
Brenda C. Spillman, Eva H. Allen and Anna Spencer
Urban Institute
Printer Friendly Version in PDF Format (65 PDF pages)
ABSTRACT
This report presents findings from the first three years of the five-year evaluation of Medicaid health homes, a new integrated care model authorized in Social Security Act Section 1945 and created by Section 2703 of the Affordable Care Act. The model is designed to target high-need, high-cost beneficiaries with chronic conditions or serious mental illness. The Urban Institute is conducting the evaluation, which will conclude in October 2016. The first three years of the evaluation focus on the structure of health homes and implementation issues. Quantitative analysis in the last two years of the evaluation will assess the impact on quality, cost, utilization patterns, and health outcomes. This evaluation will assess: (a) the care models and processes states are using; (b) the extent to which health homes result in increased monitoring and care coordination; and (c) whether these models result in better care quality; patient experience; reduced hospital, skilled nursing facility, and emergency department use; lower costs; and clinical outcomes.
The study evaluates 13 Medicaid Health Home programs created by State Plan Amendments (SPAs) approved in 11 states; these include two SPAs each for Rhode Island and Missouri, and one SPA each for North Carolina, Oregon, New York, Alabama, Iowa, Ohio, Wisconsin, Idaho, and Maine. This report focuses on providers' experiences with the implementation of program requirements, provision of health home services, and use of health information technology (HIT).
Findings from the evaluation will inform a 2017 Report to Congress.
DISCLAIMER: The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS
I. INTRODUCTION
II. METHODS
III. PROVIDERS AND HEALTH HOME IMPLEMENTATION
- Health Home Delivery Models and Providers
- Health Home Enrollees
- Responsibility for Beneficiary Enrollment
- Requirements for Participating Providers
- Technical Assistance and Other Support
- Staffing
- Getting Paid for Health Home Services
IV. DELIVERING HEALTH HOME SERVICES
- Comprehensive Care Management
- Care Coordination and Health Promotion
- Comprehensive Transitional Care
- Community Supports and Social Services
V. HEALTH INFORMATION TECHNOLOGY
- Health Information Technology Requirements
- Challenges
- Health Information Exchanges
- Population Management
- Patient Portals
VI. CONCLUSIONS
VII. ENDNOTES
LIST OF BOXES
- BOX 1. State Medicaid Director Letter, November 2010
- BOX 2. Health Home Provider Expectations
- BOX 3. Required Health Home Services
- BOX 4. New York State Health Home HIT Standards
LIST OF FIGURES
- FIGURE 1: Health Home Evaluation States
LIST OF TABLES
- TABLE 1: Health Home Providers
- TABLE 2: Health Home Eligibility Criteria and Enrollment Status in the Evaluation States
- TABLE 3: Health Home Provider Requirements and Supports
- TABLE 4: Health Home Team Composition in Evaluation States
- TABLE 5: Initial Health Home Payment Systems and Reimbursement Level
ACRONYMS
The following acronyms are mentioned in this report.
| ABD | Aged, Blind or Disabled |
|---|---|
| ACA | Affordable Care Act |
| AIDS | Acquired Immune Deficiency Syndrome |
| ARCW | AIDS Resource Center of Wisconsin |
| ASO | AIDS Service Organization |
| BMI | Body Mass Index |
| CARF | Council on Accreditation of Rehabilitation Facilities |
| CBHC | Community Behavioral Health Center |
| CCD | Continuity of Care Document |
| CCNC | Community Care of North Carolina |
| CCT | Community Care Team |
| CEDARR | Comprehensive Evaluation, Diagnosis, Assessment, Referral, Re-evaluation |
| CFR | Code of Federal Regulations |
| CHIP | Children's Health Insurance Program |
| CMHC | Community Mental Health Center |
| CMHO | Community Mental Health Organization |
| CMS | HHS Centers for Medicare and Medicaid Services |
| COPD | Chronic Obstructive Pulmonary Disease |
| CPST | Community Psychiatric Support and Treatment |
| CVD | Cardiovascular Disease |
| CYSHCN | Children and Youth with Special Health Care Needs |
| DHITT | New York Division of Health Information Technology Transformation |
| EHR | Electronic Health Record |
| FFS | Fee-For-Service |
| FQHC | Federally Qualified Health Center |
| HHS | U.S. Department of Health and Human Services |
| HIE | Health Information Exchange |
| HIPAA | Health Insurance Portability and Accountability Act |
| HIT | Health Information Technology |
| HITECH | Health Information Technology for Economic and Clinical Health Act |
| HIV | Human Immunodeficiency Virus |
| MCO | Managed Care Organization |
| MCP | Managed Care Plan |
| NCQA | National Committee for Quality Assurance |
| PCMH | Patient-Centered Medical Home |
| PCNA | Patient Care Networks of Alabama |
| PCP | Primary Care Provider |
| PCPCH | Patient-Centered Primary Care Home |
| PCPCI | Patient-Centered Primary Care Institute |
| PHQ | Patient Health Questionnaire |
| PMP | Primary Medical Provider |
| PMPM | Per Member Per Month |
| PSYCKES | Psychiatric Services and Clinical Knowledge Enhancement System |
| PTAT | Patient Tier Assignment Tool |
| QE | Qualified Entity |
| RHC | Rural Health Clinic |
| RHIO | Regional Health Information Organization |
| SAMHSA | Substance Abuse and Mental Health Services Administration |
| SBIRT | Screening, Brief Intervention, Referral, and Treatment |
| SED | Serious Emotional Disturbance |
| SHIN-NY | Statewide Health Information Network for New York |
| SMD | State Medicaid Director |
| SMI | Serious Mental Illness |
| SPA | State Plan Amendment |
| SPMI | Serious and Persistent Mental Illness |
| TCM | Targeted Case Management |
EXECUTIVE SUMMARY
The Affordable Care Act includes several provisions intended to strengthen coordination of health care services with an ultimate goal of improving quality of care and lowering health care costs. One of these provisions is a Medicaid health home option, which allows states to provide integrated care for beneficiaries with multiple chronic conditions as an optional state Medicaid plan service. Although related to the patient-centered medical home (PCMH) model, the health home model is distinguished by its focus on high-cost, high-need populations; its emphasis on whole-person care, encompassing the integration of physical and behavioral health care services; and care management that extends beyond medical services to include nonclinical supports, such as transportation and housing. Another important distinction is that while primary care providers are key players, a wide variety of providers may serve as health homes, including hospitals, care management networks, and specialized providers such as home health agencies and community mental health centers (CMHCs). As of March 2015, 28 health home programs had been approved in 20 states.
The Urban Institute is conducting the long-term evaluation of health home implementation and outcomes for the U.S. Department of Health and Human Services (HHS) Assistant Secretary of Planning and Evaluation. The evaluation includes the first 13 programs in 11 states: two programs each in Missouri and Rhode Island, and one program each in Alabama, Idaho, Iowa, Maine, New York, North Carolina, Ohio, Oregon, and Wisconsin. This report examines providers' experience with the program, focusing on implementation challenges, provision of required services, and use of health information technology (HIT). Findings are drawn from review of background materials and each State Plan Amendment, as well as qualitative data collected during site visits and annual follow-up telephone interviews with state program staff, health home providers, consumer advocates, and other key stakeholders.
Providers and Health Home Implementation
States implementing the health home program have flexibility in choice of payment system, geographic coverage, conditions targeted, and eligible populations. Although health home designs and implementation contexts are varied, three distinct health home delivery models have emerged. Medical home-like programs in Idaho, Iowa, Missouri (primary care program), and Oregon are variations on or extensions of the PCMH. Specialty provider-based programs in Missouri (mental health program), Ohio, both Rhode Island programs, and Wisconsin center on entities that traditionally serve special-needs populations but integrate specialized care with primary care. Care management network programs in Alabama, Maine, New York, and North Carolina involve consortiums of care coordination entities, direct physical and mental/behavioral health care providers, social services agencies, and other community organizations.
To qualify for health home services, Medicaid beneficiaries must have two or more chronic conditions; one chronic condition and be at risk of developing another; or one serious and persistent mental health condition. Most states in the evaluation offer health home services to a broad range of beneficiaries, including both those with physical chronic and mental health conditions. Missouri created separate health home programs for Medicaid beneficiaries with physical chronic conditions and those with mental health conditions. Similarly, Rhode Island chose to implement two programs: one for children and youth with special-needs and another for adults with mental health illness. Ohio's program focuses on adults with mental health conditions and children with serious emotional disturbance, while Wisconsin's program is limited to Medicaid beneficiaries with HIV/AIDS.
In all but one state, providers receive enhanced payment for delivering health home services to eligible persons they are able to enroll in the program. States and providers generally share responsibility for identifying beneficiaries eligible for health home services and enrolling them in the program. State Medicaid departments use claims or administrative data to identify and assign beneficiaries who qualify for health home services to providers. In a few evaluation states, providers receive lists of eligible Medicaid beneficiaries and are responsible for locating, engaging, and enrolling health home participants. Most states also allow providers to refer patients to the health homes program, and in some states, member enrollment is entirely through provider referral, subject to state verification of eligibility. Eligibility determination can be challenging if data used is incomplete or inaccurate. The Medicaid population is traditionally difficult to engage, and providers may face additional challenges with tracking down and enrolling potential beneficiaries in the health home program.
In nearly all cases, providers choose to apply for designation as health homes. Health home providers are expected to meet specific qualifications established by the state and 11 core expectations for care coordination, service delivery, quality improvement, monitoring, and reporting identified in HHS Centers for Medicare and Medicaid Services guidance. State-specific criteria may include nationally recognized certifications, such as the National Committee for Quality Assurance, or other standards the state may approve. While some evaluation states have phased in or gradually increased certain provider requirements over time, others put stricter provider standards in place from the start of the program. The resulting variation in provider qualifications across evaluation states may affect the experience of care for patients and initial quality and cost outcomes.
To assist providers with the implementation of the health home program and practice transformation, all states have provided guidance and technical support, such as trainings, webinars, learning collaboratives, and on-site practice coaching. Health home providers have also used other practice transformation resources, such as those sponsored by national and local associations, commercial health systems, health foundations, and universities. Some states have partnered with local organizations to help oversee the implementation of the program and deliver technical assistance to providers. In general, providers that we interviewed found ample opportunities for training and assistance, though in a few states providers expressed a desire for more health home-specific guidance and topics.
Nine out of 13 health home programs in our evaluation mandate specific health home team composition while the remaining states are less prescriptive in health home team design. Despite the prominent focus on integration of care, only four out of 11 states specifically mandate that both primary care and behavioral/mental health care professionals are part of a health home team. Besides clinical personnel, such as physicians, psychiatrists, and nurses, health home care teams can be diverse, including diabetes educators, nutritionists, social workers, pharmacists, community health workers, transitional care professionals, substance abuse providers, vocational specialists, community integration specialists, school personnel, peer specialists, and housing assistance representatives. Care managers and care coordinators are viewed by many as key, but pharmacists and data managers are also frequently cited as critical members of the health home team.
The health home option provides a new reimbursement authority for expanded coordination and management of medical, behavioral, and nonclinical services. To support the health home implementation, states also receive 90% federal match for specific health home services provided during the first eight quarters of the program. Although states are encouraged to develop innovative payment methodologies, all but one program use some form of capitated per member per month payments. In a few states in our evaluation, providers find the payment procedures and systems set up to bill for services complex and administratively burdensome. Overall, the majority of providers we interviewed believe the health home payment rates are adequate to cover the cost of providing required health home services, but many feel that the payments are not sufficient to support the full cost of practice transformation, such as improving or adding electronic health records (EHRs) or hiring care managers.
Delivering Health Home Services
The six core health home services designed to improve care quality and reduce inappropriate emergency department use and hospital admissions are comprehensive care management; care coordination and health promotion; comprehensive transitional care; individual and family support services; linkage and referral to community and social support services; and use of HIT as feasible and appropriate. The health home model's patient-centered approach requires many providers to take on new roles or expand services they have been providing into new domains of care. It also requires an enhanced level of communication and interaction with other providers than is typical in the current delivery system. How well providers perform as health homes depends largely on their prior experience, ability to adapt to new routines, available infrastructure, and external support.
Comprehensive care management includes, among other activities, assessing each health home member's health risks and social service needs, conducting mental health and substance abuse screenings, developing and implementing a single care plan, and engaging enrollees in the care planning process. A challenge to continuity of care and comprehensive care management noted by both state officials and providers is gaps in Medicaid enrollment. Gaps occur when beneficiaries lose eligibility because they have to "spend-down" income to eligible levels, or they fail to renew their enrollment in a timely fashion. Health home services provided during periods of temporary Medicaid ineligibility may not be reimbursed, access to other services is impaired, and enrollment discontinuities also represent an administrative burden for providers who must monitor Medicaid eligibility and re-enroll health home participants who regain Medicaid eligibility.
Because individuals with multiple or complex chronic conditions tend to see numerous providers, communication across care settings and coordination of services is crucial to improving quality of care, primary prevention and health promotion, and reducing unnecessary utilization. Besides ensuring that providers involved in care are communicating with each other and with the patient, care coordination involves making referrals to appropriate services, scheduling appointments, following up on referrals and clinical results, and performing medication management. Specially trained staff, typically nurse care managers, referral coordinators, or care coordinators, direct and monitor services for health home enrollees. Prevention and health promotion activities center on health education and disease self-management for health home members, as well as providing, or coordinating, lifestyle interventions such as smoking cessation or nutritional counseling.
A required component of care coordination in health homes is integration of behavioral/mental and physical care for all patients, regardless of whether the program is targeting primarily mental or physical health conditions. Approaches to integration vary, largely based on providers' capacity and previous experience. Some health homes screen for either physical or behavioral/mental health conditions, refer patients to appropriate services in the community, and follow up on access and treatment. Others employ part-time or full-time primary care or behavioral health consultants, and others may co-locate primary care and behavioral health services in one setting. Both primary care and behavioral/mental health care providers report some challenges in integrating care and stress the importance of developing relationships with providers throughout the community.
Effective, high-quality transitional care, which consists of a broad range of services designed to ensure continuity of care and promote safe and timely transfer of patients from one care setting to another, particularly after hospital discharge, is critical to the well-being of chronically ill patients who may transition between care settings frequently. The ability of health home providers to assure transitional care is largely dependent on their working relationships and established communication arrangements with local hospitals and other facilities. Timely admission/discharge and emergency department visit notifications, whether furnished by inpatient facilities, managed care plans, or Medicaid offices, allow health homes to follow-up with their enrollees after discharge from a hospital or emergency department. Most health home providers, however, report notifications processes are still a work in progress and timely and complete alerts for health home beneficiaries are scarce. They are virtually nonexistent for dually eligible members for whom Medicare, not Medicaid, is the primary payer.
Health home providers are required to engage enrollees in their care and refer them to community resources, social services, and supports that can meet identified needs or help enrollees accomplish health-related goals. Providers who have historically linked their patients to social services and supports, such as CMHCs, generally are able to rely on established relationships, while primary care practices, for example, report having less experience and spending more time and resources developing necessary connections. The lack of stable housing and reliable transportation are common problems for many health home enrollees. Other nonclinical services health homes assist with include access to disease self-management education, food assistance, vocational training, and medical device procurement or upgrades. In a few states, peer support specialists are used to support health home members in disease self-management and lifestyle changes.
Health Information Technology
One of the requirements placed on health homes is use of HIT to link services, as feasible and appropriate. The language of the statute is vague and broad, recognizing that any stricter or more specific HIT requirements could limit the number of providers who would qualify to become a health home. HIT systems have been largely in developmental stages in most states, and even in states where HIT is widespread, there is considerable variation among individual providers in their use of HIT. This remains true still today, even as all states in our evaluation completed their two-year intervention period. State officials and providers alike agree that the use of HIT to link health home services is a work in progress, requiring attention, investment, and time to fully develop.
Six out of 11 evaluation states require that health homes have and use EHRs. In Idaho, New York, and Ohio, HIT standards were phased in over time, affording participating providers more flexibility in the acquisition and mastery of technology. The remaining states do not specifically mandate that health home practices adopt EHRs, although they are encouraged to do so. Few states mandate that health homes connect to a health information exchange (HIE) as it becomes available.
The acquisition of or upgrades to HIT infrastructure require substantial investment from practices, in dollars and staff time, which may present a barrier, particularly for small and independent clinics. Providers note that having personnel to handle state HIT requirements can be a challenge and that there are often no additional resources to hire staff with technical expertise. Common challenges for health homes that own and operate EHRs include EHRs that may not support care planning and documentation of nonclinical needs and services or allow input from external providers. Often, individual practices and hospitals use different EHR platforms that may not be compatible with each other, which hinders seamless electronic data-sharing between providers. Regulatory restrictions on sharing of sensitive data (e.g., HIPAA privacy rules or provisions in 42 CFR Part 2 guiding disclosure of substance abuse treatment) are also perceived by many providers as barriers to the exchange of patient data.
Health home providers in most states noted that inadequate support--financial and otherwise--was a hindrance to realizing health home HIT goals and requirements. Some health home providers have been able to participate in the Medicaid or Medicare EHR Incentive Programs, which provide federal funding to eligible providers for EHR adoption. Most mental health providers, however, are currently not eligible to participate in this program, making procurement of EHRs more challenging for these providers, particularly in states that require behavioral health homes to use EHRs and connect to an HIE (Missouri and Ohio). Only a few evaluation states have provided financial support or technical assistance to health home providers to facilitate the adoption of HIT. New York, for example, provided $15 million in HIT assistance specifically for health homes, including learning opportunities for developing and effectively using HIT.
The limited ability of health home providers to obtain timely notifications of hospital admissions and discharges and emergency department use hinders health homes in providing effective transitional care. While some health homes, particularly those directly affiliated with hospitals, receive admission or discharge information regularly, others are still developing relationships with hospitals and managed care organizations to exchange data. Even when formal or informal communications have been established, health home enrollees may visit hospitals outside the local area or hospitals with whom the health home has not established procedures, making notifications more challenging. Some states are attempting to leverage their HIEs to facilitate emergency department and hospital admission notifications, with varying success. Many health homes have developed various "work-arounds" to ensure timely information sharing, including faxes, phone calls, secure email, or in-person contact.
The 11 states in our evaluation have some HIE infrastructure in place, whether state-sponsored, regional, privately-funded, or some combination of the three, but the degree to which providers connect and use the information exchange is highly variable. In some states, HIE includes a range of functions, while other states' HIE capacity may be limited to direct secure messaging or patient record look-up. Infrastructure development and subscription costs are considered the main barriers to provider involvement in HIE, but generally low participation from provider partners is also discouraging many health homes from joining. Some states have in place existing infrastructure that substitutes for or supplements electronic data management and information exchange.
Population-based health care uses data systems, such as registries, to track patient care and monitor health status over time to assess patients' needs and improvements. To a large extent, health home providers we spoke to are actively engaged in tracking and monitoring their whole patient panel, and particularly high-risk patients, though several providers expressed the need for more resources to support data management. Most providers are generating their own patient reports and also receiving patient utilization data from the state, though the utility of state-furnished reports is variable.
Several health home provides have created patient portals, which enable patients to make an appointment, access information about medications, treatment, and care plan details, or send a secure message to their provider. However, patient participation in portals remains extremely low across the evaluation states, despite efforts by health homes to enroll more members. The barriers for patients may include unfamiliarity with technology, limited access to the Internet or data for smart phone users, and sometimes mistrust of technology in general and preference for talking to a real person or face-to-face.
Conclusions
This report focuses on the challenges Medicaid health home providers have faced in implementing the model and their progress in the development of processes and tools to support the model. As is true with the rollout of any initiative, some challenges have stemmed from adopting new program infrastructure and administrative processes, which in many cases presented organizational burden and lost productivity for participating providers and slowed down the pace of implementation. While health home providers generally reported having opportunities for training, collaborative learning, technical assistance, and other support, many noted the lack of financial resources to fund practice transformation and HIT infrastructure improvements. The majority of providers across our evaluation states have had at least some prior experience with the medical home model and care management, yet many encountered challenges with delivery of required health home services and changes in the approach to care. Communication between the health home providers, hospitals and other parts of the health care system is critical to comprehensive care management and coordination, integration of physical and mental/behavioral care, and effective transitional care, but we found that relationship-building has proved to be a challenging and slow process for many health homes. HIT systems in the evaluation states seem for the most part inadequate to support the full range of health home functions, including care coordination and integration, cross-site exchange of information, and documentation of nonclinical services. Despite these challenges, health home providers believe the model presents a better way of approaching care for their high-cost, high-need patients.
I. INTRODUCTION
The Medicaid health home option is one of several Affordable Care Act (ACA) provisions designed to improve the coordination of health care services, with the ultimate goal of improving the quality of care and reducing health care costs. Medicaid health homes is a new model of care, established in Section 2703 of the ACA, signed into law in 2010, and authorized by Section 1945 of the Social Security Act, that allows states to provide integrated care for beneficiaries with multiple chronic conditions as an optional state Medicaid plan service.1 The model's aims are closely related to the patient-centered medical home (PCMH) model. The health home model, however, is distinguished by its focus on high-cost, high-need populations and its emphasis on whole-person care, encompassing the integration of physical and behavioral health care services and care coordination that extends beyond medical services to include long-term services and social and community supports, such as transportation and housing (Box 1). Another important distinction is that while primary care providers (PCPs) are key players, a wide variety of providers may serve as health homes, including hospitals, care management networks, and specialized providers such as home health agencies and community mental health centers (CMHCs).
| BOX 1: State Medicaid Director Letter, November 2010 "The health home service delivery model is an important option for providing a cost-effective, longitudinal 'home' to facilitate access to an inter-disciplinary array of medical care, behavioral health care, and community-based social services and supports for both children and adults with chronic conditions." Cindy Mann |
Thus far, the U.S. Department of Health and Human Services (HHS), Centers for Medicare and Medicaid Services (CMS) have approved State Plan Amendments (SPAs) in 20 states to implement a total of 28 health home programs (see Figure 1).2 A recent survey conducted by the Kaiser Commission on Medicaid and the Uninsured found that another 18 states were planning to pursue the health home option in 2015 and that several states were expanding programs already in place or adding programs for additional populations.3
The Urban Institute is conducting the long-term evaluation of health home implementation and outcomes mandated in the ACA, under contract to the HHS Office of the Assistant Secretary of Planning and Evaluation. The evaluation includes the first 13 programs in 11 states approved by CMS (Figure 1). Profiles of each of the 11 states and an overview of the evaluation and early implementation findings are available in the second-year report.4
This third-year report examines issues for health home providers in the 13 programs, with a focus on implementation challenges, provision of required services, and use of health information technology (HIT). Findings are drawn from information collected during site visits and follow-up telephone interviews with state policymakers, health home providers, consumer advocates, and other stakeholders.
| FIGURE 1. Health Home Evaluation States |
|---|
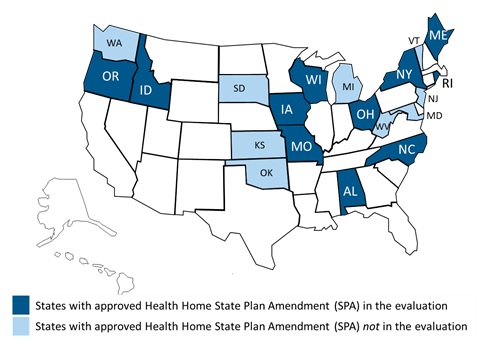 |
| SOURCE: CMS, State Health Home CMS Proposal Status, effective March 2015. |
II. METHODS
The five-year long-term evaluation of Medicaid health home programs in selected states began on October 1, 2011. The aims of the evaluation are to assess: (1) what models, providers, and processes states are choosing for health homes; (2) the extent to which state health home designs result in increased monitoring and coordination across clinical and nonclinical domains of care; and (3) whether the models result in better quality of care and outcomes, specifically, reduced use of hospitals, skilled nursing facilities, and emergency departments, and lower costs. The analysis period for each program is defined as the initial eight quarters during which an enhanced federal match for health home services was in place. The first three years of the evaluation activities have focused on qualitative and quantitative data collection, and the final two years will focus on conducting quantitative analyses, and preparation of findings for use in the Secretary's 2017 Report to Congress, required in Section 2703 of the ACA.
Qualitative activities in the first three years of the evaluation, findings of which inform this report, began with review of background materials and each SPA, and development of profiles summarizing the design and implementation context of each health home program included in the evaluation. We conducted site visits during the initial year of each program and are conducting annual follow-up telephone interviews with key informants.
At a minimum, informants we interviewed during site visits included the State Medicaid Director (SMD), the health home program director, a HIT officer, officials involved in any state evaluation of the initiative, selected participating providers, and patient and provider advocacy groups. To select providers for site visits and follow-up interviews, we asked state program officials to identify health home providers they considered representative and whose patient populations included a large enough proportion of enrollees to provide sufficient experience. We included sites ranging from sole provider rural primary care practices to large urban clinics to capture a range of experience with the new responsibilities inherent in the health home model and different patient populations.
Protocols for site visits focused on state choices of target populations and providers, the design of programs, the rationale for the design, fundamental elements of structure and processes established, and implementation issues. Follow-up protocols addressed implementation progress and challenges and any contemplated changes in program features. Topics covered included eligibility determination and enrollment of beneficiaries, provider experience with implementation and delivery of required services, payment structure and processes, training and technical assistance, availability of data and reporting requirements, use of HIT, and sustainability of the model. Protocols were customized as needed to reflect unique characteristics and evolution of each health home program. We coded interview notes from site visits and follow-up calls using NVivo (a qualitative research software program) to identify common patterns and themes and synthesize the collected information.
Additional detail about qualitative activities and methods, the quantitative component of the evaluation, and the evaluation design and timeline are available in the second-year report, along with detailed profiles for each state.5
III. PROVIDERS AND HEALTH HOME IMPLEMENTATION
Medicaid health homes are designed to transform the current fragmented system of care into a more integrated and coordinated system that can better meet the care needs of high-cost, high-need beneficiaries. Our early findings suggest that although health home designs and implementation contexts are varied, states and health home providers within those states are facing many of the same implementation challenges. These challenges arise from the need to develop new practice patterns, processes, and systems to improve care coordination, and to adopt or adapt HIT to support this work.
Evidence from studies of the PCMH indicates that the success of policies and reforms to improve health outcomes and constrain costs depends, in large part, on the ability of providers to transform the way care is delivered and translate the vision into action. In an evolving health care environment, providers must rapidly adopt new approaches to patient care, a sometimes-challenging task.6 Engagement of provider stakeholders in policy and program design, substantial financial support, reasonable expectations, and technical assistance and educational resources are needed to help providers implement and operationalize new programs or redesign existing systems of care.
Health Home Delivery Models and Providers
CMS allows states considerable latitude in designing their health home programs, in terms of the range of qualifying conditions they may choose to focus on, how health homes services are defined and reimbursed, and designated provider types. As a result, there is a considerable diversity among health home programs. Most states in our evaluation have built on prior experience with medical homes and care management initiatives, leveraging the current provider infrastructure, and continuing or expanding existing services. Even so, most states reported wide variation across individual providers in readiness and progress in meeting health home expectations, particularly in states with programs centered on PCPs.
Health home programs in the evaluation states fall into one of three general provider categories: (1) medical homes and extensions; (2) specialty provider-based; and (3) care management networks. Programs using medical home-like models and care management network models generally serve relatively broad populations, often primarily beneficiaries with chronic physical conditions, while those using specialty providers tend to focus on narrow populations they have traditionally served.
Table 1 shows the designated providers for each of the 13 programs, grouped by provider category and ordered by program effective date. Eight of the 11 states in our evaluation offer health home services statewide. The remaining three are limited, at least initially, to specific geographic areas. Alabama started in one 21-county service area and expanded its program statewide in April 2015. Ohio started in selected counties in the state but also plans to expand statewide. In Wisconsin, where the program focuses entirely on beneficiaries with HIV/AIDS, the coverage area is determined by access to a single specialized provider.
| TABLE 1. Home Health Providers | |||
|---|---|---|---|
| State/ Program | Designated Providers | Number of Providers/ Service Locations1 | Geographic Coverage |
| Patient-Centered Medicaid Home and Extensions | |||
| Oregon | PCPCHs | 198 PCPCHs | Statewide |
| Missouri (Primary care) | FQHCs, RHCs, and primary care clinics operated by hospitals | 18 FQHCs in 56 sites 6 hospitals, 14 clinics, 14 RHCs | Statewide |
| Iowa | Medicaid-enrolled providers, including primary care practices, CMHCs, FQHCs, RHCs | 32 provider organizations in 71 service locations | Statewide |
| Idaho | Medicaid-enrolled providers, including primary care practices, CMHCs, community health centers, home health agencies | 28 provider organizations in 55 service locations | Statewide |
| Specialty Provider-Based | |||
| Rhode Island (Children & youth with special health care needs) | Comprehensive Evaluation, Diagnosis, Assessment, Referral, Re-evaluation (CEDARR) Family Centers | 4 CEDARR centers | Statewide |
| Rhode Island (Mental health) | CMHOs | 6 CMHOs and 2 mental health clinics | Statewide |
| Missouri (Mental health) | CMHCs | 28 CMHCs with 120 clinics | Statewide |
| Ohio | Community Behavioral Health Centers (CBHCs) | 6 CBHCs | 5 counties |
| Wisconsin | AIDS Service Organizations (ASOs) | 1 ASO | 4 counties |
| Care Management Networks | |||
| North Carolina | CCNC and affiliated Medicaid-enrolled PCPs | 1,838 providers | Statewide |
| New York | Networks of Medicaid-enrolled providers assembled by lead organizations. An array of providers may serve as a lead organization, including hospitals, MCPs, PCPs, home health agencies, and substance abuse treatment facilities | 32 lead provider organizations operating in 48 service locations | Statewide |
| Alabama | PCNAs and Medicaid-enrolled PMPs | 3 PCNAs and 186 providers | 4 regions comprising 21 counties |
| Maine | CCTs and Medicaid-enrolled PCPs | 10 CCTs and 165 providers | Statewide |
SOURCE: Information obtained from review of CMS-approved SPAs.
| |||
Medical home-like programs follow three paths. Idaho and Oregon have built on existing medical home initiatives. (Oregon discontinued health homes as a distinct program within the medical home initiative at the end of September 2013 and withdrew its SPA effective July 31, 2014.) Iowa has used the health home model as a tool for establishing a broader medical home infrastructure. Missouri has relied on organizations already providing comprehensive care to underserved and vulnerable populations, specifically, federally qualified health centers (FQHCs), rural health clinics (RHCs), and hospital-owned primary care practices.
Specialty provider-based programs target beneficiaries with serious mental illness (SMI) served by CMHCs or organizations (Missouri, Ohio, and Rhode Island); children and youth with special health care needs (CYSHCN) served by existing specialized providers (Rhode Island); or beneficiaries with HIV/AIDS served by a single organization designed to serve them (Wisconsin).
| BOX 2: Health Home Provider Expectations Health home providers must be able to:
SOURCE: State Medicaid Director Letter Re: Health Homes for Enrollees with Chronic Conditions. |
Care management networks can provide a mechanism through which direct patient care providers can access coordination services that may not otherwise be available to them, as well as technical assistance or practice transformation resources. North Carolina used its existing care management networks, and Alabama and Maine adopted similar models, relying on care management teams collaborating with PCPs to manage the care of high-need beneficiaries. New York's model relies on a lead entity that assembles a network of provider partners who collectively have the expertise and capacity to coordinate and deliver all health home services, termed by the state a virtual "Health Home." Lead agencies may be hospitals, health and human services agencies, and other entities. For example, in Brooklyn County, lead agencies include the Maimonides Medical Center, Health and Hospitals Corporation, Community Health Care Network, and Institute for Community Living.7 The lead entity is responsible at a minimum for maintaining data, securing payment, and quality assurance.8
Regardless of the model chosen, designated providers or organizations are expected to meet specific provider qualifications established by the state and the 11 core expectations for coordinating and providing or facilitating access to comprehensive, patient-centered clinical and nonclinical services and supports shown in Box 2.9 The 11 expectations include providing, coordinating, and facilitating access to clinical and nonclinical services, developing a continuous quality improvement program, collecting and reporting data to assess population-level outcomes, and using HIT to link services and to facilitate communication among care team members and between the care team and beneficiaries. Our analyses indicate that in a few cases, the structures to accomplish the expectations are in place, but in most health homes, substantial investments of time and money to transform service delivery is required.
Health Home Enrollees
To qualify for health home services, Medicaid beneficiaries must have two or more chronic conditions; one chronic condition and be at risk of developing another, with risk defined by the state; or one serious and persistent mental health condition. Most states in the evaluation offer health home services to a broad range of beneficiaries, including both those with physical chronic conditions and mental health illness (Table 2). Missouri created separate health home programs for Medicaid beneficiaries with physical chronic conditions and those with serious mental health conditions. Three of the 11 states are focusing exclusively on narrow populations. In the programs covered by this evaluation, Rhode Island chose children and youth with special-needs and beneficiaries with serious and persistent mental illness (SPMI), later broadened to those with SMI. Ohio's program includes adults with SMI and children with serious emotional disturbance (SED), while Wisconsin's program is limited to Medicaid beneficiaries with HIV/AIDS.
Several of the 11 states have pursued new SPAs, not included in this evaluation, to deliver health home services to additional Medicaid populations. A new Rhode Island program, initiated in 2013, focuses on Medicaid enrollees with opioid addiction.10 Iowa, which included a broad chronic illness population in its initial program, has phased in a health home program for adults with SMI and children with SED beginning in 2013.11 Maine implemented behavioral health homes, also known as Stage B health homes, for eligible adults with SMI and children with SED in 2014.12 New York is in the process of developing health homes for children, with enrollment expected to begin in October 2015.13
| TABLE 2. Health Home Eligibility Criteria and Enrollment Status in the Evaluation States | |||
|---|---|---|---|
| State/ Program | Population Eligibility Criteria1 | Qualifying Conditions Covered1 | Estimated Enrollment2 |
| Patient-Centered Medical Homes and Extensions | |||
| Oregon |
| Mental health condition; substance use disorder; asthma; diabetes; heart disease; BMI over 25; BMI under age 20 at or above the 85th percentile; hepatitis C; HIV/AIDS; chronic kidney disease; chronic respiratory disease; cancer | 93,2533 |
| Missouri (Primary care) |
| Asthma; diabetes; heart disease; BMI over 25; tobacco use; developmental disabilities | 14,700 |
| Iowa |
| Mental health condition; substance use disorder; asthma; diabetes; heart disease; BMI over 25; hypertension; BMI over 85th percentile for pediatric population | 5,600 |
| Idaho |
| Mental health condition; asthma; diabetes | 9,500 |
| Specialty Provider-Based | |||
| Rhode Island (CYSHCN) |
| Mental health condition; asthma; diabetes; developmental disability; Down syndrome; Down syndrome and other intellectual disabilities; seizure disorders | 2,8553 |
| Rhode Island (Mental health) |
| Mental health condition | 6,7723 |
| Missouri (Mental health) |
| Mental health condition; substance use disorder; asthma; diabetes; heart disease; BMI over 25; developmental disability; tobacco use | 19,000 |
| Ohio |
| SPMI; SED | 12,000 |
| Wisconsin |
| HIV/AIDS | 190 |
| Care Management Networks | |||
| North Carolina |
| Blindness; chronic CVD; chronic pulmonary disease; congenital anomalies; chronic disease of the alimentary system; chronic endocrine and metabolic disease; chronic infectious disease; chronic mental and cognitive conditions; chronic musculoskeletal conditions; chronic neurological disorders | 559,8393 |
| New York |
| Mental health condition; substance use disorder; asthma; COPD; diabetes; heart disease; BMI over 25; HIV/AIDS; and other chronic conditions in major clinical risk group categories identified by the state | 158,4603 |
| Alabama |
| Mental health condition; substance use disorder; asthma; diabetes; heart disease; transplant recipients (within last 5 years); CVD; COPD; cancer; HIV; sickle cell anemia | 70,2063 |
| Maine |
| Mental health condition; substance use disorder; asthma; diabetes; heart disease; BMI over 25; tobacco use; COPD; hypertension; hyperlipidemia; developmental disabilities or autism spectrum disorders; acquired brain injury; seizure disorders; cardiac and circulatory congenital abnormalities | 50,000 |
| |||
Responsibility for Beneficiary Enrollment
In all but one state, providers receive enhanced payment for delivering health home services to eligible persons they are able to enroll in the program. States and providers generally share responsibility for identifying beneficiaries eligible for health home services, but for the most part, enrollment is primarily accomplished by health home providers. In Alabama, Maine, Missouri, New York, and Ohio, state Medicaid departments use claims or administrative data to identify and assign beneficiaries who qualify for health home services to providers. Health home eligibility algorithms consider diagnoses codes for selected qualifying conditions, but typically they also include other factors such as the number of hospital admissions or emergency department visits within a certain period, total cost of care, or enrollment in other case management programs. Generally, the identification process also takes into account existing beneficiary relationships with providers. North Carolina also uses claims and other data to identify beneficiaries eligible for health home services among the population served by its Community Care of North Carolina (CCNC), but the identification is largely administrative, since the state has made no health home-related changes in care delivery or management. North Carolina providers we spoke with were unaware of which specific patients were designated as health home enrollees.
In states other than North Carolina that use a central eligibility determination process, providers receive lists of eligible Medicaid beneficiaries and are responsible for locating, engaging, and enrolling health home participants--Idaho and New York, for example. Most states also allow providers to refer patients to the health homes program, and in some states, member enrollment is entirely through provider referral. Iowa, Oregon, Rhode Island, and Wisconsin require health home providers to identify prospective enrollees from among their existing client population or through referrals from other providers. In states where providers are responsible for enrollee identification, the state verifies and confirms enrollee eligibility. Missouri began with state identification and automatic assignment of eligible beneficiaries with the right to opt-out or choose another health home provider, but has moved to a mixed system with both state assignments and provider identification.
Eligibility determination and enrolling of eligible individuals comes with a set of challenges. Data used to make eligibility determinations may not always be complete and accurate. As a result, potential enrollees may be missed or impossible for a provider to track down in cases where contact information is missing or outdated. Recognizing that patient engagement can be challenging and time-consuming, New York pays providers 80% of the health home per member per month (PMPM) rate to cover provider costs of locating, engaging, and enrolling beneficiaries. To make eligibility determination and beneficiary tracking more efficient, Maine developed a health home portal that automatically loads eligible patient panels to respective health home providers and allows them to access the information electronically in real-time. Similar web-based portals are either in place or being developed in New York and Ohio.
In some states, it took time to develop and fine-tune eligibility algorithms and refine referral processes, resulting in low initial enrollment rates in some cases, although these problems have largely been resolved. In Maine, where Medicaid verifies eligibility of provider-identified health home enrollees and notifies potential enrollees of their choice to opt-out, providers noted a time lag in obtaining confirmation, which can result in delayed services or providing services and running the risk of not being paid if a beneficiary turns out to be ineligible. In our follow-up calls, providers we interviewed confirmed that the state had expedited this process by the second year of the program.
Requirements for Participating Providers
It is important to note that providers who become health homes have chosen to apply for health home designation and have won state approval. Although reasons for participation in the program may vary across providers, and certainly enhanced payment for care management and coordination is an incentive, we uniformly heard that providers believed the model was a better way of approaching care for their high-cost, high-need patients.
Each state establishes the qualifications that practices or organizations must meet to be designated as a health home provider. In most states with primary care-based programs, health home providers must achieve PCMH recognition from the National Committee for Quality Assurance (NCQA) or other standards the state may approve as equivalent, although the level of recognition and time allowed to do so varies across programs (Table 3). For example, Idaho requires its health home providers to achieve at least Level 1 NCQA recognition. In Oregon, health home providers were required to meet standards the state established for patient-centered primary care homes (PCPCH). For practices attaining NCQA recognition, the state accepted the level of NCQA recognition with additional state requirements.14 Similarly, Missouri required health home providers to meet NCQA "Level 1 plus," which set specific levels of performance or certain elements, and allowed leeway for the state to approve other recognition standards. Council on Accreditation of Rehabilitation Facilities (CARF)15 or other accreditation is used in some states where mental health centers are the designated health homes (Ohio, Missouri). Both CARF and the Joint Commission have developed behavioral health home standards since the initiation of the Medicaid health home option, and NCQA last year issued new standards heightening attention to integration of behavioral health in PCMH recognition.16 North Carolina, which simply identified health home-qualified beneficiaries among Medicaid enrollees served by existing CCNC and PCPs, made no health home-related changes in provider requirements.
Recognizing the challenges of delivery system transformation, some evaluation states have phased in certain provider requirements or set lower initial standards to give providers more time to develop necessary structures and processes in order to encourage broader provider participation in their health home programs. Iowa's SPA gives providers up to one year to achieve NCQA recognition, and Idaho allows providers two years to achieve at the minimum Level 1 NCQA certification. In Oregon, the state developed its own, tiered PCPCH provider standards, requiring providers to achieve a minimum number of "must-pass" criteria before being accepted into the health home program. Practices with NCQA recognition may meet standards by attesting to NCQA recognition, and meeting additional requirements set by the state.17 Regardless of the leeway states allowed in provider requirements, some providers have still struggled to meet the expectations. For example, in Maine several practices were suspended from the health home program because they had not been able to become NCQA-certified in the timeframe allotted by the state. As a result, the Coordinated Care Teams (CCTs) assigned to work with those practices terminated their relationships, with some even laying off staff due to presumed lower demand for services. The state later allowed the struggling practices to become health homes once they had achieved their NCQA recognition, but the process of re-establishing communication and referral procedures caused a substantial amount of administrative and staffing stress for the affected CCTs.
| TABLE 3. Health Home Provider Requirements and Supports | |||
|---|---|---|---|
| State | Certification/Recognition | Health Information Technology | Technical Assistance & Other Support |
| Patient-Centered Medical Homes and Extensions | |||
| Oregon | Practices must be certified by the state as PCPCHs, in some cases based on NCQA recognition with additional state-specified attributes | Use of EHR not required | PCPCI created to provide technical assistance. State practice audits, practice coaching, webinars, learning collaboratives |
| Missouri (Primary care) | Apply for NCQA Level 1 within 18 months and attain NCQA "Level 1 plus" recognition, defined as meeting specific levels of performance for certain elements identified by the state, or equivalent recognition standards the state may approve as equivalent | Use of EHR required | Practice coaching, learning collaboratives, behavioral health consultant training, monthly conference calls & webinars, peer-to-peer sharing opportunities |
| Iowa | NCQA or equivalent recognition specified by the state within the first year of operation as a health home (level not specified) | Use of EHR required; Participation in the state HIE required | Health coaching training, monthly call/webinar, HIT consultant |
| Idaho | NCQA Level 1 or higher recognition within 2 years | Use of EHR not required; Providers must use HIT for: (1) systematic follow-up on a patient's care; (2) population management; and (3) access to and use of HIE | Practice coaching, technical assistance on NCQA certification process, quality improvement specialist practice visits, quarterly webinars, website forum, lunch & learns |
| Specialty Provider-Based | |||
| Rhode Island (CYSHCN) | Providers must meet established state certification standards | Use of EHR not required | Monthly trainings, statewide learning activities, peer specialist training |
| Rhode Island (Mental health) | Providers must meet established state certification standards | Use of EHR not required | Monthly trainings, statewide learning activities, peer specialist training |
| Missouri (Mental health) | Meet NCQA Level 1 PCMH requirements as determined by a Department of Mental Health review, apply for NCQA recognition within 18 months, OR meet equivalent recognition standards approved by the state1 | Use of EHR required | Practice coaching, learning collaboratives, behavioral health consultant training, monthly conference calls & webinars, peer-to-peer sharing opportunities |
| Ohio | Providers must be certified by the Ohio Department of Mental Health as eligible to provide Medicaid-covered community mental health services. Certification includes achieving accreditation from CARF or other specified organizations | Use of EHR required, phased in over 2 years; Participation in the state HIE required when available | Learning collaboratives, staff training, technical assistance, consumer education tools, webinars, monthly coaching calls |
| Wisconsin | Providers must be accredited as a medical home by a nationally recognized certification program | Use of EHR required | SBIRT training, regular coaching calls, state implementation team available to offer assistance |
| Care Management Networks | |||
| North Carolina | Primary care practices must contract with the local CCNC and meet requirements including at least 30 office hours per week, 24/7 access to medical advice and services, and referrals for services not offered by the practice | Use of EHR not required | Lunch & learn sessions, quality improvement coaching, provider portal training webinars, HIT financial and technical assistance |
| New York | The lead health home entity must be approved by the state and demonstrate the ability to provide all health home services directly or through contractual arrangements with appropriate service providers | Use of EHR required within 18 months of becoming a health home; Participation in the regional HIE required | Bi-monthly webinars, peer-to-peer learning opportunities, statewide and regional learning collaboratives, Internet forum |
| Alabama | All health home team members must meet licensure requirements; care managers must have a bachelor's degree or be a registered nurse and have state-approved care management training, PCPs must contract with the state and their PCNA. Substance abuse and community mental health providers must be certified by the Alabama Department of Mental Health | Use of EHR and CCD not required; Providers who receive HITECH EHR incentive payments are required to connect the state HIE when available | Quarterly medical management meetings, clinical care champions |
| Maine | NCQA recognition (level not specified) | Use of EHR required | Lunch & learns sessions, weekly conference call, PCMH Pilot Learning Collaborative, practice coaching, Quality Counts support to practices and CCTs, monthly webinars, peer-to-peer sharing opportunities |
SOURCE: Information obtained from review of Health Home SPAs approved by CMS and interviews with state informants.
| |||
The flexibility states have built into provider criteria has had the effect of bringing a broad range of providers into health home programs, but in some cases has slowed the progress of implementation. State officials reported that some providers were further along in the transformation process and were better positioned to take on the new roles and responsibilities inherent in the health home model, while others were having difficulty adjusting to new ways of providing and monitoring care. This variation may affect the experience of care for patients and initial outcomes with respect to the quality and cost of care. In a care management network model where care teams support multiple practices, provider variation also means that care teams must be flexible in responding to varying needs of individual practices or partners. Iowa took a different approach, rolling out its program more slowly than anticipated because the state wanted to make sure providers were equipped to provide the required services before being designated as health homes.
In a few states, particularly where specialty providers serve as the health home, stricter provider standards are in place, allowing designation only of providers that can sufficiently demonstrate at the outset that they can meet the core expectations of the health home program. For example, in Wisconsin, two entities are serving the HIV/AIDS population, yet only one--the Aids Resource Center of Wisconsin (ARCW)--had the required structures in place to provide integrated and coordinated care (i.e., co-location of primary care, behavioral health, dental, pharmacy, and social support services). As a result, the ACRW is the only provider serving health home enrollees in the state. In Ohio, after the first phase of health home implementation, the state tightened provider qualification standards by requiring health home practices to have an electronic health record (EHR) in place when they apply to become health homes. The state also eliminated the option to perform care integration through collaborative arrangements, instead requiring that health homes in the second phase (not included in this evaluation) be able to deliver services through either a fully integrated or co-located behavioral and physical health integration model.
Technical Assistance and Other Support
All states in our evaluation have been providing some type of guidance to providers to assist with the implementation of the health home program, in the form of written policies and procedures, webinars and learning collaboratives, and on-site practice coaching and technical assistance (Table 3). Several states have encouraged and facilitated the exchange of ideas and shared problem-solving by hosting regular conference calls, seminars, and on-line forums. Topics covered in trainings range from practical procedures for determining patient eligibility, quality measurement reporting, and billing, to clinical care guidelines for behavioral and physical health integration, client assessment and care plan development, and best practices for chronic disease management and health promotion. In general, providers we interviewed found that opportunities for training and assistance were adequate, though in a few states providers expressed a desire for more health home-specific guidance and topics. This was especially true for providers in primary care settings who indicated the need for additional training to manage the mental health conditions of their patients.
Health home providers have also tapped into other available resources related to practice transformation, including trainings sponsored by national and local associations, commercial health systems, health foundations, and universities. Maine, Missouri, and Oregon partnered with local organizations to assist providers with program implementation and delivery system redesign. Maine has contracted with Maine Quality Counts to help oversee the implementation of the health home program and provide technical support to practices and CCTs in infrastructure development, leadership building, and collaborative care arrangements. Missouri received funding from the Missouri Foundation for Health, the Greater Kansas City Health Care Foundation, and the Missouri Hospital Association to support care integration trainings and learning collaboratives for participating providers. Oregon established the Patient-Centered Primary Care Institute (PCPCI) to provide technical assistance to PCPs to achieve the PCPCH recognition. The state has used funding from a State Innovation Model grant to continue the Institute after the initial contract ended with the health home program in September 2013.
In Alabama, Maine, and North Carolina, care management teams are assisting providers within their networks with quality improvement efforts. Alabama, for example, supplies networks with regularly updated reports containing patient-level information on utilization and other metrics of interest. Clinical care champions and quality improvement specialists, employed by the networks, analyze and present these data in a digestible and useful manner to providers, making specific recommendations for quality improvements. New York lead agencies we spoke with indicated that their funding was insufficient to augment technical assistance to providers offered by the state. Only one agency representative we spoke with reported doing needs assessment and training to determine where providers were in their understanding of the model and expectations, but expressed concern that they did not have the resources to continue this form of assistance.
Staffing
State approaches to health home team design as specified in their SPAs vary widely (Table 4). Nine out of 13 health home programs in our evaluation mandate specific health home team composition. Alabama does not specifically mandate who and how many health care professionals should be part of a health home team, nor does New York, North Carolina or Oregon. Several health home SPAs include lists of optional team members, allowing programs flexibility in engaging various providers depending on the needs of health homes enrollees. Despite the prominent focus on integration of care, only four states--Idaho, Missouri (both programs), Ohio, and Wisconsin--specifically mandate that both primary care and mental health care professionals are part of a health home team. All programs designate a care coordinator or a care manager as a required or optional member of a health home team.
Besides clinical personnel, such as physicians, psychiatrists, and nurses, health home care teams can be diverse, including diabetes educators, nutritionists, social workers, pharmacists, community health workers, transitional care professionals, and substance abuse providers. Less traditional health home staff found in some states include vocational specialists and community integration specialists (Rhode Island mental health program), school personnel (both Missouri programs), peer specialists (Missouri, New York, Rhode Island), and housing assistance representatives (New York).
Generally, health home programs in our evaluation have not reported persistent problems hiring and retaining appropriate staff. An exception is behavioral health professionals, particularly in rural or more remote areas where behavioral health workforce shortages are more common. As is true with implementation of any new program, health homes experienced a learning curve in determining the necessary staffing ratios, defining roles and responsibilities, and a suitable skillsets needed. In Maine, for example, CCTs quickly discovered that a great deal of high-need patients require nonclinical interventions, which prompted a shift from hiring nurse care managers to hiring licensed social workers. Missouri experienced issues with recruitment and retention of nurse care managers in the initial phases of the program implementation, attributed by some informants to insufficiently defined expectations for the role and lack of targeted training.
| TABLE 4. Health Home Team Composition in Evaluation States | |||
|---|---|---|---|
| State/ Program | Required Team Members | Optional Team Members | |
| Patient-Centered Medical Homes and Extensions | |||
| Oregon | The team is inter-disciplinary and inter-professional | Nurse care coordinator; nutritionist; social worker; behavioral health professional; other traditional or nontraditional health care workers | |
| Missouri (Primary care) | Health home director; primary care physician or nurse practitioner; nurse care manager; administrative support staff/care coordinator; licensed nurse or medical assistant; behavioral health consultant | Nutritionist; diabetes educator; school personnel; others as appropriate | |
| Iowa | Designated practitioner; dedicated care coordinator; health coach; clinic support staff | None specified | |
| Idaho | Primary care physician; mental health care provider; nurse practitioner or physician assistant | Nurse care coordinator; registered nurse; nutritionist; social worker; behavioral health professional; other traditional or nontraditional health care workers | |
| Specialty Provider-Based | |||
| Rhode Island (CYSHCN) | Licensed clinician; family service coordinator | Other medical providers as necessary | |
| Rhode Island (Mental health) | Master's team coordinator; psychiatrist; registered nurse; master's level clinician; community psychiatric support and treatment (CPST) specialist; CPST specialist/hospital liaison; peer specialist | Primary care physician; pharmacist; substance abuse specialist; vocational specialist; community integration specialist | |
| Missouri (Mental health) | Health home director; nurse care manager; administrative support staff/care coordinator; primary care physician consultant | Treating physician or psychiatrist; mental health case manager; nutritionist/dietician; pharmacist; peer recovery specialist; school personnel; others as appropriate | |
| Ohio | Health home team leader; embedded primary care clinician; care manager; qualified health home specialist | None specified | |
| Wisconsin | Primary care physician; registered nurse; case manager; mental health or substance abuse professional; dentist; pharmacist; other members as deemed necessary or desirable | None specified | |
| Care Management Networks | |||
| North Carolina | The team centers on PCPs, with wraparound clinical services provided and coordinated through the CCNC program. | None specified | |
| New York | Multidisciplinary team led by a dedicated case manager | Nutritionist/dietician; pharmacist; outreach workers (peer specialist, housing advocates) | |
| Alabama | PCNA team consists of a medical director; pharmacy director; care coordinator; and a chronic care champion team to work with PCPs | Mental health provider; substance abuse provider; care manager/coordinator; pharmacist; transitional care nurse; dietician; community health worker | |
| Maine | CCT manager, director or coordinator; medical director (at least 4 hours/month); clinical care management leader; established partnership with a health home practice | None specified | |
| SOURCE: Information obtained from review of Health Home SPAs approved by CMS. | |||
Adopting a whole-person approach to care often requires clinic staff to assume new roles, which could present a challenge for some providers. Primary care practices must screen patients for behavioral/mental health issues, while behavioral health care workers need to evaluate patients' physical conditions when completing a comprehensive assessment. For staff that are used to treating just the physical or just the behavioral health care needs of their patients, this is a major adjustment and shift in thinking. Some primary care staff we spoke to commented that they felt ill equipped to assume these new roles, and that appropriate and ongoing training was necessary to help them adapt to the new model of care. Compared with PCPs, behavioral health care providers were more likely to report that they were easily able to address the physical and social support needs of their clients after a period of adjustment.
In a team-based model of care, every member plays a crucial role, but our interviews indicate that a few key partners on the health home team are particularly valuable. Not surprisingly, care managers and care coordinators are deemed essential, but pharmacists and data managers also are cited as critical members of the health home team. Pharmacists assist with complicated medication reconciliation, particularly during care transitions, while a designated data manager is able to sift through and analyze utilization and claims data to better identify at-risk patients, as well as conduct ongoing population health management.
Getting Paid for Health Home Services
Although medical homes and care management have been reimbursable under a variety of authorities, the health home option provides a new authority for reimbursing expanded services "to build linkages to other community and social supports, and to enhance coordination of medical and behavioral health care, in keeping with the needs of persons with multiple chronic illnesses."18 As an inducement to states, the Federal Government matches health home services at a 90% rate for the first eight quarters after the SPA effective date. The increase in the match rate applies only to payments for the specified health home services shown in Box 3 and ranges from about 20 percentage points above the base match rate in Alabama, the evaluation state with the largest base rate, to 40 percentage points above the base match rate in New York, where the base match rate is the maximum 50%.
Most states reported that the enhanced match was a factor in the decision to implement health home programs, but the new reimbursement authority is the more enduring incentive for states and providers. In nearly all states, the program has provided new incentives for providers to take on the expanded set of care management activities not associated with direct patient contact, such as comprehensive case management, arrangements for nonclinical social and other services, health promotion, transitional care, and population management activities. The exception is North Carolina, which used its enhanced match to offset state costs and made no health home-related adjustments to rates paid to the existing case management networks or providers for all CCNC enrollees.
| TABLE 5. Initial Health Home Payment Systems and Reimbursement Level | |||
|---|---|---|---|
| State/ Program | Payment System | Payment Level | |
| Patient-Centered Medical Homes and Extensions | |||
| Oregon | PMPM care management fee | PMPM fee based on the PCPCH recognition level:
| |
| Missouri (Primary care) | PMPM care management fee | $58.87 | |
| Iowa | PMPM care management fee, plus lump-sum performance-based incentive | PMPM fee varies by patient acuity tiers:
Incentive pay based on achievement in 16 measures | |
| Idaho | PMPM care management fee | $15.50 | |
| Specialty Provider-Based | |||
| Rhode Island (CYSHCN) | FFS | Fixed rates of $347, $366, or $397, depending on the service Additional payments of either $9.50 or $16.63 made per quarter hour for 2 other services | |
| Rhode Island (Mental health) | PMPM care management fee | Based on 9 staff hours PMPM | |
| Missouri (Mental health) | PMPM care management fee | $78.74 | |
| Wisconsin | PMPM care management fee, plus flat fee for patient assessment |
| |
| Ohio | PMPM care management fee | Site-specific and based on costs, ranging from $270-$400 PMPM | |
| Care Management Networks | |||
| North Carolina | PMPM care management fee | PMPM fee based on beneficiary classification:
| |
| New York | PMPM care management fee | Paid at 2 levels depending on enrollee status, and tiered based on case-mix and geography | |
| Alabama | PMPM care management fee |
| |
| Maine | PMPM care management fee |
| |
| SOURCE: Information obtained from review of Health Home SPAs approved by CMS. | |||
Rate and Payment Structures
Although states were encouraged to develop innovative payment methodologies, nearly all have chosen some form of capitated PMPM payments (Table 5). The exception is Rhode Island's health home for CYSHCN, which began reimbursing through a mix of fee-for-service (FFS) payments and established rates per 15-minute increments of time, but is considering a change to a tiered PMPM payment based on an enrollee's level of need.
In some states (Alabama, Idaho, Missouri, and Wisconsin), the health home PMPM is a fixed amount. In others, the rate varies depending on enrollee health status or case-mix (Iowa, New York, and North Carolina). Oregon is the only state to base payment on the provider qualification level and used the enhanced health home match to encourage practices to become PCPCHs. Health home payments for PCPCHs were tiered so that practices attaining higher levels of recognition received a higher PMPM rate. The payments were discontinued at the end of the eight quarters over which the enhanced federal match was available as Oregon formally withdrew its SPA. The PMPM rate in Ohio is based on staffing costs, indirect costs related to health home service provision, and projected caseloads. Except for New York, the states with care management networks (Alabama, Maine, and North Carolina), have separate rates for the care management provider and the PCP. Maine substantially restructured its payments to the CCTs, which provide intense care management to the top 5% of a health home's high-needs patients, increasing PMPM payment rates from $3.00 for the entire patient panel to $129.50 for the high utilizers. In New York, the lead agency may retain up to 3% of health home payments for program administration. In addition to the PMPM rate, Iowa planned to pay its health home providers a lump-sum performance-based incentive, however, the incentive payment program has not been implemented thus far. Wisconsin also pays its health home provider a flat fee to cover the initial assessment and development of a care plan for each new enrollee, which may be billed annually if reassessment is needed. For its CYSHCN health home, Rhode Island also pays fixed rates for initial assessment and care plan and annual reassessments.
In a few states in our evaluation, providers encountered challenges with the payment procedures and systems states set up to bill for services. Providers found Oregon's attestation system required for payments to be cumbersome and difficult to work with, and the state and providers reported that payments were delayed well into the first year of the program. In Iowa, one provider described the reimbursement process as a "nightmare," overly complicated and onerous. The state developed tiered PMPM rates based on a patient's acuity, with patients in each subsequent tier having a higher number of chronic conditions, and requiring increased time to coordinate their care. Iowa providers use the Patient Tier Assignment Tool (PTAT) to determine the appropriate tier for each patient, which corresponds to the reimbursement amount for health home enrollees. Providers noted, however, that some patients who require intensive care coordination, particularly those with mental health conditions, might not qualify for a higher tier based solely on their number of chronic conditions, so that the reimbursement received would not cover the cost of their care. Another early challenge for Iowa providers was submitting claims for health home services, which required attestation to the tier assignment of every single patient and was extremely time-consuming and administratively burdensome. In response to these concerns, the state has simplified the attestation and payment procedures and made adjustments to the PTAT so providers have more control over tier assignments of patients.
Adequacy of Payment
Overall, the majority of providers we interviewed found the payment rates to be adequate to cover the cost of providing care to health home enrollees. Few states, however, have chosen to build an additional amount into provider payment rates to support infrastructure development, such as HIT and communications. Providers newly adopting an integrated approach to care frequently cited the lack of financial resources to support practice transformation as a problem. Establishing new payment and reporting systems, recruiting and training new staff, and conducting outreach and enrollment with new patients requires money and effort. The enhanced match does not necessarily cover these activities, and many providers noted that implementing health homes was coming out of their bottom line. In New York, lead health home agencies are allowed to keep 3% of the PMPM for administration services, but some lead agencies noted that this was not nearly enough to cover legal costs for developing contracts, the increased data management expenses, and staff time spent supervising partner organizations or providing technical assistance. Oregon used the enhanced payment as an incentive for PCPs to participate in the state's overall health system transformation efforts, but the supplemental payment associated with health home-eligible enrollees ended when the state folded health homes into its overall reform. Some providers reported that if they had realized how much work was involved or that the increased payments would end after two years, they might have reconsidered participating in the program.
In Maine, the new reimbursement structure for CCTs to provide health home services has caused financial difficulties for some CCTs, particularly because of lower than expected enrollment in the program. Instead of being reimbursed for a complete clinic panel size, albeit at a lower rate of $3.00 PMPM, under the health home program CCTs are now eligible to receive a higher rate of $129.50 for managing only the highest-need patients. The state provides those increased payments for no more than 5% of the total number of health home enrollees associated with a given health home practice. The expectation was that the higher PMPM payment would compensate for lower number of clients, but the enrollment in the program has been slow and some CCTs reported taking a financial hit as a result. The payment system too has been a cause of many headaches for CCTs. To receive reimbursement, CCTs have to enroll each patient through a health home portal and confirm they provided services to that patient on monthly basis, which they find time-consuming. Some CCT providers we interviewed felt that this reimbursement arrangement was closer to FFS than a PMPM.
A few states have changed or considered changing the payment levels for health home services. In New York, the targeted case management (TCM) providers who became health homes initially continued to be reimbursed at their legacy rate, with the expectation that those historical rates would be phased out over a two-year period. In our last round of follow-up calls with New York providers, the TCMs were bracing for a decrease in payments of about 25% and worried about being able to continue providing the expected level of services at a lower reimbursement rate. In Ohio, the state was contemplating a substantial adjustment to its health home rates as part of the expansion to six new counties, on the grounds that the existing rate structure was not sustainable. The first modification occurred in July 2014, reducing PMPM rate by 10%. A reduction in reimbursement for health home services from a fee ranging from $270 to $400 PMPM to a flat rate of $188 PMPM for adults and $169 for children is expected in July 2015, leaving at least some providers worried about sustainability of the services.
IV. DELIVERING HEALTH HOME SERVICES
The health home model's patient-centered approach requires many providers to take on additional activities or expand services they have been providing into new domains of care. It also requires an enhanced level of communication and interaction with other providers than is typical in the current delivery system. To select providers for site visits and follow-up interviews, we asked state program officials to identify health home providers they considered representative and whose patient populations included a sufficient proportion of enrollees to provide a varied experience. We included sites ranging from sole provider rural primary care practices to large urban clinics to capture variable experience with the new responsibilities inherent in the health home model and different patient populations. Common to both state officials and health home providers was a positive outlook on the potential of the health home model to improve care quality and care provision. A theme that we heard repeatedly, particularly in primary care settings with varied patient populations, was that transformation of service delivery applied to the care received by all patients, not just health home enrollees.
| BOX 3: Required Health Home Services
SOURCE: State Medicaid Director Letter Re: Health Homes for Enrollees with Chronic |
States must specify in their SPAs how providers will operationalize six required health home services (Box 3).19 As with all health home design features, there is variability among states in how they have defined these services in their SPAs, but in all cases, health home services must be quality-driven, cost-effective, and culturally appropriate.20 The aims of the services are to improve care quality and reduce inappropriate emergency department use and hospital admissions through comprehensive care management and coordination, including transitional care to reduce avoidable readmissions to hospitals, supports for the enrollee and family, and nonclinical supports in the community where appropriate. Health homes are encouraged to use HIT to facilitate care coordination and the integration of services, although there is considerable variation in the extent to which that has yet been accomplished. To assure that health home program designs support integration of physical and behavioral health services, regardless of whether the focus is primarily on beneficiaries with mental/behavioral or physical conditions, states are required to consult with the Substance Abuse and Mental Health Services Administration (SAMHSA) in developing their SPAs.
Comprehensive Care Management
Comprehensive care management requires health home providers to engage health home enrollees in the care planning and care process, assess health risks and social service needs, conduct mental health and substance abuse screenings, develop and implement a single care plan per enrollee, monitor progress at the individual and population level, and collect data and evaluate the impact of interventions. How well providers handle these tasks depends largely on their prior experience, ability to adapt new routines, available infrastructure, and external support. Providers with little or no experience in whole-person approaches to care may struggle with comprehensive care planning and may require more training and technical assistance in order to be successful. Integrating needs assessment and care planning into a daily routine can present a challenge to practices, particularly small ones, and temporarily disrupt clinic workflow. Most providers reported that they felt the disruptions were temporary and a natural part of the process of changing the way they deliver care.
A challenge to continuity of care and comprehensive care management noted by both state officials and providers is gaps in Medicaid enrollment when beneficiaries lose eligibility, although the extent to which this is a problem varies by state and provider. Health home enrollees may become temporarily ineligible for Medicaid coverage and have to "spend-down" excess income to eligible levels, or simply may not renew enrollment in a timely fashion. Most states reported that health homes typically continue to provide care management services for enrollees during relatively brief coverage lapses, but that other key services such as prescription drugs or primary care visits may be interrupted. Some state officials and health home providers also noted that there is a risk that services provided during periods of temporary Medicaid ineligibility may not be reimbursed, a factor of greater importance for providers with a higher share of "fluid" health home enrollees. Enrollment discontinuities also represent an administrative burden for providers who must monitor Medicaid eligibility and re-enroll patients who lose eligibility. To avoid this administrative burden and preserve continuity of care, some health home providers are counseling patients about maintaining Medicaid eligibility and assisting them with renewing Medicaid coverage.
Functioning EHRs and health information exchanges (HIEs) facilitate both the development and sharing of a care plan among health home providers, including nonclinical staff. However, based on reports from Medicaid program officials and providers, instant and seamless communication among various entities is still the goal rather than the reality. Compatible EHRs and HIEs are by no means common, so that care plans are often transmitted via fax or secure email. External provider partners do not necessarily have electronic access, and to the extent that they do, they often have read access but do not have writing privileges to contribute to the care plan.
Care Coordination and Health Promotion
Individuals with chronic conditions, particularly those who have more than one chronic disease, tend to interact with a number of health care providers across multiple settings. Lack of communication across providers and coordination of services provided can lead to duplicate diagnostic testing, unnecessary treatments, or avoidable hospitalizations.
Care coordination activities health homes typically carry out include referring enrollees to appropriate services, such as preventive and health promotion services, dental services, mental health services, and substance abuse counseling and treatment; assisting them with scheduling appointments; conducting follow-up monitoring and tracking of referrals and clinical results; performing medication management and reconciliation; and making sure all providers involved in care are communicating with each other, and with the enrollee and family. Prevention and health promotion are integral parts of a health home model, and include educational efforts to assist patients to understand their disease and learn how to self-manage their conditions. Health homes may also provide, or coordinate, lifestyle interventions such as smoking cessation, nutritional counseling, obesity reduction and prevention, and physical activity promotion. In Ohio, one health home provider offers a range of health promotion activities for their patient population, including weekly walks, a working garden, and parenting and cooking classes.
Providers in states using a medical home approach in their health home programs (Idaho, Iowa, Missouri's primary care health home, and Oregon) typically engage nurse care managers and referral coordinators to direct services for health home enrollees. These are new roles that require buy-in from physicians and office staff and may sometimes be challenging for more traditional, physician-centered practices. The team care approach may elevate the role of nurses in patient care as nurses take on more clinical responsibilities; in some practices, nurse care managers have encountered some resistance from physicians but the shift in roles seems to be happening regardless. Health homes often conduct pre-visit planning, which includes the nurse care manager, pharmacists, referral coordinator, behavioral health specialists, and others involved in a patient's care, to review a patient's history and flag any discrepancies or concerns for the attending physician. Continued monitoring of patients is also responsibility of care managers. For example, in Missouri, nurse care managers are required to be in touch with a patient every 30 days.
Relative to primary care-based health homes, specialty providers (Missouri, Ohio, Rhode Island, and Wisconsin), often reported making little change in the existing care delivery system for their patient populations. Due to the nature of their conditions, enrollees with SMI or HIV/AIDS often receive the majority of their services through specialty providers, who traditionally have offered a range of care coordination and community support services. Nevertheless, a number of mental/behavioral health providers reported that they welcomed the new focus on incorporating primary care into their service package. Some noted, however, that dealing with common but often undertreated physical health issues, such as obesity and other lifestyle-related conditions, required some adjustments to clinic workflows and ongoing staff training. Health home providers in Missouri, Ohio, Rhode Island, and Wisconsin either co-locate primary and mental/behavioral health services, or have established close relationships with clinical and social services providers in the community. For example, the ARCW offers medical, behavioral health, dental, and pharmacy services on-site, as well as legal, housing, and food pantry services. Rhode Island has introduced peer specialists to assist health home enrollees in reducing high-risk behaviors and adapting healthy lifestyles. Ohio health homes use health home aides to accompany patients to medical appointments and to help them understand and manage their conditions.
Alabama, Maine, and North Carolina have each created a health home program where PCPs work collaboratively with care management networks to manage care for health home enrollees. Care management teams act as the link between primary care, mental health care providers, specialists, hospitals, social services, and community supports. The care management networks in Alabama and North Carolina provide wraparound care management and coordination services to all health home enrollees. In Maine, primary care practices conduct care management for all patients with chronic conditions while the CCTs provide health home services only to the top 5% of high-cost, high-need patients. The health home care management network model allows for substantial flexibility and responsiveness to local realities, but depends on good working relationships between providers and care management teams. Care coordinators function as a central link between PCPs and care management networks, and are responsible for establishing relationships with practices and developing processes for referrals, care planning, communication, and reporting.
New York's health home approach relies on a lead entity to assemble an array of provider partners that collectively provide health home services. The lead agency brings together a diverse group of providers collaborating across care settings, focusing on clinical care as well as the social factors affecting the health of the Medicaid population. The health home initiative has encouraged some providers who have not worked together in the past to collaborate, and for others, it has provided a mechanism to formalize already established relationships. The lead entity is responsible for assigning enrollees to providers within its network, and for managing administrative tasks and distribution of payment. Care coordination and integration of services is provided by an inter-disciplinary team of providers, under the direction of a care manager who is accountable for ensuring a patient's access to services and community supports, as defined in the care plan. To help patients navigate the system and ensure that they get care they need, some New York health homes use peer support services and peer wellness coaches.
Integration of Behavioral and Physical Care
The Medicaid health home option is one of multiple delivery system initiatives designed to accomplish a whole-person approach to assure appropriate attention to both physical and mental/behavioral health. Medicaid beneficiaries are more than twice as likely to be diagnosed with mental illness as the general population, and roughly 49% of Medicaid beneficiaries with disabilities have a mental health illness.21 Depression has been estimated to affect 20% of Medicaid beneficiaries and 23% of those eligible for both Medicare and Medicaid.22 Behavioral and mental health conditions co-occurring with chronic medical diseases can contribute to worse overall health outcomes of affected individuals and higher health care spending.23
Regardless of whether their focus traditionally has been on physical or mental/behavioral conditions, health homes are responsible for the integration and coordination of physical and behavioral health care for all program enrollees. Some PCPs have licensed clinical social workers on staff to provide behavioral health screening and interventions, while others rely more on their nurse care managers or care management networks to identify behavioral health problems, refer patients to resources in the community, and follow up on access and treatment. Health home providers in several states have implemented depression and substance abuse screenings, such as the PHQ-9 and PHQ-2 components of the Patient Health Questionnaire (PHQ)24 for depression and Screening, Brief Intervention, and Referral to Treatment (SBIRT)25 for substance abuse, as part of the effort to integrate mental health care management into primary care. Although PCPs generally value the inclusion of mental health, they note that instituting routine screenings for all patients may mean acquiring additional staff, training existing staff, and adapting daily workflows. Additionally, the screening, referral, and follow-up model of behavioral care provision requires establishing relationships and building trust among various providers in the community, which in some cases is a laborious effort.
In an effort to integrate primary and behavioral health care, some medical home-like health homes have employed a full-time psychiatrist or social worker, or contracted with part-time mental and behavioral health consultants. One health home provider in Missouri, for example, reported that a new process for primary care physicians to recommend that a behavioral health consultant (often a social worker) be in the exam room for primary care visits, was allowing more patients access to needed services without having to schedule separate behavioral health visits. For example, a nurse care manager and a behavioral health consultant participating in a primary care visit were able to counsel and locate support resources for a distraught patient who had been skipping visits because she felt powerless to control her diabetes. Not all practices can provide ready access to mental health providers, however, particularly providers in areas where there may be shortage of mental health and substance abuse treatment programs and licensed behavioral and mental health providers. In our initial site visits with Idaho health homes, some nurse care coordinators reported that while they screen for depression or substance abuse, they felt ill equipped to manage a positive diagnosis, which highlights the challenge of integrating mental/behavioral health into primary care settings and the potential need for training and hands-on technical assistance to primary care practices.
Health home providers focusing on mental and behavioral health conditions described similar experiences and challenges with the integration of primary care. Missouri and Ohio providers, for example, reported initial resistance of staff to incorporating BMI, diabetes, and other physical health screenings into treatment plans. In both states, health homes employ primary care consultants to aid behavioral health staff with diagnoses and appropriate interventions for physical health conditions. With training and assistance, this opposition appears to have diminished over time. We learned in our follow-up conversations with providers that staff have come to better understand and appreciate the importance of physical health to overall well-being of their patients. For example, because of integration training, case workers were able to reconcile various medication regimens for their patients. Most Community Mental Health Organizations (CMHOs) in Rhode Island integrate primary care by developing memoranda of understanding with local FQHCs and other primary care practices. They have established notification and data-sharing processes so that key information is exchanged between behavioral and physical health providers attending to a particular patient.
Some behavioral health homes integrate behavioral and physical health through co-location, which many recognize as a great enabler of care integration and coordination. However, one provider in Missouri noted the importance of shared physical space in such settings; one clinic site offered behavioral and primary care in one building, but located on different floors, which created a physical barrier for some patients to access both types of services. One Rhode Island health home developed a bidirectional co-location where behavioral health staff is embedded in an FQHC, and primary care staff on site in a local CMHO. Even if a clinic offers co-located services, some patients may still choose to see a PCP in a different location, however, which can hamper coordination of services if the health home is not kept in the loop. Developing relationships and communication processes with outside health care providers is therefore equally important for co-located health homes.
Coordination with Other Organizations and Programs
As part of coordinating the care needs of health home patients, providers may need to work with other care management programs, including managed care organizations (MCOs), to avoid duplication of services. Medicaid beneficiaries, however, cannot be enrolled in both TCM and health home programs and most states allow beneficiaries to choose one or the other. Negotiation regarding the respective roles and division of care management responsibilities among various entities and establishment of processes for information sharing are required. Ohio's SPA, for example, is explicit in terms of how MCOs and health homes are expected to work together, but we heard both from the managed care plans (MCPs) and the health home providers that the division of care management responsibilities is not always clear and that processes were still being worked out. Similarly, the structures and reporting requirements of the health home program may differ from those of MCOs, creating administrative burden for both entities. In New York, health homes are required to establish relationships with numerous MCOs, each of which may have distinct processes for reporting and accessing patient information.
Idaho and Wisconsin require that Medicaid beneficiaries who are enrolled in managed care or receiving TCM or community-based waiver services disenroll from these programs if they enroll with a health home provider. In most other states, health home providers must collaborate with case management programs their health home patients maybe be enrolled in. For example, care coordination services in Alabama may be provided by health homes as well as substance abuse providers and public health departments, requiring these various organizations to work together. Care coordination efforts by multiple entities that are not coordinated may lead to inefficiencies and confuse patients. Providers in Idaho, in particular, were concerned that some enrollees may be overwhelmed by the number of care managers--hospital, MCO, health home--contacting them with potentially overlapping or contradictory advice.
Data-Sharing and Privacy
The ability to share patient data among various providers is key to successful care coordination. Not all states require health homes to have and use EHRs, and HIE systems are still in developmental stages in many states. But information sharing does not rest on modern technologies alone. In the absence of adequate HIT infrastructure, health homes often depend on traditional channels of communication, including in-person meetings, phone calls, fax, and secure messaging. This suggests that while HIT can promote efficiencies, it is not required to coordinate a patient's care. Issues relating to sharing sensitive patient information also appear to thwart effective care coordination in some cases. Providers particularly mentioned limited access to substance abuse information, HIV status, and mental health diagnoses, which are protected by federal and state regulations and often require extra levels of patient consent for sharing. Health home providers in Maine reported that the state's restrictive privacy laws have been preventing them from accessing full clinical profiles of their clients, hampering their ability to deliver necessary treatment and interventions.
Comprehensive Transitional Care
Transitional care consists of a broad range of services designed to ensure continuity of care and promote safe and timely transfer of patients from one type of care setting to another. Break-down in communications, incomplete or tardy transfer of patient data from one care setting to another, insufficient education of patients and their family, and the absence of a single point of contact to ensure continuity of care can result in unnecessary readmission rates26 and other adverse outcomes,27 as well as higher health care spending.28 Effective, high-quality transitional care is critical to the well-being of chronically ill patients, whose health status may change frequently, resulting in numerous transitions between care settings and providers.
Transitional care typically involves timely in-person or telephone contact with a patient following discharge from an inpatient facility or emergency department visit, reviewing the discharge summary, implementing the recommended treatment plan, which may include scheduling follow-up appointments and filling medication prescriptions, and helping patients with the transition back to the community after facility-based care. To ensure comprehensive transitional care, health homes must establish policies and procedures with inpatient facilities, emergency departments, and residential facilities to ensure prompt notification of an individual's admission and/or discharge to/from a respective facility.
As is true for other health home services, the ability to provide transitional care is highly individualized, and largely dependent on providers' working relationships with local hospitals and other facilities, as well as established communication arrangements with those facilities. Health home providers that are affiliated with hospitals reported that they have been able to obtain timely discharge notifications, often through daily lists of admissions. Timely notifications allow health homes to follow-up with their enrollees before or shortly after discharge from a hospital or emergency department. Some health homes--Alabama, Idaho, North Carolina, and Rhode Island--employ social workers who are either embedded in hospitals or visit several times a week to facilitate transitional care for health home clients. Notification of a hospital admission seems to be working relatively well for patients who are in MCPs and require prior authorization, as long as MCOs maintain regular communication with health homes.
For most health home providers, however, the provision of transitional care continues to be a challenge. New York distributed materials on notification responsibilities to hospitals, but the result appears to be variable. One provider said no formal process for notifications was in place and that little improvement had been seen, except when specific health homes and hospitals had set up a process. Some providers told us that they learn about an enrollee's hospitalization or emergency department visit as much as few weeks later, and often from the enrollee rather than the hospital. Receiving emergency department visit notifications about health home members seems even more challenging. Emergency department doctors or staff may not find the time to contact a patient's health home provider or even be aware that the patient is enrolled in a health home. To improve the notification process, some health homes (Ohio and Wisconsin) have created health home membership cards and are asking enrollees to carry and present the cards whenever they are admitted to a hospital or visit the emergency department. Nevertheless, human interactions are often an unreliable method of notification. Many states are working to develop their HIE infrastructure to facilitate the exchange of hospital data. Only a few states have fully functional statewide HIEs, however, and even when they are operational, not all providers are connected.
In all states, notifications of hospitalizations and emergency department use of health home enrollees who are dually eligible for Medicaid and Medicare are even more problematic because Medicare, not Medicaid, is the primary payer. For example, Missouri's MO HealthNet system maintains a prior authorization tool that requires hospitals to notify Medicaid of admissions within 24-hours, but Medicare admissions among the 34% of enrollees who are dually eligible are not included. Rhode Island has established a process for MCOs to notify health home providers of Medicaid hospital admissions for the CYSHCN health home and the 35% of CMHO enrollees who are enrolled in MCOs. No process has been established to notify health homes of Medicare admissions among the roughly 60% of CMHO health home enrollees who are dually eligible. Prior authorization is not required for emergency department visits, making it even harder for health homes to track use of emergency services by either Medicaid only or dually eligible members. One Idaho provider noted that hospitals have been somewhat cooperative in notifying providers of admissions because of efforts to reduce readmission rates and avoid associated financial penalties. This provider also mentioned that the new Medicare billing codes for transition care management have been an added incentive for his practice to track down and follow-up with dually eligible health home members after discharge from a hospital.
Community Supports and Social Services
Part of the provision of patient-centered whole-person care is involving the enrollee in the care planning process and identifying clinical and nonclinical services that can meet needs or help the enrollee accomplish health-related goals in the care plan. Health home providers are required to refer enrollees to community resources, social services, and supports. These may include peer counselors, support groups, and self-care education programs to promote the enrollee's engagement and self-management capabilities and to improve adherence to prescribed treatments. Some health homes also engage in obtaining legal services for enrollees and providing assistance with access to social support benefits.
This role requires health homes to develop partnerships with a variety of organizations, including state and local government agencies, foundations, charities, associations, private businesses, and community-based nonprofits, among others. Health home providers who have historically linked their patients to social services and supports, such as CMHCs or home health agencies, generally are able to rely on previously established relationships. Other providers, such as primary care practices, may have less experience and have to spend more time and resources developing and cultivating necessary connections throughout a community.
Locating and linking health home enrollees to chronic care educational resources seems to be a fairly straightforward task. Providers we interviewed reported no challenges in this area. Free or low-cost educational materials, care management courses, and lifestyle intervention programs (e.g., tobacco cessation, weight management, fitness classes) are available in most communities. Many health home team members are trained and certified in disease management and health education, and some provide motivational interviewing, a counseling technique to help patients establish wellness goals and elicit behavioral change. Peer supports and support groups also may be effective in engaging individuals in disease self-management and lifestyle changes, although only Missouri, New York, and Rhode Island have made peer specialists part of a health home team composition.
Typically, a designated health home team member, often a social worker, is responsible for evaluating enrollees' nonclinical needs and coordinating services as appropriate. Sometimes health home staff members conduct home visits to better assess an enrollee's environment, identify barriers to well-being, and determine what services or supports are necessary. Common nonclinical services health home providers have mentioned include assisting with access to food assistance, transportation, housing and energy assistance, vocational training, and medical device procurement or upgrades. Health home staff may assist enrollees with filling out applications for welfare programs, financial assistance, Medicaid and disability benefits, obtaining prior authorizations, government-sponsored cell phones, or translation services. Some providers reported that care coordinators or social workers may accompany enrollees to medical appointments; a nutrition counselor may go grocery shopping with an enrollee to teach them what food to buy and how to prepare it.
State officials and providers noted that the lack of stable housing and reliable transportation are common problems for health home enrollees that can interfere with the ability to focus on health issues and to get to medical appointments. Research suggests that stable and affordable housing contributes to better health, particularly for individuals living with chronic conditions, not only because it reduces stress but also because it allows chronically ill patients to maintain their treatment regimens.29 New York has designated housing as an essential service component of the health home program, and all health home lead agencies include supportive housing linkages in their provider network lists.30 To assist enrollees in finding housing, one New York health home has secured grant funding to subsidize rental units, community residence, or homeless shelter placement. New York has held several regional forums, through partnership with the Corporation for Supportive Housing, where health homes and housing providers have an opportunity to develop relationships and collaboration plans. The Wisconsin health home provides financial housing assistance, and a handful of other health homes programs employ on-site housing advocates and specialists to help beneficiaries find affordable housing, or apply for security deposit assistance or energy assistance.
Health homes have adopted various strategies to address transportation needs, which is a concern particularly in rural settings where patients may need to travel large distances to see a health care provider and where public transportation may be limited. Access to reliable transportation has been associated with more frequent health care visits, while the lack of transportation may cause some people to forgo needed medical care.31 Several health homes reported that they connect enrollees to a transportation voucher program and help them fill out necessary forms. Others have allocated budget resources or secured private funding to subsidize bus tickets, taxi vouchers, or private transportation services. Yet others have been more creative in their approaches--an Alabama health home serving rural areas has engaged in negotiations with a local nonprofit organization to bring transportation services to underserved areas, and a Maine health home provider has developed partnerships with local charities and a community college for the purpose of fixing failing cars. While charities sponsor the purchase of necessary parts, community college students perform maintenance and repairs free of charge. The same health home has also petitioned the local public transportation authority to put a bus stop near the YMCA to facilitate access for beneficiaries without cars.
V. HEALTH INFORMATION TECHNOLOGY
HIT has the potential to improve health care quality and reduce inefficiencies and waste, and improve safety.32 HIT can include a range of integrated data sources, including EHRs, Decision Support Systems, and pharmacy order systems. EHRs, for example, have been shown to improve medical practice management by increasing efficiencies and cost savings.33 Using an EHR across the continuum of care allows for improved information sharing among providers; enhanced medication reconciliations; standardization of data and care plans; improved population management capabilities; and, faster and simpler disease management, according to the Office of the National Coordinator for Health Information Technology.34
In the SMD's letter providing guidance on the implementation of health homes, CMS requires the "use of information technology to link services, as feasible and appropriate."35 The language in Section 2703 is vague, recognizing that strict HIT requirements could limit the number of providers who are able to qualify to become a health home. As a result, the penetration and use of HIT across providers within each health home program and across states is highly variable. In states where care coordination processes were already in place, the HIT use is generally more widespread and accessible to the full range of health home providers, though this is not always the case. Both state officials and providers agree that real-time data is essential for successful care coordination, but the use of HIT to link health home services continues to be a work in progress, requiring more attention, investment of resources, and time to fully develop. Health home providers are not alone in lacking high functioning HIT systems capable of meeting the demands of their broad care integration requirements. Nationally, it is still true that most providers do not have robust electronic information systems in place capable of supporting coordination of a patient's care with other providers, sharing needed information, monitoring compliance with prescribed care plans, and measuring and making improvements to performance.
Health Information Technology Requirements
Health home programs in our evaluation have given their providers considerable latitude in the area of HIT (Table 3). Iowa, Maine, Missouri, New York, Ohio, and Wisconsin require that health homes have and use EHRs. In Idaho, New York, and Ohio, HIT standards were phased in over time, affording participating providers more flexibility in acquisition and mastery of technology. New York also made available substantial grant funding and learning opportunities to support health home providers in developing and effectively using HIT. The remaining states--Alabama, North Carolina, Oregon, and Rhode Island--do not specifically mandate that health home practices adopt EHRs, though they are encouraged to do so. Providers in Oregon who have EHRs are able to earn additional points towards their qualification as a Tier 3 PCPCH. Alabama, Idaho, Iowa, New York, and Ohio require that health home providers connect to a HIE if/when it becomes available. Except for Alabama where HIE was in the testing stage last year, all these states have launched their HIEs, although some may offer limited functionality (e.g., direct secure messaging or patient record look-up only) and may not be available statewide.
Challenges
Reports from health home providers echo many of the concerns raised in a recent report reviewing the potential benefits of HIT but also the initial and ongoing direct costs and unintended consequences in terms of disruption of workflow, productivity losses, distraction from patient care, potential slowing of practice transformation during the HIT "learning curve" phase,36 and the need for technical assistance in choosing and using EHRs.
Electronic Health Records and Data-Sharing
Perhaps the biggest hurdle to fully integrating an EHR cited by providers--and an HIE, if it was available--was the financial cost associated with obtaining or modifying software, maintaining licenses, and lost productivity in a practice when staff is learning new data systems. This is particularly true for small providers who indicated that having staff "off-line" put a tremendous amount of stress on the practice. Providers also noted that having personnel able to meet state HIT requirements was a challenge and that there were no additional resources to hire staff with technical expertise. According to one provider, little consideration is given to the fact that time spent converting paper records into electronic ones or upgrading older systems and training staff takes a toll on practice productivity, especially in the early stages of a new system adoption.
While all health home practices we visited had a fully functional EHR at the practice level, accessibility across all health home team members, including those providing community and social supports, was highly variable. The same was true for accessibility across various external providers. Often multiple and not necessarily compatible EHR platforms are used by health home providers within the same state, and hospitals have their own systems that typically may not be compatible with systems in use by other providers.
We also heard about a wide range in individual EHR usability for care coordination and population management. Some providers had adapted a billing system to perform care management functions, while other providers had purchased new software with a broader range of care coordination functions. Many health home providers, for example, worked to develop a care management plan template within an existing EHR. While many states provided some technical assistance, in the form of webinars or learning collaboratives, providers we spoke to felt the need for more training on the efficient and effective use of HIT to achieve the quality improvement goals of the health home initiative.
EHR interoperability--the ability of systems to exchange and use electronic health information from other systems without special effort on the part of the user--enables better workflow and allows for the sharing and transfer of data among health home providers and partners, including nonclinical staff. True interoperability, however, is the exception among health homes rather than the rule. For example, although adoption of EHRs is widespread in Oregon, more than 100 different EHRs are being used by hospitals and providers, complicating communication and data-sharing across HIT systems.37 Providers noted that sometimes even those using the same HIT platform, such as Epic, cannot exchange data seamlessly. In some cases, health home providers have separate EHRs for primary and behavioral health information, and while efforts are underway to merge the systems, the separateness creates lags in access and lost opportunities in care coordination. Many health homes also reported having separate pharmacy data systems, making timely medication reconciliation, which is particularly important during care transitions, more difficult.
Many health home providers also regulatory restrictions on sharing of sensitive data on EHRs (e.g., HIPAA privacy rules or provisions in 42 CFR Part 2 guiding disclosure of substance abuse treatment) were creating barriers to exchange of information. Providers in a few states noted that changes in state regulations regarding sharing sensitive patient data had "ripple effects" on health home providers, causing uncertainty and confusion about the kinds of patient information that can be included in the care plan. Health homes were working out new systems of sharing and developing new rules to expand medical record access to the full range of health home providers. States that have elected an opt-in rather than an opt-out system (patients have to consent to participate before they are enrolled in the health home program) noted fewer concerns about privacy and data-sharing. Other states, Ohio and Oregon, for example, noted that there was substantial work left to be done to educate providers about what patient information can be shared, as well as educating patients about the importance of allowing the full range of health home providers access to health information to be able to fully coordinate care.
Health Information Technology Technical Assistance
Health home providers in most states noted that inadequate support--financial and otherwise--was a hindrance to realizing health home HIT goals and requirements. The Medicaid or Medicare EHR Incentive Programs,38 which provides financial assistance for HIT adoption to eligible providers, offered some health homes a stream of funding for HIT adoption.39 CMHOs, who do not qualify for the Medicaid EHR Incentive Program, were vocal about the lack of financial resources for EHR adoption, particularly in states that require behavioral health homes to use EHRs and connect to HIE (Missouri, Ohio).
| BOX 4: New York State Health Home HIT Standards Initial Standards:
Final Standards:
SOURCE: New York Department of Health. "Health Homes and Health Information Technology." |
In states that provided financial support or technical assistance to health home providers to facilitate the adoption of HIT, providers seemed to be faring better at integrating and operationalizing HIT systems. In New York, for example, Medicaid partnered with the New York State Division of Health Information Technology Transformation (DHITT) in an effort to leverage HIT to help health homes achieve the goals of increased quality and reduced health care costs.40 DHITT developed nine HIT standards to help promote better care coordination (Box 4), including the use of a Certified EHR; participation in a Regional Health Information Organization for select health care delivery organizations (New York's HIE); provision of access to a singular electronic care plan for any care team member/organization consented to by the health home patient; and, the use of electronic clinical decision support among direct care providers. The DHITT has invested over $840 million in to develop New York's HIT system as a whole.41 The state also provided $15 million in HIT assistance specifically for health homes, drawing on savings resulting from the state's Medicaid Global Spending Cap.42
Iowa has offered hands-on technical assistance to practices in setting up the necessary infrastructure to fulfill a requirement to connect to the Iowa Health Information Network (Iowa's HIE). In North Carolina, providers may participate in the Program to Advance Technology for Health, a collaboration with the BlueCross BlueShield of North Carolina and AllScripts that provides financial and technical assistance to providers in EHR adoption and use.43 CCNC offers practices in their networks ongoing technical assistance with connecting to the North Carolina HIE.44
Electronic Notifications
Limited ability of health home providers to obtain timely notifications of hospital admissions and discharges and emergency department use also hinders the ability of health homes to provide effective transitional care. While Missouri has an email notification system in place where health home providers receive daily email notifications about Medicaid-financed inpatient and emergency department usage by health home enrollees, many health home providers in other states are still developing relationships with hospitals to exchange data. Further, notifications are essentially nonexistent for health home enrollees who are also enrolled in Medicare because Medicare, not Medicaid, is the primary payer for inpatient and emergency department services.
Health home providers have engaged in several strategies to establish formal, or informal, systems and processes to efficiently send/receive emergency department and hospital admission notifications. For example, some Iowa health home providers have established quarterly meetings with local hospital staff to review notification procedures and make adjustments as necessary. The Patient Care Networks of Alabama (PCNAs) created "transitional care teams," which include nurse care managers, social workers and pharmacists, with a designated team member visiting a hospital multiple times per week to facilitate transitions for health home enrollees. Idaho health homes that are affiliated with larger hospitals have embedded a health home discharge planner to facilitate the flow of information to health home providers from the hospital, and ensure transitional care is occurring. In North Carolina, almost one-third of the state's hospitals provide twice-daily updates to CCNC on admissions, discharges, and transfers of CCNC-enrolled patients. Even when formal or informal communications have been established, health home enrollees may visit multiple hospitals within their area, making notifications more challenging.
Health homes that are directly affiliated with hospitals, including some in Idaho, Iowa, Maine, and New York, have been able to more easily establish protocols for emergency department and hospital admission notifications, and often have direct access to admission data. Missouri uses an authorization-of-stay tool that requires hospitals to alert Medicaid when any enrollee is admitted for a Medicaid-financed stay. While this system captures admissions for many health home enrollees, respondents in Missouri noted that the tool misses admissions for dually eligible beneficiaries, where Medicare is the primary payer.
Some states are attempting to use their HIEs to exchange hospital data to facilitate emergency department and hospital admission notifications, with varying success. The utility of HIEs and the rate of participation among providers vary substantially, and the full potential of HIE for the majority of health homes states has yet to be realized. Given the variability in EHR functionality across health home providers and electronic information exchange with other providers, many have developed various "work-arounds" to ensure information sharing. Work-arounds described include faxes, phone calls, secure email, or personally collecting discharge summaries, as was the case in Idaho where a health home nurse care manager would walk across the parking lot to pick up emergency department discharge paperwork, rather than waiting the typical 72 hours for the hospital to upload information to an EHR.
Health Information Exchanges
HIEs are at various stages of development and functionality in the 11 evaluation states. According to our review, all 11 have some HIE infrastructure in place, whether state-sponsored, regional, privately-funded, or some combination of the three, but the degree to which providers connect and use the information exchange is highly variable. Five of the 11 states explicitly require connection and use of a state or regional HIE when available (Table 3). Several states (Iowa, Missouri, North Carolina, and Rhode Island) have or are working towards developing a statewide system to exchange health information, while other states, for example, New York, have regional HIEs in place, often connected to hospital systems. HIE functionality varies widely. In some states, HIE includes a range of functions, such as referrals, medical event notifications, public health reporting, and analytics (e.g., Maine, Ohio), while other states may be limited to direct secure messaging and/or patient record look-up (e.g., Iowa).
Some providers reported not having the necessary infrastructure to connect to an HIE, while for others subscription costs are considered to be prohibitive. Many health home providers recognize the value of connecting to an HIE and would be willing to subscribe, but they feel that the critical mass of HIE participation among all providers that would make it worthwhile had not been reached. For example, a health home in Rhode Island reported that the state's HIE, CurrentCare, had been very slow in enrolling consumers to the frustration of physicians who, after not being able to locate information for nine out of ten patients, stopped accessing CurrentCare altogether. Hospital participation in HIE is inconsistent, with some larger hospital systems electing to use their own data systems rather than connect to the state HIE. As a result, some providers question the value of subscribing to the HIE. Providers in Idaho noted that the HIE has great potential, but until participation becomes mandatory, its utility is limited. Some states, however, have achieved a critical mass in terms of provider participation. HealthInfoNet in Maine is able to link medical information from separate health care sites to create a single electronic patient health record, which providers can pay to access.
Health home providers noted an additional complication in areas near state borders (Idaho and Ohio, for example), where patients' use of out-of-state hospitals and specialty providers is common. Electronic exchange of health information across state lines is largely limited or nonexistent, presenting hurdles for providers to share information with the health home or upload it to the appropriate HIE.
Even where HIT adoption among providers is slow or not required, some states have in place existing infrastructure that substitutes for or supplements electronic data management and information exchange. For example, Alabama has developed a Realtime Medical Electronic Data Exchange system, which supports a number of functions, including a care management tool that the networks use to document patient care, as well as verifying the required "monthly touch" with health home participants, triggering the payment to health home providers. Alabama also generates a report that provides patient-level information on utilization and other metrics of interest so that providers can identify eligible health home enrollees, as well as gaps in care. A handful of states have similar systems in place, whether they are provider portals, care management information systems, or web-based population health management tools.
Population Management
The explicit goal of the health homes initiative is to manage care for high-cost, high-need Medicaid beneficiaries. Population-based care focuses on the health of an entire patient population by systematically assessing, tracking, and managing health conditions across the entire group, rather than just responding to the individual patients seeking care.45 Population-based health care uses data systems, such as registries, to track patient care over time and monitor particular conditions, characteristics, or any other measure, to assess patients' needs and improvements. To a large extent, health home providers we spoke to recognize the importance of population management and are actively engaged in tracking and monitoring their whole patient panel, and particularly high-risk patients. Several providers, however, noted that they would benefit greatly from having a designated staff person to assess and track conditions and treatment outcomes of health home enrollees but resources to support this function are limited. The enhanced match during the first eight quarters of the initiative helped with hiring staff to perform data management, but many providers noted that without ongoing financial support, over and above the PMPM, covering a population manager's time would be a challenge.
While most providers are generating their own patient reports, most states are also furnishing providers with patient utilization data, for example HealthInfonet in Maine. Many providers found this information valuable and were receiving the data in a usable format, but some felt that information provided was often "convoluted," hard to work with, and not always timely.
Patient Portals
Engaging patients in their care is a shared goal among health homes. Several health home providers have created patient portals, where patients can request an appointment, access information about medications, treatment, and care plan details, or send a secure message to their provider. For example, health homes in Iowa are encouraged to use email, text messaging, patient web-portals, and other technology where possible to enhance patient access and self-management. However, almost universally, health home providers noted very low usage (less than 10%) among their health home enrollees. The barriers for patients may include unfamiliarity with technology, limited access to the Internet or data for smart phone users, and sometimes mistrust of technology in general and preference for talking to a real person or face-to-face. Health home staff are encouraging their patients to connect to patient portals--in some cases having health homes staff assist patients to log onto the system for the first time. In some health homes, physicians are asked to discuss the benefits of a patient portal with patients during a visit and encourage them to sign up, on the grounds that patients may be more willing to follow the advice of their doctor. Nevertheless, health home enrollee participation in patient portals has been extremely slow.
VI. CONCLUSIONS
In this third-year report on the long-term evaluation of the Medicaid Health Home option, we have focused on the implementation challenges Medicaid health home providers have faced in implementing the model and their progress in the development of processes and tools to support the model. The Medicaid health home option, established in the ACA as a State Plan benefit, aims to improve outcomes and reduce the cost of caring for Medicaid beneficiaries with serious chronic illness who require care across multiple clinical and nonclinical domains. In addition to their chronic physical or mental health conditions, many of these beneficiaries face a variety of nonclinical or behavioral challenges. Factors such as inadequate or unstable housing, inadequate food supply, lack of reliable transportation, or substance abuse can have negative consequences for both their ability to access care and their health. The health home model's whole-person approach, encompassing comprehensive care management and coordination, integration of physical and mental/behavioral care, and links to nonclinical supports, thus has the potential to improve the overall health and quality of life for some of the most vulnerable Medicaid beneficiaries. Whether the potential is realized depends on the ability of the providers who, in some cases, have to make large changes in the way they deliver care to meet the model's requirements.
Administrative issues in getting health homes up and running may slow down the pace of implementation.
As is true with the rollout of any initiative, some challenges have stemmed from adopting new program infrastructure and administrative processes. Setting aside issues of practice transformation, many state programs spent the first months, if not the first year, of the health home operation developing and adjusting the mechanics of identifying and enrolling beneficiaries, verifying and reimbursing for services provided, and distributing clinical data for population management. In some cases, the result was significant administrative burden and lost productivity for participating providers.
In states where providers were given extra time to achieve health home qualifications, many were occupied with completing certification requirements to become recognized as medical homes or implementing new information technology systems. These tasks, which sometimes involved considerable staff time and financial costs, were occurring in tandem with enrollment and treatment of health home-eligible patients.
Most providers report payments cover the cost of providing services, but not the direct costs and productivity losses associated with practice transformation and HIT infrastructure improvements.
Providers generally report having opportunities for training, collaborative learning, technical assistance, and other support provided by the states or care networks, but many noted the lack of financial resources to fund practice transformation and HIT infrastructure improvements. Some providers found themselves strained for resources, and many felt that health home payment insufficiently compensated for the costs associated with implementation of the program.
Fundamental changes in the approach to care account for a substantial part of challenges providers encounter with provision of health home services.
In some cases, becoming a health home provider meant transforming from a physician-centered practice using paper charts and traditional communication channels to a patient-centered practice using a team-based approach and modern information technologies. In other cases, providers had to learn to change focus from treating acute illness to integrating care for high-need, chronically ill patients, or move from functioning in isolation to coordinating with other parts of the health care system and nonclinical community-based providers. Although the majority of health home providers across our evaluation states have had at least some experience with the medical home model and care management, many reported that becoming a health home presented the need to enhance and complement services they were providing.
Establishing essential relationships and communication between the health home providers, hospitals and other clinical and nonclinical providers takes substantial time.
State officials and providers both indicate continued improvement is needed in these relationships and processes, which are critical to comprehensive care management and coordination, integrating physical and mental/behavioral care, and, especially, effective transitional care. Developing cooperative relationships with hospitals was cited as a thorny issue in many cases. Providers and states generally indicated improvements in the extent to which most health homes get timely notifications of Medicaid-financed hospitalizations, but much less improvement in timeliness of emergency department notifications. Dependable and timely notification of Medicare-financed admissions and emergency department use appear to be virtually nonexistent.
The HIT systems in the evaluation states are so far inadequate to support the full range of health home functions, including care coordination and integration, cross-site exchange of information, and documentation of nonclinical services.
The greatest barriers to fully integrating an EHR--and an HIE, if available--providers cited were initial and ongoing financial cost associated with obtaining or modifying software to meet needs for new functionalities, maintaining licenses, and lost productivity when staff is learning new data systems. The plethora of HIT vendors operating in many states and the variable functionality and capabilities of EHRs providers have in place complicate the interoperability that would facilitate information exchange between hospitals and unaffiliated practices and among the various providers health home enrollees use. Even where the HIE systems are in place, user fees are sometimes a barrier, particularly when the lack of a critical mass of providers participating reduces their utility, ability to support data exchange, and their usefulness for large-scale data collection for population health management efforts. In the face of absent or inadequate EHRs and HIE infrastructure, providers often rely on traditional communication channels, suggesting that provider-to-provider relationships can in some cases substitute for functioning HIT and most likely enhance the utility of HIT when it is present.
Despite challenging implementation, health home providers believe the model presents a better way of approaching care for their high-cost, high-need patients.
Implementation of the health home program placed a significant burden on participating providers, many of whom found some of the processes frustrating and requirements challenging. Nevertheless, most providers we interviewed recognize the benefits to patients from the health home model and believe it is the right way to deliver care to high-need patients. We have heard many anecdotes of health home staff who conduct home visits, transport patients to medical appointment in their cars, and generally go above and beyond to make sure enrollees are getting the right care.
VII. ENDNOTES
-
Sec. 1945 State Option to Provide Care through a Health Home for Individuals with Chronic Conditions. http://www.ssa.gov/OP_Home/ssact/title19/1945.htm.
-
Centers for Medicare and Medicaid Services. Health Home State Plan Amendments effective March 2015. Please note that we count programs rolled out geographically using more than one SPA as a single program. This was the case in New York (3 SPAs), Vermont (2 SPAs), and Washington (2 SPAs).
-
Smith, VK, K Gifford, E Ellis, R Rudowitz, L Snyder. October 2014. Medicaid in an Era of Health and Delivery System Reform: Results from a 50-State Medicaid Budget Survey for State Fiscal Years 2014 and 2015. The Kaiser Commission on Medicaid and the Uninsured.
-
Spillman, BC, E Richardson, A Spencer, E Allen. 2014. Evaluation of the Medicaid Health Home Option for Beneficiaries with Chronic Conditions: Annual Report -Year Two. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. http://aspe.hhs.gov/basic-report/evaluation-medicaid-health-home-option-beneficiaries-chronic-conditions-annualreport-year-two. Accessed March 2015.
-
Ibid.
-
Nutting, PA, WL Miller, BF Crabtree, CR Jaen, EE Stewart, KC Stange. 2009. "Initial Lessons from the First National Demonstration Project on Practice Transformation to a Patient-Centered Medical Home." Annals of Family Medicine, 7(3):254-260; Crabtree, BF, PA Nutting, WL Miller, RR McDaniel, KC Stange, CR Jaén, and EE Stewart. December 2011. "Primary Care Practice Transformation Is Hard Work: Insights From a 15-Year Developmental Program of Research." Medical Care, 49(Suppl): S28-S35.
-
Patchias, EM, A Detty, M Birnbaum. 2013. Implementing Medicaid Health Homes in New York: Early Experience. Medicaid Institute at United Hospital Fund. http://www.uhfnyc.org/publications/880881.
-
Joslyn Levy and Associates. 2014. Care Management in New York State Health Homes. New York State Health Foundation.
-
Centers for Medicare and Medicaid Services. 2010. State Medicaid Director Letter Re: Health Homes for Enrollees with Chronic Conditions. http://downloads.cms.gov/cmsgov/archived-downloads/SMDL/downloads/SMD10024.pdf.
-
Rhode Island Opioid Treatment Program Services Health Home State Plan Amendment. Approved November 6, 2013. http://www.chcs.org/media/Rhode_Island_Health_Home_State_Plan_Amendment.pdf.
-
Iowa Department of Human Services. 2013. Integrated Health Homes For Individuals with Serious Mental Illness. http://dhs.iowa.gov/sites/default/files/private/IHH_FAQ_FINAL.pdf.
-
MaineCare Services. "Behavioral Health Homes (Stage B)." http://www.maine.gov/dhhs/oms/vbp/health-homes/stageb.html.
-
Overview of Final Health Home Application to Serve Children and Other Design Updates, November 5, 2014. https://www.health.ny.gov/health_care/medicaid/program/medicaid_health_homes/docs/2014-10-5_hhsc_webinar.pdf.
-
Oregon Patient-Centered Primary Care Home Model Implementation Reference Guide, Office for Oregon Health Policy and Research Patient-Centered Primary Care Home Program, October 2011.
-
CARF International. "Who We Are." http://www.carf.org/About/WhoWeAre/. Accessed February 2015.
-
CARF International introduces accreditation for health home services. http://www.carf.org/newsReleases.aspx?id=24511&blogid=144&terms=health+home. Accessed March 2015; Behavioral Health Home Certification. http://www.jointcommission.org/accreditation/behavioral_health_home.aspx. Accessed March 2015; New NCQA Patient-Centered Medical Home Standards Raise the Bar. http://www.ncqa.org/Newsroom/NewsArchive/2014NewsArchive/NewsReleaseMarch242014.aspx. Accessed March 2015.
-
Oregon Patient-Centered Primary Care Home Model Implementation Reference Guide.
-
State Medicaid Director Letter Re: Health Homes for Enrollees with Chronic Conditions.
-
Detailed information on each state's health home services definitions is available in Spillman, BC, E Richardson, A Spencer, E Allen. 2014. Evaluation of the Medicaid Health Home Option for Beneficiaries with Chronic Conditions: Annual Report -Year Two. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. http://aspe.hhs.gov/basic-report/evaluation-medicaid-health-home-option-beneficiaries-chronic-conditions-annualreport-year-two. Accessed March 2015.
-
State Medicaid Director Letter Re: Health Homes for Enrollees with Chronic Conditions.
-
Kronick, R et al. October 2009. "The Faces of Medicaid III: Refining the Portrait of People with Multiple Chronic Conditions," Center for Health Care Strategies. http://www.chcs.org/media/Faces_of_Medicaid_III.pdf.
-
Kasper, J, M O'Malley Watts, B Lyons. July 2010. "Chronic Disease and Co-Morbidity among Dual Eligibles: Implications for Patterns of Medicaid and Medicare Service Use and Spending." Kaiser Commission on Medicaid and the Uninsured.
-
Melek, S. July 2012. "Bending the Medicaid Healthcare Cost Curve through Financially Sustainable Medical-Behavioral Integration."
-
American Psychological Association. Patient Health Questionnaire. http://www.apa.org/pi/about/publications/caregivers/practice-settings/assessment/tools/patient-health.aspx.
-
Substance Abuse and Mental Health Services Administration. Screening, Brief Intervention, and Referral to Treatment. http://www.samhsa.gov/sbirt.
-
Anderson, G. 2007. "Chronic Conditions: Making the Case for Ongoing Care." Baltimore, MD: Johns Hopkins Bloomberg School of Public Health; Bernstein AB et al. January 2004. "Health Care in America: Trends in Utilization." Hyattsville, MD: National Center for Health Statistics. DHHS pub. no. 2004-1031; Coleman EA, S Min, A Chomiak, AM Kramer. 2004. "Posthospital Care Transitions: Patterns, Complications, and Risk Identification." Health Services Research Journal, 39(5):1449-65.
-
Forster, AJ et al. 2003. "The Incidence and Severity of Adverse Events Affecting Patients after Discharge from the Hospital." Annals of Internal Medicine: Journal, 138(3):161-7; Moore C et al. 2003. "Medical Errors Related to Discontinuity of Care from an Inpatient to an Outpatient Setting." Journal of General Internal Medicine, 18(8):646-51; Tsilimingras D, DW Bates. 2008. Addressing Postdischarge Adverse Events: A Neglected Area. The Joint Commission Journal on Quality and Patient Safety, 34(2):85-97.
-
Anderson G, J Horvath. The growing burden of chronic disease in America. Public Health Rep. 2004;119:263-70; Thorpe KE, DH Howard. 2006. "The rise in spending among Medicare beneficiaries: the role of chronic disease prevalence and changes in treatment intensity." Health Affairs, 25(w3):78-88.
-
Sadowski, LS, R Kee, TJ VanderWeele, D Buchanan. 2009. Effect of a Housing and Case Management Program on Emergency Department Visits and Hospitalizations Among Chronically Ill Homeless Adults: A Randomized Trial. JAMA, 301(17):1771-1778; Buchanan, D, R Kee, LS Sadowski, D Garcia. 2009. The Health Impact of Supportive Housing for HIV-Positive Homeless Patients: A Randomized Controlled Study. American Journal of Public Health, 99(S3):S675-S680; Cameron, A, L Lloyd, W Turner, G Macdonald. 2009. Working Across Boundaries to Improve Health Outcomes: A Case Study of a Housing Support and Outreach Service for Homeless People Living with HIV. Health and Social Care in the Community, 17(4):388-395.
-
New State Department of Health. "Housing and Health Homes." https://www.health.ny.gov/health_care/medicaid/program/medicaid_health_homes/housing_and_health_homes.htm. Accessed February 2015.
-
Arcury, TA, JS Preisser, WM Gesler, JM Powers. 2005. Access to Transportation and Health Care Utilization in a Rural Region. Journal of Rural Health, 21(1):31-38; Wallace, R, P Hughes-Cromwick, H Mull, K Snehamay. 2005. Access to Health Care and Nonemergency Medical Transportation: Two Missing Links. Transportation Research Record: Journal of the Transportation Research Board, 1924:76-84; Syed, ST, BS Gerber, LK Sharp. 2013. Traveling Towards Disease: Transportation Barriers to Health Care Access. Journal of Community Health, 38(5):976-993.
-
Office of the National Coordinator. "Benefits of EHRs." http://healthit.gov/providers-professionals/medical-practice-efficiencies-cost-savings. Accessed December 2014; Silow-Carroll, S, J Edwards, D Rodin. July 2012. Using Electronic Health Records to Improve Quality and Efficiency: The Experiences of Leading Hospitals, 1608(17), Commonwealth Fund. http://www.commonwealthfund.org/~/media/Files/Publications/Issue%20Brief/2012/Jul/1608_SilowCarroll_using_EHRs_improve_quality.pdf; Bunting, MB, MF Burke, MC Hoaglin, D Blumenthal. 2011. "The Benefits of Health Information Technology: A Review of the Recent Literature Shows Predominantly Positive Results," Health Affairs, 30(3): 464-471.
-
Silow-Carroll et al. 2012.
-
Office of the National Coordinator. "Benefits of EHRs."
-
State Medicaid Director Letter Re: Health Homes for Enrollees with Chronic Conditions.
-
Moreno L, D Peikes, A Krilla. June 2010. "Necessary But Not Sufficient: The HITECH Act and Health Information Technology's Potential to Build Medical Homes." AHRQ Publication No. 10-0080-EF. Rockville, MD: Agency for Healthcare Research and Quality.
-
Otter, S, G Bianco, R Dannenhoffer, H Chin, A Fallows. December 2014. Health Information Technology: A tool for optimizing health. http://www.oregon.gov/oha/Transformation-Center/Documents/HIT_Otter.pdf. Accessed April 2015.
-
Centers for Medicare and Medicaid Services. EHR Incentive Programs. http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/index.html?redirect=/EHRIncentivePrograms/; Centers for Medicare and Medicaid Services. An Introduction to the Medicaid EHR Incentive Program for Eligible Professionals. https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/EHR_Medicaid_Guide_Remediated_2012.pdf. Accessed March 2015; Centers for Medicare and Medicaid Services. State EHR Incentive Program Milestones and Web Resources guide. https://www.cms.gov/apps/files/statecontacts.pdf. Accessed March 2015.
-
Eligible professionals under the Medicaid EHR Incentive Program include physicians (primarily doctors of medicine and doctors of osteopathy), nurse practitioners, certified nurse-midwives, dentists, and physician assistants who furnish services in a FQHC or RHC that is led by a physician assistant. For additional eligibility requirements see CMS guidelines at http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/eligibility.html#BOOKMARK1.
-
New York Department of Health. "Health Homes and Health Information Technology." http://www.health.ny.gov/health_care/medicaid/program/medicaid_health_homes/health_info_technology.htm. Accessed January 2015.
-
New York Department of Health. "Health Information Technology." http://www.health.ny.gov/technology/. Accessed January 2015.
-
New York Department of Health. "Health Information Technology, Health Homes." https://www.health.ny.gov/health_care/medicaid/program/medicaid_health_homes/hh_grants_announce.htm. Accessed January 2015.
-
BlueCross BlueShield of North Carolina. September 28, 2011. BCBSNC, Allscripts Announce New Program to Implement Electronic Health Records with More Than 750 North Carolina Physicians." http://mediacenter.bcbsnc.com/news/bcbsnc-allscripts-announce-new-216311. Accessed March 2015.
-
Community Care of North Carolina. "CCNC, NCHIE Work Together to Improve Access to Health Data." http://www.communitycarenc.com/about-us/update-archive/ccnc-nchie-work-together/. Accessed March 2015.
-
SAMSHA-Health Resources and Services Administration Center for Integrated Health Solutions. September 2014. "Population Management in Community Mental Health Center-Based Health Homes."
Evaluation of the Medicaid Health Home Option for Beneficiaries with Chronic Conditions
This report was prepared under contracts #HHSP23320100025WI and #HHSP23337001T between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and the Urban Institute. For additional information about the study, you may visit the DALTCP home page at https://aspe.hhs.gov/office-disability-aging-and-long-term-care-policy-daltcp or contact the ASPE Project Officer, Emily Jones, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, SW, Washington, DC 20201. Her e-mail address is: Emily.Jones@hhs.gov.
Reports Available
Evaluation of the Medicaid Health Home Option for Beneficiaries with Chronic Conditions: Final Annual Report - Base Year (December 2012)
Evaluation of the Medicaid Health Home Option for Beneficiaries with Chronic Conditions: Annual Report - Year Two (June 2014)
Evaluation of the Medicaid Health Home Option for Beneficiaries with Chronic Conditions: Annual Report - Year Three (July 2015)