
Monday, January 27, 2020
Printer Friendly Version in PDF Format (9 PDF pages)
Modifiable Risk Factors for Dementia Prevention
Kristine Yaffe, MD
Scola Endowed Chair & Vice Chair
Professor, Psychiatry, Neurology & Epidemiology
Weill Institute Of Neurosciences
University Of California, San Francisco
Modifiable Risk Factors of Dementia for Prevention:Best Evidence and Scalability
- Identification of modifiable risk factors can help
- Understand the mechanisms associated with dementia development
- Enhance our ability to identify those at highest risk
- Improve prevention and treatment options
- Strongest Evidence:
- Cardiovascular factors
- Physical & cognitive activity
- Sleep quality & disorders
- Traumatic brain injury (TBI)
A Life Course Framework for Dementia
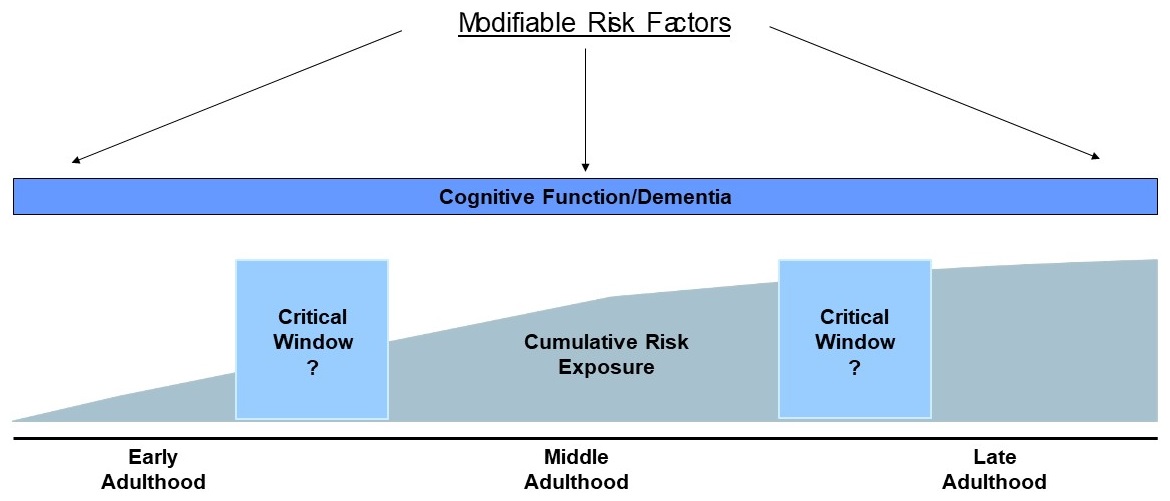 |
| K.Yaffe |
Cardiovascular Risk Factors
- Many studies on diabetes, hypertension, dyslipidemia, and obesity and increased risk of dementia
- Cardiovascular risk factors often co-occur and offer a way to identify high risk adults
- Controversy over the role of mid vs late life exposure
- Possible effects even earlier in the life course
| Late Life CVRFs and Increased Risk of Dementia |
|---|
 |
| Intensive BP Treatment & Decreased Risk of Dementia: SPRINT MIND | ||||||
|---|---|---|---|---|---|---|
| Outcomes | Treatment Group | Hazard Ratio (95% CI)[a] |
P Value | |||
| Intensive | Standard | |||||
| No. With Outcome/Person-Years |
Cases per 1000 Person-Years |
No. With Outcome/Person-Years |
Cases per 1000 Person-Years |
|||
| Probable dementia | 149/20569 | 7.2 | 176/20378 | 8.6 | 0.83(0.67-1.04) | .10 |
| Mild cognitive impairment[b] | 287/19690 | 14.6 | 353/19281 | 18.3 | 0.81(0.69-0.95) | .007 |
| Composite of mild cognitive impairment or probable dementia | 402/19873 | 20.2 | 469/19488 | 24.1 | 0.85(0.74-0.97) | .01 |
|
||||||
Yaffe et al, JAMA, 2004; Williamson et al, JAMA, 2019.
Emerging Evidence for Early Adult Risk Factors
| Cumulative Exposure in Early Adulthood & Midlife Cognition |
|---|
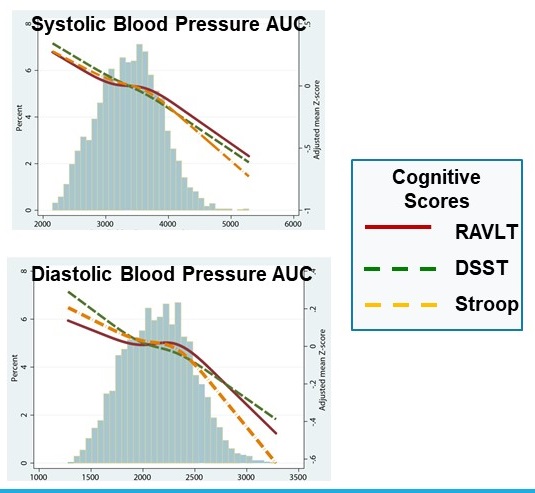 |
| Results from a Pooled Cohort Study Early Adult & Mid Life Hypertension Associated with Greater Cognitive Decline But Late Life Hypertension Associated with Less Cognitive Decline |
|---|
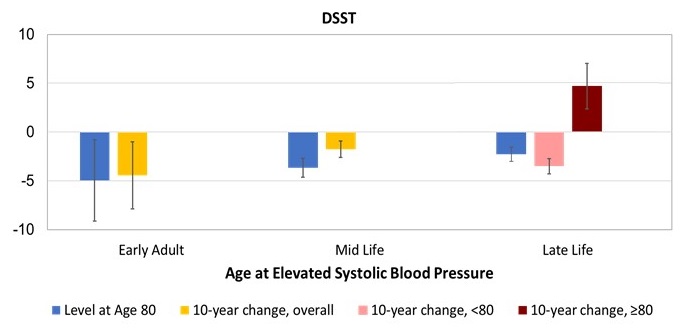 |
Yaffe et al, Circulation, 2014; Yaffe et al, AAIC, 2019.
Physical Activity
- Strong observational data
- But more randomized trials needed
- Long-term studies would help determine optimal type, intensity, and duration of physical activity
- Recent, large RCT (LIFE) did not find any benefits for cognitive function or risk of MCI/Dementia
| Walking Reduces Risk of Late Life Cognitive Decline |
|---|
 |
| Exercise Improves Cognitive Function in Older Adults with Memory Complaints |
|---|
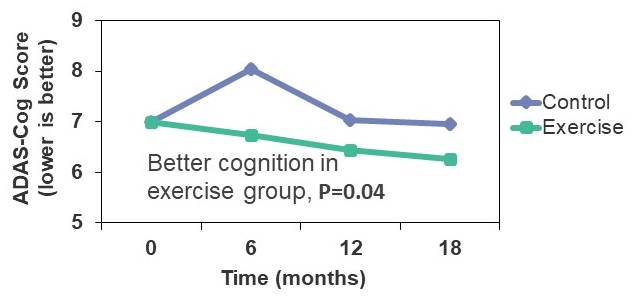 |
Yaffe et al, Arch Intern Med, 2001; Lautenschlager, JAMA, 2008
Cognitive Activity
- In observational studies, higher education, higher occupational achievement and more mentally stimulating activities are associated with better cognitive function
- Increased cognitive stimulation and activity may build 'cognitive reserve' which helps the brain function normally despite neuronal damage
- Few trials other than ACTIVE
| Cognitive Reserve Modifies the Association between Amyloid-β & Cognitive Decline |
|---|
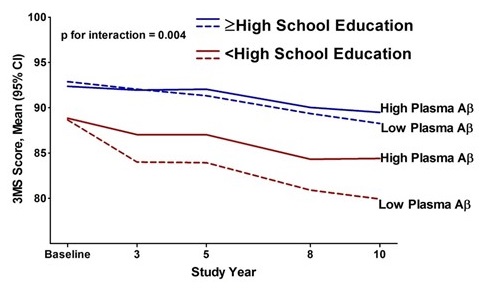 |
| ACTIVE Trial: Benefits in reasoning in reasoning training group & processing speed in speed training group over 10 years |
|---|
 |
Stern et al, Alz Dis Assoc Dis, 2005; Yaffe et al, JAMA, 2011; Rebok et al, JAGS, 2014.
Sleep Quality and Disorders
- Sleep changes with aging
- Disturbances very common in older populations
- Decreased sleep quality
- Shifted circadian rhythms
- Sleep apnea
- Overall less restorative sleep in older age
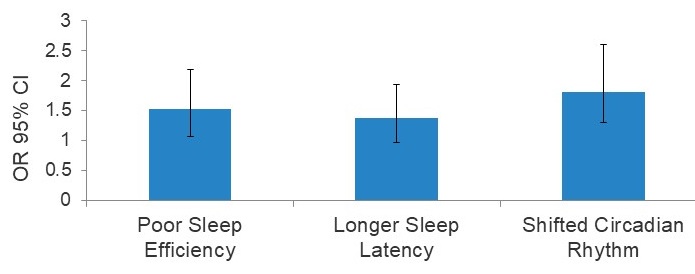
- Poor sleep efficiency, long sleep latency, abnormal circadian rhythms, and sleep apnea increase risk of developing MCI/dementia
- Additional research needed, including work on mechanisms and RCTs
| Poor Sleep Quality and Increased Risk of Dementia |
|---|
 |
| Sleep Disordered Breathing and Increased Risk of MCI/Dementia |
|---|
 |
Diem et al, AJGP, 2016; Tranah…Yaffe, Annals of Neurology, 2011; Yaffe et al, JAMA, 2011.
Increased Risk of Dementia with Traumatic Brain Injury
| Meta-analysis of Head Injury as a Risk Factor for Dementia in Observational Studies |
|---|
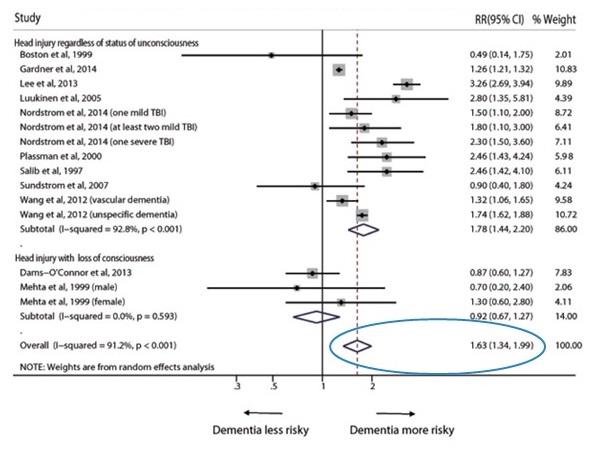 |
| TBI and Increased Risk of Dementia |
|---|
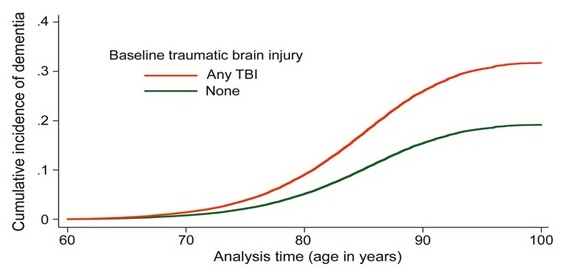 |
| Emerging Evidence for Mild TBI |
|---|
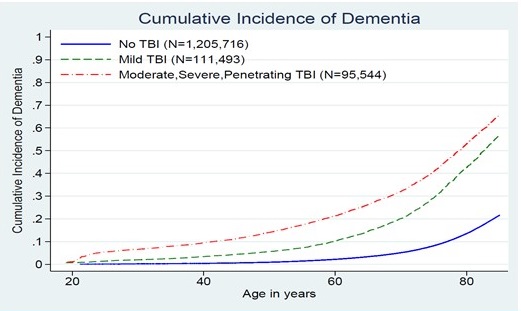 |
Li, PLOS One, 2017; Barnes…Yaffe, Neurology, 2014; Barnes…Yaffe, JAMA Neurology, 2018.
Two Different Perspectives on Modifiable Risk Factors, Prevention, and Dementia
- Preventing Cognitive Decline and Dementia: A Way Forward
- National Academies of Sciences, Engineering, and Medicine commissioned by NIA
- AHRQ systematic review of RCTs
- Sample size >500, minimum 6-months follow-up
- Encouraging but inconclusive for 3 risk factors: Cognitive training, blood pressure management, and physical activity
- More work needs to be done
- Dementia Prevention, Intervention, & Care
- The Lancet Commission of experts in the field
- "Best evidence" review of literature
- Observational studies and RCTs
- Recommend interventions for 9 risk factors: Childhood education, exercise, social engagement, smoking, and management of hypertension, hearing loss, depression, diabetes, and obesity
- "Be ambitious about prevention"
A Middle Ground?
We need to inform the public that cognition and dementia risk are also susceptible to the effects of many cardiovascular and metabolic risk factors. The concept that the brain (primarily neuronal connections) continues to grow and change even until late life is a powerful public health message.
Yaffe et al, JAMA Internal Medicine, 2018.
Potential For Primary Prevention
- Estimate impact of risk factor reduction on AD prevalence for 7 modifiable factors
- Mid-life hypertension
- Mid-life obesity
- Diabetes
- Depression
- Physical inactivity
- Low Education
- Smoking
- Population attributable risks (PARs): estimate proportion of disease caused by a given risk factor
- Calculated using risk factor prevalence & relative risk from most recent/comprehensive literature
Barnes and Yaffe, Lancet Neurology, 2011; Norton et al, Lancet Neurology, 2014.
Risk Factor Reduction Could Significantly Lower Prevalence Of AD, United States
| Risk Factor | Population Prevalence | Reletive Risk (95% CI) |
PAR % (Range) |
|---|---|---|---|
| Physical inactivity | 33% | 1.8 (1.2, 2.8) | 21% (6-37%) |
| Smoking | 21% | 1.6 (1.2, 2.2) | 11% (3-20%) |
| Depression | 19% | 1.7 (1.4, 1.9) | 11% (8-15%) |
| Mid-life hypertension | 14% | 1.6 (1.2, 2.2) | 8% (2-15%) |
| Mid-life obesity | 13% | 1.6 (1.3, 1.9) | 7% (4-11%) |
| Low education | 13% | 1.6 (1.4, 1.9) | 7% (4-10%) |
| Diabetes | 10% | 1.5 (1.2, 1.8) | 5% 2-7%) |
| Combined (max.) | 53% | ||
| Combined (adj.) | 31% |
 |
Barnes and Yaffe, Lancet Neurology, 2011; Norton et al, Lancet Neurology, 2014.
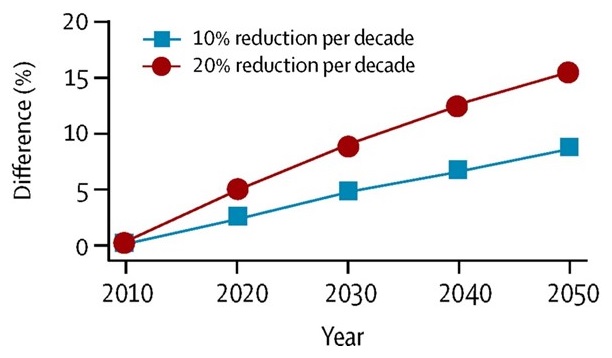
Trends For Dementia
- Lower or stable incidence of cognitive impairment or dementia in several countries
- In the Netherlands, also observed higher total brain volumes
 |
Langa et al, Alzheimer's & Dementia, 2008; Shrijvers et al, Neurology, 2012; Qiu et al, Neurology, 2013; Matthews et al, The Lancet, 2013; Satizabal et al, NEJM, 2016.
Implications
- Secular trends suggest that critical public health strategies at the societal level can impact dementia trends
- Decreased cardiovascular disease can shift dementia incidence and prevalence
- Improved education and economic well-being may also contribute to these shifts
- However, epidemics of sedentary lifestyle, obesity, and diabetes loom and could have opposite effects
Larsen, Yaffe, Langa, NEJM, 2013; Satizabal et al, NEJM, 2016.
Dementia Prevention: Multi-Domain Trials
| Trial | Population | Intervention | Results |
|---|---|---|---|
| Prevention of Dementia by Intensive Vascular Care (preDIVA) | Dementia-free MMSE>23 70-78 yrs |
CVD care: medical trt, diet and exercise counseling, smoking cessation | No benefit for cognition |
| Multidomain Alzheimer Preventive Trial (MAPT) | Memory complaints MMSE >24 > 70 yrs |
Diet counseling, exercise and cognitive training, DHA 800 mg/day | No benefit for dementia risk |
| Australian Imaging Biomarkers and Lifestyle Flagship Study of Aging (AIBL- Active trial) | Memory complaint or MCI > 1 risk factor for CVD >60 yrs |
Reduce CVD risk with physical activity and behavioral counseling | No benefit for WMH/hippocampal loss |
| Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER) | Dementia risk score>6 Mean or slightly below cognitive function 60-75 yrs |
Intensive CVD management, diet counseling, exercise and cognitive training | Benefits for cognition |
Multi-domain Alzheimer's Risk Reduction Study (SMARRT)
- Previous multi-domain interventions relatively intensive and all standardized, may be difficult to implement in real-world settings
- Personalized and pragmatic, delivered through a U.S. integrated healthcare delivery system, and leverage advancements in digital health
- Identify Higher-Risk Patients
- Age >70
- Cognitive concern
- low/normal cognitive performance
- At least 2 risk factors by EMR
- 2-year Intervention -- Personalized Risk Reduction Plan vs. Health Education
- Personalized intervention targeting cardiovascular risk factors, smoking, physical, cognitive, and social activity, depression, diet, sleep, and medication management
- Outcomes
- Cognitive function/ Dementia
- Physical performance
- Functional ability
- Quality of life
Yaffe et al, J Alzheimers Dis, 2019.
Dementia Prevention: Where Are We?
- Several promising, low risk and low cost, alone or in combination
- But controversial conclusions on quality of the evidence
- Need more longitudinal and life course studies
- Insufficient RCTs, particularly multi-domain interventions
- Ultimately, primary prevention will probably be like cardiovascular disease: managed by a combination of lifestyle factors and medications