside in personal care homes.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Personal care homes | 194* | 4,197* | 207 | 5,137 | 197 | 4,568 |
| * July 2003. | ||||||
Definition
Assisted living means the provision of personal care and the addition of supplemental services to include, but not be limited to, the provision of medical services (i.e., medication procedures and medication administration) and emergency response services.
Facility means any home or institution that (1) has sought or is currently seeking designation as a licensed facility under the terms of these regulations; or (2) is operating a home or institution unlawfully which, by its nature and operational intent, is required to be a licensed facility under the terms of these regulations.”
Personal care home--residential living. The terms “personal care home--residential” and “residential personal care home” are defined as any place or facility operating 24 hours a day, 7 days a week, accepting individuals who require personal care services or individuals who, due to functional impairments, may require mental health services to compensate for activities of daily living. Regulations by the licensing agency for such facilities are governed by the “Regulations Governing Licensure of Personal Care Homes--Residential.”
Personal care home--assisted living. The terms “personal care home--assisted living” and “assisted living personal care home” are defined as any place or facility operating 24 hours a day, 7 days a week, accepting individuals who require assisted living services as governed by the State’s regulations.
Unit Requirements
There must be at least 80 square feet for each resident in a bedroom. Residents shall not have to enter one bedroom through another bedroom. No more than four residents may share a bedroom. Separate toilet and bathing facilities shall be provided on each floor for each sex: one bathtub/ shower for every 12 residents, and one lavatory and toilet for every six residents.
Admission/Retention Policy
Personal care residential living homes may not admit non-ambulatory residents, or anyone that requires physical restraints; poses a serious threat; requires nasopharyngeal and/tracheotomy suctioning; gastric feedings; intravenous fluids, medications or feedings; indwelling catheter; sterile wound care or treatment of decubitous ulcers or exfolitative dermatitis.
Personal care assisted living homes may admit residents whose needs can be met by the licensed facility. An appropriate resident for assisted living personal care homes is primarily an aged ambulatory person who requires domiciliary care and who may require nonmedical services, medical services such as medication assistance, emergency response services, and home health services as prescribed by a physician’s order and as allowed by law. Residents who are unable to descend stairs unassisted may not be placed above the ground floor.
Tenants cannot be admitted or retained if they: require physical restraints; pose a serious threat to themselves or others; or require nasopharyngeal and/or tracheotomy suctioning; gastric feedings; intravenous fluids, medications, or feedings; an indwelling urinary catheter; sterile wound care; or treatment of decubitus ulcers or exfoliative dermatitis.
Aging in place legislation passed in 2001 that allows residents who need skilled services to continue to reside in the facility, if approved in writing by a licensed physician. No more than two residents, or ten percent of residents in the facility, whichever is greater, may receive skilled services.
Nursing Home Admission Policy
Beneficiaries qualify for the waiver if they need assistance in three ADLs or two ADLs plus a diagnosis of dementia. The assessment form is completed by a physician.
Services
Assisted living means the provision of personal care and the addition of supplemental services to include but not be limited to, the provision of medical services (i.e., medication procedures and medication administration) and emergency response. Social services and daily activities are also required.
Dietary
Facilities must provide three well-planned, attractive, and satisfying meals a day that meet the nutritional, social, emotional, and therapeutic needs of residents and that meet current recommended dietary allowances. All special diets must be planned by a licensed dietician who visits at least once every 30 days and files a consulting report. All facilities must have an employee dedicated to meal preparation and food service.
Agreements
The agreement must be signed prior to or on admission and must contain: basic charges agreed upon (room, board, laundry, and personal care); the period covered by the charges; services for which special charges are made; agreement regarding refunds for any payments made in advance; a statement that the operator shall make the resident’s responsible party aware, in a timely manner, of any changes in the resident’s status, including those which require transfer and discharge; or operators who have been designated as a resident’s responsible party shall ensure prompt and efficient action to meet resident’s needs.
In addition, facilities must give written notice when basic charges or facility policies change.
Provisions for Serving People with Dementia
Rules were adopted in 2001 that define Alzheimer’s disease as a “chronic progressive disease of unknown causes that attacks brains cells or tissues.”
The rules require three hours of nursing care per resident per day and require an RN or LPN on all shifts. Two staff must be available at all times. Staff orientation must cover the facility’s philosophy of dementia care; a description of the dementias; policies and procedures; and common behaviors and recommended behavior management. In-service training must be provided quarterly on a variety of dementia-related topics, including the development of comprehensive and individual care plans, which must be appropriate and meaningful to each resident and be based on cultural and lifestyle differences. Topics are detailed in the training section.
A complete health assessment and an assessment by a licensed practitioner, whose practice includes assessment of cognitive, functional, and social abilities, must be carried out.
Therapeutic activities must be provided 7 days a week by a certified therapeutic recreation specialist. Activities include leisure, self-care, and productive activities in the following areas: structured large and small groups; spontaneous intervention; domestic tasks; life skills; work; relationships/social; leisure; seasonal; holidays; personal care; meal time; and intellectual, spiritual, creative and physically active pursuits.
Physical environments rules require visual contrast between tables and dining utensils. Rooms can be individually identified to assist with recognition. Facilities must have policies and procedures to deal with residents who may attempt to wander outside the facility.
Medication Administration
Licensed staff may administer medications in assisted living settings. When the nurse is not on-duty, staff may use medication day planners and may pass medications to residents. In residential settings, since a nurse is not required, trained staff may assist with self-administration. Staff may determine which medication is to be taken, the dosage, or the time at which the medication is to be taken.
Public Financing
A Medicaid waiver was implemented in 2001 to serve aged, people with disabilities, and people with dementia. Six facilities contract with the Medicaid program and serve 68 residents. Over time the program will serve a maximum of 500 beneficiaries in seven pilot counties. Facilities receive a per diem rate of $33.18. The rate was developed based on case-mix adjusted rates paid to nursing homes for less impaired residents (PA1 and PA2). Average rates were computed for four nursing home rate components: direct standard care, care related rate, administrative costs, and operating costs. The payment rate consists of 40 percent of the direct care standard, 10 percent of the care related rate, and 50 percent of the administrative and operating rates. The remaining nursing home costs were considered to apply to room-and-board costs which are not covered by the Medicaid service rate.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participation | Facilities | Participation | Facilities | Participation |
| 6 | 68 | 1 | 15 | NA | NA |
Staffing
Personal care assisted living homes must have one attendant per 15 or fewer residents from 7 a.m. to 7 p.m. and one attendant per 25 residents from 7 p.m. to 7 a.m. A licensed nurse must be on the premises 8 hours a day.
Personal care residential living homes are not required to have a licensed nurse on staff.
Training
Administrator. Must be full-time and at least 21 years old and have a high school diploma or GED.
Staff. Personnel shall receive on a quarterly basis appropriate training on the topics and issues related to the population being served. The training must be documented by a narrative of the content and the signatures of those attending.
An orientation for staff in dementia care facilities must be provided that covers the facility’s philosophy, a description of the disease, the facility’s policies and procedures regarding the general approach to care including therapies provided; treatment modalities; admission, discharge and transfer criteria; basic services provided; policies regarding restraints, wandering, and egress control; medication management; nutrition management techniques; staff training; family activities; and common behavior problems and recommended behavior management.
Quarterly in-service training must be provided that covers hands-on training in at least three of the following topics: nature and progression of the disease; common behavior problems and management techniques; positive therapeutic interventions; role of the family; environmental modifications; developing individual and comprehensive care plans and how to implement them across shifts; and new developments in diagnosis and therapy.
Background Check
The administrator and all direct care staff must document that they are not listed on the Nurses Aide Abuse Registry. Effective October 2003, a criminal background check must be completed for all new employees who provide direct patient care or services and employees employed prior to July 2003 who have documented disciplinary action by the present employer. The regulations list 14 offenses for which a person may not be employed.
Monitoring
Facilities are inspected by the Mississippi State Department of Health at such intervals as the Department may direct. Operators are required to spend two concurrent days with the licensing agency for training and mentoring within 6 months of employment. The operator may be assigned within central offices or with a survey team. Surveyors who have passed the Surveyor Minimum Qualifications Test are also required to spend two concurrent days with a licensed facility for training and mentoring within 6 months of employment.
Fees
The initial application fee is $100 and $15 per bed. Renewal fees are $15 per bed. A fee is charged for modifications, renovations, expansions, conversions, or replacements at the rate of $50 per hour for review and/or inspection, not to exceed $5,000.
Missouri
Citation
Residential care facilities: Missouri revised statutes §198.003 et. seq.; Missouri code of regulations, Title 19 § 30-86.012 et seq.; Title 19 §30-88
General Approach and Recent Developments
The Department of Health and Senior Services licenses two levels of residential care facilities. Revisions to the regulations will be submitted to the Board of Health in June. Developed through consultation with a task force, the revisions will address fire safety and evacuation of residents, residential care and administrator requirements. Final rules should be promulgated by the fall. Incidents of assaultive and dangerous behavior have increased as facilities serve more clients of the Departments of Mental Health and Corrections, which are being addressed by the revised rules. Prescription drug issues have also increased as facilities serve more residents with mental health needs and frailer elderly residents using multiple medications. Supply has declined slightly as new construction replaces smaller and older facilities.
Legislation passed in 2003 requiring that protective oversight be available 24 hours a day and includes procedures to ask residents who leave the facility about their whereabouts and expected time of return. The law makes operation of an unlicensed facility a Class D felony if abuse or neglect occurs, requires that all claims of neglect or abuse be investigated within 24 hours, and maintenance of a complaint log.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Residential care facility I | 280 | 6,363 | 285 | 6,533 | 313 | 7,030 |
| Residential care facility II | 364 | 15,434 | 363 | 15,106 | 364 | 15,405 |
The State covers services in residential care facilities under the Medicaid state plan rather than an HCBS waiver.
Definition
Residential care facility I (RCF I) means any premises--other than a residential care facility II, intermediate care facility, or skilled nursing facility--which is utilized by its owner, operator, or manager to provide 24-hour care to three or more residents; who are not related within the fourth degree of consanguinity or affinity to the owner, operator, or manager of the facility; and who need or are provided with shelter, board, and with protective oversight, which may include storage and distribution or administration of medications and care during short-term illness or recuperation.
Residential care facility II (RCF II) adds to the definition of RCF I the supervision of diets, assistance in personal care, and supervision of health care under the direction of a licensed physician. Facilities can be licensed to provide both levels of care within the same facility.
Unit Requirements
Homes licensed after 1987 must provide 70 square feet of space per resident in both private and multiple-occupancy rooms. A maximum of four residents may share a room. Homes licensed prior to 1987 shall provide a minimum of 60 square feet per resident. One tub/shower must be provided for every 20 residents and one toilet and lavatory for every six residents.
Admission/Retention Policy
RCFs may admit or retain only residents who are capable mentally and physically of negotiating a normal path to safety using assistance devices or aids when necessary. The rules allow RCFs to admit any resident who can be cared for by the facility directly or in cooperation with community resources or other providers of care with whom it is affiliated or has contracts. Residents must be able to evacuate without physical assistance.
Facilities cannot serve people that are a danger to self or others, are at consistent risk of elopement, require physical or chemical restraint, require more than one person for assistance with activities of daily living (except bathing), or are bedbound or chairbound.
Nursing Home Admission Policy
Eligibility for nursing home and waiver services is determined by a scoring system. Applicants with an assessed level of 18 to 48 points qualify for intermediate care, and higher point levels qualify for skilled nursing care. Residents are assessed in nine areas: mobility; dietary (eating); restorative services; monitoring; medication; behavior; personal care (hygiene, personal grooming including dressing, bathing, oral hygiene, hair and nail care, and shaving) and bowel and bladder functions; and rehabilitation. Each area receives points based on the level of need: no points for no or very limited care; three points for minimal care; six points for moderate assistance; and nine points for maximum assistance. The rules define what qualifies as minimal, moderate, and maximum assistance.
Services
Personal care services are reimbursed through Medicaid for residents who have chronic, stable conditions. Tasks include bathing, hair care, oral hygiene, nail care, dressing, assistance with toileting, walking or transfers, meal preparation, and light housework. Advanced personal care services include assistance for persons with altered body functions who have a catheter or ostomy, who require bowel and bladder routines or range of motion exercises, who need assistance applying prescription lotions or ointments, and/or who need assistance with other tasks requiring a highly trained aide.
Dietary
At least three meals a day must be served (two must be hot). Modified diets prescribed by a physician can be provided if the resident is monitored by the physician and the diet is reviewed at least quarterly by a consulting nutritionist, dietitian, registered nurse, or physician. The modified diets must be posted in the kitchen.
Agreements
The residents’ rights regulations requires that residents be fully informed in writing prior to or at admission of the services available; related charges; charges for services not covered in the basic rate; procedures in a medical emergency; services outside the facility which may be available; individual’s right to make treatment decisions; and state laws concerning advance directives.
Provisions for Serving People with Dementia
Rules for Level II facilities serving people with dementia were effective in June 2001. Facilities must complete a disclosure form. RCF II facilities may serve people with Alzheimer’s disease if the resident is physically but not mentally capable of negotiating a normal path to safety using assistive devices or aids when certain conditions are met. They include:
-
A family member or legal representative in conjunction with a physician and the facility or legal representatives determine the facility can meet the needs of the resident.
-
The facility has an automatic sprinkler system that complies with specified codes.
-
Residents who are mentally incapable of negotiating a path to safety are housed only on the ground floor.
-
Residents have the opportunity to explore the facility and grounds.
-
The facility has an appropriate number and type of staffing 24 hours a day to provide proper care. (Every mentally incapable resident counts as three residents in determining staffing capacity.)
-
Every mentally incapable resident is assessed by a licensed professional on admission, at least every 6 months, and whenever a change in condition occurs as reported by the Minimum Data Set (MDS).
-
An individual service plan is developed.
-
Electronic personal monitoring devices are used when recommended by a physician.
-
Staff receive at least 4 hours of training on a quarterly basis of which 2 hours is targeted on dementia.
-
All self-care, productive, and leisure activities programs are provided.
-
New direct-care employees working in the Alzheimer’s unit must be given 24 hours of training within their first 30 days of employment, and 4 hours of in-service training each quarter.
New training requirements were developed by the Department of Health and Senior Services. The MDS form must be completed and individualized service plans developed.
Facilities file a disclosure on a standard form that provides information on philosophy; process and criteria for placement, transfer, or discharge; assessment and care planning process; staff training and continuing education practices; physical environment; activities; role of families; cost of care and additional fees; and safety and security measures.
Medication Administration
Medication aides may administer or assist with medications. Injections must be administered by a licensed nurse or physician except that insulin injections may be given by a certified medication technician or a Level I medication aide. Medications must be reviewed by a pharmacist or registered nurse every other month in Level II facilities and every 3 months in Level I facilities.
Public Financing
Personal care and advanced personal care services are reimbursed as a Medicaid state plan service in residential care facilities. The program serves elders, people with disabilities, people with mental retardation and developmental disabilities, and people with mental illness.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participation | Facilities | Participation | Facilities | Participation |
| 494 | 8,125* | 569 | 7,300 | 677 | 7,884 |
| * Unduplicated 2003 count. | |||||
The payment varies by resident based on an assessment and a plan of care completed by a case manager from the Division of Health and Senior Services. Effective July 1, 2003, the payment rate is $13.16 an hour for personal care aides, $15.20 an hour ($14.41 in 2000) for advanced personal care aide services, and $28.07 an hour for nursing visits. The maximum payment in FY2004 is $2,368 a month and is based on the net state cost in a nursing facility. Residents needing only personal care may receive 60 percent of the total cap. Residents who need advanced personal care services may receive the full amount of the cap.
Facilities can set their own rates for room and board. Residents can make payments by various means including SSI, Missouri Cash Grant if eligible, another state agency (such as the Department of Mental Health), and family supplementation. Type I facilities receive a room-and-board payment from SSI and State supplement of $720 a month (less the $25 personal needs allowance [PNA]), and Type II facilities receive a room-and-board payment of $856 a month (less the $25 PNA).
Staffing
Facilities must have adequate staffing. Minimum ratios are established. For Level I facilities, one employee is required for every 40 residents or portion thereof, and must be awake unless there are 20 or fewer residents. Level II facilities must have one staff for every 15 residents during the day; one to 20 beginning at 3 p.m., and one to 25 on the night shift. One licensed nurse per 30 residents is required at least 8 hours a week.
Training
Administrators. Administrators of RCF II facilities must be licensed nursing home administrators or attend at least 20 hours of continuing education each fiscal year (July through June) given or approved by the Division on Aging. They must also successfully complete a state approved Level I Medication Aide course unless a full-time licensed nurse is available. Licenses are not required for administrators of RCF I facilities, although annual attendance at in-service training sessions is required.
Staff. Prior to or on the first day that a new employee works in the facility, she/he shall receive at least a 1 hour orientation to his/her job function. The minimum orientation includes job responsibilities, how to handle emergency situations, the importance of infection control and hand washing, confidentiality of resident information, preservation of resident dignity, how to report abuse/neglect to the Division on Aging, information regarding the employee Disqualification List, and instruction regarding the rights of residents and protection of property.
A statement must be included in the personnel record of each employee that the employee was instructed on residents’ rights, facility’s policies, and job duties and that orientation was received.
Staff administering medications receive a certificate after completing a designated course developed by the University of Missouri-Columbia.
Background Check
Administrators. Administrators must not have been convicted of an offense involving the operation of a long-term care facility or similar facility.
Staff. A background check is performed on all employees. Individuals who have been convicted of a Class A or B felony of a crime against a person are not permitted to work or volunteer in the facility in any capacity. In addition, no person listed on the Employee Disqualification List maintained by the Division of Aging shall work or volunteer in the facility in any capacity.
Monitoring
Not specified.
Fees
Licensing fees are $100 for facilities of three to 24 beds, $300 for facilities with 25 to 100 beds, and $600 for facilities of more than 100 beds.
Montana
Citation
Assisted living facilities, Administrative Rules of Montana (ARM) 32§102 Subchapter 2800.
Adult foster care homes, ARM 32§100 Subchapter 100
General Approach and Recent Developments
The purpose section of the regulations states that personal care or assisted living facilities are a setting for frail, elderly or disabled persons, which provide supportive health and service coordination to maintain the resident's independence, individuality, privacy and dignity.
Legislation replacing personal care facilities with assisted living facilities was codified in October 2003. Regulations implementing the rules were published in February 2004, and became final on May 7, 2004. The major components of the new regulations include a separate section for facilities serving people with cognitive impairments and requirements for administrators. HB 681 passed in 2003 and authorizes the Board of Nursing to issue rules to implement a medication aide program in assisted living. The State's Medicaid HCBS waiver reimburses services provided in assisted living facilities (ALFs) and adult foster care homes.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted living facilities | 177 | 3,730 | 149 | 3,276 | 127 | 2,600 |
Definition
Assisted living facility means a congregate residential setting that provides or coordinates personal care, 24-hour supervision and assistance, both scheduled and unscheduled, and activities and health related services.
Activities of daily living (ADLs) means tasks usually performed in the course of a normal day in a resident’s life that include eating, walking, mobility, dressing, grooming, bathing, toileting and transferring. Assistance with, or the administration of medications, is not considered an ADL.
Three categories of facilities are defined based on the needs of residents. Category A means the residents can self medicate, need assistance with no more than 3 ADLs, and are generally in good health. Category B means residents may be in need of nursing services; be consistently and totally dependent in more than four ADLs, but may not require chemical, physical, or medical restraint or be a danger to self or others. Category C facilities serve residents with cognitive impairments who are not capable of expressing needs or making basic care decisions, who may be at risk of leaving the facility without regard to personal safety, but who may not be a danger to self or others (except for risk of leaving) and may not require physical or chemical restraint.
Unit Requirements
New facilities must limit rooms to 2 residents. Existing facilities may serve four residents in a single bedroom. Each single bedroom must contain 100 square feet and each multi-bedroom must contain at least 80 square feet per bed, excluding toilet rooms, closets, lockers, wardrobes, alcoves, or vestibules. Each resident must have access to a toilet room without entering another resident's room or the kitchen, dining, or living areas. There must be one toilet room for every four residents and one bathing facility for every twelve residents.
Kitchens or kitchenettes in resident rooms are permitted if the resident's service plan permits unrestricted use and the cooking appliance can be removed or disconnected if the service or health care plan indicates the resident is not capable of unrestricted use.
Admission/Retention Policy
Category A facilities may not serve residents needing physical or chemical restraint, stage 3 or 4 pressure sores; gastronomy or jejunostomy tubes; require skilled services on a continual basis (except administration of medications); residents who are a danger to self or others; dependent in 4 or more ADLs as a result of cognitive or physical impairment; or residents incapable of expressing needs or making basic care decisions. Category A residents may receive skilled medical services for no longer than 30 continuous days per occurrence, not to exceed 120 days in a 12-month period.
Category B facilities may serve people who are consistently and totally dependent in 4 or more ADLs; require skilled services for more 30 days per episode and more than 120 days a year if the services are provided or arranged by the facility or the resident; are not a danger to self or others; do not require physical or chemical restraints; and have a signed health care assessment by a licensed healthcare professional that is renewed quarterly.
Category C facilities serve residents who have severe cognitive impairments. Such a person is incapable of recognizing danger, self-evacuating, summoning assistance, expressing needs or making basic care decisions, are at risk of leaving the facility without regard to personal safety, and may not be a danger to self or others.
Nursing Home Admission Policy
Applicants can meet criteria in either of two areas to be eligible. The first area includes one of the following: comatose; ventilator dependency; respiratory problems requiring constant treatments, observation or monitoring under direction of registered nurse; unstable medical conditions requiring 24-hour availability of services; nasopharyngeal aspiration; cognitive impairment requiring a structured, professionally staffed environment; tube feedings; or maintenance of a tracheostomy, gastrostomy, colostomy, ileostomy, or other indwelling tubes. The second area requires two of the following: constant supervision to total human assistance in two ADLs; administration of daily medications; physical, mental, or medical needs which are deteriorating or will continue to deteriorate in the absence of monitoring or supervision; restorative nursing or therapy treatments; care of extensive decubitus ulcers or other widespread skin diseases; or requires regular intervention by a case manager.
Services
Each resident receives an initial needs assessment, prior to move in, to determine the prospective resident's needs that includes: cognitive patterns such as short-term memory, long term memory, memory recall, decision making change in cognitive status/awareness or thinking disorders; sensory patterns; activities of daily living functional performance; mood and behavior patterns such as sadness or anxiety displayed by resident, wandering, verbally abusive, physically abusive and socially inappropriate/disruptive behavior; health problems/accidents; weight/nutritional status; skin problems; medication use; and use of restraints, safety or assistive devices. A follow-up needs assessment is performed again 60 days after move in date, as needed at a significant change of condition, and no less than annually for category A residents
Facilities must provide or make provisions for personal services such as laundry, housekeeping, food service and local transportation; assistance with ADLs, as provided for in the admission agreement and service plan, and that do not require the use of licensed health care professional or licensed practical nurses; recreational activities; assistance with self-medication; 24-hour on site supervision by staff; and assistance in arranging policy-related services such as medical appointments and appointment related to hearing aids, glasses and dentures. Facilities may provide, make provisions for or allow residents to obtain third party services for administration of medications and skilled nursing or other skilled services for temporary, short-term acute illness for up to 30 consecutive days per episode up to 120 days per year.
Services include required personal care services such as: personal grooming (bathing, hand washing, shampoo, shaving, and hair care); oral hygiene and denture care; toileting and toilet hygiene; eating; use of crutches and other assistive devices; and assistance with self-medication. Other services include laundry, housekeeping, recreation activities, and food service. They also include providing or making available provision for local transportation, personal assistance with ADLs, recreational activities, and supervision of self-medication. Personal care assistance is provided while encouraging residents to maintain independence and a sense of self-direction. Administration of medications is not considered an ADL.
Licensed health care professionals conduct assessments covering specific topics in Category B facilities. Requirements are specified for incontinence care and skin care.
Category B facilities shall employ or contract with a registered nurse to provide or supervise nursing services to include: general health monitoring on each category B resident; performing a nursing assessment on category B residents when and as required; assistance with the development of the resident health care plan and, as appropriate, the development of the resident service plan; and routine nursing tasks, including those that may be delegated to licensed practical nurses (LPN) and unlicensed assistive personnel in accordance with the Montana Nurse Practice Act.
Dietary
Facilities establish and maintain policies addressing the preparation and serving of meals in amount and variety sufficient to meet the nutritional needs of each resident. Therapeutic diets must be provided when ordered by a physician. Meals must offer an alternative food or drink to give residents a choice. Staff receive training in food, nutrition, and diet planning.
Agreements
A written resident agreement is required and includes at least the following items: the criteria for requiring transfer or discharge of the resident to another level of care; a statement explaining the availability of skilled nursing or other professional services from a third party provider to a resident in the facility; the extent that specific assistance will be provided by the facility as specified in the resident service plan; a statement explaining the resident's responsibilities including but not limited to house rules, the facility grievance policy, facility smoking policy and policies regarding pets; a listing of specific charges to be incurred for the resident's care, frequency of payment and facility rules relating to nonpayment of services and security deposits, if any are required; a statement of all charges, fines, penalties or late fees that shall be assessed against the resident; a statement that the agreed upon facility rate shall not be changed unless 30 day advance written notice is given to the resident and/or their legal representative; and an explanation of the facility's policy for refunding payment in the event of the resident's absence, discharge or transfer from the facility and the facility's policy for refunding security deposits.
Provisions for Serving People with Dementia
Category C facilities must disclose the facility's overall philosophy, transfer and discharge criteria, resident assessment processes, processes for implementation and updating of health care plans, staff training, physical environment, resident activities, family involvement and costs of care. Staff must be awake and available to provide supervision and care to the resident.
Category C administrators must have three or more years experience in working in the field of geriatrics or caring for disabled residents in a licensed facility; ora documented combination of education and training that is acceptable to the Department of Health. At least eight of the 16 hours of the annual continuing education requirement must cover caring for persons with severe cognitive impairments.
Category C direct care staff must receive additional documented training in: the facility or unit's philosophy and approaches to providing care and supervision for persons with severe cognitive impairment; the skills necessary to care for, intervene with and direct residents who are unable to perform activities of daily living; techniques for minimizing challenging behavior including: wandering, hallucinations, illusions and delusions; impairment of senses; therapeutic programming to support the highest possible level of resident function (large motor activity; small motor activity; appropriate level cognitive tasks; and social/emotional stimulation); promoting residents' dignity, independence, individuality, privacy and choice; identifying and alleviating safety risks to residents; identifying common side effects and untoward reactions to medications; and techniques for dealing with bowel and bladder aberrant behaviors.
Medication Administration
Staff may assist with self-administration of medications. In Category B and C facilities, medications may be administered by licensed health care professionals or individuals delegated to do so.
HB 681 allows the board of nursing to establish qualifications for licensure of medication aides, including but not limited to educational requirements. The board may define levels of licensure of medication aides consistent with educational qualifications, responsibilities, and the level of acuity of the medication aides' patients. The board may limit the type of drugs that are allowed to be administered and the method of administration. A medication aide may perform services requiring basic knowledge of medications and medication administration under specific circumstances as determined by the board; practice only in a licensed assisted living facility; and practice only under the general supervision of a licensed professional nurse.
Public Financing
An HCBS waiver program covers elders, people with disabilities, and people with mental illness in assisted living facilities. Eligible residents receive $625 in federal SSI payment and a state supplement. Residents retain a personal needs allowance of $100 and pay $525 to the facility for room and board. Family supplementation is allowed by state policy for room and board only.
The Medicaid waiver reimburses adult foster care homes and assisted living facilities between $520 and $1,800 a month depending on the level of care needed by residents. HCBS case managers complete the assessment and determine the payment rate in accordance with state policy. In addition to the room-and-board component, the basic service payment for residents is $520 a month. Additional payments are calculated based on ADL and other impairments. Points are calculated for each impairment. The functions measured are: bathing, mobility, toileting, transfer, eating, grooming, medication, dressing, housekeeping, socialization, behavior management, cognitive functioning, and other. Each function is rated as follows:
- With aides/difficulty: needs consistent availability of mechanical assistance or expenditure of undue effort;
- With help: requires consistent human assistance to complete the activity, but the individual participates actively in the completion of the activity; or
- Unable: the individual cannot meaningfully contribute to the completion of the task.
Each point equals $33 a month. For example, a resident consistently needing help with toileting would be scored a two and would earn $66 a month for that impairment. Residents with severe impairments, totally dependent in more than three ADLs, can receive $44 a month for each point. The total payment (services and room and board) ranges from $1,045 to $2,325 a month although very few participants have been approved at the highest rate. The average payment is $44 a day.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participants | Facilities | Participants | Facilities | Participants |
| 165 | 475 | 111 | 400 | NR | 200 |
Staffing
Facilities must have a sufficient number of qualified staff on duty 24 hours a day to meet the scheduled and unscheduled needs of each resident, to respond in emergency situations, and provide all related services, including, but not limited to: maintenance of order, safety and cleanliness; assistance with medication regimens; preparation and service of meals; housekeeping services and assistance with laundry; and assurance that each resident receives the supervision and care required by the service or health care plan to meet their basic needs.
Category B facilities must employ or contract with a registered nurse.
Training
Administrator. Administrators must be licensed as a nursing home administrator in Montana or another state; or have successfully completed all of the self study modules of “The Management Library for Administrators and Executive Directors”, a component of the assisted living training system published by the Assisted Living University (ALU) or be enrolled in and complete the self study course within six months of employment.
The annual training requirement was raised from six to 16 hours covering: accounting and budgeting, basic principles of supervision, basic and advanced emergency first aid, characteristics and needs of residents, community resources, pharmacy and medication dispensing, resident and provider rights, and skills for working with residents.
Staff. The orientation and training topics covered for direct care staff have been expanded. They cover the facility’s policies and procedures manual; job description; services provided; how to perform ADL care; basic techniques in observation and reporting; changes associated with the aging process including dementia; residents’ rights; assisting with mobility and transfer; lifting techniques; food and nutrition; location of resident records and implementation of services and healthcare plans; assistance with medications; adverse and desired medication reactions; emergency procedures; safety hazards; food preparation; and abuse reporting; and the Montana resident bill of rights. Category B and C staff must receive 16 hours of training specific to direct care requirements for these facilities.
Background Check
All staff may not have convictions for a crime involving violence, fraud, deceit, theft, other deception, or a violation of 52-3-825 MCA for which the person is still under state supervision. Facilities must check with the Montana Nurse Aide Registry for any adverse actions taken against a CNA or any individual who was a CNA. Facilities are required to develop and follow policy and procedures for hiring qualified staff to ensure resident safety and well-being.
Monitoring
Unannounced on-site surveys are conducted annually, biannually, or triennially depending on whether the facility has been granted an extended license. Individuals served under the HCBS program are reassessed every six months or more frequently if needed.
Fees
$20 per bed for up to 20 beds, plus $1 per bed for each bed over 21.
Nebraska
Citation
Assisted living facilities, NAC Title 175, Chapter 4.
General Approach and Recent Developments
Assisted living rules were revised in 2003. Changes were made in the licensing requirements and procedures, with new language stating that a facility must not hold itself out as an assisted living facility or as providing health care services unless licensed under the Health Care Facility Licensure Act. Additionally, reinstatement procedures have changed. A license may now be reinstated at the end of probation, without paying a license fee, after the successful completion of an inspection, if the Department of Health determines an inspection is warranted.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted living facilities | 259 | 9,187 | 227 | 8,369 | 167 | 7,077 |
Definition
An assisted living facility is a facility where shelter, food, and care are provided for remuneration for a period of more than 24 consecutive hours to four or more persons residing at such facility who require or request such services due to age, illness, or physical disability. This definition does not include (a) those homes, apartments, or facilities providing casual care at irregular intervals and (b) those homes, apartments, or facilities in which a competent resident provides or contracts for his or her own personal or professional services and no more than 25 percent of the residents receive such services. A competent resident is someone who has the capability and capacity to make an informed decision. No facility may hold itself out to be assisted living unless it is licensed.
Unit Requirements
Newly constructed facilities must provide rooms of 100 square feet for single resident rooms and 80 square feet per resident in rooms occupied by more than one resident with a maximum of two residents. Apartment units must have 150 square feet for one resident and 110 square feet for each additional resident. Existing or newly constructed facilities may have single bedrooms with 80 square feet and multiple occupancy rooms with no more than four beds per room and at least 60 square feet per bed. Apartments must have 120 square feet for one resident and 100 square feet for each additional resident. Facilities must provide a bathing facility consisting of a tub and/or shower adjacent to each room or provide a central bathing room. Tubs and showers regardless of location must be equipped with hand grips or other assistive devices as needed or desired by the bathing resident. In new construction where a central bathing room is provided, the room must open off the corridor and contain a toilet and sink or have an adjoining toilet room. A bathing room must not directly open to a dining/kitchen area. New construction facilities must have a toilet and sink adjoining each bedroom. Existing or new facilities may have shared toilet rooms provided the following: one toilet for every six beds in existing facilities; one toilet per four beds in new facilities.
Admission/Retention Policy
Anyone needing complex nursing interventions or whose conditions are not stable and predictable may not be admitted, readmitted, or retained unless:
- The resident (or the resident’s designee if the resident is not competent), the resident’s physician, or the registered nurse agree that admission or retention is appropriate;
- The resident (or his or her designee) assumes responsibility for arranging for the resident’s care through private duty personnel, a licensed home health agency, or a licensed hospice agency; and
- The resident’s care does not compromise the facility operations or create a danger to others in the facility.
Assisted living staff while on duty must not provide complex nursing interventions for facility residents. Complex nursing interventions are defined as those which require nursing judgment to safely alter standard procedures in accordance with the needs of residents, which require nursing judgment to determine how to proceed from one step to the next, or which require a multidimensional application of the nursing process. Facilities will be able to develop their own admission and retention policies within state guidelines. The administrator has discretion regarding admission or retention of residents.
Assisted living facilities are allowed to have a facility-owned pet(s). The assisted living facility must ensure that any facility-owned pet does not negatively affect residents. Policies and procedures for pets include an annual examination by a licensed veterinarian; vaccination protocols as recommended by a licensed veterinarian; proper pet care; and responsibility for care and supervision of the pet by facility staff.
Nursing Home Admission Policy
Individuals must have:
- Limitations in three or more ADLs and require medical treatment or observation;
- Limitations in three or more ADLs and one or more risk factors;
- Limitations in three or more ADLs and one or more cognition factors;
- Limitations in one or more ADLs and one or more cognition factors and one or more risk factors.
ADLs include bathing, continence, dressing/grooming, eating, mobility, toileting, and transferring. There are three areas of risk factors: behavior, frailty, and safety. Behavior is the ability to act on one’s own behalf, including interest or motivation to eat, take medications, care for one’s self, participate in social situations and relate to others in a socially appropriate manner. Frailty means the ability to function independently without the presence of a support person. Safety is the availability of adequate housing, including the need for modification or adaptive equipment to assure safety and accessibility; the existence of formal and/or informal supports; and/or the freedom from abuse or neglect. Cognition factors address memory, orientation, communication, and judgment.
Services
Services are to be provided in accordance with resident agreements which maximize resident dignity, autonomy, privacy, and independence. Services include personal care, assistance with ADLs, health maintenance activities, transportation, laundry, housekeeping, financial assistance/ management, behavioral management, case management, shopping, beauty/barber, spiritual services, and activities. Health maintenance activities are defined as non-complex nursing interventions which can safely be performed according to exact directions, which do not require alteration of the standard procedure, and for which the results and resident responses are predictable.
Outcomes in three areas (physical well being, behavioral/emotional well being, and resident agreement) are listed that measure whether resident care is being provided in accordance with the resident’s preferences and needs. Each facility must develop and implement a process to measure consumer satisfaction.
Dietary
Facilities must ensure that daily nutritional needs are met, including special diets ordered by a physician. Written menus must be based on the Food Guide Pyramid, or equivalent, and modified to accommodate special diets. Residents must be monitored for potential nutritional problems by recording weight at admission and if a potential problem is identified, weights are recorded quarterly with follow up to address or rectify weight gains/losses greater than 7.5 percent in three months or 10 percent in six months.
Agreements
An agreement must be negotiated that delineates the services to be provided to meet the resident’s needs as identified during an evaluation. The agreement includes the services provided by the facility and other sources, and how often, when and by whom they will be delivered in order to meet the needs of residents, including those with special needs. Services may not exceed room, board, ADLs, personal care, health maintenance and other supportive services, or those that involve complex nursing interventions allowed by rule. The agreement also specifies the rights and responsibilities of the facility and residents; the costs of services and terms of payment; and the terms and conditions of continued occupancy. The agreement must be reviewed and updated as the resident’s needs change.
Provisions for Serving People with Dementia
Facilities serving special populations must identify resident abilities and special needs; provide staff trained to meet the identified needs; prepare and implement a resident agreement that addresses the special needs; and provide a physical environment that accommodates the needs. Direct care staff have training in the unit’s philosophy and approaches to providing care; the Alzheimer’s disease process; and the skills needed to care for, intervene with, and direct residents.
Each assisted living facility that specializes in providing care for persons who have Alzheimer’s disease, dementia or a related disorder must provide care and services in accordance with the resident service agreement and the stated mission and philosophy of the facility. Prior to admission the facility must inform the resident in writing of the facility’s criteria for admission, discharge, transfer, resident conduct and responsibilities and maintain a sufficient number of direct care staff with appropriate training and skills to meet the residents’ needs. Staff must remain awake at all times. Facilities may not admit or retain a resident who poses a danger to self or others or requires complex nursing interventions.
Medication Administration
Medications may be administered by licensed staff or trained medication aides. Facilities must establish policies to assure that aides demonstrate minimum competency to administer medications and to describe how direction and monitoring will be done based on the route of administration (oral, inhalation, topical, installation, or other routes) and for PRN medications.
Facilities must allow residents to self-administer medications, with or without supervision, when assessment determines the resident is capable of doing so. Residents who self-administer medications must be at least 19 years of age; have cognitive capacity to make informed decisions about taking medications; be physically able to take or apply a dose of medicine; have the capability or capacity to take the medication as prescribed; and have the capability or capacity to observe and take appropriate action regarding any desired effects, side effects, interactions, and contraindications.
Medications may be stored in the resident’s room if the resident keeps the room locked when not present, or the medications are stored in a secure location or locked container.
Public Financing
A Medicaid HCBS waiver was implemented in July 1998. Assisted living is available to elders, people with disabilities, MR/DD, and people with mental illness. The State uses a flat rate system that varies for urban/rural facilities, trust fund facilities and single/double occupancy (see table below). The SSI payment standard is $564 from which beneficiaries retain a personal needs allowance of $60 and $504 is paid for room and board. Family supplementation is not allowed.
Conversion facilities under the State’s Nursing Facility Conversion Program only receive 95% of the Medicaid service rate. Under this program, the Medicaid payment for services for single occupancy in rural areas is $1,301, and $1,539 in urban areas. Total rates for services and room and board in rural areas is $1,805, and $2,043 in urban areas. The rates include an amount for room and board paid by the resident ($504). Family supplementation is not allowed.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participants | Facilities | Participants | Facilities | Participants |
| 187 | 1,500 | 130 | 605 | 77 | 457 |
| Rural areas | Urban areas | |||
|---|---|---|---|---|
| Single Occupancy |
Double Occupancy |
Single Occupancy |
Double Occupancy |
|
| Service | $1,396 | $1,016 | $1,646 | $1,216 |
| Room & board | $504 | $504 | $504 | $504 |
| Total | $1,900 | $1,520 | $2,150 | $1,720 |
| Rural areas | Urban areas | |
|---|---|---|
| Single Occupancy | Single Occupancy | |
| Service | $1,301 | $1,539 |
| Room & board | $504 | $504 |
| Total | $1,805 | $2,043 |
Special Projects
A program providing grants or loan guarantees to nursing homes to convert wings or entire facilities was is in the completion phase. There is only one facility left to convert units. This program was a tremendous success. The majority of the assisted living apartments are full, with the exception of a few geographic regions where 1990 Census forecasts were not very accurate.
The State awarded three rounds of funding, totaling $53 million, for assisted living and money for respite and day care facilities. Awards were made to 74 nursing homes to convert beds to assisted living, including nursing homes who provide a combination of assisted living, adult day care services, and respite. Five nursing homes provide adult day care services only. The project anticipated funding, in whole or in part, 967 assisted living units and de-licensing 967 nursing home beds. In actuality, the State funded 967 assisted living units, but de-licensed more than 967 nursing home beds. This was due to the need for some nursing homes to de-license more than one bed for each assisted living unit. Some homes had to de-license two nursing home beds for every one assisted living unit. The State saved an estimated $5.5 million in annual Medicaid program savings, which will be recovered over a nine-year period of grant awards through reduced nursing home expenditures.
Grantees must agree to maintain specified occupancy levels of Medicaid beneficiaries for a period of 10 years. Grants may cover capital or one-time costs and operating losses for the first year to facilities that have participated in the Medicaid program for at least three years. Non-governmental owned facilities must provide 20 percent of the cost of conversion. Under the program, facilities may convert existing space or construct additional space to include assisted living or other alternative services. Construction of a new assisted living facility may be funded if the nursing home beds are de-licensed and the construction is more cost effective than conversion of existing space.
Staffing
The facility must maintain a sufficient number of staff with the required training and skills necessary to meet the resident population’s requirements for personal care, activities of daily living, health maintenance activities, supervision, and other supportive services.
The facility must have at least one staff person on site at all times when necessary to meet the needs of the residents as required in the resident service agreements.
Training
Staff. Orientation must be given within two weeks to each direct-care staff person of the facility and shall include as a minimum, but is not limited to, residents’ rights; resident service agreement; infection control practices; emergency procedures and information regarding advance directives; information on special care needs; information on abuse, neglect, and misappropriation of money or property of a resident; and disaster plan preparedness.
Ongoing training must be given to each direct-care staff person and shall consist of at least 12 hours per year on topics appropriate to the employee’s job duties including meeting the physical and mental special care needs of residents.
Background Check
Criminal background checks must be completed on all direct care staff. Evidence of contact with the nurse aide registry, adult central registry of abuse and neglect, and the child central registry of abuse and neglect must be obtained to verify no adverse findings concerning abuse, neglect, or misappropriation of resident property. Facilities determine how to use the information in making hiring decisions except that a person with adverse findings on the nurse aide registry may not be employed as a direct care staff.
Additionally, each facility must establish and implement policies and procedures regarding the health status of staff to prevent the transmission of disease to residents. A health history screening of each staff person must be completed prior to assuming job responsibilities. A physical examination is at the discretion of the employer based on results of the health history screening.
Monitoring
The Department may conduct an onsite inspection at any time it deems necessary. Each year a 25 percent random sample of the licensed facilities is selected for inspection, or more often due to cause or lack of selection over five years.
When an inspection reveals violations that create an imminent danger of death or serious physical harm or have a direct or immediate adverse effect on the health, safety, or security of residents, the Department must impose disciplinary action. The State then conducts a follow-up inspection within 90 days. For violations that do not constitute imminent danger, the Department may request a statement of compliance from the facility. If the statement of compliance fails to address the problem(s), the Department may initiate disciplinary action against the facility.
The Department provides education on the regulations during onsite reviews and participates with state assisted living associations to provide education at conferences.
There is good communication between the State and the facilities, and as a result overall compliance and quality of care has improved.
Fees
$800 for 1 to 10 beds; $950 for 11 to 20 beds; $1,025 for 21 to 50 beds; and $1,050 for 51 or more beds.
Nevada
Citation
Residential Facilities for Groups, Nevada Revised Statutes §449.017 et seq.; Nevada administrative code §449.156-2766
General Approach and Recent Developments
Effective January 2004 Nevada amended their HCBS waiver for the Elderly in Group Care Homes to include an assisted living service. Legislation has passed that requires licensed facilities to obtain an endorsement on its license authorizing it to operate as a residential facility which provides “assisted living services.” Facilities may not market themselves as providing assisted living services unless they obtain an endorsement from the State. Facilities will provide to any potential resident a full written disclosure describing what personalized care services will be available and the amount charged for those services. Physical plant standards will require independent units to contain toilet facilities and a sleeping area or bedroom. In facilities with 11 or more residents, units will be able to be shared by consent only. New care principles are described including the promotion of resident quality of life, individualized needs, and personal choice; creative and innovative service provision; resident autonomy; fostering a community atmosphere; and facility operations that minimize the need for residents to move out of the facility as resident needs change over time. Application fees will be $200. Revised minimum staff training requirements for residential facilities which provide services to persons with Alzheimer’s disease are being proposed.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Residential care facilities for groups | 300 | 4,021 | 374 | NR | 326 | 4,581 |
Definition
Residential facility for groups means an establishment that furnishes food, shelter, assistance and limited supervision to an aged, infirm, mentally retarded or handicapped person. The term includes, without limitation, an assisted living facility. The term does not include an establishment which provides care only during the day, persons providing care for no more than two persons in their home, persons providing care for one or more persons related to him within the third degree of consanguinity or affinity, a halfway house for recovering alcohol and drug abusers, or facilities funded by a division or program of the Department of Human Resources.
Residential facilities for groups may specialize in care for different groups: elderly and disabled, mentally ill, Alzheimer’s and related dementia, hospice care, mentally retarded adults, and persons with chronic illnesses. In order to specialize in care for different groups, a facility must obtain an endorsement on its license authorizing it to operate as a residential facility which provides care to a specific population, e.g., persons with Alzheimer’s disease.
A residential facility for elderly or disabled persons means a residential facility which provides care to persons requiring assistance and protective supervision due to infirmity or disability.
A residential facility which cares for persons with Alzheimer’s disease means a residential facility which provides care and protective supervision for persons with Alzheimer’s disease or a related disease, including, without limitation, senile dementia, organic brain syndrome, or other cognitive impairment.
Unit Requirements
Single occupant rooms must have 80 square feet of floor space and multiple resident rooms must have 60 square feet of floor space per resident. No more than three residents may share a room. One toilet and lavatory is required for every four residents. A tub or shower is required for every six residents. However, new legislation provides that units may be shared “with another occupant only upon consent of both occupants and all units must include toilet facilities. Doors of bedrooms may be equipped with locks for use by residents if the doors may be unlocked from the corridor and keys are readily available. Provisions must be made for privacy in all bathrooms and for all toilets located in bedrooms for use by more than one resident.
Facilities serving people with Alzheimer’s disease must be have sprinklers and have 24-hour awake staff. Exit doors must have alarms or time-delay locks. Local audible alarming units must be installed. Facilities serving people with Alzheimer’s disease must have a secure yard, completely fenced and gated with locking devices.
Admission/Retention Policy
Residents are considered Care Category 1 (ambulatory) and Care Category 2 (non-ambulatory). Ambulatory residents are physically and mentally capable of moving from an unsafe area to an area of safety within four minutes unassisted. Non-ambulatory residents require the assistance of at least one other person to move to a safe area within four minutes. Facilities licensed prior to January 1, 1997, are not required to meet requirements for installing automatic sprinkler systems unless they seek to serve Category 2 residents. Sprinklers must be installed prior to a change of ownership, an increase in licensed beds, or admission of non-ambulatory residents. Requirements for hard-wired smoke detectors with battery back up are also waived for small homes unless the above changes are proposed.
People who are bedfast, require 24-hour skilled nursing or medical supervision, and/or require restraints or confinement in locked quarters may not be admitted. The rules do not allow facilities to admit or retain residents with a lengthy list of health conditions with some exceptions. Residents with (or needing) catheters, colostomies or ileostomies, contractures, pressure ulcers, diabetes, unmanageable incontinence, enemas/suppositories, oxygen, injections, protective supervision, or wound care may not be admitted or retained unless the resident is physically and mentally capable of performing the required care or if the care is provided or supervised by an appropriately skilled medical professional. Residents needing gastronomy care, naso-gastric tubes, or have staph or other serious infections or tracheotomies cannot be admitted or retained unless a written request is submitted by the administrator documenting the resident’s condition and how care can be provided and the request is approved by the licensing agency. A resident who is suffering from an illness or injury from which the resident is expected to recover within 14 days after the onset of the illness or the time of the injury may be cared for in the facility. A resident may reject medical care. This rejection must be recorded and signed by the resident.
A resident may be discharged from a residential facility without his approval if he fails to pay his bill within 5 days after it is due; he fails to comply with the rules or policies of the facility; or the administrator of the facility or the bureau determines that the facility is unable to provide the necessary care for the resident.
Nursing Home Admission Policy
Individuals are nursing home eligible if the individual’s condition requires the level of services provided by either a skilled nursing facility or intermediate care facility with at least three deficits identified in the following areas: (1) self-administration of medications; (2) treatments/special needs such as oxygen, tracheostomy, suctioning, ventilator dependent, IV, central line, feeding tube, wound care, glucose monitoring, insulin coverage, as examples; (3) activities of daily living; (4) need for supervision; and (5) instrumental activities of daily living.
Services
Services provided include personal care; at least ten hours of activities a week; three meals a day; protective supervision; laundry; and assistance with access to dental, optical, social, and related services as needed by residents. Assistance with medical needs described in the Admission/Retention Policy section may be provided through a contract with a community agency or directly by staff hired by the facility. Assessments are completed by a physician.
Dietary
Three meals a day and snacks that meet the recommended dietary allowance of the Food and Nutrition Board must be provided. Meals must be nutritious, served in an appropriate manner, suitable for the residents and prepared with regard for individual preferences and religious requirements. At least three meals a day must be served at regular intervals. The times at which meals will be served must be posted. Not more than 14 hours may elapse between the meal in the evening and breakfast the next day. Snacks must be made available in between meals for the residents who are not prohibited by their physicians from eating between meals. A resident must be served meals in his bedroom for not more than 14 consecutive days if he is temporarily unable to eat in the dining room because of an injury or illness. The facility may serve meals to other residents in their rooms upon request. Special diets may be provided if ordered by a physician or dietician. Facilities with more than ten residents must consult at least quarterly with a registered dietician concerning development and review of weekly menus, training for kitchen employees, compliance with nutritional program of the facility, and other observations regarding preparation and serving of meals.
Agreements
Agreements include basic rate and the services included, schedule of payment, charges for optional services, and the refund policy.
Provisions for Serving People with Dementia
Facilities serving people with Alzheimer’s disease must obtain an endorsement on its license to do so. Administrators must have three years’ experience caring for residents with Alzheimer’s disease or a combination of education and training. The facility’s policies and procedures must include a description of the basic services, activities, the manner in which behavioral problems will be addressed, medication management, steps to encourage family involvement, criteria for admission and discharge, and steps that have been developed to prevent and respond to wandering. Facilities must offer activities related to gross motor skills, social activities, sensory enhancement activities, and outdoor activities. At least one awake staff must be on duty at all times. Within three months of employment, staff must complete eight hours of training in providing care to residents with Alzheimer’s disease and providing support to family members. Exits must have warning devices. The grounds must be secure.
Medication Administration
Facility staff may administer medication and assist with self-administration of medications when the resident’s condition is stable and following a predictable course, the amount of medication is at a maintenance level and does not require daily assessment, and a written plan of care has been prepared by a physician or registered nurse. The staff assisting with self-administration must complete a training program in medications.
Public Financing
Amendments effective January 2004 to the HCBS Waiver changed the name from Elderly in Group Care Homes to the Adult Residential Care Waiver and added an assisted living service. Participants must meet the criteria for placement in a group care home or assisted living facility and meet the 300% SSI eligibility criteria. To participate in this waiver, individuals must be placed from a nursing facility, hospital, or have been a participant in one of three other waivers serving the Frail Elderly, People with Physical Disabilities, and Persons with Mental Retardation and Related Conditions.
Under this waiver, there are two service packages: assisted living and personal care. The assisted living service package provides a greater level of choice and provides for care in a more individual apartment/studio setting that includes a kitchenette, a sleeping/living room, and private bath. Rooms may be dually occupied only by choice. The personal care package provides more direct supervision, allows individual choices but is operated in a more group format. Each package has three levels of service based upon the recipient’s functional need, determined through a comprehensive assessment process by a registered nurse or licensed social worker. Assessments are completed annually or upon a significant change in condition. A plan of care is developed from the comprehensive assessment by a social worker or a case manager, and must include the input of the recipient or the recipient’s representative.
The assisted living and personal care services packages provide for assistance with ADLs, 24-hour in-home supervision, assistance to engage in the facility’s social and recreational programming, and transportation to appointments. Services must be provided in a way that fosters independence and aging in place, and routines of service provision must be consumer-driven to the maximum extent possible, with consumers treated with dignity and respect. Caregivers must be trained in the functional care skills needed to care for each unique recipient. Training must include, but not be limited to, techniques such as transfers, mobility, positioning, use of special equipment, identification of signs of distress, First Aid, and CPR.
Medicaid payment is not available for room and board, items of comfort or convenience, or the costs of facility maintenance, upkeep and improvement. Family supplementation has been discussed but not implemented. The SSI and state supplement payment standard is $914 a month which includes a personal needs allowance of $88. For individuals who are on the Adult Residential Care Waiver, room and board fees are determined by the facility. The Medicaid service payment is $20, $45, or $60 a day (about $600, $1,350, or $1,800 a month) depending on the assessment of the level of service.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participants | Facilities | Participants | Facilities | Participants |
| 52 | 222 | 66 | 121 | 72 | 125 |
| Daily Rates | ||||
|---|---|---|---|---|
| Assisted Living Level 1 |
Supervision to minimal assistance with an ADL and a score a 3 on the Total Level of Care (LOC) Score line. | Personal Care Level 1 |
Supervision to minimal assistance with an ADL and a score a 3 on the Total Level of Care (LOC) Score Inc. | $20.00 |
| Assisted Living Level 2 |
Moderate assistance with both critical ADLs* or moderate assistance with any 4 ADLs or dependent with 1-2 ADLs or score of 2 in at least 1 critical behavior.** | Personal Care Level 2 |
Moderate assistance with both critical ADLs* or moderate assistance with any 4 ADLs or dependent with 1-2 ADLs or score of 2 in at least 1 critical behavior.** Minimal physical assistance with ADLs, with some self care tasks requiring moderate levels of assistance. | $45.00 |
| Assisted Living Level 3 |
Maximum assistance to dependent with both critical ADLs or maximum assistance with any 4 ADLs or dependent for 3 or more ADLs or score of 3 in at least one critical behavior area. | Personal Care Level 3 |
Maximum assistance to dependent with both critical ADLs or maximum assist with any 4 ADLs or dependent for 3 or more ADLs or score of 3 in at least one critical behavior area. Moderate physical assistance with ADLs, with some self care tasks requiring maximal levels of assistance. | $60.00 |
| * Critical ADLs include eating/feeding, bladder and bowel continence ** Critical behaviors include wandering, resists care, self-abusive behavior, abusive to others, and memory/cognition |
||||
Staffing
Facilities must maintain staffing patterns that are sufficient to meet the care needs of residents and to enable residents to achieve and maintain their functioning, self care, and independence. Facilities with more than 20 residents must have at least one awake staff member and an additional person available within 10 minutes. Staff of all facilities must receive annually eight hours of training that is directed toward meeting the needs of group-care residents. Facilities licensed for 20 to 49 residents must have one staff member designated to organize, conduct, and evaluate activities. Facilities with 50 or more beds must have a full-time person for activities. Volunteers may be used to supplement the services and programs of a residential facility, but may not be used to replace members of the staff of the facility.
Training
Administrators must have the necessary skills to meet or direct staff to meet the needs of residents unless such skills are met by appropriately skilled medical professionals who are employed by or contract with the facility. Administrators must receive annually eight hours of training that is directed toward meeting the needs of group-care residents.
All staff must possess the necessary skills to meet the needs of the residents in the residential facility with the exception of those needs/skills which are to be met in a contract with other service providers. Within 60 days after being employed by a residential facility for elderly or disabled persons, a caregiver must receive not less than 4 hours of training related to the care of those residents. Staff must receive annually eight hours of training that is directed toward meeting the needs of group-care residents.
Within 30 days after an administrator or caregiver of a residential facility is employed at the facility, the administrator or caregiver must be trained in first aid and cardiopulmonary resuscitation. The advanced certificate in first aid and adult cardiopulmonary resuscitation issued by the American Red Cross or an equivalent certification will be accepted as proof of that training.
Background Check
Caregivers must have no prior convictions or history of previous findings of abuse, neglect, or exploitation or other serious convictions relating to the ability to care for dependent persons. All other staff must not have any convictions or history of abuse, neglect, or exploitation. Reference checks may be used for documentation.
Monitoring
Facilities are subject to on-site inspections and complaint investigation. The State views the oversight process as less structured than nursing facility oversight, although the focus on compliance and quality of care is still paramount. They provide on-site education during the survey process, which has been more effective than a plan of correction-only approach.
Under the Adult Residential Care Waiver, case managers are required to have monthly contact and quarterly face to face contact with the recipient or the recipient’s family, in addition to supervisory home visits to conduct a random sampling of 10% of consumers quarterly and a supervisory review of a sample of case files at a minimum, annually.
Fees
Initial fees are $2,400 plus $184 per bed. Renewal fees are $1,182 plus $92 per bed. Residential facilities for groups with low-income beds have an initial fee of $2,400 plus $100 per bed. Renewal fees are $1,182 plus $35 per bed. Residential facilities for groups with less than 11 beds have an initial fee of $1,085 plus $95 per bed and renewal fees of $35 per bed for low- income beds. Residential facilities for groups with less than 11 beds that have 75% or more low-income beds pay an initial fee of $500 plus $92 per bed, and renewal fees of $35 per bed for low-income beds. Facilities that wish to increase their bed capacity must pay a flat fee of $250 and $184 for each additional bed. For beds that will serve the low-income, the fee is $100.
New Hampshire
Citation
Supported Residential Care Facilities, Chapter He-P 805
Residential Care Home Facilities, Chapter He-P-804
General Approach and Recent Developments
The State continues to regulate facilities under regulations that have expired while discussions on new regulations drafted in 2003 continue between the licensing agency and provider associations. In 1998 legislation passed that allowed facilities to serve nursing home eligible residents. In effect, the bill was interpreted as superceding more limited admission/retention criteria in the regulations. As a result, the licensing agency has observed increased acuity levels, and an increase in complaints and wandering among residents. A bill setting disclosure requirements for assisted living residences and elderly housing (HB 1220) passed and regulations were issued for comment in October 2002.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Residential care | 137 | 4,013 | 148 | 3,936 | 67 | 769 |
| Supported residential care | 75 | 2,797 | ||||
Definition
“Residential care facilities, whether or not they are private homes or other structures built or adapted for the purpose of providing residential care, offering services beyond room and board to two or more individuals who may or may not be elderly or suffering from illness, injury, deformity, infirmity, or other permanent or temporary physical or mental disability. Such facilities include those:
- Offering residents home-like living arrangements and social or health services including, but not limited to, providing supervision, medical monitoring, assistance in daily living, protective care or monitoring and supervision of medications; or
- Offering residents social, health, or medical services including, but not limited to, medical or nursing supervision, medical care or treatment, in addition to any services included under subparagraph (1). Such homes or facilities shall include, but not be limited to, nursing homes, sheltered care facilities, rest homes, residential care facilities, board and care homes, or any other location, however, named, whether owned publicly or privately or operated for profit or not.”
The statute indicates that residential care requires a minimum of regulation and reflects the availability of assistance in personal and social activities with a minimum of supervision or health care, which can be provided in a home or home-like setting. Supported residential health care reflects the availability of social or health services, as needed, from appropriately trained or licensed individuals, who need not be employees of the facility, but residents shall not require nursing services complex enough to require 24-hour nursing supervision. Such facilities may also include short-term medical care for residents of the facility who may be convalescing from an illness and these residents shall be capable of self-evacuation (with or without staff assistance). Supportive residential care serves residents who do not need 24-hour nursing care except on a short-term basis. Residents may need help with ADLs but must be able to evacuate with assistance. Residential care homes are a step below supported residential care facilities and provide supervision and some ADL assistance.
HB 1220 defines assisted living residences as any entity that provides housing and holds itself out, through marketing, advertising, or use of the term “assisted living” or a similar designation, as providing or arranging for personal assistance or any health-related or supportive service beyond room and board to one or more adults who are not related to the owner of the residence by blood or marriage.
Unit Requirements
Units must have at least 80 square feet per one bed room and 140 square feet per room with two beds, exclusive of space required for closets, wardrobe, dressers, and toilet room. Rooms may be shared by two people. Sinks, toilets, tubs, and showers shall be available for every six residents.
Admission/Retention Policy
Residential care homes can accept only those persons who are 1) mobile and can self evacuate; 2) able to initiate and accomplish most activities of daily living but may require supervision or physical assistance; 3) not in need of licensed or professional nursing or monitoring except for temporary episodic illness.
Persons admitted for short stays must have a health examination conducted within 30 days prior to admission and include any orders and medications required by the resident; an assessment focused on the services needed by the resident; and an admission agreement which lists the services to be provided during the residence.
Persons admitted for more than a short-term stay must have a health exam conducted within 30 days prior to admission which addresses medical requirements; functional activities and limitations; medication needs and orders; and dietary needs. The administrator or designee in conjunction with the resident’s provider and family/guardian must complete an initial assessment prior to admission and the administrator must ensure that assessments are completed at least every six months. The resident must receive a written list of services that will be provided; a list of services for which additional payment is required; rules of the home; information on, and procedures for, reserving a place in the home when the resident is hospitalized or out of the home for a period of time; grounds for termination of agreement; and notification required for involuntary transfer for reasons other than emergency situations.
Residential care homes may not accept any resident whose assessment indicates services are required which the facility cannot provide.
Supported residential care facilities may accept only residents who are mobile and can self-evacuate (with our without assistance); are able to initiate and accomplish some ADLs with help but require physical assistance and prompting from others; require intermittent, short-term, 24-hour nursing care or less than 24-hour nursing care on an ongoing basis; require consultation or direct care for therapeutic services (physical, occupational, recreational therapy, and mental health services); or require administration of medications.
Nursing Home Admission Policy
A person is Medicaid eligible for nursing facility services if the person requires 24-hour care for one or more of the following purposes, as determined by the Department of Health and Human Services:
- Medical monitoring and nursing care;
- Restorative nursing or rehabilitative care;
- Medication Administration (or instruction and supervision of self-medication for discharge purposes only); or
- Assistance with two or more activities of daily living.
Services
Residential care homes. Services include supervision; arrangement of appointments; crisis intervention; supervision in activities of daily living, nutrition, and medications and provision of or arrangement for transient medical care with licensed home health care providers; access to community services; and room and board.
If a resident's health status changes permanently to non-mobile or the resident requires medical or nursing care on an ongoing basis, the home must either provide medical or nursing care from a licensed home health care provider on a contract basis; seek licensure to provide a higher level of care; or transfer the resident to another facility where medical and nursing care are available.
The home is responsible for arranging the provision of additional services to residents requiring care during a temporary episodic illness or convalescence following acute hospital care.
Supported residential care facilities provide housekeeping; verbal and physical assistance with ADLs; nutrition monitoring; meals; personal supervision when required to offset cognitive deficits that pose a risk to self or others; assistance with medications (verbal prompting, reminding, and some physical assistance); and provision for administration of medications by appropriately licensed persons directly or by contract with a licensed home health agency and for treatments ordered by a physician. Facilities shall provide or arrange with a licensed home health agency for short-term intermittent nursing care and less than 24-hour nursing or other medical monitoring care on an ongoing basis.
Dietary
Staff responsible for food service must have knowledge of nutritional requirements and planning and preparation of prescribed diets. Facilities must provide three or more meals a day and snacks between meals and before retiring that meet the recommended dietary allowances of the National Research Council.
Agreements
Agreements must list the service provided, additional services available and their cost, house rules, bed hold policy, grounds for termination of the agreement, and the notification required for involuntary transfer for emergency situations.
New Hampshire implemented legislation in 2003 requiring disclosure of information to allow residents to compare assisted living residences, independent retirement communities and elder housing and make informed choices. Regulations and a standard form were issued by the licensing agency. The rules require disclosure of whether the facility is licensed, the amount of the basic rate, the services included in the rate (e.g., assistance with specific ADLs, monitoring and supervision of medications, administration of mediations, personal laundry services (number of loads per week), housekeeping services; meals provided, transportation services, recreation and leisure activities, amenities in the living unit, and staffing (24-hour availability, licensed nurse, personal care attendant, nursing assistant and maintenance staff availability; deposits/advance payment requirements and refundability; and services not included in the basic rate and their cost.
Provisions for Serving People with Dementia
Disclosure requirements for all licensed facilities apply to those serving people with dementia. The revised regulations will contain provisions for serving people with dementia.
Medication Administration
Administration of medications by licensed staff is allowed.
Public Financing
A Medicaid waiver was approved in 1999 that includes assisted living. The State also has provided a state SSI supplement for residential care facilities since the 1980s that currently totals $758 a month (federal and state) to pay for room and board, which includes a PNA of $50. Assisted living coverage is available in both non-licensed subsidized housing sites and licensed facilities. The State uses a flat Medicaid payment of $1,250 a month for services in residential care facilities and $50 per day in non-licensed elderly housing programs, including room and board paid by the resident. Family supplementation is allowed. Five of the 42 participating facilities are licensed and they serve 36 residents. The rest are elderly housing buildings.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participants | Facilities | Participants | Facilities | Participants |
| 42 | 176 | 37 | 178 | NA | NA |
Staffing
Administrators must be at least 21 and never convicted of a misdemeanor or felony. Administrators of facilities licensed for four to sixteen beds must have a high school diploma or GED plus one year of work experience in a health field or an associate’s degree from an accredited college or university in a health field.
Administrators of residential care homes licensed for 17 or more residents must have a high school diploma plus five years of direct care experience; an associate’s degree from an accredited college or university, plus three years of experience in a health or human services field; or a bachelor’s degree in a health field.
Residential care homes do not require medical directors or directors of nursing. Other staff must be at least 18 years old if they provide direct care.
Training
Administrators must have 12 hours of continuing education each year.
Staff. Personnel shall have orientation and training in the performance of their duties and responsibilities which includes job description requirements, fire safety and evacuation, medical emergency protocol, resident rights, and facility tour and familiarization. Ongoing in-service training or continuing education must be provided to address areas of weakness identified during annual performance review. In-service training shall also address new or special needs of residents and shall include training in medication supervision or administration; first aid; behavior management; personal care; fire safety and evacuation; socialization; and resident rights.
Background Check
Staff may not have been convicted of a felony and never have been convicted of abuse, assault, neglect, or exploitation of any person. A signed statement by the employee is acceptable documentation for conviction of abuse, assault, neglect, or exploitation. As of July 1, 2003 prior to a final offer of employment being made, the facility must have received and reviewed the results of criminal conviction record the division of state police.
Monitoring
The licensing agency conducts annual inspections of facilities.
Fees
$2.50 per bed.
New Jersey
Citation
Assisted Living Chapter NJAC 8:36
General Approach and Recent Developments
Regulations creating assisted living programs (ALP) in subsidized housing sites were effective in August 1996 that permit licensed service agencies to deliver services in subsidized elderly housing projects. Creating this category allows nurses to delegate medication administration, which is not allowed for regular home and community based services providers.
The regulations expire in 2004 and revisions will be published in the Fall. Some of the issues receiving attention are assessments and care planning, the resident agreement, staffing requirements, and residents’ rights. Results from a survey and the oversight process are being used to identify regulations that need to be reviewed.
The original rules governing the provision of assisted living services in assisted living residences and comprehensive personal care homes took effect in December 1993 and were revised in 1999. The regulations promote aging in place in homelike, apartment style settings for frail elders. The purpose section of the regulations describes the goals of assisted living to “maintain independence, individuality, privacy, dignity” in an environment that “promotes resident self direction and personal decision making while protecting health and safety.” The Department of Health and Senior Services permits medication administration by unlicensed personnel through the Registered Professional Nurse delegation process.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted living residences | 152 | 13,696 | 129 | 11,645 | 91 | 8,072 |
| Comprehensive personal care homes | 43 | 2,388 | 41 | 2,642 | 29 | 1,752 |
| Assisted living program | 13 | NA | 17 | NA | 16 | NA |
All new construction is purpose built, apartment style units. Only facilities licensed by the Department of Health and Senior Services prior to December 1993, the effective date of the assisted living regulations, can convert to comprehensive personal care homes and offer bedrooms rather than apartment style units with a kitchenette. The State has adopted an expedited certificate of need review for assisted living residences.
Definition
Assisted living “means a coordinated array of supportive personal and health services, available 24-hours per day to residents who have been assessed to need these services, including residents who require formal long-term care. Assisted living promotes resident self direction and participation in decisions that emphasize independence, individuality, privacy, dignity and homelike surroundings.”
Assisted living residence means a facility which is licensed by the Department of Health and Senior Services to provide apartment-style housing and congregate dining and to assure that assisted living services are available when needed, for four or more adult persons unrelated to the proprietor. Apartment units offer, at a minimum, one unfurnished room, a private bathroom, a kitchenette, and a lockable door on the unit entrance.
Comprehensive personal care home means “a facility which is licensed by the Department of Health and Senior Services to provide room and board and to assure that assisted living services are available when needed, to four or more adults unrelated to the proprietor. Residential units may house no more than two residents and have a lockable door on the unit entrance.”
Assisted living program (ALP) “means the provision of or arrangement of meals and assisted living services, when needed, to the tenants of publicly subsidized housing which because of federal, state or local housing laws, regulations or requirements cannot become licensed as an assisted living residence. An assisted living program may also provide staff resources and other services to a licensed assisted living residence and a licensed comprehensive personal care home.” In these instances, ALPs must comply with the licensing standards that are appropriate to the setting.
Unit Requirements
Each assisted living residence unit must offer a minimum 150 square feet (single occupancy) of clear and useable floor area (excluding closets, bath, and kitchen); private bathroom; a kitchenette; and a lockable door on the unit entrance. The kitchenette must include a small refrigerator, cabinet for food storage, sink, and space with outlets suitable for cooking appliances such as a microwave, cook top, or toaster oven. An additional 80 square feet of floor space must be provided for a second person occupying a unit. No more than two people may occupy a unit.
Comprehensive personal care home units must provide 80 square feet for single occupancy units and 130 square feet if the unit is occupied by two people. While a locked door is required, private baths and kitchenettes are not required.
Assisted living programs are licensed as a service. Requirements for the apartments in subsidized housing projects are specified by the source of financing and the building code.
Admission/Retention Policy
Assisted living is not appropriate for people who are not capable of responding to their environment, expressing volition, interacting, or demonstrating independent activity. Each resident receives an assessment and a care plan by a registered nurse. The residence may, but is not required to, care for people who require 24-hour, seven-day-a-week nursing supervision; are bedridden longer than 14 days; are consistently and totally dependent in four or more ADLs; have cognitive decline that interferes with simple decisions; require treatment of Stage III or IV pressure sores or multiple Stage II sores; are a danger to self or others; or have a medically unstable condition and/or special health problems. The facility must describe the assessment process and the manner in which the resident and/or his or her family will be involved. Managed risk agreements are negotiated, when appropriate, based on resident actions, choice, or preferences. Within 36 months of licensing, at least 20 percent of the residents in each licensed facility must have nursing home level of care needs.
Facilities may not serve residents who require a respirator or mechanical ventilator or people with severe behavior management problems, such as combative, aggressive, or disruptive behaviors.
Nursing Home Admission Policy
Nursing home (NH) level of care means care, treatment and services that may be provided to individuals who have chronic or unstable medical, emotional, behavioral, psychological, or social conditions resulting in the inability to care for themselves independently and/or safely. Individuals who require NH level of care are those who are fully or partially dependent in several Activities of Daily Living (ADLs), including bathing, dressing, eating, toileting, and mobility. Nursing facility level of care services allow the individual to reach his or her highest physical, mental, emotional, and functional level and also prevent unnecessary deterioration.
Services
The residence must provide personal care and provide or arrange for other services. The minimum service capacity must include personal care, nursing, pharmacy, dining, activities, recreation, and social work services to meet the individual needs of residents. Supervision, assistance with, and administration of medications by trained and supervised personnel is also required. Facilities must also be capable of providing or arranging for the provision of nursing services to maintain residents.
ALPs require contracts between service providers and the housing entity. The contracts provide that tenants will not be barred from participation because of the location of a unit and cannot be moved because of their participation. Housing owners/managers must agree to the provision of services. ALPs shall be capable of providing or arranging for assistance with personal care, nursing, pharmaceutical, dietary, and social work services, as well as transportation and recreational activities. Managed risk agreements are used when appropriate and agreed to by all relevant parties.
The rules define bounded choice, managed risk and managed risk agreements. “Bounded choice” means limits placed on a resident’s choice as a result of an assessment, in accordance with N.J.A.C. 8:36-4.17, which indicates that such resident’s choices or preferences place the resident or others at a risk of harm or lead to consequences which violate the norms of the facility or program or the rights of others.
“Managed risk” means the process of balancing resident choice and independence with the health and safety of the resident and other persons in the facility or program. If a resident’s preference or decision places the resident or others at risk or is likely to lead to adverse consequences, such risks or consequences are discussed with the resident, and, if the resident agrees, a resident representative, and a formal plan to avoid or reduce negative or adverse outcomes is negotiated, in accordance with the provisions of N.J.A.C. 8:36-4.17.
“Managed risk agreement” means the written formal plan developed in consideration of shared responsibility, bounded choice and assisted living values and negotiated between the resident and the facility or program to avoid or reduce the risk of adverse outcomes which may occur in an assisted living environment.
Dietary
Facilities must designate a food service coordinator who is either a dietician or has scheduled consultation from a dietician. If indicated by resident needs, a dietician shall be responsible for assessing nutritional needs, providing dietary services, reassessing needs, and revising the dietary portion of the health plan as needed. Three meals a day, snacks, and beverages are required based on the current recommended dietary allowances of the Food and Nutrition Board. Menus should reflect nutritional and therapeutic needs, cultural backgrounds, food habits, and personal preferences.
Agreements
Admission interviews cover the facility’s program and policies, business hours, fee schedule, services provided, resident rights, and criteria for admission and discharge. The admission agreement has to specify if the facility will retain residents with one or more of the characteristics listed above, to what extent, and the additional costs which may be charged. Documentation is included in the resident’s record. Agreements include all fees for services provided.
Provisions for Serving People with Dementia
No separate requirements.
Medication Administration
Residences are allowed to provide supervision of and assistance with self-administration of medications and administration of medications by trained and supervised personnel. Registered nurses may delegate medication administration to medication aides who are personal care assistants who have completed required training and passed a written test.
Delegation is based upon individual residents' needs and circumstances for oral, ophthalmic, otic, inhalant, nasal, rectal, vaginal, topical and injectable (subcutaneous) medication. Short term scheduled medications (II-IV) for analgesia, (pre-drawn insulins are the only injectables allowed) must be reassessed by the registered nurse at least every 72 hours, in order to determine if the medication is still required.
Public Financing
Elders and people with physical disabilities have been served through a Medicaid Waiver since 1996 in four settings: Assisted Living Residence, Comprehensive Personal Care Home, Assisted Living Program, or the Adult Family Care program. The number of people who can be served is 2,250. The bulk of the participants are in the facility based Assisted Living Residences (102 facilities with 1,416 participants) and the Comprehensive Personal Care Homes (41 facilities with 629 participants). A law was passed requiring that facilities licensed after September 2001 set aside 10 percent of their units to serve Medicaid residents within three years of licensing. The requirement shall be waived if there is a waiting list for Medicaid waiver services. Rules implementing the law will be final in April 2004. The regulations affect about 60 facilities of which 67% already participate in the Medicaid program.
Rates have been developed for each of the three licensing settings. Assisted living residences receive $630.55 for room and board from the resident’s monthly income and $1,800 a month for Medicaid services. Assisted living programs receive up to $1,200 a month (if the person is a resident for the entire month) for services. Residents are charged a percentage of their income for room and board. Comprehensive personal care homes receive $630.55 for room and board and up to $1,500 a month for services.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participants | Facilities | Participants | Facilities | Participants |
| 159 | 2,195 | 118 | 1,500 | 68 | 699 |
The SSI payment standard in assisted living is $714.05 and the personal needs allowance is $83.50. The State uses the 300 percent option for Waiver eligibility with a maintenance allowance of $714.05 a month. Facilities are not allowed to charge a higher amount for room and board to Medicaid residents with incomes that exceed the SSI payment standard. Income supplementation is allowed but only to allow a resident to occupy a larger unit. The State tracks the number of residents receiving supplementation. Forty nine facilities have received approval to receive supplements. About eight percent of the residents benefit from a supplement that averages $567 a month.
| Assisted Living Residences |
Assisted Living Programs |
Comprehensive Personal Care Homes |
|
|---|---|---|---|
| Room and board | $630.55 | NA* | $630.55 |
| Medicaid waiver services | $1,800.00 | $1,200.00 | $1,500.00 |
| Total | $2,430.55 | $1,200.00 | $2,130.55 |
| NOTE: Assisted living residents live in subsidized housing and are charged a percentage of their income for rent. Room and board amount for residents in ALRs and CPCHs does not include a personal needs allowance of $83.50 a month. | |||
Staffing
The regulations require at least one awake personal care assistant and one additional staff at all times and sufficient staffing to provide the services indicated by the assessments of resident needs. A registered nurse must be available on staff or on call 24 hours a day. ALPs must have policies which assure that at least one staff member of the ALP or the housing program is on-site 24 hours a day.
Training
Administrators in all three licensed settings must be licensed as a nursing home administrator or complete an assisted living training course, or other equivalent training, as approved by the Department and shall pass a state examination. The course includes 40 hours of classroom training and a 16-hour practicum. The administrator must also participate in at least 20 hours of continuing education every two years regarding assisted living concepts and related topics, as specified and approved by the Department of Health and Senior Services or the New Jersey Nursing Home Administrators Licensing Board.
Staff. Each personal care assistant (PCA) shall have completed:
- A nurse aide training course approved by the Department and shall have passed the Nurse Aide Certification exam; or
- A homemaker-home health aide training program approved by the Board of Nursing and shall be so certified; or
- Other equivalent training program approved by the Department.
Each PCA shall receive orientation prior to or upon employment as well as ongoing in-service education regarding the concepts of assisted living, emergency plans and procedures, and the infection and prevention program. Personal care aides must have twenty hours of training every two years, and medication aides ten hours every two years.
Background Check
Administrators must be of good moral character, good physical and mental health, and must exhibit concern for the safety and well being of residents. Facilities shall exercise good faith and reasonable efforts to ensure that staff have not been convicted of a crime relating adversely to the person’s ability to provide resident care such as homicide, assault, kidnapping, sexual offenses, robbery, and crimes against family, children, or incompetents, except where the applicant has demonstrated rehabilitation.
Monitoring
Not described.
Fees
ALR/CPCH: $1,500 plus $15 per bed for licensing; $150 annual licensing fee and a $1,500 biennial inspection fee.
ALP: $1,125.00license and annual renewal fee; $750 biennial inspection fee.
New Mexico
Citation
Adult residential care facilities, NMAC Title 7 Chapter 8 Part 2
Assisted living (Medicaid)
General Approach and Recent Developments
A committee was formed in 2003 to review the current regulations. This committee is in the final stages of its review. The primary issues being addressed include educational requirements for administrators and staff, and redefining ownership. The revisions are expected to be final by the end of 2004.
Assisted living is covered as a Medicaid waiver service. Providers may be licensed as adult residential care homes or as new or innovative programs.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Adult residential care | 346 | NR | 305 | NR | 255 | NR |
Definition
Adult residential care facility means any congregate residence, maternity shelter, or building for adults, whose primary purpose is to provide to residents, within the facility, either directly or through contract services, programmatic services, room, board, assistance with activities of daily living, in accordance with the program narrative, and/or general supervision to two or more adults who have difficulty living independently or managing their own affairs.
Assisted living is a special combination of housing and personalized health care services designed to respond to the individual needs of Medicaid waiver recipients who require assistance with activities of daily living (e.g., ability to perform tasks that are essential for self care, such as bathing, feeding oneself, dressing, toileting, and transferring) and instrumental activities of daily living (e.g., ability to care for household and social tasks to meet individual needs within the community). Assisted living is based on the following fundamental principles of practice: individuality, independence, privacy, dignity, choice, and a home-like environment. Assisted living services are packaged per individual recipient needs.
Unit Requirements
Resident rooms may be private or semi-private. Private rooms must have at least 100 square feet of floor area, not including closets and locker areas. Semi-private rooms shared by no more than two people must have at least 80 square feet of floor area per bed, not including closets and locker areas. Facilities serving people with alcohol or drug dependency may offer wards or dormitories that have 60 feet of floor area for each bed. Toilets, sinks, tubs, and showers must be provided in ratios of one for every eight residents. All facilities must have a minimum of 1 toilet and bathing facility which meets requirements for people with disabilities.
Medicaid Services must be provided in “home-like” environments which are defined as:
-
A minimum of 220 square feet of living and kitchen space (not including bathroom) for newly constructed units (rehabilitated units must provide a minimum of 160 square feet).
-
Adult residential shelter care homes must provide 100 square feet of floor area in a single bedroom (excluding closet/locker). Recipients must have access to a common living area, kitchen, and bathroom which are handicapped accessible. Eighty square feet is required for semi-private bedrooms.
Admission/Retention Policy
No resident shall be admitted or retained who is below the age of eighteen or for whom the facility is unable to provide appropriate care. The one exception is maternity shelter facilities. Facilities may not admit or retain anyone requiring continuous nursing care which includes ventilator dependency, Stage III or IV pressure sores, intravenous therapy or injections directly to veins, airborne infectious diseases, conditions requiring physical or chemical restraints, nasogastric tubes/gastric tubes, tracheotomy care, individuals presenting an imminent physical threat or danger to self or others, or individuals whose physician certifies that placement is no longer appropriate. Exceptions are allowed when a team (director, resident, agent, advocate, physician, other health professional) jointly agrees and approves a service plan identifying needs and how they will be met, ensuring maintenance of the facility’s evacuation rating and the well-being of others.
Nursing Home Admission Policy
Medical eligibility is based on nursing facility level of care general criteria and one or more clinical status factors. The general criteria require that two or more activities of daily living (ADLs) cannot be accomplished without consistent, ongoing, daily provision of some or all of the following levels of service: skilled, intermediate, and/or assistance. The functional limitations are secondary to a condition for which general treatment plan oversight of a physician is medically necessary. The clinical factors are medications, respiratory therapy and supplemental oxygen, ventilator care, ostomy care, management of decubitus ulcers, dressings, specialized rehabilitative or restorative care by qualified therapists, and “other” services such as organic brain damage, dementia, and spinal cord injury.
Services
Facilities must supervise and assist residents as necessary with health, hygiene, and grooming needs to include but not be limited to eating, dressing, oral hygiene, bathing, grooming, mobility, and toileting. Recreation/social activities, three meals a day, laundry, and housekeeping must be provided. Facilities must provide or arrange for housekeeping, laundry, and transportation services.
A resident assessment must be completed within 5 days of admission and reviewed every 6 months as part of the individual service plan. The resident assessment must establish a baseline in the resident's functional status and thereafter identify resident changes through periodic reassessments.
An individual service plan, if prompted by the resident assessment, shall be developed and implemented within 14 days of admission, and must address those areas of need as identified in the resident assessment. The individual service plan must be reviewed by a licensed nurse at least every 6 months, and revised as needed at the time of each assessment and consistently implemented in response to the resident's needs. The individual service plan must include the following:
-
Description of identified need as noted in the resident assessment.
-
Written description of what services will be provided.
-
Who will provide the services.
-
When or how often the services will be provided.
-
How the services will be provided.
-
Where the services will be provided.
-
Goal and outcome of the service.
-
Documentation of the facilities determination that it is able to meet the needs of the resident.
Medicaid. An inter-disciplinary team develops an individualized service plan (ISP) which is approved by the Department of Health waiver staff. Staff from the facility participate as a member of the team and attend team meetings.
Core services provide minimum to moderate assistance and include at a minimum: bathing, dressing, eating, personal hygiene, behavior management, opportunities for individual and group interaction, housekeeping, laundry, transportation, meal preparation and dining, 24-hour response capability to meet routine scheduled care as well as unscheduled, unpredictable needs of the recipients, capacity to provide on-going supervision of the waiver recipient within a 24-hour period, service coordination capability to arrange access to services not provided directly, provider participation in the interdisciplinary team meetings for development of the individualized service plan, and demonstrated capability to address the most common dementia related problems (e.g., memory loss, depression, sleep disorders).
In addition to the above core services, providers may provide personal services (specialized bowel and bladder program and catheter care); private duty nursing (medication management, nursing services such as injections, wound care, health status monitoring and assessment); skilled maintenance therapies (physical therapy, occupational therapy, speech); emergency response services; and other support services authorized by the Department of Health designed to maintain independence.
Services may be provided by the facility or another approved waiver provider.
Dietary
Facilities must provide three nutritionally balanced meals and evening snacks in accordance with the recommended daily dietary allowances from the basic food groups. Therapeutic diets and prescribed vitamin and mineral supplements may be given according to physician orders. Training must be appropriate to staff responsibilities.
Agreements
The agreement covers the scope of services to be provided, the cost of services and method of payment, circumstances under which the agreement can be terminated, and the bed-hold policy. A new agreement is required when services, costs, or other material terms change. An admission/discharge agreement may provide for termination by the facility when the resident's health has improved sufficiently so the resident no longer needs the services provided by the facility. Termination of an admission agreement by the facility is permitted in emergency situations for the following reasons: the transfer or discharge is necessary for the resident's welfare and the resident's needs cannot be met in the facility; the safety or health of individuals in the facility is endangered; the resident has failed to pay for a stay at the facility, as defined in the admission agreement; the facility ceases to operate or is no longer able to provide services to the resident; and due to sanctions or remedies imposed by the Department.
Provisions for Serving People with Dementia
Not specified.
Medication Administration
Medications may be administered by licensed health care professionals. Staff who have completed an approved training program may assist with medications if given permission by the resident or resident representative. Facilities must have a consulting pharmacist who reviews medications at least quarterly.
Public Financing
The HCBS Disabled and Elderly Waiver serves elders and people with disabilities. Facilities receive a flat rate of $50.50 per day (excluding room and board). Room-and-board charges are the responsibility of the recipient. The waiver sets eligibility at 300 percent of the federal SSI payment. Income supplementation is allowed.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participants | Facilities | Participants | Facilities | Participants |
| NR | 189 | NR | 76 | NR | 41 |
Staffing
Adult residential facilities. The facility must employ staff capable and trained to provide the basic care and resident assistance and supervision required, based on the assessment of the residents needs, and must employ an administrator. Direct care staff must be at least eighteen years of age. When residents are awake, all facilities must have at least one direct care staff person on-duty and awake for each 15 residents. During resident sleeping hours, facilities with 15 or fewer residents must have at least one direct care staff person on duty and responsible for the care and supervision when residents are in the facility. Facilities with 16 to 60 residents: at least one direct care staff person awake at all times and at least one additional staff person available on the premises while residents are sleeping. Facilities with 61 to 120 residents: two direct care staff persons awake at all times and at least one additional staff person immediately available on the premises when residents are sleeping. Facilities with more than 120 residents: at least 3 direct care staff persons awake at all times and one additional staff person immediately available on the premises for each additional 40 residents or fraction thereof in the facility.
The waiver guidelines require staffing ratios and patterns that will meet the individual recipient's needs as identified in the ISP.
Training
Administrators must be 21, demonstrate respect for residents, have a high school diploma or equivalent and have proven their ability to administer a facility through education or experience. Administrators must be able to communicate with the residents and other staff members in the language spoken by the majority of the residents and other employees.
Staff training, appropriate to staff responsibilities, includes, at a minimum, an orientation and an on-going, but at least annual, program which includes: fire safety; first aid; safe food handling practices; confidentiality of records and resident information; infection control; resident rights; reporting requirements on abuse, neglect, and exploitation; transportation safety for assisting residents and operating vehicles to transport residents; and providing quality resident care based on current resident needs.
Qualifications of personal care assistants. Each personal care assistant shall have completed:
- A nurse aide training course approved by the Department and shall have passed the Nurse Aide Certification exam; or
- A homemaker-home health aide training program approved by the Board of Nursing and shall be so certified; or
- Other equivalent training program approved by the Department.
Each personal care assistant shall receive orientation prior to or upon employment and ongoing in-service education regarding the concepts of assisted living.
Background Check
Applicants for the administrator position must comply with the requirements of the New Mexico Caregivers Criminal History Screening Act.
Monitoring
The Licensing Authority must perform on-site survey/monitoring visits at all adult residential care facilities to determine compliance with the regulations, to investigate complaints, or to investigate the appropriateness of licensure for any alleged unlicensed facility. If violations of the regulations are cited, the licensee or facility designee is provided with an official written report of the findings at the completion of the survey/monitoring visit or within ten working days following the visit. The Licensing Authority may utilize a committee comprised of interested parties including but not limited to advocacy, provider, consumer and state agency representation. The committee shall advise the state agency on facilities’ written requests. The licensee or facility designee shall submit a plan of correction at the time of the survey/monitoring visit or within ten working days of receipt of the official written report citing the violations. The plan of correction must: address how all violations identified in the official written report will be corrected; how the facility will identify other residents having the potential to be affected by the same deficient practice; how the facility will monitor its corrective action; specify a date upon which the corrective action will be completed. Cited violations must be corrected within thirty days from the date the survey was completed, unless the Licensing Authority approves otherwise. The Licensing Authority may accept, reject, or negotiate modifications to the plan of correction.
Fees
$30 per facility.
New York
Citation
Adult care facilities, NY Social Service Law (SSL) Article 7, Title 2
Adult homes, 18 NY Codes Rules & Regulations Part 487
Enriched housing programs, 18 NYCRR Part 488
Residences for adults, 18 NYCRR Part 490
Assisted living program, NY SSL §461-1.; 18 NYCRR Part 494
General Approach and Recent Developments
The State approaches assisted living as a service option within certain existing adult care facilities. “Assisted Living Programs” (ALPs) must be dually-certified as an adult home or enriched housing program (the housing component) and either a home care services agency, a certified home health agency, or a long-term home health care agency (the service component).
Adult homes and enriched housing programs are both certified under the State's adult care facility regulations. Both models serve five or more people and provide long-term residential care, room, board, housekeeping, personal care, and supervision. Adult homes represent the State's board-and-care model while enriched housing programs operate in community integrated settings resembling independent housing units. State statute authorizes the Medicaid program to contract for 4,200 ALP beds, most of which have been allocated. While the majority of ALP beds are in adult homes, the demand from “enriched housing” providers is increasing among purpose built facilities rather than conventional elderly housing sites.
In August 2004, the legislature passed the “assisted living reform” act, S7748, which creates a clear and flexible statutory structure, defines assisted living residence, requires a written residency agreement that contains consumer protections, enunciates and protects resident rights and provides adequate and accurate information to consumers. Assisted living residences must also hold a license as an adult care home or an enriched housing program. A ten member task force will be established by December 1, 2004 to develop regulations implementing the new law.
Recommendations from a workgroup formed to discuss policy, program and financing reforms for adult care facilities were submitted to the Commissioner of Health in October 2002. Regulations based on the recommendations were issued in 2004.
Several new State initiatives supported by the Governor are currently being implemented. These initiatives to improve the lives of adult home residents include clinical, psychiatric and functional assessments by highly qualified and trained health and mental health care providers; improved case management and coordination to assure that appropriate care and services are delivered; enhanced medication management system which better ensures that medication is being administered by qualified personnel; improved social and recreational services; and increased advocacy and legal support.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Adult care homes | 431 | 32,859 | 449 | 34,805 | 453 | 33,589 |
| Enriched housing program | 90 | 7,227 | 83 | 5,308 | 44 | 3,147 |
| Residences for adults | 6 | 200 | 8 | 345 | 8 | 464 |
Definition
Assisted living and assisted living residence (S 7748) means an entity which provides or arranges for housing, on-site monitoring, and personal care services and/or home care services in a home-like setting to five or more adults residents unrelated to the assisted living provider. An applicant…must also provide daily food service, twenty-four hour on-site monitoring, case management services, and the development of an individualized service plan for each resident. An operator shall provide each resident with considerate and respectful care and promote the resident’s dignity, autonomy, independence and privacy in the least restrictive and most home-like setting commensurate with the resident’s preferences and physical and mental status.
Enhanced assisted living certificate (S7748) means a certificate…which authorizes a residence to provide aging-in-place by retaining residents who are chronically chairfast and unable to transfer without the physical assistance of another person; chronically require physical assistance to walk, climb or descend stairs; are dependent on medical equipment and require more than intermittent or occasional assistance from medical personnel; or have chronic unmanaged urinary or bowel incontinence.
Adult care facilities (ACFs) are generally viewed as personal care settings for persons with functional impairments occasioned by age or by physical or cognitive disability. While there are by statute five different types of ACFs, the Department of Health has oversight authority for three: adult homes, enriched housing programs, and residences for adults. The other two types, shelters for adults and family-type homes, are overseen by the State Office of Temporary and Disability Assistance (OTDA) and the Office of Children and Family Services (OCFS), respectively.
An adult home is established and operated for the purpose of providing long-term residential care, room, board (three meals and a nutritious snack per day), housekeeping, personal care, and supervision to five or more adults unrelated to the operator. While adult homes serve persons at least 18 years of age, most residents are much older than 18. These are congregate settings in that they can accommodate large numbers of residents in one building--up to 200 residents in one facility (some “grandfathered” facilities accommodate more), typically with one or two residents to a bedroom. Adult homes may be proprietary, public, or non-profit.
An enriched housing program means an adult care facility established and operated for the purpose of providing long-term residential care to five or more adults, primarily persons 65 years of age or older (no more than 25 percent under 65 and all are 55 or older), in community integrated settings resembling independent housing units. Most programs are located in individual apartment settings that have kitchens and private bathrooms. Services provided are the same as those in adult homes, with the exception of supervision and personal care. An enriched housing operator is required to provide only one meal a day, which must be a hot congregate meal, and the operator must assure that there is sufficient food available in each resident’s apartment for the other two meals.
Residences for adults serve a population that is younger than that served by adult homes and enriched housing programs and generally needs a different array of services, including mental health services provided under the auspices of the Office of Mental Health (OMH). Services that must be provided by the operator of the residence include room, meals, housekeeping, case management and 24 hour-a-day supervision. Operators are not required to provide personal care. While most resident rooms are single, some are double-occupancy. Bathrooms may be shared and there is a communal dining room for meals.
Assisted Living Program (ALP) (Medicaid program) is available in some adult home and enriched housing programs, and combines residential and home care services. It is designed for individuals who may otherwise require nursing home placement for what are primarily social rather than medical reasons. The operator of the ALP is responsible for providing or arranging for resident services that must include room, board, housekeeping, supervision, personal care, case management, and home health services. While the ALP is primarily a Medicaid-funded program, some non-Medicaid ALP beds do exist.
Unit Requirements
Adult homes provide single or double occupancy bedrooms and have one toilet and lavatory for every six residents and one tub/shower for every ten residents.
Enriched housing programs must provide single occupancy units, unless shared by agreement, and each unit must include a full bathroom, living and dining space, sleeping area, and equipment for storing and preparing food. Shared units must provide for toilets, lavatory, shower, or tub shared by not more than three residents.
Residences for adults provide single or double occupancy bedrooms, with shared bathrooms and communal dining rooms.
Assisted living programs comply with the relevant requirements under which the contracting facility is licensed (i.e., adult home or enriched housing program).
Admission/Retention Policy
Adult care facility (ACF) operators may not accept or retain anyone who: requires continual nursing or medical care; suffers from a serious and persistent mental disability sufficient to warrant placement in an acute care or residential treatment facility; is a danger to self or others; requires continual skilled observation; refuses or is unable to comply with treatment; is chronically bedfast or chairfast and requires assistance from another person to transfer; regularly needs assistance from another person to walk or climb and descend stairs; has chronic un-managed urinary or bowel incontinence; has a communicable disease; is dependent on medical equipment (with exceptions); has chronic personal care needs which cannot be met by the staff; is not self-directing; and engages in drug or alcohol use which results in aggressive or destructive behavior.
Assisted Living Program (ALP) To receive Medicaid reimbursement for home care services provided in an ALP, applicants must be determined by a physician to be appropriate for this level of care. Following a review of the assessments, prior authorization must be completed by the fiscally responsible social services district. The social service district may, at their discretion, choose to conduct their own assessment prior to authorizing Medicaid payment. The applicant must then be assessed by the ALP to determine the care required and the program's ability to meet those needs. Participants must have stable medical conditions and be able to assure self-preservation in an emergency.
Assisted living S 7748 allows facilities to apply for an “enhanced assisted living certificate” to support aging in place for residents who are chronically chairfast, unable to walk or climb stairs without physical assistance; depend on medical equipment and require more than intermittent or occasional assistance; or have chronic unmanaged urinary or bowel incontinence.
Services
Adult care facilities can provide supervision, personal care, housekeeping, case management, activities, food service, assistance with medication, and activities under their certificate of operation. To operate as an assisted living program, additional services and licenses are needed. The facility may seek a license to provide nursing care and therapies, or it may contract with a home health agency or a long-term home health care program. A care plan is jointly developed by the ALP and the Certified Home Health Agency/Long Term Home Health Care Program which is based on the physician's orders and the assessment process.
The Medicaid ALP capitation rate covers personal care, home health aide, personal emergency response services, nursing services, physical therapy, occupational therapy, speech therapy, medical supplies that do not require prior authorization, and adult day health care, if needed. A Medicaid recipient's ALP services must not be discontinued solely because the costs of the recipient's care exceed the amount of the capitated payment rate. The ALP must provide case management services to Medicaid recipients who are receiving assisted living program services. The assisted living program must comply with the case management requirements which include receiving referrals for ALP services and providing information about such services; referring an ALP applicant who the program reasonably expects may be eligible for Medicaid to the social services district in which the program is located for a Medicaid eligibility determination; establishing linkages to services provided by other community agencies, providing information about these services to Medicaid recipients; and establishing criteria for referring Medicaid recipients to these services, to the maximum extent possible; achieving economic efficiencies, including, but not limited to using, shared aides consistent with the ALP’s staffing standards, and arranging for the reduction or discontinuance of a Medicaid recipient's services when the ALP reassesses the recipient and determines that the recipient's ALP services must be reduced or discontinued.
All services must be provided in accordance with the recipient's plan of care based upon the recipient's initial assessment and periodic reassessments. When a reassessment indicates that assisted living program services are no longer appropriate, services must continue to be provided in accordance with the recipient's plan of care based upon the recipient's prior assessment until alternative placement arrangements can be made.
Dietary
Adult homes and residences for adults must provide, at a minimum, three meals a day, served at regularly scheduled times, and a nutritious evening snack. The operator shall provide meals which are balanced, nutritious and adequate in amount and content to meet the daily dietary needs of residents.
Enriched housing programs (EHPs) must serve, at a minimum, one hot mid-day or evening meal a day that meets one-third of the recommended dietary allowances of the Food and Nutrition Board. EHPs must also assure that residents receive sufficient food for all non-congregate meals and snacks.
Agreements
Adult care facility admission agreements cover the due dates for payment; list of services, material, equipment, and food required by law or regulation to be provided; the basic monthly, weekly, or daily payment; a detailed schedule of other services, materials, equipment, or food the operator agrees to make available; a guarantee that charges for supplemental services that are made at the resident’s request; conditions for adjusting the rate; the actual rate charged by the operator and accepted by the resident; an offer to manage funds received by SSI or Home Relief residents; a statement that the operator will comply with SSI/Home Relief requirements; charges for temporary absences; conditions of termination; refund policy; statement that the resident will provide a signed medical statement and inform the operator of changes in health conditions, status, or medications; and a statement that the resident will comply with all reasonable rules.
S 7748 requires name, address, phone number of the residence, the owner and operator; the licensing status of the residence; providers of service; the period of the agreement; the services to be provided and the base rate; additional services available for a fee; a rate or fee schedule; process for changing the agreement; the complain resolution process; the name of the resident’s legal representative and their responsibilities; admission/retention criteria; procedures for terminating the contract, discharge and transfer; billing and payment requirements; procedure for non-payment of fees; and refund policy.
In addition to the agreement, the residence must provide a consumer information guide developed by the Department; a statement about the residence’s license and additional certificates; ownership interest in excess of 10% of any entity that provides equipment or services; a statement that the resident is able to obtain services from providers with whom the operator does not have an agreement and their right to choose health care providers; a statement about the availability of public funds; and the availability of the ombudsman.
Provisions for Serving People with Dementia
Facilities may not operate dementia units without written authorization from the Department of Health. In order to obtain written authorization, the operator must submit a complete program proposal and a description of the impact that the program will have on other residents and programs. Approval of the dementia program will be based on: the quality of the proposal; the proposal’s anticipated impact on other residents and programs, if currently certified beds are to be used; site visits if needed to verify compliance; and the demonstrated ability of the facility to provide a consistently high level of care and services to residents.
S 7748 requires that facilities serving people with special needs must submit a special needs plan to the Department that describes the specialized services, staffing levels, staff education and training, work experience, professional affiliations or special characteristics related to the population served, and environmental modifications planned or made. The Department will set standards to ensure adequate staffing and training.
Medication Administration
Assistance with self-administration of medication is allowed, including prompting, identifying the medication for the resident, bringing the medication to the resident, opening containers, positioning the resident, disposing of used supplies, and storing the medication.
Public Financing
Many adult care facility residents pay for room and board through a state supplement to the Federal SSI program. ACF rates for SSI recipients are established in state statute and cover room, board and other required services. Additional support services for SSI-eligible residents, such as personal and home health care, and mental health and medical care, are reimbursed through Medicaid.
Services in Assisted Living Programs are covered under the Medicaid state plan and the SSI state supplement. The Medicaid program will not make payments for ALP services provided to a Medicaid recipient while the recipient is receiving residential health care facility services or in-patient hospital services.
The home care service reimbursement (see attached chart) is based on 50 percent of the resident's Resource Utilization Group (RUG) which would have been paid in a nursing home. The State has created 16 RUG categories for ten geographic areas of the State. Facilities must comply with the adult home retention criteria. However, the full array of rates is shown since facilities receive a higher rate when a resident deteriorates and is retained until a nursing home placement can be made.
The reimbursement category is determined through a joint assessment by the Assisted Living Program and the designated home health agency or long-term home health care program. The assessment and the RUG category are reviewed by the Department of Social Services district office which grants prior authorization of the Medicaid home care payment.
The Medicaid rates do not include room and board. For residents who qualify, residential services (room, board, and some personal care) are covered by SSI which also varies by region. In 2004, the SSI state supplement standards were $999 in New York City, Nassau, Suffolk, and Westchester counties and $969 in the rest of the State. Beneficiaries retain a personal needs allowance of $127.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participants | Facilities | Participants | Facilities | Participants |
| 57 | 3,315 | 53 | 3,034 | 45 | 2,522 |
Staffing
Adult care facilities must have a case manager and staffing that is sufficient to provide the care needed by residents.
Training
Administrators. Program coordinators must be 21 years or older, have a master’s degree in social work and one year’s experience, or a bachelor’s degree and three years of acceptable experience.
Staff providing personal care must complete a personal care aide or home health aide training course or other examination approved by the State Department of Health. Adult care facilities must provide an orientation and in-service training in the characteristics and needs of the population served, resident rights, program rules and regulations, duties and responsibilities of all staff, general and specific responsibilities of the individual being trained, and emergency procedures.
Background Check
Criminal background checks are not currently required of operators of adult care facilities, nor of the staff within those facilities.
Monitoring
Adult Homes. In October 2002, the State implemented new policies regarding the oversight of adult homes. These new policies include: reinforcement of mandatory death reporting by homes and immediate investigations of such reports; multi-agency created profile of deaths at the homes to identify patterns; and increased surveillance, including multi-agency teams comprised of inspectors from Department of Health, Office of Mental Health and Commission on Quality of Care to complete focused surveys. These strong actions serve to further protect adult home residents and serve to make homes more accountable for the care they provide.
Adult care facilities. Inspection and supervision of adult care facilities shall be undertaken by the Department to ascertain whether all applicable provisions of law and regulations are being complied with. The Department may undertake enforcement action against any operator of an adult care facility who fails to operate the facility in compliance with applicable provisions of law and regulation.
Survey reports have to specify corrective action, and surveyors sometimes get into discussions with operators regarding ideas for corrective action. The State does offer training to operators and select staff, and will be offering training in 2004 regarding medication management in ACFs. The State issues “Dear Administrator Letters” (DALs). Since 2002, the State has issued DALs covering the following topics: reporting of deaths, attempted suicides and felony crimes; notice of regulation (failure in systemic practices and procedures); maintenance of safe and comfortable temperature levels within ACFs (Winter AND Summer); influenza prevention and control; establishment of ACF complaint “hotline”; Emergency Preparedness Guidelines; statistical report requirement; case management obligations; facility access by individuals who are not residents; sprinkler head recall; waiver request/equivalency notification; guidelines for dementia units; availability of free or low-cost resources to residents; and notice of law (Long-Term Care Resident and Employee Immunization Act).
Fees
S 7748 sets a biennial fee of $500 plus $50 per residents whose annual income is above 400% of the federal poverty level.
| RUG II Cat. |
Albany | NYC | Syracuse | Rochester | Orange | Long Island |
Erie | West- chester |
Utica | Pough- keepsie |
Bing- hampton |
Elimira | Central Rural |
Western Rural |
Glens Falls |
Northern Rural |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CA | $52.70 | $76.82 | $57.53 | $54.25 | $58.50 | $71.28 | $50.14 | $67.12 | $50.13 | $54.67 | $51.06 | $53.67 | $49.81 | $46.61 | $50.61 | $46.19 |
| BA | $53.29 | $76.34 | $57.13 | $53.77 | $58.06 | $70.82 | $49.76 | $66.59 | $49.81 | $54.22 | $50.69 | $53.37 | $49.44 | $46.26 | $50.28 | $45.92 |
| PA | $45.43 | $64.02 | $48.96 | $46.09 | $49.26 | $59.28 | $42.55 | $56.40 | $42.68 | $46.37 | $43.55 | $45.49 | $42.75 | $39.71 | $42.96 | $39.05 |
| PB | $57.68 | $83.46 | $61.78 | $58.02 | $62.89 | $77.50 | $53.72 | $72.41 | $53.71 | $58.69 | $54.74 | $57.65 | $53.23 | $49.82 | $54.42 | $49.68 |
| RA | $81.26 | $120.38 | $86.40 | $81.25 | $89.14 | $112.10 | $75.24 | $103.18 | $74.87 | $82.49 | $76.27 | $80.84 | $73.46 | $69.33 | $76.37 | $69.93 |
| RB | $88.20 | $131.55 | $93.76 | $88.06 | $96.79 | $122.58 | $81.53 | $112.39 | $81.06 | $89.60 | $82.68 | $87.57 | $79.49 | $74.98 | $82.91 | $75.85 |
| SA | $79.39 | $117.48 | $84.50 | $79.48 | $87.02 | $109.38 | $73.53 | $100.84 | $73.14 | $80.71 | $74.60 | $78.87 | $71.94 | $67.76 | $74.64 | $68.23 |
| SB | $87.03 | $128.65 | $92.29 | $87.25 | $95.57 | $119.85 | $80.58 | $110.63 | $79.96 | $88.43 | $81.50 | $86.23 | $78.46 | $74.24 | $81.54 | $74.65 |
| CB | $68.78 | $101.05 | $73.46 | $68.94 | $75.21 | $94.00 | $63.82 | $87.01 | $63.65 | $69.95 | $64.92 | $68.52 | $62.81 | $58.94 | $64.81 | $59.19 |
| CC | $73.19 | $108.03 | $78.06 | $73.23 | $80.12 | $100.54 | $67.85 | $92.74 | $67.64 | $74.37 | $68.93 | $72.93 | $66.56 | $62.59 | $68.94 | $63.04 |
| CD | $83.44 | $124.04 | $88.79 | $83.38 | $91.51 | $115.54 | $77.19 | $106.17 | $76.79 | $84.79 | $78.32 | $82.89 | $75.40 | $71.06 | $78.46 | $71.76 |
| BB | $63.94 | $93.54 | $68.39 | $64.10 | $69.83 | $86.96 | $59.41 | $80.64 | $59.35 | $65.00 | $60.48 | $63.87 | $58.61 | $54.94 | $60.32 | $55.11 |
| BC | $70.92 | $104.66 | $75.75 | $70.97 | $77.56 | $97.38 | $65.74 | $89.87 | $65.57 | $72.12 | $66.90 | $70.64 | $64.67 | $60.64 | $66.86 | $61.05 |
| PC | $63.94 | $93.54 | $68.39 | $64.10 | $69.83 | $86.96 | $59.41 | $80.64 | $59.35 | $65.00 | $60.48 | $63.87 | $58.61 | $54.94 | $60.32 | $55.11 |
| PD | $68.37 | $100.60 | $73.07 | $68.47 | $74.76 | $93.57 | $63.44 | $86.48 | $63.32 | $69.52 | $64.56 | $68.20 | $62.45 | $58.58 | $64.49 | $58.91 |
| PE | $75.93 | $112.83 | $81.10 | $75.87 | $83.08 | $105.04 | $70.27 | $96.54 | $70.04 | $77.25 | $71.54 | $75.52 | $69.03 | $64.70 | $71.61 | $65.33 |
| CA = CLINICALLY COMPLEX A BA = SEVERE BEHAVIORAL A PA = REDUCED PHYSICAL FUNCTIONING A PB = REDUCED PHYSICAL FUNCTIONING B RA = HEAVY REHABILITATION A RB = HEAVY REHABILITATION B SA = SPECIAL CARE A SB = SPECIAL CARE B |
CB = CLINICALLY COMPLEX B CC = CLINICALLY COMPLEX C CD = CLINICALLY COMPLEX D BB = SEVERE BEHAVIORAL B BC = SEVERE BEHAVIORAL C PC = REDUCED PHYSICAL FUNCTIONING C PD = REDUCED PHYSICAL FUNCTIONING D PE = REDUCED PHYSICAL FUNCTIONING E |
|||||||||||||||
| NOTE: The rates above are based on 50 percent of the nursing home rate. | ||||||||||||||||
North Carolina
Citation
Assisted living residences, NCAC Title 10A Chapter 13 Subchapters F and G; General statute 131D-2
General Approach and Recent Developments
Licensing requirements adopted in 1995 and 1996 established the umbrella term of “assisted living residences” for three types of long-term residential care settings: (1) adult care homes, formerly called domiciliary homes, which must be licensed by the State, (2) group homes for developmentally disabled adults, and (3) multi-unit assisted housing with services which are not licensed, but must be registered with the State. Adult care homes are divided into different types based on size. Family care homes provide care to no more than 6 residents and adult care homes provide care to 7 or more residents. The legislative intent behind licensure for adult care homes is to ensure that facilities provide services that assist the residents in such a way as to assure the health and safety of residents, quality of life, and maximum flexibility in meeting individual needs and preserving individual autonomy.
Several pieces of legislation were enacted in 2001 requiring the following changes: (1) the state licensing agency must develop an adult care home quality improvement consultation program; the Department of Health and Human Services, Division of Facility Services must develop an assessment tool to measure quality of care; and facilities with special care units must file separate cost reports for special care and non-special care units. All legislation was implemented except for the adult care home quality improvement consultation program which has not been formalized to date.
In 2002, the Legislature gave temporary rulemaking authority to the Division of Facility Services through July 2004. The Division formed a rules review committee to receive advice. This committee includes representatives from state and local government, provider associations, and advocacy groups whose charge is to review regulations for all licensure categories and make recommendations for rule amendments, repeals or adoptions. Recommendations are submitted from the Department of Health and Human Services to the Medical Care Commission, the formal rulemaking body for the State of North Carolina.
Changes made through temporary rulemaking are clarification of the discharge rules and compliance requirements, updating food service rules to bring menu requirements in line with current dietary recommendations, food service training, modification of tuberculosis-related rules to assure consistency with state TB control measures, and the reorganization and updating of physical plant requirements. Legislation was passed in 2003 requiring licensure fees for assisted living residences.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Adult care homes | 629 | 35,247 | 631 | 34,776 | 610 | 32,995 |
| Family care homes | 648 | 3,642 | 682 | 3,814 | 743 | 4,134 |
| Multi-unit assisted housing with services | 23 | 1,853 | 20 | 1,538 | NR | NR |
Definition
Assisted living residence means any group housing and services program for two or more adults, by whatever name it is called, which makes available, at a minimum, one meal per day and housekeeping services, and provides personal care services directly or through a formal written agreement with one or more licensed home care agencies. The Department may allow nursing service exceptions on a case by case basis. Settings in which services are delivered may include self-contained apartment units or single or shared room units with private or area baths. Assisted living residences are to be distinguished from nursing homes subject to the provisions of G.S. 131E-102. There are three types of assisted living residences: adult care homes, group homes for developmentally disabled adults, and multiunit assisted housing with services.
Adult care home is a type of assisted living residence in which the housing management provides 24-hour scheduled and unscheduled personal care services to two or more residents, either directly or through formal written agreement with licensed home care or hospice agencies. Some licensed adult care homes provide supervision to persons with cognitive impairments whose decisions, if made independently, may jeopardize the safety or well-being of themselves or others and therefore require supervision. Medication in an adult care home may be administered by designated, trained staff.
There are three types of adult care homes.
- Adult care homes licensed for seven or more beds;
- Family care home: an adult care home licensed for 2 to 6 beds; and
- Group home for developmentally disabled adults: an adult care home which is licensed for two to nine beds for developmentally disabled adult residents.
Note: Almost all group homes for developmentally disabled adults were transferred to licensure under mental health regulations (G.S.122C) in 2000. There are only a few remaining under adult care home licensure (13D-2).
Multi-unit assisted housing with services is defined as “an assisted living residence in which hands-on personal care services and nursing services, which are arranged by housing management, are provided by a licensed home care or hospice agency through an individualized written care plan.” The resident has a choice of any provider, and the housing management may not combine charges for housing and personal care services. All residents, or their compensatory agents, must be capable, through informed consent, of entering into a contract and must not be in need of 24-hour supervision. It is important to note that multi-unit assisted housing with services facilities are only required to register with the Division of Facility Services and to provide a disclosure statement. They are not licensed. The information provided below, unless it specifically references multi-unit assisted housing with services facilities, applies only to licensed facilities.
Unit Requirements
Residential building codes apply to adult care homes serving six or fewer residents and institutional building codes to adult care homes serving more than six residents. Adult care homes may serve up to four residents per bedroom. Bedrooms must be a minimum of 100 square feet, excluding vestibule and closet, for single rooms and 80 square feet per person for multiple occupancy rooms, excluding vestibule, closet or wardrobe space. One bathroom must be provided for every five residents and a tub or shower for every ten residents. Bathroom requirements include hand grips and non-skid surfacing.
Admission/Retention Policy
Adult care homes. Unless a physician determines otherwise, adult care homes may not care for people who are ventilator dependent or require continuous licensed nursing care. They may also not serve individuals whose physician certifies that placement is no longer appropriate, individuals whose health needs cannot be met in the specific adult care home as determined by the residence, and individuals with medical and functional care needs that the Social Services Commission has determined cannot be properly met.
Multi-unit assisted housing with services. Except when a physician certifies that appropriate care can be provided on a temporary basis to meet the resident's needs and prevent unnecessary relocation, multiunit assisted housing with services shall not care for individuals with any of the following conditions or care needs: ventilator dependency; dermal ulcers III and IV, except those stage III ulcers that are determined by an independent physician to be healing; intravenous therapy or injections; airborne infectious disease in a communicable state that requires isolation of the individual or requires special precautions by the caretaker to prevent transmission of the disease; psychotropic medications without appropriate diagnosis and treatment plans; nasogastric tubes; gastric tubes except when the individual is capable of independently feeding himself and caring for the tube, or as managed by a home care or hospice agency licensed in the State; requires continuous licensed nursing care; individuals whose physician certifies that placement is no longer appropriate; is total dependent in four or more of the seven ADLs as determined by a uniform assessment instrument; and individuals whose health needs cannot be met in the specific multiunit assisted housing with services as determined by the residence.
Nursing Home Admission Policy
Level of care decisions are made by nurses employed by the State’s prior authorization fiscal agent. The following factors frequently indicate the need for an intermediate level of nursing home care: services needed by a licensed professional for a minimum of eight hours a day or other personnel working under the supervision of a licensed nurse; daily observation and assessment; restorative measures (e.g., teaching self-care, transfer, and ambulation activities); assistance with ADLs; need for administration and/or control of medications; colostomy-ileostomy care; dressings requiring prescription medications and/or aseptic or sterile techniques; and diabetes.
Other combinations of conditions may also indicate need for an intermediate level of care: minimal assistance with a tracheotomy; need for teaching and counseling; ancillary therapies; injections; treatments; psycho-social considerations; behavioral problems (wandering, verbal disruptiveness, combativeness); verbal or physical abusiveness or inappropriate behavior); frequent falls; or chronic recurrent medical problems that require daily observation.
Services
All licensed facilities are required to provide three meals a day, transportation, activities, and housekeeping services. Licensed facilities may provide personal care directly or through contracts. The Medical Care Commission has the authority to limit what medical and functional care needs cannot be met in adult care homes. Nursing services may be provided by the residence on a case-by-case exception basis approved by the Department of Health and Human Services, or through licensed home care agencies. The resident of an assisted living facility has the right to obtain services from providers other than the housing management, at their own cost. Facilities may provide respite services, but provision of this service is not a condition for licensure. If respite services are provided, the facility must specify the rates for services and accommodations.
Residents in all licensed facilities must receive an assessment within 72 hours of admission using the Resident Register. The facility must complete a functional assessment of each resident within 30 days after admission and at least annually thereafter using an assessment instrument approved by the Department. The assessment is used to determine residents’ functional level, and includes measures of psychosocial well-being, cognitive status, and activities of daily living. Assessments must be completed within 10 days following a significant change in a resident’s condition. The facility must complete a care plan based upon the resident’s assessment within 30 days following admission. The care plan is an individualized written program of personal care for each resident and must include a statement of the care or service to be provided based on the assessment or reassessment, as well as the frequency of service provision.
Assessments and care plans are reviewed during oversight visits to determine whether residents are appropriate for the facility, whether the assessment was appropriately done, whether the plan of care is appropriate, and whether the facility has the capacity to meet the residents’ needs.
Dietary
Licensed facilities must provide three meals a day, snacks, and modified or therapeutic diets ordered by a physician. Menus for modified and therapeutic diets must be planned or reviewed by a registered dietician. The rules describe the content of daily menus.
Agreements
Adult care homes. At admission, the facility must give the resident a contract that specifies rates for accommodations and services, and the period of notice that will be provided for rate changes. Facilities must also provide a copy of house rules, including conditions for discharge or transfer; refund policies; policies on smoking and alcohol consumption; visitation policies; resident rights; grievance procedures; and a statement as to whether the facility complies with the Civil Rights Act.
Residents may be discharged under the following conditions only: for the resident’s welfare and when the resident’s needs cannot be met in the facility; the resident’s condition has improved sufficiently so the resident no longer needs the services provided by the facility; the health or safety of other individuals in the facility is endangered; failure to pay charges for services and accommodations; or discharge is mandated under other rules. All health or safety-related reasons for discharge must be documented by a physician, physician’s assistant, or nurse practitioner.
Multi-unit assisted housing with services programs are required to provide a disclosure statement as part of the annual rental contract. The disclosure statement must include a description of the following: emergency response system; charges for services offered; limitations of tenancy; limitations of services; resident responsibilities; financial/legal relationship between housing management and home care or hospice agencies; a listing of all home care or hospice agencies and other community services in the area; an appeals process; and procedures for required initial and annual resident screening and referrals for services.
Provisions for Serving People with Dementia
Facilities that market themselves as providing a special care unit for persons with dementia must be licensed as such. Facilities that are licensed as a special care unit, or have a section that is so designated on the license are required to provide written disclosure statements. Written disclosure statements must include, but are not limited to the following: a statement of the overall philosophy and mission of the licensed facility and how it reflects the special needs of residents with Alzheimer's disease or other dementias, a mental health disability, or other special needs disease or condition; the process and criteria for placement, transfer, or discharge to or from the special care unit; the process used for assessment and establishment of the plan of care and its implementation, including how the plan of care is responsive to changes in the resident's condition; staffing ratios and how they meet the resident's need for increased care and supervision; staff training that is dementia-specific; physical environment and design features that specifically address the needs of residents with Alzheimer's disease or other dementias; frequency and type of programs and activities; involvement of families in resident care, and availability of family support programs; and additional costs and fees to the resident for special care. Facilities that serve residents with dementia but do not market themselves as special care units are not required to comply with the disclosure provisions.
Special Care Units must have policies that describe their philosophy including the mission and objectives of the unit that address: an environment that promotes mobility and minimal use of restraints; that provides a structured but flexible lifestyle through a well developed program of care that includes activities; individual care plans; methods of behavior management that preserve dignity through design of the physical environment, physical exercise, social activity, appropriate medication administration, proper nutrition, and health maintenance.
Locking devices that meet special requirements may be used. Facilities must provide direct access to a secured outside area and avoid or minimize the use of potentially distracting mechanical noises.
Staffing. At least one staff person is required for every eight residents on the first and second shift and one staff person for every ten residents on the third shift. A care coordinator must be on duty in the unit at least 8 hours a day, 5 days a week. The care coordinator may be counted in the minimal staffing requirements. In units with more than 16 units, the care coordinator must be on staff as described in regulation, but is not counted in determining the minimal staffing requirement. Administrators must have at least 20 hours of training specific to the population served. Employees must have six hours of orientation within one week and 20 hours within six months. Six of the twelve hours of continuing education must be dementia specific.
Medication Administration
Multi-unit assisted housing with services. Assistance with self-administration of medications may be provided by appropriately trained staff when delegated by a licensed nurse according to the home care agency's established plan of care.
Adult care homes. The facility must ensure the development and implementation of written policies and procedures for the ordering, receiving, storage, discontinuation, disposition, and administration of medications, including self-administration of medications. The facility must contact a resident’s physician or prescribing practitioner for verification or clarification of medication orders.
Only staff meeting the medication aide training specified in regulations may administer and prepare medications for administration. Residents are permitted to self-administer medications as long as they are competent and physically able to do so. Self-administered medications must be prescribed by a physician or other person legally authorized to do so and specific instructions for administering medications must be contained on the medication label. Residents may store self-administered medications in their room in a safe and locked area.
Effective October 2000, medication aides who administer medications and staff supervising the administration of medications must successfully pass a written examination prior to or within 90 days of completing a clinical skills validation portion of a competency evaluation. Medication aides and their supervisors must complete 6 hours of continuing education related to medication administration annually. A licensed pharmacist, prescribing practitioner, or registered nurse must perform at least a quarterly review of each resident’s medications and the facility’s medication policies and procedures, or more frequently as identified by the Department based on documentation of specific medication problems in the facility.
Public Financing
Personal care in adult care homes is reimbursed as a state plan service through Medicaid for persons aged 65 and older, and working age adults with disabilities, mental retardation and other developmental disabilities, and mental illness. The program currently serves approximately 24,000 beneficiaries living in 2,200 adult care homes.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participants | Facilities | Participants | Facilities | Participants |
| 2,200 | 24,000 | 2,389 | 18,533 | 2,241 | Not reported |
The maximum State/County Special Assistance (SA) payment for room and board (this is a state SSI supplemental benefit standard that is based on the federal SSI payment and any other sources of income according to established eligibility requirements) is $1,066 a month plus a $46 personal needs allowance. The Medicaid payment varies with the needs of the residents. The payment methodology was modified in January 2004. Medicaid pays for personal care, transportation, and therapeutic leave for all eligible residents. The payment includes a basic amount for personal care (the amount varies for small and large facilities) and an additional “enhanced” payment for residents with heavy care needs. Heavy care means a resident needs extensive assistance or is totally dependent in eating or toileting, or both, and/or ambulation/ locomotion. Eligibility for the additional payment is based on the adult care home’s assessment, which is verified by a county case manager. Medicaid also provides payment for transportation services.
| Factor | Per Diem |
|---|---|
| Basic personal care | |
| 1-30 beds | $16.74 |
| More than 30 beds | $18.34 |
| Eating | +$10.33 |
| Toileting | +$3.69 |
| Eating and toileting | +$14.02 |
| Ambulation/locomotion | +$2.64 |
| Transportation | +$.60 |
The State is in the process of reviewing a new case-mix payment system.
Staffing
At all times there must be one administrator or supervisor-in-charge who is directly responsible for assuring that all required duties are carried out and for assuring that at no time are residents left alone without a staff member. Other staffing requirements vary by the size of the facility and shift. Facilities serving between 20 and 30 residents must have 16 hours of aide time on the first and second shifts and eight on the third shift. The amount of aide hours increases with the size of the facility and reaches 96 hours for facilities with 131 to 140 residents. A supervisor is required for facilities with 31 or more residents.
Training
Administrators. Administrators must be certified. Certification is available for people who are 21 years or older; pass a criminal background check; have completed the equivalent of two years of course work at an accredited college or university, or have successfully completed one year of college and two years of related supervisory experience. Administrators desiring to work in a home with 7 or more beds must complete a 120-hour administrator-in-training course including course work and140 hours of on-the-job training in a facility. Exceptions to this requirement include individuals with a current nursing home administrator’s license or certification from a state requiring comparable certification standards.
Staff. Staff who directly provide personal care or who directly supervise those who do, must complete an 80-hour personal care training and competency evaluation program established by the State. Family care home staff must have a 25-hour training program. Training must be completed within 6 months after hiring for staff hired after September 2003. Licensed health professionals, staff listed on the Nurse Aide Registry, or staff who document completion of a 40-45 hours or 75 - 80 hour training program or competency evaluation program since 1996 are exempt from this training requirement.
The 80-hour training program includes at least 34 hours of classroom instruction and 34 hours of supervised practical experience. The competency evaluation includes observation and documentation, basic nursing skills including special health-related tasks, personal care skills, cognitive and behavioral skills including interventions for individuals with mental disabilities, basic restorative services, and resident’s rights. Experienced staff may take the competency exam without undergoing training.
Facilities must assure that non-licensed and licensed personnel not practicing in their licensed capacity complete a one-time competency evaluation for specific personal care tasks (specified in regulation) before performing these tasks. Facilities must also assure training in the following areas: (1) care of residents with diabetes for unlicensed staff prior to the administration of insulin; and (2) care of residents with medical symptoms that warrant restraints regarding the use of alternatives to physical restraint use, and the care of residents who are physically restrained. Additionally, at least one staff person on the premises at all times must have completed, within the last 24 months, a course on CPR and choking management. Staff designated by the administrator must complete assessment training according to an instruction manual on resident assessment established by the Department.
Background Check
Family care home administrators must provide written documentation about any convictions for criminal offenses from the clerk of court in the county in which the conviction was made, including driving offenses. Administrators of adult care homes of 7+ beds must have a state fingerprint check. Facilities must perform state criminal background checks on all staff, who must have no findings of abuse or neglect listed on the North Carolina Health Care Personnel Registry.
Monitoring
County Departments of Social Services monitor adult care homes at least every other month. State staff provide consultation, technical assistance, and training to the county monitors. State staff also provide monitoring oversight and perform selected surveys of homes based on compliance history or lack of previous county monitoring.
Counties with at least one licensed adult care home must establish a community advisory committee that serves all licensed homes in the county. The committee is responsible for ensuring that residents’ rights are respected and that the overall quality of care is maintained. Rules further specify the function, size, and composition of the committees.
Fees
Adult care homes with 6 or fewer beds: $125.00/year. Adult care homes with 6 or more beds: $175.00/year plus an annual per bed fee of $6.25/bed. The State recently imposed a one-time, per project fee for the review of health care facility construction projects to ensure that the project plans and construction comply with state law. The fee shall not exceed $12,500 for any single project. Adult care homes with more than 7 beds are charged $87.00 plus .05/square foot of project space. Family care homes are charged an $87.00 flat fee.
North Dakota
Citation
Basic Care Facility, NDCC Chapter 23-09.3, NDAC Chapter 33-03-24.1
Assisted living residences, Chapter 50-32 (State Law); Chapter 75-03-34 (Administrative Rules)
General Approach and Recent Developments
A task force was formed to review rules for basic care facilities. Rather than revise the basic care facility rules, the Legislature decided to develop assisted living facility rules. Legislation took effect on August 1, 2003 replacing registration with a new licensing category. The Department of Human Services oversees licensing and rules for assisted living residences. Administrative rules were revised in August 2003 which further defines assisted living. The new rules went into effect in March 2004.
The new category addresses facilities marketed as assisted living that were previously not licensed. Private facilities were not required to be licensed as basic care facilities, as they were viewed as landlord/Admission/retention relationships. However, as more services were provided to individuals residing in such facilities, the State decided to promulgate regulations in 2001 in order to have some oversight of the industry. The State will continually review the regulations and make revisions as necessary as their knowledge of the industry grows.
Legislation authorizing coverage of Medicaid personal care services under the state plan in basic care facilities passed in 2001 (HB 1115). A moratorium on new basic care facilities is still in effect. However, dementia care facilities are exempt from the moratorium. Applications have been received from seven facilities. Four facilities have been approved by the State with 72 new dementia beds. The Department of Health establishes rules for basic care facilities.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Basic care facilities | 46 | 1,490 | 47 | 1,490 | 43 | 1,436 |
| Assisted living facilities | 42 | 1,361 | NA | NA | NA | NA |
Definition
Assisted living facility means any building or structure containing a series of living units operated as one entity to provide services for five or more individuals who are not related by blood or marriage to the owner or manager of the entity and which is kept, used, maintained, advertised, or held out to the public as a place that provides or coordinates individualized support services to accommodate an individual’s needs and abilities to maintain as much independence as possible. It does not include a congregate housing facility or a facility that is licensed as a basic care facility. Assisted living facilities must be licensed.
Basic care residences means “a residence licensed by the Department…that provides room and board to five or more individuals who are not related by blood or marriage to the owner or manager of the residence and who, because of impaired capacity for independent living, require health, social or personal care services, but do not require regular 24-hour medical or nursing services, and makes response staff available at all times to meet the 24-hour scheduled and unscheduled needs of the individual; or, is kept, used, maintained, advertised, or held out publicly as an Alzheimer’s, dementia, or specialty memory care facility to assist the residents to attain or maintain their highest level of functioning, consistent with the resident assessment and care plan, to five or more residents not related by blood or marriage to the owner or manager.”
The primary differences between assisted living residences and basic care facilities are in the way services are defined and delivered. In assisted living residences, tenants enter into a lease agreement with the residence, and purchase services a la carte based on their needs. The residence must disclose what services it will provide and the cost of those services. In basic care facilities, a resident purchases a bundled package which includes room, board, and services. Each resident may have different levels of need however the package of services is the same for everyone.
Unit Requirements
Assisted living residences: There are no unit requirements for assisted living residences. New rules define a living unit as a portion of an assisted living facility occupied as the living quarters of an individual who has entered into a lease agreement with an assisted living facility.
Basic care facility: Single rooms provide 100 square feet, double rooms at least 80 square feet per bed, and rooms for three or more, 70 square feet per bed. At least one toilet is required for every four residents, and one bath for every 15 residents.
Admission/Retention Policy
Assisted living. Participants in the Service Payments for Elderly and Disabled (SPED) program must have needs that can be met through the program. To qualify for services, residents must have impairments in four ADLs or impairments in five IADLs totaling eight points (or six points if the person lives alone) and cannot be eligible for the Medicaid HCBS waiver.
Basic care facility. While an admission policy is not outlined in the regulations, a resident is defined as an individual admitted and retained in a facility in order to receive room and board and health, social, and personal care who is capable of self-preservation, and whose condition does not require continuous, 24-hour a day on-site availability of nursing or medical care.
Nursing Home Admission Policy
In addition to criteria related to rehabilitative and medical needs, individuals are eligible for admission to a nursing facility if they need constant help 60 percent of the time with at least two ADLs (toileting, eating, transferring, and locomotion). Constant help means continual presence or help without which the activity would not be completed; the individual has dementia that requires a structured, professionally staffed environment; or the individuals needs help with two or more of the following: administration of medications, constant help 60 percent of the time with one of the above ADLs, feeding tubes, decubitus care, one or more unstable medical conditions requiring specific, individual services on a regular or continuing basis under the care of a registered nurse, or the person has restorative potential.
Services
Assisted living residences. State law allows assisted living facilities to provide health services to individuals for the purpose of preventing disease and promoting, maintaining, or restoring health or minimizing the effects of illness or disability. Assisted living facilities must provide or assure the coordination of individualized support services which means services provided to individuals who may require assistance with activities of daily living of bathing, dressing, toileting, transferring, eating, medication management, and personal hygiene. The State does not require a minimum level of services to be provided to tenants residing in assisted living. Rather, tenants in assisted living facilities purchase services a la carte. Room is separate from food services, personal care, medication management, transportation, etc. A tenant pays for the services he or she desires, much like an individual living in his or her own home.
Basic care facilities provide a bundled set of services which includes room and board and personal care (ADLs, IADLs, and observation and documentation of changes in physical, mental, and emotional functioning, as needed); arrangements to seek health care when needed; arrangements for transfer and transportation as needed; assistance with functional aids, clothing, and personal effects as well as maintenance of personal living quarters; assistance with medication administration; and social services. Nursing services must be available to meet the needs of residents either by the facility directly or arranged by the facility through an appropriate individual or agency.
Basic care facilities may also provide adult day care and respite care services under the Medicaid waiver.
Dietary
Assisted living residences. There are no dietary requirements.
Basic care facilities. A minimum of three meals and snacks between meals and in the evening must be served that meet the recommended dietary allowances of the Food and Nutrition Board of the National Research Council. If the facility accepts people who need prescribed diets, those diets must be provided and planned and reviewed by a professional, consistent with rules set by the Dietetic Practice Board.
Agreements
Assisted living facilities must maintain a written agreement with each tenant that includes the rates for rent and services provided to the tenant, payment terms, refund policies, rate changes, tenancy criteria, and living unit inspections. Additionally, each facility must include in the resident agreement specific language regarding when a tenant must be discharged due to care needs beyond what the facility can safely provide. Agreements or contracts between the resident and the facility must be kept in the resident’s record.
Provisions for Serving People with Dementia
Basic care facilities. In-service training must cover mental and physical health needs including behavior problems.
Medication Administration
Assisted living residences. Facilities must meet other state requirements and regulations for medication administration, including the Nurse Practice Act.
Basic Care Facilities must make available medication administration services. Aides who have passed required training may administer medications under supervision from a registered nurse.
Medicaid waiver program. The State's nurse practice act allows assistance with self-administration but not the direct administration except by licensed staff. No separate requirements outside the nurse practice act are included.
Public Financing
Assisted living facilities and basic care facilities. Tenants residing in licensed assisted living facilities are treated the same way as individuals residing in their own homes in relation to publicly-funded services. As a result, tenants in assisted living facilities may receive Medicaid waiver services if they are Medicaid eligible and meet nursing home level of care. Funding is also available through two state-funded programs: SPED and the expanded SPED.
The Medicaid waiver program is available to eligible tenants in assisted living facilities only. The Medicaid waiver program is not available to residents living in basic care facilities. Tenants in assisted living residences are able to receive any of the services provided by the waiver program including personal care, respite, transportation, and adult day services. The State does not use the 300 percent eligibility percent option. The medically needy income standard is $500. Low-income residents retain $375 to pay for room and board and $60 for personal needs and any remaining funds are applied to the cost of services. Facilities receive a maximum rate of $80 per day, or a monthly cap of $2,400 per 30-day month for services. Rates are based upon the tenant’s plan of care. This rate covers direct services only and does not include reimbursement for case management. Room and board is not included in the charges allowed for Medicaid beneficiaries. Family supplementation is allowed.
The expanded SPED program is a companion program to the basic care program and serves eligible persons living in their own home. Participants must be Medicaid-eligible, and are moderately impaired, typically requiring some assistance with ADLs, supervision or a structured environment. Participants served by the expanded SPED program are not as impaired as participants in the SPED program or in nursing facilities.
The SPED program serves participants who are frailer than individuals in the expanded SPED program, but not nursing home eligible. Participants must meet program financial eligibility requirements including a $50,000 liquid asset test, but do not have to be Medicaid eligible. Participants may be required to pay a portion of the costs of care. Contributions are based upon income levels and a sliding fee scale. Facilities receive a maximum rate for services of $40 per day, or a monthly cap of $1,200 per 30-day month for both the SPED and expanded SPED programs. Rates are based upon the tenant’s plan of care. A point system is used to convert unmet service functional needs to a rate. (See table below.) The total points are multiplied by a factor of eight and divided by 30 to obtain a monthly payment rate.
The State is in the process of revising the point system (table below). Some point factors will go up, and some will go down based upon a retrospective review of plans of care and determination that some services take more time than others. The State anticipates the new point system will go into effect May 1, 2004.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participants | Facilities | Participants | Facilities | Participants |
| 42 | 31* | NR | NR | 6 | 47 |
| * NOTE: Not all facilities contracting with Medicaid were serving beneficiaries. | |||||
Nursing Home Conversions
A conversion program was implemented in 2000. The State spent approximately $3.9 million from July 1, 1999 to June 30, 2003 to develop alternatives to nursing facility care. This includes both loans and grants to 20 facilities. The legislature did not provide any additional funds for the FY 2003-2005 biennium.
Staffing
Assisted living. Staff must be able to deliver the necessary services required by plans of care.
Basic care facilities. There must be awake staff on duty 24 hours a day.
Training
Administrators of basic care facilities must attend at least 12 hours of continuing education annually. No other requirements are stated.
Basic care facilities. The facility shall design, implement, and document educational programs to orient new employees and develop and improve employees’ skills to carry out their job responsibilities. On an annual basis, all employees shall receive in-service training in at least the following: fire and accident prevention and safety; mental and physical health needs of the residents, including behavior problems; prevention and control of infections, including universal precautions; and resident rights. The staff responsible for food preparation shall attend a minimum of two dietary educational programs per year. Staff responsible for activities shall attend a minimum of two activity-related educational programs per year.
Background Check
Basic care facilities: Each facility’s personnel policies must include checking state registries and licensure boards prior to employment for findings of inappropriate conduct, employment, disciplinary actions, and termination.
Monitoring
Assisted living residences. The Department receives complaints by and on behalf of tenants. The Department must forward the complaints to the appropriate agency, entity, or program for investigation. The State contracts with the State Ombudsman Program for oversight and monitoring of assisted living facilities.
Basic care facilities. On-site, unannounced surveys are conducted by the Department to determine compliance with regulations. Plans of correction must be developed by the facility if deficiencies are found. Corrections must be completed within 60 days of the survey completion date unless the Department has approved an alternative schedule. The Department will follow up on all plans of correction. Enforcement actions include a ban or limitation on admissions, suspension or revocation of license, or denial of license.
Fees
The registration fee for assisted living facilities is $75 annually. As of January 2004, basic care facilities must pay a $10 per bed licensing fee.
| Activity | Value | Activity | Value |
|---|---|---|---|
| Taking medication | 1 | Foot care | 10 |
| Temperature\pulse\respiration\blood pressure | 1 | Nail care | 10 |
| Managing money | 1 | Changing dressings | 10 |
| Communication | 1 | Apply elastic bandage | 10 |
| Shopping | 15 | Care of prosthetic | 10 |
| Housework | 10 | Medical gases | 10 |
| Laundry | 10 | Meal preparation | 20 |
| Mobility | 6 | Exercise | 20 |
| Transportation | 6 | Water bath/heat | 20 |
| Bathing | 10 | Ostomy care | 20 |
| Teeth/mouth care | 20 | Bowel program | 20 |
| Dress/undress | 15 | In-dwelling catheter | 20 |
| Toileting | 15 | Bronchial drainage | 20 |
| Transfer | 10 | Feeding/eating | 20 |
| Continence | 15 | Supervision level I | 15 |
| Eye care | 10 | Supervision level II | 30 |
| Skin care | 10 |
Ohio
Citation
Residential care facilities, Ohio Revised Code Annotated §3721 et seq.; Ohio administrative code §3701-17-50 et seq.
Adult care facilities, Ohio Revised Code Annotated 3722 et seq.; Ohio Administrative Code Chapter 3701-20-01 et seq.
General Approach and Recent Developments
Rules for residential care facilities and adult care facilities were revised in 2001. The majority of assisted living facilities in Ohio are licensed as residential care facilities (RCFs); however, some are licensed as adult care facilities (ACFs). Some facilities may be marketed as assisted living and are not required to be licensed.
Residential care facilities provide supervision, personal care services, and may administer medications, supervise special diets, and perform dressing changes. Residential care facility residents may also receive up to 120 days of nursing services on a part-time intermittent basis.
Adult care facilities provide supervision and personal care services. Unlike residential care facilities, ACFs are prohibited from administering medications, supervising special diets, or performing dressing changes. However, ACF residents with short-term illnesses may receive up to 100 days of these and other needed nursing services.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Adult care facilities | 712 | 5,66 | 805 | 5,783 | 860 | 6,017 |
| Residential care facilities | 510 | 36,255 | 462 | 31,937 | 439 | 28,139 |
Definition
Residential care facility means a home that provides either of the following:
Accommodations for 17 or more unrelated individuals and supervision and personal care services for three or more of those individuals who are dependent on the services of others by reason of age or physical or mental impairment.
Accommodations for three or more unrelated individuals, supervision, and personal care services for at least three of those individuals who are dependent on the services of others by reason of age or physical or mental impairment, and provides to at least one of those individuals any of the skilled nursing care authorized by section 3721.011 of the Revised Code.
Any entity that meets this definition must be licensed.
Adult care facility means an adult family home or an adult group home. An adult family home is a residence or facility that provides accommodations to three to five unrelated adults and supervision and personal care services to at least three of those adults. Adult group homes provide accommodations to six to sixteen unrelated adults and supervision and personal care to at least three of the unrelated adults.
If a residence, facility, institution, hotel, congregate housing project, or similar facility provides services that meet the definition of a residential care facility or an adult care facility, then it must be licensed accordingly, regardless of how the facility holds itself out to the public.
Unit Requirements
RCFs must offer 100 square feet for single occupancy rooms and 80 square feet per person in multiple occupancy rooms. No more than four people may share a room. A toilet, sink, tub/shower is required for every eight residents. If there are more than four persons of one sex to be accommodated in one bathroom on a floor, a bathroom must be provided on that floor for each sex residing on that floor.
ACFs must offer 80 square feet for single occupancy rooms and 60 square feet per person in multiple occupancy rooms. No more than three people may share a room. A toilet, sink, tub/shower is required for every eight residents.
Admission/Retention Policy
RCFs may not admit or retain individuals requiring skilled nursing care or provide skilled nursing care beyond the limits established in regulations. The statute allows residential care facilities to admit and retain residents requiring part-time, intermittent nursing care for up to 120 days. RCFs may also admit and retain residents who require dressing changes, special diets, and medication administration beyond the 120-day limit if the facility provides those services itself.
ACFs may not provide but may admit and retain individuals who need part-time, intermittent nursing care to treat a short-term illness.
Nursing Home Admission Policy
For the skilled level of care, individuals must require at least one skilled nursing service at least seven days a week, or a skilled rehabilitation service at least five days a week. For intermediate care, an individual must need hands-on assistance with at least two ADLs; or assistance with one ADL and is unable to perform self-administration of medications and requires assistance with administration; or requires one or more skilled services at less than a skilled care level (seven days per week); or the person requires the supervision of another person 24-hours a day due to dementia.
Services
RCFs may provide supervision, personal care, laundry, activities, meals, and nursing services that include supervision of special diets, application of dressings, and administration of medication, and may also provide other nursing services on a part-time, intermittent basis for a total of not more than 120 days in any 12-month period. Part-time, intermittent is defined as less than eight hours a day or less than 40 hours a week. The skilled nursing services may be provided by the RCF, a licensed hospice agency, or a certified home health agency. RCFs may not administer parenteral nutrition. In ACFs, part-time, intermittent nursing services may be provided for up to 120 days in any 12 month period by either a licensed hospice, a certified home health agency, licensed nursing home, or mental health agency to residents with short-term illnesses. Short-term illness means either a medical condition for which recovery can be expected to occur with not more than thirty-five consecutive days of skilled nursing care or a medical condition requiring skilled, nursing care provided on a periodic, scheduled basis.
A health assessment covering specific areas must be performed within 48 hours of admission and at least annually unless required sooner. The updated assessment must include change in health status. Risk agreements may be used, and are valid only if they are in writing.
In ACFS, a health assessment must be conducted by a physician or other licensed professional. The purpose of the assessment is to ensure that a resident is not being admitted with needs beyond the facility’s capacity to provide care. The assessment must be completed within 14 days of admission. Annual assessment are required or upon significant change in condition.
Facilities may enter into a risk agreement with a resident or the resident’s sponsor through which the resident or sponsor and the facility agree to share responsibility for making and implementing decisions affecting the scope and quantity of services provided by the facility to the resident. The facility also agrees to identify the risks inherent in a decision made by a resident or sponsor not to receive a service provided by the facility.
Dietary
RCF. Facilities may choose not to provide meals, or they may provide one, two, or three meals; preparation of simple diets and one, two, or three meals; preparation and supervision of simple diets and three meals; preparation and supervision of calculated diets and three meals. Meals must provide the recommended daily allowances of the Food and Nutrition Board and be based on a standard meal planning guide from a diet manual published by a dietician or registered dietician or approved by a dietician. Serving sizes and content are described in the regulations. Facilities providing special diets must monitor staff that prepare or serve the food and monitor residents. Facilities must have policies and procedures that assure that special diets are prepared and offered as ordered. Facilities that do not provide meals must ensure that each resident unit is appropriately and safely equipped with food storage and preparation appliances which the facility maintains in safe operating condition or ensure that each resident has access to such meal preparation and storage appliances.
ACF. These facilities must make three meals available that provide for the recommended dietary allowances of the Food and Nutrition Board and snacks. Special diets shall be prepared in accordance with orders from a physician or a licensed dietician.
Agreements
Agreements cover all charges including security deposits; a statement that all charges, fines, or penalties that shall be assessed are included in the agreement; a statement that the basic rate will not change without 30-days’ notice; refund policy; an explanation of the services offered and the type of skilled nursing care provided and allowed; and any limitations on the type and duration of skilled nursing and the extent and types of services that will be provided and who is responsible for payment. RCFs must explain their policy on smoking, resident’s rights, care for persons with Alzheimer’s disease, dementia, or a related disorder by means of an Alzheimer’s special care unit, ability to accommodate handicapped residents, and advance directives and issue a statement concerning discharge when the resident’s skilled nursing needs exceed their capacity.
Provisions for Serving People with Dementia
Revised rules establish disclosure requirements for RCFs that serve people with dementia. The disclosure includes the form of treatment; philosophy and mission; the process and criteria for placement, transfer, and discharge; assessment and treatment process; staff training and continuing education practices; the physical environment and design features; frequency and type of activities; involvement of families and availability of family support programs; and the cost of specialized services and additional fees.
Medication Administration
Medications may be administered in RCFs by RNs, LPNs that have completed an approved training program and under direction from an RN, and physicians. No medications may be administered to a resident unless ordered by a physician or individual authorized under state law to prescribe medications. Trained non-licensed staff of both RCFs and ACFs may assist with self-administration. Assisting with self-administration requires the resident to be mentally alert and able to participate in the medication process and includes reminders, observing, handing medications to the resident, verifying the resident's name on the label, and, for physically impaired residents, removing oral or topical medications from containers, applying medication upon request, and placing containers with medication to the mouth of the resident. Medications may be administered by a licensed hospice agency, certified home health agency, or a member of the RCF’s staff who is qualified to do so. Adult care facility staff may not administer medications. However, medications may be administered by a home health agency, hospice care program or nursing home staff.
Public Financing
No Medicaid coverage is available. The SSI payment standard, with the state supplement, is $850 and the PNA is $50. Ohio proposed an assisted living waiver during the 2004/2005 budget deliberations, but it was not adopted by the General Assembly and no funding was appropriated. The Governor, as part of the State's Olmstead plan, has called for adoption of an assisted living waiver to increase long term care options as alternatives to nursing homes for consumers with disabilities.
Staffing
Residential care facilities must have an administrator on staff at least half-time per week. At least one staff member must be on-site at all times. During the evening, the staff member on-site may be on call if the facility meets the call signal requirements established in rule. When only one staff member is on duty in the facility, the facility must designate another person who meets the same qualifications to be on call. An RN, LPN, or physician must be on duty when medications are being administered. Staff may be shared with other licensed facilities in the same building or in the same lot as long as staffing requirements for all facilities are met. A dietitian’s services are required if the facility elects to supervise special diets or perform enteral tube feedings, and sufficient nursing staff are required if the RCF elects to perform dressing changes or part-time intermittent nursing care.
ACFs, which include some semi-independent living homes, must have one staff member on site whenever a resident who requires ongoing supervision; assistance with walking, moving, bathing, toileting dressing, eating, evacuation; or PRN medications is present. When only one staff person is on duty, the facility must designate another staff person to be available immediately in case of emergency.
In addition, for both RCFs and ACFS, sufficient additional staff must be available to meet, in a timely manner, the residents’ care, supervisory, and emotional needs and reasonable requests for service, including ongoing supervision of residents with increased emotional needs or presenting behaviors that cause problems for the resident or other residents and to properly provide dietary, housekeeping, laundry, and facility maintenance services and recreational activities.
Training
RCF administrators must be a licensed nursing home administrator or have 2,000 hours of operational responsibility in related facilities, must have successfully completed 100 credit hours of post high school education in gerontology, be a licensed health professional, or hold a baccalaureate degree. RCF administrators also must receive annually nine hours continuing education in gerontology, health care, business administration, or residential care facility operation. ACF managers are required to have six hours of basic orientation and training applicable to job duties including emergency response training, and six hours of continuing education annually.
Staff. Both ACFs and RCFs must provide orientation and training for all staff in job responsibilities, facility procedures, securing emergency assistance, and resident rights. ACF and RCF staff who provide personal care must have currently valid documentation of a successfully completed first aid course. In addition, RCF staff providing personal care must have met one of the following requirements:
Successfully completed training or continuing education covering the correct techniques of providing personal care services, observational skills such as recognizing changes in residents’ normal status and the facility’s procedures for reporting changes, and communication and interpersonal skills provided by an RN or LPN;
Successfully completed the training and competency evaluation program approved or conducted by the Director under §3721.31 of the revised code; or
Successfully completed the training or testing requirements in accordance with the Medicare Conditions of Participation of home health aide services.
If an RCF serves people with emotional and behavior needs, training or continuing education in the appropriate interventions for meeting these needs and for handling and minimizing such problems must be completed. Staff members whose responsibilities include supervising special diets must be trained by a dietician.
ACF staff who provide personal care must also have successfully completed training or continuing education covering the correct techniques of personal care services. ACFs who serve individuals with mental illness must ensure that managers and staff receive orientation and 6 hours of training in caring for persons diagnosed with mental illness and how to locate crisis services.
Background Check
Criminal background checks are required for any individual used by an ACF or RCF in a position that provides direct care to older adults. Staff providing direct care services must also provide fingerprint impressions.
Monitoring
RCFs must be inspected at least once prior to the issuance of a license and one unannounced visit every 15 months by the Department of Health and the fire marshal. State or local ACFs must be inspected annually by the Department. These visits must be unannounced and with additional unannounced visits made as deemed necessary. Adult group homes must also undergo an annual fire inspection.
Inspections are compliance-based, and do not incorporate a consultative or collaborative component.
Fees
Residential care facility: licensing and renewal fee of $105 for every 50 persons, or part thereof of licensed capacity.
Adult group home: license fee is $50.
Adult family home: license fee is $25.
AGHs and AFHs must also pay an inspection fee of $10 for each licensed bed.
Oklahoma
Citation
Residential care homes: 63 Oklahoma statute §1-819 et. seq.; Oklahoma rules, §310:680:1:1 et seq.
Continuum of care and assisted living act: 63 O.S. Supp. 1997, Section 1-890.1. et seq.
Oklahoma rules: Chapter 310:663:1 et. seq.
General Approach and Recent Developments
The Continuum of Care and Assisted Living Act authorized two types of health care or residential settings: the continuum of care facility and the assisted living center. The continuum of care facility provides more services than are available in a typical nursing facility. The assisted living center offers a level of services between current nursing facilities and residential care homes.
Proposed rule changes have been made in 2004 to the physical plant standards for assisted living and continuum of care facilities. New language would require the physical plant to be designed and constructed in conformity with requirements for accessibility to physically disabled persons as established by the International Building Code. Rules prohibiting smoking except in a designated area were issued in 2002. An Alzheimer’s Disease Special Care Disclosure act passed in 1999.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Residential care homes | 103 | 3,358 | 210 | 8,620 | 147 | NR |
| Assisted living centers | 115 | 6,308 | 8 | 1,253 | 87 | NR |
Definition
An assisted living center means any home or establishment offering, coordinating, or providing services to two or more persons who:
- Are domiciled therein;
- Are unrelated to the operator;
- By choice or functional impairments, need assistance with personal care or nursing supervision;
- May need intermittent or unscheduled nursing care;
- May need medication assistance; and May need assistance with transfer and/or ambulation.
No facilities may call themselves an assisted living center or a continuum of care facility unless they are licensed. The law allows assisted living centers to be licensed as a component of a nursing facility.
A continuum of care facility means a home, establishment, or institution providing nursing facility services and at least one of the following: assisted living center services or adult day care center services.
Residential care home means any establishment or institution other than a hotel, motel, fraternity or sorority house, or college or university dormitory which offers or provides residential accommodations, food services, and supportive assistance to any of its residents or houses any resident requiring supportive assistance who is not related to the owner or administrator of the home by blood or marriage. Said residents shall be ambulatory and essentially capable of managing their own affairs and do not routinely require skilled nursing care or intermediate care.
Unit Requirements
Assisted living centers: No more than two residents may share a bedroom. Each center shall ensure privacy and independence by requiring lockable doors except in the case of documented contraindication, have individually-controlled temperature controls, and the right to use personal furnishings. No more than four residents may share bathing and toilet facilities. Shower and bathing facilities shall be occupied by no more than one resident at a time. The assisted living portion of continuum of care facilities must be physically separate from the nursing home.
Residential care home: Single rooms must have 80 square feet and multiple occupancy rooms 60 square feet per bed. The regulations do not limit the number of residents who may share a bedroom. Toilet facilities must be provided for every six residents and a tub/shower for every ten residents.
Admission/Retention Policy
Assisted living centers must describe the population to be served based on the population’s need for personal care, nursing supervision, intermittent or unscheduled nursing care, medication administration, assistance with cognitive orientation and care or service for Alzheimer’s disease, and assistance with transfer or ambulation. Each center’s admission criteria must be included in the application for licensing.
The center must use a comprehensive screening instrument to determine the appropriateness of the resident’s placement in the facility. Centers may not serve anyone whose needs are inconsistent with the services provided by the facility, whose physician determines that restraints are needed, who is a threat or danger to self or others, or whose needs for privacy and dignity cannot be met by the facility.
Residential care home. The regulations do not contain a section on admission/retention criteria. The definition states that residents may not need services provided in a skilled or intermediate care facility. Residents must be ambulatory and essentially capable of managing their own affairs. A home shall not involuntary transfer or discharge a resident except for medical reasons, for the resident’s safety, or for the safety of other residents, or for nonpayment for the resident’s stay.
Nursing Home Admission Policy
Eligibility for nursing home admission is based on the physician’s recommendation, an assessment by a department nurse, and professional judgment. The minimum criteria are high risk range on ADLs or mental state questionnaire (MSQ) scores; or a combination (2) of moderate ADL scores, moderate MSQ scores, and high risk nutrition score. Other factors include moderate risk client support score, high risk environment or moderate risk environment, and high risk social resources.
The assessment measures eight ADLs: bathing, eating, dressing, grooming, transferring, mobility, toileting, and bladder/bowel control. High risk range ADL scores means some help with four ADLs or a person cannot perform two ADLs and needs helps with one additional ADL. Moderate risk range means needs help with three ADLs; total help with two ADLs, or total help with one ADL and help with two ADLs.
Services
Assisted living centers shall not care for any resident needing care in excess of the level that the assisted living center is licensed to provide or capable of providing. The center must ensure that routines of care provision and service delivery are directed by the resident to the maximum extent possible. The center must describe the services to be provided or arranged including: personal care, meals, housekeeping, laundry, intermittent or unscheduled nursing care, nursing supervision, medication administration, assistance with cognitive orientation, specialized services for people with Alzheimer’s disease, assistance with transfer or ambulation, planned programs for socialization, and activities and exercise. Nurses are allowed to delegate tasks that are within the scope of their license to perform. Intermittent nursing care and home health aide services may be provided in an assisted living facility by a home health agency.
If a resident’s preference or decision places the resident or others at risk or is likely to lead to an adverse consequence, the assisted living center shall advise the resident and the resident’s representative of such risk or consequences. The assisted living center shall specify the cause for concern, discuss the concern with the resident and representative, if any, and attempt to negotiate a written agreement that minimizes risk and adverse consequences and offers alternatives while respecting resident preferences.
Continuum of care facilities must provide, coordinate or arrange care appropriate to the needs and capabilities of its residents, including the availability of care appropriate to a nursing facility or specialized facility. A facility may not care for residents needing care in excess of the level of care that the facility is licensed to provide.
An admission assessment specified by the State must be implemented 30 days before or at admission, and a comprehensive assessment specified by the State must be completed within 14 days after admission and updated at least annually thereafter or whenever a significant change occurs. The rules describe the content of the assessment. Assessments must be completed by the appropriate participation of health professionals trained in assessment, and coordinated and signed by a registered nurse or the resident’s physician. The assessment is used to determine the appropriateness of placement and to develop a plan of care.
A managed risk process is required when resident preferences or decisions create risk or are likely to lead to adverse consequences. The center identifies the cause for concern, attempts to negotiate an agreement that minimizes risk, and offers alternatives. Any lack of agreement must be documented. Managed risk procedures are required when needed.
Nurses remain responsible for all nursing care that a person receives under their direction. Nurses may use their professional judgment in determining which tasks may be delegated. Tasks which may not be delegated include those which require nursing assessment, judgment, evaluation, and teaching during implementation such as physical, psychological, and social assessments which require nursing judgment, intervention, referral or follow up; require formulation of a plan of nursing care and evaluation of responses to the care; or administration of medications except as authorized by regulations.
Residential care homes provide assistance with personal care; medications; three meals a day; and supportive assistance which includes housekeeping, assistance in the preparation of meals, and storage, distribution, and assistance with medications.
Dietary
Each assisted living center must use a licensed dietician or qualified nutritionist to develop the center’s diet plan and address the needs of individuals with special diets.
Residential care homes must have available a minimum of three meals per day that constitute a palatable, nutritionally adequate general diet and should include the four basic food groups in the recommended amounts. Homes with residents requiring special diets prescribed by a physician must contract with a consulting licensed/registered dietician. All special diet menus must be approved by a licensed/registered dietician.
Agreements
Assisted living centers. Each assisted living center must provide a complete and understandable contract to each resident. All rights, privileges, and assurances in the regulations are considered part of the contract. Other provisions require a clear statement and the center’s name and address; admission criteria; services provided; discharge criteria; dispute resolution and grievance procedure; the term, renewal, and cancellation provisions; conformity with state law; and in the event the resident’s condition merits transfer, the transfer shall be initiated within five days and progress noted in the resident’s record. The written contract constitutes the entire agreement between the center and the resident “not excluding the marketing materials and the requirements of this chapter.”
Residential care homes. A written contract must be executed within 120 days of admission, or when the source of resident funds changes from private to public or from public to private funds, or when the terms of the contract have changed. The contract must specify the contract terms; the services that may be provided to supplement the contract and the charges for those services; sources liable for payment; amount of deposit paid; the rights, duties and obligations of the resident; and the name of the resident’s designated representative, if any.
Provisions for Serving People with Dementia
Facilities providing specialized care in special units to persons with Alzheimer’s disease and related dementias must complete an Alzheimer’s Disease Specialized Care Disclosure Form. This form includes the philosophy of care, the process and criteria for placement and discharge, the assessment and care planning process, staff ratios, staff training and continuing education, the physical environment and design features, types and frequency of activities, the involvement of families in care planning, and the fees charged. Centers with only one direct care staff member awake at night have to disclose the staffing arrangement and have an approved plan to deal with urgent or emergency situations.
Medication Administration
Assisted living centers. Each center must provide or arrange for staff to administer medications. Unlicensed personnel administering medications must complete a training program approved by the relevant department. Medications must be reviewed monthly by a registered nurse and quarterly by a pharmacist.
Residential care homes may administer medications and assist with self-administration of medications. All direct care staff responsible for the administration of medication are required to begin training in the administration of medication within 90 days of employment, and complete 15 hours of training in the administration of medications within the first year of employment. Residents who have been deemed capable of self-administration of medications may retain the medications in a safe location in the resident’s room.
Public Financing
While there is continuing interest in covering services under Medicaid, no specific proposals have been developed. The SSI payment is $564, and the personal needs allowance is $50. Family supplementation is allowed for residents who may reside in residential settings.
Staffing
Assisted living centers. Staffing shall be available based on the needs of residents. Nursing staff shall be provided or arranged to supervise skilled interventions, document the resident’s physician of choice, and document the resident’s living will or DNR order. Centers must have a dietary consultant, pharmacy consultant, and nurse consultant if there are no nurses on staff.
Residential care homes shall employ sufficient personnel appropriately qualified and trained to provide the essential services of the home. Homes must have a minimum of ¾ hour of personnel per day per resident based on the average daily census. All homes must have a signed, written agreement with a registered nurse to act as a consultant.
Training
Assisted living center administrators must either hold a state nursing home administrator’s license, a residential care home administrator’s certification from an institution of higher learning approved by the Department, or a national recognized assisted living certificate of training and competency reviewed and approved by the Department.
Assisted living center staff providing socialization, activity, and exercise services must be qualified by training. Centers offering specialized units must ensure that staff are trained to meet the specialized needs of residents, and all direct care staff must be trained in first aid and CPR.
Residential care home administrators must receive a minimum of 50 hours of training including at least 15 hours of training in administration, supervision, reporting, record keeping, the administration of medication, IADLs and ADLs, leisure skills and recreation, and public relations. Sixteen hours of annual continuing education is required of all administrators, not counting first aid and CPR training.
Residential care home staff. All employees must be currently certified in first aid. All direct care staff must receive eight hours of in-service training within 90 days of employment. Staff responsible for administering or monitoring medications must receive eight hours of training annually in the following areas: patient reporting and observation; record keeping; independent or daily living skills; leisure skills and recreation; human relations; and such other training that is relevant to residential care program and operations.
New employee orientation programs must include: policies and procedures on abuse and neglect, resident rights, confidentiality, handling emergencies, and job descriptions.
Background Check
Assisted living. All employees are subject to requirements for criminal arrest checks applicable to nurses aides under 63 O.S. Supp. 1997, Section 1-1950.1. Employers must pay a fee of $10 to the Bureau of Investigation for checks. Reports are provided for felonies and misdemeanors for crimes against a person, public indecency or morality, domestic abuse, controlled substances, and crimes against property. Employees may not be hired if they have been convicted of crimes listed in the statute.
Residential care homes. Same provisions.
Monitoring
Assisted living centers. The State must inspect each continuum of care facility and assisted living center through unannounced inspections at least once every 15 months, with a statewide average of 12 months. If a violation is found, the State must provide written notice of all violations. The facility has 10 business days to respond with a written plan of correction. The State will review and provide the facility with its response. If an assisted living center provides or arranges skilled nursing care, the State must assess the quality of that care against applicable national standards of practice adopted by the American Nurses Association and Specialty Nursing Organizations.
Each center must have a quality assurance committee that meets at least quarterly to monitor trends, monitor customer satisfaction, and document quality assurance efforts and outcomes. The committee must include an RN or physician, the administrator, a direct care staff member, or person responsible for administering medications and a pharmacist consultant if a medication problem is to be monitored or investigated. The Department may inspect centers whenever it deems it necessary.
Residential care homes. Inspections are performed at least three times a year to determine compliance with licensure rules. At least one inspection, investigation, survey, or evaluation shall be unannounced. Any individual who discloses the planned unannounced visit may be convicted of a misdemeanor. The State shall invite one person from a statewide organization of the elderly to act as a citizen observer in any inspection. The results of all inspections are made available to the public. This report is updated monthly. The State must make at least one annual report on each home in the State. The report must include all conditions and practices not in compliance with the provisions of the Residential Care Act or rules, if a violation is corrected, or is subject to an approved plan of correction. A local or state ombudsman or case manager is authorized to accompany the State on its inspections. The State must give written notice of any violations. A residential care home may request a hearing, and submit a plan of correction within 10 business days.
Fees
Assisted living centers. There is a $10 per bed application fee, with a $1,000 cap, to establish a facility and an initial licensing fee of $10 per bed.
Residential care homes. $50 per application. Annual renewal fees are $50.
Oregon
Citation
Assisted living, OAR Division 56: 411-056-0000
Residential care facilities, OAR Division 56:411-55-000
General Approach and Recent Developments
Oregon has two types of residential care and separate licensing and regulatory requirements for each: Residential Care Facilities (RCFs) and Assisted Living Facilities (ALFs). The major distinction between ALFs and RCFs is that ALFs have private apartments whereas RCFs have both private and shared rooms and private and shared baths. The State does not allow providers to market themselves as assisted living unless they offer residents private apartments and are licensed as assisted living. The rules for assisted living and residential care facilities establish standards that promote the availability of appropriate services for elderly and disabled persons in a home-like environment that enhances the dignity, independence, individuality, privacy, choice, and decision making ability of the resident. Language about the philosophy is also contained in sections dealing with management responsibilities and service planning.
In February 2004, the State extended the moratorium on the licensing of new assisted living and residential care facilities until June 30, 2005 and changed the requirements within the moratorium rule. Licenses may be issued to: applicants who submitted construction plans prior to August 16, 2001; facilities applying for a renewal license or changing ownership, but are not increasing capacity; facilities that are relocating within the service area; or a Continuing Care Retirement Community that provides care to residents within its closed system. New applicants requesting licensure must demonstrate that the proposed facility will serve a population for whom insufficient services exist in the service area. The rule now allows facilities to request an increase in capacity by ten percent.
Effective August 1, 2004, assisted living and residential care facilities are required to develop and implement policies on the possession of firearms and ammunition within the facility. Such policies must be disclosed to residents.
Assisted Living Facilities. The State amended the assisted living rules regarding criminal background checks, changing the compliance code references in the regulations, which became effective August 1, 2004.
Residential Care Facilities. Substantial revisions to the residential care facility regulations became effective in April 2004. The revisions make the residential care facility regulations more like the assisted living facility regulations. The State will initiate another series of rule changes for residential care facilities this summer, with an expected implementation date of early Fall. Issues to be addressed include increased staff to resident ratios and required additional nurse involvement in facilities.
A consumer guide (http://www.dhs.state.or.us/seniors/publications/oregon_consumer_guide.p…) is available and a uniform disclosure form (http://afsforms.hr.state.or.us/Forms/Served/SE9098A.pdf) has been developed.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted living facilities | 190 | 12,566 | 180 | 11,998 | 138 | 8,661 |
| Residential care facilities | 236 | 8,504 | 220 | 8,227 | 187 | 6,805 |
Definition
“Assisted living facility means a building, complex or distinct part thereof, consisting of fully self-contained individual living units where six or more seniors and persons with disabilities may reside. The facility offers and coordinates a range of supportive personnel available on a 24-hour basis to meet the ADL, health services, and social needs of the residents described in these rules. A program approach is used to promote resident self-direction and participation in decisions that emphasize choice, dignity, privacy, individuality, independence and home-like surroundings.”
No facility may use the term assisted living unless it is licensed as such.
“Residential care facility means a building, complex or distinct part thereof, consisting of shared or individual living units in a home-like surrounding where six or more seniors and adult persons with disabilities may reside. The facility offers and coordinates a range of supportive services available on a 24-hour basis. Facility services address the residents’ activities of daily living, health, and social needs in a way that promotes choice, dignity, individuality and independence.”
No facility may use the term residential care facility or present itself as providing residential care services unless it is licensed as such. A residential care facility may not be operated in combination with other facilities unless it is licensed, maintained, and operated as a distinct part.
Unit Requirements
Assisted living facility. Each unit consists of individual adaptable and accessible apartments with a lockable door, private bathroom, and kitchenette facilities which include a sink, refrigerator, and cooking appliance that can be removed or disconnected. Units must provide 220 square feet of space, not including a private bathroom. Buildings must meet applicable zoning and building codes. Pre-existing structures must provide 160 square feet excluding the bathroom.
Residential care facility. Resident units may comprise individual apartments with private bathroom and kitchenette facilities or be limited to a bedroom only, with bathroom facilities centrally located off common corridors. Facilities must include a minimum of 80 square feet per resident and limit occupancy to two residents per unit. Centralized bathing facilities must be provided for every 10 residents who do not have private bathing. Toilets must be provided for every six residents. Facilities licensed, constructed or renovated after April 1, 2004 will meet accessibility requirements of the Americans with Disabilities Act under Title III as a public accommodation and the Oregon Structural 30 Specialty Code, as enforced by the Oregon Building Codes Division and local jurisdictions having authority.
Admission/Retention Policy
Assisted living facility. An initial screening is conducted to determine whether a potential resident meets the facility’s admission requirements. Based on the initial screen, an initial service plan is developed before the resident moves in to the facility and is reviewed within 30-days of move-in to ensure the services accurately reflect the resident’s needs and preferences. Facilities may, but are not required to, ask residents to move, with a 30-day notice, if their needs exceed the level of ADL services available; the resident exhibits behaviors or actions that repeatedly interfere with the rights or well being of others; the resident, due to cognitive decline, is not able to respond to verbal instructions, recognize danger, make basic care decisions, express need, or summon assistance; the resident has a complex, unstable, or unpredictable medical condition; or for non-payment of charges. Facilities are allowed to ask residents to leave with less than a 30-day notice, but not less than a 14-day notice if the resident exhibits behavior that is an immediate danger to self or others; has a sudden change in condition that requires medical or psychiatric treatment outside the facility and it is determined that the resident’s level of care exceeds the level of care of the facility; the facility is unable to accomplish resident evacuation according to the Life Safety Code rules; or the resident requires 24 hour, seven days a week nursing supervision.
Resident care facility. No residential care facility will admit individuals whose care needs exceed the classification on its license without prior written consent of the relevant department.
Two levels of licensure are available for residential care facilities based upon the qualifications and number of staff in the residential care facility. A Class I license is needed to serve residents who only require assistance with ADLs. These facilities cannot serve anyone who require full assistance in any activity of daily living. Class II facilities provide care to residents who may require full assistance in activities of daily living; and, in addition, serve people who have an increase in medical acuity.
A Class I facility may retain a resident who requires full assistance in an ADL if the provider establishes that the following criteria are met: the provider is able to provide appropriate care to the resident in addition to the care of the other residents; staff are available to meet the additional care requirements of all residents in the facility; and the fire evacuation standard for all residents and staff members can be met.
Nursing Home Admission Policy
Regulations set priorities for services based on the amount of assistance needed with a specified ADL or combination of specified ADLs and cognition. Due to recent budget constraints, the priority thresholds have been changed. Eligibility had been limited to levels 1-11 but was expanded to levels 12 and 13 July 1, 2004.
- Dependent in mobility, eating, toileting, and eating;
- Dependent in mobility, eating, and cognition;
- Dependent in mobility or cognition or eating;
- Dependent in toileting;
- Substantial assistance with mobility, assistance with toileting and eating;
- Substantial assistance with mobility and assistance with eating;
- Substantial assistance with mobility and assistance with toileting;
- Assistance with eating and toileting;
- Substantial assistance with mobility;
- Minimal assistance with mobility and assistance with toileting;
- Minimal assistance with mobility and assistance with eating;
- Assistance with mobility;
- Assistance with eating;
- Minimal assistance with mobility;
- Dependent in bathing and dressing;
- Assistance in bathing or dressing.
Services
Residential care facilities and assisted living facilities. A service planning team (including a registered nurse if the resident receives nursing services, state or Area Agency on Aging case manager, facility administrator or designee, and the resident or legal representative) conducts an assessment with each resident and develops a service plan that responds to his or her needs and reflects the principles of dignity, choice, individuality and independence, and home-like environment.
Required services include three nutritional meals and snacks a day; personal and other laundry services; a program of social and recreational activities; services to assist with ADLs; and household services. Facilities must provide or arrange for social and medical transportation, ancillary services for related medical care (physicians, pharmacy, therapy, podiatry), and maintenance of a personal fund account. Required health services include accessing first payor benefits, providing a licensed registered nurse to conduct health assessments and periodic monitoring, assigning the basic tasks of nurse delegation, providing intermittent nursing services for residents with stable and predictable medical needs, and oversight and monitoring of residents’ health status. Facilities also coordinate the provision of health services with outside service providers such as hospice, home health, physicians’ offices, etc. Other health services include health care teaching and counseling, and emergency response systems that respond to health and medical needs 24-hours a day.
The service plan describes who provides services, what, when, how, and how often services are provided and, if applicable, the desired outcome. The resident shall actively participate in the development of the service plan to the extent of his/her ability to do so. The service plan is reviewed and updated at least quarterly.
A managed risk process is used when a resident exhibits high-risk behavior or choices. The process includes presenting to the resident alternatives to and consequences of the behavior. The resident’s decision to modify the behavior or accept the consequences is documented. The resident’s preferences take precedence over those of family member(s). A managed risk plan cannot be entered into or continued with or on the behalf of a resident who is unable to recognize the consequences of his/her behavior or choices. The plan is reviewed at least quarterly.
Dietary
Residential care facility and assisted living facility. Three meals a day and snacks in accordance with the recommended dietary allowances of the USDA Food Guide Pyramid and modified special diets appropriate to the residents’ needs and choices are provided.
Agreements
Residential care facility and assisted living facility. Agreements/disclosure statements are reviewed by the licensing agency and include the terms of occupancy; payment provisions (basic rental rate and what it includes, additional services costs, billing method, payment system and due dates, and deposits/fees if applicable); policy for rate changes; refund/proration conditions; a description of the scope of services available; a description of the service planning process and the relationship to costs; additional available services; the philosophy of how health care and ADL services are provided; resident rights; the system for packaging medications and the resident’s right to choose a pharmacy; move-out policy; notice that the licensing agency has the right to review records; and the staffing plan.
Provisions for Serving People with Dementia
Residential care facility and assisted living facility. Oregon has a separate set of rules for Alzheimer’s Care Units (Chapter 411, Division 057) which apply to nursing facilities, residential care facilities, and assisted living facilities with the exception of adult foster homes.
Any facility that offers or provides care for residents with Alzheimer's disease or other dementia in an Alzheimer's Care Unit must obtain an endorsement on its facility license. The Alzheimer's Care Unit must be designed to accommodate residents with dementia in a home-like environment. The design and environment of a unit should assist residents in their activities of daily living; enhance their quality of life; reduce tension, agitation, and problem behaviors; and promote their safety. The rules further clarify physical plant standards.
Staffing. Every effort must be made to provide residents with familiar and consistent staff members in order to minimize resident confusion. All direct care staff assigned to the Alzheimer's Care Unit must be specially trained to work with residents with Alzheimer's disease and other dementias. Staffing must be sufficient to meet the needs of the residents and outcomes identified by the individual care plan and sufficient to implement the full day and evening care program. Staffing levels on the night shift depend on the sleep patterns and needs of residents (without control of sleep by medications).
Training. Facilities must provide an orientation program to all new employees assigned to the unit. Orientation must include the facility's philosophy related to the care of residents with Alzheimer's disease and other dementias in the Alzheimer's Care Unit; a description of Alzheimer's disease and other dementias; the facility's policies and procedures regarding care provided in the unit, including therapies provided and general approach; treatment modalities; admission, discharge and transfer criteria; basic services provided within the unit; policies regarding physical restraints, wandering/egress control, and medication management; staff training; and family activities; and common behavior problems and recommended behavior management. Ongoing in-service training shall be provided to all medical and non-medical staff who may be in direct contact with residents of the unit. Staff training shall be provided at least quarterly. The rules further identify the required content of the in-service trainings.
Admission/Retention Policy. Facilities with Alzheimer's Care Units must have a written policy of preadmission screening, admission and discharge procedures. Admission criteria shall require, at a minimum, a physician's diagnosis of Alzheimer's disease or other dementia. The policy shall include criteria for moving residents from within the facility, into or out of the unit. When moving a resident within the facility or transferring a resident to another facility or placement, the facility shall take into account the resident's welfare.
Agreements. Prior to admission into the Alzheimer's Care Unit, the facility shall provide the resident or the resident's legal guardian and a member of the resident's family (if appropriate), with a copy of the disclosure statement.
Services. Within seven working days of admission, the interdisciplinary staff must review the care needs of the new resident. Within 14 days of admission, the interdisciplinary staff must develop an individualized care plan which shall describe the resident's needs, choices, problems to be worked on, the desired outcomes or interventions, and the names of the staff who are to be primarily responsible for implementing the care plan. The care plan must reflect the resident as a person, with family, history and interests. Individual care plans must be developed and written by the interdisciplinary staff and signed by each member of the staff. Each care plan must be reviewed, evaluated for its effectiveness, and updated at least quarterly or more frequently if indicated by changing needs of the resident. Outcomes for the individual care of each resident shall include: promoting remaining abilities for self-care; encouraging independence while recognizing limitations; providing safety and comfort; maintaining dignity by respecting the need for privacy, treating the resident as an adult and avoiding talking as if the resident is not present; and at least one issue of a psychosocial nature related to the resident's preferred manner of living and receiving care.
All facilities with Alzheimer's Care Units must provide for activities appropriate to the needs of the individual residents. Activities which must be offered to the residents at least weekly include:
- Gross motor activities; e.g., exercise, dancing, gardening, cooking, etc.;
- Self care activities; e.g., dressing, personal hygiene/grooming;
- Social activities; e.g., games, music;
- Crafts; e.g., decorations, pictures, etc.;
- Sensory enhancement activities; e.g., distinguishing, pictures and picture books, reminiscing, and scent and tactile stimulation, etc.; and
- Outdoor activities; e.g., walking outdoors, field trips, etc.
A social worker or an assigned staff shall provide social services to both the resident and support to family members.
Medication Administration
Residential care facility and assisted living facility. The regulations allow residents to keep over-the-counter and prescription medications in their unit if they are capable of self-administration. Residents who self-administer prescription medications must have a physician’s or other legally recognized practitioner’s written order of approval. Facilities are allowed to administer medications, and they must have policies and procedures that assure all administered medications are reviewed every 90 days. Residents who self-administer medications are encouraged to have their medications reviewed every 90 days. Medication and treatment administration systems must be approved by a pharmacist consultant, registered nurse, or physician.
Public Financing
The State contracted with 170 assisted living facilities and served 3,731 beneficiaries in December 2003, compared to 172 facilities and 3,600 beneficiaries in the spring of 2002. The program also contracted with 165 residential care facilities and served 1,127 residents in December 2003. The State has an active program to identify and relocate nursing home residents to assisted living and other community settings. Beneficiaries relocating from nursing homes may receive cash grants or may be granted income exemptions to pay for transition expenses.
Assisted living. For residents who meet the nursing home level of care criteria, the State provides five levels of payment. The levels are assigned based on a service priority score determined through an assessment. (See table below.) ADLs include eating/nutrition, dressing/grooming, bathing/personal hygiene, mobility, bowel and bladder control, and behavior. Critical ADLs are toileting, eating, behavior.
The State uses the 300 percent option to determine financial eligibility, and residents are permitted to retain $565.70 as a maintenance allowance; the remainder is the residents’ cost sharing amount. Residents pay $455.70 for room and board, and keep $110 for personal needs. Supplementation is not permitted. The average monthly service costs are $1,643 a month. The distribution of residents by level is: Level 1--2 percent; Level 2--1 percent; Level 3--6 percent; Level 4--59 percent; and Level 5--32 percent.
| Impairment Level |
Service Policy | Service | R&B | Total Rate |
|---|---|---|---|---|
| Level 5 | Dependent in 3 to 6 ADLs OR dependent in behavior and 1 to 2 other ADLs. | $1,944.02 | $455.70 | $2,399.72 |
| Level 4 | Dependent in 1 to 2 ADLs OR assistance in 4 to 6 ADLs plus assistance in behavior. | $1,574.64 | $455.70 | $2,030.34 |
| Level 3 | Assistance in 4 to 6 ADLs OR assistance in toileting, eating, and behavior. | $1,204.07 | $455.70 | $1,659.77 |
| Level 2 | Assistance in toileting, eating and behavior or behavior AND eating or toileting | $910.23 | $455.70 | $1,365.93 |
| Level 1 | Assistance in 2 critical ADLs or assistance in any 3 ADLs or assistance in 1 critical ADL and 1 other ADL | $688.36 | $455.70 | $1,144.06 |
Residential Care Facilities. Medicaid also pays for services for persons who meet the nursing home level of care criteria in Level 2 residential care facilities. In the State’s 2003 budget, the RCF base service rate for all clients was $917.00 per month. Depending on impairment level, there are 3 add-on levels. Base plus 1 add-on is $1,142.00; base plus 2 add-ons is $1,367.00; base plus 3 add-ons is $1,592.00. The add-on is based primarily on how dependent a person is with ADLs.
Residents eligible for Medicaid have the same cost sharing requirements and personal needs allowance as those residing in assisted living facilities.
| 2004 | 2002 | 2000 | ||||
|---|---|---|---|---|---|---|
| Facilities | Participants | Facilities | Participants | Facilities | Participants | |
| ALF | 170 | 3,731 | 172 | 3,600 | 128 | 2,572 |
| RCF | 165 | 1,127 | NR | NR | NR | NR |
Staffing
Assisted living. Each facility must have sufficient staff to meet the 24-hour scheduled and unscheduled needs of each resident and to respond in emergency situations.
Residential care. The regulations contain staff ratio for Class I and Class II facilities that vary by time of day and the number of residents. Irrespective of minimum number of staff stated in the rules, the licensee and administrator are responsible for assuring that an adequate number of qualified staff are available at all times to meet the unique care, health and safety needs of the residents including fire safety and evacuation.
Training
Assisted living administrators shall be at least 21 years of age, have a high school diploma or equivalent and two years of professional or management experience in a health or social service field, or have a combination of experience and education; or a bachelor’s degree in a health or social service field. They must also complete 40 hours of approved classroom training, or complete a classroom training of less than 40 hours and a 40-hour internship in a licensed facility and obtain 20 hours of continuing education credits each year.
Residential care administrators shall be at least 21 years of age, have a high school diploma or equivalent and two years of professional management experience in a health or social service-related field, or have a combination of experience and education or a bachelor’s degree in a health or social service field. Administrators hired on or after January 1, 2003 must complete 40 hours of approved classroom training, or complete a classroom training of less than 40 hours and a 40-hour internship in a licensed facility and obtain 20 hours of continuing education credits each year.
Assisted living. Each facility administrator must document that staff have received assisted living training as prescribed by the State. The facility administrator is accountable for training all facility staff. That training includes: the principles of assisted living; changes associated with the aging process, including dementia; resident rights; how to perform direct ADL care; location of service plans and how to implement them; fire safety/emergency procedures; responding to behavior issues; infection control; food preparation and storage; and observation/reporting skills.
Residential care. Direct care staff must complete six hours of job related pre-service orientation covering the philosophy of residential care, review of residents’ unique needs, use of the service plan, nurse delegation, fire evacuation plans, and instruction in universal precautions. Training in the abdominal thrust, CPR and basic first aid training is recommended but not required. Twelve hours of in-service training must be completed annually.
Non-direct care staff must complete four hours of job related pre-service training that will include a review of the philosophy of residential care, 24 fire safety and fire evacuation plan, emergency procedures and instructions in universal precautions.
Background Check
Assisted living and residential care owners, administrators, and staff must satisfy a criminal records clearance under OAR Chapter 410, Division 007, and sign a criminal record authorization, Form SDS 303. A fingerprint check may be required.
Monitoring
Assisted living. State or Area Agency on Aging staff conduct periodic monitoring visits at least every two years. The facility must develop and conduct an ongoing quality improvement program that evaluates services, resident outcomes and resident satisfaction.
Residential care. Facilities are inspected at least every two years. Facilities not in compliance with the rules will submit a plan of correction that satisfies the Department within 10 days of receipt of the inspection report. In addition, the Department may impose sanctions for failure to comply with the licensing rules. Department staff may consult with and advise the facility administrator concerning methods of care, records, housing, equipment and other areas of operation.
Fees
$60 per facility.
For Alzheimer’s Care Units, there is a non-refundable endorsement fee that must accompany each application and upon license renewal. Fees are as follows:
- 16 or fewer residents: $50
- 17-50 residents: $75
- 100 or more residents: $100
Pennsylvania
Citation
Personal care homes, PC Title 55 Chapter 2620 and Chapter 20.
General Approach and Recent Developments
A major revision of the regulations for personal care homes is expected to be final in September 2004 and will be published as Chapter 2600. A draft version was published for comment in 2002. Based on over 900 comments, five subgroups were formed to make further recommendations in the areas of small and large homes; assessment and support plans; medication assistance; staffing and training; and resident’s rights. Developing a new quality assurance and improvement system is a priority of the licensing agency.
Legislation is pending that would create a licensing category for assisted living services and authorize a statewide Medicaid waiver covering assisted living services. A Medicaid waiver pilot program has been implemented in the Philadelphia area.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Personal care homes | 1,718 | 76,385 | 1,786 | 79,929 | 1,803 | 73,075 |
Definition
Personal care homes. “A premise in which food, shelter and personal assistance or supervision are provided for a period exceeding 24 hours for four or more adults who are not relatives of the operator, who do not require the services in or of a licensed long-term care facility, but who do require assistance or supervision in matters such as dressing, bathing, diet, financial management, evacuation of a residence in the event of an emergency or medication prescribed for self-administration.
Unit Requirements
The regulations require single occupancy rooms to have at least 80 square feet of floor space. If closets are built, they must be at least nine square feet and can be counted in the total required space. Multiple occupancy rooms must have at least 60 square feet per person. No more than four people may share a bedroom. Toilets must be available for every six residents, and tubs or showers for every 8 residents.
Bedrooms for one or more immobile residents may require additional square footage sufficient to accommodate the special needs of the residents, such as wheelchairs, special furniture and equipment.
Admission/Retention Policy
Homes may serve immobile residents who do not need nursing home care but do need personal care, if they meet building, fire safety, and staffing requirements. Homes may discharge anyone who is a danger to self or others; if the resident’s needs would require a fundamental alteration of the program; and residents whose functional level has advanced or declined such that the resident’s needs cannot be met in the facility even with supplemental services provided by outside providers.
Nursing Home Admission Policy
Consumers must have a medical diagnosis, illness, or condition which creates medical needs that require medical care and services which are ordered by or provided under the direction of a physician; need to be given on a regular basis and provided by or under the supervision of skilled medical professional; or because of a mental or physical disability, the individual requires nursing and related health and medical services in the context of a planned program of health care and management.
Services
Homes must have a written description of services and activities and the criteria for admission and discharge. An individual support plan is required within 30 days of completion of an assessment. Homes assist with personal hygiene and tasks of daily living as indicated in the support plan and assessment. The personal hygiene tasks include bathing, oral hygiene, hair grooming and shampooing, dressing and care of clothes, and shaving.
The tasks of daily living include securing transportation, shopping, making and keeping appointments, care of personal possessions, use of the telephone, correspondence, personal laundry, social and leisure activities, securing health care, ambulation, use of prosthetic devices and eating. Laundry service and activities are required.
Dietary
Facilities are required to provide three nutritionally well-balanced meals that follow recommended Daily Allowance of the Food and Nutrition Board. Each meal shall include an alternate food or drink item from which the resident may choose. Therapeutic diets prescribed by a physician are to be followed. In-service training requirements for administrators and staff include food handling, preparation, and sanitation.
Agreements
Agreements include the personal needs allowance; actual charges for each service or item for food, shelter, services, and additional charges and how, when, and by whom payment is to be made; personal care services provided and their cost; additional services available and their costs; the party responsible for payment; rules relating to home services; bed hold policy; refund policy; method of payment for long distance phone calls; arrangements for financial management, if any; house rules; termination conditions; resident rights; explanation of annual screening and medical evaluation requirements; provisions for handling rent rebate funds, if any; and a 30-day notice of changes in the contract.
Provisions for Serving People with Dementia
Draft rules contain provisions for securing units. Homes must notify the licensing agency of their intention to open a secured unit. Units must have adequate indoor and outdoor wandering space. Units may be shared by no more than two persons. A full medical and cognitive assessment is required. The written agreement includes disclosure of the services available and their costs, admission/discharge criteria, change in condition policies, and the special programming available to residents. Administrators and staff must have competency-based training that covers topics specified in the regulations (normal aging-cognitive, psychological, and functional abilities of older persons, definition and diagnosis of dementia, description of reversible and irreversible causes, and explanation of differences between dementia, delirium, and depression; definition of dementia and related disorders, progression, stages, and individual variability; communication techniques; description of behavioral symptoms of dementia and how to manage resident behaviors; the role of personality, culture, and environmental factors in behavioral symptoms and dementia care; philosophy of dementia care, including mission statement, goals, policies, and procedures; working with family members; resources for residents with dementia and their families; team building and stress reduction for the staff; older Adult Protective Services Act. The licensing agency may require additional staffing.
Medication Administration
A personal care home (PCH) may provide assistance with self-administration of medication. Assistance includes helping the resident to remember the schedule for taking the medication, storing the medication in a secure place and offering the resident the medication at the prescribed times. Medication not prescribed for self-administration must be administered by a licensed physician, nurse or dentist, as appropriate.
Public Financing
A pilot program, administered by the Department on Aging, operates in the Philadelphia area as a partnership at the local level between the Albert Einstein Healthcare Network and the Philadelphia Corporation for Aging (PCA), an Area Agency on Aging. The program began in June 2000 and planned to serve a projected 250 residents. About fifteen facilities were serving 60 participants in March 2004. A nurse practitioner from the Healthcare network visits participants weekly and offers monthly in-service training to personal care home staff while serving as a bridge between the primary care system and the long-term care system. The PCA case manager manages the home care benefit that includes, as indicated in a plan of care, personal care, respite care, adult day care, environmental modifications, transportation, medical equipment and supplies, personal emergency response systems, home health, and counseling. Services are delivered by outside providers rather than the facility and a consumer-directed option is pending. An exemption from state licensing provisions was granted to allow personal care homes to serve residents who qualified for admission to a nursing facility. The program expected to reduce emergency room use. An evaluation of the program will be completed and submitted to the state agencies in 2004.
The SSI/State Supplement payment in personal care homes is $958.30, which includes the personal needs allowance of $60 a month. In December 2003, there were 10,507 SSI beneficiaries in 1,726 licensed personal care homes.
Staffing
Facilities must provide a sufficient number of trained persons to provide the necessary level of care required by residents. Draft rules establish ratios for homes with mobile residents (one awake direct care staff per 15 or fewer residents, two for 16 to 30 and one for every additional 15 residents) and non-mobile residents (two for 15 or fewer residents; four for 16 to 30 residents and two more for every 15 additional residents). Additional staff hours are required to meet the laundry, food services, housekeeping, and maintenance needs.
Training
Administrators must be a licensed nursing home administrator, RN, or LPN or have an associate’s degree or 60 credit hours. Administrators must complete 40 clock hours of Department approved training which includes the following: fire prevention and emergency planning; first aid; medication procedures; medical terminology; personal hygiene; CPR and the Heimlich maneuver; local, state, and federal laws and regulations pertaining to the operation of a PCH; nutrition; food handling and sanitation; recreation; mental illness; gerontology; community resources and social services; staff supervision; development of orientation and training guidelines for the staff; and financial record keeping and budgeting.
Administrators must complete a minimum of 24 hours of annual competency-based training on first aid, medication self-administration, care for persons with dementia, infection control, personal care service needs, safety management techniques (positive interventions, reinforcing appropriate behavior, conflict resolution, identifying depression and others), mental illness and retardation if appropriate.
Administrators must complete a staff training plan that includes an annual assessment of training needs, a plan that addresses them and a mechanism to collect feedback on completed training. Each staff member must have a training plan based on education, experience and duties.
Within 30 days of employment or volunteer services, staff must receive orientation to the general operation of the home as well as training in fire prevention; smoking safety procedures; placement and use of fire extinguishers; operation of safety equipment; emergency planning and evacuation procedures and designated meeting place; resident rights; emergency medical plan; personnel policies and procedures; and general operation of the home. Direct care staff must be oriented to their duties, incident reporting and management, needs of residents, medication administration and purposes/side effects, universal precautions, and safety management techniques.
Staff receive training within six months in the following areas: medication procedures; medical terminology and personal hygiene; nutrition, food handling, and sanitation; recreation; mental illness; gerontology; and staff supervision, if applicable.
Background Check
Criminal history and background checks are required under protective services statutes.
Monitoring
The draft rules require homes to establish a quality assessment and management plan that includes incident reports, complaint procedures, staff training, monitoring licensing data and plans of correction, and resident and/or family councils. Surveys note that the most common violations are cited for housekeeping and maintenance and assistance with medications.
Penalties are assess for classes of violations, I, II or III, depending upon the severity, duration and the adverse effect on the health and safety of residents. Class I violations have a substantial probability of resulting in death or serious mental or physical harm to a resident. Class II violations have a substantial adverse effect upon the health, safety or well-being of a resident. Class III violations are minor violations which have an adverse effect upon the health, safety or well-being of a resident.
Penalties for each Class I violation is $20 per resident per day and must be corrected within 24 hours. Penalties for Class II violations are $15 per day per resident. No monetary penalties are assessed for Class III violations unless they are not corrected within 15 days which then result in a penalty of $3 a day per resident retroactive to the date of the citation.
PCH’s operating without a license are assessed a penalty $500 and $20 per resident day after 14 days, if the operator fails to file an application for a license.
Fees
Licensing fees are $15 per bed for 21 beds or less; $20 per bed for 21 to 50 beds; $30 per bed for 51 to 100 beds and $50 per bed for over 100 beds.
Rhode Island
Citation
Assisted living residence, R23-17.4 RCAL
General Approach and Recent Developments
In 2002, the rules changed the licensing category from residential care and assisted living facilities to assisted living residence, added a new section for the resident agreement, increased training requirements for administrators, and made other changes. Legislation was passed in 1997 authorizing the Rhode Island Housing and Mortgage Finance Agency (HMFA), working in collaboration with the Department of Human Services and the Department of Elderly Affairs, to serve up to 200 low- and moderate-income chronically impaired or disabled adults who are eligible for or at risk of entering a nursing home in facilities certified and financed by the HMFA.
The revised regulations were effective February 2004. The changes included a philosophy of care, new quality assurance requirements, staff training, additional requirements for Alzheimer dementia care units, reporting requirements, and a full functional assessment prior to admission, completed by a Registered Nurse.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted living facilities | 73 | 3,676 | 68 | 3,280 | 66 | 2,712 |
Definition
Assisted living residence is “a publicly or privately operated residence that provides directly or indirectly by means of contracts or arrangements personal assistance to meet the resident’s changing needs and preferences, lodging, and meals to two (2) or more adults. Assisted living residences include sheltered care homes, and board and care residences, or any other entity by any other name providing the above services which meet the definition of assisted living residence.” There are levels of licensure for residential care and assisted living facilities based on fire code requirements and need for assistance with medications. A residence may have areas within the facility that are licensed separately. The levels are:
Fire code classification:
- Level F1: licensure for residents who are not capable of self preservation; and/or
- Level F2: licensure for residents who are capable of self preservation; or
Medication classification:
- Level M1: licensure for residents who require central storage and administration of medications; or
- Level M2: licensure for facilities which only assist residents with self-administration of medications.
Alzheimer’s special care unit/program means any assisted living residence that locks, secures, segregates, or provides a special program or a special unit for residents with a diagnosis of probable Alzheimer or a related disorder, to prevent or limit access by a resident outside the designated or separated areas; and that advertises or markets the residence as providing specialized Alzheimer/dementia care. Facilities must be licensed as an “F1-M1” residence.
The State’s Medicaid waiver defines assisted living as “personal care and services, homemaker, chore, attendant care, companion services, medication oversight (to the extent permitted under state law), therapeutic social and recreational programming, provided in a home-like environment in a licensed community care facility. This service includes 24-hour, on-site response staff to meet unscheduled or unpredictable needs in a way that promotes maximum dignity and independence, and to provide supervision, safety and security.”
Unit Requirements
Resident rooms may have no more than two beds. Single rooms must have at least 100 square feet in area, and double bedrooms must be at least 160 square feet in area. There must be at least one bath per 10 beds and one toilet per eight beds or fraction thereof on each floor where residents’ rooms are located and not otherwise serviced by bathing facilities within the resident’s room. There must be an area within the resident’s bedroom and/or facility to be under lock for the safe keeping of personal possessions.
The Medicaid waiver allows sharing of units only by the consent of the residents.
Legislation authorizing the demonstration defines a unit as “an apartment, condominium, bed or other dwelling quarters in an assisted living facility as defined by this statute.”
Admission/Retention Policy
A resident must not require medical or nursing care as provided in a health care facility but who as a result of choice and/or physical or mental limitation requires personal assistance, lodging and meals and may require the administration of medication. A resident must be capable of self-preservation in emergency situations, unless the residence meets a more stringent life safety code. Persons needing medical or skilled nursing care, including daily professional observation and evaluation and/or persons who are bedbound or in need of the assistance of more than one (1) person for ambulation are not appropriate to reside in assisted living residences. However, an established resident may receive daily skilled nursing care or therapy from a licensed health care provider for a condition that results from a temporary illness or injury for up to twenty-one days or if the resident is under the care of a licensed hospice agency provided the assisted living residence assumes responsibility for ensuring that care is received.
Nursing Home Admission Policy
Nursing home residents must require the services of professional and/or qualified technical health personnel such as registered nurses, licensed practical nurses, physical therapists, occupational therapists, speech pathologists, audiologists, or require assistance with activities of daily living including walking, bathing, dressing, feeding, and toileting. The facility must provide these services under the supervision of licensed nursing personnel. Documentation of the nurse review is required monthly. Residences with a full time nurse may conduct the formal nurse reviews quarterly.
Services
A comprehensive assessment, on a form approved by the licensing agency (see http://www.health.ri.gov), is required prior to or during admission covering health, physical, social, functional, activity and cognitive needs and preferences. The form demonstrates that the resident meets the residency criteria and that the residence is able to meet their needs. A written service plan is required within a reasonable time after admission.
Services include twenty-four hour awake adult staffing; personal services; assistance with self-administration of medication or administration of medications by appropriately licensed staff; assistance with arranging for supportive services that may be reasonably required; monitoring health, safety, and well-being; housekeeping; laundry; medication assistance; and reasonable recreational, social services. Nurse review is necessary under all levels of medication licensure. A registered nurse must visit the facility at least once every 30 days to monitor the medication regimen for all residents; evaluate the health status of residents; make necessary recommendations to the administrator; follow up on previous recommendations; and provide signed, written reports to the facility documenting the visit.
Services covered by the demonstration waiver project include: personal care; homemaker; chore; attendant care; companion services; medication oversight; therapeutic, social, and recreational programming; transportation; 24-hour, on-site response staff to meet scheduled or unpredictable needs; and nursing and skilled therapy services which are incidental to the provision of supportive services.
Dietary
Facilities provide three balanced, varied meals each day and provide a diet that is appropriate to the resident’s medical regimen. The rules reference requirements in other state laws.
Agreements
Facilities are required to disclose the name of the owner and operator; the level of license with an explanation; admission and discharge criteria; services available; financial terms; terms of the residency agreement and contact information for the department, attorney general fraud and abuse unit, ombudsperson and local police offices.
The residency agreement has been modified and includes resident rights, admission criteria, discharge criteria, discharge policies, the unit to be rented, shared space and facilities, services to be provided or arranged, financial terms (basic rates, extra charges at admission or in the future, deposits and advanced fees and the rate increase policy), special care provisions, resident responsibilities and house rules, initial and ongoing assessment and service plan, and the grievance procedure.
Provisions for Serving People with Dementia
Facilities offering special care must disclose the form of care or treatment provided. The disclosure explains the philosophy and mission, the criteria for occupancy, transfer and termination; the process used for assessment and establishing the plan of service and its implementation, including the method by which the plan of service evolves and is responsive to changes in condition; staff training and continuing education practices; the physical environment and design features appropriate to support the functioning of cognitively impaired adult residents; the frequency and types of resident activities; the involvement in families and family support programs; and the cost of care and any additional fees.
A license for dementia is required when one or more resident's dementia symptoms impact their ability to function as demonstrated by any of the following: safety concerns due to elopement risk or other behaviors; inappropriate social behaviors that adversely impact the rights of others; inability to self preserve due to dementia; a physician's recommendation that the resident needs dementia support consistent with this level; or if the residence advertises or represents special dementia services or if the residence segregates residents with dementia. In addition to the requirements for the basic license, licensing requirements for the “dementia care” level shall include the following: staff training and/or requirements specific to dementia care as determined by the relevant state department; a registered nurse with special training must be on staff and available for consultation at all times; the residence shall provide for a secure environment appropriate for the resident population.
New direct service employees must receive at least twelve (12) hours of orientation and training in understanding various dementias; communicating effectively with dementia residents; managing behaviors.
Medication Administration
In M2 level facilities, unlicensed staff may only remind residents to take their medications and observe. M1 level facilities may administer medications including removing medication containers from storage, assisting with removal of a medication from a container, and/or directly administering the medication. Staff must have four hours of training by an RN regarding policies and procedures and have passed an exam based on the training.
Public Financing
The State has two waivers covering assisted living. One waiver covers a broad range of services and includes assisted living for residents who are relocating from nursing homes. Thirteen facilities contract with Medicaid and were serving 30 beneficiaries in 2002. Facilities receive a prospective Medicaid payment based on their customary rate not to exceed $1,400 a month, including room and board covered by SSI. The room and board charge is set by the facility. The SSI benefit, including the state supplement, standard is $1,159 in 2004. Beneficiaries retain $100 a month as a personal needs allowance. Income supplementation is not permitted. Nursing home residents receive case management to assist with relocation to the community. Case managers use community resources to address transitional expenses.
A second 1915 (c) waiver covers case management and assisted living services for elderly and adults with physical disabilities in a demonstration program involving the Department of Elderly Affairs and the Rhode Island Housing Mortgage and Finance Agency to develop affordable projects. Twenty-two facilities were serving 200 beneficiaries. The maximum payment from Medicaid is $37.00 per day for services. The room and board charge, usually between $800 and $900 a month, is separate from the Medicaid payment. The program will only reimburse facilities with single occupancy rooms with private baths. An additional 180 slots have been approved but not yet funded.
SSI beneficiaries that do not receive waiver services retain a PNA of $55 a month.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participants | Facilities | Participants | Facilities | Participants |
| 35 | 230 | 35 | 220 | NA | NA |
Staffing
Facilities must have a responsible adult on the premises at all times, who is in charge of the operation of the facility and who is physically and mentally capable of communication with emergency personnel. All facilities must provide staffing which is sufficient to provide the necessary care and services to attain or maintain the highest practicable physical, mental, and psycho-social well being of the residents, according to the appropriate level of licensing.
Training
Administrators must be at least 21 years old and obtain certification as a residential care/assisted living facility administrator or have equivalent training. Certification requirements include a training program covering topics referenced in the regulations. The course work must take place in a college, vocational training, state or national certification program which is approved by the Director of Health. Licensed nursing home administrators are considered certified. Administrators must complete at least 16 hours of continuing education annually.
Staff. New employees receive at least two hours of orientation and training in fire and emergency procedures; recognition and reporting of abuse, neglect, and mistreatment; assisted living philosophy (goals/values: dignity, independence, autonomy, choice); resident's rights; and confidentiality. Employees who have regular contact with residents and provide residents with personal care receive at least ten hours of orientation and training in: basic sanitation and infection control (i.e., universal precautions); food service; medical emergency procedures; basic knowledge of aging-related behaviors; personal assistance; assistance with medications; safety of residents; record-keeping; service plans; reporting; and where appropriate, basic knowledge of cultural differences. In-service training in appropriate topics is also required.
The Medicaid waiver requires a minimum one hour of orientation and twelve hours of annual in-service training for staff. Personal care services for “waiver” certified residents must be provided by Nursing Assistants.
Background Check
All employees are subject to a nationwide criminal records check through state or local police.
Monitoring
The licensing agency may inspect and investigate facilities as it deems necessary but at least once a year. Representatives of the licensing agency have the right to enter facilities any time without prior notice to inspect the premises and services. Every facility is given notice by the licensing agency of all deficiencies reported as a result of an inspection or investigation. A consultation/collaboration model may be implemented when additional staff are available. The licensing agency noted the importance of having registered nurses and pharmacy consultants available to monitor the assessment process, appropriateness of admission and medication issues.
The new rules require that residences develop, implement and maintain a documented, ongoing quality assurance program to attain and maintain a high quality assisted living residence through an on-going process of quality improvement that monitors quality, identifies areas to improve, methods to improve them, and evaluates the progress achieved. Areas subject to quality assurance review shall include at least personal assistance and resident services; resident satisfaction; and incidents (for example, resident complaints, medication errors, resident falls, and injuries of unknown origin).
The administrator is responsible for maintaining a written plan that includes three areas for quality assurance/improvement review and describe the monitoring, identification, and evaluation processes; tracking methods; and the person responsible for it.
Fees
$250 plus $50 per bed. Further increases are proposed for Fiscal Year 2005.
South Carolina
Citation
Assisted Living/Community Residential Care Facilities, R61-84
General Approach and Recent Developments
The State changed its licensing term to assisted living/community residential care facilities when revised regulations were adopted in July 2001. A Medicaid state plan amendment creating the integrated personal care program in community residential care facilities was implemented in 2002. Criminal background check guidelines were issued in October 2002. The 1976 State Code was amended by adding Section 40-30-980, allowing for the provision of selected prescribed medications by unlicensed persons with documented medication training and a skill competency evaluation.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Community residential care facilities | 504 | 16,641 | 545 | 17,761 | 553 | 16,119 |
Definition
Community residential care facility (CRCF). “A facility which offers room and board and which, unlike a boarding house, provides/coordinates a degree of personal assistance for a period of time in excess of twenty-four consecutive hours for two or more persons, eighteen years old or older, not related to the licensee within the third degree of consanguinity. It is designed to accommodate individual residents’ changing needs and preferences, maximize residents’ dignity, autonomy, privacy, independence and safety, and encourage family and community involvement. Included in this definition is any facility (other than a hospital) which offers or represents to the public that if offers a beneficial or protected environment specifically for individuals who have mental illness or disabilities.” These facilities may be referred to as Assisted Living provided they meet the definition of a community residential care facility.
Alzheimer’s Special Care Unit or Program. “A facility or area within a facility providing a secure, segregated special program or unit for residents with a diagnosis of probable Alzheimer’s disease and/or related dementia to prevent or limit access by a resident outside the designated or separated areas, and that advertises, markets, or otherwise promotes the facility as providing specialized care/services for persons with Alzheimer’s disease and/or related dementia or both.”
Unit Requirements
Bedrooms must offer 100 square feet for single rooms and 80 square feet per resident in multiple occupancy rooms. No more than three residents may share a room. One toilet is required for every six residents and one tub/shower for every eight residents. Pets are allowed.
Admission/Retention Policy
Facilities may only admit adults and may not admit anyone who is likely to endanger themselves or others, anyone suffering from acute mental illness, anyone needing hospital or nursing home care, or anyone needing continuous daily attention of a licensed nurse. Short term, intermittent nursing needs may be met by a Home Health Agency. Facilities must transfer anyone whose needs cannot be met by the facility in combination with services provided by hospice agencies or home health agencies. In June 2002, a list was issued that clarified who may not be served in CRCFs. The list includes:
- Daily skilled monitoring/observation due to an unstable/complex medical condition;
- Serious aggressive, violent, or socially inappropriate behavioral symptoms;
- Medications that require frequent dosage adjustment, regular intra-muscular and subcutaneous injections;
- Intravenous medications or fluids;
- Care of urinary catheter that cannot be cared for by the resident;
- Treatment of Stage II, III, or IV decubitus, or multiple pressure sores;
- Naso-gastric tube feeding;
- Suctioning;
- Tracheostomy or sterile care that cannot be managed by the resident;
- Receiving oxygen for the first time, which requires adjustment and evaluation of oxygen concentration;
- Dependency in all ADLs for more than 14 days; and
- Sterile dressing changes.
Nursing Home Admission Policy
Individuals qualify for an intermediate level of care if they need one of four intermediate services or meet two of four functional deficits. The criteria require either monitoring of significant medical conditions; dementia or behavior problems; or impairments requiring extensive assistance with five ADLs. The services include:
- Daily monitoring of a significant medical condition requiring overall care planning to maintain optimum health status;
- Supervision of moderate/severe memory impairment, manifested by disorientation, bewilderment, and forgetfulness which requires significant intervention in overall care planning;
- Supervision of moderately impaired cognitive skills; and
- Supervision of moderate problem behaviors manifested by verbal or physical abusiveness or socially inappropriate/disruptive behavior.
The functional deficits are:
- Requires extensive hands-on assistance with dressing and toileting and eating and physical help in bathing;
- Requires extensive assistance with locomotion;
- Requires extensive assistance to transfer;
- Requires frequent assistance with bladder or bowel care or with daily catheter or ostomy care.
Services
Facilities must provide appropriate assistance with ADLs, meals, special diets, medication assistance, at least one structured recreation activity each day, and transportation. Personal care includes assistance with ADLs; assistance with making appointments and arranging transportation to receive supportive services required in the care plan; being aware of the resident’s whereabouts; monitoring resident activities to ensure health, safety, and well-being, and arranging for routine and emergency health services, podiatry, dental, counseling, and medications.
An assessment of resident needs must be completed by a direct care staff member no later than 72 hours after admission. The facility must develop an individualized care plan with participation by the resident, administrator, and/or the sponsor or responsible party when appropriate, within seven days of admission. The plan must be reviewed and/or revised as changes in resident needs occur, but not less than semi-annually. The rules specify the content of the care plan.
Dietary
Three meals and snacks that meet dietary needs must be provided. Tray service is not permitted unless the resident is medically unable to go to the dining room or occasionally if the resident prefers. There must be trained staff/volunteers supervising food services who have a knowledge of food values to make appropriate substitution. If special diets are provided, the menus must be prepared by a professionally qualified dietician or reviewed by the physician or other qualified medical provider. The rules contain required servings by food group.
Agreements
The written agreement explains the specific care/services/equipment provided by the facility (administration of medications, special diets, assistance with ADLs), the fees for care/services/equipment, notice requirements for changes in fees, the dates a resident will receive their personal needs allowance, transportation policy, discharge/transfer provisions, and a statement of resident rights and the grievance procedure.
Provisions for Serving People with Dementia
Legislation passed in 1996 requires facilities advertised as special care facilities serving residents with Alzheimer’s disease to disclose the form of care and treatment that distinguishes it as being suitable for people with Alzheimer’s disease, the admission/transfer and discharge criteria, care planning process, staffing and training, physical environment, activities, the role of family members, and the cost of care. Staff must receive training in the care of persons with dementia, communication techniques, understanding and coping with behaviors, safety, activities, and other related topics.
Medication Administration
Facilities may administer medications and are responsible for ascertaining that medications are taken by residents in accordance with physicians’ orders. Non-licensed staff may administer medications if they have been trained by appropriately licensed individuals. Administration of medications has been expanded to include oral and topical medications, regularly scheduled insulin anaphylactic treatments under established medical protocols in addition to insulin and epinephrine injections. Flu injections and TB screening are performed by licensed nurses. Staff must verify orders for self-administration of medications.
Public Financing
The “integrated personal care program,” implemented in 2002, provides coverage of personal care in residential settings under the Medicaid state plan. The program serves elders, adults with disabilities, MR/DD, and individuals with mentally illness. To be eligible for coverage, beneficiaries must already receive the optional state supplement to the SSI program, which is available to persons residing in community residential care facilities, and require assistance with two ADLs, or need assistance with one ADL and have a cognitive impairment, be unable to live alone due to inadequate support, and need assistance to sustain maximum functional level. Facilities must contract with a licensed nurse at least one day a week who is responsible for providing personal care training to staff, and developing and monitoring care plans of individuals served by the integrated personal care program. Facilities participating in the integrated personal care program must be able to provide medical monitoring, medication administration, personal care and also be ADA compliant. The program contracts with 35 facilities serving 600 participants. Facilities receive $1,055 per participant per month, on average. This rate is calculated using a standard formula, and is comprised of a reduced optional state supplement payment, resident funds, and an integrated personal care program daily rate of $12.80 per participant per day. The optional state supplement is reduced by a calculated amount in order to draw down Medicaid match for the daily rate.
The optional state supplement program cap is $912 per month. The facility receives $865 per month for room, board and services and the resident retains a $47 personal needs allowance. Family supplementation is not allowed.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participants | Facilities | Participants | Facilities | Participants |
| 35 | 600 | NA | NA | NA | NA |
Staffing
At least one staff member shall be available for every eight residents during the day and one per 30 residents at night. Facilities with more than eight residents must have one staff member awake and dressed at night. Awake staff are required in facilities of less than eight if there are residents with dementia. In multi-story buildings, staff must be on each floor at all times that residents are present.
Training
Administrators must be licensed by the South Carolina Department of Labor, Licensing and Regulation, and be mentally and emotionally capable of meeting the responsibilities involved in operating the facility in order to ensure the facility is in compliance with the regulations and shall demonstrate adequate knowledge of the regulations.
Staff. In-service training programs shall be planned and provided for all personnel and shall include at least: basic first aid; procedures for checking and recording vital signs; care of persons with communicable diseases; use of restraints; medication management; care for persons with dementia (if applicable); CPR; confidentiality and residents’ rights; OSHA standards for blood borne pathogens; and fire response training. Staff receive basic information on these topics during orientation. Training shall be provided on a continuous basis and not less than annually.
Background Check
Staff must not have any prior convictions or pleas of nolo contendere for child or adult abuse, neglect, or mistreatment, and facilities must check appropriate registries.
Monitoring
Facilities are inspected prior to licensure and at least every three years or more frequently as needed. Facilities must submit a plan of correction to the State licensing agency when issues of noncompliance are documented. A schedule for monetary penalties is included in regulation. Consultations are available as requested by facilities or as deemed appropriate by the State.
Facilities must have a written quality improvement program. The program must establish desired outcomes and the criteria by which effectiveness is accomplished; identify and evaluate the causes of deviation from desired outcomes; develop action plans to prevent future deviations; establish quality indicators; analyze appropriateness of care plans; review all incidents and accidents including resident deaths, and infection or other occurrences that threaten the health and safety of residents; and create a systematic method of obtaining feedback from residents and other interested parties on the level of satisfaction with care and services received.
Fees
$10 per bed or $75 whichever is greater.
South Dakota
Citation
Assisted living centers, Article 44:04 et seq.
General Approach and Recent Developments
Regulations for assisted living centers are part of the chapter pertaining to medical facilities. Regulations were revised in December 2001 and further minor revisions to the regulations were final in December 2002.
The State is currently revising assisted living rules relating to the Life Safety Code. Changes will allow assisted living centers co-located with a nursing facility or other medical facility to share staff as it relates to the Life Safety Code. Additionally, assisted living centers that have sprinkler systems installed and show consistent adequate evacuation times will receive a reduced staffing ratio as it relates to the Life Safety Code.
The State’s Medicaid waiver program will be amended in 2004 to include assisted living. Currently, the Medicaid waiver program only allows for medication administration in assisted living centers. The Personal Needs Allowance will increase in FY 2005.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted living centers | 162 | 3,360 | 153 | 3,084 | 127 | NR |
Definition
An assisted living center is defined as “any institution, rest home, boarding home, place, building, or agency which is maintained and operated to provide personal care and services which meet some need beyond basic provision of food, shelter, and laundry to five or more persons in a free standing, physically separated facility.”
Unit Requirements
In newly constructed or renovated facilities, there must not be more than two residents per room. In single bedrooms, there must be a minimum area of 120 square feet, and in rooms with two beds there must be at least 200 square feet. Each resident room must have a toilet room and lavatory.
Admission/Retention Policy
Prior to admission, residents must submit written evidence from their physician of a physical examination certifying that they are in reasonable good health and free from communicable disease, chronic illness, or disability which requires any services beyond supervision, cueing, or limited hands-on physical assistance to carry out normal activities of daily living and instrumental activities of daily living. The assisted living center must conduct an evaluation of each resident's care needs at the time of admission, 30 days after admission, and annually thereafter, to determine the facility can meet the needs for each resident. The rules specify the contents of the evaluation.
Assisted living centers may not admit or retain residents who require more than intermittent nursing care or rehabilitation services. Facilities that admit or retain residents who require administration of medications must employ or contract with a licensed nurse who reviews resident care and conditions at least weekly and a registered nurse or pharmacist who provides medication administration training to unlicensed assistive personnel who administer medications.
A call system is required for facilities serving people who cannot walk independently. Other requirements affect facilities serving people needing therapeutic diets, people who are not capable of self-preservation, or who need oxygen.
The resident may remain in the facility and may not be transferred or discharged unless the resident's needs and welfare cannot be met by the facility, the resident's health has improved sufficiently so the resident no longer needs the services provided by the facility, the safety or health of individuals in the facility is endangered by the resident, the resident has failed to pay for allowable billed services as agreed to, or the facility ceases to operate.
Nursing Home Admission Policy
The medical review team may assign an individual to a nursing facility level of care classification if the individual requires any of the following services:
- Continuing direct care services which have been ordered by a physician and can only be provided by or under the supervision of a professional nurse. These services include daily management, direct observation, monitoring, or performance of complex nursing procedures. For purposes of this rule, continuing care is repeated application of the procedures or services at least once every 24 hours, frequent monitoring, and documentation of the individual's condition and response to the procedures or services;
- The assistance or presence of another person for the performance of any activity of daily living according to an assessment of the individual's needs completed according to §44:04:06:15; or
- In need of skilled mental health services or skilled therapeutic services, including physical therapy, occupational therapy, or speech/language therapy in any combination that is provided at least once a week.
Services
Skilled nursing services or rehabilitation services provided to residents of assisted living centers must be limited to less than eight hours per day and 28 or fewer hours each week. The service providing the care must specify a planned completion date based on the assessments conducted. An unlicensed employee of a licensed facility may not accept any delegated skilled tasks from any non-employed, non-contracted skilled nursing and therapy providers. Centers must provide supportive services, activities, and services to meet the spiritual needs of residents. Outside services utilized by residents must comply with and complement facility care policies. Assisted living centers must provide for the availability of physician services. All residents must be seen by a physician at least once a year.
Dietary
At least three meals must be served daily at regular times. The facility must provide environmental and social accommodations for each patient or resident to encourage eating in the common dining area. Assistance must be provided for patients or residents in need of help in eating.
There must be an organized dietetic service that meets the daily nutritional needs of residents and ensures that food is stored, prepared, distributed, and served in a manner that is safe, wholesome, and sanitary in accordance with the rules. The dietetic service must ensure that food prepared is nutritionally adequate in accordance with the Recommended Dietary Allowances. Reasonable substitutions of equal nutritional value must be available to offer patients or residents who refuse or are unable to eat the food served. A current diet manual including basic nutrition information must be available in all assisted living centers.
Centers admitting residents that need special diets that cannot be developed using a simplified diet manual must employ or contract with a dietician who shall approve written menus and diet extensions, approve special diet needs, plan individual diets, and provide guidance to dietary staff in areas of preparation, service, and monitoring. The frequency of visits is determined by the residents’ needs and the center’s ability to implement diets correctly.
Agreements
Resident agreements must be signed upon move-in and must describe the services available and the charges; other services offered and the additional charges; policies for protection of personal funds; a list of names, addresses, and phone numbers of client advocates; description of the process for filing a complaint concerning abuse, neglect, and misappropriation of funds; how to contact the resident’s physician; how to apply for Medicaid and Medicare; the center’s bed hold policy; and the responsibilities of residents and family concerning self-administration of medications. Legislation passed in 2001 (SB 244) requires disclosure of charges for resident care and accommodations.
Provisions for Serving People with Dementia
Facilities that admit or retain residents with cognitive impairments must have the resident’s physician determine and document if services offered by the facility continue to enhance the functions in ADLs and identify if other disabilities and illnesses are having an impact on the resident’s cognitive and mental functioning. All staff members must attend an annual in-service training in the care of the cognitively impaired and those with unique needs. Such facilities must have exit alarms. The facility must be licensed for medication administration.
Medication Administration
Centers serving people who require administration of medication must employ or contract with a licensed nurse who reviews resident care and conditions at least weekly and with a registered nurse or pharmacist who provides medication administration training. Aides who have passed required training may administer medications.
A resident with the cognitive ability to understand may self-administer medications or instruct another responsible person to administer the resident's medications. At least every three months, the supervising nurse or the physician must evaluate and record the continued appropriateness of the resident's ability to self-administer medications.
Concerns exist with facilities who establish policies requiring medication administration versus allowing a resident to self-administer medications by choice and ability. The State wishes to encourage resident independence, rather than require a person to have medications administered by staff.
Public Financing
Services for elders are covered by a state optional supplement program and a limited HCBS waiver. The state optional supplement program is not a state supplement to the SSI payment. It serves Medicaid eligible adult and elderly beneficiaries who meet assisted living level of care criteria, as described in Chapter 67, Section 45:01:04 of the state administrative rules. The payment rate for room, board and services is $1,094 a month, up from $1,019 a month in 2002. The state program supplements resident funds up to the monthly rate. Ninety facilities participate in the state program and serve 227 beneficiaries.
The Medicaid HCBS waiver covers a single service, medication administration, in assisted living centers. Individuals must be 65 years of age or older, financially eligible and meet nursing home level of care criteria. Centers receive a total payment of $43.92 per day or $1,317a month (30 days) which includes a room and board payment of $534 (the resident keeps $30 for personal needs allowance) from the resident and the Medicaid payment for medication administration services. Family supplementation is not allowed for either the state optional supplement or the Medicaid HCBS waiver programs. Individuals may not participate in both programs simultaneously. One hundred and forty facilities participate in the Medicaid waiver program and serve 500 residents.
| Program | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Participants | Facilities | Participants | Facilities | Participants | |
| State | 90 | 227 | NR | NR | NR | NR |
| Medicaid | 140 | 500 | 110 | 250 | 110 | 165 |
Staffing
All assisted living centers must maintain one staff person on duty at all times and a minimum of 0.8 hours of direct resident care by personnel of the center for each resident for each 24-hour period. For facilities with ten or fewer beds, one staff person is permitted during sleeping hours. This staff person may sleep if: the facility fire alarm is adequate to alert staff, a staff call system is available, the staff bedroom has an egress window, and the residents are capable of prompt evacuation. For facilities with 11 to 16 beds, one staff person who is awake is required during sleeping hours.
Training
Administrator. The administrator must have a high school diploma or equivalent and, if hired after July 1, 1995, must complete a 75-hour training program and competency evaluation. The areas covered include: communication and interpersonal skills; infection control; safety/emergency procedures; promoting resident independence; and respecting resident rights. Additional topics cover: basic nursing skills; personal care skills; mental health and social services; care of cognitively impaired residents; basic restorative services; and resident rights.
Staff. The facility must have a formal orientation program and an ongoing education program for all personnel. These programs must include the following subjects:
- Fire prevention. The facility must hold at least one fire drill for each shift each quarter;
- Emergency procedures;
- Infection control and prevention;
- Accident prevention and safety procedures;
- Proper use and documentation of restraints;
- Resident rights;
- Confidentiality of resident information;
- Incidents and diseases subject to mandatory reporting and the facility’s reporting mechanism; and
- Care of the cognitively impaired and of those patients or residents with unique needs.
The person-in-charge of dietary services shall possess a current certificate from a ServSafe Food Protection Course, the Certified Food Protection Professional's Sanitation Course from the Dietary Managers Association, or equivalent training determined by the Health Department.
Background Check
A facility may not knowingly employ any person with a conviction for abusing another person.
Monitoring
The governing body of the facility must provide for an ongoing evaluation of the quality of services provided to residents. Quality assurance evaluations must include the establishment of facility standards, interdisciplinary review of resident services to identify deviations from the standards and plans of correction, resident satisfaction surveys, utilization of services provided, and documentation of the evaluation.
The State provides extensive education and support to facilities regarding quality of care and compliance with regulations. Licensing staff are invited regularly to present at the semi-annual association meetings. The state licensing office distributes to facilities up-to-date information concerning quality and trends in assisted living. The State has established a public hearing process at least annually where providers are able to address issues with the State in an open forum.
Fees
$100 plus $3 for each licensed bed.
Tennessee
Citation
Assisted Care Living Facilities, Rules of the Department of Health, Chapter 1200-8-25 et seq.
Homes for the Aged, Chapter 1200-8-11
General Approach and Recent Developments
Assisted care living facility rules were revised in 2003. Changes were made in the provisions for the reporting of unusual events, policies and procedures for health care decision-making for incompetent residents, and the retention of residents.
Several legislative proposals dealing with fire safety are being considered in the 2004 Legislative session. Legislation requiring sprinklers in all nursing homes, Assisted Care Living Facilities (ACLFs), and Residential Homes for the Aged passed. Most ACLFs already meet the requirement for sprinklers, as the rules and licensing of ACLFs did not go into effect until 1998. ACLFs that were exempted from the requirements now have to submit a plan to come into compliance.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted care living facilities | 184 | 10,669 | 178 | 10,495 | 160 | 8,691 |
| Homes for the aged | 155 | 3,230 | 166 | 3,307 | 198 | 3,994 |
Definition
Assisted care living facility (ACLF) means a building, establishment, complex, or distinct part thereof which accepts primarily aged persons for domiciliary care and which provides on site to its residents room, board, non-medical living assistance services appropriate to the residents' respective needs, and medical services as prescribed by each resident's treating physician, limited to the extent not covered by a physician’s order to a home care organization and not actually provided by a home care organization. An ACLF may directly provide such medical services as medication procedures, topicals, suppositories and injections (excluding intravenous) pursuant to a physician’s order, and emergency response. All other skilled nursing services (part-time or intermittent nursing care, physical occupation and speech therapy, medical social services, medical supplies other than drugs and biologicals, and durable medical equipment) that a home care organization is licensed to provide may be provided in the facility only by a licensed home care organization, except for home health aide services.
Home for the aged means a home which accepts aged persons for relatively permanent, domiciliary care. A home for the aged may be any building, section of a building, or distinct part of a building, a residence, a private home, a boarding home for the aged, or other place, either for profit or not, which provides, for a period exceeding 24 hours, housing, food services, and one or more personal services for one or more aged persons who are not related to the owner or administrator by blood or marriage. Homes for the aged must have agreements with a physician who is available to render care or who will come to the home to visit residents when necessary and with a nursing home that will accept its residents who must be discharged.
Unit Requirements
Assisted care living facility. A minimum of 80 square feet of bedroom space must be provided for each resident. No more than two residents may share a bedroom. No more than six residents may share a toilet, lavatory, bath, or shower.
Home for the aged. Each resident must have at least 80 square feet of bedroom space. Bedrooms may not have more than two beds, and privacy screens or curtains must be provided and used when requested by the resident. Beds with full side rails, potty chairs, bedpans, or urinals shall not be used routinely in residents' rooms. Residents' rooms must always be capable of being unlocked by the resident.
Admission/Retention Policy
Assisted care living facilities may not admit or retain anyone who: is in the later stages of Alzheimer's disease, requires physical or chemical restraints, poses a serious threat to self or others, requires nasopharyngeal and tracheotomy aspiration, requires initial phases of a regiment involving administration of medical gases, requires a Levin (or nasogastric) tube, requires arterial blood gas monitoring, is unable to communicate his or her needs, or requires treatment of Stage III or IV decubitus ulcer or exfoliative dermatitis.
Facilities may not admit, but may retain for 21 days, any resident requiring intravenous or daily intramuscular injections or intravenous feedings; gastronomy feedings; insertion, sterile irrigation, and replacement of catheters, except for routine maintenance of Foley catheters; or requiring sterile wound care.
Under regulatory changes adopted in 2003, if a resident’s condition is stable, and the resident is able to care for his or her condition without the assistance of facility personnel or home health care and has a documented history of self-care for their medical condition for at least one year which is documented by a physician and a part of the medical record, a facility may accept for admission and allow the continued stay of a person who has in place a gastrostomy tube or percutaneous endoscopic gastrostomy tube, has in place a catheter that is their sole means of elimination of waste, or requires the routine administration of oxygen. If a person is no longer able to self-care for his or her medical condition(s), the facility must immediately transfer the resident to a licensed nursing home or hospital.
Residents with these conditions may be retained longer than 21 days if the Health Department is notified and does not object. However, residents may not be retained after 21 days if they require four or more skilled nursing visits per week for any other condition.
Home for the aged. Residents who need continual professional medical/nursing observation and/or care cannot be admitted or retained. Residents who require more technical nursing care or medical care than the personnel and the facility can lawfully provide shall be transferred to a hospital or nursing home. Homes for the aged cannot admit a person whose primary diagnosis is a mental health condition which clearly endangers himself or others and/or who is receiving active treatment from a mental health facility for a condition which clearly endangers himself and others. Homes for the aged may serve people with mental health conditions, but these residents may not make up more than 50 percent of the home’s residents. Persons in the early stages of Alzheimer’s disease and related disorders may be admitted if an interdisciplinary team made up of a physician who is experienced in the treatment of Alzheimer’s disease, a social worker, registered nurse, and a family member (or patient care advocate) determines that care can appropriately and safely be given in the home for the aged. Such residents must be reviewed at least quarterly as to the appropriateness of placement in the home.
Nursing Home Admission Policy
Care must be expected to improve or ameliorate the individual’s physical or mental condition, prevent deterioration in health status, or delay progression of a disease or disability. Individuals must have a condition that requires daily in-patient nursing care and need help with one or more of the following: transfer to and from bed, chair or toilet; mobility; eating; toileting (including use of toilet or incontinence care); expressive or receptive communication; orientation; medication administration; behavior; or skilled nursing or rehabilitative services at a greater frequency, duration, or intensity than can practically be provided through a daily home health visit. Assistance with ADLs must be daily or multiple times per week. Nursing care includes observation and assessment, administration of legend drugs, supervision of nurses aides, and other skilled nursing therapies performed by LPNs or RNs.
Services
Assisted care living facility. Personal services include supervision and assistance with ADLs (but not nursing or medical care). Medical services such as medication procedures, administration of medications, emergency response services, and home care organization services prescribed by a physician and as allowed by law may be offered.
Home for the aged. Assistance and supervision with medications is allowed and medications may be administered by a licensed nurse. Homes for the aged may not care for residents who require restraint, and so must not use restraints. Homes may provide personal care such as bathing, dressing, and grooming of hair, fingernails, and toenails. Laundry and linen services, food service, and recreational activities are also provided.
Dietary
Dietary services must be directed and staffed by adequate qualified personnel. An outside company may provide food services if they have a dietician available. An employee who is qualified by experience or training must serve as director of food and dietetic services. The facility must have access to a qualified dietician. Three meals a day are required that constitute an acceptable and/or prescribed diet. Therapeutic diets must be prescribed by a practitioner.
Agreements
Agreements must include the procedure for handling transfers or discharges. Accurate written statements regarding fees and services must be provided upon admission but are not part of the agreement.
Changes in 2003, require that each facility maintain and establish policies and procedures governing the designation of a health care decision-maker for making decisions on behalf of a resident who is incompetent or who lacks decision-making capacity, including but not limited to allowing the withholding of CPR measures from individual residents. The facility must inform the resident and/or the resident’s decision-maker of these policies and procedures upon admission or at such time as is appropriate. Rules also require a facility to identify who the decision-maker will be for a person who is incompetent or who lacks decision-making capacity.
Provisions for Serving People with Dementia
Residents in all but the latter stages of Alzheimer’s disease may be admitted only after determination by an interdisciplinary team that care can be safely and appropriately provided. This determination must be reviewed quarterly. Facilities with secure units must report on a series of items normally included in disclosure provisions such as: assessments by multi-disciplinary teams and reviews; number of deaths, hospitalizations and incidents; staffing pattern and ratios; daily group activities; and staff training.
Medication Administration
Assisted care living facility staff may assist with self-administration of medications. A licensed professional may administer medications within the scope of his or her license.
The Department of Health developed medication guidelines that outline 3 levels: (1) medication observation/assistance includes reading of labels and verbal prompting; (2) self-administered medication means that a resident is independent with medications; (3) medication administration is allowed by licensed professional staff only.
Public Financing
Assisted care living facilities. The licensing law does not authorize Medicaid coverage for medically necessary home care services provided in an assisted care living facility. The State recently received approval to expand its Medicaid waiver statewide. Although assisted living is not a covered service, facilities are reimbursed for respite care. Eligible waiver beneficiaries may receive up to nine days of respite care per year at a rate of $91.93 per day. There is no state supplement to the federal SSI payment for assisted living.
Home for the aged. Personal care is not funded by Medicaid either as a state plan service or as a waiver service. An SSI pilot program called the Quality Enabling Program provides $525,100 annually to supplement what a facility receives from a resident. The program pays up to $9 a day per resident. This program is only available in 20 counties.
Staffing
Assisted care living facilities. There must be sufficient staff to meet the needs, including medical services, of residents. Facilities must have a licensed nurse available.
Training
Assisted care living facility administrators. Administrators must be certified biannually. Certification requires 24 classroom hours of continuing education courses approved by the board that includes instruction in the following: state rules and regulations for homes for the aged/ACLFs; health care management; nutrition and food service; financial management; and healthy lifestyles.
Homes for aged administrators. The licensee of a home for the aged must be at least 18 years old. The chief administrator of the home must be certified by the Board as a residential home administrator, unless the administrator is currently licensed in Tennessee as a nursing home administrator. The licensee must have a high school diploma or equivalent; persons serving as a chief administrator of a licensed home for a continuous period of at least nine months prior to January 1990 are exempt from this requirement. Licensees must have at least 24 hours of continuing education each year. Personal care attendants must be at least 18 years old. Facilities with five or more residents whose level of evacuation capability is classified as “slow” must have a responsible attendant on duty and awake at all times.
Assisted care living facility staff. No continuing education is required for direct care staff.
Homes for aged staff must attend any training program which may be required by the Department when such programs are offered without charge in each of the three regions of the State, and no more frequently than annually.
Background Check
The administrator must not have been convicted of a criminal offense involving abuse or intentional neglect of an elderly or vulnerable individual. Facilities may not employ any person listed on the Department’s abuse registry.
Monitoring
Revised rules in 2003 added language concerning the reporting of unusual events. A facility must report the abuse of a patient or unexpected occurrence or accident that results in death, life threatening or serious injury to a patient to the Department of Health within 7 business days. Circumstances which could result in an unusual event are outlined in regulation. Specific incidents that may result in a disruption of the delivery of health care services at the facility shall also be reported within 7 business days. The facility must file with the Department of Health a corrective action report within 40 days of the identification of the event.
Inspections are conducted each year. The state inspection and monitoring process serves as a regulatory function only. However, when the State develops policy or interpretive guidelines, they do request the input of industry providers. If through the oversight process a particular problem area is identified, the State will work with the assisted living association to provide training and education at association meetings, rather than provide one on one consultation and training to individual providers.
Deficiencies must be addressed by plans of correction. Homes must comply with local fire safety authority regulations.
The Department of Health develops interpretive guidelines for regulations. Department policy was issued to all ACLFs in January 2004 to provide criteria for hospice waivers in ACLFs. Another policy bulletin was issued concerning T.C.A. 68-11-20(5)(A)(i) which prohibits residents with latter stages of Alzheimer’s disease or related disorders from being admitted or retained in an ACLF.
Fees
Fees for assisted care living facilities vary with the number of beds:
- Fewer than 25 beds ($600);
- 25 to 50 beds ($800);
- 50 to 74 beds ($950);
- 75 to 99 beds ($1,100);
- 100 to 124 beds ($1,250);
- 125 to 149 beds ($1,400);
- 150 to 174 beds ($1,550); and
- 175 to 199 beds ($1,700).
Facilities with over 200 beds are charged $1,700 plus $150 for every 25 beds or fraction thereof.
Texas
Citation
Assisted living facilities, Texas Revised Health and Safety Statutes Annotated §247.001 et. seq.;
Texas Administrative Code Title 40, Chapter 92 et seq; Title 40 §46.13; and §48.6003; §19.2409
General Approach and Recent Developments
The purpose of the regulations states that assisted living services are driven by a service philosophy that emphasizes personal dignity, autonomy, independence, and privacy. Assisted living services should enhance a person's ability to age in place in a residential setting while receiving increasing or decreasing levels of service as the person's needs change.
The State licenses several types of assisted living facilities. Regulations were revised in 2002 and 2003. Further changes were proposed in 2004 adding definitions and authorizing electronic monitoring, setting an administrative penalty schedule, and requiring central air conditioning in new facilities. Only licensed facilities may use the term assisted living, and the statute requires careful monitoring to detect and report unlicensed facilities.
Assisted living/residential care services are covered by the State's Medicaid Home and Community Based Services (CBA) waiver program in licensed assisted living facilities. Settings must be licensed as assisted living facilities and may contract with Medicaid under three models: assisted living apartments, residential care apartments, and residential care non-apartments.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted living facilities | 1,378 | 42,245 | 1,324 | 41,424 | 1,304 | 39,596 |
Definition
Assisted living facility is an establishment that furnishes, in one or more facilities, food and shelter to four or more persons who are unrelated to the proprietor of the establishment, and provides personal care services.
Facilities for persons with Alzheimer’s disease. Facilities that advertise, market, or otherwise promote their capacity to provide personal care services for people with Alzheimer’s disease must be certified as a Type B facility.
Facilities for supervision of medication and general welfare is a separate category of assisted living that provides only medication supervision.
The rules license the following types of assisted living facilities:
-
Type A home residents are capable of evacuating the facility unassisted, do not require routine attendance during night-time hours, and are capable of following directions under emergency conditions.
-
Type B facility residents may require staff assistance to evacuate, may not be able to follow directions, require attendance during the night, and while not permanently bedfast, may require assistance in transferring to and from a wheelchair.
-
Type C facilities are four-bed adult foster care facilities.
-
Type E facilities serve residents who are capable of self-evacuation and may provide general supervision and medication supervision but not assistance with activities of daily living.
Medicaid. Assisted living/residential care services provide a 24-hour living arrangement for persons who, because of a physical or mental limitation, are unable to continue independent functioning in their homes. Services are provided in assisted living facilities licensed by the Texas Department of Human Services (DHS). In effect, the rules recognize three types of units provided in licensed assisted living facilities. Community Based Alternatives (CBA) waiver participants are responsible for their room and board costs and, if applicable, a co-payment for assisted living/residential care services.
Unit Requirements
Rules require 80 square feet for single bedrooms and 60 square feet per bed for multiple occupancy rooms in Type A facilities and 100 square feet and 80 square feet respectively in Type B facilities. A maximum of four people may share a room. Units with separate living/dining and bedroom space may include 10 percent of the required bedroom space as living area. Not more than 50 percent of the beds may be in rooms of three or more. Bathrooms, including bathing units, are required for every six residents.
The Medicaid program guidelines distinguish among assisted living apartments, residential care apartments, and residential care non-apartments. Assisted living apartments must provide each participant a separate living unit to guarantee his or her privacy, dignity, and independence. Units must include individual living and sleeping areas, a kitchen, bathroom, and adequate storage. Units must provide 220 square feet, excluding bath, but units in remodeled buildings may provide 160 square feet. Double occupancy units may be provided if requested.
Residential care apartments must be double occupancy with a connected bedroom, kitchen, and bathroom area providing a minimum of 350 square feet per client. Indoor common space used by residents may be counted in the square footage requirement. Kitchens must be equipped with a sink, refrigerator, cooking appliance (stove, microwave, built-in surface unit) that can be removed or disconnected, and space for food preparation.
A residential care non-apartment means a licensed assisted living facility which does not meet either of the above definitions. These units may be double occupancy units in free standing buildings that have 16 or fewer beds.
Admission/Retention Policy
Type A facility residents must be capable of evacuating without assistance; do not require routine attendance during nighttime hours; and are capable of following directions.
Type B facility residents may require staff assistance to evacuate; be incapable of following directions; require attendance during nighttime hours; and may not be permanently bedfast but can require assistance with transfer.
Facilities may not admit or retain residents whose needs cannot be met by the facility, or residents requiring services from the facility's RN on a daily or regular basis (exceptions are made for residents with terminal conditions or for short-term needs).
Type A and B facilities may request a waiver for residents who do not meet the retention standards if there is a physician assessment stating the resident is appropriately placed and a statement from the resident that they wish to remain in the facility.
Nursing Home Admission Policy
To be eligible for the Community Based Alternatives (CBA) Program or nursing facility care, a client must require licensed nursing care (RN or LVN) or meet two or more of the criteria for nursing home risk as follows:
- Needs assistance with one or more of the activities of dressing, personal hygiene, eating, toilet use, or bathing;
- Has had a functional decline in the past 90 days;
- Has a history of a fall two or more times in the past 180 days;
- Has a neurological diagnosis of Alzheimer's, head trauma, Multiple Sclerosis, Parkinsonism, or dementia;
- Has a history of nursing facility placement within the last five years;
- Has multiple episodes of urine incontinence daily; and
- Goes out of one's residence one or fewer days a week.
Services
An assisted living facility provides home management tasks (housekeeping, changing bed linens, laundry, shopping); transportation and escort service to medical appointments, shopping, and recreation activities; 24-hour supervision; social and recreational activities; and room and meals. Activities and social programs must be available at least weekly.
An assessment that includes information on listed areas must be completed within 14 days of admission. Rules allow licensed staff to administer medications and provide occasional treatment which enables residents to maintain independence. Residents may contract to have home health services provided.
Services that can be provided through a waiver include 24-hour supervision, personal care, administration of medications, congregate meals, and social and recreational activities. Nursing services must be provided through contracts with certified home health agencies.
Dietary
Meal services include planning, cooking, and serving three meals a day that are essential to the client’s health and well-being. Meals must supply a balanced, nutritious diet as recommended by the National Food and Nutrition Board. Therapeutic diets must be provided according to a service plan. Diets that cannot be prepared by a lay person must be calculated by a qualified dietician. Dietary counseling and nutrition education must be available. Facilities designate a person who will be responsible for food service.
Agreements
Assisted living facilities are required to complete a consumer disclosure statement developed by the Department that includes pre-admission, admission, and discharge processes; resident assessment and service plans; staffing patterns; the physical environment of the facility; resident activities; and facility services. An admission agreement is required that includes the services provided and charges for services, including any nursing services, with a statement that such services and supplies could be a Medicare benefit.
Facilities must have written policies regarding admission policy, services provided, charges, refunds, responsibilities of the facility and residents, privileges of residents, and other rules and regulations which are made available to residents and staff.
Provisions for Serving People with Dementia
A disclosure statement is required that describes the nature of the care or treatment provided and describes the pre-admission process, admission process, discharge and transfer, planning and implementation of care, change in condition issues, staff training on dementia care, the physical environment, and staffing.
Alzheimer’s facilities must have activities that encourage socialization, cognitive awareness (crafts, arts, story telling, reading, music, discussion, reminiscences, and others), self-expression, and physical activity in a planned and structured program.
All staff must have four hours of dementia-specific training before assuming duties; 16 hours of on-the-job supervision during the first 16 hours of employment; and 12 hours of annual in-service training. Facilities with 17 or more residents must have an activity director 20 hours a week. Smaller facilities designate a person to plan, supply, implement, and record activities.
Medication Administration
The rules allow licensed staff and medication aides to administer medications as well as to assist with or supervise medications. Delegation to unlicensed aides is allowed.
Public Financing
A Medicaid HCBS waiver, Community Based Alternatives (CBA), covering assisted living and other services, was effective in 1994 and serves elders and adults with disabilities. Providers that participate in the waiver must meet additional Medicaid standards that include additional training for managers and staff, required services, interdisciplinary team meetings (resident, facility and the Department of Human Services’ case manager, registered nurse or contract manager). A tiered payment system was implemented in September 2000 for services covered by a Medicaid HCBS waiver. Two sets of rates have been developed, enhanced rates for providers that agree to pass through wage increases to direct care workers and a lower set of rates for other providers. Payments vary by level and by setting. The enhanced rates range from $45.74 to $59.88 a day in a single occupancy assisted living apartment; $39.15 to $53.29 a day in double occupancy apartments; and $23.21 to $37.35 in residential care non-apartments. The regular rates range from $23.20 to $39.30 a day.
The rates do not include room and board, which are paid by the resident. The State limits the amount that can be charged for room and board to Medicaid waiver clients in assisted living facilities. The amount is equal to the SSI federal benefit rate minus a personal needs allowance of $85.00, which leaves $479 for room and board. There are no restrictions on the amount that private pay residents can be charged. The waiver includes a cap that limits CBA services to no more than 100 percent of the rate paid to nursing homes. Income supplementation is not allowed.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participants | Facilities | Participants | Facilities | Participants |
| 300 | 2,851 | 309 | 2,263 | 237 | 1,748 |
| Assisted Living Apartment |
Double Occupancy Apartment |
Residential Care Non-Apartment |
|
|---|---|---|---|
| AL 1 | $59.88 | $53.29 | $37.35 |
| AL 2 | $55.78 | $49.19 | $33.25 |
| AL 3 | $50.18 | $43.59 | $27.66 |
| AL 4 | $52.38 | $45.80 | $29.85 |
| AL 5 | $47.16 | $40.58 | $24.64 |
| AL 6 | $45.74 | $39.15 | $23.21 |
Staffing
Staff ratio requirements have been deleted. Facilities must develop staffing ratios based on the needs of residents. The normal staffing pattern must be disclosed to residents on admission. Night staff in small facilities must be immediately available. Larger facilities must have staff available and awake.
Training
The Department is required to develop a training program for inspectors that emphasizes the distinction between surveying assisted living facilities and nursing facilities.
Administrators. Managers of small facilities must have a high school diploma or equivalency. Managers of assisted living facilities with 17 or more beds must have an associate’s degree in nursing, health care management, or a related field; a bachelor’s degree; or at least one year of experience working in management or in the health care industry.
Managers or supervisors of facilities that advertise or market services to residents with Alzheimer’s disease must be at least 21; have an associate’s degree in nursing, health care management, or a related field; a bachelor’s degree in psychology, gerontology, nursing, or a related field; or have at least one year of experience working with people with Alzheimer’s disease.
Managers must have completed one course of at least 24 hours on management of facilities that includes: assisted living standards; resident characteristics; resident assessment and working with residents; basic principles of management; food and nutrition services; federal laws; community resources; ethics; and financial management. An additional eight hours of training are required within the first three months of employment.
All managers must have 12 hours of annual continuing education in at least two of the following areas: resident and provider rights and responsibilities; principles of management; skills for working with residents, families, and other professional providers; resident characteristics and needs; community resources; accounting and budgeting; basic emergency first aid; or federal laws.
Administrators in special care facilities must have a college degree (psychology, social work, counseling, gerontology, nursing, or a related field); an associate’s degree in nursing or health care management; or one year experience working with persons with dementia and complete six hours of continuing education in dementia care.
Staff must receive four hours of orientation covering reporting abuse and neglect, confidentiality, universal precautions, conditions that require notification to the manager, resident rights, and emergency and evacuation procedures. Attendants must complete 16 hours of on-the-job training and supervision on: providing assistance with ADLs; health conditions and how they affect the provision of tasks; safety measures to prevent injury and accidents; emergency first-aid procedures; and managing dysfunctional behavior.
Six hours of annual continuing education are required for direct care staff, chosen from the following topics: promoting resident dignity, independence, individuality, privacy, and choice; resident rights and self-determination; communication techniques with persons with vision, hearing, or cognitive impairments; communicating with families; common physical, psychological, social, and mental disorders that may increase with aging; essential facts about common physical and mental disorders; CPR; common medications and side effects; understanding mental illness; conflict resolution and de-escalation techniques; and information about community resources. One hour must cover behavior management such as prevention of aggressive behavior, fall prevention or alternatives to restraint.
Additional training topics are included for nurses, nurses aides, and medication aides. Staff in Alzheimer’s facilities must receive:
- Four hours of dementia specific orientation on basic information about the causes, progression, and management of dementia;
- 16 hours of on-the-job supervision with 16 hours of orientation providing assistance with ADLs, emergency and evacuation procedures, and managing dysfunctional behavior; and
- 12 hours of annual in-service training regarding Alzheimer’s disease covering assessing resident capabilities and developing and implementing service plans; promoting dignity, independence, and privacy; planning and facilitating activities; communicating with families; resident rights and principles of self-determination; care of persons with physical, cognitive, behavioral, and social disabilities; medical and social needs of residents; common psycho-tropic drugs and side effects; and local community resources.
Background Check
Facilities must provide written statements concerning their policy on criminal background checks and drug testing. Offenses which preclude employment are listed in statute (Section 250.006).
Monitoring
Unlicensed facilities may be subject to civil penalties between $1,000 and $10,000 for each violation. SB 1839 (2001) contained several provisions dealing with oversight and quality. Beginning in 2002, as part of their training, surveyors must observe the operations of facilities unrelated to survey activities for a minimum of ten days. Training that addresses at least one of the ten most common violations is provided to surveyors and providers twice a year. An early warning system is being developed to detect problems with quality that includes review of financial and quality of care indicators, quality of care monitors to inspect facilities, and the use of rapid response teams to assist facilities to improve compliance prior to a regular inspection or survey. An informal dispute resolution system is also being developed.
A Medical Quality Assurance section has been formed. Quality monitor staff visit facilities and monitor compliance. The quality monitor provides information to the facility on best practices to help the facility develop a plan to maintain compliance. At this time, the quality monitors are only performing these monitors in nursing facilities, but the program will expand to the assisted living facilities. The State created a nurse liaison position in each region of the State to provide information to facilities on training opportunities and best practice information to allow the facilities to make better compliance decisions. The liaisons are currently visiting all three types of facilities, as requested or as needed.
Fees
Fees are $100 plus $5 a bed for Type A and B facilities, with a maximum of $750, and $50 for Type C facilities. In addition, an annual fee of $100 must be paid for Alzheimer’s certification. Additional fees are required for review of plans based on size, number of stories, and new construction or remodeling. In addition, additional fees are assessed and placed in a trust fund for the use of court appointed trustees. The fees (§92.20) vary by type and size of facility.
Utah
Citation
Assisted living facilities, R432-270
General Approach and Recent Developments
The initial regulations were effective July 1995 and establish assisted living as a place of residence where elderly and disabled persons can receive 24-hour individualized personal and health related services to help maintain maximum independence, choice, dignity, privacy, and individuality in a home-like environment.
A report card on facilities was prepared and posted on the bureau of licensing’s web site based on survey findings from 2000-2002. A work group is developing recommendations related to the provision of hospice care and allowing facilities to also offer adult day care services.
The State's regulations were revised in March 2001. Revisions to the construction rules were effective in March 2002. The State recognizes accreditation by national organizations.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted living facilities I | 92 | 1,678 | 108 | 1,886 | 116 | 1,954 |
| Assisted living facilities II | 49 | 2,808 | 43 | 2,460 | 26 | 1,221 |
Definition
Assisted Living Type I is a residential facility that provides assistance with ADLs and social care to two or more ambulatory residents who are capable of achieving mobility sufficient to exit the facility without assistance of another person.
Assisted Living Type II is a residential facility with a home-like setting that provides an array of coordinated supportive personal and health care services, available 24 hours a day, to residents who have been assessed.
Type I and II facilities may be classified as: large facilities (17 or more residents; facilities comply with the I-2 Uniform Building Code); small facilities (six to sixteen residents; facilities comply with the R-4 code); and limited capacity facilities (up to five residents; facilities comply with the R-3 code).
Philosophy
The philosophy is contained in requirements for assessment and care planning. Services shall be individualized to maintain capabilities and facilitate using those abilities; create options to enable individuals to exercise control over their lives; provide supports which validate self-worth; maintain areas or spaces which provide privacy; recognize individual needs and preferences, and are flexible in service delivery; and allow residents to choose how they will balance risk and quality of life.
Unit Requirements
Type I facilities. Bedrooms must be at least 100 square feet for single units and 160 square feet for double units. Facilities providing only bedrooms must provide a toilet and lavatory for every six occupants and a bathtub or shower for every 10 residents.
Type II facilities. Living units include 120 square feet for single occupancy rooms and 299 square feet for double occupancy rooms, exclusive of toilet rooms, closets, lockers, wardrobes, alcoves, or vestibules. A single occupancy unit with additional living space must be 100 square feet and a double occupancy unit 160 square feet. Type II facilities must offer private living units, unless shared by choice. A maximum of two residents may share a unit. If private baths are not part of the unit, at least one toilet and lavatory is required for every four residents and a bathtub or shower for every ten residents.
Admission/Retention Policy
Type I facilities may serve residents who are ambulatory or mobile and are capable of taking life saving action in an emergency, have stable health, do not require assistance or require only limited assistance in ADLs, and require and receive regular or intermittent care or treatment in the facility from a licensed health professional (contract or through the facility). These facilities also may not serve anyone who requires significant assistance during sleeping hours or requires close supervision and a controlled environment.
Type II facilities are intended to enable residents to age-in-place. Residents may be independent or semi-independent but not dependent.
Facilities may not serve anyone who requires in-patient hospital care or long-term nursing care; anyone who is suicidal, assaultive, or a danger to self or others; or anyone with active tuberculosis or another communicable disease that cannot be adequately treated at the facility or on an out-patient basis or that may be transmitted to other residents through a normal course of activities.
Nursing Home Admission Policy
Must document two of the following:
- Due to diagnosed medical conditions, the applicant requires at least substantial physical assistance with ADLs above the level of verbal prompting, supervision, or setting up; or
- The attending physician has determined that the applicant’s level of dysfunction in orientation to person, place, or time requires nursing facility care; or equivalent care provided through an alternative Medicaid health care delivery program; or
- The medical condition and intensity of services indicate that the care needs of the applicant cannot be safely met in a less structured setting or without the services and support of an alternative Medicaid health care delivery program.
Services
Facilities must provide personal care, food service, housekeeping, laundry, maintenance, activity programs, medication administration, and assistance with self-administration and must arrange for necessary medical and dental care. A service plan must be developed within seven days of admission. Service plans must meet the unique cognitive, medical, physical, and social needs of residents.
Type II facilities provide substantial assistance with ADLs in response to medical conditions above the level of verbal prompting, supervision or coordination, nursing services, activities, and medication administration. Residents must have a service plan that includes specified intermittent nursing services, administration of medications, support services promoting residents’ independence, and self-sufficiency. Type II facilities must employ or contract with a registered nurse to provide or supervise a nursing assessment, general health monitoring, and routine nursing tasks including those that may be delegated. Facilities do not provide skilled nursing care but assist the resident in obtaining it. Skilled tasks are determined by the complexity or specialized nature of the services. They include those tasks that can be safely or effectively performed only by or under close supervision of licensed health care professionals, and care that is needed to prevent deterioration of a condition or to sustain current capacities of the resident.
Dietary
Facilities must be capable of providing three meals a day and snacks. Facilities admitting residents with therapeutic diets must have an approved dietary manual available. Dietary staff must have six hours of training a year.
Agreements
Agreements include: room-and-board charges and charges for basic and optional services; 30- day notice of change in charges; admission, retention, transfer, discharge, and eviction policies; conditions for termination of the agreement; the name of the responsible party; notice that the state agency has the authority to examine resident records; and refund policy.
Provisions for Serving People with Dementia
Training requirements include meeting the needs of residents with dementia. Clarification of the rules for secure units are being developed.
Medication Administration
Facilities are allowed to provide medication administration by licensed staff and assistance with self-medication by unlicensed staff (opening containers, reading instructions, checking dosage against the label, reassuring the resident that the correct dosage was taken, and reminding residents that a prescription needs to be refilled).
Public Financing
The State added long term care benefits to a managed care program operating in urban parts of the State through a 1915 (a) state plan amendment. Begun in April 2000, the managed care contractors provide long term care benefits to people who relocate from nursing homes to the community. The program is operating in five counties. Five more counties in Southern Utah will be covered in July 2004 and three more counties will be added later in 2004. In 2005, six more counties will be served bringing the total to 19 of the 29 counties.
The program currently serves about 400 people, and about 80% are residents of assisted living facilities. The HMO receives a capitation payment based on the per diem paid for nursing home care. Payments to facilities are negotiated. The flexibility of capitation allows the managed care plan to pay for room and board and services. Beneficiaries retain a $45 personal needs allowance and all other income is applied to the cost of services covered by the plan. Contractors are able to allow family members to supplement the room and board payment for a larger room but the contractors have not implemented supplementation.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participants | Facilities | Participants | Facilities | Participants |
| NA | 380 | NA | 400 | NA | NA |
Staffing
Direct care staff are required on-site 24 hours a day to meet resident needs as determined by assessments and service plans. Staff providing personal care in Type II facilities must be CNAs or complete a CNA training program within four months.
Training
Administrators. Requirements vary by the type and size of the facility. Type II facility administrators must complete a national certification program and meet one of the following criteria: experience, licensing, or college degree.
Staff. Orientation shall include job descriptions; ethics, confidentiality, and resident rights; fire and disaster plan; policy and procedures; and reporting responsibility for abuse, neglect, and exploitation. In-service shall be tailored to include all of the following subjects that are relevant to the person’s job:
- Principles of good nutrition, menu planning, food preparation, and storage;
- Principles of good housekeeping and sanitation;
- Principles of providing personal care and social care;
- Proper procedures in assisting residents with medications;
- Recognizing early signs of illness and determining when there is a need for professional help;
- Accident prevention, including safe bath and shower water temperatures;
- Communication skills which enhance resident dignity;
- First aid;
- Residents’ rights and reporting requirements; and
- Needs of dementia/Alzheimer’s residents.
Background Check
Administrators must be of good moral character with no felony convictions. All direct care staff are screened through background checks which include the Adult Protective Services register. FBI checks are required if a person has not resided in Utah for five years.
Monitoring
Licenses are now issued for a two year period. Facilities are surveyed annually.
Fees
There is a $100 base fee plus $9 per bed. Additional fees are charged for plan based on size.
Vermont
Citation
Residential care homes (Level III, IV), Regulations effective 10/3/00
Assisted living residences, Regulations effective 03/15/03
General Approach and Recent Developments
Regulations for a new category of assisted living residences went into effect in March 2003. Developers of assisted living residences are continually challenged to build residences on a scale that reflect consumer preferences. The State is encouraging the development of small scale residences with mixed acuity.
Residential care home rules were revised in 2000. Assistive Community Care Services, a Medicaid state plan service, and Medicaid waiver reimbursement are available to Level III facilities and assisted living residences. The Medicaid waiver was amended to cover assisted living residences. The State has a grant from the Coming Home Program to expand affordable assisted living in rural areas.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Residential care facilities (Level III) | 95 | 2,150 | 109 | 2,213 | 114 | 2,351 |
| Residential care facilities (Level IV) | 15 | 152 | ||||
| Assisted living residences | 3 | 108 | NA | NA | NA | NA |
Definition
Assisted living residence means a program or facility that combines housing, health, and supportive services to support resident independence and aging-in-place. At a minimum, assisted living residences shall offer, within a homelike setting, a private bedroom, private bath, living space, kitchen capacity, and a lockable door. Assisted living shall promote resident self-direction and active participation in decision-making while emphasizing individuality, privacy, and dignity.
Assisted living residences must meet the applicable licensing requirements of the residential care home licensing regulations for a Level III home, and all assisted living residence units must further meet the definition for assisted living residences as described above.
Variances from regulations may be granted by the licensing agency using the same criteria and procedures set forth in the residential care home licensing regulations.
Residential care home is a place, however named, excluding a licensed foster home, which provides for profit or otherwise, room, board, and personal care to three or more residents unrelated to the licensee. Level III means a residential care home licensed to provide room, board, personal care, general supervision, medication management, and nursing overview. Level IV homes do not provide nursing overview.
Unit Requirements
Assisted living residences. Residential living space must be a minimum of 225 square feet per unit, excluding bathroom and closets. Each unit must provide accessible or adaptable sleeping, living, and eating areas, and be built in conformance with the Americans with Disabilities Act Accessibility Guidelines or the equivalent state building code specifications. Units must include a private bathroom, bedroom, living space, and kitchenette, adequate storage, lockable door, individual temperature controls and be equipped with emergency response systems to alert on-duty staff. Units may be shared only by choice. Kitchenettes must include food preparation and storage area, refrigerator with freezer, cabinets, counter space, sink and source of hot and cold running water, a stove or microwave that can be removed or disconnected, and outlets.
Pre-existing structures being converted or remodeled from another use must have a minimum of 160 square feet not including the bathroom or storage space. Kitchen capacity is not required, but a community kitchen must be available.
Residential care homes. The regulations indicate that every effort must be made to provide a home-like environment. Each private bedroom must have at least 100 square feet of usable floor space and multi-bed rooms must have 80 square feet per bed. After October 1993, all new homes may offer only single or double occupancy rooms. One bath, toilet, and sink is required for every eight residents.
Admission/Retention Policy
Assisted living residences. Residents must be age 18 and over, and may be admitted except in the following conditions:
- A serious acute illness requiring medical, surgical or nursing care provided by a general or special hospital;
- Ventilators;
- Respirators;
- Care of Stage III or IV ulcers;
- Nasopharyngeal, oral or tracheal suctioning; or
- Two-person assistance to transfer from bed or chair or to ambulate.
Current residents who develop a serious, acute illness may be retained as long as their care needs are met by appropriate licensed personnel. Facilities must provide personal care and nursing services to meet a resident’s needs if he or she has a late loss ADL score of 10, provided that the resident’s needs can be met by one staff person at a time; any cognitive impairment that is moderate or lesser degree of severity; and any behavioral symptoms consistently responding to appropriate intervention.
Residents who have an identified acute or chronic medical problem or who are deemed to need nursing overview or supervision shall be under the continuing general supervision of a physician of their choosing.
Residents may only be involuntarily discharged if they pose a serious threat to self or other residents that cannot be resolved through care planning and are not capable of entering into a negotiated risk agreement; are ordered by a court to move; or fail to pay rent, service, or care charges; the resident refuses to abide by the terms of the admission agreement; or the resident has care needs above the mandatory scope of aging in place and the assisted living residence can no longer meet the resident’s level of care needs or has a policy to discharge residents with such needs.
Residential care homes. Residential care homes may retain people who need nursing services beyond nursing overview and medication management if the following conditions are met:
- The services are received less than three times a week, or are provided seven days a week for no more than 60 days and the resident's condition is improving;
- The home has an RN on staff or a contract with a home health agency;
- The home is able to meet the resident's needs without detracting from services to other residents;
- There is a written agreement concerning which nursing services the home provides or arranges and which is explained to the resident before admission or at the time of admission; the agreement includes how services are paid for and the circumstances under which a resident will be required to move; and
- Residents are fully informed of their options and agree to such care in the residential home.
Residents requiring intravenous therapy, ventilators or respirators, daily catheter irrigation, feeding tubes, care of Stage III or IV decubitus; suctioning, or sterile dressings may only be served under a variance from the Department. Variances are considered and issued on a case by case basis. A series of requirements are described for facilities providing nursing overview, administration of medications, and nursing care.
Nursing Home Admission Policy
Eligible beneficiaries must require daily service due to impairments in ADLs or need for rehabilitation, or have one or more specific conditions and treatments, or require 24-hour care due to psycho-social factors. Eligibility is met if the person has qualifying needs in any of the three categories of service. ADL qualifying needs include the daily need for moderate or total assistance with bathing, dressing, eating, ambulation, transferring, and bowel and bladder functions (or with a combination of these needs so that daily help at the moderate or total assistance level is needed). Qualifying conditions and treatments include assistance with intravenous fluids/medications, injections, pain management, pressure sores, airway suctioning, tube feedings, ventilator or respirator care, or skilled wound care. Psycho-social factors cover persons with impaired judgment and/or confusion requiring constant or frequent direction with ADLs or behavioral symptoms such as wandering, aggression, and /or inappropriate behavior requiring a controlled environment.
Services
Assisted living residences provide services required for Level III residential homes plus:
- a program of activities and socialization opportunities, including periodic access to community resources;
- social services which include information, referral, and coordination with other community programs and resources; and,
- a negotiated risk process.
A resident care plan must be developed and maintained, describing the assessed needs and choices of the resident, and shall support the resident’s dignity, privacy, choice, individuality, and independence. The plan shall be reviewed at least annually, or upon a significant change in condition. “Negotiated risk” means a formal, mutually-agreed upon, written understanding that results after balancing a resident’s choices and capabilities with the possibility that those choices will place the resident at risk of harm. Negotiated risk does not constitute a waiver of liability.
Residential care homes provide personal care, medication management, laundry, meals, toiletries, transportation, and, in Level III homes, nursing overview. Nursing overview means a process in which a nurse assures that the health and psycho-social needs of the resident are met. The process includes: observation, assessment, goal setting, education of staff, and the development, implementation, and evaluation of a written individualized treatment plan to maintain the resident's well being.
Intravenous therapy; ventilators or respirators, daily catheter irrigation, feeding tubes, care of Stage III or IV decubitus ulcers, suctioning, and sterile dressings may not be provided to any resident unless a variance is approved by the state licensing agency.
Dietary
Residential care homes. Three well balanced, attractive, and satisfying meals and supplemental nourishment are required. The rules specify the total daily requirements for meals (required daily servings and average size). Written physicians’ orders are needed for therapeutic diets. Draft rules propose that meals served each day must provide 100 percent of the recommended daily allowances as established by the Food and Nutrition Board.
Assisted living residence. Same as above.
Agreements
Assisted living residences must disclose policies, services, and rates on a standard disclosure and in resident agreements. The Uniform Consumer Disclosure describes the services provided, services that are not provided, public programs or benefits it accepts, policies that enhance or limit aging in place, and any physical plant features that enhance or limit aging in place. It also includes service packages, tiers and rates, and a statement that rates may change due to increased needs with an explanation of the situations that would lead to an increase.
A licensee who has specialized programs such as dementia care shall include a written statement of philosophy and mission and a description of how the assisted living residence can meet the specialized needs of residents. This must be included in the admission agreement and in the Uniform Consumer Disclosure.
Negotiated risk is a formal, mutually agreed upon, written understanding that results after balancing a resident’s choices and capabilities with the possibility that those choices will place the resident at risk of harm. Negotiated risk does not constitute a waiver of liability. The Enhanced Residential Care Home Medicaid waiver for Level III and assisted living providers includes standards covering negotiated risk which is defined as “allowing residents choices in accepting certain risks. These choices are negotiated between the resident, case manager, provider, and family members with the intent of fostering independence, safety, and self-determination.”
The resident agreement differs from other states with respect to service options and rates. Vermont’s approach was informed by thinking of the resident unit as housing and considering the service option requirements of the Low Income Housing Tax Credit program. While purchase of services is optional, residences may set admission priorities based on applicants’ need and intent to purchase services. Residents have the right to arrange for third-party services not available through the residence from a provider of their choice.
Charges for occupancy of the unit and utilities may vary by size of the unit and any amenities, or any published sliding fee scale or system of housing subsidies administered by the licensee. These housing charges may not vary based on the level of care that a resident needs. Providers may offer separate rental and service agreements. While providers have the option of offering less than full meal and snack plans, they must have the capacity to deliver a full plan to any resident who wishes to purchase it.
To promote aging in place at predictable costs, personal care services must be charged as a bundled daily, weekly, or monthly fee that may vary by service tiers. The bundled approach to services and fees draws on the framework that existed in Vermont residential care homes and public reimbursement programs prior to assisted living regulations. Differences among tiers must be clearly defined and measurable. Three tiers of service are required. The first tier is known as the Basic tier and it meets the needs of residents who have personal care needs below Vermont’s nursing home level of care guidelines. (The Basic tier also corresponds to the level of care that Level III residential care homes provide without a variance from the State.) Assisted living providers are required to define two tiers or bundles above the Basic tier that are within the mandatory scope of aging in place. Providers must define additional tiers or bundles beyond the three required if they have a policy of retaining residents above the mandatory scope of aging in place.
If providers use the lower two tiers of the Enhanced Residential Care Medicaid Waiver Program to define Tiers 2 and 3 required by the assisted living regulations, the tiers might be defined as follows:
- Tier 2--serving people with ADL scores of 6 to 18, who have no cognitive impairment or a mild cognitive impairment;
- Tier 3--serving people with a total ADL score over 18; a late loss ADL score of no more than 10 (late loss ADLs include eating, toileting, transferring, locomotion and bed mobility); a cognitive impairment, if any; no greater than moderate, behavioral needs, if any, that readily respond to intervention no more than 1.25 hours per week.
Retention policy and services available above the mandatory scope of care must be disclosed.
Providers have the option of offering an independent tier or bundle for residents who do not need personal care services. Vermont anticipates that this independent tier will be most commonly used by second occupants, such as spouses who do not require personal care but elect to use meals, activities, laundry, transportation, etc.
A residence may charge on a per service basis only for those services that are not required by regulations, such as additional transportation and housekeeping services, hair dressing, or outings that are not part of the program of activities and socialization available to all residents.
Residential care homes. Agreements are required prior to or at the time of admission that include: the daily, weekly, or monthly rate charged; the services covered in the rate; all other applicable financing issues including discharge or transfer when the resident’s status changes from private pay to SSI or assisted community care services (ACCS); and how services will be provided. The agreement also covers transfer and discharge rights, the amount and purposes of any deposits, and refund policy. On admission the facility must determine if the resident has any form of advance directive and explain his or her right to formulate or not formulate a directive.
Resident agreements for Level III and assisted living providers who participate in the ACCS program must disclose the provider’s policy about accepting SSI or ACCS payments. Decisions to accept SSI or ACCS payments may be made on a case-by-case basis. Additional items are included in the agreements with ACCS participants: ACCS services, room and board rate, personal needs allowance amount, and the provider’s agreement to accept room and board and Medicaid as the sole payment.
Provisions for Serving People with Dementia
Residential care homes and assisted living residences. Special care units must be approved by the Department based on the following: statement of philosophy, definition of the categories of residents with dementia to be served, a description of the organizational structure, a description of the physical environment, criteria for admission, continued stay and discharge, unit staffing including qualifications, orientation, in-service education and specialized training, and medical management and credentialing.
Assisted living residences. Training in dementia care is required for all staff.
Medication Administration
Residential care homes and assisted living residences provide assistance with self-administration of medications and administer medications under the supervision of and the delegation by registered nurses. Each residence must have a policy on the procedures for delegation of administration, how medications will be obtained including choice of pharmacies, and documentation procedures. Trained staff must be designated to assist with or administer medications.
Public Financing
Residential care homes and assisted living residences are enrolled in one of three SSI living arrangements that apply:
| Living Arrangement | G | F | C |
|---|---|---|---|
| Licenses | Level IV RCH (all) (Do not provide nursing overview--ineligible to become Medicaid providers) |
Level III RCH & ALR that do not accept Medicaid/SSI (Private pay facilities) |
Level III RCH & ALR that do accept Medicaid/SSI (From at least some residents) |
Medicaid reimburses through two separate programs: the Assistive Community Care Services (ACCS) program and the Enhanced Residential Care Home Waiver program (ERC). Level III RCHs and ALRs that enroll as Medicaid ACCS providers deliver a bundle of services including nursing overview, personal care, health, rehabilitative and supportive services for a standard per diem rate. The rate was increased to $30.25 a day July 1, 2004.
Eligible providers who apply for and are enrolled in the ERC Medicaid waiver program include Level III RCHs and ALRs. With respect to Level III RCHs, preference is given to providers that offer single occupancy units.
This waiver covers nursing overview (assessment, oversight, monitoring, and routine tasks), personal care services, case management, medication assistance, recreational and social activities, support for individuals with cognitive impairments, and 24-hour, on-site supervision. Services must be provided in non-institutional, home-like settings.
Currently, the waiver is budgeted to serve up to 160 participants. In addition, local Medicaid waiver teams may direct up to 10 percent of a sister program’s (Home Based Medicaid Waiver) slots to residents who choose to live in enhanced residential care and assisted living residences Participants must meet the nursing home eligibility criteria and be financially eligible for Medicaid under long-term care rules, and are awarded a slot in the program based on priority need.
For ERC reimbursement, the Department of Aging and Disabilities has designed a three-tiered system that was developed using the ERC assessment tool, review of other state reimbursement systems, and assessment data. Residents receive scores in five areas: ADLs, bladder and bowel control, cognitive and behavior status, medication administration, and special programs (behavior management, skin treatment, or rehabilitation/restorative care). Residents are assigned to a level (1 or 2) based on the extent of ADL impairments. Scores of 6 to 18 are assigned to Level 1 and scores between 19 and 29 are assigned to Level 2. The four remaining areas are rated and additional points are assigned. The payment tier is determined by combining the ADL level and the additional points. The rates are: Tier I ($42.00 a day); Tier II ($48.50 a day); and Tier III ($55.00 a day). In addition to the ERC reimbursement, providers receive an Assistive Community Care Services (ACCS) daily rate of $30.25 a day. Room and board is limited to an amount that corresponds to the Federal SSI benefit (currently $564 per month). The state supplement for personal needs is $47.76.
| Program | 2004 | 2002 | ||
|---|---|---|---|---|
| Facilities | Participants | Facilities | Participants | |
| ERC waiver | 43 | 157 | 39 | 152 |
| ACCS | 85 | 487 | 73 | 468 |
| No Personal Care Needs (Independent) |
Needs Below Nursing Home Guideline (Basic) |
ERC Tier I (Often used as second ALR mandatory tier) |
ERC Tier II (Often used as 3rd ALR mandatory tier) |
ERC Tier III (Optional Service level for ALRs) |
|
|---|---|---|---|---|---|
| ACCS Medicaid State Plan | $0.00 | $30.25 | $30.25 | $30.25 | $30.25 |
| ERC Medicaid Waiver | $0.00 | $0.00 | $42.00 | $48.50 | $55.00 |
| Total | $0.00 | $30.25 | $72.25 | $78.75 | $85.25 |
Staffing
Residential care homes and assisted living residences are required to employ a manager or administrator who works in the facility an average of 32 hours per week (including any time worked providing care or services, and including vacation and sick time).
Assisted living residences must employ sufficient staff to meet the needs of each resident. At least one personal care assistant must be on duty at all times. A registered nurse shall be employed to oversee implementation of service plans, conduct nursing assessments, and provide health services. The RN shall be on-site to the degree necessary to achieve the outcomes as specified in the individual service plans.
Residential care homes must have a sufficient number of qualified staff to meet resident needs.
Training
Residential care home administrators. Managers must complete a state approved certification course.
Assisted living residence administrators. The director must be at least 21 years old and have demonstrated experience in gerontology and supervisory and management skills. Directors shall have evidence of 15 hours of training per year regarding assisted living and its principles and the care of elderly and disabled individuals.
Residential care home staff. Staff must receive 20 hours of training each year that includes at least procedures in case of fire; resident rights; and mandatory reporting of abuse, neglect, and exploitation. Training in direct care skills may be provided by a nurse.
Assisted living residence staff. All staff must be trained in the philosophy and principles of assisted living. Staff serving residents with dementia must have training in communication skills specific to dementia.
Background Check
A criminal records and adult abuse registry check is required for directors and all staff. Staff with substantiated charges of abuse, neglect, or exploitation, or those convicted of an offense relating to bodily injury, theft, or misuse of funds or property or other crimes inimical to the public welfare may not be employed or retained.
Monitoring
Residential care homes and assisted living residences. The State works with RCHs and ALRs to help them comply with the regulations. The State conducts surveys at the time of application/license issuance and at least annually thereafter. The State will investigate complaints which merit investigation. The State issues notices of violation (of law or regulation), requires corrective action plans to be submitted and completed. Sanctions may be levied. In necessary situations, the State will take “immediate enforcement action to eliminate a condition which can reasonably be expected to cause death or serious physical or mental harm to residents or staff.” Enforcement actions may also include administrative (money) penalties, action against a license (suspension, revocation, modification or refusal to renew), suspension of admissions, and transfer of residents.
Monitoring is conducted by the licensing agency and the ombudsman program.
Assisted living residences. Facilities must have a quality improvement process that includes an internal committee of the director, an RN, a staff member, and a resident. The committee must meet at least quarterly. Resident satisfaction surveys must be conducted annually and be used by the committee.
Fees
Residential care homes and assisted living residences. No fee to apply for licensure.
Summary of ERC Program Tiers and Scoring System
Note: The ERC Program Tiers 1 and 2 would correspond to the second and third bundles/tiers required by the assisted living regulations to the extent they fall within the mandatory scope of care. Tier 3 of the ERC program would be included one or more tiers above the mandatory scope of care.
Points are assigned based on findings from a standardized assessment.
| Area | Maximum Points |
Factors |
|---|---|---|
| ADLs | 29 | Eating, toileting, mobility, bathing, dressing |
| Continence | 13 | Bladder and bowel |
| Cognitive/behavior status | 65 | Sleep pattern, wandering, danger to self/others |
| Medication Administration | 5 | Administration |
| Special programs | 49 | Mood, behavior, cognitive loss. Skin: Turning/repositioning, nutrition or hydration, dressings, ulcer care, surgical wound care. Rehab: range of motion, skin brace assistance, transfer, walking, dressing/grooming, eating/ swallowing, prosthesis care, communication. |
| ADL Level 1 | ADL Level 2 | ||
|---|---|---|---|
| ERC Tier | Points | ERC Tier | Points |
| 1 | 0-30 | 1 | 0-35 |
| 2 | 31-59 | 2 | 36+ |
| 3 | 60+ | ||
Virginia
Citation
Assisted living facilities 22 VAC 40-71-10 et seq.
General Approach and Recent Developments
Revisions to the regulations were effective March 28, 2003. The Department of Social Services anticipates that further refinements will be made. The rules describe two levels of care: assisted living care and residential living care. The State provides an “auxiliary grant” under a state SSI supplement and a state funded payment for “regular” assisted living services.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted Living Facilities | 636 | 34,598 | 669 | 34,206 | 663 | 32,768 |
Definition
Assisted living facility means any congregate residential setting that provides or coordinates personal and health care services, 24-hour supervision, and assistance (scheduled and unscheduled) for the maintenance or care of four or more adults who are aged, infirm, or disabled and who are cared for in a primarily residential setting, except a facility or portion of a facility licensed by the State Board of Health or the Department of Mental Health, Mental Retardation and Substance Abuse Services (and other exceptions including HUD housing building).
Assisted living care means a level of service provided by an assisted living facility for adults who may have physical or mental impairments and require at least moderate assistance with activities of daily living. Moderate assistance mean dependent in two or more ADLs. Included in this level of services are individuals who are dependent in behavior pattern as documented on the uniform assessment instrument.
Residential living care means a level of service provided by an assisted living facility for adults who may have physical or mental impairments and require only minimal assistance with activities of daily living. Minimal assistance means dependency in only one ADL or one or more IADLs or medication administration.
Unit Requirements
Assisted living facilities (ALFs) may offer single rooms (minimum 100 square feet for newer buildings) or multiple occupancy rooms (80 square feet per occupant). A maximum of four people may occupy a room. Facilities must provide one toilet and wash basin for every seven people and one bath tub or shower for every ten people.
Admission/Retention Policy
Assisted living facilities cannot admit or retain residents with the following conditions or needs:
- Ventilator dependent;
- Dermal ulcers (III or IV) unless a Stage III ulcer is healing;
- *Intravenous therapy or injections directly into the vein except for intermittent care under specified conditions;
- Airborne infectious disease in a communicable state;
- Psychotropic medications without an appropriate diagnosis and treatment plan;
- Nasogastric tubes;
- *Gastric tubes except when an individual is capable of independently feeding himself and caring for the tube or by exception;
- Individuals who present a danger to themselves or others;
- Individuals requiring continuous nursing care (around the clock observation, assessment, monitoring, supervision, or provision of medical treatment by a licensed nurse);
- Individuals whose physician certifies that placement is no longer appropriate;
- Unless the individual's physician determines otherwise, individuals who require maximum physical assistance as documented by an assessment and meet Medicaid nursing facility level of care criteria; or
- Individuals whose health care needs cannot be met in the specific ALF as determined by the facility.
* Exceptions are allowed when requested by a resident and care is provided by a physician, a licensed nurse, or a licensed home care organization (except for Auxiliary Grant residents).
Public pay residents must have an assessment completed by a case manager or other qualified assessor. Assessments for private pay residents may be completed by a case manager or other qualified assessor, an independent physician, or an employee of the facility who has documented training in the completion of the uniform assessment instrument. Assessments completed by facility staff must be signed by the administrator or designated representative.
Nursing Home Admission Policy
Residents must meet functional and medical criteria. Functional criteria include:
- Dependent in two to four ADLs and semi-dependent or dependent in behavior pattern and orientation, and semi-dependent in joint motion or dependent in medication administration; or
- Dependent in five to seven ADLs and dependent in mobility; or
- Semi-dependent in two to seven ADLs and dependent in mobility and behavior pattern and orientation.
Medical or nursing supervision means:
- A condition that requires observation and assessment; or
- Potential for instability is high or exists; or
- Ongoing nursing services are required.
Services
The regulations offer ALFs the flexibility to develop a program that meets the following criteria:
- Meet physical, mental, emotional, and psycho-social needs,
- Provide protection, guidance, and supervision;
- Promote a sense of security and self worth; and
- Meet the objectives of the service plan.
Individualized services plans are developed to support the principles of individuality, personal dignity, freedom of choice, and home-like environment and shall include other formal and informal supports that may participate in the delivery of services. Service plans are designed to maximize the resident’s level of functional ability.
Each facility develops a written program description for prospective residents that describes the population to be served and the program components and services available. Facilities are permitted but are not required to offer all services as long as they have services that are appropriate for the needs of residents. Adult care facilities must also provide 24-hour capacity to meet scheduled and unscheduled service needs. Skilled nursing services, except continuous skilled nursing, may be provided by a facility nurse or a contracted nurse of a licensed home care organization. Eleven hours of activities per week for residential living care and 14 hours for assisted living care must be scheduled.
An assessment using the approved Uniform Assessment Instrument must be performed on all residents prior to admission, every 12 months, and whenever a change in the resident's condition warrants a level of care change. An individualized service plan or plan of care is developed from the assessment in conjunction with the resident, family, case worker, case manager, and health care providers. The service plan shall reflect the philosophy and values described above.
Dietary
A minimum of three well-balanced meals and snacks must be served that meet the USDA Food Guide Pyramid guidelines. Special diets must be provided when ordered by a physician.
Agreements
Agreements include: specific charges for accommodations, services, and care; the frequency of payment and rules relating to non-payment; description of all accommodations, services, and care offered and their related charges; amount and purpose of advance payments and refund policy; policy for increasing charges and the amount of notification; and a stipulation of the transfer of ownership of any property, real estate, or money to the facility. Facilities must provide upon admission and upon request a description of the types of staff, services provided, and the hours services are available.
Provisions for Serving People with Dementia
Special care units. At least two direct care staff must be awake and on duty at all times if residents with dementia are served unless there are no more than five residents on the unit and there are at least two other direct care staff in the building. The annual training requirement for direct care staff has been increased from 12 to 16 hours for the first year of employment. Within six months, direct care staff must complete four hours of training that includes an explanation of cognitive impairments, behavior management, communications skills, and safety considerations. Within the first year of employment, six more hours of training are required on topics that include assessment, care techniques, therapeutic environment and activity planning. Curriculum for staff must be developed by a qualified health care professional or a person approved by the Department.
Exit doors must be monitored or secured unless they lead to protected areas. Staff-supervised or secure outdoor areas must be available. The rules require an initial assessment by a physician or clinical psychologist, agreement to the placement by the resident, a guardian, relative, or physician and periodic reviews. Scheduled activities are required that include stimulation, physical, productive/work, social, and outdoor activities.
The standards differ for facilities that serve a mixed population.
Medication Administration
Residents may self-administer medications if they are capable of doing so, although assistance with self-administration is not described in the regulations. Medication Administration is permitted when licensed staff are available or a medication training program approved by the Board of Nursing has been completed.
Public Financing
The State provides an “auxiliary grant,” or an SSI state supplement, and pays for additional services using state funds. The auxiliary grant program is a state and locally funded assistance program to supplement the income of recipients of the federal Supplemental Security Income (SSI) program and certain other aged, blind, and disabled individuals residing in an assisted living facility. In 2004, the maximum auxiliary grant payment is $866 or $996 a month depending upon the area of the State. The personal needs allowance is $62 a month. The auxiliary grant rate covers room, board, basic supportive services, and supervision.
Within assisted living, there are two payment levels for recipients of an Auxiliary Grant: regular assisted living and intensive assisted living as defined by the Department of Medical Assistance Services (DMAS). Intensive assisted living services are for individuals who meet the criteria for home and community based waiver services (at risk of nursing home placement). Because the waiver was not renewed, no new individuals will receive this service. In 2003, the State provided auxiliary grants payments to 6,572 residents a month in 373 facilities.
The State supplements the Auxiliary Grant for the provision of additional personal care services in assisted living residences: a state funded payment of $3 a day for regular assisted living care services for people with two ADLs, and $6 per day for residents needing “intensive assisted living services” who formerly participated in the waiver program. The regular assisted living program served 1,592 beneficiaries compared to 1,952 beneficiaries in 2002. The intensive services program (formerly the waiver program) serves 240, down from 526 beneficiaries in 2002.
Staffing
Assisted living facilities shall have staff adequate in knowledge, skills, and abilities and sufficient in numbers to provide services to attain and maintain the physical, mental, and psycho-social well-being of each resident as determined by resident assessments and individualized service plans, and to assure compliance with regulations for assisted living facilities. At least one staff member must be awake and on duty at all times in each building except in buildings with less than 20 residents if licensed for the assisted living level of care. At least quarterly, a licensed health professional must be on-site to monitor direct care staff performance of health related activities, including the identification of any significant gaps in the staff person's ability to function competently; advise the administrator of the need for staff training; provide consultation and technical assistance to staff; directly observe every resident whose care needs are equivalent to the intensive assisted living criteria; and recommend in writing any needed changes in the care provided or in the resident's service plan.
Training
An administrator must be 21, a high school graduate with one year of post-secondary education or administrative or supervisory experience, and must, within each 12-month period, attend at least 20 hours of training related either to client specific needs or to the management and operation of a residential facility for adults. When adults with mental impairments reside in the facility, at least five of the required 20 hours of training shall focus on the resident who is mentally impaired.
Administrators of facilities providing assisted living care must have at least two years of post-secondary education or one year of courses in human services or group care administration from an accredited college or a department curriculum specific to the administration of an adult care facility.
Staff. All employees shall be made aware of: the purpose of the facility, the services provided, the daily routines, and required compliance with regulations for assisted living facilities as it is related to their duties and responsibilities.
All personnel shall be sufficiently trained in the relevant laws, regulations, and facility’s policies and procedures to implement the following:
- Emergency and disaster plans for the facility;
- Techniques of complying with emergency and disaster plans including evacuating residents where applicable;
- Use of first-aid kit and knowledge of its location;
- Observance of rights and responsibilities of residents;
- Procedures for detecting and reporting suspected abuse, neglect, or exploitation of residents;
- Techniques for assisting residents to overcome transfer trauma;
- Confidential treatment of personal information; and
- Specific duties and requirements of their positions.
Orientation must be completed within one week. All direct care staff shall have been trained to have general knowledge in the care of aged, infirm, or disabled adults with due consideration for their individual capabilities and their needs and capacities within 30 days. On an annual basis, all direct care staff shall attend at least eight hours of training. The training shall be relevant to the population in care and shall be provided through in-service training programs or institutes, workshops, classes, or conferences. When adults with mental impairments reside in the facility, at least two of the eight required hours of training shall focus on the resident who is mentally impaired. Documentation of this training shall be kept by the facility in a manner that allows for identification by individual employee.
Staff in assisted living facilities must also be trained to deal with residents who have a history of aggressive behavior or of dangerously agitated states. This training must cover information, demonstration, and practical experience in self-protection and prevention and de-escalation of aggressive behavior. Training to serve residents who are restrained is also required and covers proper techniques for applying and monitoring restraints, skin care, and active assisted range of motion exercises, assessment of blood circulation, turning and positioning, provision of sufficient bed clothing and covering to maintain body temperature, and provision of additional attention to meet the physical, mental, emotional, and social needs of restrained residents.
Assisted living care staff must attend at least 12 hours of training annually which focuses on the needs of residents who are mentally or physically impaired as appropriate to the populations served.
Background Check
The statute (§63.2-17.20) does not allow persons convicted of specific types of crimes to be employed. Staff must submit a sworn statement disclosing criminal convictions or pending charges. False statements are a Class 1 misdemeanor. An original criminal records check must be obtained by the facility from the Central Criminal Records Exchange.
Monitoring
Public pay residents receive annual reassessments by assigned case managers. Residents who require coordination of multiple services, are not able and do not have support available to assist in coordinating activities, and need a level of coordination that is beyond what the assisted living care residence is able to provide, receive Medicaid funded, targeted case management from a case manager.
Private pay residents also receive annual reassessment to assure continued appropriate placement and services.
The Department of Social Services conducts regular licensing inspections of assisted living facilities. The Department of Medical Assistance Services conducts on-site visits to monitor the quality and appropriateness of assisted living services provided to public pay residents of these facilities.
Fees
- Facilities of 1 to 12 beds ($14 per facility);
- 13 to 25 beds ($35 per facility);
- 26 to 50 beds ($70 per facility);
- 51 to 75 beds ($105 per facility);
- 76 to 200 beds ($140 per facility);
- More than 200 beds ($200 per facility).
Fees are doubled for licenses that are issued for two years.
Revised regulations for assisted living/community residential care facilities were adopted in July 2001.
Washington
Citation
Boarding homes, Chapter 388-78A
Assisted living (Medicaid), Chapter 388-110 WAC
General Approach and Recent Developments
Revisions to the licensing regulations and Medicaid contracting requirements will be effective September 2004 following public hearings in July. The revisions clarify that boarding homes will be allowed, but not required to, provide assistance with ADLs, and intermittent health support. However, facilities that do provide assistance with ADLs will address all ADLs defined by rule and will not be allowed to select among ADLs. Provisions formerly included in the Medicaid contracting requirements, e.g., negotiated service plans, have been included in the general licensing rules.
Separate requirements are used for boarding homes contracting with the Medicaid program as assisted living providers. The State has a grant from the Coming Home Program to expand affordable assisted living in rural areas. Medicaid regulations were issued in 1996 for licensed boarding homes that contract with Medicaid for residential care services that cover assisted living, enhanced adult residential care, and adult residential care. Enhanced residential care facilities provide limited nursing services and personal care while adult residential care facilities provide only personal care.
The Medicaid contracting standards require that contractors ensure that both the physical environment and the delivery of assisted living services are designed to enhance autonomy in ways which reflect personal and social values of dignity, privacy, independence, individuality, choice and decision-making of residents. The contractor shall provide the resident services in a manner which: makes the services available in a homelike environment for residents with a range of needs and preferences; facilitates aging in place by providing flexible services in an environment that accommodates and supports the resident's individuality; supports managed risk which includes the resident's right to take responsibility for the risks associated with decision-making; and develops a formal written, negotiated plan to decrease the probability of a poor outcome when a resident's decision or preference places the resident or others at risk, leads to adverse consequences, or conflicts with other residents' rights or preferences.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Boarding homes | 538 | 24,498 | 525 | 23,830 | 498 | 22,140 |
| NOTE: The summary below is based on proposed licensing regulations and contracting requirements for dementia facilities. | ||||||
Definition
Boarding home means any home or other institution, however named, which is advertised, announced, or maintained for the express or implied purpose of providing housing, basic services, and assuming general responsibility for the safety and well-being of the residents, and may also provide domiciliary care, consistent with this chapter, to seven or more residents after July 1, 2000. However, a boarding home that is licensed for three to six residents prior to or on July 1, 2000, may maintain its boarding home license as long as it is continually licensed as a boarding home. “Boarding home” does not include facilities certified as group training homes…nor any home, institution or section thereof which is otherwise licensed and regulated under the provisions of state law providing specifically for the licensing and regulation of such home, institution or section thereof. Nor shall it include any independent senior housing, independent living units in continuing care retirement communities, or other similar living situations including those subsidized by the Department of Housing and Urban Development.
Medicaid. Medicaid covers services in three types of boarding homes: assisted living, adult residential care and enhanced adult residential care. “Assisted living services is a package of services, including personal care, intermittent nursing services and medication administration services, that the department contracts with a licensed boarding home to provide in accordance with Parts I and II of this chapter.” Homes that contract to provide assisted living services must offer private apartment-like units.
“Adult residential care is a package of services, including personal care services, that the department contracts with a licensed boarding home to provide in accordance with Parts I and IV of this chapter.”
“Enhanced adult residential care is a package of services, including personal care services, intermittent nursing services, and medication administration services that the department contracts with a licensed boarding home to provide in accordance with Parts I and III of this chapter.”
Unit Requirements
Boarding home. Rooms must offer 80 square feet for single occupancy and 70 square feet per person in multiple occupancy rooms. One toilet and sink is required for every eight residents, and one bathing fixture is required for every twelve residents. Two residents may share a sleeping room that has less than 140 square feet if they have an apartment with a total square footage of 220 square feet, excluding the bathroom, and they agree to share the sleeping room.
Medicaid. To contract with Medicaid under the Assisted Living contract, facilities must provide individual units with 220 square feet including counters, closets and built-ins, and excluding the bathroom. Existing facilities may have a minimum of 180 square feet. The kitchen area must have a refrigerator, microwave or stove top, and a counter or table for food preparation. New facilities must also have a sink and counter area and storage area. Units must have lockable entry doors and a living area wired for telephone and television service, where available. Facilities must provide a home-like environment that provides residents with an opportunity for self-expression, and encourages interaction with the community, family and friends.
Admission/Retention Policy
Boarding homes may accept and retain an individual as a resident in a boarding home only if:
- The boarding home can meet the individual's needs, including providing any specialized training to resident-care staff persons that may be required;
- The individual's health care condition is stable and predictable, as determined jointly by the boarding home and the resident or the resident's representative if appropriate. When residents require services of a licensed nurse, the registered nurse must specifically assess, determine and document in the resident's record if the resident's health care condition is stable and predictable. Residents who do not require the services of a licensed nurse on the boarding home premises are assumed to have stable and predictable conditions;
- The individual is ambulatory, unless the boarding home is approved by the Washington state director of fire protection to care for semi-ambulatory or non-ambulatory residents; and
- The individual meets the acceptance criteria the boarding home described in the boarding home's disclosure information.
Nursing Home Admission Policy
Individuals eligible for admission to a nursing home and COPES waiver services must meet one of four criteria.
- Require care provided by or under the supervision of a registered nurse or a licensed practical nurse on a daily basis;
- Have an unmet need requiring substantial or total assistance with at least two or more of the following ADLs: eating, toileting, ambulation, transfer, positioning, bathing and self-medication;
- Have an unmet need requiring minimal, substantial or total assistance in three or more of the above ADL; or
- Have a cognitive impairment and require supervision due to one or more of the following: disorientation, memory impairment, impaired judgment, or wandering and have an unmet or partially met need with at least one or more of the ADLs.
Services
Boarding homes. Residents receive a preadmission assessment that covers medical history; necessary and contraindicated medications; a licensed medical or health professional's diagnosis; significant known behaviors or symptoms that may cause concern or require special care; mental illness diagnosis, except where protected by confidentiality laws; level of personal care needs; activities and service preferences; and preferences regarding other issues important to the applicant, such as food and daily routine. An initial service plan is prepared to identify the resident's immediate needs and provide direction to staff and caregivers relating to the resident's immediate needs, capabilities, and preferences. Assessors must have a master’s degree and two years experience or a bachelor’s degree and three years experience, or be a registered nurse, physician or have three years successful experience completing assessments in a boarding home. Comprehensive assessments must be completed within 14 days following the date the resident moves in, and are required annually. The regulations identify the topics that must be included in the assessment.
Negotiated service agreements must be developed based upon discussions with the resident and the resident's representative, and the preadmission assessment of a qualified assessor. The service agreement includes the care and services necessary to meet the resident's needs, defined roles and responsibilities of the resident, the boarding home staff, and resident's family or other significant persons in meeting the resident's needs and preferences; the times services will be delivered, including frequency and approximate time of day, as appropriate; the resident's preferences for activities and how those preferences will be supported; appropriate behavioral interventions, if needed; a communication plan, if special communication needs are present; the resident's ability to leave the boarding home premises unsupervised; and a prohibition against waiving resident rights, or holding resident’s liable for loss of personal property or injury.
Boarding homes must provide activities, housekeeping, laundry, meals and nutritious snacks and provide for the general safety and well being of the resident, which means providing prescribed low sodium diets, diabetic diets, mechanical soft foods, emergency assistance, monitoring, arranging health care appointments; coordinating health care services with outside providers; and assisting residents to obtain and maintain eye glasses, hearing aids, dentures and other devices. Boarding homes may provide optional services such as assistance with ADLs (bathing, dressing, eating, personal hygiene, transferring, toileting, mobility) and health support services (blood glucose testing, puree diets, calorie controlled diabetic diets, dementia care, mental health care and developmental disabilities care). Homes that do not provide assistance with ADLs may only admit residents who are independent.
Intermittent nursing services (medication administration, administration of health treatments, diabetic management, non-routine ostomy care, tube feeding and nurse delegation) may be provided and any limitations, additional services or conditions must be disclosed. Facilities must implement systems that support the safe practice of nursing.
Homes may also provide adult day care services for non-residents.
Medicaid. A formal written negotiated plan, which involves the resident, appropriate staff, the Aging and Disability Services Administration (ADSA) case manager and family members, must be completed. The contractor must provide the services agreed upon in the resident's negotiated service agreement and approved by the department case manager, including any reasonable accommodations required; and provide the resident and case manager with a copy of the negotiated service agreement.
The State's nurse practice act was amended and allows RNs to delegate tasks to nursing assistants in licensed boarding homes. Nursing assistants must complete a core training program and may perform the following delegated nursing tasks: oral and topical medications and ointments; nose, ear, eye drops, and ointments; dressing changes and catheterization; suppositories, enemas, and ostomy care; blood glucose monitoring; and gastronomy feeding in established and healed condition. Delegation is at the discretion of the nurse and only for people whose conditions are stable and predictable.
Dietary
The regulations require three meals a day at regular intervals and no more than 14 hours between the evening meal and breakfast the next day unless a nutritious snack is provided. Menus must be written at least one week in advance and delivered to residents' rooms or posted where residents can see them. Menus provide a variety of foods and are not repeated for at least three weeks, except that breakfast menus in boarding homes that provide a variety of daily choices of hot and cold foods are not required to have a minimum three-week cycle.
Agreements
Provisions regarding agreements are contained in the State’s resident rights statute. This law requires that facilities inform residents or their representative of the services, items, and activities customarily available in or arranged by the facility; the charges, including charges for items that are not included in the per diem rate; and the rules of operation. Facilities must also fully disclose to potential residents their service capabilities.
Boarding homes are required to complete a thorough disclosure forms that includes required a description of required services, level of ADL assistance, intermittent nursing services, help with medications, policy on services arranged by residents, care for residents with dementia, developmental disabilities and mental illness, transportation, ancillary services, smoking policy, payments, “bed hold” policy, Medicaid support, fire protection and security features and the licensing status.
Potential residents must be informed of their rights regarding health care decision making consistent with applicable state and federal laws and rules, before or at the time the individual moves into the boarding home.
Provisions for Serving People with Dementia
All boarding homes that serve residents with dementia must obtain information about the resident’s significant life experiences; ability to articulate personal needs and initiate activity; patterns of behavior that express concerns such as wandering, agitation, resistance to care, social isolation and aggression. Egress control may not restrict resident’s who are able to leave the home safely. Appropriate sprinkler and fire alarm systems are required for areas of restricted egress. Control devices must automatically de-activate when the fire alarm or sprinkler activates.
The training regulations require that staff receive training on: introduction to the dementias; dementia, depression, and delirium; resident-based caregiving; dementia caregiving principles; communicating with people who have dementia; sexuality and dementia; re-thinking “problem” behaviors; hallucinations and delusions; helping with activities of daily living (ADLs); and working with family and friends.
Homes that contract with Medicaid to provide enhanced adult residential-specialized dementia care have to meet additional standards. “Enhanced adult residential care-specialized dementia care services” is a package of services, including specialized dementia care assessment and care planning, personal care services, intermittent nursing services, medication administration services, specialized environmental features and accommodations, and activity programming. Contractors must complete a full re-assessment of residents on a semi-annual basis; and maintain awake staff twenty-four hours per day. The contractor must provide staffing that is adequate to respond to the assessed sleeping and waking patterns and needs of residents; and develop and implement policies and procedures. The contractor must have a plan that identifies the professional who will provide the consultation, and when and how the consultation will be utilized to manage residents who may wander; and outline actions to be taken in case a resident elopes.
Each staff who works directly with residents must have at least six hours of continuing education per year related to dementia, including Alzheimer's disease, that include but are not limited to the following topics: aggressive behaviors and catastrophic reactions; agitation and caregiving strategies; delusions and hallucinations; dementia problem-solving strategies; depression and dementia; fall prevention for dementia; personal care as meaningful activity; promoting pleasant and purposeful activity; and resistance to care.
On a daily basis, the contractor must provide residents access to opportunities for independent, self-directed activities and offer opportunities for activities that accommodate variations in a resident's mood, energy and preferences. Multiple common areas must be available, at least one of which is outdoors, that vary by size and arrangement such as: various size furniture groupings that encourage social interaction; areas with environmental cues that may stimulate activity, such as a resident kitchen or workshop; areas with activity supplies and props to stimulate conversation; a garden area; and paths and walkways that encourage exploration and walking.
Medication Administration
Boarding homes must provide medication assistance and may provide medication administration. Medication Administration means the direct application of a prescribed medication whether by injection, inhalation, ingestion, or other means, to the body of the resident by a person legally authorized to do so. Medication assistance means assistance with self-administration of medication rendered by a non-practitioner to a resident of a boarding home in accordance with chapter 246-888 WAC.
Public Financing
The State reimburses for assisted living services, enhanced adult residential care and adult residential care under an HCBS waiver and the Medicaid State plan. All three levels of services are provided by licensed boarding homes that contract with Medicaid. Enhanced adult residential care and assisted living services are provided to HCBS waiver participants. Adult residential care services are provided under the Medicaid state plan.
Assisted living services is a package of services, including personal care and limited nursing services, that the department contracts with a licensed boarding home to provide. The regulations require that assisted living services be provided to a resident in a private apartment-like unit.
Enhanced adult residential care is a package of services, including personal care and limited nursing services, that the department contracts with a licensed boarding home to provide.
Adult residential care is a package of services, including personal care services, that the department contracts with a licensed boarding home to provide.” WAC 388-110-120 et seq. The contracting regulations set standards in addition to the licensing rules.
The State replaced a four tiered payment methodology with 12 classifications for residential settings that include regional variations. The rates are based on components for provider staff, operations, and capital costs. The rates include an amount ($505.16 a month) paid by residents for room and board costs. The SSI payment standard is $564 a month in 2004 and therefore, the PNA would be $58.84. In addition to the service amounts, a capital add-on is available for newly constructed facilities whose capital costs exceed the room and board allowance. Criteria for allowing family supplementation of resident income for room and board are being revised. The pending changes may allow supplementation in limited circumstances.
| Level of Service |
2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Participants | Facilities | Participants | Facilities | Participants | |
| Assisted living services | 205 | 4,404 | 206 | 3,762 | 168 | 2,919 |
| Enhanced adult residential care | 163 | 888 | 166 | NR | NR | NR |
| Adult residential care | 158 | 443 | 167 | NR | NR | NR |
| NOTE: Facilities may contract for more than one level of service. | ||||||
Staffing
Staff must be sufficient to furnish services and care needed by residents consistent with the negotiated service agreements, maintain the home free of safety hazards, and implement fire and disaster plans.
Training
Boarding home administrators must be 21 and qualify under a number of provisions. Individuals may serve as an administrator if they were actively employed as a boarding home administrator and met existing qualifications on September 1, 2004; hold a current state nursing home administrator license; obtained a certificate for completing administrator training; or have other combinations of education and experience. Administrators must complete training in the statutes covering boarding homes; criminal history background checks; abuse of vulnerable adults; resident rights; and long-term care services training.
Boarding home staff receive orientation and training on the organization of the boarding home; its physical boarding home layout; their specific duties and responsibilities; how to report resident abuse and neglect consistent with chapter 74.34 RCW and boarding home policies and procedures; policies, procedures, and equipment necessary to perform duties; needs and service preferences identified in the negotiated service agreements of residents with whom the staff persons will be working; and resident rights, including without limitation, those specified in chapter 70.129 RCW. Managers must develop and implement a process to ensure caregivers have information from the preadmission assessment, on-going assessment and negotiated service agreement relevant to providing services to each resident with whom the caregiver works; are informed of changes in the negotiated service agreement of each resident with whom the caregiver works; and are given an opportunity to provide information to responsible staff regarding the resident when assessments and negotiated service agreements are updated for each resident with whom the caregiver works.
Direct care staff must also complete a basic training program that covers core knowledge and skills that caregivers need in order to provide personal care services effectively and safely and pass a competency test. DSHS must approve basic training curricula.
Background Check
The boarding home must ensure that staff have a criminal history background and homes may not hire individuals convicted of a crime against persons as defined in RCW 43.43.830; financial exploitation as defined in RCW 43.43.830; found in any disciplinary board final decision to have abused a vulnerable adult under RCW 43.43.830; the subject in a protective proceeding under chapter 74.34 RCW; convicted of criminal mistreatment; or found by the department to have abused, neglected, or exploited a vulnerable person in any matter in which an administrative hearing due process right is offered and the finding is upheld through the hearing process or the individual failed to timely appeal the finding.
Monitoring
The licensing agency makes periodic inspection and survey visits. The licensing agency dropped “quality improvement consultation” because of budget reductions. The service, provided upon request, helps facilities understand regulatory requirements and share best practices. Funds to continue the program have not been approved.
Case managers are a primary source of monitoring for quality assurance for Medicaid beneficiaries. During regular visits, the case manager checks to see if the client is satisfied, the negotiated service plan is being carried out, and that the plan is appropriate for the resident.
Homes may maintain a quality assurance committee that includes a licensed registered nurse, the administrator and three other members from the staff of the boarding home. When established, committees meet at least quarterly to identify issues that may adversely affect quality of care and services to residents and to develop and implement plans of action to correct identified quality concerns or deficiencies in the quality of care provided to residents. To promote quality of care through self-review without the fear of reprisal, and to enhance the objectivity of the review process, the department shall not require, and the long-term care ombudsman program shall not request, disclosure of any quality assurance committee records or reports, unless the disclosure is related to the committee's compliance with this section, if: the records or reports are not maintained pursuant to statutory or regulatory mandate; and the records or reports are created for and collected and maintained by the committee.
Fees
Facilities are charged $79 annually per licensed bed. An additional $150 is payable for facilities receiving a third site visit because of failure to respond adequately to deficiencies or facilities receiving a full out-of-sequence inspection resulting from information gathered during a complaint investigation.
| January 1, 2004 Adsa Community Residential Daily Rates | |||||
|---|---|---|---|---|---|
| CARE | King County | ||||
| AL | ARC | EARC | AFH | ||
| SSPS | W/O Cap Add-On | With Cap Add-On | |||
| Classification | Daily Rate | Daily Rate | Daily Rate | Daily Rate | Daily Rate |
| 1 | $61.90 | $66.74 | $43.77 | $43.77 | $44.38 |
| 2 | $67.02 | $71.86 | $49.67 | $49.67 | $50.36 |
| 3 | $75.20 | $80.04 | $63.44 | $63.44 | $56.35 |
| 4 | $61.90 | $66.74 | $43.77 | $43.77 | $44.38 |
| 5 | $69.07 | $73.91 | $55.57 | $55.57 | $56.35 |
| 6 | $82.36 | $87.20 | $71.31 | $71.31 | $64.32 |
| 7 | $67.02 | $71.86 | $49.67 | $49.67 | $50.36 |
| 8 | $75.20 | $80.04 | $63.44 | $63.44 | $64.32 |
| 9 | $93.62 | $98.46 | $83.12 | $83.12 | $84.27 |
| 10 | $69.07 | $73.91 | $55.57 | $55.57 | $64.32 |
| 11 | $75.20 | $80.04 | $63.44 | $63.44 | $72.30 |
| 12 | $93.62 | $98.46 | $83.12 | $83.12 | $84.27 |
| CARE | Metropolitan Counties | ||||
| AL | ARC | EARC | AFH | ||
| Classification | Daily Rate | Daily Rate | Daily Rate | Daily Rate | Daily Rate |
| 1 | $56.79 | $61.18 | $43.77 | $43.77 | $44.38 |
| 2 | $59.86 | $64.25 | $47.70 | $47.70 | $48.37 |
| 3 | $73.16 | $77.55 | $60.49 | $60.49 | $53.35 |
| 4 | $56.79 | $61.18 | $43.77 | $43.77 | $44.38 |
| 5 | $64.97 | $69.36 | $52.62 | $52.62 | $53.35 |
| 6 | $80.32 | $84.71 | $67.38 | $67.38 | $61.33 |
| 7 | $59.86 | $64.25 | $47.70 | $47.70 | $48.37 |
| 8 | $73.16 | $77.55 | $60.49 | $60.49 | $61.33 |
| 9 | $90.55 | $94.94 | $77.21 | $77.21 | $78.29 |
| 10 | $64.97 | $69.36 | $52.62 | $52.62 | $61.33 |
| 11 | $73.16 | $77.55 | $60.49 | $60.49 | $68.31 |
| 12 | $90.55 | $94.94 | $77.21 | $77.21 | $78.29 |
| CARE | Non-Metropolitan Counties | ||||
| AL | ARC | EARC | AFH | ||
| Classification | Daily Rate | Daily Rate | Daily Rate | Daily Rate | Daily Rate |
| 1 | $55.77 | $60.45 | $43.77 | $43.77 | $44.38 |
| 2 | $59.86 | $64.54 | $46.72 | $46.72 | $47.37 |
| 3 | $73.16 | $77.84 | $59.51 | $59.51 | $52.36 |
| 4 | $55.77 | $60.45 | $43.77 | $43.77 | $44.38 |
| 5 | $64.97 | $69.65 | $51.64 | $51.64 | $52.36 |
| 6 | $80.32 | $85.00 | $65.41 | $65.41 | $60.34 |
| 7 | $59.86 | $64.54 | $46.72 | $46.72 | $47.37 |
| 8 | $73.16 | $77.84 | $59.51 | $59.51 | $60.34 |
| 9 | $90.55 | $95.23 | $74.26 | $74.26 | $75.30 |
| 10 | $64.97 | $69.65 | $51.64 | $51.64 | $60.34 |
| 11 | $73.16 | $77.84 | $59.51 | $59.51 | $66.32 |
| 12 | $90.55 | $95.23 | $74.26 | $74.26 | $75.30 |
West Virginia
Citation
Assisted living residences, 64 CSR 14 et seq., in conjunction with §16-5D-1
Residential care communities, §16-5N-1 et seq.
General Approach and Recent Developments
Changes in 2003 combined personal care homes and residential board and care homes into one category of assisted living residences. Final rules for assisted living residences were promulgated in February 2004. The State is currently concerned about liability insurance for facilities. Due to the high cost of liability insurance in the State, facilities have indicated that they may need to go out of business or look to provide another kind of service. The State already revised the assisted living rules regarding the requirement to obtain liability insurance. Instead, facilities must disclose to all residents whether they hold liability insurance or not, and it is the resident’s right to make an informed decision as to whether they want to move into that facility. Concerns regarding the potential loss of facilities due to liability insurance have been raised by the Health Care Advisory Board with this information presented to the Legislature, but there has been no additional legislation offering alternatives to the assisted living residences at this time.
Rules creating a separate category for facilities serving residents with dementia were effective July 1, 2002. Rules implementing the residential care communities were effective July 1, 1999.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Assisted living residences | 113 | 3,197* | NA | NA | NA | NA |
| Personal care homes | NA | NA | 50 | 2,310 | 52 | 2,342 |
| Residential board and care | NA | NA | 82 | 1,498 | 80 | 1,197 |
| Residential care communities (apartments) | 3 | 88 | 3 | 88 | 3 | 88 |
| * Refers to bed capacity, not necessarily individual units | ||||||
Definition
Assisted living residences. Any living facility or place of accommodation in the State, however named, available for four (4) or more residents, that is advertised, offered, maintained or operated by the ownership or management, for the express or implied purpose of providing personal assistance, supervision, or both, to any residents who are dependent upon the services of others by reason of physical or mental impairment, and who may also require nursing care at a level that is not greater than limited and intermittent nursing care. A small assisted living residence has a bed capacity of four (4) to sixteen (16). A large assisted living residence has a bed capacity of seventeen (17) or more.
Residential care communities were created by Chapter 163 in1997. A residential care community means any group of 17 or more residential apartments, however named, which are part of a larger independent living community and which are advertised, offered, maintained, or operated by an owner or manager, regardless of consideration or the absence thereof, for the express or implied purpose of providing residential accommodations, personal assistance, and supervision on a monthly basis to 17 or more persons who are or may be dependent upon the services of others by reason of physical or mental impairment or who may require limited and intermittent nursing care but who are capable of self-preservation and are not bedfast.
Alzheimer’s/Dementia special care units means any licensed facilities, as defined in this rule, that provide specialized services, 24 hours per day, in a specialized unit in the facility, for residents with a diagnosis of Alzheimer’s disease or related dementia; and that advertises, markets, or otherwise promotes the facility as providing a specialized unit for residents requiring Alzheimer’s/dementia care services.
Unit Requirements
Assisted living residences must provide each resident with a bed in a bedroom. In an existing large assisted living residence, bedrooms shall contain at least 80 square feet of floor area per resident. In an existing small assisted living residence, semi-private bedrooms shall contain at least 60 square feet of floor area per resident and private rooms shall contain 80 square feet. In a newly constructed or renovated residence no more than two persons shall occupy a bedroom. Space requirements for new construction include 100square feet for a private room and 90 square feet per resident for a semi-private room. In an existing residence no bedroom shall be occupied by more residents than the bed capacity approved by the commissioner. A minimum of one toilet and lavatory is required for every six residents. A minimum of one bathing facility per floor, with a bath tub or shower, equipped with non-slip surfaces, a flushing toilet and a hand washing sink, are required for every ten residents.
Residential care communities must offer apartment units with at least 300 square feet, with lockable doors, at least one bedroom, a kitchenette with a sink and refrigerator, and one full bathroom. Multi-occupancy apartments must have at least 80 square feet of bedroom space per resident and no more than two residents may occupy an apartment.
Admission/Retention Policy
Assisted living residences may not admit individuals requiring ongoing or extensive nursing care and shall not admit or retain individuals requiring a level of service that the residence is not licensed to provide or does not provide. A resident whose condition declines after admission, and is receiving services coordinated by a licensed hospice or certified home health agency, may receive these services in the residence if the residence has a backup power generator for services using equipment that requires auxiliary electrical power in the event of a power failure. The licensee shall ensure that a resident who requires ongoing or extensive nursing care is provided the care and services necessary to meet his or her needs. The provision of services to the resident receiving nursing care or hospice care shall not interfere with the provision of services to other residents. If a resident has care needs that exceed the level of care for which the residence is licensed or can provide, the residence must inform the resident of the need to move to another facility that can provide that level of care, and assist the resident in making that transition.
If a resident exhibits symptoms of a mental or developmental disorder that seems to pose a risk to self or others, and the resident is not receiving behavioral health services, the residence must advise the resident or his or her legal representative of the behavioral health service options within the community. The resident must have thirty days to obtain necessary services. If the resident or his or her legal representative fails to seek treatment in a timely manner, then the residence, after consultation with the resident’s physician, shall refer the resident to a licensed behavioral health provider.
The residence must seek immediate treatment for a resident or may refuse to admit or retain a resident if there is reason to believe that the resident may suffer serious harm, or is likely to cause serious harm to himself, herself or to others, if appropriate interventions are not provided in a timely manner.
Facilities may not admit those who require the use of routine physical or chemical restraints, require ongoing or extensive nursing services, or require a level of service of which the home is not licensed or does not provide. Individuals who become bedfast subsequent to admission may remain in the home for 90 days during a temporary illness or when recovery from surgery if the resident’s care does not require nursing care in excess of limited and intermittent nursing care.
Residential care communities. Residents must be certified by a physician to be capable of self-preservation. Residents may need personal assistance in ADLs, supervision because of mental or physical impairment, or limited and intermittent nursing needs. Following admission, facilities may retain residents who receive hospice services. Residents who are not capable of self-preservation may be retained for 90 days during a temporary illness or recovery from surgery if they do not require nursing care that exceeds the regulations.
Services
Assisted living residences. Rather than specifying what type of services a residence must provide, ALRs must indicate up front what services they will provide to residents, as long as services are not at the level of a nursing home. ALRs may provide limited and intermittent nursing services and may provide these types of services for a longer period of time as long as home health agencies are providing long-term nursing.
Residential care communities provide personal assistance; help with self-administration of medications; and help in following planned diets, activity regimens, or use of equipment. Staff must assist in making appointments for dental and medical services. Medications may be administered by licensed staff. Facilities that provide limited and intermittent nursing services must contract with or employ a registered professional nurse.
Dietary
Three meals, snacks, and special diets are required that substantially comply with the recommended dietary allowances of the Food and Nutrition Board. Therapeutic or modified diets must be prepared according to a physician or dietician’s orders. The rules describe the variety of foods that must be served. Training must include nutrition. The residence shall accommodate residents who are unable to eat at the planned mealtime and provide for a meal substitution if the resident does not tolerate or like the foods planned for the meal.
Agreements
Assisted living residences. Agreements, at a minimum, must include the type of resident population that the residence is licensed to serve and will serve; the health and nursing care services that the residence will provide to meet the resident’s needs, including cardiopulmonary resuscitation, and how they will be provided; an annual or monthly contract price, full disclosure of all costs including what changes in care needs will result in increases, additions or modifications to the costs, the refund policy and an assurance that the resident shall not be held liable for any cost that was not disclosed; discharge criteria, including notification policies; how to file a complaint; medication storage, handling, distribution, and disposition, and responsibility for payment; management of residents’ funds; and whether or not the residence has liability insurance coverage. At the same time as providing the contract, the licensee must also provide the resident with the following information: house rules governing resident behavior and responsibilities; the resident's bill of rights; how the resident's personal property will be protected from loss and theft; the requirements for medical examinations and treatment orders; how the resident will be assisted in making appointments for medical, dental, nursing or mental health services, and how transportation to and from these services will be arranged; and how to access the residence’s policies and procedures.
Residences are prohibited from entering into a life care contract without the prior written permission of the commissioner. Residences must provide residents with a thirty day written notice for any increases, changes, or modifications to the rates.
Each resident must have a health assessment conducted by a physician not more than sixty days prior to admission, no more than five days after admission, and annually thereafter. The assessment must include a screening for tuberculosis.
Within seven days of admission, each resident must have a functional needs assessment. At a minimum, the resident's assessment shall include a review of health status and functional, psycho social, activity and dietary needs. A service plan must be developed within seven days, and is based upon the functional needs assessment.
Residential care communities. The agreement covers admission, retention, and discharge policies; assurance that the community will meet the individual’s needs; full disclosure of costs including an annual or monthly contract price; the refund policy and an assurance that the resident will not be liable for any undisclosed cost; how health care will be arranged or provided; the complaint process; how prescribed medications are obtained and responsibility for payment; and the storage, administration, and disposal of medications.
Provisions for Serving People with Dementia
Special care facilities must have a staff person with experience and training in dementia care to coordinate outside services, offer monthly educational and family support meetings, and advocate for residents. Staff training includes a minimum of 30 hours on care for residents with dementia covering the philosophy of care; nature, stages, and treatment of the disease; therapeutic interventions; communication techniques; medication management; therapeutic environmental modifications; assessment and care planning; the role of family and their need for support; staff burn-out prevention; and abuse prevention. Eight hours of annual training is required. Staffing patterns must be able to provide 2.25 hours of direct care time per resident per day. At least two staff must be present for units serving more than five residents. An RN must be available if residents require nursing procedures. Appropriate assessments must be completed and care plans developed. Appropriate activities are provided by a therapeutic specialist, occupational therapist, or activities professional. The rules describe special requirements for the physical environment with security measures; high visual contrast between floor, walls, and walkways; non-reflective surface; secured outdoor space; and other requirements.
Other licensed facilities that do not market themselves as offering special care units provide training to staff that includes activities, programs, and/or professionally-designed intervention strategies to help a resident with behavioral health needs to manage his/her own behavior. Residents with early symptoms of dementia may be served.
Medication Administration
Facilities may administer and assist with self-administration of medications. Aides who have passed required training may administer medications. A licensed health care professional shall determine whether or not a resident is capable of self-administration of medications. The residence shall keep a record of all medications given to each resident indicating each dose given. The record shall include the resident's name;the name of the medication; the dosage to be administered and route of administration; the time or intervals at which the medication is to be administered; the date the medication is to begin and end; the printed name, initials and signature of the individual who administered the medication; and any special instructions for handling or administering the medication, including instructions for maintaining aseptic conditions and appropriate storage.
Public Financing
A small HCBS waiver was approved in August 2004 to support 150 people living in elderly housing in four counties. The public housing authorities (PHAs) will renovate and obtain a license for the portion of the buildings to be used for assisted living. The PHAs will become providers of waiver services which will include personal care, homemaker, chore, attendant care, companion, medication oversight, therapeutic social and recreational programming, transportation, and periodic nursing evaluations.
The State pays, from state revenues, assisted living residences the difference between the resident’s income (minus a personal needs allowance of $69), and $924.50 a month for room, board, and personal care services for eligible individuals. This is an option that previously existed for licensed personal care homes and residential board and care homes. Family supplementation is not allowed. In order to be eligible for this payment, the resident must need personal care services as determined by a physician and a comprehensive assessment, and must not have sufficient funds to pay for the service. There are currently 47 facilities accepting state funding, with a total of 319 residents. The State does not currently reimburse assisted living under Medicaid but is exploring a method to do so.
Staffing
Assisted living residences. Administrators in large ALRs must have an associate’s degree and be at least 21 years of age. Administrators in small ALRs must have a high school diploma or GED. Each assisted living residence shall have a minimum of one direct care staff person twenty-four (24) hours per day and shall have a sufficient number of qualified employees on duty to provide the residents with all of the care and services they require. The residence shall have one additional direct care staff on the day shift for each ten residents identified on their functional needs assessment to have two or more of the following care needs: dependence on staff for eating, toileting, ambulating, bathing, dressing, repositioning, special skin care, or one or more inappropriate behaviors that reasonably requires additional staff to control, such as sexually acting out, stripping in public settings, refusing basic care, or destroying property; or injurious behavior to self or others; one additional direct care staff on the evening shift for each fifteen residents identified on their functional needs assessment to have two or more of these care needs; and one additional direct care staff on the night shift for each eighteen residents identified with two or more of these care needs. One employee who has current first aid training and current cardiopulmonary resuscitation training, as applicable, shall be on duty at all times. The licensee must have awake staff present in the residence during normal resident sleeping hours when residents require sleep time supervision. In multi-level residences, there must be at least one awake staff person on duty while residents are sleeping, unless the residents have been certified by a physician or licensed psychologist as not requiring sleep time supervision.
Residential care communities. The administrator must be at least 21 years old and have an associate’s degree or equivalent in a related field. The community must have at least one staff member on duty per shift. Sufficient staff must be available to care for residents. Awake staff are required when residents require supervision or intermittent nursing services. Multi-story facilities must have one awake staff per floor unless supervision or intermittent nursing services are not needed and there is a call system.
Training
Administrators in assisted living residences shall participate in eight (8) hours of training related to the operation of a residence annually and a record of this training shall be available for review. Staff must participate in training within the first fifteen days of hire, with topics covering emergency procedures and disaster plans; the residence’s policies and procedures; resident rights; confidentiality; abuse prevention and reporting requirements; the ombudsmen’s role; complaint procedures; specialty care based on individualized resident needs and service plans; care of residents with dementia; the provision of group and individual resident activities; and infection control.
Administrators in residential care communities must receive at least 10 hours of training related to the operation and administration of personal care homes each year.
Staff of residential care communities must receive employee orientation and training. Training shall be provided to new employees and new admissions (within the first 24 hours of association with the home) in emergency procedures, evacuation of the home, procedures to report a missing resident, medical emergencies, accidents, fire, natural disasters, or other emergencies.
The home shall maintain a written plan of orientation and training for employees. Such training will be provided within the first 15 days of employment inclusive of the following:
- Policies and procedures of the home;
- The rights and responsibilities of residents including protection of resident privacy and confidentiality;
- Complaint procedures of the home;
- Procedures and agencies available in instances of abuse, neglect, mistreatment;
- The care of aged, infirm, or disabled adults with consideration for individual capabilities and needs;
- Personal assistance procedures as needed for resident care, including at a minimum, personal grooming care, personal hygiene care, nutritional services, and signs and symptoms of alteration of skin integrity;
- Specific duties and responsibilities of the residential staff for assisting current residents of the home (i.e., a review of individualized service plans, the activities program, and/or professionally-designed intervention strategies to help a resident with behavioral health needs to manage his or her behavior);
- Cardiopulmonary resuscitation (CPR), as applicable, and First Aid; and
- Infection control.
Background Check
Assisted living residences. All staff in an ALR shall have a personal history that is free of evidence of abuse, fraud, or substantial and repeated violations of applicable laws and rules in the operation of any health or social care facility or service organization, or in the care of dependent persons; or conviction of crimes related to the care to a dependent persons as evidenced by a criminal investigative background check by the West Virginia state police through the central abuse registry.
Monitoring
The licensing agency makes on-site unannounced inspections as needed and investigates complaints. The licensing agency prepares a written report of any inspection within fifteen (15) days of the completion of the inspection and sends a report to the licensee or administrator outlining the statement of deficiencies. The licensee of an assisted living residence must develop, sign and date a plan of correction, and send it to the licensing agency within fifteen working days of the receipt of the statement of deficiencies. Immediate correction is required for violations identified as constituting immediate and serious threats to the health or safety of a resident or employee.
Fees
Fees for assisted living facilities are $6.00 per bed and $4.32 per bed for residential care communities.
Wisconsin
Citation
Residential care apartment complexes, Chapter HFS 89.
Community-based residential facilities, Chapter HFS 83.
General Approach and Recent Developments
Wisconsin has two types of residential care facilities: community-based residential facilities (CBRFs) and residential care apartment complexes (RCACs).
RCACs may be either certified or registered. Regulations providing for RCAC registration and certification were effective March 1997. Registered facilities do not receive regulatory monitoring and cannot contract with counties to serve Medicaid beneficiaries. Tenants residing in registered facilities must be notified that the department does not regularly visit or inspect these facilities. The rules state that the chapter governing RCACs is intended to ensure that all residential care apartment complexes provide each tenant with an independent apartment in a setting that is home-like and residential in character; make available personal, supportive and nursing services that are appropriate to the needs, abilities and preferences of individual tenants; and operate in a manner that protects tenants' rights, respects tenant privacy, enhances tenant self-reliance and supports tenant autonomy in decision-making including the right to accept risk.
Facilities must be certified to receive Medicaid reimbursement. To be certified, facilities must submit documents showing compliance with all applicable federal, state, and local licensing, building, zoning, and related requirements. Certified facilities may be visited to determine compliance with certification requirements.
Several levels of CBRFs are licensed based on size (small: 5 to 8 beds; medium: 9 to 20 beds; and large: 21 or more beds) and six classes of care based on whether residents are ambulatory (walk without difficulty); semi-ambulatory (able to walk with difficulty or only with assistance of an aid such as crutches, a cane, or walker); and non-ambulatory (not able to walk at all but able to be mobile with the help of a wheelchair) and when the resident can self-evacuate the building in the event of a fire. The State is currently revising the rules for CBRFs.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| RCAC certified | 85 | 3,406 | 122 | 4,452 | 94 | 3,211 |
| RCAC registered | 66 | 2,595 | ||||
| Community based residential facilities | 1,359 | 21,374 | 1,350 | 21,242 | 1,340 | 21,064 |
The Bureau of Health Care Quality created an Assisted Living Forum in 2004 to recommend revisions to the CBRF rules. Earlier proposed changes were placed on hold pending further review by the Forum, comparison to rules in other states and a review of the recommendations from the national Assisted Living Workgroup. The purpose of the rule revision is to eliminate unneeded or inefficient regulations, and to create outcome-oriented rules. The revisions will also update training standards, and replace department-approved training programs with competency testing or other methods.
Definition
A residential care apartment complex is “a place where five or more adults reside that consists of independent apartments, each of which has an individual lockable entrance and exit, a separate kitchen, including a stove, an individual bathroom, sleeping, and living areas, and that provides, to a person who resides in the place, not more than 28 hours per week of supportive, personal and nursing services. A residential care apartment complex does not include a nursing home or a community-based residential facility, but may be physically part of a structure that is a nursing home or community based residential facility.”
Facilities that are part of a nursing facility or a community based residential facility must be physically separate and distinct although they may share a common lobby and entrance. They may also share common dining and activity areas as long as they are not scheduled for concurrent use.
A community based residential facility is a place where five or more unrelated adults reside, in which care, treatment, or services above the level of room and board are provided to residents as a primary function of the facility not to exceed three hours per resident per week of nursing care.
Unit Requirements
Residential care apartment complex. The rules require units with a minimum of 250 square feet for sleeping and living areas, excluding closets. The kitchen must be a visually and functionally distinct area of the unit. Microwave ovens may be used instead of stoves. The sleeping and living areas also have to be visually and functionally distinct but not separate rooms. Variances may be granted for facilities converting to assisted living to allow up to a 10 percent reduction in square footage requirements.
Community based residential facilities. Private rooms must offer 100 square feet and double rooms 80 square feet per person. No more than two residents may share a room. Small and medium facilities must offer one bathroom and shower facility for every eight residents. Large facilities must have one toilet, bath, and shower for every eight male residents and every eight female residents.
Admission/Retention Policy
Residential care apartment complex. The rules require the development of a mutually agreed upon service agreement and signing of a negotiated risk agreement. The risk agreement identifies situations or conditions known by the facility to arise from the tenant's preferences which are contrary to the facility's advice, how they will be accommodated, alternatives offered to reduce the risk, the agreed upon course of action, and the tenant's understanding and acceptance of responsibility.
Facilities may retain tenants whose needs can be met by the facility or met by services available from another provider. Facilities may not admit anyone who has a court determination of incompetence, anyone who has an activated power of attorney for health care, anyone found by a physician or psychologist to be incapable of recognizing danger, summoning assistance, expressing need, or making care decisions, unless they share a unit with a competent person who has legal responsibility for the individual. Facilities may also retain a tenant who becomes incompetent as long as adequate oversight and service are provided and risk agreements are signed by the guardian (these residents must have a guardian) or agent with power of attorney.
Facilities may terminate agreements with tenants whose needs cannot be met by the facility if service needs exceed 28 hours a week (unless additional services are secured by the tenant from other providers), tenants require 24-hour-a-day nurse availability, the tenant is a danger to self or others, or fees have not been paid.
Community based residential facilities may not admit or retain anyone who is confined to bed by illness or infirmity (unless it is temporary); who is destructive; has physical, mental, psychiatric, or social needs that are not compatible with the CBRFs client group; needs more than three hours of nursing care per week except for a temporary condition lasting no more than 90 days; requires 24-hour supervision by an RN or LPN; has chronic personal care needs that cannot be met by the facility or a community agency; or who requires restraints. A waiver may be granted for residents needing more than three hours of skilled care a week if his or her condition is stable and the services needed are available in the facility.
In its licensing application, the facility must specify the group of residents to be served.
Nursing Home Admission Policy
Individuals qualify if they have severe medical conditions or substantial medical and social/behavioral needs. If the latter, an individual must meet all of the following eligibility criteria:
- A long-term or irreversible illness or disability;
- An unstable or stable medical or psychiatric condition requiring long-term maintenance and prevention;
- Needs help with two or more IADLs;
- Needs assistance with two or more ADLs (feeding oneself, dressing, bathing, using the toilet, getting out of bed or up from a chair, ambulation, or requires daily supervision to ensure safety or wanders, is combative or abusive, incompetent or seriously mentally ill; and
- Has no friends or relatives able or willing to provide assistance.
Substantial medical conditions include significant deterioration of physical or mental health in the past 12 months; a need for daily monitoring of fluid and solid intake; uses six or more prescriptions at least three days a week; needs assistance with medications; incontinence; physician ordered turning or repositioning; daily range of motion exercises to prevent skin breakdown; direct assistance with health care needs five days a week; over 85 and unable to manage medical conditions; and other conditions. People with dementia who do not need regular nursing care are not eligible.
Services
Residential care apartment complex. Facilities must provide or contract for services that are sufficient and qualified to meet the care needs identified in the tenant service agreement. The minimum service package includes supportive services (meals, housekeeping, laundry, arranging access to medical services, and transportation to medical services); personal services (daily assistance with ADLs); and nursing services (health monitoring, medication administration, and medication monitoring). Services above these minimums may be provided so long as the total amount of care does not exceed 28 hours per week.
A comprehensive assessment must be done and used as the basis of a service plan and risk agreement. The assessment covers: physical health; functional limitations and capacities; medication and the ability to self-administer; nutritional status and needs; mental and emotional health; behavior patterns; social and leisure needs and preferences; strengths, abilities, and capacity for self-care; situations or conditions which could put the tenant at risk; and the type, amount, and timing of services desired by the tenant.
The legislation and regulations limit the amount of supportive, personal, and nursing services that may be provided to no more than 28 hours a week. The threshold was devised to prevent facilities from discharging residents prematurely. The threshold was developed based on an analysis of the amount of care required by participants in the State's Community Options Program (Medicaid Waiver) and the Community Integration Program, and reflects a higher level of care than the average community client. RCACs must have the capacity to provide up to 28 hours of service a week as indicated by the resident assessment.
The hours of service include staff time attributable to providing or arranging supportive, personal, and nursing services including nursing assessment, documentation, and consultation and standby assistance. Services that are not counted toward the 28 hour limit are meals, laundry, social, and recreational activities. Residents have the right to contract for or arrange for additional services outside the service agreement.
RCACs must also establish a signed, negotiated risk agreement that identifies situations that could put the resident at risk and for which the resident understands and accepts responsibility.
Community based residential facilities. Residents receive an assessment upon admission, and an individualized service plan. The service plan covers specific areas and includes the goals to be accomplished and an integrated program of individually designed activities and services necessary to achieve those goals. The plan specifies which program services will be provided to meet the resident's needs as identified by the assessment and the frequency with which each service will be provided. The plan identifies the service provider responsible for each element of care or service prescribed in the plan. Facilities provide general services, medication administration and assistance, and client group-specific services. General services include supervision, information and referral, leisure time activities, community activities, family contacts, transportation, and health monitoring. Client group-specific services include personal care, independent living skills, communication skills, socialization, activity programming for persons with dementia, transitional services, and nursing care (up to three hours a week).
Negotiated Risk Agreements
Residential care apartment complex. RCACs must sign risk agreements with tenants that identify situations or conditions which should be known that involve a course of action taken or desired by the tenant that is contrary to the facility’ policy and could put the tenant at risk. The agreement describes the tenant’s preference for handing the situation and potential consequences. It also describes what the RCAC will and will not do to meet the tenant’s needs, alternatives offered to reduce or mitigate risk and the agreed course of action. The agreement does not mitigate or waive any tenant rights.
Community based residential facilities. No provisions.
Dietary
Community based residential facilities. Facilities must provide at least three nutritious meals a day and a nutritious snack that meet the recommended daily allowances in the USDA Food Guide Pyramid. Special or modified diets may be provided if ordered by a physician or a dietician. A physician must be consulted if the resident is not eating enough to maintain nutritional balance.
Residential care apartment complex. Facilities must have the capacity to provide meals. Qualified staff must be available to provide services, including meals. Meals and snacks shall be prepared, stored, and served in a safe and sanitary manner.
Agreements
Community based residential facilities. The resident agreement must be provided prior to move-in or within five days of an emergency admission. A copy of the resident’s rights and house rules must be provided prior to and upon move-in. The agreement covers the services provided; the basic daily or monthly rate; the source of payment and the time of the payment; the amount of the security deposit, if any; the entrance fee, if any; any bed hold fee; conditions for discharge or transfer; and refund policy.
Residential care apartment complex. Facilities must provide to prospective residents a schedule of fees for services that separately identify charges for rent, meals, and services; application fees, entrance fee, or deposits; and the refund policy. A service agreement is signed that includes the type, amount, and frequency of services to be provided, any additional services available for purchase, and the activities and social connection the tenant will be assisted in maintaining. Charges are also included, individually and total, as is the procedure for notifying residents of any fee increases that may occur. Supplemental fees for services not covered in the agreement must be specified.
Provisions for Serving People with Dementia
An Alzheimer’s/Dementia Special Care Unit is any licensed facility serving people with dementia that provides specialized services, 24-hours per day, in a specialized unit, for residents with a diagnosis of Alzheimer’s disease or related dementia; and that advertises, markets or otherwise promotes the facility as providing a specialized unit. These facilities must complete a disclosure form.
Residential care apartment complex. Staff must have appropriate training based on the physical, functional, and psychological characteristics of the population served.
Community based residential facilities. Residents with dementia are specified as a client group. Facilities serving people with dementia must prepare a full description of the special needs of the residents to be served and the care and services to be offered. Structured activities must be provided that reflect resident capabilities and are meant to involve residents and may include: household tasks they were doing prior to admission, activities involving past memories, repetitive and simple tasks, non-verbal creative tasks, physical activity, sensory activity, and music therapy.
Medication Administration
Residential care apartment complex. Facilities can offer medication administration and medication management (storage; preparation or organization or reminder system; assessment of effectiveness of medications; monitoring of side effects, negative reactions and drug interactions; and delegation and supervision of medication administration). Medications can be administered by a registered nurse or delegated.
Community based residential facilities. A registered nurse must supervise the administration of medications unless the medication is packaged in unit doses. Aides who have passed required training may administer medications. Injections may be administered by a registered nurse, or for people with stable medical conditions, by an LPN, or they may be delegated to a staff member and supervised by a registered nurse.
Public Financing
Residential care apartment complex (RCAC). Services are covered for Medicaid beneficiaries who meet the nursing home level of care criteria through the Medicaid Community Options Program Waiver (COP-W), the Community Integration Program II (CIP II), the Wisconsin Partnership Program and the Family Care Demonstration program. CIP II funding is only available when nursing home beds are closed and funding is transferred to provide community care to replace the closed capacity. The state-funded Community Options Program (COP) is not available to residential care apartment complex residents. Medicaid state plan personal care services are covered for beneficiaries in RCACs and CBRFs with 20 or fewer beds.
Medicaid reimbursement is limited to 85 percent of the average statewide Medicaid nursing home rate excluding room and board. Rates are negotiated between facilities and the county. The maximum spending for the resident’s total service plan is $77.81 per day. (An adjustment based on average nursing facility payments is made each year in July). This payment includes assisted living services provided by the facility and other waiver costs such as county care management, transportation, and therapies not covered by the Medicaid state plan. Despite the high maximum service payment, counties must ensure that the average cost for all waiver participants (all settings) does not exceed $41.86 per day. For every RCAC resident, counties must make sure there are sufficient participants in other settings who receive a lower cost service plan in order to bring down the average. Room and board costs are not included in this ceiling.
The state agency allows income supplementation by families to cover room and board, a private room, or for service enhancements that are not covered by the Medicaid payment. However, each county can set its own policy on family supplementation.
Persons eligible for the Medicaid waiver program under the 300 percent of SSI rule are allowed to keep a maintenance allowance of $744 a month, which can be used to pay for room and board. Counties may only contract with certified RCACs. In 2002, 125 of the RCACs, with a capacity of 4,452 units, contracted with Medicaid and served about 132 waiver participants.
Community Based Residential Facilities. CBRFs have access to the state funded COP program, COP-W, and CIP II funds. They also can access waiver programs for persons with mental retardation or other developmental disabilities and for individuals with traumatic brain injuries. There is no cap on the service payment in CBRFs. The COP program, which can also be used to supplement the resident’s room and board payment, may contract with facilities up to 20 beds. Waiver programs used to be limited to smaller facilities (20 or fewer beds) but COP-W (elderly and physical disabilities waiver) may now serve people in larger facilities if they demonstrate that the facility is non-institutional in character, and receives approval from the Bureau of Aging and Long Term Care Resources. Medicaid and state programs served 3,812 people in CBRFs in calendar 2002. The table below compares public funding participation by setting.
| 2004* | 2002 | 2000 | ||||
|---|---|---|---|---|---|---|
| Facilities | Participants | Facilities | Participants | Facilities | Participants | |
| RCAC | NA | 144 | 125 | 132 | 45 | 31 |
| CBRF | NA | 3,812 | NA | 2,473 | NA | 987 |
| * The information was reported by the Department of Health and Family Services report to the Legislature on the Community Options Program Calendar Year 2002 | ||||||
Staffing
Residential care apartment complex. The number, assignment, and responsibilities of all staff shall be adequate to provide all services identified in the tenants’ service agreements including assisting tenants with unscheduled care needs.
Community Based Residential Facilities. The staff ratio must be adequate to meet the needs of residents. At least one qualified staff must be in the facility when one or more residents are in the facility. At least one qualified staff must be on duty and awake if one resident needs continuous care. Class C facilities (21 or more) must have one staff on duty and awake at night for every 20 residents.
Training
Residential care apartment complex administrators. Each RCAC must have a service manager responsible for the day-to-day operation of the facility, including ensuring that the services provided are sufficient to meet tenant needs and are provided by qualified persons; that staff are appropriately trained and supervised; that facility policies and procedures are followed; and that the health, safety, and autonomy of the tenants are protected. The service manager shall be capable of managing a multi-disciplinary staff to provide services specified in the service agreements.
Community based residential facilities administrators must be 21 years old, have a high school diploma or GED, and have administrative experience or one post high school course in business management and one year of experience or a post high school course related to the needs of the client group.
Residential care apartment complex staff. Services shall be provided by staff who are trained in the services that they provide and are capable of doing their assigned work. Personal and supportive services shall be provided by staff who have documented training or experience in needs and techniques for assistance with tenant care and activities of daily living such as bathing, grooming, skin care, transfer, ambulation, exercise, meal preparation and eating assistance, dressing, and use of adaptive aids and equipment. All facility staff shall have training in safety procedures, including fire safety, first aid, universal precautions, the facility’s emergency plan, and facility policies and procedures relating to tenants’ rights. Staff providing assisted living services must have documented training in the following areas:
- Physical, functional, and psychological characteristics associated with aging or likely to be present in the tenant population, and their implications for service needs;
- The purpose and philosophy of assisted living, including respect for tenant privacy, autonomy, and independence; and
- Assigned duties and responsibilities, including the needs and abilities of individual tenants.
Community based residential facilities. Administrators and staff must have 45 hours of initial training covering: resident rights; recognizing and responding to challenging behaviors; client group-specific training; needs assessment of prospective residents and individualized service plans; universal precautions; and fire safety, first aid, and procedures to alleviate choking.
Administrators and appropriate staff must receive three hours of training in dietary needs, menu planning, food preparation, and sanitation. The administrator and appropriate staff must receive eight hours training in management and administration of medications. Exemptions from training are allowed for employees with specified licenses or credentials.
Administrators and staff must receive 12 hours of continuing education that is relevant to their job responsibilities beginning the second year of employment.
Background Check
Residential care apartment complex. Facilities must conduct a criminal record check with the Wisconsin Department of Justice, and with the registry for nurses aides, home health aides, and hospice aides for managers, service providers, and others.
Community based residential care facilities. Same.
Monitoring
Residential care apartment complex. The Department conducts periodic inspections of certified RCACs, and has the authority, but is not required, to inspect registered RCACS to determine compliance with regulatory requirements.
Fees
Annual fees for certified RCACs are $350 plus $6 for each apartment. Registered RCACs do not pay a fee. CBRFs pay a biennial fee of $306 plus $39.60 per bed.
| Facility type | Funding Sources |
|---|---|
| Community based residential facility | Private income/assets, including Social Security, SSI, and insurance. COP: 8 or fewer beds; with variance 9 to 20 beds. Only in 21+ beds if facility is a certified independent apartment or was licensed prior to 7/29/95 and has a variance. COP-W, CIP II: 8 or fewer beds and in certified independent apartment in any size and state plan services provided by a home health or personal care agency in facilities under 20 beds. CIP 1A/1B; BIW: when variance granted and facility has 8 or fewer beds. County funds/community aids. |
| Residential care apartment complex | Private income/assets, including Social Security, SSI, and insurance. COP-Waiver, CIP-II, and state plan services provided by a home health or personal care agency. County funds (not including community aids). |
Wyoming
Citation
CitationAssisted living licensure, Chapter 4
Assisted living program administration, Chapter 12
General Approach and Recent Developments
Rules for assisted living facilities were revised in June 2001. A Medicaid waiver was implemented in 2001.
The rules for program administration outline a philosophy for assisted living which references the desire of the State to develop reasonable and enforceable rules for the placement of individuals with disabilities in community settings such as assisted living facilities in lieu of unnecessary institutionalization.
| Category | 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|---|
| Facilities | Units | Facilities | Units | Facilities | Units | |
| Boarding homes | 17 | 315 | NR | NR | 26 | 419 |
| Assisted living facilities | 15 | 970 | 14 | 1,005 | 13 | 960 |
Definition
Assisted living means “a non-institutional dwelling operated by a person, firm or corporation engaged in providing limited nursing care, personal care and boarding home care, but not habilitative care, for persons not related to the owner of the facility.”
Boarding home care means “a non-institutional dwelling or rooming house operated by any person, firm or corporation engaged in the business of operating a home for the purpose of letting rooms for rent and providing meals and personal daily living care, but not habilitative or nursing care, for persons not related to the owner.”
Unit Requirements
Rooms must provide 120 square feet for single-bed rooms and 80 square feet per bed in multiple-bed rooms, exclusive of toilets, closets, wardrobes, alcoves, and vestibules, in both cases. No more than two people may share a bedroom. One flush toilet, lavatory and mirror is required for every two residents. One tub and shower is required for every ten residents. One-half of licensed beds must be private rooms.
Admission/Retention Policy
The regulations allow residents who need limited nursing services to be served. Residents who need continuous assistance with transfer and mobility, are unable to feed themselves, need total assistance with bathing and dressing, require catheter care, continuous oxygen and monitoring, wander excessively, need wound care requiring sterile dressings, have Stage II skin care and beyond, exhibit inappropriate social behavior, and demonstrate chemical abuse that puts residents at risk cannot be cared for by assisted living facility staff members.
Nursing Home Admission Policy
Individuals scoring 13 or more points on ten assessment items are eligible. Those items include eating, meal preparation, diet; medication management; skin care and dressing treatment; speech, vision and hearing; dressing and personal grooming; bathing; continence; mobility; behavior/motivation; and socialization. Nursing home placement is allowed for individuals who need care but for whom services are not available, who lack a support system, are intermittently confused and/or agitated and need a structured environment, who wander extensively; or who have total confusion or apathy.
Services
Assisted living facility core services include meals, housekeeping, personal and other laundry services; a safe and clean environment; assistance with transportation; assistance with obtaining medical, dental, and optometric care, and social services; assistance in adjusting to group living activities; maintenance of a personal fund account, if requested by the resident or resident’s responsible party, showing any and all deposits, withdrawals, and transactions of the account; provision of appropriate recreational activities in/out of the assisted living facility; partial assistance with personal care, e.g., bathing, shampoos; limited assistance with dressing; minor non-sterile dressing changes; stage I skin care--skin integrity intact; infrequent assistance with mobility (the resident may use an assistive device; e.g., wheelchair, walker, cane); cuing guidance with ADLs for the visually impaired resident, or the intermittently confused and/or agitated resident requiring occasional reminders to time, place and person; care of the resident who can independently manage his own catheter or ostomy, e.g., resident who can change his own catheter bags, able to clean and care for his ostomy; care of the resident incontinent of bowel or bladder if he/she can manage his condition independently; registered nurse assessments; registered nurse medication review every two (2) months or sixty-two (62) days or whenever new medication is prescribed or the resident’s medication is changed; twenty-four (24) hour monitoring of each resident; and provision of mechanically altered diets and dietary supplements; e.g., Ensure allowed, if they are required by the individual resident.
An activities program must be available to all residents and must be designed to enhance each resident’s sense of physical, psychosocial, and spiritual well-being.
Services that may not be provided in assisted living include continuous assistance with transfer and mobility; care for residents who cannot feed themselves independently; total assistance with bathing or dressing; provision of catheter or ostomy care; care of residents who are on continuous oxygen if monitoring is required; care of residents whose wandering jeopardizes the health and safety of residents or residents who exhibit inappropriate social behavior such as frequent aggression, abuse, or disruptive behavior; care of residents demonstrating chemical abuse that places himself or others at risk; or care for residents needing Stage II skin care and beyond; wound care requiring sterile dressing changes; therapeutic diets that are highly restrictive, e.g., renal diets, and incontinence care. However, care beyond what the facility provides may be delivered by an outside agency.
Assessments using the required Long Term Care 102 Form must be completed by RNs no earlier than one week prior to admission and, at a minimum, annually or upon a significant change in condition. The results of the assessment are used to develop, review, and revise the resident’s individualized assistance plan. The assistance plan must include who will provide the care/services; what care/services will be provided; when care/services will be provided; how the care/services will be provided; and the expected outcome. The resident must be included in the development of the assistance plan to the best of his or her abilities, and a relative or other interested party may participate. The plan must reflect assessed needs and resident decisions (including resident’s level of involvement); support principles of dignity, privacy, choice, individuality, independence, and home-like environment and must include significant others who participate in the delivery of services.
Dietary
A minimum of three balanced, palatable, properly prepared, and attractively served meals must be offered that meet the recommended dietary allowances. Special diets may be ordered by a physician or a registered dietician.
Agreements
An assistance plan is required that specifies the type, frequency, and duration of services and the expected outcome. A resident agreement is not required. Management is responsible for developing policies and procedures that are available to residents and staff dealing with resident rights, disciplinary procedures concerning substantiated cases of resident abuse, admission/transfer/bed holds, medication management, emergency care, fire/disaster plans, departure and return, smoking, visiting hours, activities, notification of changes in conditions, personnel policies, grievance procedure, per diem rate/charges/fees and what’s included, incident reports, notification of changes in fees, outside contractual responsibilities, and identification of changes in the resident’s condition.
Residents may not be asked to leave without fourteen days written notice, unless the resident poses an imminent danger to self and/or others. Residents may be asked to leave only for the following reasons: the facility has had its license revoked, not renewed, or voluntarily surrendered; the resident’s level of care exceeds the level of care that can be provided by an assisted living facility; the facility cannot meet the resident’s needs; the resident or responsible person has a documented established pattern, in the facility, of not abiding by agreements necessary for assisted living; non-payment of charges; or the resident engages in behavior which poses an imminent danger to self and/or to others.
Provisions for Serving People with Dementia
Facilities are required to provide cuing with guidance for people who are intermittently confused and/or agitated and who require occasional reminders to time, place, and person. Facilities cannot care for residents who wander to the point that it jeopardizes the health and safety of the resident.
Medication Administration
Registered nurses provide medication reviews every two months or whenever new medications are ordered. A registered nurse is responsible for the supervision and management of all medication administration as required by the Wyoming Nurse Practice Act, and the Wyoming Board of Nursing Rules and Regulations.
Medications may be administered by a registered nurse or LPN. The regulations allow assistance with self-administration by nurse aides which includes but is not limited to reminders, removing medication from containers, assistance with removing caps, and observation of the resident taking the medication. Residents capable of self-administration are allowed to keep prescription medications in their rooms, as long as it is deemed safe and appropriate by the registered nurse. For residents who share a room and self-medicate, an assessment will be made of each resident and his or her ability to safely have medications in the room. If safety is a factor, the medications must be kept in a locked container.
Public Financing
Since July 2001, Medicaid HCBS waiver coverage is available for individuals residing in assisted living facilities when the resident requires a service that can be provided by both the long term care and the home and community based services waiver provider and the assisted living facility, but the resident cannot afford to pay the assisted living facility for the service. The waiver case manager will ensure that the required service is provided.
Ten facilities currently participate in the Medicaid waiver program serving 100 participants. The law authorizing the waiver caps the number of people who can be served at 100. There is currently a 6 month waiting list. A three tiered rate system reimburses providers $32 to $40 per day. The payment level is based on a score derived from the Long Term Care 101 form, the required screening tool as defined by the Program Division and performed by a registered nurse. Room and board is not capped and is negotiated between the resident and the facility.
| 2004 | 2002 | 2000 | |||
|---|---|---|---|---|---|
| Facilities | Participants | Facilities | Participants | Facilities | Participants |
| 10 | 100 | 7 | 40 | NA | NA |
| Level | Payment |
|---|---|
| Level I -- 13-14 points | $32 |
| Level II -- 15-16 points | $36 |
| Level III -- 17+ points | $40 |
Staffing
Staff shall be sufficient to meet the needs of residents. There must be at least one RN, LPN, or CNA on duty every shift. At least one awake staff is required for all facilities serving eight or more residents.
Training
Administrators. Managers must meet one or more of the following requirements: complete at least 48 semester hours or 72 quarter hours of post- secondary education in health care, elderly care, health case management, facility management or related field; be a certified nursing assistant; have at least two years experience working with elderly or disabled individuals; or demonstrate knowledge, skills, and abilities in the administration of a facility. The rules outline the expectations for knowledge and experience.
Staff. Management shall provide to new employees an orientation, education regarding resident rights, evacuation and emergency procedures, and training and competent supervision designed to improve resident care.
Background Check
Central registry checks are required.
Monitoring
Facilities are surveyed no less than annually. The State has a contracted employee who performs monitoring of facilities. The contract is paid by the assisted living facilities. The survey division must provide a list of deficiencies to the facility within 10 working days of the survey. The facility has 10 calendar days to provide a plan of correction for each of the cited deficiencies. If the facility fails to provide a plan of correction, licensure revocation proceedings may ensue. Each facility must have an active quality improvement program that is re-evaluated at least annually to ensure effective utilization and delivery of services. The program must have a written description, problem areas identified, monitor identification, frequency of monitoring, a provision requiring the facility to complete annually a self-assessment survey of compliance with regulations, and a satisfaction survey must be provided to the resident, resident’s family, or resident’s responsible party at least annually. The State is responsible for receiving and investigating complaints.
Fees
- 1 to 50 beds ($100 per facility);
- 51 to 100 beds ($200 per facility);
- 101 to 150 beds ($300 per facility);
- 151 to 200 beds ($400 per facility); and
- More than 200 beds ($500 per facility).