
ADVISORY COUNCIL ON ALZHEIMER'S RESEARCH, CARE, AND SERVICES
Monday, May 3, 2021
Printer Friendly Version in PDF Format (12 PDF pages)
Improving Timely Diagnosis of Dementia in Diverse Communities: Barriers and Facilitators in Primary Care
Nicole R. Fowler, PhD, MHSA
Associate Professor, Indiana University School of Medicine
Associate Director, Indiana University Center for Aging Research
Scientist, Center for Health Innovation and Implementation Science
Conflict of Interest
- I have no potential conflicts of interest
Funding Sources
- Agency for Health Research and Quality
- K12HS019461
- National Institute on Aging
- R01AG029884;
- R01AG040220;
- R01AG056325
- Cited work
- AHRQ:R01 HS019818
- CMMI:1C1CMS331000
Primary Care
- 40-50% of dementia is unrecognized
- Impact of unrecognized or delayed dementia identification
- Higher rates of hospitalization
- Longer length of inpatient stays
- Lower quality of co-morbidity management
- Increase in unsafe activities
- Low likelihood of receiving dementia care for patient and family
- Higher career stress, burden, and isolation
Research on Early Detection
- 50% agree to dementia detection research enrollment
- 80-90% accept screening for dementia
- 7-13% screen positive
- 33-52% accept diagnostic evaluation following positive screen
- 50% are diagnosed with Dementia
- 30% are diagnosed with MCI
Who Screens Positive for Dementia in Primary Care?
- Individuals aged > 80: OR 2.5; P < 0.05
- Individuals with less than high school education: OR 3.6; P < 0.05
- Individuals with self-reported forgetfulness: OR 4.7; P < 0.05
- Screening at urban vs. suburban and rural setting: OR 2.4; P < 0.1
- Patients screened face-to-face vs. phone: OR 2.2; P < 0.1
Momentum for Early Detection
- Rapidly growing population
- Pharmacological treatments
- Evidence of suffering
- Potential to improve the journey
National Alzheimer's Project Act (NAPA)
- GOAL 1: Prevent and Effectively Treat Alzheimer's Disease and Related Dementias by 2025
- Strategy 1.C. Accelerate Efforts to Identify Early and Presymptomatic Stages of Alzheimer's Disease and Related Dementias
U.S. Preventive Services Task Force
- 1996, 2003, 2013, and 2020
- Evidence is insufficient to recommend routine screening in Primary Care
Proponents of early detection
- Identify reversible causes
- Reduce cognitive burden
- Initiate interventions
- Evaluate safety
- Validate concerns
- Planning for care
- Health promotion activities
- Target treatment
Critics of early detection
- Harms > Benefits
- Depression
- Anxiety
- Over burden health system
- Labeling
- Patients don't want to know
- No cure
Medicare Annual Wellness Visit
- Health Risk Assessment
- Health History
- Personal Risk Factor Assessment
- Other Providers and Services
- Detect Cognitive Impairment
- Vitals and Measurement
- Detect Depression and Anxiety
- Screening Schedule
- Personalized Health Advice and Referrals
Rates of Annual Wellness Visit
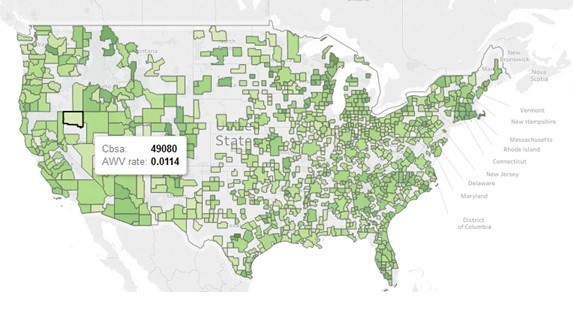 |
|
Receipt of Subsequent Cognitive Care in the Year after Index
| AWV Cohort N = 66,399 |
Control Cohort N = 66,399 |
Standard difference | |
|---|---|---|---|
| Neuropsychological testing | 0.75% | 0.55% | 0.02 |
| Imaging of the head and neck, brain, or skull | 10.68% | 11.78% | -0.04 |
| Laboratory tests (TSH, B12, Folate, Syphilis) | 7.50% | 5.11% | 0.10 |
| Diagnosis of MCI or ADRD | 6.16% | 6.86% | -0.03 |
| Initiation of any medication indicative of ADRD | 1.00% | 1.08% | -0.01 |
CHOICE Trial
- Three site, two-arm RCT
- Primary Care patients >65yo w/o dementia
- Outcomes
- Health-related quality of life
- Depression and Anxiety
- Health care utilization
- Advance care planning
- Fowler, N. R., Harrawood, A., Frame, A., Perkins, A. J., Gao, S., Callahan, C. M., Sachs, G. A., French, D. D., & Boustani, M. A. (2014). The Indiana University Cognitive Health Outcomes Investigation of the Comparative Effectiveness of dementia screening (CHOICE) study: Study protocol for a randomized controlled trial. Trials, 15(1), [209]. https://doi.org/10.1186/1745-6215-15-209
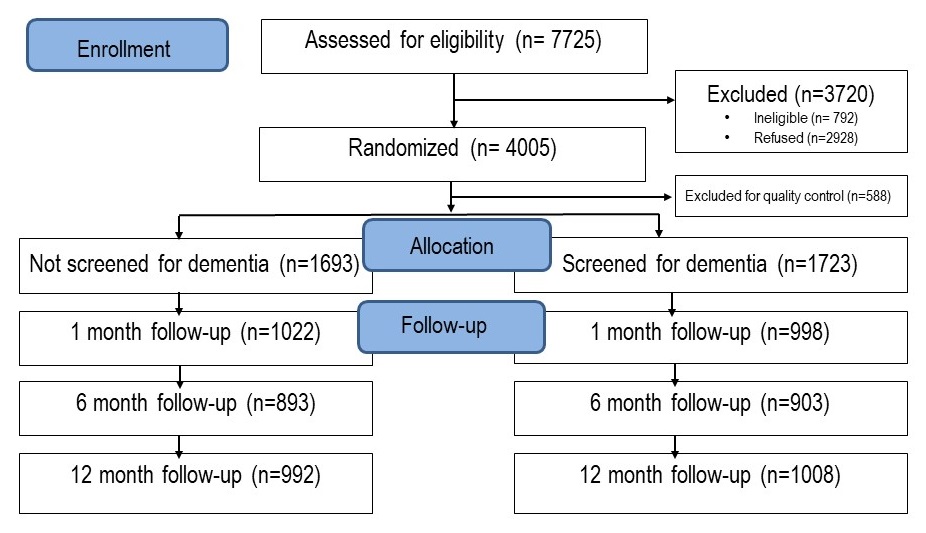 |
Characteristics of Study Patients
| Screen N = 1723 |
No Screen N = 1693 |
|
|---|---|---|
| Age, mean ± SD | 74.2±7.0 | 74.1±6.5 |
| White, n (%) | 1164 (67.6%) | 1137 (67.2%) |
| Female, n (%) | 1167 (67.7%) | 1089 (64.3.%) |
| Education level, n (%) | ||
| Less than high school | 363 (21.2%) | 357 (21.2%) |
| High school | 571 (33.4%) | 556 (33.1%) |
| Some college or college degree | 778 (45.4%) | 769 (45.7%) |
| Charlson Comorbidity Index, mean ± SD | 2.7±2.8 | 2.8±3.0 |
| Screened positive on MIS-T or Mini-Cog, n (%) | 87 (5%) | NA |
Results
- No Evidence of Harm
- No Evidence of Benefit
- No difference in health care utilization or ACP
- Lower than anticipated +
- Higher than anticipated refusal for follow-up
To test the impact of dementia screening on dyads (older adult + family member)
- Quality of life, depression, anxiety
- Caregiver preparedness, caregiving self efficacy
- Patient and family member reported cognition and PCP actions at 24 months
- Notification of - and + screening to patient, family member and PCP
- Multiple options for diagnostic follow-up
- Nicole R. Fowler, Katharine J. Head, Anthony J. Perkins, Sujuan Gao, Christopher M. Callahan, Tamilyn Bakas, Shelley D. Suarez, Malaz A. Boustani (2020). Examining the benefits and harms of Alzheimer's disease screening for family members of older adults: study protocol for a randomized controlled trial. Trials, 21(1), [202]. doi: 10.1186/s13063-019-4029-5
Relationship between Perceptions and Screening Acceptance
| Odds Ratio | P Value | |
|---|---|---|
| Perceive a Benefit of Knowing Early | 0.80 to 0.85 | 0.01 |
| Has a relative with Alzheimer’s disease | 0.43 to 0.51 | 0.014 |
| Age, years | ||
| 65-69 | [Reference] | |
| 70-74 | 1.71 to 5.65 | <0.001 |
| 75-79 | 1.02 to 3.63 | 0.01 |
| >80 | 0.9 to 2.44 | 0.13 |
|
||
48% to 67% who screen positive refuse further diagnostic work-up for dementia
- Those who live alone are less likely to seek treatment after a positive screen for dementia
- Live alone: OR 7.28; P < 0.01
- Pass temporal orientation (year, date, and day of the week): OR 1.37; P = 0.001
- Refuse screening for other conditions (colon, depression): OR 1.75; P < 0.01
- Concern of dementia-related stigma: OR 1.43; P < 0.05
- Race-Age interaction:
- African-American > 80 yrs: OR 3.1, P < 0.001
- White-American > 80 yrs: OR = 0.9, P = 0.728
- Patients may not place value on tests that seem unrelated to cognitive functioning
Summary
- Early detection of ADRD and disclosure of the diagnosis are critical to optimal care for older adults and their family members.
- Reduce public stigma of ADRD in communities.
- Raise awareness of the benefits and increase access to evidence-based programs that reduce burden and improve outcomes that matter to patients and families.
Thanks you
Relevant Published References from our Group:
- Fowler NR, Head K, Perkins AJ, Gao S, Callahan CM, Bakas T, Suarez SD, Boustani MA. Examining the benefits and harms of Alzheimer's disease screening for family members of older adults: study protocol for a randomized controlled trial. Trials 21, 202 (2020). https://doi.org/10.1186/s13063-019-4029-5
- Harrawood A, Fowler NR, Perkins AJ, LaMantia MA, Boustani MA. Acceptability and results of dementia screening among older adults in the United States. Curr Alzheimer Res. 2018;15(1):51-55 doi: 10.2174/1567205014666170908100905.
- Fowler NR, Perkins AJ, Gao S, Sachs GA, Uebelhor AK, Boustani MA. Patient characteristics associated with screening positive for Alzheimer's disease and related dementia. Clin Interv Aging. 2018;13:1779-85 doi: 10.2147/cia.S164957.
- Fowler NR, Perkins AJ, Turchan HA, Fram A, Monahan P, Gao S, Boustani MA. Older primary care patients' attitudes and willingness to screen for dementia. Journal of aging research 2015;2015:423265 doi: 10.1155/2015/423265.
- Fowler NR, Frame A, Perkins AJ, Gao S, Watson DP, Monahan P, Boustani MA. Traits of patients who screen positive for dementia and refuse diagnostic assessment. Alzheimers Dement. 2015;1(2):236-41 doi: 10.1016/j.dadm.2015.01.002.
- Fowler NR, Harrawood A, Frame A, Perkins AJ, Gao S, Callahan CM, Sachs GA, French DD, Boustani MA.The Indiana University Cognitive Health Outcomes Investigation of the Comparative Effectiveness of dementia screening (CHOICE) study: study protocol for a randomized controlled trial. Trials. 2014;15:209 doi: 10.1186/1745-6215-15-209.
- Callahan CM, Sachs GA, Lamantia MA, Unroe KT, Arling G, Boustani MA. Redesigning systems of care for older adults with Alzheimer's disease. Health Affairs (Millwood). 2014;33(4):626-32 doi: 10.1377/hlthaff.2013.1260.
- Cordell CB, Borson S, Boustani M, et al. Alzheimer's Association recommendations for operationalizing the detection of cognitive impairment during the medicare annual wellness visit in a primary care setting. Alzheimers Dement. 2013;9(2):141-50 doi: 10.1016/j.jalz.2012.09.011.
- Fowler NR, Boustani MA, Frame A, et al. Effect of patient perceptions on dementia screening in primary care. J Am Geriatr Soc. 2012;60(6):1037-43 doi: 10.1111/j.1532-5415.2012.03991.x.
- Holsinger T, Boustani M, Abbot D, Williams JW. Acceptability of dementia screening in primary care patients. Int J Geriatri Psychiatry2011;26(4):373-9 doi: 10.1002/gps.2536.
- Boustani MA, Justiss MD, Frame A, et al. Caregiver and noncaregiver attitudes toward dementia screening. J Am Geriatr Soc. 2011;59(4):681-6 doi: 10.1111/j.1532-5415.2011.03327.x.
- Boustani M, Baker MS, Campbell N, et al. Impact and recognition of cognitive impairment among hospitalized elders. J Hosp Med. 2010;5(2):69-75 doi: 10.1002/jhm.589.
- Justiss MD, Boustani M, Fox C, et al. Patients' attitudes of dementia screening across the Atlantic. Int J Geriatri Psychiatry2009;24(6):632-7 doi: 10.1002/gps.2173.
- Callahan CM, Boustani M, Sachs GA, Hendrie HC. Integrating care for older adults with cognitive impairment. Curr Alzheimer Res. 2009;6(4):368-74
- Boustani M, Perkins AJ, Monahan P, et al. Measuring primary care patients' attitudes about dementia screening. Int J Geriatri Psychiatry2008;23(8):812-20 doi: 10.1002/gps.1983.
- Brayne C, Fox C, Boustani M. Dementia screening in primary care: is it time? JAMA. 2007;298(20):2409-11 doi: 10.1001/jama.298.20.2409.
- Boustani M, Perkins AJ, Fox C, et al. Who refuses the diagnostic assessment for dementia in primary care? Int J Geriatri Psychiatry2006;21(6):556-63 doi: 10.1002/gps.1524.
- Boustani M, Callahan CM, Unverzagt FW, et al. Implementing a screening and diagnosis program for dementia in primary care. JGIM. 2005;20(7):572-7 doi: 10.1111/j.1525-1497.2005.0126.x.
- Boustani M, Watson L, Fultz B, Perkins AJ, Druckenbrod R. Acceptance of dementia screening in continuous care retirement communities: a mailed survey. Int J Geriatri Psychiatry2003;18(9):780-6 doi: 10.1002/gps.918.
- Boustani M, Peterson B, Hanson L, Harris R, Lohr KN. Screening for dementia in primary care: a summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2003;138(11):927-37.
Files
Document
mtg40-slides5.pdf (pdf, 1.44 MB)