
By Kerry Kemp,
Health Systems Research, Inc.
Summary Overview
On August 8th and 9th, 2000, the Office of the Assistant Secretary for Planning and Evaluation (ASPE), U.S. Department of Health and Human Services (DHHS), sponsored a conference at the request of the White House to clarify what is known about pricing practices within the pharmaceutical industry and the distribution chain.
ASPE's hope was that the 2-day conference would (1) clarify what is known about prescription drug pricing, utilization, and costs; (2) bring together a wide range of people to share information, insights, and perspectives strategies for realizing the benefits of prescription drugs while controlling the growth in expenditures; and (3) identify questions that are critical to address so that policymakers can make more informed decisions regarding prescription drugs in the coming years.
The conference had four main sessions:
- What's the Problem? A Synthesis of Research on Pharmaceutical Cost Pressures and Trends;
- Pricing Practices in the Pharmaceutical Market;
- Pharmaceutical Utilization Issues; and
- Strategies for Controlling Costs and Increasing Value From Pharmaceutical Expenditures.
Each session included both formal presentations and discussion by a diverse panel of about 25 people representing a wide range of stakeholders--including drug manufacturers, pharmacy benefit managers (PBMs), purchasers, health care providers, consumer advocates--as well as prescription drug researchers and general health policy analysts. The idea was to use the formal presentations as a springboard for panel members and the general audience to share their insights and perspectives.
This report summarizes the discussion at the prescription drug conference, highlights the key points raised by conference participants, and identifies unanswered questions that participants suggested be addressed as part of a research agenda in this area.
I. What's the Problem? A Synthesis of Research on Pharmaceutical Cost Pressures and Trends
The first session was an overview session highlighting research on recent trends in U.S. prescription drug expenditures and the factors and forces driving these trends. To set the context, three people gave formal presentations:
- Mark Merlis, M.A., Institute for Health Policy Solutions, reviewed four research studies on the recent double-digit growth in U.S. prescription drug expenditures and factors contributing to that growth.
- Ernst Berndt, Ph.D., Sloan School of Management, Massachusetts Institute of Technology, hypothesized that four factors, including the expansion of third-party coverage for prescription drugs and aggressive marketing efforts, have contributed to the rapid escalation in U.S. prescription drug expenditures.
- Francis Palumbo, Ph.D., J.D., Center on Drugs and Public Policy, University of Maryland, presented estimates of the number of new brand-name prescription drugs and generic prescription drugs likely to come on the market by 2004.
The session also included a Panel Discussion and a discussion of Research Questions.
1. Explaining the Growth in Prescription Drug Spending: A Review of Recent Studies--Mark Merlis, M.A.
Mr. Merlis, citing data from the U.S. Health Care Financing Administration(now known as Centers for Medicare and Medicaid Services(CMS)) (HCFA(now known as CMS)), reported that U.S. prescription drug spending grew at double the rate of total U.S. health spending between 1993 and 1998. Prescription drugs currently account for one-eighth of private insurance expenditures and one-tenth of Medicaid expenditures.
Mr. Merlis reviewed four recent studies of U.S. expenditures on prescription drugs to see whether there were any points of consensus in the studies and to explain why the studies differ in their conclusions. Three of the studies--one by Express Scripts, one by Merck-Medco, and one by Brandeis University and PCS Systems--relied on data on privately insured populations supplied by pharmacy benefit managers (PBMs). The fourth study, prepared by the Barents Group for the National Institute of Health Care Management, relied on data for the entire U.S. population.
All of the studies reviewed by Mr. Merlis suggest that the following factors account for the recent double-digit increases in U.S. prescription drug expenditures:
- A change in the mix of drugs utilized--i.e., a shift from older drugs to newer, more expensive drugs, and within the class of older drugs, a shift from less expensive drugs to more expensive ones.
- Unit price inflation--i.e., increases in the cost of a given pill over time (the price of a constant market basket of drugs has been going up about 4% per year).
- Four volume-related factors: (1) more people are getting more prescriptions; (2) those who do get prescriptions get more prescriptions a year; (3) each prescription is for a longer period on average; and (4) within each day's supply of a prescription drug, the strength and dosage are increasing.
The studies' conclusions about the relative importance of these factors differ, because studies group some of these factors together in different ways. Nonetheless, all of the studies suggest that a large portion of the prescription drug spending and spending growth in recent years is due to drugs already on the market. According to Mr. Merlis, spending increases among the privately insured populations in the Express-Scripts and Brandeis studies break down into the following components: cost increases for existing drugs, 40%; more prescriptions for existing drugs, 20%; prescriptions for new(1) drugs, 20%; higher cost of new drugs, 20%. These two studies suggest that there has been dramatic growth in the utilization of drugs in a few therapeutic categories--cardiovascular, gastrointestinal, psychotherapeutic, anti-infective, and antidiabetic medications--plus fairly uniform cost increases in every therapeutic category.
1 - "New" drugs are defined by the Brandeis Study as any drug introduced in 1995 or later, and by the Express-Scripts Study as any drug introduced in 1996 or later.
2. Factors Driving Pharmaceutical Expenditures: An Overview--Ernst Berndt, Ph.D.
Dr. Berndt said that, according to data from IMS Health, U.S. sales of prescription drugs have grown about 13% a year since 1987. Dr. Berndt hypothesized that there are four reasons behind this growth:
- The importance of being unimportant. Prescription drugs have enjoyed an era of benign neglect because they have accounted for a relatively small proportion of U.S. health expenditures in comparison with hospital care and physician fees. That share has been increasing rapidly, though, and the era of benign neglect is probably over.
- Growth in third-party insurance coverage for prescription drugs, leading to increased demand. In 1965, less than 10% of all prescription drug payments were paid by third-party insurers; by 1998, the figure had grown to 75%.
- Introduction of new pharmaceutical products. According to IMS Health, about 43% of the growth in the U.S. pharmaceutical expenditures since 1995 is due to the introduction of new products.
- Aggressive pharmaceutical technology transfer and marketing efforts. Marketing-to-sales ratios for pharmaceuticals are fairly high (10-20%), in part because pharmaceuticals are "experience goods" (i.e., goods that consumers have to try to see if they like them). In the past, pharmaceutical marketing efforts broke down as follows: detailing and sampling (75-80%), advertising in medical journals (10%), direct-to-consumer (DTC) ads (5%), and sponsorship of continuing education (10%). DTC marketing of prescription drugs, especially drugs that treat widely prevalent, non-life-threatening chronic conditions, has increased dramatically in recent years and now probably represents 10-20% of marketing efforts.
3. Projections of Drug Approvals, Patent Expirations, and Generic Entry from 2000 to 2004--Francis Palumbo, Ph.D., J.D.
According to Dr. Palumbo, 643 new prescription drugs are now in Phase II or Phase III clinical trials or are awaiting the Food and Drug Administration's (FDA) approval and potentially could enter the U.S. market by 2004. Many of these 643 products will probably not make it to the market, though, because later human trials will demonstrate lower than anticipated efficacy or unfavorable side effect profiles. Dr. Palumbo and his colleagues estimated that the patents will expire on about 45 brand-name prescription drugs each year from 2000 through 2004, potentially opening the market to generic competition. He noted, however, that brand-name drug manufacturers have several defensive strategies that they can use to block the market entry of generic products or discourage the utilization of generic products.
4. Panel Discussions: U.S. Pharmaceutical Cost Pressures and Trends
The panel discussions in this session addressed a range of different issues. Comments pertaining specifically to topics raised by the formal presenters in this session are summarized below. Additional comments by drug manufacturers, consumer representatives, health care providers, or other stakeholders or researchers on the panel are included, where appropriate, in the summaries of other conference sessions.
What Difference Does The Rapid Growth In U.S. Pharmaceutical Spending Make?
Several panel members offered their views on the question of what difference the rapid growth in U.S. expenditures on prescription drugs makes. They noted that if aggregate U.S. expenditures on prescription drugs go up 15-20% a year and nothing else changes, the fraction of people who are unable to avail themselves of the drugs will grow.
Double-digit growth in the utilization and costs of pharmaceuticals--unless that growth is perceived to have value--may lead both public and private sectors entities to cut back the health benefits they offer. Programs such as Medicaid already are struggling to pay for prescription drugs. Employers, especially small employers, are also very concerned about rising prescription drug costs and their ability to offer health insurance to their employees. Already, many elderly and uninsured people cannot afford prescription drugs. Currently, about 60 million people in the United States, or about 1 in 4 persons, have no insurance coverage for prescription drugs. One-third of Medicare beneficiaries have no prescription drug insurance, and many others have poor or unstable coverage.
Key questions facing U.S. policymakers are: How can we make drugs affordable to the people who need them? And who should pay for prescription drugs? Should pharmacy benefits be considered a privilege or an entitlement? If U.S. policymakers succeed in making drugs more affordable through a Medicare prescription drug benefit, the utilization of prescription drugs will increase--even if the drugs are used appropriately--and costs will rise accordingly. For that reason, the "billion dollar question," many panel members said, is whether society is getting adequate "value" (e.g., medical offsets or other benefits) from expenditures on prescription drugs.
Limitations of Studies Identifying Factors Contrubuting to Trends in U.S. Expenditures on Prescription Drugs
Panel members agreed that studies of factors contributing to the increases in aggregate U.S. prescription drug expenditures, such as those reviewed by Mr. Merlis, cannot answer the question of whether cost or utilization levels are appropriate. One researcher on the panel suggested that after policymakers ascertain what the trends in U.S. drug expenditures are, they should (1) decompose the factors contributing to the trends; (2) ask what forces lie behind these factors; (3) determine what difference it makes to people's health that we are seeing these trends; (4) ask what could be done to slow the growth in aggregate U.S. expenditures on prescription drugs; and (5) ask what should be done to slow aggregate spending.
Forces Contributing to Trends in U.S. Prescription Drug Expenditures
There was discussion by panel members of some of the forces contributing to increases in U.S. prescription drug expenditures.
Introduction of new prescription drugs
Much of the panel's discussion centered on the effects of new drugs on U.S. prescription drug expenditures. An important question for U.S. policymakers, some panel members said, is: How will the emergence of costly new prescription drugs affect U.S. expenditures on prescription drugs in the coming years?
A Wall Street analyst said that large molecule drugs (proteins) that have to be injected or administered intravenously and typically cost about $5,000-$15,000 per year (vs. small molecule drugs usually taken by pill, which cost $600-$900 per year) can be expected to proliferate in the market in the next 5 or 10 years. And in the next 20 years, the contribution that such drugs will make to total utilization and costs will increase dramatically.
Some panel members argued that it is important not to lose sight of how important new discoveries and new drugs are in terms of improving patients' health status. One panel member said that post-1992 drugs account for about 35% of current expenditures and 80% of the growth in expenditures--would we want to go back and shut off the valve in 1992? On the other hand, another panel member asked: What if we shut off the valve and used the savings to provide health insurance for uninsured children, elderly people, etc.? That, he said, is a choice that society is facing.
Strategies used by brand-name drug companies to encourage the utilization of brand-name rather than generic products
Several panel members suggested that brand-name prescription drug manufacturers use many strategies to encourage the utilization of brand-name rather than generic products:
- Intellectual property rights. Representatives of the generic drug industry, consumer representatives, and researchers noted that brand-name drug manufacturers often use patent rights (including trivial patents) and nonpatent forms of providing market exclusivity rights (sui generis rights, exclusivity rights, orphan drug exclusivity, pediatric drug exclusivity) to block the market entry of generics. A generic manufacturer with 52 pending generic products reported that 6-month exclusivity arrangements are blocking the market entry of at least 35 of its products. Several panel members suggested that it is important for U.S. policymakers to examine the tradeoffs in using patent extensions and exclusivity arrangements as the incentive for innovation on pediatric medications, etc., and policy makers must consider how changes in the system would affect incentives for research and development.
- Aggressive marketing of brand-name prescription drugs. Manufacturers aggressively market brand-name prescription drugs to physicians (e.g., through detailing and sampling) and are increasingly marketing them directly to consumers.
- Rebates for brand-name prescription drugs. Brand-name drug manufacturers frequently offer rebates to PBMs and other volume purchasers of prescription drugs to drive market share toward specific brand-name products.
Growth in third-party insurance coverage for prescription drugs and insured patients' insensitivity to price
Several panelists emphasized that is not simply growth in third-party coverage that has contributed to the increased utilization of prescription drugs, but also the fact that patients' sensitivity to price has been reduced by the change in patient cost-sharing arrangements from coinsurance to small copayments under managed care. People who are required to pay only a small copayment ($5 per prescription) are insensitive to the price, so the price of a prescription drug does not constrain their utilization. An important question facing U.S. policymakers, panelists noted, is: What effect will the enactment of a Medicare prescription drug benefit have on Medicare and U.S. prescription drug expenditures? Another important question is: What effect will the enactment of a Medicare prescription drug benefit have on Medicare and U.S. expenditures for health services other than prescription drugs? Additional comments about the effects of insurance coverage were made in the session on Pharmaceutical Utilization Issues (see discussion on page 16).
Fragmentation of information, financial incentives, and decisions about drugs
It was generally agreed that there is a disconnect between the parties that are responsible for making decisions about the use of prescription drugs and the information and incentives they have and the parties that are responsible for paying the bills for prescription drugs and the information and incentives they have. Physicians have information on adverse effects, safety, and efficacy, but they seldom know the costs of drugs they are prescribing or think costs should be a factor in their decisions about which drugs to prescribe. Drug manufacturers, PBMs, and some health plans have information on costs, but they lack information about which drugs are best for individual patients. In some cases, physicians who contract with a managed care organization do not feel any responsibility for the costs of prescription drugs because the drug benefit is a carveout benefit managed by a PBM. In other cases, physicians are asked by a health maintenance organization (HMO) to assume financial risk for their HMO patients' drug utilization, but the physicians have insufficient information or power to manage this risk successfully. Patients in managed care plans are insensitive to the costs of prescription drugs and generally rely on their doctors for information about which drugs are appropriate for them. There are few reliable sources of information for consumers on which prescription drugs are most appropriate for them and represent the best value for the money. All of this fragmentation needs to be reduced, so that consumers, physicians, and others making decisions about utilization have access to and are able to act upon information about the risks, benefits, and costs of pharmaceutical products.
Looking Into the Crystal Ball: What Will the Future Look Like?
What will the future look like? Panel members suggested that U.S. policymakers should consider that there will be enormous growth in the size of the U.S. elderly population in the next 10, 15, or 20 years. The introduction of yet to be discovered, probably very costly, human genomics pharmaceutical products is likely to have huge effects on patients' health, as well as on health care costs and utilization. The Internet and other technologies will transform the way people obtain information and health care products through the growth of online pharmacies virtual medicine sites that help patients manage their disease, etc. And finally, the enactment of a Medicare prescription drug benefit is likely to transform the U.S. health care system in ways that we can only begin to imagine.
5. Research Questions: U.S. Pharmaceutical Cost Pressures and Trends
Conference participants suggested that the following questions might be addressed as part of a research agenda in the area of pharmaceutical cost pressures and trends:
- What are the components of the recent double-digit growth in U.S. expenditures on prescription drugs? What policy implications flow from the finding that one factor or another--e.g., change in the mix of drugs, unit price inflation, or increased utilization of prescription--has contributed to this growth?
- What could policymakers do to slow total U.S. spending on prescription drugs? What intended and unintended effects would various strategies for slowing aggregate spending have?
- What should policymakers do to slow total U.S. spending on prescription drugs?
- What is the value of U.S. expenditures on prescription drugs from a societal perspective? In particular, how does society value these expenditures in the context of the health care system, social welfare objectives, and economic growth?
- What might be done to improve the functioning and competitiveness of the U.S. pharmaceutical market? In particular, what might be done to improve the information available to decisionmakers and align the economic incentives of various parties--Federal Government agencies, drug manufacturers, physicians, patients, PBMs, health plans--to achieve the maximum safety, value, and innovation of prescription drugs?
- What effects would the establishment of a Medicare prescription drug benefit have on the utilization and costs of prescription drugs in the United States? What effects would it have on the utilization and costs of other health services?
II. Pricing Practices in the Pharmaceutical Market
The second session of the conference explored pricing practices in the brand-name pharmaceutical market, factors influencing manufacturers' pricing decisions, pricing practices across markets and purchasers, and the potential impact of price transparency on pricing practices. The session included five formal presentations:
- Jack Hoadley, Ph.D., Division of Health Financing Policy, Office of the Assistant Secretary for Planning and Evaluation (ASPE), DHHS, presented findings from an April 2000 DHHS report indicating that pharmaceutical manufacturers charge different purchasers varying prices for prescription drugs.
- Anna Cook, Ph.D., Mathematica Policy Research, Inc., explained why different purchasers pay difference prices for prescription drugs.
- Joseph DiMasi, Ph.D., Tufts Center for the Study of Drug Development, Tufts University, presented an analysis showing the impact of new drug prices in different therapeutic classes on pharmaceutical expenditures from 1995 to 1999.
- Robert Freeman, AstraZeneca Pharmaceuticals, gave his perspectives on the factors that brand-name prescription drug manufacturers consider when deciding to invest in a new product and when setting prices for new products.
- Stephen Schondelmeyer, Pharm. D., Ph.D., PRIME Institute, University of Minnesota, argued that the U.S. pharmaceutical market is not an efficient market and recommended government regulation to increase the transparency of drug prices.
The session also included a Panel Discussion and a discussion of Research Questions.
1. Prescription Drug Coverage, Spending, Utilization, and Prices: Report to the President--Jack Hoadley, Ph.D.
Dr. Hoadley highlighted findings from the April 2000 DHHS report Prescription Drug Coverage, Spending, Utilization, and Prices: Report to the President (which is available online at aspe.hhs.gov/health/reports/drugstudy). The DHHS report documents, to the extent possible, the complex arrangements by which prices for prescription drugs are determined at different levels of the pharmaceutical distribution chain: drug manufacturers, wholesalers, retailers, insurers, PBMs, pharmacies, and consumers. As illustrated in Figure 1, different purchasers pay different prices for the same brand-name prescription drug. Cash-paying customers--i.e., individuals for whom there is no third-party payment at the point of sale--pay higher prices than do Federal facilities and agencies, insurers and PBMs, and others. These customers, who include Medicare beneficiaries with poor or no prescription drug coverage, are among the people least able to afford high prescription drug prices.
Figure 1
Prices Paid by Different Purchasers for a Brand-Name Drug
(Illustrative Example with Prices Based on Composite of Several Brand-Name Drugs).
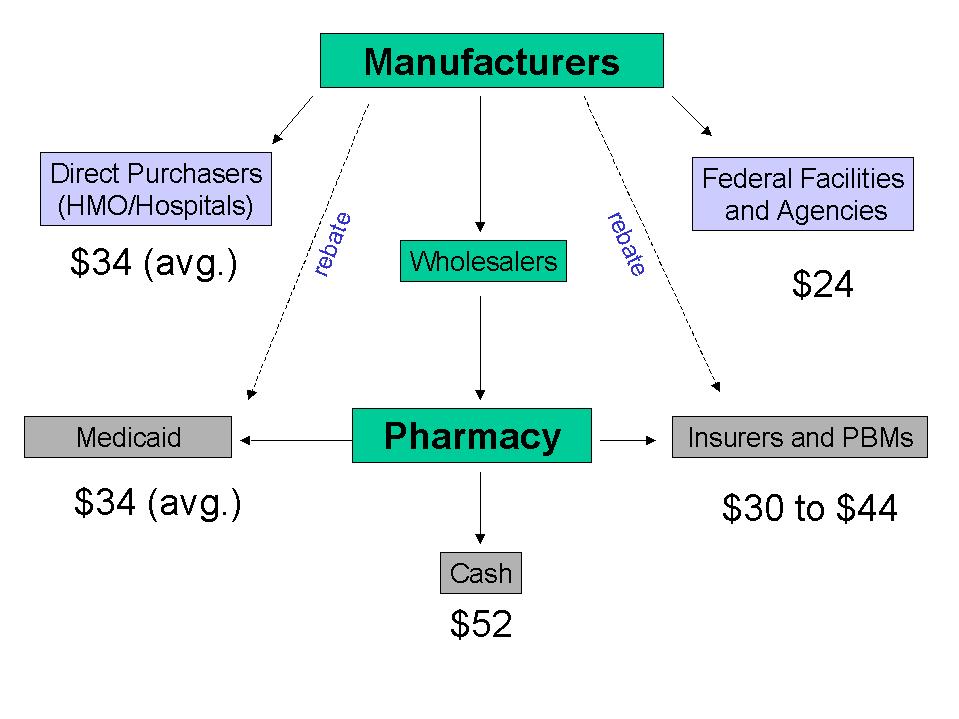
Source: Jack Hoadley, Ph.D., Office of the Assistant Secretary for Planning and Evaluation (ASPE), DHHS. Presentation to ASPE Conference on Pharmaceutical Pricing, Utilization, and Costs, Washington, DC, Aug. 8-9, 2000.
2. Why Different Purchasers Pay Different Prices for Prescription Drugs--Anna Cook, Ph.D.
Dr. Cook explained that the manufacturers of brand-name drugs charge each purchaser the highest price they can and that different purchasers have different price sensitivity.
In general, the more ability a purchaser has to drive market share toward the utilization of particular products, the more willing a brand-name drug manufacturer is to offer thatpurchaser rebates or discounts. PBMs, HMOs, and other purchasers get rebates because they can influence the utilization of drugs by applying a formulary to a broad patient base. Hospitals, clinics, and HMOs that purchase drugs directly from manufacturers get rebates because they can influence the prescribing patterns of doctors. Cash-paying customers do not have the ability to drive market share and therefore do not get rebates or discounts.
3. Price Trends for Prescription Pharmaceuticals: 1995-1999--Joseph DiMasi, Ph.D.
Dr. DiMasi presented conclusions about U.S. prescription drug pricing trends in the period 1995-1999 from an analysis he conducted as a consultant to the Drug Value Group at the Schneider Institute for Health Policy, Brandeis University:
- Prescription drug prices were related to the purchaser's price sensitivity and the drug's value (benefits and risk).
- Price trends for different therapeutic categories of prescription drugs--e.g., antiarthritics, antidepressants, antihistamines, antihyperlipidemics, antihypertensives, antiulcer drugs, and different types of antibiotics--varied over the period of the study.
- New prescription drugs varied substantially in their impact on drug expenditures over the period of the study. Some new brand-name drugs were introduced at significant discounts to existing drugs that are highly substitutable with the new drug. Entirely new classes of compounds to treat a disease or condition were often priced at a premium relative to older brand-name drugs.
- Among the factors that affected prescription drug launch prices were the drug's length of use (acute vs. chronic), convenience of use, and relative safety and efficacy. For example, patients using drugs for long periods are likely to be more price sensitive than patients using drugs for short periods, so average launch prices for drugs for acute conditions tend to be higher than drugs for chronic conditions (with some exceptions such as AIDS antivirals).
Given all the complexity in the realm of prescription drug prices, Dr. DiMasi said, it is very important to get to the issue of the proper use and true value of both new and old prescription drugs.
4. Pharmaceutical Pricing: Practices & Issues--Robert Freeman, Ph.D.
Dr. Freeman explained that brand-name prescription drug manufacturers have to develop two types of information for new brand-name products, and this requirement affects the cost of new products development and registration: (1) information needed to satisfy FDA requirements that products be safe and effective; and (2) information that can be used at launch time to market the product to key customers.
When considering how to price a new prescription drug, a brand-name drug manufacturer takes a number of factors into account. The first consideration is the new product's price and value relative to other products. Value here refers to incremental clinical and economic benefits. Different classes of customers for prescription drugs--PBMs, employers and other health plan sponsors, managed care organizations, physicians, patients, etc.--have different, and sometimes conflicting, perceptions of value.
A large determinant of what pricing strategy a drug manufacturer adopts--i.e., premium pricing, neutral pricing, or market penetration pricing--is potential customers' price sensitivity. If a product has unique value, and there is no close substitute, customers tend not to be very sensitive to price; if there are multiple products and it is easy to compare them, customers tend to be more sensitive to price. There are price differentials among pharmaceuticals in different countries, just as there are price differentials among geographic areas for virtually any goods or services.
The pharmaceutical industry is a profitable industry, and there are allegations that its pricing structure results in monopoly profits. According to Dr. Freeman, the pharmaceutical industry charges R&D capital expenditures and launch expenditures as current expenses, and this accounting practice makes the industry look very profitable. If the industry were to capitalize these expenses, its profits would be more comparable to those for other industries.
Dr. Freeman does not believe that imposing price controls at either the retail or manufacturer level is an efficient way of increasing the affordability of prescription drugs or patients' access to prescription drugs. He does, however, support improving patients' access to prescription drug coverage.
5. Role of Price Transparency in the Pharmaceutical Market--Stephen Schondelmeyer, Pharm.D., Ph.D.
Dr. Schondelmeyer said that an efficient market has four components: (1) many buyers and many sellers; (2) the existence of similar or identical substitutes; (3) complete information on product quality and price; and (4) easy market entry and transfer of resources. He believes that the U.S. market for prescription drugs lacks some of these characteristics--in particular, complete information on product quality and price.
Structural features that distinguish the U.S. pharmaceutical market from other markets include the following:
- Directed demand for pharmaceuticals. Physicians prescribe drugs for their patients.
- Differences in the economics of the pharmaceutical industry as a whole vs. individual therapeutic markets. In order to understand competition in the pharmaceutical market, it is important to look at competition in individual therapeutic classes. Nine of 12 therapeutic class markets have greater than 50% concentration, making the pharmaceutical industry a very concentrated industry.
- Insurance coverage and subsidies increasing utilization. Third-party payments account for 75-80% of all prescriptions, and people with good prescription drug coverage have few incentives to curb their prescription drug utilization. If consumers paid out of pocket for all of their prescription drugs, utilization would be much lower.
- Hidden prices, discounts, and rebates. Rebates for brand-name drugs are determined in confidential, private arrangements negotiated between manufacturers and PBMs or other purchasers, and no available data set provides information on the dollar amounts. In the April 1999 DHHS report on prescription drugs, a key limitation of the analysis was the absence of good information about rebates.
Three signals of market failure in the U.S. pharmaceutical market are the following:
- Prices are not known by decisionmakers. Physicians do not know the prices of prescription drugs or think that prices should be a factor in their prescribing decisions; patients do not know the price unless they have to pay out of pocket at pharmacy, and corporate pharmacy and therapeutics committees (which select medications for a formulary) do not know prescription drug prices net of rebates.
- Prices, discounts, and rebates are hidden in the market. Manufacturer's contracts declare that prescription drug prices and rebates are "proprietary and confidential" and cannot be disclosed to pharmacy and therapeutics committees or physicians.
- United States vs. the world ironies. The United States has the highest prescription drug prices and the greatest amount of prescription drug price inflation in the world.
Dr. Schondelmeyer advocated government regulation to increase the transparency of U.S. prescription drug prices. The goals of price transparency, he said, would be to improve economic efficiency in the prescription drug market; help get accurate price information in the market; empower buyers to better negotiate; give access to actual price information to policymakers and researchers; and make pharmaceutical firms more accountable for prices.
6. Panel Discussions: Pricing Practices in the Pharmaceutical Market
Following the formal presentations, a diverse panel of about 25 stakeholders and researchers provided their perspectives on pricing practices in the pharmaceutical market. Their comments centered around several themes as noted below.
Different Prices for Different Purchasers
One panel member argued that the focus on different prices for different purchasers is misplaced. Aggregate U.S. drug expenditures are rising at double-digit rates, while hospital costs are going up only a few percentage points a year. Although a few integrated health systems and some PBMs are better at getting prices down than others, clearly something more fundamental is going on than just steering. Another panel member commented that Figure 1 showing different prices paid by different purchasers is static, but U.S. policymakers should be concerned with what is going to happen over time.
Rebates from Brand-Name Drug Manufacturers
There was considerable discussion of drug rebates offered to PBMs and other large purchasers by brand-name drug manufacturers.
- Rebates to PBMs. A brand-name drug industry representative confirmed that a key consideration in a manufacturer's decisions to offer rebates is the purchaser's ability to drive market share toward specific brand-name products. Market share stipulations are often connected to incentives such as the inclusion by a PBM (or health plan or health plan sponsor) of a specific brand-name drug in its formulary or pharmacist and patient incentives to influence market shares of rebated products. PBM representatives on the panel explained that a PBM's ability to drive market share is a function of the willingness of the PBM's individual customers--health plans and health plans sponsors--to put into place formulary designs, copayment steerage mechanisms, etc., to drive the market toward specific brand-name products. PBMs' use of rebates and other strategies to control costs in their customers' prescription drug programs was discussed at length in the session Strategies for Controlling Costs and Increasing Value From Pharmaceutical Expenditures.
- Medicaid rebates and best price. Under the Omnibus Budget Reconciliation Act of 1990, Medicaid programs receive rebates from drug manufacturers equal to the difference between the average manufacturer price (AMP) (i.e., the average price paid by wholesalers) and the manufacturer's "best price" (i.e., lowest price the manufacturer offers to any private purchaser at any time during the year). The minimum rebate to Medicaid must be 15.1 percent of the AMP.
- Inability of retail pharmacies to negotiate rebates. A representative of a nationwide retail pharmacy chain that purchases $10 billion of pharmaceuticals a year reported that the chain has only a minimal ability to negotiate rebates with brand-name drug companies. On the other hand, the pharmacy chain is able to negotiate discounts with generic drug manufacturers.
- Inability of cash-paying customers to benefit from rebates. Many panel members expressed concern about the fact that cash-paying customers, including Medicare beneficiaries, do not benefit from drug manufacturers' rebates and pay higher prices for prescription drugs. Physicians said that some Medicare patients and uninsured patients are unable to afford the medications they need. The question that arises is: How can we deliver the same price break to uninsured people? One panel member reported that a new group of purchasers has recently been entering the prescription drug discount stream--the cash card group. This is a group of about 5 or 6 million people, many of them seniors, who have cash cards from the American Association of Retired People (AARP), Readers Digest, or other organizations. People in this group do not have prescription drug coverage, but can use their cash cards to go to pharmacies and get discounts.
Relationship Between Brand-Name Drug Manufacturers' R&D Costs and Drug Prices
Noting that manufacturers' R&D costs are typically cited as the justification for the prices of pharmaceutical products, some consumer representatives on the panel suggested that it would be helpful to have more information about what drug manufacturers spend on R&D. They noted that a Nader group study of orphan drug trials found almost no relationship between what a company spent on R&D and the prices of the drugs. Furthermore, it was reported that a transatlantic consumer group with 65 member organizations recently passed a resolution asking the European Union and the United States to move toward more transparency in drug development costs, so that better data on drug development costs will be available to consumers and others.
Profitability of the U.S. Brand-Name Pharmaceutical Industry
With regard to the pharmaceutical industry's profitability, one representative of the retail pharmacy industry commented that he understands what Mr. Freeman said re: the industry's capitalizing R&D expenses over time, but the pharmaceutical industry's after-tax profits are 20-25% vs. retail pharmacies' profits, which are about 2-3%. Even if drug manufacturers changed their accounting measures, their profits would be very high. Another panel member commented that, while manufacturer's profits should not be exorbitant, if drug manufacturers are not allowed to make profits, they will bail out of the market.
Some panel members suggested that research is needed on the relationship between reimbursement or payment levels and drug manufacturers' profitability and innovation. Specifically, research is needed to answer the following question: What effect would extending full prescription drug coverage to Medicare beneficiaries have on drug prices and ultimately the profitability and innovation of drug manufacturers--and what are the tradeoffs?
Perspectives on the "Value" of Perscription Drugs
Some panel members challenged Dr. Freeman's comment that the brand-name prescription drug industry prices its products to the value of consumers, noting, for example, that brand-name drugs are not priced to the value of an elderly person on an $8,000 income who needs three prescriptions to treat a chronic disease. A drug company representative responded that the drug industry does not sell directly to these patients. Furthermore, even if the prices were cut in half, the affordability problem for uninsured low-income people would remain. Some physicians and researchers agreed, noting that the introduction of ever-more costly drugs will only exacerbate the affordability problem for low-income patients. The fact that there are multiple, and often conflicting, perspectives on the value of prescription drug utilization and expenditures was discussed further in the session on Pharmaceutical Utilization Issues.
Problems With Coompetition in the U.S. Pharmaceutical Market
Economists on the panel agreed with Dr. Schondelmeyer's observation that in order to understand competition in the U.S. pharmaceutical market, it is important to look at the level of competition in each therapeutic class. One economist reported that the general economic literature indicates that duopolies do not do very much for competition. He suggested that the goal in the prescription drug market should be to get four or five competitors in each therapeutic class.
Several questions arose with respect to competition in the U.S. pharmaceutical industry, including:
- Why isn't there more competition within therapeutic classes when three or four or more brand-name drugs are somewhat substitutable?
- Within those pharmaceutical market segments where there is competition, why are the full benefits of competition not being realized?
Wall Street analysts on the panel reported that the generic industry remains quite competitive, even though there has been a lot of consolidation in the generic industry in the last 5-10 years. Historically, the generic industry has suffered from fratricidal competition. To encourage the development of new generic drugs that will ultimately create a more competitive marketplace, purchasers need to make sure that they operate in a way that helps keep the generic industry alive.
Another question that arose in the discussion of competition in the U.S. pharmaceutical industry was: What do we know about how the launch of generic drug products affects prescription drug utilization and costs? Some panel members, including researchers and representatives of PBMs and the generic drug industry, noted that brand-name drug manufacturers often have developed a new brand-name product with improved efficacy or reduced side effects by the time the patent on an old brand-name product expires. If patients switch to the new brand-name product, the patent expirations on their older products will not lead to as much generic competition. A representative of the generic drug industry said it would be useful to conduct research on the following question: What happens over time to a therapeutic market when there are generic product entries? Are there shifts in volume from one brand-product to another brand-product within the same therapeutic class?
Finally, one panelist asked: What do we know about how the launch of new over-the-counter (OTC) drug products affects prescription drug utilization and costs? A Wall Street analyst suggested that drug manufacturers launch an OTC version when they need to breathe new life into a product. The marketing expenses associated with the launch of OTC products are huge; and many OTC products are not profitable for several years. Some panelists noted that there is often continued use of brand-name prescription drug products even after a product comes out in an OTC form. At least for people who have prescription drug coverage with low copays, it may be cheaper to get the brand-name drug (with a low copay) than to pay out of pocket for the OTC product. Furthermore, the OTC product is typically less potent than brand-name product, so people may prefer the brand-name product. Finally, some OTC products have indications that differ from those of the prescription products (e.g., OTC form for heartburn vs. prescription form for ulcers). Some panelists said that it would be useful to conduct research on how the launch of OTC products affects prescription drug utilization and costs within therapeutic categories.
Transparency of Prescription Drug Prices
There was disagreement among panel members about Dr. Schondelmeyer's recommendation that prescription drug prices be made more transparent. Some panel members--including consumer representatives, health care purchasers, and researchers--said that it would be useful to have more transparency of prescription drug prices and drug manufacturers' R&D costs. Price disclosures could be made via any of a number of vehicles: publishing prices in the FDA Orange Book or parallel publication, publishing prices via commercial price databases, publishing prices on the Internet, disclosing actual net price on all invoices, or disclosing actual net price in all purchaser contracts. Other panel members--including drug industry representatives and some researchers--questioned whether price transparency should be required in the pharmaceutical sector, noting that it is not required in other sectors.
Pricing and Value of Brand-Name and Generic Drugs
Some panelists asked whether the enormous differences in the prices of brand-name drugs and generic drugs really represent a difference in value. One panelist suggested that the use of generics could be promoted through techniques used to promote brand-name drugs (e.g., sampling or detailing).
What Additional Information would Improve the Performance of the U.S. Pharmaceutical Market?
An economist on the panel commented that although there is a sentiment among economists that more information is better than less, when one competitive condition is absent in a market--as it is in the U.S. pharmaceutical market--getting more of one element isn't necessarily better. A question policymakers should ask, therefore, is: What kind of additional information would improve the performance of the U.S. pharmaceutical market? This question elicited numerous responses, which are summarized in Strategies for Controlling Costs and Increasing Value From Pharmaceutical Expenditures.
7. Research Questions: Pricing Practices in the Pharmaceutical Market
Conference participants suggested that the following questions might be addressed as part of a research agenda in the area of pricing practices in the pharmaceutical market:
- How do the prices and changes in the prices of U.S. pharmaceutical products compare to external benchmarks (e.g., overall inflation in the economy, overall inflation in health care, prices in other countries)?
- How competitive is the U.S. pharmaceutical market, considering it therapeutic class by therapeutic class? Are drug manufacturers making monopoly profits?
- What is the relationship between pharmaceutical companies' R&D costs and the prices of brand-name prescription drug products?
- What are the advantages and disadvantages of requiring that prescription drug manufacturers make their R&D costs more transparent?
- To what extent does the move to new, more expensive prescription drugs in different therapeutic classes represent value to society? Would the money be better spent if it were used to broaden access to prescription drugs?
- What can be done to encourage greater price competition between brand-name pharmaceutical products, generic products, and OTC products within specific therapeutic classes?
- What information might help improve the performance of the U.S. pharmaceutical market? Should the prices paid for prescription drugs (including rebates from drug manufacturers) by different purchasers and at various points along the distribution chain be made more transparent?
- How can information that might improve the U.S. pharmaceutical market's performance be developed and conveyed?
- What are the implications of the Medicaid best price?
- What, if anything, should be done to increase physicians' and insured patients' sensitivity to the prices of prescription drugs? What is the effect of three-tiered patient cost-sharing arrangements on prescription drug utilization and costs?
- How affordable are prescription drugs for Medicare beneficiaries with fixed incomes, uninsured children, disabled people with high needs and limited resources, etc.? Will making the pharmaceutical market more competitive make prescription drugs affordable for such individuals? If not, what, if anything, should be done?
- What is the relationship between third-party reimbursement levels and profitability and innovation in the prescription drug industry?
- What effects would the enactment of a Medicare prescription drug benefit that gives the Federal Government power over the prices of prescription drugs have on drug manufacturers' earnings, profitability, and ability to innovate?
III. Pharmaceutical Utilization Issues
The third session of the conference explored changing trends in the utilization of prescription drugs, the effects of health insurance on utilization, and questions pertaining to the value of prescription drug utilization and expenditures. The session opened with four formal presentations:
- Cindy Parks Thomas, Ph.D., Schneider Institute for Health Policy, Brandeis University presented data on changes in utilization and costs of prescription drugs in three therapeutic classes.
- Nancy Ostrove, Ph.D., Center for Drug Evaluation and Research, FDA, reported on the FDA's role in regulating consumer advertising of prescription drugs and on FDA's recent research on consumer-directed advertising of prescription drugs.
- John Poisal, Office of Strategic Planning, Health Care Financing Administration (HCFA(now known as CMS)), reported recent findings regarding prescription drug utilization among Medicare beneficiaries from HCFA(now known as CMS)'s Medicare Current Beneficiary Survey.
- Bruce Stuart, Ph.D., Peter Lamy Center for Drug Therapy and Aging, School of Pharmacy, University of Maryland, presented a framework for maximizing the value from prescription drug therapy.
The session also included a Panel Discussion and a discussion of Research Questions.
1. Drug Utilization Trends by Therapeutic Class--Cindy Parks Thomas, Ph.D
Dr. Thomas reported findings from a study of changes in the utilization and costs of prescription drugs in three therapeutic classes: (1) gastrointestinal disease medications, (2) antiarthritics, and (3) cholesterol-reducing medications. The study was conducted by researchers at Brandeis University and PCS Health Systems. It relied on 1996-99 prescription claims data from PCS Health Systems, a PBM, for an insured population of 1.3 million employees and their families.
The study found large increases in expenditures in all three therapeutic classes. However, the relative contribution of price and utilization differed across classes.
- Gastrointestinal disease medications. A large portion of the growth in expenditures in this category was due to increases in cost per prescription. Since the introduction of proton pump inhibitors (PPIs) (e.g., Prilosec®) in the 1990s, the cost of medication per prescription has been increasing very quickly. PPIs are much more expensive than the older H2 receptor antagonists (e.g., Cimetidine®).
- Antiarthritics. Much of the growth in expenditures in this category was due to increases in the cost per prescription. Since the market entry of Cox-2 inhibitors (e.g., Celebrex®, Vioxx®) in January 1999, the utilization of these new medications has skyrocketed. Cox-2 inhibitors are five times more expensive than traditional nonsteroidal anti-inflammatory drugs (e.g., ibuprofen).
- Cholesterol-reducing medications. The growth in expenditures in this category was due largely to increased utilization. The threshold of treatment for high cholesterol has been lowered in recent years, causing rapid growth in the number of people using statins (e.g., Lipitor®, Zocor®, and Prachol®).
2. FDA's Research About Consumer-Directed Prescription Drug Promotion--Nancy Ostrove, Ph.D.
Dr. Ostrove explained that FDA regulates the content of prescription drug ads. No Federal law or regulations have ever prohibited the advertising of prescription drugs. In the spring of 1999, FDA conducted a national survey of adults to assess the effects of FDA guidance pertaining to prescription drug ads issued in 1997 and the effects of direct-to-consumer (DTC) promotion of prescription drugs. About three-fourths of the adult respondents had seen a DTC ad for a prescription drug in the last 3 months, either on television or in a magazine. More than three-fourths of the respondents who had seen a DTC ad recalled the product's benefits, risks/side effects, who should not take the drug, and who should take the drug. Seeing product advertising was associated with an increased likelihood of asking a physician about whether there is a drug to treat the patient's condition and a specific brand. Survey respondents reported that their doctors were positive about their asking about a specific brand-name prescription drug.
3. Medicare Beneficiaries: Prescription Drug Utilization Trends--John Poisal
Mr. Poisal reported findings regarding prescription drug utilization trends based on 1993-97 data from HCFA(now known as CMS)'s Medicare Current Beneficiary Survey. HCFA(now known as CMS) compared utilization among Medicare beneficiaries with prescription drug coverage at any point during the year and at no point during the year. It used two measures of prescription drug utilization: (1) the proportion of beneficiaries filling prescriptions in a given year; and (2) the number of prescriptions per beneficiary in a given year.
During the 5-year period, the proportion of Medicare beneficiaries filling prescriptions showed an upward trend. Although the number of prescriptions per beneficiary rose for both Medicare beneficiaries with prescription drug coverage and Medicare beneficiaries without coverage, the number was higher among Medicare beneficiaries with coverage.
4. Medication Decisions Right and Wrong--Bruce Stuart, Ph.D.
In seeking to obtain the full value that pharmaceutical therapy has to offer, Dr. Stuart explained, the focus should be striking an optimal balance between maximizing appropriate use and minimizing inappropriate use.
- Appropriate use of prescription drugs requires that drugs be safe and meet the standards of good medical care. A reasonably good definition is "the right drug, for the right patient, taken in the right way, and at the right cost."
- Inappropriate use of prescription drugs encompasses overuse (medications are prescribed when other therapy is warranted), misuse (a patient needs a medication but is given the wrong one), and underuse (a patient's medication need is overlooked or ignored).
Dr. Stuart reviewed the empirical literature on the causes and consequences of inappropriate drug use in the elderly and identified needed areas of future research to help maximize value from prescription drugs. One challenge in seeking to maximize value from pharmaceutical therapy, he noted, is to relate prescription drug therapy to the whole regimen of therapies that are available. An even greater challenge is determining from whose perspective value is to be assessed.
Finally, Dr. Stuart presented a conceptual framework for assessing appropriate and inappropriate drug use that focused on the knowledge and behavior of the principal actors in the medication decisionmaking process. In an ideal scenario, he suggested, drug manufacturers, FDA, physicians, pharmacists, patients, purchasers, insurers, and others would encourage the appropriate use and discourage inappropriate use of prescription drugs (see Table 1).
Table 1
Appropriate Use of Drugs:
Responsible Parties & Roles in an Ideal Scenario
|
Right Drug |
For the Right Patient |
Taken the Right Way |
At the Right Price |
|
|
Pharmaceutical manufacturer
FDA
|
Prescriber
Dispenser
Patient
|
Prescriber
Dispenser
Patient
|
Pharmaceutical manufacturer
Purchasers, insurers, & their agents
Prescriber
Patient
|
|
Source: Bruce Stuart, Ph.D., Peter Lamy Center, University of Maryland School of Pharmacy. Presentation to ASPE Conference on Pharmaceutical Pricing, Utilization, and Costs, Washington, DC, Aug. 8-9, 2000.
5. Panel Discussions: Pharmaceutical Utilization Issues
Limitations of the Study on Drug Utilization in Three Therapeutic Classes
A few panelists noted the limitations of the study presented by Dr. Thomas on drug utilization trends by therapeutic class. One researcher, explaining that a substantial portion of the U.S. population experiences spells without health insurance, cautioned against drawing conclusions about these people from a study among people with continuous health insurance coverage. A physician on the panel warned against drawing conclusions about the appropriateness of the utilization of prescription drugs based on findings with population-based claims data in the absence of clinical data. Another panel member suggested that clinical data from individual physicians can be misinterpreted just as easily as population-based data; the two types of data are complementary.
Effects of Consumer-Directed Ads for Prescription Drugs
There was a lengthy discussion by panel members of the effects of consumer-directed ads for prescription drugs on drug utilization and costs.
AARP member survey on print DTC ads
One panel member reported that the AARP recently surveyed its members on the effects of DTC ads for prescription drugs in print media. AARP survey respondents said they wanted to see the DTC ads. Since they generally thought the ads sponsored by drug manufacturers were biased, they trusted their doctor to tell them whether a drug was good or bad for them.Perspectives on DTC ads
Several panel members gave their perspectives on DTC ads for prescription drugs:
- A representative of a major pharmaceutical company said he views DTC advertising as part of the process of making physicians and patients partners in health care.
- Several physicians on the panel said they were surprised by the FDA survey's findings that patients' doctors were positive about their patients' asking for advertised brand-name drugs. In part because managed care organizations are pushing them to see patients in 7 minutes and to view patients as customers who must be kept satisfied, physicians often succumb to pressure from their patients to prescribe specific brand-name drugs. A representative of the American Academy of Family Physicians said she believes that DTC advertising could help make physicians and patients partners in health care if physicians were not so pressed for time.
- PBM representatives said that many of their customers--HMOs, large employers, insurance carriers, etc.--hate DTC ads because they increase utilization and costs. Plan sponsors do not want to encourage prescription drug utilization, even appropriate utilization, particularly in the age 55-64 age group, because the plan sponsors won't benefit--Medicare will.
- Several panelists, including consumer representatives, suggested that consumers need information to counter DTC advertising, which is not just educational but also intended to promote the utilization of particular drugs. RXHealth Value, a coalition of organizations including AARP, believes that it is important to get information to consumers about risks and benefits and appropriate utilization in DTC advertising. A health benefits consultant said some DTC ads are irresponsible ads and suggested that government regulation is needed to curb such ads.
- One panel member, noting that much of the growth in the utilization of prescription drugs occurred before the advent of consumer-directed advertising, suggested that people who have cardiovascular problems, arthritis, or other health problems are looking for something to help them. Another panelist suggested that Baby Boomers are particularly receptive to DTC advertising that promises a pill to fix a problem.
Research questions related to DTC ads and marketing of brand-name drugs.
Several panel members suggested topics for research related to DTC ads and marketing efforts by brand-name manufacturers.
- What are the differential impacts of DTC ads on people with good prescription drug coverage and those without it? Are DTC ads more of a driver of utilization among HMO members with $5 copayments than among people without health insurance?
- Do patient requests for drugs that are advertised DTC improve the appropriateness of physician prescribing and ultimately favorably impact patients' health status, or does it promote use of more expensive drugs when there are less expansive alternatives?
- What are the effects of physician detailing and the intersection of that with DTC ads on the utilization and costs of prescription drugs? Is there anything else that might be pushing more expensive therapies that are not any better than alternative therapies?
HCFA(now known as CMS)'s Study of Drug Utilization Among Medicare Beneficiaries
Noting that the HCFA(now known as CMS) study of drug utilization patterns among Medicare beneficiaries compared beneficiaries without coverage and beneficiaries with coverage at any point during the year, a researcher on the panel said that it is important not to think of coverage as a dichotomy--i.e., having coverage or not having coverage. In terms of their prescription drug utilization patterns, people who are intermittently insured are more like people with no insurance than like people with continuous coverage. Beyond that, this researcher noted, some work suggests that when you take a group of individuals who don't have insurance coverage and give it to them, there is a big bump in utilization in the first year or two, but then utilization tends to even out. This phenomenon has an important cohort effect in studies of people who are newly covered vs. people who are continuously covered.
Appropriate Use of Drugs: Responsible Parties and Roles
Panel members discussed the table showing responsible parties and roles in the appropriate use of drugs (Table 1) at considerable length. Several panel members, including PBM representatives, observed that in the real world, we never get over to "at the right price" (on the far right side of the table). In fact, for the most part, we never get past "for the right patient."
"The Right Drug"
- Role of drug manufacturers and FDA. Before marketing a new drug, manufacturers have to (1) demonstrate the product's safety and efficacy to FDA; and (2) negotiate product labeling with FDA. A researcher on the panel asked: How much prescription drug use is off-label use? Dr. Ostrove said that off-label use is probably very high in some areas of medicine (e.g., oncology, 50-75%), but much lower in other areas. Another panel member suggested that the Federal Government should pay for clinical trials to evaluate the effects of pharmaceuticals on elderly people with multiple conditions, perhaps even taking multiple medications. Physicians and other panelists disagreed, noting the nearly insurmountable methodological challenges that such trials would pose.
"For the Right Patient, Taken the Right Way"
- Role of physicians. Some consumer organizations, including the AARP, believe the ultimate decision about what drug a patient should get should be made by the patient's physician--not a health plan, HMO, or PBM. As noted earlier, a recent AARP survey found that the current generation of elderly consumers trust their physicians to make decisions about what drugs they should get. Disturbingly, however, the survey found that 54% of respondents did not usually receive counseling about the risks and benefits of the drugs they received at the time of prescribing or dispensing. Physicians on the panel said they often just prescribe the drugs that their patients request. Although they would like to counsel their patients more than they do, they feel pressured by managed care organizations to see patients quickly and to keep them satisfied.
- Role of pharmacists and PBMs. An advocate for seriously ill or disabled patients who must take 8-15 medications from different doctors stressed that such patients do not feel they can rely on a PBM to help them manage their medications. For these patients, pharmacists are vital. Representatives of pharmacy organizations emphasized that pharmacists are trained in the appropriate use of drugs and could play a much greater role in educating patients to use their drugs appropriately. They recommended conducting research on how to restructure the reimbursement system to compensate pharmacists for counseling patients on how to take their medications. There was considerable discussion by panel members of disease management programs implemented by PBMs and others to maximize the effectiveness of therapy and minimize its costs in the session on Strategies for Controlling Costs and Increasing Value From Pharmaceutical Expenditures.
- Role of patients. Several panel members, including consumer representatives, argued that consumers need objective, factual information that they can use to make decisions about prescription drugs based on value to them, which includes considerations of risks, benefits, and costs. A health benefits consultant noted that there is a wide range of credibility and quality of the information on the Internet. At some point, we need a culling out of the most useful information and some sort of process to certify what information is "good" information. Consumer advocates noted that particular challenges will arise in developing information for low-income people without health insurance, who are disproportionately people with disabilities, people of color, and people without college degrees. These people are unlikely to use the Internet and will probably seek information from their physicians or other personal sources.
"At the Right Price"
As noted above, panel members noted that in the real world, we never get over to "at the right price" (on the far right side of Table 1).
- Role of drug manufacturers. The prices of new drugs are set by pharmaceutical manufacturers. According to one panel member, much of FDA's new drug approval process focuses on product labeling. Brand-name manufacturers make huge investments to affect the labeling that they can use to detail to physicians.
- Role of purchasers, insurers, and their agents. PBM representatives reported that many PBM customers--health plans and health plan sponsors--simply want to maximize their rebates from brand-name drug manufacturers. For customers that want to lower their net costs for prescription drugs, PBMs can implement mechanisms to steer health plan members to use generic products first, low-cost brand-name products second, and brand-name products with high rebates last. Mechanisms used by PBMs to control the costs of their customers' pharmacy benefit programs were discussed in the session on Strategies for Controlling Costs and Increasing Value From Pharmaceutical Expenditures.
- Role of physicians. There was disagreement about the role that physicians should play in ensuring that drugs are provided at the right price, but it was clear that potential conflicts of interest could arise. Physicians and consumer representatives on the panel strongly opposed having physicians put at financial risk for the prescription drug utilization of their patients. Consumers want their doctors to make decisions based on the patients' best interest, not on what puts the doctor at least financial risk. PBMs and other panel members want physicians to be educated about the comparative costs of drugs, so that they can take costs into account when writing prescriptions. As discussed in the session on Strategies for Controlling Costs and Increasing Value From Pharmaceutical Expenditures, PBM representatives hope that Palm Pilots or other hand-held e-prescribing devices can be used to make physicians more aware of price differentials and price benefits to consumers at the point of prescribing. One panel member suggested that physicians could be educated to take both their individual patients' interests and societal interests into account when prescribing prescription drugs.
- Role of pharmacists. Some PBM representatives and large employers said that they do not think that utilization controls at the level of the retail pharmacy are the answer to controlling the costs of prescription drugs. Employees do not want to go to the pharmacist to have their prescription filled only to be told (as they are now) that the drug is not approved by their health plan.
- Role of patients. PBM representatives suggested that consumers need to be held more accountable for their prescription drug utilization and costs. Increasingly, PBMs and their customers are moving toward letting employees have the choices they want, but making them pay for that privilege, for example, through the use of three-tiered copayments for prescription drugs. Patients with three-tiered copayments pay the lowest price for generic drugs, a higher price for "preferred" brand-name drugs on a plan's formulary, and the highest prices for drugs not on the formulary. As noted earlier, consumer representatives emphasized that patients need objective, factual information that they can use to make decisions about prescription drugs based on considerations of both quality and price.
Perspectives on the "Value" of Prescription Drugs
Panel members agreed that much of the debate about prescription drugs is about who should pay for them. They also agreed that the value of prescription drugs differs for different parties. Some panel members suggested that it would be helpful to obtain more information about the value of prescription drugs from different perspectives--especially from the perspective of society as a whole.
- Value to society. How does society value prescription drugs in the context of social welfare, economic growth, the U.S. health care system, etc.?
- Value to drug manufacturers. One researcher on the panel noted that in a monopolistic market, more of the value goes to the manufacturer than to other parties. Value to a prescription drug manufacturer may be very different from value to society as a whole or to individual patients.
- Value to individual patients. Some panelists noted that in some situations, consumers are willing to pay almost any price for a prescription drug that relieves their (or a loved one's) pain or suffering. They suggested that competition does not work when there is a captive market.
- Value to physicians. Physicians on the panel said that a paramount concern for them is making sure that patients get good quality care. They noted that sometimes drugs have subtle differences known to physicians that do not show up in analyses. Physicians also want to satisfy their patients and protect themselves from potential malpractice suits.
- Value to employers/sponsors of health benefits plans. According to some panel members, the objective of employee health benefits--at least in a tight labor market--is to maximize employees' well-being. For that reason, large employers who offer health benefits to their employees are reluctant to antagonize their employees by saying that they are not going to provide coverage for products that patients want (e.g., antidepressants or antihistamines). At the same time, PBM representatives suggested, most PBM customers--large employers, HMOs, insurance carriers, etc.--want to minimize the costs of their health benefit program.
6. Research Questions: Pharmaceutical Utilization Issues
Conference participants suggested that the following questions might be addressed as part of a research agenda in the area of pharmaceutical cost pressures and trends:
- What, if anything, can be done to help increase the value from prescription drug expenditures?
- Are drugs in specific therapeutic classes being appropriately used? What are the criteria for appropriate use? What outcomes research might be conducted to understand better what constitutes appropriate use of prescription drugs?
- Are drugs in specific therapeutic classes being inappropriately used--i.e., overused, misused, or underused? What are the criteria for inappropriate use? What accounts for this inappropriate use?
- Are drugs in specific therapeutic classes being appropriately used? What are the criteria for appropriate use? What outcomes research might be conducted to understand better what constitutes appropriate use of prescription drugs?
- What are the characteristics of individuals most at risk for inappropriate prescription drug use? What are the costs and consequences of treating the sequelae of inappropriate prescription drug use?
- If one defines the appropriate use of pharmaceuticals as "the right drug, for the right patient, taken in the right way, at the right cost," what could be done by the following parties to encourage the appropriate utilization of drugs by Medicare beneficiaries under a Medicare prescription drug benefit?
- Pharmaceutical manufacturers;
- Government agencies such as FDA, NIH, the Agency for Healthcare Research and Quality (AHRQ), and HCFA(now known as CMS);
- Physicians;
- Pharmacists;
- Patients;
- Managed care plans and PBMs; and
- Large employers.
- What effect does DTC advertising have on the utilization of brand-name prescription drugs? Are there differential impacts on people with good prescription drug coverage and those without it? How does it intersect with physician detailing and other strategies used to increase the utilization of specific products? What impact does DTC advertising have on physicians' prescribing patterns and patients' health outcomes?
- What are the effects of various pricing- and utilization-focused cost-control strategies, both singly and in combination, that PBMs use to control the costs of their customers' prescription drug programs--e.g., rebates, mail service pharmacies, use of drug formularies, drug utilization review, disease management programs, and patient cost-sharing arrangements?
- What role might disease management programs play in encouraging appropriate utilization and discouraging inappropriate utilization of prescription drugs among individuals with chronic medical conditions? What roles should physicians, pharmacists, PBMs, and patients play in disease management programs? What financial incentives are needed to help ensure the success of disease management programs? How should such programs be funded?
- What information is needed to enable physicians, patients, and others to encourage the appropriate utilization of prescription drugs and discourage the inappropriate utilization of prescription drugs? What is the best way of developing and conveying this information? Can new technologies such as Internet and e-prescribing initiatives play a role in encouraging the appropriate utilization of prescription drugs?
IV. Strategies for Controlling Costs and Increasing Value From Pharmaceutical Expenditures
The final session of the conference focused on the identification of strategies that might be adopted to control rising prescription drug expenditures and maximize the value for dollars spent on a pharmaceutical benefit. The session began with two formal presentations:
- David Kreling, Ph.D., R.Ph., Sonderegger Research Center, School of Pharmacy, University of Wisconsin, described strategies that PBMs have adopted to control the costs of their customers' prescription drug programs.
- Helene Levens Lipton, Ph.D., Institute for Health Policy Studies, Department of Clinical Pharmacy, University of California at San Francisco, reported on physician group practices' failed efforts to share financial risk for patients' drug costs with HMOs, as well as on hand-held, electronic prescribing devices.
The session also included a Panel Discussion and a "Lightning Round" of public policy researchers' perspectives.
1. Cost Control for Prescription Drug Programs: Pharmacy Benefit Manager (PBM) Efforts, Effects, and Implications--David H. Kreling, Ph.D., R.Ph.
1. Cost Control for Prescription Drug Programs: Pharmacy Benefit Manager (PBM) Efforts, Effects, and Implications--David H. Kreling, Ph.D., R.Ph.
Dr. Kreling noted that PBMs use two general types of strategies to control the costs of their customers' prescription drug programs: (1) pricing-focused cost-control strategies; and (2) utilization-focused cost-control strategies. Similar strategies are also used by HMOs, health plans, State governments, and other entities.
Pricing-focused cost-control strategies are aimed at obtaining rebates or discounts on prescription drugs from drug manufacturers or pharmacies:
- Discounts from pharmacies. PBMs may "negotiate" payments or reimbursements to pharmacies for prescription ingredient costs and/or dispensing fees.
- Rebates from brand-name drug manufacturers. PBMs' rebates from brand-name drug manufacturers typically have some purchaser volume or market share requirements associated with them.
- Mail service pharmacies. PBMs may encourage or require consumers to use mail service pharmacies for long-term prescription drug therapy for chronic illnesses.
- Utilization-focused cost-control strategies focus on consumers, prescribers, or pharmacies in an effort to influence which drugs and/or how many drugs are used:
- Drug formulary. A formulary is a list of drugs approved for use/reimbursement. A formulary may be a closed formulary that allows no exceptions; a partially closed formulary that allows exceptions with prior authorization or increased cost-sharing; or an open formulary that includes all drugs.
- Financial incentives to use generics. PBMs may give financial incentives to patients, pharmacists, or prescribers to use generic prescription drugs rather than brand-name drugs.
- Drug utilization review. PBMs may review drug utilization, either retrospectively or concurrent with the prescription-dispensing process, to identify and intervene to correct utilization problems.
- Disease management programs. PBMs may implement programs intended to maximize the effectiveness of drug therapy and outcomes for specific medical conditions, as well as to minimize the total treatment costs for those conditions.
- Patient cost-sharing. PBMs may require patients to share the costs of prescription drugs via copayments (paying a fixed cost per prescription) or coinsurance (sharing a direct proportion of costs). Coinsurance can sensitize consumers to differences in the costs of the drugs they use, conceivably driving drug use to lower cost (generic or discounted) drugs but may reduce consumers' access to high-cost drugs. Currently, copayments are far more common than coinsurance.
What limited research there is about the effectiveness of various types of pricing-focused and utilization-focused cost-control strategies suggests that none of the approaches is without limitations. Because of the complexity of the reasons for drug use and increasing expenditures, most of the strategies have unintended effects that may end up compromising cost-control efforts.
2. Managing the Unmanageable: Drug Payment and Utilization Management Strategies in Physician Organizations--Helene Levens Lipton, Ph.D.
Dr. Lipton discussed two strategies used by physicians to affect patients' prescription drug utilization:
- Physician groups' financial risk for HMO patients' drug costs. Physician groups throughout the country have been losing the battle in managing financial risk for HMO patients' drug costs, largely because they do not have sufficient information or control. As a result, physician groups are now trying to eliminate (or reduce) their financial risk for HMO patients' drug costs. They are moving away from capitation contracting toward "incentivized" pharmacy contracts based on formulary compliance, generic drug fill rates, etc.
- Hand-held, electronic, point-of-prescribing devices. Palm Pilots or other hand-held, electronic, point-of-prescribing devices have the potential (1) to reduce medication errors through enhanced legibility and electronic identification of potential drug therapy problems; (2) to enable physicians to access data on patient compliance, improving ability to improve outcomes; (3) to maintain a complete record of client transactions; and (4) to provide physicians immediate feedback on availability of formulary and generic drugs, with the potential to decrease costs. Dr. Lipton recommended independent controlled research trials to assess the impacts of e-prescribing technologies (e.g., hand-held e-prescribing devices, electronic medical records, and Web-based technologies).
3. Panel Discussion: Strategies for Controlling Costs and Increasing Value from Pharmaceutical Expenditures
Following the two formal presentations, panel members and members of the general audience were given an opportunity to make comments on strategies for controlling costs and increasing value from pharmaceutical expenditures.
PBMs' Pricing- and Utilization-Focused Cost-Control Strategies
Representatives of PBMs on the panel reiterated that the cost-control strategies a PBM adopts depend on what the PBM's customers--health plans and health plan sponsors--want. A few PBM customers want the PBM to intervene aggressively to control the utilization and net costs of prescription drugs. Through a combination of strategies--finding the lowest cost drug (not maximizing rebates); finding the best coinsurance or copayment design known to economists; and fully employing prior authorization programs, second opinions, and step therapies--one PBM reported that it has been able to limit growth in prescription drug expenditures to 2-5%.
Panel members agreed that further research is needed on the effects, intended and otherwise, of PBMs' pricing- and utilization-focused cost-control strategies--both alone and in combination.
PBMs' pricing-focused cost-control strategies:
- Rebates from brand-name drug manufacturers. Researchers and PBM customers said that it would be helpful to get a better understanding of PBMs and their operations. A researcher on the panel noted that PBMs used to make money processing claims, but in the last 10 or 15 years the cost of processing a claim has dropped below the cost of a postage stamp. Retail pharmacy representatives on the panel suggested that PBMs are making money via their share of rebates from brand-name drug manufacturers.
- Mail service pharmacies. Representatives of retail pharmacies said the perception is that mail order service saves money, and claims have been made that mail order service offers a better environment than the retail environment for generics. Retail pharmacists believe that these claims should be investigated through research.
PBMs' utilization-focused cost-control strategies:
- Use of drug formularies. Two integrated health systems, with their own physicians, hospitals, and pharmacists--Kaiser Permanente and the U.S. Department of Veterans Affairs (VA)--have had some remarkable successes in managing the utilization and costs of prescription drugs with their drug formularies and other mechanisms. The VA's successes were described in a recent report by the Institute of Medicine. Panel members generally agreed that the techniques used by Kaiser and the VA would not work as effectively in health care systems lacking integration. Most physicians have to deal not with a single formulary but with multiple formularies from different managed care organizations. A researcher on the panel reported that a typical family physician operates with about 6.5 contracts with managed care organizations and a specialist with about 40 contracts. Several panel members, including physicians and consumer representatives, raised concerns about formularies developed by managed care organizations and recommended research to evaluate their effects on clinical outcomes. They also suggested research comparing clinical outcomes in single-formulary environments such as the VA or Kaiser with clinical outcomes under multiple formulary environments, controlling for patients' health status. One consumer organization, the AARP, said that while it does not oppose formularies per se, it believes that it is important to have oversight of the formulary development process, external reviews, appeals, etc.
- Drug utilization review. Some PBM representatives and large employers said that they do not think that utilization controls at the level of the retail pharmacy are the answer to controlling the costs of prescription drugs. Most PBM customers, whether because of a tight labor market or a backlash against managed care decisionmaking, do not want employees to go to a pharmacy with a prescription only to be told (as they are now) that the drug is not approved by their health plan. As a result, PCS Health Systems, Express Scripts, and other PBMs are now trying to find a place in physician decisionmaking so that if the physician makes the right decision, everything cascades from there, and patients and pharmacists don't get hit with heavy regulatory PBM activity.
- Disease management programs. Panel members spent a considerable amount of time talking about disease management programs, noting that since Medicare includes many elderly and disabled beneficiaries with chronic conditions, it is going to be very important to be able to manage their drug use appropriately.
- Sponsors and incentives for disease management programs. One researcher noted that disease management programs can focus on any of several problems throughout the patient management process, and what a particular program focuses on--e.g., compliance with drug therapy, drug substitution programs--reflects the incentives of the PBM, HMO, or other program sponsor. Most disease management programs have had to show a return on investment (cost savings) in the short term--otherwise no one sponsors them. There is a lot of good disease management going on, but it is labor intensive and expensive, and not all of it reduces costs in the short term.
- Physicians' role in disease management. Physicians reported feeling buffeted by multiple and conflicting disease management strategies. A researcher on the panel said physician groups' ability to devote time and energy to clinical process design, which results in perhaps spending more on certain drugs but achieving overall cost savings, is often constrained by the push for drug component management in disease management programs.
- Pharmacists' role in disease management. Pharmacists on the panel said that there is a lot of opportunity to take advantage of the existing infrastructure of retail pharmacies for disease management. Pharmacists are trained to do excellent disease management, but with few exceptions, they are not being used for this. Financial incentives are needed to compensate retail pharmacists for disease management.
- PBMs' role in disease management. PBM representatives said that the infrastructure PBMs have put into place in the last 10-15 years offers the potential to do disease management if the economic incentives are put into place. A critical lesson for Medicare from PBM disease management programs, according to PBM representatives, is the need for an economic incentive structure to pay for case management and disease management services.
- Focus on a single disease not good for elderly with multiple conditions. One researcher suggested that disease management programs that focus on a single disease may do more harm than good in patients with multiple conditions.
- Need for outcome research. Several panelists said that the outcome science for "If I do this, then I get that" (whether measured in cost savings, quality of life, patient satisfaction) in most diseases and conditions does not exist. More research of this type is needed.
- Population-based disease management vs. privacy regulations. One panelist noted that a population-based approach to disease management is on a collision course with Federal and State privacy legislation. Currently, many disease management programs are using an opt-in voluntary strategy. Those who volunteer are the high-performing patients and will do well. People who don't volunteer typically are the more costly patients.
- Sponsors and incentives for disease management programs. One researcher noted that disease management programs can focus on any of several problems throughout the patient management process, and what a particular program focuses on--e.g., compliance with drug therapy, drug substitution programs--reflects the incentives of the PBM, HMO, or other program sponsor. Most disease management programs have had to show a return on investment (cost savings) in the short term--otherwise no one sponsors them. There is a lot of good disease management going on, but it is labor intensive and expensive, and not all of it reduces costs in the short term.
- Patient cost-sharing. Health insurers and HMOs urged policymakers not to put policies in place that would impede their ability to experiment with new ideas in the realm of prescription drugs. As noted earlier, some health plans have been moving to a three-tiered copayment structure to make consumers bear more of the costs when they opt for an expensive drug over a less expensive (but appropriate) brand-name or generic alternative. Panel members suggested that more research is needed on the effects of three-tiered and other cost-sharing arrangements on the utilization and costs of prescription drugs. Research is also needed on the effects of such arrangements on the appropriate and inappropriate use of prescription drugs and patients' health outcomes.
Utilization Management to Control Costs vs. Clinically Determining Appropriate Utilization
Physicians and other panelists emphasized that it is important not to conflate utilization management aimed at controlling costs with determining appropriate utilization clinically (i.e., determining what is clinically best for patients according to health care providers). Utilization quality controls (e.g., generic prescribing) have some underlying scientific basis; however, volume controls such as those used by the Medicaid program have no good scientific basis, may drive patients to other venues, and may have an impact on the disease process that may end up costing the program sponsor more than the costs saved in reduced volume.
What Information Might Help Improve the Performance of the U.S. Pharmaceutical Market?
In several sessions of the 2-day conference, panel members identified information that they thought could help improve the performance of the U.S. pharmaceutical market:
- Information on prescription drug prices and manufacturers' R&D costs. As noted earlier, panel members disagreed about whether prescription drug prices and manufacturers' R&D costs should be made more transparent. (See discussion in Pricing Practices in the Pharmaceutical Market)
- Information for consumers on prices and appropriateness. Consumer advocates and researchers on the panel suggested that consumers need information on drug prices and on which drugs are appropriate for them. It is important that such information be supplied by a source that is trusted by the public to provide good, unbiased information.
- Implications of the Medicaid best price. Some panel members suggested that policymakers need to know more about the implications of the Medicaid best price. If businesses are asked to take risks on pharmaceutical benefits, and if the Medicaid best price is affecting businesses' ability to take risks, policymakers should understand the implications of that.
- Economic policy research conducted from a societal perspective. One researcher argued that U.S. policymakers need good economic policy research on health care in general and pharmaceuticals in particular conducted from a societal perspective. Such research is not very forthcoming from either the academic or the policy world.
How Can Information Be Developed and Conveyed?
Panel members also discussed what mechanisms might be used to convey information about prescription drugs to consumers and other parties:
- The role of the Federal Government in developing information. Several panelists suggested that the Federal Government should play a key role in developing and conveying information for consumers on the prices and appropriateness of prescription drugs. A researcher on the panel recommended establishing a Federal agency to evaluate economic policy related to health care and pharmaceuticals from a societal perspective. Panel members noted that there are 40 to 50 million people, especially the elderly or individuals enrolled in public programs with low levels of health care literacy. Functional illiteracy is more prevalent among beneficiaries in public programs and rises with age. Such individuals will need help to navigate new systems put into place in the event of the enactment of a Medicare prescription drug benefit. AARP survey data indicate that many people in the current generation of Medicare beneficiaries rely primarily on their physicians for guidance.
- The role of new technologies in conveying information. Several panel members commented that changes in the use of technology will improve the flow of information to physicians, patients, and others. For physicians, hand-held, electronic prescribing devices now in development show considerable promise for making information--e.g., formulary information, cost information, clinical practice guidelines--available to physicians at the point of prescribing. One vehicle for conveying information to consumers is the Internet, but it will probably be used more by Baby Boomers than by the current generation of Medicare beneficiaries.
Other Strategies For Improving Competition in the U.S. Pharmaceutical Market
Some panelists supported the use of strategies to improve the operation of the U.S. pharmaceutical market to control costs and increase value from pharmaceutical expenditures without massive government intervention. Research is needed on all of these strategies:
- Reconsidering incentives for prescription drug R&D. As discussed earlier, there are many patent and patent-like protections available to brand-name drug manufacturers. Consequently, generic drug products often struggle to get in the market. An important question for U.S. policymakers is: Is what the country is buying in terms of incentives for R&D through drug patent and exclusivity arrangements worth the cost, or can we find a more cost-effective approach to promote innovation? Another question is: What can the Federal Government do to stimulate the innovation of breakthrough products rather than "me-too" products?
- Reconsidering the licensing of products developed with NIH-funded research. U.S. drug manufacturers are sometimes given an exclusive license to market new prescription drug products developed with research funded by the National Institutes of Health (NIH). These products are subject to the usual patent rules, and there are no constraints on price. A question for policymakers is: Is this practice in the best interest of consumers, and if not, what should be changed?
- Educating providers and consumers about the relative value, benefits, risks, and costs of drugs. There are often competing therapies in a given therapeutic class, but providers and consumers are not aware of it. Important questions for U.S. policymakers are: How can credible information about the relative value of different drug therapies be developed? Second, how can that information best be conveyed to the appropriate parties?
- Making physicians more aware of generic drugs. Unlike brand-name drug manufacturers, generic companies do not detail products to physicians--instead, generic companies sell their products to drug wholesalers and the chain pharmacies. A generic drug representative suggested that physicians need to be sensitized to the fact that there are generic products available that they could use as an alternative to brand-name drugs. Possible approaches for making physicians more aware of the availability of generic drugs include generic sampling or academic detailing for generic products.
- Giving consumers a choice of different pharmacy benefits, priced accordingly. An alternative to micromanaging the utilization of pharmaceutical benefits might be to give consumers different levels of pharmacy benefits, priced accordingly--for example (1) a closed formulary; (2) a formulary with a medical necessity override; (3) a three-tiered formulary, and (4) an open formulary. The pricing of the different pharmacy benefits would reflect different experiences with utilization.
- Developing measures of the value of prescription drug benefits. Health care purchasers indicated that they would like to have measures that they could use to measure the value (quality/cost) of the benefit programs they are purchasing. Consumer Reports has done some work in measuring value, as has the National Committee on Quality Assurance. More research is needed in this area.
- Reconsidering Medicaid best price. Representatives of PBMs and health plans on the panel suggested that policymakers should consider repealing the Medicaid best price and allowing the free market to work. Policymakers need to consider the following questions: Is the Medicaid best price keeping States which have a huge volume (employees and Medicaid) from getting the best price? Is the Medicaid drug rebate policy established in 1990 lowering the ability of private purchasers to negotiate steep discounts with pharmaceutical companies? One retail pharmacy representative agreed that the Medicaid Federal upper limit list needs to be reformed; however, he cautioned against repealing Medicaid best price, noting that Medicaid best prices were adopted because Medicaid was unable to negotiate effectively.
- Reconsidering the criteria for designating drugs as prescription drugs or OTC drugs. Some prescription drugs in the United States are available OTC in other countries. Blue Cross Blue Shield believes the designation should be based on safety not a pharmaceutical company's economic strategy.
Direct U.S. Government Intervention to Reduce the Prices of Prescription Drugs
A few panelists supported the direct intervention of the U.S. Government in the pharmaceutical market to control costs and increase value from pharmaceutical expenditures:
- Government price controls and regulations. Several panelists noted that a Medicare benefit prescription drug benefit can be expected to increase the utilization of prescription drugs. They argued that rather than focusing on reducing utilization--given that the problem for many Medicare beneficiaries is an inability to afford prescription drugs that they need--U.S. policymakers should focus on controlling brand-name pharmaceutical manufacturers' prices and pricing practices. Price controls are used in much of the industrialized world outside the United States, and most of these countries have lower drug prices than the United States. In the United States, however, price controls are less politically popular and there are concerns about the effects of price controls on innovation.
- Government contracts with pharmaceutical manufacturers. One panel member argued that more money for business as usual is not going to work. He recommended that the Federal Government enter into contracts with drug manufacturers to cut the prices of prescription drugs substantially (e.g., to the level of the manufacturers' marginal costs or to the Federal Supply Schedule level). Although the manufacturers would probably make up most of their lost revenue in higher volume, the Federal Government could agree to make up any lost revenue so that the drug companies would be left financially whole. In addition, to address concerns about research and innovation, the Federal Government could provide additional money to the National Institutes of Health, change intellectual property laws to encourage the development of breakthrough products, etc.
- Another panel member suggested that perhaps the Federal Government could negotiate risk-based contracts with drug anufacturers under which the drug manufacturers would share utilization risk with the Federal Government and sell their products at marginal costs. This approach, he said, would protect the manufacturers' profitability, although decreasing their profit margin, and would get more prescription drugs to the people who need them.
4. Lightning Round: Public Policy Researchers' Perspectives
Following the discussion of strategies for controlling costs and increasing value, five health policy researchers were asked to give their perspectives on everything they had heard at the conference.
Stanley Wallack, Ph.D., Brandeis University
Dr. Wallack said that if he were sitting as a key policymaker, he would expect the utilization and expenditures of prescription drugs to go up. He would be interested in the following topics:
- How efficient is the U.S. pharmaceutical market and can we make it more efficient?
- What is the "value" of pharmaceuticals from a societal perspective? Developing information to answer this question will require substantial funding from the public sector.
- Is the drug industry making monopoly profits? Conference participants gave very little attention to this question. In a monopolistic market, more value goes to the manufacturer than to other parties.
- What potential is there for increasing the utilization of generic drugs? Perhaps in the new drug approval process, brand-name drug manufacturers should be required to say how their new product will compare to generics in terms of price.
- Do we want to use information to change the U.S. pharmaceutical market generally or do we want to use targeted incentives (e.g., incentives for R&D)?
- Can disease management techniques be used for high users of prescription drugs? High users account for an increasing proportion of individuals who use prescription drugs and are at the greatest risk for drug interactions.
Robert Helms, Ph.D., American Enterprise Institute
Dr. Helms said that when talking about economic systems, the bottom line for economists is how well an economic system provides value to consumers--i.e., satisfies consumer wants and adapts technology to consumer wants in an efficient way. This is something we should keep in mind in the debate about prescription drugs--what we are after is providing what consumers want.
It is very probable that prescription drugs will be added somehow to Medicare, and when this is done, the basic debate will be whether to use a market approach or a regulatory approach. Economics offers a lot of literature about what happens under both systems, and Dr. Helms quite frankly is on the market side. He is fairly optimistic that the prescription drug market will work out. The market provides incentives for innovation. And the higher prescription drug costs go, the more incentives there are to make the pharmaceutical market work more effectively
Beth Fuchs, Ph.D., Health Policy Alternatives
Dr. Fuchs said that she came to the conference hoping that she would get more information that would help her analyze Medicare prescription drug proposals, but she is now more confused than ever because of the complexity of things. Dr. Fuchs said she believes it would be helpful to have more information about whether PBMs could help get Medicare beneficiaries access to prescription drugs in an affordable manner. What would happen if PBMs were given a free rein in a public-private approach? Could a PBM-like entity produce significant savings that would help Medicare's 40 million beneficiaries get access to prescription drugs in an affordable manner? Finally, Dr. Fuchs noted that much of the information that policymakers need to make policy regarding prescription drug benefits has been proprietary or lost in the academic literature. She encouraged drug manufacturers and policy analysts to make this information available in a form that policymakers and researchers can use.
William Scanlon, Ph.D., U.S. General Accounting Office (GAO)
Dr. Scanlon said that he felt as though lots of different boxes had been opened and everything poured out of them at this conference. He said he believes that policymakers need two types of information:
- Information related to market failure in the U.S. prescription drug market. Conference participants identified several aspects of market failure in the prescription drug market. Many of the problems are tied to a lack of information--information on the underutilization and overutilization of drugs, what prices are being paid, what utilization we should want, clinical information, etc. A key question that arises is: How do we generate more information about what pharmaceuticals can do and how they should be used? It is important to bear in mind that if a Medicare prescription drug benefit is enacted, all of the relationships and prices that exist in the U.S. prescription drug market at present will change.
- Information related to the design and management of a Medicare prescription drug benefit. In designing and managing a prescription drug benefit, policymakers will not necessarily chose between a market approach or a regulatory approach. Instead, they will probably combine the two approaches. In any event, information will be critical. It is impossible to run a market economy unless there is good information flowing freely and people are able to act on it, and it is impossible to regulate an economy without huge amounts of good information. Getting information down to the level of Medicare beneficiaries is going to be particularly important if consumers are going to play a role in health care cost containment or quality enhancement.
Judith Feder, Ph.D., Georgetown University
Dr. Feder said that it is not surprising that there are so many questions at the end of the 2-day conference. She noted, however, that policymakers do not have the luxury of certainty. They never have all the information they could use and have to make decisions with the best information available. Dr. Feder believes the discussion at this conference has two two kinds of policy implications:
- Managing prescription drug benefits for the insured. The bulk of the discussion at the conference has focused on the use and costs and prices of prescription benefits for the insured population. The consensus at this conference seems to be that the role of government--apart from examining the policies it has in place--is to facilitate the market. There was advocacy of a role for government in (1) getting more information about pricing and other behaviors; (2) creating an entity that is a source of independent information on prices and on values; and (3) promoting guidelines that give some indication of the range of ways to think about the value of prescription drug products. There was support expressed for techniques and ways to help physicians--as well as pharmacists--in the prescribing process. Given the survey data that people trust their physicians, Dr. Feder believes that enabling doctors to work with their patients to make what are inevitably difficult choices about prescription drugs is a good idea.
- Providing prescription drug benefits for the uninsured. Right now many of the people who are most in need of prescription drug coverage--elderly Medicare beneficiaries--are among the people least likely to have it. Dr. Feder concluded by saying that she absolutely believes that Medicare beneficiaries ought to have prescription drug coverage and that it ought to be an entitlement. The country does have the resources, she said--it is just a question of making a choice about how those resources are used. Having Medicare rely on best practices for managing drug utilization and costs in the private sector will lead those practices to improve over time.