
Monday, January 25, 2016
Milestones for Goals 2 and 3 of the National Alzheimer's Plan
Matthew Baumgart
Senior Director, Public Policy
Alzheimer's Association
Goal 1 Milestones
1. Prevent and Effectively Treat Alzheimer's Disease by 2025
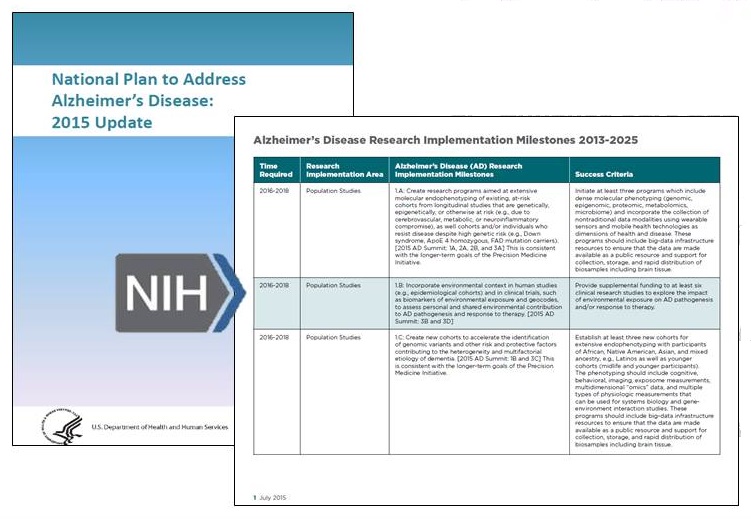 |
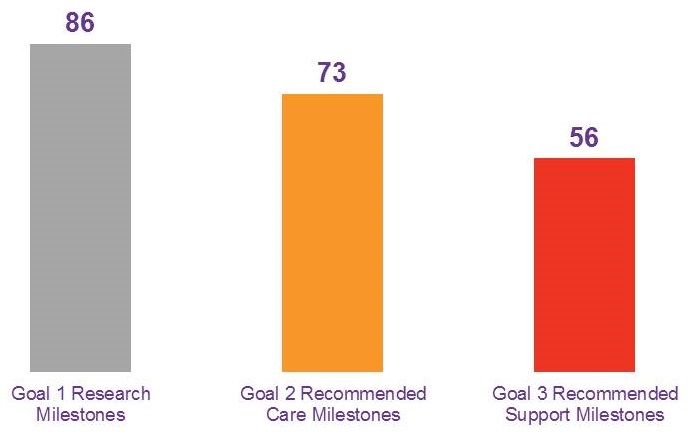
Goal 1 Milestones vs. Appendix 2
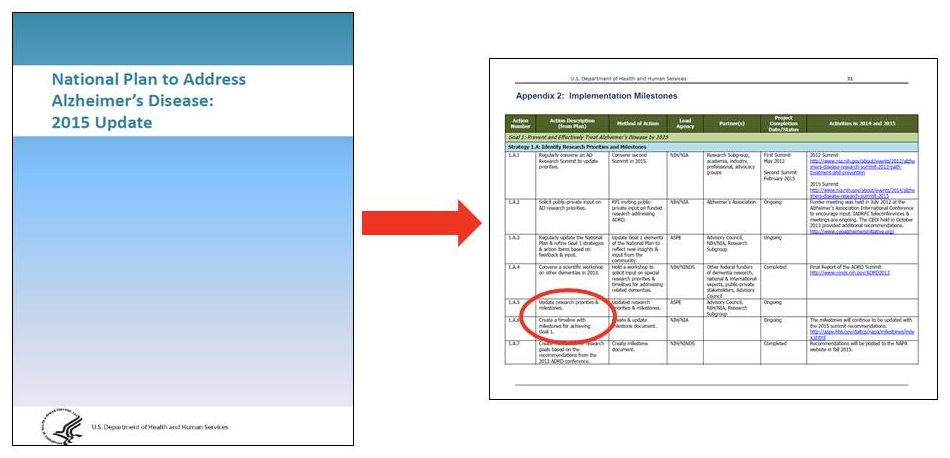 |
The Expert Workgroup
| Soo Borson University of Washington |
Lisa Gwyther Duke University |
| Malaz Boustani Indiana University |
Mary Jane Koren The Commonwealth Fund (retired) |
| Kathleen Buckwalter University of Iowa (emeritus) |
Joanne Lynn Altarum Institute |
| Lou Burgio University of Alabama |
Martha Roherty NASUAD |
| Joshua Chodosh New York University |
Cheryl Phillips Leading Age |
| Richard Fortinsky University of Connecticut |
Judah Ronch University of Maryland |
| David Gifford American Health Care Association |
Claudia Stahl Society of Hospital Medicine |
Why Create Milestones?
- The aim was NOT:
- An official set of milestones to be voted on yea/nay by the Advisory Council
- A benchmark by which to judge the activities under the National Plan
- The aim WAS:
- Itemize and demonstrate -- as the research milestones have done -- the care and support milestones needed to achieve the Plan's 2025 goals
- Stimulate and provoke thinking and ideas among the Advisory Council and the federal government
- Prompt establishment of official milestones
The Workgroup's Marching Orders
- Use the research milestones as a guide
- Work within the existing plan structure
- Establish milestones for each existing strategy
- Do not worry about process details
- Regulation vs. statute
- Existing funding capacity vs. additional funding
- Federal vs. state
- Whether realistic (at the start)
The Workgroup's Marching Order to Itself
Incorporate and expand on existing federal efforts
- HRSA = Dementia primary care curriculum
- CDC = Healthy People 2020 dementia objectives
- CMS = Annual Wellness Visit detection of cognitive impairment
- ACL = ADSSP & alzheimers.gov
The Project's Timeline
- Late September
- Individual workgroup "interviews"
- October
- Review of evidence
- Create objectives & Brainstorm
- Create preliminary milestones
- November
- Develop milestones
- Get "peer review" on milestones
- Explore issues in depth
- December
- Finalize milestones and identify metrics
- Refine & Create final materials
- Submit journal article
Where Should We Be in 2025?
2. Enhance Care Quality and Efficiency
Objective: All persons living with Alzheimer's disease and related dementias, regardless of location, race, ethnicity, sexual orientation or socioeconomic class, should receive high-quality person/family-centered care by well-trained practitioners and workers from detection and diagnosis through end-of-life, across all health care and long-term services and supports settings and systems.
Where Should We Be in 2025?
3. Expand Supports for People with Alzheimer's Disease and Their Families
Objective: People with Alzheimer's disease and related dementias, their families and their caregivers should have access to effective interventions and supports that expand their caregiving skillsets, enhance the meaningfulness and quality of their lives, and reduce the burden of Alzheimer's disease and related dementias.
Building Milestones, Timelines, Success Criteria
- Goal 2. Enhance Care Quality and Efficiency
- Strategy 2A: Build a workforce with the skills to provide high-quality care
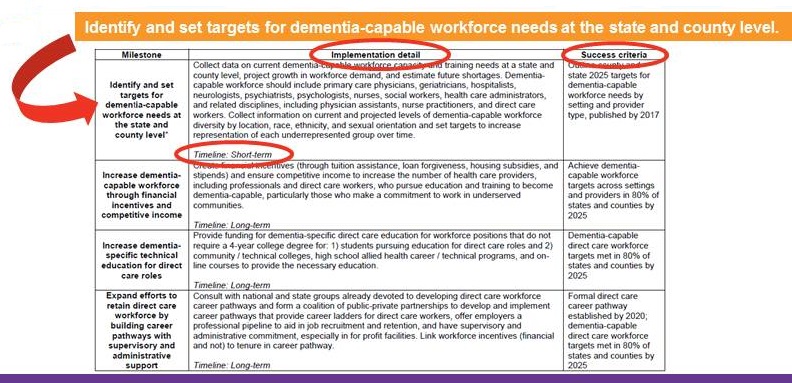
- MILESTONE SECTION: Build and retain a diverse dementia-capable workforce with the skills and capacity to provide high-quality care.
- MILESTONE: Identify and set targets for dementia-capable workforce needs at the state and county level.
- MILESTONE: Increase dementia-capable workforce through financial incentives and competitive income.
- MILESTONE: Increase dementia-specific technical education for direct care roles.
- MILESTONE: Expand efforts to retain direct care workforce by building career pathways with supervisory and administrative support.
- MILESTONE: Increase diverse dementia-capable workforce through financial incentives.
- MILESTONE SECTION: Ensure health care providers across settings are skilled and credentialed in dementia-specific care.
- MILESTONE SECTION: Ensure all direct care workers have proper training to effectively care for persons with ADRD and support their key family and friend caregivers in home, community, and institutional settings.
- MILESTONE SECTION: Build and retain a diverse dementia-capable workforce with the skills and capacity to provide high-quality care.
- Strategy 2A: Build a workforce with the skills to provide high-quality care
Building Milestones, Timelines, Success Criteria
- Goal 2. Enhance Care Quality and Efficiency
- Strategy 2A: Build a workforce with the skills to provide high-quality care
- MILESTONE SECTION: Build and retain a diverse dementia-capable workforce with the skills and capacity to provide high-quality care.
- MILESTONE: Identify and set targets for dementia-capable workforce needs at the state and county level.
- MILESTONE SECTION: Build and retain a diverse dementia-capable workforce with the skills and capacity to provide high-quality care.
- Strategy 2A: Build a workforce with the skills to provide high-quality care
 |
Final Milestones Product
 |
Some Examples
- Strategy 2B: Ensure timely and
accurate(appropriate) diagnosis.- Develop consensus on ADRD prevalence measurements and report diagnosis levels.
- Develop consensus on ADRD prevalence measurement.
- Gather and report ADRD diagnostic data.
- Raise public awareness of ADRD and encourage detection of cognitive impairment.
- Support awareness campaigns to increase understanding and encourage cognitive assessments.
- By 2018, 80% of 65+ believe ADRD is not normal sign of aging.
- By 2018, 80% of 65+ are comfortable discussing memory problems with provider.
- Activate faith- and community-based organizations to increase awareness and understanding.
- Support awareness campaigns to increase understanding and encourage cognitive assessments.
- Raise physician awareness, and equip physicians to detect, diagnosis, and disclose.
- Support education campaigns on timely detection, including on the Annual Wellness Visit.
- Encourage providers to have conversations/assessments in annual routine visits for those at risk.
- Modify reimbursement to ensure adequate time to assess impairment.
- Identify successful practices with AWV and evaluate approaches to increase participattion.
- Issue CMS subregulatory guidance on assessment tools to be used in AWV.
- Evaluate/develop guidelines for populations more likely to require specialists to diagnose.
- Equip and require physicians to disclose status in cases of clinically consequential impairment.
- Incorporate cognitive changes, diagnostic information, and caregivers into electronic health record.
- Record all cognitive changes, diagnostic information, and caregivers in all patient medical records.
- Develop consensus on ADRD prevalence measurements and report diagnosis levels.
- Strategy 2B: Ensure timely and
accurate(appropriate) diagnosis.- Develop consensus on ADRD prevalence measurements and report diagnosis levels.
- Develop consensus on ADRD prevalence measurement.
- Gather and report ADRD diagnostic data.
- Raise public awareness of ADRD and encourage detection of cognitive impairment.
- Support awareness campaigns to increase understanding and encourage cognitive assessments.
- Activate faith- and community-based organizations to increase awareness and understanding.
- Raise physician awareness, and equip physicians to detect, diagnosis, and disclose.
- Support education campaigns on timely detection, including on the Annual Wellness Visit.
- By 2018, 70% of physicians are knowledgeable on importance of detection, diagnosis, and disclosure.
- By 2022, 90%.
- Encourage providers to have conversations/assessments in annual routine visits for those at risk.
- Modify reimbursement to ensure adequate time to assess impairment.
- Identify successful practices with AWV and evaluate approaches to increase participattion.
- Issue CMS subregulatory guidance on assessment tools to be used in AWV.
- Evaluate/develop guidelines for populations more likely to require specialists to diagnose.
- Equip and require physicians to disclose status in cases of clinically consequential impairment.
- Incorporate cognitive changes, diagnostic information, and caregivers into electronic health record.
- Record all cognitive changes, diagnostic information, and caregivers in all patient medical records.
- Support education campaigns on timely detection, including on the Annual Wellness Visit.
- Develop consensus on ADRD prevalence measurements and report diagnosis levels.
- Strategy 2B: Ensure timely and
accurate(appropriate) diagnosis.- Develop consensus on ADRD prevalence measurements and report diagnosis levels.
- Develop consensus on ADRD prevalence measurement.
- Gather and report ADRD diagnostic data.
- Raise public awareness of ADRD and encourage detection of cognitive impairment.
- Support awareness campaigns to increase understanding and encourage cognitive assessments.
- Activate faith- and community-based organizations to increase awareness and understanding.
- Raise physician awareness, and equip physicians to detect, diagnosis, and disclose.
- Support education campaigns on timely detection, including on the Annual Wellness Visit.
- Encourage providers to have conversations/assessments in annual routine visits for those at risk.
- Modify reimbursement to ensure adequate time to assess impairment.
- Identify successful practices with AWV and evaluate approaches to increase participattion.
- Issue CMS subregulatory guidance on assessment tools to be used in AWV.
- Evaluate/develop guidelines for populations more likely to require specialists to diagnose.
- Equip and require physicians to disclose status in cases of clinically consequential impairment.
- By 2020, 38% of those diagnosed, or their caregivers, are aware of the diagnosis (consistent with Healthy People 2020).
- By 2025, 80%.
- Incorporate cognitive changes, diagnostic information, and caregivers into electronic health record.
- Record all cognitive changes, diagnostic information, and caregivers in all patient medical records.
- Develop consensus on ADRD prevalence measurements and report diagnosis levels.
- Strategy 2E. Explore the effectiveness of new models of care for people with AD.
- Identify state of science and develop a research road map regarding best practices.
- SHORT-TERM: Build coalition of cross-disciplinary experts to convene at a research summit on ADRD care and support.
- SHORT-TERM: Release public report on ADRD care and support evidence-based interventions.
- Convene group annually to review most current ADRD care and support research.
- Ensure geriatric research on general medical conditions incorporates persons with ADRD.
- Provide ADRD Care and Support interventions research funding, informed by Annual Summit.
- Identify state of science and develop a research road map regarding best practices.
- MEDIUM-TERM: Identify and evaluate quality outcomes and cost effectiveness of interventions.
- MEDIUM-TERM: Provide funding for community-based pragmatic and adaptive research methods in interventions.
- MEDIUM-TERM: Provide funding to stimulate and support innovative learning for new models of care for persons with ADRD.
- MEDIUM-TERM: Provide funding for ADRD care and support translation studies.
- MEDIUM-TERM: Provide funding for comparative effectiveness studies to identify most effective supportive interventions.
- LONG-TERM: Provide funding to roll out interventions proven effective, and adaptive throughout community settings.
|
Strategy 3D. Maintain the dignity, safety and rights of people with AD. |
|
|
[REVISED] Strategy 3D. Maintain the dignity and rights of people with AD. |
[NEW] Strategy 3F. Support communities that are inclusive and safe for persons with ADRD. |
|
Ensure legal, financial, and social services are equipped to serve and protect persons with ADRD. [8 milestones] |
Ensure persons with ADRD are safe and cared for in emergency situations. [5 milestones] |
|
Reduce inappropriate use of antipsychotic and other psychotropic drugs for persons with ADRD in home, community, and institutional based settings. [3 milestones] |
Ensure local community members who come in contact with persons with ADRD receive basic dementia training. [2 milestones] |
|
Provide funding for community development and scale up of evidence-based meaningful activities for persons with ADRD. [1 milestone] |
Ensure safe transportation options for persons with ADRD. [2 milestones] |
QUESTIONS?