
Identifying Medicare Beneficiaries with Disabilities: Improving on Claims-Based Algorithms
Yonatan Ben-Shalom and David Stapleton
Mathematica Policy Research
January 2014
This report was prepared under contract #HHSP23320095642WC between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and Mathematica Policy Research. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/office_specific/daltcp.cfm or contact the ASPE Project Officer, Hakan Aykan, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. His e-mail address is: Hakan.Aykan@hhs.gov.
The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS
Data Source
Study Population
Self-Reported Disability Indicators
Claims-Based Disability Indicators
Analytical Methods
Self-Reported and Claims-Based Disability
Logistic Model Estimates
Receiver Operating Characteristic Curves and Predicted Probability Thresholds
Congruence Analysis
APPENDICES
APPENDIX A: ADDITIONAL TABLES
LIST OF FIGURES
FIGURE 1: ROC Curve Versus Claims-Based Disability Flags, Intermediate Disability Measure, Age 65 or Older
FIGURE 2: ROC Curve Versus Claims-Based Disability Flags, Intermediate Disability Measure, Age 18-64
LIST OF TABLES
TABLE 1: Percentage of Medicare Beneficiaries with Disability, Self-Reported and Claims-Based
TABLE 2: Cross-Tabulation of Self-Reported Limitation in at Least One ADL and Claims-Based Disability
TABLE 3: Logistic Regression Results for Models Predicting a Limitation in at Least One ADL
TABLE 4: Characteristics for Medicare Beneficiaries Classified Congruently and Incongruently by the Predictive Model, by Self-Reported Disability Status, Age 65 or Older
TABLE 5: Characteristics for Medicare Beneficiaries Classified Congruently and Incongruently by the Predictive Model, by Self-Reported Disability Status, Age 18-64
TABLE A.1: SSA-HIT Business Rules Included in the SSA-HIT Claims-Based Indicator
TABLE A.2: Logistic Regression Results for Models Predicting a Limitation in at Least Three ADLs
TABLE A.3: Logistic Regression Results for Models Predicting a Limitation in at Least One ADL or IADL
TABLE A.4: Logistic Regression Results for Models Predicting a Long-Term Limitation in at Least One ADL
TABLE A.5: Logistic Regression Results for Models Predicting a Long-Term Limitation in at Least Three ADLs
TABLE A.6: Logistic Regression Results for Models Predicting a Long-Term Limitation in at Least One ADL or IADL
ABSTRACT
We use data on fee-for-service Medicare beneficiaries who first responded to the Medicare Current Beneficiary Survey in 2003-2006 to assess the feasibility of using existing claims-based indicators to identify community-dwelling Medicare beneficiaries with disability based solely on the conditions for which they are being treated. We construct six claims-based disability indicators and use the indicators in logistic regression models to predict three indicators of disability based on self-reports on activities of daily living (ADLs) and instrumental activity of daily living. We assess the performance of the predictive models, using receiver operating characteristic curves and misclassification analysis. At a predicted probability threshold chosen to maximize the sum of sensitivity and specificity, our model prediction is congruent with self-reports of disability for 72 percent of Medicare beneficiaries age 65 or older who reported they had a limitation in at least one ADL and 65 percent of those who did not report having any ADL limitations. We conclude that predictive models that incorporate multiple claims-based indicators provide an improved tool for researchers seeking to identify people with disabilities in claims data.
ACRONYMS
The following acronyms are mentioned in this report and/or appendices.
| Acronyms | |
| ACG | Adjusted Clinical Groups |
| ADL | Activity of Daily Living |
| ALS | Amyotrophic Lateral Sclerosis |
| ARCS | Access Risk Classification System |
| AUC | Area Under the Curve |
| CABG | Coronary Artery Bypass Grafting |
| CDPS | Chronic Illness and Disability Payment System |
| CJD | Creutzfeldt-Jakob Disease |
| CMS | HHS Centers for Medicare and Medicaid Services |
| COPD | Chronic Obstructive Pulmonary Disease |
| Dx-PM | Diagnoses-Based Predictive Model |
| ESRD | End Stage Renal Disease |
| FRDA | Fredreich's Ataxia |
| HHS | U.S. Department of Health and Human Services |
| HIT | Health Information Technology |
| IADL | Instrumental Activity of Daily Living |
| ICD-9 | International Classification of Diseases, 9th Revision |
| ICF | International Classification of Functioning, Disability and Health |
| MCBS | Medicare Current Beneficiary Survey |
| OI | Osteogenesis Imperfect |
| ROC | Receiver Operating Characteristic |
| SMA | Spinal Muscular Atrophy |
| SSA | U.S. Social Security Administration |
| SSDI | Social Security Disability Insurance |
EXECUTIVE SUMMARY
Objectives: (1) To assess the feasibility of using existing claims-based algorithms to identify community-dwelling Medicare beneficiaries with disability based solely on the conditions for which they are being treated; and (2) to improve upon these algorithms by combining them in predictive models. This capability is important for helping assess whether care coordination interventions and other programs designed to improve outcomes for a broad class of individuals are effective for the subset who have disabilities. Such information is typically unavailable in claims-based analyses.
Data Source: Data from the Medicare Current Beneficiary Survey (MCBS) and matched Medicare claims on 12,415 community-dwelling fee-for-service Medicare beneficiaries who completed the MCBS baseline questionnaire in 2003-2006.
Study Design: Using Medicare claims data, we created six potential indicators of disability and used the indicators in logistic regression models to predict three indicators of disability based on self-reports: limitation in at least three activities of daily living (ADLs), limitation in at least one ADL, and limitation in at least one ADL or instrumental activity of daily living. Using receiver operating characteristic curves, we compared the true positive (sensitivity) and true negative (specificity) rates of the individual indicators to those of the regression-based predictive models.
Principal Findings: The predictive performance of the regression-based models is better than that of the individual claims-based indicators, providing better sensitivity for any level of specificity and vice versa. For community-dwelling Medicare beneficiaries who are age 65 or older, we use a decision rule that classifies an individual as having a disability if his or her predicted probability of having a disability exceeds a specified value. This threshold value is that which maximizes the sum of sensitivity and specificity. Using this threshold, our model prediction is congruent with self-reports of disability for 72 percent of those who reported they had a limitation in at least one ADL and 65 percent of those who did not report having any ADL limitations. Examination of the incongruent cases showed that obese individuals who have a disability were especially likely to be missed by the model. For individuals ages 18-64, the model fails to identify nearly half who reported limitation in at least one ADL (sensitivity=0.54). For this group, dual-eligible beneficiaries with disabilities were especially likely to be missed by the model. In both age groups, the individuals without self-reported disabilities who are most likely to be misclassified as having disabilities were those in relatively good health (according to their self-reports) who had relatively high service use.
Conclusions: Predictive models, which may be tailored according to beneficiary subgroup and self-reported disability measure, provide a better sensitivity-specificity trade-off than individual claims-based disability flags and therefore provide an improved tool for researchers seeking to identify people with disabilities in claims data. Such models may be improved by incorporating data on service use (such as home health care and skilled nursing facilities) and prescriptions in general and Medicaid data for dual-eligible beneficiaries in particular (to capture use of long-term support services).
INTRODUCTION
Research on disability services is a top priority in the United States because people with disabilities have considerable need for long-term services and supports (Iezzoni 2013). Claims data are a potentially powerful tool for disability research, and identifying people with disabilities in claims data would help assess whether interventions designed to improve outcomes for a broad class of individuals are effective for the subset of program participants who have disabilities. However, although claims data could potentially be used to identify individuals with disabilities, current claims-based tools have limited ability to identify people with disabilities and to distinguish among important groups within this population.
Research on disability services must start by defining what is meant by disability. We use the International Classification of Functioning, Disability and Health (ICF) as a conceptual framework for defining disability and we adopt ICF definitions for disability-related terms. According to the ICF, which is emerging as an established conceptual framework for much disability research, an individual has a disability if she experiences a functional limitation as a result of the interaction between her health, personal characteristics, and environment (Jette 2009). A disability exists if the person has a decrease in the functionality of a body function or structure (an impairment), a decrease in the ability to perform an activity (an activity limitation), or a decrease in the ability to participate in basic social roles (a participation restriction). This is a very broad definition of disability and does not provide a clear distinguishing line between those with disabilities and those without a disability. Although we focus in this study on identifying those with activity limitations, our methodology could be used to support research on populations defined by alternative means.
A major challenge in identifying disability in claims data is that not all disability-related conditions generate disability-related claims. Further, the disability-related information that is included in claims is far from what would be required to determine whether a person has a disability (however defined), the severity of the disability, and whether it is a temporary or long-term disability (Iezzoni 2002, 2013).
Past efforts to identify people with disabilities using claims and other medical data have had limited success. Bogardus et al. (2004) reviewed entire medical records from 519 hospitalizations for comments regarding limitations in 14 activities of daily living (ADLs) and instrumental activities of daily living (IADLs) and compared them to interviews in which patients were asked specifically about these limitations. Using data from the medical records, they were able to correctly classify 71 percent of those who reported a limitation in any of the 14 activities and 81 percent of those who reported no limitations (sensitivity=0.71, specificity=0.81). Palsbo et al. (2008) developed the Access Risk Classification System (ARCS) algorithm using automated claims data to classify people by their ability to access routine care. When they classified individuals into two groups of those needing proactive care coordination due to "one or more chronic conditions that cause major functional limitations," and all others, they correctly classified 83 percent of those who needed care coordination but only 30 percent of those who did not (sensitivity=0.83, specificity=0.30). Sternberg et al. (2012) assessed the ability of the Adjusted Clinical Groups (ACG) diagnoses-based predictive model (Dx-PM), which is part of the Johns Hopkins ACG Case Mix System, to identify frail individuals age 65 or older. The ACG Dx-PM uses age, sex, diagnostic codes, and pharmacy data (if available) in predictions. The authors found that the ACG frailty tag identified frailty--as determined by the Vulnerable Elders Survey--with "moderate success."1
In this study, we explore the feasibility of improving upon existing claims-based algorithms and criteria that identify "disability" by combining them in predictive models tailored to the disability measure and subgroup of interest. We estimate these models and assess their predictive performance using indicators of self-reported disability based on records in the Medicare Current Beneficiary Survey (MCBS). Using receiver operating characteristic (ROC) curves (Lasko et al. 2005), we compare the sensitivity and specificity rates of the regression-based predictive models to those of the individual indicators. In addition, we compare the characteristics and service use of those for which the model prediction is congruent with self-reported disability and those for which the model prediction is incongruent with self-reports. We use the terms "congruent" and "incongruent," rather than "correct" and "incorrect", to acknowledge the fact that self-reported disability in the MCBS does not represent a gold standard for the sorting of individuals by disability status; instead, the claims-based model and the self-reports represent different classification methods.
We find that the predictive models lead to disability classifications that are substantially more congruent with MCBS self-reports than the individual claims-based disability indicators, and that congruence is much higher for Medicare beneficiaries age 65 or older than for those under age 65. Even so, for each age group the predictions of the model that produces the most congruent results differ from self-reported disability for many respondents. A few identifiable factors differentiate congruent and incongruent cases. For those over age 65, the model predicts "no disability" relatively frequently when the individual self-reports both a disability and obesity. Similarly, for those ages 18-64 the model predicts "no disability" relatively frequently when the individual reports a disability and is also eligible for Medicaid (hereafter "dual-eligible" beneficiaries). In both age groups, the model frequently predicts "disability" when the claims data show relatively high service use during the observation period but survey response indicates both no disability and relatively good health.
The findings suggest ways to produce predictions from claims data that are more congruent with survey-based self-reports of disability, especially when there is a specific research objective to guide the modeling. This includes the incorporation of data on service use (such as home health care and skilled nursing facilities), prescriptions, and long-term support services provided to dual-eligible beneficiaries (from Medicaid claims). Incorporation of other claims-based algorithms, even if not specifically designed to identify people with disability, may also improve predictive performance. Researchers interested in disability populations different from that examined in this study could use the same methodology and data to develop a model for their population of interest.
METHODS
Data Source
The MCBS is a rotating panel survey in which four overlapping panels of Medicare beneficiaries are surveyed each year (Murgolo 2010). Each panel includes a nationally representative sample of Medicare beneficiaries. Respondents are interviewed in person three times a year for four years. The MCBS includes disproportionately large samples for beneficiaries age 85 and older and those younger than 65. Individuals in the latter group are eligible for Medicare because they have been determined to have a work disability under the definition used for Social Security Disability Insurance (SSDI), or have end stage renal disease (ESRD).2 Information on respondents who live in the community is collected through a "community" interview done at their home. Information on respondents who are institutionalized at the time of the survey is collected through an "institutional" interview of knowledgeable facility staff. For both groups, a "baseline questionnaire" is administered when the respondent first enters the survey. The Access to Care data files, available since 1991, represent the "always-enrolled" Medicare population--those who were enrolled in Medicare at the beginning of the year and were still alive for the MCBS fall interview. In the fall interview, information is collected about beneficiaries' health status and functioning, access to medical providers, and satisfaction with their health care. Additional information on medical diagnoses and procedures is available in the form of matched Medicare claims.
Study Population
The analytic sample for this study pools four consecutive MCBS panels and includes respondents who completed the community baseline questionnaire in 2003-2006 and either the community or facility questionnaire in their second MCBS year. We exclude from the sample: (1) respondents who were institutionalized at baseline; (2) respondents who died before their second MCBS year; and (3) beneficiaries who were enrolled in Medicare Advantage in any month during their first and second MCBS calendar year. We exclude the first group because they can be readily identified in administrative data and the challenge for researchers is to identify community-dwelling Medicare beneficiaries who might benefit from home and community-based service interventions. We exclude the second group because we are unable to construct for them the self-reported disability indicators, which are based on responses in the second MCBS year (see below). We exclude the last group because claims data are not available for services received through Medicare Advantage plans. The study sample includes 12,415 Medicare beneficiaries (10,057 individuals age 65 or older and 2,357 ages 18-64).
Self-Reported Disability Indicators
We construct three indicators of self-reported disability based on responses collected in fall of the second MCBS year to questions regarding difficulties in performing ADLs or IADLs (Katz 1963). The ADLs include bathing/showering, dressing, eating, transferring (getting in/out of bed/chair), walking, and toileting. The IADLs include using the telephone, light housework, heavy housework, meal preparation, shopping, or managing money. For each ADL and IADL, we first create an indicator for whether the respondent reports difficulty in performing the activity or whether she does not perform the activity due to health. Our most restrictive disability indicator is for those reporting a difficulty in at least three ADLs, an intermediate indicator includes those reporting a difficulty in at least one ADL, and the broadest indicator includes those reporting a difficulty in at least one ADL or IADL.3
Claims-Based Disability Indicators
We construct six claims-based disability indicators using information in the Medicare claims. None of these indicators was specifically designed to identify those with disabilities according to the ADL/IADL definitions we have adopted for this study, but each identifies groups that seem very likely to have ADL/IADL limitations. We describe the six claims-based indicators below.
The Chronic Illness and Disability Payment System (CDPS) was developed by Kronick et al. (2000) as a diagnostic classification system states could use to risk-adjust Medicaid payments to health maintenance organizations. It is designed to predict health expenditures using International Classification of Diseases, 9th Revision (ICD-9), diagnosis codes and has been used to identify people with disabilities (Irvin and Johnson 2006; Pavetti et al. 2010). The CDPS classifies individuals into 19 diagnostic categories and further disaggregates them by cost (extra high, very high, high, medium, low, very low, and super low). Our CDPS indicator includes the diagnostic subcategories identified as "medium cost" and above, which are relevant for 14 of the CDPS diagnostic categories.4
The Access Risk Classification System (ARCS) algorithm was developed by Palsbo et al. (2008) to classify people by their ability to access routine care using automated claims data. The algorithm uses ICD-9 codes, Healthcare Common Procedure Coding System codes, and Current Procedural Terminology, 4th edition codes, as well as the number of prescriptions. Our ARCS indicator includes the algorithm's highest-risk class, which identifies individuals with "multiple chronic conditions and complex medical needs that severely impair a person's independence."5
The Social Security Administration's health information technology (SSA-HIT) business rules (SSA 2012) are being developed to identify diagnoses and procedure codes or combinations of codes that are sufficient to meet or equal SSA's Listing of Impairments--the medical criteria that SSA uses to determine eligibility for SSDI, as well as Supplemental Security Income for those under age 65. These rules cover only a subset of the impairments in the listings--those most likely to be identified in claims data--and are preliminary. Our implementation of the SSA-HIT indicator omits the few rules that include a time dimension as they would add considerably to the complexity of analyzing claims data.6
In addition to CDPS, ARCS, and SSA-HIT, we examine three claims-based disability indicators that use ICD-9 codes to identify: (1) psychiatric disorders; (2) cognitive disorders (dementia and Alzheimer's); and (3) intellectual disability. The psychiatric disorders indicator includes the ICD-9 codes beginning with 295 (schizophrenia) and 296 (affective disorder), as well as other ICD-9 codes indicating psychotic, neurotic, personality, and other nonpsychotic mental disorders;7 the dementia and Alzheimer's indicator includes the ICD-9 codes 290.2, 290.3, 290.4, 290.8, and 331.0; the intellectual disability indicator includes the ICD-9 codes 317 ("mild intellectual disability"), 318.0 ("moderate intellectual disability"), 318.1 ("severe intellectual disability"), 318.2 ("profound intellectual disability"), and 319 ("unspecified intellectual disability").8
Analytical Methods
Measuring the Performance of Claims-Based Disability Indicators in Predicting Self-Reported Disability
For each of the three self-reported disability indicators, we estimate--separately for the two age groups--a logistic model in which the disability indicator is the dependent variable and the main predictors are the six claims-based disability indicators. For both age groups, additional predictors include a small number of variables that are readily available in Medicare administrative records--age, sex, and an indicator for dual-eligibility (defined as any Medicaid participation during the year). For those who are age 65 or older, we also include an indicator for Medicare entitlement before age 65 (indicative of SSDI or ESRD prior to age 65) and interactions between this variable and each of the six disability indicators as well as the dual-eligibility indicator.9
For each of the estimated models, we construct an ROC curve which depicts all the possible sensitivity-specificity combinations for that model. Usually used to evaluate classification and prediction models in biomedical informatics research, ROC analysis evaluates the predictive performance of a model by capturing the trade-off provided between sensitivity and specificity (Lasko et al. 2005). "Sensitivity" is defined as the proportion of cases with a condition that the model correctly classifies as having the condition and "specificity" is defined as the proportion of cases not having the condition that are correctly classified as not having the condition. In our context, the "condition" is self-reported disability, as captured in the MCBS. Each point on a model's ROC curve corresponds to a threshold that could be used along with predictions from the model to classify observations for the presence of the condition: if the predicted value is above the threshold, the observation is labeled "positive;" if not, it is labeled "negative." For any given threshold, the model will classify a certain number of individuals in the sample as "positive" and the rest as "negative." At a sufficiently high threshold, all cases will be classified as negative so the true positive rate (sensitivity) will be 0.0 and the false negative rate (specificity) will be 1.0. As this threshold is reduced, more and more cases will be classified as positive; hence, sensitivity will increase and specificity will decline--eventually to a threshold at which sensitivity is 1.0 and specificity is 0.0 because all cases are classified as positive.
The ROC curve is a plot that shows how sensitivity and specificity change as the threshold varies from a value so high that all cases are classified as negative to one that is so low that all cases are classified as positive. The points are plotted on a graph in which sensitivity is measured on the vertical axis and one minus specificity (or the false positive rate) is measured on the horizontal axis, so the ROC curve starts at the (0,0) point and slopes upward until it reaches the (1,1) point. The most commonly used index for a model's accuracy is the AUC ROC. As Bamber (1975) has shown, the AUC equals the probability that the model's predicted value for a randomly chosen "positive" is greater than the predicted value for a randomly chosen "negative". The AUC for a perfect test is 1.0, while the AUC for random chance is 0.5. The latter corresponds to an ROC curve that runs diagonally from (0,0) to (1,1), and is commonly included in the ROC space (see Figure 1 and Figure 2).
In the context of this study, it is important to recognize that the terms "true" and "false" should not be interpreted as implying that the self-report of disability is "correct" and the prediction is either correct (true positive or true negative) or incorrect (false positive or false negative). Instead, "true" only means that the prediction matches the survey response and "false" means that it does not. We have adopted this terminology because it is the technical standard for the literature and because we are using the claims data to predict the survey responses.
For brevity, we limit the remainder of the analysis to just the intermediate MCBS disability indicator, which requires a limitation in at least one ADL. For each age group, we determine the point (and respective predicted probability threshold) on the ROC curve that maximizes the sum of sensitivity and specificity, also known as Youden's Index (Youden 1950). We then compare the sensitivity and specificity of the model's prediction at this point on the ROC curve to the sensitivity and specificity of the individual claims-based indicators. That is, we compare the true positive and true negative rates of the model's prediction at Youden's Index to the true positive and true negative rates achieved by using the individual claims-based indicators to directly predict self-reported disability without the use of any model.
Analysis of Congruence
Based on the model that produces predictions most congruent with self-reported disability, we conduct additional analysis to better understand the reasons why some cases are congruent and others are not. We first use the estimated logit model and its respective Youden's Index to classify the MCBS respondents in our sample into one of four groups: (1) those who self-report a disability and are also classified as having a disability according to the model ("true positives"); (2) those who self-report a disability but are classified as not having a disability ("false negatives"); (3) those who do not self-report a disability but are classified as having a disability ("false positives"); and (4) those who do not self-report a disability and are classified as not having a disability ("true negatives"). We then compare descriptive statistics for numerous characteristics across these four groups as measured in the year after baseline to identify reasons for incongruence and gain insights on how congruence might be increased. Sociodemographic characteristics include indicators for being married, employed, having income less than $25,000, and living in a metropolitan area, as well as categorical variables for race/ethnicity (White, Black, Hispanic, other), highest grade completed, and number of people in the household. Self-reported health variables include indicators for health status, social activity being limited by health, being obese, and previously being told of having the following conditions: high blood pressure, heart attack, stroke, cancer other than skin cancer, diabetes, dementia/Alzheimer's, emphysema, asthma, or chronic obstructive pulmonary disease (COPD). Measures of service use (from the MCBS Cost and Use file and for the year after baseline) include the number of and expenditures on: inpatient stays, home health visits, outpatient visits, medical provider visits, institutional events, and prescriptions.
RESULTS
Self-Reported and Claims-Based Disability
In Table 1, we show the percentages of Medicare beneficiaries in the study population classified as having a disability by each of the self-reported or claims-based disability indicators. Among individuals age 65 or older, 7.9 percent reported limitations in three or more ADLs, 26.5 percent reported a limitation in at least one ADL, and 40.3 percent reported a limitation in at least one ADL or IADL. The respective percentages are considerably higher among the subgroup who first qualified for Medicare before age 65 due to disability, and are much closer to those for the younger age group. Among individuals ages 18-64, 16.5 percent reported limitations in three or more ADLs, 44.0 percent reported limitation in at least one ADL, and 70.3 percent reported limitation in at least one ADL or IADL. Notably, close to 30 percent in this age group report no ADL or IADL even though SSA had previously determined that they were unable to work because of a disability. One possible explanation is that some who qualify for SSDI benefits due to a mental impairment or other medical conditions are highly functional in terms of performing the ADLs and IADLs. Another possibility is that some beneficiaries do not report a limitation even if they have it ("measurement error"). The CDPS, ARCS, and SSA-HIT disability indicators pick up roughly similar percentages of each age group; the psychiatric disorder and intellectual disability indicators pick up notably larger percentages of those who are ages 18-64, and the dementia/Alzheimer's indicator picks up a notably larger percentage of individuals age 65 or older.
| All | Age 65 or Older | Age 18-64 | ||||||
| All | Medicare Before Age 65 | |||||||
| Mean | SE | Mean | SE | Mean | SE | Mean | SE | |
| NOTE: Based on analysis of the MCBS. The study population includes respondents who completed the community baseline questionnaire in 2003 to 2006 and either the community or facility questionnaire in their second MCBS year. Beneficiaries enrolled in Medicare Advantage in any month during their first and second MCBS calendar year are excluded. | ||||||||
| Self-Reported Disability | ||||||||
| Three or more ADL limitations | 9.4 | 0.4 | 7.9 | 0.3 | 17.3 | 1.5 | 16.5 | 1.4 |
| One or more ADL limitations | 29.4 | 0.7 | 26.5 | 0.6 | 47.5 | 2.1 | 44.0 | 1.6 |
| One or more ADL or IADL limitations | 45.4 | 0.7 | 40.3 | 0.7 | 65.6 | 2.1 | 70.3 | 1.7 |
| Claims-Based Flag | ||||||||
| CDPS | 50.3 | 0.5 | 49.1 | 0.6 | 66.3 | 1.8 | 56.3 | 1.3 |
| ARCS | 72.8 | 0.5 | 73.2 | 0.6 | 81.1 | 1.4 | 70.5 | 1.5 |
| SSA-HIT | 26.5 | 0.5 | 26.9 | 0.6 | 40.2 | 1.8 | 24.7 | 1.1 |
| Psychiatric disorder | 18.0 | 0.4 | 14.5 | 0.4 | 22.2 | 1.7 | 35.1 | 1.4 |
| Dementia/Alzheimer's | 3.1 | 0.2 | 3.6 | 0.2 | 4.5 | 0.6 | 0.6 | 0.2 |
| Intellectual disability | 0.4 | 0.1 | 0.1 | 0.0 | 0.2 | 0.1 | 2.1 | 0.3 |
| Number of Observations | ||||||||
| Unweighted | 12,415 | 10,957 | 840 | 2,357 | ||||
| Weighted (millions) | 35.3 | 29.3 | 2.2 | 6.0 | ||||
In Table 2, we show the percentages of Medicare beneficiaries classified as having a disability by each of the claims-based disability indicators, separately for those who reported having a limitation in at least one ADL and those who did not. In each age group, the percentage of beneficiaries classified as having a disability by each claims-based disability indicator is higher for those who self-report a limitation in at least one ADL than for those who do not. The difference is not statistically significant for the indicator for intellectual disability, however. In the subgroup who first qualified for Medicare before age 65 due to disability, the differences between those who self-report a limitation in at least one ADL and those who do not are statistically significant for the CDPS, ARCS, and Dementia/Alzheimer's indicators.
| All | Age 65 or Older | Age 18-64 | ||||||
| All | Medicare Before Age 65 | |||||||
| 1+ ADL Limitation | No ADL Limitation | 1+ ADL Limitation | No ADL Limitation | 1+ ADL Limitation | No ADL Limitation | 1+ ADL Limitation | No ADL Limitation | |
NOTES: Based on analysis of the MCBS. The study population includes respondents who completed the community baseline questionnaire in 2003-2006 and either the community or facility questionnaire in their second MCBS year. Beneficiaries enrolled in Medicare Advantage in any month during their first and second MCBS calendar year are excluded.
| ||||||||
| Claims-Based Flag | ||||||||
| CDPS | 67.0a | 43.3 | 69.3a | 41.8 | 73.6a | 59.7 | 60.2a | 53.4 |
| ARCS | 82.8a | 68.6 | 85.2a | 68.9 | 87.4a | 75.3 | 75.6a | 66.5 |
| SSA-HIT | 35.3a | 22.9 | 37.7a | 23.0 | 43.2 | 37.4 | 28.2a | 21.9 |
| Psychiatric disorder | 26.3a | 14.6 | 23.0a | 11.5 | 25.0 | 19.7 | 36.1a | 34.2 |
| Dementia/ Alzheimer's | 6.7a | 1.6 | 8.6a | 1.8 | 6.9a | 2.3 | 1.0a | 0.2 |
| Intellectual disability | 0.8a | 0.3 | 0.2 | 0.0 | 0.2 | 0.2 | 2.4 | 2.0 |
| Number of Observations | ||||||||
| Unweighted | 3,899 | 8,515 | 2,953 | 7,104 | 394 | 446 | 946 | 1,411 |
| Weighted (millions) | 10.4 | 24.9 | 7.8 | 21.6 | 1.0 | 1.1 | 2.6 | 3.3 |
The percentages in Table 2 are also useful for the comparison of the performance of the predictive models to that of the individual claims-based indicators. For each claims-based indicator, the percentage among those who self-report disability that is flagged by that indicator is the indicator's true positive rate (or sensitivity) and the percentage among those who do not self-report disability that is flagged by that indicator is the indicator's false positive rate (or one minus specificity). For example, for Medicare beneficiaries age 65 or older, the CDPS indicator has sensitivity of 0.69 and one minus specificity of 0.42. Later, we plot this point, as well as points for the other claims-based flags, along with the ROC curve for our full model.
Logistic Model Estimates
In Table 3, we show the logistic regression results for the predictive models for the intermediate disability indicator--for Medicare beneficiaries age 65 or older and for those who are ages 18-64, respectively. For comparison, we also include results for a "reference model" that includes only sex and age as predictors. The reference model is useful in that it indicates the "minimum" predictive performance of our approach using only the most basic of demographic variables. In the analysis that follows, the ROC curve for the reference model will show the sensitivity-specificity trade-off under a model that predicts one or more ADLs with only minimal information in comparison to our full model that includes also the claims-based information.
| Variable | Age 65 or Older | Age 18-64 | ||
| Reference Model (odds ratio) | Full Model (odds ratio) | Reference Model (odds ratio) | Full Model (odds ratio) | |
NOTES:
| ||||
| Female | 1.32b | 1.31b | 1.11 | 1.09 |
| Age | 1.08b | 1.07b | 1.03b | 1.02b |
| Disability Flags | ||||
| CDPS | 2.12b | 1.04 | ||
| ARCS | 1.18b | 1.51b | ||
| SSA-HIT | 1.26b | 1.19 | ||
| Psychiatric disorder | 1.49b | 1.04 | ||
| Dementia and Alzheimer's | 2.47b | 4.62b | ||
| Intellectual disability | 4.83 | 1.52 | ||
| Dual-Eligiblea | 2.43b | 0.63b | ||
| Medicare Entitlement Before Age 65 | 4.17b | |||
| Interaction with Medicare Entitlement Before Age 65 | ||||
| CDPS | 0.66b | |||
| ARCS | 1.54 | |||
| SSA-HIT | 0.73 | |||
| Psychiatric disorder | 0.67 | |||
| Dementia and Alzheimer's | 0.74 | |||
| Intellectual disability | 0.16 | |||
| Dual-eligiblea | 0.55b | |||
| AUC ROC | 0.65 | 0.75 | 0.58 | 0.62 |
In the older age group, being female and of older age are both positively associated with self-reported disability (a limitation in at least one ADL), as are dual-eligibility and Medicare entitlement before age 65. Of the six claims-based disability indicators, only the indicator for intellectual disability is not a significant predictor of our intermediate disability indicator.10 The estimated odds ratios for many of the interaction terms are smaller than 1.00. This finding suggests that the claims-based indicators are more strongly associated with our intermediate disability indicator among those who aged into Medicare than those who entered Medicare before age 65 because of SSDI or ESRD. In the younger age group, being female is not significantly associated with our intermediate disability indicator, older age is positively associated with it, and dual-eligibility is negatively associated with it (as indicated by an odds ratio smaller than 1.00). Of the six claims-based disability indicators, only the indicators for ARCS and dementia/Alzheimer's are significant predictors of our intermediate disability indicator.
Receiver Operating Characteristic Curves and Predicted Probability Thresholds
In Figure 1 and Figure 2, we show the ROC curves corresponding to the full model results for the intermediate disability indicator (a limitation in at least one ADL) for Medicare beneficiaries who are age 65 or older and those who are ages 18-64, respectively. To assist the comparison of predictive performance, each figure also includes an ROC curve corresponding to the reference model that includes only sex and age as predictors. In addition, each figure includes four points corresponding to the sensitivity and specificity of the individual claims-based indicators for CDPS, ARCS, SSA-HIT, and psychiatric disorders.11
FIGURE 1. ROC Curve Versus Claims-Based Disability Flags, Intermediate Disability Measure, Age 65 or Older
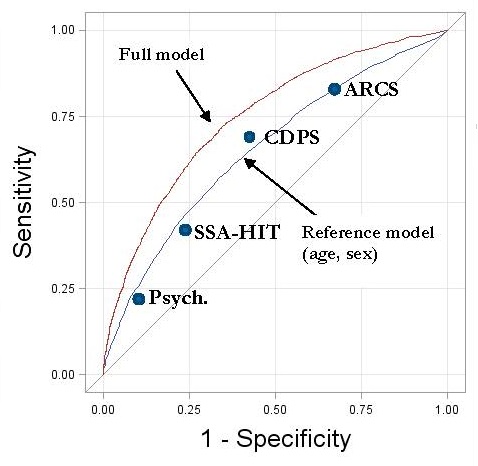
It is evident from Figure 1 that for Medicare beneficiaries who are age 65 or older, the full logistic model outperforms each of the individual claims-based indicators, allowing for both higher sensitivity and specificity in each case. The AUC is 0.75, and the point that maximizes the sum of sensitivity and specificity (not shown) corresponds to a predicted probability threshold of 0.24. Therefore, we classify Medicare beneficiaries age 65 or older as having disability (as defined by our intermediate disability measure) if their predicted value is greater than 0.24.
FIGURE 2. ROC Curve Versus Claims-Based Disability Flags, Intermediate Disability Measure, Age 18-64
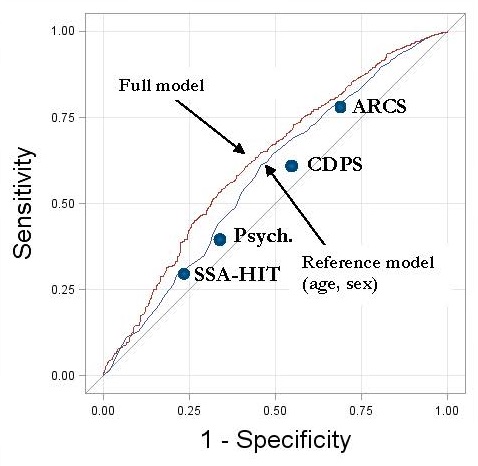
The full logistic model for Medicare beneficiaries ages 18-64 also outperforms each of the individual claims-based indicators. For this age group, none of the individual claims-based indicators perform as well as the reference model, which uses only age and sex as predictors; the points for the individual indicators are all below the ROC curve for the reference model (Figure 2). That is not remarkable for the Psychiatric and SSA-HIT indicators, as these indicators focus on identification of subpopulations with specific conditions, but it is remarkable for CDPS and ARCS, which are designed to capture broader groups. Although the full model outperforms the other options considered, its ROC curve is well below that for the older age group (AUC=0.62). The point that maximizes the sum of sensitivity and specificity (not shown) corresponds to a predicted probability threshold of 0.45. For purposes of predicting self-reported disability (based on the intermediate MCBS measure), we classify Medicare beneficiaries ages 18-64 as having disability if their predicted value is greater than 0.45.
Congruence Analysis
Age 65 or Older
At the point that maximizes the sum of sensitivity and specificity, our model prediction is congruent with self-reported disability for 5.6 million of the 7.8 million beneficiaries age 65 or older with a limitation in at least one ADL (sensitivity=0.72). The model prediction is also congruent with self-reported disability for 14.1 million of the 21.6 million without any ADL limitations (specificity=0.65). In Table 4, we summarize the demographic and health characteristics for Medicare beneficiaries who are age 65 or older, comparing those for which the model prediction is congruent with self-reported disability and those for which the model prediction is incongruent with self-reports, by self-reported disability status.
| Variable(percent unless otherwise noted) | 1+ ADL Limitation | No ADL Limitation | ||||||
| Congruent(true positive) | Incongruent(false negative) | Congruent(true positive) | Incongruent(false negative) | |||||
| Mean | SE | Mean | SE | Mean | SE | Mean | SE | |
* MCBS respondents are "true positive" if they have a limitation in at least one ADL and are predicted to have disability by the model, a "false negative" if they have a limitation in at least one ADL and are not predicted to have disability by the model, a "false positive" if they do not have a limitation in at least one ADL and are predicted to have disability by the model, and a "true negative" if they do not have a limitation in at least one ADL and are not predicted to have disability by the model.
| ||||||||
| Age at Medicare Enrollment | ||||||||
| Less than 65 | 17.9 | 0.9 | 1.6 | 0.5a | 0.6 | 0.1 | 14.3 | 0.6a,b |
| 65 or above | 82.1 | 0.9 | 98.4 | 0.5a | 99.4 | 0.1 | 85.7 | 0.6a,b |
| Age | ||||||||
| 65 to 74 | 24.3 | 1.1 | 68.5 | 1.7a,b | 73.9 | 0.5 | 28.0 | 1.0 b |
| 75 to 84 | 47.6 | 1.1 | 28.8 | 1.5a | 24.8 | 0.5 | 51.3 | 0.9a,b |
| 85 or above | 28.1 | 0.8 | 2.7 | 0.6a | 1.3 | 0.1 | 20.7 | 0.8a,b |
| Female | 65.9 | 1.0 | 53.9 | 2.0a | 48.5 | 0.8 | 62.4 | 1.0b |
| Dual-Eligible | 25.4 | 1.3 | 3.9 | 0.8a | 2.1 | 0.3 | 18.0 | 1.1a,b |
| Married | 39.2 | 0.9 | 62.5 | 1.8a | 67.1 | 0.8 | 45.9 | 1.0a,b |
| Working | 2.4 | 0.4 | 11.7 | 1.5a,b | 24.1 | 0.9 | 6.1 | 0.5a,b |
| Income Less than $25,000 | 69.9 | 1.2 | 48.0 | 1.9a,b | 37.6 | 1.0 | 61.1 | 1.3a,b |
| Race | ||||||||
| White | 83.6 | 1.2 | 90.2 | 1.3a | 90.0 | 0.8 | 86.3 | 1.1b |
| Black | 9.7 | 1.2 | 5.9 | 1.1 | 6.5 | 0.7 | 8.3 | 0.9 |
| Other | 4.2 | 0.7 | 2.1 | 0.7 | 2.8 | 0.3 | 3.2 | 0.4 |
| Hispanic | 2.2 | 0.4 | 1.7 | 0.5 | 0.7 | 0.2 | 2.1 | 0.3b |
| Highest Grade Completed | ||||||||
| Less than high school | 41.0 | 1.4 | 21.5 | 1.6a | 18.0 | 0.8 | 30.8 | 1.2a,b |
| High school/vocational | 32.8 | 1.0 | 39.1 | 1.9a | 38.5 | 1.0 | 38.3 | 1.2a,b |
| At least some college | 26.1 | 1.4 | 39.4 | 2.0a | 43.5 | 1.3 | 30.9 | 1.4 |
| Metro Area | 73.6 | 1.5 | 73.8 | 2.6 | 73.2 | 1.2 | 72.3 | 1.3 |
| Number of People in Household | ||||||||
| 1 | 36.4 | 1.0 | 23.7 | 1.6a | 22.9 | 0.8 | 39.3 | 1.1b |
| 2 | 44.6 | 1.1 | 60.3 | 2.2a | 64.1 | 0.9 | 48.7 | 1.0b |
| 3 | 10.2 | 0.7 | 8.8 | 1.2 | 9.3 | 0.5 | 7.6 | 0.6b |
| 4+ | 8.8 | 0.6 | 7.2 | 1.3b | 3.8 | 0.4 | 4.4 | 0.4b |
| Self-Reported Health | ||||||||
| Health status is good/very good/excellent | 51.9 | 1.3 | 69.2 | 1.9a,b | 93.0 | 0.4 | 80.1 | 0.8a,b |
| Health limits social activity | 38.0 | 1.2 | 17.5 | 1.7a,b | 2.7 | 0.3 | 8.8 | 0.5a,b |
| Obese | 27.2 | 1.0 | 39.0 | 2.0a,b | 20.7 | 0.7 | 19.8 | 1.0a,b |
| High blood pressure | 73.0 | 0.8 | 71.8 | 1.6b | 55.6 | 0.8 | 69.5 | 0.9a,b |
| Heart attack | 21.5 | 0.9 | 12.5 | 1.4a | 8.8 | 0.5 | 18.3 | 0.7a,b |
| Stroke | 22.8 | 0.9 | 12.5 | 1.4a,b | 5.6 | 0.4 | 12.9 | 0.7a,b |
| Nonskin cancer | 22.4 | 0.9 | 18.7 | 1.7 | 14.7 | 0.6 | 22.3 | 0.9b |
| Diabetes | 31.1 | 1.0 | 29.2 | 2.4b | 14.8 | 0.6 | 24.0 | 0.8a,b |
| Dementia/Alzheimer's | 11.4 | 0.8 | 1.5 | 0.4a | 0.7 | 0.1 | 4.0 | 0.4a,b |
| Emphysema/COPD | 23.8 | 1.0 | 17.9 | 1.7a,b | 10.7 | 0.6 | 15.8 | 0.6a,b |
| Medical Events (number of) | ||||||||
| Inpatient stays | 0.8 | 0.0 | 0.2 | 0.0a,b | 0.1 | 0.0 | 0.4 | 0.0a,b |
| Home health visits | 60.6 | 4.6 | 12.0 | 2.9a,b | 1.3 | 0.3 | 12.2 | 2.0a,b |
| Outpatient visits | 7.2 | 0.3 | 4.6 | 0.4a,b | 3.1 | 0.1 | 6.1 | 0.2a,b |
| Medical provider visits | 49.4 | 1.2 | 28.5 | 1.5a,b | 18.0 | 0.4 | 34.5 | 0.7a,b |
| Institutional events | 0.4 | 0.0 | 0.0 | 0.0a,b | 0.0 | 0.0 | 0.1 | 0.0a,b |
| Prescriptions | 51.0 | 1.2 | 35.0 | 1.4a,b | 22.7 | 0.4 | 40.0 | 0.8a,b |
| Medical Expenditures ($1,000s) | ||||||||
| Inpatient stays | 7.1 | 0.4 | 2.2 | 0.4a,b | 1.0 | 0.1 | 3.3 | 0.2a,b |
| Home health visits | 1.6 | 0.1 | 0.2 | 0.1a,b | 0.0 | 0.0 | 0.4 | 0.0a,b |
| Outpatient visits | 2.0 | 0.1 | 1.2 | 0.1a | 0.9 | 0.1 | 1.7 | 0.1b |
| Medical provider visits | 6.3 | 0.2 | 3.7 | 0.2a,b | 2.3 | 0.1 | 4.5 | 0.2 |
| Institutional events | 2.1 | 0.2 | 0.2 | 0.1a,b | 0.0 | 0.0 | 0.3 | 0.0 |
| Prescriptions | 3.2 | 0.1 | 2.4 | 0.1a,b | 1.6 | 0.0 | 2.7 | 0.1 |
| ADL Limitations | ||||||||
| Bathing/showering | 44.7 | 1.2 | 18.0 | 1.7a | ||||
| Dressing | 30.1 | 1.1 | 14.3 | 1.5a | ||||
| Eating | 11.3 | 0.8 | 4.6 | 0.9a | ||||
| Getting in/out of bed/chair | 46.3 | 1.3 | 38.6 | 2.2a | ||||
| Walking | 86.8 | 0.9 | 81.1 | 1.8a | ||||
| Using the toilet | 23.9 | 1.1 | 8.5 | 1.3a | ||||
| Claims-Based Flags | ||||||||
| CDPS | 83.7 | 0.7 | 32.0 | 2.0a,b | 21.7 | 0.8 | 79.7 | 0.7a,b |
| ARCS | 93.1 | 0.5 | 64.5 | 2.0a,b | 57.8 | 1.0 | 90.0 | 0.6a,b |
| SSA-HIT | 46.3 | 1.2 | 15.8 | 1.4a | 13.6 | 0.7 | 40.8 | 1.1a,b |
| Psychiatric disorder | 28.8 | 1.0 | 7.8 | 1.2a | 5.4 | 0.4 | 23.0 | 0.8a,b |
| Dementia/Alzheimer's | 11.9 | 0.7 | 0.2 | 0.2a | 0.1 | 0.1 | 4.9 | 0.4a,b |
| Intellectual disability | 0.3 | 0.1 | 0.0 | 0.0 | 0.0 | 0.0 | 0.1 | 0.0 |
| Number of Observations | ||||||||
| Unweighted | 2,289 | 664 | 4,189 | 2,915 | ||||
| Weighted (millions) | 5.6 | 2.2 | 14.1 | 7.5 | ||||
Those who do not self-report a disability but are classified as having a disability (false positives) are similar to those who self-report a disability and are also classified as having a disability (true positives) in many ways--not surprisingly, because of the method used to classify them and the fact that we classified those in both groups as "positive." The characteristics reported in the MCBS are not necessarily captured in the model's predictors, however, so it is also not surprising that we find some differences between the false and true positives. The false positives are in better health (according to their self-reports) than the true positives, and they have lower service use during the period examined. They are much less likely to report that their health limits social activity or that they are obese, have ever had a stroke, or currently have dementia or Alzheimer's. Further, they have had significantly fewer home health visits, medical provider visits, and inpatient or other institutional stays, as well as fewer prescriptions filled. The false positives are also up to seven percentage points less likely than the true positives to be flagged by each of the individual claims-based disability indicators.
Similarly, the composition of those who self-report disability but are classified as not having a disability (false negatives) resembles those who do not self-report disability and are also classified as not having a disability (true negatives) in many respects. However, the false negatives report worse health than the true negatives and have higher service use, including more prescriptions filled. They are also up to ten percentage points more likely than the true negatives to be flagged by each of the individual claims-based disability indicators.
Compared with true positives, false negatives (who also reported a limitation in at least one ADL but were not classified as having a disability) are especially characterized by younger ages, higher education, higher obesity rate, and lower service use; they are also substantially less likely to report a limitation in each of the individual ADLs.
Ages 18-64
Using the cutoff point that maximizes the sum of sensitivity and specificity, our model congruently classifies 1.4 million of the 2.6 million beneficiaries ages 18-64 with at least one ADL limitation (sensitivity=0.54). The model also congruently classifies 2.2 million of the 3.3 million without any ADL limitations (specificity=0.67). In Table 5, we provide a summary of the demographic and health characteristics for Medicare beneficiaries ages 18-64, comparing between those for which the model prediction is congruent with self-reported disability and those for which the model prediction is incongruent with self-reports, by self-reported disability status.
As with the older age group, false positives resemble true positives in many ways, but the false positives report better health and lower service use. Unlike the older age group, however, they are quite similar to the true positives in the percentages flagged by each of the individual claims-based disability indicators.
Also as with the older age group, the false negatives are similar to the true negatives in many ways, but the false negatives report worse health and have higher service use. They are also quite similar to the true negatives in the percentages flagged by each of the individual claims-based indicators.
| Variable(percent unless otherwise noted) | 1+ ADL Limitation | No ADL Limitation | ||||||
| Congruent(true positive) | Incongruent(false negative) | Congruent(true positive) | Incongruent(false negative) | |||||
| Mean | SE | Mean | SE | Mean | SE | Mean | SE | |
* MCBS respondents are "true positive" if they have a limitation in at least one ADL and are predicted to have disability by the model, a "false negative" if they have a limitation in at least one ADL and are not predicted to have disability by the model, a "false positive" if they do not have a limitation in at least one ADL and are predicted to have disability by the model, and a "true negative" if they do not have a limitation in at least one ADL and are not predicted to have disability by the model.
| ||||||||
| Age | ||||||||
| Less than 50 | 13.1 | 1.6 | 54.7 | 3.0a | 59.5 | 2.1 | 20.1 | 2.7b |
| 50 to 64 | 86.9 | 1.6 | 45.3 | 3.0a | 40.5 | 2.1 | 79.9 | 2.7b |
| Female | 55.4 | 3.3 | 44.5 | 2.6 | 41.2 | 2.1 | 58.9 | 3.5b |
| Dual-Eligible | 14.2 | 2.1 | 57.5 | 3.0a | 62.5 | 2.2 | 13.7 | 2.3b |
| Married | 52.2 | 3.1 | 37.4 | 3.1a | 28.5 | 2.0 | 45.5 | 3.2b |
| Working | 7.5 | 1.7 | 7.3 | 1.2b | 17.1 | 1.6 | 8.5 | 1.8b |
| Income Less than $25,000 | 67.3 | 3.0 | 79.2 | 3.1a | 84.8 | 1.7 | 68.9 | 3.1b |
| Race | ||||||||
| White | 79.9 | 2.2 | 72.7 | 3.5 | 73.5 | 2.4 | 72.8 | 3.7 |
| Black | 13.7 | 2.0 | 18.2 | 3.9 | 18.2 | 2.4 | 23.1 | 3.4 |
| Other | 3.2 | 1.1 | 4.6 | 1.3 | 4.0 | 1.0 | 2.9 | 1.3 |
| Hispanic | 2.7 | 1.1 | 4.4 | 1.0 | 4.2 | 0.7 | 1.2 | 0.5b |
| Highest Grade Completed | ||||||||
| Less than high school | 27.1 | 2.7 | 30.9 | 2.4 | 28.4 | 2.2 | 28.0 | 3.0 |
| High school/vocational | 39.4 | 3.0 | 38.1 | 2.2 | 44.1 | 2.2 | 37.3 | 3.8 |
| At least some college | 33.6 | 3.1 | 31.0 | 2.4 | 27.5 | 2.0 | 34.7 | 3.4 |
| Metro Area | 62.7 | 4.0 | 74.4 | 2.9 | 71.5 | 2.6 | 67.7 | 3.5 |
| Number of People in Household | ||||||||
| 1 | 23.7 | 2.9 | 25.7 | 2.5 | 26.1 | 2.1 | 27.8 | 3.1 |
| 2 | 42.3 | 3.0 | 32.9 | 2.6 | 32.0 | 1.7 | 42.7 | 2.9b |
| 3 | 21.9 | 2.9 | 21.8 | 2.3 | 22.2 | 1.5 | 13.2 | 2.1b |
| 4+ | 12.1 | 1.9 | 19.6 | 2.0a | 19.6 | 1.5 | 16.3 | 2.8 |
| Self-Reported Health | ||||||||
| Health status is good/very good/excellent | 23.5 | 2.7 | 25.2 | 2.3b | 55.0 | 2.1 | 47.8 | 3.6 a |
| Health limits social activity | 45.6 | 3.4 | 47.7 | 3.0b | 18.6 | 2.1 | 23.6 | 3.3a |
| Obese | 50.6 | 3.6 | 46.2 | 2.8b | 35.0 | 2.1 | 42.1 | 4.0 |
| High blood pressure | 67.7 | 2.6 | 51.2 | 2.2a,b | 41.0 | 2.2 | 62.8 | 3.3b |
| Heart attack | 19.2 | 2.7 | 9.1 | 1.5a | 5.2 | 0.9 | 18.8 | 2.9b |
| Stroke | 21.5 | 2.3 | 10.5 | 1.4a | 9.2 | 1.5 | 15.1 | 2.6 |
| Nonskin cancer | 14.0 | 2.5 | 11.3 | 2.0 | 9.1 | 1.4 | 13.6 | 2.4 |
| Diabetes | 37.1 | 2.9 | 22.1 | 2.9a | 16.7 | 1.8 | 28.4 | 3.0b |
| Dementia/Alzheimer's | 5.0 | 1.5 | 2.0 | 0.7 | 1.3 | 0.3 | 0.9 | 0.5a |
| Emphysema/COPD | 30.6 | 3.2 | 27.5 | 3.2 | 22.1 | 1.9 | 20.2 | 2.8 |
| Medical Events (number of) | ||||||||
| Inpatient stays | 0.6 | 0.1 | 0.4 | 0.0 | 0.3 | 0.1 | 0.5 | 0.1 |
| Home health visits | 35.0 | 9.0 | 30.7 | 5.3b | 7.1 | 1.4 | 8.8 | 2.9a |
| Outpatient visits | 9.3 | 0.9 | 7.0 | 0.7 | 5.6 | 0.4 | 6.8 | 0.7 |
| Medical provider visits | 44.4 | 3.1 | 27.6 | 1.9a,b | 20.2 | 1.6 | 31.9 | 2.5a,b |
| Institutional events | 0.1 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| Prescriptions | 64.7 | 3.0 | 55.0 | 3.4b | 40.1 | 2.6 | 49.0 | 2.7a |
| Medical Expenditures ($1,000s) | ||||||||
| Inpatient stays | 6.1 | 1.0 | 4.1 | 0.7 | 2.5 | 0.4 | 3.8 | 0.7 |
| Home health visits | 0.7 | 0.2 | 0.3 | 0.1b | 0.1 | 0.0 | 0.2 | 0.1 |
| Outpatient visits | 3.4 | 0.6 | 1.8 | 0.3 | 1.7 | 0.3 | 3.4 | 1.4 |
| Medical provider visits | 5.6 | 0.4 | 3.4 | 0.3a,b | 2.1 | 0.2 | 7.9 | 3.7 |
| Institutional events | 0.4 | 0.1 | 0.1 | 0.0 | 0.1 | 0.0 | 0.1 | 0.1 |
| Prescriptions | 4.4 | 0.2 | 4.8 | 0.4b | 3.5 | 0.2 | 11.4 | 7.6 |
| ADL Limitations | ||||||||
| Bathing/showering | 38.5 | 3.1 | 33.4 | 2.4 | ||||
| Dressing | 32.9 | 3.5 | 29.0 | 2.7 | ||||
| Eating | 10.8 | 1.7 | 11.7 | 1.7 | ||||
| Getting in/out of bed/chair | 56.2 | 3.2 | 51.8 | 2.9 | ||||
| Walking | 90.1 | 1.9 | 87.0 | 1.5 | ||||
| Using the toilet | 23.5 | 2.8 | 16.9 | 2.2 | ||||
| Claims-Based Flags | ||||||||
| CDPS | 73.5 | 2.5 | 44.4 | 2.7a | 43.1 | 1.9 | 72.9 | 3.0b |
| ARCS | 94.0 | 1.5 | 54.0 | 3.2a | 50.7 | 2.2 | 96.5 | 1.1b |
| SSA-HIT | 39.6 | 2.5 | 14.7 | 1.9a | 14.8 | 1.4 | 35.4 | 3.3b |
| Psychiatric disorder | 41.8 | 3.2 | 29.4 | 2.2a | 32.4 | 1.8 | 37.7 | 2.9 |
| Dementia/Alzheimer's | 1.9 | 0.9 | 0.0 | 0.0 | 0.0 | 0.0 | 0.5 | 0.4 |
| Intellectual disability | 2.6 | 0.7 | 2.1 | 0.5 | 1.4 | 0.3 | 3.0 | 0.8 |
| Number of Observations | ||||||||
| Unweighted | 381 | 565 | 1,105 | 306 | ||||
| Weighted (millions) | 1.4 | 1.2 | 2.2 | 1.1 | ||||
Compared with true positives, false negatives are especially characterized by younger ages, dual-eligibility, residence in a metro area, fewer reported illnesses, and lower service use; they are quite similar to the true positives in the percentages reporting a limitation in each of the individual ADLs.
DISCUSSION
In this study, we sought to improve upon the ability of claims-based indicators to identify Medicare beneficiaries with self-reported disabilities by using multiple indicators along with age, sex and dual-eligibility variables in predictive models. The findings indicate that the predictive models outperform the individual indicators in that they offer an improved sensitivity-specificity trade-off. We also find that the sensitivity-specificity trade-off for the models is considerably better for those who are age 65 or older compared with those ages 18-64.
The relatively low congruence of the model's predictions for the younger age group might be due to the high percentage of dual-eligibles in that group, for whom we may be missing key service use because some services for this group are covered through Medicaid and not Medicare. Another possible explanation is related to errors in the self-reporting of ADL and IADL limitations in the MCBS--the disability measures the claims-based models are designed to predict. Measurement error might account for a larger share of variation in the disability indicators for the under-65 population than for the 65-or-older population, because true variation in disability is likely higher in the latter group. SSA has determined that all those under age 65 have had a significant and long-lasting work disability at some point, whereas a substantial share of those age 65 or older have no disability of any sort. If so, the relatively poor performance for the under-65 population might arise because the claims information is a much stronger predictor of true disability than it is of measurement error.12
In many ways, beneficiaries in both age groups who do not self-report disability but are classified as having a disability by the model (false positives) are similar to those who self-report disability and are also classified as having a disability (true positives), but they report being in better health and they have lower service use, including fewer prescriptions filled. Similarly, those who selfreport disability but are classified as not having a disability (false negatives) resemble those who do not self-report disability and are also classified as not having a disability (true negatives), but they report being in worse health and have higher service use, including more prescriptions filled. These findings suggest that data on such service use as home health care and skilled nursing facilities as well as the number of prescriptions filled may further help differentiate between those with and without disabilities.
Beneficiaries who are age 65 or older and who self-report disability but are classified as not having a disability are characterized by high obesity rates. Use of obesity-related information from claims data might therefore improve the identification of those with disability in this age group--at least as disability is defined in this study. A large share of beneficiaries ages 18-64 who self-report disability but are classified by the model as not having a disability are eligibile for Medicaid as well as Medicare, which suggests that information on use of long-term support services, captured in Medicaid data, might also improve prediction.
Our analysis focused on limitations in ADLs and IADLs, but disability is a broad term that encompasses many dimensions and varies in severity. Researchers interested in disability populations different from that examined in this study could use the same methodology and data to develop a model for their population of interest. Survey-based disability definitions that rely on MCBS data are necessarily restricted by the questions included in the MCBS, which are not sufficient for researchers interested in some more specific definitions--especially those pertaining to mental impairments and participation restrictions. However, this study did not exhaust all of the disability-related questions included in the MCBS, and other disability populations can be defined. Predictive models can also be tailored to various other subgroups of Medicare beneficiaries. Other matches of administrative and survey data may also facilitate targeting of additional populations (for example, National Center for Health Statistics data linked to Medicare and Medicaid claims files).
Even within the context of MCBS analysis, however, several options might increase the congruence of claims-based predictions with self-reported disability indicators. The Medicare claims included in the MCBS exclude services not covered by Medicare--most notably those covered by Medicaid, many of which are relevant to individuals with disability. Adding data from Medicaid claims for the dually-eligible MCBS respondents would likely improve congruence. Using a larger set of claims-based indicators, with separate indicators for different categories from the CDPS and SSA-HIT rules, could also result in improved congruence. Other claims-based algorithms, even if not specifically designed to identify people with disability, might also improve performance. Relevant examples include the Centers for Medicare and Medicaid Services (CMS) Hierarchical Condition Category risk adjuster (Pope et al. 2004) and the chronic conditions included in CMS's Chronic Conditions Warehouse (Chronic Conditions Data Warehouse 2013).
One practical application of using the approach presented here is in identifying frail Medicare beneficiaries who are age 65 or older and more likely than others to benefit from certain interventions. In the past, several interventions have been deemed too costly because many who received the services did not actually need them. For example, the Medicare Coordinated Care Demonstration evaluation (Brown et al. 2012) found that while only one of the 11 demonstration sites that operated for six years significantly reduced hospitalizations overall, four of the programs significantly reduced hospitalizations for a subset of high-needs patients. For the program with significant effects, effects were due almost entirely to the large effects on the high risk subgroup. Other programs noted that one reason they felt they were unsuccessful in reducing hospitalizations was the inability to focus resources on only the subset of high risk enrollees. Improved targeting of the relevant population would improve the cost-effectiveness of the intervention because a larger proportion of those who need the services will be included.
Our approach could also be used to identify meaningful groups for subgroup analysis when a large-scale intervention is implemented among the Medicare population more generally (for example, care transition interventions to reduce readmission to hospitals). Other practical applications include identifying a sample of people with disability for a survey that focuses on disability among Medicare beneficiaries, or for preventive care outreach initiatives focused on those with disability. Those implementing such efforts may use the MCBS to define "disability" in the manner most appropriate for the application, and tailor the model to the prediction of individuals in that disability population.
REFERENCES
Bamber, Donald. 1975. "The Area Abovethe Ordinal Dominance Graph and the Area Below the Receiver Operating Characteristic Graph." Journal of Mathematical Psychology 12(4): 387-415.
Bogardus, Sidney T., Virginia Towle, Christianna S. Williams, Mayur M. Desai, and Sharon Inouye. 2001. "What Does the Medical Record Reveal about Functional Status?" Journal of General Internal Medicine 16(11): 728-736.
Brown, Randall S., Deborah Peikes, Greg Peterson, Jennifer Schore, and Carol M. Razafindrakoto. 2012. "Six Features of Medicare Coordinated Care Demonstration Programs that Cut Hospital Admissions of High-Risk Patients." Health Affairs 31(6): 1156-1166.
Chronic Condition Data Warehouse. Available at http://www.ccwdata.org/chronic-conditions/index.htm, accessed March 29, 2013.
Iezzoni, Lisa I. 2002. "Using Administrative Data To Study Persons with Disabilities." Milbank Quarterly 80(2): 347-379.
Iezzoni, Lisa I. 2013. "Imperatives for HSR Addressing: Individuals with Disabilities--The Canaries in Health Care's Coal Mine." Medical Care 51(2): 133-136.
Irvin, Carol V., and Christopher Johnson. 2006. Medicaid Populations with Chronic and Disabling Conditions: A Compilation of Data on Their Characteristics, Health Conditions, Service Use, and Medicaid Payments. Washington, DC: Mathematica Policy Research, Inc.
Jette, Alan M. 2009. "Toward a Common Language of Disablement." Journals of Gerontology Series A: Biological Sciences and Medical Sciences 64(11): 1165-1168.
Katz, Sidney, Amasa B. Ford, Roland W. Moskowitz, Beverly A. Jackson, and Marjorie W. Jaffe. 1963. "Studies of Illness in the Aged." JAMA 185 (12): 914-919.
Kronick, Richard, Todd Gilmer, Tony Dreyfus, and Lora Lee. 2000. "Improving Health-Based Payment for Medicaid Beneficiaries: CDPS." Health Care Financing Review 21(3): 29-64.
Lasko, Thomas A., Jui G. Bhagwat, Kelly H. Zou, and Lucila Ohno-Machado. 2005. "The Use of Receiver Operating Characteristic Curves in Biomedical Informatics." Journal of Biomedical Informatics 38(5): 404-415.
Murgolo, Maggie. 2010. The Characteristics and Perceptions of the Medicare Population: Data from the 2010 Medicare Current Beneficiary Survey (Appendix A: Technical Documentation for the Medicare Current Beneficiary Survey) [Cited March 26, 2013]. Available from: http://www.cms.gov/Research-Statistics-Data-and-Systems/Research/MCBS/Downloads/2010_C_and_P.zip.
Palsbo, Susan E., Clifton D. Sutton, Margaret F. Mastal, Sidney Johnson, and Anne Cohen. 2008. "Identifying and Classifying People with Disabilities Using Claims Data: Further Development of the Access Risk Classification System (ARCS) Algorithm." Disability and Health Journal 1(4): 215-223.
Pavetti, LaDonna, Michelle Derr, Jacqueline Kauff, and Allison Barrett. 2010. "Mental Disorders and Service Use AmongWelfare and Disability Program Participants in Fee-for-Service Medicaid." Psychiatric Services 61(5): 495-499.
Pope, Gregory C., John Kautter, Randall P. Ellis, Arlene S. Ash, John Z. Ayanian, Melvin J. Ingber, Jesse M. Levy, and John Robst. 2004. "Risk Adjustment of Medicare Capitation Payments Using the CMS-HCC Model." Health Care Financing Review 25(4): 119-141.
Social Security Administration. 2012. Social Security and Health IT. SSA Publication No. 02-007.
Sternberg, Shelley A., Netta Bentur, Chad Abrams, Tal Spalter, Tomas Karpati, John Lemberger, and Anthony D. Heymann. 2012. "Identifying Frail Older People Using Predictive Modeling." American Journal of Managed Care 18(10): e392-7.
Youden, W. J. 1950. "Index for Rating Diagnostic Tests." Cancer 3(1): 32-35.
APPENDIX A. ADDITIONAL TABLES
| TABLE A.1. SSA-HIT Business Rules Included in the SSA-HIT Claims-Based Indicator | |
| General Listings | Transplantsa |
| Acute rheumatic feverAmputation of both handsAmyotrophic lateral sclerosis (ALS)Aneurysm of aorta or major branchesAplastic anemiasBlindnessBurnsCerebral palsyCerebrovascular accidentComaCoronary artery bypass grafting (CABG)Creutzfeldt-Jakob disease (CJD)Cri Du Chat syndromeEdwards' syndrome (Trisomy-18)End stage renal disease (ESRD)Fredreich's ataxia (FRDA)Intellectual disabilityMyocardial infarctionNonmosaic down syndrome (Trisomy 21)Osteogenesis imperfecta (OI)Patau syndrome (Trisomy 13)Persistent vegetative stateSchizophreniaSpinal cord injuriesSpinal muscular atrophy (SMA)Tetraplegia, quadriplegia, paraplegia, diplegia Traumatic brain injury | LungHeartLiverKidneyBone marrow or stem cell |
| Cancerb | |
| Soft tissue tumors of the head and neckCancer of the skin Cancer of the soft tissueLymphoma (Hodgkin's and NonHodgkin's)Acute leukemiaChronic myelogenous leukemiaMultiple myelomaCancer of the salivary glandsCancer of the breastCancer of the skeletal systemCancer of the maxilla, orbit, or temporal fossaCancer of the lungCancer of the mediastinumCancer of the esophagusCancer of the stomachCancer of the small intestineCancer of the colonCancer of the liver, gallbladder or bile ductsCancer of the pancreasCancer of the kidney, adrenal glands, and ureters Cancer of the urinary bladderCancer of the female genital tractCancer of the prostate glandCancer of the penis | |
| |
| Variable | Age 65 or Older | Age 18-64 | ||
| Reference Model (odds ratio) | Full Model (odds ratio) | Reference Model (odds ratio) | Full Model (odds ratio) | |
| ||||
| Female | 1.39b | 1.35b | 1.04 | 1.01 |
| Age | 1.09b | 1.09b | 1.02b | 1.01b |
| Disability Flags | ||||
| CDPS | 2.44b | 1.11 | ||
| ARCS | 1.22 | 1.41b | ||
| SSA-HIT | 1.54b | 1.25 | ||
| Psychiatric disorder | 1.98b | 1.20 | ||
| Dementia and Alzheimer's | 4.14b | 5.03b | ||
| Intellectual disability | 24.8b | 2.41b | ||
| Dual-Eligiblea | 2.86b | 0.57b | ||
| Medicare entitlement before age 65 | 5.33b | |||
| Interaction with Medicare Entitlement Before Age 65 | ||||
| CDPS | 0.58 | |||
| ARCS | 2.17 | |||
| SSA-HIT | 0.43b | |||
| Psychiatric disorder | 0.51b | |||
| Dementia and Alzheimer's | 0.81 | |||
| Intellectual disability | 0.00 | |||
| Dual-eligiblea | 0.55b | |||
| AUC ROC | 0.70 | 0.82 | 0.55 | 0.62 |
| Variable | Age 65 or Older | Age 18-64 | ||
| Reference Model (odds ratio) | Full Model (odds ratio) | Reference Model (odds ratio) | Full Model (odds ratio) | |
| ||||
| Female | 1.60b | 1.65b | 1.54b | 1.50b |
| Age | 1.09b | 1.08b | 1.02b | 1.01b |
| Disability Flags | ||||
| CDPS | 2.06b | 1.07 | ||
| ARCS | 1.22b | 1.56b | ||
| SSA-HIT | 1.41b | 1.14 | ||
| Psychiatric disorder | 1.64b | 1.06 | ||
| Dementia and Alzheimer's | 3.16b | 2.72 | ||
| Intellectual disability | 5.76 | 3.68b | ||
| Dual-Eligiblea | 2.58b | 0.61b | ||
| Medicare Entitlement Before Age 65 | 5.11b | |||
| Interaction with Medicare Entitlement Before Age 65 | ||||
| CDPS | 0.80 | |||
| ARCS | 1.31 | |||
| SSA-HIT | 0.60b | |||
| Psychiatric disorder | 0.66 | |||
| Dementia and Alzheimer's | 0.58 | |||
| Intellectual disabilityb | N/A | |||
| Dual-eligiblea | 0.57b | |||
| Area Under ROC Curve | 0.67 | 0.76 | 0.57 | 0.63 |
| Variable | Age 65 or Older | Age 18-64 | ||
| Reference Model (odds ratio) | Full Model (odds ratio) | Reference Model (odds ratio) | Full Model (odds ratio) | |
| ||||
| Female | 1.52c | 1.50c | 0.97 | 0.98 |
| Age | 1.08c | 1.08c | 1.03c | 1.02c |
| Disability Flags | ||||
| CDPS | 2.02c | 1.12 | ||
| ARCS | 1.32c | 1.38c | ||
| SSA-HIT | 1.28c | 1.19 | ||
| Psychiatric disorder | 1.36c | 0.96 | ||
| Dementia and Alzheimer's | 2.84c | 4.81c | ||
| Intellectual disability | 6.63 | 1.59 | ||
| Dual-Eligibleb | 2.67c | 0.50c | ||
| Medicare Entitlement Before Age 65 | 4.08c | |||
| Interaction with Medicare Entitlement Before Age 65 | ||||
| CDPS | 0.83 | |||
| ARCS | 1.58 | |||
| SSA-HIT | 0.67c | |||
| Psychiatric disorder | 0.52c | |||
| Dementia and Alzheimer's | 0.50 | |||
| Intellectual disability | 0.25 | |||
| Dual-eligibleb | 0.49c | |||
| AUC ROC | 0.66 | 0.76 | 0.57 | 0.62 |
| Variable | Age 65 or Older | Age 18-64 | ||
| Reference Model (odds ratio) | Full Model (odds ratio) | Reference Model (odds ratio) | Full Model (odds ratio) | |
| ||||
| Female | 1.38c | 1.31c | 1.14 | 1.12 |
| Age | 1.09c | 1.09c | 1.02c | 1.01c |
| Disability Flags | ||||
| CDPS | 2.39c | 1.43 | ||
| ARCS | 0.95 | 1.82c | ||
| SSA-HIT | 1.54c | 1.38 | ||
| Psychiatric disorder | 1.80c | 0.97 | ||
| Dementia and Alzheimer's | 5.01c | 3.22 | ||
| Intellectual disability | 36.9c | 3.64c | ||
| Dual-Eligibleb | 2.87c | 0.48c | ||
| Medicare Entitlement Before Age 65 | 2.86 | |||
| Interaction with Medicare Entitlement Before Age 65 | ||||
| CDPS | 0.67 | |||
| ARCS | 4.57c | |||
| SSA-HIT | 0.54c | |||
| Psychiatric disorder | 0.40c | |||
| Dementia and Alzheimer's | 0.63 | |||
| Intellectual disability | 0.00 | |||
| Dual-eligibleb | 0.45c | |||
| AUC ROC | 0.69 | 0.82 | 0.57 | 0.67 |
| Variable | Age 65 or Older | Age 18-64 | ||
| Reference Model (odds ratio) | Full Model (odds ratio) | Reference Model (odds ratio) | Full Model (odds ratio) | |
| ||||
| Female | 1.81c | 1.87c | 1.36c | 1.36c |
| Age | 1.08c | 1.09c | 1.01c | 1.01c |
| Disability Flags | ||||
| CDPS | 2.03c | 1.11 | ||
| ARCS | 1.39c | 1.27 | ||
| SSA-HIT | 1.33c | 1.23 | ||
| Psychiatric disorder | 1.44c | 0.98 | ||
| Dementia and Alzheimer's | 3.26c | 2.93 | ||
| Intellectual disability | 7.69 | 4.63c | ||
| Dual-Eligibleb | 2.92c | 0.67c | ||
| Medicare Entitlement Before Age 65 | 5.54c | |||
| Interaction with Medicare Entitlement Before Age 65 | ||||
| CDPS | 0.89 | |||
| ARCS | 1.26 | |||
| SSA-HIT | 0.54c | |||
| Psychiatric disorder | 0.69 | |||
| Dementia and Alzheimer's | 0.66 | |||
| Intellectual disability | N/A | |||
| Dual-eligibleb | 0.50c | |||
| AUC ROC | 0.68 | 0.77 | 0.56 | 0.61 |
NOTES
-
Using ROC curves, a methodology we discuss in further detail below, Sternberg et al. (2012) report an area under the curve (AUC) of 0.62.
-
Those who become eligible for Medicare via SSDI eligibility become eligible for Medicare only after 24 months of SSDI eligibility unless they also have amyotrophic lateral sclerosis (ALS), in which case Medicare eligibility is immediate.
-
We also use responses from both the second and third MCBS year to construct measures of "long-term" disability by requiring persistence (or death) from the second MCBS year to the third MCBS year. Results using the long-term measures are qualitatively similar to those we report here (see Appendix Table A.4, Table A.5 and Table A.6).
-
Irvin and Johnson (2006) included subcategories of "low cost" and above, while Pavetti et al. (2010) included subcategories of "medium cost" and above.
-
We do not include information on prescriptions in our ARCS indicator.
-
See Appendix Table A.1 for the list of impairments included in our implementation of the SSA-HIT business rules.
-
The following ICD-9 codes were included in addition to 295 (schizophrenia) and 296 (affective disorder): 297-301, 306-7, 309-10, and 314-315.
-
We use the 2012 ICD-9 terminology. Earlier ICD-9 versions included the term "mental retardation" instead of "intellectual disability."
-
We also experimented with alternative model specifications that included either a single claims-based indicator or a single flag indicating identification by 1-6 of the claims-based indicators. For both age groups, the full models described in the text are at least as accurate as these alternative specifications. Results from the alternative models are available upon request from the authors.
-
The estimated odds ratio for the claims-based indicator for intellectual disability is likely not statistically significant because of the very small number of MCBS respondents flagged by this indicator. Of the respondents included in the analytic sample, nine who were age 65 or older were flagged by the indicator and 96 who were age 18-64 were flagged by the indicator. About half of these respondents also reported a limitation in at least one ADL.
-
Not shown here are the indicators for intellectual disability and dementia/Alzheimer's, which pick up only a tiny fraction of each age group.
-
Consideration of an extreme hypothetical case illustrates this point. Suppose that all under-65 enrollees have at least one ADL, but that 56 percent of respondents fail to report any of their ADLs, leading to the 44 percent reporting at least one ADL (see Table 1). Under this scenario, we would be using the claims information only to predict which enrollees report or fail to report their ADL; presumably the predictive power of that information would be very low.
CENTER OF EXCELLENCE IN RESEARCH ON DISABILITY SERVICES AND CARE COORDINATION AND INTEGRATION (CERDS)
REPORTS AVAILABLE
Abstracted List of Tasks and Reports
HTML http://aspe.hhs.gov/daltcp/reports/2014/CERDS.shtml
PDF http://aspe.hhs.gov/daltcp/reports/2014/CERDS.pdf
--- --- --- --- ---
Association between NCQA Patient-Centered Medical Home Recognition for Primary Care Practices and Quality of Care for Children with Disabilities and Special Health Care Needs
HTML http://aspe.hhs.gov/daltcp/reports/2014/ChildDisV3.shtml
PDF http://aspe.hhs.gov/daltcp/reports/2014/ChildDisV3.pdf
Children with Disabilities and Special Health Care Needs in NCQA-Recognized Patient-Centered Medical Homes: Health Care Utilization, Provider Perspectives and Parental Expectations Executive Summary
HTML http://aspe.hhs.gov/daltcp/reports/2014/ChildDisES.shtml
PDF http://aspe.hhs.gov/daltcp/reports/2014/ChildDisES.pdf
Descriptive Study of Three Disability Competent Managed Care Plans for Medicaid Enrollees
Executive Summary http://aspe.hhs.gov/daltcp/reports/2014/3MCPlanses.shtml
HTML http://aspe.hhs.gov/daltcp/reports/2014/3MCPlans.shtml
PDF http://aspe.hhs.gov/daltcp/reports/2014/3MCPlans.pdf
Effect of PACE on Costs, Nursing Home Admissions, and Mortality: 2006-2011
Executive Summary http://aspe.hhs.gov/daltcp/reports/2014/PACEeffectes.shtml
HTML http://aspe.hhs.gov/daltcp/reports/2014/PACEeffect.shtml
PDF http://aspe.hhs.gov/daltcp/reports/2014/PACEeffect.pdf
Effectiveness of Alternative Ways of Implementing Care Management Components in Medicare D-SNPs: The Brand New Day Study
Executive Summary http://aspe.hhs.gov/daltcp/reports/2014/OrthoV2s.shtml
HTML http://aspe.hhs.gov/daltcp/reports/2014/OrthoV2.shtml
PDF http://aspe.hhs.gov/daltcp/reports/2014/OrthoV2.pdf
Effectiveness of Alternative Ways of Implementing Care Management Components in Medicare D-SNPs: The Care Wisconsin and Gateway Study
Executive Summary http://aspe.hhs.gov/daltcp/reports/2014/OrthoV1es.shtml
HTML http://aspe.hhs.gov/daltcp/reports/2014/OrthoV1.shtml
PDF http://aspe.hhs.gov/daltcp/reports/2014/OrthoV1.pdf
Evaluating PACE: A Review of the Literature
Executive Summary http://aspe.hhs.gov/daltcp/reports/2014/PACELitReves.shtml
HTML http://aspe.hhs.gov/daltcp/reports/2014/PACELitRev.shtml
PDF http://aspe.hhs.gov/daltcp/reports/2014/PACELitRev.pdf
Factors Predicting Transitions from Medicare-Only to Medicare-Medicaid Enrollee Status
HTML http://aspe.hhs.gov/daltcp/reports/2014/MMTransV2.shtml
PDF http://aspe.hhs.gov/daltcp/reports/2014/MMTransV2.shtml
Identifying Medicare Beneficiaries with Disabilities: Improving on Claims-Based Algorithms
Executive Summary http://aspe.hhs.gov/daltcp/reports/2014/algorithmes.shtml
HTML http://aspe.hhs.gov/daltcp/reports/2014/algorithm.shtml
PDF http://aspe.hhs.gov/daltcp/reports/2014/algorithm.pdf
Impacts of Waiting Periods for Home and Community-Based Services on Consumers and Medicaid Long-Term Care Costs in Iowa
HTML http://aspe.hhs.gov/daltcp/reports/2014/IAWaitPd.shtml
PDF http://aspe.hhs.gov/daltcp/reports/2014/IAWaitPd.pdf
Integrating Physical Health Care in Behavioral Health Agencies in Rural Pennsylvania
Executive Summary http://aspe.hhs.gov/daltcp/reports/2014/ruralPAes.shtml
HTML http://aspe.hhs.gov/daltcp/reports/2014/ruralPA.shtml
PDF http://aspe.hhs.gov/daltcp/reports/2014/ruralPA.pdf
Non-Elderly Disabled Category 2 Housing Choice Voucher Program: An Implementation and Impact Analysis
Executive Summary http://aspe.hhs.gov/daltcp/reports/2014/Cat2Housinges.shtml
HTML http://aspe.hhs.gov/daltcp/reports/2014/Cat2Housing.shtml
PDF http://aspe.hhs.gov/daltcp/reports/2014/Cat2Housing.pdf
Parent Perspectives on Care Received at Patient-Centered Medical Homes for Their Children with Special Health Care Needs
Executive Summary http://aspe.hhs.gov/daltcp/reports/2014/ChildDisV2es.shtml
HTML http://aspe.hhs.gov/daltcp/reports/2014/ChildDisV2.shtml
PDF http://aspe.hhs.gov/daltcp/reports/2014/ChildDisV2.pdf
Physician Perspectives on the Influence of Medical Home Recognition on Practice Transformation and Care Quality for Children with Special Health Care Needs
HTML http://aspe.hhs.gov/daltcp/reports/2014/ChildDisV1.shtml
PDF http://aspe.hhs.gov/daltcp/reports/2014/ChildDisV1.pdf
Strategies for Integrating and Coordinating Care for Behavioral Health Populations: Case Studies of Four States
Executive Summary http://aspe.hhs.gov/daltcp/reports/2014/4CaseStudes.shtml
HTML http://aspe.hhs.gov/daltcp/reports/2014/4CaseStud.shtml
PDF http://aspe.hhs.gov/daltcp/reports/2014/4CaseStud.pdf
Transitions from Medicare-Only to Medicare-Medicaid Enrollment
HTML http://aspe.hhs.gov/daltcp/reports/2014/MMTransV1.shtml
PDF http://aspe.hhs.gov/daltcp/reports/2014/MMTransV1.pdf
To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human ServicesOffice of Disability, Aging and Long-Term Care PolicyRoom 424E, H.H. Humphrey Building200 Independence Avenue, S.W.Washington, D.C. 20201FAX: 202-401-7733Email: webmaster.DALTCP@hhs.gov
RETURN TO:
Office of Disability, Aging and Long-Term Care Policy (DALTCP) Home [http://aspe.hhs.gov/office_specific/daltcp.cfm]Assistant Secretary for Planning and Evaluation (ASPE) Home [http://aspe.hhs.gov]U.S. Department of Health and Human Services (HHS) Home [http://www.hhs.gov]
Last Updated: 05/08/2014