
November 2019
Printer Friendly Version in PDF Format (37 PDF pages)
ABSTRACT
The objective of this environmental scan is to summarize the peer-reviewed and grey literature on oversight of residential care for mental health and substance use care in the United States, excluding inpatient hospital care. The scan provides a framework for defining residential treatment services, summarizes who is treated in residential care, and outlines current policy issues relevant to regulation and oversight of residential treatment for behavioral health conditions (e.g., placement criteria, provision of evidence-based care, quality issues).
This report was prepared under contract #HHSP233201600023I between HHS's ASPE/DALTCP and Truven Health Analytics, Inc. For additional information about this subject, you can visit the DALTCP home page at https://aspe.hhs.gov/office-disability-aging-and-long-term-care-policy-daltcp or contact the ASPE Project Officers, Judith Dey and JoelDubenitz, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201; Judith.Dey@hhs.gov, Joel.Dubenitz@hhs.gov.
DISCLAIMER: The opinions and views expressed in this report are those of the authors. They do not reflect the views of the Department of Health and Human Services, the contractor or any other funding organization. This report was completed and submitted on April 24, 2019.
TABLE OF CONTENTS
- Historical Framework for Mental Health and Substance Use Disorder Residential Treatment
RESIDENTIAL TREATMENT FOR MENTAL AND SUBSTANCE USE DISORDER
- Residential Mental Health and Substance Use Disorder Treatment
THE LANDSCAPE OF RESIDENTIAL MENTAL HEALTH SERVICES IN THE UNITED STATES
- Facilities and Payers
- Oversight and Accreditation
- Assessment and Placement Criteria
- Population Treated and Care Provided
THE LANDSCAPE OF RESIDENTIAL SUBSTANCE USE SERVICES IN THE UNITED STATES
- Facilities and Payers
- Oversight and Accreditation
- Assessment and Placement Criteria
- Population Treated and Care Provided
- Research on Quality of Residential Treatment
- Quality of Residential Treatment in the Grey Literature and Popular Press
REGULATION OF RESIDENTIAL MENTAL HEALTH AND SUBSTANCE USE FACILITIES
- Current Status of Regulation
- Potential Regulatory Levers
LIST OF FIGURES
- FIGURE 1a: Mental Health Residential Treatment Programs' Profit Status
- FIGURE 1b: Mental Health Residential Treatment Programs' Payment Source
- FIGURE 2a: Licensing of Mental Health Residential Facilities
- FIGURE 2b: Accreditation of Mental Health Residential Facilities
- FIGURE 3: Mental Health Residential Facilities with Programs for Special Populations
- FIGURE 4a: Residential SUD Treatment Programs Profit Status
- FIGURE 4b: Residential SUD Treatment Programs Payment Source
- FIGURE 5a: Licensing of Residential SUD Treatment Programs
- FIGURE 5b: Accreditation of Residential SUD Treatment Programs
- FIGURE 6: Point Prevalence of Residential Treatment by Type of Residential Care
- FIGURE 7: SUD Residential Treatment Programs with Specialized Programming
- FIGURE 8: Residential SUD Facilities Offering Medications for SUD
ACKNOWLEDGMENTS
This report was generated in collaboration with colleagues at the Institute for Behavioral Health at the Schneider Institutes for Health Policy, Brandeis University.
We are indebted to input from Lindsey Browning from the National Association of Medicaid Directors, Pamela Greenberg from the National Association of Behavioral Health and Wellness, Dr. Joe Parks from the National Council for Behavioral Health, Ted Lutterman from NRI, and Melanie Witter and Rick Harwood from the National Association of State Alcohol and Drug Abuse Directors.
ACRONYMS
The following acronyms are mentioned in this report.
| AIDS | Acquired Immune Deficiency Syndrome |
|---|---|
| ASAM | American Society of Addiction Medicine |
| AUD | Alcohol Use Disorder |
| CARF | Commission on the Accreditation of Rehabilitation Facilities |
| CMS | Centers for Medicare & Medicaid Services |
| COA | Council on Accreditation |
| DMH | Department of Mental Health |
| DPH | Department of Public Health |
| HIV | Human Immunodeficiency Virus |
| IMD | Institutions for Mental Disease |
| LGBT | Lesbian, Gay, Bisexual, Transgender |
| LOCUS | Level Of Care Utilization System |
| N-MHSS | National Mental Health Services Survey |
| N-SSATS | National Survey of Substance Abuse Treatment Services |
| NASADAD | National Association of State Alcohol and Drug Abuse Directors |
| OTP | Opioid Treatment Program |
| OUD | Opioid Use Disorder |
| PTSD | Post-Traumatic Stress Disorder |
| SMI | Serious Mental Illness |
| SUD | Substance Use Disorder |
| TBI | Traumatic Brain Injury |
| TEDS | Treatment Episode Data Set |
| TJC | The Joint Commission |
EXECUTIVE SUMMARY
Objectives
The objective of this environmental scan is to summarize the peer-reviewed and grey literature on oversight of residential care for mental health and substance use care in the United States, excluding inpatient hospital care. The scan provides a framework for defining residential treatment services, summarizes who is treated in residential care, and outlines current policy issues relevant to regulation and oversight of residential treatment for behavioral health conditions (e.g., placement criteria, provision of evidence-based care, quality issues).
Methods
This scan considers adult residential care broadly but excludes facilities for those under age 18 years or over age 64 years, criminal justice facilities, and facilities specific to intellectual or developmental disabilities, except to the extent that they are combined with facilities providing residential care for persons with a mental health or substance use disorder (SUD). Information for this report is obtained from national surveys (e.g., National Mental Health Services Survey [N-MHSS], National Survey of Substance Abuse Treatment Services [N-SSATS]), English-language peer-reviewed and grey literature, and subject matter experts.
The literature search focused on the past 5 years, 2014-2018; however, we also included seminal papers and reports that were published prior to 2014 if subject matter experts identified them as key. We found peer-reviewed literature through systematic key word searches conducted using databases such as PubMed, PsycINFO, and Google Scholar. Grey literature was identified through key word searches and conversations with subject matter experts. To fill gaps in the published and grey literature, we solicited feedback through discussions with five subject matter experts. Subject matter experts from NRI and the National Association of State Alcohol and Drug Abuse Directors also reviewed and provided feedback on the outline and the final draft of the environmental scan.
Findings
Residential care is a setting for services rather than a specific type of treatment. A wide variety of residential settings for mental health and substance use disorders exists, but not all of these can be considered residential treatment. For SUD, residential settings include residential substance use treatment programs, group homes, halfway houses, detoxification, transitional living arrangements, and sober living communities. For mental health conditions, residential settings range from specialty residential treatment settings, to group homes, to community-based supportive housing. Key features of residential treatment include the provision of a range of 24-hour treatment and support services in a structured living environment for individuals who need support before living on their own. Payment for residential care is generally through public or private insurance, out-of-pocket, or public funds. Reimbursement policies may affect the delivery and oversight of residential treatment through requirements the payers place on providers.
Residential mental health treatment. In 2017, there were approximately 856 organizations providing residential mental health treatment for adults in the United States, according to the Substance Abuse and Mental Health Services Administration's N-MHSS. Most are licensed by state departments of health or departments of mental health. Some also are licensed by state substance use agencies.
Mental health care exists on a continuum in which individuals move from higher to lower levels of care. Determinations about the appropriate level of care are made by clinicians in either referring or receiving institutions, depending on where the individual is coming from, and either are reviewed or repeated by payers. The mental health field does not have a universally accepted assessment tool; instead, payers may use purchased or self-developed tools.
The range of conditions addressed in residential mental health facilities is broad, with most offering services for individuals with serious mental illness and many for co-occurring conditions. In the 2017 N-MHSS, 80% of adult residential treatment facilities offered psychotropic medications, 65% offered group psychotherapy, 60% offered individual psychotherapy, and 58% offered cognitive behavioral therapy.[1] States also identify different target or priority populations on which they may wish to focus treatment resources, for example pregnant and parenting women or homeless individuals. Specific information on the delivery of evidence-based services in residential mental health care is limited. Trauma-informed care is an evidence-based service for mental health conditions that could be used in residential programs.
Residential SUD treatment. Residential treatment for SUD is defined as nonhospital services that are short-term (30 days or less), long-term (more than 30 days), and/or detoxification-focused (i.e., withdrawal management). According to the 2017 N-SSATS, approximately 3,125 organizations are providing residential substance use treatment in the United States. Most residential substance use facilities are licensed by their state substance use agency. Unlike mental health services, substance use treatment has a commonly used set of assessment and placement criteria. The American Society of Addiction Medicine has established criteria for placement, continued stay, and transfer/discharge of patients with addiction and co-occurring conditions, including levels of care that encompass residential treatment. Residential substance use treatment programs provide a range of services and programming for patients. Many programs offer specialized services tailored for individuals with certain characteristics. Evidence-based practices delivered in residential SUD treatment may include motivational interviewing, cognitive behavioral therapy, and pharmacotherapy (or medication assisted treatment). Three medications--buprenorphine, naltrexone, and methadone--are evidence-based treatments for opioid use disorder, and naltrexone is also an effective treatment for alcohol use disorder.
Quality of residential treatment. Studies of the effectiveness of residential mental health and SUD treatment are limited. Our search did not identify any rigorous peer-reviewed studies of the effectiveness of residential treatment programs in the past 5 years. Not only is there a lack of data or research regarding residential mental health and SUD treatment, especially patient experience and outcomes, but psychiatric and SUD patients are systematically excluded from efforts that target hospital-based care (e.g., inpatient psychiatric hospitalization).
Regulation. There is no current comprehensive compilation or analysis of state regulation of residential treatment facilities for adults in the United States. Beyond requirements for licensure or certification, potential regulatory levers include staffing requirements, placement and assessment criteria, treatment and discharge planning, requirements for aftercare or follow-up services, use of evidence-based practices, and requirements related to quality improvement procedures. Care transitions are an important component of quality of care for patients in residential settings. Incorporating quality process and outcome measures in residential care oversight is also important. Medicaid directors increasingly are interested in assessing outcomes such as job placement, extent of criminal justice recidivism, and ability to live independently as indicators of successful residential treatment.
Conclusion
Individuals seeking residential mental health or substance use treatment are often vulnerable and in crisis. It is critical that all providers deliver high-quality, evidence-based services, and that quality residential treatment is available as part of the continuum of care.
INTRODUCTION
This environmental scan explores the regulation of adult residential care in the mental health and substance use disorder (SUD) systems. It examines the following key issues: defining residential treatment, quality monitoring and assurance, licensing and credentialing, facilities and payers, assessment and placement, provision of evidence-based care, and treated populations. As the mental health and SUD systems have advanced, treatment has shifted its focus to person-centered care that addresses the needs of the whole individual. However, due to differences in the patient populations and the evolution of the adult mental health and SUD systems, regulatory requirements frequently vary. In this scan, we first briefly trace the historical development of the two treatment systems. We then discuss the definition of and funding sources for residential treatment and describe the landscape of residential treatment systems separately for mental health and SUD. Last, we discuss key issues related to quality of care and other regulatory challenges in the behavioral health field.
Historical Framework for Mental Health and Substance Use Disorder Residential Treatment
Despite some recent attempts to integrate, the mental health and substance use treatment systems have historically been separate from each other and from the general medical care system.[2] These separations were due in part to institutionalization policies, regulatory structures, treatment needs, and stigma surrounding both mental health and substance use disorders (SUDs).[2] The ways in which mental health and SUD residential treatment developed as systems separate from each other and from the broader medical system are important to understand in examining the regulation of residential mental health and SUD treatment today. Although many regulatory challenges are shared across both fields, there are specific differences that stem from the different ways these treatment systems have developed.
Individuals with serious mental health conditions often were treated in institutional facilities and not in community settings until the 1960s, when the push for deinstitutionalization largely began. If individuals with mental health conditions needed more intensive help, they received short-term care within freestanding psychiatric hospitals or psychiatric units within general hospitals. Legal actions in response to the Olmstead rule have minimized the use of both inpatient and residential settings for individuals with mental illness. Today, the primary focus of the mental health field is on supporting individuals with mental health conditions living as independently as possible in their own communities, managing conditions, and improving quality of life.
SUDs historically were considered a personal failing rather than a chronic disease and were treated in a separate specialty substance use treatment system. Health insurance often did not cover SUD treatment; instead, individuals paid for care privately or relied on public funding to pay for services (block grant funds). Residential programs for SUDs were common, with 28-day residential treatment programs being one standard treatment option. Many SUD treatment programs were based on a 12-step philosophy and did not endorse medication treatment.[3] Prior to the mid-1970s, recovering individuals provided counseling services with minimal formal training. In the late 1970s, states and national associations established professional standards and credentialing processes. Advances in science now support the understanding that SUD is a chronic brain disease that can be treated and managed. Today, many evidence-based treatments for SUD are available, including motivational interviewing, trauma-informed care, recovery supports, and medications specific to opioid use disorders (OUDs) and alcohol use disorders (AUDs). Insurance coverage for behavioral health treatment was increased through the federal Mental Health Parity and Addiction Equity Act of 2008 and further expanded through the 2010 Patient Protection and Affordable Care Act.[4]
Many individuals have both mental health disorders and SUDs. Where these individuals are treated often depends on which condition is more severe or what kind of situation precipitates a particular crisis. All state-overseen SUD facilities, however, now screen each patient for mental health conditions at intake or early in the course of treatment and refer patients accordingly.[5]
RESIDENTIAL TREATMENT FOR MENTAL AND SUBSTANCE USE DISORDERS
Residential care is a setting for services rather than a specific type of treatment. A wide variety of residential settings for individuals with mental health conditions and SUD exist, but not all of these can be considered residential treatment. In theory, residential settings provide living environments but do not necessarily provide health services or treatment. In practice, it can sometimes be hard to differentiate between the two. For SUD, residential settings can include residential substance use treatment programs, group homes, halfway houses, detoxification, transitional living arrangements, and sober living communities. For mental health conditions, residential settings range from specialty and nonspecialty residential treatment settings, to group homes, to community-based supportive housing. Nursing homes are sometimes also included within the framework of residential settings for those with mental health conditions. More recently, residential mental health crisis centers and residential respite programs have been established in a number of states.
Residential treatment is less medically oriented than inpatient care. It has key features that include providing a range of 24-hour services in a structured living environment for individuals who need support for their mental health or substance use recovery before living on their own.[6] Most residential care is provided for limited periods of time with the goal of preparing people to move into the community and to a lower level of care. However, sober living communities or supportive housing, where individuals live in a group setting but receive treatment elsewhere, may entail living in that setting over an indefinite period of time.
Making a clear distinction between what counts as residential treatment and what is a residential setting is important clinically--the degree of clinical services available in a particular setting needs to be appropriate for a patient's required level of care. These distinctions are also important for payment determinations. Private health insurance may pay for residential treatment but will not pay for residential living situations. Medicaid programs pay for health care services delivered in some types of residential treatment programs but do not pay for living expenses. The institutions for mental disease (IMD) exclusion prohibits Medicaid payments for most care delivered in some psychiatric settings of more than 16 beds.[7] These payment distinctions are discussed in greater detail below.
Independent accreditation entities have created definitions and standards for residential treatment. One of these is The Joint Commission's (TJC's) Behavioral Health Survey and Accreditation Program, which defines a residential program as a "program that provides 24-hour care and services to individuals who need a less structured environment than that of an inpatient program and who are capable of self-preservation in the event of an emergency in the organization."[8]
The Commission on the Accreditation of Rehabilitation Facilities (CARF) includes more detail in its definition. It describes residential programs as follows:[9]
Funding Programs ... organized and staffed to provide both general and specialized nonhospital-based interdisciplinary services 24 hours a day, 7 days a week for persons with behavioral health or co-occurring needs, including intellectual or developmental disabilities. Residential treatment programs provide environments in which the persons served reside and receive services from personnel who are trained in the delivery of services for persons with behavioral health disorders or related problems.
These services are provided in a safe, trauma-informed, recovery-focused milieu designed to integrate the person served back into the community and living independently whenever possible. The program involves the family or other supports in services whenever possible. Residential treatment programs may include domestic violence treatment homes, nonhospital addiction treatment centers, intermediate care facilities, psychiatric treatment centers, or other nonmedical settings.
Residential Mental Health and Substance Use Disorder Treatment
Payment for residential treatment may come from out-of-pocket payments, private insurance, public funds, Medicare, or Medicaid (in institutions not subject to the IMD exclusion). The IMD exclusion to Medicaid reimbursement prevents the use of federal matching dollars for treatment in settings with more than 16 beds that primarily provide services to individuals with mental disorders, including SUDs.[10] This applies to Medicaid beneficiaries between the ages of 21 and 64 years[11] and pertains to both residential and specialty psychiatric or SUD inpatient settings. States are able to avoid the IMD exclusion and use Medicaid funds to pay for care in IMDs through: (1) use of Section 1115 waivers whereby states may apply to use federal funds for services in an IMD; (2) changes to managed care rules allowing Medicaid managed care plans to pay for treatment in an IMD "in lieu of" more expensive state plan services (e.g., care in an acute general hospital setting) for no more than 15 days in a calendar month and no more than 30 days over 2 months; and (3) use of disproportionate share hospital payments to hospitals for uncompensated care costs.[7, 10, 12]
In recent years, waivers from the IMD exclusion have increasingly been allowed for SUD treatment; the Centers for Medicare & Medicaid Services (CMS) is interested in ensuring states can offer the full continuum of SUD treatment services, including residential care. Although fewer waivers historically have been approved for mental illness, CMS recently released an opportunity for 1115 waivers to expand residential treatment for serious mental health conditions in IMDs.[13] As of June 2018, 11 states had an approved waiver of the IMD exclusion for SUD treatment alone, one state had an approved waiver for both mental health and SUD, 12 states had pending waiver requests for SUD alone, four had pending requests for both, and one state with an existing waiver was seeking expanded authority.[12] In addition to formal mechanisms to waive the IMD exclusion, states have other strategies to fund care for Medicaid beneficiaries including using small facilities with 16 or fewer beds, or using state-only funds.[14] Key informants for this report noted building multiple facilities with 16 or fewer beds may lead to an inefficient use of resources.
In addition to the three mechanisms discussed above for waiving the IMD exclusion, the Substance Use Disorder Prevention That Promotes Opioid Recovery and Treatment for Patients and Communities Act changed the law to allow the use of federal Medicaid funds for services in IMDs by creating a state option from October 1, 2019, to September 30, 2023. This state option allows Medicaid to cover residential treatment in an IMD up to 30 days in a year for individuals with a SUD. The Act also codifies regulations allowing Medicaid funds for managed care capitation payments that include IMD services up to 15 days per month.[15]
State Medicaid regulations or state Medicaid program reimbursement policies also may affect the delivery and oversight of residential treatment.[16] Similarly, private payers or states using block grant funds may impose requirements on providers as a condition of reimbursement or funding. For example, payers may require some level of nurse staffing for residential care to be reimbursable.[17] Block grant funding may impose specific requirements that concern pregnant or parenting women in SUD treatment or staff training requirements, or there may be other requirements that are state initiated as part of individual block grant applications.[18] According to our key informants, SUD programs also may be required to collect and report data about patients at intake and termination including measures indicative of outcomes.
THE LANDSCAPE OF RESIDENTIAL MENTAL HEALTH SERVICES IN THE UNITED STATES
Facilities and Payers
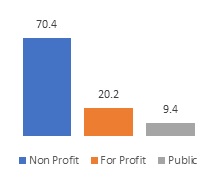
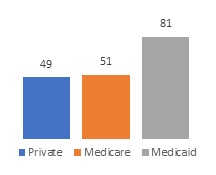
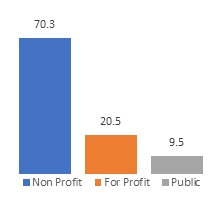
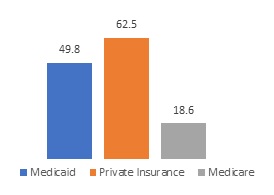
In 2017, there were approximately 856 organizations providing residential mental health treatment for adults in the United States, according to the Substance Abuse and Mental Health Services Administration's National Mental Health Services Survey (N-MHSS). The N-MHSS also includes a subset of other types of facilities that offer residential treatment as part of their treatment milieu and may or may not provide services to children. For the purposes of this environmental scan, we include only those centers that are explicitly defined in the N-MHSS as adult residential treatment centers. The N-MHSS defines such settings as "facilities not licensed as psychiatric hospitals that primarily provide individually planned programs of mental health treatment in a residential care setting for adults."[19] More than 80% of these facilities provided only mental health services, whereas 19% also provided substance use services. Most facilities were nonprofit and accepted Medicaid payments (Figure 1a and Figure 1b).[20] For-profit organizations were more likely to accept private health insurance, with 61% indicating they accept private insurance compared with 45% of nonprofits and 58% of public organizations. There was no difference by ownership in acceptance of Medicaid.[20] Private insurance generally covers residential treatment, but a national survey of private health plans found 9% nationally exclude coverage for residential treatment for mental health.[21]
| FIGURE 1a. Mental Health Residential Treatment Programs' Profit Status, % | FIGURE 1b. Mental Health Residential Treatment Programs' Payment Source, %a |
|---|---|
 |
 |
SOURCE: Authors' analysis of Substance Abuse and Mental Health Services Administration. National Mental Health Services Survey (N-MHSS): 2017. Data on Mental Health Treatment Facilities. 2018. https://www.samhsa.gov/data/sites/default/files/cbhsq-reports/2017_National_Mental_Health_Services_Survey.pdf.
|
|
Oversight and Accreditation
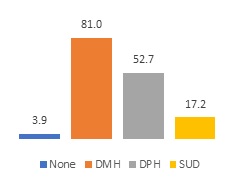
Regulation of residential mental health facilities varies by state, and facilities may be licensed by more than one state department, including departments specific to behavioral or mental health and departments that oversee health care facilities generally. Most are licensed by state departments of health or departments of mental health (Figure 2a). Some also are licensed by state substance use agencies. Mental health and SUD state authorities were traditionally separate, although they have now merged into a single agency in 40 states. It is not clear, however, what this means in terms of integration of licensing and regulations, which vary dramatically within this group. Many single state authorities have retained dual regulatory structures for the two systems. Licensing generally involves requiring facilities to adhere to a variety of standards regarding structural and process dimensions of safety, such as staffing composition and levels, limiting the use of restraint and seclusion, upholding patients' rights, and monitoring quality. These standards generally are enforced by inspections, which could be unannounced or announced, scheduled for regular intervals, or provoked by complaints received by the regulatory authority.
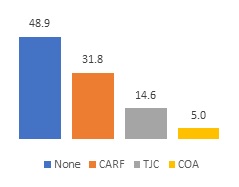
| FIGURE 2a. Licensing of Mental Health Residential Facilities, % | FIGURE 2b. Accreditation of Mental Health Residential Facilities, % |
|---|---|
 |
 |
| SOURCE: Authors' analysis of Substance Abuse and Mental Health Services Administration. National Mental Health Services Survey (N-MHSS): 2017. Data on Mental Health Treatment Facilities. 2018. https://www.samhsa.gov/data/sites/default/files/cbhsq-reports/2017_National_Mental_Health_Services_Survey.pdf. | |
However, little research has been conducted about how residential mental health facilities are licensed in each state and to what extent requirements and standards vary among states. In addition to state regulation and licensure requirements, there are private entities that accredit residential facilities providing treatment. About half of all surveyed mental health residential facilities are accredited by TJC, CARF, or the Council on Accreditation (COA) (Figure 2b). These mechanisms of accreditation provide considerable guidance as to what is quality treatment, often in greater detail than may be found in state regulations. In some states, regulations provide "deemed" status, whereby accreditation by one of these bodies is considered sufficient to satisfy at least a part of state licensure requirements.
Assessment and Placement Criteria
Mental health care exists on a continuum in which individuals move from higher to lower levels of care. Determinations about the appropriate level of care are made by clinicians in either referring or receiving institutions, depending on where the individual is coming from, and either are reviewed or repeated by payers. The mental health field does not have a universally accepted assessment tool; instead, payers may use purchased or self-developed tools.
One tool that is used by at least 16 states, and mentioned in CMS guidance,[13] is the Level Of Care Utilization System (LOCUS). Designed by the American Association of Community Psychiatrists and available only from Deerfield Solutions,[22] this tool considers six levels of care ranging from least intense (recovery maintenance) to most intense (inpatient hospital). Individuals are scored in six domains: Risk of Harm; Functional Status; Medical, Addictive, and Psychiatric Co-morbidity; Recovery Environment; Treatment and Recovery History; and Engagement and Recovery Status. Scores across the domains are used to determine appropriate placement within the continuum of care.
Population Treated and Care Provided
Residential mental health facilities treat individuals who have mental health conditions or behaviors that seriously interfere with their daily functioning. This is a population that also often experiences housing instability. The range of conditions addressed in residential mental health facilities is broad, and states also identify different target or priority populations on which they may wish to focus treatment resources, for example pregnant and parenting women or homeless individuals.
Medications and psychotherapy are provided in most, but not all, residential treatment facilities. Specifically, in the 2017 N-MHSS, 80% of adult residential treatment facilities offered psychotropic medications, 65% offered group psychotherapy, 60% offered individual psychotherapy and 57% offered activity therapy. Some facilities provide cognitive behavioral therapy (58%), integrated dual-disorders treatment (44%), trauma therapy (36%), and dialectical behavior therapy (31%).[1]
There is some evidence that different population groups respond differently to residential treatment, indicating that specialized programs for these groups might be more effective. For example, a study of gender difference in retention in residential treatment among individuals with co-occurring mental health conditions and SUD showed women were more likely to have longer retention than men; this finding suggests that efforts may be needed to improve men's retention in treatment.[23]
Most residential mental health facilities report offering programs for individuals with serious mental illness (SMI). Figure 3 shows other types of specialized programs offered in some facilities. A review of literature identified a lack of residential treatment programs for individuals with co-occurring substance use and mental health conditions as a barrier for that population to access care.[24]
| FIGURE 3. Mental Health Residential Facilities with Programs for Special Populations, % |
|---|
 |
| SOURCE: Authors' analysis of Substance Abuse and Mental Health Services Administration. National Mental Health Services Survey (N-MHSS): 2017. Data on Mental Health Treatment Facilities. 2018. https://www.samhsa.gov/data/sites/default/files/cbhsq-reports/2017_National_Mental_Health_Services_Survey.pdf. NOTE: Facilities can select multiple responses, so these categories are not mutually exclusive. |
Information on the delivery of evidence-based services in residential mental health care is limited. Trauma-informed care is an evidence-based service for mental health conditions that could be used in residential programs. TJC includes trauma-informed care in its standards, and CARF includes a reference to trauma-informed care in its definition of residential care and may require it for accreditation. Evidence-based practices that might be used in residential facilities for mental health conditions vary on the basis of condition and can include dialectical behavior therapy for borderline personality or other disorders and several that focus on post-traumatic stress disorder (PTSD). Requirements for use of specific evidence-based services are more common in mental health residential treatment programs that specialize in specific conditions. Specialty treatment programs are usually private residential treatment programs for specific disorders, such as eating disorders. The residential treatment system also includes facilities for sex offenders, and in 2016 almost 30% of patients receiving mental health residential treatment services had involuntary legal status.[25]
THE LANDSCAPE OF RESIDENTIAL SUBSTANCE USE SERVICES IN THE UNITED STATES
Facilities and Payers
The National Survey of Substance Abuse Treatment Services (N-SSATS) is conducted annually to gather information from all substance use facilities in the United States, including those regulated by states as well as facilities that are not licensed or otherwise approved by states. The N-SSATS excludes facilities only for incarcerated individuals and halfway houses that do not provide treatment services.[26] The survey is voluntary and in 2017 had a response rate of 89%. For the 2017 N-SSATS, residential treatment was defined as nonhospital services that are short-term (30 days or less), long-term (more than 30 days), and/or detoxification-focused (i.e., withdrawal management). According to the 2017 N-SSATS, approximately 3,125 organizations are providing residential substance use treatment in the United States.[27] Most residential SUD treatment facilities are nonprofit (Figure 4a).
| FIGURE 4a. Residential SUD Treatment Programs Profit Status, % | FIGURE 4b. Residential SUD Treatment Programs Payment Source, % accepting |
|---|---|
 |
 |
| SOURCE: Authors' analysis of Substance Abuse and Mental Health Services Administration. National Survey of Substance Abuse Treatment Services (N-SSATS): 2017. Data on Substance Abuse Treatment Facilities. 2018. https://www.samhsa.gov/data/sites/default/files/cbhsq-reports/2017_NSSATS.pdf. NOTE: In Figure 4b, facilities can select multiple responses, so these categories are not mutually exclusive. |
|
About half accept Medicaid, and more than 60% accept private insurance (Figure 4b). Over the past decade, there has been a shift from private nonprofit to private for-profit SUD residential treatment.[27] For-profit programs are more likely to accept private insurance. Few residential SUD treatment programs operate within hospitals, whereas about 28% of facilities identify as halfway houses, which are generally considered supervised living environments rather than treatment facilities. Among all residential substance use facilities, about 23% of these facilities have fewer than 13 residential beds, 59% of facilities have more than 18 residential beds, and 18% have 48 or more residential beds.[27]
Oversight and Accreditation
Most residential substance use facilities are licensed by their state substance use agency, which may or may not be independent of the agency overseeing mental health treatment. In some states, the department of health or mental health is responsible for licensing either in addition to or instead of the substance use agency (Figure 5a).
| FIGURE 5a. Licensing of Residential SUD Treatment Programs, % | FIGURE 5b. Accreditation of Residential SUD Treatment Programs, % |
|---|---|
 |
 |
| SOURCE: Authors' analysis of Substance Abuse and Mental Health Services Administration. National Survey of Substance Abuse Treatment Services (N-SSATS): 2017. Data on Substance Abuse Treatment Facilities. 2018. https://www.samhsa.gov/data/sites/default/files/cbhsq-reports/2017_NSSATS.pdf. | |
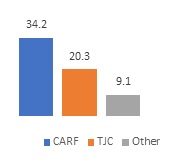
In addition, private entities including CARF and TJC offer accreditation programs for SUD treatment facilities. In addition, COA, the Health Care Facilities Accreditation Program, and other national, state, and local organizations provide accreditation.[27] However, only about half of residential substance use treatment facilities surveyed in N-SSATS indicated that they are accredited, with CARF being the most common source (Figure 5b). For-profit organizations were more likely to be accredited, with nearly 70% of facilities accredited compared with 50% of nonprofits and 60% of government-owned facilities.
A 2013 National Association of State Alcohol and Drug Abuse Directors (NASADAD) report identified the subset of states then providing "deemed" status to SUD facilities that were accredited or that held licensure from alternative entities: TJC (18 states), CARF (15 states), COA (ten states), or another entity (eight states).[28] However, these requirements were not identified as pertaining specifically to residential facilities.[28] An updated review of state regulations will identify states currently allowing deemed status for both SUD and psychiatric residential treatment. It also will capture instances in which states subsequently may have incorporated American Society of Addiction Medicine (ASAM) criteria into their regulatory structure, a process most likely to have occurred in states with recent Section 1115 SUD waivers (i.e., California, Indiana, Illinois, Kentucky, Louisiana, Maryland, Massachusetts, New Jersey, Utah, Vermont, Virginia, and West Virginia).[12]
Assessment and Placement Criteria
ASAM has established and widely-used criteria for placement, continued stay, and transfer/discharge of patients with addiction and co-occurring conditions, including levels of care that encompass residential treatment.[29] These criteria are designed to ensure patients are placed in the appropriate level of care. Whether ASAM criteria are implemented consistently in residential treatment settings is unknown. Dated information from a 2009 study showed ASAM criteria were more likely to be routinely used in outpatient facilities with a higher proportion of revenue from managed care and in CARF accredited facilities.[30] Treatment philosophy, client willingness to accept the treatment plan and an organization's capacity to offer all levels of care also may influence use of ASAM criteria.
One way to ensure more systematic use of ASAM criteria is to require it. States and managed care plans often require use of ASAM criteria. As of 2013, 24 states required some use of standardized assessment or placement criteria for all SUD provider types. The updated scan is likely to demonstrate even greater reach. Additionally, in late 2018, ASAM and CARF began a collaboration to establish a pilot national certification program for addiction treatment programs, certifying their ability to deliver services consistent with established guidelines for levels of care. The pilot is expected to launch in 2019.[31, 32]
Population Treated and Care Provided
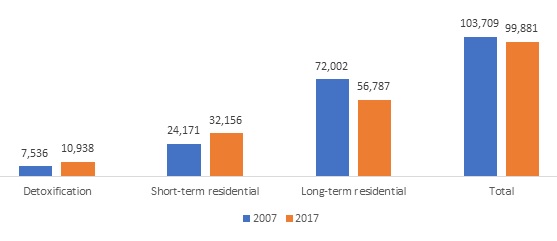
In 2017, there were about 99,881 people in residential substance use treatment on a given day in the United States. This number had declined since 2007, when there were 103,709 people in residential SUD treatment on a given day.[27] This decline was due to a decrease in the number of people in long-term residential treatment. The number of people in short-term residential treatment increased between 2007 and 2017 (Figure 6).
| FIGURE 6. Point Prevalence of Residential Treatment by Type of Residential Care |
|---|
 |
| SOURCE: Substance Abuse and Mental Health Services Administration. National Survey of Substance Abuse Treatment Services (N-SSATS): 2017. Data on Substance Abuse Treatment Facilities. 2018. https://www.samhsa.gov/data/sites/default/files/cbhsq-reports/2017_NSSATS.pdf. |
Residential substance use treatment programs treat individuals who are more severely ill than individuals treated at lower levels of care. For example, a study using a 2010 national database of discharges from publicly-funded residential substance use treatment services (Treatment Episode Data Set [TEDS]) found individuals in residential treatment were more likely to be unemployed or not in the workforce (88%), have prior substance use treatment experience (68%), and be using more than one substance (66%).[33] This profile is consistent with established patient-placement criteria such as ASAM that reserve public payment for residential care for those with greater severity or need. Because this study was based on discharge data, it did not examine prevalence of co-morbid psychiatric conditions, but these conditions also are common among individuals treated in residential SUD treatment.
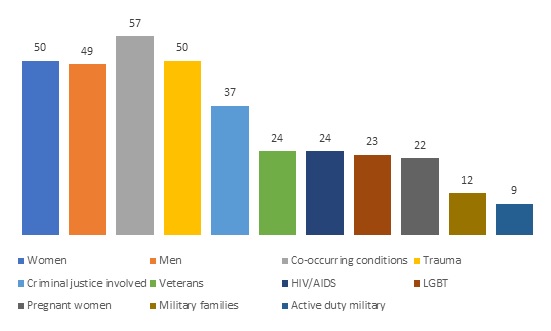
Residential substance use treatment programs provide a range of services and programming for patients. Many programs offer specialized services tailored for individuals with certain characteristics. According to the 2017 N-SSATS, residential treatment programs commonly offered programming specifically tailored for women, criminal justice involved clients, those with co-occurring conditions, and people who have experienced trauma (Figure 7).
| FIGURE 7. SUD Residential Treatment Programs with Specialized Programming, % |
|---|
 |
| SOURCE: Authors' analysis of Substance Abuse and Mental Health Services Administration. National Survey of Substance Abuse Treatment Services (N-SSATS): 2017. Data on Substance Abuse Treatment Facilities. 2018. https://www.samhsa.gov/data/sites/default/files/cbhsq-reports/2017_NSSATS.pdf. |
Three medications--buprenorphine, naltrexone, and methadone--are evidence-based treatments for OUD. Naltrexone is also an effective treatment for AUD, as are disulfiram and acamprosate. Federal regulations require that methadone be provided only in a certified Opioid Treatment Program (OTP). The vast majority of OTPs are in outpatient settings, making methadone uncommon in residential treatment. Medications for OUD have been shown to improve retention in treatment, reduce mortality, and reduce transmission of HIV and hepatitis C.[34]
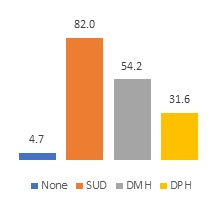
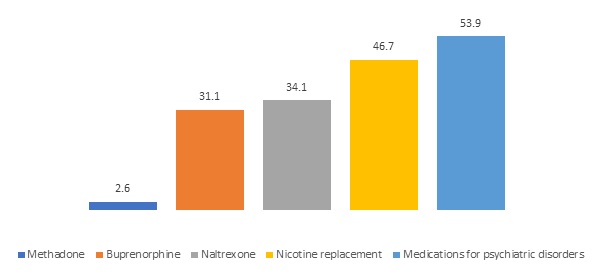
Although use of medication is an effective and cost-effective treatment for OUD and AUD, medications are not always available in substance use residential treatment programs. Some residential treatment programs are not supportive of using medications for substance use treatment.[35] In a nationally representative study of substance use treatment programs, Aletraris et al. found residential programs were less likely than programs with inpatient detoxification to offer naltrexone.[36] The 2017 N-SSATS indicates that most residential treatment programs do not offer the three most effective medications to treat OUD. About 31% of residential programs offer buprenorphine, 34% offer naltrexone, and less than 3% offer methadone, although more facilities provide nicotine replacement therapy and medications for psychiatric disorders (Figure 8).
| FIGURE 8. Residential SUD Facilities Offering Medications for SUD, % |
|---|
 |
| SOURCE: Authors' analysis of Substance Abuse and Mental Health Services Administration. National Survey of Substance Abuse Treatment Services (N-SSATS): 2017. Data on Substance Abuse Treatment Facilities. 2018. https://www.samhsa.gov/data/sites/default/files/cbhsq-reports/2017_NSSATS.pdf. |
Other evidence-based practices delivered in residential SUD treatment may include motivational interviewing and cognitive behavioral therapy. Not all programs provide evidence-based services. For example, in 2013, only two states required use of evidence-based practices in SUD residential treatment.[28] Key informants noted that clear guidelines for evidence-based SUD residential treatment are poorly developed at this time, so it is not likely that states would have regulations requiring the delivery of specific evidence-based practices.
Qualifications and credentialing of staff in residential SUD treatment programs vary. The field has evolved outside the medical system, with a significant role for individuals who have lived experience and peer counselors. A wide range of individuals may be employed, including peers in recovery, bachelor's or master's-level therapists, social workers, nurses, and physicians. States also vary in requirements for licensure of staff. Experts consulted for this project described variation in credentialing across different states as a challenge. It is important to examine who is a qualified provider and for what service.
QUALITY OF CARE
Studies of the effectiveness of residential mental health and SUD treatment are limited. Our search did not identify any rigorous peer-reviewed studies of the effectiveness of residential treatment programs in the past 5 years. There are several challenges to examining residential treatment. For example, it can be difficult to follow patients over time, resulting in high rates of loss to follow-up. Other challenges include a lack of residential mental health or SUD quality measures that can be used to examine system-wide performance and a lack of systematically collected patient-level data that would enable an analysis of patient outcomes.
Research on Quality of Residential Treatment
Because of the way that the mental health field has evolved, and the focus on moving individuals with mental health conditions from inpatient settings into community-based settings, there has been little rigorous research on the quality of care in intermediate residential settings for adults. Whereas residential treatment is widely studied and regulated for children, we found no information on standards for quality of care for adult mental health residential treatment. One study that was conducted in collaboration with a residential treatment program for individuals with co-occurring disorders identified a positive effect on health care utilization in the 6 months following discharge; however, the research relied on patient self-reported data and had a 36% loss to follow-up, so the real effect is unknown.[37]
Similarly, there is little information about the quality of residential SUD treatment. The fact that many residential substance use treatment programs do not provide medications for SUD is concerning. It is important to note that there are barriers to offering these medications. Federal regulations require methadone be provided only in approved clinics, and only waivered providers can prescribe buprenorphine. The provision of important screening tests and access to medical care may be one indicator of quality in SUD residential settings. At intake, providers generally ask about medical status and history; however, many residential substance use treatment facilities do not test for medical conditions common among individuals with SUD. In the N-SSATS, only 42% of facilities indicated that they test for HIV, 31% indicated that they test for sexually transmitted diseases, and 55% indicated that they conduct a tuberculosis screener.[38]
In addition, the extent to which states are actually able to systematically track quality and outcomes from residential treatment programs is not known. Although some data sources exist, little systematic research has been conducted using these data sources. One possible data source that could be used to study quality of SUD residential treatment is the National Outcomes Monitoring System/TEDS, developed by SAMHSA. Publicly-funded SUD treatment programs are required to collect data from all patients at discharge. Although limited to publicly-funded programs, these data are used by some states to monitor quality of SUD treatment, including residential care.
Finally, not only is there a lack of data or research regarding residential mental health and SUD treatment, especially patient experience and outcomes, but psychiatric and SUD patients are systematically excluded from efforts that target hospital-based care (e.g., inpatient psychiatric hospitalization) , such as through the Hospital Consumer Assessment of Healthcare Providers and Systems.[39] Many local and national health policy efforts to improve quality of care have focused on hospital-based general medical care. The exclusion of psychiatric and SUD patient experiences and outcomes from quality measurement efforts, even within the context of hospital-based care, suggests that attempts to improve the quality of care in residential settings is not necessarily a clear current priority in health policy reform.
Quality of Residential Treatment in the Grey Literature and Popular Press
Although there are little data on quality of care, journalists have identified several issues with residential treatment programs. Fraud, patient brokering, and "treatment" practices that cause trauma or harm are all issues recently identified in some residential SUD treatment programs.[40]
There have been well-documented examples of poorly run residential treatment facilities as well as examples of unregulated or underregulated treatment. Most reports focus on individual SUD treatment programs and may not apply only to residential service providers. Some examples of fraudulent or abusive activities include marketing or kick-back schemes, insurance overbilling or other fraud, excessive use of urine drug screens to generate billing, inadequate treatment, and trafficking of patients.[41, 42, 43, 44, 45] In 2014, the California State Auditor found insurance fraud including services reimbursed for dead people, failure by the state to refuse licenses when applications did not meet state standards, state failure to assign risk levels to treatment providers, and lack of state oversight of clinic medical directors.[46]
Insurers also are working to limit fraudulent billing for SUD treatment services[47] and to ensure compliance with federal and state regulations.[48] More information is needed on the existence and nature of state oversight requirements for SUD and psychiatric residential treatment. In addition to the tools available to regulators and those charged with oversight, it also is important to understand the extent to which states are using those tools to ensure safe, high-quality treatment and whether a lack of resources is impeding enforcement.[47]
Articles and blogs regarding the need for improved oversight and regulation of residential treatment facilities in California[17, 49]and Florida[50] provide a sense of the problems in those states in recent years caused by gaps or inconsistencies in oversight. California, for example, allowed nonmedical detoxification in residential facilities and reportedly prohibited physicians and other health professionals from working with many drug treatment programs, preventing needed medical oversight and provision of integrated care for patients. The state legislature acted to correct this problem in 2015, with implementation ongoing into 2018, after a drug treatment facility was indicted following a patient's death.[17]
Despite a lack of published literature, similar issues have been identified with respect to regulation of mental health residential settings, although the focus is often on group homes, which may or may not reach the threshold for qualifying as mental health residential treatment.[51] It is also important to note that there also is often a lack of conceptual clarity about the distinction between SUD residential treatment and other forms of SUD housing at lower levels of care in the popular press. This lack of understanding has led some to caution against a perception that the entire industry is subject to fraudulent and unethical behavior.[47] More in-depth analyses and conceptual clarity about the components of residential treatment are required to better assess quality of care in these settings.
REGULATION OF RESIDENTIAL MENTAL HEALTH AND SUBSTANCE USE FACILITIES
There is no current comprehensive compilation or analysis of state regulation of residential treatment facilities for adults in the United States. Reports have been published related to regulation of facilities for children,[52] of assisted living facilities,[53] and of residential facilities for adults with physical disabilities, expressly excluding facilities treating those with SMI or intellectual or developmental disabilities.[54, 55, 56]These reports also do not address residential facilities focused on the treatment of SUDs. A 2013 report by NASADAD provides information that is now dated on state regulation of SUD programs, which includes residential facilities, and demonstrates a range of regulatory structures across states.[28] There is no similar published report related to residential mental health programs. Consultation with key informants, however, indicates a similar patchwork of regulation, licensure, and accreditation requirements for residential psychiatric treatment.
Current Status of Regulation
The 2013 report by NASADAD looking at state regulation of SUD programs revealed that all states and the District of Columbia had regulations governing at least some SUD treatment facilities, although that differed by level of care and by whether the facilities were publicly-funded. Not all states required licensure/certification of all such facilities, and among those that did, some relied on their single state agency to oversee licensure/certification, whereas others delegated that responsibility to separate licensing boards or agencies within the state. For residential facilities, specifically, licensure/certification requirements were identified for 35 states, some of which had separate standards based on the standard length of stay being greater or less than 30 days.[28]
The NASADAD report found that staffing standards were in place for all settings (including, but not limited to, residential treatment) as follows: 17 states had standards for the president, CEO, or program director in all settings examined; 11 required a medical director for all settings; three required a weekly prescribing professional; two had staffing ratio requirements; four required a specific percentage of clinical staff to be licensed or certified; none had a required staffing ratio of medical staff to clients; and 27 required clinical supervision by a fully credentialed counselor.[28] Use of standardized assessment or placement criteria were required for all settings, with 11 requiring use of ASAM criteria and 14 requiring assessment or use of placement criteria for co-occurring mental health conditions. Treatment planning and discharge planning were required for all settings in 45 and 29 states, respectively. Aftercare or follow-up was required in eight states. Use of evidence-based practices was required by two states, and 27 required use of quality improvement procedures for all setting types.[28]
If a state deems accreditation or certification to be sufficient for licensure or operation, then requirements that are part of an accreditation entity's standards will supplement state-specific requirements. Similarly, if a state requires the use of specific assessment criteria for level of care or criteria for treatment within a given setting, those standards supplement state-specified licensure or oversight requirements. For example, ASAM level 3.1 requires, among other things, 24-hour staffing, review by an addiction professional of admission decisions to confirm clinical necessity, telephone or in-person consultation with a physician and emergency services available 24/7, and 5 hours per week of planned treatment activities directed by a clinical professional.[57] To the extent that these criteria take the place of other licensure requirements in a given state, they could be viewed as incorporated by reference into state standards. One challenge in the mental health field--in contrast to the SUD field, which has the ASAM criteria--is that there is no single commonly used placement criteria or standards for treatment at given levels of care. Although key informants indicate that some states do require use of the LOCUS for mental health settings, more concrete and current information on the existence and nature of state regulatory requirements, for both SUD and psychiatric residential treatment, is needed.
Insurance coverage and insurers' standards also influence how residential treatment is delivered in states and interact with these state regulations in the delivery of residential treatment to those who need it. Insurance coverage for residential treatment is a primary facilitator of access to care. Without coverage, individuals must pay out-of-pocket or rely on state programs. In 2010, approximately 16% of commercial managed care plans excluded coverage of residential SUD services and 7% excluded coverage for mental health services.[58] In 2014, 21 state Medicaid programs did not include coverage for either short-term or long-term residential services in their state Medicaid benefit.[59] These figures do not include coverage provided by Medicaid managed care plans, where systematic data is not available.
When residential care is covered by insurance, insurance company policies may address some of the same areas addressed in regulation. Health plan standards may include requirements for specific medical necessity and placement criteria, as well as types of treatment. They may also have quality measurement or quality standards and requirements for acceptance in their networks. It can be hard to understand how state regulations interact with insurance company requirements because health plans do not tend to release this information publicly.
Potential Regulatory Levers
Beyond requirements for licensure or certification, other potential regulatory levers identified in the 2013 NASADAD report include the following: staffing requirements, placement and assessment criteria, treatment and discharge planning, requirements for aftercare or follow-up services, use of evidence-based practices, and requirements related to quality improvement procedures. Similar regulatory levers also could be applied to residential mental health care. Little systematic information exists about any of these levers at this time. Further research is needed to help identify system challenges in this area, including what areas are often not regulated, what threats exist to adequate enforcement of regulations because of a lack of funding or inadequately trained staff, and what areas are regulated but not regularly enforced to ensure compliance.
Key informants stressed the importance of focusing on care transitions as a component of quality of care for patients in residential settings. Nearly all facilities surveyed in the N-SSATS, 99%, indicated that they create discharge plans, and 84% indicated that they have transitional aftercare services.[38] However, it is unclear how well these requirements are implemented. Guidance or regulations on how to use discharge plans might improve care transitions. Across the board, regulations will have limited impact without enforcement.
Incorporating quality process and outcome measures in residential care oversight is necessary. In addition to clinical measures of quality, key informants also mentioned that Medicaid directors increasingly are interested in assessing outcomes such as job placement, extent of criminal justice recidivism, and ability to live independently as indicators of successful residential treatment.
As noted in the 2013 NASADAD report, some states regulate or license only facilities that are recipients of state funds. The many reports of fraud and abuse in SUD facilities often point to "halfway homes," "sober living homes," or "residential treatment homes" that may not fall within the reach of existing regulations[47, 49, 60] or may not be considered residential treatment. The information available on fraud and abuse is limited to reports of poorly operated SUD facilities in different parts of the United States. A comprehensive review of regulations across the states for both psychiatric and SUD treatment is needed to obtain a more complete picture of what is regulated, thus allowing a better understanding of what is not.
Key informants stressed the challenge for health plans in managing the influx of for-profit SUD treatment programs that set themselves up as out of network. Often, health plans are not even aware that their enrollees are using the services until they get the bill; hence, they have a hard time managing utilization of these programs, despite poor quality. Regulatory efforts to ensure these programs are providing high-quality, evidence-based treatment would benefit both patients and health plans.
CONCLUSION
Individuals seeking residential mental health or substance use treatment are often vulnerable and in crisis. It is critical that all providers deliver high-quality, evidence-based services, and that quality residential treatment is available as part of the continuum of care. Key features of residential treatment include the provision of a range of 24-hour treatment and support services in a structured living environment for individuals who need support before living on their own. State licensing requirements for these types of treatment facilities provide a patchwork of standards and oversight mechanisms that vary widely and the research literature is limited in its assessment of residential treatment quality or of the effectiveness of state oversight. Important regulatory levers do exist and better understanding of the effects of standards such as those regarding treatment, follow-up planning, and quality improvement is important as states increasingly incorporate residential treatment into a more comprehensive spectrum of care.
ENDNOTES
-
Subatance Abuse and Mental Health Services Administration. National Mental Health Services Survey (N-MHSS): 2017--Data on Mental Health Treatment Facilities. 2018. https://www.samhsa.gov/data/sites/default/files/cbhsq-reports/2017_National_Mental_Health_Services_Survey.pdf.
-
Frank R, Glied S. Better But Not Well: Mental Health Policy in the United States Since 1950. Baltimore, MD: Johns Hopkins University Press; 2006.
-
Monico LB, Gryczynski J, Mitchell SG, Schwartz RP, O'Grady KE, Jaffe JH. Buprenorphine treatment and 12-step meeting attendance: Conflicts, compatibilities, and patient outcomes. J Subst Abuse Treat. 2015; 57: 89-95.
-
Humphreys K, Frank RG. The Affordable Care Act will revolutionize care for substance use disorders in the United States. Addiction. 2014; 109(12): 1957-8.
-
R. Harwood, NASADAD, personal communication, January 2019.
-
Reif S, George P, Braude L, Dougherty RH, Daniels AS, Ghose SS, Delphin-Rittmon ME. Residential treatment for individuals with substance use disorders: Assessing the evidence. Psychiatric Services. 2014; 65(3): 301-12.
-
Legal Action Center. The Medicaid IMD Exclusion: An Overview and Opportunities for Reform. July 2014. https://lac.org/wp-content/uploads/2014/07/IMD_exclusion_fact_sheet.pdf.
-
The Joint Commission (TJC). Guide to Joint Commission Behavioral Health Care Accreditation. Retrieved from The Joint Commission website on January 29, 2019 at https://www.jointcommission.org/assets/1/18/2010_bhc_accreditation_guide_w_cov.pdf.
-
Commission on the Accreditation of Rehabilitation Facilities (CARF). 2019 Behavioral Health Program Descriptions. 2019. http://www.carf.org/programdescriptions/bh/.
-
Priest KC, Leof AW, McCarty D, King V. Medicaid coverage for residential substance use disorder treatment: Addressing the institution for mental disease exclusion policy. Health Affairs Blog. August 31, 2017. https://www.healthaffairs.org/do/10.1377/hblog20170831.061745/full/.
-
Melecki S, Weider K. The Medicaid Institution for Mental Diseases (IMD) Exclusion. Medicaid and Chip Payment Access Commission; March 31, 2016. https://www.macpac.gov/wp-content/uploads/2016/03/The-Medicaid-Institution-for-Mental-Diseases-IMD-Exclusion.pdf.
-
Musumeci M. Key Questions About Medicaid Payment for Services in "Institutions for Mental Disease." Kaiser Family Foundation; June 18, 2018. https://www.kff.org/medicaid/issue-brief/key-questions-about-medicaid-payment-for-services-in-institutions-for-mental-disease/.
-
Centers for Medicare & Medicaid Services (CMS). SMD # 18-011 RE: Opportunities to Design Innovative Service Delivery Systems for Adults With a Serious Mental Illness or Children With a Serious Emotional Disturbance. November 2018. https://www.medicaid.gov/federal-policy-guidance/downloads/smd18011.pdf.
-
U.S. Government Accountability Office. Medicaid: States Fund Services for Adults in Institutions for Mental Disease Using a Variety of Strategies. August 2017. https://www.gao.gov/assets/690/686456.pdf.
-
Musumeci M, Tolbert J. Federal Legislation to Address the Opioid Crisis: Medicaid Provisions in the SUPPORT Act. Kaiser Family Foundation; October 5, 2018. https://www.kff.org/medicaid/issue-brief/federal-legislation-to-address-the-opioid-crisis-medicaid-provisions-in-the-support-act/.
-
Each state Medicaid program has an enrollment process to determine the eligibility of care providers to receive payments, although looking at enrollment standards across states that reimburse SUD residential care is beyond the scope of this project.
-
Nelson H. California Assembly Bill 848: Fixing the disconnect in California regulation of health professionals and addiction treatment. Nelson Hardiman Healthcare Lawyers. March 31, 2016. https://www.nelsonhardiman.com/california-assembly-bill-848-fixing-the-disconnect-in-california-regulation-of-health-professionals-and-addiction-treatment/.
-
Substance Abuse and Mental Health Services Administration. FFY 2018-2019 Block Grant Application: Community Mental Health Services Block grant (MHBG) Plan and Report, Substance Abuse Prevention and Treatment Block Grant (SABG) Plan and Report. 2018. https://www.samhsa.gov/sites/default/files/grants/fy18-19-block-grant-application.pdf.
-
Substance Abuse and Mental Health Services Administration. National Mental Health Services Survey (N-MHSS). 2018. https://info.nmhss.org/Definitions/index.asp.
-
Authors' analysis of Substance Abuse and Mental Health Services Administration. National Mental Health Services Survey (N-MHSS): 2017. Data on Mental Health Treatment Facilities. 2018. https://www.samhsa.gov/data/sites/default/files/cbhsq-reports/2017_National_Mental_Health_Services_Survey.pdf.
-
Hodgkin D, Horgan CM, Stewart MT, Quinn AE, Creedon TB, Reif S, Garnick DW. Federal parity and access to behavioral health care in private health plans. Psychiatric Services. 2018; 69(4): 396-402.
-
Deerfield Solutions. Deerfield LOCUS: A copyright of AACP. 2019. http://www.dbhn.com/index.cfm/software/.
-
Choi S, Adams SM, Morse SA, MacMaster S. Gender differences in treatment retention among individuals with co-occurring substance abuse and mental health disorders. Substance Use and Misuse. 2015; 50(5): 653-63.
-
Priester MA, Browne T, Iachini A, Clone S, DeHart D, Seay KD. Treatment access barriers and disparities among individuals with co-occurring mental health and substance use disorders: An integrative literature review. Journal of Substance Abuse Treatment. 2016; 61: 47-59.
-
T. Lutterman, NRI, personal communication, December 2018.
-
The inclusion of analyses using data from the Treatment Episode Data Set [TEDS] was considered, but because TEDS is limited to publicly-funded programs, we ultimately decided to focus on N-SSATS for the purposes of this scan.
-
Substance Abuse and Mental Health Services Administration. National Survey of Substance Abuse Treatment Services (N-SSATS): 2017. Data on Substance Abuse Treatment Facilities. 2018. https://www.samhsa.gov/data/sites/default/files/cbhsq-reports/2017_NSSATS.pdf.
-
National Association of State Alcohol and Drug Abuse Directors (NASADAD). State Regulations on Substance Use Disorder Programs and Counselors: An Overview. December 2012. http://nasadad.org/wp-content/uploads/2010/12/State_Regulation_of_SUD_Programs_and_Counselors-7-26-13.pdf.
-
American Society of Addiction Medicine (ASAM). The ASAM Criteria: Treatment Criteria for Addictive, Substance-Related, and Co-occurring Conditions, Third Edition. October 24, 2013. https://www.asam.org/resources/the-asam-criteria/text.
-
Chuang E, Wells R, Alexander J, Friedmann P, Lee I. Factors associated with use of ASAM criteria and service provision in a national sample of outpatient substance abuse treatment units. J Addict Med. 2009 Sep; 3(3): 139-150.
-
American Society of Addiction Medicine (ASAM). ASAM and CARF reshape addiction care with landmark treatment delivery certification: in partnership with CARF, ASAM level of care certification will provide an independent, comprehensive assessment of addiction treatment facilities' ability to deliver care consistent with the ASAM Criteria®. December 15, 2018. https://www.asam.org/resources/level-of-care-certification.
-
Commission on the Accreditation of Rehabilitation Facilities (CARF). ASAM and CARF reshape addiction care with landmark treatment delivery certification: in partnership with CARF, ASAM level of care certification will provide an independent, comprehensive assessment of addiction treatment facilities' ability to deliver care consistent with the ASAM Criteria®. December 15, 2018. http://www.carf.org/LOCcertification/.
-
Mutter R, Ali M, Strashny A. Factors associated with substance use treatment completion in residential facilities. Drug and Alcohol Dependence. 2015; 154: 291-5.
-
Substance Abuse and Mental Health Services Administration. Medications for Opioid Use Disorder, in Treatment Improvement Protocol (TIP). Series 63, Full Document. Substance Abuse and Mental Health Services Administration: Rockville, MD; 2018.
-
Hadland S, Park T, Bagley S. Stigma associated with medication treatment for young adults with opioid use disorder: a case series. Addiction Science and Clinical Practice. 2018; 13(1).
-
Aletraris L, Edmond MB, Roman PM. Insurance receipt and readiness for opportunities under the Affordable Care Act: A national survey of treatment providers for substance use disorders. Journal of Psychoactive Drugs. 2017; 49(2): 141-50.
-
Morse S, Bride BE. Reduction in healthcare utilization and costs following residential integrated treatment for co-occurring substance use and mental health disorders. Journal of Hospital Administration. 2016; 5(6): 53.
-
Authors' analysis of Substance Abuse and Mental Health Services Administration. National Survey of Substance Abuse Treatment Services (N-SSATS): 2017. Data on Substance Abuse Treatment Facilities. 2018. https://www.samhsa.gov/data/sites/default/files/cbhsq-reports/2017_NSSATS.pdf.
-
Shields MC, Stewart MT, Delaney KR. Patient safety in inpatient psychiatry: a remaining frontier for health policy. Health Affairs. 2018; 37(11): 1853-61.
-
Ehley B, Roubein R. 'I'm trying not to die right now': Why opioid-addicted patients are still searching for help. Politico. January 19, 2019. https://www.politico.com/story/2019/01/20/opioid-treatment-addiction-heroin-1088007.
-
Rothenberg Z. Avoiding fraud and abuse claims in addiction treatment: tips for getting and staying in compliance. Nelson Hardiman Healthcare Lawyers; February 22, 2017. https://www.nelsonhardiman.com/avoiding-fraud-abuse-claims-addiction-treatment-tips-getting-staying-compliance/.
-
Cohn S. Opioids' hidden epidemic-fraudulent treatment centers. CNBC. June 29, 2018. https://www.cnbc.com/2018/06/06/opioids-hidden-epidemicfraudulent-drug-treatment-centers.html.
-
Miller J. Health Net looking for fraud among treatment centers. Behavioral Healthcare Executive. January 28, 2018. https://www.behavioral.net/article/health-net-looking-fraud-among-treatment-centers.
-
Walser A. New federal drug rehab bill inspired by "Florida shuffle": Law identifies, exposes and punishes bad operators. ABC Action News. July 6, 2018. https://www.abcactionnews.com/news/local-news/i-team-investigates/new-federal-drug-rehab-bill-inspired-by-florida-shuffle-.
-
Osher C. Police found fraud, sex crimes in a Colorado sober-living home empire. The state doesn't regulate the industry. Denver Post. March 11, 2018. https://www.denverpost.com/2018/03/11/colorado-sober-living-homes-opioid-crisis-christopher-bathum/.
-
Jewett C, Evans W. State audit confirms weak oversight, potential fraud at rehab clinics. Reveal Health Care. August 19, 2014. https://www.revealnews.org/article-legacy/state-audit-confirms-weak-oversight-potential-fraud-at-rehab-clinics/.
-
Nelson H. Addiction treatment is booming and under-regulated. Behavioral Healthcare Executive. April 6, 2016. https://www.behavioral.net/article/addiction-treatment-booming-and-under-regulated.
-
MidState Health Network. Policies and Procedures Manual: Quality--Monitoring & Oversight of SUD Service Provider Procedures. March 2018. https://midstatehealthnetwork.org/application/files/9815/4239/9975/Quality_Monitoring__Oversight_of_SUD_Providers_Procedure_2.0_Clean.pdf.
-
M&R Blog. CA state legislature clamps down on residential treatment centers. Michelman & Robinson, LLP. May 11, 2016. https://www.mrllp.com/blog-ca-state-legislature-clamps-down-on-residential-treatment-centers.
-
Becker D. Reports of rehab scams raise concerns about addiction treatment quality. WBUR. September 1, 2017. https://www.wbur.org/commonhealth/2017/09/01/addiction-treatment-quality.
-
Damon A. Nevada is still housing mentally ill clients in filthy conditions despite promise to fix. Reno Gazette Journal. January 17, 2018. https://www.rgj.com/story/news/2018/01/17/nevada-still-housing-mentally-ill-clients-filthy-conditions-despite-promise-fix/1041688001/.
-
Ireys H, Achman L, Takyi A. State Regulation of Residential Facilities for Children With Mental Illness. Substance Abuse and Mental Health Services Administration; 2006. https://www.mathematica-mpr.com/-/media/publications/pdfs/residfacilchildren.pdf.
-
National Center for Assisted Living. 2018 Assisted Living Regulatory Review. 2018. https://www.ahcancal.org/ncal/advocacy/regs/Documents/2018_reg_review.pdf.
-
Carder P, O'Keefe J, O'Keefe C. Compendium of Residential Care and Assisted Living Regulations and Policy: 2015 Edition. Office of the Assistant Secretary for Planning and Evaluation; 2015. https://aspe.hhs.gov/basic-report/compendium-residential-care-and-assisted-living-regulations-and-policy-2015-edition.
-
Carder P, O'Keefe J, O'Keefe C, White E, Wiener J. State Regulatory Provisions for Residential Care Settings: An Overview of Staffing Requirements. RTI Press Publication; July 2016. https://www.rti.org/sites/default/files/resources/State_Regulatory_Provisions_for_Residential_Care_Settings.pdf.
-
Greene AM, Lepore M, Lux L, Porter K, Vreeland E. Understanding Unlicensed Care Homes: Final Report. Office of the Assistant Secretary for Planning and Evaluation; September 2015. https://aspe.hhs.gov/basic-report/understanding-unlicensed-care-homes-final-report.
-
Centers for Medicare & Medicaid Services (CMS). Medicaid Innovation Accelerator Program. Overview of Substance Use Disorder (SUD) Care Clinical Guidelines: A Resource for States Developing SUD Delivery System Reforms. April 2017. https://www.medicaid.gov/state-resource-center/innovation-accelerator-program/iap-downloads/reducing-substance-use-disorders/asam-resource-guide.pdf.
-
Horgan CM, Stewart MT, Reif S, Garnick DW, Hodgkin D, Merrick EL, Quinn AE. Behavioral health services in the changing landscape of private health plans. Psychiatr Serv. 2016: 67(6); 622-9.
-
Grogan C, Andrews C, Abraham A, Humphreys K, Pollack H, Smith B, Friedmann P. Survey highlights differences in Medicaid coverage for substance use treatment and opioid use disorder medications. Health Affairs. 2016: 35(12).
-
Moore H. Scottsdale takes largely 'hands-off' approach on residential treatment houses/sober living homes. AZ Family. March 15, 2018. https://www.azfamily.com/archives/scottsdale-takes-largely-hands-off-approach-on-residential-treatment-houses/article_f2de2609-d5b0-5f0e-89ec-a21e80bbb214.html.