
Monday, August 1, 2016
The UCLA Alzheimer's and Dementia Care program
Lee A. Jennings, MD, MSHS--Evaluator
Zaldy Tan, MD--Medical Director
David B. Reuben, MD--Program Director
The UCLA Alzheimer's and Dementia Care Program
- Clinical program with goals:
- Maximize patient function, independence, & dignity
- Minimize caregiver strain
- Reduce unnecessary costs
- Began in 2011 with philanthropic funds
- Planned 250 patients
- Round 1 CMMI Award July 2012--Dec 2015
- To expand the program to 1,000 patients
- Today, over 1800 patients enrolled
- Approaches the patient and caregiver as a dyad; both need support
- Recognizes that this care is a long journey
- Provides comprehensive care based in the health system that reaches into the community
- Uses a co-management model with Nurse Practitioner Dementia Care Manager (DCM) who does not assume primary care of patient
- Works with physicians to care for patients by
- Conducting in-person needs assessments
- Developing and implementing individualized dementia care plans
- Monitoring response and revising as needed
- Providing access 24 hours/day, 365 days a year
Patients
- Must have diagnosis of dementia
- Live outside nursing home
- Must have a referring/partnering UCLA physician
Community-based Organization (CBO) Services
- Direct services to patients and families
- Adult day care
- Counseling
- Case management
- Legal and financial advice
- Workforce development focusing on training family and caregivers
- Paid for using voucher system
Enrollment to Date (7/20/16)
- Patients enrolled: 1,825
- Referrals waiting to be seen: 125
- 1-year follow-ups conducted: 722
- 2-year follow-ups conducted: 309
- 3-year follow-ups conducted: 52
Patients in the Program
- Mean age 82; 66% female
- Diagnosis
- Alzheimer's disease: 35%
- Lewy-Body: 4%
- Vascular: 4%
- Other, mixed or unknown: 53%
- Mean MMSE score 17.4
- Caregiver: 34% spouse, 54% child
- Dually insured 18%
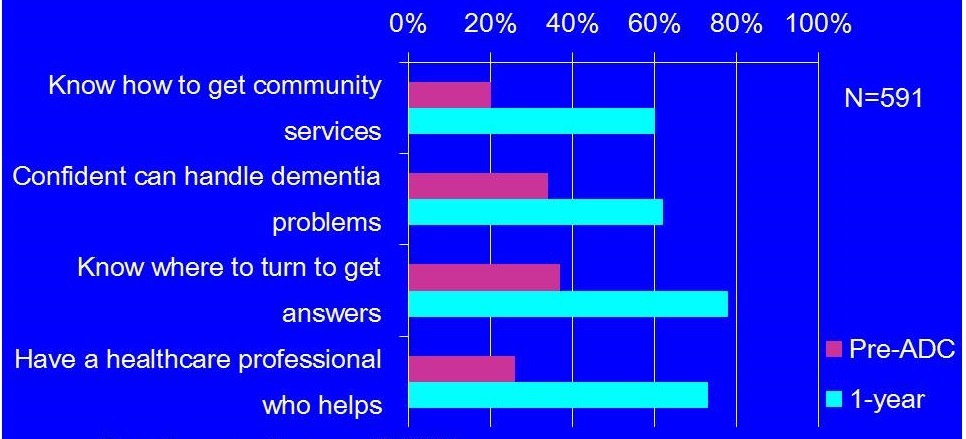
Caregivers at Baseline
- Depression & strain
- 14% mod/sev depressive sx
- 36% high stress
- Low self-efficacy
- 21% knew how to access services
- 36% confident handling dementia problems
- 26% have healthcare professional who helps work through dementia issues
Services Provided
- Support group referral: 84%
- Caregiver training: 75%
- Refer to CBO: 56%
- Recommend additional evaluation: 25%
- Adjust medication: 16%
- POLST: 20%
Caregiver Satisfaction
- 90% felt the intake visit was time well spent
- 91% felt concerns listened to and addressed
- 92% would recommend the program to others
Physician Satisfaction
- Valuable medical recommendations: 61%
- Valuable behavioral recommendations: 85%
- Enhanced MD relationship with patient: 68%
- Saved MD time: 56%
- Would recommend for other patients: 90%
Overall Dementia Quality of Care (ACOVE-3 and PCPI QIs)*
- Community-based physicians 38%
- Community-based physicians & NP 60%
- UCLA Alzheimer's and Dementia Care 92%
* Based on medical record abstraction
Jennings LA, et al. J Am Geriatr Soc, Jun 2016. PMID: 27355394
1-year Changes in Caregiver Experience and Self-efficacy
 |
1-year Outcomes: Patients
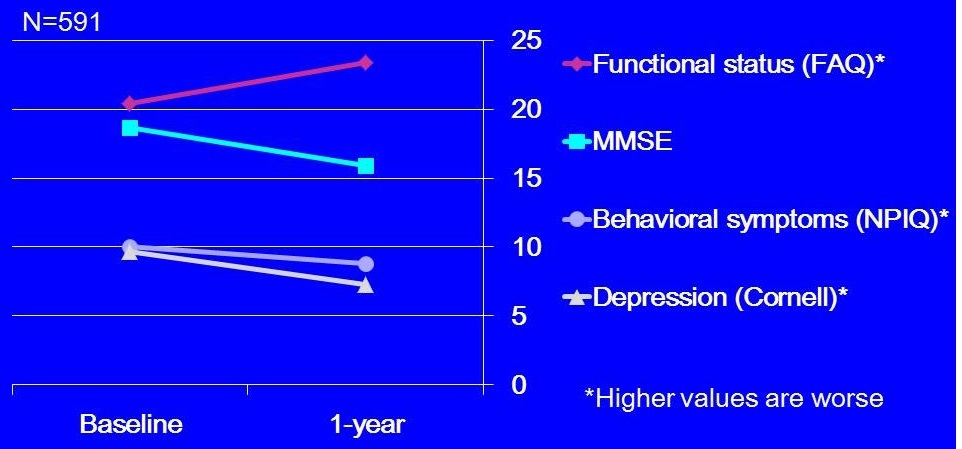 |
| For all baseline and year 1 comparisons, p<0.001. |
2-year Outcomes: Patients
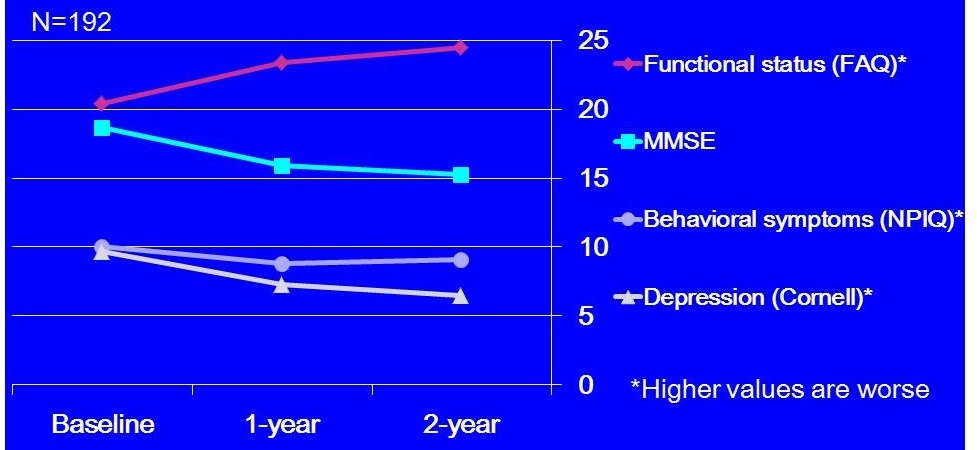 |
| For all baseline and year 2 comparisons, p<0.001, except behavioral symptoms, p=0.07. |
1-year Outcomes: Caregivers
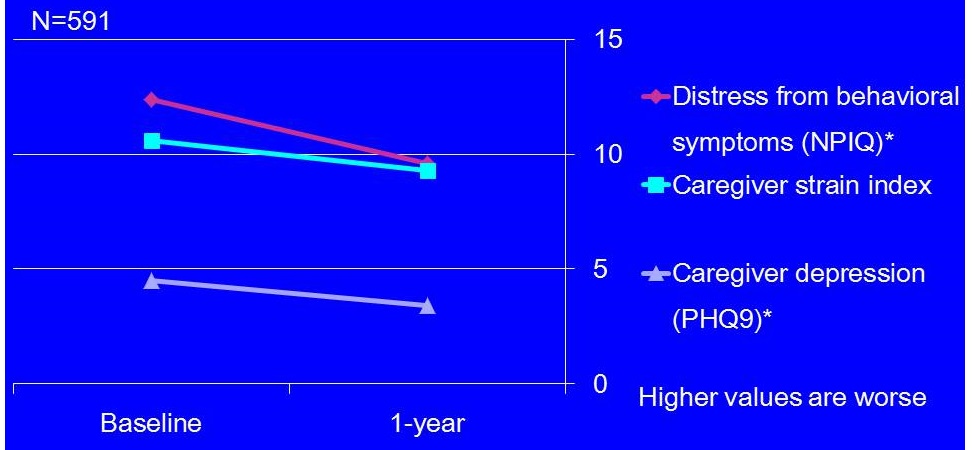 |
| For all baseline and year 1 comparisons, p<0.001. |
2-year Outcomes: Caregivers
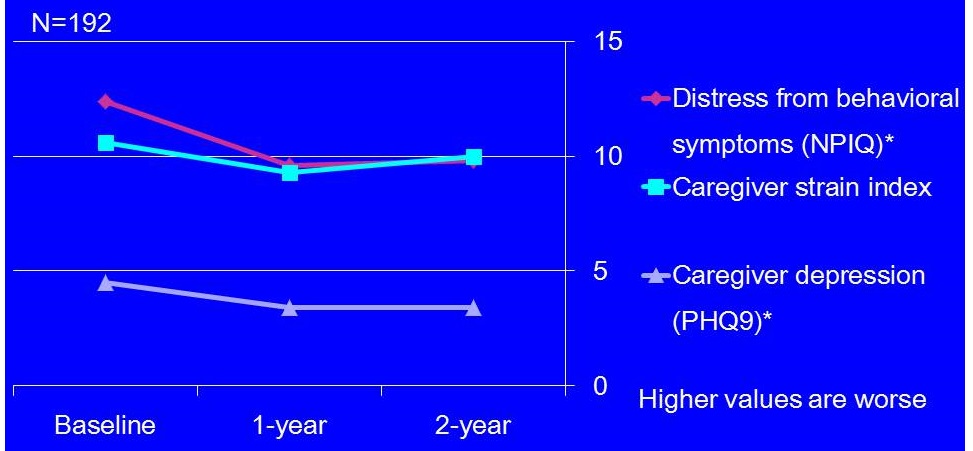 |
| *Baseline and year 2 comparisons, p<0.01. |
Spinoffs
- Infrastructure
- Dementia Care Management Software
- Website with caregiver training videos and webinars (http://dementia.uclahealth.org)
- Enhanced support for caregivers
- I-CareD (personalized caregiver training program)
- TIMEOUT@UCLA (student respite program)
- Support Groups (English, Spanish, Early Onset, FTD, and Lewy Body)
Goals for the Future
- Sustaining the program
- Increasing the number served
- Enhancing services
- Disseminating the model
Costs of Program (per 1250 participants)
- 5 FTE Nurse Practitioner DCMs
- 2 FTE DCM Assistants
- 0.5 FTE Medical Director
- 1 FTE Program Administrator
- 0.15 FTE Psychologist Support Group Leader
- Software maintenance and supplies
- Vouchers for community-based organizations
Comparative Costs of Program
| UCLA ADC | $1400/y | ($4/d) |
|---|---|---|
| Donepezil (generic) | $2190/y | ($6/d) |
| Memantine | $2880/y | ($8/d) |
| Donepezil & Memantine | $5070/y | ($14/d) |
Current Business Model
- Bill for Medicare-allowed services (3%)
- All other services free of charge
- Care coordination with PCPs and CBOs
- Telephone follow-up
- Support groups
- Education
- Some institutional support, both in-kind and short-term funds (29%)
- Ongoing grants and philanthropy (68%)
Barriers to Dissemination
- Current Medicare coverage for program
- For in-person visits, nurse practitioners are reimbursed 85% of what physicians are paid
- For all clinical work that is not in-person, there is no reimbursement
- No coverage for CBO services
- Shortage of qualified nurse practitioners
In Summary
- UCLA ADC Program proof of concept
- Bringing program to scale
- Longitudinal, co-management model
- Patients and doctors like it
- Filling a gap in care
- Improving outcomes for patients and caregivers
- But no current economic model under Medicare
Files
Document
Mtg21-Slides2.pdf (pdf, 1.92 MB)