
U.S. Department of Health and Human Services
A Framework for Identifying High-Impact Interventions to Promote Reductions in Late-Life Disability
Vicki A. Freedman, Nancy Hodgson, Joanne Lynn, Brenda Spillman, Timothy Waidmann, Anne Wilkinson, and Douglas A. Wolf
Project Team
September 27, 2006
PDF Version (90 PDF pages)
This report was prepared under contract #HHS-100-03-0011 between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and the Urban Institute. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officers, William Marton and Hakan Aykan, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. Their e-mail addresses are: William.Marton@hhs.gov and Hakan.Aykan@hhs.gov.
The Project Team (authors) are listed alphabetically. Jeannette Rogowski also served as a consultant to the project. The project team thanks Karen Kohn for her excellent assistance with identifying and tracking references. The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS
- I. INTRODUCTION
- A. Purpose
- B. Background
- C. Extensions of Existing Framework
- II. CONCEPTUAL FRAMEWORK
- A. Definitions and Scope
- B. The Proposed Framework
- C. What Constitutes High-Impact?
- III. LITERATURE REVIEWS
- A. Methodology
- B. Reviews
- IV. COMPARISONS BASED ON CONCEPTUAL FRAMEWORK AND LITERATURE REVIEW
- A. Comparison of Short-Term Effects
- B. Comparison of Long-Term Effects
- C. Illustration of Long-Term Effects of Interventions
- VI. APPENDIX: METHODOLOGY TO IDENTIFY ILLUSTRATIVE HIGH IMPACT INTERVENTIONS
- A. Approach
- B. Findings
- VII. LITERATURE CITED
- LIST OF FIGURES
- FIGURE 1: Illustration of Functional Ability Before Death for Three Illnesses Trajectories
- FIGURE 2: Illustration of Functional Trajectories, Disability, and Death from Age 65 through 100
- FIGURE 2b: Illustration of Disease, Functional Limitation, Disability, and Death from Age 65 through 100, With and Without Interventions
- FIGURE 3: Proportion of Individual Lifetime and Years Lived in Each State: 3 Baseline Illustrations
- FIGURE 4: Proportion of Cohorts Remaining Lifetime Spent in Each State: 1 Baseline Illustration and 2 Intervention Illustrations
- FIGURE 5: Point-in-Time Distribution of Population by Disease/Disability State, by Age
- LIST OF TABLES
- TABLE 1: Illustrative Scenarios to Achieve 1% Decrease in Disability Prevalence in 1 Year
- TABLE 2: Assumptions for Simulation
- TABLE 3: Results of Simulation Designed to Demonstrate Long-Term High Impact Effects
- TABLE 4: Comparisons of Illustrative Interventions
- TABLE 5: Results of Simulation Designed to Demonstrate Long-Term Effects of Interventions
- TABLE A-1: Rankings of 12 Interventions with Respect to Short-Term Disability, Long-Term Disability, Length of Life, and Number of People Potentially Affected
- TABLE A-2: Patterns of High Ranking Interventions
ABSTRACT
Considerable evidence now suggests that the prevalence of disability among older Americans is declining; however, how best to implement intervention strategies to promote continued or accelerated declines in disability prevalence remains unstudied. The purpose of this report is to develop and begin to demonstrate a new framework for comparing the population-level effects of different types of interventions. Drawing upon elements of the proposed framework, we reviewed the literature for seven illustrative interventions and also conducted several simple modeling exercises. Of the seven approaches we reviewed, evidence of modest reductions in the risks of disability is strongest for exercise programs that increase strength, balance, and physical activity of older adults; depression screening, combined with referral and feedback and a treatment program combining therapy with pharmacologic treatment; and multi-factor fall prevention programs. Because they can be targeted at potentially large populations, widespread implementation of such interventions could potentially reduce the prevalence of disability in the short run if adherence issues could be successfully addressed. Little evidence exists, however, about the long-term effects of such interventions. This exercise has also provided several additional insights into how to reduce population-level disability prevalence among the elderly population. Our most striking finding is that efforts with the largest potential for success are those targeted at individuals whose life experience is exemplified by a prolonged period of disability and frailty before death. Multi-factor interventions that are targeted at frail individuals and that address individualized needs appear to be the most promising. Both short and long-term effects are critical to consider when evaluating the population-level impact of such interventions.
EXECUTIVE SUMMARY
Motivation and purpose. Considerable evidence now suggests that the prevalence of disability among older Americans is declining. This finding suggests that not only are older people living longer, but they may be enjoying more years of active life.
How best to implement intervention strategies to promote continued or accelerated declines in disability prevalence remains unstudied. Studies of disability trends among the population ages 65 and older have focused almost exclusively on establishing trends in disability prevalence and, to a lesser extent, potential explanations for those trends. Studies of individual interventions occasionally include projected effects at the population level, but in general such studies do not facilitate explicit comparisons among various types of interventions.
Identifying high-impact interventions to reduce disability prevalence requires reconceptualizing disability at the individual level and translating those ideas into population-level implications. The purpose of this report is to develop and begin to demonstrate a new framework for comparing the population-level effects of different types of interventions.
With the framework in mind, we reviewed the literature for seven illustrative interventions, seeking to learn how existing strategies compare. To focus the scope of this exercise, we purposefully limited our attention to interventions that were existing but not already widespread, had some published evidence demonstrating efficacy, and if implemented, could provide benefit within a few years. We selected the following interventions from a list of 12 by tabulating rankings provided by external reviewers with input from the Office of the Assistant Secretary for Planning and Evaluation and project team members:
- Implement smoking cessation programs for the older population.
- Improve exercise. The literature review focuses on exercise interventions in frail but otherwise healthy elderly people.
- Implement good chronic disease care. To narrow this set of interventions, we focus on chronic disease care for a commonly disabling condition: congestive heart failure (CHF).
- Implement depression screening, treatment, and follow-up.
- Implement fall prevention systems for frail elderly persons.
- Modify homes and provide assistive devices.
- Implement widespread care planning for seriously ill people.
We also reviewed the relatively limited literature evaluating multi-component interventions aimed at preventing or alleviating disability in late-life.
Conceptual underpinnings of framework. The proposed conceptual framework extends existing frameworks and models in several ways. First, building on the Institute of Medicines disablement process framework,1 the approach distinguishes among interventions designed to affect an individuals risk along different junctures of the disablement process from onset of disease to death. Second, building on Lunney and colleagues,2, 3 the proposed approach explicitly recognizes that interventions are often designed for and targeted at individuals with specific diseases and injuries, many of which conform to one of three prototypical trajectories: (1) a short period of evident decline (e.g., in patients with cancers); (2) moderate and slowly declining functioning with intermittent exacerbations and sudden dying (e.g., organ system failures); and (3) a prolonged period of disability before death (e.g., dementia, disabling strokes and frailty). Third, we extend well-established notions in the epidemiological literature about risk factors and health outcomes to explicitly address the effect of interventions aimed at altering distributions of risk factors for late-life disability.
Key factors to consider. The change in cross-sectional disability prevalence that would emerge in the presence and absence of an intervention(s), depends on three key factors:
- At which trajectory(ies) and at what point in the disablement process is the intervention targeted? What are the competing risks for other trajectories, causes of disability, and death?
- What is the size of the target population among the current older population and among future cross-sections? That is, how large a target population has the risk factor(s) targeted by the given intervention?
- What is the effect of the intervention on disability (either directly on disability or indirectly through shifts in functioning or illness trajectories) and mortality? The effect in the population will be influenced by:
- the risk factors influence on disability and mortality;
- the interventions efficacy in reducing the risk factor (how well it works in ideal circumstances) over time;
- the likely extent of adherence to the intervention in the target population (what percent maintain the protocol) in the short-run and longer-run; and
- the generalizability of study results (i.e., the difference between the composition of the at-risk population and those in clinical trials in factors related to the efficacy of the intervention).
In the proposed framework we consider disability to be the inability to carry out tasks independently, that is, without help from another person. Thus, in this framework, an environmental modification (e.g., addition of grab bars or ramp) that allows an individual to maintain independence would be considered an intervention that reduces the prevalence of disability. The approach we develop allows for a discussion of tradeoffs in both the short-term and long-term.
What is high-impact? Our interest is in identifying and comparing potentially high-impact interventions. We estimate that in a one-year period, it would take approximately 175,000 fewer people ages 65 and older with disability to generate a 1% decline in disability (e.g., from 20% to 19.8%). To gain a sense of what a high-impact intervention might achieve in the longer term, we created a very simple simulation to suggest what combinations of: (1) trajectory dynamics, (2) target population size, and (3) effects on disability and mortality, would be needed to sustain a 1% per year decline in disability. Our calculations suggest that a number of scenarios could move the age-adjusted disability rate, for instance, from 20% to 16% in 20 years. For example, one scenario would require interventions that would drastically reduce the expected years with a disability with no improvements in longevity for people in two trajectories--from 2.0 to 0.5 for people who die from cancer and from 3.0 to 1.0 for people who experience organ failure. A less drastic, but still sizeable, compression would be required for interventions aimed at the third trajectory (frailty/dementia). That is, the disability rate would be reduced by 1% per year from an intervention that reduced the expected years with a disability from 5.0 to 3.6 but did not alter life expectancy among people in this trajectory. Similar reductions could be achieved by postponing the onset of all three trajectories and adding four years of active life on average over the next 20 years.
Short-term comparisons. To compare short-run effects of the illustrative interventions, we compared interventions along three dimensions: size of the population with the targeted risk factor; short-term risk of disability associated with the targeted risk factor; and short-term effectiveness of the intervention in alleviating targeted risk factor. We found that comparisons across studies were particularly challenging because measures of disability, composition of study populations, and follow-up periods varied widely. Moreover, we were unable to identify a comprehensive study documenting either the relative importance of or co-occurrence of the environmental, physical, and psychological causes of disability. Nevertheless, we found:
-
Variation in the size of population with targeted risk factor. Interventions vary widely in the size of the population with the targeted risk factor. Three of the seven interventions we reviewed may be aimed at a large (10-18 million) target population: exercise, fall prevention, and depression screening and treatment; three other interventions--smoking cessation, management of CHF, and advanced care planning--target a substantially smaller population. Depending on how the target population is defined, assistive technology/home modifications fall somewhere in between.
-
Variation in short-term risk of disability associated with targeted risk factor. Interventions vary in effectiveness in part because they target fundamentally different kinds of risk factors for disability. One can, however, group risk factors (and intervention efforts) by the stage of the disablement process at which they are targeted. All else equal, secondary (CHF management, depression management, fall management) and tertiary prevention efforts (assistive technologies and environmental modifications) aimed at groups already experiencing disease or disability will have the greatest effect in the short run. Primary prevention strategies aimed at disease onset (exercise, smoking cessation) will have a weaker impact in the short-run.
-
Effects of intervention on risk factors and on disability. Of the seven interventions reviewed, there was evidence of a potentially modest effect on risk factors of interest for four of them: smoking cessation programs that combine counseling with pharmacologic treatment; exercise programs that increase strength, balance, and physical activity of older adults; depression screening, combined with referral and feedback, and combination therapy/pharmacologic treatment; and multi-factor fall prevention programs. Of those four, only three have been linked to reductions in risks of disability: exercise, depression screening and treatment, and fall prevention programs. The short-term effects of a population-based exercise intervention and of depression screening and treatment on disability risks are likely to be modest whereas multi-factor programs that successfully reduce the risk of falling could potentially have a large effect on the risks of disability.
Long-term comparisons. To compare long-term effects of the illustrative interventions, we considered three additional dimensions: How will the size and composition of the target population change in the future? At which trajectory is the intervention targeted and what are the competing risks? What are the effects of the intervention over the remaining lifetime? In particular, how will the intervention affect mortality as well as disability? We found:
-
Some targeted risk factors are already on the decline. Several well-known demographic trends have been identified which will influence the effectiveness of interventions--the aging of the population, its increasing racial and ethnic diversity, increases in obesity and related chronic conditions, and increases in educational attainment. In addition, for several of the interventions investigated here, we found evidence of ongoing trends. For instance, four of the seven risk factors of interest--inactivity, smoking, depression treatment, and assistive technology/home modification--appear to be moving already in a direction consistent with disability decline. There is also some evidence that injuries due to non-fatal falls have decreased and that advance care planning is increasing slowly. In contrast, CHF appears to be increasing. Limited information is available on trends in the joint distribution of these risk factors.
-
Variation in trajectories targeted and competing risks. Each of the illustrative interventions we reviewed may be targeted at one or more illness trajectories. Exercise and fall prevention, for example, are primarily targeted to older adults whose life experience is exemplified by a prolonged period of disability and frailty before death. CHF management is clearly targeted to a specific type of organ failure. Smoking cessation is likely to be geared toward people who go on to develop cancer or organ failure. Depression screening and treatment, assistive technology and environmental modifications, and advanced care planning are not unique to any one trajectory but may be targeted at all three. The issue of competing risks arises mainly for interventions targeted at the prevention of diseases with earlier ages of onset. That is, interventions designed to prevent cancer or organ failure, if successful, could allow people to experience the longer-lived frailty trajectory. Of the seven illustrative interventions reviewed here, consideration of competing risks is most important for smoking cessation.
-
Important relationships between lifetime disability and prevalence of disability. In longer-run comparisons it is important to understand the interventions effect not only on disability but also upon the length of life and whether (or what proportion of) additional years are free from disability. Intervention studies rarely examine effects beyond a year or two after the intervention, so we turned to life table analyses for insights into this issue. Using life table principles, we demonstrated the comparative effects on cross-sectional disability of hypothetical interventions affecting disease prevention (through shifts in trajectories), disease management (with and without mortality effects), and disability. We found that:
Disease prevention/trajectory shift: Interventions aimed at preventing disease or shifting people from cancer or organ failure trajectories to the longer-lived frailty trajectory resulted in no perceptible change in the population-level prevalence of disability, due to countervailing effects of reduced mortality and increased number of years lived with disability. For example, cutting the chances of eventually dying from cancer or organ failures by half has a negligible effect on the cross-sectional rate of disability.
Disease management: Interventions aimed at managing the course of disease will result in declines in disability prevalence only if: (a) the intervention does not alter the risk of mortality, or (b) resulting changes in disability-free life expectancy exceed changes in disabled life expectancy. For example, the exercise interventions discussed in the literature appear to be targeted at the frailty trajectory and have no apparent effect on mortality. If they delay disability onset by one year in this population (increasing disability-free life expectancy by one year), the estimated effect on disability prevalence is a reduction from 20.3% to 17.6%. Alternatively, suppose that smoking cessation interventions aimed at older people with a diagnosis of cancer or organ failure coincided with such diagnoses and resulted in an extension of life for both trajectories. In this case the disability rate would increase to 21.8%.
Shift in the disability threshold: Whether a limitation in functioning results in disability depends in part on the environment in which tasks take place. If home modifications or assistive technologies could reduce the amount of time spent living with a disability by 25%, disability prevalence would decline from 20.3% to 16.3%. Much smaller reductions (say of 5%) would still yield declines in disability (for example from 20.3% to 19.5%). The role of the environment as a component of late-life disability is not well understood, but merits further consideration.
Mortality-only interventions: An intervention to increase advance care planning may have the effect of reducing the period of disability at the end of life for frail individuals; but, as currently practiced, efforts to increase advance care planning would have practically no effect on the cross-sectional prevalence of disability.
Summary of key findings. Of the seven illustrative approaches we reviewed, evidence of reducing the risks of disability is strongest for exercise interventions, depression screening and treatment, and multi-factor fall prevention efforts. Because they can be targeted at potentially large populations, and may have modest or even potentially large effects on the risks of disability, widespread implementation of such interventions could potentially reduce the prevalence of disability in the short run if adherence issues could be addressed. Little evidence exists, however, about the long-term effects of such interventions on disability and its interplay with length of life.
This exercise has also provided several additional insights into how to reduce population-level disability prevalence among the elderly population. Our most striking finding is that efforts with the largest potential for success are those targeted at individuals whose life experience is exemplified by a prolonged period of disability and frailty before death. Multi-factor interventions that are targeted at frail individuals and that address individualized needs appear to be the most promising. However, both short and long-term effects are critical to consider when evaluating the population-level impact of such interventions.
I. INTRODUCTION
A. Purpose
Considerable evidence now suggests that older Americans are not only living longer, but rates of disability in late-life are declining.4, 5, 6 Whether the declines reported over the last decade or two will continue is the subject of much debate.7, 8, 9, 10, 11, 12, 13, 14, 15, 16 These trends, and their potential continuation, are of great interest for several reasons. In view of the large growth in both the absolute and relative numbers of older people in the population, the care needs and costs, both public and private, of meeting those needs, are widely thought to present major fiscal and public-health challenges in coming decades. Furthermore, disability is closely related to the quality of life not only of those with disabilities, but their family members as well.
Projections of the older population suggest that continued declines in rates of disability will be important to achieve. One set of projections, which assumes continued declines in mortality and disability of 0.6% per year, suggests the number of older Americans with disability will increase from about six million today to over ten million in 2050.17 Others have noted that impending shifts in risk factors related to disability--(such as education)18 or obesity13--might make it difficult to achieve continued declines on the order observed over the past decade or two. Based on a series of alternative projections,19 one study concludes that whether the decline in population-level disability continues has enormous implications for the size of the disabled population in the future and for the ability of the society to care for its disabled elderly members.
To date, the discussion has not focused per se on how best to implement intervention strategies to promote continued declines in the prevalence of disability. Identifying high-impact interventions to reduce population-level disability requires a new and broad-based approach to thinking about disability at the individual-level, from onset through the end of life and translating those ideas into population-level implications. The purpose of this report is to develop and begin to demonstrate a new framework for comparing the effects of different types of interventions on a consistent set of population outcomes.
The report is divided into five major sections. The rest of this chapter summarizes the literature that we drew upon in creating the framework that we then use to compare the population-level effectiveness of interventions to promote disability decline. Chapter II presents the framework for comparing population-level effects of interventions to reduce the prevalence of late-life disability. Chapter III presents the methodology used to select and carry out comparisons among seven illustrative interventions and provides a summary of relevant evidence from randomized controlled trials (RCTs) regarding each of the seven interventions. Chapter IV provides insight into the extent of available information for quantitative comparisons of short-term and long-term differentials in the effectiveness of the illustrative interventions. Chapter V summarizes major findings.
B. Background
Three distinct literatures bear on the development of a conceptual framework for evaluating the relative merits of late-life disability interventions. Two emphasize conceptual models of disability--both conceived of at the individual level. A third set of quantitative studies from the epidemiologic and public-health literature has emphasized the etiology of disability, quantifying the extent of disability attributable to various chronic conditions, and linking risk factors and disease distributions to disability prevalence.
The Disablement Process and Conceptual Models of Disability
A conceptual framework for understanding the disablement process at the individual level and identifying strategic points for preventive intervention was developed by the Institute of Medicine (IOM).1 In this model, the concepts of pathology, impairment, and functional limitation represent deficits or damage at the cellular, organ, and person level, respectively. Disability is socially defined, as it depends upon an interaction of an individuals functional limitations with the demands imposed by the environment and his or her own expectations about daily life.
As discussed in the IOM report, the standard public-health model distinguishes three types of prevention efforts: primary, defined as efforts to avoid the onset of pathological processes; secondary, defined as efforts aimed at slowing the progression of disease; and tertiary, which includes strategies that restore function and increase autonomy among people with reduced functional capacity.1 Examples of primary prevention efforts include educating about health habits (e.g., smoking, alcohol, obesity) and fall prevention. Secondary prevention measures include chronic disease management efforts and screening for potentially complicating co-morbidities. Tertiary prevention includes rehabilitation of physical, cognitive, and functional deficits and the introduction of environmental modifications and assistive technology.
The disabling effects of impairments can be reduced or potentially eliminated by changes in either the abilities of the individual or the demands of the environment.20 These adaptations include: ability modification (where the individuals capabilities are enhanced through medical intervention and rehabilitation or through the use of assistive devices) and environmental modification (where the demands of the physical environment are reduced through change of residence or installing architectural enhancements).21
The disablement process model is completely general and describes, at the individual level, a dynamic process comprising onset of and recovery from disease and injury, use and effectiveness of treatments, adaptive responses, and feedback mechanisms. A more recent development emphasizes trajectories at the end of life.
Illness Trajectories at the End of Life
Lynn and colleagues have advanced the notion of the trajectory of fatal chronic illness which denotes the usual course of illness severity and care needs over time.22 Three prototypical pathways distinguished by the course of functioning in the years before death have been suggested: (1) a short period of evident decline (e.g., in patients with cancers); (2) moderate and slowly declining functioning with intermittent exacerbations and sudden dying (e.g., organ system failures); and (3) a prolonged period of disability before death (e.g., as seen in dementia, disabling strokes and frailty). Recent attempts to verify and quantify these trajectories2, 22 have upheld these conceptual distinctions, suggesting that cancer and organ system failure account for about 1/5 of deaths each and frailty for up to 40% of deaths. A fourth, smaller group is characterized by having no disability and a sudden death (7%-16%).
The terminal illness (e.g., advanced or metastatic cancer) trajectory (top panel of Figure 1) is characterized by a short period of decline. The typical cancer patient comes to diagnosis with few symptoms and the physical distress associated with the illness is due, at least initially, to cancer treatments. These patients may function reasonably well with their illness for quite some time before the disease becomes overwhelming and non-responsive to treatment. At that point, they usually die within a 6-8 week terminal phase.23, 24, 25, 26, 27 Among the major causes of death, only cancer routinely manifests a clearly defined phase of worsening functional, emotional, and social impairment with a high prevalence of symptoms.28 Some cancers do not behave this way, most notably breast and prostate cancer; and sometimes AIDS and other conditions can follow this pattern.
The advanced, chronic organ system failure trajectory (middle panel of Figure 1) has emerged only recently, as the result of sophisticated medications, antibiotics, and mechanical ventilation, which have improved the likelihood of surviving acute disease exacerbations that would have proved fatal in earlier times for individuals. This trajectory includes conditions that tend to have erratic and unpredictable courses, set against a backdrop of progressive decline and physical disability. Hospitalization rates and survival are predictable for populations, though not for individuals.29 These patients have long periods of relative stability punctuated by episodes of acute illness for which the outcome is always uncertain. This trajectory includes individuals who die within a few years, but the persistent uncertainty of prognosis keeps them from being acknowledged as terminally ill. The illness course is characterized by moderate and slowly declining functional limitations between exacerbations. Each exacerbation could result in death, but usually these patients have many such episodes over the course of several years.30, 31 If they survive an acute exacerbation, typically they return to stability but often with diminished functional capacity. Examples of such diseases are congestive heart failure (CHF) and chronic obstructive pulmonary disease (COPD).32, 33
Finally, the dementia/frailty disease trajectory (bottom panel, Figure 1) is characterized by a long period with a low level of function with a slower decline, and with steadily progressive disability, loss of independence, and increasing need for supervision and assistance. This course can arise from stroke, Parkinsons disease, Alzheimers disease, multi-infarct dementia, or just the declining function of various organs that is associated with advanced old age. Individuals with these conditions are likely to lose much of their function in the course of their disease and yet live on, experiencing intermittent, often small, changes in their functional status as they near death. The most severely deteriorated patients are dependent in all or most of their activities of daily living (ADLs), are unable to engage in purposeful activities, have speech limitations, and typically are no longer able to recognize their loved ones. People with severe frailty without dementia often die of complications following falls or sepsis, and many have delirium or depression as part of the experience of their last months.
Population Epidemiology and Public-Health
A distinct set of studies in the epidemiology and public-health literature has raised issues at the population level, focusing on the etiology of disability, the extent of disability attributable to specific diseases, and how changes in distributions of risk factors or disease might affect population-level prevalence of functional limitations and/or disability.
Etiology of disability. Embedded in both the disablement process and the illness trajectories is the notion that disability can be attributed to a physical or mental illness or injury, or to physiological changes associated with aging. Several investigators have found that, among people ages 65 and over reporting disability, arthritis and other musculoskeletal conditions are the most common conditions reported as causes.4, 34, 35 In their review of the literature, Fried and Guralnik36 cite 13 chronic diseases associated consistently with the development of physical disability in older adults: arthritis, hip fracture, diabetes, stroke, heart disease (myocardial infarction, angina, and CHF), claudication, COPD, visual impairment, depression, and cognitive impairment.
For the purposes of identifying high-impact interventions, such simplistic classifications pose several problems. First, a substantial number of older people attribute their disability to old age.37 Second, as people age, the likelihood of a single medical cause for disability decreases. More than half of older people with a disability have multiple chronic diseases or impairments.38, 39 In some instances a disease may not be sufficient to cause substantial disability in itself, but may increase risk of subsequent functional decline if another condition develops.36 By extension, in some circumstances attention to one disease might be sufficient to alleviate disability; in other cases multiple underlying problems must be identified and addressed. Third, classification according to medical cause ignores the critical role of the environment in defining disability. Environmental modifications in the home, for example, might enable an older person to remain independent despite the onset of chronic disease or injury.
Studies of population attributable proportion. A few investigators have attempted to quantify what proportion of disability in the population is attributable to different chronic conditions.40, 41 The population attributable proportion can be estimated from information about the relative risk of disability given a specific chronic condition and the prevalence of that condition in the population. For example, one study of adults ages 16 and older in the Netherlands from 1989 to 1992 found 25% of disability could be attributed to musculoskeletal conditions, and 4% to neurological conditions such as stroke.40 Similarly, analysis of data from seniors in the Framingham Heart Study interviewed during the 1980s found 15% of disability was attributable to osteoarthritis (OA), 10% to depression, 9% to heart disease, and 9% to neurological diseases such as stroke.41 Both studies controlled for the presence of co-morbidities but did not investigate the joint distributions of multiple causes. Moreover, in practice, relative risks are generally drawn from cross-sectional prevalence data; hence, whereas they provide some insight into the relative contributions of various diseases in a cross-section, they do not provide insights into the relationship between the risks of disease and disability over the remaining lifetime. Nor have environmental components of disability been incorporated into such frameworks.
Disease elimination studies. A related set of studies has addressed the tradeoffs from eliminating different chronic diseases. Boult and colleagues, for example, demonstrated the future effects on person-years of functioning of controlling for six fatal and nonfatal conditions.42 Assuming the prevalence of other chronic conditions remained constant, they found that decreasing the prevalence of arthritis by 1% every two years would lead to a much greater reduction in functional limitation between 2001 and 2049 than would decreasing any of the other conditions by the same amount. Decreases in two fatal conditions (cancer and coronary artery disease (CAD)) would lead to increases in functional limitation. Similarly, Nusselder and colleagues evaluated the effect of eliminating a specific disease on the mortality, long-term disability, and health status in the Dutch population.43 Assuming independence among competing causes of death, they found that eliminating disabling nonfatal diseases such as arthritis/back complaints results in a decline in life expectancy with disability--that is, an absolute compression of morbidity. Eliminating highly fatal diseases such as cancer leads to an increase in the number of years and the proportion of life with disability--that is, a relative expansion of morbidity. As with the studies of population attributable proportion, cause elimination studies do not take into account the multi-factorial nature of disability, nor do they provide insight into the extent to which the environment could be altered to alleviate disability.
Studies of population avoidable risk. A set of papers from on the Global Burden of Disease project, a collaborative project between Harvard University School of Public Health, the World Health Organization, and the World Bank, for example, explicitly focuses on the burden of risk factors for death and disability.44 The analyses draw upon an epidemiologic framework that attributes the burden of disease or injury in a population (expressed as prevalence) to the distribution of exposure to risk factors in the past. The approach they have developed allows one to calculate the extent of disability/injury that could have been averted in the population if that risk factor had been eliminated, or changed to another distribution, presumably through interventions. They use the term avoidable disability to denote the extent of future disability that could be avoided due to future changes in the distribution of risk factors. Although the authors do not explicitly address the link between interventions and risk factors, the general approach is useful in that it sets the stage for thinking about the potential future effect of interventions at the population level.
C. Extensions of Existing Framework
The proposed conceptual framework for comparing population-level effectiveness of interventions to promote disability decline integrates and extends existing frameworks and models in several ways:
-
First, building on the IOM framework, the approach distinguishes among interventions designed to affect an individuals risk along different junctures of the disablement process, from onset of disease to death.
-
Second, building on Lynn and colleagues, the proposed approach explicitly recognizes that interventions are often designed for and targeted at individuals with specific diseases and injuries, many of which conform to one of three prototypical functional pathways discussed earlier.
-
Third, we extend the epidemiological risk factor approach to explicitly include interventions designed to alter the distribution in a population of risk factors for late-life disability. The framework recognizes the multi-factorial nature of interventions and risk factors--that is, they do not have a simple one-to-one correspondence.
-
Fourth, the approach allows for a discussion of tradeoffs in both the short-term and long-term. That is, the approach recognizes that there may be short-term effects (e.g., benefits from interventions in a one-year period), and/or long-term effects (e.g., over the remaining lifetime of successive cohorts of the older population), and that ultimate effects depend on the point in the disablement process in which the intervention is introduced and the risks involved in experiencing alternative (competing) trajectories.
II. CONCEPTUAL FRAMEWORK
A. Definitions and Scope
Our focus here is on interventions late in life (specifically for populations ages 65 and older) designed to alter the distribution in the population of one or more modifiable risk factors and, therefore, reduce the population-level prevalence of disability.
We define interventions to include strategies that might be effective in delaying indefinitely or postponing disability onset, slowing the course of decline, or promoting recovery and/or independence. Strategies might also modify the risks at any point along the disablement process, by altering the risk of disease or injury, functional limitations, or death. Our interest is in understanding both the short-term and long-term effectiveness of such interventions.
Effectiveness in this context is defined as the benefit of an intervention for a given group in the population, and takes into account both the efficacy (under ideal conditions of investigation) and the acceptance and implementation of the intervention by those in the general population of older adults. Thus the effectiveness takes into account issues not included in clinical trials, such as compliance and differential efficacy for varying groups.
Risk factors in this context refer to any factor that may increase an individuals chances of living with a disability--either by influencing his or her chances of developing a disease, having functional limitations, experiencing disability, or dying. Modifiable risk factors include behavioral, medical, social, and environmental factors. Non-modifiable risk factors--such as demographic characteristics and genetic makeup--may be important in predicting disability onset, recovery, and death but are less relevant for our purposes here because one cannot (currently) alter the distributions of such factors through interventions in late-life. We refer to an individuals unique set of non-modifiable and modifiable risk factors related to their risk of disability as their disability risk profile.
One of the major challenges in summarizing the literature is the wide variety of disability-related outcome measures used in late-life intervention studies. Two widely used approaches differ by whether they measure the extent of underlying difficulty--without help or assistive devices--or, the extent of residual difficulty--with help or assistive technology if used. A third commonly used approach is to determine if help or assistive devices are used to carry out basic activities. In the proposed framework in this report, we define disability as the inability to carry out tasks independently, that is, without help from another person. Thus, in this framework, an environmental modification (e.g., addition of grab bars or ramp) that allows an individual to maintain independence would be considered an intervention that reduces the prevalence of disability.
To focus the scope of this project, we have purposefully limited consideration to interventions that are: (a) existing; (b) not already widespread; (c) have some published evidence demonstrating efficacy; and (d) if implemented, might provide benefit within a few years in terms of reducing disability prevalence in the older population (rather than waiting for decades or having most effect upon early or mid-life populations).
Finally, we explicitly recognize the multi-factorial nature of interventions, risk factors, and disability. A given intervention, for example, exercise, might affect the distribution of more than one risk factor for disability (e.g., recovery from surgery and the risk of injury from a fall). In addition, the distribution of a single risk factor (e.g., injury from fall) may be influenced by multiple interventions. For example, exercise and home modifications both reduce the prevalence of injuries from falls and may have larger effects together than either has alone. Thus, we recognize that the effects of implementing multiple interventions may not be strictly additive, but may have synergistic effects (interacting in either a positive or negative direction).
B. The Proposed Framework
The proposed framework consists of three perspectives: individual, cohort, and cross-sectional. To fully understand the population-level phenomena, one must first begin by understanding the complexities at the individual level among interventions, risk factors, and illness trajectories. We then describe potential intervention effects in terms of a single cohort. Finally, we develop an account of how interventions effects on successive cohorts of individuals will alter cross-sectional snapshots of disability prevalence.
Individual-Level Dynamics
The four trajectories in Figure 2 show prototypical patterns of functioning over an individuals lifetime. Each can be taken to represent distinctive manifestations of risk profiles taking effect as the person ages.
The approach considers not just a single point in ones life, but what might happen over the course of an individuals potential lifetime, from ages 65 and beyond. In this context, potential lifetime extends to some possibly arbitrarily assumed upper limit. For simplicity, here the hypothetical lifetime is set to 100 years.a
The solid line represents a minimum level of physical or cognitive functioning necessary to care for oneself. In other words, it may be considered a threshold below which a functional limitation results in disability.
The figures demonstrate four prototypical experiences. At one extreme, individuals who reach age 65 and develop cancer, for example, ordinarily experience the onset of disease early on and eventually evidence a rapid decline. In contrast, individuals who develop dementia experience a slow and steady decline in functioning for a much longer time period.
Figure 2b illustrates several different ways that an intervention may alter the risks of disability. The top panel illustrates approaches that may be used to target individuals who experience organ failure. Disease management programs, such as those developed to manage CHF, shift both functioning and years lived. The bottom panel illustrates approaches that may be targeted at individuals whose experience exemplifies the frailty trajectory. For example, exercise programs targeted at the frail elderly population, may target maintenance of functioning (at a level above the threshold for disability), without shifting risks of mortality. In both the upper and lower panels, the effect of home modification programs is illustrated. Changes to the environment affect disability by shifting the disability threshold, rather changing functional status per se.
In addition, although not explicitly illustrated in the figure, interventions designed to delay or postpone indefinitely the onset of a trajectory, for example, by delaying or preventing cancer or organ failure, may increase the risk of another trajectory, for example, the risk of experiencing the frailty/dementia trajectory may increase.
The bars in Figure 3 summarize for each of the illustrative individuals in Figure 2--each following a different prototypical trajectory--how much time that person will spend in each of five states of the disablement process: healthy, with disease or injury but no limitation, functionally limited but without a disability, with a disability (defined as dependence), and dead. Thus, Figure 3 summarizes, from the perspective of an initial point (e.g., age 65), the disease, functional limitation, and disability (and death) trajectory that lies ahead.
Starting with the first bar, the hypothetical individual who dies from a solid tumor cancer spends five of the 35 potential years between age 65 and 100 (14%) in a healthy state, two years (6%) with disease but no limitation, one year (1%) with functional limitation but no disability, and about two years (6%) with a disability before dying at age 75. In this scenario, 26 potential years of life (73%) are foregone. The second bar illustrates the proportion and years lived in each state for a typical older person with organ failure. In this illustration, five years are spent healthy, six years with disease but with no functional limitations, one year with functional limitations and about three years with disability before dying at age 80. The final bar illustrates the proportion and years spent for a typical older person who is frail and develops dementia, with 15 years spent without the disease, one year spent with the disease but no limitations, one year with limitations but no disability, and five years with disability before dying at age 87.
We focus here on illustrative trajectories that are most prevalent. About 22% of the population dies from solid tumors, 16% from organ failure, 46% with dementia or frailty.3 However, we recognize that there are additional trajectories that may involve fewer states. For example, an individual who has a spinal cord injury early in life might live to age 80, and spend 15 of the years between age 65 and death with a disability; alternatively, an individual may live to age 80 in a healthy state (with no signs of disease) and die suddenly from cardiac arrest. Or, an individual who has experienced repeat episodes of depression over his or her lifetime may never develop functional limitations but may have periods where he or she is unable to perform basic ADLs without help. Nevertheless, emphasizing the three most common trajectories will provide the basis for exploring the experience of nearly 85% of the population.
Population-Level Implications: Cohort Perspective
The future experience of a group of people who are all age 65 today--a cohorts future experience--is the average of all the individuals experiences in the population. Figure 4 shows for a hypothetical cohort of individuals who are all age 65 today the average amount of time spent in each state, for a baseline case (with no interventions) and for the illustrative cases of two different types of hypothetical and purposefully exaggerated interventions. That is, suppose at the end of 35 years of an intervention for a cohort, the cohorts experience is apportioned into the five states as shown in the Figure. Starting with the first bar, the baseline case, the hypothetical cohort age 65 today will die on average at the age of 82. Of the 35 years between age 65 and 100, the cohort will spend on average 11 years in a healthy state (31% of the 35 potential years), two years (6%) on average with disease but no limitations, one year (3%) with a functional limitation, three years (9%) with a disability, and 18 years (51%) foregone.
Just as individuals in the cohort have unique disability risk profiles, the cohort has a unique distribution of these profiles, and distributions of factors that make up the profile. Some of these distributions--such as age, sex, race, and cumulative experiences to date--will change in the future but are not modifiable per se whereas others--distributions of current and future diseases, behaviors, and the environment--may be altered. Thus, over the remaining course of the cohorts lifetime, the cumulative amount of time the group experiences disability--and the severity of that disability--might be affected by interventions that alter the distributions of individuals disability risk profiles.
The second bar in Figure 4 illustrates a hypothetical intervention that works primarily by altering the environment so that the risk of either onset of disability is very low, or the risk of recovery from an episode so high, that the average number of years spent with a disability is less than one. In the extreme, picture the smart house or other supportive environment in which technology makes it possible to be independent in instrumental daily activities despite substantial underlying functional limitations. Because the risks of developing disease, functional limitations, and dying are not affected, the average number of years lived with disability is close to one; at the same time the average number of years lived with functional limitations increases from one to three on average, (or from 3% to 9% of the cohorts potential remaining lifetime).
The third bar in Figure 4 illustrates a more complex hypothetical intervention--one that works by both reducing the likelihood of developing a disability, and by lowering the risk of death. Given this more complex (and more realistic) set of possibilities, it now becomes possible that a population may spend on average more years of life with a disability, or without, or the additional years of life may be divided somehow between the two. This bar illustrates a potential shift in the average amount of lifetime spent with a disability due to interventions targeted at both disability and death. Suppose, for example, that some intervention--the addition of grab bars and a stool to the shower--allows an individual to shower independently and reduces the risk of dying from an injury, thereby altering both the risk of disability and death. At the end of 100 years this intervention might result in more years lived on average (so the average age at death is 84 instead of 82). It might also result in a higher average number of years spent with a disability (four years instead of three) and with a limitation (two years instead of one).
Not shown in the figure are more complex examples of interventions that target risk factors earlier in the disablement process--for example exercise--which operate on the risks of developing a disease (e.g., CHF) and injury (e.g., from a fall). These illnesses and injuries then in turn alter an individuals risk of developing later in life functional limitations, disability, and ultimately death. Over the lifetime of a cohort such interventions might change the cohorts experience with disability in complex ways. The cohort-level predictions are even more complicated by the issue of competing risks--for example, if CHF and falls are eliminated, how many more cases of Alzheimers disease will develop? In other words, because an individual will usually go on to develop other illnesses, with different prototypical trajectories (potentially ones with a greater risk of disability for a longer time period), preventing a disease with an intervention does not necessarily result in a lower proportion of a cohorts potential lifetime spent with a disability.
Population-Level Implications: Cross-Sectional Perspective
Now imagine successive cohorts of individuals ages 65 and older. If we classified all individuals born over the last 100 years into one of the five states in Figure 4 (healthy, has disease but no limitation, has limitation but no disability, has a disability, dead), the distribution across those states would depend on the age distribution of the population and the experience of the cohort over the past 100 years--both modifiable and non-modifiable risk factors. The short-run impact of an intervention at the population level will depend upon not only the relative short-term effectiveness of that intervention for persons at each age, but on the relative size of each age group and the baseline distribution of each age group across disease and disability groups. One such possibility is pictured in Figure 5. Figure 5 represents a point-in-time picture of the population arrayed by age (along the horizontal axis) and across states (vertical axis). The solid lines show the baseline distribution, while the dashed lines depict an alternative distribution in the presence of a hypothetical intervention (alternatively, the reader can view the dashed lines as a picture of the same population one year later, after the previous years 64-year-olds have aged into it). Again, we include those who have died, but could potentially have lived past age 65.
Finally, imagine moving forward in time, and having each cohort that reaches age 65 exposed to an intervention beginning the day they turn 65. The longer-run impact of a sustained intervention effort will play out over time. The change in cross-sectional distributions of the five states that would emerge in the presence and absence of such intervention(s) depends on three key factors:
- At which trajectory(ies) and at what point in the disablement process is the intervention targeted? What are the competing risk for other trajectories, causes of disability, death?
- What is the size of the target population among the current older population and among future cross-sections.
- What is the effect of the intervention on disability (either directly on disability or indirectly through shifts in functioning or illness trajectories) and mortality? The effect in the population will be a the influenced by:
- the risk factors influence on disability and mortality;
- the interventions efficacy in reducing the risk factor (how well works in ideal circumstances) over time;
- the likely extent of adherence in the target population (what percent maintain the protocol) in the short-run and longer-run; and
- the generalizability of study results (i.e., the difference between the composition of the at-risk population and those in clinical trials in factors related to the efficacy of the intervention).
C. What Constitutes High-Impact?
The proposed framework allows for comparisons across the five key factors but does not in and of itself delineate the exact meaning of high-impact. Here we discuss briefly the policy-relevant context for establishing a definition of high-impact in both the short-term and long-term.
Because policy makers are often concerned with year-to-year variation over time, we assume a priori that the goal is to reduce the cross-sectional disability prevalence rate. A one-year unit of time is often used to track changes in policy-relevant measures. However, when considering the long-term outcomes, other appropriate measures of disability that take into account individuals remaining lifetimes could also be considered--for example, years of active life, proportion of life spent active.
Over the last two decades, the prevalence of disability with ADL or instrumental activities of daily living (IADLs) tasks, has decreased approximately 1% per year.5 According to the National Long Term Care Survey, for example, the cumulative effects over the 20 year period have been to decrease the rate of chronic disability in the older population from approximately 19.8% in 1984 to 15.9% in 1999,6 and this trend has been considered by policy makers and scientists alike to be quite substantial. Others surveys that do not focus on chronic disability (lasting three months or more) have found comparable declines in terms of percentages, although they report somewhat higher levels of disability prevalence (around 20% at the beginning of the 21st century, which we adopt here).
Although some have argued that the future holds promise for continued declines, others have pointed out countervailing factors that might offset future gains.13, 18 The debate about future trends (in the absence of widespread interventions) is relevant to a discussion of identifying high-impact interventions in that these impending changes make it challenging to sort out the appropriate comparison group. Disability interventions take time to implement and the full effect will only emerge as all birth cohorts are exposed to the intervention. Future cohorts of older people will look very different from those today, and while some of these impending changes are predictable (for example, education levels), others are quite uncertain (for example, activity levels). Moreover, interventions may be more or less effective for different population groups, so demographic trends will undoubtedly mingle with intervention effects.
Still, given the enormous attention paid to declines over the past decade of on average 1% per year, we contend that an intervention that results in an average annual decline of this size would be considered high-impact. Over the next 20 years, such an intervention or group of interventions, all else equal, could push the disability rate down from approximately 20% today to 16% in the year 2030. Here we provide some insights into the size of the target population and effect size that would be required to achieve such declines in both the short-term (one-year) and long-term (sustained for 20-year) time frame.
Short-run perspective. First, we calculate the relative risk and population size needed to generate a 1% decline in disability in a one-year period. Based on Census figures, mortality data from the National Center for Health Statistics (NCHS), and published estimates of late-life disability incidence, recovery, and mortality,45 we assume the following:
- 7.4 out of 35 million people ages 65+ have a disability at the beginning of year;
- 3.3 million new cases occur during the year among those without a disability;
- 0.3 out of 2 million new 65 year olds enter with a disability;
- 1.9 million people with disability at the beginning of the year recover by the end;
- Among people with disability at the beginning of the year 1.6 million die during the year, an additional 600,000 people without disability at the beginning of the year die during the year.
Under these circumstances, it would take approximately 175,000 fewer people ages 65 and older with disability to generate a 1% decline in disability (from 21% to 20.8%) in one year.
This target could be achieved a number of ways, including by decreasing incidence rates or increasing recovery rates. Table 1 illustrates for several scenarios the impact an intervention must have and how widespread the effect must be for a specific age group in order to reduce disability prevalence by this amount. For example, if the population ages 65-74 without disability (14.9 million people) had 0.90 the risk of developing disability (a 10% reduction in risk), 175,000 fewer people would develop disability during the year. Or, if half the population ages 65-74 without a disability (7.4 million) had 0.80 the risk of developing disability (a 20% reduction in risk), a similarly sized decline would occur. Alternatively, doubling the risks of recovering among 25% of those ages 75-84 with a disability (1.2 million people) would also achieve the reduction of 175,000 cases.
Long-term perspective. The short-run perspective does not take into account the fact that interventions may have effects well beyond a one-year period. To gain a sense of what a high-impact intervention might achieve in the long-term, we created a very simple simulation. The approach suggests what combinations of: (1) trajectory dynamics, (2) target population size, and (3) effects on disability and mortality, would be needed to sustain a 1% per year decline in disability. Using calculations based on the National Mortality Followback Survey, reweighted to represent a cohort of people ages 65 and older in 2000, we assign each trajectory, j, the expected values of both life expectancy (LEj) and disability-free life expectancy (DFLEj).
The simulation makes the following assumptions:
- When an individual reaches age 65, they will take one of four trajectories to the end of life.
- 22% of individuals will experience the Cancer trajectory with LE of 9.5 years and DFLE of 7.5 years (see Table 1).
- 16% will be in the Organ Failure trajectory (LE=15, DFLE=12).
- 46% of the cohort will experience the Frailty/Dementia trajectory (LE=22, DFLE=17).
- The remaining individuals will have a life expectancy of 11.5 years with 11 of them lived disability-free.
In a stable population, we can estimate the population prevalence of disability by dividing the expected years lived with a disability by the total expected years lived.
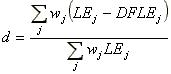 |
In the baseline scenario, average life expectancy at age 65 is 16.5 years, and the disability prevalence rate is 20.1%.
Our calculations suggest that a number of scenarios could move the disability rate from 20% to 16% in 20 years. We provide assumptions for three such illustrations in Table 2, and present results of the simulation in Table 3. One scenario would require interventions that would drastically reduce the expected years with a disability with no improvements in longevity for people with cancer and organ failure: from 2.0 to 0.5 for people with cancer and from 3.0 to 1.0 for people with organ failure. A less drastic, but still sizeable, compression would be required for interventions aimed at the frailty trajectory. That is, the disability rate would be reduced by 1% per year from an intervention that reduced the expected years with a disability from 5.0 to 3.6 but did not alter life expectancy among people in this trajectory. Similar reductions could be achieved by accelerating increases in years of active life--gaining four years over the next 20 years--thereby postponing the onset of all three trajectories.
Translating these figures into the type of information more readily (although not consistently) found in the literature, such as target population and effect sizes, is not straightforward. Each year of active life expectancy gained could represent infinite number of combinations of target population size and disability effect. For example, if 16.1 million older people are estimated to be following a course consistent with frailty/ dementia, a one year decrease in expected years with disability could involve an intervention that reduces disability by one year for all 16 million people, or by two years for 8 million (50%) people, or completely for 3.2 million (20%). Moreover, effect sizes are rarely if ever reported in terms of effect on remaining lifetime or years of disability over the remaining lifetime; and if they are, they are generally based on life table calculations drawn from age-specific incidence and recovery rates over a much shorter (generally one or two year) period. Such estimates of lifetime effects based on age-specific one-year incidence rates will be biased if the timing of the intervention in the trajectory course matters.
III. LITERATURE REVIEWS
A. Methodology
Selection of Illustrative Interventions
The project team called upon six external reviewers to rank 12 interventions (see Appendix for details). To focus the scope of this exercise, we purposefully limited our attention to interventions that were existing but not already widespread, had some published evidence demonstrating efficacy, and if implemented, could provide benefit within a few years (rather than waiting for decades or having most effect upon early or mid-life populations). We selected the following interventions from a list of 12 by tabulating rankings provided by external reviewers with input from the Office of the Assistant Secretary for Planning and Evaluation and project team members:
- Implement smoking cessation programs for the older population.
- Improve exercise. The literature review focuses on exercise interventions in frail but otherwise healthy older people.
- Implement good chronic disease care. To narrow this set of interventions, we focus on chronic disease care for a commonly disabling chronic condition: CHF.
- Implement depression screening, treatment, and follow-up.
- Implement fall prevention systems for frail elderly people.
- Modify homes and provide assistive devices. Because we expect interventions in the literature to combine home modifications and portable assistive technologies, we combine them here into one review.
- Implement widespread care planning for seriously ill.
Search Strategy
We focused our search on randomized trials so that to the extent possible, we could identify successful components for interventions. We also examined several important descriptive studies although, with regard to particular target populations, these studies cannot control for variables that may explain the underlying risk factors. We purposefully did not replicate previous systematic reviews of the literature, and relied on existing reviews from Cochrane and other sources where possible.
Relevant studies were located through a Search of MEDLINE, Ageline, Cochrane Library, EBM Reviews, CINAHL, and Psych Abstract using the Reed and Baxter approach.46 The search was limited to articles published in English since 1980. Search terms were limited to elderly samples and randomized controlled trials. The searches were conducted with a combination of keywords using the following terms: outcome assessment (health care), intervention studies, treatment outcome, AND one of the following terms: Smoking cessation; Exercise; Exercise therapy; Heart failure, congestive; Depression; Accidental falls/prevention and control; Self help devices; Assistive devices; Home modification; Advanced care planning; and Terminal care.
The abstracts for each of these publications were subsequently examined by two analysts to determine their applicability for review. Relevant studies were defined to be those that included any discussion of disability, although studies did not have to include disability as their main focus. Abstracts were included if they met the following criteria:
- Sample included only older adults 60 years and older.
- Methods included of some type of intervention.
- Sampling included use of a comparison/control group.
- The number of participants in the study groups was specified.
- Sufficient information was provided to determine a rate of difference in the outcome measure.
For each study meeting the inclusion criteria, the design, subjects, disability-related outcomes, and results were summarized in tabular form. Interventions were classified in terms of their dosage or the strength of the interventions. To facilitate comparisons, the effect sizes for continuous outcomes were calculated as the mean difference in the outcome of interest between treatment and control group and for dichotomous outcomes was calculated in terms of odds ratios.b Special attention was given to understanding the extent of adherence associated with each type of intervention, and to issues surrounding moving from efficacy associated with controlled clinical trial circumstances generally carried out with a homogeneous sample, to a widespread intervention with a more heterogeneous population.
B. Reviews
Implement Smoking Cessation
The U.S. Surgeon General, in a report on the health consequences of smoking, recently concluded that smoking harms nearly every organ of the body, causing many diseases and reducing the health of smokers in general and that quitting smoking has immediate as well as long-term benefits.47 The risk of disability onset is highest among current smokers, followed by former smokers, and then non-smokers;48 cumulative years of smoking appears to influence the risk of developing smoking-related disease and associated mortality. One study suggests current smokers have one and one half times the risk of non-smokers of reporting an activity limitation.49
Size of the target population. In 2002, 45.2 million adults (22.5%) in the United States were current smokers (25.2% of men and 20% of women), down from 24.1% in 1998. Compared to other age groups, the elderly population has a much lower rate of smoking--9.3% or 3.3 million smokers, compared to 28.5% among those aged 18-24.50
Nature of interventions. A total of 35 citations were reviewed, including four intervention studies that focused on older adults.51, 52, 53, 54 Interventions included counseling, clinician advice, buddy support programs, age-tailored self-help materials, telephone counseling, and nicotine replacement therapies. The interventions aimed at people ages 65 and older all involved combined intervention strategies. Follow-up ranged from one year to six years.
Efficacy. A comprehensive review for Centers for Medicare and Medicaid Services (CMS) indicates that in the general population individual, telephone, and group counseling, and pharmacotherapy are all effective in promoting smoking cessation, raising the odds of quitting by approximately 1.7.54 The Surgeon Generals 2000 report47 also evaluated a number of smoking prevention and cessation interventions aimed at the general population, including increasing the cost of cigarettes, increasing clean indoor air regulations, reducing treatment cost by providing insurance coverage, implementing telephone smoking quit-lines, offering treatment to smokers every time they are seen in health care systems, and implementing media campaigns to encourage smokers to quit. Pharmacologic treatment of nicotine addiction, combined with behavioral support, is estimated to enable 20%-25% of users to remain abstinent at one year post treatment. Less intense measures, such as physicians advising their patients to quit smoking, are estimated to produce cessation of 5%-10%.
Age does not appear to diminish the benefits of quitting smoking.55 Interventions that used a combined and comprehensive approach in late-life were able to achieve moderate increases in smoking cessation. For example, a preventive health care and group support intervention with older adults found quit rates were only slightly higher in the intervention group than in the control group (24.2% vs. 17.9%, P=0.09) over two years.52 Moreover, not all groups experience equal benefits. In a study of elderly patients ages 60-82 receiving nicotine dependence counseling and education over four years abstinence was more likely if patients were, for example, hospitalized at the time of the intervention and married to a non-smoker.51 Preliminary results from a CMS Medicare demonstration project56 suggest that a smoking cessation benefit (e.g., a quitline and reimbursement for nicotine replacement therapy) may increase quit rates by as much as three-fold at six months post treatment.
Existing studies have not explored whether individuals who receive the intervention experience reduced rates of disability.
Extent of adherence. Adherence in this literature was discussed primarily in terms of smoking cessation rates, rather than adherence to particular aspects of the intervention (e.g., support group attendance, adherence to pharmacologic protocols).
Generalizability. Most of the research has been done on populations under age 65. However, samples in at least two of the four RCT studies of the 65 and older population were drawn from Medicare beneficiary populations.
Stage in the disablement process/trajectory. Interventions have primarily been directed toward prevention of younger persons starting smoking and supporting adults who wish to stop smoking. The primary goal is to prevent disease from occurring. Disease consequences of smoking occur disproportionately among the elderly population, due to the long duration of cumulative injury. Excess mortality is most commonly due to cardiovascular disease and lung cancer.57
Improve Exercise
The scientific literature has established a positive link between physical activity (strength/resistance and aerobic exercise) and the prevention of sarcopenia (losses of muscular strength, muscle mass, quality, bone mineral density), declines in physical performance (strength, balance, flexibility, and mobility), decreases in maximal oxygen consumption (VO2max), prevention of diseases (e.g., coronary heart disease, hypertension, colon cancer, and diabetes), overall risk of falling, and decreased mortality.58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70 However, the proper quantity and quality of exercise necessary to increase physical fitness in the elderly population remains unclear.71, 72 Findings from the limited research on the impact of exercise on disability are, however, inconsistent.73, 74
Size of target population. Despite the well-known benefits of physical activity for older adults in improved well-being and the prevention or delay of disease, as many as 70% of people ages 50 years old or older remain under-active.75, 76 Thirty-three percent of men and 50% of women age 75 or older engage in no leisure time physical activity. Rates also vary by race, with African Americans less active on average than Whites.77
Nature of interventions. Over 140 articles were reviewed. Approximately 62 RCTs were reviewed with the rest of the literature comprised of observational studies or reviews of the literature. The majority of interventions involved aerobic exercise alone or compared against resistance training, strength or endurance training, and quadriceps training, though the operationalization of these terms varied greatly. Other interventions included: walking, cardiac rehabilitation, electrical stimulation of muscles, electro-acupuncture, drug interventions, etc.
The description of randomization also varied from explicit to implied, making comparisons across studies difficult. Comparison/control groups varied widely across the literature; with some groups receiving a portion of the intervention, an alternative intervention (e.g., strength vs. endurance training), or no intervention, but there was no systematic pattern. Almost all of the studies compared baseline performance among groups to post outcome measures. Most studies were small and had small samples or short follow-up periods (ranging from six weeks to two years). One study on prevention and health promotion in the elderly population (that included exercise as part of the intervention), followed subjects for eight years, but this study was a notable exception.
Outcomes included measures of physical performance (e.g., exercise capacity/ tolerance, mobility, muscle strength, endurance, functional capacity, ADL/IADL disability, pain, sensory limitations, cardiovascular endurance (e.g., VO2max, heart rate, etc.), walking velocity, gait, ambulation, weight-bearing ability, range of motion, and days of restricted activity. Psycho-social outcomes focused on measures of psychological well-being, quality of life, and depression. Many exercise interventions were aimed at individuals with specific diseases (e.g., OA or rheumatoid arthritis; Parkinsons disease, CHF, COPD, diabetes, Alzheimers disease, post femoral fracture) or with specific symptoms (e.g., pain; back pain, limited of movement) and thus did not include representative sample populations.
Efficacy. The preponderance of the literature suggests that both aerobic and strength/resistance training offer a wide range of benefits to older adults.78, 79, 80, 81, 82, 83, 84, 85, 86, 87, 88, 89 Hurley and Rother58 found strength gains of greater than 30% and muscle mass increases of 12% after two months of heavy resistance training in 65-75 year olds. Lemura and colleagues71 examined studies (n=27) of physical training on functional capacity in older adults (ages 46-90) years and found a significant difference in functional capacity between studies of exercise intensity > to 80% of VO2max compared to those with training intensities of 60-75% of VO2max (p0.001) and exercise duration. (Exercise of >30 minutes duration produced significantly greater improvement in VO2max vs. less than 30 minutes, p0.002). Lazowski and Ecclestone90 in a meta-analysis of 16 RCTs of physical training on performance in institutionalized adults 70 years of age or older found physical training improved muscle strength, mobility, gait speed, balance, wheelchair propulsion, ADL function, endurance, and range of motion. The meta-review found no RCT showing any negative results from physical training; however, ADL improvement in one study reviewed was only for the most dysfunctional subjects. Range of motion training did not prevent functional decline in institutionalized elderly people.91
The effects of exercise interventions on disability were inconsistent. In a review of 41 RCTs, Latham and colleagues found that progressive resistance training moderately increased walking speed but had no effect on physical disability.73 Chin and colleagues in an exercise intervention in 157 independently living frail elderly people (mean age: 78.7 years), found performance and fitness were significantly enhanced (+8% in exercise vs. -8% in controls; difference in change: 1.9 points, p0.001; +3% vs. -2%; difference in change: 0.9 points, p=0.05) but no effects on disability were observed.82 In contrast, Binder and colleagues found moderate short-term improvements on physical function and pre-clinical disability in 115 elderly frail men and women (1.0-5.0 points; 0.9-3.6 mL/kg/min for VO2 peak; 1.6-4.9 points for FSQ; 95% CI).79 Kahana and colleagues found that exercise was predictive of fewer IADL limitations and greater longevity, positive affect, and meaning over an eight year follow-up.92 Keysor and Jette,93 in a review of the literature on the degree to which exercise enhances physical function and/or improves disability in late-life, found small to moderate positive effects on physical disability in 35% (five of 14 studies) of the studies reviewed (range of effect size: 0.26-0.58) though three of the studies were with people with OA and three included samples of elderly people living in residential nursing care who had functional limitations or disabilities. One study showed a large positive effect of exercise on physical disability only for those members of the sample stratified into a high disability group.
Penninx and colleagues81 found that exercise prevented incident ADL disability in 250 subjects with knee OA (relative risks=0.60; 95% CI 0.38-0.97; P=0.04 for resistance and 0.53; 95% CI 0.33-0.85; P=0.009 for aerobic exercise). Cumulative ADL incidence was 37% in exercise group versus 53% in controls (P=0.02). After adjustment for demographics and baseline physical function, the relative risk of incident ADL disability for assignment to exercise was 0.57 (95% CI 0.38-0.85; P=0.006). Both exercise programs prevented ADL disability; the relative risks were 0.06 (95% CI 0.38-0.97; P=0.04) for resistance exercise and 0.53 (95% CI 0.33-0.85; P=0.009) for aerobic exercise. The lowest ADL risks were found for participants with the highest adherence to the exercise regimen. Though it is unclear whether exercise prevents or minimizes physical disability, a number of prospective studies show a protective effect from exercise; that is, people who were physically active (at least two X/week) were less likely to develop ADL disability.94, 95, 96, 97, 98
Finally, a preventive home-based physical therapy program (including progressive balance and conditioning exercises) produced modest but consistent effects on functional decline among physically frail older persons.99, 100 However, the authors discuss the difficulty that older frail subjects had in advancing to more intense training levels.101
Extent of adherence. Adherence in this literature was discussed primarily in terms of completion of the trial and, when reported, ranged from 60%-90% completion of exercise interventions. However, in one long-term study, adherence to exercise regimens after two years was substantially lower.102 Other research has indicated that an enhancement of motivation and a reduction in the burden on subjects are necessary for improving individual adherence to an exercise program.103, 104, 105
Generalizability. Exercise interventions focused mostly on healthy patients as well as patients with neck or low back pain, OA and rheumatoid arthritis. Some research reviewed focused on patients with myocardial infarction, hip fracture/post falls, stroke, Alzheimers disease, CHF, COPD, and has included sedentary and functionally impaired individuals. Many studies used convenience samples of asymptomatic older adults, limiting the generalizability of the results.
Samples ranged from individuals in their 20s to their 90s, with many interventions focusing on the elderly population (65+) and the very old (70-90 years of age). There is little evidence on the impact among ethnic, socioeconomic, and chronic disease subgroups.
The RCTs and observational studies were well designed and used analytical techniques to account for many biases, such as loss to follow-up and adherence with exercise protocol and completion rates. However, many studies, including the RCTs, were unable to assess (and therefore control for) differences between treatment and control groups in the level of physical inactivity at baseline.
Stage in the disablement process/trajectory. Exercise interventions focused on primary and secondary prevention and were thus aimed at the full range of elderly individuals: the healthy elderly, individuals in the early stages of the chronic illness trajectories (e.g., knee OA with limited range of movement), older people with a condition and some disability (e.g., CAD with two disabilities), and a few interventions were targeted to those of very old age (70+) as well as on later stage trajectory populations (e.g., late stage cardiac patients, COPD patients, Alzheimers patients, or nursing home patients).
Implement Good Chronic Disease Care for Congestive Heart Failure
CHF is a fundamentally progressive and highly lethal, disabling condition and is the only major cardiovascular disease with increasing incidence and prevalence, especially in the over 65 population. CHF is the leading cause of hospitalization and death in adults older than 65.106, 107, 108 More than half of inpatients older than 65 with CHF are readmitted within 3-6 months of hospital discharge.109, 110 Despite treatment advances, heart failure has a significant mortality rate, causing more than 52,000 deaths annually.106 Data suggest that approximately 20%-25% of heart failure patients die within one year after diagnosis, one-third of patients die within two years, more than half of patients die within five years.111, 112, 113, 114, 115 Women survive longer than men, but fewer than 15% of women survive more than 8-12 years after diagnosis.112 Heart failure has been found to have the greatest impact on patient quality of life. Wolinsky and colleagues114 found that having been hospitalized for CHF was consistently associated with greater increases in the number of functional limitations (basic ADLs, household ADLs, advanced ADLs, lower body limits, and upper body limits).
Size of target population. Improvements in survival after myocardial infarction, better management of diabetes and hypertension, and an increase in the aging population have contributed to the rise in CHF. More than five million Americans currently have a diagnosis of CHF and 550,000 new cases are diagnosed each year.106 Approximately 1% of persons aged 50-59 have CHF compared with 2%-7% of those aged 70-74 and 10% of persons 75 years or older.116 One postmortem examination study found prevalence rates as high as 18%-25% in the elderly population.117 As more patients survive myocardial infarctions, as treatments continue to improve for CHF, and as the Baby Boom generation ages, the number of patients who have CHF is expected to grow.
Nature of interventions. Approximately 75 studies, discussion papers, and meta-analyses of RCTs and cohort studies were evaluated (1985-2004). Most studies were published between 1990 and 2001. Sample sizes ranged from less than 20 to 11,942 (this range included a number of large meta-analyses), with the usual number of participants around 100-200. Baseline clinical characteristics of patients in treatment and control groups were usually well matched. Outcomes focused on readmission rates and length of stay (hospitalizations or emergency room visits); angiotensin converting enzyme inhibitor (ACEI) use at follow-up, all cause mortality, heart failure related mortality, costs, provider adherence to evidence-based medical management guidelines, patient adherence with treatment and medication regimens, quality of life, mortality/survival. Disability was evaluated primarily as a component of quality of life and not explicitly assessed in most of the trials reviewed.
Three general types of interventions for CHF patients were reported in the literature reviewed: drug interventions, exercise interventions, and disease management interventions; roughly equivalent to the primary, secondary, and tertiary prevention approach of public-health and medicine. Disease management programs (secondary prevention) were the largest category of intervention studied, but the actual programs varied most widely and fall on a continuum from secondary to tertiary prevention rather than into discrete categories. It was hard to distinguish many programs labeled disease management from those labeled multidisciplinary care management. Outcome measures included reduction of exacerbations and utilization (ER, hospital), improved quality of life, mortality, readmission rates, and symptoms. Follow-up ranged from three months to 2-3 years.
Efficacy. Numerous studies have examined the efficacy of specific drug therapies in CHF patients118, 119, 120 while other studies examined the efficacy of home inotropic therapy in advanced heart failure.121 Overall, most heart failure medications have been shown to alleviate symptoms, improve clinical status, and reduce mortality among CHF patients, with a clear dose-response effect. Only very elderly or very advanced patients were found to benefit less or experience serious complications and side effects from different CHF medications.122, 123 However, physician adherence to recommended medication prescribing guidelines remains poor.
Exercise interventions for rehabilitation of patients with heart disease generally found positive results in exercise tolerance, performance, and balance without adverse effects and with less fatigue.124, 125, 126, 127 However, most of these studies were based on samples of young and middle-aged males (45-65 years of age). Exercise trials in the very old CHF population are limited and adherence to exercise in the elderly population is low.
Disease management interventions differed widely on intensity (e.g., number of program components) and length of intervention (short-term vs. long-term). Interventions ranged from single component (e.g., the provision of written educational materials or telephone monitoring) to multi-component programs (e.g., a registered nurse led cardiac rehabilitation clinics and more comprehensive case management interventions marshalling multi-disciplinary health and social service management with allied health professionals included in the team). A number of reviews109, 128, 129, 130, 131 as well as reports of individual programs have been conducted on differing disease management interventions.132, 133, 134, 135, 136, 137, 138, 139, 140, 141 Overall, multi-component interventions achieved greater reductions in utilization and improvements in quality of life than single component interventions.
For example, an analysis of the literature by Rich found that an average 61% reduction in hospitalizations (range: 14%-87% and an average 85% reduction in hospital days, range: 22%-92%) and improved quality of life, functional capacity, patient satisfaction, enhanced exercise tolerance, aerobic capacity, capacity to perform routine daily activities, improved patient adherence with diet and medications, patient satisfaction, and lower overall costs of care for patients in multi-component interventions.142 Similarly, Ahmed found a 13% lower risk of hospitalization (summary RR 0.87; 95% CI 0.79-0.96; heterogeneity among studies, P=0.003) in multi-component specialized heart failure disease management and multi-disciplinary home management (summary RR 0.77; 95% CI 0.68-0.86; heterogeneity, P>0.50). Single interventions (telephone follow-up by a primary care physician) showed no effect. There was no association between the interventions and mortality.128 Phillips et al. found a 25% relative reduction in the risk of readmission (RR 0.64; 95% CI 0.32-1.28; X2/3=18.43; heterogeneity0.001, n=4 studies), a trend toward a 13% relative reduction in all cause mortality (RR 0.87; 95% CI 0.73-1.03; X2/13=17.79, heterogeneity=0.06, n=14 studies), and improved quality of life (P=0.01) but no difference in ACEI use at follow-up or length of stay for comprehensive post-discharge interventions.109
Overall, comprehensive, multi-component interventions achieved significant reductions in utilization, ranging from 50% to 85%, with somewhat uniform positive impact on improved quality of care, patient management, and improved quality of life, depending upon the comprehensiveness of the interventions employed. Reductions in disability and impact on mortality have yet to be demonstrated. The impact of these interventions in the most advanced stage illness populations also remains to be demonstrated.
Extent of adherence. CHF readmissions are suggested to reflect poor clinical management (a lack of familiarity or adherence to established protocols/guidelines), sub-optimal assessment of readiness for discharge, a breakdown in communication and information transfer between hospital-based and community physicians, inadequate post-discharge care and follow-up, or some combination of these processes.143, 144 RCTs of physician prescribing practices for CHF have shown that younger physicians are more likely than older physicians to select agents consistent with guideline recommendations and that physicians in general did not follow guidelines when initiating treatment in black patients, older patients, and those with mild renal failure. A number of interventions to increase physician adherence have shown mixed results.145
Although adherence to a drug, exercise, and symptom recognition regimens have repeatedly shown a positive impact on patient quality of life and utilization, patient adherence is poor. Poor patient adherence has been attributed to factors such as lack of understanding of the treatment plan; poor understanding of the disease, its prognosis and course, and how to manage their symptoms at home; lack of motivation or lack of conviction about treatment; inability to follow the treatment plan due to memory problems; depression; or financial or other constraints.146, 147, 148, 149, 150 It is unclear how much of this non-adherence is due fragmentation in the medical system and poor management by physicians and how much is due to individual factors.
Generalizability. The extensive RCT literature on drug, exercise, and disease management interventions for CHF patients are consistently positive for comprehensive, multi-component interventions. While the early research (1990s) focused primarily on heterogeneous samples of 55-65 year old men with CHF with no co-morbidities (especially the drug intervention literature), recent studies have become more representative, incorporating a wide range of CHF stage patients (e.g., NYHA Class III and IV), age (50-80 years old), and diverse ethnic groups. The major current limitation in the literature is in relation to the very old (80+) and women, both groups not yet systematically included in the trials.
Stage in the disablement process/trajectory. Most interventions targeted the mid-stage of the CHF trajectory with secondary and tertiary prevention programs aimed at minimizing the impact of the disease and managing symptoms (mid to late stage on the trajectory).
Implement Depression Screening, Treatment, and Follow-up
Depressive disorders in the older population are common, chronic, and costly. The World Health Organization identified major depression as the fourth leading cause of worldwide disease, causing more disability than either heart disease or cerebrovascular disease. The diagnosis of depression is significantly associated with an older adults transition into disability status as well as the presence of stable functional disability.
Depressive symptoms have been shown to predict both onset of impairments in mobility and functioning, and declines in physical health in the older population.151 Depressive symptoms also have an interactive effect with physical functioning in old age, compounding associated disability.152 Despite its high prevalence in primary care and its substantial economic impact, depression often goes unrecognized in older adults seen in primary care settings and under-treated in older adults referred to the mental health system.153 One cause is primary health care providers' failure to recognize symptoms,154 which can present or be described differently in older patients,155 or be seen as side effects of medical illness or part of the aging process.156 However, even when major depression is diagnosed, it often remains under-treated or wrongly treated (e.g., with benzodiazepines, or not long enough).157, 158, 159
Several risk factors common in the older population seem particularly amenable to community-level screening prevention programs: a prior history of depression, complicated bereavement (multiple losses), and the presence of vascular disease. There are currently no population-based screening programs to identify late-life depression.
Size of target population. Epidemiological studies suggest that the prevalence of major depression in the community-based older population is between 1% and 3%.160 This has led to speculation that depression declines in old age,161, 162 but this point is arguable.162 Most studies find much greater non-response rates among people with health or cognitive problems,157, 163 which are important risk factors in this population. Major depression occurs in up to 25% of older people with co-morbid conditions such as ischemic heart disease, stroke, cancer, chronic lung disease, arthritis, and Parkinson's disease.164 Major depression is also very common in other important subpopulations commonly excluded from epidemiological studies, such as nursing home residents.165 One study (using self-report, not diagnostic interview) found an 8.7% community prevalence of DSM-IV criteria for Major Depression.160 Additional disabling depressive illnesses include dysthymia and minor depression. Studies using age-specific instruments or not using strict DSM or ICD cut-off scores find a high rate of disabling depressive symptoms in older people. For example, a large community-based study, using the Centre for Epidemiological Studies Depression Scale,157 found the prevalence of major depression to be 2.02%, but 12.9% had "minor depression," and a further 14.9% had significant depressive symptoms indicative of dysthymia.
The National Institute of Mental Health (NIMH) estimates that of the 33 million Americans currently over the age of 65, approximately six million (18%) experience depressive symptoms, which can include persistent sadness, sleeplessness and changes in body weight. The NIMH also estimates that only 10% of the elderly people with depression ever receive appropriate treatment for this illness. In older adults, depression is associated with high levels of chronicity and high relapse rates.164
In the older population with vascular disease, the neurovegetative symptoms of depression were often attributed to the side effects of their illness rather than investigated as evidence of depression.156 For example, post-stroke depression is common, with prevalence estimates of 10%-64%.166 One study reported a 23% one-year prevalence of post-stroke major depression, and 18% for minor depression.167 Vascular disease, or even risk of vascular disease in the absence of stroke, is also a major risk factor for late-onset depression. Patients with late-onset depression were significantly more likely than younger subjects to have two or more risk factors for vascular disease.168 The term "vascular depression" was proposed, emphasizing the fact that depression is not necessarily a unitary syndrome.
Nature of interventions. We identified 19 RCTs examining the effectiveness of screening for depression in older an adults. In eight studies, the only intervention was screening for depression in primary care settings. Integrated programs included feedback to providers and/or patient education, access to case management and/or mental health care, and telephone follow-up. The trials reported various outcomes including recognition of depression, rates of treatment and clinical improvements among patients with depression.
Treatments for major depression include antidepressent medications for major depression, including tricyclic antidepressants (TCAs) and selective serotonin reuptake inhibitors (SSRIs), psycho-social and psycho-therapeutic interventions, and combinations.
Efficacy.
Screening. In seven trials, routine depression screening with feedback of screening results to providers generally increased recognition of depression especially major depression, by a factor of 2-3 compared with usual care. Eleven trials measured the effect of screening and feedback on the receipt of treatment from one month to two years after the interventions. The results of these studies showed mixed results: in four fair to good quality trials that used feedback only, there was no significant effect on treatment rates, but five of the seven trials that combined feedback with treatment advice or other system supports reported large increases in treatment rates (e.g., 15% for usual care vs. 70% among those combining feedback and advice) in the intervention groups compared with usual care. Outcomes improved significantly in several of the studies when the screening and management programs were integrated into usual (primary) care. The combined screening/treatment groups resulted in a small but significant reduction (effect size=-0.041) in depression symptoms. These trials suggest that the benefits from screening are unlikely to be realized unless support systems in the primary care and mental health settings are functioning well.
Many tools that screen for depression in older adults are available, but there was little evidence to recommend one over another. Most have relative good sensitivity (80%-90%) but only fair specificity (70%-80%). Most screening instruments are easy to use and can be administered in less than five minutes. Shorter screening tests, including simply asking questions about depressed mood and anhedonia, appear to detect the majority of incident cases of depression in older adults and sometimes performed better than the original, more complex instrument.
Treatment. Antidepressent medications for major depression, including TCAs and SSRIs were clearly more effective than placebos in the Cochrane studies reviewed. Depressed older adults report a 60-80% response rate to pharmacotherapy. Psycho-social and psycho-therapeutic interventions were also shown to be as effective as antidepressant medications for major depression, but they are also more time intensive and costly. The benefit of psycho-therapy on other depressive illnesses was less well-studied.
Two randomized control studies of combined psycho-therapy and medication (nortriptylene) involving older people demonstrated a beneficial effect compared to placebo and medication clinic visits.164, 169 One study demonstrated a significant reduction in recurrence of a major depressive episode from 90% among placebo group to 20% among treatment group (relative risk of 0.22). The other study demonstrated significantly different remission rates from a major episode following bereavement due to the death of a spouse (69% with treatment, 45% with placebo, relative risk 1.5). Similarly sized results were found in a review of 16 clinical trials, with 932 adult patients randomized to pharmacotherapy alone and 910 to combined treatment (OR=1.86; 95% CI=1.38, 2.52) for combined therapy versus medication alone).170 Others have suggested that with adequate screening and treatment, the rate of recovery and relapse for many older people with depression is estimated to be the same as in younger cohorts.158
Studies focusing on functional outcomes typically had small samples with small improvements after treatment or remission, usually in IADLs or in cognitive functioning.171, 172, 173, 174 Recently, Callahan and colleagues172 found moderate improvements in physical functioning (change of 1.71 on the 12-item physical component summary and -0.15 on an IADL scale) among patients randomized to receive treatment from a depression clinical specialist coordinating with the primary care physician.
Extent of adherence. Having depression is a risk for non-adherence with medical treatment recommendations.170, 175 In trials with older patients 18%-22% refused treatment, were non-compliant, or left the study for medical reasons.164, 169 A comprehensive review of studies with adult patients in 16 studies suggested combined non-response and dropout rates for medication only were on average 46% (ranging from 0%-71%) and for medication and therapy were on average 36% (range: 11%-55%).170
Generalizability. Sample selectivity and non-random sample attrition is one common but rarely addressed threat to the generalizability of the findings from the RCT literature. The existing literature suggests that screening tests perform well in cognitively intact elders but the issue of cognitive impairment was not addressed. Rates of depression are also higher among older adults that do not participate in screening such as those with common co-morbid conditions (e.g., diabetes and arthritis). Moreover, subjects in the reviewed RCTs were often homogenous with regards to race and ethnicity.
Stage in the disablement process/trajectory. Depression screening interventions are targeted early in the disablement process during the early pathology stage. Depression in the older adult population has been characterized as following a chronic relapsing course, with slow recovery and increasingly brief periods between episodes.176 Untreated depression in later life is a risk factor for other negative events such as excess physical and social disability, exacerbation of co-existing illness, and earlier death. Therefore, primary prevention through screening and treatment early in the illness trajectory has been identified as a potentially effective intervention strategy.
Implement Fall Prevention Systems for Frail Elderly People
As a leading cause of functional impairment and disability, the subject of falls has received growing attention among clinicians and researchers who have identified many diverse risk factors for falls. The nature of falling is multi-factor that is, there is not a single cause for falls but rather a combination of multiple risk factors that put an older adult at risk for falling.177, 178, 179, 180, 181, 182 The risk for fall related disability is due to the high rate of sustained physical injury and fear resulting from a serious fall.
Size of target population. The target population for a fall prevention intervention focuses on those individuals that without intervention would go on to fall and receive an injury in a given year. It is estimated that one-third of adults ages 65 years and older fall each year.183, 184, 185 For older adults residing in long-term care settings the risk of falling approaches 50%.186, 187 Of those who fall, 20%-30% suffer severe injuries such as hip fractures or head traumas that increase disability and the risk of premature death.188, 189 Another 3%-5% of older adult falls cause fractures of the vertebrae, forearm, leg, ankle, pelvis, upper arm, and hand.190, 191, 192
Of all adverse fall-related outcomes, hip fractures cause the greatest number of deaths and leads to the most resulting disability.193, 194 Most patients with hip fractures are hospitalized for about one week195 and 25% of community-dwelling older adults who sustain hip fractures remain institutionalized for at least a year.196
Nature of interventions. Approximately 82 studies (76 RCTs and six quasi or non-RCT) were reviewed. Seven papers were excluded because they were descriptions of earlier studies published by the same research group and added no new information. Most studies were published between 2000 and 2003. About 70% were carried out in the United States. Most studies contained between 100 and 200 participants and were conducted over 3-12 months. The primary outcome measures were: (1) fall rate, (2) injury rate from fall, and (3) performance on balance tests. The qualifying literature fell into two themes: (1) single interventions versus no intervention, and (2) multi-component interventions versus no intervention.
Single intervention versus no intervention. Each of the 56 single comparison studies used a comparison group for which no intervention took place. The most common single intervention tested was exercise (23 studies). Studies focusing on single interventions provided conflicting evidence on the reduction of fall rates or improvement in function.91, 190, 191, 192, 197 Indeed, the American Geriatrics Society Fall Prevention Panel observed that while a single intervention focused on one risk factor could be the most cost effective way to reduce falls, there is little evidence in the literature to support this practice.
Multi-component intervention versus no interventions. The strongest results were found in the 26 studies that included a broad range of multi-component interventions. Multi-factor interventions that involve a comprehensive fall assessment and an individualized management program seem to be the most promising approach. Absolute changes after these interventions in the reduction of fall risk varied between 0.29 and 0.36.198 Unfortunately, the literature to date provides no definitive guidance on the specific components of multi-factor interventions or on whether the benefits of such interventions justify costs of an intervention. Effective interventions in the reviewed studies often combined different measures of health and environment and diverse intervention strategies, and most were not designed in a way to determine which components of a multi-factor intervention would be most effective.199, 200, 201, 202
Efficacy. The effect of a multi-factor interventions on fall rates was based on the relative risk reductions or odds ratios reported in the reviewed studies for evidence of effectiveness. We only used those effect size findings reported in systematic reviews193, 203, 204, 205, 206, 207 and did not perform additional analysis (e.g., meta-analysis). The effectiveness of the interventions in these reviews varied widely, with the average efficacy of the intervention on preventing falls in the range of 20%-30% (Peto OR 0.77; 95% CI 0.64-0.91). Few studies reported systematic long-term follow-up. The longest duration of follow-up was conducted by Tinetti and colleagues.199 The investigators reported that interventions to reduce five specific risk factors resulted in a 30% reduction in fall risk over one year in a prospective community cohort. The targeted risk factors were postural hypotension, use of any benzodiazepine or sedative-hypnotic medication, use four or more medications, presence of environmental hazards, muscular strength or range of motion impairments.
Extent of adherence. No estimates of adherence with protocol were reported.
Generalizability Because many of the reviewed studies used small sample sizes and inadequately described the precise number and standardization of interventions, their generalizability and reproducibility is limited.
Stage in the disablement process/trajectory. Fall prevention interventions are targeted early in the impairment pathway, when an older adult is identified as a fall risk. Fall prevention interventions are not typically aimed at particular diseases but rather are targeted to individuals with a predisposition to frailty or in the early stages of frailty.
Modify Homes and Provide Assistive Devices
Home modifications and the use of assistive technologies such as ramps, shower seats, wheelchairs, walkers, and the like, offer one way for older adults to cope with age-related limitations in activity. Recent increases in the use of assistive devices in the older population with disabilities have been noted.6, 208
Size of target population. According to NCHS, 38% of community residing adults over age 65 have some limitation in functioning caused by chronic conditions. The functional problem most commonly reported is difficulty climbing up and down stairs (35%). The other most frequently reported problems include difficulty walking, getting outside, and bathing.
National estimates from the Asset and Health Dynamics Among the Oldest Old study suggest that 40% of the older population have modified their homes by installing items such as grab bars and shower seats, railings, ramps, modification for wheelchairs, and call devices. The proportion of households that reported some home modification was 34% among those age 70-79, 47% among those 80-89, and 60% among those over age 90.209
Nature of interventions. We identified 17 studies that met the inclusion criteria for this review and included seven RCTs, ten descriptive studies. Most studies were published between 1999 and 2002 and were carried out in the United States. The sample size averaged 40 subjects (range 9-249). The primary outcome measures were assistive technology adherence and functional performance over time.
The most commonly tested assistive device in the RCTs was wheelchair seat cushions. Seat cushions can significantly affect sitting balance during reaching tasks as well as prevent sitting acquired pressure ulcers.210, 211, 212 The most common types of home modifications were related to bathing, for example, grab bars and seats in the tub or shower area. These home modifications account for 27% of homes among those age 70 and over. The second most common home modification was wheelchair access. Approximately 12% of older adults have homes modified for indoor wheelchair use. Call buttons and railings are the third most common modification, accounting for 10% of home modifications among the older population.
Intervention efficacy. Data from the RCTs were not sufficiently similar to allow for the combination of data by statistical analyses.213 However analysis of national survey data using household production function model estimated that the use of home modification in bathing, such as the installation of grab bars and shower seats significantly increased bathing functioning. The size of the effect was estimated to be equal the functionality that is lost when an 80 year old loses when they age into their 90s.214 Assistive device was estimated to add twice as much bathing functionality when compared to home modification, such that an 80 year old could gain more functionality through assistive devices than is lost through sever stroke.214
Only one RTC of high methodological quality noted significant differences in disability rates resulting from assistive device use and home modification. In this study, the control group demonstrated a 2.7%-13% greater decline in functioning than the treatment group receiving assistive devices and home modifications. These results translated into the control group requiring 2-4 minutes of additional assistance with ADLs than the treatment group.215
Extent of adherence. One important issue addressed in the literature was how and whether or not assistive technology was used when it was prescribed. Functional improvements (at follow-up) corresponded with device nonuse. Because of the high rate of non-adherence with assistive technology use (29.3%-45%),216 the primary emphasis among the descriptive studies was on factors associated with use and substitution for personal care. Although third party payers cover relatively few assistive devices and home modification interventions, there was little evidence to suggest the financial resources increased the rate of adherence. The most frequent reason given for nonuse was that the device was no longer needed. Moreover, older adults in these studies often reported not liking to use devices or not knowing how to use them properly. Attitudes towards social acceptability typically affected the rate of adherence.
Generalizability. Small samples sizes (50) in a majority of these studies limits the generalizability of the findings. Samples were also not representative of the general older population.
Stage in the disablement process/trajectory. The chronic health conditions commonly associated with the frailty trajectory such as stroke, arthritis, and dementia all reduce functional abilities such as ambulating and bathing, with severe stroke having the strongest impact.214 Thus, interventions that include assistive device use and home modifications are typically aimed at the later stages of the frailty trajectory, after the onset of functional limitation. Individuals with advanced cancer and lung disease also have high rates of functional disability. Therefore, these interventions may be viewed as appropriate for individuals at the later stages of the cancer and organ failure trajectories
Implement Widespread Care Planning for Seriously Ill
Advance care planning (ACP) is a holistic, palliative approach to decision-making, involving a process of thinking ahead to treatment choices.217 In addition, ACP encompasses implementing specific steps to make it easier to comply with the preferences of the patient and family. Sometimes legal documents called advanced directives (ADs), are included that state specific instructions for care (e.g., circumstances in which life sustaining treatment is to be provided or forgone) or that name a proxy/surrogate decision-maker (e.g., durable power of attorney).
Size of the target population. Approximately two million individuals die in the United States each year, 80%-85% of which are 65 years or older and covered by Medicare (representing 4.7% of Medicare beneficiaries).218 NCHS vital statistics data show that heart disease and cancer are the leading causes of death in the elderly population, accounting for more than half of deaths in 1997. A random sample of all deaths in the United States revealed that about 9% of decedents had issued an AD at the time of their death.219 Estimates on current AD completion rates nationally hover around 15%-20%.220
Nature of interventions. Fifty articles from the literature (1992-2004) on ADs and advanced care planning were reviewed. Eleven articles were discarded as not applicable or with insufficient information. The 39 remaining studies included 22 RCTs, 13 observational studies, and four literature reviews.
Most interventions involved education activities (either single or combined) designed to increase awareness of specific components of ADs (e.g., durable power of attorney/health care proxy, DNR, CPR, acceptance or rejection of ventilation), completion rates, and documentation in the patients medical record. Single interventions included educational materials, AD discussion guides for providers, and providing a uniform place for the AD in the medical record.221 Multi-component interventions combined a variety of single approaches together. Follow-up was usually short, from weeks to months, with few studies conducting follow-up beyond a year. Specific information on comparison groups and details on complex interventions were often missing from the abstracts. Samples, other than in the SUPPORT study, were small and non-representative (e.g., ambulatory care clinic patients, nursing home patients, CHF/COPD patients).
Efficacy. Results from the intervention studies were mixed. Most studies that used a single educational intervention component had little or no impact on AD completion rates or subsequent medical care.222 Interventions that used a combined method were able to achieve a moderate increases in AD completion rates, ranging between an increase of 10%-20%. One study identified a completion rate of 33% in an HMO, but only 15% of patients who had an AD had discussed it with their physician.223
A review of the literature by the Agency for Healthcare Research and Quality found that ADs were not effective in influencing end of life care not only because of low rates of completion but because the language in ADs was usually too non-specific and general to provide clear instruction.224 An exception in the literature was a retrospective analysis of 540 decedents, which found that a comprehensive, community-wide AD intervention had positively affected the prevalence of documented ADs, showing an increased completion rate from 15% in 1991 to 85% in 1998.217, 221, 225
Extent of adherence. Adherence in this literature was discussed primarily in terms of completion rates of an AD. Overall, interventions produced small to moderate effects on completion rates (10%-20%).
Generalizability. Most of the studies conducted on improving completion of an AD are not RCTs but rather observational or descriptive studies, using small, non-representative samples (e.g., ambulatory care clinic patients) and comparing outcomes only on completion rates and documentation. Generalizability is thus limited due to sample selectivity and homogeneity with samples, small sample size, and low rates of adherence.
Stage in the disablement process/trajectory. Interventions to implement advanced care planning have primarily focused on the ill elderly population (65 or older) and those in the very late stages of serious, life threatening illness.
IV. COMPARISONS BASED ON CONCEPTUAL FRAMEWORK AND LITERATURE REVIEW
With the framework we have outlined and the literature we have reviewed, we can begin to compare alternative interventions. We first focus on the short-run (one-year time frame), quantifying comparisons where possible. We then discuss longer-run comparative effects. Recognizing that longer-run effects could not be easily quantified based on the literature, we instead demonstrate some basic principles about the likely effects of types of interventions using a simple simulation model. Comparisons are summarized in Table 4.
A. Comparison of Short-Term Effects
Three key pieces of information are needed to compare short-term effects of interventions: (1) the size of the population with the targeted risk factor; (2) the short-term risk of disability associated with the presence of the targeted risk factor; and (3) the effectiveness of the specific intervention in remedying/reducing the risk factor. The latter is a combination of the interventions efficacy, adherence rates, and important differences between study populations and a population-based target population.
Size of Target Population with Risk Factor
The seven interventions we reviewed vary widely in terms of the size of the target population. Those interventions aimed at the largest populations, all else equal, will have the greatest effect on disability rates. Three interventions may be aimed at a large target population: exercise, fall prevention, and depression screening and treatment; three other interventions--smoking cessation, management of CHF, and advanced care planning--target a substantially smaller population. Depending on how the target population is defined, assistive technology/home modifications fall somewhere in between.
The three interventions that stand out as potentially reaching a large target population--exercise, fall prevention, and depression screening and treatment--could reach between 10 and 18 million people. Of the 35 million people ages 65 and older, 51%, or about 18 million people, report having no physical activity according to Healthy People 2010.226 About a third of people age 65 or older, or nearly 12 million people, fall annually. It has been estimated that nearly 30% of Americans age 65 or older, more than 10 million persons, have some depressive symptoms, with 2% (707,000) having major depression, about 13% (4.5 million) having minor depression, and the remaining 15% (5.2 million) with significant depressive symptoms.
It is less straightforward to identify the target population for assistive technology and home modifications. Perhaps the population with functional limitations is the most relevant target population for an intervention increasing knowledge of and extent of assistive technology and home modifications because they have the ability to reduce or delay onset of dependence. National estimates indicate that 13-17 millionc community residing adults age 65 or older have some limitation in functioning, most commonly walking, followed by bathing and outdoor mobility. About 14% (roughly five million) of community-dwelling elderly population age 65 or older in the National Long-Term Care Survey identified additional home modifications that would make things easier or more comfortable.d Similarly, Newman found in 1995 that 14% of elderly individuals (roughly five million) had a housing-related disability, defined as difficulty, use of assistance, or need of assistance in functioning in the home, that might be amenable to home modifications.227 Another study228 suggests that among older people reporting difficulty with mobility (roughly 25% of the older population or nine million people), one-third use only equipment, one-third use no equipment or help, and the remaining third receive some sort of help with mobility tasks.
Three interventions--smoking cessation, management of CHF, and advanced care planning among the severely ill--were clearly designed to reach narrower populations. About 9.3% of those age 65 or older, or 3.3 million persons, were current smokers in 2002. CHF, the leading diagnosis in hospitalizations of older persons, affects a total of about 3 million older Americans (550,000 new cases per year), about 5% of the population age 65-69 and 10% of the population age 70 or older.229 Advanced care planning could potentially affect about 1.6 million older persons who die each year and a larger percentage for which we have no good estimate who are in advanced stages of disease; less than half of severely or terminally ill patients currently have an AD and many are not specific enough to influence treatment decisions at the end of life.230
Short-Term Risk of Disability Associated with Risk Factor
A second important factor in sorting out short-term effects of interventions is the relationship between the risk factor and the risk of disability. To quantify these comparisons properly requires us to be able to identify from the literature the prevalence, incidence rate, and recovery rate the population stratified by each risk factor and combination of risk factors. Although some of this information is available from epidemiologic and observational studies (for a review see,48 the measures of disability, composition of study populations, and follow-up periods vary markedly across studies, making comparisons difficult.
Instead, we group interventions by the stage of the disablement process to which they are most relevant (i.e., those related to disease onset (primary prevention efforts), to disease management and functioning (secondary prevention), to the environmental components of disability (tertiary prevention), and to the very end of life). The risks of developing disability increase with each stage of the disablement process; moreover, the risks of disability recovery apply only to the group who has already experienced disability. Secondary and tertiary prevention measures, all else equal, are likely to have a greater impact on disability rates in the short-run than primary prevention efforts.e
Consider, for example, the relative risks for disability associated with risk factors related to primary disease prevention--inactivity and smoking. Disability incidence rates among seniors with no limitations at baseline, for example, have been estimated after a two-year follow-up period to be approximately 10% among non-walkers and 5% among walkers (who walk at least one mile one day/week)--a relative risk of 2.0 associated with inactivity.94 Similar relative risks are evident for those with moderate and severe functioning limitations at baseline. The short-term risks of disability incidence associated with smoking are also relatively moderate (although the cumulative lifetime risks are higher). Among the elderly population, the functioning scores are consistently lowest among recent quitters and current smokers than among never smokers.231
Much higher rates of disability incidence are associated with CHF, depression, and falling. For example, people with CHF have eight times the risk of severe mobility difficulty as other older people. Estimates from one study of older persons hospitalized with CHF found that a third were receiving formal assistance a year after hospital discharge. Population-based observational studies suggest that depressive symptoms increase the relative risk for incident ADL disability by 4-5 times among high functioning older adults232 and 1½-2 times in the general older population.233, 234 About 20%-30% of those who fall each year--roughly three times the average rate of disability incidence--suffer severe injuries such as hip fracture or head trauma that may lead to death, disability, and/or institutionalization.
Assistive technology and home modification may play a preventive role or may be used to facilitate recovery among those with disability. There are very few estimates as to the number of older people who could alleviate their disability through home modifications or the use of assistive technology, or the relative risk of disability in the absence of such devices.
The overwhelming majority of individuals who die in a given year experience disability at the very end of life. Based on estimates provided by Leveille and colleagues45 we calculate that of the 2.2 million deaths to older America each year, 1.6 million have a disability at the beginning of the year and 600,000 do not. Based on work by Lunney and colleagues,2, 3 84%-93% of deaths involve some amount of disability during the last year of life.
Effectiveness of Interventions
A number of challenges complicate the comparisons of effectiveness of interventions. Because most of the interventions studied here require behavioral changes, adherence is a major challenge. Rates of adherence with protocols and drop-out rates were not systematically reported and are difficult to compare across interventions. Studies commonly target select populations, making it difficult to determine (and compare) likely population-based effects. In addition, the outcomes examined in the studies we reviewed--particularly those targeted at disease prevention or functioning--rarely included include direct effects on disability. Instead, they provide evidence regarding the effectiveness in altering the risk factor (e.g., smoking, inactivity) or related physiologic (strength, aerobic capacity, functioning) or service use (hospitalizations, depression treatment) measures. Where disability measures are included, they vary widely across studies. Notwithstanding these complications, here we attempt to compare the strength of the evidence regarding the effect of each intervention(s) first on the risk factors of interest and then on the risks of disability.
Effects on risk factors of interest. Of the seven interventions reviewed, four stand out as likely to have modest effects on risk factors of interest: smoking cessation programs that combine counseling with pharmacologic treatment; exercise programs that increase strength, balance, and physical activity of older adults; depression screening, combined with referral and feedback, and combination therapy/pharmacologic treatment; and multi-factor fall prevention programs. Of the remaining three interventions we reviewed, the beneficial effects of assistive technology/home modifications have not been adequately tested with the older population; interventions for CHF management have shown a wide range of effects on hospitalizations and hospital days; and as currently practiced completion of ADs appear to have little or no effect on treatment decisions at the end of life.
Effects on risks of disability. Of the four interventions that might have a modest effect on risk factors, only three have been linked to reductions in risks of disability: exercise, depression screening and treatment, and fall prevention programs. The effects of a population-based exercise intervention on disability risks are likely to be modest, in part because of low adherence rates,102 and the difficulty older frail individuals have in progressing to more intense levels of activity.101 With respect to depression screening and treatment, although screening programs with feedback and referral increase treatment rates by over four-fold, and combined medication and therapy result in relative risks of remission of 1.5-1.8, studies focusing on functioning as an outcome typically found only small improvements in functioning after treatment, usually IADL and/or cognitive functioning. Hence, we conclude that depression and screening programs would have a small to modest effect on disability risks. Only one of the seven interventions reviewed has the potential to produce large effects on the risks of disability: multi-factor fall prevention strategies. Comprehensive interventions combining factors such as education about risks, exercise, home safety and health assessments, appeared to show a modest benefit in preventing falls for older populations, reducing the risk of falling in some cases by 30%-50% (RR 0.5-0.7), but the relationship between falling and disability is strong (RR 4.0-6.0). Consequently, programs that successfully reduce the risk of falling could potentially have a large effect on the risks of disability.
B. Comparison of Long-Term Effects
For longer-run comparisons, several additional issues emerge. How will the size and composition of the target population change in the future? At which trajectory is the intervention targeted and what are the competing risks? What are the effects of the intervention over the remaining lifetime? How will intervention affect mortality as well as disability? We discuss each of these issues in more detail below.
Shifting Target Populations
Several demographic trends are underway that will continue into the next 20 years. Most obviously, the United States population is aging; by 2020, 14.1% will be age 65 and older (compared to 10.9% in 2000); and 2.2% will be 85 and older (compared to 1.5% in 2000).235 The composition of the older population is also shifting--over the next two decades the older population will continue to experience increases in educational attainment18 and become more racially and ethnically diverse.235 Several health-related trends have also been apparent that show no signs of abating: obesity13 and reports of related cardiovascular diseases such as diabetes236 have been steadily increasing. Together, these changes are likely to influence the effectiveness of interventions in the future--although the net effects are unclear. On the one hand, individuals with more years of education are more likely to comply with protocols and invest in their future health and well-being. On the other hand the increasing diversity and co-morbidities of the older population will continue to challenge population-wide implementations of interventions.
For several of the interventions investigated here, we found evidence of ongoing trends. For instance, four of the seven risk factors of interest--inactivity, smoking, depression treatment, and assistive technology/home modification--appear to be moving already in a direction consistent with disability decline. There is also some evidence that injuries due to non-fatal falls have decreased and that ACP is increasing slowly. In contrast, CHF appears to be increasing. Limited information is available on trends in the joint distribution of these risk factors. More details on trends follows:
-
Inactivity among adults, particularly seniors, is reportedly declining.237 Based on data from the Center for Disease Controls Healthy People 2010, the percentage of adults ages 65-74 who were inactive (no leisure time physical activity in the past month) declined from 51% in 1997 to 47% in 2002; among those ages 75 and older, the percentage of inactive adults declined from 64% in 1997 to 61% in 2002. (The target for 2010 is 20%.)
-
Smoking in the non-institutionalized population age 65 or older has declined by about 2.5% per year for women and about 4.3% per year for men between 1985 and 2000.47
-
Depression. In the general population, the rate of outpatient treatment for depression increased from 0.73 per 100 persons in 1987 to 2.33 in 1997 (P0.001).238 Among the older population, between 1985 and 1993-1994, a significant increase in the rate of depression diagnosis was seen, but no change was observed between 1993-1994 and 1998-1999. Rates of prescribing of antidepressants more than doubled between 1985 and 1998-1999.239
-
Use of assistive technology only (without personal care) to carry out personal care activities doubled among older Americans (from 1.6% in 1984 to 3.0% in 1999 among all older Americans and from 7% to 15% among those with chronic disability.6 The presence of home modifications among older people reporting a housing-related disability nearly doubled from 26% in 1978 to 49% in 1995.240
-
According to the CDCs injury surveillance system, age-adjusted non-fatal injuries among the 65 and older population due to falls have declined over the last three years from 4.67 to 4.53 per 100,000.
-
Data from the National Health and Nutrition Examination Survey indicate that the prevalence of CHF more than doubled for persons age 65 and age 75 between 1976-1980 and 1988-1991.229 More recent studies have found a continuing increase in CHF prevalence in the general population between 1989 and 1999,241 with no increase in incidence but a decline in mortality.242
-
Since no study documents the prevalence of ACP or ADs, documenting trends is somewhat uncertain. Nevertheless, more reports are surfacing about care systems with high rates,225, 243, 244, 245, 246 whereas essentially no one had advance care plans 25 years ago. In many reports, the baseline rates among seriously ill persons tend to run 15%-30%. In special programs with a focus upon planning ahead, the rates can be around 90%. A recent report from Oregon showed that nursing home residents there are now running about 70%.247 In short, there is evidence that ACP is increasing slowly, but definitive population-based rates are not available.
Competing Risks
Each of the illustrative interventions we reviewed may be considered to be targeted at one or more illness trajectories. Exercise and fall prevention, for example, are primarily targeted to older adults in the frailty/dementia trajectory. CHF management is clearly targeted a specific type of organ failure. Smoking cessation is likely to be geared toward people who go on to develop cancer or organ failure (e.g., COPD, CHF or other cardiovascular disease). Depression screening and treatment, assistive technology and environmental modifications, and advanced care planning are not unique to any one trajectory but may be targeted at all three.
The issue of competing risks arises mainly for interventions targeted at the prevention of diseases with earlier ages of onset. That is, interventions designed to prevent cancer or organ failure, if successful, could allow people to survive longer and be at risk for the frailty/dementia trajectory. Of the seven illustrative interventions reviewer here, smoking cessation is the only intervention for which competing risks is an issue to be taken into consideration. The question is, if a very effective smoking cessation intervention reduces deaths from cancer or organ failure, will a larger proportion of the older population survive to follow a longer course of disability associated with frailty and/or dementia? (We explore this point further in the simulation in Section C.)
Mortality
In the longer-run comparisons it is important to understand the interventions effect not only on disability but also upon the length of life, and whether (or what proportion of) additional years are free from disability. In order for an intervention to result in a decline in disability, any increase in life expectancy must contribute proportionally more to active life expectancy than to years with disability. For example, a 1% increase in life expectancy will be accompanied by a decline in disability only if it results in a greater percentage increase in active life expectancy (and symmetrically, a smaller percentage increase in disability).
Intervention studies rarely quantify effects beyond a year or two after the intervention. Still, we speculate based on findings from the literature that, except for smoking cessation, the interventions reviewed here are unlikely to have large effects on mortality. Still, exercise, screening and treatment for depression, fall prevention, and the use of home modifications and assistive devices may possibly confer increases in longevity. To investigate this issue further, we turned to cohort studies and/or life table analyses.
C. Illustration of Long-Term Effects of Interventions
Table 5 illustrates the effects of several stylized interventions using the simplified model described in Chapter II. Recall that the baseline prevalence of disability in a population with assumptions in Table 2 is 20.1%. We demonstrate the comparative impacts on cross-sectional disability of interventions affecting disease prevention (through shifts in trajectories), disease management (with and without mortality effects), and disability.f
Disease prevention/trajectory shift. In order to illustrate the impact of shifts between trajectories that might occur with disease prevention programs, we assume that the three main trajectories (Cancer, Organ Failure, and Dementia/Frailty) are sequentially dependent. This implies that persons in whom cancer is prevented by an intervention will experience the same relative risks of the organ failure (20.5%) as others who do not get cancer. However, because it is typically experienced later in life, reducing organ failure has no effect on the probability of the cancer trajectory. 74.2% of persons who survive both the cancer and organ failure trajectories will experience the frailty trajectory.g By definition, the other trajectory captures any remaining members of the cohort after accounting for the other risks.
If an intervention were able to reduce cancers by half to 11% of the cohort, this model would predict an increase in organ failure to 18.3%, an increase in frailty/dementia to 52.5% and an increase in others to 18.3%. For even this extremely large impact on cancer deaths, the resulting change in disability prevalence would be an almost imperceptible decrease to 20.0% because the percentage change in years with disability would be only slightly smaller than the percentage gain in total life expectancy.
An intervention that reduced organ failures by half would have no effect on cancers, but would increase frailty/dementia to 51.9% and others to 18.1%. The disability rate would be unchanged, with countervailing effects of reduced mortality and increased number of years lived with disability.
If we simulate reductions in both the cancer and organ failure trajectories, for example due to a smoking intervention that shifts the risks of disease onset, we estimate no additional decrease in disability prevalence. It can be argued that smoking prevention and cessation interventions could have the effect of shifting individuals between trajectories. As discussed above, an intervention targeted at the elderly population for the purpose of preventing chronic disease would likely have a much smaller effect on disease prevalence than those simulated, but the simulations here demonstrate that population-level disability prevalence is essentially unaffected (20.0%) by any such intervention.
Disease management. Interventions may also have the effect of reducing disability alone or in combination with changes in longevity. If the intervention does not alter the risk of morality, or if changes in DFLE exceed changes in disabled life expectancy, then we can expect the cross-sectional prevalence rate to decline.
For example, the exercise interventions discussed in the literature appear to be targeted at the frailty trajectory and have no apparent effect on mortality. If they delay disability onset by one year in this population (increasing DFLE by one year), the estimated effect on disability prevalence is a reduction from 20.1% to 17.3%.
Similarly, the CHF management programs might minimize the number of flare-ups that are often accompanied by disability, without shifting the mortality course. If such an intervention lessens the number of months of disability in the organ failure trajectory by six months (increasing DFLE by six months), the estimated effect on disability prevalence is a reduction from 20.1% to 19.4%.
Alternatively, suppose that smoking cessation interventions aimed at older people with a diagnosis of cancer or organ failure coincided with such diagnoses and resulted in an extension of life for both trajectories of 2.8 years total (by adding 1.5 years of DFLE and 1.3 years of disabled life expectancy to each so the percentage change in the latter was greater than the percentage change in DFLE). In this case the disability rate would increase to 21.8.
Shift in the disability threshold through environmental changes. The next two columns simulate a home modification or assistive technology intervention that reduces environmental demands for persons in the organ failure and frailty trajectories by 25% and 5% respectively. We assume the rate of decline in function from the disability threshold to death is approximately constant and that there is no effect of the intervention on mortality so that the intervention results in reductions of 25% and 5% in the amount of time spent living with a disability. These assumptions imply a reduction of the numerator in the disability prevalence formula but no change in the denominator, and thus unambiguously reduce prevalence to 15.8% and 19.2% respectively.
Mortality only interventions. An intervention to increase ACP may have the effect of reducing the period of disability at the end of life for frail individuals. If the average effect of ACP were a reduction of one month in life expectancy with no decrease in DFLE, under the assumptions of our model, the population disability rate would decline from 20.1% to 19.9%.
V. SUMMARY OF FINDINGS
While the scope of this study and available research did not allow us to definitively quantify the impact of illustrative interventions on cross-sectional disability rates, we are able to suggest approaches that seem more likely to have a high-impact in the short-run than others. Of the seven approaches we reviewed, evidence of modest reductions in the risks of disability is strongest for exercise programs that increase strength, balance, and physical activity of older adults; depression screening, combined with referral and feedback and a treatment program combining therapy with pharmacologic treatment; and multi-factor fall prevention programs. Because they can be targeted at potentially large populations, widespread implementation of such interventions could potentially reduce the prevalence of disability in the short-run if adherence issues could be successfully addressed. Little evidence exists, however, about the long-term effects of such interventions.
This exercise has also provided several additional insights into how to reduce population-level disability prevalence among the elderly population. Our most striking finding is that efforts with the largest potential for success are those targeted at individuals whose life experience is exemplified by a prolonged period of disability and frailty before death. Multi-factor interventions that are targeted at frail individuals and that address individualized needs appear to be the most promising. Both short and long-term effects are critical to consider when evaluating the population-level impact of such interventions. More detail on each of these points follows.
Target Older Frail, Functionally Limited Populations
Both because of the numbers affected and because of the expected length of time spent with a disability, interventions aimed at reducing disability risk in the frail, functionally limited subpopulation have a relatively large payoff as measured by prevalence rates. In contrast, because of the advanced age at which disability tends to occur for this population, efforts that succeed in preventing diseases that typically cause shorter spells of disability earlier in life--while they will likely add to life expectancy--are unlikely to result in substantial reductions in disability prevalence.
Historically frail, functionally limited individuals are often left out of clinical studies examining disability interventions. While credibly controlling for baseline functioning and health in a population with multiple co-morbidities is difficult, the importance of including this group in clinical trails is clear if we wish to identify potentially high-impact interventions. To that end, Ferucci and colleagues have recently recommended strategies for including frail elderly population in clinical trials.248 Studies of the benefits of managing physical and mental health conditions, injury avoidance, and adaptation of the environmental should all be considered with this population, particularly those who have already reached very old age.
Tailor Multi-Factor Disability Intervention to Individual Needs
Based on our literature review, there appears to be evidence that multi-factor interventions and interventions tailored to individual needs work best. This seems especially relevant to persons in the frailty trajectory who do not have single, well-defined conditions linked to their disability.
Indeed, randomized trials of multi-factor home-based interventions aimed averting or delaying functional decline have been undertaken with mixed results. According to a recent review,249 modest reductions in disability incidence and functional decline may be achieved by home-based interventions that include multi-dimensional assessments with follow-up (RR 0.76; 95% CI 0.64-0.91); however, benefits are generally limited to subjects with relatively low mortality (generally less than age 80). These trials have also reduced mortality by similar amounts, hence the ultimate effect on prevalence in the longer-run remain unclear. The proposed framework highlights several key issues that may be useful in fine tuning these multi-factor strategies to identify components likely to have substantial impact at the population level both in the short-run and over a longer time horizon. Government efforts to identify multi-component strategies for disability reduction should include research support for additional work in this area.
Consider Both Short and Long-Term Effects of Interventions
In evaluating population-level impacts of interventions involving the elderly population, it is important to consider both short and long-term effects. As we have demonstrated in this report, an interventions effects are not uniform in the short and long-term, and what appears to be high-impact over a one or two year period may be ineffective--or lead to increases in disability prevalence--over a longer term horizon.
At the individual level, the effect of an intervention may change over the course of an older individuals life. Older individuals who experience disability may face multiple underlying causes that may shift over time. Removing or reducing one potential cause may have little or no impact on disability in the presence of other causes. One can imagine an intervention, such as installation of grab bars or other environmental modification, which allows the individual to maintain his or her independence for only a brief time until their physical and cognitive functioning declines. Other protocols--such as exercise or muscle strengthening--may become more effective in postponing disability as time goes on. Thus, at the individual level, interventions may have fundamentally different effects in the short and longer term.
In addition, interventions that alter the risk of disability may also affect survival and hence the length of life lived with disability. In doing so, interventions that delay disability in the short-run but put individuals on a path to the longer-lived frailty trajectory may ultimately lead to additional years lived with disability. Our simplistic simulations highlight possible conflicting short and long-term effects at the population level. For instance, a successful smoking cessation intervention aimed at older people with a diagnosis of cancer or organ failure resulting in reduced risk of disability and an extension of life for both trajectories could lead ultimately to an increase in the prevalence of disability. Notably, programs aimed at increasing the independence of older frail adults without increasing longevity--either through disease management or environmental modifications--do not pose such contradictions, but unequivocally decrease the prevalence of disability both in the short and longer term.
To fully understand the interplay of interventions with disability and mortality requires consideration of interventions effects over a prolonged follow-up period. Such a strategy, if incorporated into disability intervention research, would allow better estimation of the overall merits, rather than only the short-term merits, of a proposed intervention.
VI. APPENDIX: METHODOLOGY TO IDENTIFY ILLUSTRATIVE HIGH-IMPACT INTERVENTIONS
A. Approach
To help focus the literature review around a limited set of key interventions, we employed the Delphi method250 to distill the opinions of an expert group to identify interventions that are likely to have a significant impact on population-level disability prevalence. As is common in the application of this technique, we asked nine experts on late-life disability and disability trends to rank 12 interventions from 1 to 12 (with 1 most important and 12 least important) according to four criteria:
- short-term effectiveness in enhancing independence;
- long-term effectiveness;
- effect on length of life; and
- numbers of older people who could benefit from the intervention.
Experts also had the opportunity to add to their own interventions to the list. Six external experts and six members of the project team provided rankings.
To focus the scope of this exercise, we purposefully limited the proposed list of interventions to those that were: (a) existing; (b) not already widespread; (c) had some published evidence demonstrating efficacy; and (d) if implemented, could provide benefit within a few years in terms of reducing disability in the older population (rather than waiting for decades or having most effect upon early or mid-life populations). Interventions included:
- Improve exercise for those in fairly good health.
- Improve diet for those in fairly good health.
- Modify homes to enhance ease of use and safety.
- Provide assistive devices.
- Encourage smoking cessation.
- Encourage stroke prevention.
- Implement good chronic disease care for mild to moderate illness.
- Implement widespread care planning for serious illness and death.
- Provide more organ and joint replacements.
- Implement fall prevention systems for frail elderly.
- Implement depression screening, treatment, and follow-up.
- Provide cognitive training.
- Other.
B. Findings
Combing both internal and external responses, Table A-1 shows the rankings for each of the four outcomes.
Based on these results, the team classified the interventions into illustrative groupings that will help demonstrate different aspects of the conceptual framework under development (see Table A-2). The classification revealed the following:
- Encouraging smoking cessation among the older population.
- Implementing good chronic disease care for mild to moderate illness ranked high on all four outcomes.
- Improving exercise and encouraging stroke prevention ranked high on the same three outcomes.
- Implementing depression screening ranked high on two outcomes.
- Modifying homes and implementing fall prevention systems ranked high on short-term disability; encouraging smoking cessation ranked high on length of life and improving diet on number of people.
- Cognitive training, widespread care planning, providing more organ and joint replacements, and providing assistive devices were not viewed as high ranking in any of the four outcomes.
Although there was considerable overlap between top rankings of external experts and project team members, one salient area of inconsistency emerged worth noting. Rankings were widely dispersed for widespread care planning for serious illness and death.
VII. LITERATURE CITED
-
Pope AM, Tarlov AR. Disability in America: Toward a National Agenda for Prevention. Washington, DC: National Academies Press; 1991.
-
Lunney JR, Lynn J, Hogan C. Profiles of older Medicare decedents. Journal of the American Geriatrics Society. June 2002; 50(6):1108-1112.
-
Lunney JR, Lynn J, Foley DJ, Lipson S, Guralnik JM. Patterns of functional decline at the end of life. Journal of the American Medical Association. May 14, 2003; 289(18):2387-2392.
-
Freedman VA, Crimmins E, Schoeni R, et al. Resolving discrepancies in old-age disability trends across national surveys: Report from a technical working group. Demography. 2004; 41(3):417-441.
-
Freedman VA, Martin LG, Schoeni RF. Recent trends in disability and functioning among older adults in the United States: A systematic review. Journal of the American Medical Association. 2002; 288(24):3137-3146.
-
Spillman BC. Changes in elderly disability rates and the implications for health care utilization and cost. Milbank Quarterly. 2004; 82(1):157-194.
-
Lakdawalla D, Bhattacharya J, Goldman DP. A response to the points by Manton and Williamson. Medical Care. January 2003; 41(1):28-31.
-
Lakdawalla D, Goldman DP, Bhattacharya J, Hurd MD, Joyce GF, Panis CW. Forecasting the nursing home population. Medical Care. January 2003; 41(1): 8-20.
-
Manton KG. Forecasting the nursing home population. Medical Care. January 2003; 41(1):21-24.
-
Cutler DM. Declining disability among the elderly. Health Affairs. November-December 2001; 20(6):11-27.
-
Cutler DM. The reduction in disability among the elderly. Proceedings of the National Academy of Sciences of the United States of America. June 5, 2001; 98(12):6546-6547.
-
Cutler DM. Disability and the future of Medicare. New England Journal of Medicine. September 11, 2003; 349(11):1084-1085.
-
Sturm R, Ringel JS, Andreyeva T. Increasing obesity rates and disability trends. Health Affairs. March-April 2004; 23(2):199-205.
-
Singer BH, Manton KG. The effects of health changes on projections of health service needs for the elderly population of the United States. Proceedings of the National Academy of Sciences of the United States of America. December 22, 1998; 95(26):15618-15622.
-
Wolf SL, Sattin RW, OGrady M, et al. A study design to investigate the effect of intense Tai Chi in reducing falls among older adults transitioning to frailty. Controlled Clinical Trials. December 2001; 22(6):689-704.
-
Wolf DA. Population change: friend or foe of the chronic care system? Health Affairs. 2001; 20(6):28-42.
-
Tilly J, Goldenson SM, Kasten J. Long-Term Care: Consumers, Providers, and Financing: A Chart Book. Washington, DC: Urban Institute; 2001.
-
Freedman VA, Martin LG. The role of education in explaining and forecasting trends in functional limitations among older Americans. Demography. 1999; 36(4):461-473.
-
Waidmann TA, Liu K. Disability trends among elderly persons and implications for the future. Journals of Gerontology B: Social Sciences. September 2000; 55(5):S298-307.
-
Verbrugge LM, Jette AM. The disablement process. Social Science and Medicine. January 1994; 38(1):1-14.
-
Agree EM. The influence of personal care and assistive devices on the measurement of disability. Social Science and Medicine. February 1999; 48(4):427-443.
-
Lynn J. Perspectives on care at the close of life. Serving patients who may die soon and their families: The role of hospice and other services. Journal of the American Medical Association. February 21, 2001; 285(7):925-932.
-
Teno JM, Weitzen S, Fennell ML, Mor V. Dying trajectory in the last year of life: Does cancer trajectory fit other diseases? Journal of Palliative Medicine. Winter 2001; 4(4):457-464.
-
Twycross R, Lichter I. The terminal phase. In: Doyle D, Hanks GWC, MacDonald N, eds. Oxford Textbook of Palliative Medicine, 2nd ed. London: Oxford University Press; 1999:977-994.
-
Wachtel T, Allen-Masterson S, Reuben D, Goldberg R, Mor V. The end stage cancer patient: Terminal common pathway. Hospice Journal. 1988;4(4):43-80.
-
Morris JN, Suissa S, Sherwood S, Wright SM, Greer D. Last days: A study of the quality of life of terminally ill cancer patients. Journal of Chronic Diseases. 1986; 39(1):47-62.
-
Murray SA, Boyd K, Kendall M, Worth A, Benton TF, Clausen H. Dying of lung cancer or cardiac failure: Prospective qualitative interview study of patients and their carers in the community. British Medical Journal. October 26, 2002; 325(7370):929.
-
McCarthy EP, Phillips RS, Zhong Z, Drews RE, Lynn J. Dying with cancer: Patients' function, symptoms, and care preferences as death approaches. Journal of the American Geriatrics Society. May 2000; 48(5 Suppl):S110-121.
-
Knaus WA, Harrell FE Jr., Lynn J, et al. The SUPPORT prognostic model. Objective estimates of survival for seriously ill hospitalized adults. Study to understand prognoses and preferences for outcomes and risks of treatments. Annals of Internal Medicine. February 1, 1995; 122(3):191-203.
-
Juenger J, Schellberg D, Kraemer S, et al. Health related quality of life in patients with congestive heart failure: Comparison with other chronic diseases and relation to functional variables. Heart. March 2002; 87(3):235-241.
-
Cowie MR, Fox KF, Wood DA, et al. Hospitalization of patients with heart failure: A population-based study. European Heart Journal. June 2002; 23(11):877-885.
-
McCormick TR, Conley BJ. Patients' perspectives on dying and on the care of dying patients. Western Journal of Medicine. September 1995; 163(3):236-243.
-
Longino CF Jr. Pressure from our aging population will broaden our understanding of medicine. Academic Medicine. October 1997; 72(10):841-847.
-
Verbrugge LM, Patrick DL. Seven chronic conditions: Their impact on US adults' activity levels and use of medical services. American Journal of Public Health. February 1995; 85(2):173-182.
-
Ettinger WH Jr., Fried LP, Harris T, Shemanski L, Schulz R, Robbins J. Self-reported causes of physical disability in older people: The Cardiovascular Health Study. CHS Collaborative Research Group. Journal of the American Geriatrics Society. October 1994; 42(10):1035-1044.
-
Fried LP, Guralnik JM. Disability in older adults: Evidence regarding significance, etiology, and risk. Journal of the American Geriatrics Society. January 1997; 45(1):92-100.
-
Williamson JD, Fried LP. Characterization of older adults who attribute functional decrements to "old age". Journal of the American Geriatrics Society. December 1996; 44(12):1429-1434.
-
Verbrugge LM, Lepkowski JM, Imanaka Y. Comorbidity and its impact on disability. Milbank Quarterly. 1989; 67(3-4):450-484.
-
Campbell AJ, Busby WJ, Robertson MC, Lum CL, Langlois JA, Morgan FC. Disease, impairment, disability and social handicap: A community based study of people aged 70 years and over. Disability and Rehabilitation. April-June 1994; 16(2):72-79.
-
Picavet HS, van den Bos GA. The contribution of six chronic conditions to the total burden of mobility disability in the Dutch population. American Journal of Public Health. October 1997; 87(10):1680-1682.
-
Guccione AA, Felson DT, Anderson JJ, et al. The effects of specific medical conditions on the functional limitations of elders in the Framingham Study. American Journal of Public Health. March 1994; 84(3):351-358.
-
Boult C, Altmann M, Gilbertson D, Yu C, Kane RL. Decreasing disability in the 21st century: The future effects of controlling six fatal and nonfatal conditions. American Journal of Public Health. October 1996; 86(10):1388-1393.
-
Nusselder WJ, van der Velden K, van Sonsbeek JL, Lenior ME, van den Bos GA. The elimination of selected chronic diseases in a population: The compression and expansion of morbidity. American Journal of Public Health. February 1996; 86(2):187-194.
-
Murray CJ, Lopez AD. SUMMARY: The Global Burden of Disease: A comprehensive assessment of mortality and disability from diseases, injuries, and risk factors in 1990 and projected to 2020. Harvard School of Public Health; 1996.
-
Leveille SG, Penninx BW, Melzer D, Izmirlian G, Guralnik JM. Sex differences in the prevalence of mobility disability in old age: The dynamics of incidence, recovery, and mortality. Journals of Gerontology B: Social Sciences. January 2000; 55(1):S41-50.
-
Reed JG, Baxter PM. Using reference databases. In: Cooper H, Hedges LV, eds. The Handbook of Research Synthesis. New York, NY: Russell Sage Foundation; 1994:58-70.
-
National Center for Health Statistics. Health, United States, 2003. Rockville, MD: Author; 2003.
-
Stuck A, Walthert J, Nikolaus T, Bula C, Hohmann C, Beck J. Risk factors for functional status decline in community-living elderly people: A systematic literature review. Social Science and Medicine. February 1999; 48(4):445-469.
-
Rogers RG, Nam CB, Hummer RA. Activity limitation and cigarette smoking in the United States: Implications for health expectancies. In: Mathers CD, McCallum J, Robine JM, eds. Advances in Health Expectancies. Canberra, Australia: Australian Institute of Health and Welfare; 1994:337-344.
-
Centers for Disease Control and Prevention. Cigarette smoking among adults -- United States, 2002. Morbidity and Mortality Weekly Report. May 28, 2002; 53(20):427-431.
-
Dale LC, Olsen DA, Patten CA, et al. Predictors of smoking cessation among elderly smokers treated for nicotine dependence. Tobacco Control. Autumn 1997; 6(3):181-187.
-
Burton LC, Paglia MJ, German PS, Shapiro S, Damiano AM. The effect among older persons of a general preventive visit on three health behaviors: Smoking, excessive alcohol drinking, and sedentary lifestyle. The Medicare Preventive Services Research Team. Preventive Medicine. September 1995; 24(5):492-497.
-
Henderson PN, Rhoades D, Henderson JA, Welty TK, Buchwald D. Smoking cessation and its determinants among older American Indians: The Strong Heart Study. Ethnicity and Disease. Spring 2004; 14(2):274-279.
-
Centers for Medicare and Medicaid Services. Interventions to Promote Smoking Cessation in the Medicare Population. Washington, DC: Author; September 12, 2002.
-
American Lung Association, Santa Clara Chapter. Even seniors who quit smoking gain extra years. Ashkickers Newsletter. Available at: http://www.lungsrus.org/Newsletters/AKC/AKC%20June-0r.htm. Accessed July, 2004.
-
Centers for Medicare and Medicaid Services. Available at: http://www.cms.hhs.gov/researchers/demos/healthyaging/1b.asp. Accessed September 24, 2005.
-
Burns DM. Cigarette smoking among the elderly: Disease consequences and the benefits of cessation. American Journal of Health Promotion. July-August 2000; 14(6):357-361.
-
Hurley BF, Roth SM. Strength training in the elderly: Effects on risk factors for age-related diseases. Sports Medicine. October 2000; 30(4):249-268.
-
Oida Y, Kitabatake Y, Nishijima Y, et al. Effects of a 5-year exercise-centered health-promoting programme on mortality and ADL impairment in the elderly. Age and Ageing. November 2003; 32(6):585-592.
-
Evans WJ. Exercise as the standard of care for elderly people. Journals of Gerontology A: Medical Sciences. May 2002; 57(5):M260-261.
-
Nelson ME, Layne JE, Bernstein MJ, et al. The effects of multidimensional home-based exercise on functional performance in elderly people. Journals of Gerontology A: Medical Sciences. February 2004; 59(2):M154-160.
-
Baker K, McAlindon T. Exercise for knee osteoarthritis. Current Opinion in Rheumatology. September 2000; 12(5):456-463.
-
Oldridge N. Cardiac rehabilitation in the elderly. Aging (Milano). August 1998; 10(4):273-283.
-
Meek C, Pollock A, Potter J, Langhorne P. A systematic review of exercise trials post stroke. Clinical Rehabilitation. February 2003; 17(1):6-13.
-
Brill PA, Cornman CB, Davis DR, et al. The value of strength training for older adults. Home Care Provider. April 1999; 4(2):62-66.
-
Satariano WA, McAuley E. Promoting physical activity among older adults: From ecology to the individual. American Journal of Preventive Medicine. October 2003; 25(3 Suppl 2):184-192.
-
U.S. Department of Health and Human Services. Physical Activity and Health A Report of the Surgeon General. Atlanta, GA: Author; 1996.
-
Kaplan GA, Seeman TE, Cohen RD, Knudsen LP, Guralnik J. Mortality among the elderly in the Alameda County Study: Behavioral and demographic risk factors. American Journal of Public Health. March 1987; 77(3):307-312.
-
Morey MC, Zhu CW. Improved fitness narrows the symptom-reporting gap between older men and women. Journal of Women's Health. May 2003; 12(4):381-390.
-
Seguin R, Nelson ME. The benefits of strength training for older adults. American Journal of Preventive Medicine. October 2003; 25(3 Suppl 2):141-149.
-
Lemura LM, von Duvillard SP, Mookerjee S. The effects of physical training of functional capacity in adults. Ages 46 to 90: A meta-analysis. Journal of Sports Medicine and Physical Fitness. March 2000; 40(1):1-10.
-
Singh MA. Exercise comes of age: Rationale and recommendations for a geriatric exercise prescription. Journals of Gerontology A: Medical Sciences. May 2002; 57(5):M262-282.
-
Latham N, Anderson C, Bennett D, Stretton C. Progressive resistance strength training for physical disability in older people. Cochrane Database of Systematic Reviews. 2003(2):CD002759.
-
Keysor JJ. Does late-life physical activity or exercise prevent or minimize disablement? A critical review of the scientific evidence. American Journal of Preventive Medicine. October 2003; 25(3 Suppl 2):129-136.
-
Brawley LR, Rejeski WJ, King AC. Promoting physical activity for older adults: The challenges for changing behavior. American Journal of Preventive Medicine. October 2003; 25(3 Suppl 2):172-183.
-
Stewart AL, Verboncoeur CJ, McLellan BY, et al. Physical activity outcomes of CHAMPS II: A physical activity promotion program for older adults. Journals of Gerontology A: Medical Sciences. August 2001; 56(8):M465-470.
-
Robert Wood Johnson Foundation. National Blueprint: Increasing Physical Activity Among Adults Age 50 and Over. Princeton, NJ: Author; 2001.
-
Marchionni N, Fattirolli F, Fumagalli S, et al. Improved exercise tolerance and quality of life with cardiac rehabilitation of older patients after myocardial infarction: Results of a randomized, controlled trial. Circulation. May 6, 2003; 107(17):2201-2206.
-
Binder EF, Schechtman KB, Ehsani AA, et al. Effects of exercise training on frailty in community-dwelling older adults: Results of a randomized, controlled trial. Journal of the American Geriatrics Society. December 2002; 50(12):1921-1928.
-
Bearne LM, Scott DL, Hurley MV. Exercise can reverse quadriceps sensorimotor dysfunction that is associated with rheumatoid arthritis without exacerbating disease activity. Rheumatology (Oxford, England). February 2002; 41(2):157-166.
-
Penninx BW, Messier SP, Rejeski WJ, et al. Physical exercise and the prevention of disability in activities of daily living in older persons with osteoarthritis. Archives of Internal Medicine. October 22, 2001; 161(19):2309-2316.
-
Chin A, Paw MJ, de Jong N, Schouten EG, Hiddink GJ, Kok FJ. Physical exercise and/or enriched foods for functional improvement in frail, independently living elderly: A randomized controlled trial. Archives of Physical Medicine and Rehabilitation. June 2001; 82(6):811-817.
-
Mitchell SL, Stott DJ, Martin BJ, Grant SJ. Randomized controlled trial of quadriceps training after proximal femoral fracture. Clinical Rehabilitation. June 2001; 15(3):282-290.
-
King AC, Pruitt LA, Phillips W, Oka R, Rodenburg A, Haskell WL. Comparative effects of two physical activity programs on measured and perceived physical functioning and other health-related quality of life outcomes in older adults. Journals of Gerontology A: Medical Sciences. February 2000; 55(2):M74-83.
-
Deyle GD, Henderson NE, Matekel RL, Ryder MG, Garber MB, Allison SC. Effectiveness of manual physical therapy and exercise in osteoarthritis of the knee. A randomized, controlled trial. Annals of Internal Medicine. February 1, 2000; 132(3):173-181.
-
O'Reilly SC, Muir KR, Doherty M. Effectiveness of home exercise on pain and disability from osteoarthritis of the knee: A randomised controlled trial. Annals of the Rheumatic Diseases. January 1999; 58(1):15-19.
-
Mangione KK, McCully K, Gloviak A, Lefebvre I, Hofmann M, Craik R. The effects of high-intensity and low-intensity cycle ergometry in older adults with knee osteoarthritis. Journals of Gerontology A: Medical Sciences. April 1999; 54(4):M184-190.
-
Rydwik E, Frandin K, Akner G. Effects of physical training on physical performance in institutionalised elderly patients (70+) with multiple diagnoses. Age and Ageing. January 2004; 33(1):13-23.
-
Hurley BF, Hagberg JM. Optimizing health in older persons: Aerobic or strength training? Exercise and Sports Sciences Reviews. 1998; 26:61-89.
-
Lazowski DA, Ecclestone NA, Myers AM, et al. A randomized outcome evaluation of group exercise programs in long-term care institutions. Journals of Gerontology A: Medical Sciences. December 1999; 54(12):M621-628.
-
Mulrow CD, Gerety MB, Kanten D, et al. A randomized trial of physical rehabilitation for very frail nursing home residents. Journal of the American Medical Association. February 16, 1994; 271(7):519-524.
-
Kahana E, Lawrence RH, Kahana B, et al. Long-term impact of preventive proactivity on quality of life of the old-old. Psychosomatic Medicine. May-June 2002; 64(3):382-394.
-
Keysor JJ, Jette AM. Have we oversold the benefit of late-life exercise? Journals of Gerontology A: Medical Sciences. 2001; 56(7):M412-423.
-
Miller ME, Rejeski WJ, Reboussin BA, Ten Have TR, Ettinger WH. Physical activity, functional limitations, and disability in older adults. Journal of the American Geriatrics Society. October 2000; 48(10):1264-1272.
-
Wu SC, Leu SY, Li CY. Incidence of and predictors for chronic disability in activities of daily living among older people in Taiwan. Journal of the American Geriatrics Society. September 1999; 47(9):1082-1086.
-
Wang L, van Belle G, Kukull WB, Larson EB. Predictors of functional change: A longitudinal study of nondemented people aged 65 and older. Journal of the American Geriatrics Society. September 2002; 50(9):1525-1534.
-
Simonsick EM, Lafferty ME, Phillips CL, et al. Risk due to inactivity in physically capable older adults. American Journal of Public Health. October 1993; 83(10):1443-1450.
-
Seeman TE, Berkman LF, Charpentier PA, Blazer DG, Albert MS, Tinetti ME. Behavioral and psychosocial predictors of physical performance: MacArthur studies of successful aging. Journals of Gerontology A: Medical Sciences. July 1995; 50(4):M177-183.
-
Gill T, Baker D, Gottschalk M, Peduzzi P, Allore H, Byers A. A program to prevent functional decline in physically frail, elderly persons who live at home. New England Journal of Medicine. October 3, 2002; 347(14):1068-1074.
-
Gill T, Baker D, Gottschalk M, Peduzzi P, Allore H, Van Ness P. A prehabilitation program for the prevention of functional decline: Effect on higher-level physical function. Archives of Physical Medicine and Rehabilitation. July 2004; 85(7):1043-1049.
-
Gill T, Baker D, Gottschalk M, et al. A prehabilitation program for physically frail community-living older persons. Archives of Physical Medicine and Rehabilitation. March 2003; 84(3):394-404.
-
Hauer K, Pfisterer M, Schuler M, Bartsch P, Oster P. Two years later: A prospective long-term follow-up of a training intervention in geriatric patients with a history of severe falls. Archives of Physical Medicine and Rehabilitation. October 2003; 84(10):1426-1432.
-
King AC, Haskell WL, Taylor CB, Kraemer HC, DeBusk RF. Group- vs home-based exercise training in healthy older men and women. A community-based clinical trial. Journal of the American Medical Association. September 18, 1991; 266(11):1535-1542.
-
Marcus BH, Banspach SW, Lefebvre RC, Rossi JS, Carleton RA, Abrams DB. Using the stages of change model to increase the adoption of physical activity among community participants. American Journal of Health Promotion. July-August 1992; 6(6):424-429.
-
Lorig KR, Sobel DS, Stewart AL, et al. Evidence suggesting that a chronic disease self-management program can improve health status while reducing hospitalization: A randomized trial. Medical Care. January 1999; 37(1):5-14.
-
American Heart Association. Heart Disease and Stroke Statistics--2004 Update. Author. Available at: http://www.americanheart.org/downloadable/heart/1079736729696HDSStats200....
-
DesHarnais S, Hogan AJ, McMahon LF, Jr., Fleming S. Changes in rates of unscheduled hospital readmissions and changes in efficiency following the introduction of the Medicare prospective payment system. An analysis using risk-adjusted data. Evaluation and the Health Professions. June 1991; 14(2):228-252.
-
Rich MW, Freedland KE. Effect of DRGs on three-month readmission rate of geriatric patients with congestive heart failure. American Journal of Public Health. June 1988; 78(6):680-682.
-
Phillips CO, Wright SM, Kern DE, Singa RM, Shepperd S, Rubin HR. Comprehensive discharge planning with postdischarge support for older patients with congestive heart failure: A meta-analysis. Journal of the American Medical Association. March 17, 2004; 291(11):1358-1367.
-
Vinson JM, Rich MW, Sperry JC, Shah AS, McNamara T. Early readmission of elderly patients with congestive heart failure. Journal of the American Geriatrics Society. December 1990; 38(12):1290-1295.
-
Massie BM, Shah NB. Evolving trends in the epidemiologic factors of heart failure: Rationale for preventive strategies and comprehensive disease management. American Heart Journal. June 1997; 133(6):703-712.
-
Chin MH, Goldman L. Correlates of early hospital readmission or death in patients with congestive heart failure. American Journal of Cardiology. June 15, 1997; 79(12):1640-1644.
-
Ho KK, Anderson KM, Kannel WB, Grossman W, Levy D. Survival after the onset of congestive heart failure in Framingham Heart Study subjects. Circulation. July 1993; 88(1):107-115.
-
Wolinsky FD, Gurney JG, Wan GJ, Bentley DW. The sequelae of hospitalization for ischemic stroke among older adults. Journal of the American Geriatrics Society. May 1998; 46(5):577-582.
-
Pantilat SZ, Steimle AE. Palliative care for patients with heart failure. Journal of the American Medical Association. May 26, 2004; 291(20):2476-2482.
-
Tresch DD. The clinical diagnosis of heart failure in older patients. Journal of the American Geriatrics Society. September 1997; 45(9):1128-1133.
-
Buchanan A, Tan RS. Congestive heart failure in elderly patients. The treatment goal is improved quality, not quantity, of life. Postgraduate Medicine. October 1997; 102(4):207-208, 211-205.
-
Garg R, Yusuf S. Overview of randomized trials of angiotensin-converting enzyme inhibitors on mortality and morbidity in patients with heart failure. Collaborative Group on ACE Inhibitor Trials. Journal of the American Medical Association. May 10, 1995; 273(18):1450-1456.
-
Group TCTS. Effects of enalapril on mortality in severe congestive heart failure. Results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). New England Journal of Medicine. June 4, 1987; 316(23): 1429-1435.
-
Fonarow GC, Chelimsky-Fallick C, Stevenson LW, et al. Effect of direct vasodilation with hydralazine versus angiotensin-converting enzyme inhibition with captopril on mortality in advanced heart failure: The Hy-C trial. Journal of the American College of Cardiology. March 15, 1992; 19(4):842-850.
-
Harjai KJ, Mehra MR, Ventura HO, et al. Home inotropic therapy in advanced heart failure: Cost analysis and clinical outcomes. Chest. November 5, 1997; 112(5):1298-1303.
-
Pitt B, Segal R, Martinez FA, et al. Randomised trial of losartan versus captopril in patients over 65 with heart failure (Evaluation of Losartan in the Elderly Study, ELITE). Lancet. March 15, 1997; 349(9054):747-752.
-
Sin DD, McAlister FA. The effects of beta-blockers on morbidity and mortality in a population-based cohort of 11,942 elderly patients with heart failure. American Journal of Medicine. December 1, 2002; 113(8):650-656.
-
Koch M, Douard H, Broustet JP. The benefit of graded physical exercise in chronic heart failure. Chest. May 1992; 101(5 Suppl):231S-235S.
-
Sullivan MJ, Higginbotham MB, Cobb FR. Exercise training in patients with severe left ventricular dysfunction. Hemodynamic and metabolic effects. Circulation. September 1988; 78(3):506-515.
-
Coats AJ, Adamopoulos S, Radaelli A, et al. Controlled trial of physical training in chronic heart failure. Exercise performance, hemodynamics, ventilation, and autonomic function. Circulation. June 1992; 85(6):2119-2131.
-
King L. The effects of resistance exercise on skeletal muscle abnormalities in patients with advanced heart failure. Progress in Cardiovascular Nursing. Fall 2001; 16(4):142-151.
-
Ahmed A. Quality and outcomes of heart failure care in older adults: Role of multidisciplinary disease-management programs. Journal of the American Geriatrics Society. September 2002; 50(9):1590-1593.
-
Rich MW, Nease RF. Cost-effectiveness analysis in clinical practice: The case of heart failure. Archives of Internal Medicine. August 9-23, 1999; 159(15): 1690-1700.
-
Philbin EF. Comprehensive multidisciplinary programs for the management of patients with congestive heart failure. Journal of General Internal Medicine. February 1999; 14(2):130-135.
-
Weingarten SR, Henning JM, Badamgarav E, et al. Interventions used in disease management programmes for patients with chronic illness-which ones work? Meta-analysis of published reports. British Medical Journal. October 26, 2002; 325(7370):925.
-
Goodwin BA. Home cardiac rehabilitation for congestive heart failure: A nursing case management approach. Rehabilitation Nursing. July-August 1999; 24(4):143-147.
-
Henrick A. Cost-effective outpatient management of persons with heart failure. Progress in Cardiovascular Nursing. Spring 2001; 16(2):50-56.
-
Rich MW, Vinson JM, Sperry JC, et al. Prevention of readmission in elderly patients with congestive heart failure: Results of a prospective, randomized pilot study. Journal of General Internal Medicine. November 1993; 8(11):585-590.
-
Rich MW, Beckham V, Wittenberg C, Leven CL, Freedland KE, Carney RM. A multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failure. New England Journal of Medicine. November 2, 1995; 333(18):1190-1195.
-
Rich MW, Gray DB, Beckham V, Wittenberg C, Luther P. Effect of a multidisciplinary intervention on medication compliance in elderly patients with congestive heart failure. American Journal of Medicine. September 1996; 101(3):270-276.
-
Kornowski R, Zeeli D, Averbuch M, et al. Intensive home-care surveillance prevents hospitalization and improves morbidity rates among elderly patients with severe congestive heart failure. American Heart Journal. April 1995; 129(4): 762-766.
-
West JA, Miller NH, Parker KM, et al. A comprehensive management system for heart failure improves clinical outcomes and reduces medical resource utilization. American Journal of Cardiology. January 1, 1997; 79(1):58-63.
-
Stewart S, Pearson S, Horowitz JD. Effects of a home-based intervention among patients with congestive heart failure discharged from acute hospital care. Archives of Internal Medicine. May 25, 1998; 158(10):1067-1072.
-
Whellan DJ, Gaulden L, Gattis WA, et al. The benefit of implementing a heart failure disease management program. Archives of Internal Medicine. October 8, 2001; 161(18):2223-2228.
-
Akosah KO, Schaper AM, Havlik P, Barnhart S, Devine S. Improving care for patients with chronic heart failure in the community: The importance of a disease management program. Chest. September 2002; 122(3):906-912.
-
Rich MW. Heart failure disease management: a critical review. Journal of Cardiac Failure. March 1999; 5(1):64-75.
-
Ashton CM, Kuykendall DH, Johnson ML, Wray NP, Wu L. The association between the quality of inpatient care and early readmission. Annals of Internal Medicine. March 15, 1995; 122(6):415-421.
-
Marcantonio ER, McKean S, Goldfinger M, Kleefield S, Yurkofsky M, Brennan TA. Factors associated with unplanned hospital readmission among patients 65 years of age and older in a Medicare managed care plan. American Journal of Medicine. July 1999; 107(1):13-17.
-
Tierney WM, Overhage JM, Murray MD, et al. Effects of computerized guidelines for managing heart disease in primary care. Journal of General Internal Medicine. December 2003; 18(12):967-976.
-
Zambroski CH. Qualitative analysis of living with heart failure. Heart Lung. January-February 2003; 32(1):32-40.
-
Gibbs JS, McCoy AS, Gibbs LM, Rogers AE, Addington-Hall JM. Living with and dying from heart failure: The role of palliative care. Heart. October 2002; 88 Suppl 2:ii36-39.
-
Dracup K, Baker DW, Dunbar SB, et al. Management of heart failure. II. Counseling, education, and lifestyle modifications. Journal of the American Medical Association. November 9, 1994; 272(18):1442-1446.
-
Cowper PA, DeLong ER, Whellan DJ, Allen LaPointe NM, Califf RM. Economic effects of beta-blocker therapy in patients with heart failure. American Journal of Medicine. January 15, 2004; 116(2):104-111.
-
Allen LaPointe NM, Kramer JM, Hammill BG, et al. Long-Term Adherence to Evidence-Based Therapies for Coronary Artery Disease and Heart Failure in the Outpatient Setting. Journal of the American College of Cardiology. March 19, 2003; 41(6 Sup A):517A.
-
Penninx BW, Leveille S, Ferrucci L, van Eijk JT, Guralnik JM. Exploring the effect of depression on physical disability: Longitudinal evidence from the established populations for epidemiologic studies of the elderly. American Journal of Public Health. September 1999; 89(9):1346-1352.
-
Unutzer J, Patrick DL, Marmon T, Simon GE, Katon WJ. Depressive symptoms and mortality in a prospective study of 2,558 older adults. American Journal of Geriatric Psychiatry. September-October 2002; 10(5):521-530.
-
Andrews G, Sanderson K, Slade T, Issakidis C. Why does the burden of disease persist? Relating the burden of anxiety and depression to effectiveness of treatment. Bulletin of the World Health Organization. 2000; 78(4):446-454.
-
Baker FM. An overview of depression in the elderly: A US perspective. Journal of the National Medical Association. March 1996; 88(3):178-184.
-
Christensen H, Jorm AF, Mackinnon AJ, et al. Age differences in depression and anxiety symptoms: A structural equation modelling analysis of data from a general population sample. Psychological Medicine. March 1999; 29(2):325-339.
-
Mulsant BH, Ganguli M. Epidemiology and diagnosis of depression in late life. Journal of Clinical Psychiatry. 1999; 60 Suppl 20:9-15.
-
Beekman AT, Deeg DJ, Braam AW, Smit JH, Van Tilburg W. Consequences of major and minor depression in later life: A study of disability, well-being and service utilization. Psychological Medicine. November 1997; 27(6):1397-1409.
-
Alexopoulos GS, Meyers BS, Young RC, et al. Recovery in geriatric depression. Archives of general psychiatry. April 1996; 53(4):305-312.
-
Addonizio G, Alexopoulos G. Affective disorders in the elderly. International Journal of Geriatric Psychiatry. 1993; 8:41-47.
-
Roberts RE, Kaplan GA, Shema SJ, Strawbridge WJ. Does growing old increase the risk for depression? American Journal of Psychiatry. October 1997; 154(10):1384-1390.
-
Henderson S, Jorm AF, Korten AE, Jacomb P, Christensen H, Rodgers B. Symptoms of depression and anxiety during adult life: Evidence for a decline in prevalence with age. Psychological Medicine. November 1998; 28(6):1321-1328.
-
Snowdon J. Depression in old age: questions concerning prevalence studies. International Journal of Geriatric Psychiatry. October 1997; 12(10):1043-1045.
-
Schoevers RA, Geerlings MI, Beekman AT, et al. Association of depression and gender with mortality in old age. Results from the Amsterdam Study of the Elderly (AMSTEL). British Journal of Psychiatry. October 2000; 177:336-342.
-
Reynolds CF 3rd, Kupfer DJ. Depression and aging: a look to the future. Psychiatric Services. September 1999; 50(9):1167-1172.
-
Hyer L, Blazer D. Depressive symptoms: Impact and problems in long term care facilities. International Journal of Behavioral Geriatrics. 1982; 1(3):33-44.
-
Aben I, Verhey F, Honig A, Lodder J, Lousberg R, Maes M. Research into the specificity of depression after stroke: A review on an unresolved issue. Progress in Neuro-Psychopharmacology and Biological Psychiatry. May 2001; 25(4):671-689.
-
Andersen G, Vestergaard K, Riis J, Lauritzen L. Incidence of post-stroke depression during the first year in a large unselected stroke population determined using a valid standardized rating scale. Acta psychiatrica Scandinavica. September 1994; 90(3):190-195.
-
Hickie I, Scott E, Naismith S, et al. Late-onset depression: Genetic, vascular and clinical contributions. Psychological Medicine. November 2001; 31(8):1403-1412.
-
Reynolds CF 3rd, Miller MD, Pasternak RE, et al. Treatment of bereavement-related major depressive episodes in later life: A controlled study of acute and continuation treatment with nortriptyline and interpersonal psychotherapy. American Journal of Psychiatry. February 1999; 156(2):202-208.
-
Pampallona S, Bollini P, Tibaldi G, Kupelnick B, Munizza C. Combined pharmacotherapy and psychological treatment for depression: A systematic review. Archives of General Psychiatry. 2004; 61(7):714-719.
-
Butters MA, Becker JT, Nebes RD, et al. Changes in cognitive functioning following treatment of late-life depression. Am J Psychiatry. December 2000; 157(12):1949-1954.
-
Callahan CM, Kroenke K, Counsell SR, et al. Treatment of Depression Improves Physical Functioning in Older Adults. Journal of the American Geriatrics Society. 2005; 53(3):367-373.
-
Chemerinski E, Robinson RG, Arndt S, Kosier JT. The effect of remission of poststroke depression on activities of daily living in a double-blind randomized treatment study. J Nerv Ment Dis. July 2001; 189(7):421-425.
-
Heiligenstein JH, Ware JE, Jr., Beusterien KM, Roback PJ, Andrejasich C, Tollefson GD. Acute effects of fluoxetine versus placebo on functional health and well-being in late-life depression. Int Psychogeriatr. 1995; 7 Suppl:125-137.
-
DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment: Meta-analysis of the effects of anxiety and depression on patient adherence. Archives of Internal Medicine. July 24, 2000; 160(14):2101-2107.
-
Reynolds CF 3rd, Alexopoulos GS, Katz IR, Lebowitz BD. Chronic depression in the elderly: Approaches for prevention. Drugs and Aging. 2001; 18(7):507-514.
-
American Geriatrics Society, British Geriatrics Society, American Academy of Orthopaedic Surgeons Panel on Falls Prevention. Guideline for the prevention of falls in older persons. Journal of the American Geriatrics Society. May 2001; 49(5):664-672.
-
Graafmans WC, Ooms ME, Hofstee HM, Bezemer PD, Bouter LM, Lips P. Falls in the elderly: A prospective study of risk factors and risk profiles. American Journal of Epidemiology. June 1, 1996; 143(11):1129-1136.
-
Bell AJ, Talbot-Stern JK, Hennessy A. Characteristics and outcomes of older patients presenting to the emergency department after a fall: A retrospective analysis. Medical Journal of Australia. August 21, 2000; 173(4):179-182.
-
Lord SR, Caplan GA, Ward JA. Balance, reaction time, and muscle strength in exercising and nonexercising older women: A pilot study. Archives of Physical Medicine and Rehabilitation. August 1993; 74(8):837-839.
-
Ray WA, Griffin MR. Prescribed medications and the risk of falling. Topics in Geriatric Rehabilitation. 1990; 5(2):12-20.
-
Tinetti ME, Speechley M. Prevention of falls among the elderly. New England Journal of Medicine. April 20, 1989; 320(16):1055-1059.
-
Hausdorff JM, Rios DA, Edelberg HK. Gait variability and fall risk in community-living older adults: A 1-year prospective study. Archives of Physical Medicine and Rehabilitation. August 2001; 82(8):1050-1056.
-
Hornbrook MC, Stevens VJ, Wingfield DJ, Hollis JF, Greenlick MR, Ory MG. Preventing falls among community-dwelling older persons: Results from a randomized trial. Gerontologist. February 1994; 34(1):16-23.
-
MMWR. Incidence and costs to Medicare of fractures among Medicare beneficiaries aged > or = 65 years--United States, July 1991-June 1992. Morbidity and Mortality Weekly Report. October 18, 1996; 45(41):877-883.
-
Centers for Disease Control and Prevention. Web-based Injury Statistics Query and Reporting System (WISQARS). Available at: http://www.cdc.gov/ncipc/wisqars. Accessed May 18, 2004.
-
Rubenstein LZ, Josephson KR, Robbins AS. Falls in the nursing home. Annals of Internal Medicine. September 15, 1994; 121(6):442-451.
-
Alexander BH, Rivara FP, Wolf ME. The cost and frequency of hospitalization for fall-related injuries in older adults. American Journal of Public Health. July 1992; 82(7):1020-1023.
-
Murphy SL. Deaths: Final data for 1998. National Vital Statistics Report. July 24, 2000; 48(11):1-105.
-
Cooper C, Campion G, Melton LJ 3rd. Hip fractures in the elderly: A world-wide projection. Osteoporosis International. November 1992; 2(6):285-289.
-
Scott JC. Osteoporosis and hip fractures. Rheumatic Diseases Clinics of North America. August 1990; 16(3):717-740.
-
Wilkins K. Health care consequences of falls for seniors. Health Reports. Spring 1999; 10(4):47-55(ENG); 47-57(FRE).
-
Wolinsky FD, Fitzgerald JF, Stump TE. The effect of hip fracture on mortality, hospitalization, and functional status: A prospective study. American Journal of Public Health. March 1997; 87(3):398-403.
-
Hall SE, Williams JA, Senior JA, Goldswain PR, Criddle RA. Hip fracture outcomes: Quality of life and functional status in older adults living in the community. Australian and New Zealand Journal of Medicine. June 2000; 30(3):327-332.
-
Popovic JR. 1999 National Hospital Discharge Survey: annual summary with detailed diagnosis and procedure data. Vital and Health Statistics 13. September 2001(151):i-v, 1-206.
-
Magaziner J, Hawkes W, Hebel JR, et al. Recovery from hip fracture in eight areas of function. Journals of Gerontology A: Medical Sciences. September 2000; 55(9):M498-507.
-
Wolf SL, Barnhart HX, Kutner NG, McNeely E, Coogler C, Xu T. Reducing frailty and falls in older persons: An investigation of Tai Chi and computerized balance training. Atlanta FICSIT Group. Frailty and Injuries: Cooperative Studies of Intervention Techniques. Journal of the American Geriatrics Society. May 1996; 44(5):489-497.
-
Steinberg M, Cartwright C, Peel N, Williams G. A sustainable programme to prevent falls and near falls in community dwelling older people: Results of a randomised trial. Journal of Epidemiology and Community Health. March 2000; 54(3):227-232.
-
Tinetti ME, Baker DI, McAvay G, et al. A multi-factorial intervention to reduce the risk of falling among elderly people living in the community. New England Journal of Medicine. September 29, 1994; 331(13):821-827.
-
Wagner EH, LaCroix AZ, Grothaus L, et al. Preventing disability and falls in older adults: A population-based randomized trial. American Journal of Public Health. November 1994; 84(11):1800-1806.
-
Ray WA, Taylor JA, Meador KG, et al. A randomized trial of a consultation service to reduce falls in nursing homes. Journal of the American Medical Association. August 20, 1997; 278(7):557-562.
-
Close J, Ellis M, Hooper R, Glucksman E, Jackson S, Swift C. Prevention of falls in the elderly trial (PROFET): A randomised controlled trial. Lancet. January 9, 1999; 353(9147):93-97.
-
Chang JT, Morton SC, Rubenstein LZ, et al. Interventions for the prevention of falls in older adults: Systematic review and meta-analysis of randomised clinical trials. British Medical Journal. March 20, 2004; 328(7441):680.
-
Cumming RG. Epidemiology of medication-related falls and fractures in the elderly. Drugs and Aging. January 1998; 12(1):43-53.
-
Gillespie LD, Gillespie WJ, Cumming R, Lamb SE, Rowe BH. Interventions for preventing falls in the elderly. Cochrane Database of Systematic Reviews. 2000(2):CD000340.
-
Hill-Westmoreland EE, Soeken K, Spellbring AM. A meta-analysis of fall prevention programs for the elderly: How effective are they? Nursing Research. January-February 2002; 51(1):1-8.
-
Chang JT, Morton SC, Rubenstein LZ, et al. Interventions for the prevention of falls in older adults: Systematic review and meta-analysis of randomised clinical trials. British Medical Journal. March 20, 2004; 328(7441):680.
-
Russell JN, Hendershot GE, LeClere F, Howie LJ, Adler M. Trends and differential use of assistive technology devices: United States, 1994. Advance Data. November 13, 1997(292):1-9.
-
Kutty NK. Demand for home modifications: A household production function approach. Applied Economics. 1999; 31(10):1273-1281.
-
Aissaoui R, Boucher C, Bourbonnais D, Lacoste M, Dansereau J. Effect of seat cushion on dynamic stability in sitting during a reaching task in wheelchair users with paraplegia. Archives of Physical Medicine and Rehabilitation. February 2001; 82(2):274-281.
-
Fuhrer MJ. Assistive technology outcomes research: Challenges met and yet unmet. American Journal of Physical Medicine and Rehabilitation. July 2001; 80(7):528-535.
-
Rosenthal MJ, Felton RM, Hileman DL, Lee M, Friedman M, Navach JH. A wheelchair cushion designed to redistribute sites of sitting pressure. Archives of Physical Medicine and Rehabilitation. March 1996; 77(3):278-282.
-
Lyons RA, Sander LV, Weightman AL, et al. Modification of the home environment for the reduction of injuries. Cochrane Database of Systematic Reviews. 2003; 4(CD003600).
-
Kutty NK. The production of functionality by the elderly: A household production function approach. Applied Economics. 2000; 32(10):1269-1280.
-
Mann WC, Ottenbacher KJ, Fraas L, Tomita M, Granger CV. Effectiveness of assistive technology and environmental interventions in maintaining independence and reducing home care costs for the frail elderly. A randomized controlled trial. Archives of Family Medicine. May-June 1999; 8(3):210-217.
-
Chen LK, Mann WC, Tomita MR, Burford TE. An evaluation of reachers for use by older persons with disabilities. Assistive Technology. 1998; 10(2):113-125.
-
Romer AL, Hammes BJ. Communication, trust, and making choices: Advance care planning four years on. Journal of Palliative Medicine. April 2004; 7(2):335-340.
-
Hogan C, Lynn J. Medicare beneficiaries' costs and use of care in the last year of life. Washington, DC: Medicare Payment Advisory Commission; May 2000; 00-1.
-
Hanson LC, Rodgman E. The use of living wills at the end of life. A national study. Archives of Internal Medicine. May 13, 1996; 156(9):1018-1022.
-
Nolan MT. Could lack of clarity in written advance directives contribute to their ineffectiveness? A study of the content of written advance directives. Applied Nursing Research. February 2003; 16(1):65-69.
-
Hammes BJ. Update on Respecting Choices four years on. Innovations in End-of-Life Care. 2003; 5(2).
-
Investigators TSP. A controlled trial to improve care for seriously ill hospitalized patients. The study to understand prognoses and preferences for outcomes and risks of treatments (SUPPORT). Journal of the American Medical Association. November 22-29 1995; 274(20):1591-1598.
-
Gordon NP, Shade SB. Advance directives are more likely among seniors asked about end-of-life care preferences. Archives of Internal Medicine. April 12, 1999; 159(7):701-704.
-
Teno JM, Licks S, Lynn J, et al. Do advance directives provide instructions that direct care? SUPPORT Investigators. Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatment. Journal of the American Geriatrics Society. April 1997; 45(4):508-512.
-
Hammes BJ, Rooney BL. Death and end-of-life planning in one midwestern community. Archives of Internal Medicine. February 23, 1998; 158(4):383-390.
-
U.S. Department of Health and Human Services. Healthy People 2010, with Understanding and Improving Health and Objectives for Improving Health. Vol 2. 2nd ed. Washington, DC: U.S. Government Printing Office; 2000.
-
Newman SJ. Housing policy and home-based care. Milbank Quarterly. 1995; 73(3):407-441.
-
Agree EM, Freedman VA, Sengupta M. Factors influencing the use of mobility technology in community-based long-term care. Journal of Aging and Health. 2004; 16(2):267-307.
-
National Heart Lung and Blood Institute. National Institutes of Health. Data Fact Sheet: Congestive Heart Failure in the United States: A New Epidemic. Available at: http://library.thinkquest.org/27533/facts.html?tqskip1=1. Accessed August 2004.
-
Kass-Bartelmes BL, Hughes R, Rutherford MK. Advance care planning: Preferences for care at the end of life. Research in Action. March 2003; 12.
-
Arday DR, Lapin P, Chin J, Preston JA. Smoking patterns among seniors and the Medicare stop smoking program. Journal of the American Geriatrics Society. October 2002; 50(10):1689-1697.
-
Bruce ML, Seeman TE, Merrill SS, Blazer DG. The impact of depressive symptomatology on physical disability: MacArthur studies of successful aging. American Journal of Public Health. November 1994; 84(11):1796-1799.
-
Gallo JJ, Rabins PV, Lyketsos CG, Tien AY, Anthony JC. Depression without sadness: Functional outcomes of nondysphoric depression in later life. Journal of the American Geriatrics Society. 1997; 45(5):570-578.
-
Penninx BW, Guralnik JM, Ferrucci L, Simonsick EM, Deeg DJ, Wallace RB. Depressive symptoms and physical decline in community-dwelling older persons. Journal of the American Medical Association. June 3, 1998; 279(21):1720-1726.
-
U.S. Census Bureau. U.S. Interim Projections by Age, Sex, Race, and Hispanic Origin. Author. May 18, 2004. Available at: http://www.census.gov/ipc/www/usinterimproj/. Accessed August 10, 2004.
-
Freedman VA, Martin LG. Contribution of chronic conditions to aggregate changes in old-age functioning. American Journal of Public Health. 2000; 90(11):1755-1760.
-
DiPietro L. Physical activity in aging: Changes in patterns and their relationship to health and function. Journals of Gerontology A. October 2001; 56 Spec No 2: 13-22.
-
Olfson M, Marcus SC, Druss B, Elinson L, Tanielian T, Pincus HA. National trends in the outpatient treatment of depression. Journal of the American Medical Association. January 9, 2002; 287(2):203-209.
-
Harman JS, Crystal S, Walkup J, Olfson M. Trends in elderly patients' office visits for the treatment of depression according to physician specialty: 1985-1999. Journal of Behavioral Health Services and Research. July-September 2003; 30(3):332-341.
-
Newman SJ. The living conditions of elderly Americans. Gerontologist. February 2003; 43(1):99-109.
-
McCullough PA, Philbin EF, Spertus JA, Kaatz S, Sandberg KR, Weaver WD. Confirmation of a heart failure epidemic: Findings from the Resource Utilization Among Congestive Heart Failure (REACH) study. Journal of the American College of Cardiology. January 2, 2002; 39(1):60-69.
-
Levy D, Kenchaiah S, Larson MG, et al. Long-term trends in the incidence of and survival with heart failure. New England Journal of Medicine. October 31, 2002; 347(18):1397-1402.
-
Lynn J, Schall M, Milne C, Nolan K, Kabcenell A. Quality improvements in end of life care: Insights from two collaboratives. Joint Commission Journal on Quality Improvement. 2000; 26(5):254-267.
-
National Coalition on Health Care, Institute for Healthcare Improvement. Promises to Keep: Changing the Way We Provide Care at the End of Life. Washington, DC: Author; October 2000.
-
Bookbinder M, Romer AL. Raising the standard of care for imminently dying patients using quality improvement. Journal of Palliative Medicine. 2002; 5(4):635-644.
-
Lynn J, Schuster JL, Kabcenell A. Improving Care for the End of Life: A Sourcebook for Health Care Managers and Clinicians. New York, NY: Oxford University Press; 2000.
-
Hickman SE, Tolle SW, Brummel-Smith K, Carley MM. Use of the physician orders for life-sustaining treatment program in Oregon nursing facilities: Beyond resuscitation status. Journal of the American Geriatrics Society. September 2004; 52(9):1424-1429.
-
Ferrucci L, Guralnik JM, Studenski S, Fried LP, Cutler GB, Jr., Walston JD. Designing randomized, controlled trials aimed at preventing or delaying functional decline and disability in frail, older persons: A consensus report. Journal of the American Geriatrics Society. April 2004; 52(4):625-634.
-
Stuck A, Egger M, Hammer A, Minder C, Beck J. Home visits to prevent nursing home admission and functional decline in elderly people: Systematic review and meta-regression analysis. Journal of the American Medical Association. February 27, 2002; 287(8):1022-1028.
-
Linstone HA, Turoff M, eds. The Delphi Method--Techniques and Applications. Reading, MA: Addison-Wesley; 1975.
NOTES
-
To fully take into account the effects of interventions that alter not only illness trajectories but also the timing of death, we must pick a reasonable number of years to represent a complete lifetime. We are not suggesting as some have (e.g., Fries and others) that a limit exists, only use this figure (100 years) to facilitate comparisons over time in the illustration. The logic of the framework is not altered if we pick 100, 120 or some other limit.
-
An effect size of 0.2 or less was considered weak, between 0.2 and 0.8 moderate, and above 0.8 strong. An odds ratio of 1.2 or less was considered weak, up to 1.8 moderate, and over 1.8 strong.
-
Unpublished tabulations from the 1999 National Long-Term Care Survey.
-
Unpublished tabulations from the 1999 National Long-Term Care Survey.
-
We recognize that many of the interventions can be targeted at multiple junctures in the disablement process--for example, smoking cessation may be pursued to avoid disease onset (although lifetime smokers generally enter late-life with multiple chronic illnesses) or to manage disease; home modifications may be installed in an effort to avoid disability or to promote recovery from dependence.
-
In all cases, we make the simplifying assumption of a stable population in which entering cohorts are of the same size. Under that condition, the experience of a cohort followed until death will also reflect the experience of cross-section of the population age 65 or older. In fact, the cross-sectional outcome in a real population would be highly sensitive to changes in the size of entering cohorts.
-
We acknowledge that those who do not develop organ failure will be exposed to the risk of later life cancers, such as late onset prostate cancer, but such cancers typically do not behave like early onset cancers and are unlikely to alter the ultimate trajectory.
FIGURES AND TABLES
| FIGURE 1. Illustration of Functional Ability Before Death for Three Illness Trajectories |
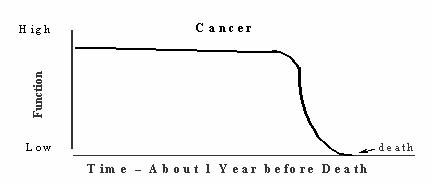 |
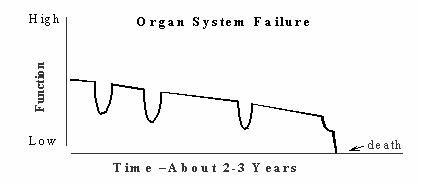 |
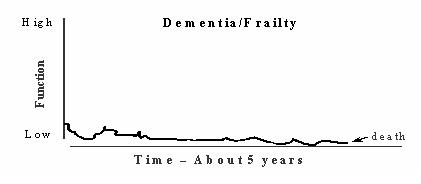 |
| FIGURE 2. Illustration of Functional Trajectories, Disability, and Death from Age 65 through 100 |
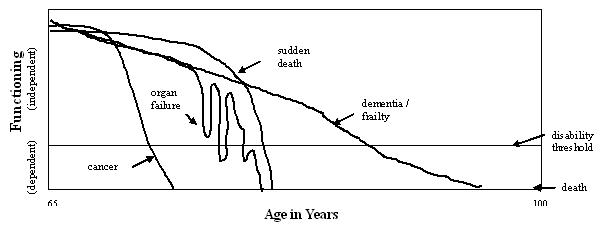 |
| FIGURE 2b. Illustration of Disease, Functional Limitation, Disability, and Death from Age 65 through 100, With and Without Interventions |
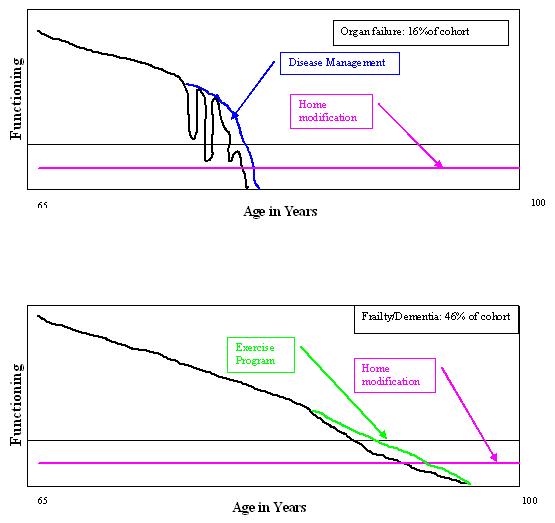 |
| FIGURE 3. Proportion of Individual Lifetime (Ages 65-100) and Years Lived in Each State: 3 Baseline Illustrations |
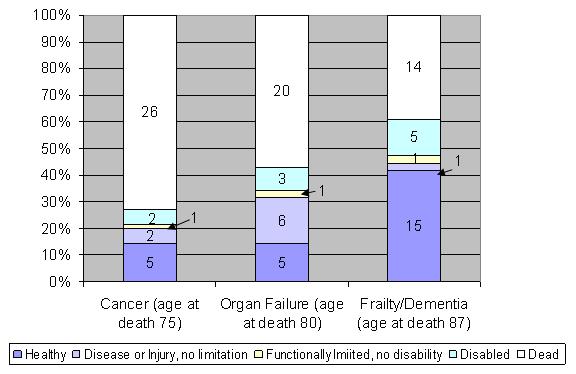 |
| FIGURE 4. Proportion of Cohorts Remaining Lifetime Spent in Each State: 1 Baseline Illustration and 2 Intervention Illustrations |
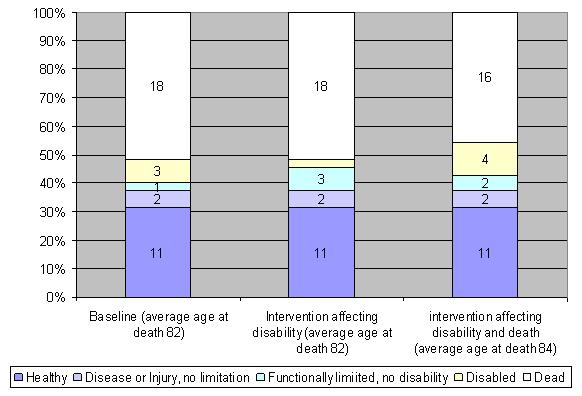 |
| FIGURE 5. Point-in-Time Distribution of Population by Disease/Disability State, by Age |
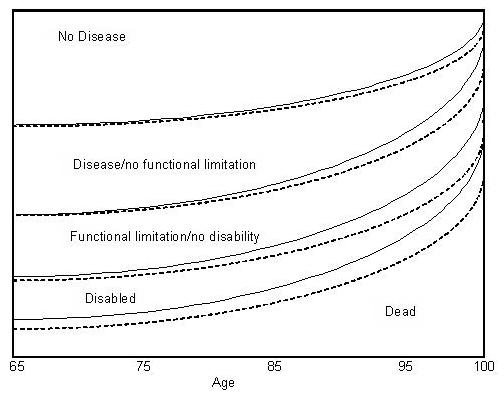 |
| TABLE 1. Illustrative Scenarios to Achieve 1% Decrease in Disability Prevalence in 1 Year | |||
| Intervention Target(Number in Age Group in Millions; % in with Disability) | Relative Risk of Disability Given Intervention(Number Targeted in Millions) | ||
| % of Age Group Affected | |||
| 100% | 50% | 25% | |
| Incidence among 65-74 years olds (18 m; 17.5%) | 0.90 (14.9m) | 0.8 (7.4m) | 0.6 (3.7m) |
| Recovery among 75-84 year olds (12 m; 40%) | 1.25 (4.8m) | 1.5 (2.4m) | 2 (1.2m) |
| TABLE 2. Assumptions for Simulation | |||||
| % Distribution in Population | Est. Population Size (in million) | Expected Years Lived | |||
| Active | Disabled | Total | |||
| Cancer | 22.0 | 7.7 | 7.5 | 2.0 | 9.5 |
| Organ Failure | 16.0 | 5.6 | 12.0 | 3.0 | 15.0 |
| Frailty/Dementia | 46.0 | 16.1 | 17.0 | 5.0 | 22.0 |
| Other | 16.0 | 5.6 | 11.0 | 0.5 | 11.5 |
| TABLE 3. Results of Simulation Designed to Demonstrate Long-Term High-Impact Effects | ||||
| Baseline | Large Reduction in Disabilityfor Cancer and Organ Failure1 | Modest Reduction in Disabilityfor Frailty/Dementia2 | Accelerated Increase inYears Without Disability3 | |
| Stable Population Disability Prevalence | 20.1% | 16.1% | 16.1% | 16.1% |
| Expected years with disability | 3.3 | 2.7 | 2.7 | 3.3 |
| Expected years without disability | 13.2 | 13.8 | 13.8 | 17.2 |
| Total life expectancy | 16.5 | 16.5 | 16.5 | 20.5 |
| ||||
| TABLE 4. Comparisons of Illustrative Interventions | |||||||
| Risk Factor/Intervention | Short-Term Considerations | Additional Long-Term Considerations | |||||
| Estimated Size of Target Population (Millions) | Stage of Disablement Process at which Intervention is Targeted (Type of Prevention) | Effectiveness in Altering: | Trends in Age-Specific Rates of Risk Factor | Primary Targeted Trajectory (Competing Risk) | Effects of Intervention on Mortality | ||
| Risk Factor Distributions | Risks of Disability | ||||||
| Smoking/ Cessation | 3.3 | Disease onset (primary) | Modest in adult population (1.7 relative risk of cessation) | Unknown | Decreasing | Cancer, organ failure (frailty/ dementia) | Large |
| Inactivity/ Exercise | 18 | Disease onset and disease management (primary, secondary) | Modest (0.5-0.7 relative risk of disability given exercise) | Modest | Decreasing | Frailty/ dementia | Possibly small to moderate |
| CHF Flareups/ CHF Management | 3 | Disease management (secondary) | Wide range of effects on hospitalization and hospital days | Unknown | Increasing | Organ failure (frailty/ dementia) | Small to none |
| Unrecognized/ Untreated Depression/ Screening and Treatment | 10 | Disease management (secondary) | Modest (1.5-1.8 increased risk of remission) | Small to modest | Treatment increasing | All | Possibly |
| Fall/ Fall Prevention | 12 | Disease management (secondary) | Modest (0.5-0.7 relative risk of falling) | Potentially large | Decreasing | Frailty/ dementia | Possibly small |
| Environmental Barrier/ AT or Home Modification | 5 to 17 | Disability onset/recovery (secondary, tertiary) | Not adequately tested | Not adequately tested | Increasing dramatically | All | Possibly very small |
| Severely Ill with No Advance Care Plan/ Advance Care Planning | 1.6 | End of life | Currently not effective | None | Decreasing | All | No |
| TABLE 5. Results of Simulation Designed to Demonstrate Long-Term Effects of Interventions | ||||||||||
| Baseline | Trajectory Shift | Disease Management | Reduce Environmental Demand By | Mortality Only | ||||||
| Reduce Cancer Trajectory by Half | Reduce Organ Failure Trajectory by Half | Reduce Both Cancer & Organ Failure by Half | Slow Frailty/ Dementia --No Mortality Effect | Improve Organ Failure Management --No Mortality Effect | Smoking Cessation & Extension of Life | 25% | 5% | Reduce Lingering Disability Among Frailty Dementia by One Month | ||
| Stable Population Disability Prevalence | 20.1% | 20.0% | 20.1% | 20.0% | 17.3% | 19.4% | 21.8% | 15.8% | 19.2% | 19.9% |
| Expected Years with Disability | 3.3 | 3.5 | 3.4 | 3.6 | 2.8 | 3.2 | 4.0 | 2.6 | 3.2 | 3.3 |
| Expected Years Without Disability | 13.2 | 13.9 | 13.4 | 14.3 | 13.6 | 13.4 | 14.4 | 13.8 | 13.3 | 13.2 |
| Total Life Expectancy | 16.5 | 17.4 | 16.8 | 17.8 | 16.5 | 16.6 | 18.4 | 16.5 | 16.5 | 16.4 |
| TABLE A-1. Rankings of 12 Interventions with Respect to Short-Term Disability, Long-Term Disability, Length of Life, and Number of People Potentially Affected | ||||
| Short-Term Disability | Long-Term Disability | Length of Life | Number of People | |
| Implement Depression Screening | 1 | 4 | 6 | 5 |
| Modify Homes | 2 | 6 | 9 | 7 |
| Implement Good Chronic Disease Care | 2 | 2 | 3 | 2 |
| Implement Fall Prevention Systems | 2 | 7 | 7 | 6 |
| Improve Exercise | 5 | 1 | 1 | 1 |
| Encourage Stroke Prevention | 6 | 3 | 4 | 4 |
| Provide Assistive Devices | 7 | 9 | 10 | 10 |
| Improve Diet | 8 | 5 | 5 | 3 |
| Provide More Organ and Joint Replacements | 9 | 10 | 8 | 11 |
| Encourage Smoking Cessation | 10 | 8 | 2 | 8 |
| Implement Widespread Care Planning | 11 | 11 | 10 | 9 |
| Provide Cognitive Training | 12 | 12 | 12 | 11 |
| TABLE A-2. Patterns of High Ranking Interventions | ||||
| Ranking Pattern | Outcome | |||
| Short-Term Disability | Long-Term Disability | Length of Life | Number of People | |
| Ranking | ||||
| Ranks High on All 4 Outcomes | ||||
| Implement Good Chronic Disease Care* | 2 | 2 | 3 | 2 |
| Ranks High on 3 Outcomes | ||||
| Improve Exercise* | 1 | 1 | 1 | |
| Encourage Stroke Prevention | 3 | 4 | 4 | |
| Ranks High on 2 Outcomes | ||||
| Implement Depression Screening* | 1 | 4 | ||
| Ranks High on 1 Outcome | ||||
| Modify Homes* | 2 | |||
| Implement Fall Prevention Systems* | 2 | |||
| Encourage Smoking Cessation | 2 | |||
| Improve Diet | 3 | |||
| Ranks High on None | ||||
| Implement Widespread Care Planning* | ||||
| Provide Cognitive Training | ||||
| Provide More Organ and Joint Replacements | ||||
| Provide Assistive Devices* | ||||
| * Indicates intervention recommended for literature review. | ||||