
Jesse Hinde, PhD, Jennifer Hayes, BA, Tami Mark, PhD, Shampa Bernstein, JD, BA, and Sarita L. Karon, PhD
RTI International
September 29, 2017
Printer Friendly Version in PDF Format (76 PDF pages)
ABSTRACT
This report summarizes financing and workforce policies that can be used by states to expand treatment access and capacity for opioid use disorder (OUD), focusing especially on medication-assisted treatment (MAT). Our evaluation team used a case-study approach and conducted an environmental scan and stakeholder interviews for five states: California, Missouri, New Hampshire, Ohio, and Virginia. The results highlight key levers each state is using to expand or improve access to MAT, summarize common themes among financing and workforce policies, and map the policy levers to different settings in which a patient could start MAT, describing ways to build local capacity.
DISCLAIMER: The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS
1. BACKGROUND
1.1. The Opioid Epidemic
1.2. Why Medication-Assisted Treatment?
1.3. Treatment Settings for Opioid Use Disorder
1.4. Financing for Treatment
3. STATE AND LOCAL INNOVATIONS
3.1. California
3.2. Missouri
3.3. New Hampshire
3.4. Ohio
3.5. Virginia
4.1. Expand Medicaid Eligibility
4.2. Medicaid 1115 Substance Abuse Disorder Waiver
4.3. Federal Grant Funding
4.4. Public/Private Contracting
4.5. Regulations for Public/Private Insurance
5. WORKFORCE DEVELOPMENT APPROACHES
5.1. Workforce Barrier #1: There are Not Enough Waivered Physicians
5.2. Workforce Barrier #2: Provider Access in Rural Areas is Poor
5.3. Workforce Barrier #3: There is a Lack of Support for Small, Non-specialist Physicians
5.4. Workforce Barrier #4: There is a Lack of Infrastructure to Support Treatment
5.5. Workforce Barrier #5: Stigma and Knowledge Gaps Exist
7. CONCLUSION
APPENDICES
- APPENDIX A: Differences Among Opioid Use Disorder Medications
- APPENDIX B: State Opioid Epidemic Profiles
LIST OF BOXES
- BOX 1. The Hub and Spoke Model in Vermont
- BOX 2. What is a PPS and How Does it Incentivize Quality and Efficiency?
- BOX 3. Project ECHO
LIST OF EXHIBITS
- EXHIBIT 1: Academic Detailing to Increase the Number of Waived Providers
- EXHIBIT 2: SBIRT at a Glance
- EXHIBIT 3: Ohio's Proposed Emergency Department Implementation Models
- EXHIBIT 4: Common Financing Approaches for MAT Expansion and Perceived Benefits
- EXHIBIT 5: Common Workforce Issues and Potential Solutions
- EXHIBIT 6: Building Local MAT Capacity
- EXHIBIT A-1: Differences among OUD Medications
ACRONYMS
The following acronyms are mentioned in this report and/or appendices.
| ACA | Patient Protection and Affordable Care Act |
|---|---|
| ARTS | Addiction Recovery Treatment Service |
| ASAM | American Society of Addiction Medicine |
| ASPE | HHS Office of the Assistant Secretary for Planning and Evaluation |
| BDAS | New Hampshire Bureau of Drug and Alcohol Services |
| BH | Behavioral Health |
| CARA | Comprehensive Addiction and Recovery Act |
| CCBHC | Certified Community Behavioral Health Clinic |
| CDC | HHS Centers for Disease Control and Prevention |
| CHIP | Children's Health Insurance Program |
| CIMOR | Customer Information Management, Outcomes and Reporting |
| CMS | HHS Centers for Medicare & Medicaid Services |
| CSB | Community Service Board |
| DATA 2000 | Drug Addiction Treatment Act of 2000 |
| DBHDS | Virginia Department of Behavioral Health Developmental Services |
| DEA | DoJ Drug Enforcement Administration |
| DHCS | California Department of Health Care Services |
| DMC | Drug Medi-Cal |
| DMH | Missouri Department of Mental Health |
| DoJ | U.S. Department of Justice |
| ECHO | Extension for Community Healthcare Outcomes |
| ED | Emergency Department |
| FDA | HHS Food and Drug Administration |
| FFS | Fee-For-Service |
| FPL | Federal Poverty Level |
| FQHC | Federally Qualified Health Center |
| FY | Fiscal Year |
| HHS | U.S. Department of Health and Human Services |
| HRSA | HHS Health Resources and Services Administration |
| IDN | Integrated Delivery Network |
| JAMA | Journal of the American Medical Association |
| LADC | Licensed Alcohol and Drug Counselor |
| MAT | Medication-Assisted Treatment |
| MCO | Managed Care Organization |
| MHPAEA | Mental Health Parity and Addiction Equity Act |
| MU | Medication Unit |
| NHHPP | New Hampshire Health Protection Program |
| NIAAA | National Institute on Alcohol Abuse and Alcoholism |
| NIDA | National Institute on Drug Abuse |
| NP | Nurse Practitioner |
| NSDUH | National Survey of Drug Use and Health |
| NTP | Narcotic Treatment Program |
| OBOT | Office-Based Opioid Treatment |
| ODS | Organized Delivery System |
| OMHAS | Ohio Mental Health and Addiction Services |
| OTP | Opioid Treatment Program |
| OUD | Opioid Use Disorder |
| P.L. | Public Law |
| PA | Physician Assistant |
| PCSS | Provider's Clinical Support System |
| PDOA | Prescription Drug and Opioid Addiction |
| PPS | Prospective Payment System |
| QHP | Qualified Health Plan |
| SAMHSA | HH Substance Abuse and Mental Health Services Administration |
| SAPT | Substance Abuse Prevention and Treatment |
| SBIRT | Screening, Brief Intervention, and Referral to Treatment |
| SSA | Single State Agency |
| STR | State Targeted Response |
| SUD | Substance Use Disorder |
EXECUTIVE SUMMARY
Objective
This report summarizes financing and workforce policies that can be used by states to expand treatment access and capacity for opioid use disorder (OUD), focusing especially on medication-assisted treatment (MAT). Our evaluation team used a case-study approach and conducted an environmental scan and stakeholder interviews for five states: California, Missouri, New Hampshire, Ohio, and Virginia. The results highlight key levers each state is using to expand or improve access to MAT, summarize common themes among financing and workforce policies, and map the policy levers to different settings in which a patient could start MAT, describing ways to build local capacity.
Why Medication-Assisted Treatment?
Since 2000, drug overdose death rates increased by 137 percent, including a 200 percent increase in the rate of overdose deaths involving opioid pain relievers and heroin.1, 2 Nearly every state has a rate of OUD that eclipses treatment capacity.3 There is a large range of treatment options for individuals with OUD, including individual and group counseling or behavioral therapy, abstinence and 12-step fellowships, inpatient or residential treatment, intensive outpatient treatment, case or care management, peer or recovery supports, and pharmacotherapy, such as MAT.4
MAT is a combination of medication, counseling and behavioral therapy that has shown to be effective in treating alcohol and opioid dependency. Currently, there are three medications approved by the U.S. Department of Health and Human Services Food and Drug Administration for OUD treatment: (1) methadone, (2) naltrexone, and (3) buprenorphine. MAT for OUD is effective in reducing opioid use and opioid-related overdose deaths and endorsed by the National Institutes of Health5, 6, 7, 8 and the World Health Organization.8 Despite its effectiveness, many patients encounter barriers accessing evidence-based MAT for OUD, including coverage, limited behavioral health workforce, and lack of perceived need for treatment, among others.9, 10, 11
Paths to Treatment for Opioid Use Disorder
Individuals with OUD can access MAT in various settings. Methadone can only be dispensed at a certified Opioid Treatment Program (OTP). Buprenorphine can be prescribed by a licensed medical provider (i.e., a physician, psychiatrist, physician assistant [PA], or nurse practitioner [NP]) with a U.S. Department of Justice Drug Enforcement Administration registration and a buprenorphine waiver. Naltrexone can be prescribed by any licensed medical provider. Therefore, patients can be treated with buprenorphine and naltrexone through most medical facilities, including office-based physician practices, Federally Qualified Health Centers, hospitals and emergency departments, and other specialized settings including OTPs, residential substance abuse facilities, or outpatient behavioral health organizations.
Clinical guidelines recommend a formal assessment before starting MAT, and the appropriate treatment will depend on the severity of the diagnosis, comorbid factors, current clinical context (i.e., in withdrawal or recovering from overdose), patient preferences, and the supply of providers licensed to provide these therapies. Many medical facilities do not have the expertise to conduct formal assessments, and the linkage between medical and substance use disorder (SUD) settings is not generally a strong one, which creates a barrier for many patients and medical providers. Many states have relatively low numbers of OTPs or waived providers to meet patient demand, especially in rural areas.3
Access to MAT and other SUD treatment often depends on health insurance coverage. Not all Medicaid programs and private insurers cover all three types of MAT. Medicaid and private insurers often require prior authorizations before starting MAT, causing administrative delays and denials for patients. Some insurance plans also require co-payment or patient cost-sharing for SUD services, which may be challenging for some patients to meet.
Levers Used by States to Expand Treatment and Recovery Capacity
Based on an environmental scan of policies in five states and discussions with a total of 15 stakeholders in those states, the following policy levers were commonly cited to expand MAT provision:
-
Expand Medicaid coverage and access to MAT by expanding services covered under the optional Medicaid benefits; expand Medicaid access to low-income, childless adults to increase access to SUD treatment services; or use Medicaid waivers to expand or develop enhanced SUD systems of care.
-
Develop systems of care in which a central specialty SUD provider (or hub) has expertise to start patients on MAT, treat severely ill patients, and provide consultation and support to less experienced office-based prescribers of MAT (spoke).
-
Hubs are clinics that provide specialized expertise in opioid treatment by assessing opioid users, determining the most optimal medication, initiating MAT treatment, providing ongoing care, and transferring stable patients back into primary care.
-
Spokes serve as a regional network of MAT prescribers that manage medication maintenance and provide recovery support or counseling services.
-
Spokes can implement MAT support teams to ensure medications are being appropriately prescribed, conduct patient assessments, and coordinate medical and social services.
-
-
Use targeted grant funds for start-up and to address service gaps.
-
Increase the number of providers with a waiver to prescribe buprenorphine by subsidizing training, expanding the scope of practice for NPs and physician's assistants, and through targeted recruiting.
-
Modify regulations that impede MAT delivery, such as reducing prior authorization requirements and barriers to entry for private OTPs.
-
Implement programs that combat stigma and resistance, such as training, coordinated outreach, and the Screening, Brief Intervention and Referral for Treatment program.
Endnotes
-
Centers for Disease Control and Prevention. (2011). Vital signs: Overdoses of prescription opioid pain relievers--United States, 1999-2008. Morbidity and Mortality Weekly Report, 60(43), 1487-1492.
-
Centers for Disease Control and Prevention. (2017). Opioid Data Analysis: Categories of Opioids. Retrieved from https://www.cdc.gov/drugoverdose/data/analysis.html.
-
Jones, C.M., Campopiano, M., Baldwin, G., & McCance-Katz, E. (2015). National and state treatment need and capacity for opioid agonist medication-assisted treatment. American Journal of Public Health, 105(8), e55-e63. Retrieved from DOI: 10.2105/AJPH.2015.302664.
-
Substance Use and Mental Health Services Administration. (2016). Treatments for Substance Use Disorders. Retrieved from https://www.samhsa.gov/treatment/substance-use-disorders.
-
Legal Action Center. (2015). The Case for Eliminating Barriers to Medication-Assisted Treatment of Heroin and Opioid Addiction.
-
Kampman, K., & Jarvis, M. (2015). American Society of Addiction Medicine (ASAM) national practice guideline for the use of medications in the treatment of addiction involving opioid use. Journal of Addiction Medicine, 9, 1-10.
-
Tai, B., Saxon, A.J., & Ling, W. (2013). Medication-assisted therapy for opioid addiction. Journal of Food and Drug Analysis, 21(4), S13-S15. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4175918/.
-
National Institute on Drug Abuse. (2016). Effective Treatments for Opioid Addiction. Retrieved from https://www.drugabuse.gov/publications/effective-treatments-opioid-addiction/effective-treatments-opioid-addiction.
-
Volkow, N.D., Frieden, T.R., Hyde, P.S., & Cha, S.S. (2014). Medication-assisted therapies--tackling the opioid-overdose epidemic. New England Journal of Medicine, 370(22), 2063-2066.
-
Sigmon, S.C. (2015). The untapped potential of office-based buprenorphine treatment. JAMA Psychiatry, 72(4), 395-396.
-
Park-Lee, E., Lipari, R., Hedden, S., Kroutil, L., & Porter, J. (2017). Receipt of services for substance use and mental health issues among adults: Results from the 2016 National Survey on Drug Use and Health. NSDUH Data Review.
1. BACKGROUND
1.1. The Opioid Epidemic
Drug overdose is the leading cause of accidental death in the United States, surpassing motor vehicle deaths by over 10,000 deaths in 2015.12 In that same year, over 52,000 deaths in the United States were attributed to drug poisoning, and over 33,000 (63 percent) of these involved some type of opioid (prescription or illicit). Since 2000, drug overdose death rates have increased by 137 percent, and the rate of overdose deaths involving opioid pain relievers and heroin has increased by 200 percent.1, 2, 12 In 2015, 3.8 million people misused prescription pain relievers, and 2.2 million people--or 0.8 percent of the United States population over the age of 12--had a disorder related to their misuse of prescription pain relievers.13 According to the 2015 National Survey on Drug Use and Health, OUD was most prevalent among individuals aged 18-25 years: about 1.2 percent of young adults aged 18-25 reported a pain reliever use disorder within the past year.13
There is a large range of treatment options for individuals with OUD, including individual and group counseling or behavioral therapy, abstinence and 12-step fellowships, inpatient or residential treatment, intensive outpatient treatment, case or care management, peer or recovery supports, and pharmacotherapy.4 Despite the toll of this epidemic, nearly every state has a rate of opioid use disorder (OUD) that eclipses treatment capacity.3 Fewer than half of those with an OUD receive treatment and even fewer receive treatment of adequate duration.14 More specifically, many patients may encounter access barriers to evidence-based medication-assisted treatment (MAT) for OUD including coverage, limited behavioral health workforce, and lack of perceived need for treatment, among others.9, 10, 11
1.2. Why Medication-Assisted Treatment?
MAT is the use of medications, in combination with counseling and behavioral therapies, to provide a comprehensive approach to the treatment of substance use disorder (SUD).9 Evidence of the effectiveness of MAT for OUD in reducing drug use is well-established, and the use of MAT has been endorsed by the National Institutes of Health5, 6, 7, 8 and the World Health Organization.8 However, in the United States, only 30 percent of SUD specialty treatment programs offer medications for individuals experiencing OUD.15 Additionally, of the 2.5 million Americans aged 12 or older who misused or were dependent on opioids in 2012, fewer than 1 million received appropriate pharmacological treatment.9
Currently, there are three medications approved by the U.S. Department of Health and Human Services (HHS) Food and Drug Administration (FDA) for OUD treatment: (1) methadone (a full agonist), (2) naltrexone (an antagonist), and (3) buprenorphine (a partial agonist). Appendix A provides an in-depth description of each medication. The medications work to stabilize brain chemistry and ease cravings and other withdrawal symptoms.
As a full agonist, methadone works to block the effects of heroin and other opioids by activating receptors in the brain that trigger cravings, replacing the effects of opioids.16 Methadone is a Schedule II medication, which means that although it has a high potential for abuse and may lead to severe psychological or physical dependence, it is still defined as having currently accepted medical use, albeit with certain restrictions.17 Because of its risk of diversion, methadone can only be prescribed in highly regulated Opioid Treatment Programs (OTPs). As of July 2016, there were approximately 1,400 OTPs across the country that typically treat approximately 350,000 patients on any given day.18
Buprenorphine is a partial agonist. Buprenorphine, however, is a Schedule III medication because it has a lower potential for abuse than methadone. To further reduce the abuse potential, buprenorphine is often formulated with naloxone, a drug that reverses the effects of opioids. Buprenorphine can be prescribed in a general physician's office, but physicians must undergo an 8-hour training and receive a special waiver created through the Drug Addiction Treatment Act of 2000 (DATA 2000), and must be registered with U.S. Department of Justice (DoJ) Drug Enforcement Administration (DEA). As of March 2017, a total of 37,526 physicians across the country had obtained a DATA 2000 waiver to prescribe buprenorphine.19 Physicians are initially limited to prescribing buprenorphine to a maximum of 30 patients at a time under the waiver, increasing the patient limit to 275 over time.20 The Comprehensive Addiction and Recovery Act (CARA) of 2016 allows advanced practice nurses and physician assistants (PAs) to qualify for a waiver for up to 30 patients from 2016 through 2021 if they complete 24 hours of training. To prescribe, MAT, their state license must also include prescribing authority for Schedule III, IV, or V medications for the treatment of pain.21
As an antagonist, naltrexone blocks the euphoric effects of opioids, diminishing the reinforcing effects of use. Naltrexone can be prescribed in any setting by any provider who is licensed to prescribe medications and is not considered a controlled substance.6 One formulation of naltrexone is a long-lasting injection that works for 30 days per dose (i.e., Vivitrol).
1.3. Treatment Settings for Opioid Use Disorder
Individuals with OUD can access MAT in various settings. While methadone can only be dispensed at a certified OTP, buprenorphine can be prescribed by any licensed and waived medical provider (i.e., a physician, PA or nurse practitioner [NP]) and naltrexone can be prescribed by any licensed medical provider. Thus, in theory, if they have prescribing professionals on staff, most medical facilities could provide buprenorphine and naltrexone, including through office-based physician practices, Federally Qualified Health Centers (FQHCs), hospitals and emergency departments, and other specialized settings including OTPs, residential substance abuse facilities, or outpatient behavioral health organizations.
Clinical guidelines recommend a formal assessment before starting MAT, and the appropriate treatment will depend on the severity of the diagnosis, comorbid factors, current clinical context (i.e., in withdrawal or recovering from overdose), patient preferences and the supply of providers licensed to provide these therapies.22 Many medical facilities do not have the expertise to conduct formal assessments and there is not generally a strong linkage between medical and SUD settings, creating a barrier for many patients and medical providers.
Buprenorphine is by far the most common type of MAT prescribed for patients with OUD. In 2016, 12.5 million prescriptions were written for buprenorphine, compared to only 64,000 prescriptions for long-acting injectable Vivitrol (in 2014) and 473,000 for oral naltrexone (a portion of which are used to treat alcohol use disorders, not OUD). Assuming an individual with OUD receives, on average, three prescriptions a year,23 this would amount to approximately 4.1 million people receiving buprenorphine, 21,333 people receiving Vivitrol, and 157,667 people receiving oral naltrexone. Approximately 330,308 individuals receive methadone treatment for OUD. Based on these conservative assumptions, more than eight times as many people receive buprenorphine for OUD than the other three medications combined.
Within the SUD treatment system, facilities vary significantly in their MAT options for OUD patients. Of all facilities that provide SUD treatment, only 17 percent offer injectable naltrexone, whereas 35 percent of methadone-dispensing OTPs provide buprenorphine in addition to methadone. Twenty-five percent of all SUD facilities provide buprenorphine.18 About 2 percent of all clients received buprenorphine in OTP facilities and 4.2 percent received buprenorphine in non-OTP facilities.
Of the total 1,305,647 clients in OUD/SUD treatment in 2015, 29 percent received MAT in OTP facilities. Across all facilities that provide SUD treatment services, 22 percent of patients received methadone in 2005, compared with 27 percent of patients receiving methadone in 2015. Although the overall change in proportion was small, the number of patients receiving methadone increased by 51 percent. Buprenorphine was administered to less than 1 percent in 2005 and was administered to 6 percent of all patients in 2015, representing a 1,385 percent increase in the number of patients. Finally, patients receiving extended-release, injectable naltrexone was less than 1 percent in 2013 and in 2015.18
A recent study showed that nearly every state has OUD rates higher than their waived buprenorphine provider treatment capacity. Another study conducted in 2012 found that among states and the District of Columbia, 96 percent had OUD or opioid dependence rates higher than their buprenorphine treatment capacity rates; 37 percent had a gap of at least five per 1,000 people. Thirty-eight states (77.6 percent) reported at least 75 percent of their OTPs were operating at 80 percent capacity or more.3
1.4. Financing for Treatment
Several payment options exist for SUD treatment and different payers (i.e., private insurers, Medicaid/Medicare, or other state and local payers) have different payment procedures for specific providers and services. One option is to pay cash for these services through cash-based providers or clinics. Access to most treatment depends on insurance coverage of MAT and other SUD services. Of people who use illicit drugs, used as a proxy for OUD, 49 percent have private insurance coverage, 27 percent are covered by Medicaid, and 7 percent are under Medicare. The remaining 18 percent reported no health insurance coverage. Of people who reported prescription opioid misuse in the past year, about 28 percent of them were covered by Medicaid.3
There are publicly-funded facilities that accept Medicaid or other insurance-based fee-for-service (FFS) or managed care payments. FFS is a payment model in which each service is paid for separately; an FFS payment is often triggered by the submission of a claim by the provider to either the state Medicaid agency or the insurance company stating that a service was provided. In contrast, under managed care, the state pays a fee to a managed care plan for each person enrolled in the plan and, in turn, the plan pays providers for all services an enrollee may need that are included in the plan's contract with the state. These contracts establish a set network of providers or hospitals that enrollees can visit and are monitored by the managing organization.
Many state Medicaid programs exclude or "carve-out" SUD services from these managed care contracts, and SUD services are then delivered or financed through a separate contractual agreement or in an FFS system. Recently, many states have begun to "carve-in" SUD services into their general managed care contracts so that virtually all services covered, though some exceptions may exist for selected drugs.24
State and private insurance policies can include a wide array of requirements with which providers must comply to receive payment for SUD services. In particular, providers often are required to first obtain approval to provide a service to be eligible for payment, or "prior authorization." Prior authorizations are used to ensure that the service is covered by the insurance provider, appropriate for the enrollee who is to receive the service, and sometimes to determine the maximum amount of services that the enrollee may receive within a given timeframe (these are referred to as "lifetime limits" or "caps").
Medicaid and private insurers often require a formal OUD diagnosis and prior authorizations before starting MAT, causing administrative delays for patients. Further, some insurance plans require co-payment or patient cost-sharing (e.g., the share of costs covered by insurance that patients must pay out of their own pocket25) for SUD services, which may be challenging for some patients to meet.
Overall, SUD expenditures are less than mental health and physical health expenditures and have followed different trends across payers. As of 2014, SUD treatment spending accounted for only 1.2 percent of all health expenditures compared to 6.8 percent for mental health. Whereas the relative share of mental health expenditures has shifted from state and local funding to Medicare, Medicaid and private insurance, SUD expenditures remain largely funded by state and local revenues and federal block grants. In 2014, Medicare, Medicaid, and private insurance covered 68 percent of mental health expenditures relative to 20 percent state and local revenues and federal block grants. Since 1986, Medicare, Medicaid, and private insurance have funded approximately 46 percent of expenditures for SUD compared to approximately 40 percent by state and local revenues and federal block grants. For comparison with all health expenditures, state and local revenues and federal block grants account for 11 percent of expenditures, whereas Medicare, Medicaid, and private insurance account for 73 percent of all expenditures.26
Per the IMS Institute for Health Informatics, buprenorphine prescription payments are generally correlated with Medicaid expansion: more than 40 percent of buprenorphine prescriptions are covered by Medicaid programs in the eight states that have expanded Medicaid under the Affordable Care Act (ACA) of 2014. Those states with expanded Medicaid coverage are likely to have a higher proportion of buprenorphine prescriptions covered by Medicaid and a smaller proportion paid for by cash compared to states that have not expanded Medicaid coverage. Interestingly, states with higher opioid misuse rates tend to have low Medicaid funding rates for buprenorphine; of the ten states with the highest prescription opioid use relative to their population, eight states have a level of Medicaid funding for buprenorphine use that is lower than national average.27
To respond to the opioid epidemic and increase the capacity to provide high-quality MAT, the 21st Century Cures Act appropriated $1 billion in grant funding to all 50 states and United States territories over 2 years to combat OUD by increasing access to treatment, reducing unmet treatment need, and reducing opioid overdose related deaths through the provision of prevention, treatment, and recovery activities.28 Specifically, the grant will help to improve prescription drug monitoring programs, implement prevention activities, train health care providers, and expand access to OTPs.29 Each state can then appropriate the funds as needed, based on the needs of their population.30 $485 million was authorized for fiscal year (FY) 2017.30
Several federal agencies are funding grants and technical assistance efforts at the state and local level. Recently, CARA authorized $181 million to combat the opioid crisis in all 50 states through discretionary grants.31 At both the state and local level, the HHS Substance Abuse and Mental Health Services Administration (SAMHSA) discretionary grant programs, including Planning Grants for Certified Community Behavioral Health Clinics (CCBHC), Grants to Prevent Prescription Drug/Opioid Overdose-Related Deaths, Cooperative Agreement for the Provider's Clinical Support System--Medication Assisted Treatment (PCSS-MAT), and Target Capacity Expansion: Medication Assisted Treatment--Prescription Drug and Opioid Addiction (MAT-PDOA) are other important sources of funding.
The HHS National Institute on Drug Abuse (NIDA), the U.S. Department of Defense, the FDA, and the DoJ, the HHS Centers for Disease Control and Prevention (CDC), and HHS Health Resources and Services Administration (HRSA) also fund MAT expansion as well.32 As an example, HRSA awarded $94 million to 271 FQHCs in FY 2016 to support the improvement and expansion of SUD services, with a focus on MAT.33
2. DATA AND METHODS
In consultation with the HHS Office of the Assistant Secretary for Planning and Evaluation (ASPE), our evaluation team selected five states for a case-study approach to understanding the MAT workforce and financing policy innovations: California, Missouri, New Hampshire, Ohio, and Virginia. We worked with ASPE to develop a plan for state selection that ensured representation across the following dimensions: (1) policies targeting workforce development among private providers; (2) policies targeting workforce development among public providers; (3) Medicaid MAT financing; (4) private reimbursement policy, including payment bundling and other incentives; and (5) geographic representation. The evaluation team reviewed publicly available resources across all states to identify key innovations and consulted with ASPE on ongoing federal evaluations to preliminarily rank states for inclusion. This initial scan yielded 12 states. The evaluation team then produced a detailed rationale that justified why each of the initial 12 states merit selection and from that recommended five states. The seven states that were not chosen were: Kentucky, Maryland, Massachusetts, Minnesota, Rhode Island, Vermont, and West Virginia.
The five states selected in the end are geographically spread across the United States, politically and demographically diverse, and represent both urban and rural populations. Two of the states, Virginia and Missouri, have not expanded their Medicaid programs. Each state has received a different mix of federal funding targeting MAT expansion, including SAMHSA state targeted response (STR) and Targeted Capacity Expansion--Medication Assisted Treatment: Prescription Drug and Opioid Addiction grants (two states), SAMHSA CCBHC planning grants (three states), CDC "Prevention for States" grants (three states), HRSA Targeted Capacity Expansion grants (all five states), and Medicaid 1115 demonstration waivers related to behavioral health (three states). California and Ohio are top five states in the number of buprenorphine waivers obtained and rely on decentralized MAT administration through county agencies and regional administration through large providers. Virginia also manages public MAT delivery through county agencies, whereas Missouri and New Hampshire do not.
For each state, we conducted an in-depth review of state and local policies using an environmental scan and discussions with stakeholders at both the local and state levels. Analysis of the output from the scan and stakeholder discussions was qualitative and descriptive. No formal qualitative coding analysis was conducted. Analyses focused on expansion of treatment and recovery support services and largely excluded preventive services, such as naloxone distribution.
We scanned Single State Agency (SSA) and other public agencies, and behavioral health advocacy and provider organization websites to obtain the following information: specialty and non-specialty MAT treatment systems; existing MAT capacity and workforce issues; key policies, procedures, reports or other documents related to workforce and financing challenges; and performance metrics used to evaluate policy changes. We also reviewed the existing formal and gray literature. The evaluation team tracked information from the scan in a spreadsheet and used the information to develop a comprehensive profile for each states' MAT system and relevant policies.
The environmental scan also helped identify key stakeholders for discussions. We had discussions with three stakeholders in each state (15 in total) to confirm the accuracy of information gathered during the scan, provide additional context and perspective to the review, and gather additional detail on policy innovations. Stakeholders included state level officials, such as state Medicaid or substance abuse SSA staff; local officials, such as regional or county behavioral health agency directors; and other payer or provider organizations that provide a state or local perspective.
In consultation with ASPE, the study team developed a guide to facilitate discussions with state and local level public program officials, health plan administrators, and treatment providers. The content of the guide was tailored to each stakeholder and broadly focused on the following topics: (1) overview of opioid use and MAT in the state/locality; (2) description of existing specialty and non-specialty treatment systems; (3) key issues concerning MAT infrastructure, legislation, and reimbursement; (4) key issues concerning MAT workforce training, recruitment, and retention; (5) challenges and barriers at the federal, state, and local level for providing MAT; (6) promising/pilot policies for expansion of treatment and recovery support services; and (7) recommendations on policy changes to address identified challenges and barriers. Two evaluation team members conducted 45-minute to 60-minute discussions over the phone with each stakeholder and discussions were audio-recorded to ensure accuracy of the notes. Following the discussion, the evaluation team sent each stakeholder a summary of key points in the discussion and asked the stakeholder to review for accuracy.
The RTI International Institutional Review Board did not deem this evaluation as generalizable research.
3. STATE AND LOCAL INNOVATIONS
3.1. California
California's behavioral health delivery system is largely organized around counties. Counties receive funding from federal block grants, Medicaid and state revenues to administer SUD services to Medicaid enrollees and the uninsured. Services are provided directly through county agencies or contracted through private providers. Historically, MAT has been provided through Narcotic Treatment Programs (NTPs) and limited mostly to methadone. In California, an NTP is synonymous with an OTP. NTPs are licensed by the Department of Health Care Services (DHCS) and programs are required to submit an application that includes a protocol describing the program's operational procedures, organizational structure, and treatment concepts. In addition to obtaining licensure approval from DHCS, NTPs must also receive approval from the DEA and SAMHSA before program operations can commence.34 NTPs provide detoxification and maintenance treatment services to help the patients reintegrate into society. Currently, California has 152 NTPs and they are unevenly distributed through the state--28 out of California's 58 counties (many concentrated in the northern, rural part of the state) do not currently have an NTP.35 Rural areas sometimes cannot justify a full NTP within their area due to smaller populations and larger geographic spread.
Outside of NTPs, the behavioral health workforce historically included a large number of independent providers, many of whom came into the field by virtue of recovery, rather than treatment, and are therefore mainly trained in abstinence-based treatment. Many providers are unwilling to adopt MAT given their training and beliefs, slowing the adoption of MAT more broadly in California. Although stakeholders have not given up pitching the idea of MAT to resistant SUD providers, the State of California is focusing on organizations that are already using MAT to find ways to make it more successful and overcome any reimbursement or organizational challenges that exist. Even when medical providers were willing to adopt MAT, it was difficult for providers to link clients to other SUD treatment services due to multiple points of entry into the county system and the fragmented independent provider network. Counties must coordinate with and leverage their county provider networks to facilitate access to integrated care, including the medications for individuals with SUD. It is key to ensure that there are adequate linkages to assessment and OUD diagnosis for potential MAT patients in medical settings.
Medicaid has become an important source of coverage and funding for MAT. As of January 1, 2017, approximately one-third of Californians--13.5 million individuals--are enrolled in Medicaid (i.e., Medi-Cal).36 The ACA funding given to California for the Medi-Cal expansion group is anticipated to be approximately $17 billion in 2017-2018. Of the approximately 4 million people newly enrolled in Medi-Cal, an estimated 450,000 have an SUD.
Medi-Cal previously offered a very limited set of OUD/SUD benefits that were "carved-out" under the Drug Medi-Cal (DMC) program and separate from medical or mental health managed care and FFS plans. DMC is a treatment funding source for Medi-Cal clients; for DMC to pay for covered services, Medi-Cal clients must receive substance abuse services at a program that is DMC-certified (by submitting an application packet to the DHCS). Previously offered services included outpatient counseling, methadone, and naltrexone only for pregnant or postpartum women and at-risk youth. However, in 2014, Medicaid expansion broadened the SUD services available to all Medi-Cal and DMC enrollees, including intensive day treatment, residential treatment, and inpatient detoxification. Under DMC, MAT must be deemed medically necessary, provided under physician supervision, and provided at a DHCS-certified site. Most SUD services for Medi-Cal beneficiaries are provided through DMC and are generally administered through the county-based system, which includes NTPs and other treatment agencies and providers. Additionally, managed care organizations (MCOs), which typically covered only "general mental health care" that could be provided by a general health care practitioner,37 have new responsibilities to cover SUD services, and some SUD services are also available through FFS Medi-Cal. Individuals who receive medical care through managed care plans must sign up for a plan. Importantly, MAT in outpatient settings can be covered either through Medi-Cal MCO or Medi-Cal FFS, depending on the medication.
On December 1, 2014, buprenorphine/naloxone sublingual film was added to Medi-Cal's list of Contract Drugs. On January 1, 2015, Medi-Cal removed prior authorization requirements for buprenorphine for waived physicians. Beginning on November 2, 2016, long-acting injectable naltrexone (Vivitrol) benefits were extended from only justice-involved Medi-Cal beneficiaries to those served by Local Specialty Mental Health Plan sites of care, which includes county mental health or behavioral health departments and/or associated contracted providers.
Although all three FDA-approved medications for MAT are available to Medi-Cal beneficiaries, California shows relatively low utilization of buprenorphine compared to other states. In 2015, the number of buprenorphine Medi-Cal providers was 1,406, but only 8,542 Medi-Cal beneficiaries received buprenorphine. In other words, there are six beneficiaries receiving buprenorphine per prescriber. Additionally, there is only one Medi-Cal beneficiary receiving buprenorphine for every four patients receiving methadone.38
California is working to overcome three major barriers to expanding MAT. First, NTPs have not traditionally used buprenorphine or naltrexone and there is resistance in the treatment community against MAT. Second, although physicians can bill Medi-Cal FFS/MCOs through Medicaid expansion, there is little integration with the SUD system and prescribing rates are low due to a lack of support. Third, there is also little infrastructure for MAT in rural areas. Infrastructure includes capacity, such as the physical facilities and associated workforce of the SUD treatment system and the range of SUD services that can be provided, as well as system organization, such as the level of coordination within SUD treatment system and the level integration with the physical and mental health system. California began addressing these barriers through several initiatives, including the 1115 Medicaid Waiver, Cures Act funding, the use of FQHCs, and physician mentoring programs.
3.1.1. 1115 Medicaid Waiver
In July 2015, the HHS Centers for Medicare & Medicaid Services (CMS) issued a guidance letter to State Medicaid Directors to inform states of opportunities to design and test innovative policy and delivery approaches for individuals with SUDs.39 California was the first state to receive approval under this guidance, establishing the Medicaid Section 1115 Drug Medi-Cal--Organized Delivery System (DMC-ODS) Demonstration Waiver. DMC-ODS is a voluntary, opt-in pilot program allowing counties to expand access to high-quality care for Medi-Cal beneficiaries who have SUDs. The DMC-ODS Waiver allows for local control of the DMC provider network and administration, and greatly expands DMC services. Participating counties are required to offer a full continuum of care for SUD treatment, including MAT, outpatient services, and residential care modeled after the American Society of Addiction Medicine (ASAM) criteria. In FYs 2016-2017, California spent approximately $140 million in General Fund spending to support implementation of DMC-ODS.40
DMC-ODS improves financing and access to MAT by increasing the scope of MAT in NTPs and financing additional services outside of NTPs. Before Medicaid expansion, buprenorphine was covered under MCOs and FFS Medi-Cal plans for outpatient settings, but not under the SUD package in DMC. DMC now requires all MAT medications to be offered in NTPs, including buprenorphine, in counties that participate in the 1115 Waiver.
Further, counties can directly contract out additional MAT and SUD services covered by the waiver with providers outside of NTP services. Although outpatient physicians could and can still bill for MAT medications under Medi-Cal FFS/MCOs, the waiver better funds additional services under DMC, such as intake, counseling, and medication management, that are associated with MAT. Beyond the additional covered services, counties can vary the rates within the county to account for different costs of living in urban and rural areas. While medication reimbursement did not necessarily increase under the DMC waiver, more costs are now covered related to administration and management.
Ultimately, the waiver is intended to better align the SUD system under DMC. Counties pay providers for their services, then counties submit invoices to the state and settle for costs at the end of the fiscal year. Then, whatever is not matched by Medicaid will come out of the county realignment funds. Funding predominately comes from federal Medicaid match and county realignment funds now, shifting away from state general revenue. While counties and providers get up to speed with the new reimbursement model, block grant funding serves as bridge funding or "fillers" for gaps in the continuum of care that remain uncovered by Medi-Cal/DMC. These gaps lie largely within residential treatment, particularly room and board costs, which are generally funded by federal block grants.
Because counties must actively opt into the DMC-ODS program, there is concern about a potential gap in coverage for Medi-Cal beneficiaries living in opt-out counties that do not have methadone providers. To assuage this, DHCS can directly contract with NTP providers in counties, like San Diego, that chose not to contract with NTP providers through the waiver program.41 DMC-ODS also gives counties the opportunity to propose alternative regulatory and billing models to the state that further facilitate treatment integration. The state has not received any proposals from counties yet.
One key workforce component of the waiver is that it funds peer support workers. Peer recovery navigators, though not formally certified by the state, are billable under the waiver. To obtain certification, they must register with one of the DHCS-approved certifying organizations. Then, from the date of registry, counselors have 5 years to become certified.42 The state allows registered care navigators to bill for services for these 5 years until they get state certified.42
3.1.2. Cures Funding
The 21st Century Cures Act grants allotted $44.7 million to California for the first year of the STR to the Opioid Crisis Grant program.43 The grant focuses on two projects in California specifically: the California Hub and Spoke System and the Tribal MAT Project.43 As of June 2017, California was in the process of meeting with tribal stakeholders to design the Tribal MAT project.
| BOX 1. The Hub and Spoke Model in Vermont |
|---|
| The Hub and Spoke model was first implemented in Vermont. It is a way to develop a system of care to expand MAT via organized regional networks of opioid treatment. In Vermont's model, Hubs are clinics that provide specialized expertise in opioid treatment by assessing opioid users, determining the most optimal medication (methadone, buprenorphine, or naltrexone), inducting patients (e.g., treatment initiation for MAT); providing ongoing care, and transferring stable patients back into primary care. On the other hand, Spokes serve as a regional network of buprenorphine waivered physicians working in primary care settings. Members of these regional Hub and Spoke networks then regularly hold interactive learning collaboratives to develop working relationships, review data on the functioning of the network, and brainstorm solutions for obstacles to network functioning. Lastly, Vermont incorporated MAT support teams comprised of behavioral health staff (counselors, social workers, nurses) who provide support to medical doctors and provide behavioral treatment to augment the medical care and medication provided by the waivered physicians. |
California's Hub and Spoke system is modeled after Vermont's (see Box 1 for more information) and represents an infrastructure investment, as opposed to a change in financing or coverage. In July 2017, 19 treatment centers were selected to serve as the Hubs and will cover 32 counties, seven of which are among the top ten counties with the highest opioid overdose rates. Over the course of the grant, these entities are projected to serve over 24,000 patients.44 NTPs will act as the Hubs and the physicians who prescribe buprenorphine in office-based settings will function as the Spokes. Hubs will serve as the regional consultants and subject matter experts on opioid dependence and treatment. Hubs can also dispense methadone and buprenorphine, provide care to the clinically complex buprenorphine patients, start patients on buprenorphine inductions when needed, and provide support to the Spokes when they need clinical or programmatic advice. Spokes will provide ongoing care for patients with "milder" or more stable SUD, managing both induction and maintenance. A Spoke consists of at least one prescriber and a MAT team to monitor adherence to treatment, coordinate access to recovery supports, and provide counseling. Patients can move between the Hub and Spoke based on clinical severity.38 Professional service fees, including prescribing physician, PA, and NP costs, cannot be reimbursed with the grant funding except in cases where limited initial start-up costs are required or for uninsured patients not eligible for other coverage.
Due to the lack of NTPs that can serve as Hubs in rural areas, implementation efforts are instead focusing on developing the Spokes. In rural areas where there are no NTPs, Medication Units (MUs) will be used as temporary Spokes and work in conjunction with the nearest licensed NTPs. MUs are smaller facilities whose main task is to dispense medications. Patients receive their physical, induction, counseling, and other services at the NTP; however, once stabilized, they can receive their medications at the MU in their community. These MUs will provide medication and testing services and will then be linked to the nearest NTP if the patient requires further treatment. This new Hub and Spoke infrastructure is intended to increase the availability of appropriate medications for patients in rural areas.
3.1.3. Federally Qualified Health Centers
FQHCs are federally-funded non-profit health care centers or clinics that serve medically underserved populations and areas. As of August 2016, there were 954 active FQHCs in California, the largest number among all states, treating more than 3.4 million patients each year. They are primarily engaged in providing services that are typically furnished in an outpatient clinic. Among California FQHCs in 2014, almost all provided mental health and/or substance misuse treatment counseling.45 FQHCs provide an efficient model of integrated care coordination as SUD screening occurs within the county health systems and referrals to physicians for MAT evaluation or counseling are readily available through county SUD services. FQHCs have been growing in number and overall capacity recently, driven largely by Medi-Cal FFS/MCO payment rates that exceed the Medi-Cal FFS/MCO physician fee schedule and by federal grants. This rapid growth particularly affects publicly-funded insurance and its enrollees.
In California, many FQHCs have begun providing MAT, but face a large barrier of same-day billing issues. Medi-Cal FFS/MCOs cover the costs of the physician services in primary care settings, whether the visit is for primary care or SUD treatment. However, covering the costs of other SUD-related services, such as behavioral health treatment, behavioral health counseling, and group therapy, is not as simple. Both medical and behavioral health providers in FQHCs can bill Medi-Cal FFS/MCOs for services, but not on the same day. FQHCs cannot bill for two separate provider visits on a single day, limiting the clinics' ability to offer same-day integrated services such as MAT and behavioral counseling. Thus, a behavioral health provider visit in the FQHC may not get reimbursed if the patient needs to see a medical provider on the same day. Organizations find grants that reimburse these support and other recovery services so that office visits are more efficient and convenient for patients, thus increasing treatment adherence. As of January 2017, 36 California FQHCs received funding from HRSA to provide MAT services.38 One stakeholder associated with an FQHC noted the use of HRSA's 340B Drug Pricing Program to cover the other related cost of buprenorphine and oral naltrexone administration.46 The 340B program allows the FQHC to purchase medications at a discounted price, but still charge the normal reimbursement rate. This allows the FQHC to recover other costs of administration.
FQHCs may also serve as Spokes under the Hub and Spoke system being implemented in California, especially in rural areas. Thus, FQHCs have become mainstays of local health care safety nets, not only for primary care, but also for specialized care and support services associated with SUD.
3.1.4. Mentoring Programs
In California, as many as two-thirds of physicians who are waivered to prescribe buprenorphine are not prescribing it. Stakeholders believe that more physicians would prescribe buprenorphine if they had more clinical guidance from experts on how to treat patients with MAT. Thus, California is using federal grants to fund mentoring programs for waivered physicians to learn how to manage MAT patients and build support networks with other office-based physicians and treatment centers.
California is also using academic detailing (see Exhibit 1 for more information47) to assist in efforts to identify and train buprenorphine prescribers. Academic detailing identifies waivered prescribers that can become champions in their community and encourage other physicians, NPs, and PAs to become waivered. Additionally, the California Department of Public Health contracted with San Francisco County for academic detailing services, and a curriculum was developed through this project that can be utilized across the state to support activities in MAT expansion. California will also promote the use of the National Clinician Consultation Center's Substance Use Warmline which provides substance use evaluation and management advice to health care providers on behalf of HRSA. Warmline's goal is to provide "real time" education and clinical decision support via case-based telephone consultation to primary care providers. Consultation is free and confidential.
| EXHIBIT 1. Academic Detailing to Increase the Number of Waived Providers |
|---|
 |
| ALT Text: Exhibit 1 is a diagram that visualizes academic detailing to increase the number of waived providers. The left side of the exhibit has a circle with 4 benefits of academic detailing in bubbles at the top, bottom, and either side of the circle. In the top circle is "Convenience for the provider," in the bottom circle is "Digestible information," in the left circle is "Engaging presentation," and in the right circle is "One-on-one interaction." In the center of the main circle is another circle with text reading "Academic Detailing." A speech bubble to the right of the 2 concentric circles reads, "Pharmaceutical companies have proven that detailing--using brief, in-person visits to share 'details' about a drug's efficacy--is an effective sales tool. 'Academic detailing' borrows these techniques to support health care goals, including promoting toolkits and training materials to support safer opioid prescribing practices. Academic detailing is an interactive educational outreach method to engage physicians around evidence-based information to improve patient care." |
With the help of the California Health Care Foundation and other federal funding, efforts to increase use of MAT in primary care have been launched, including learning collaboratives for community health centers and DATA 2000 waiver trainings. These mentoring programs aim to improve quality of care downstream for all SUD patients.
3.2. Missouri
Missouri's public MAT delivery system is centralized through the state and is not highly utilized. Missouri's average rate of buprenorphine use is in the lowest third of all states. Per IMS, there were 22 buprenorphine prescriptions per 1,000 persons in Missouri in 2016, relative to a national average of 39 prescriptions per 1,000 persons.27 The rate of buprenorphine use in Missouri was 2.6 per 100 opioid prescriptions, relative to the national average of 5.6 per 100.27 Historically, MAT has been provided through OTPs and other residential treatment centers certified by the state that focus on short-term residential treatment to stabilize and release patients. SUD treatment sites are reimbursed by Medicaid for these acute interactions through an FFS payment structure. Because Vivitrol is more expensive than other medications, there is financial incentive for OTPs and residential treatment centers to do a rapid detox, administer Vivitrol, and get the patient discharged. Current preferences for Vivitrol could also be partially cultural in that providers might be more receptive to giving an opioid antagonist, like Vivitrol, rather than an agonist, like buprenorphine or methadone.
Stakeholders indicated that the largest obstacle to MAT delivery is the lack of willing prescribers. There are workforce shortages in every mental health discipline--licensed counselors, licensed social workers, nurses, physicians, even technicians.
Missouri did not expand Medicaid in 2014, therefore, they predominately use federal Substance Abuse Prevention and Treatment (SAPT) block grant funds and state general revenues to finance most MAT services for the uninsured, limiting overall funding. Given stagnant block grant and state revenues, it is difficult to expand MAT. The SSA, the Department of Mental Health (DMH) Division of Alcohol and Drug Abuse, has limited resources to initiate new contracts with office-based physicians and thus expanding access to buprenorphine through office-based physicians is a challenge. As the SAPT block grants and other opioid-related funding mechanisms come through the SSA, it is cumbersome to reroute these funds to general medical providers and FQHCs. Likewise, partner agencies, such as Medicaid, can fund MAT, but lack the coordination or funding for related counseling and other SUD services. Although funding is theoretically available, the siloed nature of funding mechanisms to certain agencies inhibits disbursement. Stakeholders cited a need for umbrella agreements that can be flexibly disbursed. Multiple stakeholders acknowledged that expanding Medicaid could address some of this and receiving the enhanced federal matching funds would greatly increase capacity.
Outside of the contracting process, there is significant administrative burden for prior authorizations and other assessment and eligibility paperwork. For example, MAT is available under private insurance but providers noted insurers are tough to navigate. For patients, many insurers apply high deductibles and cost-sharing burden and set low treatment limits. For providers, many insurers require prior authorization 24 hours in advance and often exclude professional fees from bundled payments.
3.2.1. Altering Contracts to Better Use States Revenues and Block Grants
Even with stagnant funding, the state has been able to increase MAT funding through modifications to its contracting process with existing providers. The state has prioritized buprenorphine and a disease management model that shifts away from the strong reliance on residential treatment. Stakeholders indicated that the current system incentivizes residential care that is expensive and potentially inconsistent with the evidence-base.
Although the state is limited in the ability to initiate contracts with new providers, they have modified contracts and requirements for existing providers that have increased funding for buprenorphine and other related services with a strong evidence-base. In a formal memorandum, the state noted that MAT must be prescribed according to the evidence-based practices and informed providers that the state would monitor treatment patterns for compliance.27 Missouri's DMH mandates that in order to remain certified and contracted with DMH, an agency must ensure the availability of all forms of MAT for OUD, including buprenorphine products and injectable and oral naltrexone.48
The state has an advanced data system--the Customer Information Management, Outcomes and Reporting (CIMOR) system--that monitors service provision and expenditures. CIMOR helps inform compliance by providing a database model of all client admissions and discharges, program assignments, demographics, services provided and various other outcomes reports required by the state.49 Through an open dialogue, state-contracted providers indicated that reimbursement levels were inadequate to cover actual implementation and pharmacy costs of MAT. In response, the state is also using this data system to work with providers to analyze their expenditures and increase reimbursement rates to better cover MAT overhead costs. By increasing reimbursement for more cost-effective, longer-term MAT care, the state hopes to offset spending on residential treatment.
Private providers have also found a way to integrate office-based physicians and other providers that can prescribe MAT. One approach by a private behavioral health treatment agency is to act as "middle man" for prescribers: the agency created an informal local network of subcontracted, independent providers to prescribe MAT. The providers bill the agency for MAT, and the agency bills the state. This arrangement is easy and attractive for independent providers and has allowed the behavioral health network to quickly increase their prescribing capacity. The network also noted their recruitment strategy focused first on selling the business case to office managers, highlighting guaranteed payment at predetermined rates and that the network was easier to work with than most insurance companies. For the network, it allows broader access to Medicaid, block grants, and other state revenues since they can tap these mechanisms to not only pay for medications, but laboratory tests and provider time.
A final contracting mechanism leverages the state's purchasing power to establish agreements with pharmaceutical companies to cut the expense of Vivitrol and with laboratories that perform tests at a much lower cost than larger hospital laboratories. Volume purchase contracts save dollars and make MAT services available to a broader population.
3.2.2. Reducing Administrative Barriers to MAT in Medical Settings
Previously, Missouri had a challenging prior authorization process to induct patients on buprenorphine: a patient originally had to have a full work-up diagnosis and complete assessment to be granted admission into a Medicaid-funded or state-funded SUD program, followed only then by a referral to MAT. One provider noted that it could take 4-6 hours to obtain prior authorization for a single patient. Missouri recently changed its prior authorization policies for buprenorphine and buprenorphine/naloxone to require only a diagnosis of opioid drug dependence in the last 2 years; a current assessment can then occur within a 30-day grace period. This reduces the time to induct patients on buprenorphine treatment. Another policy change allows the prescribing providers to complete the MAT screening and eligibility protocol instead of first needing a behavioral health provider to file a referral, thus further cutting down time it takes to induct individuals on MAT. Allowing these administrative functions to be completed once treatment has already begun and removing that additional hurdle before treatment initiation has significantly increased access to and initiation of MAT for individuals covered by Missouri's Medicaid.
3.2.3. CCBHC PPS
In 2016, Missouri was one of only eight states selected by SAMHSA and CMS to pilot implementation of a Medicaid prospective payment system (PPS) for community behavioral health services. Missouri's CCBHCs serve a number of counties that have been designated by HRSA as medically underserved areas and mental health professional shortage areas. All individuals with a behavioral health diagnosis are eligible for services in Missouri under this Demonstration Project. The demonstration award provides an enhanced federal match for 2 years and a platform for the federal recognition of CCBHCs. This will help to transform them closer to the FQHC model of service and reimbursement by shifting Medicaid reimbursement for CCBHCs from an FFS model to a cost-based reimbursement model that promotes more cost-efficient quality care.50 Missouri's CCBHC PPS Demonstration Project integrates services related to mental health and substance use treatment services that were previously funded through the SSA into Missouri's Medicaid State Plan. CCBHCs have not traditionally treated SUD, but were used for addressing serious mental illness and comorbid physical conditions like diabetes. Federal requirements changed, and now CCBHCs are required to have a waivered buprenorphine prescriber and to offer MAT.
The Demonstration Project, which began on July 1, 2017, and will run through June 30, 2019, is designed to demonstrate the cost-effectiveness of converting Medicaid reimbursement for CCBHCs from an FFS system to a PPS system while improving the availability, accessibility, and quality of community behavioral health care. Participation in the Demonstration Project meant that organizations would no longer be reimbursed on an FFS basis for services, but rather the costs of those services were built into each organization's PPS rate. As one stakeholder noted, it is often inefficient to bill in 15-minute increments for patients with chronic conditions of SUD and may encourage volume billing. PPS shifts emphasis away from volume to quality. It is hoped that the PPS system will allow for more flexibility for providers in how they spend their time and more individualization of treatment for patients than did the FFS system. In developing PPS rates, many providers had never done detailed cost reports and had to use existing service expenditures as well as anticipated costs under the demonstration project. The state and the CCHBC worked with a private contractor to review cost reports and made recommendations for the rates.
| BOX 2. What is a PPS and How Does it Incentivize Quality and Efficiency? |
|---|
| Prospective Payment System (PPS) is a system with a fixed payment amount per patient that applies uniformly to all CCBHC services rendered by a certified clinic during a patient visit. Missouri chose a daily payment rate, allowed under CMS guidance, which is (PPS-1), calculated by dividing total annual allowable expected CCBHC costs by the total annual number of CCBHC daily visits. This results in uniform payment amount per day, regardless of the intensity of services or individual needs of clinic users on that day. Missouri developed a "blended PPS-1 rate" that deviates the CMS CCBHC rate by adjusting for the types of specialized staff each clinic may use. PPS rates vary from $178.63 to $252.26 for the initial year. If CCBHCs meet defined outcome goals for six different quality measures, it triggers a 1 percent bonus payment. These goals will be set by using the FY 16 state-wide Missouri DMH average as a benchmark. An individual CCBHC will have "met goal" for a specific measure if it performs above the benchmark rate or if it shows improvement over its own FY 16 rate during the Demonstration Year. This is intended to reward both high performance and continuous quality improvement for all CCBHCs. |
This switch to PPS, although ideal in theory, required retooling the state's information systems, which proved to be complicated given the limited state agency staff and information technology resources that would be needed to train providers on the new standards. Both the DMH and MO HealthNet information systems will require substantial programming and development to process reimbursements and collect the required data. Ultimately, though, stakeholders hope this shift in payment structure will make reimbursement rates more sensible for providers (reimbursement rates may in fact rise) as they are based on actual costs, and make the SUD treatment system more effective. State-contracted providers outside of the demonstration are preparing to switch to this system in several years and think it will be beneficial to them as well.
3.2.4. Using Grants to Expand MAT in Other Settings
Using multiple federal grants, Missouri is improving different aspects of its SUD delivery system. Missouri is largely using its $20 million in Cures Act funding to hire multi-disciplinary implementation teams to build capacity in emergency departments and primary care. Stakeholders believe that by hiring experts who are knowledgeable about MAT and financing those individuals to provide training, education, and resource development, they can build capacity outside of the behavioral health system. This way, the funding will go toward coordinating existing resources and capitalizing on existing infrastructure and programming to enhance access across systems. Stakeholders felt like this would be more effective than funding services in a newer setting for a limited period.
The multi-disciplinary teams are comprised of a physician, nurse, addiction counselor, peer support worker, and a billing administrator. The teams train medical providers, help to reduce stigma and negative attitudes towards MAT, and span across medical and behavioral health networks to break down barriers. In funding these teams, the state hopes to overcome large start-up costs and knowledge deficits in these new settings. The teams also work with providers to figure out how to tap existing state funding available in other agencies outside of the SSA.
Additionally, the state offers providers a $500 incentive from Cures funding for completing the buprenorphine waiver training and is funding mentoring and support programs for new providers to help ensure a sufficient workforce, especially in rural areas. Additionally, telehealth has helped to bridge the gap with medication services in rural areas where a lack of public transportation and immense poverty make finding a reliable ride to a doctor's appointment particularly challenging.
The SSA cannot directly reimburse MAT at FQHCs because they are not certified by the state to provide SUD treatment. The HRSA program grants are supporting seven Missouri FQHCs in their efforts to expand SUD treatment. Additionally, provider partnerships with FQHCs and local doctors were formed to address needs on a local level, promote community partnerships and leveraging of resources as well as implement telehealth strategies.
Missouri also was awarded an MAT-PDOA from SAMHSA in 2015, which provides $1 million per year for 3 years. The funding will focus on increased MAT capacity in two high-risk areas: suburban St. Louis and "SA 17," a group of eight counties in southeast Missouri. The funding was directed to existing MAT providers to implement integrated care and disease management models for treating SUDs, including outreach and peer support to increase long-term utilization of MAT in accordance with evidence base.
3.3. New Hampshire
Publicly-funded behavioral health care and MAT have been under-developed in New Hampshire until recently. Prior to expansion, Medicaid offered limited SUD benefits--although the MAT prescriptions were covered by Medicaid, almost no other services were. New Hampshire Medicaid now covers methadone under FFS and MCO plans. Under FFS plans, methadone is covered only as a medical benefit for use in accredited outpatient NTPs; primary care practices generally do not provide MAT.51 Methadone is only offered through eight NTPs across the State of New Hampshire, leading to wait lists of up to 2 months52and discouraging referrals. To help alleviate this, the New Hampshire Bureau of Drug and Alcohol Services (BDAS) currently contracts with 15 SUD treatment providers across the state to provide a wide and comprehensive set of services, including MAT. Approximately 5.5 percent of the estimated 106,000 New Hampshire residents aged 12 and over who meet criteria for SUD receive SUD treatment services under BDAS-contracted services. Another 18 percent of individuals access SUD treatment services through the New Hampshire Health Protection Program (NHHPP), the Medicaid-funded health care program for low-income residents, or through standard Medicaid. That leaves over 76 percent of New Hampshire residents who are not receiving state-supported services for SUD; some of these individuals may be able to access SUD treatment services through private insurance or self-pay.53, 54
New Hampshire faces many workforce challenges, some specific to MAT and others more broadly. As with many states, there are not enough prescribing doctors in New Hampshire that are interested in, willing to, or have the capacity to prescribe any form of MAT. Specifically, recovery support services are an under-developed service area with only 26 recovery support workers certified by the state.52 Further, there are only 49 active providers that can prescribe Suboxone in the state.52 According to several stakeholders, many providers simply cannot take on another patient population. There is also stigma against MAT from the recovery community itself that stems from abstinence-based programs, further hindering recruitment of providers.
Geography plays an important role in the workforce shortage. In the southern part of the state with a higher population density, many people live in New Hampshire, but work in Massachusetts for a significantly higher salary. This wage discrepancy causes major workforce shortages in New Hampshire as providers are incentivized to do the same work across state lines for more money. Turnover and limited provider supply are large concerns. Northern New Hampshire is very rural, and transportation, workforce, and infrastructure are large issues. Telehealth has become a popular and effective strategy to address shortages in rural areas, especially by increasing staff retention and eliminating long travel times for patients to get to the nearest provider in the city. However, connectivity issues with the Internet and cell service in many rural areas may make telehealth less viable.
An essential workforce development program in New Hampshire has been the State Loan Repayment Program for providers. This program implements loan repayment incentives for health care professionals working in medically underserved areas of the state and who are willing to commit and contract with the state for a minimum of 3 years. This program serves as one of the only ways that rural hospitals can retain their workforce. There currently is an initiative to increase the amount of state funding for the loan repayment program.
New Hampshire also has limited data infrastructure to understand demand or performance. Long wait lists for treatment continue to be a problem, and one stakeholder pointed out that they do not know how many unique patients are in queue.
3.3.1. Medicaid Expansion
Medicaid expansion is a cornerstone of broadening access to MAT in New Hampshire. Estimates suggest one in six individuals that gained coverage under the expansion have extensive mental health or substance use needs.55 New Hampshire's Medicaid program started offering comprehensive SUD benefits in August 2014, through fully insured, qualified health plans (QHPs) under the umbrella of the NHHPP. QHPs were offered through the state's online insurance exchange and available to all individuals in the state. Most Medicaid beneficiaries are covered under the QHPs and the state subsidizes the plan. Unlike the FFS/MCO models in traditional Medicaid, the QHPs are subject to parity laws and regulated by the Department of Insurance. By expanding coverage via QHPs, many more individuals can access services that are reimbursed by private insurance companies. This has created both opportunities--an increase in coverage for funding services is an opportunity to build capacity--and challenges, as both insurance companies and SUD service providers work to become familiar with new legal requirements and reimbursement systems.
New Hampshire's QHPs include a robust SUD benefit package with peer recovery services, intensive outpatient detox, and counseling as part of the medical component of MAT. Under expanded Medicaid in QHPs, these covered services are also reimbursed at a higher rate than under the pre-expansion psychotherapy benefit. Providers can seek reimbursement for these additional services now, and with higher reimbursement rates overall, it incentivizes providers to expand behavioral services and provide integrated care. This adjustment is beneficial for both patients and providers as it is now possible to treat the "whole person" in one setting rather than just the "medical" components previously billable to Medicaid.
Medicaid expansion also freed up more general state revenue dollars for infrastructure and workforce development. Stakeholders noted that it was a critical shift of state revenues to move from funding services to funding infrastructure, allowing for expansion of MAT. A contract with Bi-State Primary Care Association provides $870,000 to recruit primary care, behavioral health, and SUD professionals to practice in New Hampshire.56 The state invested funds from the Governor's Commission on Alcohol and Drug Abuse Prevention, Treatment, and Recovery to focus on building MAT in community health centers and hospitals. Because hospitals own most of the primary care practices in rural communities, investment in the hospital associations can help primary care practices start offering MAT. Additionally, Senate Bill 533 authorized BDAS to enter an agreement that provides $2 million to support direct grants for the creation, initiation, expansion, and/or operational costs for peer recovery support services.56
Medicaid expansion also introduced a billing challenge for independent behavioral health providers. With an increase in insurance coverage, providers now had to navigate patient's insurance coverage more often and handle claims. To help independent behavioral health providers navigate the new coverage system, the New Hampshire Provider Association created a third-party billing service to help process claims. The service costs a monthly fee of 8 percent.
3.3.2. 1115 SUD Waiver
New Hampshire obtained an 1115 SUD Waiver to combat the opiate crisis via three important pathways: improve care transitions, promote integration of physical and behavioral health, and build behavioral health treatment capacity. The key drivers of this delivery system reform are Integrated Delivery Networks (IDNs): seven new, regionally-based networks of physical and behavioral health providers as well as community supports. IDNs serve all Medicaid beneficiaries through the FFS system or Medicaid Care Management program. The waiver will increase community-based behavioral health service capacity through the education, recruitment, and training of a peer workforce and fostering collaboration among partners including FQHCs, mental health providers, SUD clinics, hospitals, primary care providers, peer support counselors, and others. To overcome significant shortages of licensed professional, the state is currently examining whether unlicensed workers, such as peer recovery workers could provide certain types of billable services under the waiver. One stakeholder noted that New Hampshire has a strong hospital association and strong hospital delivery system in the south which will be instrumental in anchoring the IDNs.
Funding for this transformation waiver provides up to $150 million over 5 years, with performance-based funding distribution and support for transition to alternative payment methods. Up to 65 percent of Year 1 funding will be specifically routed for capacity building and planning. Over the 5 years, accountability will shift from process metrics, such as steps taken by the state to manage the waiver program or steps taken by an IDN to organize its network, to performance metrics, such as quality, access, and utilization indicators that measure state-wide and local impact. Then, payments from CMS to the state and from the state to IDNs will be contingent upon meeting these established performance metrics. The state will move Medicaid payment from volume-based to primarily value-based payment over the course of the demonstration years. New Hampshire's funding model will be better suited for long-term sustainability post-demonstration by moving at least 50 percent of payments to Medicaid providers into alternative payment models to reward performance consistent with IDN objectives and measures.
Although this approach is still in an early implementation phase, stakeholders noted that each of the seven IDNs have chosen an SUD-specific project for Years 2 and 3 of implementation.
3.3.3. Reducing Administrative Barriers
In November 2015, the New Hampshire Insurance Department began a Market Conduct Examination of private insurance company practices when providing coverage for substance use treatment. They specifically examined preauthorization, claim denials, and utilization review practices for SUD claims. The Department will determine whether carriers are complying with applicable legal requirements, including the mental health parity laws.56 Additionally, in July 2017, HHS finalized the tools that will be used by New Hampshire's two MCOs to complete the Parity Analysis to be submitted to CMS in October.57 This examination aims to reduce the administrative barriers imposed by private insurers for individuals seeking SUD treatment.
In an effort to improve access to care for those obtaining SUD services through private insurance, Senate Bill 576 removed barriers to accessing treatment and increased the likelihood of timely treatment at the appropriate level of care. The legislation approved immediate access for crisis situations and requires insurance companies to use the ASAM criteria when determining whether an SUD treatment service is "medically necessary" (and thus covered by insurance). Requiring insurance companies to use the same ASAM criteria that the treatment providers already use will facilitate direct communication and explanation of level of care decisions. The Bill also mandates that insurance companies cannot require prior authorizations for the first two routine outpatient visits for SUD treatment services associated with a particular episode of care.56 In 2017, New Hampshire passed additional legislature (Senate Bill 158) that restricts public and private insurance carriers from requiring prior authorizations for MAT more than once per 12-month period. Previously, prior authorizations were required every 30 days for these medications. The new once-yearly policy lessened that burden for both prescribers and patients.
The state has also been proactive in fighting other coverage barriers in the Medicaid program, such as a cap on the number of urine analyses per month and same-day FQHC billing. Medicaid caps the number of urine screens to 1-2 per month, but providers feel that is not sufficient when initiating new patients on MAT. The state is still working through how to establish the appropriate number of urine analyses for MAT patients and maximize the ones allowed. Additionally, although FQHCs can receive reimbursement for two encounters in 1 day if one is a behavioral health visit and one is a medical visit, MAT is considered a medical visit. This poses problems if a patient needs MAT and another medical visit, such as a prenatal appointment or a primary care visit, on the same day due to transportation issues or other convenience factors. Modifiers were added to medical codes to indicate that if a patient has two appointments in 1 day, one of the appointments was specifically coded as MAT and thus billable as well. These reforms will allow Medicaid patients to receive more integrated and efficient treatment at FQHCs.
3.3.4. Expansion into Primary Care and FQHCs through Grants and General Revenue Investment
FQHCs have effectively been implementing the Screening, Brief Intervention and Referral for Treatment (SBIRT) program. SBIRT is an early intervention and treatment service for individuals with or who are at-risk to develop SUD; it can be integrated effectively into general medical settings and is a major federal policy initiative (see Exhibit 2).58 Universal screening in medical and community settings offers a chance to identify non-dependent substance misuse and a brief intervention can reduce at-risk substance misuse to a lower level of severity. To complete the continuum of care required with SBIRT, referrals to appropriate treatment can be made for those who need it.59
| EXHIBIT 2. SBIRT at a Glance |
|---|
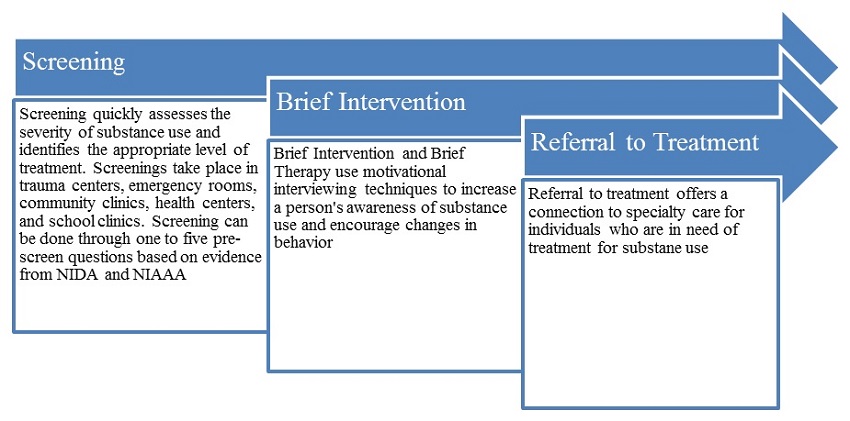 |
| ALT Text: Exhibit 2 is a flow chart that visualizes SBIRT at a glance. The 3 components of SBIRT, screening, brief intervention, and referral to treatment, are displayed in 3 overlapping arrows pointing to the right. Below each arrow is a box describing that component of SBIRT. The box under "Screening" reads, "Screening quickly assesses the severity of substance use and identifies the appropriate level of treatment. Screenings take place in trauma centers, ERs, community clinics, health centers, and school clinics. Screening can be done through 1 to give pre-screen questions based on evidence from NIDA and NIAAA." The box under "Brief Intervention" reads, "Brief Intervention and Brief Therapy use motivational interviewing techniques to increase a person's awareness of substance use and encourage changes in behavior." The box under "Referral to Treatment" reads, "Referral to treatment offers a connection to specialty care for individuals who are in need of treatment for substance use." |
FQHCs and community clinics are now leveraging the momentum from SBIRT to add MAT. SBIRT helped to pave the way because centers were already implementing SBIRT so the shift was more acceptable and justifiable. This also helped providers who currently had SBIRT services recognize that many of their current patients need MAT, therefore debasing the argument that "they do not want MAT patient populations in their clinics."
Provider associations are also working toward recruiting varying education levels of providers for FQHCs such as physicians, PAs, and NPs, that will support MAT services. PAs and NPs can become waivered to prescribe buprenorphine now, and the first phase of training proved to be very popular among health centers. Provider retention and burnout is a critical issue, especially in smaller centers where there is only one waivered physician; training and certifying physician's assistants and NPs to also be able to prescribe will go a long way to help with this problem. Estimates from stakeholders suggest 150 additional providers have been waived during the initial training sweep. Guidance modules for providers on MAT best practices were developed by the state and have been very well-received and implemented. Bi-State Primary Care Association and the New Hampshire Medical Society have also partnered to facilitate a support community of MAT providers. A key strategy is providers working with other providers and hearing from peers that MAT works, is manageable, and is an important part of SUD treatment. The Governor's Commission created a Healthcare Task Force that includes key people in the medical community as strong partners to educate and encourage participation in these training programs.
The Foundation for Healthy Communities, a non-profit organization that engages in innovate partnerships to improve health and health care in New Hampshire, has also contracted to work with hospital-based primary care clinics in order to make the transition for all primary care easier. Approximately 90-95 percent of all primary care practices are within a hospital network in New Hampshire, so working with hospital networks to get MAT established is essential. The Foundation will work with Chief Medical Officers and personnel in the records departments of hospitals, so that when other primary care offices decide to offer MAT as well, the infrastructure and foundation will already be set. Hospital networks already have behavioral health staff that they can leverage for care coordination to make the transition easier for physicians. The Foundation's contract calls for ten primary care practices to offer MAT within the next year, but stakeholders are confident that that expectation will be exceeded by the end of July.
Bi-State is following a similar approach with FQHCs to have behavioral health staff, SUD treatment professionals and case management staff on board already so implementation of MAT is more seamless going forward.
3.3.5. Credentialing Reciprocity
To address the behavioral health workforce shortage, New Hampshire is simplifying the licensing process for licensed alcohol and drug counselors (LADCs) from other states to move to and practice in New Hampshire. The program does not apply to providers that could prescribe MAT, as LADCs cannot prescribe MAT medications, but addresses a significant shortage of SUD service providers that support prescribers. A new bill was put forward that requires the New Hampshire Board of Licensing for Alcohol and Other Drug Use Professionals to look at reciprocal license applications, and if a decision is not made within 60 days, they must give LADCs and mental health counselors a provisional license for 60 days until they decide. Stakeholders noted that there is a delicate balance between ensuring that there are quality providers and that they get through the licensure process quickly; it is important that providers receive enough supervision and continue to be required to undergo supervision even after licensure, but it's also important not to overdo it and put too much strain on the workforce. The legislation is not an external signal as much as an internal enforcement mechanism for the licensing board.
3.4. Ohio
Publicly-funded behavioral health care in Ohio is a state-supervised, county-administered system of care through Alcohol, Drug Addiction, and Mental Health Boards, a.k.a. "county boards." County boards do not actually provide services, but are responsible by state statute for planning, evaluating, and contracting for SUD services for their counties with state oversight. Ohio Mental Health and Addiction Services (OMHAS) allocates funds to each of the 51 county and multi-county board areas which, in turn, contract with treatment providers to provide MAT treatment services. Specifically, boards work on recovery support that Medicaid does not cover, including housing and transportation services.60 County boards support specialty SUD treatment services using state and local appropriations (county tax levies) combined with the federal SAPT block grant. Due to this county-level responsibility and discretion, the county board structure creates many contrasting payer environments in Ohio.
The use of county levies to fund MAT and recovery support services is also critical to the system, supplying $400 million in funding. However, not all counties have a levy, and there are large funding gaps between the 75 counties with levies and 13 counties without. These 13 counties without levies are mostly concentrated in rural areas in southeast Ohio or along the Ohio River, where the opioid epidemic is worse. One stakeholder noted that rural counties that have even a small levy (e.g., $250,000) fare better than those with no levy at all. One consequence of the levy system is that the opioid epidemic is causing counties to divert levy funds away from mental health.
Stakeholders report the county programs are often at capacity, overwhelmed, and patients endure long wait lists. Broadly, detoxification and residential treatment capacity is low, especially in rural areas. OTP support is low, as there are only 11 operating clinics in the state and entry processes are arduous. Additionally, state regulations previously required community SUD services providers be certified by state for a minimum of 2 years prior to becoming licensed to provide methadone treatment at an OTP.
There are strong regional biases towards certain medications. Many rural providers are concerned with diversion of buprenorphine products. Thus, even though the state passed legislation to better monitor prescribing (House Bill 93 enhanced Ohio's Automated Rx Review System, limited prescribers' ability to personally furnish certain drugs, and improved licensing of and law enforcement involving pain management clinics), more expensive Vivitrol is preferred in many parts of the state. However, one stakeholder noted that a patient needs to be opiate-free for at least 7 days prior to Vivitrol injection, which complicates induction due to a lack of appropriate facilities and prescribing providers.
3.4.1. Leveraging Medicaid to Reform MAT Delivery
Ohio has been implementing comprehensive Medicaid reforms to expand access to SUD treatment services since 2011.61 Three initial reforms included shifting responsibility to provide Medicaid matching funds from county boards to the state, adding coverage of MAT to Medicaid,62 and Medicaid expansion. The shift in the matching funds meant that overall, more state resources were spent on Medicaid and less burden was placed on local resources. This ensures a more consistent provision of Medicaid treatment services state-wide. Together, these three reforms added more than $1 billion to Ohio's behavioral health system capacity.62
Medicaid expansion in particular made a significant impact on MAT delivery. As of May 2016, Medicaid expansion had provided health insurance coverage to over 700,000 Ohioans. Before Medicaid expansion in Ohio, adults with an SUD were not covered by Medicaid because addiction was not considered a disability on its own. Adults could only enroll in Medicaid if they had a comorbid disability. Coverage was expanded to 400,000 residents with behavioral health needs who previously relied on county-funded services or went untreated. Among those newly-covered after the expansion, 32.3 percent were diagnosed with SUD or dependence, and 3.6 percent were specifically diagnosed with OUD and opioid dependence.63 The expansion of Medicaid to include low-income adults was an instrumental benefit to SUD treatment facilities within Ohio; one stakeholder noted that "if [Ohio] lost expansion on a federal level, it would be a devastating hit to MAT." Medicaid expansion also indirectly increased service provision to the remaining uninsured by freeing up local funds to focus on local needs, like housing and employment supports. Stakeholders noted that the increased demand for MAT and other SUD services highlighted medical and behavioral health workforce shortages and SUD knowledge gaps among the medical community for policy makers, increasing the priority of workforce development and training at the state level.
More recently, Ohio began implementing a redesign of Medicaid behavioral health services (the "Behavioral Health Redesign"). Ohio is updating and modernizing Medicaid's behavioral health insurance codes and practices to meet national coding standards (American Medical Association, Healthcare Common Procedure Coding System, Medicare, and National Correct Coding Initiative/Medically Unlikely Edits), and is moving every individual with behavioral health needs to a private sector Medicaid managed care plan beginning in January 2018.64 The redesign is separating and repricing 17 existing bundled service codes (e.g., community psychiatric supportive, case management, health home) and providing lower acuity service coordination and support services. In total, 150 codes are being implemented. Specifically, the redesigned reimbursement policy now allows a provider to bill for day treatment and group counseling on the same day, and to bill for a physician visit (E&M code) and a nurse visit (H-code, T-code) on the same day.64 Elevating the behavioral health code standards will allow for the reimbursement system to more accurately reflect the services provided and the providers' levels of expertise and training, and to demonstrate clarity on coding as both behavioral and physical health are fully integrated into managed care.64 It is anticipated that although per-service reimbursement will be lower, expansion in the number of billable service codes will increase total provider reimbursement.
The redesign also requires providers employed by community behavioral health agencies to enroll in Medicaid managed care plans and to be reported on Medicaid claims, an operational change for SUD providers. For SUD services, the redesign represents a "carve-in" of Medicaid SUD services. Some SUD providers have reported concerns that the redesign will increase the stringency of prior authorizations and that the provider enrollment process into the eight different managed care programs may deter some providers, especially small, rural providers. For physical and mental health providers already enrolled, these operational changes may not be as much of a concern.
3.4.2. Expansion in Emergency Departments
In the spring of 2017, Ohio received a $26 million 21stCentury Cures Act grant60 and is using this grant funding to facilitate MAT induction in emergency departments, bridging long waiting lists for patients to enter office-based opioid treatment (OBOT) and OTPs. Emergency departments are only allowed to give patients 3 days' worth of medication, so after someone gets inducted in MAT within an emergency department, they have to be transferred elsewhere. Emergency departments can apply for a grant to help facilitate care coordination, but they must agree to one of four models of care; Exhibit 3 outlines these four models. Essentially, to ease the patients' transition from the emergency department, the four models provide an interim layer of primary care physicians for intermediate care to those individuals while they are on wait lists for OBOT or OTPs. MAT in emergency departments is thus provided using co-located providers and care coordinators, and clients are linked to telehealth or in-person counseling services, OBOTs, OTPs or detoxification centers to promote a continuum of care. MAT patients would be able to seamlessly flow from induction in an emergency department to interim care by a primary care physician and then to an OBOT or OTP. Targeted case managers contracted by the hospitals and funded by the behavioral health redesign would oversee this transition. Similarly, Ohio is also encouraging FQHCs to participate in ambulatory detoxification and to connect clients to SUD treatment through a partnership with the Ohio Departments of Medicaid and Mental Health and Addiction Services.65 Expanding MAT induction into emergency departments will help individuals who need ambulatory care to stay connected to a continuum of care after discharge.
| EXHIBIT 3. Ohio's Proposed Emergency Department Implementation Models |
|---|
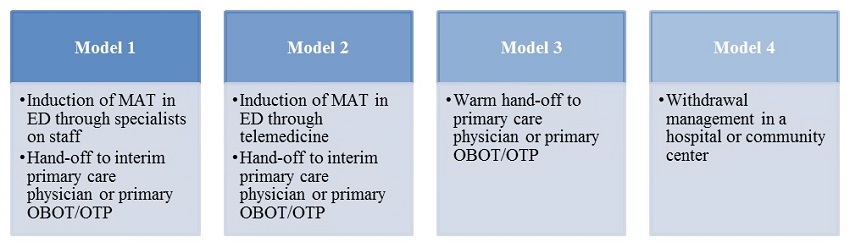 |
| ALT Text: Exhibit 3 is a row of 4 boxes representing Ohio's proposed ED implementation models. The first box represents Model 1, which involves induction of MAT in ED through specialists on staff and handoff to interim primary care physician or primary OBOT/OTP. The second box represents Model 2, which involves induction of MAT in ED through telemedicine and handoff to interim primary care physician or primary OBOT/OTP. The third box represents Model 3, which involves warm handoff to primary care physician or primary OBOT/OTP. The fourth box represents Model 4, which involves withdrawal management in a hospital or community center. |
3.4.3. Easing Regulations for OTPs and Implementing Medication Units
On January 4, 2017, Ohio passed legislation (Senate Bill 319, Common Sense Regulation for Methadone Clinics) that allows for-profit methadone clinics to open and waives the statutory requirement that community SUD services providers must be certified by OMHAS for at least 2 years prior to becoming licensed to maintain methadone treatment at an OTP.66 Allowing for-profit methadone clinics to operate will increase the availability of treatment options. As of January 2017, there were 26 OTPs in Ohio, and the number is expected to grow as a result of removing the requirements.67 Beginning in 2017, Ohio's Department of Health began also allowing OTPs to bill Medicaid for buprenorphine administration.65 These reforms will increase access for privately insured individuals as well as those covered by Medicaid.
Updated regulations for OTPs were also effective on June 1, 2017. OTPs requested a code to bill for direct observation of oral administration of MAT, and the state agreed to work through policy and operational guidance for this moving forward.68 Ohio will now allow OTPS to establish MUs in rural areas, similar to the Hub and Spoke model. Clients may have to go to an OTP once a month for counseling, but can go to MUs for dosing, allowing increased access to MAT. The new rules also require patients receive a minimum 50 minutes of counseling per week during the first 90 days of treatment.
3.4.4. Targeted Recruitment
Recognizing a shortage of waivered physicians prescribing medication--over 10 percent of counties have no MAT prescribers at all--the state used DEA registration numbers to match physicians who prescribed buprenorphine product in the last 12 months and identify shortage areas. They used this data as well as data on which areas of the counties have the highest overdose deaths to identify various "tiers." These tiers then determined areas for targeted outreach leveraging the Cures Act grant funding based on level of need for OUD treatment. OMHAS will use Cures Act funding to facilitate a series of workforce development strategies aimed at recruitment and expansion of MAT prescribers, mentoring new prescribers through Extension for Community Healthcare Outcomes (ECHO), and maintaining their level of MAT competence over time.60 Training for PAs and NPs is offered for free via PCSS-MAT--a national training and mentoring project on opioid misuse and the availability of pharmacotherapies to address OUD. As such, Cures Act funding is specifically targeting specialty physicians, such as primary care physicians, obstetrics and gynecology physicians, and emergency department physicians. Another strategy will be to provide free online trainings for Ohio physicians, PAs and advanced practice nurses to obtain their DATA 2000 waiver and to learn more about ASAM multi-dimensional assessment and levels of care. Enhanced, in-person ASAM trainings will include eight additional hours targeting stigma and knowledge gaps around SUD (e.g., withdrawal management) and providers will be eligible for a $1,300 incentive to compensate for their lost productivity during these 8 hours.
3.4.5. Expansion of MAT in Private Health Systems
Discussions with private stakeholders indicated Medicaid expansion has been critical in their ability to expand MAT in more rural areas and across multiple settings. Because more services were covered, they could afford to take on more patients. Still, much of their expansion efforts rely on internal funding and grants through agencies such as AmeriCorps or United Way. The system also held fundraisers, raising hundreds of thousands of dollars, to finance OUD-related services.
One stakeholder was piloting emergency room, primary care, and pain management MAT programs as a model for the larger system. It takes several years to build these programs and only recently are they getting money to pilot and implement MAT. Although they are a large health system, many hospitals are run independently. Corporate buy-in is needed but there is a lot of legwork to bring in different parts of the system. One challenge they face is that reimbursement for doctors providing MAT services is not high enough, which makes the recruitment case hard. Once the hospital is on board, it is easier to recruit physician practices where they have more leverage. Having physician champions is effective for recruitment at the both the system and facility level.
In another approach, a large health system is spreading out inpatient detoxification to other hospitals and increasing their own wrap around services with the condition that patients agree to go to MAT and intensive outpatient programs. Currently, they are using community partnerships for these services but their goal is to build internal capacity. They are not set up for county contracts or able to tap into local levies. They do not see community partnerships as sustainable and rather a barrier to expansion across their system, given the number of partnerships they need to establish and maintain. Their long-term strategy is to vertically integrate recovery support and wrap around services. They have started by funding patient navigators, a role that many partnerships currently fill. This increases the effectiveness of the warm hand-off to other parts of the system.
In pain management clinics, the stakeholders rely heavily on free Vivitrol. Although they can offer buprenorphine, their clients want Vivitrol due to the ease of administration. Although Medicaid and private insurance cover Vivitrol, it is expensive and not sustainable. To meet current demands, they work directly with pharmaceutical companies to get free or reduced prices. It is effective in the short term, while they figure out the kinks and build capacity. For other settings, providers are resistant to buprenorphine due to diversion concerns.
3.4.6. SBIRT
Ohio is leveraging a 5-year cooperative agreement from SAMHSA SBIRT program as a powerful physician engagement and recruitment tool. Currently, Ohio is enhancing its existing SBIRT services to focus on counties with the highest level of need for OUD treatment. One private stakeholder noted that physicians in their network are generally not supportive of MAT, either because of knowledge gaps in SUD care or because they are overwhelmed with patient loads and feel they cannot take on a new population. SBIRT is being used to "connect the dots" for physicians by documenting OUD among their existing patient base to overcome resistance to MAT. While SBIRT staff are currently engaging emergency departments to implement SBIRT, they will also work to onboard hospitals and health centers to undertake both SBIRT and MAT coordinated care services.60 Pairing SBIRT along with additional training is increasing physician awareness of the need for expanding MAT implementation.
3.5. Virginia
MAT in Virginia is primarily delivered through 40 Community Service Boards (CSBs) that are funded predominately by public services, and private, cash-based clinics. In some areas, the CSBs are a part of the local government and in other areas the CSB serves across multiple counties and is a quasi-government agency. The state does not provide services, but funds contracts to the CSBs. The CSBs function as the single point of entry into the publicly-funded behavioral health system and operate under a performance contract with the Virginia Department of Behavioral Health and Developmental Services (DBHDS) to implement MAT. These boards can also obtain funding from the local governments in which they reside, but these dollars can vary widely depending on their local jurisdiction. CSBs are the largest MAT providers, either providing it directly or contracting with providers. In addition to accepting Medicaid, state funding and block grants, CSBs accept private insurance and charge fees on a sliding scale. Even though some CBSs only charge $15/day for some services, stakeholders report that the sliding fee model is a significant deterrent if you do not have a stable income.
There are 35 OTPs in Virginia and all but four of them are private. Only one program is a non-profit and most programs operate on a cash-only basis. Only about 6 percent of OTP patients receive buprenorphine. Stakeholders reported 500 waivered physicians practice in the state, but only 400 are on the public list. Diversion is a large concern in the state. Stakeholders indicated there is so much buprenorphine on the street that some people feel they can manage their SUD without engaging treatment providers. Many of the cash programs dispense the mono-product (i.e., buprenorphine without naloxone, or Subutex), which causes concern due to its higher potential for misuse. Buprenorphine with naloxone cannot be melted down and injected, as the naloxone would render the buprenorphine inactive; however, the mono-product is much less expensive. Diversion is a significant obstacle in recruiting physicians; stakeholders reported that physicians do not want to be part of the problem as they see MAT as dangerous to their practice.
Given the rurality of Virginia, it is difficult to provide outpatient SUD treatment. In many areas, it is a 2-hour to 3-hour drive to the nearest OTP. Because OTPs require daily visits by methadone patients, rural residents who are frequently required to drive extended distances every day to receive their needed medication often shoulder these transportation costs and other time burdens. Finally, there are shortages of medical and behavioral health providers, especially in rural areas.
Virginia has not expanded Medicaid to-date. There is restricted eligibility for Medicaid: pregnant women and children up to age 18 cannot have income higher than 133 percent of federal poverty level (FPL), elderly and disabled people cannot have income higher than 80 percent of FPL, and working parents cannot have income higher than 30 percent of FPL.69 This leaves many MAT-needing patients only covered under block grants and state revenues that have been stagnant since 2002.
3.5.1. 1115 Waiver
Until a recent 1115 SUD Medicaid waiver, the Medicaid program did not generally cover MAT services and had a limited SUD benefits package restricted to individuals under 21 years old. Broadly, the waiver implements a comprehensive continuum of SUD treatment services and significantly increases the reimbursement rates for existing services (referred to as the Addiction Recovery Treatment Service [ARTS] benefit). It also covers all three major MAT medications and includes peer support and case management as billable services. Expanded benefits to all Medicaid enrollees include the following services: inpatient detoxification and inpatient SUD treatment for up to 15 days (previously only available to children); residential detoxification and residential SUD treatment; and peer supports for individuals with SUDs or mental health conditions to provide intensive short-term and long-term recovery coaching. Prior to the 1115 waiver, there were four residential treatment centers accepting Medicaid and now there are 71 facilities. Likewise, there are now 28 Medicaid providers that provide combined MAT and counseling services, up from zero.
For OBOTs previously enrolled in Medicaid managed care, the waiver represents a carve-in of MAT benefits, making it easier to start billing Medicaid. For SUD providers who have not billed Medicaid previously, this is a significant change as it greatly expands access for Medicaid enrollees.
Once enrolled, the waiver also expedites access to different SUD services through modifications to the licensing process. Providers licensed for high levels of ASAM care can provide certain lower level services without a specific license or can be fast-tracked for additional licenses. Peer services were billable effective July 1, 2017, and had a low credentialing burden to enhance recruitment. The peer services credential does not require a college degree and only requires 48 hours of didactic training and 500 hours of supervised work.
The ARTS benefit also incentivizes providers to integrate buprenorphine in physician's offices with what is called the "Gold Card Model." There are currently 27 Gold Card providers comprised of CSBs and private clinics. This "Gold Card Model" increases reimbursement rates for different services up to 400 percent if counseling and psychosocial supports are delivered by primary care clinics with co-located MAT prescribers. A licensed behavioral health provider is required to be on-site at least three times a week, and services are bundled into a package rate. Likewise, OTPs can co-locate a medical provider. The bundle includes a care management component intended to create linkage to other physical care providers (e.g., primary care doctor or obstetrician, orthopedist, or dentist) to facilitate open communication between the waived prescriber and other providers so they understand that patient has SUD and is being treated accordingly. Gold-Card status has removed prior authorization requirements for buprenorphine and allows billing for care coordination services. In addition, payment for SUD case management was increased by 50 percent and payment for SUD partial hospitalization, intensive outpatient services, and the counseling component of MAT was quadrupled.20 This benefit was carved into standard managed care contracts to promote integration with medical and mental health care for both patients and clinicians. Providers not enrolled in the Gold Card Model may still bill Medicaid MCOs as before. The state felt multiple tracks would allow flexibility to maintain capacity, as many providers may not be able to co-locate services.
Stakeholders had mixed opinions on the Gold Card plan. Some felt that it was a great way to engage community providers in SUD treatment and the payment model would be attractive to providers. Other stakeholders thought the benefit would not expand OBOT, given that most providers were not set-up or ready for co-location.
Two challenges have arisen with implementation of the waiver. First, there is a steep learning curve in learning how to bill Medicaid, given the number of cash-based OTPs and other clinics. The state is working to help facilities understand how to obtain authorization and bill. One helpful policy has been the implementation of a uniform authorization request that spans across all Medicaid MCOs.
Second, Medicaid regulations are very prescriptive as to which services can be billed for by a licensed professional versus a certified counselor. The waiver has illuminated many of these discrepancies, noting that certified counselors may have been billing for services that required a license. Stakeholders mentioned that the waiver has magnified a shortage of licensed professionals.
3.5.2. Cures Act Funding
Of the $9.7 million Virginia received from the Cures Act, $5 million is being directed to 18 CSBs to increase capacity. The funding provides 90 days of treatment free to the client. The goal is that after those 90 days, the patient will be stabilized and hopefully earning some income so they can help pay for their treatment on a sliding scale and open up a free slot for another patient. The grant can provide $10,000 worth of treatment per patient per year; most counties can only budget $3,000 per patient per year without the grant.
| BOX 3. Project ECHO |
|---|
| What is Project ECHO? Extension for Community Healthcare Outcomes, or "Project ECHO," is a model that uses teleconsultation to expand SUD treatment capacity in remote and underserved areas. Project ECHO allows primary care clinicians to treat patients with common, complex diseases in their own communities, reducing travel costs and wait times, and avoiding complications. Overall, this results in a higher percentage of patients being managed by the primary care clinician and reserves referrals to specialists for complex, high-risk patients. The ECHO model is a collaborative practice model where the primary care clinician retains responsibility for patient care, but sessions also allow for a team of "Hub" specialists in addiction disease management to consult on de-identified real patient cases via video conferencing to primary and other providers across Virginia. Sessions include a brief didactic session on predetermined lessons, and Continuing Medical Education is available for free to all participants. This model fosters knowledge-sharing and collaboration across providers and builds up the confidence and capacity of providers to provide MAT and treat SUD effectively. |
In addition, DBHDS is working with Virginia Department of Health to use these funds to support implementation of the ECHO model that uses teleconferencing to monitor individuals using MAT in parts of the state that do not have enough clinicians (see Box 3 for more detail70). Stakeholders noted that once the ECHO model is operational, it will provide continued medical education credits at no cost and prescribers will be able to participate in courses by smart phone, to increase interest and participation. Funds will also support pilot programs using certified peer specialists to assist in emergency departments when individuals are admitted for opioid overdose.
3.5.3. Addressing Diversion
To combat diversion, the Virginia Board of Medicine recently passed stringent standards that restricted the use of mono-product only to pregnant women and patients converting from methadone, and only in non-tablet formulations.71 OTPs and clinics pushed back fiercely on the new regulations because the mono-product is a large source of profit to the clinics. The Board gave prescribers an allowance of 3 percent of their population that is not pregnant and not on methadone to give prescribers some more flexibility. Additionally, prescribers are required to conduct urine drug screens or check serum medication levels at least every 3 months for the first year of treatment and at least every 6 months thereafter to help reduce the chances of diversion.
3.5.4. Private Performance Initiatives
One private health plan is implementing value-based contracts with large providers that use bundled services or performance incentives for MAT treatment. Contracts may include bonuses or withholdings based on treatment retention, adherence, and other utilization measures. Measures include the numbers of appointments kept by the member each month, the number of therapy appointments kept, number of individual appointments kept, medication adherence, use of emergency department services, and any follow-up or rehab stay during the period of the contract. They have set up a bundled flat rate that can be lowered if appropriate services in the bundle are not provided. An example is a comprehensive program that would include family therapy, individual therapy, drug testing, and the administration of the medication. Stakeholders noted that often the organization sees a patient not adhere with therapy, so the performance incentives encourage the provider to keep those members engaged over the long run.
3.5.5. Coordinated Outreach
Physicians that serve as both public and private champions are key to engaging other physicians in MAT. Several state health agencies and medical and provider associations are partnering to deliver comprehensive MAT training for physicians, counselors, nurses, social workers, care coordinators, case managers, and recovery coaches. The state is also partnering with the National Governor's Association to participate in a learning collaborative focused on developing and implementing trainings.
3.5.6. Tuition Reimbursement
One CSB that has a large shortage of licensed providers is offering tuition assistance of $1,500/semester, as well as initial license reimbursement and certification in addiction specialties to "grow [their] own licensed individuals."
4. FINANCING APPROACHES
The environmental scan and discussions with stakeholders identified five broad financing approaches to expand MAT capacity and Exhibit 4 describes the perceived benefits and disadvantages of each approach. States are using a variety of legal authorities to expand access to treatment as well as the number of individuals eligible for such care. These include expanding coverage of Medicaid OUD services under optional benefits, using 1115 demonstration waivers, and using federal grants.
Across the different approaches, policy actions had three broad themes. First, policies often worked to finance integrated physical and behavioral health delivery systems to provide more effective, whole person care. This involved incentivizing MAT within the SUD system, incentivizing linkages between the SUD system to MAT providers external to the SUD system, and integrating SUD treatment within primary care.
Second, financing policies often leveraged strengths of the existing infrastructure. Although MAT delivery systems are not wholly efficient or organized, stakeholders reported that subtle tweaks to these systems could provide effective and efficient progress (e.g., resolving coding issues). Small changes could lead to increases within the existing capacity of the system by making MAT provision easier. With large system transformations, stakeholders reported significant start-up and development costs (e.g., additional state technical and contract staff, data systems, or physical facilities). These changes are important in the long run to address the overall MAT delivery system. Still, stakeholders noted that policies that maintain flexibility, such as allowing old billing practices to continue in the short-term, or leveraging block and grant discretionary grant funding, are effective means of maintaining capacity as the delivery system changes broadly.
Third, financing policies are being used to promote evidence-based practices for OUD treatment, such as integrated pharmacotherapy and behavioral support, in both SUD and non-SUD settings.
Nearly every stakeholder suggested that insurance coverage of OUD treatment and MAT had historically been too limited. Although increasing funds seems like a straightforward solution (e.g., authorizing optional SUD benefits under Medicaid), public stakeholders felt little ability to operationalize this at the state level. A common theme was that inflation-adjusted state revenues and block grants have been constant or decreasing and that directing funds to a specific issue, such as the opioid epidemic, often meant diverting those funds away from other services. Both private and public stakeholders noted that OUD is one of many broader health challenges their states face and only recently have states rallied behind policy action. More so, OUD and broader SUD services have lagged behind physical and mental health in funding and infrastructure, especially in rural areas.
| EXHIBIT 4. Common Financing Approaches for MAT Expansion and Perceived Benefits | ||
|---|---|---|
| Financing Approaches in the Five States | Perceived State and Local Stakeholder Benefits | Perceived Disadvantages |
Expand Medicaid coverage of SUD using optional benefits
|
|
|
Expand Medicaid Eligibility
|
|
|
Medicaid 1115 Waiver
|
|
|
Federal Grant Funding
|
|
|
Public/Private Contracting
|
|
|
Regulations for Public/Private Insurance
|
|
|
Among the medications, most policy focused on expansion of buprenorphine use. Methadone must be delivered in the context of an OTP, and building and staffing new facilities was a noted challenge. Some local stakeholders indicated that Vivitrol was in high demand from patients due to the long-lasting dosage, a huge benefit in rural areas, and from certain providers since it cannot be diverted. Stakeholders also noted that Vivitrol was a high priority among criminal justice stakeholders for these same reasons. A noted concern with Vivitrol is the detoxification period needed before administration, and stakeholders across all states noted a lack of accessible detoxification services. Stakeholders also noted that Vivitrol is much more expensive to acquire. Thus, an overall theme was that buprenorphine is a cost-efficient option on a large scale, given existing infrastructure. Because buprenorphine is thought to be most effective in combination with counseling and other supportive and recovery services, many financing interventions are targeted at increasing capacity for these related treatment and support services as well.
4.1. Expand Medicaid Eligibility
Medicaid recently became an important source of MAT coverage, providing states with an opportunity to leverage their large patient pools in different contracting arrangements and to incentivize network structures and service provision. Most states cover some form of MAT through their Medicaid drug formulary. Methadone maintenance is covered by Medicaid in 34 states (with two others in process); buprenorphine is covered by Medicaid in 45 states; and naltrexone is covered by Medicaid in 43 states.72 The five states studied here covered each medication.
In the three states in this report that expanded Medicaid, stakeholders cited the expansion as a game-changer for MAT coverage in their state, while the two non-expanding states suggested expansion would be a boon for their state. Since states do not recognize OUD as a disability, many low-income adults with OUD, especially males, were not previously eligible. It was expected that many low-income adults would gain eligibility, have an existing SUD, and increase the demand for SUD services.73 A recent study suggested that Medicaid-covered buprenorphine prescriptions increased by 70 percent and overall spending on buprenorphine increased by 50 percent after the initial 28 states expanded Medicaid in 2014.74
Stakeholders cited the stability of Medicaid funding as an anchor for expanding MAT. First, stakeholders indicated that they observed an increase in demand from newly-covered individuals and that providers were anecdotally more willing or able to accept Medicaid beneficiaries. In some instances, a patient may have been under charity care and was now Medicaid eligible. Stakeholders in the expanding states indicated that Medicaid reimbursement for MAT was still too low, but that the overall increase in reimbursement from federal funds has been helpful in increasing MAT provision.
Second, stakeholders reported they could expand the range of OUD services available. Medicaid expansion increased the federal match of Medicaid financing, 100 percent in 2014 and reduced to 90 percent by 2020, for newly eligible individuals, and provided states leeway to expand coverage for behavioral services for the newly eligible. These provisions were also enacted simultaneously with the final implementation of the Mental Health Parity and Addiction Equity Act (MHPAEA) rules that removed barriers to benefits that were already part of the insurance product.75 The three expanding states had historically limited SUD benefits packages and stakeholders indicated that their states took advantage of expansion to increase the overall SUD benefit package.
Third, since many of the newly eligible individuals had previously received services financed through block grants and state revenues, and because federal funds were used to cover their Medicaid services, stakeholders stated that expansion allowed them to re-allocate block grants toward services not covered by Medicaid and to re-direct state revenues from service provision to infrastructure and workforce development. Thus, Medicaid indirectly increased MAT capacity by freeing state resources.
Moving forward, ACA Medicaid expansion may not be a viable policy option for states that chose not to expand. Likewise, expanding states note that the gains they have made are not sustainable in the absence of federal funding for the newly eligible. Expanding states also noted that expansion has highlighted workforce and infrastructure concerns for expanding MAT. Although stakeholders indicated the benefits of expansions outweigh the costs of increased pressure on the system, expansion did not address their historically fragmented SUD systems.
4.2. Medicaid 1115 SUD Waiver
Starting in 2015, CMS offered states the opportunity to pursue Medicaid demonstration projects authorized under Section 1115 to test Medicaid coverage of a full SUD treatment service array in the context of overall SUD service delivery transformation, provided participating states meet specific requirements.39 These specific requirements included the following: comprehensive evidence-based design, appropriate standards of care, strong network development, care coordination, integration of physical and SUD treatment, program integrity safeguards, benefit management, community integration, strategies to address prescription drug misuse and OUD, services to youth and adolescents with SUD, reporting of quality metrics, and collaboration with the SSA for substance abuse. Three states in our sample (California, New Hampshire, and Virginia) are implementing 1115 waivers that mandate coverage of MAT and expand recovery and support services; these states are also attempting to better coordinate medical and behavioral health services. Again, all three states cited historical deficiencies in Medicaid SUD benefits and a lack of treatment that were targeted with the waiver. Common to the waivers is the requirement to use the ASAM criteria for assessment and treatment planning. Other states not in our sample are also implementing waivers (e.g., Maryland).
California is using the waiver as an impetus to better coordinate care at the county level, and New Hampshire is using it to improve coordination at the regional level. For California, the waiver mandates buprenorphine provision in their NTPs to increase its traditionally low use, and raises reimbursement for costs associated with induction and management for NTPs and non-NTPs. Although OBOTs could bill traditional Medicaid, counties can use the waiver to contract with OBOTs to better link support and other SUD services with the broader county SUD system. With this, stakeholders report a trend towards vertical integration of providers to the county or with large provider networks. New Hampshire does not have the same county level-system, and the waiver instead leverages hospitals and their large primary care networks. As opposed to funding services, initial waiver funding is directed to capacity building and planning of the networks. Both California and New Hampshire promoted alternative payment methods under the waiver, but stakeholders from both states indicated that progress has not been made in developing these models.
Whereas California and New Hampshire are using the waiver to build upon Medicaid expansion, Virginia is using the waiver to expand MAT provision in the absence of expansion to childless, low-income adults. The waiver increases the types of SUD services available to the existing Medicaid population, increases reimbursement rates broadly, and requires MCOs to retain care coordinators. Specifically, the ARTS benefit increased reimbursement for the counseling component of MAT by 400 percent. By carving in SUD benefits, the waiver puts some pressure on cash-based providers and is beneficial to OBOTs that are already enrolled for non-SUD services.
The waivers are demonstration projects and are proposed to be cost-neutral. Because the waivers involve system transformation, stakeholders report start-up costs and lags in development. Start-up costs involve significant engagement and training efforts with providers using state resources. California and Virginia invested state resources separate from the waiver to support these initial costs. Stakeholders in California noted that several counties served as test cases and are serving as consultants for other counties who are starting to implement the waiver. Counties have not really had a chance to assess implementation of alternative payment models yet.
4.3. Federal Grant Funding
Federal funds have been integral in the expansion of MAT provision across the country. Stakeholders cited various federal grants as helpful in expanding MAT capacity, whether through infrastructure investments and pilot programs, hiring champions and implementation teams, or financing services not covered by other programs. Grants can be targeted to local organizations in specific regions or counties with high need to address a variety of local needs. Moreover, these grants can bridge different state agencies, such as departments of health and criminal justice agencies, to promote a more coordinated and collaborative model for treatment services. Although states still have the authority to use the funds however they see fit, the block grants and other opioid-related funding mechanisms may come through the states' SSA, making it harder to route these funds to general medical providers and FQHCs.
Whereas Medicaid funding can "follow the person" across sites of care and services, and 1115 waivers can affect the broader Medicaid delivery system, grant funds, on the other hand, are often focused specifically on programs or services that Medicaid cannot cover. Federal grants can be instrumental in building capacity in settings such as emergency departments and FQHCs, however they are usually not sustainable and limited in scope. Some stakeholders also noted that grants may not allow adequate time for disbursement of funds for direct services or adequate planning time for infrastructure investments.
4.4. Public/Private Contracting
The use of contracts by states and private agencies is another mechanism that can affect MAT capacity, allowing the funder (i.e., SSAs, Medicaid, or county boards) to dictate types of services covered and how or where the services can be provided. Specifically, states and organizations can require through contract the provision of MAT (e.g., Missouri), co-location of providers (e.g., Virginia), as well as any performance or outcome measurement data collected (e.g., Virginia). For example, Missouri's DMH requires that to be contracted with the state, an agency must ensure the availability of all forms of MAT for OUD. The ARTs benefit in Virginia provides increased reimbursement when a behavioral health provider is located and private insurers in Virginia tied payments to service delivery and patient retention using value-based contracts.
Contracting arrangements can allow more flexibility at the local level and introduce challenges. In California, Ohio, and Virginia, the state initiates contracts with county agencies that directly provide services or further subcontract out to providers. County boards directly contract with treatment providers to provide MAT treatment services in both Ohio and Virginia. In California, counties can directly contract with SUD treatment providers in NTPs under the DMC-ODS waiver. This leads to both positives and negatives. Local resources are used to organize public providers or initiate contracts with providers, freeing state agency resources from certain administrative costs. Counties and local authorities may also be more effective at understanding and addressing treatment needs of the local population. However, these types of performance contracts create variation in MAT utilization across the state due to differences in local preferences and capacity. Counties and local authorities may also have access to differing local resources, (e.g., county levies) that create treatment gaps for poorer areas.
Neither Missouri nor New Hampshire have county organizations, and contracts are left to the state or private agencies to manage and implement. Thus, more state resources are needed to initiate contracts with new providers and more start-up costs are incurred to organize the system. For example, using state revenues New Hampshire contracted with the Foundation for Healthy Communities to work with hospital-based primary care clinics to establish MAT services. Another possibility for expansion is informal local networks. In Missouri, a local behavioral health network set up a system of subcontracts with independent providers to prescribe MAT. The providers bill the network for MAT services, and the network, in turn, bills the state. This type of network developed organically through collaborations between state agencies and local champions and may not be widely applicable.
One other state contracting option is volume-based contracts. States can leverage their buying power for cost advantages in pharmaceuticals and laboratory costs, initiating high volume contracts directly with an organization as demonstrated in Missouri for Vivitrol and urine analysis. These contracting mechanisms allow for increased reimbursement rates and expansion of evidence-based services.
4.5. Regulations for Public/Private Insurance
In 2008, the MHPAEA required group health plans and health insurance issuers to provide equivalence in the way that mental health or SUD benefits are treated with respect to annual and lifetime dollar limits, financial requirements, and treatment limitations. In 2010, the ACA amended this law to also apply to individual health insurance coverage, and the final rule in 2016 addressed the application of these parity requirements to Medicaid MCOs, Medicaid benchmark and benchmark-equivalent plans, and Children's Health Insurance Program (CHIP).76
Still, although stakeholders indicated that private insurers will pay for MAT, they continued to cite prior authorization procedures as rigorous and co-payments and co-insurance as high. Although the ACA requires many insurers to cover SUD treatment benefits, many policies impose onerous prior authorization requirements, place arbitrary limits on medication dosage and length of treatment, or require patients to "fail first" at other treatments for one or even all medications. Through Insurance Commissioners and legislature, states can reduce barriers to prescriptions under private insurance, such as prior authorization requirements and treatment limits. Stakeholders also mentioned that many networks and insurance companies are piloting pay-for-performance and bundled contracts with incentives around MAT provision.
As of March 2017, Aetna, Anthem, and Cigna stopped requiring doctors to seek approval from the insurance company before prescribing Suboxone (buprenorphine/naloxone) as a way to ensure coverage parity for patients needing treatment for SUD. States have also begun to ease regulations in commercial insurance, such as only requiring a diagnosis of OUD in the past 2 years to start MAT, allowing the prescribing physician to conduct MAT screening instead of a separate behavioral health provider, or prohibiting prior authorizations more frequently than once a year for certain medications. Decreasing administrative barriers and eligibility requirements for MAT then eases the recruitment of independent providers into local networks or partnerships and reduces time to MAT induction.
5. WORKFORCE DEVELOPMENT APPROACHES
Stakeholders in each state cited significant workforce shortages among medical and behavioral health providers needed to provide MAT, especially in rural areas. Exhibit 5 describes five workforce barriers specific to MAT that were common across the five states, as well as the approaches the states are taking to increase the MAT workforce.
| EXHIBIT 5. Common Workforce Issues and Potential Solutions | |||
|---|---|---|---|
| Not enough waivered physicians | |||
| |||
| Provider access in rural areas | |||
| |||
| Lack of support for small, non-specialist physicians | |||
| |||
| Lack of infrastructure to support treatment | |||
| |||
| Stigma | |||
| |||
5.1. Workforce Barrier #1: There are Not Enough Waivered Physicians
Although no definitive data exist to accurately reflect the supply of professionals available to treat individuals with SUDs, some estimates exist in the literature, and a shortage is clear according to stakeholders. As of March 2017, only 37,526 physicians across the country--approximately 4 percent of all physicians in the United States--had obtained a DATA 2000 waiver to prescribe buprenorphine.19, 77, 78 The average state had 9.2 waivered physicians per 100,000 residents, compared with 206.5 non-waivered physicians per 100,000 residents, with significant variation in the number of waived physicians per capita across the states.79 Most counties in the country have no physicians with these waivers, leaving more than 30 million people without access to office-based treatment for OUD.
Although a variety of professionals--including SUD and mental health counselors, psychiatrists, addiction medicine physicians, other physicians, psychologists, social workers, NPs, case managers, peer support specialists, and recovery coaches--can provide SUD treatment services, only those with the required training and waiver can prescribe buprenorphine. Stakeholders indicated problems recruiting these professionals, often citing at least one unfilled full-time equivalent position. These difficulties can be attributed largely to insufficient numbers of applicants who meet minimum qualifications, a small applicant pool in certain geographic areas, and a lack of interest due to salary and limited funding. Specifically, a lack of support for existing and potential prescribers of MAT can deter physician participation, including insufficient ancillary services for referral or access to expert consultation.20
Many stakeholders cited the waiver process as a large barrier to getting medical providers prescribing buprenorphine. Stakeholders and providers argued that no waiver is needed to prescribe general opioids for pain, so requiring one to prescribe buprenorphine is not realistic or logical. Several stakeholders suggested repealing the waiver process entirely; other stakeholders were more concerned about diversion and suggested that regulatory balance is necessary. One stakeholder indicated that physicians were prescribing to their limits and that the patient caps were preventing growth in MAT provision. Stakeholders agreed that the patient limits should be increased.
Stakeholders cited incentive programs and outreach efforts by other MAT-prescribing providers as effective in getting providers to take the waiver training. Missouri and Ohio were providing a direct monetary incentive using grant funding. These trainings also included additional SUD treatment and ASAM content, with the hope of increasing effective prescribing behavior once waived. Several states are implementing mentoring and community-building programs to support MAT provision among independent physicians. These initiatives are especially important for rural physicians that lack local support.
Missouri and California are using academic detailing for targeted recruitment, whereas Ohio used internal data assessment to identify critical shortage areas. Multiple stakeholders suggested medical champions and doctor-to-doctor outreach as effective means of engaging physicians. All states were leveraging their medical and hospital associations for awareness and networking campaigns.
Several stakeholders also cited recent legislation to allow NPs and PAs to prescribe MAT as a boon, given provider supply, provider interest, and cost reasons. Stakeholders see NPs and PAs as the largest sources of untapped potential supply, and efforts to increase their scope of practice and reduce prescribing limits could greatly increase access to MAT. Local stakeholders indicated their NPs and PAs were very interested in MAT.
Measurement of the success of waiver recruitment and training programs is still in the early stages. As a part STR grants, one state listed numerical goals for recruitment and training targets. Two other states listed generic goals to increase MAT instead of specific targets. Stakeholders from these states indicated they did not have a strong sense yet of what would constitute success and that it was too early to tell how much of an impact the programs were having.
5.2. Workforce Barrier #2: Provider Access in Rural Areas is Poor
As noted in the previous section, the supply of waived physicians in rural areas is a large barrier to MAT expansion. California, Missouri, and Ohio are actively implementing Project ECHO and working to build online learning and support communities to bolster support of waived physicians in rural areas. Further, one Ohio provider was using telehealth services as a back-up to ensure continuation of care in case the provider was not available. Stakeholders in New Hampshire and Virginia were still evaluating telehealth as an option and noted poor Internet access as a significant barrier to telehealth initiatives in the most remote areas.
Both Virginia and New Hampshire stakeholders noted the need to increase funding for HRSA and state-specific loan repayment programs to address the broader physician shortage in rural areas. New Hampshire is implementing a broader workforce development program for primary care physicians focused reducing physician turnover. Stakeholders noted that these broader challenges need to be addressed concurrently with the opioid epidemic.
Another challenge stakeholders reported is that recruiting is a zero-sum game. For example, in New Hampshire, an urban clinic may have a single waived provider (or behavioral health provider), and recruiting that provider to a rural clinic reduces MAT provision in the urban area.
Across all five states, stakeholders cited NPs/PAs as the best option for expanding MAT in rural areas.
5.3. Workforce Barrier #3: There is a Lack of Support for Small, Non-specialist Physicians
Across many discussions, stakeholders noted that MAT provision is just one component of an individual's care, and that SUD patients require a wide range of medical and behavioral health care. Since MAT is often best implemented in combination with counseling and other SUD treatment and recovery support services, stakeholders reported that many physicians are resistant to prescribing MAT because they cannot provide these other services or know to whom to refer their patient. This is a different kind of support than managing medications of a patient.
Another common approach in the five states is the use of peer support workers. In addition to their critical role in patient recovery efforts, stakeholders note that peer support workers can often help patients understand how the treatment system work and may act as advocates on their behalf. Virginia, New Hampshire, and California all recently added peer support workers as billable service under Medicaid and the certification requirements were intended to be minimally burdensome. For example, California allows a 5-year grace period before formal certification is needed and Virginia does not require a college degree for certification.
In Missouri, one stakeholder noted that they cannot find enough peer support workers. Once patients leave treatment, they struggle to maintain contact to provide continued care.
5.4. Workforce Barrier #4: There is a Lack of Infrastructure to Support Treatment
One concern related to supporting waived physicians is a weak behavioral health workforce to support treatment. Behavioral health organizations often have trouble hiring medical providers that can prescribe MAT. In addition to difficulties associated with connecting doctors to the SUD treatment system, there are also difficulties associated with connecting the SUD treatment system to medical providers who can prescribe.
Again, stakeholders cite fully integrated models, such as FQHCs, as a potential area to better link these services. Stakeholders from New Hampshire noted that FQHCs pay higher wages than traditional SUD settings and can use that as a recruiting tool. These stakeholders caution that this is a tricky strategy, though, because simply moving providers from an SUD setting to an FQHC is a zero-sum game. Rather, they are focusing on increasing credentialing and licensure for existing uncredentialled staff to transition into roles in FQHCs.
Stakeholders noted that building formal or informal Hub and Spoke systems is an effective way to build MAT capacity. California was using Cures funding to implement a formal Hub and Spoke system, and Missouri stakeholders reported an organic, informal network arising through behavioral health organizations. Promoting MAT in FQHCs is another strategy, since FQHCs often provide comprehensive services, including behavioral health, and have some capacity to provide MAT-related services. As another option, California and Ohio are using MUs to overcome the lack of NTPs and OTPs in rural areas. Patients still receive SUD services at the NTP or OTP, but do not have to travel often to get medications.
5.5. Workforce Barrier #5: Stigma and Knowledge Gaps Exist
Stakeholders also cited stigma as a large barrier in both medical and behavioral health care. Although providers recognize the dangers of the opioid epidemic, stakeholders suggested that many of their providers do not recognize OUD in their patient population, have significant misunderstanding about treating SUD, and may believe MAT is a replacement addiction treatment rather than a treatment.
In medical settings, several stakeholders cited SBIRT as a key physician recruiting tool. By identifying existing patients with OUD, SBIRT helps to break down resistance against providing MAT to a "totally new population of patients."
Several states are offering enhanced training with ASAM content to broad provider groups to combat knowledge gaps regarding SUD treatment and MAT, specifically. These enhanced trainings go beyond the required waiver content. Stakeholders noted that most medical residency programs require 6 or less hours on SUD treatment and that these trainings may meet or exceed the previous amount of training received. Also, in Missouri, Cures-funded implementation teams work in primary care and emergency departments to address knowledge gaps. One stakeholder noted that most emergency departments can already bill for and have staff licensed to provide medical detoxification and MAT induction, but staff are afraid to or do not know how to manage the process. While enhanced training is one side of the equation, the implementation teams provide on-the-ground capacity building.
Many stakeholders cited fierce resistance to MAT by behavioral health providers and noted that outreach and education are also just as needed in the recovery community. In addition to outreach campaigns for the medical communities, provider associations in California and New Hampshire are attempting to make in-roads among the SUD treatment community. Stakeholders in New Hampshire and Virginia discussed initiatives aimed at modifying or improving curriculum in academic programs to better recruit and develop a new wave of behavioral workers who are less entrenched in abstinence-based methods.
6. LOCAL POLICY INTERVENTIONS
The previous two sections separately highlight common themes among financing and workforce policy to build MAT capacity. The examined states often leveraged their existing strengths to improve MAT capacity and noted a confounding paradox they tried to address: the interrelatedness of workforce and financing issues. Stakeholders noted that they struggle to pick a starting point for policy action. For example:
-
Is it better to invest in physical capacity for OTPs or in higher reimbursement levels for MAT?
-
If there is not enough OTP capacity, will providers feel supported? Are reimbursement rates high enough to get providers interested without more support?
There is not one solution to this complex issue and it is important to recognize that MAT capacity varies at the local level, depending on the concentration of available setting and provider types. Exhibit 6 provides a menu of potential ways in which these policies can be combined at the local level to develop MAT capacity. For each of five settings, we describe key financing and workforce barriers and potential interventions to expand access to MAT and related services. These options include short-term solutions that unlock or use existing capacity more efficiently and longer-term solutions that may expand overall capacity.
| EXHIBIT 6. Building Local MAT Capacity | |||||
|---|---|---|---|---|---|
| Setting | Strength/Advantage | Key Financing Barrier(s) | Key Financing Intervention(s) | Key Workforce Barrier(s) | Key Workforce Intervention(s) |
| Office-Based Physicians |
|
|
|
|
|
| FQHCs |
|
|
|
|
|
| Hospitals/ Emergency Departments |
|
|
|
|
|
| OTPs |
|
|
|
|
|
| Outpatient BH Organization |
|
|
|
|
|
7. CONCLUSION
This report summarizes policy and programmatic options to expand treatment capacity for OUD, focusing especially on MAT, a combination of medication, counseling, and behavioral therapy that has shown to be effective in treating alcohol and opioid dependency. We used a case-study approach and conducted an environmental scan and stakeholder interviews for five states: California, Missouri, New Hampshire, Ohio, and Virginia. We highlighted key levers each state is using to expand or improve access to MAT, summarized common themes among financing and workforce policies, and mapped the policy levers to different settings in which a patient could star MAT, describing ways to build local capacity.
This list of financing and workforce policy levers is not exhaustive, and though they are intended to be broadly applicable, the results are limited to the context of the five studied states. State and local policy makers should careful consider the existing strengths and needs of their system. Beyond the specific policy levers mentioned here, state and local stakeholders must recognize broader fragmentation in the behavioral health delivery system and resistance against OUD and SUD in general within the medical community. Most policy levers mentioned here include MAT, but extend beyond the scope of MAT. Individuals with OUD often have complex medical and behavioral needs, and policy changes should consider the broader spectrum of services these individuals require.
ENDNOTES
-
Centers for Disease Control and Prevention. (2011). Vital signs: Overdoses of prescription opioid pain relievers--United States, 1999-2008. Morbidity and Mortality Weekly Report, 60(43), 1487-1492.
-
Centers for Disease Control and Prevention. (2017). Opioid Data Analysis: Categories of Opioids. Retrieved from https://www.cdc.gov/drugoverdose/data/analysis.html.
-
Jones, C.M., Campopiano, M., Baldwin, G., & McCance-Katz, E. (2015). National and state treatment need and capacity for opioid agonist medication-assisted treatment. American Journal of Public Health, 105(8), e55-e63. Retrieved from DOI: 10.2105/AJPH.2015.302664.
-
Substance Use and Mental Health Services Administration. (2016). Treatments for Substance Use Disorders. Retrieved from https://www.samhsa.gov/treatment/substance-use-disorders.
-
Legal Action Center. (2015). The Case for Eliminating Barriers to Medication-Assisted Treatment of Heroin and Opioid Addiction.
-
Kampman, K., & Jarvis, M. (2015). American Society of Addiction Medicine (ASAM) national practice guideline for the use of medications in the treatment of addiction involving opioid use. Journal of Addiction Medicine, 9, 1-10. Retrieved from https://www.asam.org/docs/default-source/practice-support/guidelines-and-consensus-docs/asam-national-practice-guideline-jam-article.pdf?sfvrsn=0.
-
Tai, B., Saxon, A.J., & Ling, W. (2013). Medication-assisted therapy for opioid addiction. Journal of Food and Drug Analysis, 21(4), S13-S15. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4175918/.
-
National Institute on Drug Abuse. (2016). Effective Treatments for Opioid Addiction. Retrieved from https://www.drugabuse.gov/publications/effective-treatments-opioid-addiction/effective-treatments-opioid-addiction.
-
Volkow, N.D., Frieden, T.R., Hyde, P.S., & Cha, S.S. (2014). Medication-assisted therapies--tackling the opioid-overdose epidemic. New England Journal of Medicine, 370(22), 2063-2066.
-
Sigmon, S.C. (2015). The untapped potential of office-based buprenorphine treatment. JAMA Psychiatry, 72(4), 395-396.
-
Park-Lee, E., Lipari, R., Hedden, S., Kroutil, L., & Porter, J. (2017). Receipt of services for substance use and mental health issues among adults: Results from the 2016 National Survey on Drug Use and Health. NSDUH Data Review.
-
National Center for Health Statistics. National Vital Statistics System.
-
Substance Use and Mental Health Services Administration.Key Substance Use and Mental Health Indicators in the United States: Results from the 2015 National Survey on Drug Use and Health (NSDUH).
-
National Institute on Drug Abuse. (2017). Expanding Medication Assisted Treatment for Opioid Use Disorders in the Context of the SAMHSA Opioid STR Grants (R21/R33). Retrieved from https://grants.nih.gov/grants/guide/rfa-files/RFA-DA-18-005.html.
-
Bureau of Drug and Alcohol Services & New Hampshire Center for Excellence. (2016). Guidance Document on Best Practices: Key Components for Delivering Community-Based Medication Assisted Treatment Services for Opioid Use Disorders in New Hampshire.
-
World Health Organization. (2005). WHO Report on Neuroscience of Psychoactive Substance Use and Dependence.
-
Drug Enforcement Administration. Drug Scheduling. Retrieved from https://www.dea.gov/druginfo/ds.shtml.
-
Substance Abuse and Mental Health Services Administration. (2015). National Survey of Substance Abuse Treatment Services (N-SSATS): 2015: Data on Substance Abuse Treatment Facilities. BHSIS Series S-88, HHS Publication No. (SMA)17-5031. Rockville, MD: SAMHSA. Retrieved from https://www.samhsa.gov/data/sites/default/files/2015_National_Survey_of_Substance_Abuse_Treatment_Services.pdf.
-
Substance Abuse and Mental Health Services Administration. (2017). Buprenorphine Waiver Management. Retrieved from https://www.samhsa.gov/medication-assisted-treatment/buprenorphine-waiver-management.
-
Medicaid Medicaid and CHIP Payment and Access Commission. (2017).Report to Congress on Medicaid and CHIP. Retrieved from https://www.macpac.gov/wp-content/uploads/2017/06/June-2017-Report-to-Congress-on-Medicaid-and-CHIP.pdf.
-
Comprehensive Addiction and Recovery Act (CARA) of 2016, P.L.114-198.
-
American Society of Addiction Medicine. (2015). The National Practice Guideline for the Use of Medications in the Treatment of Addiction Involving Opioid Use.
-
Daubresse, M., Saloner, B., Pollack, H.A., & Alexander, G.C. (2017). Non-buprenorphine opioid utilization among patients using buprenorphine. Addiction, 112(6), 1045-1053. DOI: 10.1111/add.13762. Epub 2017 Feb 23.
-
Henry F. Kaiser Family Foundation. (2015). Medicaid Reforms to Expand Coverage, Control Costs and Improve Care: Results from a 50-State Medicaid Budget Survey for State Fiscal Years 2015 and 2016. Retrieved from http://www.kff.org/report-section/medicaid-reforms-to-expand-coverage-control-costs-and-improve-care-managed-care-reforms/.
-
Centers for Medicare & Medicaid. Cost Sharing. Retrieved from https://www.healthcare.gov/glossary/cost-sharing/.
-
Mark, T.L., Yee, T., Levit, K.R., Camacho-Cook, J., Cutler, E., & Carroll, C. D. (2016). Insurance financing increased for mental health conditions but not for substance use disorders, 1986-2014. Health Affairs, 35(6), 958-965.
-
IMS Institute for Healthcare Informatics. (2016). Use of Opioid Recovery Medications: Recent Evidence on State Level Buprenorphine Use and Payment Types. Retrieved fromhttps://www.iqvia.com/-/media/iqvia/pdfs/institute-reports/use-of-opioid-recovery-medications.pdf?la=en&hash=71AAEA662C0B362E34ED2C84C0422F3E3F8F00EC&_=1533137775369.
-
Substance Abuse and Mental Health Services Administration. (2016). State Targeted Response to the Opioid Crisis Grants: Initial Announcement. Retrieved from https://www.samhsa.gov/grants/grant-announcements/ti-17-014.
-
21st Century Cures Act, Section 1003: Account for the State Response to the Opioid Abuse Crisis.
-
Department of Health and Human Services. (2017). Trump Administration Awards Grants to States to Combat Opioid Crisis. Retrieved from https://www.hhs.gov/about/news/2017/04/19/trump-administration-awards-grants-states-combat-opioid-crisis.html.
-
Community Anti-Drug Coalitions of America. (2016). The Comprehensive Addiction and Recovery Act (CARA). Retrieved from http://www.cadca.org/comprehensive-addiction-and-recovery-act-cara.
-
Grants.gov. (2017). #FundingFriday: Federal Grants Addressing the Ongoing Opioid Epidemic in the US. Retrieved from https://blog.grants.gov/2017/03/17/fundingfriday-recent-federal-grant-announcements-addressing-the-ongoing-opioid-epidemic-in-the-us/.
-
Department of Health and Human Services. (2016). HHS Awards $94 million to Health Centers to Help Treat Prescription Opioid Abuse and Heroin Epidemic in America. Retrieved from http://wayback.archive-it.org/3926/20170127185615/https://www.hhs.gov/about/news/2016/03/11/hhs-awards-94-million-to-health-centers.html.
-
California Health and Human Services Agency, Department of Health Care Services. (2017). Narcotic Treatment Program License Application. Retrieved from http://www.dhcs.ca.gov/individuals/Documents/Narcotic_Treatment_Program_License_Application_12.15.2016.pdf.
-
California Department of Health Care Services, Substance Use Disorder Compliance Division. (2017). Narcotic Treatment Programs. Retrieved from http://www.dhcs.ca.gov/individuals/Pages/NTP.aspx.
-
California Department of Health Care Services, Research and Analytic Studies Division. (2017). Medi-Cal Monthly Enrollment Fast Facts: Characteristics of the Medi-Cal Population as Captured by the Medi-Cal Eligibility Data System (MEDS). Retrieved from http://www.dhcs.ca.gov/dataandstats/statistics/Documents/Fast_Facts_January_2017_ADA.pdf.
-
Senator Holly Mitchel, 30th Senate District. Senate Bill 1335: Improving Access to Drug Medi-Cal. http://hcpsocal.org/wp-content/uploads/2016/04/Mitchell.pdf.
-
TI-17-014 MAT Expansion Project. Retrieved from http://californiamethadone.org/wp-content/uploads/2017/02/COMP-PDF.pdf.
-
Centers for Medicare & Medicaid Services. (2015). New Service Delivery Opportunities for Individuals with a Substance Use Disorder. SMD #15-003. Retrieved from https://www.medicaid.gov/federal-policy-guidance/downloads/smd15003.pdf.
-
Legislative Analyst's Office, California Legislature's Nonpartisan Fiscal and Policy Advisor. (2017). The 2017-18 Budget: Analysis of the Medi-Cal Budget. Retrieved from http://www.lao.ca.gov/Publications/Report/3612.
-
California Senate Legislature. (2014). The Administration's Drug Medi-Cal--Organized Delivery System Proposed Waiver. Joint Hearing of the Senate Budget and Fiscal Review Committee and Senate Health Committee.
-
California Department of Health Care Services. Counselor Certification. Retrieved from http://www.dhcs.ca.gov/provgovpart/Pages/CounselorCertification.aspx.
-
California Department of Health Care Services. SAMHSA Opioid State Targeted Response (STR). Retrieved from http://www.dhcs.ca.gov/individuals/Pages/State-Targeted-Response-to-Opioid-Crisis-Grant.aspx.
-
California Health and Human Services Agency, Department of Health Care Services. (2017). Letter: Application Awards to NTP Providers. Retrieved from http://www.dhcs.ca.gov/individuals/Documents/CA_HSS_Awards_7.21.17.pdf.
-
California Health Care Foundation. (2016). Stepping Up to the Plate: Federally Qualified Health Centers Address Growing Demand for Care. Retrieved from https://www.chcf.org/publication/stepping-up-to-the-plate-federally-qualified-health-centers-address-growing-demand-for-care/.
-
Medicare Payment Advisory Commission. (2015). Report to the Congress: Overview of the 340B Drug Pricing Program. Retrieved from http://www.medpac.gov/docs/default-source/reports/may-2015-report-to-the-congress-overview-of-the-340b-drug-pricing-program.pdf?sfvrsn=0.
-
California Health Care Foundation. (2017). Webinar--Academic Detailing: Changing Prescriber Behavior Through Brief, In-Person Encounters.
-
Missour Department of Mental Health. (2016). Memo: Certification Requirements for Medication Assisted Treatment. Retrieved from https://dmh.mo.gov/docs/ada/mat_certification_memo10-25-16.pdf.
-
Mathematica Policy Research. CCBHC Evaluation State Delivery System Profile: Missouri.
-
Missouri Department of Mental Health. (2017). Legislator Briefing: Mental Health Highlights and Issues. Retrieved from https://dmh.mo.gov/opla/pubs/docs/DMHLegislatorBriefing2017.pdf.
-
American Society of Addiction Medicine. Medicaid Coverage of Medications for the Treatment of Opioid Use Disorder: New Hampshire. Retrieved from https://www.asam.org/docs/default-source/advocacy/state-medicaid-reports/state-medicaid-reports_nh.pdf?sfvrsn=6.
-
Community Health Institute/JSI, New Hampshire Center for Excellence. (2014). Substance Use Disorder Treatment and Other Service Capacity in New Hampshire.
-
New Hampshire's Substance Use Disorder Treatment System. (2016). Issue Brief. Retrieved from http://governor.nh.gov/commissions-task-forces/medicaid-care/documents/….
-
Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality. National Survey on Drug Use and Health, 2012 and 2013.
-
Centers for Medicare & Medicaid Services. Special Terms and Conditions, New Hampshire Building Capacity for Transformation.
-
Hassan, M., & Vara, J. The Opiate/Opioid Public Health Crisis: Update on the State of New Hampshire's Comprehensive Response.
-
Mental Health (MH) and Substance Use Disorder (SUD) Parity. Retrieved at https://www.dhhs.nh.gov/ombp/medicaid/parity.htm.
-
Babor, T.F., McRee, B.G., Kassebaum, P.A., Grimaldi, P.L., Ahmed, K., & Bray, J. (2007). Screening, Brief Intervention, and Referral to Treatment (SBIRT): Toward a public health approach to the management of substance abuse. Subst Abuse, 28, 7-30.
-
Substance Abuse and Mental Health Services Administration. (2017). About Screening, Brief Intervention, and Referral to Treatment (SBIRT). Retrieved from https://www.samhsa.gov/sbirt/about.
-
Ohio Opioid STR Project. Retrieved from http://mha.ohio.gov/Portals/0/assets/Funding/CURES/CURES-project-narrative.pdf.
-
Ohio's Medicaid Behavioral Health Redesign. Retrieved from http://www.healthtransformation.ohio.gov/LinkClick.aspx?fileticket=2p-58m6D8tw%3d&tabid=122.
-
Ohio Governor's Cabinet, Opiate Action Team. (2017). Combating the Opiate Crisis in Ohio. Retrieved from http://mha.ohio.gov/Portals/0/assets/Initiatives/GCOAT/Combatting-the-Opiate-Crisis.pdf.
-
Ohio Department of Medicaid. Ohio Medicaid Group VIII Assessment: A Report to the Ohio General Assembly.
-
Behavioral Health Redesign is Ready for July 1, 2017. Retrieved from http://bh.medicaid.ohio.gov/portals/0/about/bh-redesign-update_04252017.pdf?ver=2017-04-25-142616-910.
-
Ohio Department of Health. Governor's Cabinet, Opiate Action Team. (2017). New Strategies to Fight the Opiate and Fentanyl Crisis in Ohio (2016-17). Retrieved from http://mha.ohio.gov/Portals/0/assets/Initiatives/GCOAT/New-Strategies-to-Fight-Opiate-and-Fentanyl-2016-17.pdf.
-
Ohio Legislative Service Commission. (2016). Fiscal Note and Local Impact Statement. Retrieved from https://www.legislature.ohio.gov/download?key=5525&format=pdf.
-
Ohio Mental Health and Addiction Services. Opiate Therapies. Retrieved from http://mha.ohio.gov/Default.aspx?tabid=97.
-
Ohio Governor's Office of Health Transformation. (2016).Overview of Ohio's Redesign of Community Behavioral Health Medicaid Program. Retrieved from http://bh.medicaid.ohio.gov/Portals/0/Users/008/08/8/BH-Redesign-101-slides-OACBHA-5.04.16.pdf?ver=2016-05-19-103018-023.
-
Commonwealth Institute & Virginia Poverty Law Center. How Medicaid Works: A Chartbook for Understanding Virginia's Medicaid Insurance and the Opportunity to Improve it. Retrieved from http://www.thecommonwealthinstitute.org/wp-content/uploads/2013/01/chartbook_2013_v6_rev.pdf.
-
Virginia Department of Health. (2017). Virginia Project ECHO, Request for Proposal.
-
Virginia Department of Health Professions, Board of Medicine. (2017). Retrieved from https://www.dhp.virginia.gov/medicine/newsletters/OpioidPrescribingBuprenorphine03142017.pdf.
-
Henry J. Kaiser Family Foundation. (2017). Medicaid's Role in Addressing the Opioid Epidemic. Retrieved from http://www.kff.org/infographic/medicaids-role-in-addressing-opioid-epidemic/.
-
Busch, S.H., Meara, E., Huskamp, H.A., et al. (2013). Characteristics of adults with substance use disorders expected to be eligible for Medicaid under the ACA. Psychiatric Serv, 64, 520-526.
-
Wen, H., Hockenberry, J.M., Borders, T.F., & Druss, B.G. (2017). Impact of Medicaid expansion on Medicaid-covered utilization of buprenorphine for opioid use disorder treatment. Medical Care, 55(4), 336-341.
-
Beronio, K., Glied, S., & Frank, R. (2014). How the Affordable Care Act and Mental Health Parity and Addiction Equity Act greatly expand coverage of behavioral health care. Journal of Behavioral Health Services and Research, 41(4), 410-428.
-
Centers for Medicare & Medicaid Services. (2016). Medicaid and Children's Health Insurance Programs; Mental Health Parity and Addiction Equity Act of 2008; the Application of Mental Health Parity Requirements to Coverage Offered by Medicaid Managed Care Organizations, CHIP, and Alternative Benefit Plans. Federal Register. Retrieved from https://www.federalregister.gov/documents/2016/03/30/2016-06876/medicaid-and-childrens-health-insurance-programs-mental-health-parity-and-addiction-equity-act-of.
-
Henry J. Kaiser Family Foundation. (2017). Total Professionally Active Physicians. Retrieved from https://www.kff.org/other/state-indicator/total-active-physicians/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D.
-
Rosenblatt, R.A., Andrilla, C.H., Catlin, M., & Larson, E.H. (2015). Geographic and specialty distribution of US physicians trained to treat opioid use disorder. Ann Fam Med, 13(1), 23-26. DOI: 10.1370/afm.1735. PubMed PMID: 25583888
-
Knudsen, H.K., Lofwall, M.R., Havens, J.R., & Walsh, S.L. (2015). States' implementation of the Affordable Care Act and the supply of physicians waivered to prescribe buprenorphine for opioid dependence.Drug Alcohol Depend, 157, 36-43. DOI: 10.1016/j.drugalcdep.2015.09.032. Epub 2015 Oct 9. PubMed PMID: 26483356; PubMed Central PMCID: PMC4663127.
APPENDIX A. DIFFERENCES AMONG OPIOID USE DISORDER MEDICATIONS
| EXHIBIT A-1. Differences among OUD Medications1,2,3 | |||
|---|---|---|---|
| Prescribing Considerations | Methadone | Naltrexone | Buprenorphine |
| Product/Formulation | Methadose, Diskets, Dolophine | Extended-release injectable/depot/xr-npx, Vivitrol; oral, ReVia, Depade | Suboxone*, Subutex, Zubsolv*, Bunavail*, Buprenex, Butrans, Probuphine |
| Mechanism of Action and Effects | Full agonist (Binds to and activates MU opioid receptors): Long-acting for 36-72 hours, providing steady blood levels which avoid reward (euphoria) due to peak effects and avoids withdrawal or craving due to low blood levels; reduce opioid cravings and withdrawal symptoms | Antagonist (binds and completely blocks opioid reward effects); diminish the reinforcing effects of opioids (potentially extinguishing the association between conditioned stimuli and opioid use) | Partial agonist (binds to and partially activates MU opioid receptors): Long-acting, providing steady blood levels which avoid reward (euphoria) due to peak effects and avoids withdrawal or craving due to low blood levels; relieve opioid cravings and withdrawal symptoms |
| Route of Administration | Oral tablet or liquid | Intramuscular injection or oral | Sublingual tablet or sublingual or buccal film; FDA recently approved an implant to deliver at a low dose over 6 months |
| Frequency of Administration | Daily | Monthly (injection) or daily (oral) | Daily |
| Regulatory Context | Can only be dispensed at a certified OTP | No restrictions. Any health care provider who has a license to prescribe medications (i.e., physician, PA, NP) can prescribe it. It can only be delivered after complete detoxification from opioids. | Only a licensed physician with a DEA registration and a buprenorphine (DATA 2000) waiver can prescribe it in an office-based setting. Waivered physicians can then only prescribe buprenorphine to a regulated maximum number of patients (can be 30, 100, or 275 patients, depending on the waiver). |
| Controlled Substance Schedule | Schedule II | Not a scheduled medication | Schedule III |
| Level of Engagement | All patients diagnosed with a SUD can benefit from recovery support programs | ||
NOTES:
* Suboxone, Zubsolv, and Bunavail contain both buprenorphine and naloxone. Naloxone is an antagonist typically used to reverse the effects of opioid overdose. When combined with buprenorphine, however, it is used to avoid the use of this drug intravenously. If intravenous abuse occurs, then the person will experience immediate withdrawal compared to taking the medication as prescribed. | |||
APPENDIX B. STATE OPIOID EPIDEMIC PROFILES
Profile References
TI-17-014 MAT Expansion Project. Retrieved from http://californiamethadone.org/wp-content/uploads/2017/02/COMP-PDF.pdf.
California Department of Public Health. (2016). State of California Strategies to Address Prescription Drug (Opioid) Misuse, Abuse, and Overdose Epidemic in California.
IMS Institute for Healthcare Informatics. (2016). Use of Opioid Recovery Medications: Recent Evidence on State Level Buprenorphine Use and Payment Types. Retrieved fromhttps://www.iqvia.com/-/media/iqvia/pdfs/institute-reports/use-of-opioid-recovery-medications.pdf?la=en&hash=71AAEA662C0B362E34ED2C84C0422F3E3F8F00EC&_=1533137775369.
Virginia Medicaid and CHIP Data Book. (2016).
Virginia Department of Medical Assistance Services, Medicaid Program. (2017). Medicaid at a Glance.
Ohio Mental Health and Addiction Services. (2017). CURES Workforce Development.
Ohio Governor's Cabinet, Opiate Action Team. (2017). Combating the Opiate Crisis in Ohio. Retrieved from http://mha.ohio.gov/Portals/0/assets/Initiatives/GCOAT/Combatting-the-Opiate-Crisis.pdf.
Henry J. Kaiser Family Foundation. (2015). Opioid Overdose Deaths and Opioid Overdose Deaths as a Percent of All Drug Overdose Deaths. Retrieved from https://www.kff.org/other/state-indicator/opioid-overdose-deaths/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D.
Bureau of Drug and Alcohol Services & New Hampshire Center for Excellence. (2016). Guidance Document on Best Practices: Key Components for Delivering Community-Based Medication Assisted Treatment Services for Opioid Use Disorders in New Hampshire.
New Hampshire Prescription Drug Monitoring Program. Annual Report October 1,2015 - September 20, 2016.
Griffin, M. (2017). Missouri Senate passes prescription drug monitoring program, with some changes. St. Louis Public Radio. Retrieved from http://news.stlpublicradio.org/post/missouri-senate-passes-prescription-drug-monitoring-program-some-changes#stream/0.
Centers for Disease Control and Prevention. (2016). Increases in drug and opioid-involved overdose deaths--United States, 2010-2015. Morbidity and Mortality Weekly Report. Retrieved from https://www.cdc.gov/mmwr/volumes/65/wr/mm655051e1.htm.
Graves, S. (2013). California Budget Project. Looking Toward 2014: Key Facts About the Medi-Cal Expansion.
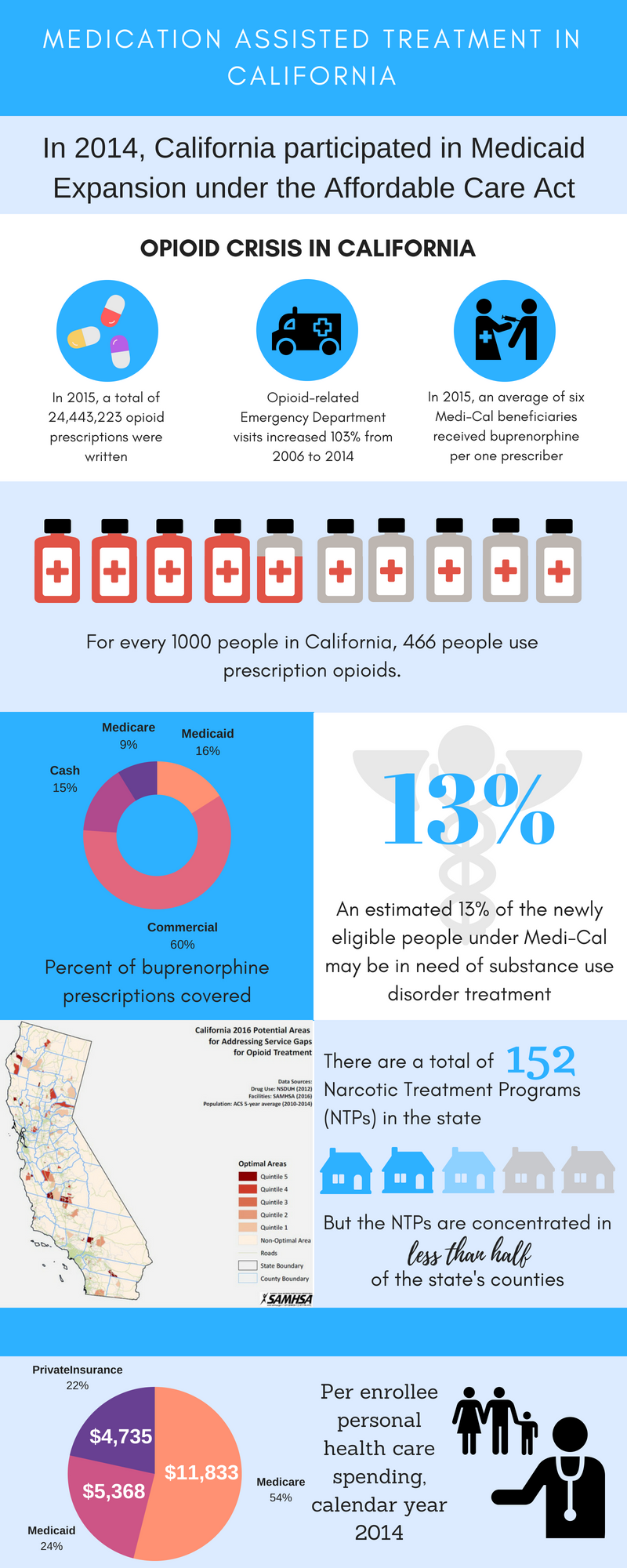 |
| ALT Text: This image is an infographic illustrating medication-assisted treatment in California. At the top of the infographic is text that reads, "In 2014, California participated in Medicaid Expansion under the Affordable Care Act." Below that is a series of three icons that illustrate the opioid crisis in California. The first icon is of 3 pills, and below that is text reading, "In 2015, a total of 24,443,223 opioid prescriptions were written." The second icon is of an ambulance, and below that is text reading, "Opioid-related Emergency Department visits increased 103% from 2006 to 2014." The third icon is of a health care provider giving an injection to a patient, and below that is text reading, "In 2015, an average of 6 Medi-Cal beneficiaries received buprenorphine per 1 prescriber." Below that group of icons is an image of 10 medicine vials arranged in a row. Four and two-thirds of the vials appear to be full, and the others are empty. Text below the image reads, "For every 1000 people in California, 466 people use prescription opioids." Below the 10 medicine vials and their associated text is a group of 4 images. Moving clockwise from the left, the first image is a doughnut chart illustrating the percent of buprenorphine prescriptions covered. Sixty percent of buprenorphine prescriptions covered are commercial, 16% are Medicaid, 15% are cash, and 9% are Medicare. The second image shows a caduceus (symbol of medicine) in the background. Superimposed on top of it is "13%." The text below reads, "An estimated 13% of the newly eligible people under Medi-Cal may be in need of substance use disorder treatment." The third image is a map of California titled "California 2016 Potential Areas for Addressing Service Gaps for Opioid Treatment." Data sources for the map are NSDUH (2012) for drug use, SAMHSA (2016) for facilities, and ACS 5-year average (2010-2014) for population. The map is divided into 5 quintiles. The fifth quintile represents the most optimal area for addressing service gaps, and the first quintile represents the least optimal area. The legend also displays non-optimal areas, roads, state boundaries, and county boundaries. The SAMHSA logo is displayed at the bottom of the map image. The fourth image has the text, "There are a total of 152 Narcotic Treatment Programs (NTPs) in the state," followed by a row of 5 icons shaped like houses, with more text below the houses reading, "But the NTPs are concentrated in less than half of the state's counties." In the image, the number "152" and the text "less than half" are formatted differently from the surrounding text so they stand out. At the bottom of the infographic is a pie chart that displays per enrollee personal health care spending for calendar year 2014. Medicare spending represented $11,833 or 54%, Medicaid spending represented $5,368 or 24%, and private insurance spending represented $4,735 or 22%. To the right of the pie chart is an icon of a family of 3 (husband, wife, and child) beside an icon of a health care provider wearing a stethoscope. |
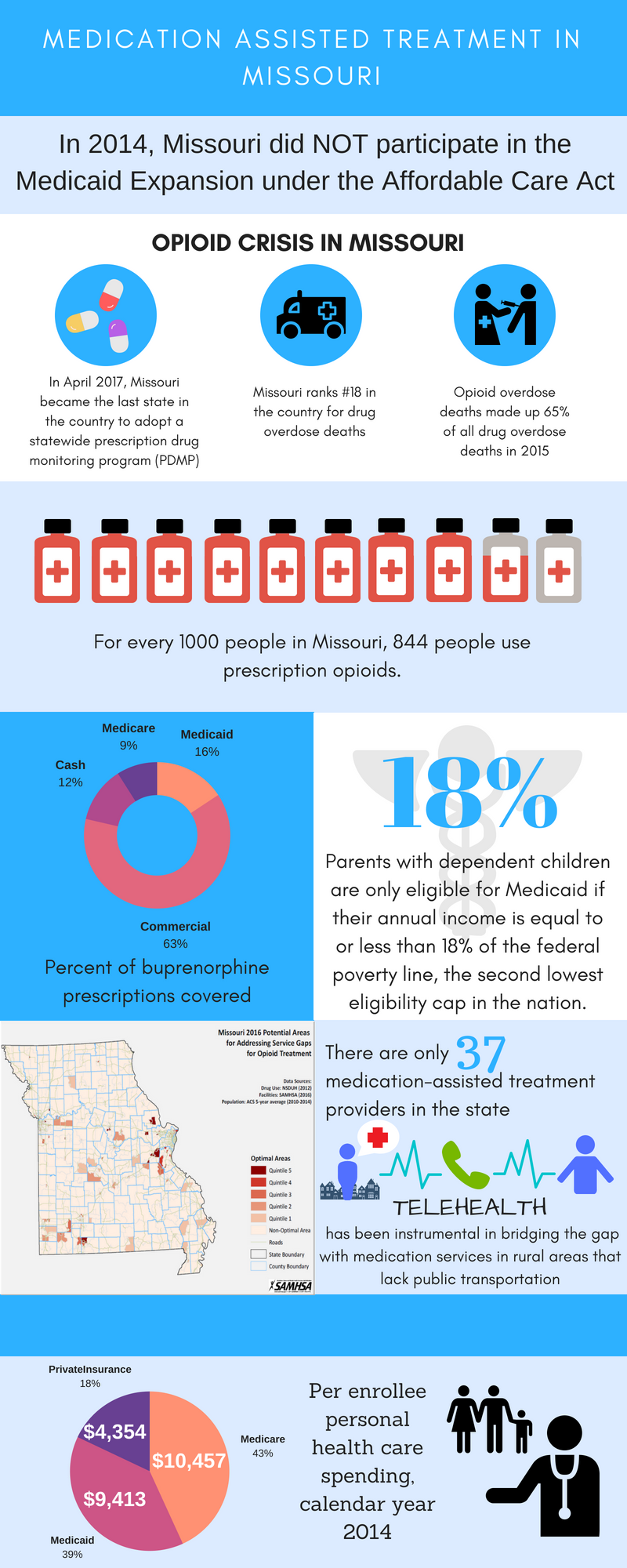 |
| ALT Text: This image is an infographic illustrating medication-assisted treatment in Missouri. At the top of the infographic is text that reads, "In 2014, Missouri did NOT participate in the Medicaid Expansion under the Affordable Care Act." Below that is a series of 3 icons that illustrate the opioid crisis in Missouri. The first icon is of 3 pills, and below that is text reading, "In April 2017, Missouri became the last state in the country to adopt a statewide prescription drug monitoring program (PDMP)." The second icon is of an ambulance, and below that is text reading, "Missouri ranks #18 in the country for drug overdose deaths." The third icon is of a health care provider giving an injection to a patient, and below that is text reading, "Opioid overdose deaths made up 65% of all drug overdose deaths in 2015." Below that group of icons is an image of 10 medicine vials arranged in a row. Eight and two-thirds of the vials appear to be full, and the other is empty. Text below the image reads, "For every 1000 people in Missouri, 844 people use prescription opioids." Below the 10 medicine vials and their associated text is a group of 4 images. Moving clockwise from the left, the first image is a doughnut chart illustrating the percent of buprenorphine prescriptions covered. Sixty-three percent of buprenorphine prescriptions covered are commercial, 16% are Medicaid, 12% are cash, and 9% are Medicare. The second image shows a caduceus (symbol of medicine) in the background. Superimposed on top of it is "18%." The text below reads, "Parents with dependent children are only eligible for Medicaid if their annual income is equal to or less than 18% of the federal poverty line, the second lowest eligibility cap in the nation." The third image is a map of Missouri titled "Missouri 2016 Potential Areas for Addressing Service Gaps for Opioid Treatment." Data sources for the map are NSDUH (2012) for drug use, SAMHSA (2016) for facilities, and ACS 5-year average (2010-2014) for population. The map is divided into 5 quintiles. The fifth quintile represents the most optimal area for addressing service gaps, and the first quintile represents the least optimal area. The legend also displays non-optimal areas, roads, state boundaries, and county boundaries. The SAMHSA logo is displayed at the bottom of the map image. The fourth image has the text, "There are only 37 medication-assisted treatment providers in the state," followed by an icon of a treatment provider in a city speaking on the phone with a patient, with more text below the icon reading, "Telehealth has been instrumental in bridging the gap with medication services in rural areas that lack publication transportation." In the image, the number "37" and the text "Telehealth" are formatted differently from the surrounding text so they stand out. At the bottom of the infographic is a pie chart that displays per enrollee personal health care spending for calendar year 2014. Medicare spending represented $10,457 or 43%, Medicaid spending represented $9,413 or 39%, and private insurance spending represented $4,354 or 18%. To the right of the pie chart is an icon of a family of 3 (husband, wife, and child) beside an icon of a health care provider wearing a stethoscope. |
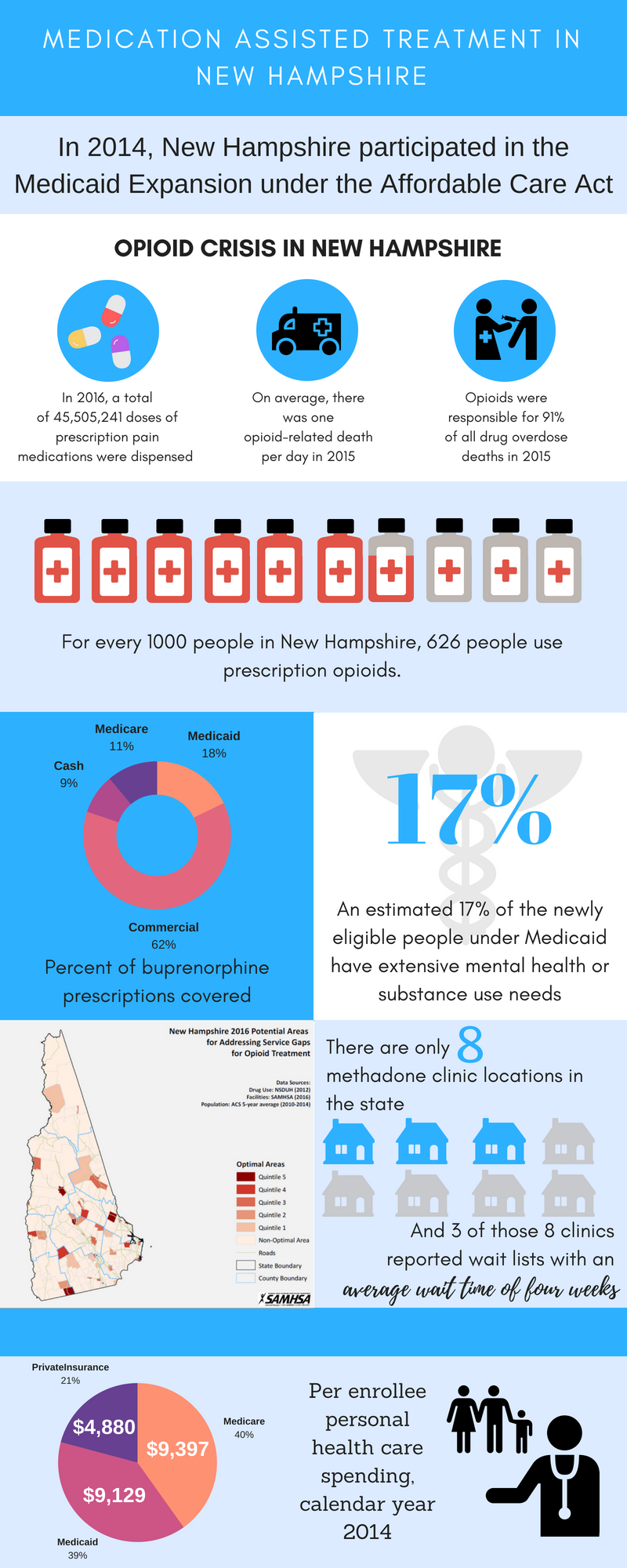 |
| ALT Text: This image is an infographic illustrating medication-assisted treatment in New Hampshire. At the top of the infographic is text that reads, "In 2014, New Hampshire participated in the Medicaid Expansion under the Affordable Care Act." Below that is a series of 3 icons that illustrate the opioid crisis in New Hampshire. The first icon is of 3 pills, and below that is text reading, "In 2016, a total of 45,505,241 doses of prescription pain medications were dispensed." The second icon is of an ambulance, and below that is text reading, "On average, there was 1 opioid-related death per day in 2015." The third icon is of a health care provider giving an injection to a patient, and below that is text reading, "Opioids were responsible for 91% of all drug overdose deaths in 2015." Below that group of icons is an image of 10 medicine vials arranged in a row. Six and two-thirds of the vials appear to be full, and the other 3 are empty. Text below the image reads, "For every 1000 people in New Hampshire, 626 people use prescription opioids." Below the 10 medicine vials and their associated text is a group of 4 images. Moving clockwise from the left, the first image is a doughnut chart illustrating the percent of buprenorphine prescriptions covered. Sixty-two percent of buprenorphine prescriptions covered are commercial, 18% are Medicaid, 11% are Medicare, and 9% are cash. The second image shows a caduceus (symbol of medicine) in the background. Superimposed on top of it is "17%." The text below reads, "An estimated 17% of the newly eligible people under Medicaid have extensive mental health or substance use needs." The third image is a map of New Hampshire titled "New Hampshire 2016 Potential Areas for Addressing Service Gaps for Opioid Treatment." Data sources for the map are NSDUH (2012) for drug use, SAMHSA (2016) for facilities, and ACS 5-year average (2010-2014) for population. The map is divided into 5 quintiles. The fifth quintile represents the most optimal area for addressing service gaps, and the first quintile represents the least optimal area. The legend also displays non-optimal areas, roads, state boundaries, and county boundaries. The SAMHSA logo is displayed at the bottom of the map image. The fourth image has the text, "There are only 8 methadone clinic locations in the state," followed by 8 house icons with 3 of them colored blue, with more text below the house icons reading, "And 3 of those 8 clinics reported wait lists with an average wait time of 4 weeks." In the image, the number "8" and the text "average wait time of 4 weeks" are formatted differently from the surrounding text so they stand out. At the bottom of the infographic is a pie chart that displays per enrollee personal health care spending for calendar year 2014. Medicare spending represented $9,397 or 40%, Medicaid spending represented $9,129 or 39%, and private insurance spending represented $4,880 or 21%. To the right of the pie chart is an icon of a family of 3 (husband, wife, and child) beside an icon of a health care provider wearing a stethoscope. |
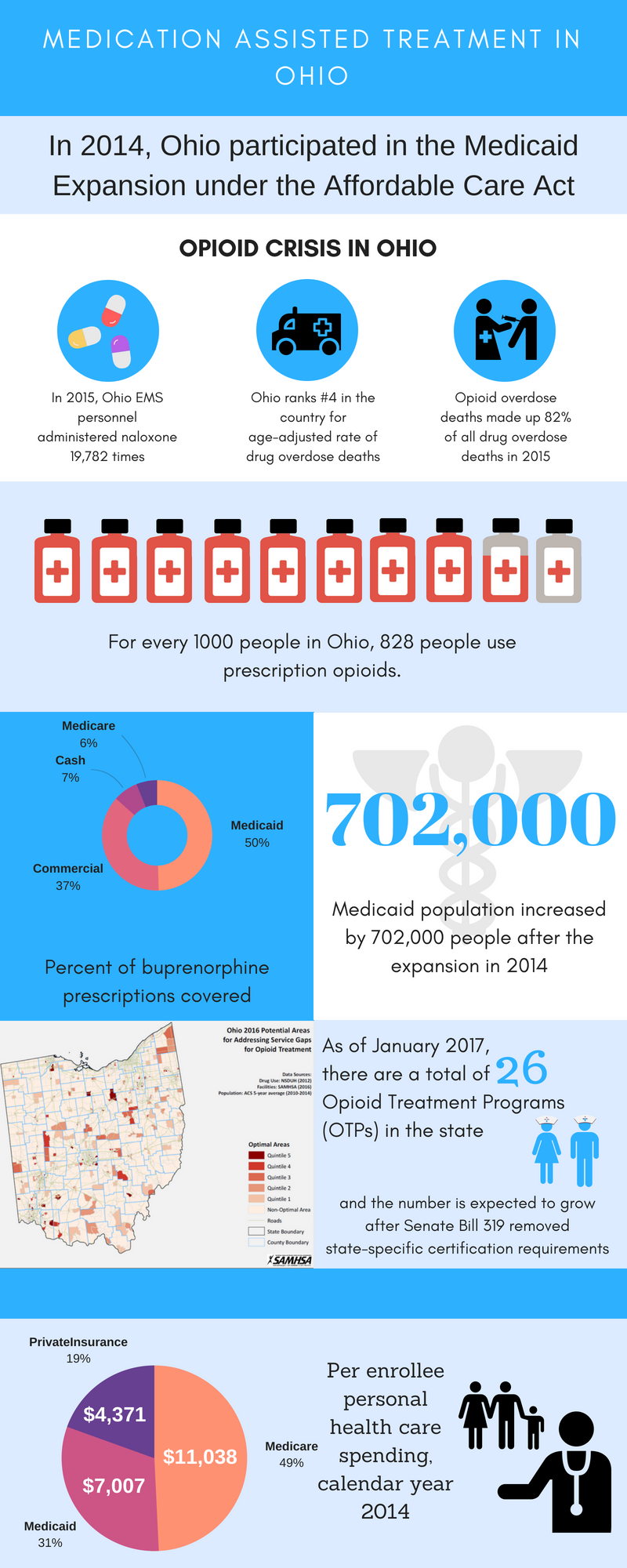 |
| ALT Text: This image is an infographic illustrating medication-assisted treatment in Ohio. At the top of the infographic is text that reads, "In 2014, Ohio participated in the Medicaid Expansion under the Affordable Care Act." Below that is a series of 3 icons that illustrate the opioid crisis in Ohio. The first icon is of 3 pills, and below that is text reading, "In 2015, Ohio EMS personnel administered naloxone 19,782 times." The second icon is of an ambulance, and below that is text reading, "Ohio ranks #4 in the country for age-adjusted rate of drug overdose deaths." The third icon is of a health care provider giving an injection to a patient, and below that is text reading, "Opioid overdose deaths made up 82% of all drug overdose deaths in 2015." Below that group of icons is an image of 10 medicine vials arranged in a row. Eight and two-thirds of the vials appear to be full, and the other is empty. Text below the image reads, "For every 1000 people in Ohio, 828 people use prescription opioids." Below the 10 medicine vials and their associated text is a group of four images. Moving clockwise from the left, the first image is a doughnut chart illustrating the percent of buprenorphine prescriptions covered. Fifty percent of buprenorphine prescriptions covered are Medicaid, 37% are commercial, 7% are cash, and 6% are Medicare. The second image shows a caduceus (symbol of medicine) in the background. Superimposed on top of it is "702,000." The text below reads, "Medicaid population increased by 702,000 people after the expansion in 2014." The third image is a map of Ohio titled "Ohio 2016 Potential Areas for Addressing Service Gaps for Opioid Treatment." Data sources for the map are NSDUH (2012) for drug use, SAMHSA (2016) for facilities, and ACS 5-year average (2010-2014) for population. The map is divided into 5 quintiles. The fifth quintile represents the most optimal area for addressing service gaps, and the first quintile represents the least optimal area. The legend also displays non-optimal areas, roads, state boundaries, and county boundaries. The SAMHSA logo is displayed at the bottom of the map image. The fourth image has the text, "As of January 2017, there are a total of 26 Opioid Treatment Programs (OTPs) in the state," followed by an icon of a female nurse standing beside an icon of a male nurse, with more text below the nurse icons reading, "and the number is expected to grow after Senate Bill 319 removed state-specific certification requirements." In the image, the number "26" is formatted differently from the surrounding text so it stands out. At the bottom of the infographic is a pie chart that displays per enrollee personal health care spending for calendar year 2014. Medicare spending represented $11,038 or 49%, Medicaid spending represented $7,007 or 31%, and private insurance spending represented $4,371 or 19%. To the right of the pie chart is an icon of a family of 3 (husband, wife, and child) beside an icon of a health care provider wearing a stethoscope. |
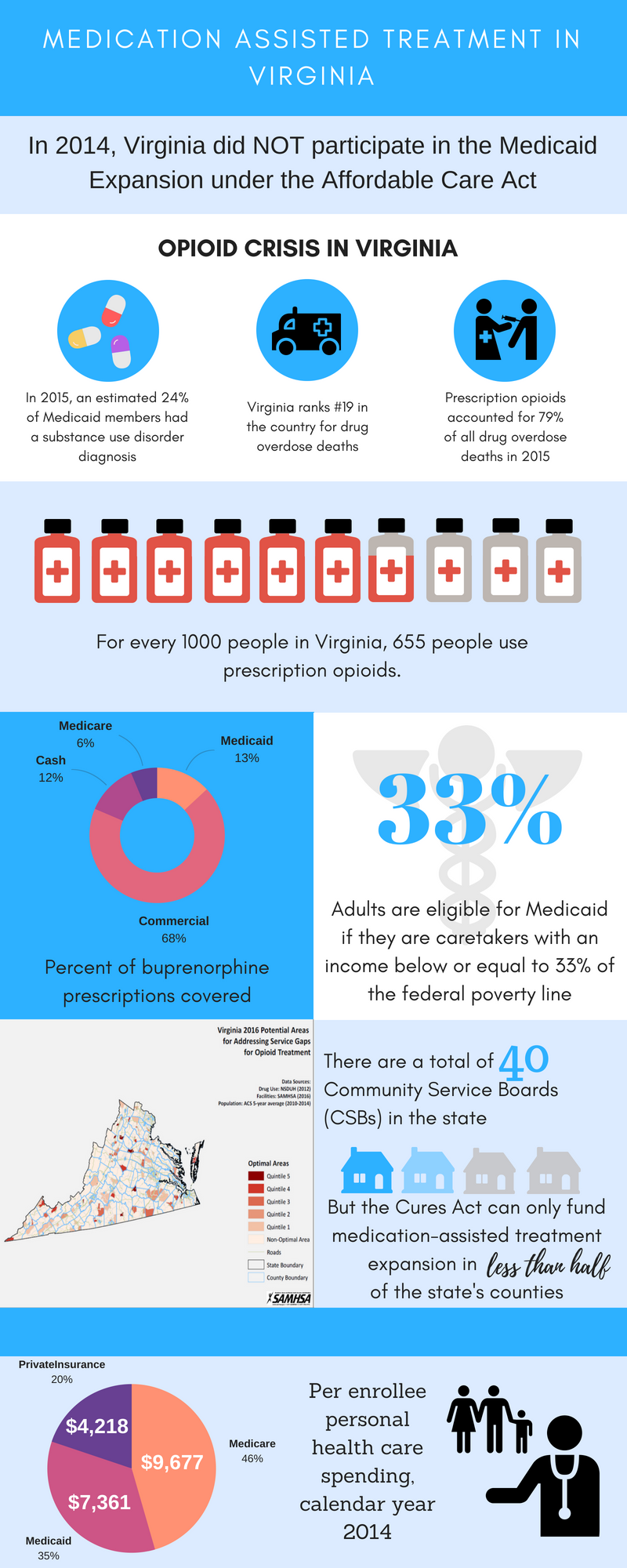 |
| ALT Text: This image is an infographic illustrating medication-assisted treatment in Virginia. At the top of the infographic is text that reads, "In 2014, Virginia did NOT participate in the Medicaid Expansion under the Affordable Care Act." Below that is a series of 3 icons that illustrate the opioid crisis in Virginia. The first icon is of 3 pills, and below that is text reading, "In 2015, an estimated 24% of Medicaid members had a substance use disorder diagnosis." The second icon is of an ambulance, and below that is text reading, "Virginia ranks #19 in the country for drug overdose deaths." The third icon is of a health care provider giving an injection to a patient, and below that is text reading, "Prescription opioids accounted for 79% of all drug overdose deaths in 2015." Below that group of icons is an image of 10 medicine vials arranged in a row. Six and two-thirds of the vials appear to be full, and the other three are empty. Text below the image reads, "For every 1000 people in Virginia, 655 people use prescription opioids." Below the 10 medicine vials and their associated text is a group of 4 images. Moving clockwise from the left, the first image is a doughnut chart illustrating the percent of buprenorphine prescriptions covered. Sixty-eight percent of buprenorphine prescriptions covered are commercial, 13% are Medicaid, 12% are cash, and 6% are Medicare. The second image shows a caduceus (symbol of medicine) in the background. Superimposed on top of it is "33%." The text below reads, "Adults are eligible for Medicaid if they are caretakers with an income below or equal to 33% of the federal poverty line." The third image is a map of Virginia titled "Virginia 2016 Potential Areas for Addressing Service Gaps for Opioid Treatment." Data sources for the map are NSDUH (2012) for drug use, SAMHSA (2016) for facilities, and ACS 5-year average (2010-2014) for population. The map is divided into 5 quintiles. The fifth quintile represents the most optimal area for addressing service gaps, and the first quintile represents the least optimal area. The legend also displays non-optimal areas, roads, state boundaries, and county boundaries. The SAMHSA logo is displayed at the bottom of the map image. The fourth image has the text, "There are a total of 40 Community Service Boards (CSBs) in the state," followed by a row of 4 icons shaped like houses, with more text below the houses reading, "But the Cures Act can only fund medication-assisted treatment expansion in less than half of the state's counties." In the image, the number "40" and the text "less than half" are formatted differently from the surrounding text so they stand out. At the bottom of the infographic is a pie chart that displays per enrollee personal health care spending for calendar year 2014. Medicare spending represented $9,677 or 46%, Medicaid spending represented $7,361 or 35%, and private insurance spending represented $4,218 or 20%. To the right of the pie chart is an icon of a family of 3 (husband, wife, and child) beside an icon of a health care provider wearing a stethoscope. |
Analyses of Disability, Aging, and Long Term Care Policy and Data
This report was prepared under contract #HHSP233201600021I between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and RTI International. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/office-disability-aging-and-long-term-care-policy-daltcp or contact the ASPE Project Officers, Helen Lamont, Laurel Fuller and Judith Dey, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201; Helen.Lamont@hhs.gov, Laurell.Fuller@hhs.gov, Judith.Dey@hhs.gov.
Reports Available
An Overview of Long-Term Services and Supports and Medicaid: Final Report
-
HTML: https://aspe.hhs.gov/basic-report/overview-long-term-services-and-supports-and-medicaid-final-report
-
PDF: https://aspe.hhs.gov/pdf-report/overview-long-term-services-and-supports-and-medicaid-final-report
State and Local Policy Levers for Increasing Treatment and Recovery Capacity to Address the Opioid Epidemic: Final Report